Embed Size (px)
Citation preview

CONTINUING EDUCATION
SWITCH for Safety: PerioperativeHand-off ToolsFAY JOHNSON, BSN, RN, CNOR; PATTY LOGSDON, MSN, RN, CNOR;
KIM FOURNIER, ADN, RN, CNOR; SANDRA FISHER, BS, RN, CNOR 2.3www.aorn.org/CE
Continuing Education Contact Hoursindicates that continuing education (CE) contact hours are
available for this activity. Earn the CE contact hours by
reading this article, reviewing the purpose/goal and objectives,
and completing the online Examination and Learner Evalua-
tion at http://www.aorn.org/CE. A score of 70% correct on the
examination is required for credit. Participants receive feed-
back on incorrect answers. Each applicant who successfully
completes this program can immediately print a certificate of
completion.
Event: #13532
Session: #0001
Fee: Members $13.80, Nonmembers $27.60
The CE contact hours for this article expire November 30,
2016. Pricing is subject to change.
Purpose/GoalTo provide knowledge specific to improving hand-off com-
munications during perioperative transfers of care from one
health care provider to another.
Objectives
1. Discuss the leading cause of reported sentinel events.
2. Identify barriers to communication.
3. Describe hand-off communications.
4. Identify standardized formats used for hand offs.
5. Discuss SWITCH tools used for perioperative hand offs.
AccreditationAORN is accredited as a provider of continuing nursing
education by the American Nurses Credentialing Center’s
Commission on Accreditation.
494 j AORN Journal � November 2013 Vol 98 No 5
ApprovalsThis program meets criteria for CNOR and CRNFA
recertification, as well as other CE requirements.
AORN is provider-approved by the California Board of
Registered Nursing, Provider Number CEP 13019. Check
with your state board of nursing for acceptance of this activity
for relicensure.
Conflict of Interest DisclosuresMs Johnson, Ms Logsdon, Ms Fournier, and Ms Fisher
have no declared affiliations that could be perceived as
posing potential conflicts of interest in the publication of
this article.
The behavioral objectives for this program were created
by Rebecca Holm, MSN, RN, CNOR, clinical editor, with
consultation from Susan Bakewell, MS, RN-BC, director,
Perioperative Education. Ms Holm and Ms Bakewell have
no declared affiliations that could be perceived as posing
potential conflicts of interest in the publication of this
article.
Sponsorship or Commercial SupportNo sponsorship or commercial support was received for this
article.
DisclaimerAORN recognizes these activities as CE for RNs. This rec-
ognition does not imply that AORN or the American Nurses
Credentialing Center approves or endorses products mentioned
in the activity.
http://dx.doi.org/10.1016/j.aorn.2013.08.016
� AORN, Inc, 2013

SWITCH for Safe
ty: PerioperativeHand-off ToolsFAY JOHNSON, BSN, RN, CNOR; PATTY LOGSDON, MSN, RN, CNOR;KIM FOURNIER, ADN, RN, CNOR; SANDRA FISHER, BS, RN, CNOR 2.3www.aorn.org/CE
ABSTRACT
Communication breakdown is the leading cause of reported sentinel events in the
perioperative setting. Barriers to optimal communication include noise, stress,
multitasking, and rapid turnover between procedures. AORN has identified commu-
nication during personnel changes (ie, hand offs) as a point of vulnerability for the
surgical patient. A standardized hand-off method provides an opportunity for
personnel to ask and answer questions and should be available in the perioperative
setting. At one facility, the standardization of hand-off reporting resulted in the
development of new hand-off tools specific to the perioperative environment. A
standardized reporting method enabled health care providers to address commu-
nication barriers and to maintain their focus on the patient during critical moments
(eg, shift changes), thereby improving patient safety. AORN J 98 (November 2013)
495-504. � AORN, Inc, 2013. http://dx.doi.org/10.1016/j.aorn.2013.08.016
Key words: communication tools, communication breakdown, hand-off tools, hand-
off reports, patient safety, hand-off communication.
Communication of essential information
during the transfer of patient care from
one perioperative care provider to another
is critical to patient safety and continuity of care.
