Embed Size (px)
Citation preview
Thorax (1966), 21, 67.
Symptomatic hiatus hernia:A study of the pyloro-duodenal region and the rationale of vagotomy
in its treatment
HAROLD W. BURGE, ALAN MORTON GILL,CHARLES D. T. MAcLEAN, AND RONALD H. LEWIS
From the West London Hospital, London, W.6
The association of duodenal ulceration andsymptomatic hiatus hernia, with or without pepticoesophagitis, is well recognized. Casten, Bernhang,Nach, and Spinzia (1963) found it in 50% of theircases.
Pyloric channel disease is, in our experience,more frequently associated with symptomatichiatus hernia than is duodenal ulceration.Unfortunately, this benign disease at the pylorushas in the past been frequently ovrlo'oked, bothon radiographic examination and at operation.
In 1935 Winkelstein described peptic oeso-phagitis for the first time in medical history. Ofhis five patients, three had associated duodenalulceration and one.had a gastric ulcer.'If, as webelieve (Burge, Gill,. and Lewis, 1963),'less*e curvegastric ulcer is caused by antral retention second.,ary to pyloric channel or duodenal disease, thenfour of his five patients had pathology at thegastric outlet.Twenty years later Winkelstein, Wolf, Som, and
Marshak (1954) described 20 patients with pepticoesophagitis; 16 had associated duodenal ulcera-tion and three had gastric ulceration; 19 of their20 patients had, on the same reasoning, duodenalor pyloric disease. Since pyloric channel diseasewas not generally recognized in the past-orindeed even to-day-it is possible that all these 25patients did in fact have disease either in theduodenum or at the pylorus.Palmer (1952) suggested that peptic oesophagitis
was prone to occur in patients with pyloricstenosis. Both pyloric channel disease and duo-denal ulceration may give rise to recurrenttransient gastric retention. Especially is this so inpyloric channel disease, for an acute ulcer on anotherwise normal pyloric ring will produce intensepylorospasm and, from this, gastric retention andvomiting.
Dr. J. D. Stewart, taking part in a discussionfollowing Herrington's paper on vagotomy andpyloroplasty in the treatment ofjhiatus hernia withoesophagitis, said: 'We have been impressed bythe frequency with whiclr evidence of pylorichypertrophy can be fou)i in these patients. Inmany cases the pyloric ring is hypertrophied,much as it would be found in the infant withcongenital hypertrophic pyloric stenosis. I believethat this is a very important consideration in theoperation' (Herrington, 1960.
Wieser, Allgower, Flury, and Markoff (1963),describing the radiological appearances of whatey.regarded as pyloric hypertrophy in the adult,
noted that 20% of their '44 patients with thishiYpertrophy%alsolad hiatus hernia.eThe assCciation of, congenital hypertrophicpyJoric stenosis with hiatus 4ernia in babies iswell documented. -Roviralta*,(19,52) de4cribed thisassociation -as the phreno-pyloric. syndrome. Hebelieved that the, raised. intratastric pressuresecondary to the obstructive pyloric lesion forcedthe stomach into the chest.
In this connexion, the paper by Johnston (1960)is important. He. wrote: 'Some of the clinicalfeatures of infantile hiatus hernia, even when thereis no associated hypertrophic pyloric stenosis, alsosuggest the presence of a gastric emptying dis-order. . . Interference with gastric emptying issuggested by the frequent clinical finding of visiblegastric peristalsis and by the fact that the vomitingitself ... is usually forcible or even projectile....'
Winkelstein (1935) found high fasting gastricacid levels in all his patients with peptic oeso-phagitis. Fasting free HCI is almost entirelycephalic-phase in origin, and this phase isabolished by vagotomy. Casten et al. (1963) found,on average, that fasting gastric acid levels werehigher in patients with symptomatic hiatus hernia
67
on 30 March 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.21.1.67 on 1 January 1966. D
ownloaded from
68 Harold W. Burge, Alan Morton Gill, Charles D. T. MacLean, and Ronald H. Lewis
without oesophagitis than in an asymptomaticgroup.
