Embed Size (px)
Citation preview
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 1/56
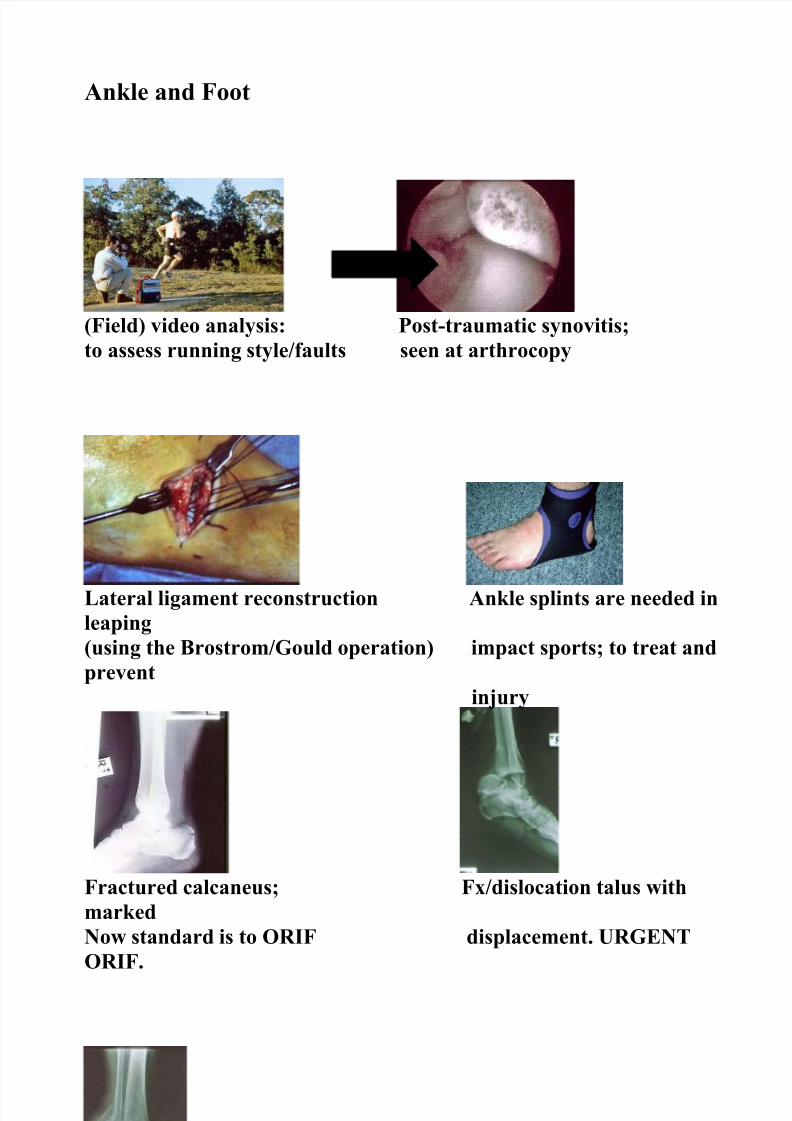
Ankle and Foot
(Field) video analysis: Post-traumatic synovitis;to assess running style/faults seen at arthrocopy
Lateral ligament reconstruction Ankle splints are needed inleaping(using the Brostrom/Gould operation) impact sports; to treat andprevent
injury
Fractured calcaneus; Fx/dislocation talus withmarkedNow standard is to ORIF displacement. URGENTORIF.
Fractured ankle;Reduce in ER, to lessenSoft tissue damage then ORIF.
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 2/56

