Embed Size (px)
Citation preview
SWL 579 A: Interdisciplinary Approaches to Prevention
Science
Week 6: Preventive Interventions in Week 6: Preventive Interventions in Pregnancy, Infancy and Early Pregnancy, Infancy and Early Childhood Childhood
Guest: Susan Spieker, Ph.D.Guest: Susan Spieker, Ph.D.
November 4, 2009November 4, 2009
Dimensions of Implementation Fidelity
Program Definition/ Description Program Definition/ Description (manuals, training and technical (manuals, training and technical support).support).
Adherence: Adherence: the degree to which the intervention the degree to which the intervention
process was implemented as the developer intendedprocess was implemented as the developer intended Dosage or exposure: Dosage or exposure: how much of the how much of the
complete program did the implementer deliver? complete program did the implementer deliver?
Quality: Quality: the degree to which the intervention was the degree to which the intervention was delivered competently, with enthusiasm, in an delivered competently, with enthusiasm, in an
engaging wayengaging way Participant responsiveness: Participant responsiveness: the degree to the degree to
which participants in an intervention are engaged or which participants in an intervention are engaged or involved in the intervention. involved in the intervention.
Assessing Preventive Interventions: Dimensions
What risk and protective factors are What risk and protective factors are addressed?addressed?
Describe the focal or targeted population.Describe the focal or targeted population. Describe the intervention.Describe the intervention. Describe the research design and Describe the research design and
methods. Are threats to internal validity methods. Are threats to internal validity adequately ruled out?adequately ruled out?
