Embed Size (px)
Citation preview
http://pmj.sagepub.com/Palliative Medicine
http://pmj.sagepub.com/content/18/1/75.2The online version of this article can be found at:
DOI: 10.1177/026921630401800118
2004 18: 75Palliat MedKathleen L Sherry
Symptom prevalence and the use of systematic symptom assessment
Published by:
http://www.sagepublications.com
can be found at:Palliative MedicineAdditional services and information for
http://pmj.sagepub.com/cgi/alertsEmail Alerts:
http://pmj.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://pmj.sagepub.com/content/18/1/75.2.refs.htmlCitations:
What is This?
- Jan 1, 2004Version of Record >>
at NORTH CAROLINA STATE UNIV on November 6, 2013pmj.sagepub.comDownloaded from at NORTH CAROLINA STATE UNIV on November 6, 2013pmj.sagepub.comDownloaded from at NORTH CAROLINA STATE UNIV on November 6, 2013pmj.sagepub.comDownloaded from

The role of automatic externalde� brillators
Sir ¡/ We agree with Thorns and Gannon1 that thedevelopment and increasing use of automatic externaldefibrillators (AEDs) has sparked a debate with regard totheir potential role in palliative care inpatient units.However, we disagree with a number of points raised inthis article.
All of the evidence supporting the effectiveness ofAEDs has been gathered from previously healthy peoplewho suffered a witnessed cardiac arrest. Extensive clinicalexperience would suggest that the vast majority ofpalliative care inpatients do not suddenly collapse whenthey die, but rather that they deteriorate slowly and thatdeath usually occurs after respiratory arrest.
The proportion of palliative care patients sufferingventricular fibrillation or pulseless ventricular tachycar-dia amenable to defibrillation is likely to be tiny,although we acknowledge that there are an increasingnumber of patients referred to palliative care services withintractable ischaemic heart disease and cardiac failure.
The authors imply that minimal training is required touse AEDs, and that they can be used in isolation withoutother basic life support, such as cardiac massage andairway management. The Resuscitation Council Guide-lines state that AEDs are always used in association withbasic life support.2
The authors also omit to mention that if defibrillationis successful, the patient will need aftercare, usually in anintensively monitored environment, which inevitablymeans a transfer to hospital. This is likely to causefurther distress to the patient and their family, in analready traumatic situation.
Thorns and Gannon touch only briefly on staff andvisitors and do not mention volunteers. It is likely thatvisitors and volunteers in hospices will on average beolder than people in other public places, and therefore,more at risk of sudden cardiac events. If AEDs areeffective at saving lives of previously healthy people whocollapse in public places, then there may be a role for
AEDs in hospices. However, there is conflicting evidenceas to whether AEDs in public places do actually increasethe number of lives saved: Pell et al . calculated thatAEDs in public places only improved overall survivalfrom cardiac arrest by 1.3%3 (because most cardiacarrests occur in patients’ homes), and that to achievethis approximately 26 000 AEDs would be required inEngland and Wales alone at a cost of many millions ofpounds.
We do not agree that AEDs have a role to play in thecare of palliative care inpatients based on currentevidence and that further studies are required to justifytheir implementation in hospices as ‘public places’ forvolunteers, staff and visitors who suffer a cardiac arrest.
Emma J HallConsultant in Palliative Medicine,St. Christopher’s Hospice,51¡/59 Lawrie Park Road, Sydenham,London SE26 6DZ, UKE-mail: [email protected]
Debra E SwannConsultant in Palliative Medicine,St. Christopher’s Hospice and Mayday UniversityHospital NHS Trust,London Road, Thornton Heath,Surrey CR7 7YE, UKE-mail: [email protected]
References
1 Thorns A, Gannon C. The potential role for automaticexternal de� brillators in palliative care units. Palliat Med2003; 17: 465 ¡/67.
2 Resuscitation Council (UK). Resuscitation Council Guide-lines , 2000.
3 Pell JP, Sirel JM, Marsden AK, Ford I, Walker NL,Cobbe SM. Potential impact of public access de� brillatorson survival after out of hospital cardiopulmonary arrest:retrospective cohort study. BMJ 2002; 325: 515 ¡/17.
Symptom prevalence and the use ofsystematic symptom assessment
Sir ¡/ We are currently reviewing our clinical practice anddocumentation when assessing patients referred to theHospital Palliative Care Team based in a District GeneralHospital. We were interested in the symptom prevalencesdescribed by Potter et al .1 in relation to hospital patients,
and we, therefore, reviewed the initial assessments of 160patients referred to our Team over a six month period.This included our own HPCT multidisciplinary objectivelist of priorities/problems identified on initial assessmentand POS scores (Palliative Care Outcome Scale).2 TheHPCT routinely uses the POS: a validated outcome mea-sure for patients with advanced cancer and their families.This is completed by the patient in the majority of cases.
