Embed Size (px)
Citation preview

Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/305718630
SystematicClinicalReasoninginPhysicalTherapy(SCRIPT):AToolforthePurposefulPracticeofClinicalReasoningin...
ArticleinPhysicalTherapy·July2016
DOI:10.2522/ptj.20150482
CITATIONS
0
READS
263
8authors,including:
EvanPetersen
UniversityoftheIncarnateWord
6PUBLICATIONS94CITATIONS
SEEPROFILE
AllcontentfollowingthispagewasuploadedbyEvanPetersenon29October2016.
Theuserhasrequestedenhancementofthedownloadedfile.

Systematic Clinical Reasoning inPhysical Therapy (SCRIPT): Tool forthe Purposeful Practice of ClinicalReasoning in Orthopedic ManualPhysical TherapySarah E. Baker, Elizabeth E. Painter, Brandon C. Morgan, Anna L. Kaus,Evan J. Petersen, Christopher S. Allen, Gail D. Deyle, Gail M. Jensen
Background and Purpose. Clinical reasoning is essential to physical therapist prac-tice. Solid clinical reasoning processes may lead to greater understanding of the patientcondition, early diagnostic hypothesis development, and well-tolerated examination and inter-vention strategies, as well as mitigate the risk of diagnostic error. However, the complex andoften subconscious nature of clinical reasoning can impede the development of this skill.Protracted tools have been published to help guide self-reflection on clinical reasoning butmight not be feasible in typical clinical settings.
Case Description. This case illustrates how the Systematic Clinical Reasoning in PhysicalTherapy (SCRIPT) tool can be used to guide the clinical reasoning process and prompt aphysical therapist to search the literature to answer a clinical question and facilitate formalmentorship sessions in postprofessional physical therapist training programs.
Outcomes. The SCRIPT tool enabled the mentee to generate appropriate hypotheses, planthe examination, query the literature to answer a clinical question, establish a physicaltherapist diagnosis, and design an effective treatment plan. The SCRIPT tool also facilitated thementee’s clinical reasoning and provided the mentor insight into the mentee’s clinical reason-ing. The reliability and validity of the SCRIPT tool have not been formally studied.
Discussion. Clinical mentorship is a cornerstone of postprofessional training programs andintended to develop advanced clinical reasoning skills. However, clinical reasoning is oftensubconscious and, therefore, a challenging skill to develop. The use of a tool such as theSCRIPT may facilitate developing clinical reasoning skills by providing a systematic approachto data gathering and making clinical judgments to bring clinical reasoning to the consciouslevel, facilitate self-reflection, and make a mentored physical therapist’s thought processesexplicit to his or her clinical mentor.
S.E. Baker, PT, DPT, DSc, Army-Baylor University Doctoral Fellow-ship in Orthopaedic Manual Phys-ical Therapy, Brooke ArmyMedical Center, Fort Sam Hous-ton, TX 78234 (USA). Address allcorrespondence to Dr Baker at:[email protected].
E.E. Painter, PT, DPT, DSc, Army-Baylor University Doctoral Fellow-ship in Orthopaedic ManualPhysical Therapy, Brooke ArmyMedical Center.
B.C. Morgan, PT, DPT, DSc, Army-Baylor University Doctoral Fellow-ship in Orthopaedic ManualPhysical Therapy, Brooke ArmyMedical Center.
A.L. Kaus, PT, DPT, Department ofRehabilitation Medicine, BrookeArmy Medical Center.
E.J. Petersen, PT, DPT, DSc, Army-Baylor University Doctoral Fellow-ship in Orthopaedic ManualPhysical Therapy, Brooke ArmyMedical Center.
C.S. Allen, PT, DSc, Army-BaylorUniversity Doctoral Fellowship inOrthopaedic Manual PhysicalTherapy, Brooke Army MedicalCenter.
Author information continues onnext page.
Case Report
Post a Rapid Response tothis article at:ptjournal.apta.org
January 2017 Volume 97 Number 1 Physical Therapy f 1

The mentoring process is critical tothe physical therapist professionand a requirement of residency
and fellowship education. Mentoring inadvanced clinical training extendsbeyond entry-level clinical supervisionby guiding and facilitating the mentoredphysical therapist’s continual learning inthe development of advanced practice.Clinical mentoring centers on patientmanagement, with an emphasis on devel-oping advanced clinical reasoning andreflective practice skills.1
Clinical reasoning is an ongoing decision-making process used throughout the epi-sode of care.2–6 Sound clinical reasoning,to include using a systematic patient-tailored approach to data gathering andforming early prioritized diagnostichypotheses,7 followed by a carefullyselected interactive patient history tak-ing and examination to test hypotheses,may reduce cognitive bias and lead to agreater understanding of the patient pre-sentation.7,8 This greater understandingreduces the risk of diagnostic error andoverly aggressive, poorly tolerated phys-ical therapy sessions.9,10 When clinicalreasoning generates diagnostic hypothe-ses requiring medical management,incorporating best-evidence screeningstrategies may facilitate timely andappropriate medical care.11
Clinical reasoning is more complex thanapplying an analytical, deductive pro-cess.2–6 Practitioners must engage in ana-lytical and inductive (narrative) thinkingthat helps uncover important contextualelements that contribute to uncertainty.3
Practitioners must systematically con-sider and prioritize variable and uncer-tain factors, such as understanding thepatient’s environment, beliefs, and val-ues, as part of the clinical reasoning pro-cess, ultimately leading to the ability tomake appropriate clinical judgments.The ability to probe deeper with appro-priate follow-up questions often stemsfrom a more complete understanding ofthe patient’s story.12,13 As such, clinicalreasoning is best developed withinthe context of a patient encounterand includes reflecting on previousencounters.14,15
Although substantial literature attests tothe diagnostic accuracy of physical ther-apists,16–19 the inherent complexity ofdifferential diagnosis requires careful,consistent clinical processes. Break-downs in clinical processes, such as fail-ure to document differential diagnoses,leads to increased incidence of diagnos-tic error.9 Clinical reasoning strategies toprevent diagnostic error should focus onsystematic data gathering, synthesis, anddocumentation.14 Formal training in clin-ical reasoning facilitates the mental agil-ity to appropriately consider and docu-ment alternative diagnostic hypothesesin physical therapist practice.15 Purpose-ful practice in reasoning strategies inboth didactic and clinical environmentsis key to developing expertise.15,20 Theseadvanced clinical skills, combined with awillingness to search the literature foranswers to diagnostic questions, mayassist appropriate screening and accuratedifferential diagnosis.11
Clinical reasoning is a challenging skill todevelop because it is a high-level andtypically subconscious cognitive pro-cess.14 Reasoning must be exercised con-sciously to facilitate self-reflection,change professional behaviors andthought processes, and improve diagnos-tic accuracy.3,14,21 Mentors must be pres-ent and fully engaged to understand theirmentees’ thinking as mentees gather andinterpret evidence to manage thepatient. In other words, mentors need away for their mentees to “show theirmath” to make the mentees’ thinkingexplicit. An important learning strategyfor making the mentee’s thinking moreexplicit is facilitating reflection.22,23
Reflection is part of a process of self-monitoring, called meta-cognition orthinking about your thinking.22,23 A toolthat provides a framework for the learnerto critically examine his or her thoughtprocesses may be an important teachingand learning instrument for facilitatingreflection.
