Embed Size (px)
Citation preview

Sustaining Improvement in Daily WorkKevin Little, PhD – IHI Improvement Adviser
Jeff Rakover, MPP – IHI Research Associate
Richard Scoville, PhD – IHI Improvement Adviser
Learning Lab SL4
The presenters have
nothing to disclose
Sunday, December 10, 2017
#IHIFORUM
Presenters
Kevin Little, PhD – IHI Improvement Adviser
Jeff Rakover, MPP – IHI Research Associate
Richard Scoville, PhD – IHI Improvement Adviser
P2
Objectives of this Learning Lab
Distinguish between management for quality control,
quality improvement, and quality assurance
Use IHI’s quality control framework to design a system
for sustaining quality at the front-line
Create a plan for testing and implementing a quality
control system at your own organization.
P3

How Do Leading Organizations Sustain?
Interviews with 10 leading North American healthcare organizations.
Three in-depth case studies
Literature review
“By focusing first on implementing standard work with frontline clinical units and managers, such as a charge nurse or team lead, organizations can build a solid ‘bottom-up’ foundation for Quality Control and Quality Improvement that then supports more robust high-performance management at the system level.”
http://www.ihi.org/resources/Pages/IHIWhitePapers/Sustaining-Improvement.aspx
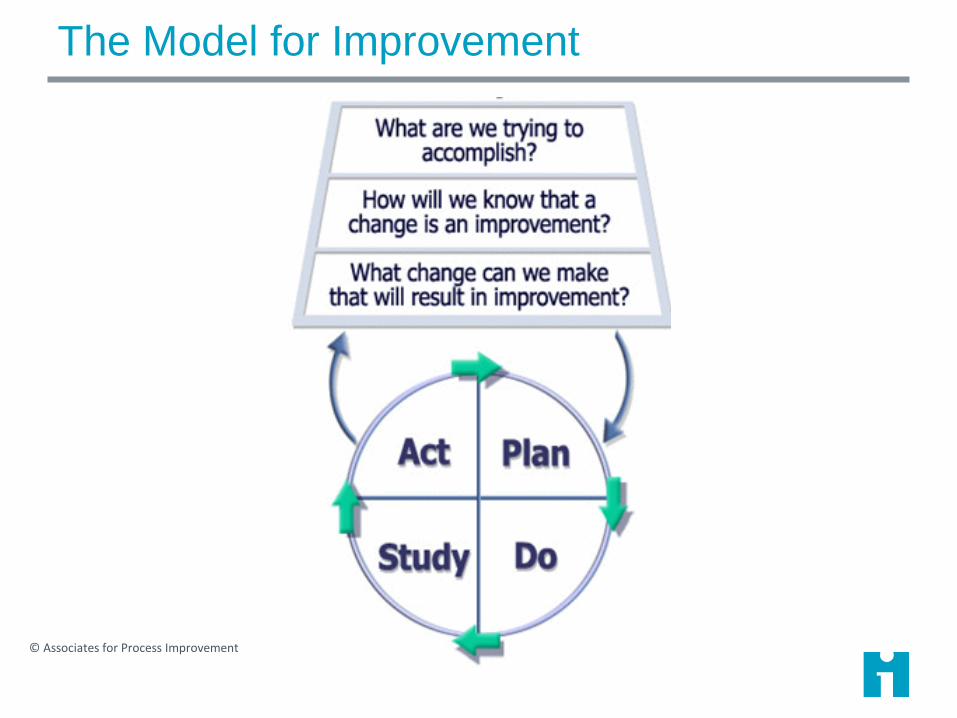
The Model for Improvement
© Associates for Process Improvement
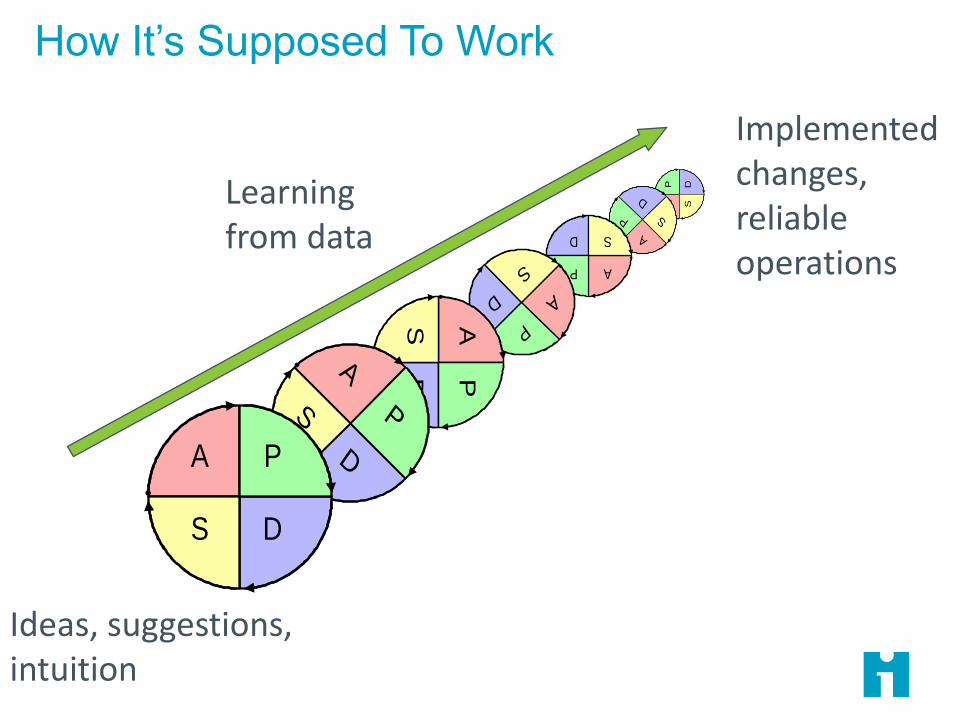
How It’s Supposed To Work
AP D
S
A
P
D
S
AP
D S
A
P
D
S
APD
S
A
P
D
S
A P
DS
Ideas, suggestions, intuition
Implemented changes, reliable operations
Learning from data

Change ideas, suggestions, intuition
Permanent, reliable, sustained improvement!?
But What Goes Up…
Same old dysfunctional system
…Too Often Backslides!
Juran’s Trilogy
Reliability & Sustainability
Quality Trilogy
✓ Control
✓ Improvement
✓ Planning
P8

Definition of Reliability for Health Care
The capability of a process, procedure or health service to
perform its intended function in the required time under
existing conditions.*
The system’s ability to do what it is supposed to do, for
every patient, every time.
Reliable execution of standard process is the
‘platform’ upon which clinicians can best
exercise their craft.

Measuring Reliability
Reliability =
Number of Actions That Achieve The Intended Result
Total Number of Opportunities for Action
Reliability measures are very common, based on standard protocols:
• Percent of diabetic patients with foot exams at previous visit
• Percent of surgeries with checklist completed
• Percent of sepsis patients with antibiotics administered within 1
hour of recognition of sepsis.
• Percent of patients who received all VAP bundle elements
• Percent of service users seen within 28 days of referral
How to Maintain Reliable Performance?
Our research and testing has led us to conclude:
“The key to sustaining improvement is to focus on the daily
work of frontline managers, supported by a high-
performance management system that prescribes standard
tasks and responsibilities for managers at all levels of the
organization.”
Scoville, R., K. Little, J. Rakover, K. Luther and K. Mate. Sustaining Improvement. IHI White Paper. Cambridge,
Massachusetts: Institute for Healthcare Improvement; 2016. IHI Whitepaper. Cambridge, MA, Institute for Healthcare Improvement. Avaliable at IHI.ORG.
Improvement alone is not enough.

Joseph Juran: The Quality Trilogy
Manage the work
Improve the work
Design and manage systems
capable of delivering quality
“Quality Control”
“Quality Improvement”
“Quality Planning”
Source: Juran Institute

The Trilogy in Action
Source: Juran Institute
Better
ImprovementControl
Control
?
How can we manage to build and operate systems that meet patient (client, customer) needs
consistently over time?
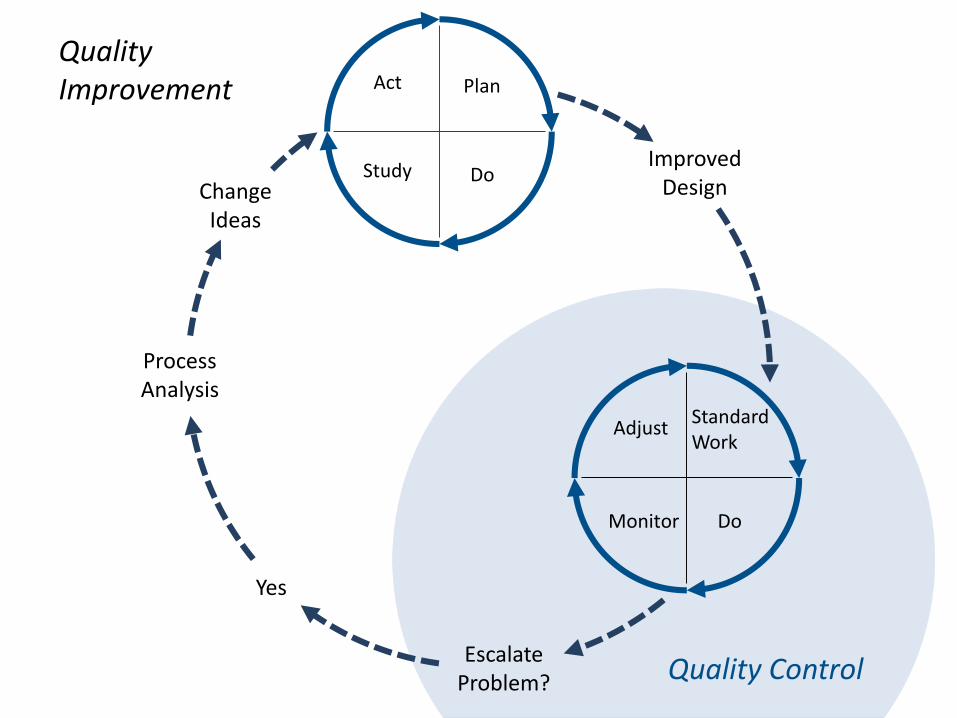
StandardWork
DoMonitor
Adjust
Plan
DoStudy
Act
ImprovedDesign
EscalateProblem?
Yes
ProcessAnalysis
ChangeIdeas
Quality Control
Quality Improvement
Exercise: Your System
1. Discuss with the person sitting next to you:
What key process are you focused on today?
What measure(s) could (do) you use to assess the
reliable performance of that process?
2. Share at your table:
Adapt PDSA Testing a Reliability Measure file to plan
a test of a reliability measure in your 'own' project next
week.
P15

Control Systems in Action (Part 1)
Drivers of sustained quality control
Example: Ambulatory Surgery
P16

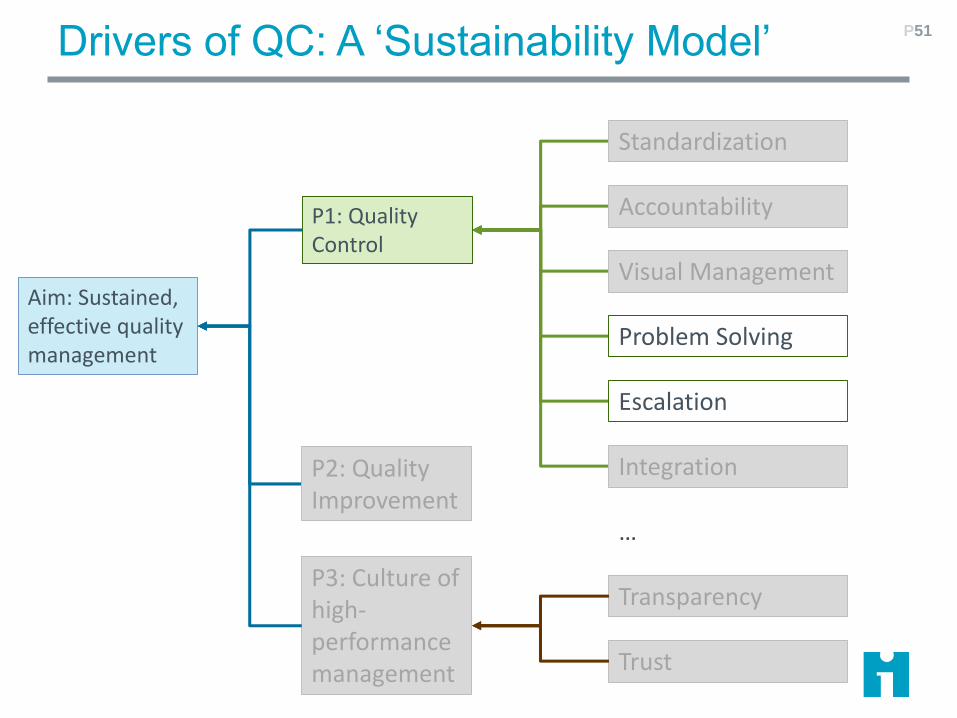
Drivers of QC: A ‘Sustainability Model’ P17
Aim: Sustained, effective quality management
P1: Quality Control
P2: Quality Improvement
P3: Culture of high-performance management
Standardization
Visual Management
Problem Solving
Escalation
Integration
Accountability
Transparency
Trust
…
Drivers of Quality Control (for your notes)
1. Standardization: Once a process has been improved, sustaining it requires the
elaboration of standard work by staff in the service unit. Roles and responsibilities of staff
and front-line managers, along with detailed, checklist-based work routines are
documented, maintained, and monitored on a daily basis.
2. Accountability: Brief, daily front-line huddles involving unit staff and supervisors focus
the team’s attention on the performance of standard work. Regular review and
participation by higher level managers sustains the huddles, and provides opportunities
for managers to fully understand front-line issues and coach staff.
3. Visual Management: Simple data displays provide the backdrop for the daily huddles.
These displays show performance on key process indicators and outcomes over time, log
front-line problems and their disposition, and track the progress of improvement projects.
4. Problem-solving and Improvement: Huddles reveal everyday issues and difficulties
with standard work processes. Many of these can be speedily resolved by front line staff;
others require investigation and testing of possible solutions. Front line staff need basic
proficiency in techniques such as root cause analysis and Plan-Do-Study-Act testing to
achieve workable solutions.
5. Escalation: Problems that require substantial process redesign or inter-department
coordination cannot be solved at the front-line and may trigger a formal quality
improvement project. Emergent issues such as critical equipment failures or serious
patient harm may require immediate escalation to top management. Explicit procedures
are needed to triage problems and escalate them to the proper level of management.
6. Integration: Effective operational management and strategic improvement require that
the organization operate as a coordinated whole. Process goals, standard work, and QI
project aims must be integrated across organizational levels and coordinated among units
and departments through a standard planning and reporting process.
P18

