Embed Size (px)
Citation preview

Synovial Fibroblasts and Synovial Macrophages FromPatients With Rheumatoid Arthritis and OtherInflammatory Joint Diseases Show ChromosomalAberrations
Raimund W. Kinne,1* Elke Kunisch,1 Volkmar Beensen,2 Thomas Zimmermann,3 Frank Emmrich,3
Peter Petrow,4 Wolfgang Lungershausen,5 Gert Hein,6 Rudolf K. Braun,6 Martin Foerster,6 Claus Kroegel,6
Rando Winter,7 Eckehard Liesaus,7 Renee A. Fuhrmann,7 Andreas Roth,7 Uwe Claussen,2 and Thomas Liehr2
1Experimental Rheumatology Unit, Friedrich Schiller University Jena, Jena, Germany2Institute of Human Genetics and Anthropology, Friedrich Schiller University Jena, Jena, Germany3Institute of Clinical Immunology and Transfusion Medicine, University of Leipzig, Leipzig, Germany4Institute of Pathology, Friedrich Schiller University Jena, Jena, Germany5Department of Traumatology, Friedrich Schiller University Jena, Jena, Germany6Clinic of Internal Medicine IV, Friedrich Schiller University Jena, Jena, Germany7Clinic of Orthopedics, Friedrich Schiller University Jena, Jena, Germany
Chromosomal aberrations were investigated in nuclei extracted from synovial tissue and first-passage synovial fibroblasts (P-1SFB, 98% enrichment) or macrophages (P-1 M�) from patients with rheumatoid arthritis (n � 10). The findings werecompared with those in other rheumatic diseases (osteoarthritis, n � 14; reactive arthritis, n � 1), as well as with those inchronic obstructive pulmonary disease (n � 8). Controls were paired peripheral blood lymphocytes from arthritic patients,synovial tissue or SFB/M� from joint trauma/normals (n � 9), and peripheral blood monocytes from normal donors (n � 10).GTG banding of metaphase chromosomes and interphase fluorescence in situ hybridization with centromere-specific probeswere used. Comparable chromosomal aberrations were observed in synovial tissue and P-1 SFB of patients with rheumatoidarthritis, osteoarthritis, and reactive arthritis (polysomy 7 and aneusomies of chromosomes 4, 8, 9, 12, and 18). Notably,aneusomies of chromosomes 4, 6, 7, 8, 9, 11, 12, and/or X were also detected in P-1 synovial M� from rheumatoid arthritis(90% of the cases), osteoarthritis (93%), and reactive arthritis (1/1), as well as bronchial M� from chronic obstructivepulmonary disease (25%). No aberrations were detected in paired peripheral blood lymphocytes (except for one osteoarthritiscase with a karyotype 45,X[10]/46,XX[17]), or in peripheral blood monocytes and synovial tissue of normals/joint trauma.Because M� aberrations were common to chronic joint and pulmonary disease, chronic inflammatory stress may inducechromosomal aberrations with potential functional relevance in local mesenchymal cells and infiltrating leukocytes in anorgan-independent fashion. © 2003 Wiley-Liss, Inc.
INTRODUCTION
Human rheumatoid arthritis (RA) is character-ized by chronic inflammation and destruction ofmultiple joints, perpetuated by an invasive pannustissue. Activated synovial fibroblasts (SFB),whether reversibly stimulated by the inflammatorymicroenvironment (Fassbender, 1983; Fox et al.,1990; Aicher et al., 1994; Kinne et al., 1995) orirreversibly transformed (Fassbender, 1983; Aicheret al., 1994; Firestein, 1998; Nishioka et al., 1998),are a major component of the pannus and contrib-ute to the joint destruction by secretion of pro-inflammatory cytokines and tissue-degrading en-zymes (Kinne et al., 1995; Hirth et al., 2002). The“semi-transformed” character of RA-SFB has beenaddressed by analyzing their (proto)-oncogene ex-pression (reviewed in Kinne et al., 1995), their rateof proliferation/apoptotic cell death (Nishioka etal., 1998), their capacity to erode cartilage in SCID-
mice transfer models (Firestein, 1998; unpublisheddata), and their karyotype alterations (Ermis et al.,1993, 1995; Mertens et al., 1993; Weiss et al., 1999).
Whereas specific chromosomal aberrations are ofparticular interest with regard to malignant trans-formation and biological behavior of cells (e.g., in-vasiveness, in analogy to observations in hemato-logical malignancies and solid tumors; Mertens et
Supported by: German Federal Ministry of Education and Re-search (BMBF); Grant number: 01KS9504; Interdisciplinary Centerfor Clinical Research (IZKF) Leipzig; Grant numbers: 01VM9311/3and 01ZZ9602; IZKF, Jena; Thuringian Ministry of Science, Re-search, and Art; Grant number: B311-00026.
*Correspondence to: Dr. R. W. Kinne, Experimental Rheumatol-ogy Unit, Friedrich Schiller University Jena, Winzerlaer Str. 10,D-07745 Jena, Germany. E-mail: [email protected]
Received 4 February 2003; Accepted 8 May 2003DOI 10.1002/gcc.10242
GENES, CHROMOSOMES & CANCER 38:53–67 (2003)
© 2003 Wiley-Liss, Inc.

al., 1993), recent evidence indicates that chromo-somal abnormalities may also be of biological rele-vance in non-transformed cells, including synovialcells derived from patients with RA (Ermis et al.,1993, 1995; Johansson et al., 1993; Mertens et al.,1993, 1996; Weiss et al., 1999; Kinne et al., 2001).However, these karyotype alterations do not ap-pear to be restricted to RA, given that they werealso observed in pigmented villonodular synovitis(Mertens et al., 1993), osteoarthritis (OA) (Mertenset al., 1996; Kinne et al., 2001), and, for that matter,in normal brain tissue (Heim et al., 1989).
The question of whether chromosomal aberra-tions in chronic joint disease are restricted to SFBor apply more broadly to different cell types can beanswered best by analyzing in parallel synovialmacrophages (M�), a major infiltrating inflamma-tory cell type in the RA synovial membrane. M�are present in high numbers in RA synovial tissue,show a high activation status, and are subject to thesame inflammatory microenvironment (Kinne etal., 2000). It has recently been demonstrated thatpaired synovial M� and SFB can be isolated fromthe primary culture of synovial cells by use ofanti-CD14-Magnetobeads (Zimmermann et al.,2001). This avoids the repeated passaging that typ-ically leads to complete loss of synovial M� duringthe culture process.
Thus, the goals of the present study were: (1) toassess whether, in addition to first-passage (P-1)SFB, synovial M� (P-1) in RA are also affected bychromosomal aberrations, and to distinguish therelative contribution of these two major synovialcell populations to the chromosomal aberrationsobserved in whole synovial membrane samples;and (2) to analyze the specificity of the aberrationsfor RA by comparison with other rheumatic dis-eases (inflammatory/degenerative), joint trauma/normals, and (for tissue M�) chronic obstructivepulmonary disease (COPD). The first point was aparticular focus of the present study because todate analyses of trisomy/polysomy 7 (�7) have usu-ally been carried out either in non-separated syno-vial cells (including a mixture of mesenchymal andinflammatory cells), or in repeatedly passaged SFB(Ermis et al., 1993, 1995; Mertens et al., 1993, 1996;Weiss et al., 1999).
MATERIALS AND METHODS
Patients
Inflamed synovial tissue and paired, heparinizedperipheral blood (for lymphocyte culture) were ob-
tained from RA patients (n � 10), OA patients (n �14), and from one patient with reactive arthritis(Table 1). The patients were classified according tocriteria from the American College of Rheumatol-ogy/American Rheumatism Association (Altman etal., 1986; Arnett et al., 1988). Controls were: (1)synovial tissue/cells from nine patients with eitherno joint disease or recent joint trauma; and (2)peripheral blood monocytes from 10 normal do-nors, derived either by consecutive application of aFicoll-hypaque gradient (d � 1.077 g/ml) and ad-herence on glass slides in QuadriPERM wells(Heraeus, Hanau, Germany) or by flow cytometrysorting from the buffy coat (Table 1). Disease con-trols for synovial M� were M� from the broncho-alveolar lavage (BAL) fluid of eight patients withCOPD (total count of nucleated cells � 1.6 �0.3 � 107 cells; mean � SE; Table 1).
BAL was performed according to the technicalrecommendations and guidelines of the TaskGroup on BAL of the European Society of Pneu-mology. Briefly, 3 � 50 ml of a 0.9% NaCl solutionwere instilled in the middle lobe, immediately as-pirated into plastic tubes by use of a vacuum suc-tion system, and subsequently stored at 4°C untiluse. BAL samples were first filtered through a two-layer gauze. Cells were then centrifuged at 500 � gfor 10 min followed by removal of the supernatant.After cytocentrifugation and staining with May–Grunwald–Giemsa, the relative proportions of thevarious leukocyte subpopulations in BAL fluidwere determined by a differential cytologic countof 1,000 cells. The total count of nucleated BALcells was determined in a Neubauer chamber afterKimura staining.
Paired synovial tissue and peripheral blood sam-ples were obtained during open joint replacementsurgery or arthroscopic synovectomy at the Depart-ment of Orthopedics, University of Leipzig, andthe Clinic of Orthopedics, Eisenberg, Germany.The study was approved by the ethics committeesof the respective universities. Blood samples wereimmediately transferred to the Institute of HumanGenetics for lymphocyte culture and karyotype/FISH analysis. Synovial tissue was placed in cellculture medium at ambient temperature and sub-jected to tissue digestion within 2 hr.
Tissue Digestion, Cell Culture, and SFB/M�
Isolation
Synovial M� and SFB were obtained by colla-genase/trypsin digestion of synovial tissue, 7 days/primary culture of synovial cells, and subsequent
54 KINNE ET AL.