The purpose of this case report is todescribe the application of a teachingtool developed by an orthopaedic man-ual physical therapy fellowship programtitled the Systematic Clinical Reasoningin Physical Therapy (SCRIPT). In thiscase, the SCRIPT served as a teaching
G.D. Deyle, PT, DPT, DSc, Army-Baylor Uni-versity Doctoral Fellowship in OrthopaedicManual Physical Therapy, Brooke Army Med-ical Center.
G.M. Jensen, PT, PhD, FAPTA, Department ofPhysical Therapy, School of Pharmacy andHealth Professions, and Center for HealthPolicy and Ethics, Creighton University,Omaha, Nebraska.
[Baker SE, Painter EE, Morgan BC, et al. Sys-tematic Clinical Reasoning in Physical Ther-apy (SCRIPT): tool for the purposeful prac-tice of clinical reasoning in orthopedicmanual physical therapy. Phys Ther.2017;97:xxx–xxx.]
© 2016 American Physical Therapy Association
Published Ahead of Print:July 28, 2016
Accepted: July 7, 2016Submitted: August 27, 2015
SCRIPT in Orthopedic Manual Physical Therapy
2 f Physical Therapy Volume 97 Number 1 January 2017

and learning tool for facilitating clinicalreasoning within the patient encounterand clinical case analysis in one physicaltherapy education program. This casereport describes: (1) the mentee’s man-agement and use of evidence in a patientcase and (2) the teaching and learningoccurring in the clinical reasoningprocess.
Case DescriptionTo our knowledge, the only clinical rea-soning tool published in the peer-reviewed literature is used in a pediatricresidency.24 Other clinical reasoningforms published in textbooks aredetailed, yet lengthy,21,25 potentially pos-ing challenges to utilizing the form dur-ing a typical patient encounter, and maybe more useful retrospectively.
In 1994, the Army-Baylor University Doc-toral Fellowship Program in OrthopaedicManual Physical Therapy faculty begandeveloping an expedient tool using acombination of sources, including work-sheets from other programs, clinicalexperience, and examples from a varietyof unpublished sources, with feedbackfrom fellows-in-training and other fac-ulty. This tool, titled the SCRIPT, wasdesigned primarily to develop clinicalreasoning skills during a patient encoun-ter, appropriately tailor examination andintervention strategies, promote diagnos-tic accuracy, and assist with planningsubsequent patient encounters (eAppen-dix, available at ptjournal.apta.org). Theform is completed for initial patientencounters during formal one-on-onementorship sessions between the fellow-in-training (mentee) and the fellowship-trained faculty (mentor) and during sub-sequent encounters to reflect on initialhypothesis formation and decision mak-ing.26 The SCRIPT is a tool that providesstructure for the mentee and insight intothe mentee’s clinical reasoning process.The SCRIPT also facilitates individualself-reflective practice and guides patientcase discussions between physical ther-apists in clinical and educational settings.
The ProcessThe SCRIPT facilitates planning and exe-cuting a comprehensive, yet well-tolerated, history taking and examinationby delineating current symptom inten-sity and behavior, as well as the most
likely and alternate hypotheses for allareas of symptoms. The tool helps prior-itize and focus intervention strategies at adose that is likely to be effective andwell-tolerated by the patient, minimizingthe potential to irritate painful structuresor exacerbate the condition while maxi-mizing the opportunity to understandthe patient’s problem and achieve thepatient’s goals.27 The SCRIPT also mayhelp identify potential pathologies out-side the scope of physical therapist prac-tice that need to be screened for andruled out. When the standard of screen-ing for a diagnostic hypothesis isunknown, a physical therapist shouldgenerate appropriate diagnostic ques-tions and search the professional litera-ture for best-evidence screeningstrategies.11
Section I: Guiding HypothesisGeneration and DifferentialDiagnosisSection I guides the mentee’s hypothesisdevelopment and consideration of differ-ential diagnoses early in the patient-physical therapist interaction. Afterestablishing the patient’s profile, includ-ing age, sex, work, and recreational hab-its, the mentee gathers information on allareas of symptoms by completing a bodychart or symptom map. Accuracy anddetail of the body chart, including thelocation, behavior, character or quality,and intensity of all symptoms, are crucialto understanding the patient’s baselinepresentation and are the foundation forearly comprehensive diagnostic hypoth-esis generation.
The mentee places a check mark overpotentially relevant areas on the bodychart that are screened and determinedto be asymptomatic. To help preventmisunderstanding, the mentee touchesthe patient or points to the body regionand asks the patient appropriate screen-ing questions such as, “Do you have any-thing that is not normal or recentlychanged here?”25 Determining and doc-umenting relationships between areas ofsymptoms on the body chart is helpful tohypothesis formation and the differentialdiagnosis process. For example, when a“primary concern” area of symptoms(labeled as P1), such as mid-lumbar pain,increases, a secondary area of symptoms
(labeled as P2), such as lateral thigh pain,also might increase, thereby suggestingthe 2 areas of symptoms are related.25
A novice physical therapist might mistak-enly assume that patients will indicate allareas of symptoms on a body chart andthat any other body region is symptom-free.2 Additionally, a novice physicaltherapist might limit gathering the his-tory and body chart information to onlyone area of symptoms.2 Reasons for thisdecision could include time limitations,an attempt to focus on the areas of symp-toms for which the patient was referredfor physical therapy, or to mitigate asense of being overwhelmed in complexcases or cases with multiple areas ofsymptoms. This rather limited approachcould hinder the physical therapist’s abil-ity to recognize relationships betweenareas of symptoms2 or patterns indicativeof nonmusculoskeletal conditions, suchas systemic illness. Pattern recognitionmay assist experienced physical thera-pists with early hypothesis formation.28
However, a physical therapist workingsolely from pattern recognition of com-mon causes in cases such as this mightassume21 that all cases of back and con-current leg pain are of the same originand overlook other potential sources ofunrelated leg pain, such as tumor, deepvenous pathology, peripheral neuritis, ora distinct local musculoskeletal problem.Expert clinicians may use pattern recog-nition in the differential diagnosis pro-cess but also must maintain an openmind and a willingness to generate, doc-ument, and systematically test multiplealternative hypotheses.7,18,21,29,30
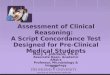
The flow of the typical formal mentor-ship session is illustrated in Figure 1.After completing the body chart, the firstof two 5- to 10-minute pauses occursaway from the patient to allow the men-tee to complete section I of the SCRIPT.These pauses are critical to clinical men-torship, enabling the mentee to reflecton action,6 plan the remaining examina-tion, ask the mentor questions, and gainguidance. This approach also providesan opportunity for the mentor to gaininsight into the mentee’s clinical reason-ing, reinforce their positive decisions,and make suggestions and pose ques-
SCRIPT in Orthopedic Manual Physical Therapy
January 2017 Volume 97 Number 1 Physical Therapy f 3

tions to highlight alternatives inreasoning.