Both duodenal ulceration and pyloric channeldisease are best treated surgically by vagotomyand pyloroplasty. This operation cures both theseconditions in spite of the fact that pyloric channeldisease is frequently associated with hyposecretionor absence of HCI in the fasting stomach and a
low response to histamine. This state of affairsmight well be called a vagal paradox. We haveyet to explain it.To treat hiatus hernia by any operation without
at the same time attempting to cure the moredistal lesion, whether it be duodenal ulcerationor pyloric channel disease, seems irrational.
THE PRESENT STUDY
When, in 1962, we found not only duodenalulceration but also pyloric channel diseaseassociated with symptomatic hiatus hernia, we
began to study the duodenum and the pylorus inall patients with hiatus hernia subjected to opera-tion. This association of symptomatic hiatushernia and pyloric channel disease has alreadybeen reported by one of us (Burge, 1964). In our
present study we made use of the following:
HISTORY This we regard as most important.Almost invariably in this series of patients theonset of dysphagia and heartburn from refluxhas been preceded by a history, often long, ofpain one to two hours after food, typical of duo-denal ulcer or of pyloric channel disease. In manypatients there has been a history of intermittentvomiting of food which had clearly entered thestomach one or more hours previously. Wepresume this vomiting was caused by intermittentpyloric or duodenal disease.
PRE-OPERATIVE RADIOLOGY It is essential that theradiologist should be familiar with all the appear-ances found in pyloric channel disease. Theremust be excellent pictures of both the pyloric ringand the prepyloric stomach, and careful studiesshould be made for evidence of gastric retention.Figures 1 to 7 are examples taken from our series.
EXTERNAL EXAMINATION OF PYLORUS AND DUO-
DENUM AT OPERATION Peritoneal scarring in duo-denal ulceration is frequently found, and thetypical stippling is produced by rubbing the sur-
face of the duodenum with a swab. Occasionally,scarring exactly at the pylorus is found, but thisis rare because the thick pyloric muscle separates
the peritoneal surface from the underlyingmucosal disease.
INTERNAL EXAMINATION OF PYLORIC RING THROUGHA PREPYLORIC GASTROTOMY INCISION It is import-ant to understand the normal state when thepyloric ring is examined digitally in this way.Considerable experience is necessary.
EXAMINATION OF MUCOSA FOR ULCERATION ANDMUSCLE FOR HYPERTROPHY WHEN THE GASTROT-OMY INCISION IS CARRIED ACROSS THE PYLORUSIN MAKING THE PYLOROPLASTY Pyloric and pre-pyloric muscle hypertrophy is commonly foundin pyloric channel disease. Again the normal mustbe known.
RESULTS
Since we first appreciated the association ofpyloric channel disease with hiatus hernia, 44 con-secutive cases have been treated by vagotomy andpyloroplasty together with repair of the hernia.Thirty (67%) of our patients gave a history ofintermittent vomiting of food, which had clearlyentered the stomach before the onset of dysphagiaand reflux; 12 (27%) showed evidence of gastricretention on radiological examination.Concomitant duodenal ulceration was present in
22 (50%) and pyloric disease in 34 (77%). Thisapparent discrepancy is due to the not infrequentassociation of basal duodenal disease with pyloricchannel disease in the same patient. When duo-denal ulceration has been the associated disease,the lesion has almost always been in the base ofthe duodenal cap, where it can easily (fromoedema, spasm, or fibrosis) obstruct the pyloriccanal.
Lesser curve gastric ulcer was found in sixpatients (14%). In each of these either pyloricchannel disease or duodenal ulceration waspresent.
In only one patient in this series was there noclinical, radiological, or surgical evidence ofpyloric or duodenal disease. This patient hadatypical symptoms and has had severe psychiatricillness since the operation. We believe she was acase of asymptomatic hernia unwisely treated byoperation.There were seven patients in this series with
peptic oesophageal stricture from peptic oeso-phagitis. In five of these gastric acid studies couldnot be made because a naso-gastric tube couldnot be passed. In the other two there was con-
on 30 March 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.21.1.67 on 1 January 1966. D
ownloaded from

FIG. 1. Associated duodenal ulceration.Shows a fibrotic oesophageal stricture (S).The duodenal cap is deformed (DU) fromchronic vIkeration. Barium meal showedgastric retention in the two-hourfilm.