separation of synovial M� and SFB by use ofDynabeads M-450 CD14 (Zimmermann et al.,2001).
Flow Cytometry
FACS analyses of isolated synovial M� and SFBwere performed on a FACScan (Becton Dickinson,San Jose, CA) according to standard procedures(Pelegri et al., 1996), by use of isotype-matchedmonoclonal antibodies as specificity controls. Un-conjugated SFB negatively isolated with Dyna-beads M-450 CD14 showed a high enrichment(typically �95% prolyl 4-hydroxylase�/�92% Thy-1/CD90�; Hirth et al., 2002), with a contaminationof �2% leukocytes or endothelial cells (Zimmer-mann et al., 2001; Hirth et al., 2002).
M� positively isolated from primary culture byuse of Dynabeads M-450 CD14 showed �90%enrichment, as assessed by small, round morphol-ogy and attached Dynabeads M-450 CD14 uponreculture (Zimmermann et al., 2001). M� fromBAL and monocytes from normal peripheral blood
also showed �90% enrichment by May–Grun-wald–Giemsa staining/FACS analysis with anti-CD14 monoclonal antibodies (mAbs) (M�P9; Bec-ton Dickinson, Heidelberg, Germany) or anti-CD68 mAbs (PG-M1), except for cases BAL5a(83.7%) and BAL5b (76.5%).
GTG-Banding and Fluorescence in SituHybridization
Cytogenetic studies of peripheral blood lympho-cytes (PBLs) were performed according to standardmethods (RPMI medium with 10% FCS and 1.2%phytohemagglutinin in a 72-hr culture). For cyto-genetic studies of primary-culture synovial cells(collagenase digest; i.e., adherent synovial cells),SFB (P-1), and synovial M� (P-1; for culture timessee Table 2), cells were seeded at a density of0.5 � 105 cells/glass slide in QuadriPERM-wells(Heraeus). Primary-culture synovial cells and SFBwere treated at near confluency with Colcemid (1�g/ml) for 1.75 hr, followed by hypotonic treatment
TABLE 1. Clinical Characteristics of the Patients at the Time of Synovectomy/Sampling
Patients(total)
Gendera
(M/F)Age
(years)Disease
duration (years)RFb
(�/)ESRc
(mm/1 hr)CRPd
(mg/L)No. of ARA
criteria (RA)eConcomitant
medication (n)f
Rheumatoid arthritis10 4/6 66.3 � 3.4 8.9 � 3.1
(n.d. � 1)6/1
(n.d. � 3)38.8 � 9.0(n.d. � 2)
34.1 � 7.6 5.1 � 0.3 MTX (5)Prednisolone (8)Sulfasalazine (2)Leflunomide (1)NSAIDs (8)
Osteoarthritis14 2/12 70.3 � 1.6 6.8 � 2.0
(n.d. � 10)0/1
(n.d. � 13)17.4 � 3.9(n.d. � 5)
8.2 � 1.8(n.d. � 1)
0.4 � 0.1 Prednisolone (1)NSAIDs (8)None (6)
Reactive arthritis1 1/0 43 8 n.d. 60 8.5 1 None
Joint trauma6 3/3 30.2 � 4.4 0.7 � 0.4 n.d. n.d. n.d. 0.0 � 0.0 None
Normals (synovial membrane n � 3; peripheral blood monocytes n � 10)13 7/6 43.8 � 5.0 0.0 � 0.0 n.d. n.d. n.d. 0.0 � 0.0 None
Chronic obstructive pulmonary disease WBC8 5/3 55.0 � 3.7 5.9 � 3.2
(n.d. � 1)n.d. 31.7 � 22.7
(n.d. � 5)38.6 � 22.6(n.d. � 4)
10.4 � 0.9(n.d. � 1)
Erythromycin (2)ClarythromycinCotrimoxazole (1)Bleomycin (1)(esophageal carc.)NSAIDs (1)None (4)
aM, male; F, female.bRF, rheumatoid factor; �/, positive/negative.cESR, erythrocyte sedimentation rate (mm).dCRP, C-reactive protein, normal range: �5 mg/L.eARA, American Rheumatism Association (now American College of Rheumatology); n.d., not determined; WBC, white blood cell count (�109/L).fMTX, methotrexate; NSAIDs, non-steroidal anti-inflammatory drugs; data are shown as means � SEM.
55CHROMOSOMAL ABERRATIONS IN SYNOVIAL FIBROBLASTS/MACROPHAGES

with 0.2% MgCl2/0.4% sodium citrate solution for10 min, both at 37°C. The cells were fixed withthree changes of methanol/acetic acid (3:1; 10 mineach; room temperature) and air-dried underlaminar flow. GTG-banding was performed ac-cording to standard protocols (Seabright, 1971)on 10 –50 metaphase cells/case. Karyotypes weredescribed according to the ISCN (Mitelman,1995). M� and monocytes were analyzed after 1day of adherence by fluorescence in situ hybrid-ization (FISH) only.
Extraction of nuclei from formalin-fixed/paraf-fin-embedded or cryofixed tissue was performedaccording to Liehr et al. (1995, 1996). FISH anal-ysis of the copy number of particular chromosomesin interphase nuclei was performed according tostandard protocols (Vysis, Downers Grove, IL) byapplying fluorescence-labeled, repetitive, -satel-lite DNA probes (Vysis), specific for the centro-meric region of each chromosome. Normally,centromere probes for four different chromo-somes were used per case, selected on the basisof previous literature reports and clonal or non-clonal numerical aberrations detected by GTGbanding. One hundred cells/sample were exam-ined by applying dual-color FISH. Because inmost cases ex vivo data (i.e., nuclei extractedfrom synovial tissue) or data from mixed synovialcells (collagenase digest) could be compared toin vitro data (P-1 SFB or P-1 M�), paired valuesfor individual patients were included/reportedeven if they did not reach the cutoff level (Ta-bles 3– 6; Figs. 1–3).
Data were analyzed and depicted either on thebasis of the total polysomy of nuclei, that is, irre-spective of the underlying mechanism and pointedto the total gain of potential gene transcriptionunits, or selectively on the basis of trisomic nuclei,
focusing on non-disjunction as a possible underly-ing mechanism.
In the present study, only RA/OA patients withcytogenetic findings in synovial M� were included(in almost all cases paired with SFB). This resultedin numerical differences from previously publisheddata (Kinne et al., 2001), but without changes inthe overall findings.
Statistical Analysis
Because of multiple comparisons, the data werefirst subjected to the multi-group Kruskal–Wallistest. The non-parametric Mann–Whitney u testwas then applied to analyze differences betweendata of different disease groups. The SpearmanRank correlation test was used to analyze correla-tions among parameters and between these param-eters and the clinical status/treatment of individualpatients. In all cases, differences were consideredstatistically significant at P � 0.05. Analyses wereperformed by use of the SPSS 9.0 program (SPSS,Chicago, IL).
RESULTS
Cutoff Gates for Numerical ChromosomalAberrations in Synovial Tissue, Primary-CultureSynovial Cells, SFB, and Synovial/Bronchial M�
For synovial tissue, primary-culture synovialcells, and SFB (P-1), cutoff gates of 4% for trisomicand/or polysomic nuclei and of 7% for monosomicnuclei were set (numerical chromosomal aberra-tions as detected by interphase FISH), based onresults from normal bone marrow cells, amniocytes,PBLs, and skin fibroblasts (Gebhart et al., 1993;unpublished data). For trisomic/polysomic inter-phase nuclei, these values were higher than previ-ously published for trisomic interphase nuclei in
TABLE 2. Culture Time (Days) of Synovial Cells in Primary Culture (Collagenase Digest), Synovial/Pulmonary Macrophages,and Synovial Fibroblasts From Patients With Rheumatoid Arthritis, Osteoarthritis, Reactive Arthritis, Joint Trauma, and Chronic
Obstructive Pulmonary Disease*
Source of cellsSynovial cells
(collagenase digest)Synovial/pulmonary macrophages
or monocytes, first passageSynovial fibroblasts,
first passage
Rheumatoid arthritis 9.2 � 3.3 (n � 5) 8.6 � 0.4 (n � 7) 13.4 � 2.1 (n � 7)Osteoarthritis 7.3 � 1.4 (n � 11) 8.0 � 0.0 (n � 14) 14.2 � 2.1 (n � 13)Reactive arthritis 5.0 (n � 1) 8.0 (n � 1) 20.0 (n � 1)Joint trauma 5.0 (n � 1) 21.3 � 7.8 (n � 3) 23.3 � 6.2 (n � 3)Chronic obstructive
pulmonary disease n.a. 1.0 � 0.0 (n � 8) n.a.Normal donors
(peripheral blood) n.a. 1.0 � 0.0 (n � 10) n.a.
*Data are shown as means � SEM; n.a., not analyzed.
56 KINNE ET AL.

