Embed Size (px)
Citation preview

510 MINERVAANESTESIOLOGICA May2011
O R I G I N A L A R T I C L E
Anno: 2011Mese: MayVolume: 77No: 5Rivista: MINERVA ANESTESIOLOGICACod Rivista: Minerva Anestesiol
Lavoro: titolo breve: SYSTEMATIC APPROACH TO SEVERE RESPIRATORY FAILURE DUE TO NOVEL A (H1N1) INFLUENZAprimo autore: CORNEJOpagine: 510-21
InApril2009,anovelinfluenzaA(H1N1)vi-rusappearedinMexico,causinganoutbreak
of respiratorydisease.1 It rapidly spreadwidelyaround the world, acquiring the characteristicsofpandemicdisease.During2009,12302caseswereconfirmedinChile.Nevertheless,368129patientsmetcriteriaofsuspiciouscasesand1622developedsevereillness,resultinginoneofthehighestratesofinfectionworldwide.2
Despite the low lethality among the globalpopulation,thehightransmissibilityoftheviruscausedseriousdifficultiesinhealthcaresystemsaround the globe.3 Among the critically ill in-fluenzapatients, ahigh incidenceof severehy-poxemia, early development of multiple organdysfunction syndrome (MODS), and frequentnecessityofrescuetherapieswereobservedfromthebeginningofthepandemic.1,4-11Themortal-
SystematicapproachforsevererespiratoryfailureduetonovelA(H1N1)influenza
R.CORNEJO1,E.TOBAR1,G.DÍAZ1,C.ROMERO1,O.LLANOS1,L.R.GÁLVEZ1,A.ZAMORANO1,L.FÁBREGA1,W.NEIRA1,D.ARELLANO1,C.REPETTO1,D.AEDO1,
J.CARLOSDÍAZ2,R.GONZÁLEZ3
1IntensiveCareUnit,DepartmentofMedicine,HospitalClínicoUniversidaddeChile.Santiago,Chile;2DepartmentofRadiology,HospitalClínicoUniversidaddeChile,Santiago,Chile;3MedicineStudent,FacultyofMedicine,UniversidaddeChile,Santiago,Chile
A B S T R A C TAim.InApril2009,anovelinfluenzaA(H1N1)virusappearedinMexico.Itrapidlyacquiredthecharacteristicsofapandemicdisease.Ourobjectiveistopresentacaseseriesofmechanicallyventilatedpatientswithsevereinfluenza,treatedwithasystematicapproach.Methods.Prospective,observational,single-centerstudyinaUniversityHospital.A(H1N1)viruswasconfirmedbyrRT-PCR.Inthisreport,weonlyconsideredpatientsthatrequiredmechanicalventilation(MV).Allpatientsreceivedantibiotics,steroidsandoseltamivirfromthetimeofadmission.Themainstrategiesincorporatedinthesystematicapproachwerealung-protectivestrategy,PEEPadjustedforeachpatient,protocol-guidedsedoanalgesia,restrictivefluidmanagement,weaningprotocol, andprolongedprone ventilation and extracorporealmembraneoxygenation(ECMO)asrescuetherapies.Results.Westudied19patients:age41±13yearsold,APACHEII16±7andSOFA8±4.AllpatientspresentedPaO2/FiO2≤200beforeconnectiontoMV.Theirworstvalueswithinthefirst24hoursforoxygenationindex,PaO2/FiO2,andPaCO2onMVwere21.8±13,98±39,and48±16mmHg,respectively.SixteenpatientsachievedARDS;threeexhibitedacute lung injurycriteria.Tenrequiredaproneposition,andtworequiredECMO(onepatientrequiredboththerapies).TimeonMVwas16±13days.LengthofstayintheICUandinhospitalwas18±12and28±17days,respectively.Mortalitywas21%.Conclusion.Severehypoxemiaandahighrateofrescuetherapieswereobservedamongourpatients.Nevertheless,mortalitywaslowerthanpreviouslyreportedincomparablepopulations,whichmayberelatedtothemanagementbyacriticalcareteamandtheuseofasystematicapproachforventilatoryandnon-ventilatorytherapeuticstrategies.(Minerva Anestesiol 2011;77:510-21)Key words: Respiratorydistresssyndrome,adult-Respiration,artificial-Influenza,human.
MINERVA MEDICA COPYRIGHT®
Thi
s do
cum
ent i
s pr
otec
ted
by in
tern
atio
nal c
opyr
ight
law
s. N
o ad
ditio
nal r
epro
duct
ion
is a
utho
rized
. It i
s pe
rmitt
ed fo
r pe
rson
al u
se to
dow
nloa
d an
d sa
ve o
nly
one
file
and
prin
t onl
y on
e co
py o
f thi
s A
rtic
le. I
t is
not p
erm
itted
to m
ake
addi
tiona
l cop
ies
(eith
er
spor
adic
ally
or
syst
emat
ical
ly, e
ither
prin
ted
or e
lect
roni
c) o
f the
Art
icle
for
any
purp
ose.
It is
not
per
mitt
ed to
dis
trib
ute
the
elec
tron
ic c
opy
of th
e ar
ticle
thro
ugh
onlin
e in
tern
et a
nd/o
r in
tran
et fi
le s
harin
g sy
stem
s, e
lect
roni
c m
ailin
g or
any
oth
er m
eans
whi
ch
may
allo
w a
cces
s to
the
Art
icle
. The
use
of a
ll or
any
par
t of t
he A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed. T
he c
reat
ion
of d
eriv
ativ
e w
orks
from
the
Art
icle
is n
ot p
erm
itted
. The
pro
duct
ion
of r
eprin
ts fo
r pe
rson
al o
r co
mm
erci
al u
se is
not
per
mitt
ed. I
t is
not p
erm
itted
to r
emov
e, c
over
, ove
rlay,
obs
cure
, blo
ck, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost o
n th
e A
rtic
le. I
t is
not p
erm
itted
to fr
ame
or u
se fr
amin
g te
chni
ques
to e
nclo
se a
ny tr
adem
ark,
logo
, or
othe
r pr
oprie
tary
tio
n of
the
Pub
lishe
r.

SYSTEMATICAPPROACHTOSEVERERESPIRATORYFAILUREDUETONOVELA(H1N1)INFLUENZA CORNEJO
Vol.77-No.5 MINERVAANESTESIOLOGICA 511
ityrateinmechanicallyventilatedadultpatientsranged from 20% to 46%.1, 4-10 Most ICUsadoptedalung-protectivestrategysimilartothatrecommendedforacuterespiratorydistresssyn-drome(ARDS) fromothercauses,maintaininglowtidalvolumesandplateaupressures<30-35cmH2O. Nevertheless, A(H1N1) can result inrapidly progressive respiratory failure refractoryto conventional mechanical ventilation (MV).This forced intensivists toemploy sophisticatedMV support and different adjunct therapies,among them: airway pressure released ventila-tion(APRV),highfrequencyoscillatoryventila-tion(HFOV),pronepositionandextracorporealmembraneoxygenation (ECMO).6-11However,thesetherapiescanpotentiallycauseharmifnotimplementedinacoordinatedmannerbyacriti-calcareteamwithadequateexpertiseandinstitu-tionalsupporttofacilitatetimelytreatment.
Bundles applied to different areas of inten-sivecarehavedemonstratedthatsystematicap-proachescanminimizebiasandmedicalerrors,andimproveclinicaloutcomes.11-16Thisconceptpromptedourcriticalcareteamtoassessastrictmultifacetedmanagementprotocol,incorporat-ingevidence-basedstrategiesintheformofven-tilatory and non-ventilatory strategies, to treatthemostseverely ill subsetofpatientswith in-fluenzaA(H1N1)virusinfection.Inthismanu-script,wereportourexperience.
Materials and methods
This observational study was conducted inourcriticalcareservicewhichincludes55beds,12 in ICU and 43 in intermediate care units.AllinfluenzapatientsrequiringMVweretrans-ferred to ICU for management and isolation.Thestudywasapprovedbytheinstitutionalre-viewboardandsurrogatessignedtheirinformedconsent.
Patients
Patientswereclassifiedassuspiciouscasesac-cording to the case definition adopted by theMinistry of Health of Chile,2 as confirmed bytestingrespiratory specimenswithreal-timere-verse transcription-polymerase chain reaction
(rRT-PCR).17BetweenJune13andAugust27,2009, 68 confirmed adult cases were admittedto our hospital, 36 of whom were sent to thecriticalcareservice.Amongthese36patients,19requiredMV(Figure1). Forthepurposeofthisreport, we only considered those patients thatrequiredMV.Patients’medicalrecordswerecol-lectedfortheanalysisofdemographics,clinicalfindings, and outcomes. Septic shock was de-finedaccordingtothesurvivalsepsiscampaigndefinitions.18 Acute Physiology and ChronicHealth Evaluation II score (APACHE II) andSequential Organ Failure Assessment score(SOFA)werecalculatedatICUadmission.19,20
Fromthe timeofhospitaladmission,allpa-tientsreceivedoseltamivir(75mgBIDfor7-10days),ceftriaxonepluslevofloxacin(astreatmentfor severe community-acquired pneumonia),andcorticosteroids(hydrocortisone300mgperday,for7-10days).
