Embed Size (px)
Citation preview

Gynecologic Oncology 114 (2009) 293–298
Contents lists available at ScienceDirect
Gynecologic Oncology
j ourna l homepage: www.e lsev ie r.com/ locate /ygyno
Synuclein-γ (SNCG) may be a novel prognostic biomarker in uterine papillaryserous carcinoma☆
Jacqueline Morgan a, Anna V. Hoekstra a, Eloise Chapman-Davis a, Jennifer L. Hardt b,J. Julie Kim b, Barbara M. Buttin a,⁎a Department of Obstetrics and Gynecology, Division of Gynecologic Oncology, Northwestern University Feinberg School of Medicine, Chicago, IL, USAb Division of Reproductive Biology Research, Northwestern University Feinberg School of Medicine, Chicago, Illinois, USA
☆ This work was presented at the 2nd Annual Oncolog2009, Miami, Florida.⁎ Corresponding author. Division of Gynecologic Onco
and Gynecology, and Robert H. Lurie Comprehensive CaStreet, 5-2168, Chicago, IL 60611, USA. Fax: +1 312 472
E-mail address: [email protected] (B.M. Buttin).
0090-8258/$ – see front matter © 2009 Elsevier Inc. Adoi:10.1016/j.ygyno.2009.04.036
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 24 February 2009Available online 24 May 2009Keywords:Synuclein-γUterineSerous carcinomaBiomarkerPrognosisDrug resistance
Objectives. SNCG in breast cancer is a marker for advanced and aggressive disease thereby correlatingwith a poor prognosis in patients. We set out to determine if SNCG expression in UPSC correlates withaggressive cellular properties, poor prognosis, and chemoresistance, and if silencing SNCG can reverse theseattributes in vitro.
Methods. A focused, real time PCR array was performed comparing a papillary serous (SPEC2) and anendometrioid (Ishikawa) endometrial cancer cell line. SNCG was the most differentially expressed gene.SNCG expression was confirmed by real time PCR, Western blot, and immunohistochemistry (IHC) andcorrelated with outcomes in a pilot set of 20 UPSC patients. A stably transfected SPEC2 cell line was createdusing shSNCG oligonucleotides. The effect of SNCG knockdown in SPEC2 cells on cell proliferation andsensitivity to paclitaxel-induced apoptosis was measured using a cell viability assay, BrdU incorporation
assay, as well as cleaved PARP analyses.Results. SNCG mRNA as well as protein was highly expressed in SPEC2 cells while minimally toundetectable in several endometrioid endometrial cancer and normal endometrial cell lines. IHC alsoconfirmed unique SNCG expression in UPSC tumors compared to low grade endometrial cancers. In UPSCpatients, SNCG expression by IHC correlated with advanced stage and decreased progression-free survival.Knockdown of SNCG in SPEC2 cells caused a significant decrease in cell proliferation and increased sensitivityto paclitaxel-induced apoptosis.
Conclusions. SNCG is a novel biomarker for aggressive disease and chemoresistance in UPSC and meritsfurther investigation both as a prognostic tool and as a therapeutic target.
© 2009 Elsevier Inc. All rights reserved.
Introduction
Uterine papillary serous carcinoma (UPSC) is an uncommon butaggressive histologic subtype of endometrial carcinoma accountingfor only 10% of all cases but almost 40% of endometrial cancer deaths[1,2]. UPSC exhibits early intraabdominal and retroperitoneal spreadeven in the absence of traditional risk factors, such as deepmyometrial invasion, tumor size, and lymph vascular space invasion[3]. Little is known about the genetic events that lead to thedevelopment of UPSC and contribute to its aggressive behavior.
Histologically, UPSC resembles papillary serous carcinoma of theovary. However, despite this similarity response rates to chemother-
y Biomarkers Meeting, January
logy, Department of Obstetricsncer Center, 250 East Superior4688.
ll rights reserved.
apy and disease-specific survival rates are lower for UPSC than forovarian cancer patients [4]. UPSC is therefore viewed as relativelychemoresistant. More recently, several investigators reported caseseries of UPSC patients treated with paclitaxel with or withoutplatinum showing response rates in the 60–80% range [5–8]. None-theless, most of these responses are not durable and have nottranslated into improved survival rates.