leukemia (3%; Gebhart et al., 1993), to account forthe unknown tissue investigated and to consider aspathological values only those that exceeded vari-
ations in cells from normal tissue. In the case ofsynovial M� (derived from joint trauma, RA, OA,and reactive arthritis) or BAL M� from COPD,
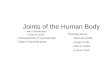
Figure 1. Numerical chromosomal aberrations in the RA synovial membrane. Polysomy (hatched bars)and trisomy (shaded bars) of the individual chromosomes are depicted as means � SE of n � 1–10 patients.Normal cutoff levels are indicated by broken lines. P-0, primary culture; P-1, first passage.
57CHROMOSOMAL ABERRATIONS IN SYNOVIAL FIBROBLASTS/MACROPHAGES

cutoff gates of 2% for trisomic and/or polysomicnuclei and of 7% for monosomic nuclei were setbased on results in normal peripheral blood mono-cytes (n � 10; Table 3).
Numerical Chromosomal Aberrations in RAPatients
Peripheral blood lymphocytes
As previously published (Kinne et al., 2001),PBLs showed normal findings in all RA patients(Table 4).
Synovial M�
P-1 synovial M� showed numerical chromo-somal aberrations exceeding cutoff levels in 9/10RA patients (90%), consisting of gains or losses ofchromosomes 6, 7, 8, 9, and 12 (Table 4). Thechromosome predominantly affected was 7 (8/9cases with alterations).
SFB
P-1 SFB of 6/9 RA patients (66%) displayednumerical chromosomal aberrations involving chro-
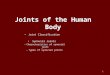
Figure 2. Numerical chromosomal aberrations in the OA synovial membrane. Polysomy (hatched bars)and trisomy (shaded bars) of the individual chromosomes are depicted as means � SE of n � 2–14 patients.Normal cutoff levels are indicated by broken lines. P-0, primary culture; P-1, first passage.
58 KINNE ET AL.

mosomes 4, 7, 8, 9, 12, and 18 (Table 4). As forsynovial M�, chromosome 7 was the one predom-inantly affected (6/6 patients).
Numerical Chromosomal Aberrations in OAPatients
Peripheral blood lymphocytes
Except for one patient with a karyotype45,X[10]/46,XX[17] (i.e., a mosaic form of theTurner syndrome) and previously published struc-tural aberrations without pathologic relevance (fordetails see Kinne et al., 2001), PBLs showed nor-mal cytogenetic findings in all OA patients forwhom karyotype analysis was performed (Table 5).
Synovial M�
In 13/14 OA patients (93%), synovial M� (P-1)showed numerical chromosomal aberrations ex-ceeding cutoff levels, including gains or losses ofchromosomes 4, 6, 7, 8, 9, 11, 12, X, and Y (Table5). As in RA patients, chromosome 7 was predom-inantly affected (11/13 cases with alterations).
SFB
In 12/12 OA patients for whom analysis wasperformed (100%), P-1 SFB showed numericalchromosomal aberrations involving chromosomes4, 5, 6, 7, 8, 9, and 12 (Table 5). Chromosome 7 waspredominantly affected (11/12 patients).
Quantitative Comparison of the Mean Level ofPolysomies/Monosomies for DifferentChromosomes ex Vivo and in Vitro in RA and OA
Although clearly above the cutoff levels (4%) inindividual patients (Tables 4 and 5), the meanpercentages for polysomies of chromosomes 4, 6, 8,9, and/or 18 in synovial tissue of RA or OA patientsdid not exceed cutoff levels (Figs. 1 and 2; notably,the marginal increase for polysomy 8 in RA and OAhas not been confirmed in a larger group of pa-tients; Kinne et al., 2001). The same was true formonosomies of chromosomes 7 and 18, althoughthe percentage of P-1 synovial M� monosomic forchromosome 7 in RA (7.6%) marginally exceededthe 7% cutoff. In P-1 SFB, only polysomies forchromosomes 4 and/or 7 exceeded cutoff levels(Figs. 1 and 2). The most consistent changes wereobserved for polysomy 7; the mean percentage wassimilarly elevated in synovial tissue and collage-nase digest. Both synovial M� (RA: 4.3%, n � 10;OA: 9.0%, n � 14) and, predominantly, SFB (RA:13.0%, n � 7; OA: 16.1%, n � 12) contributed topolysomy 7 in synovial tissue (Figs. 1 and 2).
If only trisomic nuclei were considered (Figs. 1and 2; shaded bars), the percentage of cells withaberrations was generally lower, indicating thatboth non-disjunction and endoreduplication con-
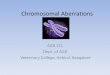
Figure 3. Comparison of numerical chromosomal aberrations in theRA, OA, and normal/joint trauma (JT) synovial membrane. Trisomies ofchromosome 7 in extracted nuclei from synovial tissue, non-separatedsynovial cells (collagenase digest), isolated macrophages (P-1), and iso-lated synovial fibroblasts (FB; P-1) are depicted as means � SE of n �1–14 patients. # P � 0.05 vs. normal/JT; (#) borderline significantdifference (P � 0.08) vs. normal/JT; * P � 0.05 vs. RA.
59CHROMOSOMAL ABERRATIONS IN SYNOVIAL FIBROBLASTS/MACROPHAGES

