Embed Size (px)
Citation preview
Case Report
1st Departmical School, Hi
CorrespondIraklion, Athe
Ann Vasc Surghttp://dx.doi.or� 2014 Elsevi
Manuscript r
December 29,
Synovial Cyst of the AntecubitalFossa Mimicking a Brachial ArteryPseudoaneurysm: Report of a Case
Konstantinos Filis, George Galyfos, Andreas Larentzakis, Evridiki Karanikola,
and Constantinos Zarmakoupis, Athens, Greece
Pseudoaneurysms of the brachial artery are common following a percutaneous cardiac catheter-ization. Synovial cysts are a commonly identified entity in patients with rheumatic diseases aswell. We present a rare case of a synovial cyst in the elbow masquerading as an iatrogenic pseu-doaneurysm of the brachial artery. A 51-year-old female patient presented with a pulsatile andpainful mass in the right antecubital fossa. The medical history revealed a recent diagnostic car-diac catheterization at the same site and rheumatoid arthritis under oral treatment. Imaginginvestigations were not fully diagnostic. Because of the clinical suspicion of a thrombosed pseu-doaneurysm, exploratory surgery was indicated. The pathologic examination of the specimenconfirmed the diagnosis of a synovial cyst. Ultrasonography and computed tomography imagingare valuable in the everyday clinical practice but they do not always exclude an iatrogenic pseu-doaneurysm, especially when the medical history is suspicious. Surgical removal is the propertreatment and pathologic examination sets the final diagnosis in such cases of diagnosticdifficulty.
Synovial cysts of the upper extremities and particu-
larly of the antecubital fossa are not uncommon in
patients with a history of rheumatoid arthritis.1,2
However, a pulsatile mass in the same anatomic
area with a former brachial artery catheterization
is commonly the result of an arterial pseudoaneur-
ysm formation.3e5 We present an unusual case of
a patient with a synovial cyst of the right elbow
masquerading as an iatrogenic pseudoaneurysm
and we discuss proper diagnostic and therapeutic
management.
ent of Propaedeutic Surgery, University of Athens Med-ppokration Hospital, Athens, Greece.
ence to: George Galyfos, 6 Melinas Merkouri Street, Neonns 14122, Greece; E-mail: [email protected]
2014; -: 1–4g/10.1016/j.avsg.2013.12.033er Inc. All rights reserved.
eceived: December 17, 2013; manuscript accepted:
2013; published online: ---.
CASE REPORT
A 51-year-old female patient was referred to our depart-
ment for evaluation because of a growing and painful
mass in her right antecubital fossa. The patient com-
plained of a rapidly enlarging mass in her right elbow
during the last month, with accompanying discomfort
during the last 2 weeks. Her medical history revealed
rheumatoid arthritis under treatment with oral cortico-
steroids for the last 3 years. Additionally, she mentioned
a painful and ineffective arterial puncture during a diag-