In an effort to identify genes differentially expressed in UPSCversus endometrioid endometrial cancers, we performed a focused,real time PCR array using a low grade endometrioid (Ishikawa) anda UPSC (SPEC2) cell line. The most highly expressed gene in theSPEC2 cell line relative to Ishikawa was synuclein-γ (SNCG) whichis a prometastatic oncogene located on chromosome 10q23. SinceSNCG is associated with aggressive disease, metastasis, and drugresistance in breast cancer, we set out to determine if SNCGexpression in UPSC correlates with an aggressive tumor phenotype,poor prognosis, and chemoresistance, and if inhibition of SNCGexpression in a UPSC cell line could reverse some of its aggressiveproperties.

294 J. Morgan et al. / Gynecologic Oncology 114 (2009) 293–298
Materials and methods
Reagents
The SNCG monoclonal antibody was purchased from ProMabBiotechnologies (Albany, CA), the ECL Plus Western Blotting DetectionSystem from Amersham Biosciences (Buckinghamshire, UK), TriR-eagent from Sigma, and M-MLT reverse transcriptase along with cellculture media and supplements from Invitrogen (Carlsbad, CA). QuickCell Proliferation Assay Kit was obtained from BioVision ResearchProducts (Mountain View, CA). Mission Lentiviral shRNA transductionagents and reagents were purchased from Sigma, (St Louis, MO) andBrdU detection kit from Roche (Indianapolis, IN).
Endometrial cancer tissues and cell lines
After Institutional Review Board (IRB) approval was obtained,endometrial cancer tissue was collected prospectively at surgery. Allpatients provided informed consent for the research use of theirtissue. Histological classification and grading of tumors was assignedby a pathologist according to the World Health Organization criteria.
For the prognostic study, patients with UPSC were identifiedretrospectively from the tumor registry at Northwestern MemorialHospital after IRB approval was obtained. Twenty patients wereidentified who had both archival tumor tissue and medical recordsavailable for review.
SPEC2 cells were obtained from I. Fidler (MD Anderson, Houston,Texas). This cell line was developed by Drs. J. Boyd and D.G. Kaufmanat the University of North Carolina (Chapel Hill, North Carolina) from ahighly metastatic UPSC tumor. Ishikawa and ECC1 cell lines from B.Lessey (Greenville Hospital System, Greenville, South Carolina) andHec1B cells were purchased from ATCC. The hTERT-EEC cell line wasprovided by T. Klonisch (Winnipeg, Manitoba). All cell lines werecultured at 37 °C in a C02 incubator. SPEC2 cells were cultured inDMEM supplemented with 10% fetal bovine serum (FBS), sodiumpyruvate, L-glutamine, non-essential amino acids, multivitamins andantibiotics (5000 U/mL penicillin G, 5000 μg/mL streptomycin).Ishikawa and HEC1B cells were cultured inMEM, ECC1 and hTERT-EECcells were maintained in MEM/F12 and all media were supplementedwith 10% FBS, sodium pyruvate and antibiotics.
Cell viability and proliferation assays
Cells were seeded at 1×104 cells per well onto 96-well flat-bottomed tissue culture plates and incubated at 37 °C for 24 h. QuickCell Proliferation Assay Kit was used to quantify cell viability, whichmeasures the level of WST-1 cleavage to formazan by cellularmitochondrial dehydrogenases. The absorbance of the wells wasmeasured using a microtiter plate reader at 440 nm and 650 nm.BrdU assay was used to evaluate cell proliferation by the level ofincorporation of BrdU into proliferating cells detected by colorimetricanalysis using a microplate reader per the manufacturer'sinstructions.