Microbiologic studies
Nasopharyngeal-swabspecimenswerecollect-edathospitaladmission,andbronchial-aspiratesampleswereobtainedaftertrachealintubationoncepatientshadenteredtheICU.Inadditionto specific rRT-PCRtesting forA(H1N1), res-piratoryspecimensweretestedwithDFI(DNAfragmentationindex)assayorviralpanel.Bloodand urinary cultures, as well as measurementof urinary antigens of Legionella pneumophilaandStreptococcuspneumoniaewereperformeduponadmissiontothehospital.
Oxygen exchange, respiratory mechanics and me-chanical ventilator settings
The partial pressure of oxygen in arterialblood/fraction of inspired oxygen ratio (PaO2/FiO2)wasmeasuredatthetimeofconnectiontoMV(T0),whichcorrespondstothebeginningof the systematic approach, and at 48 and 72hoursafter(T48andT72,respectively).Inaddi-tion,theworstPaO2:FiO2at12to24hoursafterinitiatingthesystematicapproachwasincluded(T12-24).Tidalvolume(TV),positiveend-ex-piratorypressure(PEEP),plateaupressure,staticcomplianceoftherespiratorysystem(Crs),and
MINERVA MEDICA COPYRIGHT®
Thi
s do
cum
ent i
s pr
otec
ted
by in
tern
atio
nal c
opyr
ight
law
s. N
o ad
ditio
nal r
epro
duct
ion
is a
utho
rized
. It i
s pe
rmitt
ed fo
r pe
rson
al u
se to
dow
nloa
d an
d sa
ve o
nly
one
file
and
prin
t onl
y on
e co
py o
f thi
s A
rtic
le. I
t is
not p
erm
itted
to m
ake
addi
tiona
l cop
ies
(eith
er
spor
adic
ally
or
syst
emat
ical
ly, e
ither
prin
ted
or e
lect
roni
c) o
f the
Art
icle
for
any
purp
ose.
It is
not
per
mitt
ed to
dis
trib
ute
the
elec
tron
ic c
opy
of th
e ar
ticle
thro
ugh
onlin
e in
tern
et a
nd/o
r in
tran
et fi
le s
harin
g sy
stem
s, e
lect
roni
c m
ailin
g or
any
oth
er m
eans
whi
ch
may
allo
w a
cces
s to
the
Art
icle
. The
use
of a
ll or
any
par
t of t
he A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed. T
he c
reat
ion
of d
eriv
ativ
e w
orks
from
the
Art
icle
is n
ot p
erm
itted
. The
pro
duct
ion
of r
eprin
ts fo
r pe
rson
al o
r co
mm
erci
al u
se is
not
per
mitt
ed. I
t is
not p
erm
itted
to r
emov
e, c
over
, ove
rlay,
obs
cure
, blo
ck, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost o
n th
e A
rtic
le. I
t is
not p
erm
itted
to fr
ame
or u
se fr
amin
g te
chni
ques
to e
nclo
se a
ny tr
adem
ark,
logo
, or
othe
r pr
oprie
tary
tio
n of
the
Pub
lishe
r.

CORNEJO SYSTEMATICAPPROACHTOSEVERERESPIRATORYFAILUREDUETONOVELA(H1N1)INFLUENZA
512 MINERVAANESTESIOLOGICA May2011
oxygenationindex(OI)wereregisteredperiodi-cally.OIwascalculatedasmeanairwaypressure(Paw)×FiO2×100/PaO2.
ARDSwasdefinedaccordingtotheAmerican-European Consensus Conference,21 and SevereARDSwasdefinedaspersistenceof anOI≥15and PaO2/FiO2≤100 mmHg, after recruitmentmaneuversandPEEPadjustment.22,37,38
Ventilatory management
Alung-protectivestrategyincludinglowtidalvolume and lowplateaupressureswas applied,according to standard recommendations.23 AllpatientswereventilatedwithaPuritan-Bennett840VentilatorSystem(NellcorPuritanBennett,CA).Aclosedtrachealsuctionsystemwasused.FiO2andrespiratoryrate(RR)wereadjustedtomaintainoxygensaturation≥90%andpH>7.2.
Recruitmentmaneuvers(RM)wereperformedbefore a decremental PEEP trial, using thepressure-controlledmode. ForRM,weused45cmH2Oas total inspiratorypressure (PEEP20
cmH2O+delta-inspiratorypressure25cmH2O),I:Eratio1:1,RR15perminute,for1min.RMwereappliedpredominantlywithinthefirst48hoursofMV,afterhemodynamic stabilization,beforeeachPEEPchange,aftereverydisconnec-tionfromtheventilator,andaftereveryposturalchange(supine–prone).
The PEEP trial was performed by settingPEEPaccordingtoaHickling’smodifiedstrat-egy,24 applying a constant TV and decreasinglevelsofPEEP.PEEPwasreducedprogressivelyfrom20cmH2O,instepsof2cmH2O.A2sec-ond-inspiratorypausewasappliedwitheachre-ductionofPEEP,andCrswascalculated.PEEPlevelwasset(afteranewRM)at2cmH2Oabovethe reduction inPEEP that generated a fall inCrsduringthedecrementalPEEPtrial.
Rescue therapies: prolonged prone ventila-tionandECMOwereusedasrescuetherapies,each applied following established criteria.22, 25Patientsweremaintainedinthepronepositionfor48hoursoruntiltheyreachedanOI≤10ontwoconsecutivemeasurements.Aspecificnurs-
Figure1.—Flowchart.APACHEII:AcutePhysiologyandChronicHealthEvaluationIIscore;8SOFA:SequentialOrganFailureAssessmentscore.9SepticshockwasdefinedaccordingtotheSurvivingSepsisCampaign:Internationalguidelinesformanagementofseveresepsisandsepticshock.23MV:mechanicalventilation;PPV:prolongedproneventilation;ECMO:extracorporealmem-braneoxygenation.Non-invasiveventilationwasusedincasesofchronicobstructivepulmonarydiseaseexacerbation(2patients),congestiveheartfailure(2patients),andhumanimmunodeficiencyvirus(HIV)instageC3(1patient).
APACHE II 10±3SOFA 4±2
Septic shock: 0
APACHE II 16±7SOFA 8±4
Septic shock: 13 patients
Hospitalized patientsN.=68
Medical ward (cohort isolation)N.=32
Critical care serviceN.=36
Intensive care unitsN.=19
All patients were mechanically ventilated
Immediate care unitsN.=17
Survivors: 12 Survivor: 1 Non-survivor: 1Survivors: 5 Survivors: 7Non-survivor: 1
Survivors: 7Non-survivors: 2
Oxygen therapyN.=12
Non-invasive ventilationN.=5
Only protective MVN.=8
PPVN.=9
ECMON.=1
ECMO+PPVN.=1
MINERVA MEDICA COPYRIGHT®
Thi
s do
cum
ent i
s pr
otec
ted
by in
tern
atio
nal c
opyr
ight
law
s. N
o ad
ditio
nal r
epro
duct
ion
is a
utho
rized
. It i
s pe
rmitt
ed fo
r pe
rson
al u
se to
dow
nloa
d an
d sa
ve o
nly
one
file
and
prin
t onl
y on
e co
py o
f thi
s A
rtic
le. I
t is
not p
erm
itted
to m
ake
addi
tiona
l cop
ies
(eith
er
spor
adic
ally
or
syst
emat
ical
ly, e
ither
prin
ted
or e
lect
roni
c) o
f the
Art
icle
for
any
purp
ose.
It is
not
per
mitt
ed to
dis
trib
ute
the
elec
tron
ic c
opy
of th
e ar
ticle
thro
ugh
onlin
e in
tern
et a
nd/o
r in
tran
et fi
le s
harin
g sy
stem
s, e
lect
roni
c m
ailin
g or
any
oth
er m
eans
whi
ch
may
allo
w a
cces
s to
the
Art
icle
. The
use
of a
ll or
any
par
t of t
he A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed. T
he c
reat
ion
of d
eriv
ativ
e w
orks
from
the
Art
icle
is n
ot p
erm
itted
. The
pro
duct
ion
of r
eprin
ts fo
r pe
rson
al o
r co
mm
erci
al u
se is
not
per
mitt
ed. I
t is
not p
erm
itted
to r
emov
e, c
over
, ove
rlay,
obs
cure
, blo
ck, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost o
n th
e A
rtic
le. I
t is
not p
erm
itted
to fr
ame
or u
se fr
amin
g te
chni
ques
to e
nclo
se a
ny tr
adem
ark,
logo
, or
othe
r pr
oprie
tary
tio
n of
the
Pub
lishe
r.