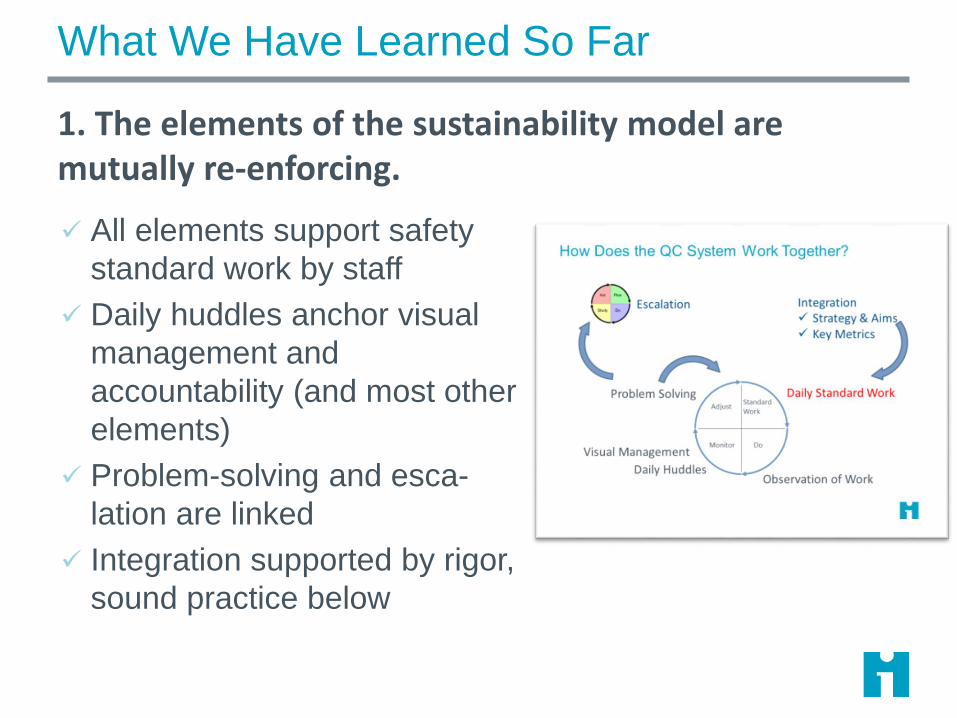
How Does the QC System Work Together?19
Daily HuddlesObservation of Work
Problem Solving
Visual Management
Daily Standard WorkStandardWork
DoMonitor
Adjust
Integration✓ Strategy & Aims✓ Key Metrics
Escalation
Putting the Drivers to Work 20
• Standard work for managers
Anchored by daily huddles
• Accountability Regular review of standard work
• Visual management Making performance a daily concern
• Problem-solving & escalation
Appropriate responses to daily problems
• Integration Aligned standard work at all levels of the org chart
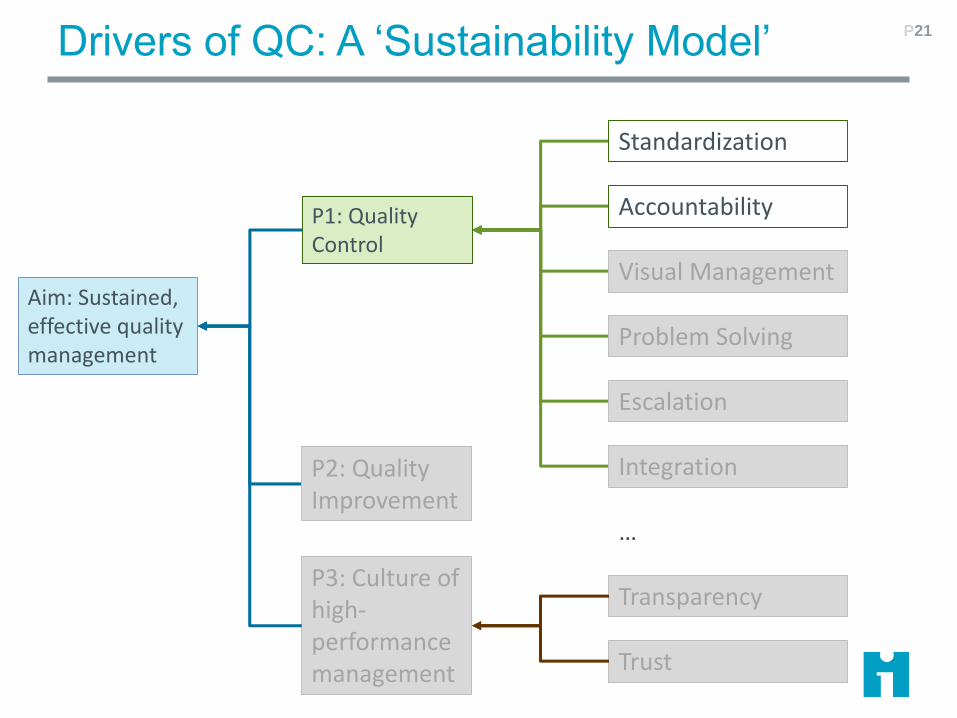
Drivers of QC: A ‘Sustainability Model’ P21
Aim: Sustained, effective quality management
P1: Quality Control
P2: Quality Improvement
P3: Culture of high-performance management
Standardization
Visual Management
Problem Solving
Escalation
Integration
Accountability
Transparency
Trust
…
AHRQ’s Safety Program for Ambulatory Surgery
Overview
✓ Funded by Agency for Healthcare Research and
Quality (AHRQ) as part of the National Action Plan to
Prevent Healthcare-Associated Infections (HAI)
✓ 665 registered ASCs from 47 States and DC
participated in 8 program cohorts
Objectives
✓ Reduce surgical infection and complication rates
✓ Improve safety culture through improved teamwork
and communication
http://www.ahrq.gov/professionals/quality-patient-safety/hais/tools/ambulatory-
surgery/index.html
22
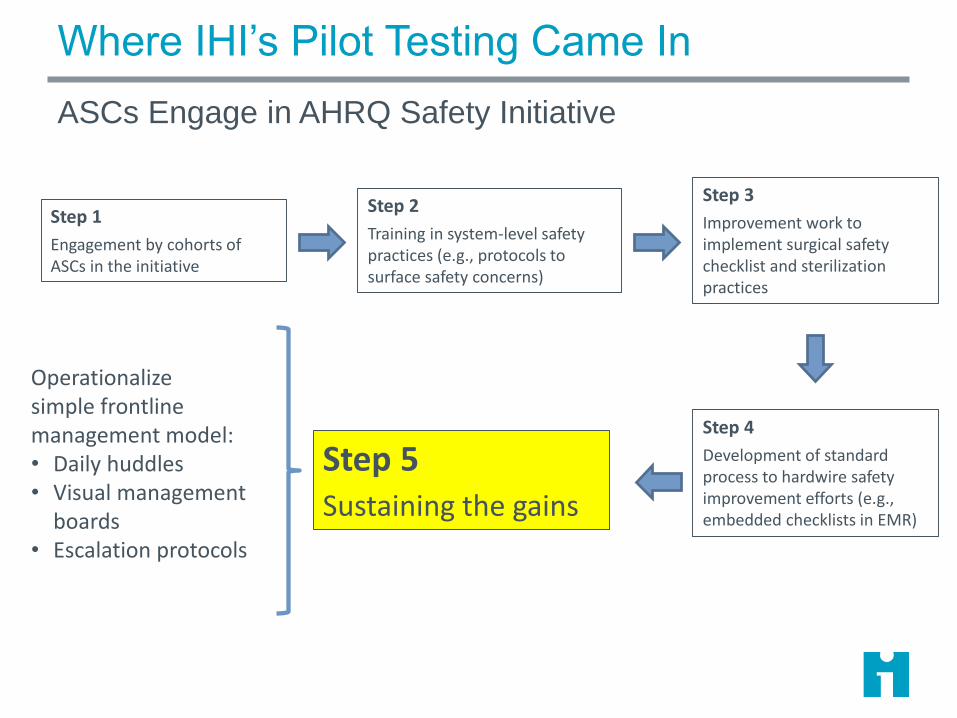
Where IHI’s Pilot Testing Came In
ASCs Engage in AHRQ Safety Initiative
Step 1
Engagement by cohorts of ASCs in the initiative
Step 4
Development of standard process to hardwire safety improvement efforts (e.g., embedded checklists in EMR)
Step 3
Improvement work to implement surgical safety checklist and sterilization practices
Step 2
Training in system-level safety practices (e.g., protocols to surface safety concerns)
Step 5Sustaining the gains
Operationalizesimple frontline management model:• Daily huddles• Visual management
boards• Escalation protocols
IHI’s Pilot Testing
Main testing took place over three month period
HRET improvement advisers assisted in site selection
and recruitment
Site visits were two-days, with assistance from quality
specialists working in the ASCs
Work focused on testing and implementing the
sustainability model
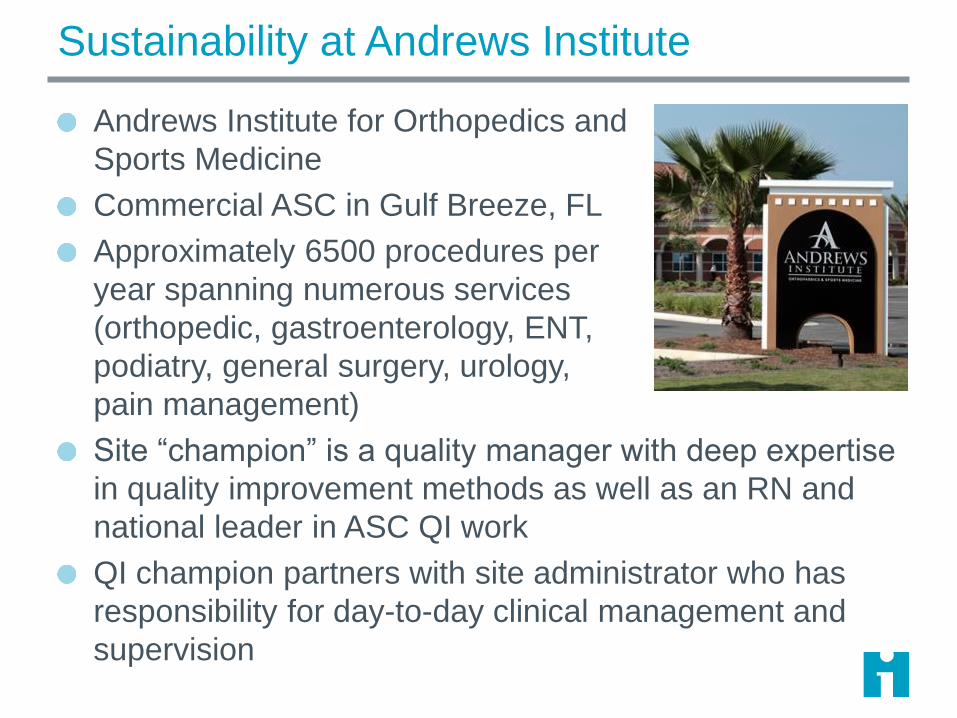
Sustainability at Andrews Institute
Andrews Institute for Orthopedics and
Sports Medicine
Commercial ASC in Gulf Breeze, FL
Approximately 6500 procedures per
year spanning numerous services
(orthopedic, gastroenterology, ENT,
podiatry, general surgery, urology,
pain management)
Site “champion” is a quality manager with deep expertise
in quality improvement methods as well as an RN and
national leader in ASC QI work
QI champion partners with site administrator who has
responsibility for day-to-day clinical management and
supervision