Quantitative real time PCR
RNA was isolated from cells using Tri Reagent according to themanufacturer's protocol. Concentration and purity of extracted RNAwere determined using the ND-1000 Spectrophotometer (NanoDrop,Wilmington, DE). Total RNA samples were DNase treated to removeany contaminating DNA. Briefly, RNA was added to 10′ Dnase 1reaction buffer (1 μL), Dnase 1 Amp grade (1 μL), andmade up to 10 μLwith DEPC treated water. The solution was incubated at roomtemperature for 15 min, the reaction was quenched by addition of25 mM EDTA (1 μL) and heated for another 10 min at 65 °C. Total RNAwas reverse transcribed in a total volume of 20 μL for the synthesis of
cDNA using M-MLT reverse transcriptase according to the manu-facturer's protocol. A focused real time PCR array was used to comparethe expression of genes associated with cancer in the Ishikawa andSPEC2 cell lines. Specifically, the Human Cancer Pathway Finder GeneArray that contains 84 cancer-related genes associated with sixbiological pathways including Cell Cycle Control, DNA Damage Repair,Apoptosis and Cell Senescence, Signal Transduction Molecules andTranscription Factors, Adhesion and Angiogenesis, and Invasion andMetastasis (SuperArray Biosciences Corp., Frederick, MD) was used.Each well in the 96-well plate contained specific primers for each ofthese genes. All reactions were carried out on an ABI PRISM 7700Sequence Detection System (Applied Biosystems, Foster City, CA) for40 cycles (95 °C for 15 s, 60 °C for 1 min) after 10 min incubation at95 °C. SNCG specific primers (Taqman) were utilized. Results of boththe SPEC2 and Ishikawa cells were expressed as the fold changerelative to the housekeeping gene TBP (TATA-binding protein).
Immunohistochemistry (IHC)
Tissueswere fixed in formalin, paraffin-embedded, and 4 μm tissuesections were placed on glass slides. Tissue sections were incubatedin 3% hydrogen peroxide at room temperature and rinsed with Tris-buffered NaCl solutionwith 0.1% Tween-20 (0.2M Tris (pH 7.6),1.37MNaCl, TBS-T). Protein Block (DAKO, Fort Collins, CO) was applied andslides were incubated at 4 °C in a humidified chamber overnight witha monoclonal anti-SNCG antibody (ProMab Biotechnologies, Albany,CA) at a 1:500 dilution. Slides were rinsed in TBS-T and anti-mousesecondary antibody conjugated to a dextran labeled polymer andhorseradish peroxidase (DAKO) was applied. TBS-T was then used torinse the slides twice and DAB solution (DAKO) was applied. Slideswere rinsed in distilled water and counterstained in Mayer'sHematoxylin (Sigma) followed by a rinse in running tap water.Following another rinse in running distilled water, slides wereincubated in ammonia water (4 mL of 28% ammonium hydroxide in1 L of distilled water) and then rinsed in tap and distilled runningwater. Dehydration and clearing of the slides was accomplishedthrough two changes of 95% ethanol, two changes of 100% ethanol,and two changes of xylene (10 dips per solution). Slides weremounted using the xylene-based Cytoseal-XYL (Richard-Allan Scien-tific). Blinded for tissue type, the intensity of staining was designatedas absent (0) versus present (1+, 2+, 3+) by two investigatorsindependently. Both nuclear and cytoplasmic staining was used toevaluate overall designation. Human hippocampal tissue was used asthe positive and negative control for SNCG expression.
Western blot analysis
Cells were harvested at 80% confluency with RIPA buffer (50 mMTris–HCL, pH 8.0, 150 mM NaCl, 0.5% sodium deoxycholate, 1% IGEPAL(Sigma), 0.1% SDS) plus protease inhibitors (Sigma) on ice. Proteinconcentration was determined with the Micro BCA protein assay kit(Pierce, Rockford, IL). Protein extract was heated at 95 °C for 3 minand run on a precast 2–15% acrylamide gel (Biorad), and transferredonto a PVDF membrane (Whatman). Membranes were blocked with5% milk in Tris Buffered Saline with 0.1% Tween-20 (TBS-T) and thenincubated with primary antibody at 1:1000 dilution of anti-SNCGantibody, or 1:1000 dilution of anti-cleaved PARP, followed byincubation with secondary peroxidase-conjugated goat anti-mouseIgG (Biorad) or goat anti-rabbit IgG at 1:10,000 dilution. Membraneswere then washed and developed using either the ECL Plus WesternBlot Detection System kit (Amersham, Piscataway, NJ) or theSupersignal West Dura Extended Duration Substrate (Pierce).Membranes were stripped with Restore Western Blot StrippingBuffer (Pierce) and re-probed with a monoclonal antibody to beta-actin (1:10,000, Sigma). All Western blots are representative of 3independent experiments.