The leading cause of reported sentinel events in the
OR is communication breakdown.1,2 “A sentinel
event is an unexpected occurrence involving death
or serious physical or psychological injury, or the
risk thereof. Serious injury specifically includes
loss of limb or function. . . . Such events are called
‘sentinel’ because they signal the need for imme-
diate investigation and response.”3 Barriers to
concise communication include noise, information
overload, inattention, stress, multitasking, and
time pressures caused by rapid turnover between
procedures.4 More than 3,000 sentinel events
http://dx.doi.org/10.1016/j.aorn.2013.08.016
� AORN, Inc, 2013
analyzed from 1995 to 2004 revealed that 65% of
reported problems were caused by poor communi-
cation.5 In 2005, that percentage increased to 70%,
of which half of reported events occurred during
the hand-off communication period.5 Communi-
cation during personnel changes is a point of
vulnerability during which incorrect information
can be conveyed or crucial information omitted,
leading to medical error. Hand offs are the most
common health care transaction prone to error.6
In 2006, The Joint Commission published
National Patient Safety Goal 2E. The purpose of
this safety goal was to guide providers in imple-
menting a standardized approach to hand-off
communications, including ensuring that they have
an opportunity to ask and respond to questions.5
November 2013 Vol 98 No 5 � AORN Journal j 495

November 2013 Vol 98 No 5 JOHNSON ET AL
In an effort to deal with communication failures,
The Joint Commission revised and expanded that
safety goal in 2008 to require the following:
1. Interactive communications allowing for the
opportunity for questioning between the giver
and the receiver of patient information.
2. Up-to-date information regarding the patient’s
care, treatment, services, condition, and any
recent or anticipated changes.
3. A process for verification of the received in-
formation, including the use of repeat-back and
read-back, as appropriate.
4. An opportunity for the receiver of the handoff
information to review relevant patient histor-
ical data, which may include previous care,
treatment, and services.
5. Interruptions during handoffs are limited to
minimize the possibility that information would
fail to be conveyed or would be forgotten.7
Health care facility management personnel should
develop and implement a process to comply with
this safety goal.5
HAND-OFF COMMUNICATION
The terms hand-off, handover, sign-over, and shift
report are synonymous. A “hand off” may be de-
scribed as the transfer of patient information, along
with the authority and responsibility to care for that
patient, from one health care provider to another
during the transfer of care.8,9 For example, a hand
off in the OR may be from one RN circulator to
another RN circulator or from one scrub person to
another scrub person. The “hand-off communica-
tion report must be complete, concise, concrete,
clear, and accurate.”4(p5) All team members in-
volved should have the opportunity to ask ques-
tions, respond to questions, and discuss patient care
provided by the previous clinician and care that
will be required by the next clinician. Standardized
hand-off systems and techniques are widely avail-
able and include the following formats:
n SBAR: situation, background, assessment,
recommendation;
496 j AORN Journal
n I PASS the BATON: introduction, patient,
assessment, situation, safety concerns, (the)
background, actions, timing, ownership, next;
n SHARQ: situation, history, assessment, recom-
mendations, questions;
n Five Ps: patient, plan, purpose of plan, problem,
precaution; and
n Five Ps, second version: patient, precautions,
plan of care, problems, purpose.10,11
Although these hand-off methods help to ensure
clear and complete hand-off communication, none
are specific to the needs in the perioperative
environment.
SETTING
As a result of a 2010 safety survey, members
of the Surgical Services Partnership Council at
Providence St Vincent Medical Center, Portland,
Oregon, learned of perioperative nurses’ concerns
regarding inconsistencies in hand-off reporting.
Although the SBAR method was used for hand-off
communications throughout the hospital, it did
not address specific and critical information that
needed to be relayed during the intraoperative hand
off. The result was inconsistent use of SBAR by
health care providers or personnel performing their
own version of SBAR. Critical information related
to surgical patientsdsuch as totals of medications
administered, instruments off the sterile field, and
details about specimens or countsdoften may not
be communicated for various reasons (eg, distrac-
tions, need for rapid room turnover). Such incon-
sistency was creating a patient safety issue.
In response to these concerns and after review-
ing resources about hand-off communication for
guidance,11,12 council members decided that
a standardized hand-off tool designed specifically
for the OR was needed. Council members then
identified barriers to effective communication at
the facility, which included the following:
n the lack of an established process or written
script for hand offs;

PERIOPERATIVE HAND-OFF TOOLS www.aornjournal.org
n reports given verbally (ie, no written report
template), which forced individuals to rely on
memory alone;
n personnel breaks taken without team members
performing a thorough hand-off report;
n noise distractions (eg, music playing, back-
ground conversations, equipment noise);
n personnel who multitasked (eg, completing
documentation, performing the surgical prep,
positioning the patient) during the hand off;
n personnel feeling pressured to perform rapid
turnovers between procedures;
n the inconvenient timing of the hand off in re-
lation to the status of the procedure (eg, a hand
off occurring during the beginning or end of the
procedure or at a critical point in the procedure,
such as during positioning or counting); and
n the facility’s recent conversion to electronic
charting and the subsequent increase in charting
demands, which affected the intraoperative
workflow.