HU
DD
LE B
OA
RD

Huddles “Anchor” Other Drivers P31
Visual Management
• Metrics viewed & remarked
• Team updates data daily
Accountability• Supervisors monitor
huddles, feed back huddle compliance to teams
Escalation• Team escalates issues
beyond its immediate control.
Problem Solving
• Team reviews / disposes current issues in huddle.
Integration• Team selects local
metrics that align with strategic goals.
Standard Agenda for a Daily 5m Huddle P32
1. Concerns, problems observed in past day:
• Patients
• Staff
• Process, equipment, etc.
2. Anticipated issues for today
3. Review of tracked problems
4. Input from staff
5. Announcements
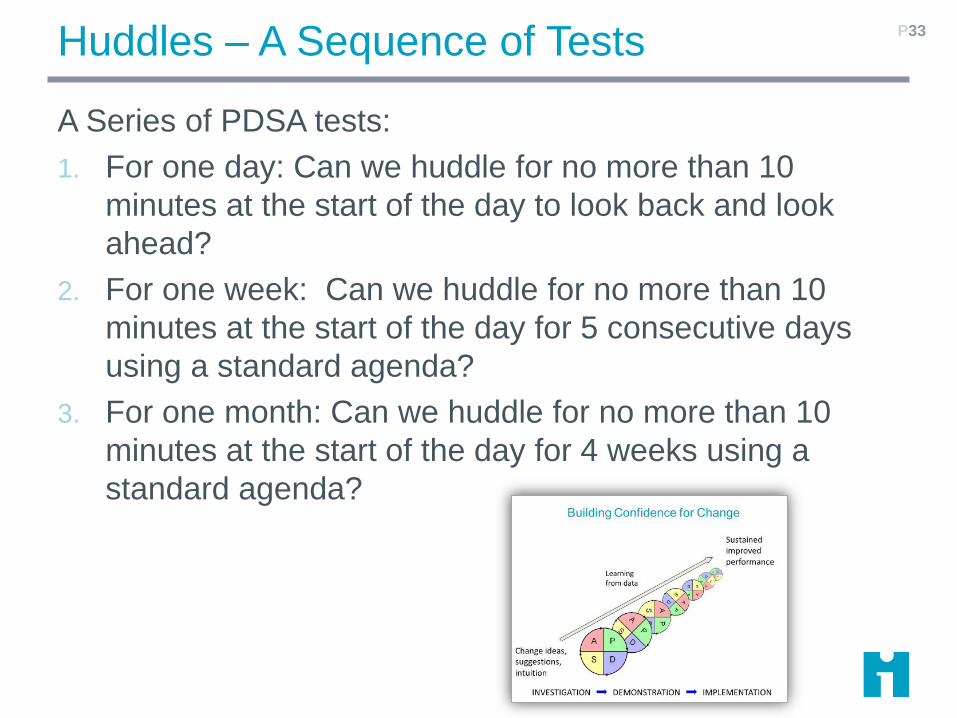
Huddles – A Sequence of Tests
A Series of PDSA tests:
1. For one day: Can we huddle for no more than 10
minutes at the start of the day to look back and look
ahead?
2. For one week: Can we huddle for no more than 10
minutes at the start of the day for 5 consecutive days
using a standard agenda?
3. For one month: Can we huddle for no more than 10
minutes at the start of the day for 4 weeks using a
standard agenda?
P33
Exercise: Testing Huddles in Your System
Adapt PDSA Testing Daily Huddles file to your 'own'
project:
Design 3 sequential PDSAs to test huddles in your
system, to be completed next week:
✓ Where and when will the huddle(s) occur
✓ Who will lead them? What preparation is required?
✓ How will you know that the huddles are working well?
✓ How will you use the learning from each PDSA cycle
to inform the next?
P34
Control Systems in Action (Part 2)
Example: Greater Baltimore Medical Center
Visual Management
Involving Leadership
P35

Drivers of QC: A ‘Sustainability Model’ P36
Aim: Sustained, effective quality management
P1: Quality Control
P2: Quality Improvement
P3: Culture of high-performance management
Standardization
Visual Management
Problem Solving
Escalation
Integration
Accountability
Transparency
Trust
…
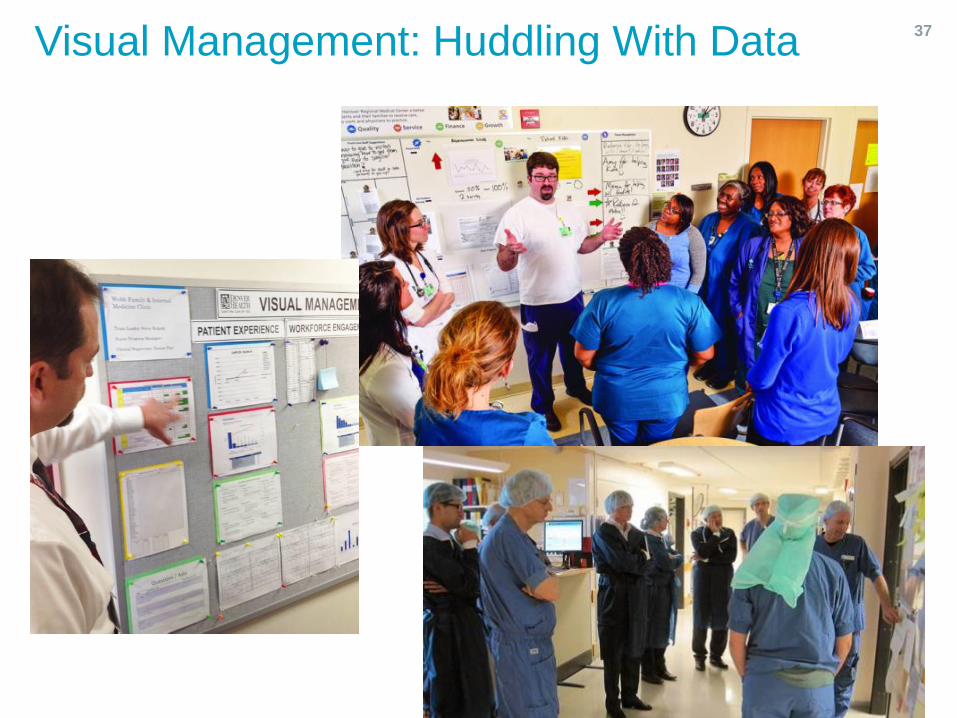
Visual Management: Huddling With Data 37
GBMC Healthcare, Inc. Baltimore, MarylandP38
Greater Baltimore Medical Center is a 281-bed acute care not-for-profit community hospital that opened in 1965.
Located on a 72 acre campus in Towson serving patients primary residing in Baltimore and Harford Counties as well as Baltimore City.
52,916 ED visits annually27,651 Surgical procedures (IP & OP)
3,893 Births

