-
Systems Pharmacology Approach to
Modelling Pharmacokinetics in
Pregnancy
Amin Rostami-Hodjegan, PharmD, PhD, FCP
Professor of Systems Pharmacology University of Manchester,
Manchester, UK
& Vice President R&D
Simcyp , Sheffield, UK
[email protected]
http://www.manchester.ac.uk/index.phphttp://www.simcyp.com/
-
PBPK/IVIVE Linked Models
Physiologically-Based Pharmacokinetics Joined with In Vitro-In
Vivo
Extrapolation of ADME: A Marriage under the Arch of Systems
Pharmacology
Amin Rostami-Hodjegan
July Issue of CPT – Online now
http://www.manchester.ac.uk/index.php
-
PricewaterhouseCoopers: Pharma 2020
.... proposes that new technologies will enable the adoption of
virtual R&D; and by
operating in a more connected world, the industry in
collaboration with researchers,
governments, healthcare payers and providers, can address the
changing needs of
society more effectively.
Kate Moss June 2008
(1) Requires More
Data not Less!
(2) Requires Different
Type of Data
(3) Requires Huge
Integration Task
(4) Appropriate Tools
Are Essential
http://www.manchester.ac.uk/index.php
-
Systems Approach: e.g. Inter-Individual Variability in PK
CYP3A4
CYP3A5
Americans/Europeans
Japanese/Chinese Age / Genetics / Environment / Disease
http://www.manchester.ac.uk/index.php
-
Blo
od
Lung
Rapidly perfused
organs
Slowly perfused
organs
Kidney
Liver
Intestines
Blo
od
Elimination
Dosing
ADME, PK, PD and
MOA
Metabolism
Active transport
Passive diffusion
Protein binding
Drug-drug interactions
Receptor binding
System component
(drug-independent)
PBPK Model
Predict, Learn, Confirm
Drug-dependent
component
A. Intrinsic/extrinsic Factors B. PBPK Model components
Huang and Temple, 2008
Individual or combined effects
on human physiology
Zhao P, et al Clin Pharmacol Ther 2011
EXTRINSIC
INTRINSIC
DDI
Environment
Medical Practice
Regulatory Alcohol
Smoking
Diet
Age
Race
Disease
Gender
Genetics
Pregnancy
Lactation
Organ Dysfunction
Well Recognised by Leading Regulatory Agencies
http://www.manchester.ac.uk/index.php
-
Summary of PBPK-IVIVE M&S in Submissions
(Zhao et al., 2011)
From July 2008 to June 2010, the FDA reviewed seven
investigational
new drug (IND) and six new drug applications (NDA)
submissions
containing PBPK modeling and simulations conducted by the
sponsors. In
addition, FDA reviewers conducted PBPK modeling and simulations
to
support clinical pharmacology reviews of another four NDA
submissions
for which the sponsors did not use PBPK. As a comparison, in the
3
years before 2008, FDA received only two submissions containing
PBPK
modeling and simulations. Many of the PBPK modeling and
simulation
evaluations addressed questions relating to drug–drug
interactions;
others addressed pediatric dosing, the impact of hepatic
impairment on
drug exposure, and the impact of multiple factors on drug
exposure
(Table 1).
0.66 per year 8.5 per year
http://www.manchester.ac.uk/index.php
-
ASCPT 2012
YES NO
http://www.manchester.ac.uk/index.php
-
Pregnancy as Another Example
Time –varying component to account for changes
to the system (anatomical, physiological and
biological; CYPs abundance, etc.)