SYSTEMATICAPPROACHTOSEVERERESPIRATORYFAILUREDUETONOVELA(H1N1)INFLUENZA CORNEJO
Vol.77-No.5 MINERVAANESTESIOLOGICA 513
ingcareprotocolwasappliedwhilepatientswerein the prone position.22 ECMO was appliedthroughaveno-venoussystem,andtheCESARguidelinesformanagementandcareofpatientsinECMOwerefollowed.25
Non-ventilatory management
Analgesia-basedsedationwasguidedbypro-tocol: this protocol is based on fentanyl andmidazolam.Dailygoalsof sedationbasedweredefined based on the sedation agitation scale(SAS),26 and doses were adjusted accordingly.Neuromuscular blockagewasusedonly for se-vereARDSpatients.AvalidatedSpanishConfu-sionAssessmentMethod in the IntensiveCareUnit (CAM-ICU)wasapplied fordeliriumdi-agnosiswhenpatientsachievedaSASlevel3.27
Restrictivefluidmanagement: oncehemody-namicstabilitywasachievedandhypoperfusionwasexcluded,weusedrestrictivefluidmanage-ment,similartotheARDS-networkstrategy.28Iffurosemidewas indicated,andplasmaalbuminwas lower than2.5mg/dL,we added albumin(20gQID).
A weaning protocol guided by respiratorytherapists was systematically applied.29 If thepatient satisfied goals of oxygen exchange, res-piratory rate, blood pressure, heart rate andconsciousness,aspontaneousbreathingtrialwasperformed.Ifthetrialwassuccessful,thepatientwasextubated.
Early physical and occupational therapy inmechanically ventilated patients: once clinicalstabilitywasachieved,earlyexerciseandmobi-lizationwereusedinaccordancewitharecentlypublished strategy.30Unresponsivepatientsun-derwent passive range of motion exercises foralllimbs.Forinteractivepatients,activeassisted(withmanualassistance)andactive (independ-ent) range of motion exercises were applied inthe supineposition. If theseexerciseswere tol-erated,treatmentwasadvancedtobedmobilityactivities, including transfer to upright sitting.Critical illness neuromuscular abnormalities(CINMAs)wereperiodicallyevaluated.31
Early percutaneous tracheostomy using thefiberoptic bronchoscopy-assisted Ciaglia BlueRhino technique (Cook Critical Care, Bloom-
ington,IN)32wasconsideredwhenthepredict-edtimeonMVwasmorethan7days.Thispro-tocolalsoincludedthesemirecumbentposition,early enteral feeding, thrombosis prophylaxis,andulcerprevention.
Although the assessment of potentially re-cruitable lungwasnot included aspart of thisprotocol,foursevereARDSpatientsunderwentwhole-lungcomputedtomography(CT)duringbreath-holding sessions at consecutive airwaypressuresof5and45cmH2O,asintheGatti-noniet al.trial.33Imageswereanalyzedmanuallywith Pulmo® software (Siemens). The percent-age of potentially recruitable lung was definedas:(nonaeratedtissue[NAT]at5-NATat45cmH2O)/totalweight.Inthesamepatients,weevaluatedtheeffectofincreasingPEEPfrom5to15cmH2O,withandwithout interposedRM,whilemeasuringarterialbloodgases20minutesafterincreasingPEEP.
Follow-up and outcomes
Time on MV, infectious complications, in-cidence of delirium and CINMAs, use of tra-cheostomy and continuous renal replacementtherapies(CRRT),lengthofstayatICUandathospital,mortality,andone-yearfollow-up,wererecorded.
Statistical analysis
StatisticalanalysiswasperformedusingSPSS17.0 software for Windows. The Kolmogorov-Smirnov test was used to test the normalityof data distributions. Results are expressed asmean±SD, median (IQR), or percentage. Nu-merical variables were compared by Student’st-testorMann-Whitneyranksumtest,andcate-goricalvariableswerecomparedbyFisher’sexacttest.Atwo-sidedpvalue<0.05wasconsideredstatisticallysignificant.
Results
Characteristicsofthe19patientsareshowninTableI. Themeanagewas41±13yearsold;10patientswerefemale.Fifteenpatientshadpreex-istingmedicalconditions,andinfourpatients,
MINERVA MEDICA COPYRIGHT®
Thi
s do
cum
ent i
s pr
otec
ted
by in
tern
atio
nal c
opyr
ight
law
s. N
o ad
ditio
nal r
epro
duct
ion
is a
utho
rized
. It i
s pe
rmitt
ed fo
r pe
rson
al u
se to
dow
nloa
d an
d sa
ve o
nly
one
file
and
prin
t onl
y on
e co
py o
f thi
s A
rtic
le. I
t is
not p
erm
itted
to m
ake
addi
tiona
l cop
ies
(eith
er
spor
adic
ally
or
syst
emat
ical
ly, e
ither
prin
ted
or e
lect
roni
c) o
f the
Art
icle
for
any
purp
ose.
It is
not
per
mitt
ed to
dis
trib
ute
the
elec
tron
ic c
opy
of th
e ar
ticle
thro
ugh
onlin
e in
tern
et a
nd/o
r in
tran
et fi
le s
harin
g sy
stem
s, e
lect
roni
c m
ailin
g or
any
oth
er m
eans
whi
ch
may
allo
w a
cces
s to
the
Art
icle
. The
use
of a
ll or
any
par
t of t
he A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed. T
he c
reat
ion
of d
eriv
ativ
e w
orks
from
the
Art
icle
is n
ot p
erm
itted
. The
pro
duct
ion
of r
eprin
ts fo
r pe
rson
al o
r co
mm
erci
al u
se is
not
per
mitt
ed. I
t is
not p
erm
itted
to r
emov
e, c
over
, ove
rlay,
obs
cure
, blo
ck, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost o
n th
e A
rtic
le. I
t is
not p
erm
itted
to fr
ame
or u
se fr
amin
g te
chni
ques
to e
nclo
se a
ny tr
adem
ark,
logo
, or
othe
r pr
oprie
tary
tio
n of
the
Pub
lishe
r.

CORNEJO SYSTEMATICAPPROACHTOSEVERERESPIRATORYFAILUREDUETONOVELA(H1N1)INFLUENZA
514 MINERVAANESTESIOLOGICA May2011
these were severe comorbidities. Six patientswereobese.ThreepatientsweretransferredfromotherICUsbecauseofsevereARDS;onewasawoman inher fourthpostpartumday.At ICUadmission, eighteen patients satisfied the casedefinition criteria,2 and16 fulfilled the criteriaforARDS.21TheAPACHEII scorewas16±7;SOFA scorewas8±4.Fifteenpatients requiredvasopressor drugs (13 developed septic shock).Timefromillnessonsettoinitiationofantiviraltreatmentwas5.1±2.6days.
Microbiologic studies
Six patients had evidence of influenzaA in-fection, as determined either by viral panel orbyimmunofluorescence.Bacteriallungcoinfec-tionbyStreptococcus pneumoniaewas identifiedinthreepatients.
Chest X-ray and CT findings
Allpatientshadabnormalitiesontheirchestradiographsatadmission(TableI).Onepatient
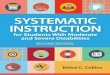
whohadasthmapresentedaspontaneouspneu-momediastinum.High-resolutionCTconfirmedthefindingsrevealedbychestX-rayandrevealedscarringandfibrosisin4patientsatlaterstages(Figure2).Pulmonaryembolismwasidentifiedinonepatient12daysafteradmission.
Oxygen exchange, respiratory mechanics and me-chanical ventilation settings
Time between illness onset and connectionto MV was 6.2±2.6 days. Individual values ofPaO2/FiO2 for the 19 patients atT0,T12-24,T48andT72,aswellasothervariablesofoxy-genationandrespiratorymechanicsareshowninTable II. The worst values for PaO2/FiO2, OI,andPaCO2withinthefirst12to24hoursafterinitiating the systematic approachwere98±39,21.8±13, and 48±16 mmHg, respectively.The PaO2/FiO2 of patients who required andthosewhodidnotrequirerescuetherapieswas93±28and122±33mmHg, respectively, atT0(P=0.079);77±23and128±37mmHgatT12-24 (P=0.002); 154±64 and 242±59 mmHg at
TableI.—Individual characteristics of the 19 patients at ICU admission.
Case(N.)
Age(years)
GenderM/F
ComorbiditiesYes/No
ChestX-ray APACHEII SOFA SS
Yes/NOARDS/ALI*
1 39 M Yes8 Mixed 16 8 No ARDS2 35 F No* Mixed 24 8 Yes ARDS3 58 M Yes1,3 Mixed 19 10 Yes ARDS4 36 M Yes4 Mixed 6 5 Yes ARDS5 18 F Yes2 Mixed 26 15 Yes ARDS6 49 M Yes1 Mixed 12 5 No ARDS7 24 F Yes5 Interstitial 8 3 No ARDS8 36 F No Patchy 10 7 Yes ARDS9 51 M No Patchy 22 9 Yes ARDS10 26 M Yes8 Mixed 8 4 No ARDS11 42 M Yes8 Mixed 11 7 Yes ARDS12 54 M Yes1,8 Mixed 16 7 Yes ARDS13 52 F Yes1,8 Mixed 18 9 Yes ARDS14 63 F Yes1,2,4 Interstitial 27 13 No ALI15 41 F No Patchy 12 7 Yes ALI16 53 M Yes1,6,7 Patchy 11 11 Yes ARDS17 32 M Yes5 Interstitial 11 5 No ALI18 23 F Yes2 Interstitial 25 16 Yes ARDS19 45 F Yes8 Interstitial 24 11 Yes ARDS
Comorbidities:1hypertension,2chronicliverdisease,3orthothopiclivertransplantunderimmunosuppressivetherapy,4diabetesmellitus,5asthma,6chronicrenalfailure,7connectivetissuedisease,8obesity.