GBMC Vision Phrase and Quadruple AIM
Vision Phrase:
To every patient, every time, we will provide the care that
we would want for our own loved ones.
Quadruple AIM:
1. Better Health Outcomes
2. Best Care Experience
3. Least Waste (Lower Cost)
4. Most Joy for those providing
care
P39
Improvement Journey
Lean Journey – Begins 2010
• Waste Walks / Education
• Rapid Cycle Improvement (Kaizen) events
• Interdepartmental 4.5 day events
• Value-Stream Mapping or Transactional Process
Improvement
Fragmented Results / Culture not evolving
- Improvement interpreted as an event, not every day work.
- Tools learned are not used often. People lose confidence to
enroll others.
Lean Daily Management – Begins 2013
P40

Goals for LDM (Lean Daily Management)
1. Culture change. Improvement IS our daily work.
2. Front line engagement. Learn ability to see
opportunities and the tools to solve them.
3. Manager accountability. Identify the metrics, engage
team in problem solving, refine standard work/visual
management.
4. Executives as coaches/mentors and barrier busters.
Keep focus on our AIMS.
P41
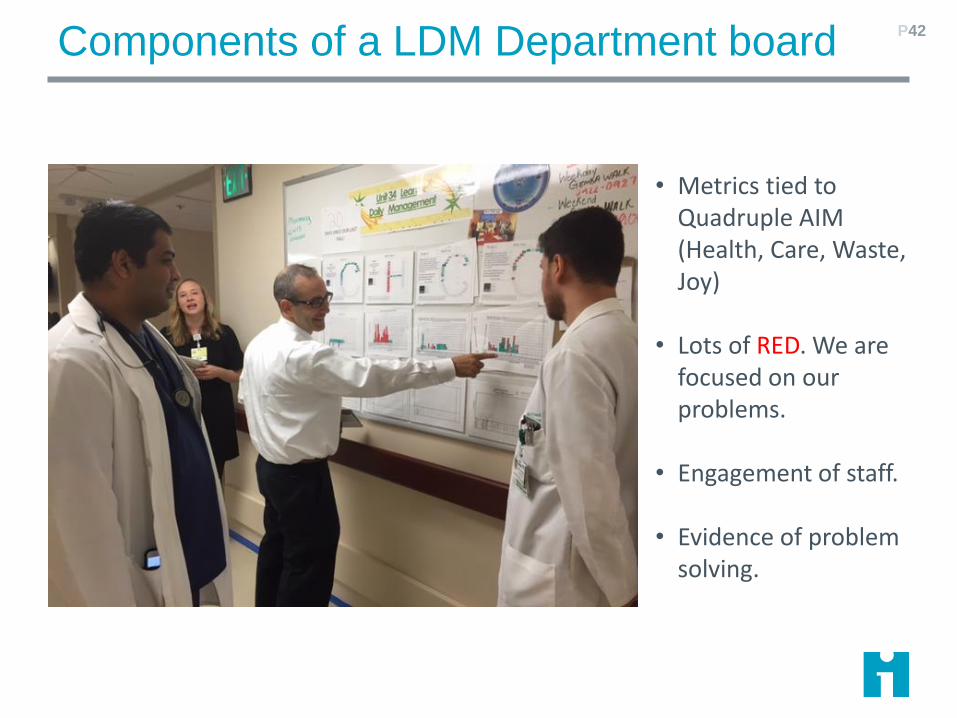
Components of a LDM Department board P42
• Metrics tied to Quadruple AIM (Health, Care, Waste, Joy)
• Lots of RED. We are focused on our problems.
• Engagement of staff.
• Evidence of problem solving.
GBMC LDM gemba walk
9:00 AM Executive Huddle
Begin gemba walk. (5 teams/routes, 2 weeks per route)
Department LDM board presentation.
Post-walk huddle.
Share learning. Email to ALL staff on executive metrics
and learning.
GBMC LDM is conducted 365 days/year. On weekends
and holidays, the administrator on call walks to all of the
boards.
P43

LDM Executive Engagement
• Be present.
• Connect to vision.
• Say “Thank You”.
• Provide coaching
using inquiry.
• Remove barriers.
P44
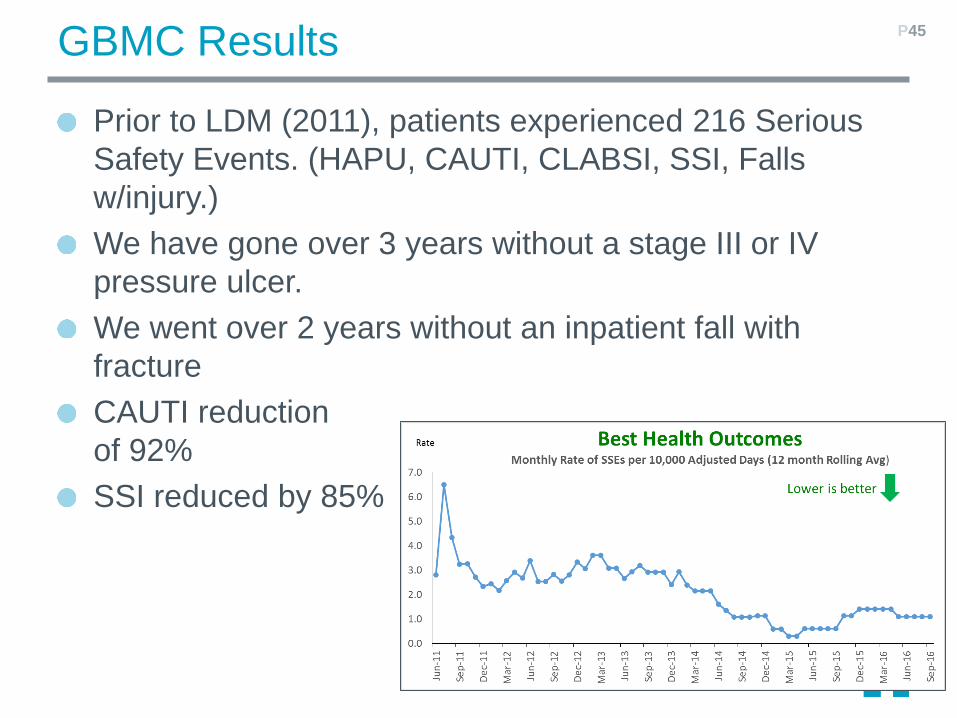
GBMC Results
Prior to LDM (2011), patients experienced 216 Serious
Safety Events. (HAPU, CAUTI, CLABSI, SSI, Falls
w/injury.)
We have gone over 3 years without a stage III or IV
pressure ulcer.
We went over 2 years without an inpatient fall with
fracture
CAUTI reduction
of 92%
SSI reduced by 85%
P45
A Few Simple Rules…
1. Keep the aim of the Visual Management board in mind:
performance at a glance
2. The main users are you and your staff
3. Choose just a few items to start off
4. Choose items you can update regularly
5. Choose a space convenient for daily huddles to keep
your board
6. A dedicated whiteboard proves convenient, but you can
start with paper if easier