The mentee lists all structures that mustbe considered as possible sources of thepatient’s symptoms, to include joints andbony structures; muscles, tendons, andsoft tissue structures; structures that mayrefer symptoms into the area of concern;and other structures or conditions thatmust be considered or ruled out, such asvisceral pathology, infections, space-occupying lesions, and systemic non-musculoskeletal pathology. This proac-tive planning makes explicit theconnections between thinking andfuture actions.
After completing section I, the menteeformalizes their differential thought bygenerating and prioritizing the most
likely, less likely, and remote hypothesesin section II of the SCRIPT. The mentorreviews the form with the mentee, pro-viding immediate feedback and helpingto refine or provide additional hypothe-ses.31 The mentor ensures that the men-tee has a plan to effectively utilize theremaining patient history to refine andprioritize competing hypotheses withcarefully selected and formulated ques-tions and to determine likely symptombehavior during the physical examina-tion and intervention. Hypothesesderived and prioritized during the his-tory taking are subsequently examinedwith appropriate tests and measures, andlater by the patient’s response to inter-vention, thereby requiring both deduc-tive (analytical) and inductive thinking.
During a mentorship session, the secondplanned pause occurs at the conclusionof the history taking for the mentee tocomplete sections II, III, and IV of theSCRIPT.
Section II: Making ClinicalJudgmentsSection II requires judgments on the con-structs of severity and irritability of symp-toms and nature, stage, and stability ofthe disorder, collectively referred to asSINSS.25 The SINSS, initially described byMaitland and elaborated on by variousother authors,25,32,33 are evaluated foreach symptomatic area, as different areasof symptoms may have different symp-tom behavior and possibly different ori-gins (Fig. 2). The SINSS are determinedby analyzing information gathered dur-ing the history taking.25,32,33 This con-cept helps determine the extent andvigor of the examination and treatmentthat are likely to be well-tolerated.27,33
For example, if a mentee judges apatient’s symptoms to be severe (highintensity) and irritable (easily provokedand persisting), the examination shouldbe limited to the first onset or increase ofsymptoms, and the overall number ofexamination procedures should bereduced accordingly.25 Conversely, apatient whose symptoms display mildseverity and irritability might tolerateexamination including provocative diag-nostic special tests, manual examinationto end of range of motion (ROM), andcombined or repeated motions.34–36 The
nature of the disorder is a multifactorialjudgment based on the mentee’s percep-tion of unique factors associated with theprobable condition, such as typical mus-culoskeletal origin, nontypical presenta-tion requiring screening, complex disor-ders (eg, whiplash, acute radiculitis), andpersonal factors (eg, being a singleworking parent, exhibiting high fear-avoidance behavior).25,32,37 Stage refersto the duration of symptoms, classified asacute, subacute, or chronic or a combi-nation of stages (eg, acute andchronic).25,32 Stage can be an importantfactor directly related to the nature of theproblem, particularly in disorders withhealing tissues or inflammatory pro-cesses. Stability may be characterized asa sign or symptom improving, worsen-ing, or not changing over the courseof the present episode or previousepisodes.25,32
Section III: ConsideringAdditional Contributing FactorsCompleting section III prompts the men-tee to consider additional factors contrib-uting to the patient’s condition, such aspoor conditioning or psychosocial fac-tors, that may change the prognosis orrequire therapeutic attention. These fac-tors are considerations but should not beoverly weighted in the differential diag-nosis process. A patient with decondi-tioning or psychosocial issues wouldhave as many possible sources of symp-toms as a patient who is more physicallyfit or emotionally stable, and those pos-sible sources should be systematicallyconsidered and ruled out.38 This patient,however, did not display contributingfactors that required additionalconsideration.
Sections IV and V: Planning theExaminationSection IV provides a flexible frameworkfor planning the examination. The men-tee refers to the hypotheses in section Iand reprioritizes the most likely hypoth-eses based on information obtained dur-ing the remainder of the history taking.Tests and measures typically prioritizedand selected for the initial examinationprovide essential evaluation of the mostlikely hypotheses and rule out potentiallyserious conditions (Fig. 3). The vigor ofthe examination is strongly influenced by
Figure 1.Flow diagram of how to use the SystematicClinical Reasoning in Physical Therapy(SCRIPT) tool during a mentorship session.
SCRIPT in Orthopedic Manual Physical Therapy
4 f Physical Therapy Volume 97 Number 1 January 2017

the judged SINSS of the patient’s symp-toms. The examination also is used toidentify impairments amenable to physi-cal therapy interventions. Relevantexamination procedures deferred duringthe initial examination should be docu-mented and prioritized for completion insubsequent sessions.
Sections VI–VIII: Recording,Reprioritizing, and Making thePrognosisPrior to implementing treatment, thementee communicates to the mentor thementee’s differential diagnosis, keyexamination findings, and plan of carewhile in front of the patient. The mentorprovides any immediate feedback or
guidance and may assist in treatment asneeded. Sections VI through VIII arecompleted at the conclusion of the initialpatient encounter. Section VI is usedto record the intervention, patientresponse, and prescribed reinforcingexercises. In section VII, the menteeapplies deductive and inductive thinkingto reprioritize the hypotheses based onthe supporting evidence accumulatedduring the examination and treatment.The mentee then quickly reassesseswhether there has been any change inSINSS or additional screening is needed.Finally, the mentee records importantbaseline findings from the patient’s his-tory and examination that should berechecked at subsequent visits to accu-
rately determine the patient’s responseto intervention. In section VIII, the men-tee records prognostic information. If apatient is not responding according tothe prognosis evidence and the mentee’sclinical experience, further consider-ation of alternate hypotheses, additionalexamination, or more formal screeningmay be warranted. The mentee’s abilityto assess a patient’s response to interven-tion in order to test diagnostic hypothe-ses, combined with the ability to exam-ine and treat patients over multipleclinical sessions, should improve diag-nostic accuracy, particularly when clini-cal reasoning is utilized throughout theepisode of care.10,11
Application of the ProcessWe present a patient case where theSCRIPT guided the clinical reasoningprocess during a patient encounter witha 64-year-old retired man who wasreferred by a physician for physical ther-apy with a diagnosis of axial back pain.The patient reported a primary com-plaint of chronic lower back pain (LBP)and a secondary complaint of bilateralplantar foot tingling. The care of thispatient met Health Insurance Portabilityand Accountability Act (HIPAA) require-ments of the institution for disclosure ofprotected health information.
In the case example below, the patientidentified his primary complaint as a con-stant, but variable in intensity, deep acheor stiffness in his central lower lumbarspine (P1) (Fig. 4). He also describeddeep, constant tingling of variable inten-sity on the plantar surfaces of both feet,more pronounced in the right foot (P2)than the left foot (P3). The patientreported that there was no relationshipamong the areas of symptoms.
Using the information from section I, thementee considered degenerative disk dis-ease with central or bilateral foraminalstenosis as the most likely hypotheses.The mentee judged chronic lower lum-bar dysfunction with a separate periph-eral neuropathic disease (PND) to be aless likely hypothesis. The mentee tai-lored the history to further test the mostlikely and alternative hypotheses (Fig. 4).