tributed to the aberrations observed ex vivo and invitro. The specificity of the changes for trisomy/monosomy 7 was further emphasized in this casebecause none of the other aberrations exceededcutoff levels (Figs. 1 and 2).
Comparison of ex Vivo and in Vitro Findings forIndividual Patients
Numerical aberrations observed in RA and OAtissue as a whole (i.e., in nuclei extracted from thesynovial membrane; Tables 4 and 5) showed goodcorrespondence with the findings in the collage-nase digest (adherent mixture of synovial cells; invitro culture for �7–9 days). In addition, the valuesobserved in isolated, P-1 synovial M� (in vitroculture for �8–9 days) and P-1 SFB (in vitro cul-ture for �13–14 days) were compatible with thevalues obtained for the collagenase digest (35%CD14-positive M�; 56% CD14-negative cells; n �9) or in synovial tissue (containing both non-adher-ent and adherent cells; Tables 4 and 5). In fact,there were significant positive correlations in RAbetween the percentages of polysomies for chro-mosome 7 in collagenase digest and P-1 SFB (n �5; P � 0.028; rho 0.918) and in OA between thepercentages of trisomies for chromosome 7 in col-lagenase digest and P-1 SFB (n � 8; P � 0.009; rho0.837). Also, the percentages of trisomies for chro-mosome 7 in P-1 synovial M� and P-1 SFB weresignificantly correlated in both RA (n � 7; P �0.031; rho 0.800) and OA (n � 12; P � 0.018; rho0.667).
Numerical Chromosomal Aberrations in OtherJoint Diseases
Whereas PBLs showed no cytogenetic abnormal-ities, numerical chromosomal aberrations were ob-
served in one patient with reactive arthritis [i.e., inP-1 M� (monosomy 7) and SFB (polysomy 10?)],indicating that the aberrations were not restrictedto RA and OA, but extended to other rheumaticdiseases (Table 6).
Limited Degree of Chromosomal Aberrations inNormal/Joint Trauma Patients
Nuclei extracted from synovial tissue, collagenasedigest, synovial M�, and SFB
In nine control patients (six joint trauma andthree normal donors), the nuclei extracted fromsynovial tissue and/or mixed synovial cells (colla-genase digest) showed normal cytogenetic findings(Table 6). In two joint trauma patients, polysomiesof multiple chromosomes exceeding the cutoff lev-els were present in P-1 synovial M� and SFB(Table 6).
The mean percentages for polysomies 4 (3.3%),6 (2.5%), 7 (5.3%), and 9 (2.7%) in P-1 synovial M�from joint trauma patients exceeded cutoff levels(2%). This was not the case if only trisomic nucleiwere considered (data not shown).
Direct Comparison Between NumericalChromosomal Aberrations in the SynovialMembrane of RA, OA, and Normal/Joint TraumaPatients
Both OA and RA displayed an elevation of poly-somy 7 in synovial tissue in comparison to normal/joint trauma; however, only the difference betweenOA and controls reached statistical significance(Zimmermann et al., 2001). In RA and OA, bothsynovial M� and SFB contributed to the polysomy7 observed in nuclei from synovial tissue and col-lagenase digest (containing a mixture of synovial
TABLE 3. Signal Distribution of -satellite DNA Probes for Chromosomes 1, 3, 4, 6, 7, 8, 9, 10, 12, and 18 on Interphase Nucleiof Peripheral Blood Monocytes From Normal Donors
ChromosomeNo. ofdonors
Mean percentage (range) of nuclei showing n signals
n � 0 n � 1 n � 2 n � 3 n � 4
1 9 0 1.2 (0–6) 98.8 (94–100) 0 03 9 0 1.1 (0–3) 98.9 (97–100) 0 04 10 0 1.6 (0–3) 98.3 (97–100) 0.1 (0–1) 06 10 0 2.4 (0–5) 97.6 (95–100) 0.2 (0–2) 07 10 0 1.1 (0–3) 98.9 (97–100) 0 08 9 0 1.4 (0–4) 98.2 (96–100) 0.3 (0–2) 09 9 0 2.3 (0–5) 97.6 (95–100) 0.1 (0–1) 0
10 9 0 2.4 (1–5) 97.4 (95–99) 0.1 (0–1) 011 9 0 2.7 (0–6) 97.2 (94–99) 0.1 (0–1) 012 9 0 3.1 (0–6) 96.4 (92–100) 0.3 (0–2) 0.1 (0–1)18 10 0 3.2 (0–6) 96.7 (94–100) 0.1 (0–1) 0
60 KINNE ET AL.

TA
BLE
4.C
ytog
enet
icFi
ndin
gsin
Peri
pher
alBl
ood
Lym
phoc
ytes
,Nuc
leiE
xtra
cted
from
Syno
vial
Tis
sue,
Col
lage
nase
Dig
est,
Syno
vial
Mac
roph
ages
,an
dSy
novi
alFi
brob
last
sof
Patie
nts
with
Rhe
umat
oid
Art
hriti
s*
Patie
ntID
Kar
yoty
pe/F
ISH
Peri
pher
albl
ood
lym
phoc
ytes
Nuc
leie
xtra
cted
from
syno
vial
tissu
eC
olla
gena
sedi
gest
Syno
vial
mac
roph
ages
,firs
tpa
ssag
eSy
novi
alfib
robl
asts
,firs
tpa
ssag
e
L07
46,X
Yn.
a.n.
a.FI
SH:�
6[4%
];�
7[3%
];�
7[33
%];
�8[
17%
]46
,XY
L12
46,X
Yn.
a.n.
a.FI
SH:�
9[3%
];�
6[68
%];
�7[
34%
];�
8[27
%]
46,X
YEB
646
,XX
FISH
:�6[
7%];
�7[
12%
];�
8[2%
];8[
0%];�
18[8
%]
incl
.pol
yplo
id[1
%]
n.a.
FISH
:�6[
1%];�
7[9%
];�
8[0%
];8[
3%];
18
[0%
]47
,XX
,�7[
6]/4
6,X
X[6
]FI
SH:�
6[3%
];�7[
40%
];�
8[5%
];�
8[8%
];�
18[9
%]
EB20
46,X
YFI
SH:n
orm
alFI
SH:�
7[2%
];�12
[5%
]46
,XY
FISH
:�7[
4%];
�12
[5%
]FI
SH:�
6[3%
];�
7[8%
];�
12[1
0%];
incl
.pol
yplo
id[1
%]
46,X
YFI
SH:�
7[9%
];�
12[1
4%];
incl
.pol
yplo
id[1
%]
EB23
46,X
XFI
SH:n
orm
aln.
a.46
,XX
FISH
:�7[
4%];
�9[
3%]
FISH
:�7[
5%];
�9[
4%]
46,X
XFI
SH:�
7[9%
];�
9[5%
]EB
2546
,XX
FISH
:nor
mal
FISH
:6[
0%];�
7[4%
];�
8[5%
];
9[0%
]n.
a.FI
SH:�
6[20
%];
�7[
2%];�
8[0%
];�9[
8%]
n.a. FI
SH:n
orm
alEB
2646
,XY
FISH
:nor
mal
FISH
:�7[
8%];
�8[
n.a.
]46
,XY
FISH
:�7[
12%
];�
8[3%
]
FISH
:�7[
5%];
�8[
1%]
46,X
YFI
SH:�
7[14
%];
�8[
5%];
incl
.pol
yplo
id[2
%]
EB27
46,X
XFI
SH:n
orm
alFI
SH:�
7[0%
];�8[
8%];
�18
[7%
]n.
a. FISH
:�7[
7%];
�8[
n.a.
];�18
[n.a
.]
FISH
:�7[
3%];
�8[
n.a.
];�18
[n.a
.]47
,XX
,�7[
2]FI
SH:�
7[13
%];
�8[
n.a.
];�18
[n.a
.]in
cl.p
olyp
loid
[2%
]EB
3046
,XX
FISH
:nor
mal
n.a.
n.a.
FISH
:nor
mal
n.a.
EB31
46,X
X,1
6qh�
FISH
:nor
mal
n.a.
46,X
X,1
6qh�
FISH
:�
4[1%
];�7[
4%]
FISH
:�4[
1%];�
7[3%
]46
,XX
,16q
h�FI
SH:�
4[5%
];�
7[5%
];in
cl.p
olyp
loid
[5%
]
*Val
ues
abov
eno
rmal
cuto
ffle
vels
are
indi
cate
din
bold
.Pai
red
valu
esfo
rex
vivo
data
(i.e.
,nuc
leie
xtra
cted
from
syno
vial
tissu
e),d
ata
from
mix
edsy
novi
alce
lls(c
olla
gena
sedi
gest
),an
din
vitr
oda
ta(P
-1SF
Bor
P-1
M�
)ar
ere
port
edin
italic
sev
enif
they
did
not
reac
h/ex
ceed
the
cuto
ffle
vel.
N.B
.Exc
ept
for
the
resu
ltsof
syno
vial
mac
roph
ages
(col
umn
5)al
loth
erre
sults
wer
epu
blis
hed
prev
ious
ly(R
.W.K
inne
etal
.,20
01)
and
are
incl
uded
only
toal
low
the
com
pari
son
betw
een
syst
emic
(blo
od)
and
loca
l(sy
novi
altis
sue)
aber
ratio
nsor
betw
een
tissu
ean
dis
olat
edce
lls.
61CHROMOSOMAL ABERRATIONS IN SYNOVIAL FIBROBLASTS/MACROPHAGES