Relying on memory, being distracted by noise
and other activities, and adjusting to new work-
flows all interfered with accurate reporting. In
addition, the preceding items indicated that per-
sonnel at our facility were encountering several
barriers to optimal communication, namely not
having a standardized hand-off approach or accu-
racy in reporting, followed closely by a lack of
completeness and clarity during the information
exchange. Given the perioperative team members’
variety of experiences, training, and backgrounds,
council members decided that a standardization
tool was necessary to improve processes and ensure
patient safety.
After careful assessment of safety concerns and
the identified barriers to hand-off communication,
the council decided to develop and implement its
own scripted solution. This resulted in SWITCH
(Figure 1), a new hand-off tool for improved
communication. The acronym SWITCH stands for
n surgical procedure,
n wet (ie, fluids),
n instruments,
n tissue (ie, specimen),
n counts, and
n have you any questions?
Each of the SWITCH acronym categories permitted
additional subcategories, such as medications in the
wet category, to allow perioperative team members
to adequately address communication specific to
their various roles and hand-off needs. Similar to
other communication techniques, SWITCH is easy
to remember because, as an acronym, it spells
a word that conveys the critical activities that occur
when personnel care for the patient. Unlike other
communication techniques, however, the SWITCH
tool is geared toward the specialized needs of the
perioperative environment. The council’s goal in
developing the SWITCH tool was to standardize
the hand-off reporting process and to ensure that
a face-to-face hand off occurred between outgoing
and incoming personnel.
ROLLOUT
In preparation for implementing the SWITCH tool,
the council considered how difficult change can
be for individuals. An individual’s resistance to
change can be attributed to factors such as habits,
complacency, disorganization, perceived loss of
power, and not understanding the need for change.13
To alleviate the potential for any resistance to
change, council members made sure that all
personnel were aware of the need for and the
reasoning behind the change. This occurred during
several inservice meetings led by council members.
Input received from perioperative personnel during
these inservice meetings guided council members in
the development of the SWITCH tool and was es-
pecially helpful in delineating subcategories. An
early paper version of the tool was tested by peri-
operative personnel for several weeks, and feedback
that council members received on the written layout
and content was taken into consideration before
rollout of the final version.
The official rollout of SWITCH began with
council members educating personnel about the
AORN Journal j 497

SWITCH for OR Hand Off
S Surgical procedure
□ Diagnosis □ Stage of procedure (ie, beginning, middle, end) □ Specific patient concerns (eg, allergies, implants, health status) □ Imaging needed (eg, x-ray) □ Incision type/dressings needed □ Plan for postoperative patient disposition □ Procedure to follow
W Wet (ie, fluids)
□ Medications on the sterile field (ie, type, amount) □ Irrigation (ie, type, amount) □ Blood loss and blood products available □ Urine out □ Drains
I Instruments
□ Need to reprocess instruments for to-follow cases □ Instruments on hold □ Implants needed
T Tissue (ie, specimen)
□ Specimen (ie, name, source of specimen) □ Grafts (ie, type, source of graft, location of graft [eg, specimen refrigerator, dry storage
cabinet]) □ Type of laboratory procedure (eg, frozen, touch prep)
C Counts
□ Sponges, needles, sharps, and instruments □ Items off the sterile field or in body cavities
H Have you any questions?
□ Status of charting?
Figure 1. Initial use of the new SWITCH tool was for the hand off between two RN circulators or scrub person toscrub person. Modified and used with permission from Providence St Vincent Medical Center, Portland, OR.
November 2013 Vol 98 No 5 JOHNSON ET AL
new tool. During mandatory inservice programs for
personnel from each shift, council members re-
viewed the reasons for changing hand-off reporting
and presented the SWITCH tool itself. Next, peri-
operative personnel participated in role-playing
exercises and an activity of matching hand-off
information to the correct SWITCH category. All
personnel, including those who were not able to
attend, were assigned an electronic learning module
498 j AORN Journal
that council members created to orient personnel to
and further educate them about SWITCH.
To promote awareness and aid in retention
during the rollout, council members distributed
paper SWITCH forms to each of the ORs in the
facility. These forms used bullet points to illustrate
each category of the hand-off tool. Laminated
forms also were available at the RN circulators’
computer work station, to be used with a dry-erase
PERIOPERATIVE HAND-OFF TOOLS www.aornjournal.org
marker for written hand-off reporting. This lam-
inated form allowed the RN circulator to write key
notes that would prepare him or her to give a hand-
off report efficiently and remember critical patient
information. Another large laminated SWITCH
tool was placed on the wall near the scrub person’s
back table. It permitted the scrub personnel to easily
read the form and to give his or her hand off in a
standardized fashion. Council members also dis-
tributed smaller versions of the laminated cards to
team members to wear behind their name tags.
The SWITCH tool provided personnel a frame-
work with which to improve their hand-off skills
and prevent communication errors. For example,
during a hand off for a patient who is undergoing
a right mastectomy with a sentinel node biopsy and
breast reconstruction with placement of a tissue
expander, the hand-off report between two RN
circulators when one is leaving for a break
(Figure 2) would include the following:
n S: surgerydright mastectomy, sentinel node
biopsy, reconstruction with tissue expander
Figure 2. Two RN circulators perform a SWITCH hand off
placement; patient is allergic to penicillin;
patient will be transferred to the postanesthesia
care unit (PACU) after surgery
n W: wetd0.25% bupivacaine plain (30 mL),
50,000 units of bacitracin diluted in 1,000 mL
of 0.9% sodium chloride irrigation solution, two
15-Fr closed collapsible drains opened on sterile
field
n I: instrumentsdusing the two trays of mastec-
tomy instruments; tissue expanders available
in room
n T: tissuedone specimen: right breast to be sent
to pathology for permanent section and two
sentinel nodes sent to pathology for touch prep
n C: countsdverify count board: 20 laparotomy
sponges, 12 suture needles, six knife blades, two
electrosurgical unit tips
n H: have you any questions? What is the status of
filling out the implant card?
An example of a scrub person’s hand off to another
scrub person (Figure 3) for the same patient might
include the following:
before a shift change.
AORN Journal j 499
Figure 3. One scrub person performs a SWITCH hand off with another scrub person before a shift change.
November 2013 Vol 98 No 5 JOHNSON ET AL
n S: surgerydright mastectomy, sentinel node
biopsy, reconstruction with implant; have two
separate Mayo stands and back tables; patient is
allergic to penicillin
n W: wetd0.25% bupivacaine plain (30 mL),
50,000 units of bacitracin diluted in 1,000 mL
of 0.9% sodium chloride irrigation solution, two
15-Fr closed collapsible drains opened on sterile
field
n I: instrumentsdusing the two trays of mastec-
tomy instruments; tissue expanders in room but
not opened
n T: tissuedthree specimens: right breast to be
sent to pathology for permanent section and
two sentinel nodes sent to pathology for touch
prep handed off the surgical field to the
RN circulator
n C: countsdverify change of shift count: eight
laparotomy sponges in sponge counting bag
off the field, 12 laparotomy sponges on the field,
500 j AORN Journal
12 sutures, six knife blades, two electrocautery
unit tips
n H: have you any questions?
EXPANSION
After implementation of SWITCH, the council
redesigned the tool’s concept so that it could be
used for indirect perioperative patient care areas
throughout the OR. The charge nurses at the OR
front desk did not have a standardized reporting
method, and the outgoing charge nurse sometimes
failed to relay critical information to the oncoming
charge nurse. The partnership council member who
initiated the SWITCH concept was also the week-
end charge nurse. She proposed a modification of
the SWITCH tool that would make the front desk
scheduling charge reports more efficient and ef-
fective (Figure 4). By adjusting the SWITCH cat-
egories (ie, changing the words associated with
each letter of the acronym), a revised version of the
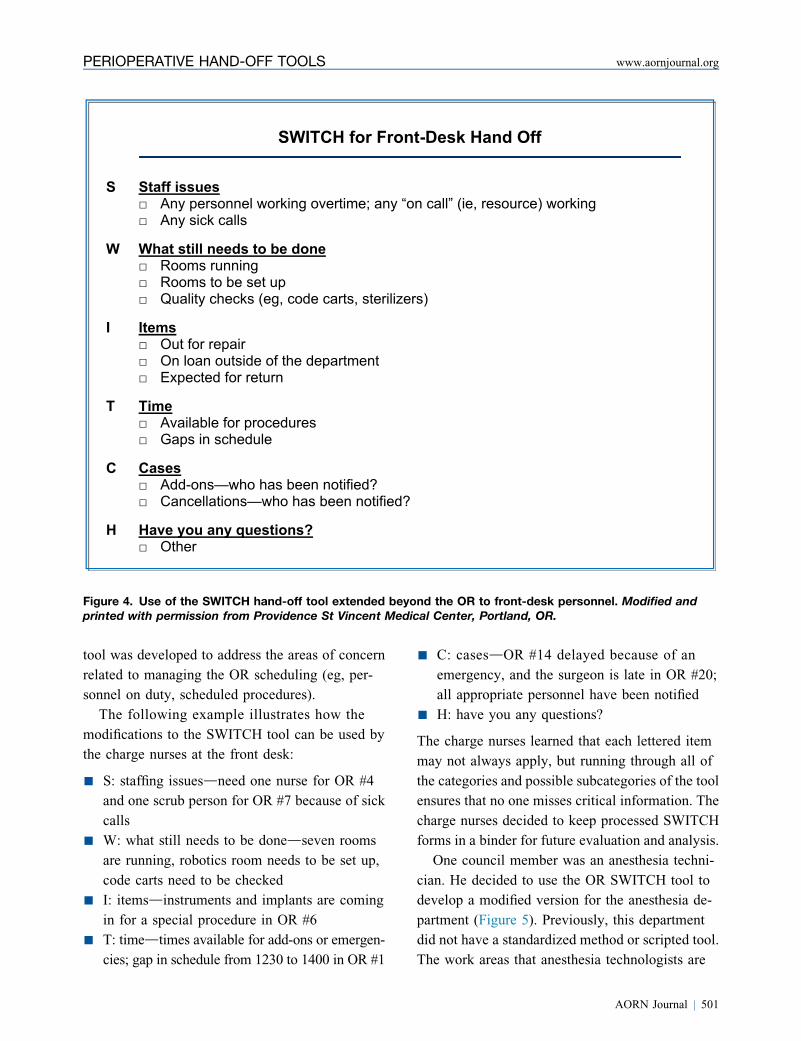
SWITCH for Front-Desk Hand Off
S Staff issues
□ Any personnel working overtime; any “on call” (ie, resource) working □ Any sick calls
W What still needs to be done
□ Rooms running □ Rooms to be set up □ Quality checks (eg, code carts, sterilizers)
I Items
□ Out for repair □ On loan outside of the department □ Expected for return
T Time
□ Available for procedures □ Gaps in schedule
C Cases
□ Add-ons—who has been notified? □ Cancellations—who has been notified?