8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 3/56
Children
Children are more prone to head injuries andShould wear helmets in most sports
Avulsion tibial spine Dislocated patella, easy to reduce
( carries the ACL). but slow rehab.Re-attach ( see Fig. below).
Kohler’s disease, AVN talus Fractures of the hip= disaster inchildren;Looks dramatic, but heals high complication rate. ORIF stat.
Spontaneously.
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 4/56
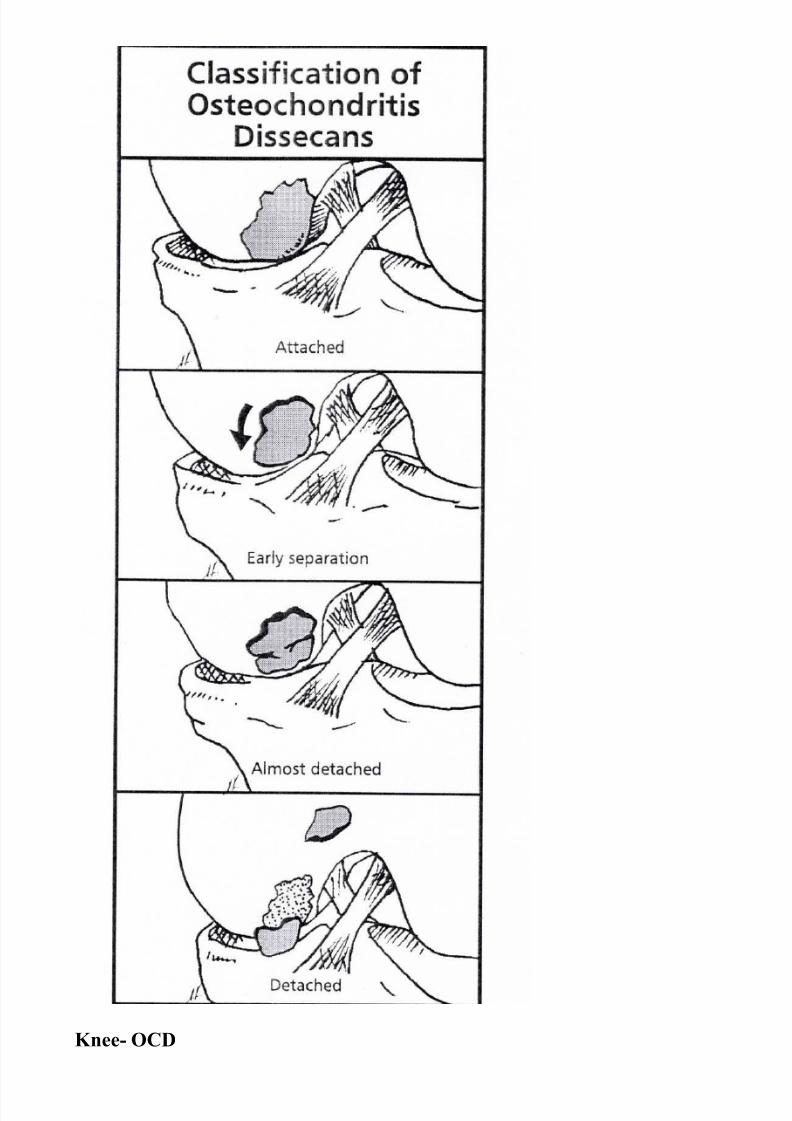
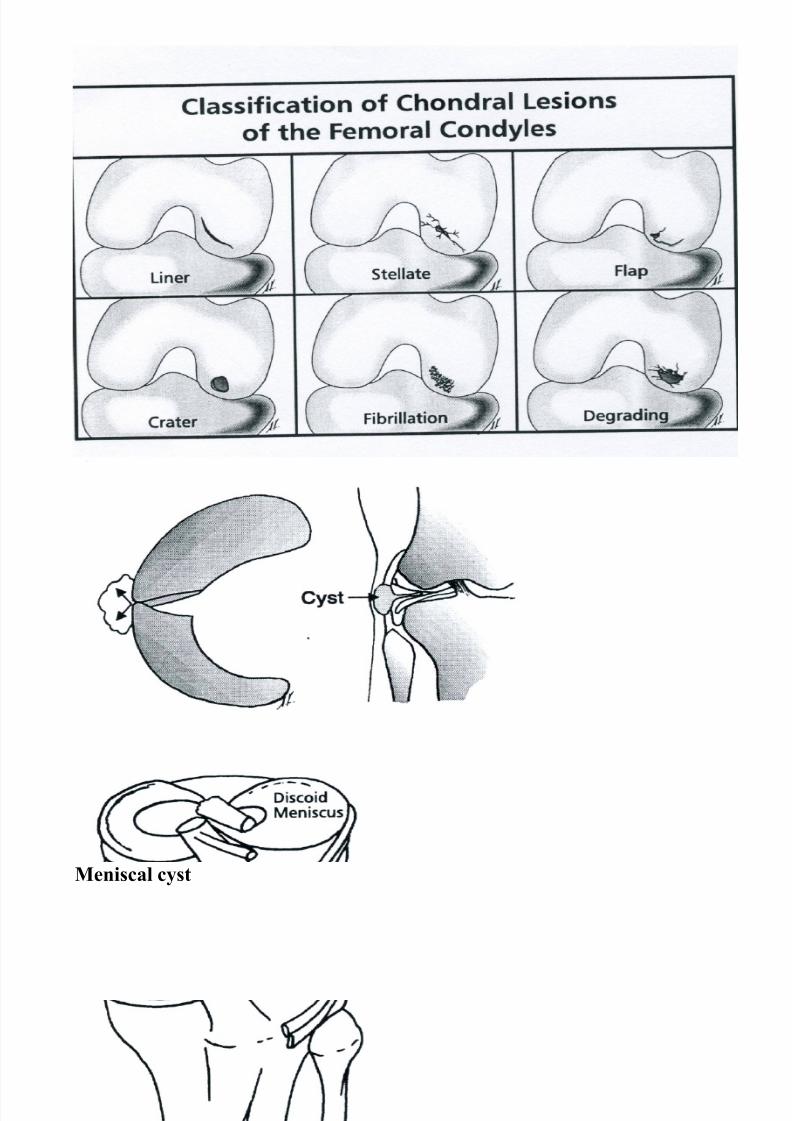
Knee- OCD
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 5/56
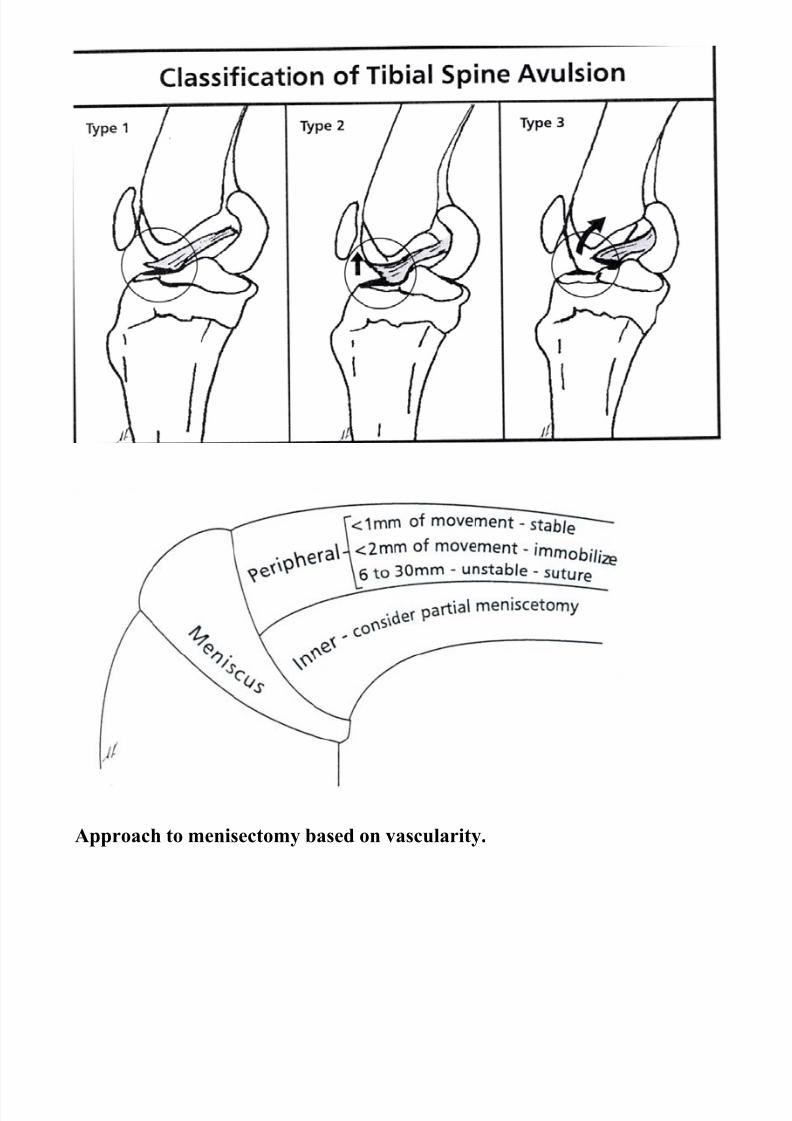
Approach to menisectomy based on vascularity.
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 6/56
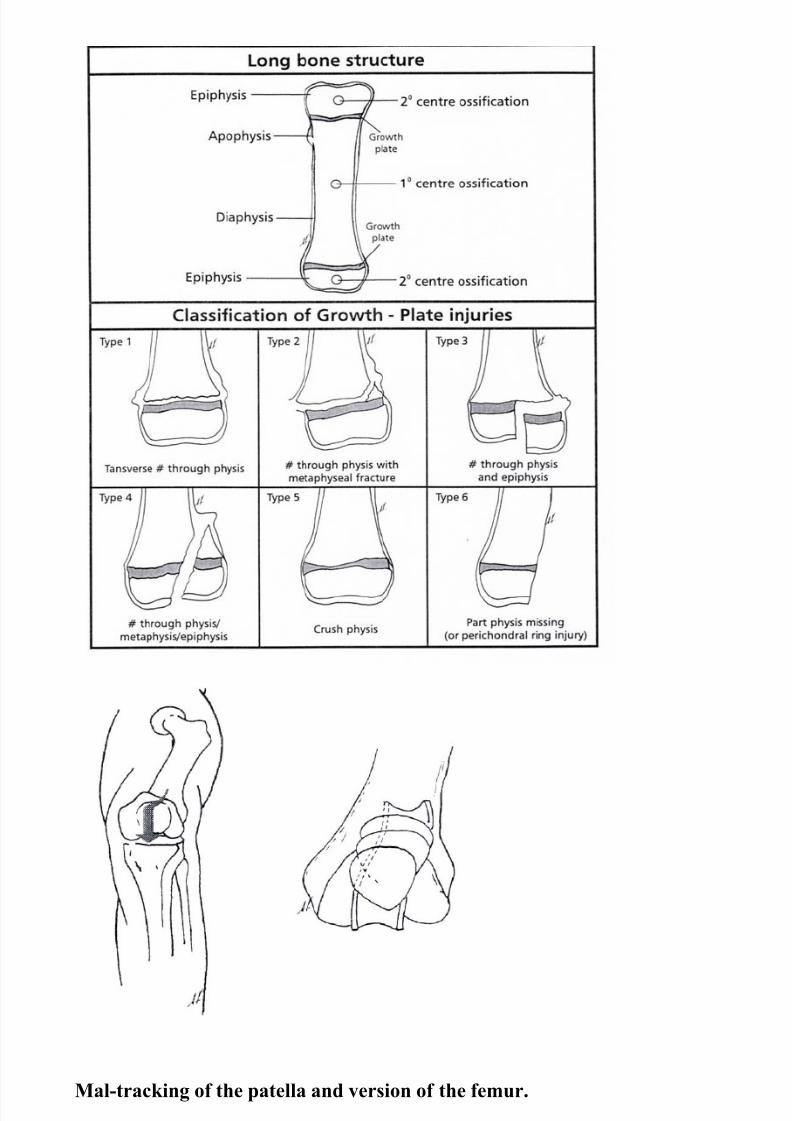
Mal-tracking of the patella and version of the femur.
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 7/56
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 8/56
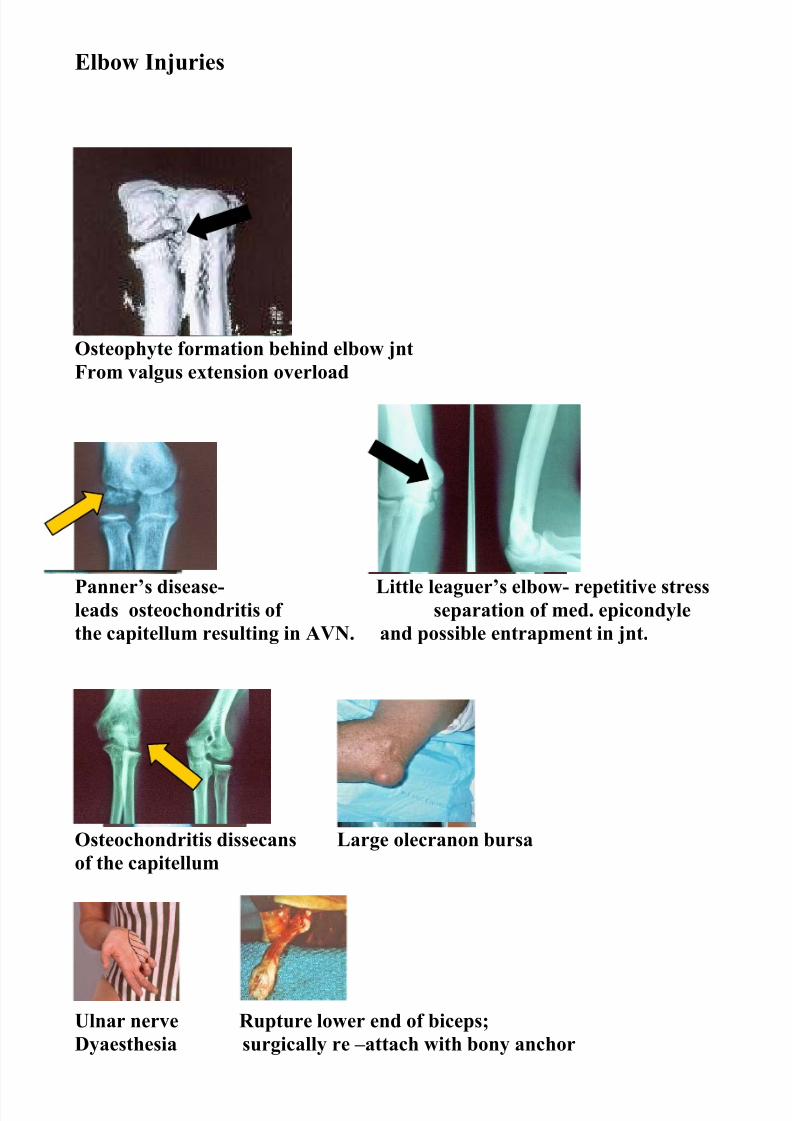
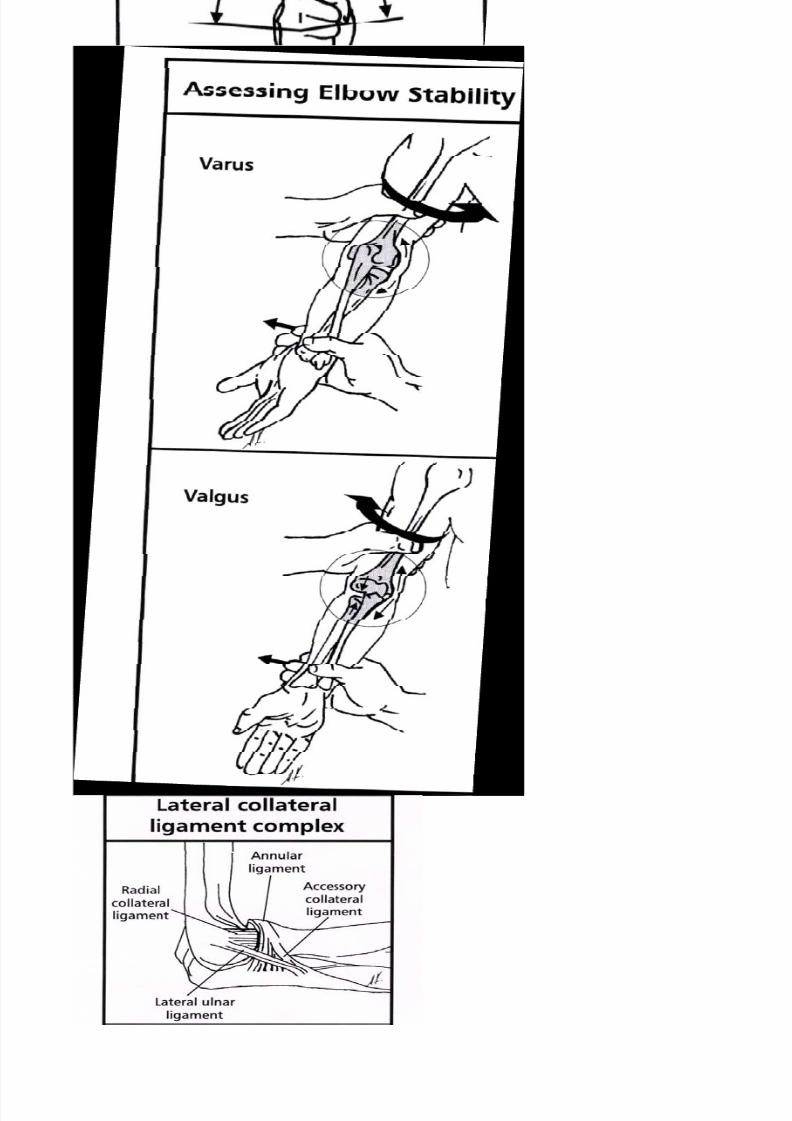
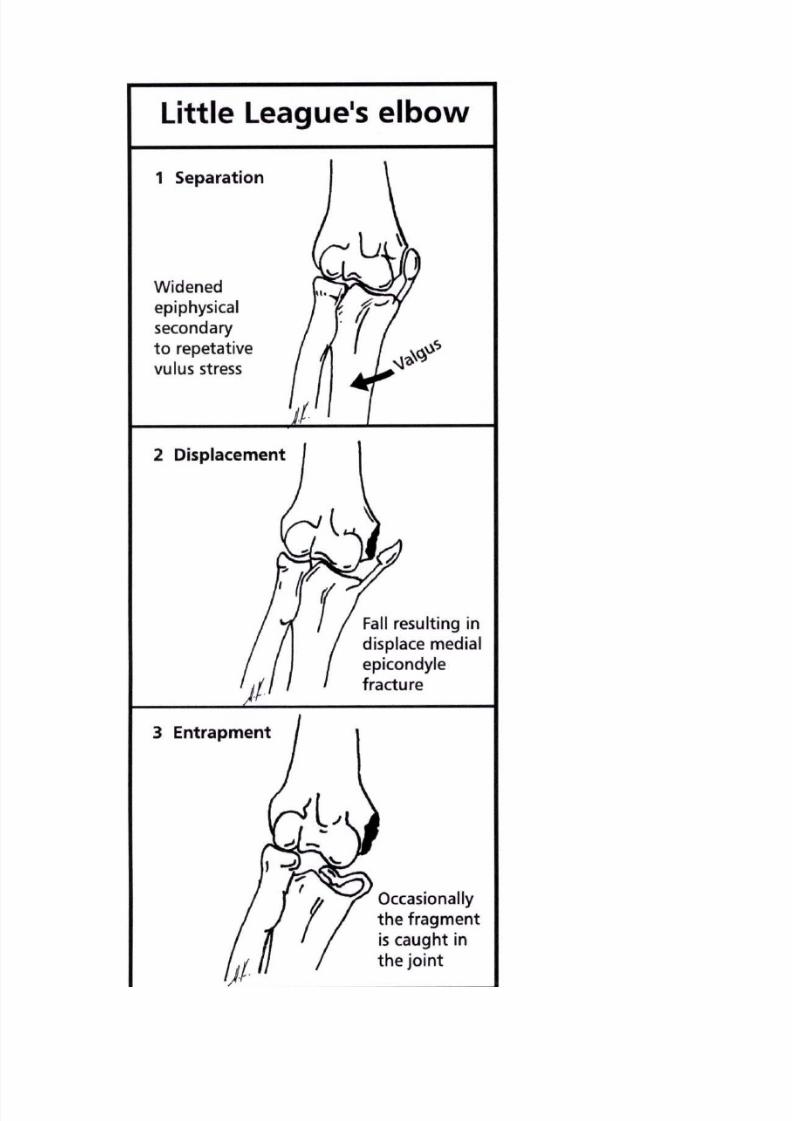
Elbow Injuries
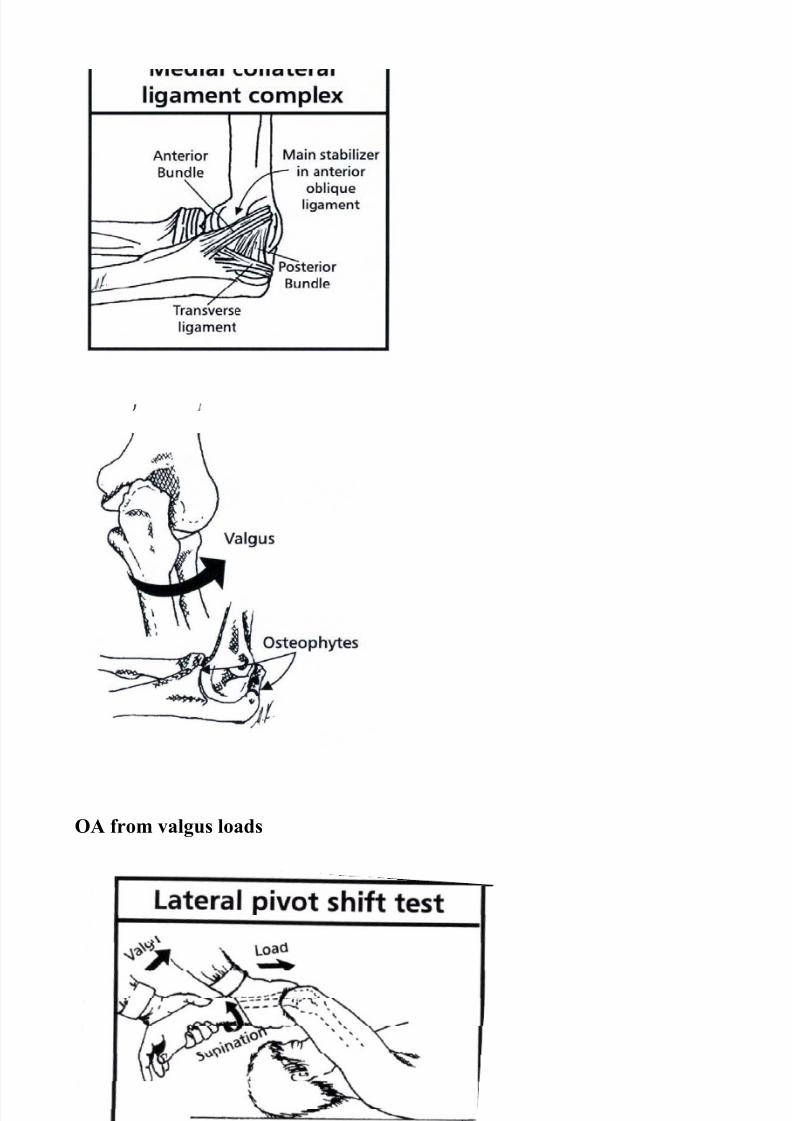
Osteophyte formation behind elbow jntFrom valgus extension overload
Panner’s disease- Little leaguer’s elbow- repetitive stressleads osteochondritis of separation of med. epicondylethe capitellum resulting in AVN. and possible entrapment in jnt.
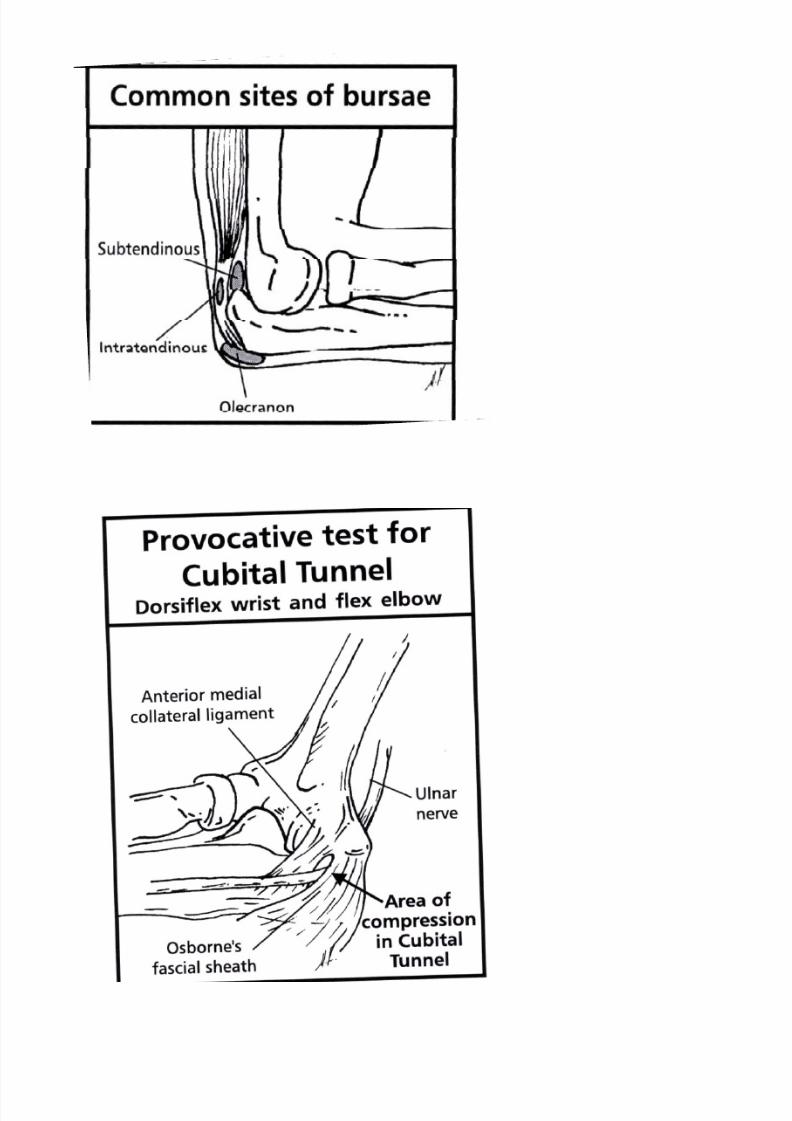
Osteochondritis dissecans Large olecranon bursaof the capitellum
Ulnar nerve Rupture lower end of biceps;Dyaesthesia surgically re –attach with bony anchor
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 9/56
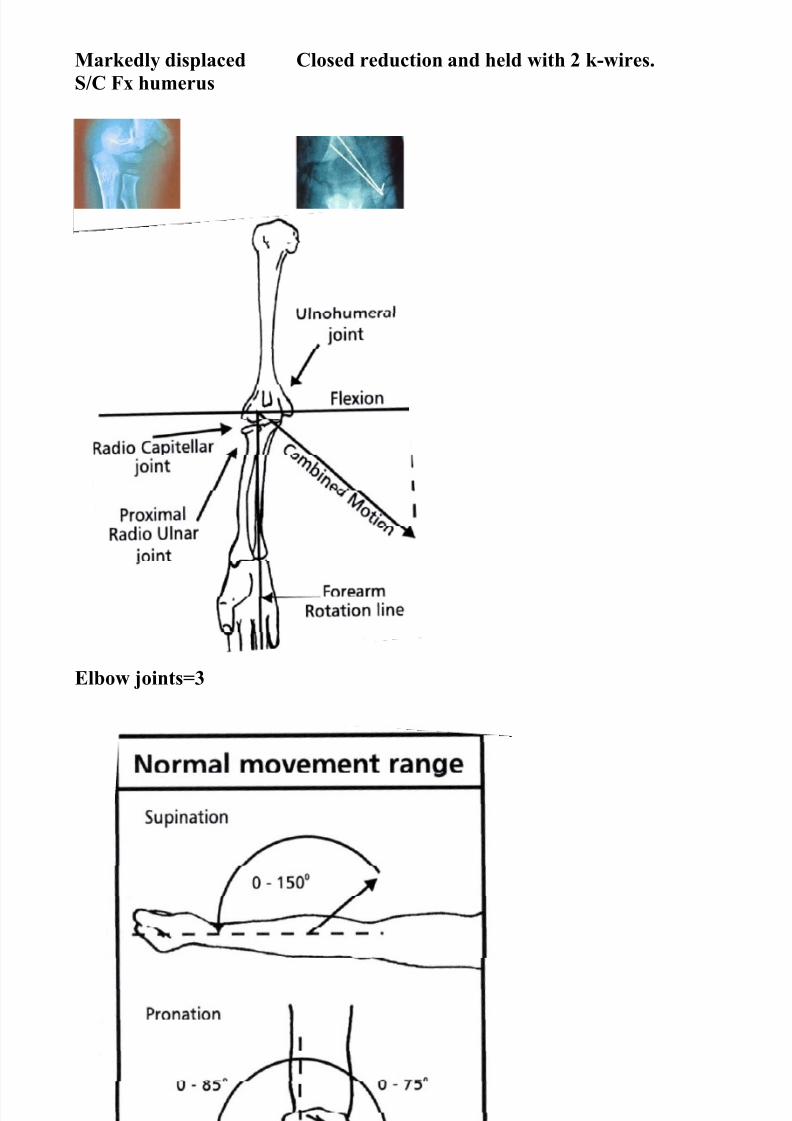
Markedly displaced Closed reduction and held with 2 k-wires.S/C Fx humerus
Elbow joints=3
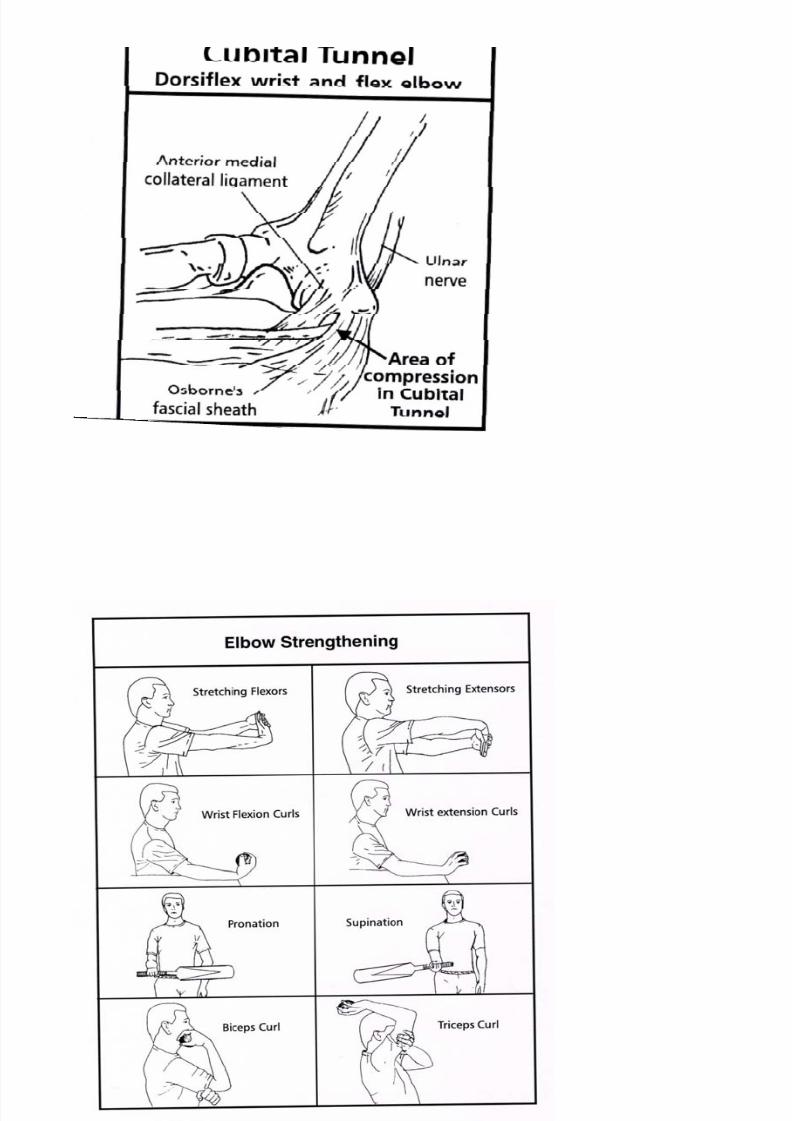
Elbow ROM.
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 10/56
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 11/56
OA from valgus loads