II. INFLUENCE OF THE SYMPTOMS ON THE EXAM. Detailed by Area of Symptoms as Mapped on Body Chart.Px Severity Irritability Nature Stage Stability Limit
ExamP1 Moderate Mild MSK, postsurgical,
degenerativeChronic Not changing N
P2 Mild–moderate
Mild MSK, nerve, possible systemic disease contribution
Chronic Worsening N
P3 Mild–moderate
Mild MSK, nerve, possible systemic disease contribution
Chronic Worsening N
MildModerateSevere
MildModerateSevere
(Healing, fragile tissues, inflammatory, psychosocial)Non-MSK/MSK/both
Acute, subacute, chronicAcute on chronicSubacute on chronic
ImprovingWorseningNot changing
Yes= YNo=N
What will be the vigor of your exam? P1 P2 P3 Do the nature, diagnosis, or comorbidities warrant special caution for exam or treatment? What? Y/N(eg, trauma/red flags/instability/pathological process)No
Examine to first onset or change in painExamine to end of active range of motion/ACTIVE limit X
Examine to end of passive range of motion/PASSIVE limit
Which symptoms will be desirable to reproduce?Back pain (P1) and peripheral symptoms (P2 and P3)
Examine with OVERPRESSURE sufficient to determine end feel
Do you expect a comparable sign to be EASY or HARD to reproduce?Easy in lumbar spine, hard in periphery
Use sustained, repeated, or combined movements
X X
What do you expect to be treating?(Circle one)
PAIN
RESISTANCE RESPECTING PAIN
RESISTANCE
PAIN
RRRRREEEEESSSSSIISSTANCE RESPECTING PAIN
RESISTANCE
Figure 2.Section II of the Systematic Clinical Reasoning in Physical Therapy (SCRIPT).MSK�musculoskeletal, Px�area of symptoms, P1�primary area of symptoms,P2�secondary area of symptoms, P3�tertiary area of symptoms.
SCRIPT in Orthopedic Manual Physical Therapy
January 2017 Volume 97 Number 1 Physical Therapy f 5

The patient’s history revealed previousbilateral L3–L5 hemilaminectomy proce-dures and lateral recess decompressionfor spinal stenosis 1 year prior, with noeffect on the feet tingling. Therefore, ste-nosis did not seem likely to be the pri-mary cause of his tingling. Additionally,the patient had medically managed type2 diabetes mellitus. As PND is prevalentin the diabetic population and neurolog-ical symptoms associated with this con-dition may be similar to those seen witha variety of lumbar conditions, the alter-native hypothesis of PND could not beruled out and was documented on theSCRIPT.39 Other potential sources ofLBP, such as neoplasm, infection, or aor-tic abdominal aneurysm, were judged tobe remote hypotheses for this 64-year-old immunocompetent patient who hadnever smoked and was without generalhealth changes and, therefore, did notrequire additional screening at this point.
During the history taking, the patientreported unchanging LBP for 2 years andbilateral foot tingling for 4 to 5 years, butthat these symptoms had worsened inintensity and frequency over the pastyear. His LBP and tingling both increasedafter standing for 30 minutes and easedwith walking for 10 minutes. He usedCelebrex (Pfizer Inc, New York, NewYork) daily for his LBP and Percocet(Endo Pharmaceuticals Inc, Malvern,Pennsylvania) occasionally for break-through pain. His sleep and activities ofdaily living were not limited. Therefore,the mentee judged the severity of his LBPas mild to moderate and the severity ofhis irritability as mild. The LBP seemedmechanical in nature, whereas the foot
tingling seemed to change more than theback symptoms, suggesting that it wasless stable and potentially of a differentorigin than the LBP. Due to the overallmild severity and irritability, the menteedecided to examine the patient to theextent necessary to elicit all areas ofsymptoms. A neurological screening alsowas deemed necessary due to the pres-ence of peripheral tingling.
The examination planned for this caseincluded neurological screening, lumbarROM testing, soft tissue and lumbarmobility assessment, and neural tensiontests. Standing lumbar extension activeROM was limited, with increased LBP atend range that quickly returned to base-line upon return to neutral. The neuro-logical screening demonstrated reducedright ankle reflex, reduced sensation onthe right plantar foot and heel to lighttouch, and absent Babinski and clonustests. Bilateral lower extremities demon-strated 5/5 strength in L2–S1 myotomes.Passive mobility assessment of the lum-bar spine demonstrated hypomobilityand localized pain, with central and rightunilateral posterior-to-anterior mid-rangemobilization at L3–L5, but did not affectthe patient’s foot tingling, nor did activeROM testing of the lumbar spine. Bilat-eral straight-leg-raising tests with sensitiz-ing maneuvers did not reproduce orchange lower extremity symptoms.Although it seemed likely based on thesefindings that the LBP and the neurologi-cal symptoms were of distinct origins,the examination did not adequately dis-tinguish between the 2 hypotheses.Given the diagnostic uncertainty, thementee chose to use the patient’s
response to lumbar intervention to helpdetermine the relationship between theLBP and foot tingling.
Interview and physical examination find-ings are documented in the patientrecord, and key findings are marked withasterisk signs to denote them as impor-tant parts of the baseline presentation.These key findings are frequently reex-amined to determine patient response toexamination and treatment. These keybaseline findings are recorded in sectionV of the SCRIPT (Fig. 5).
In this case, manual treatment with rein-forcing exercise was initiated to addressimpaired lumbar spine extension.Because the key finding of lumbar symp-toms during passive mobility assessmentof the L3 vertebral segment was mostcomparable with the patient’s primarycomplaint, treatment at the initial visitconsisted of six 30-second bouts of gradeIV central posterior-to-anterior mobiliza-tions directed to the L3 vertebral seg-ment, followed by supine pelvic rockingmotions in a painless ROM. After treat-ment, the patient’s lumbar extension andpain were moderately improved, but thetingling remained unchanged (Fig. 6).The prognosis of long-standing sensorychanges suggested it may be difficult toinfluence these symptoms in one treat-ment session, further contributing todiagnostic uncertainty.
The diagnostic uncertainty at the end ofthe initial examination and the docu-mented alternative hypotheses noted insection VII of the SCRIPT warrantedadditional screening for the cause of thefoot tingling before completing sectionsVII and VIII of the SCRIPT. Peripheralneuropathy in patients with diabetesincreases the risk of foot ulceration andinfection by up to 7-fold,34 highlightingthe importance of early identification.Therefore, the mentee performed a liter-ature search11 to find the best screeningstrategies to answer the following clini-cal question: “In a 64-year-old man withtype 2 diabetes and chronic LBP, what isthe best way to screen for a diabetic PNDas the source of plantar foot tingling?”