Describe the evidence of implementation.Describe the evidence of implementation. Describe the outcomes.Describe the outcomes.
Identifying Effective Programs: Identifying Effective Programs: CriteriaCriteria
• Does the program include those at risk for the problem to be prevented?
• Does the program target key risk and/or protective factors?
• Is the program model structured on a solid theoretical framework that guides each program component?
• Has the program been tested using an experimental design with randomized control group?
• Is there evidence of clinically significant outcomes with sustained effects?
• Is there evidence of a long term return on investment?• Is the model replicable?• Is the program developer committed to high quality
replication and available for consultation?

Nurse-Family Partnership
Program Goals
Positive Pregnancy
Outcomes
Improved Child Health
and Development
Parental Economic Self-
Sufficiency
Key Program Components
Serve low-income, first-time mothers Enroll as early in pregnancy as possible Voluntary for clients Home visitors are trained nurses Guideline-driven and family centered Visit from pregnancy through child age 2 Visit weekly to bi-weekly 100 family site with specific staffing Caseload of 25 families per full-time nurse CIS monitors program implementation
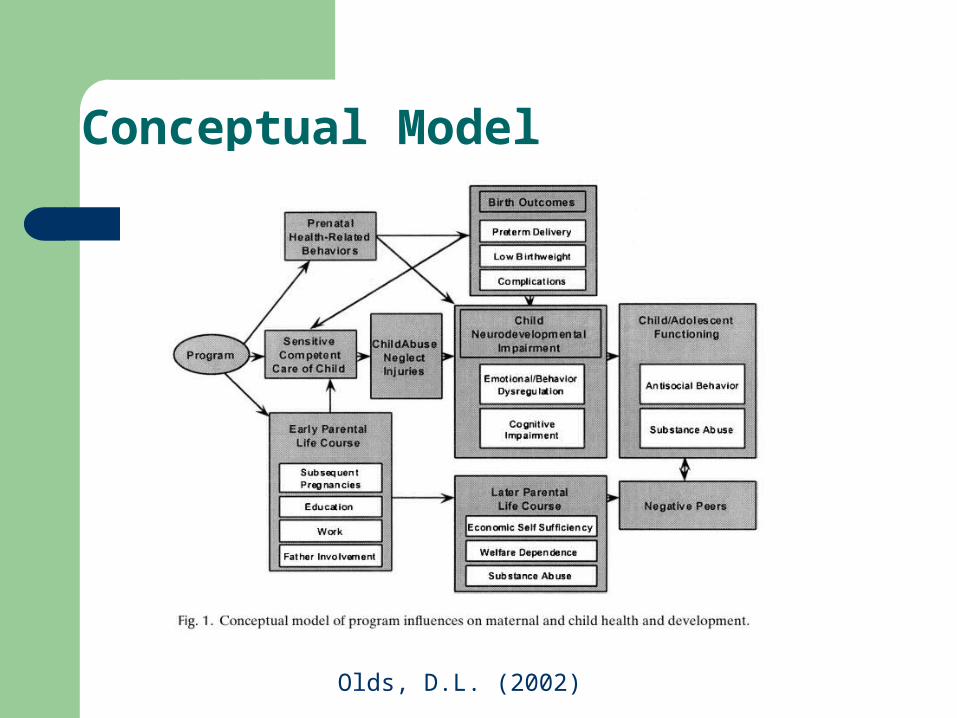
Conceptual Model
Olds, D.L. (2002)
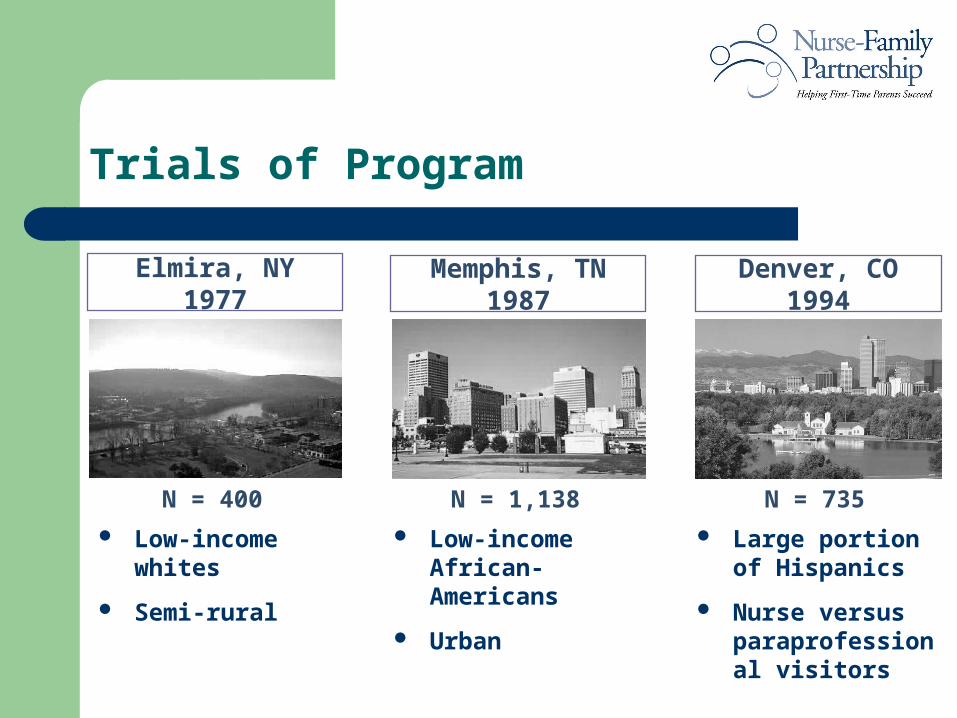
Trials of Program
Low-income whites
Semi-rural
Low-income African-Americans
Urban
Large portion of Hispanics
Nurse versus paraprofessional visitors
Elmira, NY1977
N = 400
Memphis, TN1987
N = 1,138
Denver, CO1994
N = 735
Evidence of Program Effects: Elmira Follow-up
48% reduction in child abuse and neglect 61% reduction in the arrest rate of the mothers and 75% fewer