8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 12/56
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 13/56
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 14/56
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 15/56
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 16/56
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 17/56
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 18/56
EYE
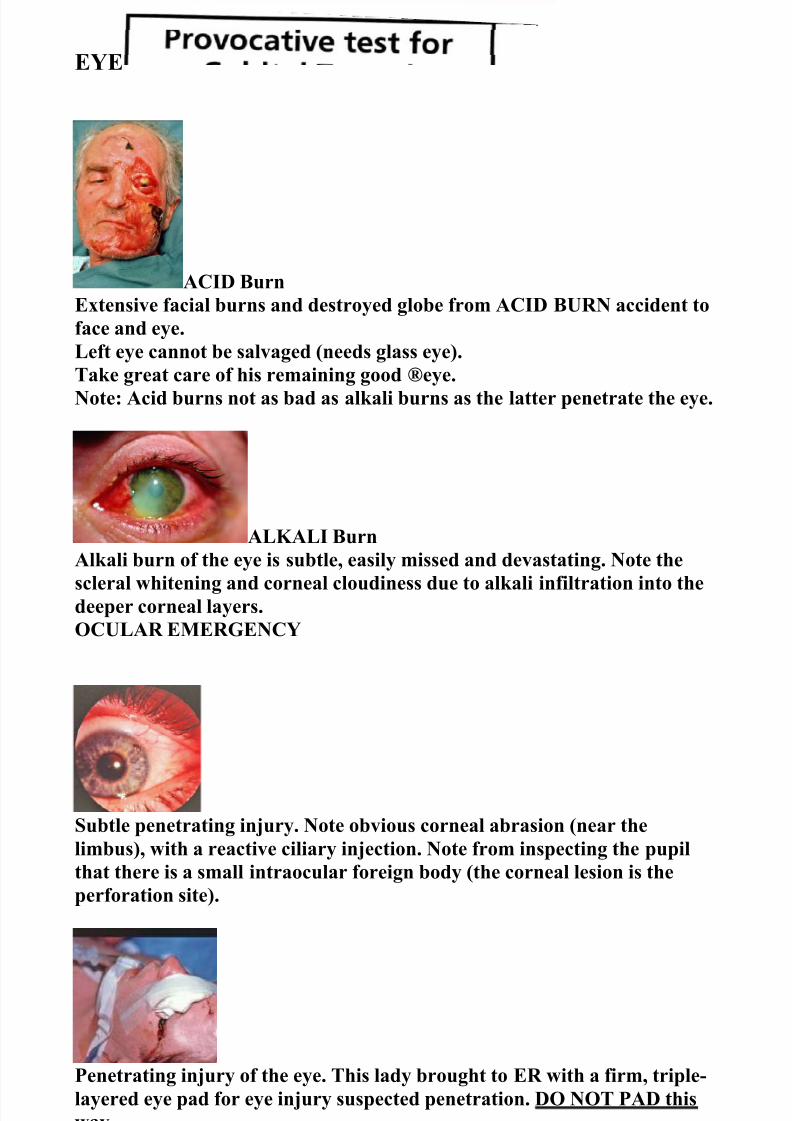
ACID BurnExtensive facial burns and destroyed globe from ACID BURN accident toface and eye.Left eye cannot be salvaged (needs glass eye).Take great care of his remaining good ®eye.Note: Acid burns not as bad as alkali burns as the latter penetrate the eye.
ALKALI BurnAlkali burn of the eye is subtle, easily missed and devastating. Note the
scleral whitening and corneal cloudiness due to alkali infiltration into thedeeper corneal layers.OCULAR EMERGENCY
Subtle penetrating injury. Note obvious corneal abrasion (near thelimbus), with a reactive ciliary injection. Note from inspecting the pupilthat there is a small intraocular foreign body (the corneal lesion is theperforation site).
Penetrating injury of the eye. This lady brought to ER with a firm, triple-layered eye pad for eye injury suspected penetration. DO NOT PAD thisway.
Note damage done to the eye if intra-ocular pressure is increased in thepresence of ocular penetration.Never firmly pad or manipulate a suspected penetrating injury of the eye.
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 19/56
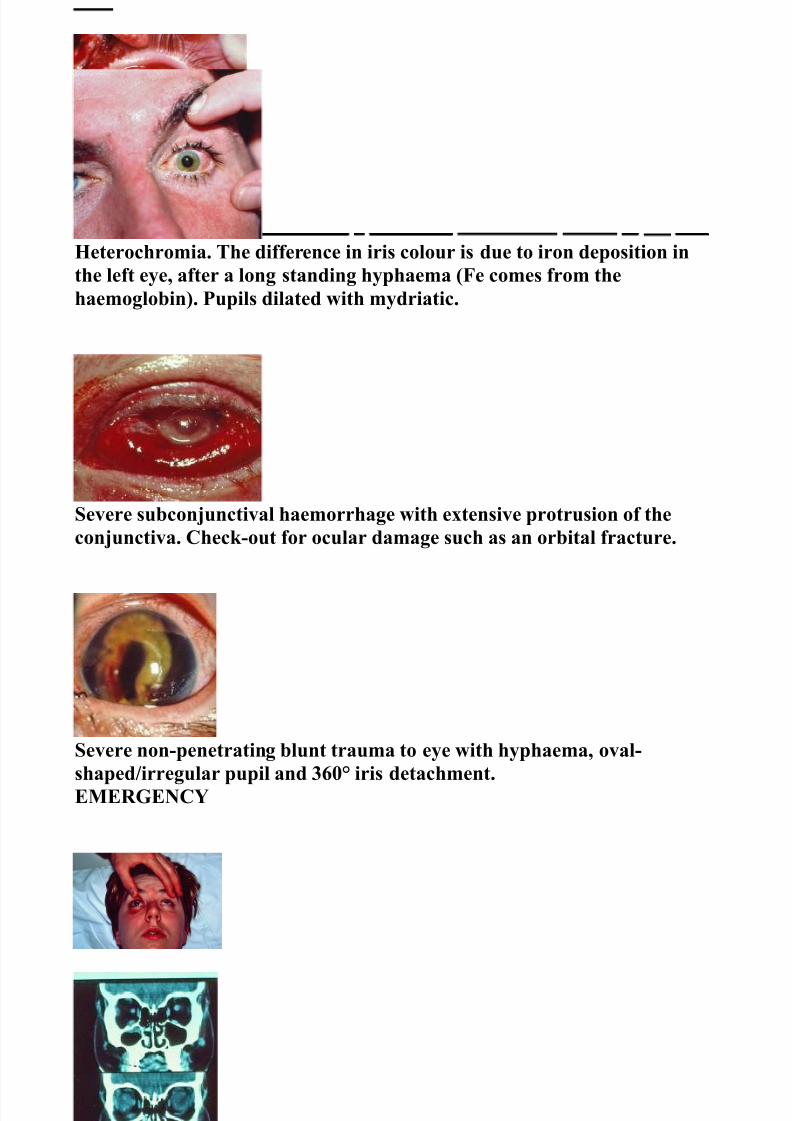
Heterochromia. The difference in iris colour is due to iron deposition inthe left eye, after a long standing hyphaema (Fe comes from thehaemoglobin). Pupils dilated with mydriatic.
Severe subconjunctival haemorrhage with extensive protrusion of theconjunctiva. Check-out for ocular damage such as an orbital fracture.
Severe non-penetrating blunt trauma to eye with hyphaema, oval-shaped/irregular pupil and 360° iris detachment.EMERGENCY
CT scan shows obvious Fx in Right orbit with herniation of intra-oculartissue( fat or inferior rectus muscle).
Fundoscopy shows a Fractional retinal detachment from a penetrating eyeinjury.
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 20/56
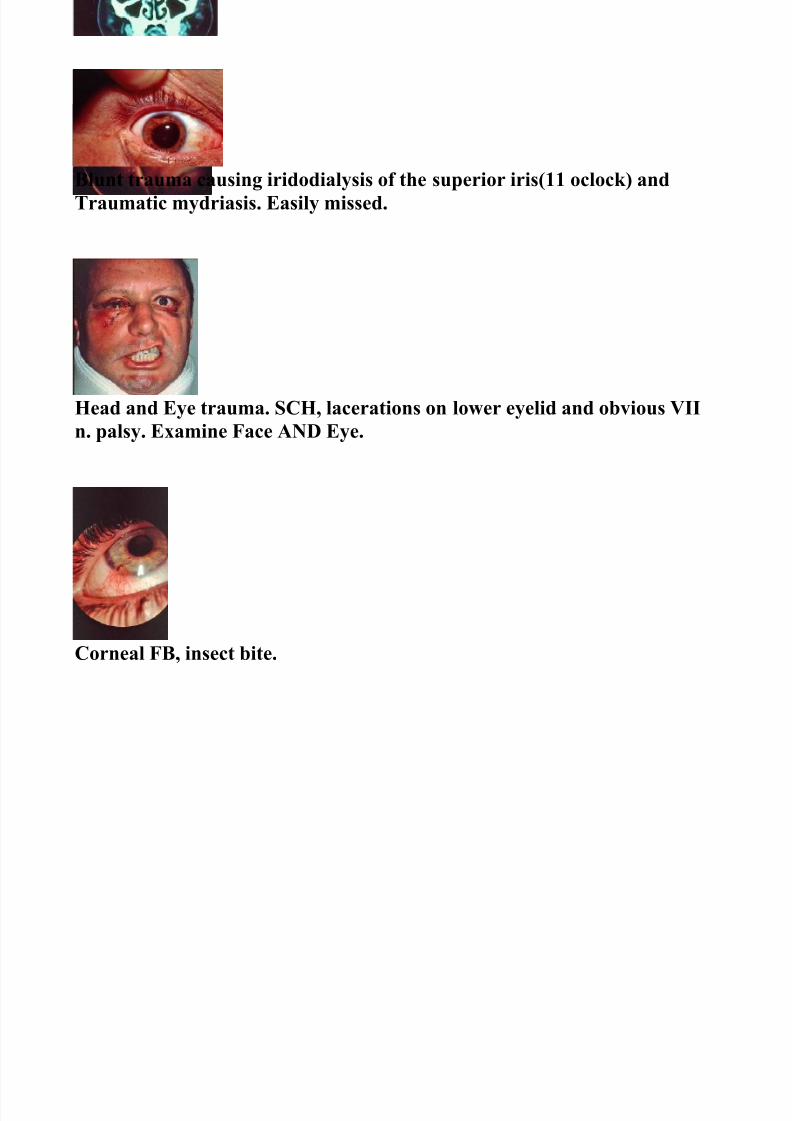
Blunt trauma causing iridodialysis of the superior iris(11 oclock) andTraumatic mydriasis. Easily missed.
Head and Eye trauma. SCH, lacerations on lower eyelid and obvious VIIn. palsy. Examine Face AND Eye.
Corneal FB, insect bite.