Clinical practice guidelines recommendusing a cluster of tests to screen for dia-
IV. PLANNED EXAM PROCEDURES: Prioritize based on most likely hypotheses and SINSS.Day/Visit 1Lumbar AROM, LE neurological exam, SLR, palpation exam of lumbar spine, segmental mobility of lumbar spine
Day/Visit 2MNSI: inspection of feet, vibrationSlump test for neural tension symptomsProne knee bend to assess anterior hip structure flexibility
Day/Visit 3Repeated motions to assess for centralization/ peripheralizationClear hip/SIJ
Figure 3.Section IV of the Systematic Clinical Reasoning in Physical Therapy (SCRIPT). SINSS�severity,irritability, nature, stage, stability; AROM�active range of motion; LE�lower extremity;SLR�straight leg raise; MNSI�Michigan Neuropathy Screening Instrument, SIJ�sacroiliacjoint.
SCRIPT in Orthopedic Manual Physical Therapy
6 f Physical Therapy Volume 97 Number 1 January 2017

betic neuropathy, including foot andlower limb inspection and sensory test-ing.35 The literature indicated that theMichigan Neuropathy Screening Instru-
ment (MNSI), consisting of a foot inspec-tion, ankle reflexes, and vibration per-ception, has been validated in the type 2diabetic population as a screening tool
for diabetic PND.36 A score of �2 has aspecificity of 83% (95% confidence inter-val�75%, 89%) and a positive likelihoodratio of 3.9 (95% confidence inter-val�2.5, 6.1), suggesting that furtherquantitative neurological testing wasappropriate.36
Based on the literature, the menteeplanned to administer the MNSI at thefollowing visit to further differentiate thegenesis of the peripheral symptoms(Fig. 7). Subsequent examination demon-strated a reduced ankle reflex on theright and absent vibratory sense at bothankles, resulting in an MNSI score of 2.5and the need for further screening. Thediagnostic gold standard for diabeticPND is electromyography and nerve con-duction study (EMG/NCS) testing.34 Dueto the patient’s complaints of worseninglower extremity neurological symptoms,the physical therapist communicatedwith the patient’s primary care provider,who ordered EMG/NCS testing.
The EMG/NCS testing demonstrated milddemyelinating PND affecting the sensoryand motor fibers in the lower extremi-ties, as well as evidence of chronic bilat-eral L5 and S1 radiculopathies that didnot warrant surgical intervention. Thisknowledge helped the mentee deter-mine the likely clinical diagnoses andoverall prognosis (Fig. 7). Physical ther-apy treatment would likely influence thepatient’s chronic LBP more than thechronic neurological symptoms. How-ever, understanding the contributions ofthe diabetic PND to the patient’s symp-toms enabled the mentee to provideappropriate patient education, devise atreatment plan respective of the patient’scomorbidity and reconnect the patientwith his primary care provider for con-tinued medical management.
In accordance with the Guide to Physi-cal Therapist Practice,37 the appropriateclinical care for this patient includedtreating the LBP consistent with best-evidence strategies and referring thepatient for further evaluation of his PND.The data from the SCRIPT helped guideclinical reasoning and plan managementthroughout the episode of care.
I. WHAT AREAS/STRUCTURES MUST BE CONSIDERED AS POSSIBLE SOURCE(S) OF SYMPTOMS? Joints and bony structures UNDER the area of symptoms
Muscles, tendons, and other soft tissue UNDER and IN the area of symptoms
Pain-producing structures that may REFER into the area of symptoms
OTHER structures or conditions that must be considered or ruled out
-Bilateral lower lumbar facet joints-Bilateral lower lumbar vertebral joints-Bilateral ilium-Sacrum-Bilateral sacroiliac joints-Bilateral hindfoot joints-Bilateral tarsal joints-Bilateral tarsometatarsaljoints-Bilateral metatarsal phalangeal joints
-Lower lumbar paravertebralmuscles-Bilateral quadratus lumborum muscles-Bilateral proximal gluteal muscles-Bilateral footintrinsic muscles-Bilateral plantar fascia-Bilateral lower extremity peripheral nerves (tibial, deep/superficial fibular, medial/lateralplantar)
- Lower extremity vascular- GI system- GU system- Space-occupying lesion (tumor)- Spinal infection
Most Likely Hypotheses: Less Likely Hypotheses: Remote Hypotheses:
P1: central low back pain; achy, stiff, deep2–10/10Resting pain 2/10
P2 (left foot) and P3 (right foot):bilateral, foot tingling,deep, constant, 2–5/10Resting pain 2/10
� Chronic central lower lumbar dysfunction with bilateral radiculopathy/radiculitis,most likely of S1 nerve root
� Chronic central lower lumbar dysfunction with peripheral neuropathic disease (polyneuropathy or mononeuropathy)
� Spinal stenosis withneurogenic claudication
� Myofascial pain status post lumbar surgery with bilateral chronic neural tension symptoms
� Space-occupying lesion in the lumbar spine
� Lower extremity or abdominal vascular pathology
� Referred pain from viscerogenic pathology
� Spinal infection
-Lower thoracic spine-Upper lumbar spineMidlumbarspine-Upper, mid, and lower lumbar disks-Bilateral sacroiliac joints-Bilateral hip joints-Bilateral talocrural joints
Figure 4.Section I of the Systematic Clinical Reasoning in Physical Therapy (SCRIPT).GI�gastrointestinal, GU�genitourinary, P1�primary area of symptoms, P2�secondary areaof symptoms, P3�tertiary area of symptoms.
SCRIPT in Orthopedic Manual Physical Therapy
January 2017 Volume 97 Number 1 Physical Therapy f 7

OutcomeUtilizing the SCRIPT tool enabled thementee to generate appropriate hypoth-eses and create an examination plan tosystematically test the hypotheses, ulti-mately leading the mentee to query theliterature to answer a clinical question,establish a physical therapy diagnosis,and design a treatment plan that entailedcontinued physical therapy to addressthe patient’s LBP and a referral to thepatient’s primary care provider for con-tinued management of the PND. Thepatient elected to continue physical ther-apy at another clinic closer to his home,so no additional information is knownabout subsequent physical therapy inter-vention or changes in his symptoms asso-ciated with the treatment that hereceived. In addition to facilitating thementee’s clinical reasoning processes toestablish a diagnosis and plan of care, theSCRIPT tool provided the mentor withinsight into the mentee’s clinical reason-ing. Although the SCRIPT was beneficialin the clinical reasoning and mentoringprocesses for this patient case, the reli-ability and validity of the SCRIPT toolhave not been formally studied. Future
research is needed to examine the use-fulness of the SCRIPT in the postprofes-sional academic setting.