A Visual Management Board Example 47
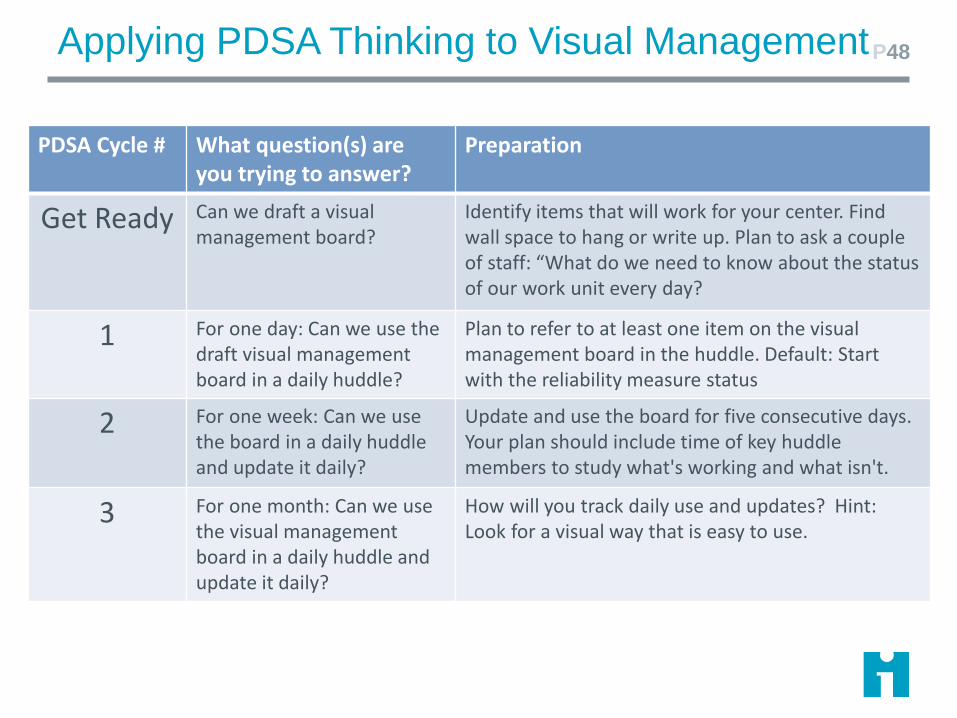
Applying PDSA Thinking to Visual ManagementP48
PDSA Cycle # What question(s) are you trying to answer?
Preparation
Get Ready Can we draft a visualmanagement board?
Identify items that will work for your center. Find wall space to hang or write up. Plan to ask a couple of staff: “What do we need to know about the statusof our work unit every day?
1 For one day: Can we use the draft visual management board in a daily huddle?
Plan to refer to at least one item on the visual management board in the huddle. Default: Start with the reliability measure status
2 For one week: Can we use the board in a daily huddle and update it daily?
Update and use the board for five consecutive days. Your plan should include time of key huddle members to study what's working and what isn't.
3 For one month: Can we use the visual management board in a daily huddle and update it daily?
How will you track daily use and updates? Hint: Look for a visual way that is easy to use.
Exercise: Develop and Test your Visual Board
• Get Ready: Identify and sketch
ingredients for your 'own' project visual
board
--why is each ingredient necessary?
• Draft PDSA cycles 1-3 (as far as time
allows)
49
Problem Solving and Escalation
P50
Drivers of QC: A ‘Sustainability Model’ P51
Aim: Sustained, effective quality management
P1: Quality Control
P2: Quality Improvement
P3: Culture of high-performance management
Standardization
Visual Management
Problem Solving
Escalation
Integration
Accountability
Transparency
Trust
…
Accountability and Integration
Observation of standard work (huddle attendance and
gemba walk) are basis for next level leader standard
work.
Consider huddle of unit leaders to discuss inter-
department issues (e.g., sterilization, scheduling,
handoffs).
Expand observation beyond basic standard work (e.g., a
safety checklist) to multiple types of standard work (e.g.,
handoffs, patient education, longitudinal care)
Remember to report progress to senior leaders to ensure
continuous buy-in and help remove barriers to progress,
as well as to encourage use of similar systems at other
levels of organization (e.g., executive huddles)
Two Types of Problems
TYPE 1
Coping with the immediate issue; getting on with the
work
TYPE 2
Taking action so that the problem does not recur.
P53
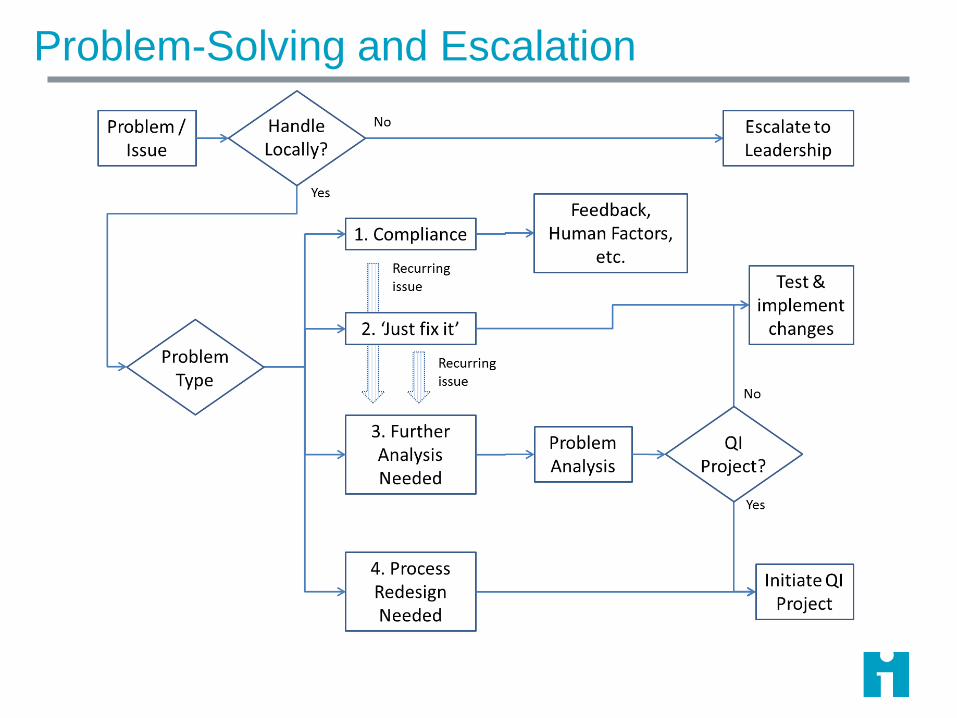
Problem-Solving and Escalation

Examples of Problems 55
Type of Problem
Who Can Solve? Type 1 – Cope Type 2 - Prevent
Us • Find a staff sub• Borrow missing
supplies• Calibrate a device
• Change process sequence for flash sterilization
• Reorganize surgical packs to minimize missing items
Others • Call in additional staff for emergency situation
• Raise immediate safety concern
• Improve handoff to post-op to reduce wait
• Implement follow up calls with patients to coach on PT compliance.
Exercise: Examples of Problems
For your own process, generate examples for each of
the cells in the 2 x 2 table.
56
Who Can Solve Type 1 Type 3
Our Team
Others
Type of Problem
Exercise: PDSAs for Management Pull
Who should be invited to observe your huddles and
interact with you on problems that require help beyond
your team?
What do want to accomplish with the observation?
How will you know if you accomplished your aim?
Generate a sequence of PDSA cycles to test a link
between your daily huddle and 'next level' of management
in your 'own' project.
57
Problem-Solving: Some Tips
Problem solving aims to at reliable performance
If your organization has a standard problem-solving
method, learn to use it
Use root cause analysis to investigate and document
harm or other problematic events
Incorporate routine use of CUS or a similar method into
frontline work
Praise problem-raising, avoid blame.
Focus on causes and testable solutions.
P58
Summary and Wrap-Up
What We Have Learned So Far
P59
What We Have Learned So Far
✓ All elements support safety
standard work by staff
✓ Daily huddles anchor visual
management and
accountability (and most other
elements)
✓ Problem-solving and esca-
lation are linked
✓ Integration supported by rigor,
sound practice below
1. The elements of the sustainability model are mutually re-enforcing.