295J. Morgan et al. / Gynecologic Oncology 114 (2009) 293–298
Stable transfection with short hairpin RNA
SPEC2 cells were stably transfected with short hairpin RNA toeither random non-sense oligonucleotides (shControl) or sequencesspecific to SNCG, using the Lentiviral Mission shRNA transductionsystem incorporating a viral vector (Sigma, St. Louis, MO). Fivedifferent sequences specific to SNCG were used. Cells were pretreatedwith hexamethadine. Cells achieving successful incorporation ofshSNCG were selected using puromycin. Real time PCR was used toquantify the level of SNCG knockdown in each developed clonerelative to the housekeeping gene TBP. The two clones with the mostsignificant reduction in SNCG expressionwere used for all subsequentexperiments. Confirmation of SNCG protein silencing was undertakenwith western blot analysis as outlined above. Interferon Responsedetection assay (System Biosciences, Mountain View, CA) wasperformed per manufacturer's instructions to confirm that thetransduction process did not alter other cellular pathways non-specifically. Six separate primers were used, targeting β-actin, OAS1,OAS2, MX1, ISGF3y and IFITM1 in both SPEC2 shControl and SPEC2shSNCG stably transfected cells by real time PCR.
Statistical analysis
Analysis of variance (ANOVA) was used to determine if there aresignificant differences between groups (Pb0.05). For experimentalgroups that satisfy the initial ANOVA criterion, individual comparisonswere performed using post hoc Bonferroni t tests based on theassumption of two-tail distribution and two samples with equalvariance. χ2 tests were used to test for association of SNCG expressionwith disease stage. Survival curves for the PFS endpoints were gene-rated separately for patients expressing and not expressing SNCG
Table 1Genes up- and down-regulated in SPEC2 compared to Ishikawa cells.
Gene Full name
SNCG SNCG synuclein, gamma (breast cancer-specific protein 1) aPLAU PLAU plasminogen activator, urokinaseIL8 IL8 interleukin 8MTSS1 MTSS1 metastasis suppressor 1SERPINB5 SERPINB5 serpin peptidase inhibitor, clade B (ovalbumin), mFGFR2 FGFR2 fibroblast growth factor receptor 2 (bacteria-express
craniofacial dysostosis 1, Crouzon syndrome, Pfeiffer syndroIFNA1 IFNA1 interferon, alpha 1JUN JUN jun oncogeneRB1 RB1 retinoblastoma 1 (including osteosarcoma)MMP1 MMP1 matrix metallopeptidase 1 (interstitial collagenase)NFKBIA NFKBIA nuclear factor of kappa light polypeptide gene enhaMET MET met proto-oncogene (hepatocyte growth factor receptoTIMP3 TIMP3 TIMP metallopeptidase inhibitor 3 (Sorsby fundus dyITGA3 ITGA3 integrin, alpha 3 (antigen CD49C, alpha 3 subunit ofPDGFA PDGFA platelet-derived growth factor alpha polypeptideTNF TNF tumor necrosis factor (TNF superfamily, member 2)MMP9 MMP9 matrix metallopeptidase 9 (gelatinase B, 92 kDa gelaFOS FOS v-fos FBJ murine osteosarcoma viral oncogene homologNFKB1 NFKB1 nuclear factor of kappa light polypeptide gene enhanTIMP1 TIMP1 TIMP metallopeptidase inhibitor 1SERPINE1 SERPINE1 serpin peptidase inhibitor, clade E (nexin, plasminETS2 ETS2 v-ets erythroblastosis virus E26 oncogene homolog 2 (UCC1 EPDR1 ependymin related protein 1 (zebrafish)ITGA2 ITGA2 integrin, alpha 2 (CD49B, alpha 2 subunit of VLA-2 reTWIST1 TWIST1 twist homolog 1 (acrocephalosyndactyly 3; SaethreMYC MYC v-myc myelocytomatosis viral oncogene homolog (aviaITGB3 ITGB3 integrin, beta 3 (platelet glycoprotein IIIa, antigen CDMMP2 MMP2 matrix metallopeptidase 2 (gelatinase A, 72 kDa gelaITGA1 ITGA1 integrin, alpha 1COL18A1 COL18A1 collagen, type XVIII, alpha 1CDKN2A CDKN2A cyclin-dependent kinase inhibitor 2A (melanoma,TGFB1 TGFB1 transforming growth factor, beta 1 (Camurati–EngelmPDGFB PDGFB platelet-derived growth factor beta polypeptide (simNME4 NME4 non-metastatic cells 4TNFRSF25 TNFRSF25 tumor necrosis factor receptor superfamily, mem
using the Kaplan–Meier method. The curves were then comparedusing a log-rank test, and Cox proportional hazards models.
Results
Differential gene expression in SPEC2 versus Ishikawa cells
The Human Cancer Pathway Finder Gene Array was usedto identify differentially expressed genes in SPEC2 and Ishikawacells. This targeted PCR array demonstrated that SNCG wasmost highly expressed in SPEC2 cells compared to Ishikawacells (Table 1). Therefore, we conducted further studies on this gene.
Expression of SNCG in endometrial cancer cell lines and tumor tissues
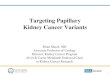
The differential expression of SNCG in SPEC2 cells compared toother type 1 endometrial cancer cell lines was confirmed at both themRNA and protein levels. SNCG mRNA expression was 746-fold up-regulated in SPEC2 versus Ishikawa cells. This differential expressionwas confirmed by real time PCR using another set of primers specificto SNCG. Furthermore, SNCG protein levels were high in SPEC2whereas levels were undetectable in the type I endometrial cancer celllines Ishikawa, ECC, and Hec1B, as well as the immortalized normalendometrial epithelial cell line, hTERT-EEC (Fig. 1A). These datastrongly suggest that SNCG expression is specific to UPSC. In order todetermine if SNCGwas expressed in UPSC tumors, IHC staining using amonoclonal antibody to SNCG was performed on paraffin-embeddedtissue samples. Strongly positive staining for SNCG was noted in fourof four UPSC tumor specimens and negative staining was noted in fiveof five grade 1 and 2 endometrioid tumors as well as two normalendometrial samples (Fig. 1B).
Fold up-regulated
ka SR; BCSG1 745.81250.259.5628.59
ember 5 19.19ed kinase, keratinocyte growth factor receptor,me, Jackson–Weiss syndrome)
17.41
10.399.378.678.59
ncer in B-cells inhibitor, alpha 7.7r) 6.61strophy, pseudoinflammatory) 5.78VLA-3 receptor) 5.65
5.614.85
tinase, 92 kDa type IV collagenase) 4.794.7
cer in B-cells 1 (p105) 4.594.47
ogen activator inhibitor type 1), member 1 4.31avian) 3.83
3.8ceptor) 3.77–Chotzen syndrome) (Drosophila) 3.26n) 3.1461) −206.69tinase, 72 kDa type IV collagenase) −106.58
−31.97−19.24
p16, inhibits CDK4) −17.36ann disease) −15.48ian sarcoma viral (v-sis) oncogene homolog) −15.33
−11.71ber 25 −9.5

Fig. 1. SNCG protein expression in endometrial cancer cell lines and tumor tissues. (A) Levels of SNCG protein in endometrial cancer cell lines Ishikawa, ECC1, SPEC2, Hec1B, and theimmortalized normal endometrial epithelial cell line, hTert-EEC1 by Western blot. (B) Representative immunohistochemical staining for SNCG on a paraffin-embedded grade 1endometrioid adenocarcinoma (c) and uterine papillary serous carcinoma (d) with hippocampal tissue as positive and negative controls (a, b). Magnification is 200×.
Fig. 2. SNCG knockdown in SPEC2 cells by lentiviral transduction of shRNA. (A) SNCGprotein levels after shSNCG transduction into SPEC2 cells wasmeasured byWestern blot.(B) Cell proliferation was measured in the stably transduced SPEC2 cell lines by BRDUassay. Data shown represent the mean+SEM of experiments done in triplicate.
296 J. Morgan et al. / Gynecologic Oncology 114 (2009) 293–298
SNCG as a regulator of cell proliferation in SPEC2 cells
It has been shown that SNCG is involved in cell proliferation inbreast cancer cell lines [9]. To determine whether or not SNCG isassociated with SPEC2 cell proliferation, SPEC2 cells were stablytransfected with shSNCG or shControl oligonucleotides, respectively,using the Lentiviral transduction system in order to silence SNCG.SNCGwas efficiently knocked down as shown in Fig. 2A. Real time PCRinterferon assay was conducted on the stably transduced cell lines andno statistically significant differences were noted for any of the sixinterferon genes used in the assay (data not shown), demonstratingthe absence of non-specific effects of gene silencing. The effect ofSNCG knockdown on cell proliferation was evaluated in SPEC2 cellswith a BrdU assay. A modest but statistically significant decrease incell proliferation was seen in the shSNCG SPEC2 cells compared to theshControl SPEC2 cells suggesting that SNCG is involved in regulatingthis process (Fig. 2B).