convictions (for poor, unmarried women only) 59% reduction in the arrest rate of juveniles (for children of poor,
unmarried women only) 25% reduction in smoking during pregnancy (poor, unmarried) 44% reduction in problems associated with drug and alcohol abuse by
mothers (poor, unmarried women only) 2 year greater interval between first and second children (for poor,
unmarried women only) $2.88 to $1 return on investment (per Washington State Institute for Public
Policy, 2004 and RAND, 2005- looking at benefits to the whole sample)
Recognition: Awards
Model crime prevention program: United States Department of Justice
Model program for the prevention of severe behavioral problems among
teens: Report to President Bush by the President’s New Freedom
Commission
The Lela Rowland Prevention Award - National Mental Health Association
Recognition Award from the Office of Juvenile Justice and Delinquency
Prevention (OJJDP)
One of eleven national model “Blueprint” programs by the Office of Juvenile
Justice and Delinquency Prevention and the Center for the Study and
Prevention of Violence (2000)
Exemplary Substance Abuse Prevention Program Award from the Center for
Substance Abuse Prevention
Exemplary proven program – Surgeon General’s Report on Youth Violence
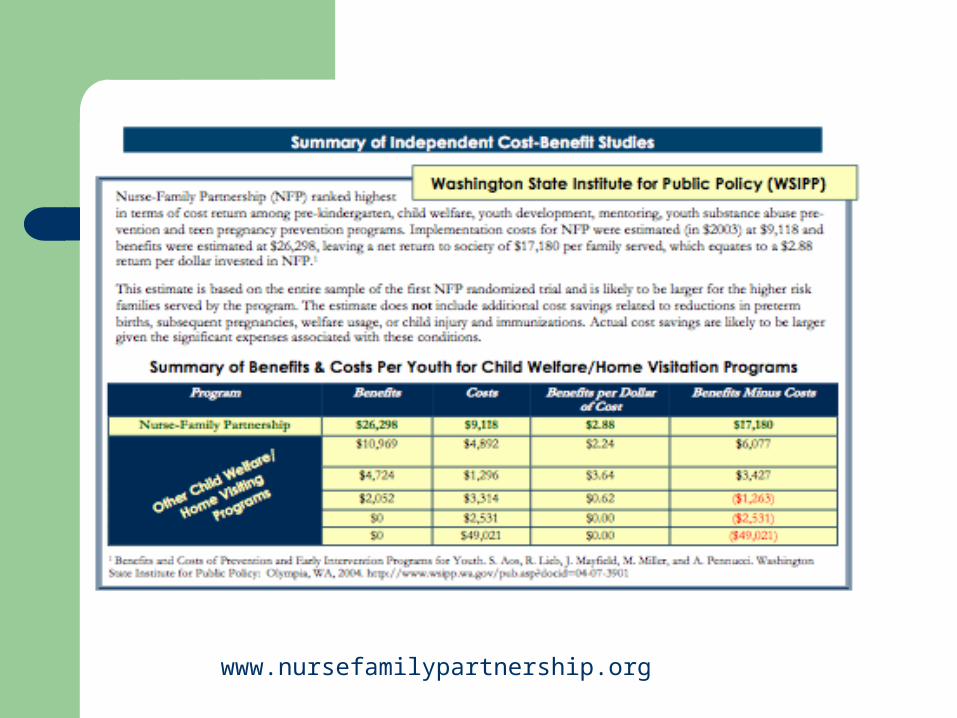
www.nursefamilypartnership.org
Translating Research into Practice
Example:
Colorado’s Invest In Kids statewide initiative.
O’Brien, R.A. (2005)
Invest in Kids
Improving the lives of Colorado’s children through advancing programs
that work
Mission
Invest in Kids partners with Colorado communities to improve the health and well-being of young children, particularly those of low-income families, through effective, research-based programs.