(b)FIG. 2. Associated pyloric channel disease: (a) hiatushernia (HH) and gastric retention (GR); (b) an irregularpyloric canal (AA). Internal digital examination revealed asevere mucosal stenosis at the pylorus.
(a)
on 30 March 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.21.1.67 on 1 January 1966. D
ownloaded from
70 Harold W. Burge, Alan Morton Gill, Chtl.s D. T. MzcLean, and Ronald H. Lewis
PD
( )
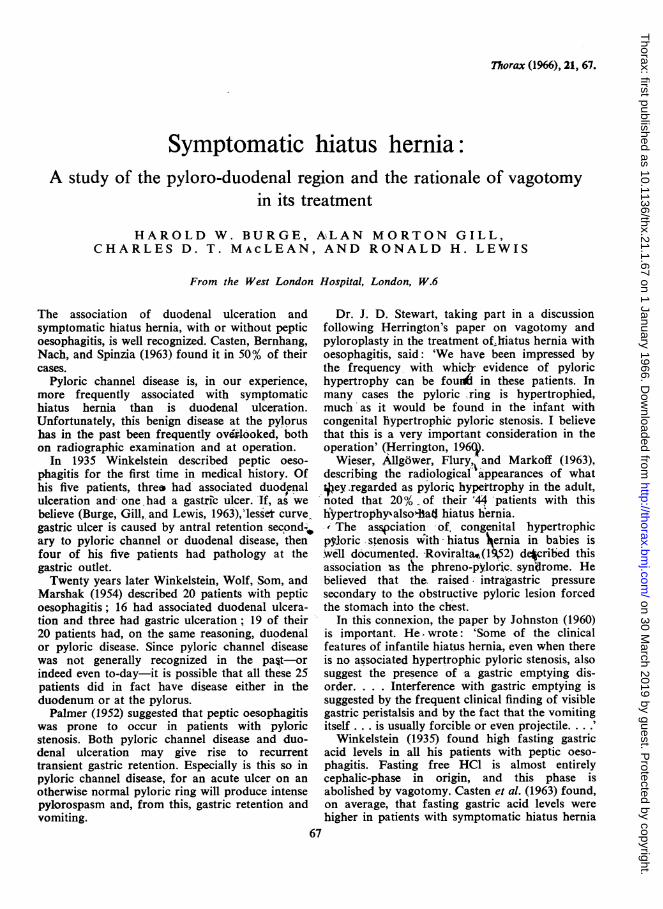
FIG. 3. Associatedpyloric channel disease: (a) there is grossradiological abnormality from pyloric channel disease(PD); (b) the hiatus hernia (HH) and the pyloric channeldisease (PD).
siderable hypersecretion of free HCI in the fastingstomach and in response to histamine. In one thefasting secretion was 10 mEq/hr., and in theother 9 mEq/hr. (normal= 1-4 mEq/hr.). Themaximal histamine test in these two patients gave39 mEq/hr. and 36 mEq/hr. (normal=21 mEq/hr.). In one of these two patients, nine monthsafter vagotomy and pyloroplasty and repair ofthe hernia, the fasting acid secretion was 1-7 mEq /hr. and, after maximal histamine stimulation,9 1 mEq/hr.
In those patients without peptic oesophagitisthe acid levels have either been normal or haveshown a picture of hyposecretion, often withabsent free HCl in the resting juice and a lowresponse to histamine.The incidence of gall-bladder disease is always
of interest in symptomatic hiatus hernia becauseof the significant frequency with which it isreported. Gall-stones were present in five (9%)of our patients.