Letters to the editor 75
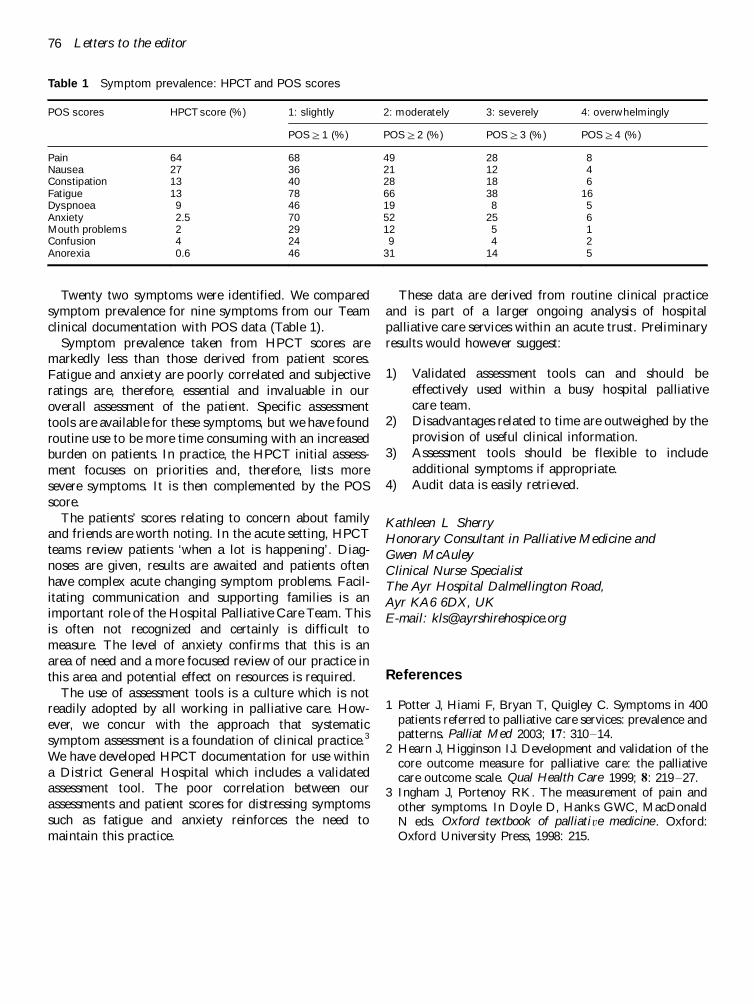
Twenty two symptoms were identified. We comparedsymptom prevalence for nine symptoms from our Teamclinical documentation with POS data (Table 1).
Symptom prevalence taken from HPCT scores aremarkedly less than those derived from patient scores.Fatigue and anxiety are poorly correlated and subjectiveratings are, therefore, essential and invaluable in ouroverall assessment of the patient. Specific assessmenttools are available for these symptoms, but we have foundroutine use to be more time consuming with an increasedburden on patients. In practice, the HPCT initial assess-ment focuses on priorities and, therefore, lists moresevere symptoms. It is then complemented by the POSscore.
The patients’ scores relating to concern about familyand friends are worth noting. In the acute setting, HPCTteams review patients ‘when a lot is happening’. Diag-noses are given, results are awaited and patients oftenhave complex acute changing symptom problems. Facil-itating communication and supporting families is animportant role of the Hospital Palliative Care Team. Thisis often not recognized and certainly is difficult tomeasure. The level of anxiety confirms that this is anarea of need and a more focused review of our practice inthis area and potential effect on resources is required.
The use of assessment tools is a culture which is notreadily adopted by all working in palliative care. How-ever, we concur with the approach that systematicsymptom assessment is a foundation of clinical practice.3
We have developed HPCT documentation for use withina District General Hospital which includes a validatedassessment tool. The poor correlation between ourassessments and patient scores for distressing symptomssuch as fatigue and anxiety reinforces the need tomaintain this practice.
These data are derived from routine clinical practiceand is part of a larger ongoing analysis of hospitalpalliative care services within an acute trust. Preliminaryresults would however suggest:
1) Validated assessment tools can and should beeffectively used within a busy hospital palliativecare team.
2) Disadvantages related to time are outweighed by theprovision of useful clinical information.
3) Assessment tools should be flexible to includeadditional symptoms if appropriate.
4) Audit data is easily retrieved.
Kathleen L SherryHonorary Consultant in Palliative Medicine andGwen McAuleyClinical Nurse SpecialistThe Ayr Hospital Dalmellington Road,Ayr KA6 6DX, UKE-mail: [email protected]
References
1 Potter J, Hiami F, Bryan T, Quigley C. Symptoms in 400patients referred to palliative care services: prevalence andpatterns. Palliat Med 2003; 17: 310 ¡/14.
2 Hearn J, Higginson IJ. Development and validation of thecore outcome measure for palliative care: the palliativecare outcome scale. Qual Health Care 1999; 8: 219 ¡/27.
3 Ingham J, Portenoy RK. The measurement of pain andother symptoms. In Doyle D, Hanks GWC, MacDonaldN eds. Oxford textbook of palliative medicine . Oxford:Oxford University Press, 1998: 215.
Table 1 Symptom prevalence: HPCT and POS scores
POS scores HPCT score (%) 1: slightly 2: moderately 3: severely 4: overwhelmingly
POS]/1 (%) POS]/2 (%) POS]/3 (%) POS]/4 (%)
Pain 64 68 49 28 8Nausea 27 36 21 12 4Constipation 13 40 28 18 6Fatigue 13 78 66 38 16Dyspnoea 9 46 19 8 5Anxiety 2.5 70 52 25 6Mouth problems 2 29 12 5 1Confusion 4 24 9 4 2Anorexia 0.6 46 31 14 5
76 Letters to the editor












,firstpublishedin1998,isa30-itemself-report measure](https://img.pdfslide.us/doc/110x75/5eb5753c3edc0459a63cccb3/systematic-review-of-the-multidimensional-fatigue-symptom-the-multidimensional.jpg)