8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 21/56
Facial Skeleton
Subcondylar Fx fixed with arch bars and guiding elastics.
CT of zygomatic Fx
Internal fixation of mandibular Fx( mini-plates).
Angle Fx, involving impacted 3 rd molar tooth.
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 22/56
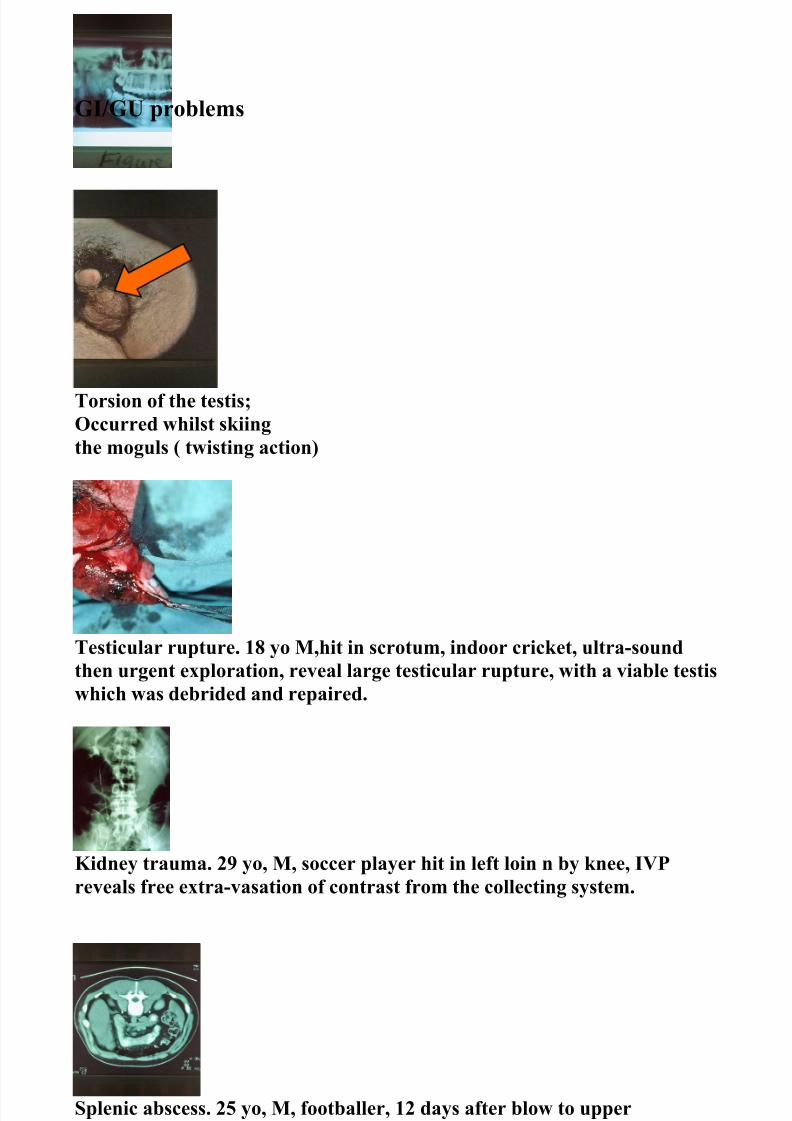
GI/GU problems
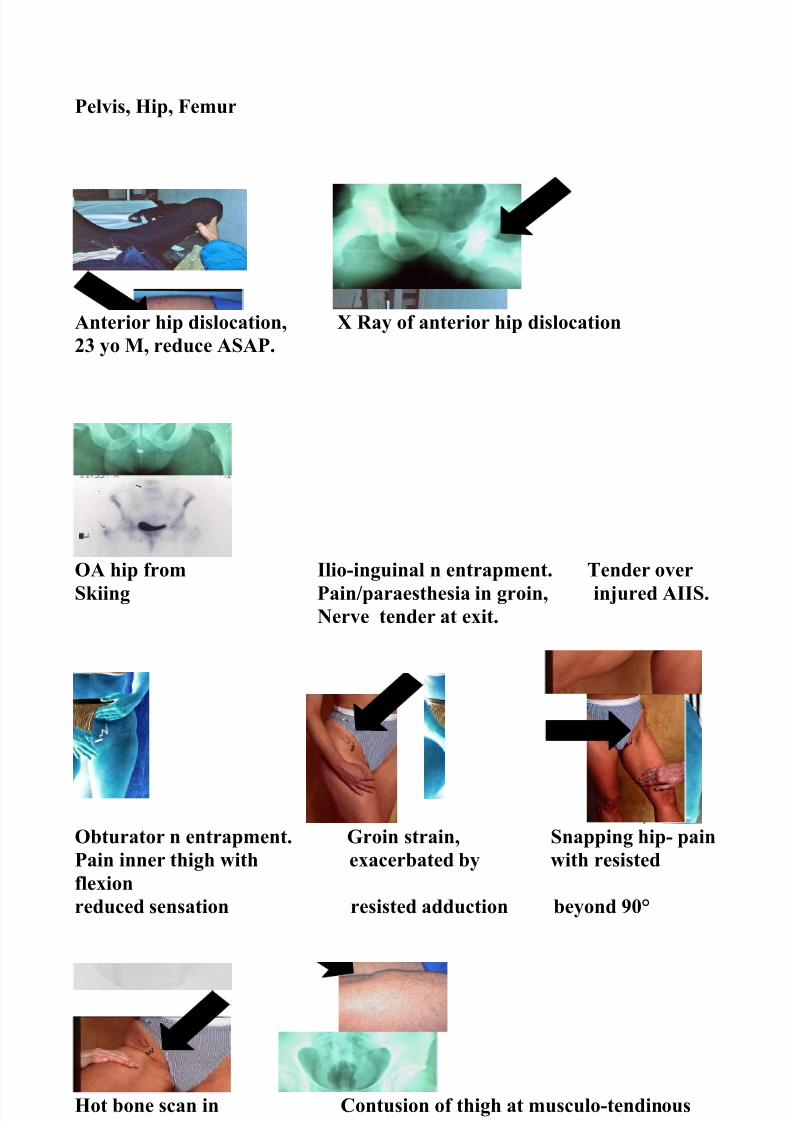
Torsion of the testis;Occurred whilst skiingthe moguls ( twisting action)
Testicular rupture. 18 yo M,hit in scrotum, indoor cricket, ultra-soundthen urgent exploration, reveal large testicular rupture, with a viable testiswhich was debrided and repaired.
Kidney trauma. 29 yo, M, soccer player hit in left loin n by knee, IVPreveals free extra-vasation of contrast from the collecting system.
Splenic abscess. 25 yo, M, footballer, 12 days after blow to upperquadrant, pain and fevers. CT reveals splenic abscess drained bypercutaneous drainage.
Avulsed shattered both spleen
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 23/56
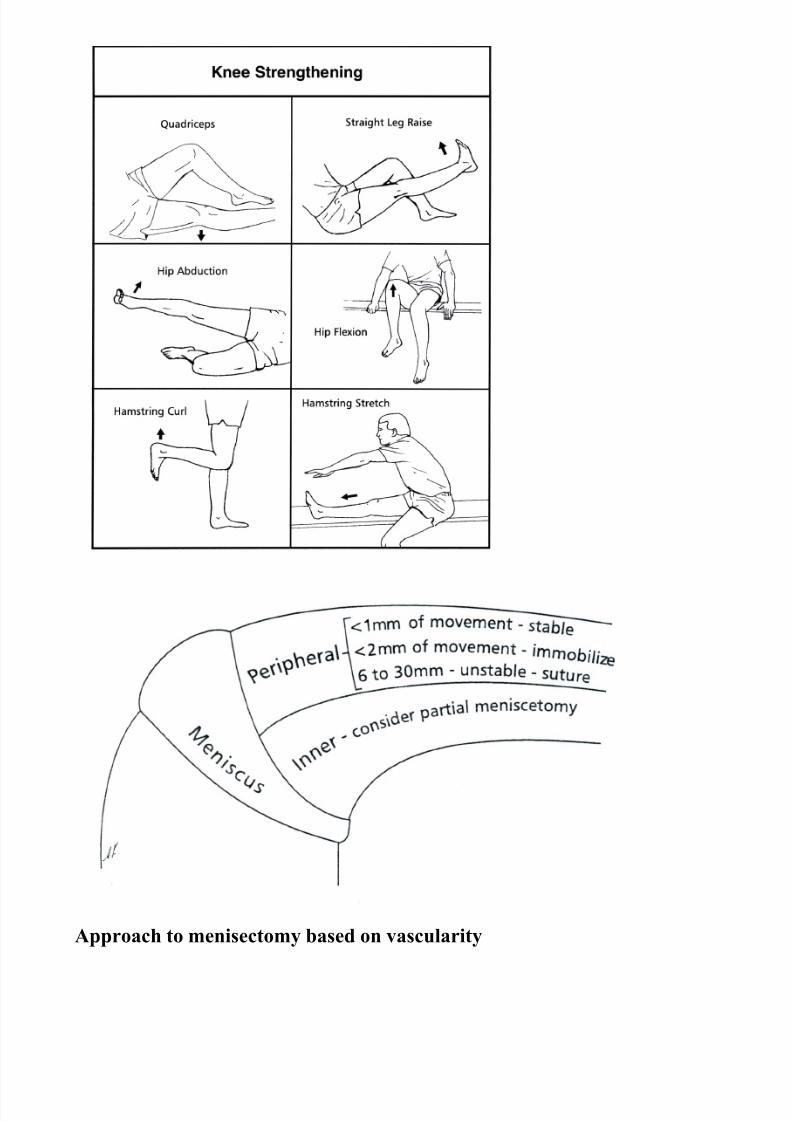
Approach to menisectomy based on vascularity
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 24/56
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 25/56
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 26/56

8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 27/56
Myositis ossificans Labral detachment at arthroscopyof the quads withmature bone formed
Hamstring sprain in resited extension in rugby tackle.
Groin strain in cutting sports, side-stepping or pivoting

8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 28/56
Hip pointer from direct blow to iliac crest
Main nerves about the hip
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 29/56
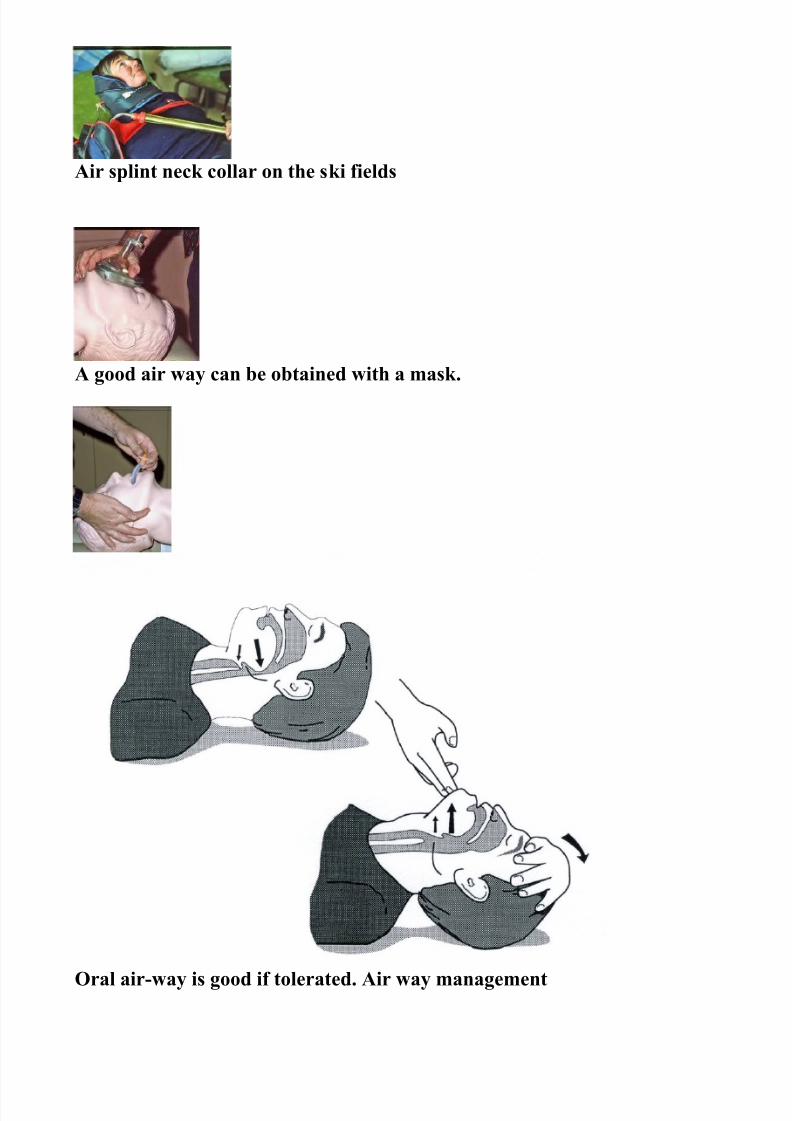
Air splint neck collar on the ski fields
A good air way can be obtained with a mask.
Oral air-way is good if tolerated. Air way management