In the first nine patients we used the Allisontype of repair of the hernia, done from belowthe diaphragm; the results were disappointing interms of radiological evidence of recurrence, andoccasionally symptoms of reflux persisted. Ourearlier experience of the Allison type of repairthrough both the abdomen and the chest, togetherwith a study of the long-term results, influencedus considerably. We have since used the Nissentechnique of fundoplication together with snugclosure of the crura around the oesophagus. Thisoperation has been associated with bilateral selec-tive vagotomy and preservation of the left gastricartery. Preservation of the artery is importantwhen the Nissen method is used. Completenessof nerve section has been proved by the electricalstimulation test in every case.
DISCUSSION
The incidence of associated duodenal ulcerationand symptomatic hiatus hernia in this series agreeswith the findings of Casten et al. (1963).
Since we have recognized pyloric channeldisease, both on radiological examination and atoperation, we have found it to be even morecommonly associated with symptomatic hiatushernia than duodenal ulceration. Frequently thetwo co-exist, and especially is this so when theduodenal ulceration is in the base of the cap whereit lies up against the pyloric ring; then bothdiseases seem to be one. Usually, however, pyloricchannel disease occurs without evidence of duo-
on 30 March 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.21.1.67 on 1 January 1966. D
ownloaded from
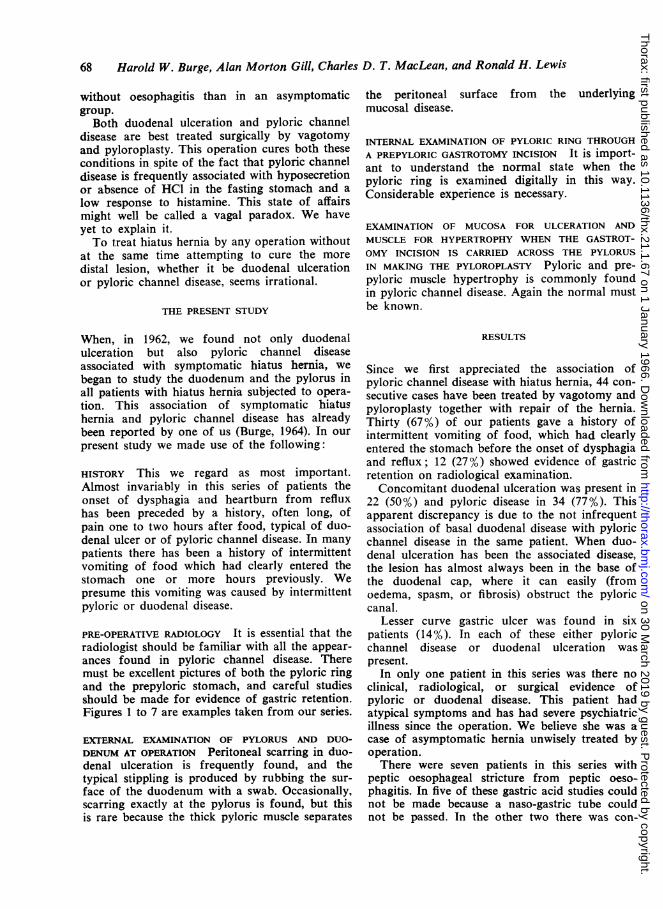
FIG. 4. Associated pyloric channeldisease. The barium meal showeda persistent filling defect whichwas thought to be malignant (FD).This was in fact benign pyloricchannel disease.