*Postpartumwomen.APACHEII:AcutePhysiologyandChronicHealthEvaluationIIscore;8SOFA:SequentialOrganFailureAssessmentscore.9SS:Septicshock.SepticshockwasdefinedaccordingtoSurvivingSepsisCampaign:Internationalguidelinesformanagementofseveresepsisandsepticshock.23ARDS*:acuterespiratorydistresssyndromecriteria,accordingtotheAmerican-EuropeanConsensusConference,10wereevalu-atedafterconnectiontomechanicalventilation.
MINERVA MEDICA COPYRIGHT®
Thi
s do
cum
ent i
s pr
otec
ted
by in
tern
atio
nal c
opyr
ight
law
s. N
o ad
ditio
nal r
epro
duct
ion
is a
utho
rized
. It i
s pe
rmitt
ed fo
r pe
rson
al u
se to
dow
nloa
d an
d sa
ve o
nly
one
file
and
prin
t onl
y on
e co
py o
f thi
s A
rtic
le. I
t is
not p
erm
itted
to m
ake
addi
tiona
l cop
ies
(eith
er
spor
adic
ally
or
syst
emat
ical
ly, e
ither
prin
ted
or e
lect
roni
c) o
f the
Art
icle
for
any
purp
ose.
It is
not
per
mitt
ed to
dis
trib
ute
the
elec
tron
ic c
opy
of th
e ar
ticle
thro
ugh
onlin
e in
tern
et a
nd/o
r in
tran
et fi
le s
harin
g sy
stem
s, e
lect
roni
c m
ailin
g or
any
oth
er m
eans
whi
ch
may
allo
w a
cces
s to
the
Art
icle
. The
use
of a
ll or
any
par
t of t
he A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed. T
he c
reat
ion
of d
eriv
ativ
e w
orks
from
the
Art
icle
is n
ot p
erm
itted
. The
pro
duct
ion
of r
eprin
ts fo
r pe
rson
al o
r co
mm
erci
al u
se is
not
per
mitt
ed. I
t is
not p
erm
itted
to r
emov
e, c
over
, ove
rlay,
obs
cure
, blo
ck, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost o
n th
e A
rtic
le. I
t is
not p
erm
itted
to fr
ame
or u
se fr
amin
g te
chni
ques
to e
nclo
se a
ny tr
adem
ark,
logo
, or
othe
r pr
oprie
tary
tio
n of
the
Pub
lishe
r.

SYSTEMATICAPPROACHTOSEVERERESPIRATORYFAILUREDUETONOVELA(H1N1)INFLUENZA CORNEJO
Vol.77-No.5 MINERVAANESTESIOLOGICA 515
T48(P=0.008);and180±75and242±59mmHgatT72(P=0.011).Inaddition,patientstreatedwithrescuetherapieshadhigherPEEP(14±3vs.10±3 cmH2O, P=0.042); higher plateau pres-sures (28±4 vs. 25±2 cmH2O, P=0.035), andhigherOI(32±12vs.13±7,P=0.001),comparedtopatientswhodidnotrequirerescuetherapies(TableII).
Thepercentageofpotentiallyrecruitablelungobtainedfrom4patientswas30±7%(Figure3).Inthesepatients,performinganRMbeforein-creasingPEEPto15cmH2OresultedinhigherPaO2(168±4vs.109±7mmHg,P=0.027),high-
erPaO2:FiO2(159±3vs.104±2,P=0.015)andlowerOI(12±3vs.18.5P=0.006)thanwhentheincreaseinPEEPwasnotprecededbyanRM.
Rescue therapies
Eleven patients required rescue therapies: tenrequired prolonged prone position and two re-quiredECMO,withonepatientrequiringboththerapies. The time between onset of MV andpronation was 26±27 hours. Patients remainedin the prone position for 82±49 straight hours.Three patients required a second period in the
Figure2.—RadiologicalpatternsofpatientswithsevererespiratoryfailureduetonovelA(H1N1)virusinfection.CTslicesofthethoraxobtainedfrom4patientswithsevererespiratoryfailureexclusivelyduetothenovelinfluenza,showingdifferentradiologicalpatterns:focalandscatteredground-glass(A,case3),unilateralconsolidation(B,case8),bilateralpatchyalveolaropacitiesplusareaswithmixedinterstitial-alveolarpatternconsistentwithARDS(C,case1),andinterstitialthickeningwithpleuralreactionandbronchialdilatationfromapatientwhoevolvedtofibrosis(D,case12).
MINERVA MEDICA COPYRIGHT®
Thi
s do
cum
ent i
s pr
otec
ted
by in
tern
atio
nal c
opyr
ight
law
s. N
o ad
ditio
nal r
epro
duct
ion
is a
utho
rized
. It i
s pe
rmitt
ed fo
r pe
rson
al u
se to
dow
nloa
d an
d sa
ve o
nly
one
file
and
prin
t onl
y on
e co
py o
f thi
s A
rtic
le. I
t is
not p
erm
itted
to m
ake
addi
tiona
l cop
ies
(eith
er
spor
adic
ally
or
syst
emat
ical
ly, e
ither
prin
ted
or e
lect
roni
c) o
f the
Art
icle
for
any
purp
ose.
It is
not
per
mitt
ed to
dis
trib
ute
the
elec
tron
ic c
opy
of th
e ar
ticle
thro
ugh
onlin
e in
tern
et a
nd/o
r in
tran
et fi
le s
harin
g sy
stem
s, e
lect
roni
c m
ailin
g or
any
oth
er m
eans
whi
ch
may
allo
w a
cces
s to
the
Art
icle
. The
use
of a
ll or
any
par
t of t
he A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed. T
he c
reat
ion
of d
eriv
ativ
e w
orks
from
the
Art
icle
is n
ot p
erm
itted
. The
pro
duct
ion
of r
eprin
ts fo
r pe
rson
al o
r co
mm
erci
al u
se is
not
per
mitt
ed. I
t is
not p
erm
itted
to r
emov
e, c
over
, ove
rlay,
obs
cure
, blo
ck, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost o
n th
e A
rtic
le. I
t is
not p
erm
itted
to fr
ame
or u
se fr
amin
g te
chni
ques
to e
nclo
se a
ny tr
adem
ark,
logo
, or
othe
r pr
oprie
tary
tio
n of
the
Pub
lishe
r.

CORNEJO SYSTEMATICAPPROACHTOSEVERERESPIRATORYFAILUREDUETONOVELA(H1N1)INFLUENZA
516 MINERVAANESTESIOLOGICA May2011
proneposition.Onlyminor complicationswereobservedduringpronepositioning:fourpatientsdeveloped grade II pressure ulcers, and one pa-tientdevelopedagradeIIIpressureulcer.ECMOwas started6hoursafteradmission inonecase,andonday3ofMVintheother.ThesepatientsremainedonECMOfor10and9days,respec-tively.Onlythesecondpatientdiedduetomulti-pleorganfailure.
Follow-up and outcomes
Five patients acquired respiratory infectionsduringthehospitalstay.Onepatientdevelopedcandidemia.Twopatientsdevelopedorganizingpneumonia,confirmedbylungbiopsy,andweresuccessfully treated with high-dose corticoster-oids.34Elevenpatientspresenteddelirium,sevendevelopedCINMAs, sixwere tracheostomized,
andfourpatientsrequiredCRRTforacuterenalfailure.
The mean time on MV was 16±13 days.LengthofstayatICUandhospitalwas18±12and28±17days,respectively.Fourpatientsdied,andfifteenweredischarged ingoodcondition.On the follow-upatoneyear,onepatienthadcommitted suicide.The restof thepatients re-mainedingoodcondition.Amongallregisteredparameters, severe comorbidities and SOFAscoreatadmissionweretheonlyfactorsassoci-atedwithmortality(TableIII).
Discussion
AhighfrequencyofsevereARDSwithnovelinfluenzaA(H1N1)virusinfectionwasobservedinthiscaseseries.Morethanhalfofmechanicallyventilatedpatientsrequiredrescuetherapiesdue
TableII.—Clinical variables before and after rescue therapies, and outcome of the 19 patients.