nostic cardiac catheterization through the ipsilateral
brachial artery 2 months before. The rest of the medical
or surgical history was unremarkable. There was no his-
tory of trauma as well.
During the physical examination, a soft and pulsatile
mass, almost 3 cm in diameter, was palpated on the ante-
romedial aspect of the right upper extremity, at the level of
the antecubital fossa. No obvious hematoma or ecchy-
mosis was noted. There were no signs of ischemia or clau-
dication of the ipsilateral forearm or hand nor any
neurologic deficits. The ultrasonographic assessment of
the region revealed a cystic lesion of unknown origin in
the near of the brachial artery and no flow disturbance
1
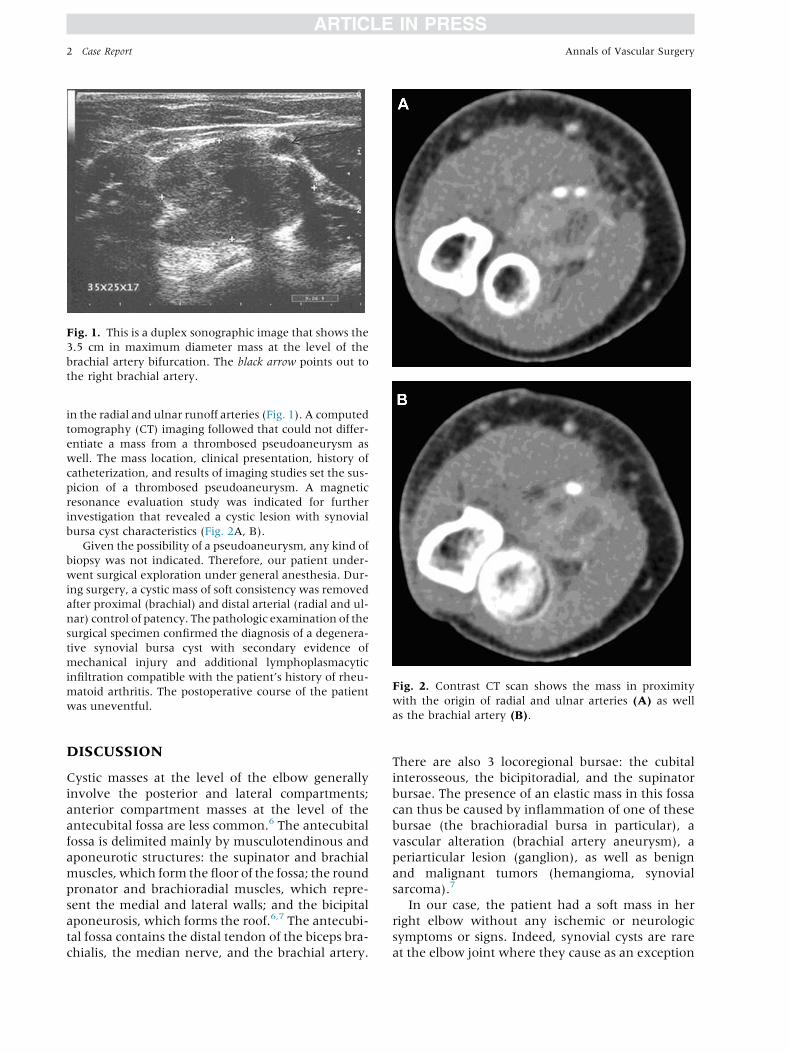
Fig. 1. This is a duplex sonographic image that shows the
3.5 cm in maximum diameter mass at the level of the
brachial artery bifurcation. The black arrow points out to
the right brachial artery.
Fig. 2. Contrast CT scan shows the mass in proximity
with the origin of radial and ulnar arteries (A) as well
2 Case Report Annals of Vascular Surgery
in the radial and ulnar runoff arteries (Fig. 1). A computed
tomography (CT) imaging followed that could not differ-
entiate a mass from a thrombosed pseudoaneurysm as
well. The mass location, clinical presentation, history of
catheterization, and results of imaging studies set the sus-
picion of a thrombosed pseudoaneurysm. A magnetic
resonance evaluation study was indicated for further
investigation that revealed a cystic lesion with synovial
bursa cyst characteristics (Fig. 2A, B).
Given the possibility of a pseudoaneurysm, any kind of
biopsy was not indicated. Therefore, our patient under-
went surgical exploration under general anesthesia. Dur-
ing surgery, a cystic mass of soft consistency was removed
after proximal (brachial) and distal arterial (radial and ul-
nar) control of patency. The pathologic examination of the
surgical specimen confirmed the diagnosis of a degenera-
tive synovial bursa cyst with secondary evidence of
mechanical injury and additional lymphoplasmacytic
infiltration compatible with the patient’s history of rheu-
matoid arthritis. The postoperative course of the patient
was uneventful.
as the brachial artery (B).DISCUSSION
Cystic masses at the level of the elbow generally
involve the posterior and lateral compartments;
anterior compartment masses at the level of the
antecubital fossa are less common.6 The antecubital
fossa is delimited mainly by musculotendinous and
aponeurotic structures: the supinator and brachial
muscles, which form the floor of the fossa; the round
pronator and brachioradial muscles, which repre-
sent the medial and lateral walls; and the bicipital
aponeurosis, which forms the roof.6,7 The antecubi-
tal fossa contains the distal tendon of the biceps bra-
chialis, the median nerve, and the brachial artery.