8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 30/56
Removing helmet when neck suspected injured
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 31/56
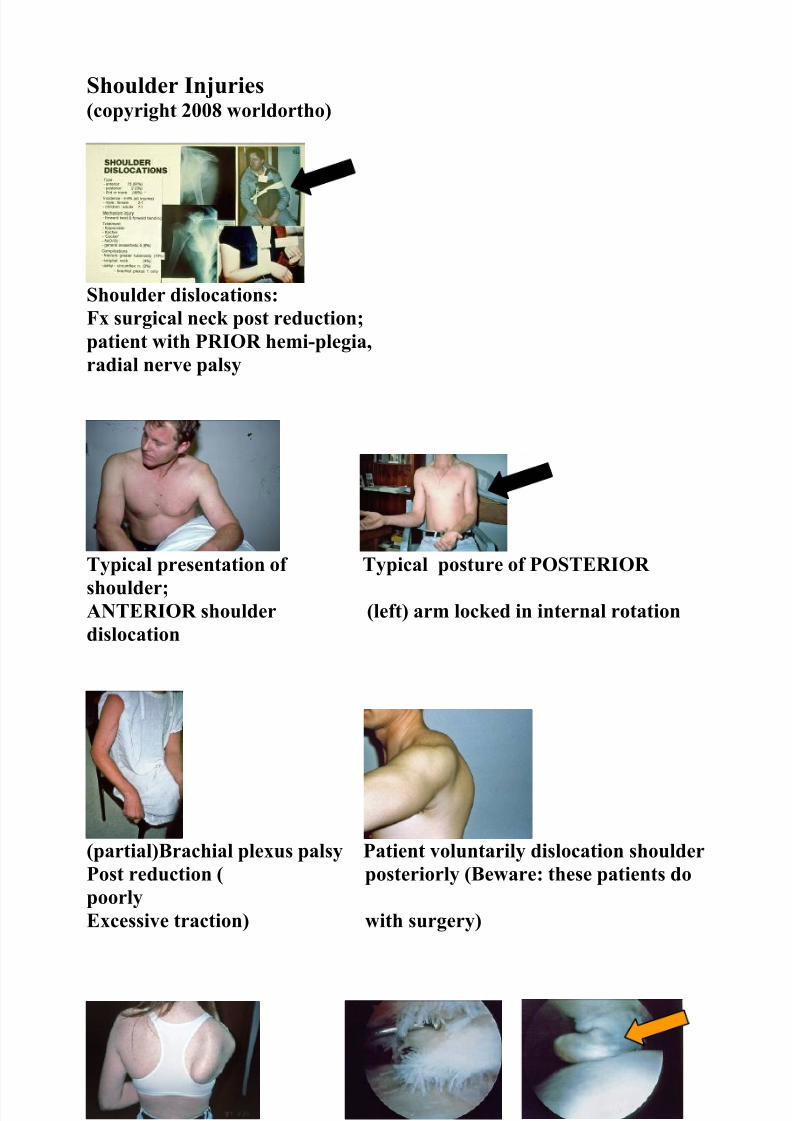
Shoulder Injuries(copyright 2008 worldortho)
Shoulder dislocations:Fx surgical neck post reduction;patient with PRIOR hemi-plegia,radial nerve palsy
Typical presentation of Typical posture of POSTERIOR
shoulder;ANTERIOR shoulder (left) arm locked in internal rotationdislocation
(partial)Brachial plexus palsy Patient voluntarily dislocation shoulderPost reduction ( posteriorly (Beware: these patients dopoorlyExcessive traction) with surgery)
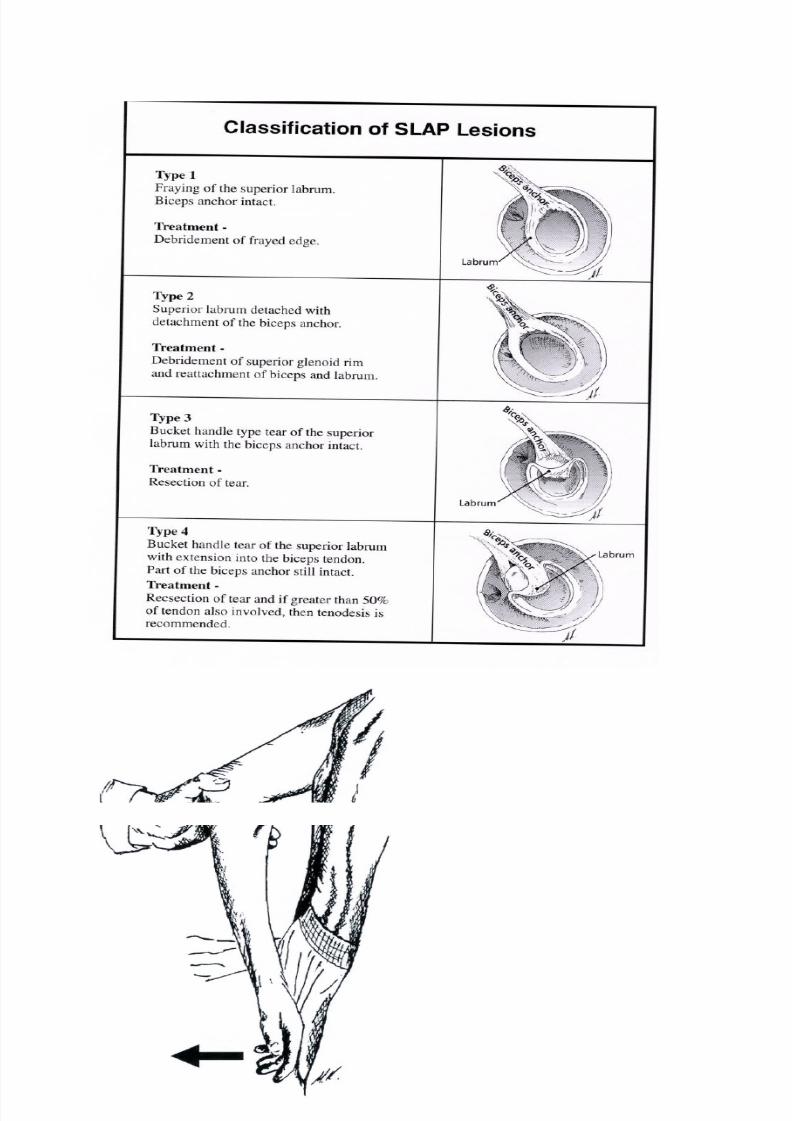
Winging of the scapula Rotator cuff tear SLAP lesion(see Fig.below)
Following shl dislocation(damage to long. th. N)
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 32/56
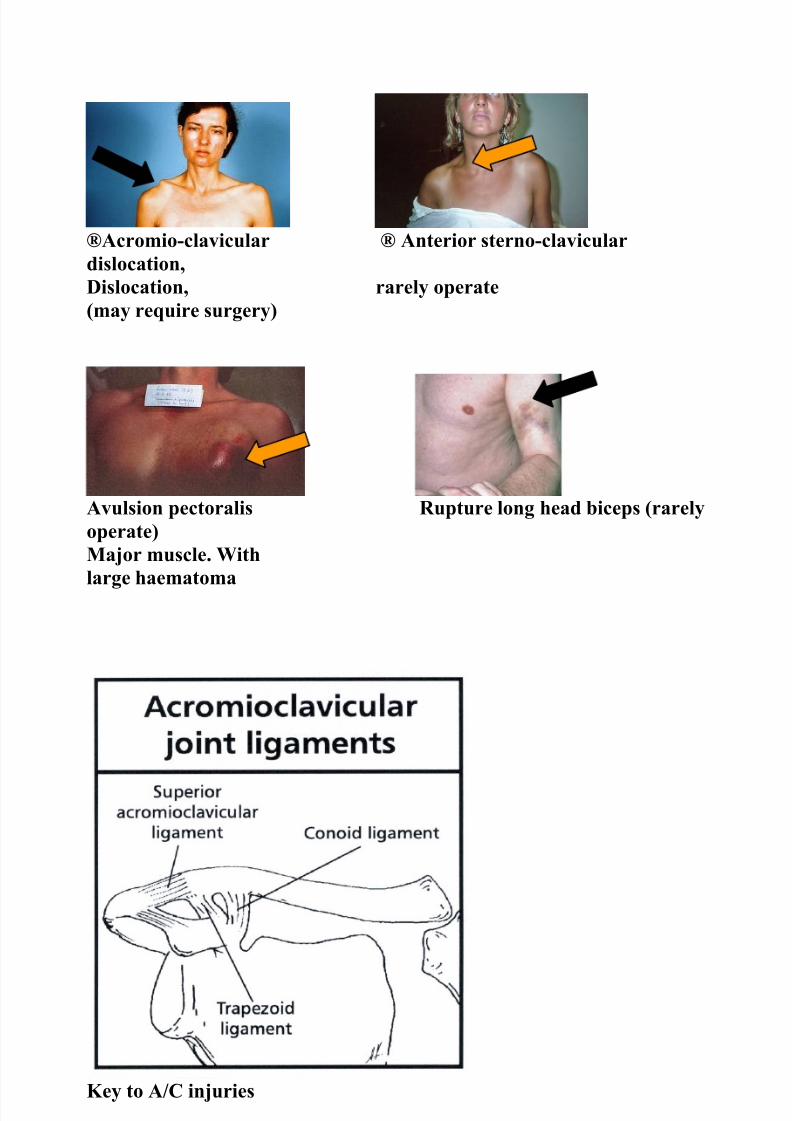
®Acromio-clavicular ® Anterior sterno-claviculardislocation,Dislocation, rarely operate(may require surgery)
Avulsion pectoralis Rupture long head biceps (rarelyoperate)Major muscle. Withlarge haematoma
Key to A/C injuries
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 33/56
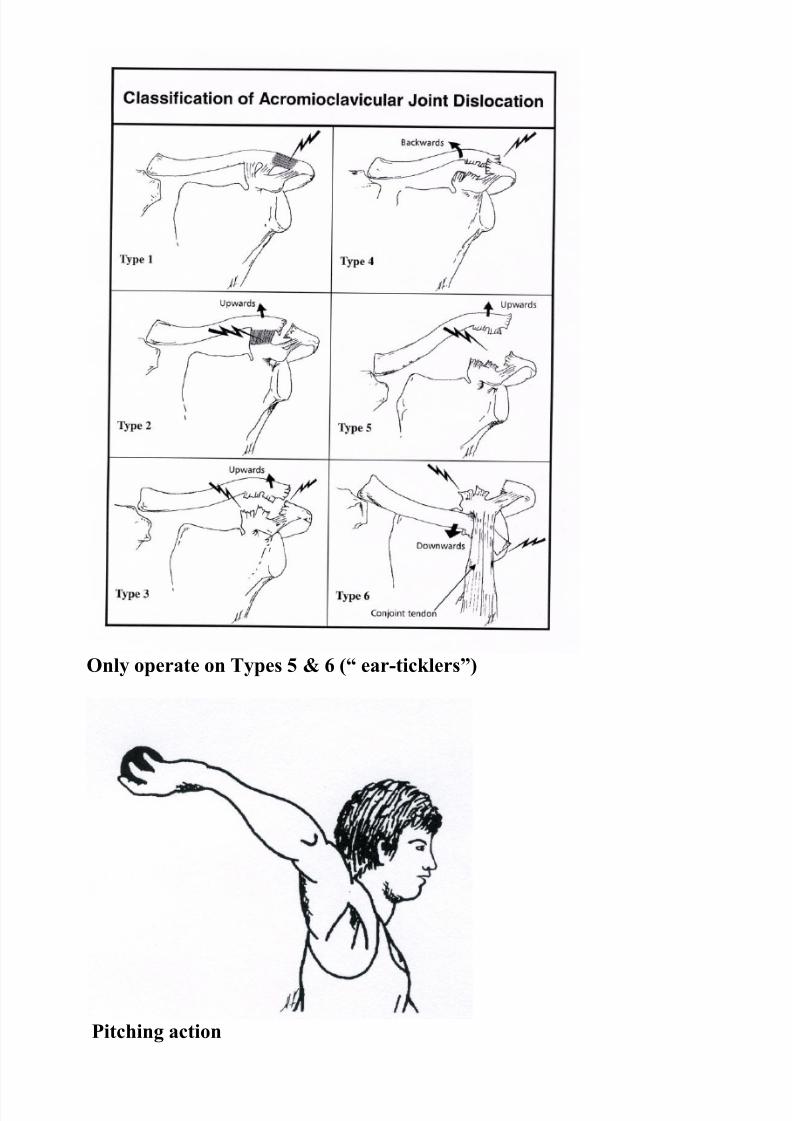
Only operate on Types 5 & 6 (“ ear-ticklers”)
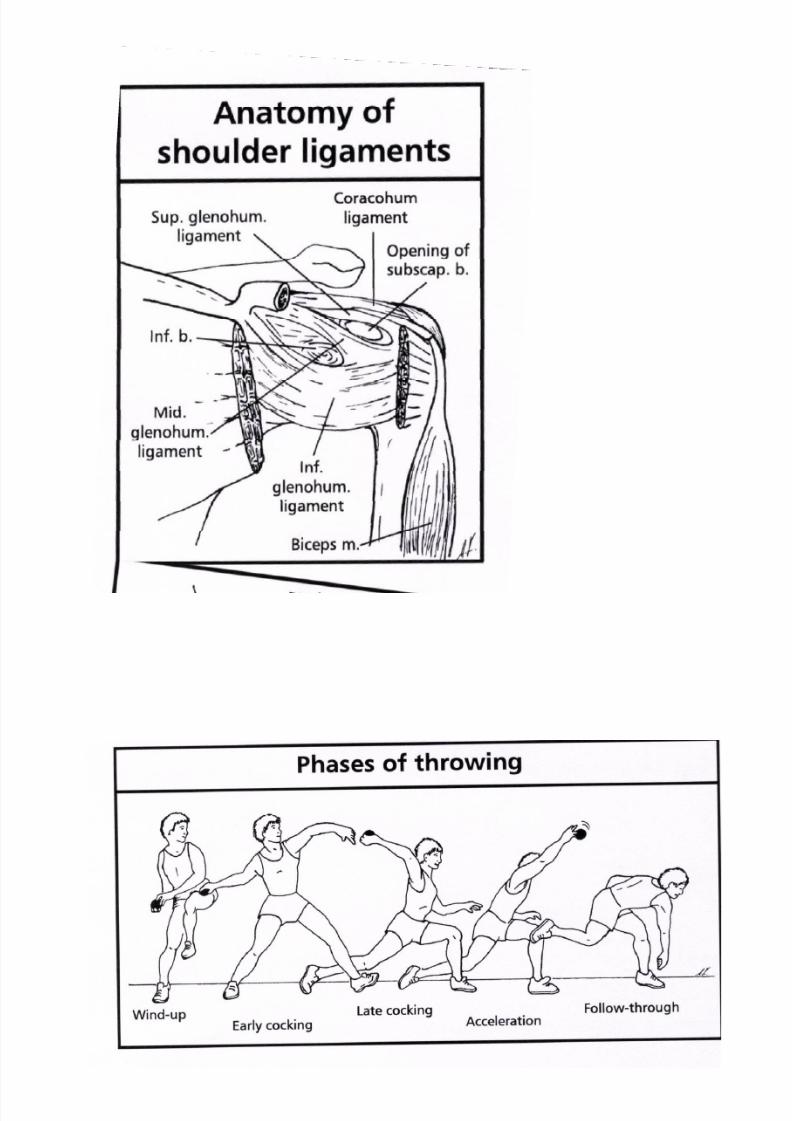
Pitching action
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 34/56
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 35/56
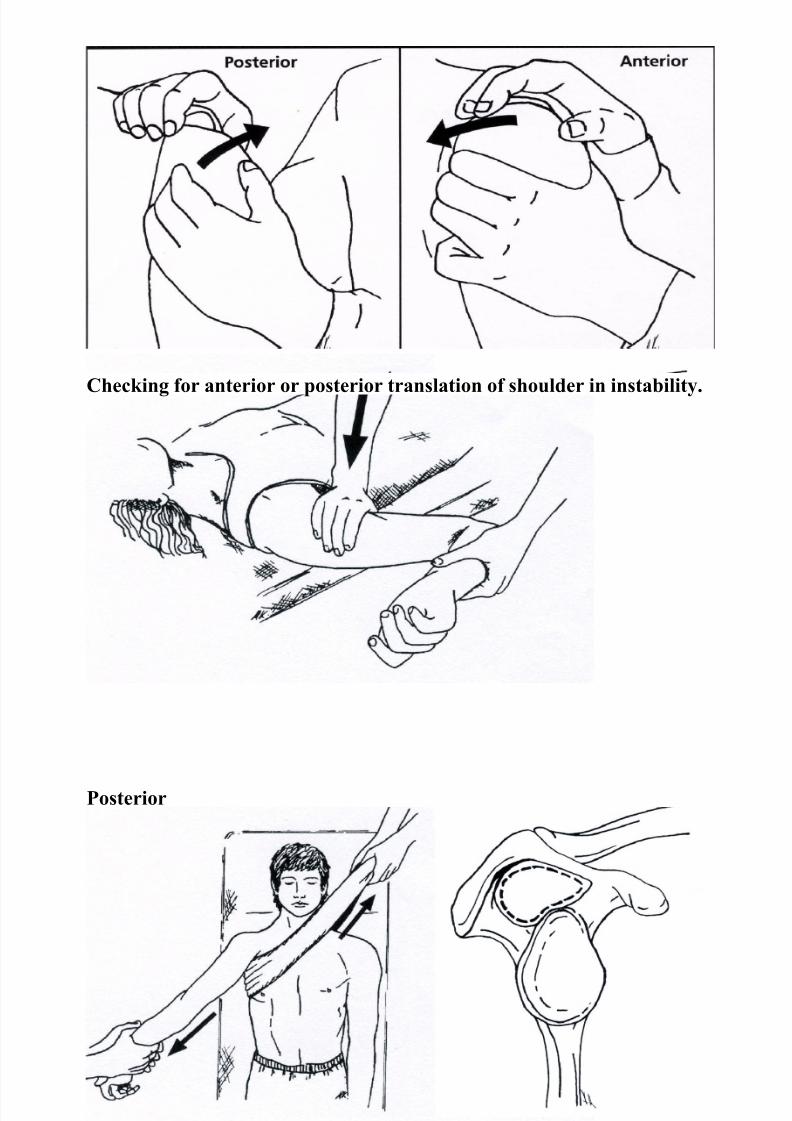
Checking for anterior or posterior translation of shoulder in instability.
Posterior
Hippocratic way to reduce shoulder Y-appearance of lateralscapula
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 36/56
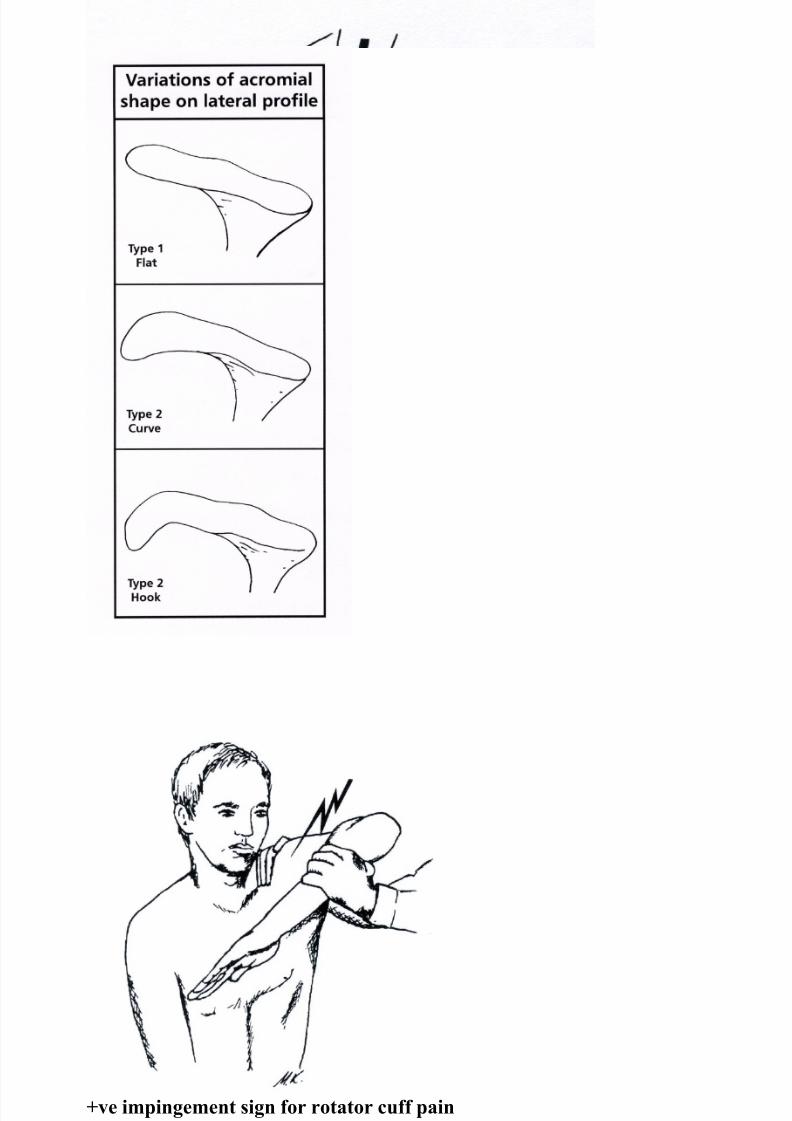
+ve impingement sign for rotator cuff pain
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 37/56
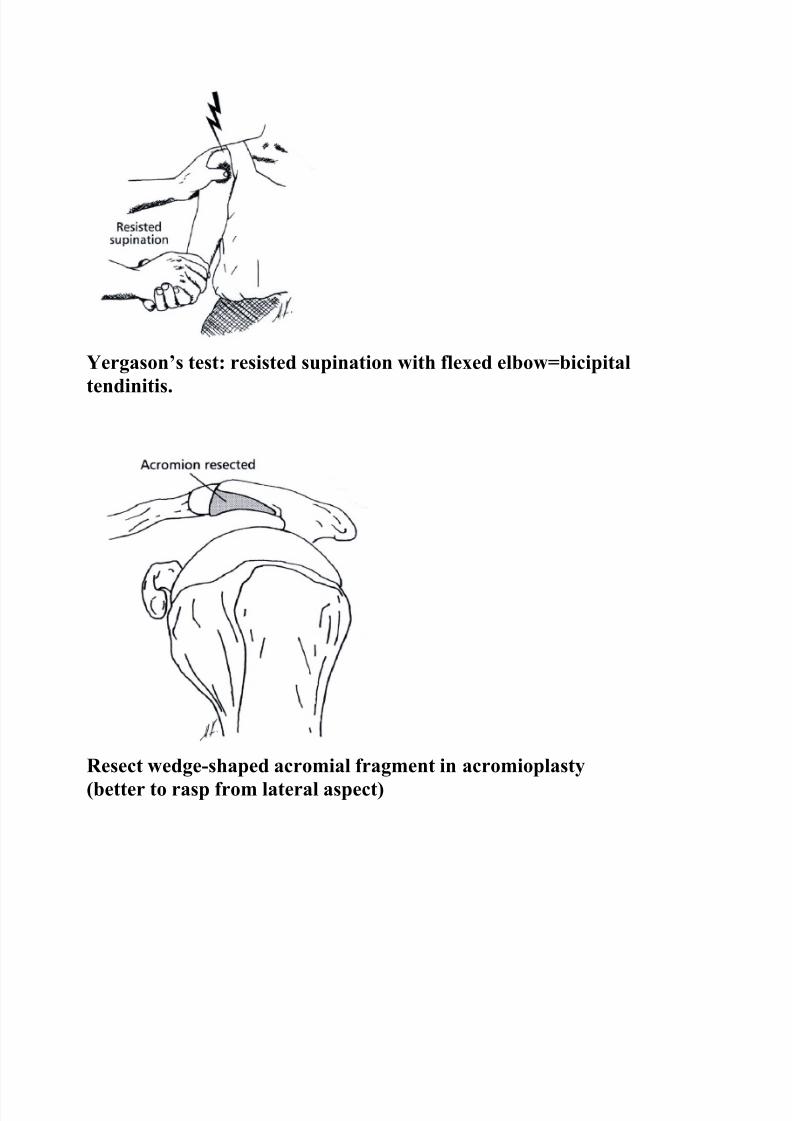
Yergason’s test: resisted supination with flexed elbow=bicipital
tendinitis.
Resect wedge-shaped acromial fragment in acromioplasty(better to rasp from lateral aspect)
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 38/56
Lift-off test for subscapularis pathology( pain/rupture)

