Embed Size (px)
Citation preview

Sustained Inflation and its role in the delivery room management
Gianluca Lista MD
NICU Ospedale dei Bambini «V.Buzzi»
-ICP-Milano Italy

Disclosure (Dr.Lista)
I have no actual or potential conflict of
interest in relation to this presentation

Reduction incidence death/BPD < 30 wks’GA: NNT of 35
Reduction incidence death/BPD < 32 wks’GA: NNT of 25
COIN (2008) CNRN (2009) SUPPORT (2010) CURPAP (2011) DRM (2011) AMV (2011) TAKE CARE (2013)

50-67 % of VLBW infants initially in nCPAP required MV COIN and SUPPORT (2008-2010) 52 % of 26-29+6 GA infants initially in nCPAP required MV VON trial (2011)
Background: NCPAP failure rate

Respiratory transition in the newborn: a three-phase process.
Hooper SB, Te Pas AB, Kitchen MJ
«We propose that the respiratory transition at birth passes through three distinct,
but overlapping phases, which reflect different physiological states of the
lung……..During the first phase, the airways are liquid-filled and so no
pulmonary gas exchange can occur. Respiratory support should, therefore, be
focused on clearing the gas exchange regions of liquid.In the absence of gas
exchange, little or no CO2 will accumulate within the airways and, therefore,
interrupting inflation pressures to allow the lung to deflate and exhale CO2 is
unnecessary. This is the primary rationale for administering a sustained
inflation at birth»

Vt
ml/Kg
TIME
sec
0
4
2
1
6
10
12
8
0 3 2 4
First breath
30 sec
10’,60’,90’
days
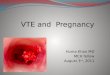
Fig. 1.14 Schematic representation of the average spirogram
of the first breat and those at 10’,30’and at few days after birth
Term newborn
Karlberg P, J Pediatr 1960, vol.56, 585-604

“The opening pressure”
First breath
Later


• Population: inborn preterm infants (25.0-28.6 wks’ GA);16 NICUs
• Intervention: SLI + CPAP + possible actions according to AAP
• Control: CPAP + possible actions according to AAP
• Outcome: need for MV in the first 72 hours of life
• Time: september 2011-january 2013

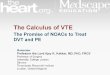
294 Randomized
144 Allocated to the control group
142 Received allocated treatment
2 Did not received allocated treatment 1 Treated with SLI 1 Stillborn
150 Allocated to the SLI group
148 Received allocated treatment 2 Did not received allocated treatment 1 Randomized in error
1 Stillborn
131 Alive at discharge 12 Died during in-hospital stay
1 Stillborn
131 Alive at discharge 17 Died during in-hospital stay
1 Randomized in error 1 Stillborn
143 Included in the intention-to-treat analysis
1 Excluded from the intention-to-treat analysis
1 Stillborn
148 Included in the intention-to-treat analysis
2 Excluded from the intention-to-treat analysis
1 Randomized in error
1 Stillborn
354 Screened for eligibility
60 Not eligible 9 Congenital malformation 4 Foetal hydrops
43 Consent not given 14 Other reasons
Population
TRIAL diagram




Infants initially treated with a SI had improved short-term respiratory outcomes (reduced need of tracheal intubation and MV within 72hrs of life, (NNT = 10),
however BPD and/or death occurrence were not improved




Hooper S, Lista G, Cavigioli F, A te Pas et al (Osaka-Synchroton radiation, June 2015)

Respiratory Inductance Plethysmography (RIP)
Respiratory Function Monitor (RFM)
Volumetric CO2 monitor
T-piece resuscitator

• Prospective observational study • 2 NICUs ( Leiden and Milan) • 15 preterm infants; GA 28 (27-31) wks;BW 1080 (994-1300) g • Measurements= Vte, changes in plethysmography (RIP bands), ECO2 (volumetric CO2 monitor)
• During SI,PPV and CPAP

At the end of 1° SI
Breathing infants during SI
(11 out of 15)
Apneic infants during SI
(4 out of 15)
SBs (average) n° 4(3) 0
Vte (range) ml/Kg 5.9 (2.4-8.2) 5.2 (0.2-6.0) p<0.005
ECO2 (range) mmHg 16.0 ( 10-30) 5.0 (2.0-15.0) p<0.01
At the end of 2° SI
Breathing infants during SI
(4 out of 5)
Apneic infants during SI
(1 out of 5)
SBs (average) n° 2(1) 0
Vte (range) ml/Kg 5.2 (0.2-6.0) 4.6 p=NS
ECO2 (range) mmHg 16.0 ( 4-25) 4.0 p=NS

Spontaneuos breathing appears to play an important part in the success
of ventilation given at birth

G.Lista et al. 2015, data submitted

A. No breaths B. Inspiration without expiration C. Expiratory braking maneuvers D. Inspiration immediately followed by expiration
G.Lista et al. 2015, data submitted
Fig.1
SI ….works

No flow signal during the Sustained inflation, no breaths…..Glottis closure?
G.Lista et al. 2015, data submitted
Fig.2
SI ….does not work

Gr1 (no SBs) N=11
Gr2 (yes SBs) N=19
Statistics
GA (wks) 26 (25-26.5) 28 (26.5-29) p=0.004
BW (g) 700 (591-810) 839 (725-932) p=0.04
SI duration (sec) 15 (13-18) 15 (13-18) p=NS
SBs (number) NA 3 (1.5-5.5) NA
IT of SBs (sec) NA 0.52 (0.45-0.56) NA
Vti (ml/Kg) NA 5.9 (3.3-11) NA
Vte (ml/Kg) NA 2.7 (0-3.1) NA
Calculated gain in lung volume (ml/Kg)
4.1 (3.2-6) 21.8 (11.1-27.4) p=0.02
G.Lista et al. 2015, data submitted

• The neonatologist in DR…..to consider and allow “respiratory transition”
• Infants initially treated with a SI had improved short-term respiratory outcomes : reduced
need of tracheal intubation and MV within 72hrs of life (NNT =10) (BPD and/or death occurrence not improved)
• SI is only “one step” (1st phase of the respiratory transition) within a “respiratory strategy” (DR..NICU) to try to improve long term-respiratory outcome
• SI greater than 5” may be considered in individual clinical circumstances or research settings (Neonatal Resuscitation Guidelines 2015)
• To evaluate SI efficiency :both tidal volumes and ECO2 levels should be taken into account
• SI successful seems to be related to gestational age (less activity in the lowest GA) and the
presence of active breathing (glottis open)
• Further clinical studies are needed to evaluate the efficacy of SI including : • Setting of SI maneuver (optimal duration and peak pressure) • Selection of patients (rescue or prophylactic procedure?) • Evaluation of long term outcomes (BPD/Death) as primary outcome • Timing of surfactant administration
Take Home Messages