Cases (N.)PaO2/FiO2(mmHg) TV€
(ml/kg)PEEP*
(cmH2O)Plateau¶
(cmH2O)Crs#
(ml/cm/cmH2O)
OI∞ NEdose&
(μg/kg/min)
RT(Yes/No)
VM(days)
UCI(days)
Outcome(S/NS) T0 T12-24 T48 T72
1 116 60 274 327 6.5 17 29 46 36,3 - Yes(1) 25 27 S2 NA 52 85 102 6.3 18 30 29 42,3 0.32 Yes(2) 21 21 S3 60 83 116 176 6.4 10 20 45 18,3 0.13 Yes(1) 15 15 NS4 131 119 158 144 6.7 16 28 40 16.9 0.12 Yes(1) 31 33 S5 101 49 64 86 5.1 14 31 15 51.4 0.35 Yes(1.2) 11 11 NS6 70 101 124 145 6.2 11 29 30 18.8 - Yes(1) 39 10 NS7 120 90 161 134 6.7 8 26 20 ,38.9 - No 37 36 S8 110 129 341 330 7.2 12 28 28 11.6 0.08 No 37 12 S9 148 98 217 266 6.7 10 22 41 12.2 0.28 No 14 14 S10 93 81 173 218 6.9 10 21 54 18.7 - Yes(1) 11 13 S11 117 102 186 228 5.9 14 28 31 21,3 0.08 Yes(1) 39 12 S12 NA 84 165 145 5.7 16 31 27 20.3 0.13 Yes(1) 50 51 S13 48 65 105 132 6.5 18 30 32 35.5 0.13 Yes(1) 38 39 S14 NA 200 254 380 7.1 13 28 28 37.5 0.05 No 38 39 S15 148 159 215 340 6.6 11 25 37 38.1 0.13 No 33 38 S16 68 99 215 222 6.3 14 26 40 18.1 0.12 No 33 12 S17 165 138 315 348 7.1 6 22 33 8, 0.05 No 34 35 S18 99 115 221 258 6.3 13 26 24 18,3 0.13 No 38 38 NS19 104 49 247 285 5.7 10 33 13 43,3 0.43 Yes(1) 24 28 SMean±SD 106±33 98±39 191±75 224±92 6.5±0,5 12.7±3 27±3 32±10 21.8±13 0.15±0.1 16±13 18±12
PaO2/FiO2:partialpressureofoxygeninarterialblood/inspiredoxygenfractionratiowasmeasuredatthetimeofconnectiontomechanicalventilationandinitiationthesystematicapproach(T0)andat48and72hoursafterinitiationofthesystematicapproach(T48andT72.respectively).Inaddition:theworstPaO2/FiO2.betweenthefirst12to24hoursafterinitiatingthesystematicapproachwasincluded(T12-24).TV:meantidalvolumeemployedinthefirst72hours;PEEP:highestpositiveend-expiratorypressure;Plateau:highestplateaupressure;OI:highestoxygenationindex;Crs:lowestcomplianceoftherespira-torysystem;NEdose:highestnorepinephrinedose;RT:rescuetherapies,1:prolongedproneventilation,2:extracorporealmembraneoxygenation;MV:timeonmechanicalventilation;ICU:lengthatintensivecareunit;S:survivors.NS:non-survivors.NA:Datafromthreepatientswerenotavailable:twoofthemweretransferredfromotherscenters.
MINERVA MEDICA COPYRIGHT®
Thi
s do
cum
ent i
s pr
otec
ted
by in
tern
atio
nal c
opyr
ight
law
s. N
o ad
ditio
nal r
epro
duct
ion
is a
utho
rized
. It i
s pe
rmitt
ed fo
r pe
rson
al u
se to
dow
nloa
d an
d sa
ve o
nly
one
file
and
prin
t onl
y on
e co
py o
f thi
s A
rtic
le. I
t is
not p
erm
itted
to m
ake
addi
tiona
l cop
ies
(eith
er
spor
adic
ally
or
syst
emat
ical
ly, e
ither
prin
ted
or e
lect
roni
c) o
f the
Art
icle
for
any
purp
ose.
It is
not
per
mitt
ed to
dis
trib
ute
the
elec
tron
ic c
opy
of th
e ar
ticle
thro
ugh
onlin
e in
tern
et a
nd/o
r in
tran
et fi
le s
harin
g sy
stem
s, e
lect
roni
c m
ailin
g or
any
oth
er m
eans
whi
ch
may
allo
w a
cces
s to
the
Art
icle
. The
use
of a
ll or
any
par
t of t
he A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed. T
he c
reat
ion
of d
eriv
ativ
e w
orks
from
the
Art
icle
is n
ot p
erm
itted
. The
pro
duct
ion
of r
eprin
ts fo
r pe
rson
al o
r co
mm
erci
al u
se is
not
per
mitt
ed. I
t is
not p
erm
itted
to r
emov
e, c
over
, ove
rlay,
obs
cure
, blo
ck, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost o
n th
e A
rtic
le. I
t is
not p
erm
itted
to fr
ame
or u
se fr
amin
g te
chni
ques
to e
nclo
se a
ny tr
adem
ark,
logo
, or
othe
r pr
oprie
tary
tio
n of
the
Pub
lishe
r.

SYSTEMATICAPPROACHTOSEVERERESPIRATORYFAILUREDUETONOVELA(H1N1)INFLUENZA CORNEJO
Vol.77-No.5 MINERVAANESTESIOLOGICA 517
torefractoryhypoxemia.Nevertheless,observedmortalitywaslowerthanpredictedaccordingtoARDS severity and comparable with the low-estmortalityratesobtainedindevelopedcoun-
tries.6-8Theseresultsmayberelatedtomanage-mentbyanintensivecareteamwithexperienceinsevereARDSandsystematicuseofventilatoryand non-ventilatory strategies. Although the
Figure3.—Potentiallyrecruitablelung:chestCTimagesobtainedduringbreath-holdingsessionsatconsecutiveairwaypressuresof5and45cmH2O,withthepatientinthesupineposition.Thepercentageofpotentiallyrecruitablelungwasdefinedastheproportionoflungtissueinwhichaerationisrestoredwhenincreasingairwaypressuresfrom5to45cmH20.13CTslicesofthelungobtained2cmabovethediaphragmdomeatairwaypressuresof5cmH20(left)and45cmH20(right)fromtwopatientswithARDSduetothenovelinfluenzavirus.Thepercentageofpotentiallyrecruitablelungwas35%inpatientA(case4),and30%inpatientB(case16).
MINERVA MEDICA COPYRIGHT®
Thi
s do
cum
ent i
s pr
otec
ted
by in
tern
atio
nal c
opyr
ight
law
s. N
o ad
ditio
nal r
epro
duct
ion
is a
utho
rized
. It i
s pe
rmitt
ed fo
r pe
rson
al u
se to
dow
nloa
d an
d sa
ve o
nly
one
file
and
prin
t onl
y on
e co
py o
f thi
s A
rtic
le. I
t is
not p
erm
itted
to m
ake
addi
tiona
l cop
ies
(eith
er
spor
adic
ally
or
syst
emat
ical
ly, e
ither
prin
ted
or e
lect
roni
c) o
f the
Art
icle
for
any
purp
ose.
It is
not
per
mitt
ed to
dis
trib
ute
the
elec
tron
ic c
opy
of th
e ar
ticle
thro
ugh
onlin
e in
tern
et a
nd/o
r in
tran
et fi
le s
harin
g sy
stem
s, e
lect
roni
c m
ailin
g or
any
oth
er m
eans
whi
ch
may
allo
w a
cces
s to
the
Art
icle
. The
use
of a
ll or
any
par
t of t
he A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed. T
he c
reat
ion
of d
eriv
ativ
e w
orks
from
the
Art
icle
is n
ot p
erm
itted
. The
pro
duct
ion
of r
eprin
ts fo
r pe
rson
al o
r co
mm
erci
al u
se is
not
per
mitt
ed. I
t is
not p
erm
itted
to r
emov
e, c
over
, ove
rlay,
obs
cure
, blo
ck, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost o
n th
e A
rtic
le. I
t is
not p
erm
itted
to fr
ame
or u
se fr
amin
g te
chni
ques
to e
nclo
se a
ny tr
adem
ark,
logo
, or
othe
r pr
oprie
tary
tio
n of
the
Pub
lishe
r.

CORNEJO SYSTEMATICAPPROACHTOSEVERERESPIRATORYFAILUREDUETONOVELA(H1N1)INFLUENZA
518 MINERVAANESTESIOLOGICA May2011
limitednumberofpatientsdoesnotallowmajorconclusionstobedrawn,webelievethatasimi-larstrategycouldbeusedtotreatseverecasesofA(H1N1)influenzainothercountries.
Asinrecentpublications,patientswereyoungadultsandpreviouslyhealthyorobese,withoutany risk factor for complications of seasonalinfluenza.1,3-11Notably,allofourdeceasedpa-tientshadcomorbidities.Mostpatientsreceivedvasopressordrugs,butonlyaminorityrequiredhigh-dose norepinephrine. Patients had pro-longed ICUstay and timeofMV,aswell as ahighrateofrespiratoryinfections,delirium,andCINMAs.Thiswasprobablyduetosevereandprolongedrespiratoryfailure.