DiscussionThis case illustrates how the SCRIPTguided the clinical reasoning process fora patient with symptoms commonly seenin an outpatient physical therapy prac-tice. Using the SCRIPT to identify a spec-trum of potentially involved structuresenabled the mentee to consider alterna-tive diagnostic hypotheses. The SCRIPTprovided the mentee with a systematicway to gather information to guide clin-ical reasoning and reflection while alsoproviding the mentor with valuableinsight to help usher the mentee’s clini-cal reasoning to the level of an expertclinician.40 Additionally, the tool spurredthe mentee to search the literature whenthe origin of the foot tingling wasunclear and more information wasneeded to evaluate potential alternativehypotheses. Although not rapidly pro-gressing or life threatening, this systemicnerve condition will likely require medi-cal management and influences thepatient’s overall prognosis. Physical ther-
apists in all settings should be able tosearch, find, and apply or recommendscreening strategies when clinical rea-soning suggests they are appropriate.The SCRIPT provides a systematic meansof considering examination-derived datafor the purpose of formulating diagnostichypotheses and determining the appro-priate scope and vigor of the examina-tion and intervention. In this case, theSCRIPT guided the mentee to conduct aninitial intervention that allowed thepatient to leave the clinic with less LBPwhile providing the mentee withdiagnostically helpful information ofunchanged symptoms in the patient’sfeet, facilitating the appropriate addi-tional screening.
Published clinical reasoning tools areavailable for pediatric physical therapistpractice.24,41 To our knowledge, thepeer-reviewed literature does not have atool to guide clinical reasoning in otherareas of practice. The SCRIPT could beused to teach and structure clinical rea-soning for a number of educational andprofessional development activities,such as clinical mentorship, case-basedtutorial sessions, new-employee orienta-tion and mentorship,42 assessing a phys-ical therapist’s clinical reasoning skills,42
and self-reflective practice.
The SCRIPT provides a framework fordeveloping clinical reasoning for usethroughout the patient encounter. Struc-tured processes to develop clinical rea-soning skills improve the differentialdiagnosis process,2 reduce the risk ofdiagnostic error,9 and facilitate well-tolerated examination and interventionstrategies.9,25 Similar to Atkinson andNixon-Caves’24 pediatric clinical reason-ing tool, additional research is needed todemonstrate the SCRIPT’s influence onclinical reasoning thought processes,utility in developing a novice to anexpert clinician, and effectiveness as anaid to reflective practice. It ultimatelymay be useful in a variety of academicand clinical settings.
As with any tool, however, the SCRIPThas its limitations and challenges. Bornout of a manual physical therapy fellow-ship program, the verbiage in the SCRIPTis biased toward the typical practice pat-
V. EXAM FINDINGS Important baseline findings from patient history:
Important baseline exam findings:
Stand >30 min produces back and peripheral symptoms Walk >15–30 min produces peripheralsymptoms
Reduced reflex right ankle, reduced sensationto light touch in right plantar foot
Standing lumbar extension 10%, 5/10 pain
Figure 5.Section V of the Systematic Clinical Reasoning in Physical Therapy (SCRIPT).
VI. TREATMENT PROVIDEDManual Therapy Treatment
Direction Grade Amount Duration Reinforcing Exercises:
Pelvic anterior and posterior rocks in hook-lying position
1stL3
Central posterior-anterior
IV 3 reps 30 s
2ndL3
Central posterior-anterior
IV 3 reps 30 s
Response to Treatment:Lumbar extension movement was symmetrical to 25% of the range before limited by 2–3/10 low back pain. No effect on peripheral symptoms.
Figure 6.Section VI of the Systematic Clinical Reasoning in Physical Therapy (SCRIPT). Grade IV�50%of normal movement within resistance, reps�repetitions.
SCRIPT in Orthopedic Manual Physical Therapy
8 f Physical Therapy Volume 97 Number 1 January 2017

terns of a manual physical therapist andutilizes verbiage best known from Mait-land’s work.25 Additionally, utilizing atool such as the SCRIPT requires dedi-cated time and effort, which may proveto be obstacles to its utilization in typicalclinical practice. Our program allots 90minutes to an initial evaluation in orderto allow for the 2 planned pauses awayfrom the patient and the ongoing discus-sion between the mentee and mentorduring the examination and treatment. It
may be of benefit to have a third plannedpause after the examination to discusskey findings, reprioritize diagnostichypotheses, and plan treatment. Thisthird planned pause may be well worththe additional cost of time for novices ormentees who the mentor identifies asstruggling with a particular patientencounter. Lastly, although the SCRIPTattempts to concisely marry thehypothetico-deductive reasoning strate-gies with narrative reasoning, the
SCRIPT is not an exhaustive tool. A moremeticulous tool may be necessary for amore novice physical therapist. Forexample, the SCRIPT attempts to helpidentify relevant psychosocial factors butdoes not inherently prompt an in-depthexamination of such factors.
The development of clinical reasoningskills is a defining feature of residencyand fellowship education1 and central todeveloping expertise. Expertise is not astatus solely acquired through residencyor fellowship education but is a processof continued development. An expert’scareer advances through continuouslearning and progressive problem solv-ing, a process called “adaptive exper-tise.”43 Meta-cognition is a criticalelement of progressive problem solv-ing44,45; some authors22,46 argue that thisis the most important component of pro-fessional competence.
Expert clinicians differ from noviceswith respect to their use of clinical rea-soning strategies and their ability andwillingness to consider, document, andtest alternate hypotheses and to controlthe environment of the patient encoun-ter.3,5,21,28,40 Mentorship in residencyand fellowship programs is paramount tothe development of advanced clinicalreasoning skills and developing exper-tise,1 yet we have much to understandand discover in the teaching and learningprocess for developing clinical reasoningskills. Clinical reasoning tools, such asthe SCRIPT, may help clinicians developconsistent clinical processes that aid inthe differential diagnosis process. Resi-dency and fellowship education withthis central focus on clinical reasoning isa rich environment for continuedresearch.47,48
All authors provided concept/idea/projectdesign and writing. Dr Deyle and Dr Bakerprovided project management. Dr Jensenprovided consultation (including review ofmanuscript before submission).
DOI: 10.2522/ptj.20150482
VI I. ASSESSMENT END OF DAY 1Most Likely Hypothesis:Chronic central lower lumbar dysfunction with peripheral neuropathic disease (polyneuropathy or mononeuropathy)Supporting Evidence:Lumbar exam and treatment did not change peripheral symptoms, potentially pointing to 2separate origins of symptoms. Central technique applied to lumbar spine improved lumbar symptoms.Reduced reflex in right ankle, reduced sensation to light touch in right plantar foot.Absence of motor weakness in S1 myotome.
Alternate Hypotheses:Chronic central lower lumbar dysfunction with bilateral radiculopathy/radiculitis, most likely of S1 nerve root.
Supporting Evidence:Central technique applied to lumbar spine improved lumbar symptoms. Long-standing sensory changes associated with radiculopathy may be difficult to influence in one visit , limiting ability to exclude a root- level lesion.Peripheral symptoms in S1 dermatomal pattern.Reduced reflex in right ankle, reduced sensation to light touch in right plantar foot.
Has there been a change in your assessment of SINSS? What? NoIs there a need for additional screening? What? Why? Yes, diagnostic uncertainty at end of initial evaluation; risk of ulceration and infection in patients with diabetic neuropathy. MNSI is warranted.
VIII . PROGNOSIS
What is the natural history of the disorder? Chronic, progressive lumbar pain with uncertainty surrounding peripheral symptomsExpected level and rate of recovery based on evidence for prognosis:
Short Term: Stand 45 min without worsening back pain.Long Term: Walk 45 min without worsening back or foot symptoms.