TA
BLE
5.C
ytog
enet
icFi
ndin
gsin
Peri
pher
alBl
ood
Lym
phoc
ytes
,Nuc
leiE
xtra
cted
From
Syno
vial
Tis
sue,
Col
lage
nase
Dig
est,
Syno
vial
Mac
roph
ages
,an
dSy
novi
alFi
brob
last
sof
Patie
nts
With
Ost
eoar
thri
tis*
Patie
ntID
Kar
yoty
pe/F
ISH
Peri
pher
albl
ood
lym
phoc
ytes
Nuc
leie
xtra
cted
from
syno
vial
tissu
eC
olla
gena
sedi
gest
Syno
vial
mac
roph
ages
,firs
tpa
ssag
eSy
novi
alfib
robl
asts
,firs
tpa
ssag
e
EB12
45,X
[10]
/46,
XX
[17]
FISH
:�4[
0%];�
7[12
%];
�8[
12%
];
8[0%
];�
9[4%
]
n.a.
FISH
:�4[
1%];�
7[18
%];
�8[
2%];
8[
8%];�
9[12
%]
48,X
X,�
7,�
4o
r�
5[3]
/46,
XX
[4]
FISH
:X
[32%
]FI
SH:�
4[4%
];�7[
42%
];�
8[0%
];
8[3%
];�9[
11%
]EB
1446
,XX
FISH
:�7[
14%
];�
8[0%
];�
X[4
%]
n.a.
FISH
:�7[
11%
];�
8[5%
];�
9[3%
];�
X[4
%]
incl
.pol
yplo
id[3
%]
47,X
X,�
7[3]
/46.
XX
[7]
FISH
:nor
mal
FISH
:�7[
10%
];�
8[0%
];�X
[6%
]FI
SH:�
7[36
%];
�8[
2%];�
X[0
%]
EB15
46,X
Xn.
a.n.
a.FI
SH:�
6[8%
];�
6[1%
];�7[
6%];
�8[
0%];�
9[4%
]46
,XX
FISH
:nor
mal
FISH
:6[
0%];�
6[7%
];�
7[10
%];
�8[
7%];
�9[
10%
];in
cl.p
olyp
loid
[7%
]EB
1646
,XX
n.a.
FISH
:�6[
5%];
�7[
18%
];�
8[0%
];�
X[0
%];�
X[1
8%]
FISH
:�6[
0%];�
7[0%
];�8[
6%];
�X
[4%
];�
X[1
0%]
n.a.
FISH
:nor
mal
EB17
46,X
Xn.
a.46
,XX
,chr
b(1)
(q12
)[2]
/46
,XX
[4]
FISH
:�4[
2%];�
6[2%
];�7[
4%];
�8[
0%];�
11[1
0%];
�12
[0%
];�
12[1
0%]
46,X
XFI
SH:n
orm
alFI
SH:�
4[17
%];
�6[
3%];�
7[4%
];�
8[3%
];�11
[0%
];�
12[1
%];
12[4
%]
FISH
:�4[
16%
];�
6[6%
];�
7[1%
];�
8[4%
];�11
[4%
];�12
[5%
];
12[4
%]
incl
.pol
yplo
id[1
%]
EB18
46,X
Xn.
a.46
,XX
FISH
:�7[
2%];�
8[4%
]46
,XX
FISH
:nor
mal
FISH
:�7[
1%];
�8[
0%]
FISH
:�7[
5%];
�8[
4%]
EB19
46,X
XFI
SH:�
7[18
%];
�8[
2%];
�9[
4%];�
12[4
%];
incl
.pol
yplo
id[2
%]
46,X
XFI
SH:�
7[16
%];
�8[
4%];
�9[
3%];
�12
[4%
]47
,XX
,�7[
2]/4
6,X
X[7
]FI
SH:n
orm
alFI
SH:�
7[14
%];
�8[
0%];�
9[0%
];�
12[0
%]
incl
.pol
yplo
id[1
%]
FISH
:�7[
10%
];�
8[0%
];�9[
4%];
12[7
%]
EB21
46,X
Xn.
a.46
,XX
FISH
:�4[
6%];
�6[
6%];
�7[
10%
];�
9[4%
];in
cl.
poly
ploi
d[2
%]
46,X
XFI
SH:n
orm
alFI
SH:�
4[17
%];
�6[
7%];
�7[
11%
];�
9[17
%];
incl
.po
lypl
oid
[5%
]
FISH
:�4[
3%];�
6[3%
];�7[
5%];
�9[
3%];
incl
.pol
yplo
id[1
%]
Con
tinue
d
62 KINNE ET AL.

TA
BLE
5.C
ytog
enet
icFi
ndin
gsin
Peri
pher
alBl
ood
Lym
phoc
ytes
,Nuc
leiE
xtra
cted
From
Syno
vial
Tis
sue,
Col
lage
nase
Dig
est,
Syno
vial
Mac
roph
ages
,and
Syno
vial
Fibr
obla
sts
ofPa
tient
sW
ithO
steo
arth
ritis
*(C
ontin
ued)
Patie
ntID
Kar
yoty
pe/F
ISH
Peri
pher
albl
ood
lym
phoc
ytes
Nuc
leie
xtra
cted
from
syno
vial
tissu
eC
olla
gena
sedi
gest
Syno
vial
mac
roph
ages
,firs
tpa
ssag
eSy
novi
alfib
robl
asts
,firs
tpa
ssag
e
EB22
46,X
Yn.
a.n.
a.FI
SH:�
4[2%
];�7[
4%];
incl
.pol
yplo
id[1
%]
46,X
YFI
SH:n
orm
alFI
SH:�
4[4%
];�7[
7%];
incl
.pol
yplo
id[1
%]
FISH
:�4[
2%];�
7[6%
];in
cl.p
olyp
loid
[1%
]EB
2446
,XX
FISH
:�4[
0%];�
6[3%
];�
7[7%
];�
9[3%
]n.
a.FI
SH:�
4[1%
];�6[
4%];
�7[
13%
];�
9[6%
]46
,XX
FISH
:nor
mal
FISH
:�4[
8%];
�6[
8%];
�7[
25%
];�
9[8%
];in
cl.p
olyp
loid
[7%
]
FISH
:�4[
9%];
�6[
2%];�
7[33
%];
�9[
3%];
incl
.pol
ypoi
d[2
%]
EB29
46,X
XFI
SH:n
orm
aln.
a.n.
a.FI
SH:n
orm
aln.
a.
J4n.
a.FI
SH:�
4[5%
];�
7[14
%];
incl
.pol
yplo
id[1
%]
n.a.
FISH
:�4[
3%];
�7[
24%
];in
cl.p
olyp
loid
[1%
]46
,XX
FISH
:�4[
1%];�
7[6%
];in
cl.p
olyp
loid
[1%
]J5
n.a.
FISH
:�4[
5%];
�7[
13%
]n.
a.FI
SH:�
4[0%
];�7[
12%
]n.
a.FI
SH:�
4[1%
];�7[
15%
]FI
SH:�
4[1%
];�
7[20
%]
EB61
46,X
Yn.
a.45
,X,�
Y[4
]/46
,XY
[3]
FISH
:�6[
0%];�
7[6%
];�
X[3
%];
�Y
[8%
]n.
a.n.
a.n.
a.FI
SH:�
6[8%
];�
7[19
%];
Y[
2%]
incl
.pol
yplo
id[2
%]
*Val
ues
abov
eno
rmal
cuto
ffle
vels
are
indi
cate
din
bold
.Pai
red
valu
esfo
rex
vivo
data
(i.e.
,nuc
leie
xtra
cted
from
syno
vial
tissu
e),d
ata
from
mix
edsy
novi
alce
lls(c
olla
gena
sedi
gest
),an
din
vitr
oda
ta(P
-1SF
Bor
P-1
M�
)ar
ere
port
edin
italic
sev
enif
they
did
not
reac
hth
ecu
toff
leve
l.N
.B.E
xcep
tfo
rth
ere
sults
ofsy
novi
alm
acro
phag
es(c
olum
n5)
allo
ther
resu
ltsw
ere
publ
ishe
dpr
evio
usly
(R.W
.Kin
neet
al.,
2001
)an
dar
ein
clud
edon
lyto
allo
wth
eco
mpa
riso
nbe
twee
nsy
stem
ic(b
lood
)an
dlo
cal(
syno
vial
tissu
e)ab
erra
tions
orbe
twee
ntis
sue
and
isol
ated
cells
.
63CHROMOSOMAL ABERRATIONS IN SYNOVIAL FIBROBLASTS/MACROPHAGES