We systematically applied a lung-protectivestrategyinanattempttoachieve6ml/kgofTVandplateaupressures≤30cmH2O.However,insomepatients,despiteourbestefforts,wewereunabletomaintaintheseparameterswithintherecommended limits23 before theuse of rescuetherapies (TableII).RMwasperformedbeforesettingPEEPtooptimizeoxygenexchangeandas part of a physiologic approach to set PEEP.
Although the use of higher PEEP levels inARDShasbeenassociatedwithlowerincidenceofrefractoryhypoxemiaandlessneedofrescuetherapies,itmaybeuselessifnotappliedonanindividualbasis.35Apparently,higherPEEPlev-els shouldbe reserved forARDSpatientswithabundantpulmonaryedema,collapse,andlungrecruitability.33, 36 Indeed, in this series, thosepatientswithhighpotentially recruitable lung,as assessedbyCTscan, requiredhigh levelsofPEEP(14-18cmH2O).
Given thatmortality riskof themost severeinfluenzapatientsseemstobehigherwhennottreatedwithrescuetherapies1,5,10andthatdif-ferent advanced therapies are difficult to com-pare in a pandemic context, the implementa-tionoffeasible,reproducibleandsafestrategiesasdeterminedbythelocalresourcesavailableismandatory.Afewyearsago,weimplementedanalgorithmforthemanagementofpatientswithsevereARDS,withprolongedproneventilationasthecornerstoneoftreatment.22Proneventila-tionisafeasible,relativelysafeandinexpensivetherapy, which results in better oxygenation,
TableIII.—Comparison of clinical variables between survivors and non-survivors.
Variables NS,n=4 S,n=15 p
Age(years) 37±20 42±11 0,480Gender(Male:Female) 2:2 7:8 0,910BMI(kg/m2) 22.2±5.4 28.8±6.4 0,076Comorbidities 4/4 7/15 0,103Severecomorbidities 3/4 1/15 0,016Timetotreatment(days) 3±2 5.6±2 0,063TimetoMV(days) 4.3±1.5 6.7±2.7 0,104APACHEII 21±6 15±7 0,155SOFA 12±5 8±3 0,05WBCx(10x3/mm3) 15±5 10.9±9 0,407Plateletsx(10x3/mm3) 170±96 188±147 0,821LDH(U/l) 881±315 1218±596 0,297CRP(mg/l) 85±31 211±149 0,1151PaO2/FiO2(mmHg) 82±20 114±33 0,1012PaO2/FiO2(mmHg) 87±29 101±42 0,527OI 26.6±16.6 20.5±12.6 0,434Rescuetherapies 3/4 4/15 0,603BMI:bodymass index;Severe comorbiditiesweredefinedaccordingAcutePhysiologyandChronicHealthEvaluation II score (APACHEII)criteria.17Time to treatment:Timebetweenonset illness andOseltamivir treatment;Time toMV:Timebetweenonset illness andmechanicalventilation;SOFA:Sequential Organ Failure Assessment score.9 WBC: white blood cells;LDH:lactate dehydrogenase; CRP:C-reactive protein;1PaO2:FiO2beforeconnectiontomechanicalventilationandinitiationofofthesystematicapproach;2PaO2/FiO2:partialpressureofoxygeninarterialblood/inspiredoxygenfractionratioworstvaluesbetweenthefirst12to24hafterinitiatingthesystematicapproach.OI:oxygenationindexmeasuredatthesametimethan2PaO2/FiO2
MINERVA MEDICA COPYRIGHT®
Thi
s do
cum
ent i
s pr
otec
ted
by in
tern
atio
nal c
opyr
ight
law
s. N
o ad
ditio
nal r
epro
duct
ion
is a
utho
rized
. It i
s pe
rmitt
ed fo
r pe
rson
al u
se to
dow
nloa
d an
d sa
ve o
nly
one
file
and
prin
t onl
y on
e co
py o
f thi
s A
rtic
le. I
t is
not p
erm
itted
to m
ake
addi
tiona
l cop
ies
(eith
er
spor
adic
ally
or
syst
emat
ical
ly, e
ither
prin
ted
or e
lect
roni
c) o
f the
Art
icle
for
any
purp
ose.
It is
not
per
mitt
ed to
dis
trib
ute
the
elec
tron
ic c
opy
of th
e ar
ticle
thro
ugh
onlin
e in
tern
et a
nd/o
r in
tran
et fi
le s
harin
g sy
stem
s, e
lect
roni
c m
ailin
g or
any
oth
er m
eans
whi
ch
may
allo
w a
cces
s to
the
Art
icle
. The
use
of a
ll or
any
par
t of t
he A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed. T
he c
reat
ion
of d
eriv
ativ
e w
orks
from
the
Art
icle
is n
ot p
erm
itted
. The
pro
duct
ion
of r
eprin
ts fo
r pe
rson
al o
r co
mm
erci
al u
se is
not
per
mitt
ed. I
t is
not p
erm
itted
to r
emov
e, c
over
, ove
rlay,
obs
cure
, blo
ck, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost o
n th
e A
rtic
le. I
t is
not p
erm
itted
to fr
ame
or u
se fr
amin
g te
chni
ques
to e
nclo
se a
ny tr
adem
ark,
logo
, or
othe
r pr
oprie
tary
tio
n of
the
Pub
lishe
r.

SYSTEMATICAPPROACHTOSEVERERESPIRATORYFAILUREDUETONOVELA(H1N1)INFLUENZA CORNEJO
Vol.77-No.5 MINERVAANESTESIOLOGICA 519
more homogeneous distribution of aeration,and probably reduces lung stress and strain inearly ARDS.37, 38 Although the impact of pro-longed prone ventilation on the most relevantclinical outcomes remains to be demonstrated,some meta-analyses suggest that only patientswithsevereARDS,39,40suchasthepatientsthatreceived prone ventilation in our series, couldbenefitfromthistherapy.
From the timeof admission to the ICU, allpatients received antiviral drugs, antibioticsand corticosteroids and were treated with sev-eral evidence-based strategies included in thenon-ventilatory approach to patient manage-ment.Theroleofcorticosteroidsinthissettingis unclear and controversial.Two patientswhodevelopedorganizingpneumonia responded tohigh-dosecorticosteroids.34 Inaddition, allpa-tientsreceivedhydrocortisone300mg/dayfromthetimeofadmission.ThesedosesdonotseemtoincreasetherisksandmightbehelpfulinALI/ARDS.41Therealcontributionofcorticosteroidstotheoutcomeof influenzapatientsshouldbefurtherevaluatedinalargerseries.
The implementationofaprotocolwithven-tilatoryandnon-ventilatorystrategieswasbasedontheobservationthatthemosteffectiveinter-ventionsinICUseemtobemultifaceted.Thereisevidencedemonstratingthebenefitofbundlesindifferentcontexts,suchasventilator-associat-edpneumonia,12,13catheter-relatedbloodstreaminfections,14 sedation, 15 and 6-hour and 24-hoursepsiscarebundles.16However,bundlesarenotuniversallysuccessful.Lackofresources,lowcompliancerateandlowadherencearesomeofthereasonsforthislackofsuccess.Additionally,skepticsofwhattheycall“protocol-basedmedi-cine”areconcernedthatthesemaysupplantclin-ical judgment, creatingcomplacencyandmak-ing learning more difficult. However, far fromimpedingthedevelopmentofclinicalexpertise,bundles are therapeutic tools to facilitate deci-sionmakingusingthebestavailableevidence,al-lowingvaluabletimeforassessingclinicaldetailsandreasoningonacase-by-casebasis.
Ourstudyhasthelimitationsofasingle-cent-er case series focused only on the most severesubgroup of patients with influenza A(H1N1)requiring MV. However, the study has several
strengths:applicationofauniformandsystem-aticapproachtoventilatoryandnon-ventilatorytherapies,avoidanceofadelayininitiatingpo-tential life-saving maneuvers; prolonged proneposition, an inexpensive and highly availabletherapy,asthecornerstoneofadvancedtherapy;andone-yearfollow-up.
For abriefperiodof time,our12 ICUbedsharboredonlysevereinfluenzapatients,withtwooftheminECMOandsixintheproneventila-tionatthesametime.Itisdifficulttoinferben-efits directly related to this systematic approachand even more difficult to compare our resultswith those obtained by other groups that usedmainlyECMOasrescuetherapy6duetobaselinedifferencesinusualcare,thepotentialforselectionbiasanddifferencesbetweengroups.However,webelieve thatourstrictmultifacetedmanagementprotocolwassafe,useful,andhelpfulinovercom-ing the difficulties inherent to the treatment ofseverelyillpatientsinthecontextofapandemic.