Clinical Pharmacokinetics 2012
http://www.manchester.ac.uk/index.php
-
Homogenisation
HOMOGENATE
S9
Nuclear / Mitochondrial pellet
Centrifugation @
9,000g
Centrifugation @
100,000g
Cytosol
Microsomes
CYP450 FMO
Aldehyde oxidase MAO
Aldehyde dehydrogenase Epoxide hydrolase
Xanthine oxidase Esterases
UGT
HLM HIM HKM rhCYP rhUGT
hepatocytes
hepatocytes
S9
S9
cytosol
Aldehyde oxidase SULT
Glutathione S transferase Alcohol dehydrogenase
Xanthine oxidase
In Vitro Drug Metabolism Tools
http://www.manchester.ac.uk/index.php
-
SIMCYP Pregnancy PBPK Model
http://www.manchester.ac.uk/index.php
-
Foetal volume (ml) = 0.01 · exp [(0.955 / 0.0702) · (1- exp (-
0.0702· GA))]
Placenta volume (ml) = - 0.716 GA + 0.9149 GA2 - 0.0122 GA 3
Amniotic Fluid (ml) = 1.9648 GA -1.2056 GA2 + 0.2064 GA3 -
0.0061 GA4+0.00005 GA5
GA= gestational age
(week)
Gestational Time- Dependent Parameter Description
http://www.manchester.ac.uk/index.php
-
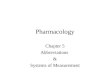
0
1
2
3
4
5
6
7
0 5 10 15 20 25
Pla
sm
a c
on
ce
ntr
ati
on
(m
g/L
)
Time (h)
Non-pregnant women
Predictions
Brazier 1983 (n=4)
0
1
2
3
4
5
6
7
0 5 10 15 20 25
Pla
sm
a c
on
ce
ntr
ati
on
(m
g/L
)
Time (h)
Pregnant women
Predictions
Brazier 1983 (n=8)
PK Parameter
Pregnant women Non-pregnant women Fold change in Pregnancy
Observed Simulated Ratio Observed Simulated Ratio Observe
d
Simulate
d Ratio
Cmax (mg/l) 4.58 (1.2) 3.26 0.71 6.02 (1.8) 3.59 0.60 ↓0.76
↓0.91 1.19
Tmax (h) 1.5 1.5 1.00 0.75a 0.97 1.29 ↑2.00 ↑1.55 0.77
AUC24h
(mg/l/h) 52 47 0.91 26 24 0.92 ↑2.00 ↑1.96 0.98
Simulated versus mean observed (Brazier et al 1983) PK
parameters for 150 mg caffeine
Results
http://www.manchester.ac.uk/index.php
-
CYP2D6 activity was detectable and concordant with genotype by 2
weeks of
age, showed no relationship with gestational age, and did not
change with post
natal age up to 1 year.
Scratching Surface
Clin Pharmacol Ther 2007
However: we know that:
Thus, the development of renal
function from birth may change in
parallel with the development of the
enzyme such that the
drug/metabolite ratio may be
relatively constant !!!!
http://www.manchester.ac.uk/index.php
-
Clin Pharmacol Ther 2008
Figure 1. Changes in CYP2D6 (a) and CYP3A4 (b) activity relative
to adult values.
The data of Blake et al, corrected for the development of renal
function, are
indicated by the diamonds. The simulated change in in the
activity of each enzyme
(solid line) was derived from in vitro data on hepatic enzyme
expression and
increase in liver weight with age.
0
0.2
0.4
0.6
0.8
1
0 4 8 12Age (Months)
CY
P2
D6
ac
tiv
ity
(D
M/D
X
rati
o r
ela
tiv
e t
o a
du
lt
0
0.2
0.4
0.6
0.8
1
0 4 8 12Age (Months)
CY
P3
A4
ac
tiv
ity
(D
X/3
HM
rati
o)
rela
tiv
e t
o a
du
lt
(A) (B)
Looking Deeper
http://www.manchester.ac.uk/index.php
-
Assessment of CYP1A2 Activity
http://www.manchester.ac.uk/index.php
-
Du
od
en
um
Je
jun
um
I
Jeju
nu
m I
I
Ileu
m I
Ileu
m I
I
Ileu
m I
II
Ile
um
IV
Co
lon
Segregated Blood Flows
Stomach
Emptying
Luminal
Transit
Systems Approach: Absorption
Enzymes (CYP3A4)
vs
Transporters (Pgp)
http://www.manchester.ac.uk/index.php
-
Qbulk QCsink
QSsink
QS
in
QS
ou
t
Qbrain Qbrain Brain blood
Brain mass
Cranial CSF
Spinal CSF
• Passive permeability at three interfaces
• Active transporters at BBB/BCSFB
CL
Bin
CL
Bo
ut
CL
Cin
CL
Co
ut
PSE
PS
B
PS
C
• CSF: circulation, pH, volume, …
• Brain: anatomy, physiology, …
Volume
pH
Volume
pH
Volume
pH
Volume
pH
CLmet
(Eyal et al., 2009)
Systems Approach: Brain
http://www.manchester.ac.uk/index.php
-
Kidney Permeability-Limited Model
Transporters are available in all
three proximal tubule cell
compartments on the apical and
basal membrane.
The model can handle:
• regional distribution/activity of
transporters
• nephrotoxicity as well as
changes in systemic exposure
• interplay between uptake, efflux
and passive permeation
• metabolism and transport
interplay
Filtration
Secretion (passive + active)
Reabsorption (passive + active) Urinal tubule Cell (renal mass)
Renal blood
http://www.manchester.ac.uk/index.php
-
FDA / U Washington in Seattle /Simcyp
Midazolam, Nifedipine, Indinavir Pharmacometric & Systems
Pharmacology (to appear soon)
http://www.manchester.ac.uk/index.php
-
Final Word: Model-Based Drug Development
(1) All Models Are Wrong, but Some Models Are Useful !
George EP Box 1987
WE ALL KNOW that:
WE SHOULD ALSO KNOW that:
(2) Science is built of facts as a house is built of stones; but
an accumulation of facts is no more science than a pile of stones
is a house.
Henri Poincare, 1902
http://www.manchester.ac.uk/index.php