How many visits over what period of time do you expect to see this patient?6–8 visits over 4 wkFactors that may limit rate or extent of recovery:History of diabetes mellitus and associated limited ability to heal. Two back surgeries with minimal change in lumbar pain.Likelihood of recurrence: MILD/MODERATE/HIGH
How will you attempt to prevent a recurrence of symptoms?Patient education, maintenance HEP of lumbar mobility and strengthening exercises, regular low-impact aerobic exercise
At the next visit, what treatment will you choose if the patient is:Better:Progress depth of CPA mobilization at L3, increase number of bouts of treatment.
Same:Continue and progress central PA mobilization at L3. Layerin CPA at additional levels (L4, L 5).
Worse:Layer in CPA at adjacent levels (L2, L4). Defer CPA at L3.
Figure 7.Sections VII and VIII of the Systematic Clinical Reasoning in Physical Therapy (SCRIPT).SINSS�severity, irritability, nature, stage, stability; MNSI�Michigan Neuropathy ScreeningInstrument; HEP�home exercise program; CPA�central posterior to anterior.
SCRIPT in Orthopedic Manual Physical Therapy
January 2017 Volume 97 Number 1 Physical Therapy f 9

References1 American Board of Physical Therapy Resi-
dency and Fellowship Education. Mentor-ing resource manual. August 2014. Avail-able at: http://www.abptrfe.org/ForPrograms/MentoringResourceManual/. Accessed April 8,2015.
2 Jones MA. Clinical reasoning in manualtherapy. Phys Ther. 1992;72:875–884.
3 Edwards I, Jones M, Carr J, et al. Clinicalreasoning strategies in physical therapy.Phys Ther. 2004;84:312–330; discussion331–335.
4 Wainwright SF, Shepard KF, Harman LB,Stephens J. Factors that influence the clin-ical decision making of novice and expe-rienced physical therapists. Phys Ther.2011;91:87–101.
5 Jensen GM, Shepard KF, Gwyer J, HackLM. Attribute dimensions that distinguishmaster and novice physical therapy clini-cians in orthopedic settings. Phys Ther.1992;72:711–722.
6 Schon DA. The Reflective Practitioner:How Professionals Think in Action. NewYork, NY: Basic Books; 1984.
7 Lawson AE, Daniel ES. Inferences of clini-cal diagnostic reasoning and diagnosticerror. J Biomed Inform. 2011;44:402–412.
8 Kempainen RR, Migeon MB, Wolf FM.Understanding our mistakes: a primer onerrors in clinical reasoning. Med Teach.2003;25:177–181.
9 Singh H, Giardina TD, Meyer AN, et al.Types and origins of diagnostic errors inprimary care settings. JAMA Intern Med.2013;173:418–425.
10 Rhon DI, Deyle GD, Gill NW. Clinical rea-soning and advanced practice privilegesenable physical therapist point-of-caredecisions in the military health care sys-tem: 3 clinical cases. Phys Ther. 2013;93:1234–1243.
11 Crowell MS, Tragord BS, Taylor AL, DeyleGD. Integration of critically appraised top-ics into evidence-based physical therapistpractice. J Orthop Sports Phys Ther. 2012;42:870–879.
12 Greenfield BH, Jensen GM. Understandingthe lived experiences of patients: applica-tion of a phenomenological approach toethics. Phys Ther. 2010;90:1185–1197.
13 Greenfield BH, Jensen GM. Phenomenol-ogy: a powerful tool for patient-centeredrehabilitation. Phys Ther Rev. 2012;17:417–424.
14 Ajjawi R, Higgs J. Learning to reason: ajourney of professional socialisation. AdvHealth Sci Educ Theory Pract. 2008;13:133–150.
15 Moulton CE, Regehr G, Mylopoulos M,MacRae HM. Slowing down when youshould: a new model of expert judgment.Acad Med. 2007;82(10 suppl):S109–S116.
16 Boissonnault WG, Ross MD. Physical ther-apists referring patients to physicians: areview of case reports and series. J OrthopSports Phys Ther. 2012;42:446–454.
17 Deyle GD. Direct access physical therapyand diagnostic responsibility: the risk-to-benefit ratio. J Orthop Sports Phys Ther.2006;36:632–634.
18 Mathers JJ. Differential diagnosis of apatient referred to physical therapy withneck pain: a case study of a patient with anatypical presentation of angina. J ManManip Ther. 2012;20:214–218.
19 Moore JH, Goss DL, Baxter RE, et al. Clin-ical diagnostic accuracy and magnetic res-onance imaging of patients referred byphysical therapists, orthopaedic surgeons,and nonorthopaedic providers. J OrthopSports Phys Ther. 2005;35:67–71.
20 Ericsson KA, Prietula MJ, Cokely ET. Themaking of an expert. Harv Bus Rev. 2007;87:215–251.
21 Jones MA, Rivett DA. Clinical Reasoningfor Manual Therapists. Oxford, UnitedKingdom: Butterworth-Heinemann; 2003.
22 Epstein RM, Siegel DJ, Silberman J. Self-monitoring in clinical practice: a challengefor medical educators. J Contin EducHealth Prof. 2008;28:5–13.
23 Eva KW. What every teacher needs toknow about clinical reasoning. Med Educ.2005;39:98–106.
24 Atkinson HL, Nixon-Cave K. A tool for clin-ical reasoning and reflection using theinternational Classification of Function-ing, Disability and Health (ICF) frame-work and patient management model.Phys Ther. 2011;91:416–430.
25 Maitland G; Hengeveld E, Banks K, eds.Maitland’s Vertebral Manipulation: Man-agement of Neuromusculoskeletal Disor-ders—Volume 1. 8th ed. London, UnitedKingdom: Churchill Livingstone; 2013.
26 Beeton K, Langendoen J, Maffey L, et al.International Federation of OrthopaedicManipulative Physical Therapists: Educa-tional Standards in Orthopaedic Manipula-tive Therapy, Part A: Educational Stan-dards. Available at: http://www.ifompt.com/site/ifompt/files/pdf/XXIFOMPT_Educ_Standards_IM_Doc_Merged.pdf. AccessedJune 30, 2014.
27 Deyle GD, Gill NW. Well-tolerated strate-gies for managing knee osteoarthritis: amanual physical therapist approach toactivity, exercise, and advice. PhysSportsmed. 2012;40:12–25.
28 Jensen GM, Gwyer J, Shepard KF. Expertpractice in physical therapy. Phys Ther.2000;80:28–43; discussion 44–52.
29 Trowbridge RL. Twelve tips for teachingavoidance of diagnostic errors. MedTeach. 2008;30:496–500.
30 Croskerry P. The importance of cognitiveerrors in diagnosis and strategies to mini-mize them. Acad Med. 2003;78:775–780.
31 Kassirer JP. Teaching clinical reasoning:case-based and coached. Acad Med. 2010;85:1118–1124.
32 Koury MJ, Scarpelli E. A manual therapyapproach to evaluation and treatment of apatient with a chronic lumbar nerve rootirritation. Phys Ther. 1994;74:548–560.
33 Smart K, Doody C. The clinical reasoning ofpain by experienced musculoskeletal phys-iotherapists. Man Ther. 2007;12:40–49.