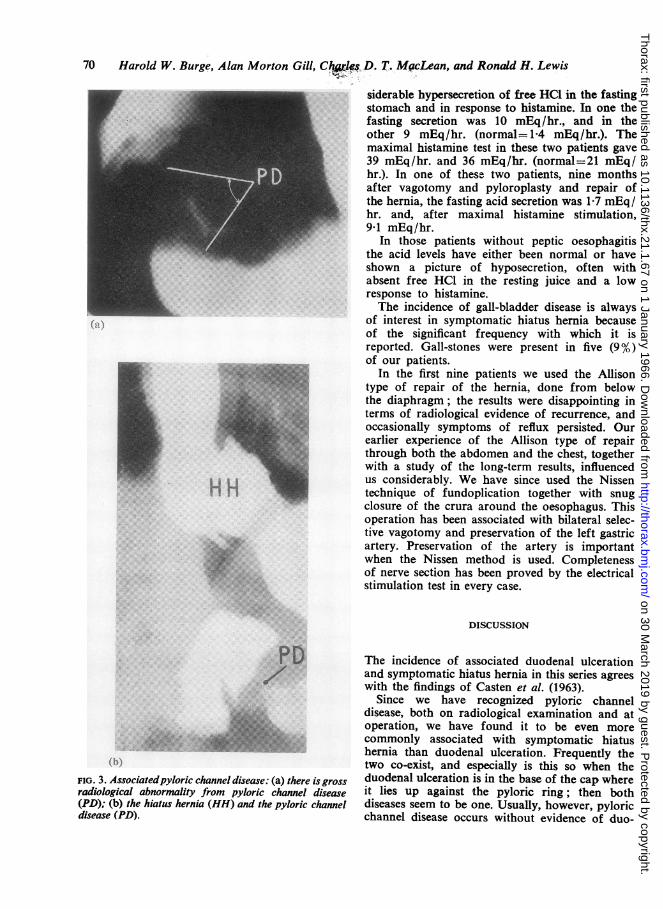
FIG. 5. Associated pyloric channeldisease. In this case there are astenosed pyloric channel (SPC)and gastric retention (GR).
G
on 30 March 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.21.1.67 on 1 January 1966. D
ownloaded from
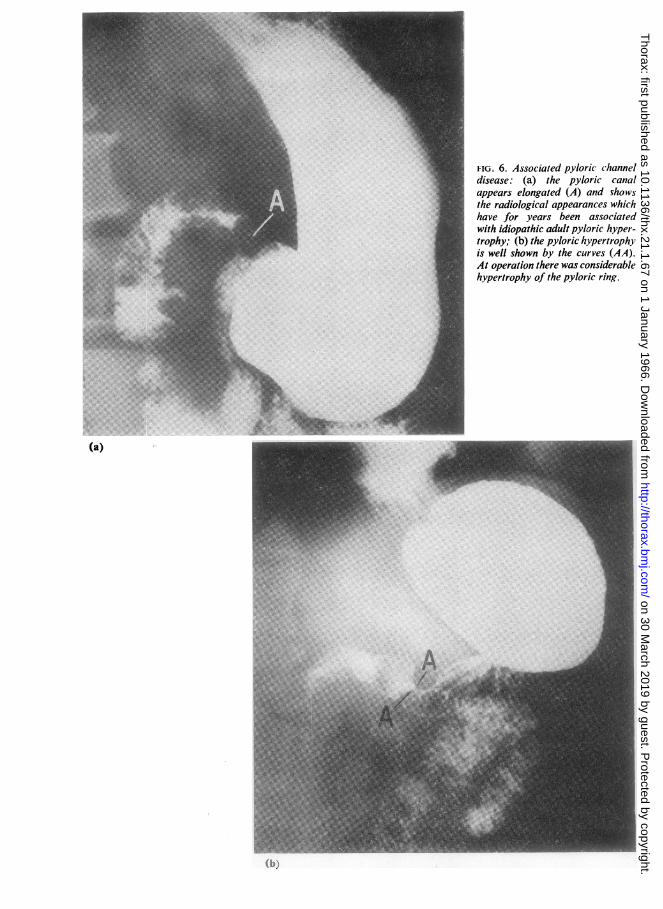
FIG. 6. Associated pyloric channeldisease: (a) the pyloric canalappears elongated (A) and shovsthe radiological appearances whichhave for years been associatedwith idiopathic adult pyloric hyper-trophy; (b) the pyloric hypertrophyis well shown by the curves (AA).At operation there was considerablehypertrophy of the pyloric ring.