Conclusions
Severehypoxemiawithahighrequirementforrescuetherapieswasobservedinourcriticallyillinfluenza patients. Nevertheless, mortality waslower than previously reported in comparablepopulations,whichmayberelatedtotheman-agementby a critical care teamand systematicuseofventilatoryandnon-ventilatorystrategies.Theseresultsshouldbeviewedwithcautionduetothelimitednumberofpatientsandlackofacontrolgroup.
References
1. Perez-PadillaR,delaRosa-ZamboniD,PoncedeLeonS,HernandezM,Quiñones-FalconiF,BautistaE et al.Pneu-moniaandrespiratoryfailurefromswine-origininfluenzaA(H1N1)inMexico.NEnglJMed2009;361:680-9.
2. MinisteriodeSalud.GobiernodeChile.InfluenzaPandé-mica(H1N1)2009[Internet].Availablefromhttp://www.minsal.cl[cited2011,Mar2].
3. MillerRR3rd,MarkewitzBA,RolfsRT,BrownSM,Das-combKK,GrissomCK et al.Clinicalfindingsanddemo-graphic factors associated with ICU admission in Utahdue to novel 2009 influenza A(H1N1) infection. Chest2010;137:752-8.
4. Intensive-Care Patients With Severe Novel Influenza A(H1N1)Virus Infection. Michigan, June 2009. MMWRJuly10,2009/58(Dispatch);1-4.
5. Domínguez-Cherit G, Lapinsky S, Macias A, Pinto R,
MINERVA MEDICA COPYRIGHT®
Thi
s do
cum
ent i
s pr
otec
ted
by in
tern
atio
nal c
opyr
ight
law
s. N
o ad
ditio
nal r
epro
duct
ion
is a
utho
rized
. It i
s pe
rmitt
ed fo
r pe
rson
al u
se to
dow
nloa
d an
d sa
ve o
nly
one
file
and
prin
t onl
y on
e co
py o
f thi
s A
rtic
le. I
t is
not p
erm
itted
to m
ake
addi
tiona
l cop
ies
(eith
er
spor
adic
ally
or
syst
emat
ical
ly, e
ither
prin
ted
or e
lect
roni
c) o
f the
Art
icle
for
any
purp
ose.
It is
not
per
mitt
ed to
dis
trib
ute
the
elec
tron
ic c
opy
of th
e ar
ticle
thro
ugh
onlin
e in
tern
et a
nd/o
r in
tran
et fi
le s
harin
g sy
stem
s, e
lect
roni
c m
ailin
g or
any
oth
er m
eans
whi
ch
may
allo
w a
cces
s to
the
Art
icle
. The
use
of a
ll or
any
par
t of t
he A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed. T
he c
reat
ion
of d
eriv
ativ
e w
orks
from
the
Art
icle
is n
ot p
erm
itted
. The
pro
duct
ion
of r
eprin
ts fo
r pe
rson
al o
r co
mm
erci
al u
se is
not
per
mitt
ed. I
t is
not p
erm
itted
to r
emov
e, c
over
, ove
rlay,
obs
cure
, blo
ck, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost o
n th
e A
rtic
le. I
t is
not p
erm
itted
to fr
ame
or u
se fr
amin
g te
chni
ques
to e
nclo
se a
ny tr
adem
ark,
logo
, or
othe
r pr
oprie
tary
tio
n of
the
Pub
lishe
r.

CORNEJO SYSTEMATICAPPROACHTOSEVERERESPIRATORYFAILUREDUETONOVELA(H1N1)INFLUENZA
520 MINERVAANESTESIOLOGICA May2011
Espinosa-PérezL,delaTorreA et al.CriticallyIllPatientsWith2009InfluenzaA(H1N1)inMexico.JAMAJAMA.2009;302:1880-7.
6. KumarA,ZarychanskiR,PintoR,CookDJ,Marshall J,LacroixJ et al.CriticallyIllPatientsWith2009InfluenzaA(H1N1)inCanada.JAMA.2009;302:1872-9.
7. Davies A, Jones D, Bailey M, Beca J, Bellomo R, Black-wellN et al.TheAustraliaandNewZealandExtracorporealMembrane Oxygenation (ANZ ECMO) Influenza Inves-tigators*ExtracorporealMembraneOxygenationfor2009InfluenzaA(H1N1)AcuteRespiratoryDistressSyndrome.JAMA.2009;302:1888-95.
8. RelloJ,RodríguezA,IbañezP,SociasL,CebrianJ,MarquesA. et al.IntensivecareadultpatientswithsevererespiratoryfailurecausedbyInfluenzaA(H1N1)inSpain.CritCare2009;13:R148.
9. RodríguezA,SocíasL,GuerreroJE,FigueiraJC,GonzálezN, Maraví-Poma E et al. Grupo Español de Trabajo deGripeAGrave/SociedadEspañoladeMedicina Intensiva,Crítica yUnidadesCoronarias. [Pandemic influenzaA inthe ICU:experience in Spain and Latin America. GET-GAG/SEMICYUC/(Spanish Working Group on SeverePandemic Influenza A/SEMICYUC)]. Med Intensiva2010;34:87-94.
10. Estenssoro E, Ríos FG, Apezteguía C, Reina R, NeiraJ, Ceraso DH et al. Registry of the Argentinian Societyof Intensive Care SATI. Pandemic 2009 influenza A inArgentina:a study of 337 patients on mechanical ventila-tion.AmJRespirCritCareMed.2010;182:41-8.
11. GrasselliG,FotiG,PatronitiN,GiuffridaA,CortinovisB,ZanellaAet al.AcaseofARDSassociatedwithinfluenzaA-H1N1infectiontreatedwithextracorporealrespiratorysupport.MinervaAnestesiol2009;75:741-5.
12. HaweCS,EllisKS,CairnsCJ,LongmateA.Reductionofventilator-associatedpneumonia:activeversuspassiveguide-lineimplementation.IntensiveCareMed2009;35:1180-6.
13. BirdD,ZambutoA,O’DonnellC,SilvaJ,KornC,BurkeR et al.Adherencetoventilator-associatedpneumoniabun-dleandincidenceofventilator-associatedpneumoniainthesurgicalintensivecareunit.ArchSurg.2010;145:465-70.
14. PronovostP,NeedhamD,BerenholtzS,SinopoliD,ChuH,CosgroveS et al.Aninterventiontodecreasecatheter-relatedbloodstreaminfectionsintheICU.NEnglJMed2006;355:2725-32.
15. MorandiA,WatsonPL,TrabucchiM,ElyEW.Advancesin sedation for critically ill patients. Minerva Anestesiol.2009;75:385-91.
16. GaoF,MelodyT,DanielsDF,GilesS,FoxS.Theimpactofcompliancewith6-hourand24-hoursepsisbundlesonhospitalmortalityinpatientswithseveresepsis:aprospec-tiveobservationalstudy.CritCare2005;9:R764-R770.
17. CDCprotocolofrealtimeRTPCRforinfluenzaA(H1N1).Geneva: World Health Organization, April 2009 [Inter-net].Availabefrom,athttp://www.who.int/csr/resources/publications/swineflu/CDCRealtimeRTPCR_SwineH1As-say-2009_20090430.pdf[cited2011,Mar2].
18. DellingerRP,LevyMM,Carlet JM,BionJ,ParkerMM,JaeschkeR et al.SurvivingSepsisCampaign:Internationalguidelines for management of severe sepsis and septicshock:2008.IntensiveCareMed2008;34:17-60.
19. Knaus WA, Draper EA, Wagner DP, Zimmermann JE.APACHEII:aseverityofdiseaseclassificationsystem.CritCareMed1985;10:818-29.
20. Vincent JL, de Mendonça A, Cantraine F, Moreno R,TakalaJ,SuterPM et al.UseoftheSOFAscoretoassesstheincidenceoforgandysfunction/failureinintensivecareunits:results of a multicenter, prospective study. Workinggroupon“sepsis-relatedproblems”oftheEuropeanSocietyofIntensiveCareMedicine.CritCareMed1998;26:1793-800.
21. Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K,
HudsonL et al.TheAmerican-EuropeanConsensusCon-ferenceonARDS.Definitions,mechanisms,relevantout-comes, and clinical trial coordination. Am J Respir CritCareMed1994;149:818-24.
22. RomeroCM,CornejoR,GálvezLR,LlanosOP,TobarE,BerasaínMA et al.Extendedpronepositionventilationinsevereacuterespiratorydistresssyndrome:apilotfeasibilitystudy.JCritCare2009;24:81-8.
23. TheAcuteRespiratoryDistressSyndromeNetwork*.Venti-lationwithlowertidalvolumesascomparedwithtraditionaltidalvolumesforAcuteLungInjuryandtheAcuteRespira-toryDistressSyndrome.NEnglJMed2000;342:1301-8.
24. HicklingKG.Bestcomplianceduringadecremental,butnotincremental,positiveend-expiratorypressuretrialisre-lated to openlung positive end-expiratory pressure. Am JRespirCritCareMed2001;163:69-78.
25. PeekGJ,MugfordM,TiruvoipatiR,WilsonA,AllenE,Thalanany MM et al. Efficacy and economic assessmentof conventional ventilatory support versus extracorporealmembraneoxygenationforsevereadultrespiratory failure(CESAR):a multicentre randomised controlled trial. Lan-cet.2009;374:1351-63.
26. RikerRR,PicardJT,FraserGL.ProspectiveevaluationoftheSedation-AgitationScaleforadultcriticallyillpatients.CritCareMed1999;27:1325-9.
27. TobarE,RomeroCM,GalleguillosT.FuentesP,CornejoR,LiraMT et al.ConfusionassessmentmethodforICUpatients (CAM-ICU) for delirium diagnosis:Cultural Ad-aptationandValidationforSpanishversion.MedIntensiva2010;34:4-13.
28. WiedemannHP,WheelerAP,BernardGR,ThompsonBT,HaydenD,deBoisblancB et al.TheNationalHeart,Lung,andBlood InstituteAcuteRespiratoryDistressSyndrome(ARDS)ClinicalTrialsNetwork,Comparisonoftwofluid-management strategies in acute lung injury. New Engl JMed2006;354:2564-75.
29. ElyEW,BennettPA,BowtonDL,MurphySM,FloranceAM, and Haponik EF. Large Scale Implementation of aRespiratoryTherapist–drivenProtocolforVentilatorWean-ing.AmJRespirCritCareMed1999;159:439-46.
30. Schweickert WD, Pohlman MC, Pohlman AS, Nigos C,PawlikAJ,EsbrookCL. et al.Earlyphysicalandoccupation-altherapyinmechanicallyventilated,criticallyillpatients:arandomisedcontrolledtrial.Lancet2009;373:1874-82.
31. DeJongheB,SharsharT,LefaucheurJP,AuthierFJ,Du-rand-ZaleskiI,BoussarsarM et al.Paresisacquiredintheintensivecareunit:aprospectivemulticenterstudy.JAMA2002;288:2859-67.
32. RomeroCM,MarambioA,LarrondoJ,WalkerK,LiraMT,TobarE et al.Swallowingdysfunctioninnon-neurologicalcriticallyillpatientswhorequirepercutaneousdilatationaltracheostomy.CHEST2010;137:1278-82.
33. GattinoniL,CaironiP,CressoniM,ChiumelloD,RanieriVM,QuintelM et al.Lung recruitment inpatientswiththe acute respiratory distress syndrome. N Engl J Med2006;354:1775-86.
34. Cornejo R, Llanos OP, Fernández C, Díaz JC, CardemilG,SalgueroJ et al.OrganizingpneumoniainpatientswithsevererespiratoryfailureduetonovelA(H1N1)influenza.BMJCaseReports2010;doi:10.1136/bcr.02.2010.2708
35. BrielM,MeadeM,MercatA,BrowerRG,TalmorD,Wal-terSD et al.Highervslowerpositiveend-expiratorypres-sure inpatientswith acute lung injury andacute respira-torydistresssyndrome:systematicreviewandmeta-analysis.JAMA2010;303:865-73.
36. CaironiP,CressoniM,ChiumelloD,RanieriM,QuintelM,RussoSG et al.Lungopeningandclosingduringven-tilationofacuterespiratorydistresssyndrome.AmJRespirCritCareMed.2010;181:578-86.
37. GattinoniL,ValenzaF,PelosiP,MascheroniD.Pronepo-sitioninginacuterespiratoryfailure.In:TobinMJ,editor,
MINERVA MEDICA COPYRIGHT®
Thi
s do
cum
ent i
s pr
otec
ted
by in
tern
atio
nal c
opyr
ight
law
s. N
o ad
ditio
nal r
epro
duct
ion
is a
utho
rized
. It i
s pe
rmitt
ed fo
r pe
rson
al u
se to
dow
nloa
d an
d sa
ve o
nly
one
file
and
prin
t onl
y on
e co
py o
f thi
s A
rtic
le. I
t is
not p
erm
itted
to m
ake
addi
tiona
l cop
ies
(eith
er
spor
adic
ally
or
syst
emat
ical
ly, e
ither
prin
ted
or e
lect
roni
c) o
f the
Art
icle
for
any
purp
ose.
It is
not
per
mitt
ed to
dis
trib
ute
the
elec
tron
ic c
opy
of th
e ar
ticle
thro
ugh
onlin
e in
tern
et a
nd/o
r in
tran
et fi
le s
harin
g sy
stem
s, e
lect
roni
c m
ailin
g or
any
oth
er m
eans
whi
ch
may
allo
w a
cces
s to
the
Art
icle
. The
use
of a
ll or
any
par
t of t
he A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed. T
he c
reat
ion
of d
eriv
ativ
e w
orks
from
the
Art
icle
is n
ot p
erm
itted
. The
pro
duct
ion
of r
eprin
ts fo
r pe
rson
al o
r co
mm
erci
al u
se is
not
per
mitt
ed. I
t is
not p
erm
itted
to r
emov
e, c
over
, ove
rlay,
obs
cure
, blo
ck, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost o
n th
e A
rtic
le. I
t is
not p
erm
itted
to fr
ame
or u
se fr
amin
g te
chni
ques
to e
nclo
se a
ny tr
adem
ark,
logo
, or
othe
r pr
oprie
tary
tio
n of
the
Pub
lishe
r.

SYSTEMATICAPPROACHTOSEVERERESPIRATORYFAILUREDUETONOVELA(H1N1)INFLUENZA CORNEJO
Vol.77-No.5 MINERVAANESTESIOLOGICA 521
Principlesandpracticesofmechanicalventilation.2ndedi-tion.NewYork:McGraw-Hill;2006.p.1081-92.
38. GaliatsouE,KostantiE,SvarnaE,KitsakosA,KoulourasV,EfremidisSC. et al.Pronepositionaugmentsrecruitmentandpreventsalveolaroverinflationinacutelunginjury.AmJRespirCritCareMed2006;174:187-97
39. SudS,FriedrichJO,TacconeP,PolliF,AdhikariNK,LatiniR et al.Proneventilationreducesmortalityinpatientswithacute
respiratoryfailureandseverehypoxemia:systematicreviewandmeta-analysis.IntensiveCareMed2010;36:585-99.
40. Gattinoni L, Carlesso E, Taccone P, Polli F, Guérin C,ManceboJ.Pronepositioning improves survival in severeARDS:a pathophysiologic review and individual patientmeta-analysis.MinervaAnestesiol2010;76:448-54.
41. ThompsonBT.CorticosteroidsforARDS.MinervaAneste-siol2010;76:441-7.
Conflicts of interest.—Theauthorsdeclarethattheyhavenocompetinginterests.Acknowledgments.—WethankDr.AlejandroBruhnforhiscriticalcommentsandsuggestions,aswellasthenurses,respiratorytherapists,medicalstaffandauthoritiesfromHospitalClínicoUniversidaddeChilefortheirsupportandcooperation.Funding.—PartiallyfundedbyResearchGrantFondecytNº.11070156,Chileangov.ReceivedonMarch29,2010-AcceptedforpublicationonMarch2,2011.Correspondingauthor:R.CornejoMD,SantosDumont999,Independencia,Santiago,Chile.E-mail:[email protected]
MINERVA MEDICA COPYRIGHT®
Thi
s do
cum
ent i
s pr
otec
ted
by in
tern
atio
nal c
opyr
ight
law
s. N
o ad
ditio
nal r
epro
duct
ion
is a
utho
rized
. It i
s pe
rmitt
ed fo
r pe
rson
al u
se to
dow
nloa
d an
d sa
ve o
nly
one
file
and
prin
t onl
y on
e co
py o
f thi
s A
rtic
le. I
t is
not p
erm
itted
to m
ake
addi
tiona
l cop
ies
(eith
er
spor
adic
ally
or
syst
emat
ical
ly, e
ither
prin
ted
or e
lect
roni
c) o
f the
Art
icle
for
any
purp
ose.
It is
not
per
mitt
ed to
dis
trib
ute
the
elec
tron
ic c
opy
of th
e ar
ticle
thro
ugh
onlin
e in
tern
et a
nd/o
r in
tran
et fi
le s
harin
g sy
stem
s, e
lect
roni
c m
ailin
g or
any
oth
er m
eans
whi
ch
may
allo
w a
cces
s to
the
Art
icle
. The
use
of a
ll or
any
par
t of t
he A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed. T
he c
reat
ion
of d
eriv
ativ
e w
orks
from
the
Art
icle
is n
ot p
erm
itted
. The
pro
duct
ion
of r
eprin
ts fo
r pe
rson
al o
r co
mm
erci
al u
se is
not
per
mitt
ed. I
t is
not p
erm
itted
to r
emov
e, c
over
, ove
rlay,
obs
cure
, blo
ck, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost o
n th
e A
rtic
le. I
t is
not p
erm
itted
to fr
ame
or u
se fr
amin
g te
chni
ques
to e
nclo
se a
ny tr
adem
ark,
logo
, or
othe
r pr
oprie
tary
tio
n of
the
Pub
lishe
r.