What We Have Learned So Far
2. Daily Huddles Provide the Ritual for Paying Attention
to Process
Empower staff –gives everyone a voice; culture is blame-averse
Forum for problem identification and tracking solutions
Visual management at huddles keeps quality metrics in view
Daily rhythm builds habits, gives management system visibility and structure
What We Have Learned So Far
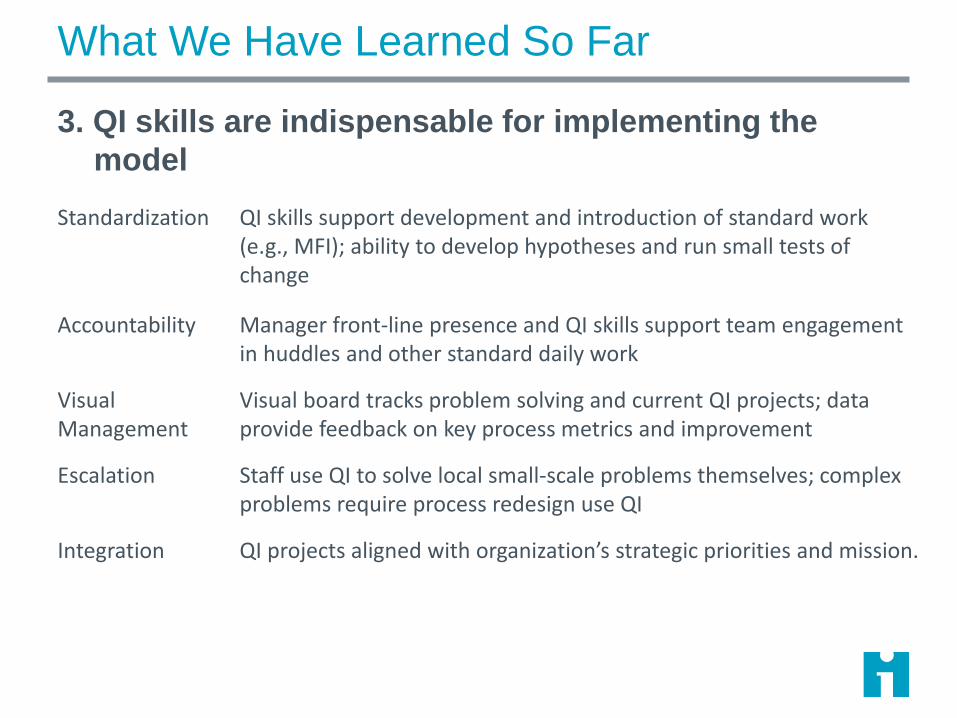
3. QI skills are indispensable for implementing the
model
Standardization QI skills support development and introduction of standard work (e.g., MFI); ability to develop hypotheses and run small tests of change
Accountability Manager front-line presence and QI skills support team engagement in huddles and other standard daily work
Visual Management
Visual board tracks problem solving and current QI projects; data provide feedback on key process metrics and improvement
Escalation Staff use QI to solve local small-scale problems themselves; complex problems require process redesign use QI
Integration QI projects aligned with organization’s strategic priorities and mission.

What We Have Learned So Far4. Problem Solving and Escalation Both Needed
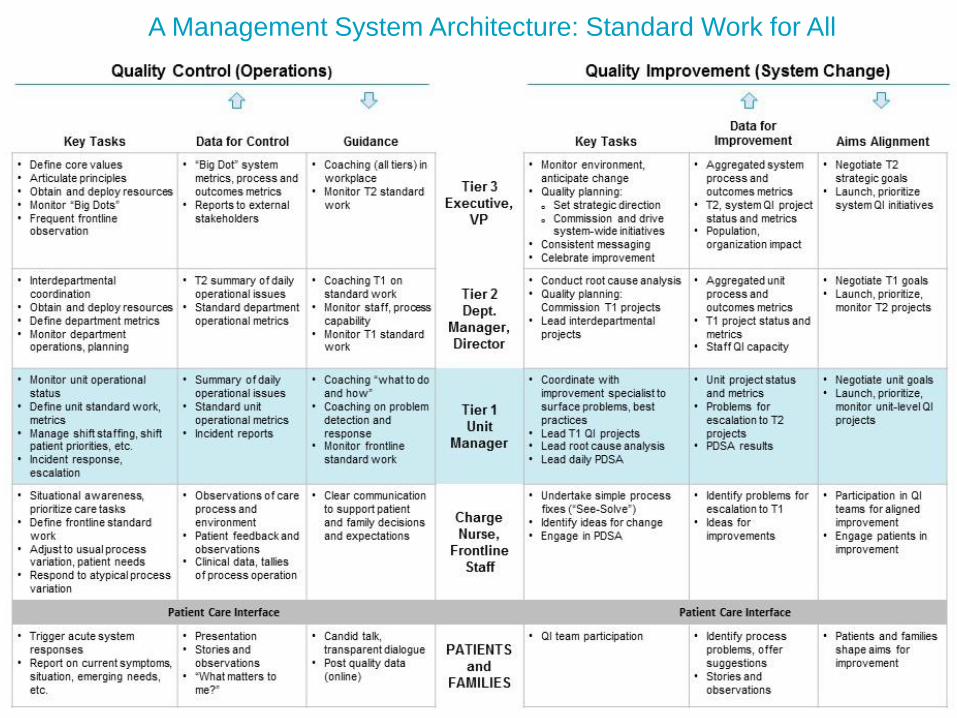
A Management System Architecture: Standard Work for All
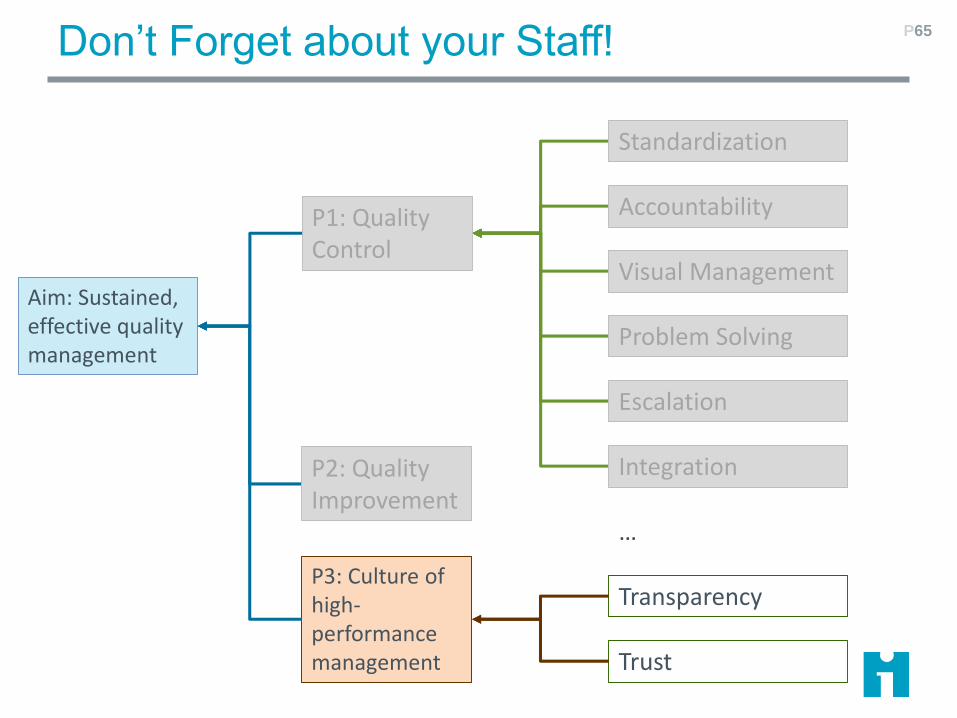
Don’t Forget about your Staff! P65
Aim: Sustained, effective quality management
P1: Quality Control
P2: Quality Improvement
P3: Culture of high-performance management
Standardization
Visual Management
Problem Solving
Escalation
Integration
Accountability
Transparency
Trust
…
Where to Start?
Choose a pilot unit with certain characteristics
Stability: Low staff churn, few symptoms of
burnout
Alignment around goals: Managers
understand what’s expected of them, how
their work is going to change, why the
changes are important.
Management ‘hygiene’: Regular
management practices are in place; effective
budgeting, relatively stable processes
Engagement: Have a respected local
champion who can build excitement for
change, encourage participation, coach,
celebrate success
P66