There are also 3 locoregional bursae: the cubital
interosseous, the bicipitoradial, and the supinator
bursae. The presence of an elastic mass in this fossa
can thus be caused by inflammation of one of these
bursae (the brachioradial bursa in particular), a
vascular alteration (brachial artery aneurysm), a
periarticular lesion (ganglion), as well as benign
and malignant tumors (hemangioma, synovial
sarcoma).7
In our case, the patient had a soft mass in her
right elbow without any ischemic or neurologic
symptoms or signs. Indeed, synovial cysts are rare
at the elbow joint where they cause as an exception

Vol. -, No. -, - 2014 Case Report 3
a compression of the ulnar nerve or the brachial
artery.8 A history of osteoarthritis or inflammatory
joint diseases increases the possibility of the diag-
nosis of a synovial cyst, as it was in our case.9 On
the other hand, the palpitation of a pulsatile mass
in the antecubital fossa, given a history of brachial
artery puncture, raises the suspicion of an iatrogenic
pseudoaneurysm, as it was also the case with our
patient. Brachial artery puncture and catheteriza-
tion are thought to be a viable, safe, and efficient
alternative to the transfemoral approach in a center
that is experienced with the arm approach, when
radial or femoral access is not possible.3,10 However,
the formation of an iatrogenic hematoma or a pseu-
doaneurysm is common in the literature.11e14
Regarding the imaging work-up of masses in this
region, ultrasound is considered the first-level study
of choice for ‘‘cystic’’ lesions of the elbow because it
is easy to perform, rapid, relatively low in cost, and
widely available.15 The combination of sonographic
and color Doppler imaging techniques can be used
to distinguish solid and fluid-filled masses, but it
also represents a simple and safe method for identi-
fying vascular lesions.16 Thanks to its high spatial
resolution; ultrasound is also useful for identifying
the lesion’s relations with the joint capsule. Ultra-
sound has been shown to be better than physical ex-
amination and even better than arteriography.16
This is because many aneurysms cannot be detected
through arteriography, as they are occupied by
thrombus. An ultrasound lets not only the aneu-
rysm walls but also the internal clots be seen. It
has also been shown that aneurysm size and ultra-
sound extension correlate well with surgical find-
ings. However, sonographic assessment in our case
revealed the patency of the blood vessels, but could
not clearly differentiate a pseudoaneurysm from
another type of cystic mass.
A history of iatrogenic arterial trauma raises the
possibility of an arterial pseudoaneurysm.17 The arte-
rial flow inside an aneurysmal sac can be detected by
vascular ultrasound, CTwith intravenous contrast, or
digital angiography. However, there are reports of a
solidmass in the thighmimicking a femoral pseudoa-
neurysm.18,19 CT may not always be able to differen-
tiate a thrombosed pseudoaneurysm from a solid or
cystic mass of other origin, as it was in our case. In
addition, thrombosed pseudoaneurysms do not
show either arterial flow or a communication be-
tween the aneurysm and the feeding artery.16 Thus,
in these cases, magnetic resonance imaging (MRI)
could add further information regarding themorpho-
logic features of a mass, because the majority of the
aforementioned lesions have characteristic MRI ap-
pearances that allow a confident diagnosis, obviating
the need for additional imaging or interventional
procedures.20,21 However, our patient underwent a
surgical procedure for final diagnosis despite the
valuable information acquired by the MRI study.
Most of the times, patients have to be operated
in an exploratory manner under extremely
different surgical treatment plans that include
arterial reconstruction or a mass exclusion. Surgi-
cal access to the antecubital fossa may be required
in the presence of tumors or nerve compression.22
The latter is caused usually by fractures, ganglia,
or neoplasms. However, our patient did not pre-
sent with any neurologic symptoms. Surgery can
be associated with early and late complications.
The former is frequently vascular in nature and
include hematomas caused by injury to the basilic,
cephalic, or median cubital vein.23 Late complica-
tions are generally functional and may include
limitation of flexion/extension of the elbow
caused by the formation of adhesions.24 Delayed
vascular complications are less common, but
they are reported from time to time. These phe-
nomena are frequently caused by trauma; as post-
operative complications, they are relatively rare.
They generally consist of pseudoaneurysms of
the brachial artery.17 Fortunately, there were no
complications in our patient after surgical removal
of the synovial cyst.
In conclusion, definite diagnosis in similar situa-
tions may not always be possible preoperatively.
The case illustrates the value of ultrasound and CT
in the diagnosis of fluid-filled lesions of the elbow,
including those that are rare and unexpected,
although these investigations do not always set the
definite diagnosis. Thus, surgeons and clinicians
must be very suspicious and cautious concerning
their treatment plans. A fast decision toward a
biopsy may be lethal in case of an aneurysm,
whereas a prolonged delay in a case of a tender
aneurysm can be dangerous because of the risk of
rupture. Thus, surgical removal is the proper treat-
ment and pathologic examination sets the final
diagnosis in such cases of diagnostic difficulty.
REFERENCES
1. Beaman FD, Peterson JJ. MR imaging of cysts, ganglia, and
bursae about the knee. Radiol Clin North Am 2007;45:
969e82.
2. Mainard D, Saury P, Delagoutte JP. Ulnar nerve compres-
sion at the elbow caused by synovial cyst of rheumatoid
origin. Rev Rhum Mal Osteoartic 1991;58:611e4.
3. Gan HW, Yip HK, Wu CJ. Brachial approach for coronary
angiography and intervention: totally obsolete, or a feasible
alternative when radial access is not possible? Ann Acad
Med Singapore 2010;39:368e73.
4 Case Report Annals of Vascular Surgery
4. Watkinson AF, Hartnell GG. Complications of direct brachial
artery puncture for arteriography: a comparison of tech-
niques. Clin Radiol 1991;44:189e91.
5. Heintzen MP, Strauer BE. Peripheral arterial complications
after heart catheterization. Herz 1998;23:4e20.6. Ellis H, Feldman S, Harrup-Griffiths W. The clinical anat-
omy of the antecubital fossa. Br J Hosp Med (Lond)
2010;71:M4e5.
7. Bortolotto C, Carone L, Draghi F. An antecubital fossa ‘‘cyst’’
caused by postoperative kinking of the brachial artery.
J Ultrasound 2013;16:29e31.
8. Monacelli G, Spagnoli AM, Pardi M, et al. Double compres-
sion of the ulnar nerve at the elbow and at the wrist (dou-
ble-crush syndrome). Case report and review of the
literature. G Chir 2006;27:101e4.
9. Hayashi A, Matsumura T, Komoto M, et al. Multiple rheu-
matoid bursal cysts that were finally effectively treated by
combining surgical resection and sclerotherapy. J Plast
Reconstr Aesthet Surg 2012;65:e29e32.
10. Basche S, Eger C, Aschenbach R. Transbrachial angiog-
raphy: an effective and safe approach. Vasa 2004;33:
231e4.
11. Hildick-Smith DJ, Khan ZI, Shapiro LM, et al. Occasional-
operator percutaneous brachial coronary angiography:
first, do no arm. Catheter Cardiovasc Interv 2002;57:
161e5.
12. Muller DW, Shamir KJ, Ellis SG, et al. Peripheral vascular
complications after conventional and complex percuta-
neous coronary interventional procedures. Am J Cardiol
1992;69:63e8.
13. Baudouin CJ, Belli AM, Peck RJ, et al. The complications of
high brachial artery puncture. Clin Radiol 1990;42:277e80.
14. Fransson SG, Nylander E. Vascular injury following cardiac
catheterization, coronary angiography, and coronary angio-
plasty. Eur Heart J 1994;15:232e5.
15. Draghi F, Danesino GM, de Gautard R, et al. Ultrasound of
the elbow: examination techniques US appearance of the
normal and pathologic joint. J Ultrasound 2007;10:76e84.
16. Weiner SN, Hoffman J, Bernstein RG, et al. The value of ul-
trasound in the diagnosis of popliteal artery aneurysms.
Angiology 1983;34:418e27.
17. Moran D, Roche-Nagle G, Ryan R, et al. Pseudoaneurysm of
the brachial artery following humeral fracture. Vasc Endo-
vascular Surg 2008;42:65.
18. Lu KH. An unusual case of meniscal hematoma mimicking a
medial meniscal cyst. Arthroscopy 2002;18:E22.
19. Filis K, Toutouzas K, Lagoudianakis E, et al. Schwannoma of
thigh mimicking pseudoaneurysm of the profunda femoral
artery. Ann Vasc Surg 2008;22:449e52.
20. Perdikakis E, Skiadas V. MRI characteristics of cysts and
‘‘cyst-like’’ lesions in and around the knee: what the radiol-
ogist needs to know. Insights Imaging 2013;4:257e72.21. Papp DF, Khanna AJ, McCarthy EF, et al. Magnetic reso-
nance imaging of soft-tissue tumors: determinate and inde-
terminate lesions. J Bone Joint Surg 2007;89:103e15.
22. McFarlane J, Trehan R, Olivera M, et al. A ganglion cyst at
the elbow causing superficial radial nerve compression:
a case report. J Med Case Rep 2008;25:122.
23. Verhaar J, van Mameren H, Brandsma A. Risks of neurovas-
cular injury in elbow arthroscopy: starting anteromedially or
anterolaterally? Arthroscopy 1991;7:287e90.
24. Zancolli ER 3rd, Zancolli EP 4th, Perrotto CJ. New mini-
invasive decompression for pronator teres syndrome.
J Hand Surg Am 2012;37:1706e10.