Strategy
1. Identify high quality, research-based programs
2. Facilitate implementation of programs in communities throughout Colorado
3. Promote sustainability of programs
Step One: IDENTIFY
Our Approach to Identifying Effective Programs
• Meet with local leaders throughout the state to ascertain where their greatest needs are for services
• Target search based on meeting the identified needs
• Focus on programs serving predominantly low-income children, ages 0-5, and their families
• Focus on programs that have been demonstrated, through rigorous research, to be effective and show cost savings
Questions for Program Developers re: Research
• Are there long range positive impacts?• Has the program been evaluated by an independent
researcher? • Has the research been published in a peer reviewed
journal? • Are you involved in ongoing research with the model? • Is the program culturally competent? Are there
different effects with different populations (e.g. age, gender, ethnicity, income, etc.)?
Questions for Program Developers re: Replication
• Do you have strategies to ensure successful replication?• Do you know which are the core components, what the
ideal dosage is and how to make adaptations in local communities?
• Do you have established:• training/TA• staffing guidelines• systems for ongoing evaluation• continuous improvement activities?
• What, if any obstacles, have there been to large scale implementation?

Step Two: Facilitate Implementation
Facilitate Implementation: Invest in Kids’ Role
• Planning • Funding • Training and Technical Assistance• Evaluation • Quality Improvement
Invest in Kids employs an intensive community based approach to replication.
We believe that broad-based community support and involvement are critical because:
• The programs are proscribed models that must be embraced by the community
• The involvement of diverse stakeholders leads to improved coordination and less duplication of services
• The involvement promotes long-term sustainability of the programs both through political support and through invested local leadership
Facilitate Implementation: Planning
We build (or work with existing) local community coalitions that:
• Assess the needs of their communities to decide whether and/or how these programs would complement the current services being provided
• Decide collaboratively which local agencies would be the best fit to actually implement the programs
• Help those implementing agencies coordinate this new program with the existing programs
• Help market the programs to encourage further involvement and community support (which can be financial or moral)
• Act as advisory boards to whom regular reports are given on the programs’ progress
Facilitate Implementation: Planning
Facilitate Implementation: Planning
Who are the “diverse stakeholders” we engage?
In most communities the players include:• Directors of Health Departments/nurses• Existing visitation and parenting program staff• Early childhood experts • Directors of Departments of Social Services• Potential referral sources and referral linkages• Representatives from the schools• Law enforcement• Members of the judicial system including local judges• State legislators and county commissioners• Lay community members – e.g. business leaders and philanthropists• Members of the faith community
Facilitate Implementation: Planning
Invest in Kids as Bridge between Research and Practice…
• Created step by step Community Guides for successful planning, implementation and sustainability of our programs
• Created Community Workplans and Agency Readiness Documents to assess fit of programs and readiness of agencies to implement them
• Treat the communities and implementing agencies as our “customers” so that we are their advocates with the program developers and their funders
Facilitate Implementation: Funding
Invest in Kids was instrumental in securing the following funding:
• State funding (tobacco dollars)
• Almost $300 million over 20 years ($10 million for FY 06-07)
• Federal funding (Medicaid match)
• $1.3 million this year
Invest in Kids set up the following structure: • Funding runs through Colorado’s state health department
• Competitive granting process – local health departments (and some other agencies) employ the nurses and provide the services
• Gradual ramp up
Facilitate Implementation: Training and Technical Assistance
• Training - Standardized training for all nurses throughout the country is provided by National Nurse-Family Partnership
• Technical Assistance and Ongoing Professional Development
• Through our technical assistance, Invest in Kids has identified gaps in nurses’ knowledge and skills, and filled those gaps by bringing on highly specialized experts to provide that additional support
• State meeting, regional meetings, newsletters, list serves, etc.
Facilitate Implementation: Evaluation and Quality Improvement
Although traditional evaluation and quality improvement strategies are not implemented until a program is up and running – it is critical that they are a part of the early planning and implementation processes.

Program Implementation to Date
Nurse-Family Partnership
Since its inception in 2000, the program has served over 6,000 families in 51 of Colorado’s 64 counties.
This year alone, it is serving nearly 2,200 families.
Statewide Outcomes (2004-05)
Program accomplishments for infants:
Immunization rates for NFP infantsare over 95% vs. state immunizationrate of 77%
A lower premature birth rate than Colorado rate (9.2% vs. 9.8%)
Only 9% of these highest risk children showed the potential for delayed language skills, according to the NFP’s language screening test
Statewide Outcomes (2004-05)
Program accomplishments for mothers:
20% reduction in cigarette smoking among NFP moms during pregnancy
Significant reductions in nearly every measure of family/domestic violence (physical, emotional and sexual)
41% of the clients who started the program without a high school diploma earned a diploma/GED by the time their babies were two years old, 17% were working toward their diploma/GED and 13% were enrolled in education beyond high school
Step Three: Sustain
Sustaining Model Programs: The Keys
Invest in Kids believes the keys to sustainability mirror the keys to successful implementation. Again, they are:
Planning Funding Training and Technical Assistance Evaluation Quality Improvement
Sustaining Model Programs: Planning
Once a program has been implemented – what planning is left?
Communities and local agencies must plan for:
• Growth• Capacity Building • Sustained agency and community support (e.g.
celebrations, press, etc.)
Sustaining Model Programs: Funding
What are the key strategies for funding?• Securing continued funding sources that match well with the program, as
designed • Continuing to recruit political and other community leaders who are willing
to fight for funding and for strict adherence to the program model• Continuing to enlist members of the community coalitions to lobby their
local legislators and encourage other funders to provide support• Raising the level of knowledge of community leaders and funders to
understand the importance and value of research based program • Advocating to have ineffective program sites (of your model programs)
closed down so you maintain your credibility and accountability to those funders and families
• Never assuming the funding will remain - constantly working to ensure it stays in place
Sustaining Model Programs: Training and Technical Assistance
What supports does a program site need post initial training to ensure sustainability?
• Ongoing support to service providers in the field• Flexibility to identify what the areas of need are and then hire experts
to provide that specialized training• Moral support • Ongoing training and professional development opportunities for staff
who’ve been trained• Additional trainings available and affordable for new staff in the
programs• Dissemination of lessons learned from other sites (e.g. state and
regional meetings, newsletters and list serves)• Acknowledgement and CELEBRATION!
Sustaining Model Programs: Ongoing Evaluation
Why is ongoing evaluation so important if we already know these programs “work?”
• Ongoing evaluation is critical for several reasons:• We know these programs are effective when implemented with fidelity• We also know there are differences between the research context and
the community context• We know that every community is unique and there are a lot of
pressures to adapt programs to meet those unique needs• We have seen that programs can be “watered down” in a matter of
weeks or months• We “buy” these programs based on their reported outcomes and need
to be able to report back on how effective they are in practice • MOST IMPORTANTLY…we want to be sure we’re getting good
outcomes for the children and families we all got into this business to support!