(a)
...q -..:
..!: ..: i1, -.M. bko....:4
on 30 March 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.21.1.67 on 1 January 1966. D
ownloaded from
Symptomatic hiatus hernia
HH
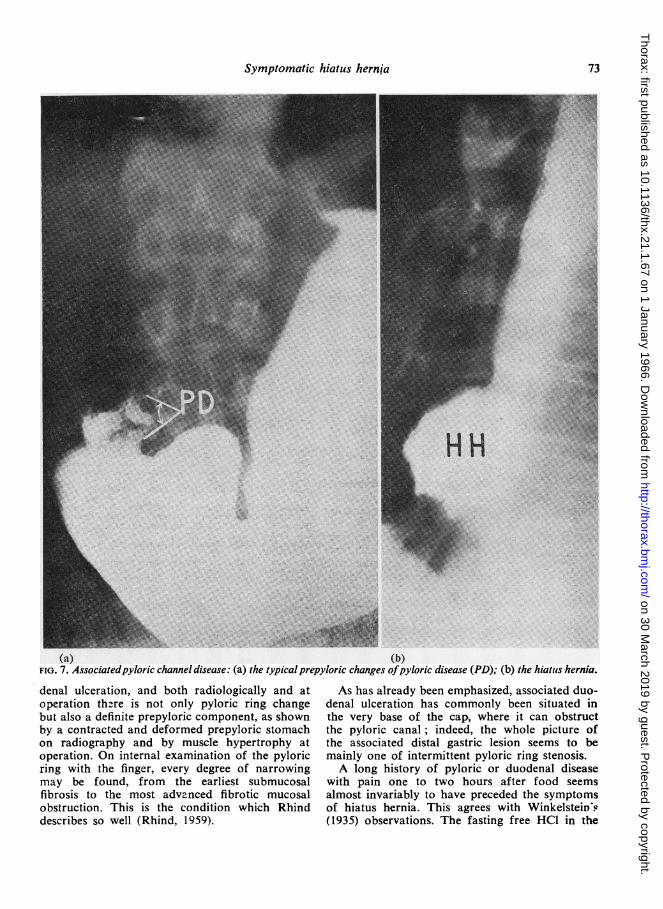
(a) (b)FIG. 7. Associatedpyloric channel disease: (a) the typical prepyloric changes ofpyloric disease (PD); (b) the hiatuis hernia.
denal ulceration, and both radiologically and atoperation there is not only pyloric ring changebut also a definite prepyloric component, as shownby a contracted and deformed prepyloric stomachon radiography and by muscle hypertrophy atoperation. On internal examination of the pyloricring with the finger, every degree of narrowingmay be found, from the earliest submucosalfibrosis to the most advanced fibrotic mucosalobstruction. This is the condition which Rhinddescribes so well (Rhind, 1959).
As has already been emphasized, associated duo-denal ulceration has commonly been situated inthe very base of the cap, where it can obstructthe pyloric canal; indeed, the whole picture ofthe associated distal gastric lesion seems to bemainly one of intermittent pyloric ring stenosis.A long history of pyloric or duodenal disease
with pain one to two hours after food seemsalmost invariably to have preceded the symptomsof hiatus hernia. This agrees with WinkelsteiD's(1935) observations. The fasting free HC1 in the
73
on 30 March 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.21.1.67 on 1 January 1966. D
ownloaded from
74 Harold W. Burge, Alan Morton Gill, Charles D. T. MacLean, and Ronald H. Lewis
two patients with peptic oesophagitis and stricturein whom acid estimations were done was high,and this finding, too, agrees with that of Winkel-stein. The remarkable long-term results in theseven patients with peptic stricture make it clear,in our view, that no major operation should beundertaken in the treatment of benign oesophagealstricture, no matter how severe, until vagotomyand pyloroplasty has been tried.The gastric acid levels in the patients without
evidence of oesophagitis have been either normalor low. The picture has generally been one ofhyposecretion. These findings agree with ourearlier observations of acid levels in pyloricchannel disease (Burge et al., 1963).When duodenal ulceration is present, whether
it be juxtapyloric or not, vagotomy and pyloro-plasty should be added to the hiatal repair.We have given much thought to the possibility
that our findings with regard to the pylorus arefalse and that we have mistaken the normal forthe abnormal; we do not think this is so. In manycases the pyloric changes have been too grossto allow error. Nevertheless, we feel that this maybe one criticism levelled against the work. Onmany occasions visiting surgeons, greatly experi-enced in gastric work, have assisted at theseoperations and have agreed that the pyloric canal,on internal digital examination, has beenabnormal. Pyloric channel disease with its mucosalstenosis and pyloric and prepyloric muscle hyper-trophy, as well as its mucosal gastritis, is, and haslong been, a well-recognized lesion.
It is interesting, therefore, to read in this issueof Thorax the description of a case in which thereis a mucosal stenosis of the distal duodenum withgastric retention, hiatus hernia, peptic oesophagitis,and stricture (Johnston and Stevenson, 1966). Thiscase is basically the same as our pyloric onesexcept that the obstructive lesion is more distaland is considered to be congenital.
SUMMARY
The literature concerning the association ofsymptomatic hiatus hernia with duodenal ulcera-tion is briefly reviewed. The relationship of hiatushernia and congenital pyloric stenosis in the infantis discussed. This paper records the incidence ofduodenal ulceration and of pyloric channel diseasein 44 consecutive cases of symptomatic hiatushernia with or without peptic oesophagitis andstricture. Fifty per cent. of patients were foundto have concomitant duodenal ulceration and77% pyloric channel disease. Lesser curve gastriculcer was found in 14%. Of the seven patientswith peptic oesophageal stricture, very markedhyperchlorhydria was found in the two patientsin whom acid studies were possible. The effectof vagotomy in these patients is recorded. Therationale of vagotomy and pyloroplasty togetherwith a hiatal repair is considered. Bilateral selec-tive vagotomy and the Nissen repair have beenused in all patients.
REFERENCES
Burge, H. (1964). Vagotomy, p. 197, Edward Arnold, London.Gill, A. M., and Lewis, R. H. (1963). The pyloric-channel syn-drome and gastric ulceration. Lancet, 1, 73.
Casten, D. F., Bernhang, A., Nach, R. J., and Spinzia, J. (1963). Aphysiological basis for the surgical treatment of sliding esopha-geal hiatus hernia. Surg. Gynec. Obstet., 117, 87.
Herrington, J. L. (1960). Hiatal hernia with esophagitis: treatment byhernia repair, vagotomy and pyloroplasty or antrectomy. Ann.Surg., 151, 812.
Johnston, J. H. (1960). Hiatus hernia in childhood. Arch. Dis.Childh., 35, 61.
Johnston, S. W., and Stevenson, H. M. (1966). Reflux oesophagitissecondary to a duodenal diaphragm in an adult. Thorax, 21, 65.
Palmer, E. D. (1952). The Esophagus and its Diseases, Hoeber, NewYork.
Rhind, J. A. (1959). Mucosal stenosis of the pylorus. Brit. J. Surg.,46, 534.
Roviralta, E. (1952). Les Vomissements du Nourrisson. Flammarion,Paris.
Wieser, C., Allg6wer, M., Flury, A., and Markoff, N. (1963). Diegutartige Pylorushypertrophie des Erwachsenen im Rontgenbild.Raliol. clin. (Basel), 32, 77.
Winkelstein, A. (1935). Peptic esophagitis: a new clinical entity.J. Amer. med. Ass., 104, 906.Wolf, B. S., Som, M. L., and Marshak, R. H. (1954). Peptic
esophagitis with duDdenal or gastric ulcsr. Ibid., 154, 885.
on 30 March 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.21.1.67 on 1 January 1966. D
ownloaded from


![Right congenital pleuro-peritoneal hiatus hernia · Right congenital pleuro-peritoneal hiatus hernia 155 References [1] Adzick NS, Harrison MR, Glick PL, Nakayama DK, Manning FA,](https://img.pdfslide.us/doc/110x75/5b8bb26309d3f231638bd035/right-congenital-pleuro-peritoneal-hiatus-hernia-right-congenital-pleuro-peritoneal.jpg)


