34 Kanji JN, Anglin RE, Hunt DL, Panju A.Does this patient with diabetes have large-fiber peripheral neuropathy? JAMA. 2010;303:1526–1532.
35 Boulton AJ, Vinik AI, Arezzo JC, et al. Dia-betic neuropathies: a statement by theAmerican Diabetes Association. DiabetesCare. 2005;28:956–962.
36 Moghtaderi A, Bakhshipour A, Rashidi H.Validation of Michigan NeuropathyScreening Instrument for diabetic periph-eral neuropathy. Clin Neurol Neurosurg.2006;108:477–481.
37 Guide to Physical Therapist Practice 3.0.Alexandria, VA: American Physical Ther-apy Association; 2014. Available at: http://guidetoptpractice.apta.org/content/1/SEC1.body.
38 Ramond A, Bouton C, Richard I, et al. Psy-chological risk factors for chronic lowback pain in primary care: a systematicreview. Fam Pract. 2011;28:12–21.
39 American Diabetes Association. Standardsof medical care in diabetes—2011. Diabe-tes Care. 2011;34(suppl 1):S11–S61.
40 May S, Withers S, Reeve S, Greasley A. Lim-ited clinical reasoning skills used by novicephysiotherapists when involved in theassessment and management of patientswith shoulder problems: a qualitative study.J Man Manip Ther. 2010;18:84–88.
41 Kenyon LK. The Hypothesis-Oriented Pedi-atric Focused Algorithm: a framework forclinical reasoning in pediatric physical ther-apist practice. Phys Ther. 2013;93:413–420.
42 Atkinson H, Nixon-Cave K. Implementa-tion of the Physical Therapy Clinical Rea-soning and Reflection Tool (PT-CRT). Pre-sented at: NEXT Conference andExposition of the American Physical Ther-apy Association; June 3–6, 2015; NationalHarbor, Maryland.
43 Hatano G, Inagaki K. Two courses ofexpertise. In: Stevenson HA, Hakuta K,eds. Child Development and Educationin Japan. New York, NY: Freeman; 1986:262–272.
44 Bereiter C, Scardamalia M. SurpassingOurselves: An Inquiry Into the Natureand Implications of Expertise. Chicago,IL: Open Court Publishing Co; 1993.
45 Irby DM, Cooke M, O’Brien BC. Calls forreform of medical education by the Carne-gie Foundation for the Advancement ofTeaching: 1910 and 2010. Acad Med.2010;85:220–227.
46 Epstein RM. Defining and assessing profes-sional competence. JAMA. 2002;287:226–235.
47 Robertson EK, Tichenor CJ. Postprofes-sional cartography in physical therapy:charting a pathway for residency and fel-lowship training. J Orthop Sports PhysTher. 2015;45:57–60.
48 Rodeghero J, Wang YC, Flynn T, et al. Theimpact of physical therapy residency orfellowship education on clinical outcomesfor patients with musculoskeletal condi-tions. J Orthop Sports Phys Ther. 2015;45:86–96.
SCRIPT in Orthopedic Manual Physical Therapy
10 f Physical Therapy Volume 97 Number 1 January 2017

eAppendix.Systematic Clinical Reasoning in Physical Therapy (SCRIPT) Blank Forma
I. WHAT AREAS/STRUCTURES MUST BE CONSIDERED AS A POSSIBLE SOURCE(S) OF SYMPTOMS?
Joints and bonystructuresUNDER the areaof symptoms
Muscles,tendons, andother soft tissueUNDER and INthe area ofsymptoms
Pain-producingstructuresthat mayREFER intothe area ofsymptoms
OTHERstructures orconditions thatmust beconsidered orruled out
Most Likely Hypotheses: Less Likely Hypotheses: Remote Hypotheses:
II. INFLUENCE OF THE SYMPTOMS ON THE EXAM. Detailed by Area of Symptoms as Mapped on Body Chart.
Px Severity Irritability Nature Stage Stability Limit Exam
MildModerateSevere
MildModerateSevere
(Healing, fragile tissues,inflammatory,psychosocial)Non-MSK/MSK/both
Acute, subacute, chronicAcute on chronicSubacute on chronic
Improving 1Worsening 2Not changing
Yes�YNo�N
What will be the vigor of yourexam?
P1 P2 P3 P4 Do the nature, diagnosis, or comorbiditieswarrant special caution for exam ortreatment? Y/N What? (eg, trauma/red flags/instability/pathological process)Examine to first onset or
change in pain (P1)
Examine to end of active rangeof motion/ACTIVE limit
Examine to end of passiverange of motion/PASSIVE limit
Which symptoms will be desirable toreproduce?
Examine with OVERPRESSUREsufficient to determine endfeel
Do you expect a comparable sign to beEASY or HARD to reproduce?
Use sustained, repeated, orcombined movements
What do you expect to be treating? (Circleone)PAINRESISTANCE RESPECTING PAINRESISTANCE
(Continued)
SCRIPT in Orthopedic Manual Physical Therapy
January 2017 (eAppendix, Baker et al) Volume 97 Number 1 Physical Therapy f 1

eAppendixContinued
III. INFLUENCING FACTORS: Are there contributing factors that need to be addressed with this patient? (check all that apply)
Posture Ergonomics Conditioning Psychosocial Factors Other
IV. PLANNED EXAM PROCEDURES: Prioritize based on most likely hypotheses and SINSS.
Day/Visit 1 Day/Visit 2 Day/Visit3
V. EXAM FINDINGS
Important baseline findings from patient history Important baseline exam findings:
VI. TREATMENT PROVIDED
Manual TherapyTreatment
Direction Grade Amount Duration Reinforcing Exercises:
1st
2nd Response to Treatment:
VII. ASSESSMENT END OF DAY 1
Most Likely Hypothesis:
Supporting Evidence:
Alternate Hypotheses:
Supporting Evidence:
Has there been a change in your assessment of SINSS? What?
Is there a need for additional screening? What? Why?
VIII. PROGNOSIS
What is the natural history of the disorder?
Expected level and rate of recovery based on evidence for prognosis:Short Term:Long Term:
How many visits over what period of time do you expect to see this patient?
Factors that may limit rate or extent of recovery:
Likelihood of recurrence: MILD/MODERATE/HIGH
How will you attempt to prevent a recurrence of symptoms?
At the next visit, what treatment will you choose if the patient is:
Better: Same: Worse:
a Developed for Army-Baylor University Doctoral Fellowship in Orthopaedic Manual Physical Therapy. Px�area of symptoms, P1�primary area of symptoms,P2�secondary area of symptoms, P3�tertiary area of symptoms, P4�quaternary area of symptoms, MSK�musculoskeletal; SINSS�severity, irritability,nature, state, stability. The Systematic Clinical Reasoning in Physical Therapy (SCRIPT) may not be used or reproduced without written permission from theauthors.
SCRIPT in Orthopedic Manual Physical Therapy
2 f Physical Therapy Volume 97 Number 1 January 2017 (eAppendix, Baker et al)
View publication statsView publication stats