8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 39/56

8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 40/56
SportHazards of the EnvironmentDrugs in Sport
(Copyright 2008 WorldOrtho)
Essential for safe scuba diving Gastric erosion at endoscopy
Death from decompression sickness. Barotrauma- telltalesign=blood in the there is gross oedema and rash. mask.
Training in a hypobaric chamber Mountaineers are prone toaltitude sickness for Everest from rapid ascent
Frostbite with gangrene Re-warming with inhalational technique

8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 41/56
Decompression sickness, DCS
Exercise-induced asthma, EIA.Office spirometry to diagnose.FEV1 and peak flow rate-a fall of >15% post-exercise confirms EIA.

8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 42/56
ECG: Athlete’s Heart (Sinus bradycardia, first degree AV block, tallQRSIn praecordial leads, Ts may be inverted).
Sites of possible blood loss and iron deficiency
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 43/56
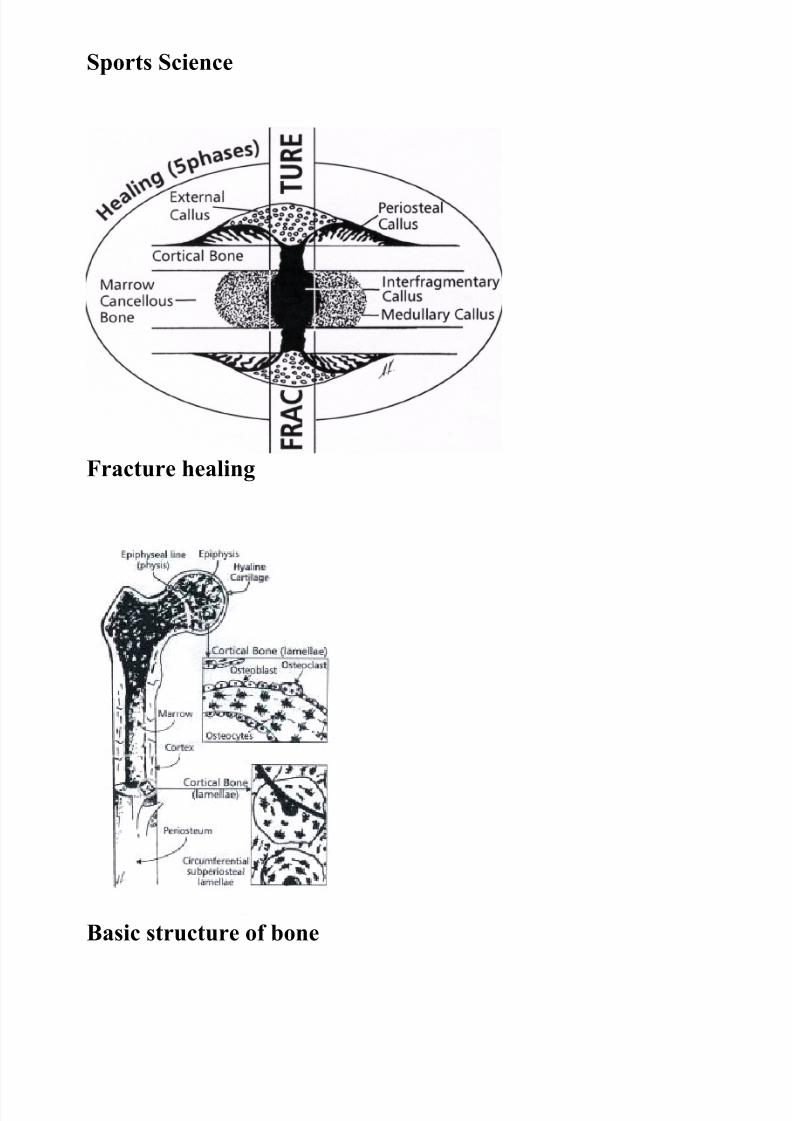
Sports Science
Fracture healing
Basic structure of bone
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 44/56
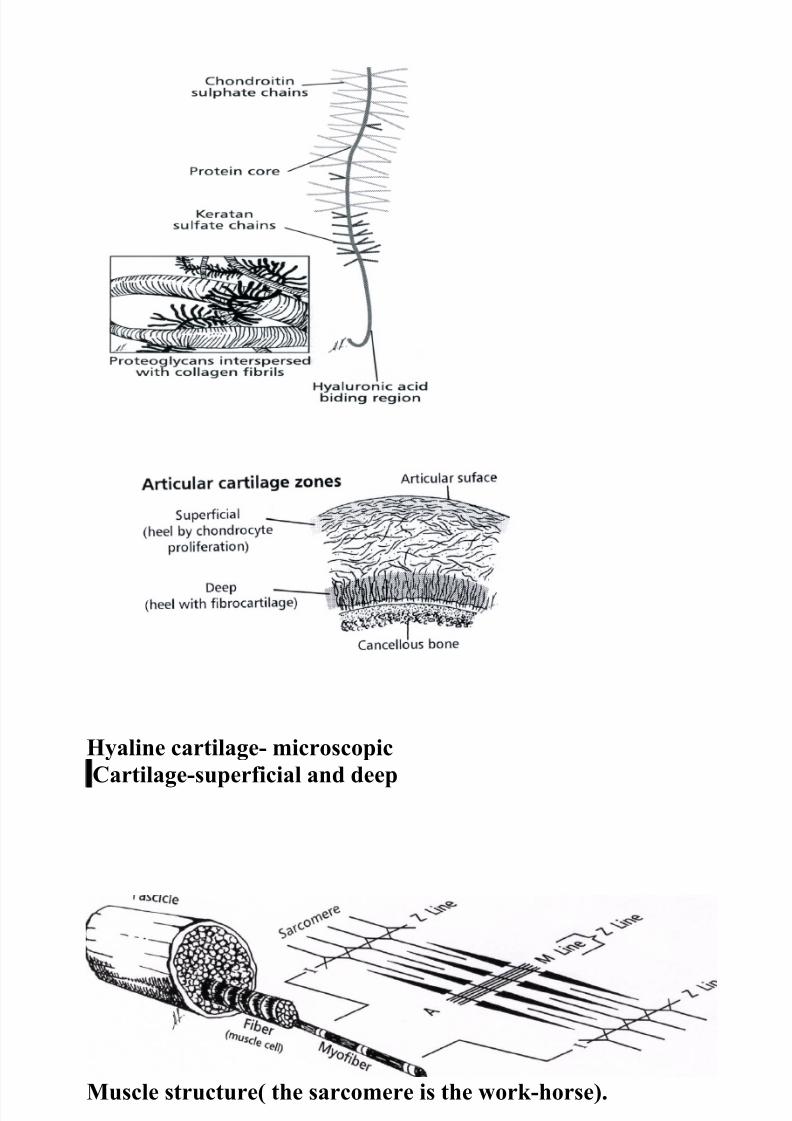
Hyaline cartilage- microscopicperfiial and deep
Cartilage-superficial and deep
Muscle structure( the sarcomere is the work-horse).

8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 45/56
Length-tension curve of muscle action
Peripheral nerves: sensory & motor
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 46/56
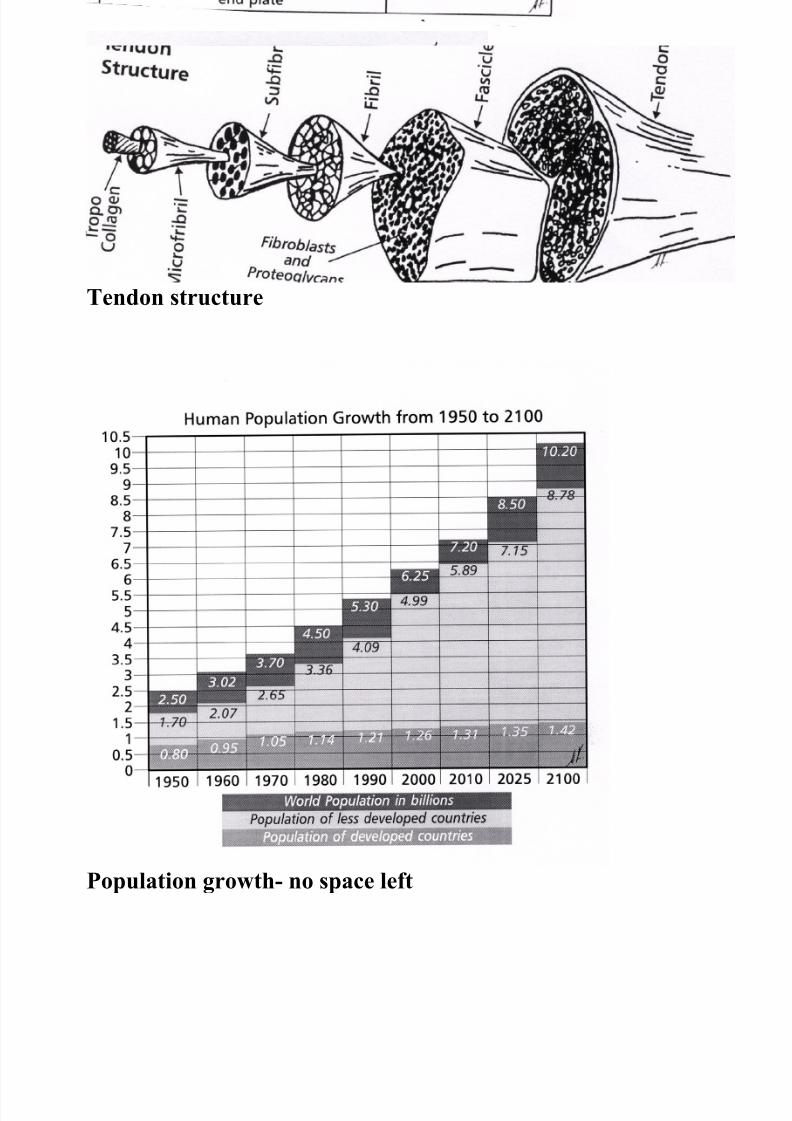
Tendon structure
Population growth- no space left

8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 47/56
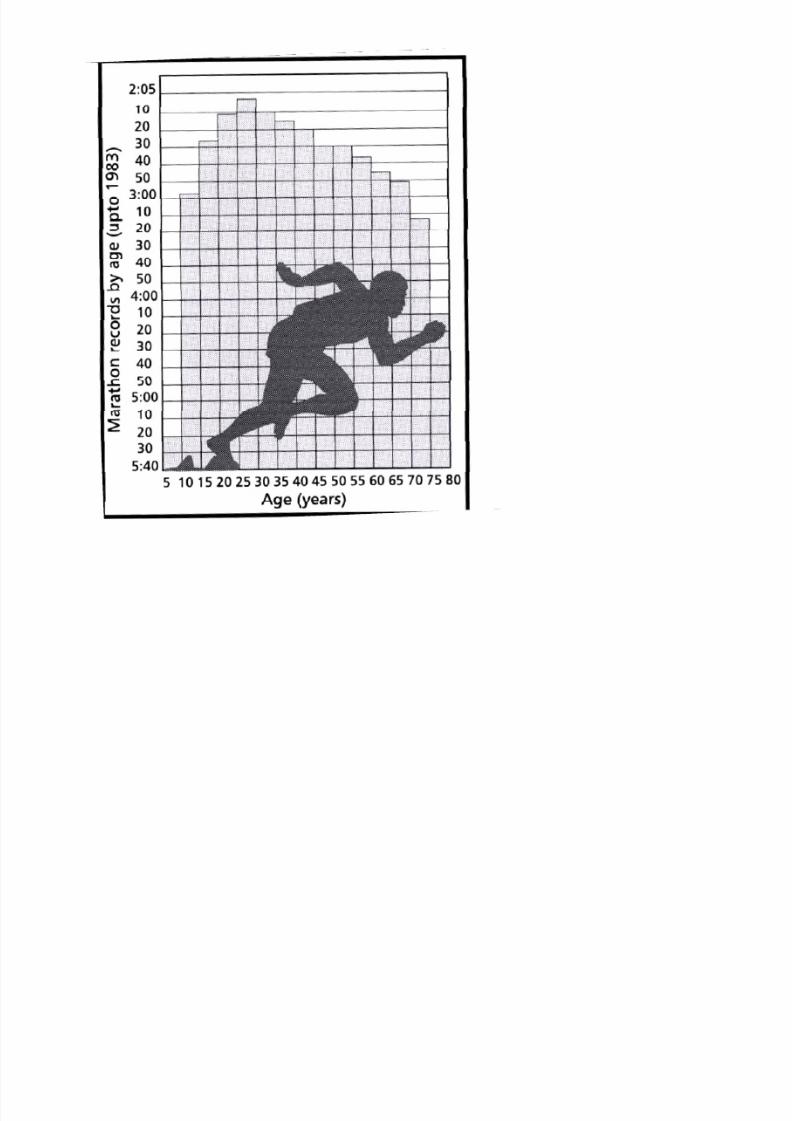
The Mature Athlete
Biking for active lifestyle
Bone density studies determine risk of fracture.
Osteoarthritis is more commonin elite athletes. EnduranceRunners and in power sports(here is a knee replacement).
Mature endurance athletes (e.g. X-country skiers) need more carbs &May dehydrate.