Where to Start? – 2
Consider the type of unit as well:
P67
Easier
• Currently defined standard processes; may resemble an assembly line
• Examples:✓Surgical unit✓Endoscopy suite✓Radiology unit
Harder
• Widely varying processes; a lot of custom work
• Examples:✓General medical unit✓ED✓Narrow sub-specialty with
broad diagnostic variety
Lessons
You can get started at the unit level
You can make some progress
You will eventually hit a ceiling
Ultimately, interrelated units (the units that your unit
depends on for patients and sends patients to) need to
be applying these management methods too
AND, your senior leaders need to have their own
standard work, fluency with problem solving, and ideally
huddles and visual management methods that ensure
that they remove barriers to your progress in a timely
manner– so that they lift the ceiling or blow the roof!
68
Summary
Sustaining improvement (i.e. Quality Control; high
reliability) means paying continual attention to the
process at the front line. Huddles are fundamental.
Juran’s Trilogy provides a conceptual framework for
Quality Control.
Drivers: Standardization; Accountability; Visual
Management, Problem Solving & Escalation; Integration.
Lean Daily Management is an example, used at GBMC
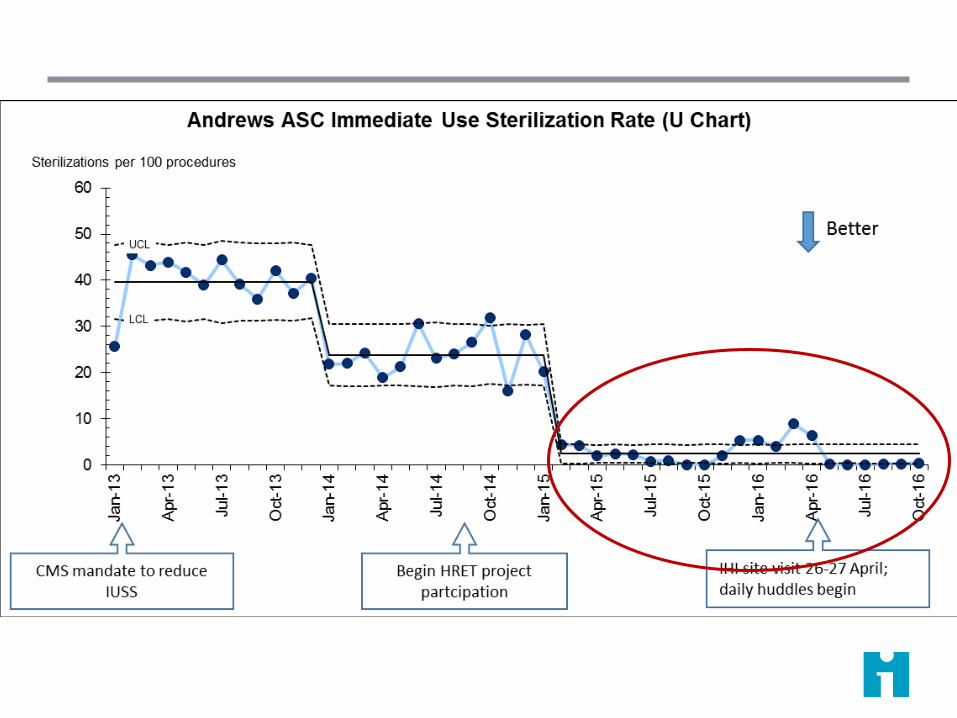
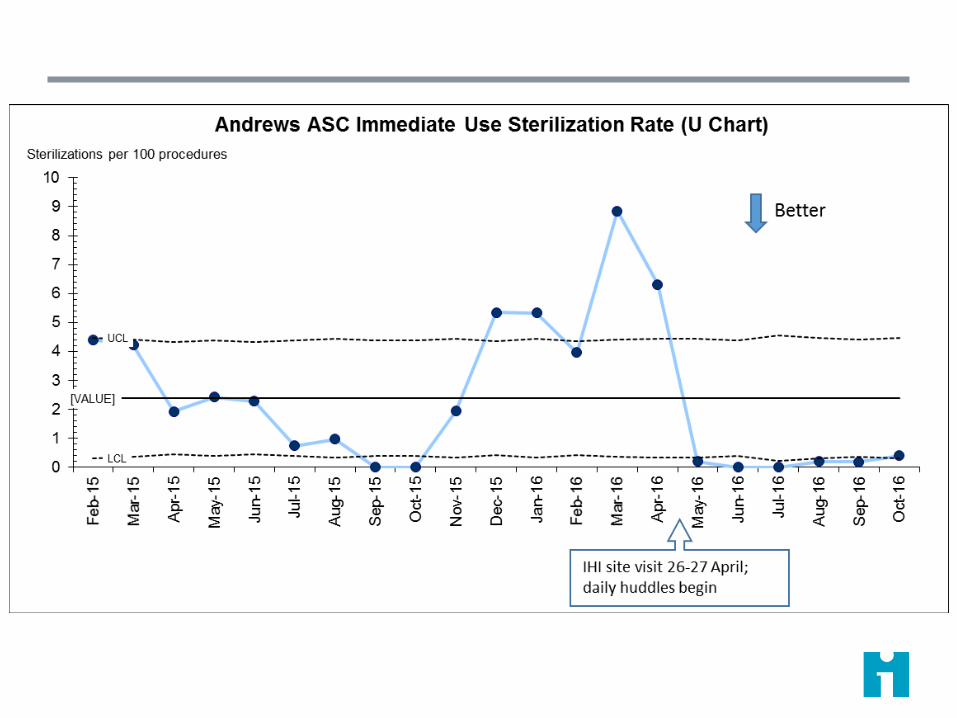
IHI pilot tested the Sustainability Model at Andrews and 1
other ASC: uptake was enthusiastic.
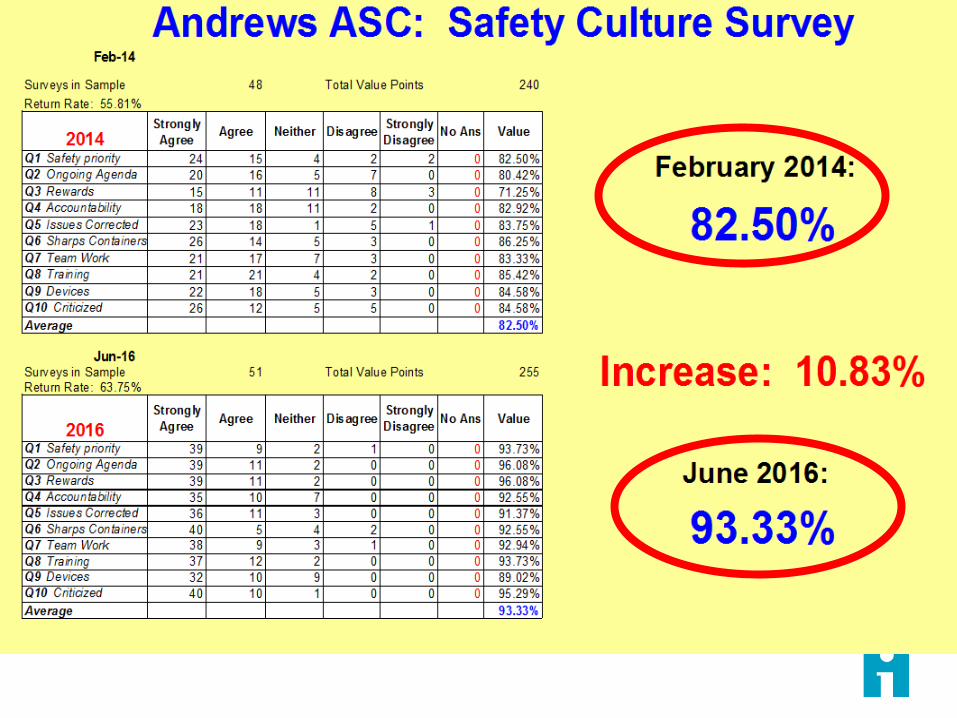
Andrews ASC attributes increased safety practices and
culture to the Model.
Huddle-based problem solving & escalation process
maintains control over time.
P69

P70

Contact
Kevin Little
Jeff Rakover
Richard Scoville
P71

For additional study
J. Lancaster (2017) The Work of Management: A Daily Path to Sustainable Improvement, LEI, Cambridge, MA
D. Mann (2015) Creating a Lean Culture: Tools to Sustain Lean Conversions, 3rd edition, CRC Press, Boca Raton, FL.
R. Scoville et al. (2014). ‘Sustaining Improvement.’ IHI White Paper. Cambridge, Massachusetts: Institute for Healthcare Improvement. Available at http://www.ihi.org/resources/Pages/IHIWhitePapers/Sustaining-Improvement.aspx
Kevin Little's blog postsdaily-huddles-1-helping-people-do-a-better-job
daily-huddles-2-setting-the-stage-for-organizational-learning
self-control-for-individuals-and-teams
enhancing-experience-intuition-and-guts
P72



![L29 Presentation.ppt [Read-Only] - IHI Home Pageapp.ihi.org/FacultyDocuments/Events/Event-2491/Presentation-10640/...management from data systems and sustaining relationships ... Data](https://img.pdfslide.us/doc/110x75/5b3430f37f8b9aa0238da72c/l29-read-only-ihi-home-pageappihiorgfacultydocumentseventsevent-2491presentation-10640management.jpg)

















![[SUSTAINING IMPACT]](https://img.pdfslide.us/doc/110x75/626ca8abff2bfc61932b3923/sustaining-impact.jpg)





