Embed Size (px)
Citation preview

Sustained effect of Ex Vivo Lung Perfusion on Nitric Oxide
Metabolite levels in Lung Tissue after Transplantation
By
Farshad Tavasoli
A thesis submitted in conformity with the requirements
for the degree of Master of Science
Institute of Medical Science
University of Toronto
© Copyright by Farshad Tavasoli 2014

ii
Sustained effect of Ex Vivo Lung Perfusion on Nitric Oxide
Metabolite levels in Lung Tissue after Transplantation
Farshad Tavasoli
Master of Science
Institute of Medical Science
University of Toronto
2014
Abstract
Limited availability of donor lungs results in high mortality of patients waiting for lung
transplantation. Modern techniques such as ex vivo lung perfusion (EVLP) or interleukin-10 (IL-
10) gene therapy expand the donor pool and may improve the quality of donor organs and
outcomes following lung transplantation remain inferior compared to other organ
transplantations. Alterations in metabolic pathways, such as L-arginine/nitric oxide (NO)
metabolism can contribute to post-transplantation organ dysfunction. We investigated the L-
arginine/NO metabolism in pig models of lung transplantation. We found significant
differences in the L-arginine/NO metabolism in lungs from brain death compared to non-brain
death donors after prolonged hypothermic preservation. Moreover, we found that EVLP
decreased NO metabolite concentrations in lung, a sustained effect after transplantation that was
unaffected by IL-10 gene therapy during EVLP. In conclusion, donation circumstances and
preservation methods may alter the L-arginine/NO metabolism in transplanted lungs, which may
contribute to clinical outcomes after transplantation.

iii
Acknowledgments
First and foremost, I would like to acknowledge the support and direction of my supervisor,
Dr. Hartmut Grasemann. Not only he gave me an amazing opportunity to study a fascinating
project in his lab, he also encouraged me throughout the study with his generous share of
knowledge. Further, I would like to give recognition for my colleagues and friends whose
presence assisted the completion of this project greatly. I thank Hailu Huang, M.D. for her
help with q-PCR experiments and NO measurement. I thank Darakhshanda Shehnaz, Ph.D.
for technical help, sample processing, Western blotting and enzyme activity measurements. I
thank Jalil Nasiri MSc, Peyman Ghorbani MSc and David Douda Ph.D. for their technical
help.
I wish to acknowledge my advisory committee members, Dr. Mingyao Liu, Dr. Nades
Palaniyar and Dr. Jaques Belik for their guidance, comments, patience and support. I value
their input as it was remarkably beneficial to this thesis.
I would like to give special thanks to Dr. Shaf Keshavjee for his support as well as for his
generosity for providing mass spectrometry data and all tissue samples for this study.
I gratefully acknowledge Dr. David Grant and SickKids Research Institute for providing
funding for this study.
I would also like to acknowledge Dr. Tiago Machuca and Dr. Riccardo Bonato who
performed large animal lung transplantation surgeries. I thank Dr. Marcelo Cypel and Dr.
Michael Hsin for providing metabolomic data and helpful discussions.
I thank May Brydges, Jeff Patton, Paul Chartrand and Ivone Ornelas for their administrative
help.
Last but not least, I would like to thank my wife Sheida Aminkhadem and my daughter Nikki
Tavassoli for their love and support.

iv
Table of contents
Chapter 1: Background & Introduction ...................................................................................... 1
1.1 Lung transplantation ......................................................................................................... 2
1.1.1 Brain death donors .................................................................................................... 5
1.1.2 Donation after cardiac death ..................................................................................... 8
1.2 Preservation of harvested lung ....................................................................................... 10
1.2.1 Cold static preservation........................................................................................... 10
1.2.2 Ex vivo perfusion..................................................................................................... 11
1.3 Primary graft dysfunction (PGD) ................................................................................... 16
1.3.1 Risk factors for PGD ............................................................................................... 18
1.3.2 Molecular markers of PGD ..................................................................................... 20
1.3.3 Prevention and management ................................................................................... 20
1.4 Ischemia reperfusion injury ............................................................................................ 23
1.5 Inter interleukin-10 in lung transplantation .................................................................... 23
1.6 The L-arginine/NO metabolism ..................................................................................... 25
1.6.1 L-arginine synthesis ................................................................................................ 25
1.6.2 L-arginine transport ................................................................................................ 26
1.6.3 L-arginine catabolism ............................................................................................. 26

v
1.6.4 Arginase .................................................................................................................. 28
1.6.5 Nitric oxide synthase............................................................................................... 28
1.6.6 Nitric oxide ............................................................................................................. 28
1.6.7 L-arginine bioavailability........................................................................................ 29
1.6.8 Asymmetric dimethylarginine ................................................................................ 30
1.7 Rationale......................................................................................................................... 33
1.8 Hypothesis ...................................................................................................................... 35
1.9 Specific aims .................................................................................................................. 35
1.9.1 Specific aim 1 ......................................................................................................... 35
1.9.2 Specific aim 2 ......................................................................................................... 36
Chapter 2: Materials and Methods ............................................................................................ 37
2.1 Lung transplantation ....................................................................................................... 38
2.1.1 Animals ................................................................................................................... 38
2.1.2 Anesthesia ............................................................................................................... 38
2.1.3 Brain death .............................................................................................................. 38
2.1.4 Lung retrieval .......................................................................................................... 39
2.1.5 Ex vivo lung perfusion ............................................................................................ 39
2.1.6 Ex vivo viral delivery .............................................................................................. 41

vi
2.1.7 Ex vivo evaluation of lung function during EVLP .................................................. 41
2.1.8 Evaluation of lung function after transplantation ................................................... 41
2.2 Biopsies .......................................................................................................................... 41
2.3 Homogenization ............................................................................................................. 42
2.4 Protein assay ................................................................................................................... 42
2.5 Sample preparation for liquid chromatography mass spectrometry............................... 44
2.6 LC/MS/MS ..................................................................................................................... 44
2.7 NO metabolite measurement .......................................................................................... 44
2.8 Quantitative polymerase chain reaction ......................................................................... 45
2.8.1 Assessing RNA yield and quality ........................................................................... 46
2.8.2 Complementary deoxyribonucleic acid .................................................................. 47
2.8.3 Real time PCR......................................................................................................... 47
2.9 Western blotting ............................................................................................................. 48
2.10 Arginase activity measurement ...................................................................................... 50
2.11 Statistics ......................................................................................................................... 51
Chapter 3: The L-arginine metabolic profile in lungs differs between donations after brain
death compared to prolonged cold ischemia. ................................................................................ 54
3.1 Abstract .......................................................................................................................... 55

vii
3.2 Introduction .................................................................................................................... 57
3.3 Study designs and experimental approach ..................................................................... 58
3.4 Results ............................................................................................................................ 62
3.4.1 Length of cold static preservation does not affect the levels of L-arginine and its
metabolites ............................................................................................................................. 62
3.4.2 Reperfusion of lungs from bran death donor after 24 hours cold ischemia results in
different L-arginine and L-citrulline levels compared to lungs from non brain death donors
after 30 hours of hypothermic preservation ........................................................................... 66
3.5 Discussion ...................................................................................................................... 71
Chapter 4: NO metabolite and L-citrulline concentrations are decreased after EVLP
independent of IL-10 gene therapy and remain decreased after transplantation. ......................... 75
4.1 Abstract .......................................................................................................................... 76
4.2 Introduction .................................................................................................................... 78
4.3 Study designs and experimental approach ..................................................................... 79
4.4 Results ............................................................................................................................ 83
4.4.1 Length of cold ischemia time does not affect L-arginine metabolism.................... 83
4.4.2 EVLP decreases NOx concentrations in lung tissue. .............................................. 85
4.4.3 NOx is decreased after lung transplantation and reperfusion following EVLP or
EVLP+IL-10 .......................................................................................................................... 93
4.5 Discussion ...................................................................................................................... 97

viii
4.5.1 Cold ischemia does not cause alteration in the L-arginine/NO metabolism ........... 97
4.5.2 NOx and L-citrulline in lung tissue decrease after EVLP and remained below
normal after reperfusion ........................................................................................................ 98
Chapter 5: Discussion, conclusion and future directions........................................................ 104
5.1 Regulation of NO production ....................................................................................... 105
5.1.1 NOS expression and activity ................................................................................. 105
5.1.2 ADMA an endogenous NOS inhibitor .................................................................. 106
5.1.3 L-arginine availability for NOS ............................................................................ 106
5.1.4 Arginase expression and activity .......................................................................... 107
5.2 Other possible causes for decreased NOx and L-citrulline .......................................... 107
5.3 Interleukin (IL)-10........................................................................................................ 109
5.4 Conclusions .................................................................................................................. 109
5.5 Future directions ........................................................................................................... 110
References ................................................................................................................................... 112
Appendix ..................................................................................................................................... 133

ix
List of Abbreviations
0h CIT Time of harvesting
30h CIT/1h post rep One hour after reperfusion in the non brain death group
30h CIT 30 hours after cold ischemia
6h CIT 6 hours after cold ischemia
ABH 2(S)-amino-6-boronohexanoic acid
ACTH Adrenocorticotropic hormone
ADC Arginine decarboxylase
ADH Anti-diuretic hormone
ADMA Asymmetric dimethylarginine
ALI Acute lung injury
AM Alveolar macrophage
ANOVA Analysis of variance
ARDS Acute respiratory distress syndrome
ASS Argininosuccinate synthetase
ASL Argininosuccinate Lyase
ATP Adenosine tri-phosphate
AUC Area under the curve
BAL Bronchoalveolar lavage
BCP 1-Bromo-3-choloro-propane
BD Brain death
BD+24h CIT Cold ischemia time in the brain death group (24 hours)

x
BD+24h/1h post rep One hour after reperfusion in the brain death group
BH4 Tetrahydrobiopterin
BOS Bronchiolitis obliterans syndrome
BSA Bovine serum albumin
BUN Blood urea nitrogen
CAT Cationic amino acid transporter
CCL2 Chemokine CC motif ligand 2
cDNA Complementary DNA
CF Cystic fibrosis
CIT Cold ischemia time
cNOS Constitutive NOS
COPD Chronic obstructive pulmonary diseases
CPB Cardiopulmonary bypass
CPR Cardiopulmonary resuscitation
CRP C-reactive protein
CVA Cerebrovascular accident
CXC 10 Chemokines motif ligand 10
DC Dendritic cells
DCD Donors after cardiac death
DDAH Dimethylarginine dimethylaminohydrolase,
DEPC Diethylpyrocarbonate
DIC Disseminated intravascular coagulation

xi
DTT Dithiothreitol
ECMO Extracorporeal membrane oxygenation
ED Emergency department
EDTA Ethylenediaminetetraacetate
eNOS Endothelial nitric oxide synthaes
EVLP Ex vivo lung perfusion
FAD Flavin adenine dinucleotide
FeNO Fractional exhaled nitric oxide
FiO2 Fraction of inspired oxygen
FMN Flavin mononucleotide
HPLC-MS High-performance liquid chromatography mass spectrometry
I/R Ischemia- reperfusion
ICP Intracranial pressure
ICU Intensive care unit
IFN Interferon
IL Interleukin
iNOS Inducible nitric oxide synthase
IP-10 Inducible protein 10
IPF Idiopathic pulmonary fibrosis
ISHLT International Society for Heart and Lung Transplantation
ISPF α-Isonitrosopropiophenone
LA Left atrium

xii
LC/MS/MS Liquid chromatography-tandem mass spectrometry
LPDG Low-potassium dextran glucose
LTx Lung transplantation
MCP Monocyte chemotactic protein
MMA Mono-methylarginine
mRNA Messenger RNA
NADPH Nicotinamide adenine dinucleotide phosphate
NF-κB Nuclear factor- κB
nNOS Neuronal NOS
NO Nitric oxide
NO2- Nitrite
NO2 Nitrogen dioxide
NO3- Nitrate
NOS Nitric oxide synthase
NOS1 (= nNOS) Neuronal NOS
NOS2 (= iNOS) Inducible NOS
NOS3 (= eNOS) Endothelial NOS
NOx Nitric oxide metabolites
NPE Neurogenic pulmonary edema
OAT Ornithine aminotransferase
OD Optical density
ODC Ornithine decarboxylase

xiii
OPTN Organ Procurement and Transplantation Network
OTC Ornithine carbamoyltransferase
OTC Ornithine transcarbamoylase
PA Pulmonary artery
PaO2 partial pressure of oxygen in arterial blood
PGD Primary graft dysfunction
PI Protease inhibitor
PMSF Phenylmethylsulfonyl fluoride
PO2 Oxygen pressure
PRMT Protein arginine methyltransferases
PV Pulmonary vein
PVR Pulmonary vascular resistance
REP Reperfusion
RNA Ribonucleic acid
ROS Reactive oxygen species
RPM Rate per minute
q-PCR Quantitative polymerase chain reaction
sCR1 Soluble complement receptor-1 inhibitor
SDMA Symmetric dimethylarginine
SDS Sodium dodecyl sulfate
SEM Standard error of mean
SLC7 Solute carriers 7

xiv
SNO S-nitrosothiol
sRAGE Soluble receptor for advanced glycation end-products
T3 Tri iodothyronine
TGH Toronto General Hospital
TNF Tumor necrosis factor
TOH Time of harvesting
TRALI Transfusion-related lung injury
TSH Thyroid stimulating hormone
V/Q Ventilation perfusion ratio
VEGF Vascular endothelial growth factor
vWF Von Willebrand factor

xv
List of Figures
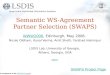
Figure 1-1: A, Number of patients on the transplantation waiting list for all organs is much
higher than organ donors in Ontario;6 B, Number of patients on lung transplantation waiting list
is higher than number of lung donors in Canada.7 .......................................................................... 3
Figure 1-2: Brain death can induce systemic inflammatory responses by 1- Metabolic and
hormonal changes, 2- Catecholamine storm, 3- Neuropeptides, 4- Circulating inflammatory
mediators.31
..................................................................................................................................... 7
Figure 1-3: Schematic of ex vivo lung perfusion (EVLP) circuit.14
............................................. 14
Figure 1-4: Balance of the L-arginine/NO metabolism by NOS and arginase.99
......................... 27
Figure 1-5: Biological effects of nitric oxide.116
NO plays essential roles in several physiological
responses. ...................................................................................................................................... 32
Figure 2-1: Protocol for measurement of arginase activity in tissue homogenates according to
Corraliza. 172
.................................................................................................................................. 52
Figure 3-1: Pig lung transplantation study designs. The study was designed to investigate the
effects of different lung preservation time and conditions on the L-arginine/NO metabolism. ... 61
Figure 3-2: Different length of cold ischemia time does not affect the levels of amino acids or
ADMA in donor lungs (one way ANOVA). ................................................................................. 63
Figure 3-3: A, The L-arginine metabolism by arginase and NOS; B, Decreased L-ornithine/L-
citrulline ratios in donor lungs were observed after 6 h cold ischemia time (6h CIT) but not 30h
CIT; *p<0.05, one way ANOVA, Tukey's multiple comparison test. ......................................... 67
Figure 3-4: A, Comparing the brain death and non brain death groups, before transplantation L-
citrulline was higher in the brain death group, but after transplantation and reperfusion L-

xvi
citrulline was higher in the non brain death group ; B, L-ornithine/L-citrulline ratio is higher after
transplantation and reperfusion in the brain death group; C, L-arginine after transplantation and
reperfusion decreases in the brain death groups (unpaired t test). ................................................ 70
Figure 4-1: Pig lung transplantation study designs. The study was designed to investigate the
effects of EVLP and IL10 gene therapy during EVLP on the L-arginine/NO metabolism. ......... 81
Figure 4-2: Different length of cold ischemia has no effect on NOx concentration or expression
of iNOS, arginase 1 or arginase2 mRNA in lung tissue (Kruskal-Wallis test). ............................ 84
Figure 4-3: Concentrations of NOx and L- citrulline was decreased after EVLP (* p<0.05,
Kruskal-Wallis test, Dunn's multiple comparison test); A, NOx (mol/g protein); B, L-citrulline
(nmol/mg protein). ........................................................................................................................ 87
Figure 4-4: EVLP does not affect iNOS expression but increases arginase1 and arginase2 mRNA
expression in lung; * p<0.05, Kruskal-Wallis test, Dunn's multiple comparison test. ................. 90
Figure 4-5: NOx and L-citrulline levels decrease after lung transplantation and reperfusion while
global L-arginine availability increases (* p<0.05, Kruskal-Wallis test, Dunn's multiple
comparison test). ........................................................................................................................... 95
Figure 4-6: Arginase1 and arginase2 mRNA expression is not different in recipient left lung
compared to 0h CIT (unpaired t test). Arginase1 and arginase2 mRNA expressions increase after
lung transplantation and reperfusion (**p<0.01; * p<0.05, Kruskal-Wallis test, Dunn's multiple
comparison test). ........................................................................................................................... 96

xvii
List of Tables
Table 1-1: Traditional criteria for selection of donor lung for lung transplantation.8, 9
................. 4
Table 1-2: Modified Maastricht classification of DCD.11
.............................................................. 9
Table 1-3: Grading schema of primary graft dysfunction according to the International Society
for Heart and Lung Transplantation (ISHLT).61
........................................................................... 17
Table 1-4: Possible risk factors for primary graft dysfunction.65
................................................. 19
Table 1-5: Biomarkers which have been studied for prediction of primary graft dysfunction.60
. 21
Table 1-6: Indicators of L-arginine/NO metabolism .................................................................... 31
Table 2-1: Composition* of STEEN solution™
163 ...................................................................... 40
Table 2-2: Volume and concentration of standard solution for protein estimation. ..................... 43
Table 2-3: Details of antibody used for Western blotting. ............................................................ 49
Table 2-4: Volumes and concentrations of standard solution for arginase activity measurement 53
Table 3-1: Lung amino acid and ADMA levels at different time points in the brain death and non
brain death groups ......................................................................................................................... 64
Table 3-2: Indices of L-arginine bioavailability and NOS impairment in lung at different time
points in the brain death and non brain death groups ................................................................... 65
Table 4-1: Expression of arginases and iNOS mRNA in lungs at different time points in the
“EVLP” and “no EVLP” groups. .................................................................................................. 88
Table 4-2: Concentrations of amino acids and ADMA in lung at different time points in the
“EVLP” and “no EVLP” groups and in recipient left lungs. ........................................................ 89

xviii
Table 4-3 Indices of L-arginine bioavailability and NOS impairment in lungs at different time
points in the “EVLP” and “no EVLP” groups and in recipient left lungs .................................... 91
Table 4-4: Lung NOx concentrations and in vitro arginase activity in “EVLP” and “no EVLP”
groups and in recipient left lungs. ................................................................................................. 92

1
Chapter 1: Background & Introduction

2
1.1 Lung transplantation
Lung transplantation is considered an ultimate treatment for end-stage pulmonary disease
including chronic obstructive pulmonary diseases (COPD), idiopathic pulmonary fibrosis (IPF)
and cystic fibrosis (CF).1 The first successful lung transplantation was performed at the Toronto
General Hospital by Dr. Joel Cooper in 1983.2 Modern techniques of preservation resulted in
improvement of post-transplantation outcomes and median survival.1, 3
In general, based on the Organ Procurement and Transplantation Network (OPTN) data as of
June 21, 2013, brain death donors are the main source for all organ donations.4 However, the
outcomes of organ transplantation from living donors are better in comparison to brain death
donors.5 According to Trillium Gift of Life Network
6 and the Canadian Institute for Health
Information (CIHI)7 the number of organ donors is much lower than the number of patients on
the waiting lists for organ transplantation (Figure 1-1), resulting in progressively longer waiting
lists. In addition, the majority of retrieved lungs from deceased donors do not fulfill traditional
criteria for lung transplantation4 as highlighted in Table 1-1.
8, 9 Different approaches have been
taken in order to expand the donor pool such as improving the rate of organ donation or using
marginal organs.3 Today, donations after cardiac death (DCD) are considered alternative sources
for organ donation.3, 10, 11
Additionally, modern methods of organ preservation, such as
normothermic ex vivo preservation, could improve the quality of marginal organs to fulfill
transplantation criteria.12-26
These techniques also provide the opportunity for evaluation of organ
function and therapeutic modifications before transplantation.12-26
Nevertheless, short and long
term complications following organ transplantation such as primary graft dysfunction (PGD),
infection, malignancy, and bronchiolitis obliterans (BO) still are serious causes of morbidity and
mortality.27
The mechanisms of these complications are complicated and incompletely
understood. Understanding the alteration in metabolic pathways, for example the L-arginine/NO
metabolism, during and after each step in transplantation could provide additional keys to assess
donor lung, improve the quality of donor organ and predict post-transplant outcomes.

3
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
0
500
1000
1500
2000
2500Waiting list
Donor
A: All organs
Pate
ints
nu
mb
er
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
0
100
200
300
400Waiting list
Transplant
B: Lung
Pate
ints
nu
mb
er
Figure 1-1: A, Number of patients on the transplantation waiting list for all organs is much
higher than organ donors in Ontario;6 B, Number of patients on lung transplantation waiting list
is higher than number of lung donors in Canada.7

4
Table 1-1: Traditional criteria for selection of donor lung for lung transplantation.8, 9
Age, 55 years or less
Blood group compatibility
Clear chest radiography
PaO2 ≥300 mm Hg on FiO2=1.0, 5cm H2O PEEP
Smoking history, 20 pack years or less
No chest trauma
No evidence of aspiration at broncoscopy
No evidence of sepsis
No microbiologic endobronchial organisms
No purulent secretions at bronchoscopy
No evidence of viral infections i.e. HIV, hepatitis B or hepatitis C
No history of cardiopulmonary surgery
No active malignancy
No history of chronic pulmonary disease
HIV, human immunodeficiency virus; PaO2, partial pressure of oxygen in arterial blood; FiO2,
fraction of inspired oxygen; PEEP, positive end expiratory pressure.

5
1.1.1 Brain death donors
Brain death is defined as an irreversible total loss of brain stem function.5 Depending on the
damages to different parts of the brain stem, brain death causes distinctive physiological
responses.5, 28
It triggers sympathetic storm, inflammatory responses, metabolic modifications
and endocrine changes which cause injuries in the donor organs and result in further
complications after transplantation such as ischemia reperfusion (I/R) injury.5, 28, 29
Damages in
the brain stem result in serious hemodynamic instability.5, 29, 30
Brain death is associated with
transient hypertension and bradycardia, followed by a rapid release of catecholamines which is
known as the catecholamine storm. The catecholamine storm can result in: 5, 29, 30
1- Intestinal ischemia which can consequently release cytokines.
2- A shift to anaerobic metabolism and consequently activation of nuclear factor- κB (NF-κB).
3- Flow-induced shear stress of the endothelial cells.
Avlonitis et al. summarized different theories and mechanisms which were described for the
pathogenesis of lung injuries after brain death. 5 Central nervous system injuries after brain death
lead to α-adrenergic stimulation which causes systemic vasoconstriction and consequently
increased systemic vascular resistance, decreased left ventricular output and increased left atrial
pressure. Simultaneously, due to systemic vasoconstriction, a large volume of blood moves to the
pulmonary circulation and results in acute pulmonary artery hypertension.5 Acute immense
alterations in pulmonary capillary pressure lead to damages to the capillary endothelium.5 The
structural damages in addition to elevated hydrostatic pressure lead to pulmonary edema.5
After a few minutes, in the next phase, vascular tone, cardiac output and peripheral resistance
decrease extremely. These changes result in hypotension and extensive reduction in organ
perfusion, predominantly in abdominal organs.5, 28
Anaerobic metabolism as a result of poor
oxygenation causes acidosis, increased levels of free fatty acids and subsequently reduction in
insulin secretion and hyperglycemia.30
In liver, hepatic sinusoidal perfusion decreases and
glycogen depletes.29
Peripheral vasodilatation, drop in metabolic rate, loss of muscular activity,
and damages to the hypothalamic temperature control after brain death cause hypothermia.29
The

6
activation of coagulation pathways, as a result of tissue thromboplastin released by brain necrotic
tissue, might lead to disseminated intravascular coagulation (DIC).29
The most susceptible organ
to the damaging effects of brain death is the lung.31
The rate of rejection and bronchiolitis
obliterans is higher in lungs that were transplanted from donors with traumatic brain injury
compared to non traumatic brain injury as a result of neuroimmunologic effects.30
Currently only
about 20 % of donor lungs satisfactorily meet criteria for transplantation.16, 22, 32
Neurogenic
pulmonary edema (NPE), a common lung injury following brain death, is one of the
complications which occurs following intracranial injuries.5, 29
Hydrostatic forces and
inflammatory responses make the lungs vulnerable to NPE.5, 29
In lung tissue, high pulmonary
capillary pressure may cause direct damages to the endothelial bed.5, 29
These changes could make the lungs susceptible to NPE.5, 29
Although the catecholamine storm
leads to changes in the permeability of pulmonary capillaries, the mechanisms involved in NPE
are incompletely understood.31
Brain death also leads to remarkable endocrine changes mainly
by anterior and posterior pituitary failure and disruption of the hypothalamic pituitary axis.5, 28, 29
In the vast majority of brain stem dead organ donors, early reduction in blood levels of anti-
diuretic hormone (ADH) results in diabetes insipidus.28, 29
Cortisol blood levels decrease
considerably due to the failure of the anterior lobe of the pituitary gland to secrete
adrenocorticotropic hormone (ACTH) after brain death, which plays a role in donor stress
response impairment.29
A drop in plasma level of insulin following brain death causes
intracellular glucose reduction.5, 28-30
A decline in thyroid stimulating hormone (TSH) blood level
after brain death leads to a decrease in free plasma tri-iodothyronine (T3).5, 28, 29
These
hemodynamic and hormonal alterations trigger extensive cellular and mitochondrial metabolic
dysfunction, initiating anaerobic metabolism and lactic acidosis followed by the production of
destructive enzymes and reactive oxygen species (ROS) which can be enhanced by cold
ischemia and reperfusion.5, 28, 29
Systemic immunologic responses and inflammation are induced by brain death via several
mechanisms (Figure 1-2).5, 31
In animal models, levels of circulating inflammatory mediators
such as cytokines increase after brain death.31
In humans, the serum level of interleukin (IL)-6

7
Figure 1-2: Brain death can induce systemic inflammatory responses by 1- Metabolic and
hormonal changes, 2- Catecholamine storm, 3- Neuropeptides, 4- Circulating inflammatory
mediators.31

8
increases sharply after brain death, which is associated with an increase in C-reactive protein
(CRP) levels in serum.5, 31
Increased levels of inflammatory mediators in donor organs are
correlated with poor outcomes after transplantation.31
For instance, the mRNA expression of IL-
6 and cytokines such as tumor necrosis factor (TNF)-α in donor lungs are known to predict
recipient mortality in the first 30 days after lung transplantation.33
The nervous system also
releases neuropeptides after brain death, which can induce systemic inflammatory response.31
In addition, the etiology and mechanisms of brain death – such as trauma and cerebrovascular
accident (CVA), the management and treatment strategies before and after brain death such as
mechanical ventilation, cardiopulmonary resuscitation (CPR) and other concurrent incidents such
as aspiration and pneumonia – also may be involved in triggering inflammatory responses.31
Activation of proinflammatory mediators, endothelial cells and platelets in organs after brain
death, make them more prone to the recipient’s immune system.29
Therefore, the risk of acute
rejection of organs from brain death donors is higher when compared with organ transplantation
from living donors.29
1.1.2 Donation after cardiac death
The demand for organ transplantation has increased tremendously.7 Marginal cadaveric donors
including obese, elderly, and non-heart beating donors are considered potential sources of
organs.3, 34
Lungs harvested from DCD are now accepted as an alternative source for lung
transplantation.3 Death in donors after cardiac death is confirmed by using circulatory criteria. In
1995 in Maastricht at the first international workshop on DCD, the Maastricht categories of
donations after cardiac death were introduced.10
Currently, the modified Maastricht classification
is commonly applied to classify DCD (Table 1-2).11
Uncontrolled DCD, including categories I
(dead on arrival), II (unsuccessful resuscitation), and V (unexpected arrest in ICU patient), refers
to retrieval of donor organ following an irreversible and unexpected cardiac arrest, whereas
controlled DCD categories III (anticipated cardiac arrest) and IV (cardiac arrest in a brain-dead
donor) indicate organ retrieval subsequent to planned removal of cardiorespiratory support
system.11

9
Table 1-2: Modified Maastricht classification of DCD.11
Category Description
I, uncontrolled Dead on arrival to hospital
II, uncontrolled Dead after unsuccessful resuscitation
III, controlled Cardiac arrest in whom treatment withdrawal is planned
IV, controlled Cardiac arrest in brain-dead patients
V, uncontrolled Unexpected cardiac arrest of admitted patients in hospital
ICU; intensive care unit.

10
The warm ischemic period, which is the time between the beginning of asystole and the start of
cold perfusion in organs from controlled DCD is longer in brain death donors.3, 11
In uncontrolled
DCD warm ischemia can be even longer than controlled DCD at the retrieval time.3, 11
Although
lungs which are kept inflated with oxygen seem to be less susceptible to warm ischemia than
other organs, a longer ischemic period increases the risks of primary graft failure.3, 11
Nonetheless, organs from DCD are not exposed to inflammatory responses and sympathetic
storm after brain death.11
Indeed, the outcomes of lung transplantation in controlled DCD donors
are predominantly better than brain death donors.3 Moreover, organs from DCD are not exposed
to the cardiopulmonary consequences of inflammatory responses after brain death, so lungs from
these donors therefore benefit more from ex vivo lung perfusion techniques.11
1.2 Preservation of harvested lung
1.2.1 Cold static preservation
Cooling down the organ is critical in preservation of organ function as hypothermia inhibits
cellular metabolic activity, the aerobic pathways, and enzyme activities.21, 26, 35
Cold static
preservation is a main part of lung preservation which results in lower metabolic activity to
maintain cell viability during ischemia. Six to 9 hours of cold static preservation is considered
optimal for harvested lungs in terms of maintaining post-transplantation pulmonary function
such as gas exchange.21
Nevertheless, the gold standard temperature for lung cold static
preservation is controversial. Generally lungs are kept at 4°C after retrieval; however, some
studies have suggested that lung preservation at 10°C resulted in better pulmonary function
compared to lungs stored at 4°C.26, 36, 37
On the other hand, hypothermia leads to cell injury and
destructive effects to the plasma membranes, microtubules and mitochondria which can lead to
serious physiologic disruptions.36, 37
ATPase activity, which is temperature dependent, decreases
following hypothermia.36
The decline in ATPase activity interrupts the cellular ATPase-
dependent ion balance, which results in membrane disruption, cellular edema and cell death.36
Low temperature in lung tissue causes an increase in extra vascular fluid, pulmonary
vasoconstriction and altered oxygen exchange.26, 36
It has been demonstrated that mechanical
properties of the lung including airway resistance and tissue elasticity of lung parenchyma were

11
altered after 9 hours of cold ischemic preservation in a rat model.38
In addition, it has been
shown that the innate immune system is activated after reperfusion in response to preservation
injuries, which consequently stimulates the adaptive immune system.26, 39
An improvement of the preservation process would ameliorate the long term outcomes of lung
transplantation.26
The chemical composition of preservation solutions plays a crucial role in
prevention of lung injuries during preservation.37
In the 1980s, lungs were flushed at 4C with
modified Euro-Collins solution and the rates of ischemia reperfusion injury and early mortality
were considerable.37, 40
Later on, studies on University of Wisconsin solution also did not
demonstrate remarkable clinical benefits.37, 41
The use of low-potassium dextran glucose (LPDG)
which is similar to extracellular fluids, considerably improved post-transplantation lung
function.42-44
In addition, LPDG also decreases the rate of severe primary graft dysfunction.37
In
1990s Perfadex
and Celsior
were introduced as LPDG.37
1.2.2 Ex vivo perfusion
Ex vivo organ perfusion was reported in 1935 by Carrel and Lindbergh. They demonstrated that
organs, such as kidney and heart, were capable of keeping cell proliferation and function for
several days while kept in an ex vivo organ perfusion system.45
These ex vivo organ perfusion
settings were used primarily for research in physiology. 45
In 2003 Steen et al. used ex vivo lung
perfusion for the evaluation of lung function from DCD.46
Afterwards, ex vivo lung perfusion
was used for transplantation of initially rejected lung.16
Generally, an ex vivo artificial perfusion system can provide continuous oxygen and nutrient
supply to accomplish the organ’s metabolic requirements and remove the metabolic waste
materials and toxins to maintain a physiologic environment.12, 13, 23, 32
It also renders a constant
circulation to maintain the micro-circulation.34
Currently, the ex vivo organ perfusion is an
alternative method in organ preservation.26, 35
Three methods of ex vivo reperfusion has been
described, hypothermic, normothermic and subnormothermic perfusion. In hypothermic
perfusion organs are kept at 4 to 10°C. Therefore, organs benefit from a low metabolic rate and
lower demand of oxygen and essential nutrients in addition to the benefits of ex vivo organ

12
perfusion.35
However, the risk of shear stress increases due to the rigidity of the endothelium,
high viscosity of the solution at low temperatures, and the swelling of the endothelial cells due to
Na/K pump dysfunction.47
In normothermic perfusion the organs were kept at 37ºC. Thus, organs can be protected from
both ischemia and hypothermia; subsequently, tissue injuries during the preservation period can
be minimized.13, 35
Injury to the grafted organ depends on the duration of the cold ischemia
period. Direct effects of cooling are avoided in normothermic perfusion. Theoretically,
normothermic systems extend the duration of organ storage without increasing the risk of tissue
damage.34, 35
Normothermic techniques can reverse injuries sustained by warm and cold
ischemia. It improves the quality and condition of the graft from both brain death donors and
DCD.34, 48
Tissue repair can be started in the physiologic environment provided by normothermic
perfusion systems.34, 35
Viability parameters can be assessed during the preservation period. In
addition, normothermic perfusion systems can decrease the risk of non-functioning grafts.35
Ex
vivo normothermic perfusion allows the opportunity for pharmacological interventions, such as
delivery of cytoprotective and immunoregulatory agents as well as gene therapy to the specific
organ itself without side effects on other organs.13
In subnormothermic perfusion the temperature is kept higher than hypothermic but lower than
normothermic perfusion systems (between 20-28C). Mitochondrial functions in subnormal
temperature are preserved while the side effects of normothermic reperfusion are avoided.
However, more investigation is needed to substantiate this finding.35
Disadvantages of the ex vivo reperfusion include:
1- The endothelium could be injured by the perfusion flow itself.
2- Risk of bacterial contamination in ex vivo perfusion methods especially in normothermic
perfusion system is higher than cold static preservation.47
3- The perfusion devices are relatively complicated and unmovable; therefore, the organ must be
preserved in cold static preservation to be transported to a transplant center.13

13
4- Perfusion machines are not user friendly and personnel must be specifically trained.
5- The operation of perfusion devises and their maintenance are relatively expensive.13
1.2.2.1 Ex vivo lung perfusion (EVLP)
Ex vivo lung perfusion (EVLP) is a novel strategy which expands the time of preservation and
provides the chance for evaluating lung function.17, 46
Post-transplantation outcomes in recipients
of lungs after EVLP are similar to recipients of lungs after standards lung preservation.12
In
addition, EVLP could provide the opportunity for recovery of lung tissue and possible medical
interventions before transplantation.12, 14, 17, 20
In EVLP lung circulation is re-established by a
centrifugal pump while the lung is ventilated by a ventilator (Figure 1-3).14
Modern ex vivo lung perfusion was developed by the Steen group to evaluate lung function from
DCD.46
In 2005 Steen et.al. reconditioned an initially rejected lung using EVLP and transplanted
a single lung in a human successfully.49
Later, their group reported the first six double lung
transplantations using EVLP to recondition donor lungs initially rejected for transplantation.50
Cypel et al. for the first time described a reliable technique for long-term (12 h) ex vivo lung
perfusion which resulted in excellent lung function during EVLP and after transplantation.14
Lung oxygenation post-transplantation is improved significantly in lungs that went through
EVLP compared to lungs preserved at low temperatures.12, 14, 20, 22
Adenosine triphosphate (ATP)
levels in the lung tissue are improved by EVLP resulting in recovery of marginal donor lungs.12,
20 Tissue level of ATP, which represents lung tissue energy level, decreases after warm ischemia.
Four hours of EVLP causes a significant increase in ATP level in lung tissue.20
In addition, the
rate of lung edema formation following transplantation is lower in lungs which underwent EVLP
than after cold static preservation.17, 19
To improve pulmonary edema surgeons can use a
perfusate solution with physiologic osmolarity and high oncotic pressure. 19, 23

14
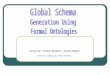
Figure 1-3: Schematic of ex vivo lung perfusion (EVLP) circuit.14
A centrifugal pump (1) circulates the perfusate to a membrane for gas exchange (2) and a filter
(3) for leukocyte removal. The perfusate enters into the lung through the pulmonary artery. It is
collected from the left atrial cannula to a reservoir (4). The lungs are kept in a specifically
designed lung enclosure (XVIVO, Vitrolife) while ventilated with a standard ICU-type ventilator
(5).

15
In a pig model of lung transplantation PVR in lungs after 10 hours of brain death followed by 24
hours of cold ischemia, at the beginning of EVLP, was significantly higher than in control lungs
harvested from living donors followed by one hour of cold ischemia before EVLP.25
However,
PVR was decreasing during EVLP and it was measured close to the level of PVR in the control
group after 12 hours of EVLP.25
In addition, the analysis of data for pulmonary artery (PA)
pressure during EVLP in the same animals demonstrated that PA pressure decreases significantly
after 6 hours and 12 hours of EVLP compared to the beginning of EVLP in the “EVLP+IL-10”
group (Dr. Keshavjee’s lab, not published).
Lung function during EVLP can be assessed using pulmonary dynamic compliance, flow rate,
pulmonary artery pressure, peak inspiratory pressure, resistance of small airways and blood
gas.12, 18, 23
Therefore, EVLP potentially provides reliable criteria to predict lung function after
transplantation.12, 20, 23
Assessment of biological markers in perfusate, bronchoalveolar lavage
fluid or lung tissue can help surgeons reassess the lung carefully in order to avoid transplanting
an injured lung which is initially considered transplantable, or discarding a lung which is initially
considered non-transplantable.12, 18, 20, 23, 51
Metabolic biomarkers are more sensitive indices than
physical parameters for evaluating lung quality and function.52
For example, the concentration of
lactate in perfusate increases during EVLP in a pig model.53
Lactate is cleared from the
circulation by other organs such as muscles, kidney and liver which are not available in EVLP
settings.53
In a pig model of EVLP, Valenza et al. showed that lung function was reduced in
lungs with higher utilization of glucose during EVLP. They discussed that metabolic rate and
glucose consumption in organs with inflammation is higher than in normal organs, thus the
metabolic rate of glucose could be used as a biomarker for evaluating lung quality.54
EVLP renders the opportunity to perform therapeutic interventions to the isolated lung tissue.23
Medications could be administered through the perfusate. For example, it has been shown that
the administration of dibutyryl cyclic adenosine monophosphate (db-cAMP) and nitroglycerine
to the perfusate improved post-transplant lung function.20
Moreover, medical interventions could
be performed through the airways. For instance, it has been demonstrated that inhaled NO or
carbon monoxide during EVLP can improve lung function.55, 56

16
As the cellular metabolisms are maintained in lung tissue during EVLP, isolated therapeutic
interventions can be performed before transplantation to the lung tissue to avoid side effects to
other organs.16
For instance, pulmonary embolisms can be treated without the risk of bleeding or
high dose antibiotics can be provided to the isolated lung without the risk of intoxicating other
organs.57, 58
Half-lives of medications that are cleared by the liver and kidneys are prolonged in
the EVLP system.16
Moreover, novel therapeutic strategies such as stem cell therapy and gene
therapy can also be applied in the isolated lung without life threatening side effects on other
organs such as liver or kidney.16
1.3 Primary graft dysfunction (PGD)
PGD is a type of severe acute lung injury (ALI) that develops following allograft lung
transplantation.1, 59, 60
Non-cardiogenic pulmonary edema within the first 72 hours following
transplantation with no other secondary causes is considered PGD.1 The pathogenesis of PGD is
multifactorial. Ischemia-reperfusion is considered the main cause of PGD.1, 60
However, other
factors during the transplantation process such as inflammatory events, surgical trauma, and
lymphatic disruption may play a role in PGD as well.60
PGD is the most common cause of early
death following transplantation.59
In recipients with severe PGD, mortality rates in the first
month after lung transplantation are up to eightfold higher compared with patients without
PGD.60
Moreover, the risk of chronic allograft rejection and BOS is significantly higher in PGD
survivors.60
PGD is diagnosed based on the presence of radiographic opacities in the transplanted
lung(s) within 72 hours of transplantation, hypoxemia and absence of secondary etiology such as
pneumonia, atelectasis, volume overload, obstruction of pulmonary vein outflow and rejection.59
Diffuse microscopic alveolar damage in PGD results in decreased lung compliance and severely
impaired oxygenation.60
Diffuse pulmonary infiltrates can be found in radiographic images,
comparable to patients with acute respiratory distress syndrome (ARDS).59
The International
Society for Heart and Lung Transplantation (ISHLT) suggested a definition and grading system
for PGD in 2005. This grading is based on the ratio of partial pressure of oxygen in arterial blood
(PaO2) over fraction of inspired oxygen (FiO2) and the assessment of chest infiltrates at time
points up to 72 hours (Table 1-3).61
It has been shown that the length of stay in intensive care

17
Table 1-3: Grading schema of primary graft dysfunction according to the International Society
for Heart and Lung Transplantation (ISHLT).61
Grade PaO2/FiO2 ratio
0 >300 No evidence for pulmonary edema on chest X-ray
1 >300 Signs of pulmonary edema on chest X-ray
2 200–300 Signs of pulmonary edema on chest X-ray
3 <200 Signs of pulmonary edema on chest X-ray
Time points for assessment: 0, 6, 24, 48, and 72 hours after reperfusion. PaO2; partial pressure of
oxygen in arterial blood, FiO2, fraction of inspired oxygen.

18
units (ICU) and hospitals plus short-term and long-term mortality, were significantly higher in
patients with a PaO2/FiO2 ratio <200 within 48 hours after lung transplantation. The long-term
survival in PGD grades 1 and 2 was not significantly different.60
1.3.1 Risk factors for PGD
All components of the lung transplant procedure, including donor’s cause of death, changes in
donor hemodynamics, hypothermic preservation, surgical procedure and organ reperfusion, play
crucial roles in the development of PGD (Table 1-4).60
Early detection of PGD in recipients is
important in the management of PGD. Understanding the biochemical factors and genetic
markers in donor lung and/or recipient that are associated with PGD can result in better donor-
recipient matching, facilitate early diagnosis and reduce risks of PGD, ultimately improving
outcomes of transplantation.60
1.3.1.1 Donor risk factor
Risk factors associated with PGD in donor lungs include the donor age, gender and race. The risk
of PGD is higher in lungs from donors older than 45 or younger than 21 years, females and
African-Americans.59, 60
In addition, low PaO2/FiO2 ratio, prolonged mechanical ventilation,
infection, trauma, smoking history, inflammatory response and hemodynamic instability in
donors after brain death are associated with higher incidence of PGD.59, 60
An increase in
interleukin-8 level in donor bronchoalveolar lavage (BAL) fluid is also associated with a higher
risk of severe PGD.59
1.3.1.2 Recipient risk factors
All studies, with the exception of one, regarding recipient-related risk factors for PGD following
lung transplantation were unable to demonstrate a significant correlation between PGD and
recipient age, gender, race, body weight, diabetes, hepatic failure, renal failure, left heart disease,
or medication use such as steroids.60, 62
In contrast, recipient pulmonary artery hypertension is
associated with a significantly higher risk of PGD.60, 63, 64
The risk of PGD is higher in recipients

19
Table 1-4: Possible risk factors for primary graft dysfunction.65
*The most consistently reported risk factors.
Category Risk Factor for PGD
Donor’s age >45* or <21
Donor’s race African American
Donor’s gender Female
Donor’s history of smoking >10 pack-years
Donor’s clinical conditions Prolonged mechanical ventilation, aspiration,
trauma, hemodynamic instability post–brain death
Recipient’s medical conditions Diagnosis of idiopathic pulmonary arterial
hypertension*, elevated pulmonary arterial pressure
at time of surgery*, diagnosis of diffuse
parenchymal lung disease
Pre and post-transplant conditions
Preservation solution and flush technique,
prolonged ischemic time*, use of cardiopulmonary
bypass, blood product transfusion

20
with higher mean pulmonary arterial pressures at the time of surgery independent of primary
condition.60, 63
Diffuse parenchymal lung disease such as idiopathic pulmonary fibrosis is also
associated with higher risk of PGD.60, 62
The risk of PGD in recipients with COPD is the
lowest.60
1.3.1.3 Operative risk factors
As described earlier, the rate of severe PGD can be decreased by using LPDG.37
The use of
cardiopulmonary bypass (CPB) and blood products during and following lung transplantation is
associated with a higher risk of PGD development.60
Blood transfusion can lead to transfusion-
related lung injury (TRALI).60, 66
The clinical picture in TRALI and PGD is identical.60
The
association between the risk of PGD development and type of transplant procedure (single vs.
bilateral) has not been consistently demonstrated.60
Similarly, graft ischemic time has not been
shown to be an independent risk factor for PGD.59, 60
However, ischemic time beyond 6 hours
can be considered a risk factor for PGD.59
1.3.2 Molecular markers of PGD
A practical cost effective and universally accepted biomarker for the prediction of PGD which
can lead to earlier diagnosis has not been discovered. Several studies have investigated potential
biomarkers (Table 1-5). So far it has been shown that the ratio of interleukin IL-6/IL-10
expression is the most predictive factor of first month mortality.60
1.3.3 Prevention and management
1.3.3.1 Prevention
To prevent I/R injury and PGD, preservation techniques and components of preservation
solutions have been studied previously. The composition of preservation solution has been
optimized for longer ischemic times and better post-transplant lung function. Inhaled nitric
oxide (NO) is a selective and effective pulmonary vasodilator.67, 68
Although NO improves gas

21
Table 1-5: Biomarkers which have been studied for prediction of primary graft dysfunction.60
Biomarker
Chemokines MCP-1, CCL2 IP-10, CXC10, IFN-γ
Anti-inflammatory cytokines IL-13, IL-10
Proinflammatory cytokines IL-2R, TNF-α, IL-8, IL-6
Others VEGF, sRAGE, protein C, type I
plasminogen activator inhibitor, plasma
intercellular adhesion molecule-1, vWF
IL, interleukin; IP-10, interferon -inducible protein 10; CXC10, chemokines CXC motif ligand
10; MCP-1, monocyte chemotacticprotein-1; CCL2, chemokine CC motif ligand 2, sRAGE,
soluble receptor for advanced glycation end-products; TNF-α, tumor necrosis factor-alpha;
VEGF, vascular endothelial growth factor; vWF, von Willebrand factor.

22
exchange in patients with established PGD it is not considered an effective prophylactic agent.65,
69 The administration of NO at the onset or 10 minutes after reperfusion does not significantly
affect the incidence of PGD.65, 69
Other therapeutic interventions are also examined for PGD
prevention, for example, using the soluble complement receptor-1 inhibitor (sCR1) results in
earlier extubation after lung transplantation, shorter mechanical ventilation time and ICU stay.65,
70 Nonetheless, PaO2/FiO2 ratio was not improved significantly by sCR1.
65, 70 In human lung
transplantation, the administration of platelet-activating factor antagonist during flushing of the
lung and after reperfusion temporarily improves oxygenation scores and radiographic findings up
to12 hours.71
Many other investigations for the prevention of PGD are being performed in animal
models with new agents and innovative techniques.60, 65
1.3.3.2 Treatment
Treatment of severe PGD is supportive aiming to prevent barotrauma by using low-stretch
ventilation and restriction of fluid, similar to the management of patients with ARDS.59, 65
Severely ill patients can be effectively stabilized by inhaled NO and extracorporeal life support
in some situations.59
The effect of inhaled NO is controversial.72, 73
In some studies,
administration of inhaled NO improved the clinical picture of PGD72, 74
whereas other studies
showed patients with PGD did not benefit from inhaled NO.69, 72, 73
Generally, inhaled NO is
recommended in the management of PGD while its use is possibly reasonable in selected cases
of severe hypoxemia and/or pulmonary hypertension.65, 72, 73
However, the effect of inhaled NO
is transient.65, 75
Alveolar collapse following ischemia and reperfusion has been reported as a result of pulmonary
surfactant dysfunction.65, 75
It leads to ventilation-perfusion mismatch and decreased oxygenation
which can contribute to PGD.65, 75
Administration of exogenous surfactant in animal model of
PGD improved pulmonary compliance and oxygenation.65, 73, 76-78
In humans, exogenous
surfactant administration via bronchoscopy in patients with severe ischemia reperfusion injury
resulted in resolution of radiological infiltrates within 24 hours and improvement of survival
within 19 months.79
These strategies among other methods such as extracorporeal membrane

23
oxygenation (ECMO) and administration of N-acetylcysteine must be investigated for more
extensive use.65
1.4 Ischemia reperfusion injury
I/R related injuries can lead to acute and chronic graft dysfunction.80
I/R injury is a common
cause of morbidity and mortality after solid organ transplantation and occurs in up to 15% of
cases after lung transplantation.81
It has also been identified as a risk factor for bronchiolitis
obliterans.80, 82
In lung transplantation, I/R injury is characterized by nonspecific alveolar,
epithelial and endothelial cell dysfunction that occurs within 72 hours after transplantation
leading to ventilation-perfusion mismatch, lung edema and hypoxemia.72, 83
The mechanisms that
lead to I/R injury are incompletely understood, however I/R injury results in decreased tissue
perfusion due to an increase in vascular smooth muscle tone and vascular resistance.80
I/R injury in the lung occurs in two phases, an early and a late (delayed) phase.72, 84
In the early
phase, activation of donor alveolar macrophages (AM) have been described as a significant
contributor.72, 85, 86
The production of proinflammatory cytokines in the early phase of I/R injury
mainly by macrophages leads to subsequent activation of neutrophils and induction of the late
phase of I/R injury.72
In some cases the administration of inhaled NO, as an effective and selective pulmonary
vasodilator, is an essential treatment strategy in reperfusion and management of postoperative
graft dysfunction following heart or lung transplantation.67, 69, 87
In experimental rat lung
transplantation, I/R injury is associated with increased inducible nitric oxide synthase (iNOS)
expression and activity, while the activity of constitutive NOS was found to be decreased.88
1.5 Inter interleukin-10 in lung transplantation
IL-10 can be expressed and produced by different cells in both the innate immune system, such
as macrophages, and the adaptive immune systems, such as T helper-1cells.89
The effects of IL-
10 are mostly studied in animal models of infectious diseases. In all infectious models regardless
of the source of IL-10, it inhibits the function of macrophage and dendritic cells (DC).

24
Subsequently, it suppresses the response of T helper-1 and T helper-2 cells.90
IL-10 is an
important regulator of inflammatory responses.91
Recently, it has been shown that human IL-10
gene therapy reduced inflammation in injured human donor lung.16
In the setting of ischemia reperfusion injury, proinflammatory cytokines, such as IL-8 and IL-6,
and anti-inflammatory cytokines, such as IL-10, play significant roles in induction and/or
prevention of I/R injury.33, 92
Pro-inflammatory factors are considered risk factors for post-
transplantation mortality. 33
On the other hand, IL-10 is known as a protective factor.33
In donor
lung tissue, the ratio of IL-6/IL-10 before transplantation is recognized as an index for post-
transplantation mortality in recipients.33
In addition, when the level of IL-8 in the donor lung is
higher, the early lung function following lung transplantation is lower and recipient mortality
rate is increased.92
In the early phase of I/R injury, IL-10 is a strong inhibitor of production of
proinflammatory cytokines.92
IL-10 inhibits synthesis of pro-inflammatory cytokines such as
TNF-α by macrophages.93
It has also been shown that the administration of IL-10 in rat lung
transplantation reduced lung ischemia-reperfusion injury whereas anti IL-10 intensified lung
injury.93
Adenoviral IL-10 gene therapy is considered a novel strategy for reducing inflammation in lung
tissue before transplantation.15, 94
Gene therapy could abbreviate the process of recovery in
injured donor organs and reduce inflammation before transplantation.94
In a rat model, it has
been shown that in vivo human IL-10 gene therapy in donor lungs improved lung function.95
In
addition, in injured human lungs it has been demonstrated that ex vivo administration of human
IL-10 gene followed by 12 hour EVLP noticeably improved lung function.15
Human IL-10 gene
therapy in donor lungs leads to less inflammation, helps repair cytoskeletal structure and
enhances lung function. Subsequently, this approach could result in using organs which would
otherwise not be considered suitable for transplantation according to current criteria.15
Effective therapeutic levels of gene expression for reperfusion time were attained 6 to 12 hours
after the delivery of gene vector to the airways when the lungs were harvested from donors.96
In
humans in vivo gene therapy cannot be applied routinely due to important limiting factors such
as the inflammatory responses to the adenoviral vector and the side effects on other organs of the

25
donor.94
During cold static preservation ex vivo adenoviral gene therapy caused low level of gene
expression at the time of perfusion and after transplantation, which could be caused by
hypothermia.97
Normal temperature and preserved metabolic activity in addition to acellular
perfusion in isolated lung during EVLP provide the opportunity for effective gene expression,
limited inflammatory responses to the vector and better lung function before and after
reperfusion.15, 24
Fascinatingly, the acellular perfusate in EVLP flushes out the inflammatory
cells from the lung, thus immune responses to viral vector in EVLP are limited because of the
lack of neutrophils and inflammatory cells.16
1.6 The L-arginine/NO metabolism
In animal cells L-arginine (2-amino-5-guanidinovaleric acid) is a precursor for the production of
NO, L-citrulline, L-ornithine, urea, creatine, agmatine, polyamines, proline, glutamate, and
proteins. In healthy adult humans L-arginine is a non-essential amino acid.98
However; it is
considered essential during certain physiological conditions such as development and pregnancy
or pathological conditions such as sepsis or trauma.98
1.6.1 L-arginine synthesis
The supplies for plasma L-arginine are diet (exogenous), whole-body protein turnover and
synthesis from L-citrulline (endogenous).98, 99
Endogenous L-arginine synthesis changes
according to the developmental phase, nutritional condition and species.98
In adult humans 5 to
15% of L-arginine flux derives from de novo synthesis.98, 100
The intestinal-renal axis is
responsible for the main part of endogenous arginine synthesis.98, 100
Enterocytes convert
glutamine, glutamate and proline to L-citrulline or L-arginine.98-100
L-citrulline released by the
small intestine into the blood stream is predominantly absorbed and converted to L-arginine in
the proximal convoluted tubules of the kidney.98, 99
In addition, the liver and NO-producing cells
such as macrophages are able to produce L-arginine.98, 99

26
1.6.2 L-arginine transport
L-arginine, in mammalian cells, is transported into the cell by specific transmembrane
transporters, cationic amino acid transporters (CAT) such as systems y+, b
o,+, B
o,+ or y
+L.
98, 99
Cationic amino acids, lysine, ornithine and canavanine and positively charged analogues such as
certain nitric oxide synthase (NOS) inhibitors can competitively inhibit L-arginine transport.98, 99
In the majority of cell types, system y+ is the most essential transporter mechanism for L-lysine,
L-ornithine and L-arginine uptake.98
L-arginine transport systems regulates substrate availability
for L-arginine-catabolising enzymes.98
The ratio of L-arginine over L-ornithine and L-arginine
over L-ornithine + L-lysine can be used as indicators for intracellular bioavailability of L-
arginine for NOS at a given L-arginine concentration.98
Different cell types express different transporters which can be activated and regulated by
specific stimuli, such as inflammatory cytokines and bacterial endotoxin.98
The CATs including
CAT-1, -2A, -2B, -3 and -4 are part of the family of solute carriers 7 (SLC7).99, 101
At
physiological pH all CATs (except CAT-4) are selective, Na+-independent transporters.
101 CAT-
1 is expressed in all tissues except liver.99, 101
In the liver CAT-2A is mainly expressed, CAT-3 is
expressed during embryonic development in large quantities and in adults it is limited to brain
tissue.99, 101
Pro-inflammatory mediators such as lipopolysaccharide (LPS) and interferon-γ (IFN-
γ), which induce iNOS, up-regulate L-arginine uptake which is linked with CAT-2B up-
regulation.99, 101
1.6.3 L-arginine catabolism
The L-arginine metabolome (Figure 1-4) refers to the complete set of enzymes, metabolites and
inhibitors involved in the L-arginine/NO metabolism.102
L-arginine can be catabolised through
various pathways. In the same cell different L-arginine catabolising enzymes, for example, iNOS
and arginase can be co-expressed, which causes complicated interactions by which the activity of
one enzyme may be inhibited by the product of another.98
NOSs and arginases compete for the
same substrate, L-arginine.98, 99
Inhibition of arginase can cause increased NO and L-citrulline
production from NOS.103

27
Figure 1-4: Balance of the L-arginine/NO metabolism by NOS and arginase.99
ARG, arginase (EC 3.5.3.1); OTC, ornithine carbamoyltransferase (EC 2.1.3.3); ODC, ornithine
decarboxylase (EC 4.1.1.17); ADC, arginine decarboxylase (EC 4.1.1.19); NOS, nitric oxide
synthase (EC 1.14.13.39); OAT, ornithine aminotransferase 2.6.1.13); OTC, Ornithine
transcarbamoylase (EC2.1.3.3); ASS: argininosuccinate synthetase (EC 6.3.4.5), ASL:
argininosuccinate Lyase (EC 4.3.2.1), DDAH, dimethylarginine dimethylaminohydrolase;
ADMA, asymmetric dimethylarginine; NO, nitric oxide; PRMT, Protein arginine
methyltransferases.

28
The enzyme expression in different cells varies extensively. However, in almost any cell type
iNOS is expressed in response to an appropriate stimulus.98
1.6.4 Arginase
Arginase catabolizes L-arginine to L-ornithine and urea.98
In mammalian cells two isoforms of
the enzyme exist.98, 99
These two isoenzymes are coded by different genes.98, 99
Arginase 1 is a
cytosolic enzyme which is primarily expressed in liver.98
Arginase 2 is a mitochondrial enzyme
and is mainly expressed in the kidney.98, 99
However, both isoforms of arginases are expressed in
liver and other tissues including the lung.98, 99, 104
L-ornithine is a precursor for the production of
polyamines and collagen, both of which contribute to chronic tissue repair and remodelling.105-107
1.6.5 Nitric oxide synthase
Nitric oxide synthase (NOS) catabolises L-arginine to L-citrulline and NO.98, 99
Three genes
encode the different NOS isoenzymes.98
In the absence of inflammation NO is primarily
produced by the constitutive NOS (cNOS) isoenzymes, neuronal NOS (nNOS, NOS1) and
endothelial NOS (eNOS, NOS3).98, 108
In response to bacterial endotoxin and inflammatory
cytokines, inducible NOS (iNOS, NOS2) produces NO. iNOS is essential in acute and chronic
inflammatory responses.98, 108, 109
The activity of cNOS is regulated by Ca2+
/calmodulin, however
iNOS activity is not calcium-dependent.98
1.6.6 Nitric oxide
NOS isoforms produce NO from L-arginine in the presence of oxygen (O2), nicotinamide
adenine dinucleotide phosphate (NADPH), tetrahydrobiopterin (BH4), flavin adenine
dinucleotide (FAD), flavin mononucleotide (FMN) and heme.98, 99, 110, 111
NO production can be
regulated at the pre-transcriptional, transcriptional and post-transcriptional level.111, 112
NO plays
important roles in various physiological processes such as relaxation of smooth muscle,
inhibition of platelet aggregation, regulation of immune response and neurotransmission (Figure
1-5).73, 98, 99, 104, 113-117
NO is synthesized intracellularly.98
Alterations in the L-arginine/NO
metabolism have been shown in either acute or chronic pathological states in the lung.104, 113, 115,

29
118-123 The fraction of NO in exhaled air (FeNO) is a non-invasive indicator of airway
inflammation.124-126
FeNO decreases in airways in pathologic conditions such as COPD and
cystic fibrosis.124, 125
The L-arginine/NO metabolism is important in innate and acquired immunity and
inflammation.109
Most interestingly, the balance between NOS and arginase expression is crucial
in polarization and function of alveolar macrophages with iNOS being expressed by M1 and
arginase by M2 subtypes.127
Macrophages are able to convert their phenotype in response to
environmental stimuli, proinflammatory cytokines such as IL-8 and anti-inflammatory cytokines
such as IL-10. NO produced by macrophages and neutrophils plays a critical role in pathological
situations including I/R injury.127
1.6.7 L-arginine bioavailability
Availability of L-arginine and cofactors play a critical role in post-transcriptional regulation of
NO production by NOS.109
The substrate for NOS, L-arginine, is also the substrate for
arginase.128
Pulmonary vascular resistance (PVR) can be decreased by L-arginine as a
vasodilator agent in the pulmonary circulation.129-131
The limitation of L-arginine availability for
NOS by increased arginase activity has recently been shown to represent an important
posttranscriptional mechanism for the regulation of NOS activity in different cardio-vascular and
lung conditions.88, 105, 132-134
The ratio of L-arginine/L-ornithine (arginase substrate/product) is considered an indirect index of
arginase activity and consequently L-arginine bioavailability for NOS.115
The ratio of L-arginine/
(L-ornithine+L-lysine) is considered an index for intracellular L-arginine bioavailability for NOS
as these amino acids compete for CAT for intracellular uptake.98, 99
The ratio of L-arginine/ (L-
ornithine+L-citrulline) is defined as global L-arginine bioavailability and is considered an
indirect index for arginase activity and consequently L-arginine bioavailability.115
Recently,
many studies have demonstrated the correlation of global arginine bioavailability and prognosis
of cardiovascular events.115, 135, 136
All above ratios was calculated in serum at a given
concentration of L-arginine.

30
The role of L-arginine bioavailability for NO production has been shown in several studies and
in different diseases. For example, in asthma and cystic fibrosis substrate availability for NO
production was decreased. It also has been demonstrated that increased arginase activity led to
decreased NO.119, 122
Decrease in L-arginine availability results in iNOS uncoupling. Uncoupling of iNOS leads to the
production of reactive oxygen species including superoxide.99
The reaction between NO and
superoxide anion generates peroxynitrite which plays an important role in airway inflammation
and hyperresponsiveness.137
In addition to substrate availability, the activity of NOS is also
dependent on endogenous inhibitors such as asymmetric dimethylarginine (ADMA).138, 139
Increased ADMA in lung contributes to smooth muscle constriction and airway obstruction in
patients with cystic fibrosis and in asthma.140, 141
The ratio of products of competing enzymes –L-ornithine/L-citrulline – can be used as an index
of the balance between arginase and NOS the L-arginine metabolizing enzymes. A change in this
ratio is a sign of a change in NOS activity (Table 1-1).121
1.6.8 Asymmetric dimethylarginine
Protein arginine residues are methylated by protein arginine methyltransferases (PRMT), a
family of 9 enzymes.142
These enzymes in mammalian cells are classified depending on their
specific activity into type I, II, III and IV. In the first step, types I and II produce mono-
methylarginine (MMA) from L-arginine. In the next step, type I PRMTs (PRMT1, 3, 4, 6 and 8)
produces ADMA, whereas types II PRMTs (PRMT5, PRMT7) produce symmetric
dimethylarginine (SDMA). 142
Free MMA, SDMA, or ADMA are released from cells following
proteolytic degradation of methylated intracellular proteins.123, 142
They can be cleared from the
body through kidney and liver.123, 142

31
Table 1-6: Indicators of L-arginine/NO metabolism
L-arginine/L-ornithine L-arginine bioavailability (Indirect index of arginase
activity
L-arginine/(L-ornithine+L-lysine) L-arginine bioavailability (Amino acids compete for
CAT)
L-arginine/(L-ornithine+L-citrulline) L-arginine bioavailability (Indirect index for arginase
activity)
L-ornithine/L-citrulline Arginase- NOS balance (Index of the balance between
arginase and NOS)
L-arginine/ADMA NOS impairment (Index for NOS inhibition)
CAT, cationic amino acid transporter; NOS, nitric oxide synthase; ADMA, Asymmetric
dimethylarginine

32
Figure 1-5: Biological effects of nitric oxide.116
NO plays essential roles in several physiological
responses.

33
Furthermore, dimethylarginine dimethylaminohydrolases (DDAH) 1 and 2 metabolize MMA and
ADMA to L-citrulline and mono- or di- methylamines.123, 142
DDAH is predominantly expressed
in the liver, but it is also expressed in the kidney, endothelial cells, the pancreas and the lung.123
ADMA is removed to some extent through urinary excretion.123
Cells can uptake ADMA via the
cationic amino acid (y+) transporters.123
ADMA is a competitive inhibitor of all isoforms of
NOS and is an endogenous regulator of the L-arginine/NO metabolism in vivo.143
NOS activity
depends on the ratio of L-arginine over ADMA concentrations.144
This ratio is considered a
better index for NOS inhibition than ADMA concentration alone (Table 1-6).144
An increase in
ADMA concentration in normal L-arginine concentration results in decreased NO production.118
However, increase in L-arginine levels can compensate the inhibitory effect of ADMA.118
The
correlation of increased ADMA concentration and cardiovascular diseases has been
demonstrated previously.145
In patients with chronic heart failure with elevated ADMA
concentrations, the administration of L-arginine resulted in improved endothelium-dependent
vasodilatation.118
In healthy participants, however, endothelium-dependent vasodilatation is not
altered by L-arginine supplementation.118
Changes in ADMA concentration are associated with the pathogenesis of many clinical disorders
including pulmonary hypertension, cystic fibrosis and asthma.140, 141, 146
The important role of the
L-arginine bioavailability and the presence of endogenous NOS inhibitor ADMA for NO
production and airways obstruction in patients with CF and asthma have just recently
established.140, 141
However, the role of the L-arginine/NO metabolism has not been reported in
the setting of lung transplantation.
1.7 Rationale
The role of changes in the L-arginine/NO metabolism including increased arginase expression
and activity, changes in L-arginine availability for NOS, decrease in NO production and release
of reactive oxygen species has been demonstrated in primary graft dysfunction for liver, kidney
and heart.147-149
However, changes in the arginine metabolism following transplantation of the
lung have not been characterized extensively so far. Moreover, qualities of potential donor lungs
are assessed subjectively by experienced surgeons using criteria including clinical history, the

34
external appearance, bronchoscopic finding and gas exchange.8, 9
Clinical assessments of donor
lungs prior to transplantation might not provide sufficient information for the prediction of short
term and long term complications after transplantation. For instance, in a pig model of injured
lung for transplantation, it has been demonstrated that ex vivo PO2 by itself cannot be considered
a first indicator of lung injury.25
Additional biomarkers could potentially help the evaluation of
donor lungs and predict outcomes of transplantation.
The roles of NO in many physiological processes such as regulation of smooth muscle tone and
regulation of immune response have been described previously.73, 98, 99, 104, 113-117
Noticeable
vasodilatation is induced as a result of smooth muscle relaxation due to the effect of NO.112, 150
Inhaled NO suppresses pulmonary hypertension after lung reperfusion following ischemia
without disturbing systemic arterial pressure, and is used to manage pulmonary hypertension
following transplantation.72
Clinically, I/R injury leads to acute increased smooth muscle contractility with subsequent
reduction in organ perfusion, ventilation perfusion (V/Q) mismatch in the lungs, and chronic
tissue damages such as fibrosis and remodelling of the transplanted organ.72
Pre-treatment with
low doses of inhaled NO prior to harvesting of lungs decreases the rate of early lung allograft
reperfusion injury.151
Additionally, administration of low doses NO prior to the harvesting of the
lung results in lower IL-8 levels and consequently lower risk of I/R injury.151
The effects of cold ischemia and reperfusion on the L-arginine/NO metabolism have been shown
in some studies in lung transplantation.73
NO production decreases in lung allograft for the
duration of the perioperative period.152
In a pig model of lung transplantation, administration of
L-arginine in the first 10 minutes of reperfusion resulted in improvement of pulmonary
function.153
These findings suggested that the L-arginine/NO metabolism was altered in the lung
after reperfusion. Decreased NO production due to increased arginase expression and activity in
I/R injury following warm ischemia in coronary artery obstruction has been already
demonstrated in a pig model. Interestingly, in this setting vasodilatation was restored by either
arginase inhibitor or L-arginine supplementation.154
The concentrations of L-arginine,

35
endogenous NOS inhibitors and L-arginine in the lung during different steps of transplantation
have not been investigated yet.
IL-10 gene therapy during EVLP is an innovative approach to reduce inflammation in donor
lung. IL-10 gene therapy decreases the rate of primary graft dysfunction and results in
improvement of lung function but the mechanisms leading to these improvements are
incompletely understood.155
We are interested in investigation of L-arginine/NO metabolism in
donor lungs after IL-10 gene therapy because NO production and iNOS expression can be
suppressed by IL-10 in macrophages.51, 156-158
IL-10 also reduces transcription of CAT 2, a
transporter for L-arginine, and leads to decreased L-arginine bioavailability for intracellular NOS
in murine activated macrophages.51
Therefore, it is possible that some of the effects of IL-10
gene therapy could be related to an effect on the L-arginine/NO metabolism51, 155
but, the
alterations in the L-arginine/NO metabolism following lung transplantation and the effect of IL-
10 gene therapy on the L-arginine/NO metabolism have not been published yet.
1.8 Hypothesis
We hypothesize that lung transplantation results in dysregulation of the L-arginine/NO
metabolism and a reduction in L-arginine availability which leads to a decrease in NO
production. Some of the beneficial effects of IL-10 will be mediated through the L-arginine/NO
metabolism. IL-10 gene therapy will prevent these alteration and results in better lung function.
1.9 Specific aims
1.9.1 Specific aim 1
The first specific aim for this project is to characterize alterations in the L-arginine/NO
metabolism at different steps of lung transplantation. Therefore, we analyzed data from a model
of pig lung transplantation using lung samples after different lengths of hypothermic
preservation, after brain death followed by cold ischemia and after transplantation of these lungs.
This study design allowed us to investigate the concentrations of L-arginine and its metabolites

36
at different time points to understand whether different stages in lung transplantation caused an
alteration of the L-arginine/NO metabolism.
1.9.2 Specific aim 2
The second specific aim for this thesis is to study the effects of EVLP and of IL-10 gene therapy
during EVLP on the L-arginine/NO metabolism in lung tissue at the steps between harvesting
and lung transplantation. To achieve this specific aim, we processed samples from another
model of lung transplantation in pigs. In this model we collected samples at different time points
before and after transplantation from pig lungs which underwent prolonged hypothermic
preservation, EVLP or IL-10 gene therapy during EVLP, and transplantation.

37
Chapter 2: Materials and Methods

38
2.1 Lung transplantation
Pig Lung tissue from different studies was generously provided by Dr. Keshavjee’s lab, Latner
Thoracic Surgery Research Laboratories, University Health Network, Toronto General Hospital
(TGH).
2.1.1 Animals
Male Yorkshire domestic pigs (25 to 35 kg) were used for the experiments. All animals were
treated humanely based on the “Principles of Laboratory Animal Care” prepared by the National
Society for Medical Research and the “Guide for the Care of Laboratory Animals” by the
National Institutes of Health. The experimental protocol had been approved by the Animal Care
Committee of the Toronto General Hospital Research Institute.24, 25
2.1.2 Anesthesia
Ketamine (40 mg/kg intramuscularly) was used for sedation followed by inhaled Isoflurane 5%
volume/volume (v/v) for induction of anesthesia. Propofol (5–8 mg/kg/hour) and fentanyl citrate
(2–20 mg/kg/hour) were infused intravenously to maintain anesthesia during surgery. Pigs were
intubated with an appropriate endotracheal tube and ventilated using a volume-controlled
ventilator.24, 159
2.1.3 Brain death
Brain death induction in pigs was performed as previously described in the baboon by Novitzky
et al.160
In brief, temporal bone was drilled after anesthesia and a Foley catheter was place in the
extradural space. The Foley catheter was inflated slowly while the intracranial pressure (ICP)
was monitored. The goal was to keep the ICP at least 50 mmHg higher than mean arterial
pressure.160
The criteria for confirmation of brain death include:
1- Absence of cerebral blood flow, which was confirmed by cerebral angiography.
2- Absence of motor exam.

39
3- Absence of brainstem reflexes.
4- Negative atropine stimulation test. The atropine stimulation test is considered negative when
the increase in heart rate is less than 3% in response to intravenous injection of atropine.161
2.1.4 Lung retrieval
Lungs retrieval process from donor animals was described previously by Pierre et al.162
Harvested lungs were flushed through the pulmonary artery using Perfadex
(low-potassium
dextran glucose preservation solution) while the lungs were ventilated. Then lungs were inflated
and the trachea was clamped and cut. At the end of retrieval, removed lungs were flushed
retrogradely with Perfadex
.162
In the non brain death group, double lung block retrieval was
performed after anesthesia of living pigs. In the brain death group, lungs were harvested 10 hours
after brain death. After sedation and intubation, animals were ventilated by a volume-controlled
ventilator. The lungs were kept at 4 C for various periods of time depending on study design.
Following cold ischemia the lungs went through normothermic ex vivo lung perfusion for 12
hours and then the left lung was transplanted to the recipient animal.
2.1.5 Ex vivo lung perfusion
Normothermic acellular ex vivo lung perfusion (EVLP) in an isolated circuit was performed as
described by Steen and others.14, 46
In brief, the trachea was intubated and cannulae were attached
to the left atrium (LA) and the pulmonary artery (PA).15
A retrograde flow with an acellular
perfusate (Steen solution, Vitrolife) containing heparin 10,000 U, Solu-Medrol 500 mg, and
Cefazolin 1g (Table 2-1) was started slowly to eliminate air from the circuit.15, 24
Then the PA
cannula was connected to the system and anterograde flow initiated at 150 ml/min at room
temperature.14
The perfusate temperature was increased slowly to 37°C.14, 15
Mechanical
ventilation was started when temperature reached 32°C to 34°C (usually within 30 min) at a rate
of 7 breaths/minute, and the flow rate of the perfusate was increased gradually.15, 24
Meanwhile,
carbon dioxide was added to the inflow perfusate using a gas exchange membrane.14

40
Table 2-1: Composition* of STEEN solution™
163
Water
Human serum albumin
Dextran 40
Glucose
Sodium chloride
Potassium chloride
Sodium dihydrogen phosphate
Sodium bicarbonate
Calcium chloride
Magnesium chloride
* Concentrations are not available as STEEN solution™ is a trade mark product.

41
The lung block temperature was reduced in the circuit to 20°C following the last ex vivo
assessment.14
Subsequently, FiO2 was increased to 0.5 for lung storage before perfusion and
ventilation were stopped.14
In order to keep the lungs inflated, the trachea was clamped.14
Then
the lungs were stored in Perfadex
in a standard sterile organ bag at 4°C until transplantation.14
2.1.6 Ex vivo viral delivery
One hour after establishing EVLP one group of pigs was treated with an adenovector to deliver
the human IL-10 gene.159
The diluted adenoviral vector was delivered through a flexible fiber-
optic bronchoscope into each segmental bronchus at the beginning of EVLP as previously
described by Cypel et.al. In brief, following vector delivery, an inspiratory hold was performed
(recruitment maneuver), and then for the next 15 min lungs were ventilated with a tidal volume
of 6-8 ml/kg to facilitate distribution of the vehicle throughout the lung. All donor lungs were
transplanted after 12 hours of EVLP.14, 15, 24
2.1.7 Ex vivo evaluation of lung function during EVLP
To evaluate lung function during EVLP, PO2 of the perfusate was measured in the left atrium
and pulmonary artery every hour following a recruitment maneuver. In addition, pulmonary
vascular resistance, pulmonary artery flow, peak airway pressure, and airway plateau pressure
were monitored simultaneously.14
2.1.8 Evaluation of lung function after transplantation
Blood gas was measured in left pulmonary vein blood samples in order to analyze gas-exchange
one hour after transplantation.14
2.2 Biopsies
Lung biopsies were taken from the superficial tissue at the lower lobe of the right lung at time
points before transplantation and from the lower lobe of the left lung after transplantation. The
samples were immediately snap frozen and kept at – 80ºC for further processing.

42
2.3 Homogenization
Tissue samples were homogenized with lysis buffer for the measurement of in vitro arginase
activity, Western blotting, quantitative polymerase chain reaction (q-PCR) and measurement of
NO metabolites. Frozen tissue samples were kept on ice and the lysis buffer containing 25 mM
tris-HCl (pH=7.4), 10% (v/v) glycerol and 1% (v/v) Triton X100, 1 mM phenylmethylsulfonyl
fluoride (PMSF) (Calbochem, LaJolla, CA, USA), 2 mM ethylenediaminetetraacetate (EDTA), 2
μg/ml pepstatin A, 2 μg/ml leupeptin and 1mM dithiothreitol (DTT) were added approximately
1:5 weight/volume (w/v). Samples were chopped the using a pair of scissors and homogenised in
2 ml microtubes with a hand held rotor stator (Polytron PT 1200 E, Kinematica AG,
Switzerland) for 30 sec homogenization and 10 sec pause followed by another 30 sec
homogenization. The homogenates were kept on ice for one hour and vortexed every 10 min.
Tubes were centrifuged for 20 min at 14500 × g at 4C. The supernatant was aliquotted into 1.5
ml micro tubes and stored in -80C.
2.4 Protein assay
Protein content of the extracts was determined using the Bradford protein assay.164, 165
We
prepared the standards in acrylic cuvettes using bovine serum albumin (BSA) according to Table
2-2. Samples were diluted with water to fit into the standard curve range, and then 4 μl of diluted
sample plus 796 μl milli Q water and 200 μl of Bradford dye reagent were pipetted to the
cuvettes. All samples and standards were prepared in duplicate. The cuvettes were incubated at
room temperature for 5 min and the light absorption was measured by spectrophotometer at
595nm. The spectrophotometer deducted the blank value of absorbance automatically. The
standard curve was plotted using Microsoft Excel program according to the absorbance values of
BSA concentration. Protein concentrations in the samples were calculated according to the
equation of the standard curve and dilution factor.164, 165

43
Table 2-2: Volume and concentration of standard solution for protein estimation.
BSA (0.05 mg/ml) μl H2O μl Final protein content
μg*
0 800 Blank
50 750 2.5
100 700 5
200 600 10
300 500 15
400 400 20
BSA, Bovine serum albumin.* 200l Bradford
dye reagent were added to all standards.

44
2.5 Sample preparation for liquid chromatography mass spectrometry
Samples were deproteinized, butylated, and reconstituted for liquid chromatography-tandem
mass spectrometry (LC/MS/MS) for the measurement of amino acids and ADMA according to
the method developed previously in Dr. Grasemann’s lab in conjunction with Dr. Pencharz’s lab.
In brief, in order to deproteinize the samples, 30- 50 μl of tissue homogenate was mixed with 2
volumes of methanol and vortexed. The mixture was centrifuged for 20 min at 14,500 RPM at
4C. The supernatant was collected and 10 μl of internal standard mixture of all analytes,
labelled with stabilized isotopes, was used to spike samples and standards to identify the peaks of
analytes and calculate the ratio of the unlabelled and labelled peak. The mixture was evaporated
to dryness under nitrogen stream. 100 μl of 3 M hydrochloric acid in butanol was added and
topped with nitrogen gas. The mixture was incubated at 65C for 20 minutes followed by
evaporating to dryness under nitrogen gas stream. The dried contents were reconstituted with
0.1% (v/v) formic acid and submitted for LC/MS/MS. The concentrations were calculated
according to the equation of the calibration curves, made from standards butylated in parallel
with the samples, and dilution factor. Standard curve concentrations for ADMA were 0.01 μM to
10 μM whereas, for L-arginine, L-ornithine and L-citrulline the standard concentrations were 0.1
μM to 100 mΜ.140
2.6 LC/MS/MS
The concentrations of L-arginine, L-ornithine, and ADMA in lung tissue homogenates were
measured using LC/MS/MS provided by the Analytical Facility for Bioactive Molecules of The
Centre for the Study of Complex Childhood Diseases at The Hospital for Sick Children, Toronto,
Canada. The results were normalized based on the protein concentration of the homogenates.
2.7 NO metabolite measurement
Nitric oxide metabolites (NOx) were measured, including nitrates (NO3¯), nitrites (NO2
¯) and S-
nitrosothiols (SNOs) using chemiluminescence analyzer (Eco Physics, Switzerland) as
previously reported.166, 167
The NO analyzer generates ozone (O3) in its reaction cell. NO reacts

45
with O3 to form O2 and nitrogen dioxide (NO2). A portion of NO2 is produced in an electrically
excited state with unstable electrons. These electrons release energy when they return to their
original ground state and emit photons which can be converted into measurable electrical signals.
The method is highly sensitive and specific for NO and can detect NO in a range of 0-5,000 ppb
and detection level is 0.06 ppb. 168
NO and its oxidation products can be measured with the NO
analyzer using the liquid purge vessel system. Chemical reducing agents in the vessel convert
products of NO including nitrate/ nitrite/ nitrosothiols to NO. Vanadium (V) (III) chloride (0.05
M in 1N hydrochloric acid is used to convert nitrate, nitrite and S-nitrosothiol compounds to NO
(2 NO3¯+ 3 V
3+ + 2 H2O 2 NO + 3 VO2
+ + 4 H
+).
169 Five mM sodium nitrate was serially
diluted to prepare standard solutions. 100 μl stock nitrate was added to 900 μl milli Q water to
make 500μM nitrate, next 100 μl of 500 mM was added to 400 μl to make 100 μM (Tube S1)
and then serially diluted using μl milli Q water (S2-S9). (Standard concentrations = 100 (S1), 50
(S2), 25 (S3), 12.5 (S4), 6.25 (S5), 3.125 (S6), 1.5625 (S7).
All samples were deproteinated using Amicon Ultracel-0.5 10K centrifugal filters (Millipore
catalogue # UFC501096) and centrifuged at 14,500 × g for 15 min. Twenty five μl of samples
were injected in the liquid purge vessel system of the NO analyzer, then Δt and mean were
measured and area under the curve (AUC) for each samples were calculated. Subsequently,
based on the standard curve, the concentration for NOx concentration was calculated. Limit of
blank (mean blank + 1.645(SD blank) for AUC measurement in our assay was 351.1913 and limit of
detection (limit of blank + 1.645 (SD low concentration sample) was 825.5216. We calculated and
normalized our results base on protein concentrations on our samples. These calculations cannot
be applied to blanks as they do not contain proteins. However, all measurements were in the
detection range of the NO analyzer.
2.8 Quantitative polymerase chain reaction
q-PCR was used to quantify gene expression of enzymes involved in the L-arginine/NO
metabolism.170
In this set of samples we measured changes in arginase and iNOS gene
expression in comparison to the beta actin gene expression used as a house keeping gene. We

46
considered the first time point, time of harvesting (0h CIT), as control and calculated the gene
expression at other time points as fold change from 0h CIT.
Pig lung tissue samples were homogenized for q-PCR in TRI reagent solution (1/10 w/v) and
incubated for 5 min at room temperature. Then the homogenates were centrifuged at 12,000 × g
for 10 min at 4ºC and the supernatants were transferred to fresh tubes. 100 μl of 1-bromo-3-
choloro-propane (BCP) per 1 ml of TRI reagent solution was added, mixed well for 15 sec, and
incubated at room temperature for 5-15 min. The tubes were centrifuged again at 12,000 × g for
another 10-15 min at 4ºC, and then the aqueous phase was transferred to a fresh tube. 500 μl of
isopropanol was added per 1 ml of TRI reagent solution, vortexed at moderate speed for 5-10
sec, and incubated at room temperature for 5-10min. The mixture was centrifuged at 12,000 × g
for 10 min at 4ºC, and the supernatant was discarded. 1 ml of 75% (v/v) ethanol was added per 1
ml TRI reagent solution, and then centrifuged at 7,500 × g for 5 min at 4ºC. The centrifugation
was repeated at 12,000 × g for 5 min to consolidate the pellet at the bottom of the tube. Ethanol
was removed and the tubes were centrifuged again to remove all residual ethanol by removing
the ethanol that collects with a fine tip pipette. In the next step ribonucleic acid (RNA) was air-
dried for 3-5 min. RNA pellet was dissolved in the nuclease-free water and stored at 4ºC for
immediate analysis (for long storage, stored at -70ºC or colder).170
All Reagents were purchased
from Invitrogen (Life Technologies Inc. Burlington, ON).
2.8.1 Assessing RNA yield and quality
To assess the concentration of mRNA solution, the absorbance was read in a traditional
spectrophotometer at 260 nm and calculated the concentration RNA (μg /ml) = A260dilution
factor 40). To test the quality of RNA, agarose gel electrophoresis was run and we calculated
the ratios of 28S and 18S bands which should be around 2 and then we checked RNA purity – A
260/ A 280 ratio which should be around 1.8-2.2.170

47
2.8.2 Complementary deoxyribonucleic acid
Reagents: SuperScript II First-Strand Synthesis SuperMix for q-PCR with Random Hexamers
(Invitrogen). RT Reaction mix, RT Enzyme Mix, RNA and DEPC water were added into one
tube and gently mixed and incubated at 25°C for 10 min. Then the tube was incubated at 50°C
for 30 min for the reaction. After that, the reaction was terminated at 85°C at 5 min, followed by
cooling down on ice. Next, RNase H was added and the tube was incubated at 37°C for 20 min,
and then stored at -20°C.170
2.8.3 Real time PCR
Reagent: Power SYBR Green PCR Master Mix with Ampli Taq Gold Polymerase (Invitrogen).
Primers:
Pig arginase1: Sus scrofa arginase, liver (arginase1), Messenger RNA (mRNA)
Product length = 163
Forward primer 1: ACAATCCATCGGGATCATCGGAGC 24
Reverse primer 1: AGGGACATCAGCAAAGCACAGGT 23
Pig arginase: Sus scrofa arginase, type II (arginase 2), mRNA
Product length = 229
Forward primer 1: TGCATTTGACCCTACCCTGGCT 22
Reverse primer 1: TCCCTCCCTTGTCTGCCCAAAACT 24
Pig –iNOS: Sus scrofa iNOS, mRNA
Product length = 187

48
Forward primer 1: TTTCAGGAAGCATCACCCCCGT 22
Reverse primer 1: TGCATGAGCACAGCGGCAAAGA 22
Complementary deoxyribonucleic acid (cDNA) was diluted 10 times, reagents, primer-F, primer-
R, cDNA, and diethylpyrocarbonate (DEPC) water were added followed by thermal cycle (95°C,
10 min → denature 95°C 15 sec, 60°C 1min, for 40 cycles on the machine).170
2.9 Western blotting
The expression of proteins was analyzed in pig lung tissue extracts as follows. Polyacrylamide
gel electrophoresis was prepared on denaturing gels using the mini –PROTEAN 3 gel system
(Bio-Rad Laboratories, Hercules, CA). Arginase isoforms were separated on a 10% (w/v)
acrylamide gel. Sample buffer contained 30% (v/v) glycerol, 0.012% (w/v) bromophenol blue,
10% (w/v) sodium dodecyl sulfate (SDS) and 0.6 M DTT. Samples were diluted according to the
protein concentration target for 100 μg protein in 25 μl. Then samples were mixed with sample
buffer and incubated in 95C for 10 min. Each well was loaded with 25 μl samples and
electrophoresis ran on running buffer, containing tris base 0.3% (w/v), 1.44% (w/v) glycine,
0.1% (w/v) SDS, at 140 volts (V) for approximately 70 min. Proteins were transferred to
nitrocellulose membrane in transfer buffer – containing tris base 0.3% (w/v), 1.44% (w/v)
glycine, 20% (v/v) Methanol – at 100 V for 75 min. Membranes were blocked in 1% (w/v)
skimmed milk over night at 4C. The membranes were washed, and then incubated at room
temperature with primary antibodies for 60 min followed by washing and incubation with
secondary antibody for another 60 min also at room temperature. Membranes were incubated
with Super Signal West Pico chemiluminescent substrate (Thermo scientific, IL) for 5 min and
exposed to autoradiography film (HyBlot, DENEVILLI scientific INC, NJ). All antibodies were
purchased from Santa Cruz Biotechnologies (Santa Cruz, CA). Details of each antibody are
provided in Table 2-3. In this set of data the changes in arginases protein expression were
measured in comparison to protein expression of a house keeping protein actin in the same
sample and expressed as relative of target protein to actin density.171

49
Table 2-3: Details of antibody used for Western blotting.
Target Epitope Catalogue number Isotype
Actin C-terminus (Human) sc-1616 (I-19) Goat polyclonal IgG
Arginase 1 N-terminus (Human) sc-18531 (N-20) Goat polyclonal IgG
Arginase 2 C-terminus (Human) sc-18537 (N-20) Goat polyclonal IgG
IgG, immunoglobulin G; all antibodies purchased from Santa Cruz Biotechnology Inc.

50
2.10 Arginase activity measurement
Arginase activity in lung tissue extract was measured according to the method published by
Corraliza et al.172
Briefly, in 2 ml boil-proof micro tubes (PROGENE) samples were diluted to a
final protein concentration of 4 mg/ml with lysis buffer, containing proteinase inhibitors. The
samples were mixed with manganese chloride (MnCl2)10 mM in 25 mM tris–HCl, pH= 7.4 in
equal volume as the enzyme cofactor, and incubated at 56C for 10 min to activate the enzyme.
The substrate of arginase, L-arginine (20mM, pH=9.7), was added to the extract containing
activated enzyme and incubated at 37C for 60 min. The reaction was stopped with an acid
mixture containing 1% (v/v) sulphuric acid (H2SO4) and 3% (v/v) phosphoric acid (H3PO4).
Standards were prepared according to Table 2-4. All samples and standards were prepared in
triplicate (Table 2-4).172
The dye, α-isonitrosopropiophenone (ISPF), was added to standards and
samples and all tubes were incubated at 100C for 90 min followed by 15 min incubation at
room temperature in the dark. The samples and standards were pipetted into FALCON 96 well
plate. The reaction of urea with ISPF was evaluated by absorbance values measured at 540 nm
(Figure 2-1). Limit of blank (mean blank + 1.645(SD blank) for optical density (OD) measurement
in our assay was 0.09 and limit of detection (limit of blank + 1.645(SD low concentration sample) was
0.13.173
The blank value of absorbance was deducted automatically by the spectrophotometer.
This method is highly sensitive. Urea amounts of 0.02-0.05 mol can be measured by this assay.
In addition, the method is highly specific and does not interfere with other metabolites in the
homogenates.172
The standard curve was plotted using the absorbance values of urea
concentration. Urea concentrations in the samples were calculated from the equation of the
standard curve and the dilution factor. The activity of the enzyme was calculated based on the
amount of substrate converted to product per unit of time. The arginase activity was calculated
using the urea concentration in each tube divided by 60 min to calculate the unit (μ mol/min).
We corrected the values based on the protein concentration and expressed data as munit/ mg
protein. Data for blanks were not normalized based on protein concentrations as they do not
contain proteins. However, all OD measurements were in the detection range of the assay.

51
2.11 Statistics
All data were shown as mean± standard error of the mean (SEM). For comparison between three
groups or more, one-way ANOVA and Tukey’s multiple comparison test, or Kruskal-Wallis test
and Dunn's multiple comparison test were used based on the distribution of data. For comparison
between two groups unpaired or paired t-test, Wilcoxon matched paired test or Mann-Whitney
test were used where appropriate. Statistical software package in Prism 5 (GraphPad Software,
San Diego, CA) was used for statistical analysis. Probability values less than 0.05 (p
values<0.05) were considered to represent statistically significant differences between group of
samples.

52
Figure 2-1: Protocol for measurement of arginase activity in tissue homogenates according to
Corraliza. 172
OD, optical density; ISPF, α-isonitrosopropiophenone.

53
Table 2-4: Volumes and concentrations of standard solution for arginase activity measurement
Urea 0.5mg/ml (μl) Lysis buffer mixture*
0 50
2 48
4 46
8 42
16 34
24 26
32 18
40 10
PI, protease inhibitor; Tris-HCl, Trizma® base (SIGMA- ALDRICH®) + HCl. 50l 25
mM tris–HCl pH= 9.7 and 800 l of acid mixture (1% (v/v) H2SO4+ 3% (v/v) H3PO4 in
water) was added to all tubes.* Lysis buffer mixture contained lysis buffer + PIs+ MnCl2
10 mM in 25 mM tris–HCl , pH= 7.4 (μl).

54
Chapter 3: The L-arginine metabolic profile
in lungs differs between donations after
brain death compared to prolonged cold
ischemia.

55
3.1 Abstract
Background: Currently, brain death donors are the major source of donation for lung
transplantation. However, brain death leads to metabolic changes which can contribute to I/R
injury and PGD. NO plays important roles in both development and management of I/R injury.
Therefore, this study was designed to characterize the L-arginine/NO metabolism after different
length of cold ischemia and after EVLP followed by transplantation and reperfusion in different
types of donors. However, the effects of EVLP on the L-arginine/NO metabolism in lungs have
not been studied previously.
Methods: Pig lung samples were taken from lungs which were preserved in cold ischemia for
different length of time, and lungs obtained after brain death and cold ischemia. Lungs from
brain death and lungs preserved for 30h were subjected to 12 hours EVLP followed by
transplantation. Levels of amino acids involved in the L-arginine/NO metabolism were measured
using high performance liquid chromatography mass spectrophotometery (HPLC-MS) by
Metabolon Inc.
Results: Duration of hypothermia has no effects on L-arginine, L-ornithine, L-lysine or ADMA
levels or on indices of L-arginine bioavailability and NOS impairment. However L-citrulline
levels were higher after cold ischemia in the brain death group. The L-ornithine/L-citrulline ratio
was decreased after 6 hours of cold ischemia, but not after prolonged cold ischemia. After EVLP
and transplantation of lung in the non brain death donors L-citrulline levels were higher than in
lungs from brain death donors resulting in a lower ratio of L-ornithine/L-citrulline in the non
brain death group. In prolonged hypothermic preserved lung L-citrulline levels were higher after
EVLP and transplantation compared to after cold ischemia. Additionally, in lungs from the brain
death donors L-arginine levels were lower after EVLP followed by transplantation and
reperfusion compared to after cold ischemia.
Conclusion: Based on these findings we conclude that changes in the L-ornithine/L-citrulline
ratio after 6 hours of cold preservation may reflect a shift in the metabolism of L-arginine toward
NOS. In addition, the L-arginine metabolic profile in lungs from the prolonged hypothermic

56
preserved group when compared to “brain death” group at different stages of lung transplantation
were significantly different, which could potentially correlate with the short term outcomes after
transplantation.

57
3.2 Introduction
NO plays crucial roles in numerous physiological processes such as regulation of smooth muscle
tone, inhibition of platelet aggregation, regulation of immune response and neurotransmission.73,
98, 99, 104, 113-117 It has been shown that some complications after lung transplantation are correlated
with alterations of the L-arginine/NO metabolism.73
The amino acid L-arginine is a substrate of
NOSs for NO production.98
Studies have demonstrated that alterations in L-arginine metabolism
and availability result in changes in NO production.109, 111, 112, 132
The production of NO is
decreased in the lung following cold preservation.152, 174
While NO is known to act as a
vasodilator,68, 175, 176
it can also react with oxygen species to produce toxic radicals, which plays
an important role in the development of I/R injury and PGD.72, 81
PGD is a serious complication that can occur within 72 hours following lung transplantation,1, 59,
60 and is a type of severe acute lung injury which in some cases can be managed clinically by
inhaled NO.74, 177, 178
As mentioned earlier in this thesis, I/R injury can result in acute and chronic
graft dysfunction.83, 179
I/R injury leads to increased vascular smooth muscle tone, vascular
resistance and decreased tissue perfusion.72
Inhaled NO in some cases is effective in
management of I/R injury.67, 83
Moreover, in a rabbit model of lung transplantation, L-arginine
supplementation resulted in lower rates of I/R injury by maintaining NO production and
endothelium function.180
In a pig model of isolated reperfusion of heart and lung, the
administration of L-arginine improved oxygenation and lung compliance.153
In a model of
isolated lung perfusion in rabbits, L-arginine supplementation resulted in maintained endothelial
function and NO production.153, 180
Prolonged hypothermic preservation is a risk factor for PGD.59
Cell injuries following
hypothermia such as decreased ATPase activity and subsequently interruption in ion balance lead
to cellular edema and cell death.36, 37
Specifically in the lung, hypothermia causes altered oxygen
exchange due to increase in extravascular fluid and pulmonary vasoconstriction.26, 36
In North America, lungs for transplantation are typically harvested from donors after brain death
or in some cases after cardiac death.4, 6
Brain death leads to hydrostatic insults and inflammatory

58
responses and hormonal changes in lung tissue resulting in massive changes in cellular
metabolism such as lactic acidosis and production of ROS, which can be deteriorated by
hypothermic preservation and reperfusion.5, 28-31
Donor organs obtained after cardiac death
experience warm ischemia which can also result in lung tissue damage.3, 11
EVLP is a modern technique which provides opportunity for prolonged preservation, evaluation
of lung function and possible medical interventions,12, 14, 17, 20
without increasing the risk of
complications such as I/R injury.12
In injured lungs in the brain death pigs with significantly
higher PVR after cold ischemia compared to the control, 12 hours EVLP lead to a significant
decrease in PVR.25
In addition, administration of inhaled NO during EVLP resulted in
improvement of lung function in a rat model.55, 56
Possible alterations in the L–arginine/NO metabolism at different steps of lung transplantation
may contribute to I/R induced lung injuries. Therefore, the objective of the present study is to
examine metabolites related to the L-arginine/NO metabolism in lung tissues at different time
points in a pig model of lung transplantation to characterize the L-arginine/NO metabolism
during lung transplantation.
3.3 Study designs and experimental approach
Samples were taken by a group of surgeons at the Latner Thoracic Surgery Research
Laboratories, University Health Network, Toronto General Hospital (TGH). This animal model
of lung transplantation was designed to study the effects of different lung preservation times and
conditions on the L-arginine/NO related metabolism.
As described earlier in previous chapter 2, based on current regulations and guidelines male
Yorkshire domestic pigs (25 to 35 kg) were used for these experiments.24, 25
Animals were
anesthetized and intubated.24, 159
In the brain death group brain death was induced by inflating a
foley catheter to increase the ICP.181
In all animals lungs were retrieved from donor animals and
flushed antegradely and retrogradely using Perfadex
.162
Depending on study design lungs were
kept at 4C for different periods of time. Next, for 12 hours lungs underwent normothermic
acellular EVLP in an isolated circuit14, 46
followed by left lung transplantation and reperfusion.

59
Samples were taken from the lungs and immediately snap frozen in liquid nitrogen and then kept
at -80ºC. Samples from studies of lung transplantation in pig models were collected as follows
(Figure 3-1). In this study lungs were preserved at 4ºC beyond the time period that is clinically
accepted. Therefore, in this study lungs were severely injured to magnify metabolic alterations.
A. In the “control” group, samples were taken from normal pig lung immediately after organ
retrieval. These lungs were flushed with Perfadex
and did not undergo cold ischemia
preservation. Therefore, they were named 0h CIT and considered normal controls (n=5).
B. In the “less injured lung” group samples were taken after 6 hours of cold static
preservation which simulates current clinical practice. This group was named 6h CIT
(n=6).
C. In the prolonged hypothermic preservation group lungs were harvested from normal
animals and kept at 4C for 30 hours, which was denoted as 30h CIT (n=5) prolonged
cold ischemia leads to severe injuries in donor lung which could magnify metabolic
alterations.
D. In the brain death group lungs were harvested 10 hours after induction of brain death in
animals followed by 24 hours of cold static preservation. Samples were collected after 24
hours of cold ischemia, which was marked as BD+24h CIT (n=4).
The lungs in the brain death group were also preserved in cold ischemia for longer period than in
real clinical conditions (24 hours). Although this period is shorter than the preservation time in
the non brain death group (30hours), alterations in metabolic biomarkers in these lungs could
provide evidences for further investigations. In addition, in human lung transplantation, donor
lung are preserved in cold ischemia of different lengths of time. Therefore, in this study we
included and analysed data from donor lungs after brain death.
All above samples were blood free. However, the following samples which were taken after lung
transplantation and reperfusion contained blood. Lung transplantation after prolonged
preservation leads to I/R injury. Therefore, another sample was taken after 12 hours of EVLP
followed by 1 hour reperfusion.

60
E. In the non brain death group 1 hour after transplantation and reperfusion which was
named 30h CIT/1h post rep (n=5).
F. In the brain death group 1 hour after transplantation and reperfusion, BD+24h/1h post rep
(n=5).
All samples were sent to Metabolon Inc. Durham, NC, USA, for processing and measuring
several biomarkers in lung tissue homogenates using HPLC-MS in collaboration with Dr.
Keshavjee’s lab. Data for the levels of L-arginine, L-ornithine, L-citrulline, L-lysine and ADMA
were provided to us by Dr. Keshavjee’s lab for detailed analysis.
These data were not expressed as true concentrations. Metabolon Inc. used a standard method to
log-normalize the data and present the results as a scaled intensity (relative quantification).182
All data are shown as mean±SEM. For comparison between three groups or more, one-way
ANOVA and Tukey’s multiple comparison test, or Kruskal-Wallis test and Dunn's multiple
comparison test, and for comparison between two groups unpaired or paired t-test were used
where appropriate. Statistical software package in Prism 5 (GraphPad Software, San Diego, CA)
was used. A p values<0.05 was considered to represent significant differences between group of
samples.

61
Figure 3-1: Pig lung transplantation study designs. The study was designed to investigate the
effects of different lung preservation time and conditions on the L-arginine/NO metabolism.
Samples were taken at different time points as follows: A:0h CIT, after harvesting the lung from
donor and flushing with Perfadex
; B:6h CIT, after 6 hours of cold ischemia in the non brain
death animals; C:30h CIT, after 30 hours of cold ischemia in the non brain death group;
D:BD+24h CIT, after 24 hours of cold ischemia in the brain death group; E: 30h CIT/1h post
rep , after transplantation and reperfusion of 30h CIT group; F:BD+24h/1h post rep, after
transplantation and reperfusion of BD+24h CIT group, EVLP, ex vivo lung perfusion; CIT, Cold
ischemia time; TOH, time of harvesting; LTx, lung transplantation.

62
3.4 Results
Analysis of the levels of L-arginine and its metabolites at different time points allowed us to
study the effects of length of cold ischemia on L-arginine metabolism. Additionally, we were
able to investigate whether the levels of L-arginine and its metabolites were different in lungs
after prolonged cold preservation (30h CIT) compared to lungs after brain death followed by
cold preservation (BD+24h CIT). This study design also allowed us to assess if and at what time
point the cause of death leads to differences in the L-arginine metabolism after lung
transplantation and reperfusion.
3.4.1 Length of cold static preservation does not affect the levels of L-arginine and its
metabolites
The levels of L-arginine, L-ornithine, L-citrulline, L-lysine and ADMA in lung tissue at the time
of harvesting, 6 hours after cold ischemia and 30 hours after cold ischemia are provided in Table
3-1. There were no significant differences between the groups (one way ANOVA) (Figure 3-2).
ADMA is a competitive endogenous NOS inhibitor.143
High concentration of ADMA in serum is
correlated with impairment in NO-mediated vasodilatation.144
Several studies have shown that
the L-arginine/ADMA ratio is correlated with NO-mediated vasodilation.144
This ratio is
considered an index for NOS impairment.144
The L-arginine/ADMA ratio was also not different
at various lengths of cold ischemia points in our study (Table 3-2) (one-way ANOVA).
The substrate-to-product ratio for arginase, L-arginine/L-ornithine, can be used as an index for
L-arginine bioavailability for NOS.115
Arginase and NOS are intracellular enzymes and L-
arginine competes with L-ornithine and L-lysine for transport into the cell by CATs. Intracellular
L-arginine bioavailability for NOS can also be expressed as the ratios of L-arginine/ (L-
ornithine+L-lysine).98, 99
These ratios were not different at different time points after cold
ischemia compared to the time of harvesting (Table 3-2) (one way ANOVA).

63
0h C
IT
6h C
IT
30h C
IT
0
1
2
3
A
L-a
rgin
ine
log
-no
rmalized
data
as a
scale
d in
ten
sit
y
0h C
IT
6h C
IT
30h C
IT
0
1
2
B
L-o
rnit
hin
e
log
-no
rmalized
data
as a
scale
d in
ten
sit
y
0h C
IT
6h C
IT
30h C
IT
0.0
0.5
1.0
1.5
2.0
2.5
C
L-c
itru
llin
e
log
-no
rmalized
data
as a
scale
d in
ten
sit
y
0h C
IT
6h C
IT
30h C
IT
0
2
4
6
D
L-l
ysin
e
log
-no
rmalized
data
as a
scale
d in
ten
sit
y
0h C
IT
6h C
IT
30h C
IT
0
1
2
3
4
E
AD
MA
log
-no
rmalized
data
as a
scale
d in
ten
sit
y
Figure 3-2: Different length of cold ischemia time does not affect the levels of amino acids or
ADMA in donor lungs (one way ANOVA).
A, L-arginine; B, L-ornithine; C, L-citrulline; D, L-lysine; E, ADMA; log-normalized data as a
scaled intensity; samples were taken at different time points as follows: 0h CIT, time of
harvesting lung from donor; 6h CIT, after 6 hours of cold ischemia in the non brain death group;
30h CIT, after 30 hours of cold ischemia in the non brain death group.

64
Table 3-1: Lung amino acid and ADMA levels at different time points in the brain death and non
brain death groups
Num
ber o
f
samples
L-arg
inin
e
L-o
rnith
ine
L-citru
lline
L-ly
sine
AD
MA
0h CIT 5 1.120.25 0.850.19 0.700.09 2.120.90 1.530.62
6h CIT 6 1.540.35 0.670.17 1.100.23 0.950.15 1.110.20
30h CIT 5 1.240.21 0.900.11 0.570.12 0.950.11 1.010.13
BD+24h CIT 4 1.69.0.33 2.591.39 1.090.19 2.211.03 2.551.22
30h CIT/1h post
rep 5 0.710.09 1.320.26 1.360.08 0.860.12 0.740.08
BD+24h/1h post
rep 5 0.590.09 1.850.15 1.060.09 0.880.13 0.770.11
Log-normalized data as a scaled intensity for amino acids and ADMA are shown as meanSEM.
Samples were taken at different time points as follows: 0h CIT, time of harvesting lung from
donor; 6h CIT, after 6 hours of cold ischemia in the non brain death group; 30h CIT, after 30
hours of cold ischemia in the non brain death group; BD+24h CIT, after 10 hours of brain death
followed by 24 hours of cold ischemia; 30h CIT/1h post rep , 1 hour after transplantation and
reperfusion of 30h CIT group; BD+24h/1h post rep , 1 hour after transplantation and
reperfusion of BD+24h CIT group.

65
Table 3-2: Indices of L-arginine bioavailability and NOS impairment in lung at different time
points in the brain death and non brain death groups
Num
ber o
f
samples
L-arg
inin
e/L-
orn
ithin
e
L-arg
inin
e/ (L-
orn
ithin
e+L
-
lysin
e)
L-arg
inin
e/ (L-
orn
ithin
e+L
-
citrullin
e)
L-o
rnith
ine/L
-
citrullin
e
L-arg
inin
e/
AD
MA
0h CIT 5 1.450.37 0.50.16 0.700.11 1.300.32 1.210.35
6h CIT 6 2.590.64 0.910.18 0.880.19 0.580.10 1.320.23
30h CIT 5 1.380.14 0.670.08 0.830.04 1.750.32 1.240.14
BD+24h CIT 4 1.791.10 0.560.25 0.740.31 2.350.88 0.920.21
30h CIT/1h post
rep 5 0.620.12 0.350.05 0.270.04 0.970.18 0.980.13
BD+24h/1h post
rep 5 0.340.07 0.220.04 0.210.04 1.750.08 0.7600.4
Ratios for L-arginine availability and NOS impairment are shown as meanSEM. Samples were
taken at different time points as follows: 0h CIT, time of harvesting lung from donor; 6h CIT,
after 6 hours of cold ischemia in the non brain death group; 30h CIT, after 30 hours of cold
ischemia in the non brain death group; BD+24h CIT, after 10 hours of brain death followed by
24 hours of cold ischemia; 30h CIT/1h post rep , 1 hour after transplantation and reperfusion of
30h CIT group; BD+24h/1h post rep , 1 hour after transplantation and reperfusion of BD+24h
CIT group.

66
The L-ornithine/L-citrulline ratio can be used as a measure of the balance between arginase and
NOS, as L-ornithine is the product of arginase and L-citrulline the product of NOS activity. This
ratio is inversely related to the consumption of L-arginine toward NOS and NO production.
Therefore, a change in the ratio can be considered an indicator of a change in arginase/NOS
balance.121
Lower L-ornithine/L-citrulline ratio in lungs after 6 hours cold ischemia compared to
the control suggests that a short period of cold preservation may alter the L-arginine/NO
metabolism. In lungs after 30 hours of cold ischemia this ratio was significantly higher than in
lungs after 6 hours of cold ischemia (p<0.05, one way ANOVA, Tukey's multiple comparison
test) (Figure 3-3). This finding suggests that the effects of hypothermic preservation on the L-
arginine/NO metabolism cannot be sustained in prolonged hypothermic preservation.
3.4.2 Reperfusion of lungs from bran death donor after 24 hours cold ischemia results in
different L-arginine and L-citrulline levels compared to lungs from non brain death
donors after 30 hours of hypothermic preservation
It is known that prolonged preservation (30h CIT) and brain death donation followed by 24 hours
of cold preservation can induce acute lung injury after transplantation. EVLP may provide a
time-window to resume lung metabolism and improve lung function after transplantation. To
determine whether EVLP and lung transplantation procedure can affect the L-arginine/NO
metabolism in donor lung, we examined the levels of L-arginine and its metabolites one hour
after transplantation and reperfusion.
To avoid over expression, the data were demonstrated on one graph. Data for after
transplantation and reperfusion in lungs from the brain death animals (BD+24h CIT/1h post rep)
are incomparable to data for after 30 hours of cold ischemia (30h-CIT). Similarly, the
comparison of data from the non brain death animals after transplantation and reperfusion (30h
CIT/1h post rep) to the brain death group after cold ischemia (BD+24h CIT) is invalid. No three
sets of data were comparable; therefore, ANOVA is an inappropriate test. Thus, we used
unpaired t test.

67
0h C
IT
6h C
IT
30h C
IT
0
1
2
3*
L-o
rnit
hin
e/L
-cit
rull
ine
Figure 3-3: A, The L-arginine metabolism by arginase and NOS; B, Decreased L-ornithine/L-
citrulline ratios in donor lungs were observed after 6 h cold ischemia time (6h CIT) but not 30h
CIT; *p<0.05, one way ANOVA, Tukey's multiple comparison test.
Samples were taken at different time points as follows: 0h CIT, time of harvesting lung from
donor; 6h CIT, after 6 hours of cold ischemia in the non brain death group; 30h CIT, after 30
hours of cold ischemia in the non brain death group.

68
The L-citrulline level in the brain death group after cold ischemia (BD+24h CIT) was higher
than in the prolonged hypothermic group (30h CIT) (p=0.049, unpaired t test). However, for
other amino acids and ADMA comparing between these two groups did not show differences. It
was reported that the outcome of lung transplantation and reperfusion in the brain death group
was worse than in prolonged hypothermic group.25
Therefore, higher L-citrulline level after cold
preservation, may be relevant to the clinical condition of the recipient after transplantation and
reperfusion.
Levels of L-arginine, L-ornithine, L-lysine and ADMA were not different (unpaired t test) after
transplantation and reperfusion in lungs from the brain death animals (BD+24h CIT/1h post rep)
compared to the non brain death animals (30h CIT/1h post rep ). The ratios of L-arginine/L-
ornithine or L-arginine/ (L-ornithine+L-lysine) as well as L-arginine/ADMA in lungs from both
the brain death and the non brain death animals were similar after transplantation and
reperfusion. The level of L-citrulline in lung tissues from the non brain death group was higher
after transplantation and reperfusion than in the brain death group after transplantation and
reperfusion (p=0.04, unpaired t test) (Figure 3-4-A).
In the prolonged preservation group levels of L-arginine, L-ornithine, L-lysine or ADMA in lung
tissues after cold ischemia were not different compared to after transplantation and reperfusion
(unpaired t test). However, L-citrulline in lungs after transplantation and reperfusion (30h CIT/1h
post rep ) was higher compared to after 30 hours of cold ischemia (30h-CIT) (p= 0.0006,
unpaired t test) (Figure 3-4-A).
The ratio of L-ornithine/L-citrulline in lungs from the brain death donors was higher than in
lungs from the non brain death donors after transplantation and reperfusion (p=0.004, unpaired t
test) (Figure 3-4-B). This finding could be a reflection of shift of L-arginine metabolism toward
consumption by NOS after transplantation and reperfusion in the non brain death group as
previously described.
In the brain death group, levels of L-ornithine, L-citrulline, L-lysine or ADMA were not
different in lungs before transplantation compared to after transplantation and reperfusion

69
(unpaired t test). However, the level of L-arginine in lung tissues homogenates after
transplantation and reperfusion (BD+24h/1h post rep ) was lower compared to after cold
ischemia (BD+24h CIT) (p= 0.008, unpaired t test) (Figure 3-4-C).

70
30h C
IT
30 C
IT /1
h pos
t rep
BD
+24h C
IT
BD
+24h C
IT/1
-h p
ost r
ep
0.0
0.5
1.0
1.5
2.0
0.049
0.042
0.0006
AL
-cit
ru
llin
e
log
-no
rm
ali
zed
da
ta
as
a s
ca
led
in
ten
sity
30h C
IT
30 C
IT /1
h pos
t rep
BD
+24h C
IT
BD
+24h C
IT/1
-h p
ost r
ep
0
1
2
3
4
50.004
B
L-o
rn
ith
ine/L
-cit
ru
llin
e
30h C
IT
30 C
IT /1
h pos
t rep
BD
+24h C
IT
BD
+24h C
IT/1
-h p
ost r
ep
0
1
2
3 0.008
C
L-a
rg
inin
e
log
-no
rm
ali
zed
da
ta
as
a s
ca
led
in
ten
sity
Figure 3-4: A, Comparing the brain death and non brain death groups, before transplantation L-
citrulline was higher in the brain death group, but after transplantation and reperfusion L-
citrulline was higher in the non brain death group ; B, L-ornithine/L-citrulline ratio is higher after
transplantation and reperfusion in the brain death group; C, L-arginine after transplantation and
reperfusion decreases in the brain death groups (unpaired t test).
Hollow symbols represent blood free samples; solid symbols represent samples containing
blood; log-normalized data as a scaled intensity; Samples were taken at different time points as
follows: 30h CIT, after 30 hours of cold ischemia in the non brain death group; 30h CIT/1h
post rep, 1 hour after transplantation and reperfusion of 30h CIT group; BD+24h CIT, after 10
hours of brain death followed by 24 hours of cold ischemia; BD+24h/1h post rep, 1 hour after
transplantation and reperfusion of BD+24h CIT group; data for 30h CIT in Figure 3-4-B are
identical to the same data in Figure 3-2 and Figure 3-3.

71
3.5 Discussion
In this chapter we found that length of cold ischemia time did not result in changes in the levels
of L-arginine and its metabolites, indices of L-arginine bioavailability or NOS impairment.
However, the index for balance in L-arginine metabolism by arginase and NOS, the L-
ornithine/L-citrulline ratio, was lower after 6 hours of cold ischemia, suggesting a possible
alteration in the L-arginine/NO metabolism. In addition, after cold ischemia in lung from the non
brain death donors, the L-citrulline level was lower than in the brain death donors. However,
after transplantation and reperfusion in lung from the non brain death donors, the L-citrulline
level was higher than in the brain death donors. This observation suggested that NOS activity
was increased in prolonged hypothermic preserved lungs after transplantation. Decreased L-
ornithine/L-citrulline ratio in the non brain death group may also reflect an imbalance in L-
arginine metabolism by arginase and NOS.
Cold preservation is a necessary step in lung transplantation, but prolonged cold ischemia causes
oxidative stress, sodium pump inactivation and intracellular calcium overload.72
These changes
can lead to cell death and release of pro-inflammatory mediators and consequently alterations in
the expression and activity of enzymes including those involved in L-arginine homeostasis such
as NOSs.72, 183
Analysis of data showed that the length of cold ischemia did not significantly affect L-arginine,
L-ornithine, L-citrulline, L-lysine or ADMA. Interestingly however, a lower L-ornithine/L-
citrulline ratio in lungs after 6 hours of cold ischemia compared to the lungs at the time of
harvesting and to the lungs after 30 hours of cold ischemia was observed. A decrease in L-
ornithine/L-citrulline ratio can be explained by either a decrease in L-ornithine or an increase in
L-citrulline, or disproportional changes in activities of arginase and NOS. The L-ornithine/L-
citrulline ratio can be considered an index to estimate the balance in L-arginine metabolism by
arginase and NOS121
and the observed changes in the L-ornithine/L-citrulline ratio may indicate
changes in the balance of arginase and NOS.

72
In a rat model of lung transplantation NO production was decreased after 6 hours of cold
preservation in 4C compared to fresh lungs.174
In addition, it was demonstrated that
hypothermia suppressed iNOS and nNOS activity in endothelial cells independent of L-arginine
concentration which resulted in reduced NO production.184
In our study the decrease in L-
ornithine/L-citrulline ratio could reflect of a shift in L-arginine metabolism toward consumption
by NOS.121
However, these data were not expressed as true concentration and changes in the
ratios may therefore not accurately reflect changes in arginase/NOS balance. Measuring NOx
concentrations would provide a better estimate of NOS activity.
As described earlier, the L-arginine/L-ornithine ratio and L-arginine/ (L-ornithine+L-lysine) in
serum are indices of L-arginine bioavailability for intra-cellular NOS at a given L-arginine
concentration.98, 99, 115
It is possible that these indices in tissue homogenate may not reflect
intracellular L-arginine availability for NOS.
We did not find evidence for inhibition of NOS by ADMA. ADMA is a competitive endogenous
inhibitor of NOS143
and impairment in NO-mediated vasodilatation correlates with high
concentration of serum ADMA and low L-arginine/ADMA ratio.144
Cold ischemia did not affect
ADMA concentration nor the L-arginine/ADMA ratio in lung tissue.
Catecholamine storm following brain death results in increased intracellular calcium ion and
induces inflammatory responses which could result in activation of inflammatory biomarkers and
iNOS.31, 181
Analysis of data for L-arginine and its metabolites in lung comparing different organ
damage severity showed that in lungs after 24 hour of cold ischemia in the brain death group
levels of L-citrulline were significantly higher than in lungs after prolonged (30 h) hypothermic
preservation in non brain death group.
Evaluation of L-arginine and its metabolites in the lungs after transplantation and reperfusion in
the brain death group compared to the non brain death group is important because the type of
donors would result in differences in the rate of complications after lung transplantation such as
I/R injury.185, 186
After transplantation and reperfusion L-citrulline levels were higher in lungs
from the non brain death group compared to the brain death group. A significantly lower L-

73
ornithine/L-citrulline ratio in the non brain death group was also observed. As previously
discussed, the decreased L-ornithine/L-citrulline ratio could reflect a shift of L-arginine
metabolism toward NOS.
We compared the levels of L-arginine and its metabolites in lung tissue after cold ischemia to
after transplantation and reperfusion in both the brain death and non brain death group. We
observed changes from before to after transplantation and reperfusion in L-arginine levels in the
brain death group. L-citrulline levels changed from before to after transplantation and
reperfusion in the non brain death group. These differences are important because the L-arginine
level in the same samples were low while L-citrulline levels were high, which demonstrates that
different donor types have different L-arginine metabolic profiles. Therefore, these changes
might be caused by a metabolic change in lung tissue. However, the comparisons of lungs after
cold ischemia to lungs after transplantation and reperfusion must be interpreted with caution as
blood contamination may cause changes in the levels of biochemical markers in the tissue
homogenates. In addition, starvation, blood loss, dehydration and renal failure due to the surgery
could result in differences in concentration of biochemical markers.187, 188
For instance, L-
citrulline concentration depends on renal function and it is therefore considered a marker for
acute and chronic renal failure.189
Blood levels of amino acids were not measured in recipient
animals. Therefore, it is not clear whether the differences in pre-transplantation compared to
post-transplantation and reperfusion samples were caused by alteration in L-arginine metabolism
in lung tissue or reflect changes of metabolisms in other organs of the recipient. These findings
suggest that after EVLP and reperfusion the L-arginine/NO metabolism was altered differently in
the brain death group compared to prolonged preserved group.
These findings also indicated that changes occurred after cold ischemia, but levels of L-arginine
and its metabolites were not measured after EVLP. Therefore the differences are due to
combined effects of EVLP and transplantation and reperfusion. It is unclear whether they were
caused by EVLP or, transplantation and reperfusion or both.
It has been previously demonstrated that gene expression of iNOS and protein expression of
iNOS and eNOS in a rat model were increased after transplantation of lung tissue.190
Other

74
studies also showed that NO production increased after ischemia and reperfusion.179
This
increase in NO production was a result of an increase in expression and activity of iNOS.179
In
all previously reported models donor lung was harvested from the non brain death animals. In the
present study although L-citrulline levels, another product of NOS activity, after transplantation
and reperfusion in the non brain death group was higher compared to after cold ischemia, the NO
concentration was not measured. Therefore, we are not able to comment on changes in NO
production by NOS.
There are other limitations to this study. In this experiment proper controls for lungs after
transplantation and reperfusion were not available. Unflushed normal lungs could be an
appropriate reference for concentrations of amino acids and ADMA after transplantation and
reperfusion in lung tissue. In addition, these samples were collected from different studies
specifically to measure several metabolites using HPLC-MS. Changes in the expression and
activity of enzymes as well as the concentration of NO and its metabolites were not investigated
in these samples. The concentrations of L-arginine metabolites in lung tissue were not measured
before transplantation (after EVLP). As a result the effects of EVLP on the L-arginine
metabolism in lung tissue could not be evaluated. Data were expressed as log-normalized data on
scale intensity. Therefore, the numbers as well as the ratios must be interpreted carefully. For a
better understanding of the changes in the L-arginine/NO metabolism, specifically interpretation
of L-arginine availability ratios, accurate concentrations of amino acids and ADMA should be
determined.
In brief, in a pig model of lung transplantation, analysis of data revealed that 6 hours of
hypothermic preservation leads to a shift in consumption of L-arginine toward NOS, an effect
that was not seen in prolonged cold preservation. However, this alteration was not driven by
changes in L-arginine bioavailability or NOS impairment. Clinical outcomes after transplantation
of these lungs to recipients were recently reported by Yeung et al.25
Clinical outcomes after lung
transplantation in the brain death group were worse than in prolonged cold preservation group.25
Our study demonstrated that L-arginine metabolic profiles in prolonged hypothermic
preservation group were different from the brain death group.

75
Chapter 4: NO metabolite and L-citrulline
concentrations are decreased after EVLP
independent of IL-10 gene therapy and
remain decreased after transplantation.

76
4.1 Abstract
Background: The availability of donor lungs for transplantation is one of the major obstacles in
lung transplantation resulting in high wait list mortality. EVLP renders the opportunity to
evaluate marginal organs and to perform medical interventions such as IL-10 gene therapy in
order to improve the quality of the organs and expand the donor pool. However, our knowledge
of the biochemical alterations, including the L-arginine/NO metabolism, is limited. In this study
we investigated the effects of EVLP and IL-10 gene therapy during EVLP on the L-arginine/NO
metabolism in lungs before and after transplantation.
Methods: In a pig model, we collected samples from lungs preserved in hypothermia of different
lengths. We also collected samples after EVLP, after EVLP+IL-10 and after transplantation and
reperfusion of these lungs. We measured concentrations of L-arginine, L-ornithine, L-citrulline
LC/MS/MS. We used a chemiluminescence analyzer to measure concentration of NO
metabolites. In addition, we measured iNOS and arginases mRNA expression using quantitative
polymerase chain reaction (q-PCR). Moreover, we quantified in vitro arginase activity based on
the rate of urea production.
Results: We show that cold ischemia had no effect on the concentration of NO metabolites,
mRNA expression of iNOS, mRNA expression of arginases or in vitro arginase activity.
However, after EVLP or after EVLP+IL-10 gene therapy, NOx levels were significantly lower
than 6h CIT (before EVLP). L-citrulline and NOx levels were also lower after EVLP compared
to the timed control group, 18h CIT. Additionally, EVLP or EVLP+IL-10 led to an increase in
arginase 1 and 2 expressions, which may be responsible for the observed decrease in NO
production. Furthermore, after transplantation and reperfusion of lungs which underwent EVLP
or EVLP+IL-10, NOx and L-citrulline levels were lower than normal. Moreover, after
transplantation and reperfusion arginase1 and 2 mRNA expression was still higher in these lungs
than normal control.
Conclusion: These findings suggest that cold ischemia do not cause changes in the L-
arginine/NO metabolism. EVLP may cause a reduction in NOS activity independent of IL-10

77
gene therapy which may be driven by an increase in arginase expression. These differences were
still appearing after transplantation and reperfusion. Importantly, the metabolic profile of the L-
arginine/NO metabolism in lungs after cold ischemia followed by EVLP or EVLP+IL-10 is
different from lungs which preserved only in hypothermia. These differences could contribute to
clinical outcomes of transplantation.

78
4.2 Introduction
In the last decade the number of lung transplantations in Canada increased almost two fold.7
Donor lungs are usually selected based on traditional criteria such as donor’s age, clear chest
radiography, clinical history and gas exchange capacity (Table 1-1).8, 9
Currently less than 20%
of lungs from multi-organ donors fulfill criteria for transplantation22, 32
, while the Canadian
Institute for Health Information (CIHI) reported that more than 21% of patients in Canada died
waiting on the lung transplantation lists in 2011.7 Using marginal organs and donation after
cardiac death could be immediate solutions to expand the donor pool, increase organ availability
and decrease wait list mortality.3, 10, 11
However, transplantation of marginal lungs could
potentially result in an increase in complications and consequently increased post-transplant
morbidity and mortality. 3, 11
EVLP allows surgeons to evaluate lung function after organ harvest
but prior to transplantation.18, 23
EVLP provides physiological conditions for maintaining cellular
metabolism in the lungs as well as the opportunity for recovery from tissue injury.12, 14, 17, 20
In
addition, EVLP provides the opportunity for therapeutic interventions before transplantation.12,
14, 17, 20, 46 For instance, IL-10 gene can be delivered during EVLP.
15 IL-10 gene therapy is a
potential therapeutic intervention to ameliorate inflammatory injuries in the donor lung as a
result of anti-inflammatory effects of IL-10.15, 94
Lung function during EVLP is usually assessed using physiological parameters such as
pulmonary dynamic compliance and blood gas analysis.12, 18, 23
Physical factors such as dry/wet
weight ratio, flow rate and perfusion pressure are also considered important factors.52
However,
metabolic biomarkers are more sensitive indices than physical parameter for the evaluation of
lung quality and function.52
Metabolites of the L-arginine/NO metabolism could potentially be
used as biomarkers to assess lung function during and after EVLP, but the L-arginine/NO
metabolism has not been studied in the setting of EVLP and IL-10 gene therapy in lung
transplantation.
NO is an endogenous regulator of many physiological responses.104, 113, 114, 124, 151, 190
NO plays
important roles in vascular resistance and in inflammatory responses.68, 116
For instance, NO is a
smooth muscle relaxant which can reduce vascular resistance.68, 98, 114, 130
Inhaled NO can be used

79
therapeutically as a pulmonary vasodilator agent to decrease PVR.176
Gas exchange and
oxygenation properties, the ratio of arterial oxygen tension to inhaled oxygen fraction
(PaO2/FiO2), was improved in patients that underwent inhaled NO therapy for treatment or
prevention of early allograft dysfunction following lung transplantation.87
In addition, it was
shown that administration of inhaled NO during EVLP led to improvement in oxygenation of
lungs and pulmonary artery blood flow after transplantation in a rat model.56
The cytokine IL-10 plays crucial roles in the regulation of inflammatory responses.91
IL-10
inhibits macrophages and dendritic cells function and subsequently suppresses T helper-1 and -2
cell responses.90
In addition, in macrophages IL-10 inhibits synthesis of pro-inflammatory
cytokines such as TNF-α.93
While IL-6 and IL-8, are considered risk factors for post-
transplantation mortality, IL-10 is known as a protective factor.33
In the donor lung the ratio of
IL-6 to IL-10 prior to transplantation has been demonstrated as a predictor for early mortality
following lung transplantation.33
Increased IL-8 levels in the donor lung are associated with early
lung dysfunction and higher mortality rate following lung transplantation.92
IL-10 can reduce NO
production in macrophages.51, 156-158
In a study of murine activated macrophages it was shown
that in addition to inhibition of iNOS protein expression, IL-10 causes suppression of CAT 2
transcription, a transporter for cationic amino acids including L-arginine, which can result in
reduce L-arginine bioavailability for intracellular NOS.51
It has been demonstrated that IL-10
gene therapy reduced inflammation and improved lung function in the human lungs that were
rejected for transplantation.15
In this chapter we characterized the L-arginine/NO metabolism at different time points in a pig
model of lung transplantation (specific aim 1). Furthermore, we investigated the effects of IL-10
gene therapy on the L-arginine/NO metabolism in lung transplantation to accomplish specific
aim 2.
4.3 Study designs and experimental approach
Lung tissue samples were taken from a pig model of lung transplantation study performed by a
group of surgeons at the Latner Thoracic Surgery Research Laboratories, University Heath

80
Network, Toronto General Hospital (TGH). This study was designed to understand different
effects of EVLP and EVLP+IL-10 gene therapy during EVLP on the L-arginine/NO metabolism.
In chapter 2 we described the procedure of lung transplantation. In brief, according to regulations
and guidelines male Yorkshire domestic pigs (25 to 35 kg) were used in our model.24, 25
Following induction of anesthesia and intubation24, 159
, lungs were retrieved, flushed with
Perfadex162
from animals in all groups and kept at 4ºC. There were different experimental
groups in the study design. In the “no EVLP” group, lungs were kept at 4 C for 18 hours
followed by left lung transplantation. In the “EVLP” group lung were kept at 4 C for 6 hours
before undergoing 12 hours of EVLP followed by left lung transplantation and reperfusion.14, 46
In the “EVLP+IL-10”group, lungs were preserved at 4C for 6 hours followed by 12 hours of
EVLP. Adenoviral vector containing the human IL-10 gene was delivered to the airways through
a flexible fiber-optic bronchoscope approximately one hour after EVLP was started.24
The left
lungs were then transplanted into the recipient animals.
To study the L-arginine/NO metabolism during different stages of lung transplantation and
following therapeutic interventions, we collected lung tissue samples at different time points as
specified below (Figure 4-1):
A. 0h CIT: time of harvesting the lungs in all animals, samples were taken from flushed lungs
with Perfadex
prior to CIT.
6h CIT: in the “EVLP” and “EVLP+IL-10” groups samples were taken 6 hours after cold static
preservation. Six hours is accepted as an optimal time for lungs to maintain pulmonary function
after transplantation.21
B. 18h CIT (timed control): in the “no EVLP” group samples were collected after 18 hours of
cold ischemia. This group was the timed control group in this study as in other groups the
lungs were transplanted after 6 hours of cold ischemia followed by 12 hours of EVLP.
C. 6h CIT+12h EVLP: in the “EVLP” group samples were taken after 12 hours of EVLP using
acellular perfusate, STEEN solution™.

81
Figure 4-1: Pig lung transplantation study designs. The study was designed to investigate the
effects of EVLP and IL10 gene therapy during EVLP on the L-arginine/NO metabolism.
Samples were taken at different time points as follows: A:0h CIT, Time of harvesting of the
lung from donor after flushing with Perfadex
; B:6h CIT, after 6 hours of cold ischemia; C:18h
CIT (timed control), after 18 hours of cold ischemia; D:6h CIT+12h EVLP, 6 hours of cold
ischemia followed by 12 hours of EVLP; E: 6h CIT+12h EVLP+IL-10, after 6 hours of cold
ischemia followed by IL-10 gene therapy and 12 hours of EVLP, F: 18h CIT/1h post rep, 1
hour after transplantation and reperfusion of 18h CIT group; G:EVLP/1h post rep, 1 hour after
transplantation and reperfusion of 6h CIT+12h EVLP group; H:EVLP+IL-10/1h post rep, 1
hour after transplantation and reperfusion of 6h CIT+12h EVLP+IL-10 group; I: recipient left
lung, immediately after removal of lung from recipient animals; EVLP, ex vivo lung perfusion;
CIT, cold ischemia time; TOH, time of harvesting; LTx, lung transplantation; RLL, recipient
left lung; IL-10, interleukin-10.

82
6h CIT+12h EVLP+IL-10: in the “EVLP+IL-10” group samples were taken after 12 hours of
EVLP using a cellular perfusate, STEEN solution™. Twelve hours of EVLP provides a time
window after delivery of the IL-10 gene vector to the airways for effective therapeutic levels of
gene expression at reperfusion time.96
D. 18h CIT/1h post rep: in the “no EVLP” group samples were taken 1 hour after transplantation
and reperfusion.
E. EVLP/1h post rep: in the “EVLP” group samples were taken 1 hour after transplantation and
reperfusion.
F. EVLP+IL-10/1h post rep: in the “EVLP+IL-10” group samples were taken 1 hour after
transplantation and reperfusion.
G. Recipient left lung: samples were collected immediately after removal of the left lungs in
recipients as normal control lungs. These samples allow a comparison of lung after
transplantation and reperfusion with perfused normal lung.
We analysed the samples as follows, which are explained in detail in chapter 2:
1. L-arginine, L-ornithine, L-citrulline and ADMA concentrations were measured using
LC/MS/MS. Concentrations were measured in lung tissue homogenates from recipient left
lung as well as in lungs before and after transplantation and reperfusion in the “no EVLP” and
“EVLP” groups. These data were expressed as true concentrations and normalized for protein
content in the homogenates.
NOx including NO3¯, NO2
¯ and SNOs were measured using chemiluminescence analyzer (Eco
Physics, Dűrnten, Switzerland).168
2. Arginase 1, arginase 2 and iNOS mRNA expression in lung tissue was measured using q-
PCR. The data for mRNA expressions in normal lungs and donor tissue samples at the time of
harvesting (0h CIT) were expressed as a ratio of target mRNA over beta actin mRNA
expression for other time points data were expressed as fold changes from 0h CIT.
3. Protein expression of arginase 1 and arginase 2 were measured using Western blot analysis.

83
In vitro arginase activity was measured based on the rate of urea production from L-arginine,
according to a protocol previously published by Corraliza.172
NOx concentrations, mRNA expression, protein expression and arginase activity were measured
in lung tissue homogenates at all time point in all groups.
All data are shown as the mean ± SEM. Comparison between three groups or more was done
using one-way ANOVA and Tukey’s multiple comparison test, or Kruskal-Wallis test and
Dunn's multiple comparison test was used. Between two groups unpaired or paired t-test was
used where appropriate. Statistical software package in Prism 5 (GraphPad Software, San Diego,
CA) was used for statistical analysis. p values of <0.05 were considered to represent significant
differences between group of samples.
4.4 Results
In the previous chapter we described evidence for possible changes in the balance of arginase
and NOS activity. However, concentrations of NOx were not measured in those samples. The
present study design allowed us to measure NOx concentrations in tissue samples after cold
ischemia of different lengths. These data help us understand whether the length of the cold
ischemia time has any effect on NO production. The current study design also let us investigate
whether EVLP or EVLP plus IL-10 gene therapy lead to changes in the L-arginine/NO
metabolism compared to the lungs after 6 hours of cold ischemia (before EVLP) or to the lungs
after 18 hours of cold ischemia (timed control). Furthermore we were able to compare the L-
arginine/NO metabolism in transplanted lungs to naive control lung (recipient left lung).
4.4.1 Length of cold ischemia time does not affect L-arginine metabolism.
NOx concentration after different lengths of cold ischemia was measured to study if the duration
of hypothermic preservation causes changes in NOx. Our data showed that concentrations of
NOx in lungs obtained after different lengths of cold ischemia time were not different from those
of normal control lung at the time of harvesting (0h CIT) (Kruskal-Wallis test)(Figure 4-2-A).
Expression of mRNA for iNOS (Figure 4-2- B) arginase 1(Figure 4-2-C), and arginase 2

84
0h C
IT
6h C
IT
18h
CIT
(tim
ed con
trol
)
0
2
4
6
A
NO
x (
mo
l/g
pro
tein
)
0h C
IT
6h C
IT
18h
CIT
(tim
ed con
trol
)
0
2
4
6
8
1020
25
C
Arg
inase 1
mR
NA
(Fo
ld c
han
ge f
ro
m 0
h-C
IT)
0h C
IT
6h C
IT
18h
CIT
(tim
ed con
trol
)
0
5
10
15
20
40
60
D
Arg
inase 2
mR
NA
(Fo
ld c
han
ge f
ro
m 0
h-C
IT)
0h C
IT
6h C
IT
18h
CIT
(tim
ed con
trol
)
0
2
4
6
8
10
B
iNO
S m
RN
A
(Fo
ld c
han
ge f
ro
m 0
h-C
IT)
Figure 4-2: Different length of cold ischemia has no effect on NOx concentration or expression
of iNOS, arginase 1 or arginase2 mRNA in lung tissue (Kruskal-Wallis test).
A, NOx (mol/g protein); B, iNOS mRNA (fold change to time of harvesting); C, arginase1
mRNA (fold change to time of harvesting); D, arginase 2 mRNA (fold change to time of
harvesting). Samples were taken at different time points as follows: 0h CIT, after harvesting the
lung from donor and flushing with Perfadex
; 6h CIT, 6 hours after cold ischemia; 18h CIT
(timed control), 18 hours after cold ischemia. Data for 6h CIT and 18h CIT are identical to
Figure 4-3.

85
(Figure 4-2-D) (Table 4-1) were also not different between groups (Kruskal-Wallis test).
Importantly, this finding confirms the observation in previous chapter which levels of L-arginine
and its metabolites also were not different after different length hypothermic preservation.
4.4.2 EVLP decreases NOx concentrations in lung tissue.
Effects of EVLP and IL-10 gene therapy during EVLP on the L-arginine/NO metabolism have
not been studied previously. Therefore, we analyzed the samples to understand if EVLP and/or
IL-10 gene therapy affect the L-arginine/NO metabolism. Interestingly, compared to 6h CIT,
NOx levels were significantly reduced after EVLP (p<0.05, one way ANOVA, Tukey's multiple
comparison test) or after EVLP + IL-10 (p<0.01, one way ANOVA, Tukey's multiple
comparison test). NOx levels after EVLP were also lower than in the timed control (18h CIT)
group. Although this did not quite reach statistical significance, demonstrated that NOx was not
reduced over the time. After EVLP+IL-10 NOx concentration was significantly lower than timed
control group (p<0.05, Kruskal-Wallis test, Dunn's multiple comparison test) (Figure 4-3-A).
The concentration of L-citrulline, was also lower after EVLP compared to timed controls and
again did not quite reach statistical significance (p= 0.067, unpaired t test) (Figure 4-3-B).
Parallel decreases in NOx and L-citrulline concentrations after EVLP likely reflect a decrease in
NOS activity. Increased levels of NOS inhibitors can result in decreased NO production.
However, the concentration of ADMA, as well as the L-arginine/ADMA ratio, an index for NOS
impairment, was not different after EVLP compared to timed controls. In addition, there were no
changes in the expression of iNOS mRNA comparing 6h CIT and to timed controls (Figure 4-4-
A, Table 4-1, Table 4-2).
On the other hand, compared to 6h CIT, arginase 1 mRNA expression was significantly
increased after EVLP (p<0.05, Kruskal-Wallis test, Dunn's multiple comparison test or
EVLP+IL-10 (p<0.05, Kruskal-Wallis test, Dunn's multiple comparison test (Figure 4-4-B).
Similarly, arginase 2 mRNA expression was increased after EVLP (p<0.05, Kruskal-Wallis test,
Dunn's multiple comparison test of after EVLP + IL-10 (p<0.05, Kruskal-Wallis test, Dunn's
multiple comparison test compared to 6h CIT (Figure 4-4-C). Arginase competes for L-arginine

86
as substrate which can cause low L-arginine bioavailability for NOS and decreased NO
production. The indices for L-arginine bioavailability, L-arginine/L-ornithine ratio and L-
arginine/ (L-ornithine+L-citrulline) ratio were not different after EVLP compared to timed
controls (Table 4-3). Moreover, in vitro arginase activity was not different comparing lungs
before and after EVLP in all groups (Table 4-4). These findings suggest that EVLP could cause
alterations in the L-arginine/NO metabolism and low NO production which cannot be explained
by measures of L-arginine availability or NOS expression. The changes in the L-arginine/NO
metabolism which caused by EVLP cannot be prevented by IL-10 gene therapy.

87
18h
CIT
(tim
ed con
trol
)
6h C
IT+1
2h E
VLP
6h C
IT+1
2h E
VLP
+IL-
10
0.0
0.5
1.0
1.5
2.0
A *
NO
x (
mo
l/g
pro
tein
)
18-h
CIT
(tim
ed con
trol
)
6h C
IT+1
2h E
VLP
0
2
4
6
8
0.067B
L-cit
ru
llin
e
nm
ol/
mg
pro
tein
Figure 4-3: Concentrations of NOx and L- citrulline was decreased after EVLP (* p<0.05,
Kruskal-Wallis test, Dunn's multiple comparison test); A, NOx (mol/g protein); B, L-citrulline
(nmol/mg protein).
Samples were taken at different time points: 6h CIT, 6 hours after cold ischemia; 18h CIT
(timed control), 18 hours after cold ischemia; 6h CIT+12h EVLP, 6 hours of cold ischemia
followed by 12 hours of EVLP, 6h CIT+12h EVLP+IL-10, 6 hours of cold ischemia followed
by 12 hours of EVLP in the “EVLP+IL-10” group. Data for 18h CIT is identical to Figure 4-2.

88
Table 4-1: Expression of arginases and iNOS mRNA in lungs at different time points in the
“EVLP” and “no EVLP” groups.
Num
ber o
f
samples
Arg
inase1
mR
NA
expressio
n
Num
ber o
f
samples
Arg
inase2
mR
NA
expressio
n
Num
ber o
f
samples
iNO
S m
RN
A
expressio
n
0h CIT 10 1±0 10 1±0 10 1±0
6h CIT 10 1.26±0.27 12 9.50±5.34 11 1.70±0.40
18 h CIT (timed
control) 4 1.88±0.82 4 4.51±2.57 4 3.74±1.64
6h CIT+12h EVLP 5 7.00±3.46 5 13.68±9.76 4 2.56±0.86
6h CIT+12h EVLP
+IL-10 6 4.35±1.21 5 6.89±1.94 5 1.02±0.26
18h CIT/1h post rep 4 2.73±.073 4 13.60±5.75 4 3.55±1.67
EVLP/1h post rep 6 6.67±1.99 5 8.13±2.76 6 1.39±0.35
EVLP+IL-10/1h post
rep 5 8.93±2.64 5 10.85±3.11 5 0.87±0.42
Fold changes of mRNA expression to the time of harvesting for arginase1, 2 and NOS are shown
as meanSEM. Samples were taken at different time points as follows: 0h CIT, after harvesting
the lung from donor and flushing with Perfadex
; 6h CIT, 6 hours after cold ischemia; 18h CIT
(timed control), 18 hours after cold ischemia; 6h CIT+12h EVLP, 6 hours of cold ischemia
followed by 12 hours of EVLP, 6h CIT+12h EVLP+IL-10, 6 hours of cold ischemia followed
by 12 hours of EVLP in the “EVLP+IL-10” group; 18h CIT/1h post rep, 1 hour after
transplantation and reperfusion of 18h CIT group; EVLP/1h post rep, 1 hour after
transplantation and reperfusion of 6h CIT+12h EVLP group; EVLP+IL-10/1h post rep, 1 hour
after transplantation and reperfusion of 6h CIT+12h EVLP+IL-10 group.

89
Table 4-2: Concentrations of amino acids and ADMA in lung at different time points in the
“EVLP” and “no EVLP” groups and in recipient left lungs.
Num
ber o
f
samples
L-arg
inin
e
L-o
rnith
ine
L-citru
lline
AD
MA
18 h CIT (timed
control) 4 28.402.23 5.800.68 3.540.58 0.190.04
6h CIT+12h EVLP 6 42.82±11.61 4.70±1.54 1.60±0.50 0.22±0.05
18h CIT/1h post rep 4 35.23±4.16 8.43±1.29 5.06±0.66 0.16±0.03
EVLP/1h post rep 6 32.31±5.16 4.93±0.80 3.11±0.48 0.13±0.02
Recipient left lung 5 30.81±2.03 6.85±1.14 5.82±0.28 0.16±0.01
Concentrations of amino acids and ADMA (nmol/mg protein) are shown as meanSEM.
Samples were taken at different time points: 18h CIT (timed control), 18 hours after cold
ischemia; 6h CIT+12h EVLP, 6 hours of cold ischemia followed by 12 hours of EVLP, 18h
CIT/1h post rep, 1 hour after transplantation and reperfusion of 18h CIT group; EVLP/1h post
rep, 1 hour after transplantation and reperfusion of 6h CIT+12h EVLP group; Recipient left
lung, normal lung tissue samples.

90
6hCIT
18h
CIT
(tim
ed con
trol
)
6h C
IT+1
2h E
VLP
6h C
IT+1
2h E
VLP
+IL-
10
0
2
4
6
8
10
A
iNO
S m
RN
A
(Fo
ld c
han
ge f
ro
m 0
h-C
IT)
6hCIT
18h
CIT
(tim
ed con
trol
)
6h C
IT+1
2h E
VLP
6h C
IT+1
2h E
VLP
+IL-
10
0
2
4
6
8
1020
25 **B
Arg
inase 1
mR
NA
(Fo
ld c
han
ge f
ro
m 0
h-C
IT)
6hCIT
18h
CIT
(tim
ed con
trol
)
6h C
IT+1
2h E
VLP
6h C
IT+1
2h E
VLP
+IL-
10
0
5
10
15
20
40
60*
*C
Arg
inase 2
mR
NA
(Fo
ld h
an
ge f
ro
m 0
h-C
IT)
Figure 4-4: EVLP does not affect iNOS expression but increases arginase1 and arginase2 mRNA
expression in lung; * p<0.05, Kruskal-Wallis test, Dunn's multiple comparison test.
A, iNOS mRNA (fold change to time of harvesting); B, arginase1 mRNA (fold change to time of
harvesting); C, arginase2 mRNA (fold change to time of harvesting). Samples were taken at
different time points: 6h CIT, 6 hours after cold ischemia; 18h CIT (timed control), 18 hours
after cold ischemia; 6h CIT+12h EVLP, 6 hours of cold ischemia followed by 12 hours of
EVLP, 6h CIT+12h EVLP+IL-10, 6 hours of cold ischemia followed by 12 hours of EVLP in
the “EVLP+IL-10” group. Data for 6h CIT and 18h CIT are identical to Figure 4-2.

91
Table 4-3 Indices of L-arginine bioavailability and NOS impairment in lungs at different time
points in the “EVLP” and “no EVLP” groups and in recipient left lungs
Num
ber o
f
samples
L-arg
inin
e/L-
orn
ithin
e
L-arg
inin
e/ (L-
orn
ithin
e+L
-
citrullin
e)
L-o
rnith
ine/L
-
citrullin
e
L-arg
inin
e/
AD
MA
18 h CIT (timed
control) 4 5.18±0.97 3.07±0.36 1.80±0.35 159.7±26.88
6h CIT+12h EVLP 6 11.65±3.03 7.89±1.79 3.29±0.69 188.1±19.86
18h CIT/1h post rep 4 4.55±0.91 2.77±0.48 1.71±0.30 232.1±26.15
EVLP/1h post rep 6 7.12±1.14 4.13±0.37 1.62±0.20 240.5±17.29
Recipient left lung 5 4.93±0.82 2.51±0.27 1.16±0.16 194.4±20.63
Ratios for amino acids availability and NOS impairment are shown as meanSEM. Samples
were taken at different time points: 18h CIT (timed control), 18 hours after cold ischemia; 6h
CIT+12h EVLP, 6 hours of cold ischemia followed by 12 hours of EVLP, 18h CIT/1h post
rep, 1 hour after transplantation and reperfusion of 18h CIT group; EVLP/1h post rep, 1 hour
after transplantation and reperfusion of 6h CIT+12h EVLP group; Recipient left lung, normal
lung tissue samples.

92
Table 4-4: Lung NOx concentrations and in vitro arginase activity in “EVLP” and “no EVLP”
groups and in recipient left lungs.
Num
ber o
f
samples
Arg
inase
activity
Num
ber o
f
samples
NO
x
0h CIT 16 11.12±1.81 15 2.14±0.39
6h CIT 11 10.6±1.54 9 2.26±0.52
18 h CIT (timed control) 4 10.22±2.85 4 1.37±0.21
6h CIT+12h EVLP 6 6.71±0.83 6 0.71±0.19
6h CIT+12h EVLP +IL-10 8 8.15±2.02 7 0.47±0.15
18h CIT/1h post rep 4 9.80±2.41 4 1.79±0.29
EVLP/1h post rep 6 9.78±1.37 6 1.32±0.16
EVLP+IL-10/1h post rep 8 8.58±1.86 7 1.30±0.37
Recipient left lung 13 13.24±1.27 9 2.56±0.22
Concentrations of NOx (mol/g protein) and in vitro arginase activity(mUnit/ mg protein) are
shown as meanSEM. Samples were taken at different time points as follows: 0h CIT, after
harvesting the lung from donor and flushing with Perfadex
; 6h CIT, 6 hours after cold
ischemia; 18h CIT (timed control), 18 hours after cold ischemia; 6h CIT+12h EVLP, 6 hours of
cold ischemia followed by 12 hours of EVLP, 6h CIT+12h EVLP+IL-10, 6 hours of cold
ischemia followed by 12 hours of EVLP in the “EVLP+IL-10” group; 18h CIT/1h post rep, 1
hour after transplantation and reperfusion of 18h CIT group; EVLP/1h post rep , 1 hour after
transplantation and reperfusion of 6h CIT+12h EVLP group; EVLP+IL-10/1h post rep, 1 hour
after transplantation and reperfusion of 6h CIT+12h EVLP+IL-10 group ; Recipient left lung,
normal lung tissue samples.

93
4.4.3 NOx is decreased after lung transplantation and reperfusion following EVLP or
EVLP+IL-10
To investigate the effects of EVLP and IL-10 gene therapy during EVLP on the L-arginine/NO
metabolism in lungs after transplantation and reperfusion, we analyzed the samples from lungs 1
hour after transplantation and reperfusion. We found that NOx concentrations were decreased
after transplantation and reperfusion in the “EVLP” group (p<0.05, Kruskal-Wallis test, Dunn’s
multiple comparison) or the “EVLP+IL-10” group (p<0.05, Kruskal-Wallis test, Dunn’s multiple
comparison) when compared to control recipient left lung, respectively (Figure 4-5-A).
In addition, L-citrulline levels in the “EVLP” group were lower after 1 hour of transplantation
and reperfusion than in control recipient left lung (p<0.05, Kruskal-Wallis test, Dunn’s multiple
comparison) (Figure 4-5-B). In contrast, concentrations of L-arginine, L-ornithine and ADMA
were not different in lung 1 hour after transplantation and reperfusion after EVLP or after 18h
hypothermic preservation (timed control) when compared to the normal control group (Kruskal-
Wallis test) (Table 4-2). Again, similar changes in NOx and L-citrulline are suggestive of
reduced NOS activity.
iNOS expression was not different after reperfusion in any groups compared to the time of
harvesting (Kruskal-Wallis test) (Table 4-1). However, in the “EVLP” or “EVLP+IL-10” groups
arginase 1 mRNA expression was significantly higher 1 hour after transplantation and
reperfusion than at the time of harvesting (0h CIT) (p<0.01, Kruskal-Wallis test, Dunn’s multiple
comparison) (Figure 4-6-B). Additionally, arginase 2 expression 1 hour after transplantation and
reperfusion was significantly higher than at the time of harvesting (0h CIT) in all groups (p<0.05
for 18h CIT/1h post rep and EVLP/1h, p<0.01 for EVLP+IL-10/1h post rep, Kruskal-Wallis
test , Dunn’s multiple comparison). Increased arginase activity could contribute to decreased NO
production. Interestingly, however, the L-arginine/ (L-ornithine+L-citrulline) ratio, an index of
global L-arginine bioavailability, was higher in lungs 1 hour after transplantation and reperfusion
in the “EVLP” group than in normal lungs (p<0.05, Kruskal-Wallis test, Dunn’s multiple

94
comparison) (Figure 4-6-D). Moreover, in vitro arginase activity was not different in any groups
after transplantation and reperfusion compared to normal controls (Kruskal-Wallis test) (Table
4-4).
We must mention that, the mRNA expression for arginase 1 and arginase 2 (ratio of
arginases/actin) was not different in recipient left lung (unpaired t test), which contained blood,
and donor lungs at the time of harvesting (0h CIT), which were blood free (Figure 4-6-A, Figure
4-6-C). Thus for analysis of arginase mRNA expression we used data from lungs at the time of
harvesting for comparison of all time points including sample from lungs 1 hour after
transplantation and reperfusion.
These analyses revealed that NO production is reduced after EVLP, EVLP + IL-10 or one hour
after transplantation and reperfusion of lungs.

95
Rec
ipie
nt le
ft lu
ng
18h
CIT
/1-h
pos
t rep
EVLP
/1-h
pos
t rep
EVLP
+IL-
10/1
-h p
ost r
ep
0
2
4
6*
*AN
Ox (
mo
l/g
pro
tein
)
Rec
ipient
left lu
ng
18h
CIT
/1h
post rep
EVLP/1
h po
st rep
0
2
4
6
8 *B
L-c
itru
llin
e
nm
ol/
mg
pro
tein
Rec
ipient
left lu
ng
18h
CIT
/1h
post rep
EVLP/1
h po
st rep
0
2
4
6
*C
L-a
rg
inin
e/L
-orn
ith
ine+
L-c
itru
llin
e
Figure 4-5: NOx and L-citrulline levels decrease after lung transplantation and reperfusion while
global L-arginine availability increases (* p<0.05, Kruskal-Wallis test, Dunn's multiple
comparison test).
A, NOx (mol/g protein); B, L-citrulline (nmol/mg protein); C, global L-arginine availability.
Samples were taken at different time points as follows: 18h CIT/1h post rep, 1 hour after
transplantation and reperfusion of 18h CIT group (timed control); EVLP/1h post rep, 1 hour
after transplantation and reperfusion of 6h CIT+12h EVLP group; EVLP+IL-10/1h post rep, 1
hour after transplantation and reperfusion of 6h CIT+12h EVLP+IL-10 group; Recipient left
lung, normal lung tissue samples.

96
0h C
IT
Rec
ipient
left lu
ng
0
2
4
6
A
Arg
1/
acti
n
0h C
IT
Rec
ipient
left lu
ng
0
2
4
6
8
10
B
Arg
2/
acti
n
0h C
IT
18h
CIT
/1-h
pos
t rep
EVLP
/1-h
pos
t rep
EVLP
+IL-
10/1-h
pos
t rep
0
5
10
15
20
25
**
**C
Arg
inase 1
mR
NA
(Fo
ld C
han
ge f
rom
0h
-CIT
)
0h C
IT
18h
CIT
/1-h
pos
t rep
EVLP
/1-h
pos
t rep
EVLP
+IL-
10/1-h
pos
t rep
0
5
10
15
20
40
60
***
*D
Arg
inase 2
mR
NA
(Fo
ld C
han
ge f
rom
0h
-CIT
)
Figure 4-6: Arginase1 and arginase2 mRNA expression is not different in recipient left lung
compared to 0h CIT (unpaired t test). Arginase1 and arginase2 mRNA expressions increase after
lung transplantation and reperfusion (**p<0.01; * p<0.05, Kruskal-Wallis test, Dunn's multiple
comparison test).
A, arginase1 mRNA (arginase1/β actin); B, arginase2 mRNA (arginase2/β actin); C, arginase1
(fold change to time of harvesting); D, arginase2 (D) mRNA (fold change to time of harvesting).
Samples were taken at different time points: 18h CIT/1h post rep, 1 hour after transplantation
and reperfusion of 18h CIT group (timed control); EVLP/1h post rep, 1 hour after
transplantation and reperfusion of 6h CIT+12h EVLP group; EVLP+IL-10/1h post rep, 1 hour
after transplantation and reperfusion of 6h CIT+12h EVLP+IL-10 group; Recipient left lung,
normal lung tissue samples.

97
4.5 Discussion
In this section we measured NOx concentrations as well as the expression and activity of
arginases in lung tissue in order to study effects of cold ischemia on the balance of arginase and
NOS activity. We also measured concentrations of L-arginine and its metabolites as well as
tissue expression of arginase isoforms and total arginase activity to study the effects of EVLP
and of IL-10 gene therapy during EVLP on the L-arginine/NO metabolism in the lung. In
addition, we studied the effects of these interventions during lung preservation on concentrations
of L-arginine and its metabolites as well as on arginase expression and activity in lungs 1 hour
after transplantation and reperfusion. Our data demonstrated that 6 or 18 hours of cold
preservation had no effects on the L-arginine/NO metabolism in lung tissue. In contrast, after
EVLP or EVLP+IL10 gene therapy NOx levels were lowered. L-citrulline levels in lungs after
EVLP were also lower than timed control. Moreover, arginase 1 and 2 mRNA expressions were
increased in lungs after EVLP or EVLP+IL-10 compared to normal controls. We also observed
reduced NOx and L-citrulline levels in addition to increased arginase1 and 2 mRNA expression
in the EVLP and EVLP+IL-10 groups one hour after transplantation and reperfusion. Therefore,
EVLP caused changes in the L-arginine/NO metabolism in lungs an effect that was sustained one
hour after transplantation and reperfusion. IL-10 gene therapy during EVLP did not affect these
alterations.
4.5.1 Cold ischemia does not cause alteration in the L-arginine/NO metabolism
It is well known that cold ischemia results in metabolic changes in the lung.72, 183
In the previous
chapter however, we had found that cold ischemia had no significant effect L-arginine, L-
ornithine, L-citrulline or ADMA in lung homogenates, when expressed as log-normalize data as
a scaled intensity (relative quantification). Small differences did however result in a lower L-
ornithine/L-citrulline ratio after 6 hours of cold ischemia compare to the time of harvesting (0h
CIT). This observation could be reflective of a change in the balance of arginase and NOS
activity.121

98
In the previous chapter HPLC-MS was used to quantify the L-arginine metabolites but NOx, a
surrogate marker of NOS activity, was not measured in those samples. Therefore, for this part of
the thesis, we processed lung tissue samples after cold ischemia of different lengths for NOx
measurements, iNOS gene expression, arginases gene expression and total arginase activity. Our
data showed that none of these measures were affected by 6 or 18 hours of cold ischemia (Table
4-1, Table 4-4). Therefore, we concluded that cold ischemia has no effect on the L-arginine/NO
metabolism in lung tissue.
In a different study of lung transplantation in the rat it was shown that NO production after 6
hours of cold preservation was decreased compared to fresh lungs.174
In this model NO was
directly measured using an electrode on the surface of the lung tissue,174
which is different from
our study as we measured stable NO metabolites including nitrites, nitrates and S-nitrosothiols in
lung tissue homogenates. NO is produced intracellular and NO production on the surface of lung
tissue might not represent NO production by all cell types in the lung tissue. On the other hand,
similar to our study in pigs, in a model of lung transplantation in the rat the expression of all
isoforms of NOS remained unchanged after 12 hour of cold preservation compared to the
baseline.190
Results from this study also supports the idea that hypothermic preservation does not
affect the L-arginine/NO metabolism.
4.5.2 NOx and L-citrulline in lung tissue decrease after EVLP and remained below
normal after reperfusion
Normothermic EVLP provides physiological conditions12, 14, 17, 25
but may cause changes in
cellular metabolism in lung tissue over time.191
However, to our knowledge, the NO metabolism
in lung tissue has not been previously described after EVLP. Thus, in the next step we tried to
determine whether EVLP had an effect on the L-arginine metabolism.
Our data revealed that lung NOx concentrations after 12 hours of EVLP were lower than after 6h
CIT (before EVLP) (Figure 4-3-A). In addition, NOx and L-citrulline concentrations, both
products of NOS activity, were lowered after EVLP compared to the timed control group (18h
CIT) (Figure 4-3-A, B). Similar to our study, it was shown that FeNO, one other surrogate

99
measure of lung NO production, was reduced in the isolated perfused and ventilated pig lung.192
Decreased NOx and L-citrulline concentrations were also demonstrated after transplantation and
reperfusion in the “EVLP” group (Figure 4-5-A, B). Hence, based on parallel changes of both
products of NOS we concluded that EVLP resulted in decreased NOS activity which was not
resolved 1 hour after transplantation and reperfusion. Interestingly, IL-10 gene therapy during
EVLP had no measurable effect on NO metabolites after EVLP or after transplantation and 1
hour reperfusion.
Members of Dr, Keshavjee’s lab from the Toronto lung transplant program reported that the
physiological assessment of animals, such as PaO2, after transplantation and reperfusion in the
no EVLP (timed control) group was lower than in EVLP group (unpublished data). Thus, it is
possible that changes in NO production from NOS contribute to clinical outcomes. IL-10 gene
therapy during EVLP resulted in better lung function 7 days after transplantation (Dr,
Keshavjee’s lab, unpublished data). Hence, evaluation of the L-arginine/NO metabolism after
EVLP and 1 hour after reperfusion may not be an indicator for long term effects of IL-10.
To investigate potential causes of decreased NOx and L-citrulline concentrations, the NOS
inhibitor ADMA, mRNA expression of iNOS and arginase isoforms as well as in vitro arginase
activity were measured. As explained earlier, L-arginine is metabolized to L-citrulline and NO
by NOS isoforms, ADMA is an endogenous competitive inhibitor of NOS and arginase competes
with NOS for L-arginine as substrate.98, 99
Alterations in the expression and activity of NOS can
lead to changes in NO production. We did not find significant changes in mRNA expression of
iNOS. NOS expression and activity were investigated in a few earlier studies in lung
transplantation, with conflicting results.56, 190, 193
Similar to our study, 15 minutes after EVLP
using STEEN solution™ as perfusate, iNOS gene expression was not affected in lungs in a rat
model of EVLP.56
Conversely, the expression of iNOS mRNA in allograft lungs after ex vivo
reperfusion was higher than in normal lung in other rat models of lung transplantation190, 193
while eNOS expression decreased.190
These models were designed to mimic the acute rejection
or I/R injury after lung transplantation. In our study samples were collected from lungs that
mimicked clinically accepted lungs without serious injuries. Sever lung injuries may contribute
to high expression of iNOS in response to inflammation in other studies.190

100
We found similar levels of ADMA and L-arginine/ADMA ratios at different time points in all
groups (Table 3-1). The L-arginine/ADMA ratio can be used as an index for NOS impairment, as
ADMA acts as a competitive and reversible inhibitor of NOS.144
These findings indicated that
ADMA is not responsible for reduced NO production. In the previous chapter we also observed
that ADMA levels after transplantation and reperfusion in lungs from different types of donor
were similar.
The availability of L-arginine for NOS is a critical factor for NO production.98, 99
Other authors
used indices such as L-arginine/L-ornithine and arginine/L-ornithine+L-citrulline in serum to
estimate the L-arginine bioavailability for intracellular NOS at a given L-arginine
concentration.98, 99, 115, 135, 136
We used tissue homogenates to measure concentrations of amino
acids. Therefore, changes in intracellular L-arginine availability may not be reflected by these
ratios in tissue homogenates. We did not find changes in these indices at different time points
with the exception of an increased L-arginine/ (L-ornithine+L-citrulline) ratio at 1 hour post-
transplantation and reperfusion in the “EVLP” group compared to control (recipient left lung)
(p=0.0083, unpaired t test) (Figure 4-5-C). However, measurements of expression and activity of
amino acid transporters are needed to understand changes in the cellular L-arginine uptake
during transplantation.
Another contributor for decreased L-arginine bioavailability for NOS is increased expression and
activity of arginases, competing enzymes for NOS.122
The expression of arginase isoforms and in
vitro arginase activity after lung transplantation and reperfusion were not published previously.
Our data showed that mRNA expression of arginase isoforms was increased after EVLP, and
transplantation and reperfusion of the “EVLP” and “EVLP+ IL-10” groups compared to the time
of harvesting which could explain reduced NO production. However, in vitro arginase activity
was not changed. Moreover, concentration of L-ornithine, a product of arginase activity, was
similar at all time points.
Urea, the other product of arginase activity,99
cannot be used as a reliable indicator for in vivo
arginase activity as urea concentrations depend on other variables such as dehydration and renal
function. Blood urea nitrogen (BUN) is higher in dehydrated patients because urine flow rate

101
decreases and renal urea reabsorption increases in dehydration state.187
In addition, insufficient
clearance of urea from the blood because of renal dysfunction during and after surgery can result
in very high concentration of urea.188
There are also other important sources of urea. For
example, urea can be produced from ammonium by hepatocytes via the urea cycle.194
Therefore
we did not measured urea concentrations in our study.
There was a possibility that in the isolated circuit of EVLP the differences in NOx and L-
citrulline were caused by dilution effects of acellular perfusate, which contained human serum
albumin, dextran, electrolyte, heparin, Solu-Medrol, and Cefazolin (Table 2-1).15, 24, 163
NOx
concentration in the perfusate was significantly lower than in lung tissue homogenates
(2.417±0.3708 in perfusate vs. 197.1±19.53 µM before correction with protein concentration in
tissue homogenates, p<0.0001, unpaired t test). However, importantly no differences were found
for any of the other amino acids that were measured and of ADMA (Table 4-2). If acellular
perfusate had dilution effects on L-citrulline and NOx, we should expect that concentrations of
other amino acids after EVLP should also be lower than before EVLP. Therefore, lower NOx
and L-citrulline concentrations after EVLP are unlikely to be caused by a dilution effect of the
perfusate.
Systemic changes in the L-arginine metabolism in the recipient during the transplantation
procedure may contribute to changes in L-citrulline and NOx levels in lungs after transplantation
and reperfusion compared to recipient left lung. Samples from the recipient left lung were taken
about 2 hours after induction of anesthesia in the recipient, while the samples from re-perfused
lungs were taken from the same animals 3 to 4 hours later. Therefore, longer period of surgery
and longer starvation time as well as blood loss, dehydration and renal failure due to the surgery
could result in differences in biochemical markers.188, 195
However, transplantation and
reperfusion had no effect on concentrations of L-arginine, L-ornithine or ADMA in lungs
compared to recipient left lungs (Table 4-2). Thus, we have evidence that systemic changes in
the L-arginine/NO metabolism are not responsible for the decrease in NOx and L-citrulline
concentrations. Decreased NO production after transplantation and reperfusion has been
previously described in a rat model of lung transplantation, which is in agreement with our
conclusion.174

102
There are a number of limitations of this study. Western blotting for protein expression of
arginase isoforms were not run in a same blot for electrophoresis because only 15 wells were
available in each blot. Therefore, a comparison of data from Western blotting could be
problematic and must be interpreted with caution. Although we calculated the ratio of target
proteins to housekeeping protein (β actin), the observed differences might be influenced by other
factors. For instance, films are extremely sensitive to chemiluminescent signals but the dynamic
range of quantification is limited, small differences in the length of exposure time to the films
would result in remarkable differences in the density.196
Therefore, data from western blotting
were not used in this study (appendix).
Moreover, the expression of eNOS and nNOS mRNA as well as the protein expression for all
isoforms of NOSs and activity of each isoforms of NOS were not measured in the present study.
Therefore we can only speculate that changes in NOx concentration would not be driven by
changes iNOS at mRNA transcriptional level. Furthermore, in the present study concentrations
of L-arginine, L-ornithine, L-citrulline and ADMA in the lungs were not measured at the time of
harvesting (0h CIT) and at 6 hours cold ischemia in the “EVLP” and “no EVLP” groups as well
as all time points in the “EVLP+IL-10” group. Data for these time points may have allowed us to
understand whether IL-10 gene therapy had an effect on the L-arginine/NO metabolism in lung
tissue.
To quantify arginase activity in vitro, we provided high concentrations of L-arginine, i.e. 20
mM172
compare to normal plasma concentration of 150-250 µM.197
Consequently, the effect of
substrate availability and the role of endogenous competitive enzyme inhibitors are eliminated.
Therefore, the results of in vitro arginase activity may not accurately reflect in vivo enzyme
activity. However, we did not find differences in the concentration of L-ornithine, a product of
arginase activity, in lung homogenates at different time points in different groups which
suggested that arginase activity was not altered in vivo.
Furthermore, the L-arginine ratios might not be appropriate indices in our study as we measured
these amino acids in tissue homogenate but not serum. Therefore, these ratios in our study might
not reflect the bioavailability of L-arginine for intracellular NOS.

103
In summary, in this chapter we found that hypothermic preservation of up to 18 hours did not
result in changes in the L-arginine/NO metabolism in lung tissue. These finding are consistent
with findings in the previous chapter, where concentrations of L-arginine, L-ornithine and L-
citrulline after different lengths of cold ischemia remained unchanged. Interestingly, NO
production by NOS in lung tissue was decreased after EVLP and stayed below normal 1 hour
after transplantation and reperfusion. These alterations were not driven by changes in iNOS
mRNA expression or ADMA concentration. After EVLP, transplantation and reperfusion the
expression of arginases was increased. IL-10 gene therapy during EVLP did not prevent changes
in the L-arginine/NO metabolism introduced by EVLP.
Further investigations of for instance the L-arginine transporters systems may help understand
causes of the observed alteration in the L-arginine/NO metabolism. Overall, our findings suggest
that EVLP resulted in a decrease in lung NOS activity that was sustained after transplantation
and reperfusion and was unaffected by IL-10 gene therapy during EVLP.

104
Chapter 5: Discussion, conclusion and future
directions

105
NO plays important roles in I/R injury and in rejection following lung transplantation.88, 179
The
design of our study allowed us to investigate effects of different length of cold ischemia on the
L-arginine/NO metabolism. We were able to characterize the L-arginine/NO metabolism in the
lungs of brain death donors in comparison to lungs with prolonged preservation. The model also
provided an opportunity to investigate effects of EVLP and of IL-10 gene therapy during EVLP
on the L-arginine/NO metabolism at different stages of lung transplantation. We observed that
different lengths of cold ischemia had no effect on concentration of L-arginine and its
metabolites in lung tissue. Metabolic profile of the L-arginine metabolism was different in lungs
of brain death donors compared to lungs after prolonged cold preservation. Importantly, we
found that lung L-citrulline and NOx concentrations following EVLP were decreased, and
remained decreased after transplant and reperfusion. IL-10 gene therapy during EVLP had no
effect on NOx or L-citrulline levels after transplantation.
5.1 Regulation of NO production
5.1.1 NOS expression and activity
NO production by iNOS in cells can be regulated at gene transcription levels in response to
inflammation.111, 112
Therefore, iNOS mRNA expression at different stages of lung
transplantation was investigated in our study. Expression and activity of NOS have been
investigated in other studies in lung transplantation settings. For instance, in a rat model of lung
transplantation, it was shown that 12 hours of cold preservation had no effect on iNOS mRNA
expression, however, iNOS was increased significantly 2 hours after reperfusion.190, 193
Increased
iNOS expression and higher NO production was described at the early phases of acute lung
rejection after transplantation.193, 198, 199
The severity of acute lung rejection after transplantation
was attenuated after inhibition of iNOS in a rat model.200
Protein expression of iNOS and eNOS
in lung tissue increased significantly after reperfusion while total NOS activity was not changed
and stayed at very low levels in a rat model.190
We did not find any differences in iNOS mRNA
expression at different time points which means that cold ischemia, EVLP, IL-10 gene therapy
during EVLP or transplantation and reperfusion did not result in detectable induction of iNOS
expression in lung.

106
5.1.2 ADMA an endogenous NOS inhibitor
NOS inhibitors such as ADMA can cause a significant decrease in NO production.77, 118
Changes
in ADMA concentration contribute to the pathogenesis of pulmonary diseases such as asthma
and cystic fibrosis.118, 139
The ratio of L-arginine/ADMA is considered as an index for
impairment of NOS activity.144
Our data did not show differences in ADMA concentration or L-
arginine/ADMA ratio at different time points of lung transplantation, suggesting that ADMA did
not contribute to changes in NOS activity following lung transplantation.
5.1.3 L-arginine availability for NOS
Changes in concentration and availability of substrate L-arginine would result in changes in NO
production by NOS.98
Arginase and NOS are intracellular enzymes.98, 99
L-arginine, L-ornithine
and L-lysine compete for intracellular uptake via amino acid transporters.98, 99
Thus, the ratios of
L-arginine/L-ornithine and of L-arginine/ (L-ornithine+L-lysine) in serum can be used as indices
for L-arginine availability for intracellular NOS at a given L-arginine serum concentration.98, 99,
115 Additionally, in studies of cardiovascular disease, the ratio of L-arginine/ (L-ornithine+L-
citrulline) in serum, the products of enzymatic conversion from L-arginine by arginase and NOS,
is used as an index for global L-arginine availability.135, 136
The use of L-arginine bioavailability
indices has not been reported in lung transplantation previously. However, effects of L-arginine
supplementation during and after lung transplantation were investigated in some studies.73, 153, 180,
201 For instance, L-arginine supplementation in preservation solution during prolonged lung
preservation in a dog model of lung transplantation improved pulmonary endothelium dependent
relaxation.201
We did not find differences in L-arginine concentration at different time points in
our model. However, the L-arginine/ (L-ornithine+L-citrulline) ratio in lung from the “EVLP”
group was higher after transplantation and reperfusion than in normal control lungs, suggesting
that substrate availability was increased, not decreased.
In our study, amino acids and ADMA were measured in lung tissue homogenates. Calculation of
ratios in lung tissue may not accurately represent intracellular L-arginine availability for NOS as
these indices in serum represent L-arginine bioavailability. However, differences in these ratios

107
at different time points may reflect alterations in the L-arginine/NO metabolism. Additional
studies are needed for an interpretation of the evidence for increased global L-arginine
bioavailability after transplantation and reperfusion. For example, measurement of amino acid
concentration in serum and perfusate would be helpful. Investigation of expression and activity
of arginases would also provide supporting data for possible changes in L-arginine availability.
5.1.4 Arginase expression and activity
Changes in arginase expression and activity can alter L-arginine bioavailability for NO
production, as arginase and NOS compete for L-arginine as substrate. Increased arginase
expression and activity leads to reduced L-arginine availability for NOS and consequently
decreased NO production.132, 202, 203
Increased protein expression of arginase isoforms and
arginase activity have been shown in acute rejection in a rat model of lung transplantation204
where they resulted in higher peak airway pressure and increased collagen deposition.204
These
changes could be prevented by pirfenidone, an antifibrotic medication which reduces arginase
expressions and activity.204
Furthermore, administration of the arginase inhibitor 2(S)-amino-6-
boronohexanoic acid (ABH) during EVLP improved dynamic compliance in human lungs which
were deemed unacceptable for transplantation.205
In this study, the authors did not find
differences in arginase 1 and arginase 2 expression, using Western blotting at different time
points.205
We demonstrated that the length of cold ischemia had no effect on the concentration of
L-ornithine, a product of arginase activity, expression of arginase 1 and arginase 2 mRNA, or in
vitro activity of arginase. However, after EVLP mRNA expression of arginase 1 and 2 in lung
homogenates was higher than in controls, which did not result in differences in L-ornithine
concentration or arginase activity in vitro. Therefore, the observed effects of transplantation on
lung tissue levels of products of NOS activity (NOx and L-citrulline) are unlikely to be caused
by decreased L-arginine availability due to increased arginase activity.
5.2 Other possible causes for decreased NOx and L-citrulline
Decreased NO production in the presence of L-arginine and unchanged NOS mRNA expression
could be caused by co-factor deficiency. Co-factors including NADPH, BH4, FMN and FAD are

108
essential for the activity of NOS isoforms.98, 99, 110, 111
Ischemia causes oxidative stress which
results in oxidation of BH4 and consequently uncoupling of NOS. This means that BH4
deficiency causes decreased NO but increased oxygen free radical production by NOS.206
This
process can contribute to I/R injury following lung transplantation.81
Therapeutic effects of BH4
via the NO pathway after ischemia and reperfusion were previously demonstrated. In a pig
model administration of BH4 during preservation and after reperfusion ameliorated post-
transplant edema and I/R injury.207
Concentrations of co-factors for NOS were not measured in
our study.
Consumption of NO rather than decreased production would also result in decreased NOx
concentrations. For example, limited L-arginine availability for iNOS leads to iNOS uncoupling
and production of oxygen radicals which then interact with NO to produce peroxynitrite.99
It was
shown in humans that after acute lung injuries peroxynitrite was produced, which may contribute
to inflammatory responses.208
Peroxynitrite was not measured in our study. It is also conceivable
that NO after reperfusion is bound to circulating haemoglobin, which would result in decreased
NOx concentration in lung tissue.
The metabolism of L-citrulline is complex as it can be produced by NOS but also other
pathways. For example, OTC metabolizes L-ornithine to form L-citrulline and phosphate, while
DDAH uses ADMA to produce L-citrulline and dimethylamine. L-citrulline can also be
produced by proteolysis activities. On the other hand argininosuccinate synthetase (ASS) can
convert L-citrulline to argininosuccinate.195
Therefore, alterations in L-citrulline production or
catabolism through other pathways can also change L-citrulline concentrations, and L-citrulline
concentrations may not accurately reflect NOS activity.
There are other factors, e.g. changes in pH, which may results in changes in NO production.99, 111,
150, 209 Acidosis for instance can result in up-regulation of iNOS activity in macrophages.
210
However, in this thesis the pH of lung tissue samples was not measured. Endogenous NOS
inhibitors other than ADMA may also result in decreased NO production. For example, in a
mouse model of allergic asthma it was shown that the polyamine spermin contributed to NOS
inhibition causing airways hyper-responsiveness.211
Polyamines are interesting as they are L-

109
ornithine derived and changes in arginase activity may therefore result in differences in
polyamine biosynthesis.119, 122
However, polyamines were not measured in this study and are
unlikely to be affected in our model as L-ornithine concentration was not altered.
5.3 Interleukin (IL)-10
IL-10 is an immunoregulatory cytokine that has been shown to suppress iNOS212, 213
and
decrease NO production in mouse macrophages and human keratinocytes.51, 158
Alveolar
macrophages in donor lung contribute to the early phase of I/R injury72, 85, 86
as they are a
primary source of cytokines (specifically IL-8, IL-10 and TNF-α) and peroxynitrite.214
The
balance between iNOS and arginase expression has been demonstrated to play an important role
in polarization of alveolar macrophages in response to environmental stimuli.127
Plasticity of
macrophages (i.e. phenotype switch) results in alterations of the production of proinflammatory
and anti-inflammatory cytokines such as IL-8 and IL-10 by macrophages, which are important in
the induction and prevention of I/R injury, respectively.72
Beneficial effects of IL-10 gene therapy during EVLP were reported previously.15, 24
In our
study, PaO2/FiO2, an indicator of lung quality, was not different one hour after reperfusion when
comparing the “EVLP+IL-10” and “EVLP” groups. However, seven days after transplantation
PaO2/FiO2 was significantly higher in the “EVLP+IL-10” group compared to the “EVLP” group
(Dr. Keshavjee’s lab, not published). Therefore, IL-10 gene therapy during EVLP resulted in
better long term lung function following lung transplantation compared to lungs which
underwent EVLP but no IL-10 gene therapy. Thus, beneficial effects reported at later time points
may not be reflected in metabolic changes at the earlier time points. Whether IL-10 gene therapy
during EVLP may have effects on the L-arginine/NO metabolism at later time points needs to be
investigated.
5.4 Conclusions
Marginal organs, such as donations after cardiac death, are considered an immediate solution to
expand the donor pool for solid organ transplantation. 3, 10, 11
The rate of morbidity and mortality
following transplantation of marginal lungs is potentially higher than those from standard

110
donors. 3, 11
Understanding alterations in biochemical pathways such as the L-arginine/NO
metabolism in lung tissue during transplantation has the potential to not only provide new
biomarkers for the assessment of donor lungs, but may also help identify pathways that can serve
as targets for novel therapeutic interventions.
In this thesis we demonstrated that the concentrations of L-arginine and its metabolites in lung
remained unchanged during hypothermic preservation independent of the length of cold ischemia
in organs from non-brain death donors. L-citrulline in lungs from brain death donors after 24
hours of cold ischemia was higher compared to lungs after 30 hours of cold ischemia in non
brain death group. We did find evidence for a shift of the L-arginine metabolism toward NOS
after 6 hours of cold ischemia however, a similar effect was not observed after 30 hours of
hypothermic preservation.
The L-arginine/NO metabolism was dissimilar in lungs of different types of donation (i.e. brain
death vs. non-brain death donors). Differences in the L-arginine/NO metabolism could
potentially contribute to the physiological responses and clinical outcomes after transplantation,
as injured lungs from brain death donors had significantly higher PVR after cold ischemia (at the
beginning of EVLP) and the worst post-transplant outcome.25
NOx concentrations were
decreased after EVLP an effect that was sustained after transplantation and reperfusion of these
lungs. Interestingly, arginase mRNA expression was found to be higher than normal after
transplantation and reperfusion, which may lead to decreased L- arginine availability for NOS
and thus contribute to decreased NO production. IL-10 gene therapy did not affect these
alterations in the L-arginine metabolism. Our findings suggest that EVLP results in alterations in
the L-arginine/NO metabolism in lung and strongly support the first part of the hypothesis that
dysregulation of the L-arginine/NO metabolism after transplantation leads to a decrease in NO
production in lung.
5.5 Future directions
This study provided evidence of alterations in the L-arginine/NO metabolism in lung after EVLP
and after transplantation and reperfusion. These changes may have consequences for the clinical

111
outcome after transplantation. Further investigations using different models of lung
transplantation would help to better understand the correlations between alterations in the L-
arginine/NO metabolism and lung function after transplantation. Assessment of the L-
arginine/NO metabolism 7 days after transplantation and reperfusion, where IL-10 treatment
resulted in a difference in physiological measures, would be interesting as this could help link the
metabolism to lung transplantation outcomes.
The investigation of the L-arginine/NO metabolism in serum, bronchoalveolar lavage fluid,
exhaled NO or perfusates from EVLP also could be considered additional approaches to detect
changes in the L-arginine/NO metabolism. Possible correlation between these measures and lung
function could help surgeons make better decisions in selecting donor lungs for transplantation.
The effect of therapeutic interventions during EVLP, for example a study using NO donors or
inhaled NO, or the use of arginase inhibitors may also be worth studying. Arginase inhibitors
decrease arginase activity and thus increase arginine availability for NOS, which could
potentially result in increased NO production and better post-transplantation outcomes.

112
References

113
1. Kotloff R. M., Thabut G. (2011) Lung transplantation. Am. J. Respir. Crit. Care Med.
184, 159-171. 10.1164/rccm.201101-0134CI
2. Cooper J., Pearson F., Patterson G., Todd T., Ginsberg R., Goldberg M. & DeMajo W.
(1987) Technique of successful lung transplantation in humans. J. Thorac. Cardiovasc.
Surg. 93, 173.
3. Dark J. H. (2008) Lung transplantation from the non-heart beating donor.
Transplantation 86, 200-201. 10.1097/TP.0b013e31817c87b6
4. Organ Procurement and Transplantation Network, OPTN. (2011) Annual report of the
U.S. organ procurement and transplantation network and the scientific registry of
transplant recipients: transplant data 2001, 2006 &2011. Department of Health and
Human Services, Health Resources and Services Administration, Healthcare Systems
Bureau, Division of Transplantation, Rockville, MD; United Network for Organ Sharing,
Richmond, VA; University Renal Research and Education Association, Ann Arbor, MI.
Available from:
http://srtr.transplant.hrsa.gov/annual_reports/2011/flash/06_lung/index.html#/16/.
Accessed September 25, 2013-Homepage/Web site:
http://optn.transplant.hrsa.gov/latestData/step2.asp?.
5. Avlonitis V. S., Fisher A. J., Kirby J. A. & Dark J. H. (2003) Pulmonary transplantation:
the role of brain death in donor lung injury. Transplantation 75, 1928-1933.
10.1097/01.TP.0000066351.87480.9E
6. Trillium Gift of Life Network. (2013) Availablefrom:
http://www.giftoflife.on.ca/en/stats.htm. Accessed September 25, 2013-Homepage/Web
site: http://www.giftoflife.on.ca/en/.
7. The Canadian Institute for Health Information (CIHI). Availablefrom:
https://secure.cihi.ca/free_products/2013_CORR_Annua_Report_EN.pdf. Accessed
November 7,2013-Homepage/Web site:
http://http.myaccess.library.utoronto.ca//www.cihi.ca.
8. Botha P. (2009) Extended donor criteria in lung transplantation. Curr. Opin. Organ.
Transplant. 14, 206-210. 10.1097/MOT.0b013e328326c834
9. Sommer W., Kuhn C., Tudorache I., Avsar M., Gottlieb J., Boethig D., Haverich A. &
Warnecke G. (2013) Extended criteria donor lungs and clinical outcome: Results of an
alternative allocation algorithm. J. Heart Lung Transplant. 32, 1065-1072.
10.1016/j.healun.2013.06.021
10. Kootstra G., Daemen J. H. & Oomen A. P. (1995) Categories of non-heart-beating
donors. Transplant. Proc. 27, 2893-2894.

114
11. Manara A., Murphy P. & O'Callaghan G. (2012) Donation after circulatory death. Br. J.
Anaesth. 108, i108-i121. 10.1093/bja/aer357
12. Aigner C., Slama A., Hotzenecker K., Scheed A., Urbanek B., Schmid W., Nierscher F.
J., Lang G. & Klepetko W. (2012) Clinical ex vivo lung perfusion--pushing the limits.
Am. J. Transplant. 12, 1839-1847. 10.1111/j.1600-6143.2012.04027.x
13. Brockmann J., Reddy S., Coussios C., Pigott D., Guirriero D., Hughes D., Morovat A.,
Roy D., Winter L. & Friend P. J. (2009) Normothermic perfusion: a new paradigm for
organ preservation. Ann. Surg. 250, 1. 10.1097/SLA.0b013e3181a63c10
14. Cypel M., Yeung J. C., Hirayama S., Rubacha M., Fischer S., Anraku M., Sato M.,
Harwood S., Pierre A. & Waddell T. K. (2008) Technique for prolonged normothermic
ex vivo lung perfusion. J Heart Lung Transplant. 27, 1319-1325.
10.1016/j.healun.2008.09.003
15. Cypel M., Liu M., Rubacha M., Yeung J. C., Hirayama S., Anraku M., Sato M., Medin J.,
Davidson B. L. & de Perrot M. (2009) Functional repair of human donor lungs by IL-10
gene therapy. Sci Transl Med 1, 4ra9. 10.1126/scitranslmed.3000266
16. Cypel M., Keshavjee S. (2012) The clinical potential of ex vivo lung perfusion. Expert
Rev. Respir. Med. 6, 27-35. 10.1586/ers.11.93
17. Cypel M., Rubacha M., Yeung J., Hirayama S., Torbicki K., Madonik M., Fischer S.,
Hwang D., Pierre A., Waddell T. K., de Perrot M., Liu M. & Keshavjee S. (2009)
Normothermic ex vivo perfusion prevents lung injury compared to extended cold
preservation for transplantation. Am. J. Transplant. 9, 2262-2269. 10.1111/j.1600-
6143.2009.02775.x
18. Cypel M., Yeung J. C., Liu M., Anraku M., Chen F., Karolak W., Sato M., Laratta J.,
Azad S., Madonik M., Chow C. W., Chaparro C., Hutcheon M., Singer L. G., Slutsky A.
S., Yasufuku K., de Perrot M., Pierre A. F., Waddell T. K. & Keshavjee S. (2011)
Normothermic ex vivo lung perfusion in clinical lung transplantation. N. Engl. J. Med.
364, 1431-1440. 10.1056/NEJMoa1014597
19. Erasmus M. E., Fernhout M. H., Elstrodt J. M. & Rakhorst G. (2006) Normothermic ex
vivo lung perfusion of non-heart-beating donor lungs in pigs: from pretransplant function
analysis towards a 6-h machine preservation. Transpl. Int. 19, 589-593. 10.1111/j.1432-
2277.2006.00318.x
20. Nakajima D., Chen F., Yamada T., Sakamoto J., Ohsumi A., Bando T. & Date H. (2012)
Reconditioning of lungs donated after circulatory death with normothermic ex vivo lung
perfusion. J. Heart Lung Transplant. 31, 187-193. 10.1016/j.healun.2011.11.007
21. Pegg D. E. (1986) Organ preservation. Surg. Clin. North Am. 66, 617-632.

115
22. Sanchez P. G., D'Ovidio F. (2012) Ex-vivo lung perfusion. Curr. Opin. Organ.
Transplant. 17, 490-495. 10.1097/MOT.0b013e328357f865
23. Sanchez P. G., Bittle G. J., Burdorf L., Pierson R. N.,3rd & Griffith B. P. (2012) State of
art: clinical ex vivo lung perfusion: rationale, current status, and future directions. J.
Heart Lung Transplant. 31, 339-348. 10.1016/j.healun.2012.01.866
24. Yeung J. C., Wagnetz D., Cypel M., Rubacha M., Koike T., Chun Y. M., Hu J., Waddell
T. K., Hwang D. M., Liu M. & Keshavjee S. (2012) Ex vivo adenoviral vector gene
delivery results in decreased vector-associated inflammation pre- and post-lung
transplantation in the pig. Mol. Ther. 20, 1204-1211. 10.1038/mt.2012.57
25. Yeung J. C., Cypel M., Machuca T. N., Koike T., Cook D. J., Bonato R., Chen M., Sato
M., Waddell T. K., Liu M., Slutsky A. S. & Keshavjee S. (2012) Physiologic assessment
of the ex vivo donor lung for transplantation. J. Heart Lung Transplant. 31, 1120-1126.
10.1016/j.healun.2012.08.016
26. Yuan X., Theruvath A. J., Ge X., Floerchinger B., Jurisch A., Garcia-Cardena G. &
Tullius S. G. (2010) Machine perfusion or cold storage in organ transplantation:
indication, mechanisms, and future perspectives. Transpl. Int. 23, 561-570.
10.1111/j.1432-2277.2009.01047.x
27. Ailawadi G., Lau C. L., Smith P. W., Swenson B. R., Hennessy S. A., Kuhn C. J.,
Fedoruk L. M., Kozower B. D., Kron I. L. & Jones D. R. (2009) Does reperfusion injury
still cause significant mortality after lung transplantation? J. Thorac. Cardiovasc. Surg.
137, 688-694. 10.1016/j.jtcvs.2008.11.007
28. Marshall, V(2001) Pathophysiology of brain death: effects on allograft function.
Transplant. Proc. 33, 845-846. 10.1016/S0041-1345(00)02342-3
29. Smith M. (2004) Physiologic changes during brain stem death—lessons for management
of the organ donor. J. Heart Lung Transplant. 23, S217-S222.
10.1016/j.healun.2004.06.017
30. Floerchinger B., Oberhuber R. & Tullius S. G. (2012) Effects of brain death on organ
quality and transplant outcome. Transplant. Rev. 26, 54-59. 10.1016/j.trre.2011.10.001
31. Barklin A. (2009) Systemic inflammation in the brain‐dead organ donor. Acta
Anaesthesiol. Scand. 53, 425-435. 10.1111/j.1399-6576.2008.01879.x
32. Roman M. A., Nair S., Tsui S., Dunning J. & Parmar J. S. (2013) Ex vivo lung perfusion:
a comprehensive review of the development and exploration of future trends.
Transplantation 10.1097/TP.0b013e318295eeb7
33. Kaneda H., Waddell T., De Perrot M., Bai X. H., Gutierrez C., Arenovich T., Chaparro
C., Liu M. & Keshavjee S. (2006) Pre‐implantation multiple cytokine mRNA expression

116
analysis of donor lung grafts predicts survival after lung transplantation in humans. Am J
Transplant. 6, 544-551. 10.1111/j.1600-6143.2005.01204.x
34. Vogel T., Brockmann J. G. & Friend P. J. (2010) Ex-vivo normothermic liver perfusion:
an update. Curr. Opin. Organ. Transplant. 15, 167. 10.1097/MOT.0b013e328337349d
35. Monbaliu D., Brassil J. (2010) Machine perfusion of the liver: past, present and future.
Curr. Opin. Organ. Transplant. 15, 160-166. 10.1097/MOT.0b013e328337342b
36. Kelly R. F. (2000) Current strategies in lung preservation. J. Lab. Clin. Med. 136, 427-
440. 10.1067/mlc.2000.110906
37. Van Raemdonck D. (2010) Thoracic organs: current preservation technology and future
prospects; part 1: lung. Curr. Opin. Organ. Transplant. 15, 150.
10.1097/MOT.0b013e3283373b7e
38. Ikeyama K., Sakai H., Omasa M., Nakamura T., Hamakawa H., Fujinaga T., Fukuse T. &
Wada H. (2005) Effects of cold preservation on the lung mechanical properties in rats.
Eur. Surg. Res. 37, 85-91. 10.1159/000084538
39. Kim I. K., Bedi D. S., Denecke C., Ge X. & Tullius S. G. (2008) Impact of innate and
adaptive immunity on rejection and tolerance. Transplantation 86, 889-894.
10.1097/TP.0b013e318186ac4a
40. Haverich A., Aziz S., Scott W. C., Jamieson S. W. & Shumway N. E. (1986) Improved
lung preservation using Euro-Collins solution for flush-perfusion. Thorac. Cardiovasc.
Surg. 34, 368-376. 10.1055/s-2007-1022176
41. Hardesty R. L., Aeba R., Armitage J. M., Kormos R. L. & Griffith B. P. (1993) A clinical
trial of University of Wisconsin solution for pulmonary preservation. J. Thorac.
Cardiovasc. Surg. 105, 660-666.
42. Keshavjee S. H., Yamazaki F., Cardoso P. F., McRitchie D. I., Patterson G. A. & Cooper
J. D. (1989) A method for safe twelve-hour pulmonary preservation. J. Thorac.
Cardiovasc. Surg. 98, 529-534.
43. Maccherini M., Keshavjee S. H., Slutsky A. S., Patterson G. A. & Edelson J. D. (1991)
The effect of low-potassium-dextran versus Euro-Collins solution for preservation of
isolated type II pneumocytes. Transplantation 52, 621-626. 10.1097/00007890-
199110000-00008
44. Yamazaki F., Yokomise H., Keshavjee S. H., Miyoshi S., Cardoso P. F., Slutsky A. S. &
Patterson G. A. (1990) The superiority of an extracellular fluid solution over Euro-
Collins' solution for pulmonary preservation. Transplantation 49, 690-694.
10.1097/00007890-199004000-00007

117
45. Carrel A., Lindbergh C. A. (1935) The culture of whole organs. Science 81, 621-623.
10.1126/science.81.2112.621
46. Steen S., Liao Q., Wierup P. N., Bolys R., Pierre L. & Sjöberg T. (2003) Transplantation
of lungs from non–heart-beating donors after functional assessment ex vivo. Ann. Thorac.
Surg. 76, 244-252. 10.1016/S0003-4975(03)00191-7
47. Vekemans K., Liu Q., Pirenne J. & Monbaliu D. (2008) Artificial circulation of the liver:
machine perfusion as a preservation method in liver transplantation. Anat. Rec.
(Hoboken) 291, 735-740. 10.1002/ar.20662
48. García-Valdecasas J. C., Fondevila C. (2010) In-vivo normothermic recirculation: an
update. Curr. Opin. Organ. Transplant. 15, 173. 10.1097/MOT.0b013e3283373488
49. Steen S., Ingemansson R., Eriksson L., Pierre L., Algotsson L., Wierup P., Liao Q.,
Eyjolfsson A., Gustafsson R. & Sjöberg T. (2007) First human transplantation of a
nonacceptable donor lung after reconditioning ex vivo. Ann. Thorac. Surg. 83, 2191-
2194. 10.1016/j.athoracsur.2007.01.033
50. Ingemansson R., Eyjolfsson A., Mared L., Pierre L., Algotsson L., Ekmehag B.,
Gustafsson R., Johnsson P., Koul B. & Lindstedt S. (2009) Clinical transplantation of
initially rejected donor lungs after reconditioning ex vivo. Ann. Thorac. Surg. 87, 255-
260. 10.1016/j.athoracsur.2008.09.049
51. Huang C. J., Stevens B. R., Nielsen R. B., Slovin P. N., Fang X., Nelson D. R. &
Skimming J. W. (2002) Interleukin-10 inhibition of nitric oxide biosynthesis involves
suppression of CAT-2 transcription. Nitric Oxide 6, 79-84. 10.1006/niox.2001.0402
52. Rhoades R. A. (1984) Isolated perfused lung preparation for studying altered gaseous
environments. Environ. Health Perspect. 56, 43-50. 10.2307/3429834
53. Koike T., Yeung J. C., Cypel M., Rubacha M., Matsuda Y., Sato M., Waddell T. K., Liu
M. & Keshavjee S. (2011) Kinetics of lactate metabolism during acellular normothermic
ex vivo lung perfusion. J. Heart Lung Transplant. 30, 1312-1319.
10.1016/j.healun.2011.07.014
54. Valenza F., Rosso L., Pizzocri M., Salice V., Umbrello M., Conte G., Stanzi A., Colombo
J., Gatti S., Santambrogio L., Iapichino G. & Gattinoni L. (2011) The consumption of
glucose during ex vivo lung perfusion correlates with lung edema. Transplant. Proc. 43,
993-996. 10.1016/j.transproceed.2011.01.122
55. Dong B., Stewart P. W. & Egan T. M. (2013) Postmortem and ex vivo carbon monoxide
ventilation reduces injury in rat lungs transplanted from non-heart-beating donors. J.
Thorac. Cardiovasc. Surg. 146, 429-36.e1. 10.1016/j.jtcvs.2012.11.005

118
56. Dong B. M., Abano J. B. & Egan T. M. (2009) Nitric oxide ventilation of rat lungs from
non-heart-beating donors improves posttransplant function. Am. J. Transplant. 9, 2707-
2715. 10.1111/j.1600-6143.2009.02840.x
57. Inci I., Zhai W., Arni S., Inci D., Hillinger S., Lardinois D., Vogt P. & Weder W. (2007)
Fibrinolytic treatment improves the quality of lungs retrieved from non-heart-beating
donors. J. Heart Lung Transplant. 26, 1054-1060. 10.1016/j.healun.2007.07.033
58. Machuca T. N., Hsin M. K., Ott H. C., Chen M., Hwang D. M., Cypel M., Waddell T. K.
& Keshavjee S. (2013) Injury-specific ex vivo treatment of the donor lung: pulmonary
thrombolysis followed by successful lung transplantation. Am. J. Respir. Crit. Care Med.
188, 878-880. 10.1164/rccm.201302-0368LE
59. Christie J. D., Sager J. S., Kimmel S. E., Ahya V. N., Gaughan C., Blumenthal N. P. &
Kotloff R. M. (2005) Impact of primary graft failure on outcomes following lung
transplantation. Chest 127, 161-165. 10.1378/chest.127.1.161
60. Lee J. C., Christie J. D. & Keshavjee S. (2010) Primary graft dysfunction: definition, risk
factors, short- and long-term outcomes. Semin. Respir. Crit. Care. Med. 31, 161-171.
10.1055/s-0030-1249111
61. Christie J. D., Carby M., Bag R., Corris P., Hertz M. & Weill D. (2005) Report of the
ISHLT working group on primary lung graft dysfunction part II: definition. A consensus
statement of the International Society for Heart and Lung Transplantation. J. Heart Lung
Transplant. 24, 1454-1459. 10.1016/j.healun.2004.11.049
62. Barr M. L., Kawut S. M., Whelan T. P., Girgis R., Bottcher H., Sonett J., Vigneswaran
W., Follette D. M., Corris P. A. & ISHLT Working Group on Primary Lung Graft
Dysfunction. (2005) Report of the ISHLT working group on primary lung graft
dysfunction part IV: recipient-related risk factors and markers. J. Heart Lung Transplant.
24, 1468-1482. 10.1016/j.healun.2005.02.019
63. Diamond J. M., Lee J. C., Kawut S. M., Shah R. J., Localio A. R., Bellamy S. L., Lederer
D. J., Cantu E., Kohl B. A., Lama V. N., Bhorade S. M., Crespo M., Demissie E., Sonett
J., Wille K., Orens J., Shah A. S., Weinacker A., Arcasoy S., Shah P. D., Wilkes D. S.,
Ware L. B., Palmer S. M., Christie J. D. & Lung Transplant Outcomes Group. (2013)
Clinical risk factors for primary graft dysfunction after lung transplantation. Am. J.
Respir. Crit. Care Med. 187, 527-534. 10.1164/rccm.201210-1865OC
64. Whitson B. A., Nath D. S., Johnson A. C., Walker A. R., Prekker M. E., Radosevich D.
M., Herrington C. S. & Dahlberg P. S. (2006) Risk factors for primary graft dysfunction
after lung transplantation. J. Thorac. Cardiovasc. Surg. 131, 73-80.
10.1016/j.jtcvs.2005.08.039
65. Lee J. C., Christie J. D. (2009) Primary graft dysfunction. Proc. Am. Thoracic Soc. 6, 39-
46. 10.1513/pats.200808-082GO

119
66. Webert K. E., Blajchman M. A. (2003) Transfusion-related acute lung injury. Transfus.
Med. Rev. 17, 252-262. 10.1016/S0887-7963(03)00039-7
67. Lindberg L., Sjöberg T., Ingemansson R. & Steen S. (1996) Inhalation of nitric oxide
after lung transplantation. Ann. Thorac. Surg. 61, 956-962.
68. Palmer R., Ferrige A. & Moncada S. (1987) Nitric oxide release accounts for the
biological activity of endothelium-derived relaxing factor. Nature 327, 524-526.
69. Meade M. O., Granton J. T., Matte-Martyn A., McRae K., Weaver B., Cripps P.,
Keshavjee S. H. & Toronto Lung Transplant Program. (2003) A randomized trial of
inhaled nitric oxide to prevent ischemia-reperfusion injury after lung transplantation. Am.
J. Respir. Crit. Care Med. 167, 1483-1489. 10.1164/rccm.2203034
70. Keshavjee S., Davis R. D., Zamora M. R., de Perrot M. & Patterson G. A. (2005) A
randomized, placebo-controlled trial of complement inhibition in ischemia-reperfusion
injury after lung transplantation in human beings. J. Thorac. Cardiovasc. Surg. 129, 423-
428. 10.1016/j.jtcvs.2004.06.048
71. Wittwer T., Grote M., Oppelt P., Franke U., Schaefers H. J. & Wahlers T. (2001) Impact
of PAF antagonist BN 52021 (Ginkolide B) on post-ischemic graft function in clinical
lung transplantation. J. Heart Lung Transplant. 20, 358-363. 10.1016/S1053-
2498(00)00226-6
72. de Perrot M., Liu M., Waddell T. K. & Keshavjee S. (2003) Ischemia-reperfusion-
induced lung injury. Am J Respir Crit Care Med. 167, 490. 10.1164/rccm.200207-670SO
73. Mehl A., Grasemann H. (2010) Alterations in L-arginine metabolism after lung
transplantation. Open Nitric Oxide J 2, 55-63. 10.2174/1875042701002020055
74. Date H., Triantafillou A. N., Trulock E. P., Pohl M. S., Cooper J. D. & Patterson G. A.
(1996) Inhaled nitric oxide reduces human lung allograft dysfunction. J. Thorac.
Cardiovasc. Surg. 111, 913-919. 10.1016/S0022-5223(96)70364-1
75. Shargall Y., Guenther G., Ahya V. N., Ardehali A., Singhal A., Keshavjee S. & ISHLT
Working Group on Primary Lung Graft Dysfunction. (2005) Report of the ISHLT
working group on primary lung graft dysfunction part VI: treatment. J. Heart Lung
Transplant. 24, 1489-1500. 10.1016/j.healun.2005.03.011
76. Hohlfeld J. M., Struber M., Ahlf K., Hoeper M. M., Fraund S., Krug N., Warnecke G.,
Harringer W., Haverich A. & Fabel H. (1999) Exogenous surfactant improves survival
and surfactant function in ischaemia-reperfusion injury in minipigs. Eur. Respir. J. 13,
1037-1043. 10.1034/j.1399-3003.1999.13e17.x

120
77. Kimoto M., Whitley G. S., Tsuji H. & Ogawa T. (1995) Detection of NG,NG-
dimethylarginine dimethylaminohydrolase in human tissues using a monoclonal
antibody. J. Biochem. 117, 237-238. 10.1093/jb/117.2.237
78. Warnecke G., Struber M., Fraud S., Hohlfeld J. M. & Haverich A. (2001) Combined
exogenous surfactant and inhaled nitric oxide therapy for lung ischemia-reperfusion
injury in minipigs. Transplantation 71, 1238-1244. 10.1097/00007890-200105150-00010
79. Kermeen F. D., McNeil K. D., Fraser J. F., McCarthy J., Ziegenfuss M. D., Mullany D.,
Dunning J. & Hopkins P. M. (2007) Resolution of severe ischemia-reperfusion injury
post-lung transplantation after administration of endobronchial surfactant. J. Heart Lung
Transplant. 26, 850-856. 10.1016/j.healun.2007.05.016
80. Fiser S. M., Tribble C. G., Long S. M., Kaza A. K., Kern J. A., Jones D. R., Robbins M.
K. & Kron I. L. (2002) Ischemia-reperfusion injury after lung transplantation increases
risk of late bronchiolitis obliterans syndrome. Ann. Thorac. Surg. 73, 1041-1048.
10.1016/S0003-4975(01)03606-2
81. den Hengst W. A., Gielis J. F., Lin J. Y., Van Schil P. E., De Windt L. J. & Moens A. L.
(2010) Lung ischemia-reperfusion injury: a molecular and clinical view on a complex
pathophysiological process. Am. J. Physiol. Heart Circ. Physiol. 299, H1283-99.
10.1152/ajpheart.00251.2010
82. van der Kaaij Niels, K.J., Jack H., den Bakker Michael L. B., Burkhard L. & de Bruin
Ron B. A. (2008) Ischemia of the lung causes extensive long-term pulmonary injury: an
experimental study. Respir. Res. 9, 28. 10.1186/1465-9921-9-28
83. Solomon M., Grasemann H. & Keshavjee S. (2010) Pediatric lung transplantation.
Pediatr. Clin. North Am. 57, 375-391. 10.1016/j.pcl.2010.01.017
84. Fiser S. M., Tribble C. G., Long S. M., Kaza A. K., Cope J. T., Laubach V. E., Kern J. A.
& Kron I. L. (2001) Lung transplant reperfusion injury involves pulmonary macrophages
and circulating leukocytes in a biphasic response. J. Thorac. Cardiovasc. Surg. 121,
1069. 10.1067/mtc.2001.113603
85. Gazoni L. M., Tribble C. G., Zhao M. Q., Unger E. B., Farrar R. A., Ellman P. I.,
Fernandez L. G., Laubach V. E. & Kron I. L. (2007) Pulmonary macrophage inhibition
and inhaled nitric oxide attenuate lung ischemia-reperfusion injury. Ann. Thorac. Surg.
84, 247-253. 10.1016/j.athoracsur.2007.02.036
86. Naidu B. V., Krishnadasan B., Farivar A. S., Woolley S. M., Thomas R., Van Rooijen N.,
Verrier E. D. & Mulligan M. S. (2003) Early activation of the alveolar macrophage is
critical to the development of lung ischemia-reperfusion injury. J. Thorac. Cardiovasc.
Surg. 126, 200-207. 10.1016/S0022-5223(03)00390-8

121
87. Yerebakan C., Ugurlucan M., Bayraktar S., Bethea B. T. & Conte J. V. (2009) Effects of
inhaled nitric oxide following lung transplantation. J. Card. Surg. 24, 269-274.
10.1111/j.1540-8191.2009.00833.x
88. Lu Y. T., Liu S. F., Mitchell J. A., Malik A. B., Hellewell P. G. & Evans T. W. (1998)
The role of endogenous nitric oxide in modulating ischemia-reperfusion injury in the
isolated, blood-perfused rat lung. Am. J. Respir. Crit. Care Med. 157, 273.
10.1164/ajrccm.157.1.97-03057
89. Moore K. W., O'garra A., Malefyt R. W., Vieira P. & Mosmann T. R. (1993) Interleukin-
10. Annu. Rev. Immunol. 11, 165-190. 10.1146/annurev.iy.11.040193.001121
90. Couper K. N., Blount D. G. & Riley E. M. (2008) IL-10: the master regulator of
immunity to infection. J. Immunol. 180, 5771-5777.
91. Fiorentino D. F., Zlotnik A., Mosmann T., Howard M. & O'garra A. (1991) IL-10 inhibits
cytokine production by activated macrophages. J Immunol. 147, 3815-3822.
92. Fisher A. J., Donnelly S. C., Hirani N., Haslett C., Strieter R. M., Dark J. H. & Corris P.
A. (2001) Elevated levels of interleukin-8 in donor lungs is associated with early graft
failure after lung transplantation. Am. J. Respir. Crit. Care Med. 163, 259-265.
10.1164/ajrccm.163.1.2005093
93. Eppinger M. J., Ward P. A., Bolling S. F. & Deeb G. M. (1996) Regulatory effects of
interleukin-10 on lung ischemia-reperfusion injury. J. Thorac. Cardiovasc. Surg. 112,
1301-1306. 10.1016/S0022-5223(96)70144-7
94. Moore D. J., Markmann J. F. & Deng S. (2006) Avenues for immunomodulation and
graft protection by gene therapy in transplantation. Transplant Int. 19, 435-445.
10.1111/j.1432-2277.2006.00314.x
95. Fischer S., Liu M., MacLean A. A., de Perrot M., Ho M., Cardella J. A., Zhang X. M.,
Bai X. H., Suga M., Imai Y. & Keshavjee S. (2001) In vivo transtracheal adenovirus-
mediated transfer of human interleukin-10 gene to donor lungs ameliorates ischemia-
reperfusion injury and improves early posttransplant graft function in the rat. Hum. Gene
Ther. 12, 1513-1526. 10.1089/10430340152480249
96. Cassivi S. D., Cardella J. A., Fischer S., Liu M., Slutsky A. S. & Keshavjee S. (1999)
Transtracheal gene transfection of donor lungs prior to organ procurement increases
transgene levels at reperfusion and following transplantation. J. Heart Lung Transplant.
18, 1181-1188. 10.1016/S1053-2498(99)00095-9
97. Chapelier A., Danel C., Mazmanian M., Bacha E. A., Sellak H., Gilbert M. A., Herve P.
& Lemarchand P. (1996) Gene therapy in lung transplantation: feasibility of ex vivo
adenovirus-mediated gene transfer to the graft. Hum. Gene Ther. 7, 1837-1845.
10.1089/hum.1996.7.15-1837

122
98. Wu G., Morris Jr S. M. (1998) Arginine metabolism: nitric oxide and beyond. Biochem.
J. 336, 1.
99. Racké K., Warnken M. (2010) L-arginine metabolic pathways. Open Nitric Oxide J 2, 9-
19. 10.2174/1875042701002010001
100. Selamnia M., Robert V., Mayeur C., Delpal S. & Blachier F. (1998) De novo synthesis of
arginine and ornithine from citrulline in human colon carcinoma cells: metabolic fate of
L-ornithine. Biochim. Biophys. Acta 1425, 93-102. 10.1016/S0304-4165(98)00056-7
101. Closs E., Boissel J. P., Habermeier A. & Rotmann A. (2006) Structure and function of
cationic amino acid transporters (CATs). J. Membr. Biol. 213, 67-77. 10.1007/s00232-
006-0875-7
102. Lara A., Khatri S. B., Wang Z., Comhair S. A. A., Xu W., Dweik R. A., Bodine M.,
Levison B. S., Hammel J. & Bleecker E. (2008) Alterations of the arginine metabolome
in asthma. Am. J. Respir. Crit. Care Med. 178, 673. 10.1164/rccm.200710-1542OC
103. Tenu J. P., Lepoivre M., Moali C., Brollo M., Mansuy D. & Boucher J. L. (1999) Effects
of the new arginase inhibitor N (omega)-hydroxy-nor-L-arginine on NO synthase activity
in murine macrophages. Nitric Oxide 3, 427. 10.1006/niox.1999.0255
104. Ashutosh K. (2000) Nitric oxide and asthma: a review. Curr. Opin. Pulm. Med. 6, 21-25.
10.1097/00063198-200001000-00005
105. North M. L., Khanna N., Marsden P. A., Grasemann H. & Scott J. A. (2009) Functionally
important role for arginase 1 in the airway hyperresponsiveness of asthma.
Am. J. Physiol. Lung Cell. Mol. Physiol. 296, L911. 10.1152/ajplung.00025.2009
106. Maarsingh H., Pera T. & Meurs H. (2008) Arginase and pulmonary diseases. Naunyn
Schmiedebergs Arch. Pharmacol. 378, 171-184. 10.1007/s00210-008-0286-7
107. Belik J., Shehnaz D., Pan J. & Grasemann H. (2008) Developmental changes in arginase
expression and activity in the lung. Am. J. Physiol. Lung Cell. Mol. Physiol. 294,
L498. 10.1152/ajplung.00242.2007
108. Ricciardolo F. (2003) Multiple roles of nitric oxide in the airways. Thorax 58, 175.
10.1136/thorax.58.2.175
109. Li P., Yin Y. L., Li D., Woo Kim S. & Wu G. (2007) Amino acids and immune function.
Br. J. Nutr. 98, 237-252. 10.1017/S000711450769936X
110. Chen K., Pittman R. N. & Popel A. S. (2008) Nitric oxide in the vasculature: where does
it come from and where does it go? A quantitative perspective. Antioxid. Redox Signal.
10, 1185-1198. 10.1089/ars.2007.1959

123
111. Luiking Y. C., Engelen M. P. & Deutz N. E. (2010) Regulation of nitric oxide production
in health and disease. Curr. Opin. Clin. Nutr. Metab. Care 13, 97-104.
10.1097/MCO.0b013e328332f99d
112. Forstermann U., Sessa W. C. (2012) Nitric oxide synthases: regulation and function. Eur.
Heart J. 33, 829-37, 837a-837d. 10.1093/eurheartj/ehr304
113. Grasemann H., Ratjen F. (2012) Nitric oxide and L-arginine deficiency in cystic fibrosis.
Curr. Pharm. Des. 18, 726-736. 10.2174/138161212799315911
114. Ignarro L. J. (2002) Nitric oxide as a unique signaling molecule in the vascular system: a
historical overview. J. Physiol. Pharmacol. 53, 503-514.
115. Morris C. R., Kato G. J., Poljakovic M., Wang X., Blackwelder W. C., Sachdev V.,
Hazen S. L., Vichinsky E. P., Morris Jr S. M. & Gladwin M. T. (2005) Dysregulated
arginine metabolism, hemolysis-associated pulmonary hypertension, and mortality in
sickle cell disease. J. Am. Med. Assoc. 294, 81-90. 10.1001/jama.294.1.81
116. Stamler J. S., Singel D. J. & Loscalzo J. (1992) Biochemistry of nitric oxide and its
redox-activated forms. Science 258, 1898-1902. 10.1126/science.1281928
117. Xie Q., Nathan C. (1994) The high-output nitric oxide pathway: role and regulation. J.
Leukoc. Biol. 56, 576-582.
118. Boger R. H. (2004) Asymmetric dimethylarginine, an endogenous inhibitor of nitric
oxide synthase, explains the "L-arginine paradox" and acts as a novel cardiovascular risk
factor. J. Nutr. 134, 2842S-2847S; discussion 2853S.
119. Grasemann H., Shehnaz D., Enomoto M., Leadley M., Belik J. & Ratjen F. (2012) L-
ornithine derived polyamines in cystic fibrosis airways. PLoS One 7, e46618.
10.1371/journal.pone.0046618
120. Maarsingh H., Bossenga B. E., Bos I. S., Volders H. H., Zaagsma J. & Meurs H. (2009)
L-arginine deficiency causes airway hyperresponsiveness after the late asthmatic
reaction. Eur. Respir. J. 34, 191-199. 10.1183/09031936.00105408
121. Maarsingh H., Dekkers B. G., Zuidhof A. B., Bos I. S., Menzen M. H., Klein T., Flik G.,
Zaagsma J. & Meurs H. (2011) Increased arginase activity contributes to airway
remodelling in chronic allergic asthma. Eur. Respir. J. 38, 318-328.
10.1183/09031936.00057710
122. Morris C. R., Poljakovic M., Lavrisha L., Machado L., Kuypers F. A. & Morris S. M.,Jr.
(2004) Decreased arginine bioavailability and increased serum arginase activity in
asthma. Am. J. Respir. Crit. Care Med. 170, 148-153. 10.1164/rccm.200309-1304OC

124
123. Zakrzewicz D., Eickelberg O. (2009) From arginine methylation to ADMA: a novel
mechanism with therapeutic potential in chronic lung diseases. BMC Pulm. Med. 9, 5-
10.1186/1471-2466-9-5. 0.1186/1471-2466-9-5
124. Habib S. S. (2008) Exhaled nitric oxide: an emerging marker of inflammation in
respiratory diseases. Saudi Med. J. 29, 1697-1702.
125. Kharitonov S. A., Barnes P. J. (2006) Exhaled biomarkers. Chest 130, 1541-1546.
10.1378/chest.130.5.1541
126. Silkoff P. E., Caramori M., Tremblay L., McClean P., Chaparro C., Kesten S., Hutcheon
M., Slutsky A. S., Zamel N. & Keshavjee S. (1998) Exhaled nitric oxide in human lung
transplantation. A noninvasive marker of acute rejection. Am. J. Respir. Crit. Care Med.
157, 1822-1828. 10.1164/ajrccm.157.6.9707159
127. Gordon S. (2003) Alternative activation of macrophages. Nat. Rev. Immunol. 3, 23-35.
10.1038/nri978
128. Kepka-Lenhart D., Mistry S. K., Wu G. & Morris S. M.,Jr. (2000) Arginase I: a limiting
factor for nitric oxide and polyamine synthesis by activated macrophages? Am. J.
Physiol. Regul. Integr. Comp. Physiol. 279, R2237-42.
129. Vainikka T., Heikkilä L., Kukkonen S. & Toivonen H. J. (2001) L-Arginine in lung graft
preservation and reperfusion. J. Heart Lung Transplant. 20, 559-567. 10.1016/S1053-
2498(00)00332-6
130. Bueno M., Wang J., Mora A. L. & Gladwin M. T. (2013) Nitrite signaling in pulmonary
hypertension: mechanisms of bioactivation, signaling, and therapeutics. Antioxid. Redox
Signal. 18, 1797-1809. 10.1089/ars.2012.4833
131. Goret L., Tanguy S., Guiraud I., Dauzat M. & Obert P. (2008) Acute administration of l-
arginine restores nitric oxide-mediated relaxation in isolated pulmonary arteries from
pulmonary hypertensive exercise trained rats. Eur. J. Pharmacol. 581, 148-156.
10.1016/j.ejphar.2007.11.037
132. Li H., Meininger C. J., Hawker J. R., Haynes T. E., Kepka-Lenhart D., Mistry S. K.,
Morris S. M. & Wu G. (2001) Regulatory role of arginase I and II in nitric oxide,
polyamine, and proline syntheses in endothelial cells.
Am. J. Physiol. Endocrinol. Metab. 280, E75.
133. Forstermann U., Munzel T. (2006) Endothelial nitric oxide synthase in vascular disease:
from marvel to menace. Circulation 113, 1708.
10.1161/CIRCULATIONAHA.105.602532

125
134. Grasemann H., Schwiertz R., Matthiesen S., Racke K. & Ratjen F. (2005) Increased
arginase activity in cystic fibrosis airways. Am. J. Respir. Crit. Care Med. 172, 1523.
10.1164/rccm.200502-253OC
135. Nicholls S. J., Wang Z., Koeth R., Levison B., DelFraino B., Dzavik V., Griffith O. W.,
Hathaway D., Panza J. A. & Nissen S. E. (2007) Metabolic profiling of arginine and
nitric oxide pathways predicts hemodynamic abnormalities and mortality in patients with
cardiogenic shock after acute myocardial infarction. Circulation 116, 2315-2324.
10.1161/CIRCULATIONAHA.107.693986
136. Tang W. H. W., Wang Z., Cho L., Brennan D. M. & Hazen S. L. (2009) Diminished
global arginine bioavailability and increased arginine catabolism as metabolic profile of
increased cardiovascular risk. J. Am. Coll. Cardiol. 53, 2061-2067.
10.1016/j.jacc.2009.02.036
137. Pacher P., Beckman J. S. & Liaudet L. (2007) Nitric oxide and peroxynitrite in health and
disease. Physiol. Rev. 87, 315-424. 10.1152/physrev.00029.2006
138. Klein E., Weigel J., Buford M. C., Holian A. & Wells S. M. (2010) Asymmetric
dimethylarginine potentiates lung inflammation in a mouse model of allergic asthma.
Am. J. Physiol. Lung Cell. Mol. