Embed Size (px)
Citation preview

System Build
Health Information Technology Toolkit for Chiropractic Offices

2
Presenter• Margret Amatayakul
RHIA, CHPS, CPHIT, CPEHR, FHIMSS
President, Margret\A Consulting, LLCSchaumburg, IL
• Independent consultant, who focuses on achieving value from electronic health records, HIPAA/HITECH, and health information exchange. Developer of tools in Toolkit
• Adjunct faculty College of St. Scholastica, Duluth, MN, masters program in health informatics
• Founder and former executive director Computer-based Patient Record Institute, associate executive director AHIMA, associate professor University of Illinois
• Active participant in standards development, former HIMSS BOD, and co-founder of and faculty for Health IT Certification
2

3
Stratis Health● Stratis Health is a nonprofit organization that leads
collaboration and innovation in health care quality and safety, and serves as a trusted expert in facilitating improvement for people and communities
● Stratis Health works toward its mission through initiatives funded by federal and state government contracts, and community and foundation grants, including serving as Minnesota’s Medicare Quality Improvement Organization (QIO)
● Stratis Health operates the Health Information Technology Services Center for health care organizations seeking to use health information technology in support of their clinical transformation

4
• Understanding system build• System build tasks• Data conversion• Chart conversion• Interfaces• Legal health record
Agenda

5
• Install– Setting up hardware– Loading software onto hardware
• Implement– All activities associated with installation and hardware
configuration, workflow and process improvement, loading tables with your organization’s specifications, and building the system to meet your requirements (system build), testing, training, and support for actual use (go live)
• Adopt– State where intended users actually use the system to achieve
specified, measureable goals
Definition of Terms

6
• Configuration of software to meet internal policies, workflows, and process requirements– Also referred to as software configuration
• Configure = arrange parts in a specific way for a specific purpose
Understanding System Build
Copyright © 2005-8, Margret\A Consulting, LLC. Used with permission of author.
Floor
4Bed
2W
Mary Smith

7
• Master files and tables/data dictionary build– Relational database– Values of variables– Metadata– Change control– Screen layout– Data entry shortcuts– Alerting strategies
System Build Tasks

8Copyright © 2005-8, Margret\A Consulting, LLC. Used with permission of author.
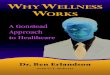
Relational DatabasePatient File
Med Rec # Name Birth date Street City, State Insurance
123498 Pam Bell 01121989 123 River Small, ST BCBS
125678 Jo Smith 10301972 RR 3 Rural, ST Aetna
Admission File
Name Date Time Mode Chiropractor Adm Dx
Pam Bell 02142008 0900 Ambulance Dan James Fracture
Insurance Table
Aetna
BCBS
Paywell
Provider
TableNPI
Pat Carson, PA 8876
Chiropractor 7543
Ted Smith, DO 1264
Dx Table
AMI
COPD
Fracture
Dan James
ChiropractorVariable
Value

9
• All computers that use a relational database to process data collect values of variables from tables to form files
• Some of these variable values are known to you and are relatively stable, such as names and credentials of chiropractors, etc.
• Vendors ask you to capture these values to be pre-loaded into system master files and tables, by the vendor or by you, using a computer wizard
Values of Variables

10
• Data values for system build may come from a variety of sources:– A database or directory you maintain (data dictionary/metadata)– Various forms you use (Form and Reports Inventories)
• Data values relative to payer rules, formularies, drug knowledge are acquired by the vendor from their source (e.g., PBM) or a third party (e.g., ICD, CPT), with any subscription fees passed to users
• Standard vocabularies recommended for use by the federal government include:
– SNOMED – LOINC– RxNorm– UMDNS
Sources of Data Values

11
• SNOMED (SNOMED International) – Originally developed by College of American Pathologists and now distributed by
International Health Terminology Standards Development Organization, Denmark, SNOMED is licensed for use in U.S. by National Library of Medicine. It is a systematically organized computer processable collection of over 0.5 M medical concepts and 1.5 M semantic relationships covering most areas of clinical information such as diseases, findings, procedures, microorganisms, and pharmaceuticals for consistent indexing, storage, retrieval, and aggregation of clinical data across specialties and sites of care.
• LOINC (Logical Observations Identifiers Names and Codes) – Developed and maintained by Regenstrief Institute, includes over 41,000 names of
laboratory terms, as well as nursing diagnosis, nursing interventions, outcomes classification, and patient care data set. Each database record includes six fields for the unique specification of each identified single test, observation, or measurement:
Standard Vocabularies
Copyright © 2005-8, Margret\A Consulting, LLC. Used with permission of author.

12
• RxNorm Provides standard names for clinical drugs (active ingredient + strength + dose form) and for dose forms as administered to a patient. It provides links from clinical drugs, both branded and generic, to their active ingredients, drug components (active ingredient + strength), and related brand names. NDCs (National Drug Codes) for specific drug products (where there are often many NDC codes for a single product) are linked to that product in RxNorm. RxNorm links its names to many of the drug vocabularies commonly used in pharmacy management and drug interaction software, including those of First Databank, Micromedex, MediSpan, Gold Standard Alchemy, and Multum. By providing links between these vocabularies, RxNorm can mediate messages between systems not using the same software and vocabulary.
• Universal Medical Device Naming System (UMDNS)A standard international nomenclature and computer coding system for medical devices used in applications ranging from hospital inventory and work-order controls to national agency medical device regulatory systems and from e-commerce and procurement to medical device databases. UMDNS is maintained by ECRI and contains nearly 7,500 unique medical device concepts and definitions (preferred terms), along with an additional 8,000 entry terms to facilitate classifying of biomedical information
Standard Vocabularies

13
Metadata• Data about data
– Describes structured, or discrete, data element properties
– Must be kept up-to-date – Changes must be
documented (change control or configuration management)
Attributes Original
Name Chiropractor
Table Chiropractor
DB Name Chiro
Synonyms Admitting staff
Definition Chiropractic staff who may admit patients
Reference Organizational bylaws
Source Admission screen
Derivations None
Valid Values Alphabetic
Conditionality Required
Default None
Lexicon (Standard
Vocabulary)
None
Relationship None
Access Any staff
(CDS) Process Rule
Convert to NPI for billing
Dan James
Chiropractor

14
• External reporting:– Common meaning?– Common representation?
• All data required to “fire” a rule must be present for a clinical decision support rule to work correctly– Changing the definitions of the data or requirements for their entry puts use of
the rule at risk– Changes to metadata may be admissible in a court of law if there is a question
as to spoliation of evidence
• A data administrator is often responsible for maintaining the integrity of a data dictionary; a database administrator makes the physical changes in the metadata registry
• Clinicians should approve all changes to the data dictionary, especially as they impact clinical decision support
• Degree of flexibility an organization has in managing changes to metadata varies with product
Importance of Metadata

15
• A data element may now be required to be entered (e.g., dose for a drug prescribed), but someone asks for it to be changed to optional (e.g., so dose would not always have to be entered).
• The decision to make such a change should be a thoughtful one, with an appreciation for its impact – If dose is not recorded, will the system automatically record a default,
or can the user expect a call from the pharmacy?– If something goes wrong in the future (e.g., default dose was not
changed when necessary), will you be able to track why and when the system change was made if necessary?
– If a future version of the software depends on this data element to be required and will not work properly as a result, will you be able to track that it was this change that is the cause of the problem now?
Example of Need for Change Control

16
• Some vendors enable screen design changes. Consider making such changes:– Only when absolutely necessary– For an entire group or organization– Such changes are costly to make and maintain
• Consider size and resolution of display screen– Not only will some screens not display well on smaller devices used for mobile
professionals,– But mobile professionals may use a variety of devices
• Consider user familiarity with computers– Data entry and retrieval must be intuitive
• Instructions must be clear, but not to obstruct power user• Icons must be able to be quickly understood (without mouse-over delays) within context
– Navigating multiple screens may result in power users getting lost• Balance reduction of complexity with need for information density
– Regenstrief Institute discovered that once a person begins to use an EHR, one denser screen is preferred to multiple screens
Screen Layout

17Copyright © 2005-8, Margret\A Consulting, LLC. Used with permission of author.
Screen Layout Strategies• Size and resolution of monitor (tablets
vs. notebooks vs. desktops)• User familiarity with computers
– Balance reduction of complexity with need for information density
• Sequencing, nesting, spacing, color, icons, navigation
• Alerting– Active
– Passive
• Variable Selection– Balance flexibility with standardization
• Data entry shortcuts• Templates

18Copyright © 2005-8, Margret\A Consulting, LLC. Used with permission of author.
Data Entry ShortcutsSTRUCTURED DATA ENTRY• “Click” boxes• Drop down • Type ahead- - - - - - - - - - - - - - - - - - - • “Smart text” or macros• Default values• Cut (copy) and paste• Drag and drop• Drawing tools• Speech commands
ABILITY TO CONVERT VALUES OF VARIABLES TO STANDARD NARRATIVE
• Click boxes:– Check box = multiple options
may be selected– Radio button = only one choice
can be selected
UNSTRUCTURED DATA ENTRY• Dictation/speech dictation• Typing• Handwriting recognition

19
Alerting Strategies• Sounds or messages to
pagers, phone• In-basket functionality• Color, sound, &/or symbols
and indicators• Pop-up boxes (active alert)• Appearance of message or
icon (passive alert)• Context-sensitive templates
Copyright © 2005-8, Margret\A Consulting, LLC. Used with permission of author.

20
• Data conversion = permanently replacing data from one application to another, such as moving the patient schedule from a PMS to an EHR
• Interface = an interface sends data from one system to anothe, where both systems continue to operate on the data as applicable
• Master file and table build = allows stable data to be pre-loaded into new system
• Chart conversion = Making selected content of paper charts accessible/usable in EHR
Data Conversion
Copyright © 2005-8, Margret\A Consulting, LLC. Used with permission of author.
OLDNEW
DataConversion
Ch
art
Co
nve
rsio
n

21
• Chart conversion options– Scan vs. abstract– Staff/contractor vs. chiropractor– All of record vs. parts of record– All records vs. active records
• Other issues– Policy on chart availability after conversion– Closing charts after conversion– File records after conversion vs. warehousing vs. destruction– Legal aspects
Chart Conversion

22
• Start early– Prior to contracting, identify all interfaces– Determine if EHR vendor can write all interfaces
• Is a third party interface developer (system integrator) needed?
• Interface issues:– Uni-directional or bi-directional– What data? (all or some)– Will a portal do as well?
• Need is to view information, not data (e.g., results review)• Need is to access and use applications
Interface Build

23
• Interface – data entered into one system is also sent to another system
• Portal – entranceway to access applications and perform work at another site to which you are authorized
Interface vs. Portal
Copyright © 2005-8, Margret\A Consulting, LLC. Used with permission of author.
CPOE
HospitalClinic

24
Representative List of Interfaces
Copyright © 2005-8, Margret\A Consulting, LLC. Used with permission of author.

25
• Subset of all patient-specific data created or accumulated by a chiropractor that may be released to third parties in response to legally permissible requests
• Federal Rules of Evidence: “that information kept in the course of a regularly conducted business activity.”
• Rules of e-Discovery, however, do not preclude metadata from being further requested via court order – Metadata includes data dictionary definitions and changes, as
well as date/time stamps of user entries and audit trails identifying what user accessed what data
Legal Health Record

26
• Will structured data entry result in:
– Structured data output for subsequent processing?
– Print files intended to represent legal health record but are not customary or interoperable?
– Need to produce a screen shot for achieving the legal health record?
– Reports representing various needs, including for auditors, legal health record, subsequent use?
Converting Data to Output for Legal Health Record
Copyright © 2005-8, Margret\A Consulting, LLC. Used with permission of author.

27
Contact:Stratis Health
2901 Metro Dr., Suite 400
Bloomington, MN 55425
952-854-3306
1-877-787-2847 (toll free)
www.stratishealth.orgCopyright © 2011 Stratis Health. Funded by Chiropractic Care of Minnesota, Inc. (ChiroCare), www.chirocare.com
__________________________________________________________________________________________
Adapted from Stratis Health’s Doctor’s Office Quality – Information Technology Toolkit, © 2005, developed by Margret\A Consulting, LLC, and produced under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services.
For support using the toolkit
Stratis Health Health Information Technology Services
952-854-3306 [email protected]
www.stratishealth.org
For More Support





![A Consumer’s Guide to Chiropractic Care · California Board of ChiropraCtiC ExaminErs [ 3 ] What is a Chiropractic Adjustment and Chiropractic Care? A chiropractic adjustment is](https://img.pdfslide.us/doc/110x75/5afc83ce7f8b9a68498b9600/a-consumers-guide-to-chiropractic-board-of-chiropractic-examiners-3-what.jpg)