Improved sensitivity to paclitaxel after SNCG knockdown
We compared the response to paclitaxel exposure of a type 1endometrial cancer cell line, Ishikawa, to the response of the UPSC cellline, SPEC2. Both cell lines were exposed to various paclitaxelconcentrations for 24 h and cell viability was measured using a cellviability assay. SPEC2 cells responded differently to paclitaxel thanIshikawa cells in that the number of viable cells remained significantlyhigher despite escalating paclitaxel concentrations (Fig. 3A). SinceSNCG expression has been shown to correlate with paclitaxelresistance in breast cancer cells and partial reversal of this resistancewas achieved by SNCG inhibition [10,11], the role of SNCG in thepaclitaxel sensitivity of SPEC2 cells was further explored. Utilizing the

Fig. 3. Effect of SNCG knockdown on SPEC2 cell viability and proliferation with increasing concentrations of paclitaxel. (A) SPEC2 and Ishikawa cells were treated with increasingconcentrations of paclitaxel and a cell viability assay was done. (B) The shSNCG and shControl SPEC2 cell lines were treated with paclitaxel for 48 h and cell proliferation using theBrdU incorporation assay was measured. Data represent the mean+SEM of three independent experiments. ⁎ denotes Pb0.05.
297J. Morgan et al. / Gynecologic Oncology 114 (2009) 293–298
previously created stably transfected shSNCG or shControl SPEC2 cells,cell proliferation was quantified after incubation with 20 nMpaclitaxel for 48 h. There was a significant decrease in cell proli-feration in the presence of paclitaxel in the shSNCG cells compared toshControl cells (Fig. 3B).
Increased apoptosis after paclitaxel exposure with SNCG knockdown
In order to determine whether SNCG was associated withpaclitaxel-mediated apoptosis, shControl and shSNCG cells weretreated with paclitaxel for 48 h and Western blot analysis was donefor cleaved PARP. While paclitaxel treatment increased levels ofcleaved PARP in both shControl and shSNCG cells, the levels of cleavedPARP were higher in the shSNCG cells treated with paclitaxel (Fig. 4)indicating a higher percentage of cells undergoing apoptosis. Thesedata suggest that silencing the SNCG gene may partially reversepaclitaxel resistance in the SPEC2 cell line.
Possible correlation of SNCG expression in UPSC tumors with advancedstage and decreased progression-free survival in UPSC patients
In a pilot series of 20 patients with UPSC from our institution, all ofwhomwere surgically staged, seven patients had stage I disease while13 had stage II–IV disease. 14 (70%) tumors stained positive for SNCGby IHC. Eleven of 14 (79%) SNCG+ patients had advanced stage
Fig. 4. Effect of SNCG knockdown on paclitaxel-induced apoptosis in SPEC2 cells.shSNCG and shControl cells were treated with paclitaxel. Apoptosis was detected byincreased levels of cleaved PARP using Western blot.
Fig. 5. Correlation of SNCG expression and adverse outcomes in UPSC patients. (A)Decreased progression-free survival in UPSC patients expressing SNCG compared tononexpressors. (B) Decreased overall survival in the same cohort.

298 J. Morgan et al. / Gynecologic Oncology 114 (2009) 293–298
disease compared to only 2 of 6 (33%) SNCG− patients. Median PFSand OS in the SNCG+ group were 20.92 and 38.05 months versus81.87 and 81.90 months in the SNCG− group (Figs. 5A and B). Whilethere appears to be a trend toward a correlation between SNCGexpression and advanced stage/decreased PFS/OS, in the context of asmall pilot series, the true significance of these findings remainsuncertain.
Discussion
Reasons for the relative chemoresistance of UPSC remain unknownat this time. Many oncologists recommend treating all women withUPSC with some form of adjuvant chemotherapy recognizing the highrisk for systemic recurrences even in those with stage I disease.Additionally, adjuvant pelvic radiotherapy alone is less effective inUPSC due to the high incidence of extrapelvic recurrences [12].Therefore, at this time the use of taxane and platinum based chemo-therapy is common in UPSC, although its efficacy is disappointing.
We identified SNCG as the most highly expressed gene in the UPSCcell line SPEC2 relative to the endometrioid cell line Ishikawa. SNCGwas first named Breast cancer-specific gene 1 (BCSG1) as it is highlyexpressed in advanced breast cancer and almost undetectable innormal breast epithelium or benign breast lesions. It belongs to afamily of small, soluble, highly conserved neuronal proteins that havebeen implicated in both neurodegenerative diseases and cancer. Theirexact biologic function is largely unknown. Aberrant SNCG expressionhas been found in many other solid tumors including colon, gastric,pancreatic, ovarian, and lung cancer [13–15]. This study is the firstreport of SNCG expression in UPSC.
SNCG is well studied in breast cancer where its expressioncorrelates with advanced stage and aggressive disease as well asresistance to microtubule-disrupting agents such as paclitaxel. Denovo expression of SNCG in SNCG-negative breast cancer cell linescauses a significant increase in cell motility and invasiveness in vitro aswell as an increased amount of metastasis in nude mice [16]. Our datasimilarly demonstrate a small but significant decrease in SPEC2 cellproliferation when SNCG expression is suppressed by shRNA sugges-ting that SNCG has a role in this process.
We found that SPEC2 cells are significantly less sensitive topaclitaxel than Ishikawa cells. This observation parallels the aggressiveclinical behavior of UPSC. Since this resistance appears to be affectedby SNCG knockdown, we suspect that it may be mediated by SNCGexpression. Such a finding would make SNCG attractive as a potentialtherapeutic target. Paclitaxel was initially expected to show particularpromise in treating UPSC due to its ability to induce p53 independentapoptosis in vitro and in vivo [17]. However, SNCG may specificallyinterfere with this mechanism and protect cancer cells frompaclitaxel-induced apoptosis by modulating pathways involving twomitogen-activated kinases (MAPKs), extracellular signal-regulatedprotein kinases 1/2 (ERK1/2) and c-Jun N-terminal kinase 1 (JNK1)[18]. Additionally, SNCG interferes with paclitaxel-induced mitoticarrest by interacting with BubR1, a mitotic check point kinase thatnormally prevents cells with misaligned chromosomes from exitingmitosis [19].
The results of SNCG staining and clinical correlation in our pilotseries of 20 UPSC patients demonstrate a trend toward decreasedsurvival and advanced stage in the 70% of patients whose tumorsexpress SNCG. Although these preliminary data must be interpretedwith caution, we believe that if these results are confirmed in a largercohort, SNCG could be developed as a prognostic biomarker correla-ting with poor outcomes and chemoresistance in patients with UPSC.Confirmatory studies to better elucidate the role of SNCG in thetumorigenesis and the aggressive, chemoresistant phenotype of UPSCare currently ongoing in our laboratory.
In summary, UPSC is a rare but deadly malignancy for whichneither its pathogenesis nor the nature of its aggressive behavior andchemoresistance is well understood. Overexpression of SNCG in UPSChas not been previously reported. Our findings suggest that SNCGplays a role both in cell proliferation in the SPEC2 cell line and in itsrelative resistance to taxanes. Our future goal is to determine if SNCGis a key component of a pathway leading to taxane resistance in UPSCand if its inhibition could provide an opportunity to develop noveltargeted treatment strategies specific to the subset of UPSC patientswith the worst prognosis.
Conflict of interest statementNone of the authors have any conflicts of interest to disclose.
Acknowledgments
The authors would like to thank Parin Patel for his excellenttechnical assistance, Yi Lu for his assistance with interpretation of IHCresults, and Monica Gard for her critical review of the manuscript.
Funded by Kimmel Scholar Award from the Sidney KimmelFoundation for Cancer Research (BB) and a grant from the Friends ofPrentice (BB and JJK).
References
[1] Hendrickson M, Ross J, Eifel P, Martinez A, Kempson R. Uterine papillary serouscarcinoma: a highly malignant form of endometrial adenocarcinoma. Am J SurgPathol 1982;6:93–108.
[2] Hamilton CA, Cheung MK, Osann K, et al. Uterine papillary serous and clear cellcarcinomas predict for poorer survival compared to grade 3 endometrioid corpuscancers. Br J Cancer 2006;94:642–6.
[3] Goff BA, Kato D, Schmidt RA, et al. Uterine papillary serous carcinoma: patterns ofmetastatic spread. Gynecol Oncol 1994;54:264–8.
[4] Nicklin JL, Copeland LJ. Endometrial papillary serous carcinoma: patterns of spreadand treatment. Clin Obstet Gynecol 1996;39:686–95.
[5] Hoskins PJ, Swenerton KD, Pike JA, et al. Paclitaxel and carboplatin, alone or withirradiation, in advanced or recurrent endometrial cancer: a phase II study. J ClinOncol 2001;19:4048–53.
[6] Ramondetta L, Burke TW, Levenback C, Bevers M, Bodurka-Bevers D, GershensonDM. Treatment of uterine papillary serous carcinoma with paclitaxel. GynecolOncol 2001;82:156–61.
[7] Zanotti KM, Belinson JL, Kennedy AW,Webster KD,MarkmanM. The use of paclitaxeland platinum-based chemotherapy in uterine papillary serous carcinoma. GynecolOncol 1999;74:272–7.
[8] Vaidya AP, Litell R, Krasner C, Duska LR. Treatment of uterine papillary serouscarcinomawith platinum-based chemotherapy and paclitaxel. Int J Gynecol Cancer2006;16:267–72.
[9] Lu A, Zhang F, Gupta A, Liu J. Blockade of AP1 transactivation abrogates the abnormalexpression of breast cancer specific gene 1 in breast cancer cells. J Biol Chem 2002;277:31364–72.
[10] Zhou Y, Inaba S, Liu J. Inhibition of synuclein-gamma expression increases thesensitivity of breast cancer cells to paclitaxel treatment. Int J Oncol 2006;29:289–95.
[11] Singh VK, Zhou Y, March JA, et al. Synuclein-gamma targeting peptide inhibitorthat enhances sensitivity of breast cancer cells to antimicrotubule drugs. CancerRes 2007;67:626–33.
[12] Kelly MG, O'Malley DM, Hui R, et al. Improved survival in surgical stage I patientswith uterine papillary serous carcinoma (UPSC) treated with adjuvant platinum-based chemotherapy. Gynecol Oncol 2005;98:353–9.
[13] Bruening W, Giasson BI, Klein-Szanto AJ, Lee VM, Trojanowski JQ, Godwin AK.Synucleins are expressed in the majority of breast and ovarian carcinomas and inpreneoplastic lesions of the ovary. Cancer 2000;88:2154–63.
[14] Liu H, Liu W, Wu Y, et al. Loss of epigenetic control of synuclein-gamma gene as amolecular indicator of metastasis in a wide range of human cancers. Cancer Res2005;65:7635–43.
[15] Li Z, Sclabas GM, Peng B, et al. Overexpression of synuclein-gamma in pancreaticadenocarcinoma. Cancer 2004;101:58–65.
[16] Jia T, Liu YE, Liu J, Shi YE. Stimulation of breast cancer invasion and metastasis bysynuclein gamma. Cancer Res 1999;59:742–7.
[17] Lanni JS, Lowe SW, Licitra EJ, Liu JO, Jacks T. p53-independent apoptosis induced bypaclitaxel through an indirect mechanism. Proc Natl Acad Sci U S A 1997;94:9679–83.
[18] Pan ZZ, Bruening W, Glasson BI, Lee VM, Godwin AK. Gamma-synuclein promotescancer cell survival and inhibits stress- and chemotherapy drug-induced apoptosisby modulating MAPK pathways. J Biol Chem 2002;277:3505–60.
[19] Gupta A, Inaba S, Wong OK, Fang G, Liu J. Breast cancer-specific gene 1 interactswith the mitotic checkpoint kinase BubR1. Oncogene 2003;22(48):7593–9.













![Preclinical development of a vaccine against oligomeric alpha-synuclein … · 2017. 11. 15. · gated alpha-synuclein [6–9]. Alpha-synuclein (a-syn) is an abundant protein in the](https://img.pdfslide.us/doc/110x75/5fc07f533588d914ed7a20f9/preclinical-development-of-a-vaccine-against-oligomeric-alpha-synuclein-2017-11.jpg)