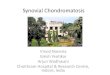
cells). These findings were confirmed if only tri-somic nuclei were considered, although in this casetrisomy 7 in RA synovial tissue was borderlinesignificantly higher in comparison with normal/joint trauma tissue (Fig. 3). Interestingly, trisomy 7in synovial M� from RA and OA (but also fromjoint trauma) was significantly higher than that innormal peripheral blood monocytes (Fig. 4), indi-cating that joint trauma of limited duration (0.7 �0.4 years; Table 1) may already result in numericalchromosomal aberrations of synovial M�.
Similar Occurrence of Chromosomal Aberrationsin M� From Chronic Joint and Pulmonary Disease
BAL M� derived from COPD were also ana-lyzed to answer the question of whether the occur-rence of numerical chromosomal aberrations in tis-sue M�, as observed in RA, OA, and reactivearthritis, was unique to chronic inflammation in thejoint. The bronchial M� displayed gains of chro-mosomes 4 and 7 in 2/8 patients (25%), indicatinga generalized effect of chronic inflammation on
TABLE 6. Cytogenetic Findings in Peripheral Blood Lymphocytes, Nuclei Extracted From Synovial Tissue, Synovial Cells in theCollagenase Digest, Synovial Macrophages (or Bronchial Macrophages From Patients With COPD), and Synovial Fibroblasts of
Patients With Different Joint Diseases and Normals*
Patient ID diagnosisa
Karyotype/FISH
Peripheral bloodlymphocytes
Nuclei extracted fromsynovial tissue (Synovial) macrophages
Synovial fibroblasts,first passage
EB32/ReA 46,XY n.a. FISH: �7[11%] 46,X,�10?[4]46,XY FISH:normal (only
probes forchromosomes 4and 7)
FISH:normal(synovial cells;collagenase digest)
EB72/JT (cryostat sections) n.a. FISH:normal n.a. n.a.J1/JT (1 month culture) n.a. n.a. FISH:normal 46,XX
FISH:normalJ2/JT (3 weeks culture) n.a. FISH:normal FISH:�4[7%];�7[7%];
�9[5%];�10[5%];incl. polyploid [5%]
46,XX46, XX FISH:�4[2%];�7[2%];
�9[5%];�10[5%];incl. polyploid [2%]
FISH:normal(synovial cells;collagenase digest)
J6/JT (2 weeks culture) n.a. n.a. FISH:�6[2%];�7[6%];�12[n.a.]
46,XYFISH:�6[5%];�7[5%];�12[12%]
J11/JT (cryostat sections) n.a. FISH:normal n.a. n.a.J12/JT (Cryostat sections/2
weeks culture)n.a. FISH:normal n.a. n.a.
FISH:normalSynS7/Nor. (paraffin
sections)n.a. FISH:normal n.a. n.a.
B1/Nor. (cryostat sections) n.a. FISH:normal n.a. n.a.NST1/Nor (cryostat
sections)n.a. FISH:normal n.a. n.a.
BAL1/COPD n.a. n.a. FISH:4[3%];�7[9%] n.a.BAL2/COPD n.a. n.a. FISH:�4[3%] n.a.BAL3/COPD n.a. n.a. FISH:normal; �4[1%] n.a.BAL4/COPD n.a. n.a. FISH:normal n.a.BAL5/COPD n.a. n.a. FISH:normal n.a.BAL5a/COPD n.a. n.a. FISH:normal n.a.BAL5b/COPD n.a. n.a. FISH:normal;
�7[1%];�18[2%]n.a.
BAL6/COPD n.a. n.a. FISH:normal;6[5%];�7[1%]
n.a.
*Values above normal cutoff levels are indicated in bold. Paired values for in vitro data (P-1 SFB or P-1 M�) are reported in italics even if they did notreach the cutoff level; numerical aberrations in bronchial macrophages � the maximal levels for individual chromosomes in normal peripheral bloodmonocytes are reported in italics for general interest.N.B. Except for the results of (synovial) macrophages (column 5) all other results were published previously (R.W. Kinne et al., 2001) and are includedonly to allow the comparison between systemic (blood) and local (synovial tissue) aberrations and/or between tissue and isolated cells.aReA, reactive arthritis; JT, joint trauma; Nor., normal; BAL, broncho-alveolar lavage fluid; COPD, chronic obstructive pulmonary disease.
64 KINNE ET AL.

tissue M�, irrespective of their anatomical site (Ta-ble 6). In addition, 5/8 patients (63%; Table 6)showed gains or losses of chromosomes 4, 6, 7, and18 equal to or exceeding the maximal levels forthese chromosomes in normal peripheral bloodmonocytes (Table 2). However, the frequency ofnumerical aberrations was lower in COPD than inthe RA and OA joint (e.g., for chromosome 7, P �0.006 and P � 0.005, respectively; Fig. 4).
DISCUSSION
Trisomy/polysomy 7 was the most significantnumerical chromosomal alteration in RA patients.This alteration was limited to the chronically in-flamed synovial compartment, given that pairedskin FB (Kinne et al., 2001) and blood lymphocytes(as well as joint trauma/control samples) were vir-tually normal. Alterations were not specific for RA,given that OA and reactive arthritis showed thesame type of alterations (in OA even partially ex-ceeding the extent observed in RA). Thus, suchalterations (in analogy to somatic mutations) maynot be functional to a particularly aggressive phe-notype of RA-SFB, but rather reflect a commonresponse to the inflammatory microenvironment inrheumatic diseases (Tak et al., 2000; Dahlen et al.,2001). Also, at the present state of knowledge, notonly does a disease-promoting effect of these alter-ations have to be considered, but also the possibil-ity of compensatory/repair processes.
In paired samples from either RA or OA patients,numerical chromosomal aberrations were presentnot only in SFB but also in synovial M� (althoughto a lesser extent). Gains or losses affected chro-
mosomes 6, 7, 8, 9, and 12 in RA, and 4, 6, 7, 8, 9,11, 12, X, and Y in OA (i.e., a pattern similar to thatpreviously observed in SFB) (Kinne et al., 2001). InRA and OA M�, chromosome 7 was predominantlyaffected. These findings show, on one hand, thatboth synovial M� and SFB contribute to the tri-somy/polysomy 7 observed in the synovial mem-brane as a whole. On the other hand, they empha-size that the major infiltrating inflammatory celltype (i.e., the synovial M�) carries chromosomalaberrations in chronic inflammatory joint diseases.Such alterations may represent a common responseto chronic inflammation in different organs becausegains of chromosomes 4 and 7 (and low-grade gains/losses of chromosomes 6 and 18) were also docu-mented in isolated bronchial M� from patientswith COPD. Notably, and in contrast to RA-SFB,the percentage of RA synovial M� monosomic forchromosome 7 was higher than that of trisomic/polysomic M�, suggesting that losses of chromo-some 7 may not severely impair the survival of RAsynovial M�.
In both RA and OA, there was a significantpositive correlation between the degree of alter-ations for chromosome 7 in synovial M� and SFB.This supports the hypothesis that not clonal-likechanges inherent to the SFB population (which arerather polyclonal in nature; Broberg et al., 1998;Kinne et al., 2001), but rather the local inflamma-tory microenvironment favors or dictates such al-terations. The similarity between the changes insynovial and pulmonary M� further stresses thishypothesis. However, systemic alterations of circu-lating monocytes in RA (Stuhlmuller et al., 2000),as well as the almost complete lack of M� prolif-eration in the RA and OA synovial membrane(Schaser et al., 1996), raise the question whetherprecursor cells of the myelo-monocytic lineage (oreven common precursor cells of SFB and M�;Gunsilius et al., 2000) may already be affected bychromosomal aberrations.
Parallel aberrations of different chromosomeswere not restricted to SFB (Bonnici et al., 1992;Ermis et al., 1993; Mertens et al., 1993, 1996; Kinneet al., 2001; this study), but also occurred in syno-vial M�. Whereas a general chromosomal instabil-ity remains a possibility, the preferential alterationof chromosome 7 in synovial M� and SFB of bothRA and OA patients argues for selective affectionor advantage of this chromosome.
A link between chronic disease and the magni-tude of numerical chromosomal aberrations wassuggested by a significant positive correlation be-tween the disease duration in RA patients and the
Figure 4. Comparison of numerical chromosomal aberrations innormal peripheral blood monocytes, synovial M� from RA, OA, andjoint trauma (JT), as well as bronchial M� from chronic obstructivepulmonary disease (COPD). Trisomies of chromosome 7 in mono-cytes/M� are depicted as means � SE of n � 3–14 donors. # P � 0.05vs. normal peripheral blood monocytes; * P � 0.05 versus RA synovialM�; § P � 0.05 vs. OA synovial M�.
65CHROMOSOMAL ABERRATIONS IN SYNOVIAL FIBROBLASTS/MACROPHAGES