H Have you any questions?
□ Other
Figure 4. Use of the SWITCH hand-off tool extended beyond the OR to front-desk personnel. Modified andprinted with permission from Providence St Vincent Medical Center, Portland, OR.
PERIOPERATIVE HAND-OFF TOOLS www.aornjournal.org
tool was developed to address the areas of concern
related to managing the OR scheduling (eg, per-
sonnel on duty, scheduled procedures).
The following example illustrates how the
modifications to the SWITCH tool can be used by
the charge nurses at the front desk:
n S: staffing issuesdneed one nurse for OR #4
and one scrub person for OR #7 because of sick
calls
n W: what still needs to be donedseven rooms
are running, robotics room needs to be set up,
code carts need to be checked
n I: itemsdinstruments and implants are coming
in for a special procedure in OR #6
n T: timedtimes available for add-ons or emergen-
cies; gap in schedule from 1230 to 1400 in OR #1
n C: casesdOR #14 delayed because of an
emergency, and the surgeon is late in OR #20;
all appropriate personnel have been notified
n H: have you any questions?
The charge nurses learned that each lettered item
may not always apply, but running through all of
the categories and possible subcategories of the tool
ensures that no one misses critical information. The
charge nurses decided to keep processed SWITCH
forms in a binder for future evaluation and analysis.
One council member was an anesthesia techni-
cian. He decided to use the OR SWITCH tool to
develop a modified version for the anesthesia de-
partment (Figure 5). Previously, this department
did not have a standardized method or scripted tool.
The work areas that anesthesia technologists are
AORN Journal j 501
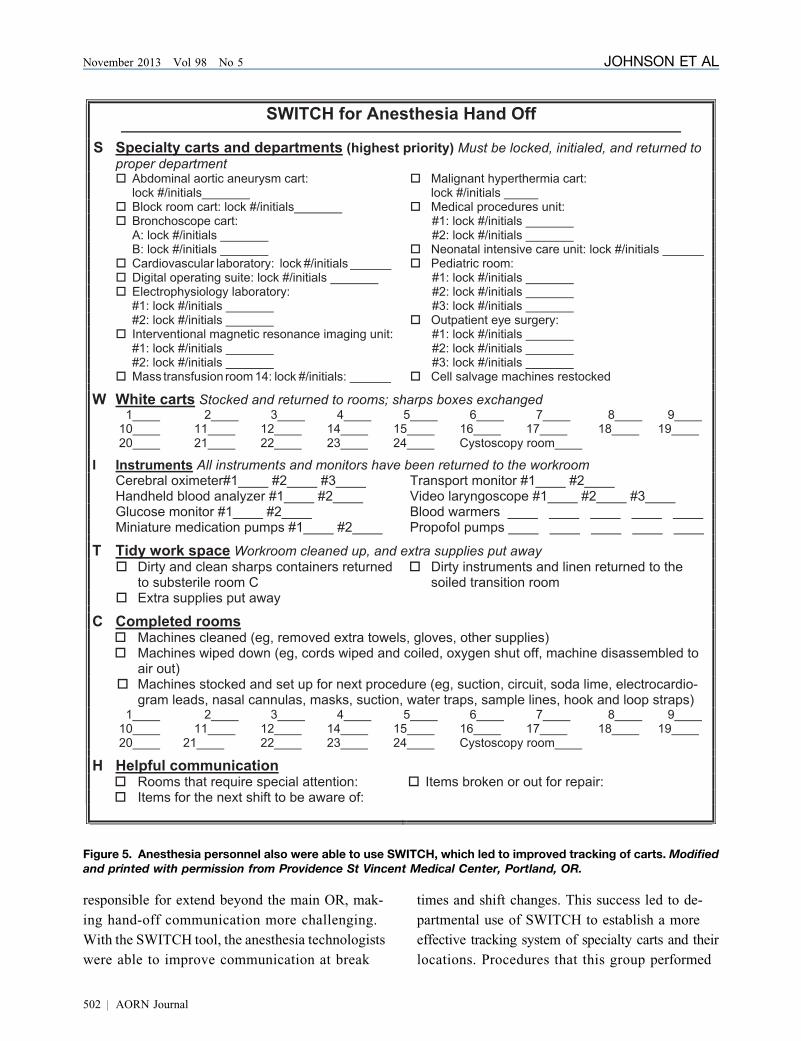
Figure 5. Anesthesia personnel also were able to use SWITCH, which led to improved tracking of carts. Modifiedand printed with permission from Providence St Vincent Medical Center, Portland, OR.
November 2013 Vol 98 No 5 JOHNSON ET AL
responsible for extend beyond the main OR, mak-
ing hand-off communication more challenging.
With the SWITCH tool, the anesthesia technologists
were able to improve communication at break
502 j AORN Journal
times and shift changes. This success led to de-
partmental use of SWITCH to establish a more
effective tracking system of specialty carts and their
locations. Procedures that this group performed

PERIOPERATIVE HAND-OFF TOOLS www.aornjournal.org
outside the main OR became more easily tracked,
and less time was spent locating lost equipment
in different departments. Equipment from radi-
ology, the catheterization laboratory, endoscopy, and
the neonatal intensive care unit stopped getting mis-
placed, which improved efficiency and reduced
replacement costs. The hand-off tool also made it
easier for anesthesia technologists to identify which
carts need to be cleaned and restocked, which resulted
in a more efficient and effective department. Having
equipment readily available also hasmade it safer for
the patients.
At Providence St Vincent Medical Center, the
anesthesia professional is typically accompanied to
the PACU by the surgeon, resident, or physician
assistant. The anesthesia professional gives the
main hand-off report to the PACU nurse. The RN
circulator may call the PACU nurse with a specific
patient concern before the patient is transferred to
the PACU or may accompany the anesthesia pro-
fessional to the PACU if he or she has specific
hand-off information that may not be given by the
anesthesia professional. This variability facilitates
faster room turnover. A standardized hand-off tool
is being developed at this time for the hand-off
communication between the anesthesia profes-
sional and PACU RN.
FEEDBACK AND SUCCESS
A council member shared the SWITCH hand-off
tool for the RN circulator and scrub person with
personnel from several other hospitals in the Port-
land area. Additionally, council members presented
the tool at a local AORN chapter meeting, on
AORN MemberTalk (ie, AORN listserv), and as
a poster presentation at the 2012 AORN Congress
in New Orleans, Louisiana. The council received
positive feedback regarding the hand-off tool. After
using SWITCH for one year, Surgical Services
Partnership Council members presented a survey to
measure compliance with the tool’s use. Of the 33
team members (ie, 20 nurses, 12 surgical technol-
ogists, one anesthesia technologist) who completed
the survey, 97% thought that the SWITCH hand-off
tool was very important for patient safety and 87%
thought it was easy to use. Council members have
listened to the comments of the survey. As a result,
council members added a subcategory to the form
for dressings and drains. Other comments received
were that
n personnel want to be able to give their report
without feeling rushed or interrupted,
n the script provides a verbal and written report
but also allows time for asking and answering
questions,
n nurses like the versatility of having both lami-
nated and paper forms of the tool available, and
n standardization of hand-off reports keeps the
care provider’s focus on the patient and in-
creases patient safety.
Managerial feedback expressed support and en-
couragement for using SWITCH for every patient
every time, and managers have requested audits
of the paper version of the tool to document
compliance.
Council members successfully implemented the
Universal ProtocolTM for time outs14 and, subse-
quently, the World Health Organization Surgical
Safety Checklist.15 Equally important to managers
and council members alike, as well as to patient
safety, has been the successful implementation of
the SWITCH hand-off tool. Hand-off reports are
a time for health care providers to focus on the
transfer of care without interruption, a time to
pause, and a time to “SWITCH for Safety.” The use
of the SWITCH tool at our facility has kept the
focus of the hand-off exchange on the care of the
patient and, in fact, has spotlighted patient safety
while at the same time ensuring concise and
complete reporting. Perioperative services is
a specialized service area in which using a stan-
dardized, scripted tool has benefited all RN circu-
lators, scrub personnel, anesthesia technologists,
and indirect patient care providers but, most im-
portantly, the patients.
AORN Journal j 503

November 2013 Vol 98 No 5 JOHNSON ET AL
Editor’s note: The Universal Protocol for Pre-
venting Wrong Site, Wrong Procedure, Wrong
Person Surgery is a trademark of The Joint
Commission, Oakbrook Terrace, IL.
References1. Nagpal K, Vats A, Lamb B, et al. Information transfer
and communication in surgery: a systematic review. Ann
Surg. 2010;252(2):225-239.
2. Taneva S, Grote G, Easty A, Plattner B. Decoding the
perioperative process breakdowns: a theoretical model
and implications for system design. Int J Med Inform.
2010;79(1):14-30.
3. Sentinel event. The Joint Commission. http://www.joint
commission.org/sentinel_event.aspx. Accessed August 9,
2013.
4. Hospital and Health Service Performance Division.
Promoting Effective Communication Among Healthcare
Professionals to Improve Patient Safety and Quality of
Care. Melbourne, Australia: Victoria Government De-
partment of Health; 2010:1-12.
5. The Joint Commission. Improving handoff communica-
tions: meeting National Patient Safety Goal 2E. Joint
Perspect Patient Safety. 2006;6:9-15.
6. Van Dam S. A process prone to error and needing im-
provement. Forum. 2007;25(1):14-15.
7. 2008 Hospital Patient Safety Goals: Implementation
expectations for handoffs. The Joint Commission. http://
www.jointcommission.org/NR/rdonlyres/82B717D8-
B16A-4442-AD00-CE3188C2F00A/0/08_HAP_NPSGs_
Master.pdf. Accessed October 2, 2013.
8. Friesen MA, White SV, Byers JF. Handoffs: implications
for nurses. In: Patient Safety and Quality: An Evidence-
Based Handbook for Nurses. Rockville, MD: Agency for
Healthcare Research and Quality; 2008:1-17.
9. Hand-off communications. Healthcare Inspirations.
http://www.healthcareinspirations.com/hci_hand-off_
communications.html. Accessed August 9, 2013.
10. Sandlin D. Improving patient safety by implementing
a standardized and consistent approach to hand-off
communications. J Perianesth Nurs. 2007;22(4):289-292.
11. Patient Hand Off Communication Tool Kit. AORN, Inc.
http://www.aorn.org/Clinical_Practice/ToolKits/Patient
_Hand_Off_Tool_Kit/Patient_Hand_Off_Tool_Kit.aspx.
Accessed August 30, 2013.
12. Transitions of care (TOC) portal. The Joint Commission.
http://www.jointcommission.org/toc.aspx. Accessed
August 9, 2013.
13. Simms E. The components of change: creativity and
innovation, critical thinking and planned change. In:
504 j AORN Journal
Roussel L, Swansburg R, eds. Management and Lead-
ership Administration for Nurse Administrators. 4th ed.
Sudbury, MA: Jones and Bartlett Publishers; 2006:55-80.
14. The Universal Protocol. The Joint Commission. http://
www.jointcommission.org/standards_information/up
.aspx. Accessed August 9, 2013.
15. Surgical Safety Checklist. The World Health Organiza-
tion. http://www.who.int/patientsafety/safesurgery/tools
_resources/SSSL_Checklist_finalJun08.pdf. Accessed
August 9, 2013.
Fay Johnson, BSN, RN, CNOR, is a clinical
level 4 perioperative nurse in the OR at
Providence St Vincent Medical Center, Portland,
OR. Ms Johnson has no declared affiliation
that could be perceived as posing a potential
conflict of interest in the publication of this
article.
Patty Logsdon, MSN, RN, CNOR, is a peri-
operative nurse in the OR at WakeMed Health
and Hospitals, Raleigh, North Carolina. Ms
Logsdon has no declared affiliation that could be
perceived as posing a potential conflict of in-
terest in the publication of this article.
Kim Fournier, ADN, RN, CNOR, is a clinical
level 4 perioperative nurse in the OR at
Providence St Vincent Medical Center, Portland,
OR. Ms Fournier has no declared affiliation that
could be perceived as posing a potential conflict
of interest in the publication of this article.
Sandra Fisher, BS, RN, CNOR, is a clinical
ladder level 4 perioperative nurse in the OR at
Providence St Vincent Medical Center, Portland,
OR. Ms Fisher has no declared affiliation that
could be perceived as posing a potential conflict
of interest in the publication of this article.
EXAMINATION
CONTINUING EDUCATION PROGRAM2.3
www.aorn.org/CESWITCH for Safety: PerioperativeHand-off Tools
PURPOSE/GOAL
�
To provide knowledge specific to improving hand-off communications during
perioperative transfers of care from one health care provider to another.
OBJECTIVES
1. Discuss the leading cause of reported sentinel events.
2. Identify barriers to communication.
3. Describe hand-off communications.
4. Identify standardized formats used for hand offs.
5. Discuss SWITCH tools used for perioperative hand offs.
The Examination and Learner Evaluation are printed here for your conven-
ience. To receive continuing education credit, you must complete the Exami-
nation and Learner Evaluation online at http://www.aorn.org/CE.
QUESTIONS
1. The leading cause of reported sentinel events in
the OR is
a. assessment.
b. communication breakdown.
c. the physical environment.
d. medication management.
2. Barriers to concise communication include
1. inattention.
2. information overload.
3. multitasking.
4. noise.
5. stress.
6. time pressures.
a. 1, 3, and 5 b. 2, 4, and 6
AORN, Inc, 2013
c. 2, 3, 5, and 6 d. 1, 2, 3, 4, 5, and 6
3. The most common health care transactions prone
to error are
a. billing.
b. electronic data interchange.
c. hand-off communication.
4. A hand off includes the transfer of
1. patient information.
2. the authority to care for the patient.
3. the responsibility to care for the patient.
4. staff department meeting information.
a. 1 and 3 b. 2 and 4
November 2013 Vo
c. 1, 2, and 3 d. 1, 2, 3, and 4
5. Standardized formats for hand offs include
1. SBAR.
2. I PASS the BATON.
3. SHARQ.
l 98 No 5 � AORN Journal j 505

November 2013 Vol 98 No 5 CE EXAMINATION
4. Five Ps.
5. Five Ps, second version.
a. 4 and 5 b. 1, 2, and 3
506 j AORN Journal
c. 1, 2, 3, and 4 d. 1, 2, 3, 4, and 5
6. In the OR, the SWITCH acronym stands for
surgical procedure, what needs to be done,
instruments, time, counts, and have you any
questions.
a. true b. false
7. According to the OR SWITCH tool, the plan for
postoperative patient disposition belongs in the
___________ section.
a. surgical procedure
b. wet
c. tissue
d. have you any questions?
8. According to the OR front-desk SWITCH tool,
identifying gaps in the OR schedule belongs in
the ___________ section.
a. staff issues b. items
c. time d. have you any questions?
9. According to the anesthesia SWITCH tool, iden-
tifying items that are broken or out for repair
belongs in the ___________ section.
a. specialty carts and departments
b. white carts
c. instruments
d. helpful communication
10. Of the 33 team members who completed a survey
after using the SWITCH hand-off tool for a year,
97% thought that the SWITCH hand-off tool was
very important for patient safety.
a. true b. false

LEARNER EVALUATION
CONTINUING EDUCATION PROGRAM2.3
www.aorn.org/CESWITCH for Safety: PerioperativeHand-off Tools
This evaluation is used to determine the extent
to which this continuing education program
met your learning needs. Rate the items as
described below.
OBJECTIVES
To what extent were the following objectives of this
continuing education program achieved?
1. Discuss the leading cause of reported sentinel events.
Low 1. 2. 3. 4. 5. High
2. Identify barriers to communication.
Low 1. 2. 3. 4. 5. High
3. Describe hand-off communications.
Low 1. 2. 3. 4. 5. High
4. Identify standardized formats used for hand offs.
Low 1. 2. 3. 4. 5. High
5. Discuss SWITCH tools used for perioperative hand
offs. Low 1. 2. 3. 4. 5. High
CONTENT
6. To what extent did this article increase your
knowledge of the subject matter?
Low 1. 2. 3. 4. 5. High
7. To what extent were your individual objectives met?
Low 1. 2. 3. 4. 5. High
8. Will you be able to use the information from this
article in your work setting? 1. Yes 2. No
� AORN, Inc, 2013
9. Will you change your practice as a result of reading
this article? (If yes, answer question #9A. If no,
answer question #9B.)
9A. How will you change your practice? (Select all that
apply)
1. I will provide education to my team regarding
why change is needed.
2. I will work with management to change/
implement a policy and procedure.
3. I will plan an informational meeting with
physicians to seek their input and acceptance
of the need for change.
4. I will implement change and evaluate the
effect of the change at regular intervals until
the change is incorporated as best practice.
5. Other: ________________________________
9B. If you will not change your practice as a result of
reading this article, why? (Select all that apply)
1. The content of the article is not relevant to my
practice.
2. I do not have enough time to teach others
about the purpose of the needed change.
3. I do not have management support to make
a change.
4. Other: ________________________________
10. Our accrediting body requires that we verify
the time you needed to complete the 2.3 con-
tinuing education contact hour (138-minute)
program: _________________________________
November 2013 Vol 98 No 5 � AORN Journal j 507