8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 48/56
Injuries of the Mature Athlete
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 49/56
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 50/56
The physically challenged Athlete
16yo skier with hemiparesis
( from MVA at age 5)
Sports Wheelchair design; critical at Olympic Competition

8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 51/56
Top Athletes
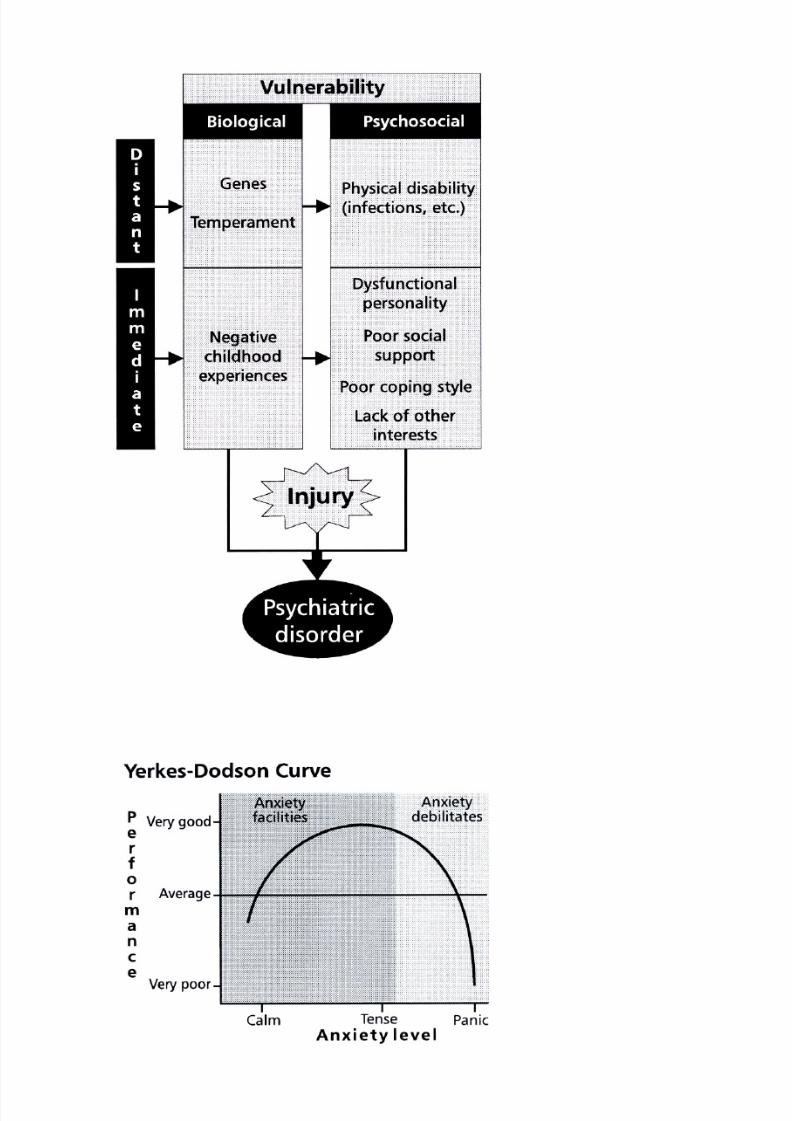
Dangerous attitudes can disrupt the safe return to sport
Leg press used early in rehab
Assessing gastroc tension
Assessing pelvic stability
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 52/56
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 53/56
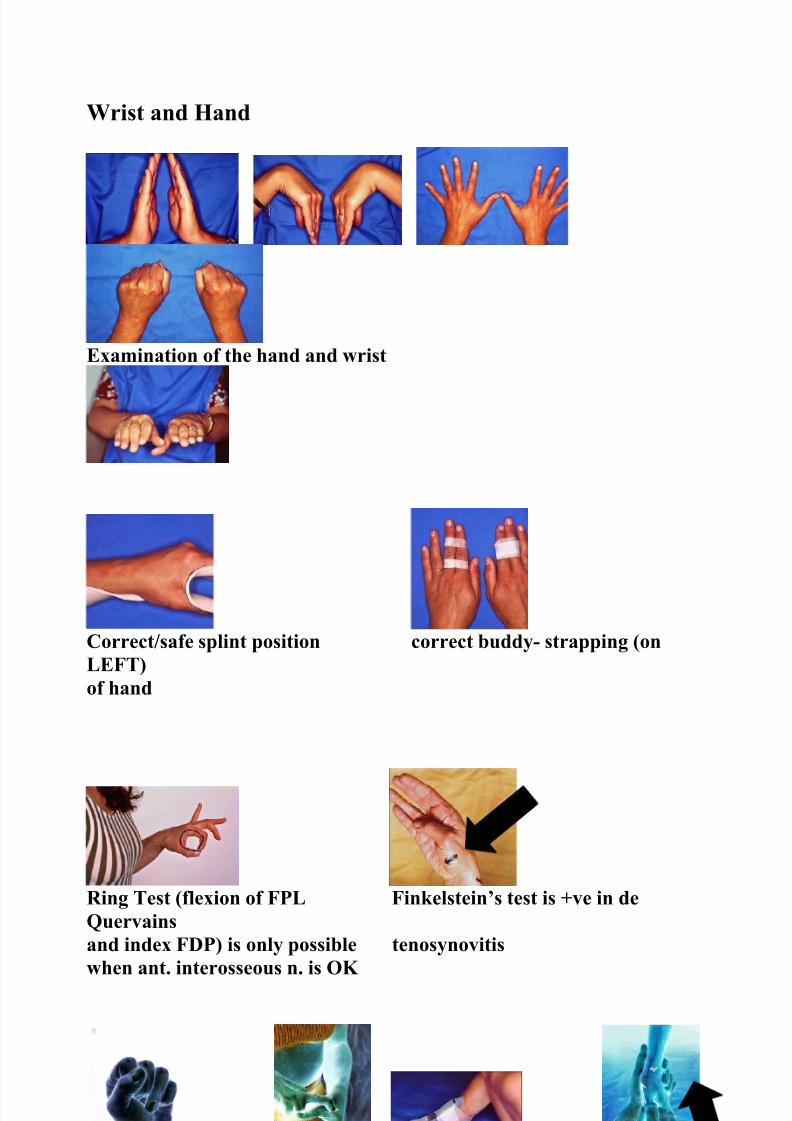
Wrist and Hand
Examination of the hand and wrist
Correct/safe splint position correct buddy- strapping (onLEFT)of hand
Ring Test (flexion of FPL Finkelstein’s test is +ve in deQuervainsand index FDP) is only possible tenosynovitiswhen ant. interosseous n. is OK
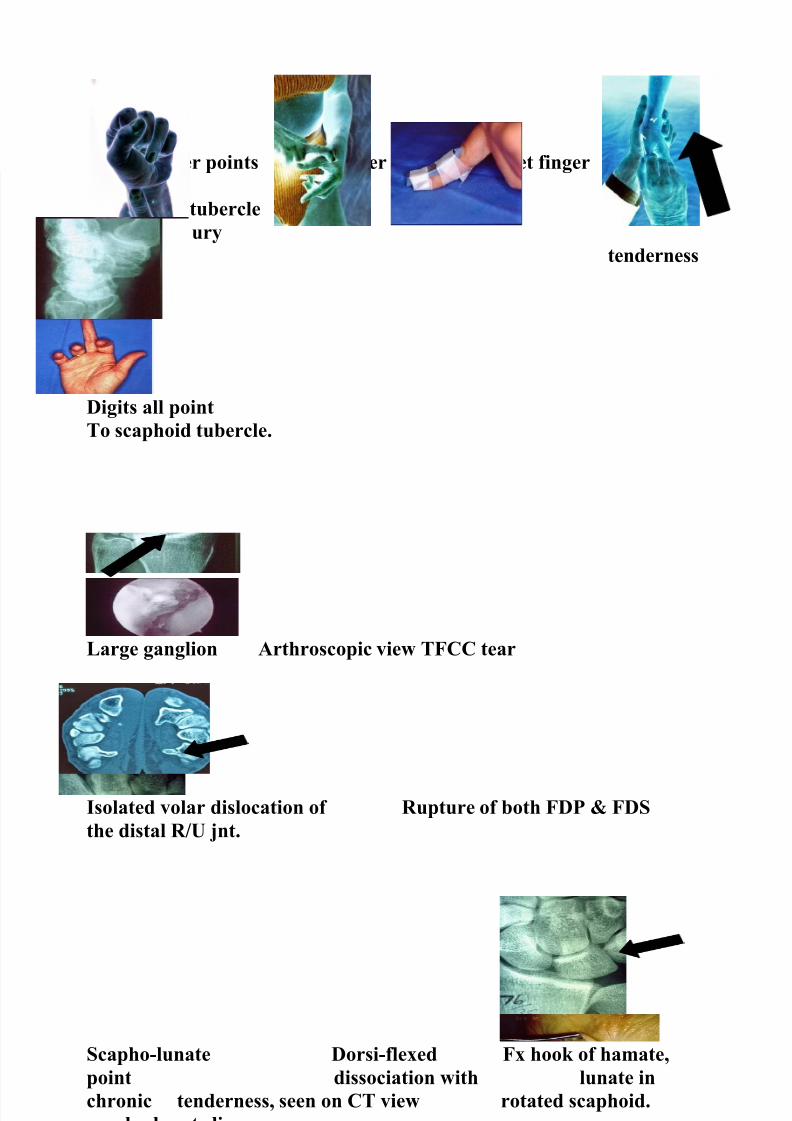
Flexed finger points Mallet finger Splint for mallet finger ScaphoidImpactionto scaphoid tubercle forscaphoid injury
tenderness
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 54/56
Digits all pointTo scaphoid tubercle.
Large ganglion Arthroscopic view TFCC tear
Isolated volar dislocation of Rupture of both FDP & FDSthe distal R/U jnt.
Scapho-lunate Dorsi-flexed Fx hook of hamate,point dissociation with lunate inchronic tenderness, seen on CT view rotated scaphoid.scapho-lunate lig.
Surface anatomy, with ref. Subtle step in line- up lunate&triquetrum
in mid-carpal instability.

8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 55/56
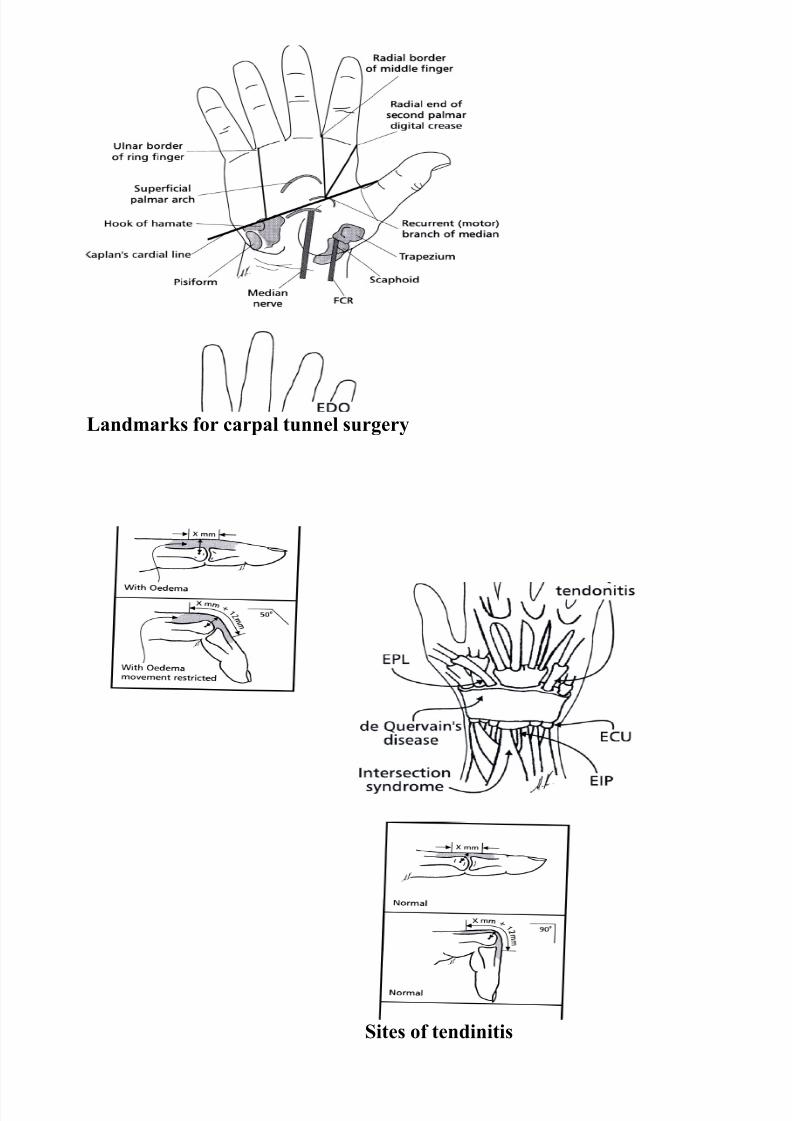
Landmarks for carpal tunnel surgery
Sites of tendinitis
8/7/2019 SYMPOSIUM Sporting Injuries. Clinical Care
http://slidepdf.com/reader/full/symposium-sporting-injuries-clinical-care 56/56





