levels of polysomies for chromosomes 6 (n � 5; P �0.014; rho 0.947) and 8 (n � 4; P � 0.050; rho 0.949)in P-1 SFB. However, acute disease may also favorthe development of polysomies, as suggested by asignificant positive correlation between levels ofpolysomy for chromosome 7 in RA collagenase di-gests and the serum levels of CRP (n � 5; P �0.041; rho 0.894). In the case of synovial M�, aninfluence of the disease status on the occurrence/magnitude of numerical chromosomal aberrationswas noted only in OA patients. In P-1 M� of OApatients, in fact, there was a significant correlationbetween the disease duration and the levels ofpolysomy for chromosome 7 (n � 4; P � 0.05; rho0.949), as well as between the levels of polysomy 4and the serum levels of CRP (n � 7; P � 0.026; rho0.813).
Trisomy 7 appears to accumulate with age inboth solid tumors and non-neoplastic synovialmembrane from normal donors (Broberg et al.,2001), a point of particular importance in thepresent study because both RA and OA patientshad a significantly higher age than normal/jointtrauma and BAL patients (see Table 6). In agree-ment with this contention, the age of the OA pa-tients showed a significant positive correlation withthe levels of polysomy 9 in nuclei extracted fromsynovial tissue (n � 5; P � 0.041; rho 0.894) and inthe collagenase digest (n � 7; P � 0.023; rho 0.823).In contrast, the age of the RA patients negativelycorrelated with the level of polysomy 6 in P-1 SFB(n � 6; P � 0.046; rho 0.820), indicating that atleast in RA inflammatory stimuli may also stronglyinfluence the occurrence and frequency of chromo-somal aberrations, in analogy to brain and thyroidtumors (Broberg et al., 2001).
Concurrent treatment is also suspected to play arole in the occurrence of chromosomal alterations(Hazleman, 1982; Keshava et al., 1997). In thepresent study, however, there was a significant neg-ative correlation between the levels of polysomyfor chromosome 7 in RA synovial M� and concur-rent treatment with MTX (n � 10; P � 0.004; rho0.821), rather suggesting that efficacious anti-in-flammatory treatment with MTX may help to pre-vent chromosomal aberrations. This result parallelsprevious similar observations in RA-SFB (Kinne etal., 2001).
Chromosome 7 carries a number of potentiallyrelevant genes, implying functional consequencesfor �7 SFB and M� (e.g., cytokines/growth factorsand their receptors; transcription factors; signaltransduction molecules; and molecules involved inmatrix formation and cell-extracellular matrix; De-
loukas et al., 1998). Indeed, both RA and OA SFBwith �7 appear to have a selective growth advan-tage (Ermis et al., 1993, 1995; Mertens et al., 1996;Kinne et al., 2001). Also, dysplastic �7 cells inBarrett’s esophagus overexpress epidermal growthfactor (Garewal et al., 1990), and passaged OA sy-novial cells with high frequencies of trisomy 7produce four times more versican than their di-somic counterparts (Eklund et al., 2002). Furtherstudies will be necessary to fully elucidate thealterations of gene expression and cell functionscaused by trisomy 7 in OA and RA-SFB.
In summary, comparable chromosomal aberra-tions were observed in synovial tissue and early-passage SFB or M� of patients with RA and otherrheumatic diseases, as well as M� in chronic pul-monary disease. Thus, chronic inflammatory stressmay induce simultaneous cytogenetic alterations inmesenchymal and inflammatory cells independentof the organ involved. Because of its partial simi-larity to the alterations in malignancy, this intrigu-ing and nontypical feature of non-neoplastic, ac-quired chromosome aberration may reflect anintermediate status between self-limiting inflam-mation and transformation.
ACKNOWLEDGMENTS
Prof. Dr. J. Dippold and Prof. Dr. G. von Salis-Soglio, Department of Orthopedics, University ofLeipzig; Prof. R. Venbrocks, Clinic of Orthopedics,Friedrich Schiller University Jena, Germany, aregratefully acknowledged for providing patient ma-terial; and Dr. Robert Pfeiffer and Dr. Hans-DetlevStahl, Institute of Clinical Immunology and Trans-fusion Medicine, University of Leipzig, for patientcharacterization. Prof. U. G. Froster and H. Hol-land, Institute of Human Genetics, University ofLeipzig, Germany, are acknowledged for perform-ing cytogenetic analyses in selected samples.
Dr. H.-J. Thude and Prof. D. Barz, Institute ofTransfusion Medicine, Friedrich Schiller Univer-sity Jena, as well as Dr. Dornheim, Red CrossBlood Bank Suhl, are acknowledged for providingbuffy coats; and Barbel Ukena and Juliane Prech-tel, Experimental Rheumatology Unit, FriedrichSchiller University Jena for expert technical assis-tance.
Dr. Ernesta Palombo-Kinne is gratefully ac-knowledged for critical revision of the manuscript.
This research was funded in part by grants fromthe German Federal Ministry of Education andResearch (BMBF), 01KS9504 to T.Z.; Interdisci-plinary Center for Clinical Research (IZKF),Leipzig; 01VM9311/3 and 01ZZ9602 to R.W.K.,
66 KINNE ET AL.