Sustaining Model Programs:Ongoing Quality Improvement
How do you do effective Quality Improvement work? We: • Use hard data from our evaluation• Use more subjective data from all of our technical assistance
providers and the front line workers
To:• Create site specific plans for quality improvement• Identify needs that are consistent across the state • Create strategies to address those state-wide issues• Connect sites so that they can mentor each other in areas of
strength • Take large issues back to program developers to encourage them
to develop national quality improvement initiatives
Potential Roles for Funders
Provide direct funding– Invest in evidence based programs– Invest in promising programs– Invest in other programs
Use your funding to leverage public dollars– The Colorado Trust’s investment in Invest in Kids
Use your clout and resources to convene communities
– The Gates Foundation -- Thrive by Five

For More Information:
Visit website:www.iik.org
Contact:
Jennifer AtlerExecutive DirectorInvest in Kids
303-839-1808 [email protected]
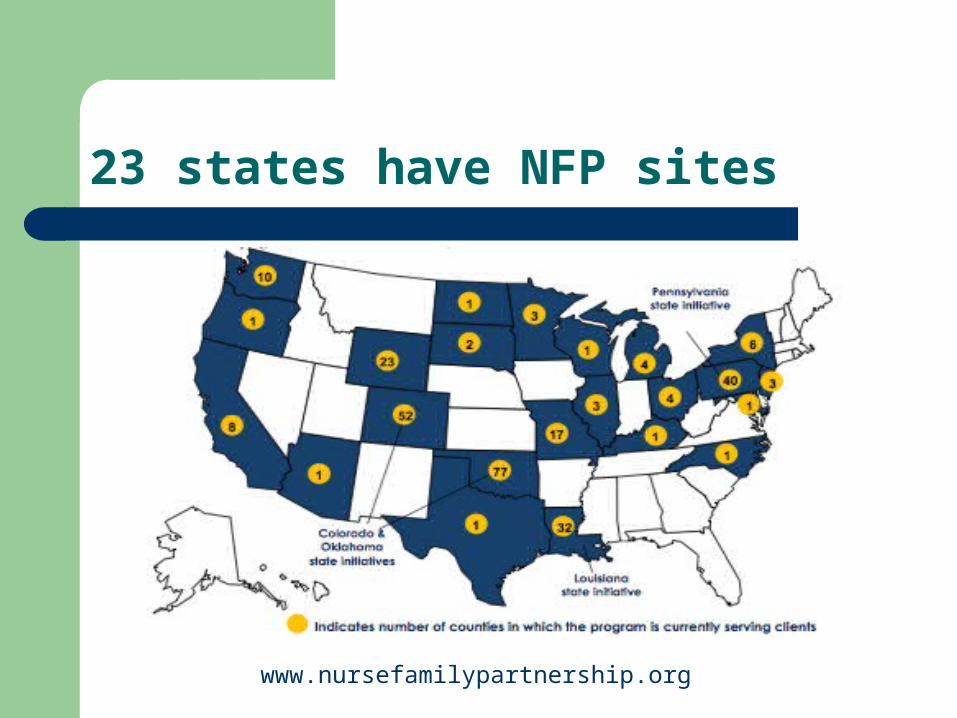
23 states have NFP sites
www.nursefamilypartnership.org
Translating Research into Practice
Replicated in 22 states, 260 counties, 5,000+ participants
Caseload per fulltime nurse= 25 families Visit-by-visit guidelines, adapted as necessary to
address individual needs Visit weekly during 1st mo., every other week through
pregnancy, weekly for 1st 6 weeks postpartum, & every other week until 21 mo. old
Overall, data from replication sites are promising, although effects are somewhat weaker than those observed in RCTs.
O’Brien, R.A. (2005)
Translating Research into Practice
The Federal FY 08 Omnibus Appropriations Act just signed into law includes the creation of a new $10 million evidence-based home visitation program at HHS, which is designed to provide seed money to scale up research-proven models such as the Nurse Family Partnership. The final Congressional language directs HHS to “ensure that States use the funds to support models that have been shown, in well-designed randomized controlled trials, to produce sizeable, sustained effects on important child outcomes such as abuse and neglect . . . [and] not to incorporate any additional initiatives that have not met these high evidentiary standards.”
Coalition for Evidence Based Policy
References
www.nursefamilypartnership.org O’Brien, R.A. (2005). Translating a research intervention into
community practice: The Nurse Family Partnership, The Journal of Primary Prevention, 26(3), 241-257.
Olds, D.L. (2002). Prenatal and infancy home visiting by nurses: From randomized trials to community replication. Prevention Science, 3(3), 153-172.
Atler, J. (2006). Invest in Kids: Implementing Nurse Family Partnerships in Colorado. Presentation to NW Grantmakers Forum, Seattle, WA. (September)