G.H., R.K.B., C.K., and U.C.; IZKF, Jena; grant forjunior researchers to E.K.; and the ThuringianMinistry of Science, Research, and Art (B311-00026 to R.W.K.).
REFERENCES
Aicher WK, Heer AH, Trabandt A, Bridges SL Jr, Schroeder HW Jr,Gay RE, Eibel H, Peter HH, Siebenlist U, Koopman WJ, Gay S.1994. Overexpression of zinc-finger transcription factor Z-225/Egr-1 in synoviocytes from rheumatoid arthritis patients. J Immu-nol 152:5940–5948.
Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K,Christy W, Cooke TD, Greenwald R, Hochberg M, Howell D,Kaplan D, Koopman W, Longley S 3rd, Mankin H, McShane DJ,Medsger T Jr, Meenan R, Mikkelsen W, Moskowitz R, MurphyW, Rothschild B, Segal M, Sokoloff L, Wolfe F. 1986. Develop-ment of criteria for the classification and reporting of osteoarthri-tis. Classification of osteoarthritis of the knee. Diagnostic andTherapeutic Criteria Committee of the American RheumatismAssociation. Arthritis Rheum 29:1039–1049.
Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, CooperNS, Healey LA, Kaplan SR, Liang MH, Luthra HS, Medsger TAJr, Mitchell DM, Neustadt DH, Pinals RS, Schaller JG, Sharp JT,Wilder RL, Hunder GG. 1988. The American Rheumatism As-sociation 1987 revised criteria for the classification of rheumatoidarthritis. Arthritis Rheum 31:315–324.
Bonnici AV, Birjandi F, Spencer JD, Fox SP, Berry AC. 1992.Chromosomal abnormalities in Dupuytren’s contracture and car-pal tunnel syndrome. J Hand Surg (Br) 17:349–355.
Broberg K, Hoglund M, Lindstrand A, Toksvig-Larsen S, MandahlN, Mertens F. 1998. Polyclonal expansion of cells with trisomy 7in synovia from patients with osteoarthritis. Cytogenet Cell Genet83:30–34.
Broberg K, Toksvig-Larsen S, Lindstrand A, Mertens F. 2001.Trisomy 7 accumulates with age in solid tumors and non-neoplas-tic synovia. Genes Chromosomes Cancer 30:310–315.
Dahlen A, Broberg K, Domanski HA, Toksvig-Larsen S, LindstrandA, Mandahl N, Mertens F. 2001. Analysis of the distribution andfrequency of trosomy 7 in vivo in synovia from patients withosteoarthritis and pigmented villonodular synovitis. Cancer GenetCytogenet 131:19–24.
Deloukas P, Schuler GD, Gyapay G, Beasley EM, Soderlund C,Rodriguez-Tome P, Hui L, Matise TC, McKusick KB, BeckmannJS, Bentolila S, Bihoreau M, Birren BB, Browne J, Butler A, CastleAB, Chiannilkulchai N, Clee C, Day PJR, Dehejia A, Dibling T,Drouot N, Duprat S, Fizames C, Fox S. 1998. A physical map of30,000 human genes. Science 282:744–746.
Eklund E, Broberg K, Westergren-Thorsson G, Bjardahlen A, Hed-lund M, Malmstrom A. 2002. Proteoglycan production in disomicand trisomy 7-carrying human synovial cells. Matrix Biol 21:325–335.
Ermis A, Hopf T, Hanselmann R, Remberger K, Welter C, DooleyS, Zang KD, Henn W. 1993. Clonal chromosome aberrations incell cultures of synovial tissue from patients with rheumatoidarthritis. Genes Chromosomes Cancer 6:232–234.
Ermis A, Henn W, Remberger K, Hopf C, Hopf T, Zang KD. 1995.Proliferation enhancement by spontaneous multiplication of chro-mosome 7 in rheumatic synovial cells in vitro. Hum Genet 96:651–654.
Fassbender HG. 1983. Histomorphological basis of articular cartilagedestruction in rheumatoid arthritis. Coll Relat Res 3:141–155.
Firestein GS. 1998. Novel therapeutic strategies involving animals,arthritis, and apoptosis. Curr Opin Rheumatol 10:236–241.
Fox DA, Millard JA, Kan L, Zeldes WS, Davis W, Higgs J, EmmrichF, Kinne RW. 1990. Activation pathways of synovial T lympho-cytes. Expression and function of the UM4D4/CDw60 antigen.J Clin Invest 86:1124–1136.
Garewal H, Meltzer P, Trent J, Prabhala R, Sampliner R, Korc M.1990. Epidermal growth factor overexpression and trisomy 7 in acase of Barrett’s esophagus. Dig Dis Sci 35:1115–1120.
Gebhart E, Trautmann U, Reichardt S, Liehr T. 1993. Chromo-somal heterogeneity of aneuploid leukemic cell populations de-tected by conventional caryotyping and by fluorescence in situhybridization (FISH). Anticancer Res 13:1857–1862.
Gunsilius E, Duba HC, Petzer AL, Kahler CM, Grunewald K,Stockhammer G, Gabl C, Dirnhofer S, Clausen J, Gastl G. 2000.
Evidence from a leukaemia model for maintenance of vascularendothelium by bone-marrow-derived endothelial cells. Lancet355:1688–1691.
Hazleman BL. 1982. The comparative incidence of malignant dis-ease in rheumatoid arthritics exposed to different treatment reg-imens. Ann Rheum Dis 41(Suppl. 1):12–17.
Heim S, Mandahl N, Jin Y, Stromblad S, Lindstrom E, Salford LG,Mitelman F. 1989. Trisomy 7 and sex chromosome loss in humanbrain tissue. Cytogenet Cell Genet 52:136–138.
Hirth A, Skapenko A, Kinne RW, Emmrich F, Schulze-Koops H,Sack U. 2002. Cytokine mRNA and protein expression in pri-mary-culture and repeated-passage rheumatoid arthritis synovialfibroblasts. Arthritis Res 4:117–125.
Johansson B, Heim S, Mandahl N, Mertens F, Mitelman F. 1993.Trisomy 7 in nonneoplastic cells. Genes Chromosomes Cancer6:199–205.
Keshava C, Keshava N, Whong WZ, Nath J, Ong TM. 1997. Inhi-bition of methotrexate-induced chromosomal damage by vanillinand chlorophyllin in V79 cells. Teratog Carcinog Mutagen 17:313–326.
Kinne RW, Palombo-Kinne E, Emmrich F. 1995. Activation ofsynovial fibroblasts in rheumatoid arthritis. Ann Rheum Dis 54:501–504.
Kinne RW, Brauer R, Stuhlmuller B, Palambo-Kinne E, BurmesterGR. 2000. Macrophages in rheumatoid arthritis. Arthritis Res2:189–202.
Kinne RW, Liehr T, Beensen V, Kunisch E, Zimmermann T,Holland H, Pfeiffer R, Stahl H-D, Lungershausen W, Hein G,Roth A, Emmrich F, Claussen U, Froster UG. 2001. Mosaicchromosomal aberrations in synovial fibroblasts from patients withrheumatoid arthritis, osteoarthritis, and other inflammatory jointdiseases. Arthritis Res 3:319–330.
Liehr T, Grehl H, Rautenstrauss B. 1995. FISH analysis of inter-phase nuclei extracted from paraffin-embedded tissue. TrendsGenet 11:377–378.
Liehr T, Grehl H, Rautenstrauss B. 1996. A rapid method for FISHanalysis on interphase nuclei extracted from cryofixed tissue.Trends Genet 12:505–506.
Mertens F, Orndal C, Mandahl N, Heim S, Bauer HF, Rydholm A,Tufvesson A, Willen H, Mitelman F. 1993. Chromosome aberra-tions in tenosynovial giant cell tumors and nontumorous synovialtissue. Genes Chromosomes Cancer 6:212–217.
Mertens F, Palsson E, Lindstrand A, Toksvig-Larsen S, Knuutila S,Larramendy ML, El-Rifai W, Limon J, Mitelman F, Mandahl N.1996. Evidence of somatic mutations in osteoarthritis. HumGenet 98:651–656.
Mitelman F. 1995. An international system for human cytogeneticnomenclature. Basel: S. Karger.
Nishioka K, Hasunuma T, Kato T, Sumida T, Kobata T. 1998.Apoptosis in rheumatoid arthritis: a novel pathway in the regula-tion of synovial tissue. Arthritis Rheum 41:1–9.
Pelegri C, Kuhnlein P, Buchner E, Schmidt CB, Franch A, CastellM, Hunig T, Emmrich F, Kinne RW. 1996. Depletion of gamma/delta T cells does not prevent or ameliorate, but rather aggravates,rat adjuvant arthritis. Arthritis Rheum 39:204–215.
Schaser K, Kinne RW, Beil H, Kladny B, Sto� B. 1996. Proliferationvon T-Zellen, Makrophagen, neutrophilen Granulozyten und Fi-broblasten-ahnlichen Zellen in der Synovialmembran von Pati-enten mit rheumatoider Arthritis. Verh Dtsch Ges Pathol 80:276–280.
Seabright M. 1971. A rapid banding technique for human chromo-somes. Lancet 2:971–972.
Stuhlmuller B, Ungethum U, Scholze S, Martinez L, Backhaus M,Kraetsch H-G, Kinne RW, Burmester GR. 2000. Identification ofknown and novel genes in activated monocytes from patients withrheumatoid arthritis. Arthritis Rheum 43:775–790.
Tak PP, Zvaifler NJ, Green DR, Firestein GS. 2000. Rheumatoidarthritis and p53: how oxidative stress might alter the course ofinflammatory diseases. Immunol Today 21:78–82.
Weiss KR, Georgescu HI, Gollin SM, Kang R, Evans CH. 1999.Trisomy 7 in synovial fibroblasts obtained from arthritic joints.Inflamm Res 48(Suppl. 2):S132–S133.
Zimmermann T, Kunisch E, Pfeiffer R, Hirth A, Stahl H-D, Sack U,Laube A, Liesaus E, Roth A, Palombo-Kinne E, Emmrich F,Kinne RW. 2001. Isolation and characterization of rheumatoidarthritis synovial fibroblasts from primary culture—primary-cul-ture cells markedly differ from fourth-passage cells. Arthritis Res3:72–76.
67CHROMOSOMAL ABERRATIONS IN SYNOVIAL FIBROBLASTS/MACROPHAGES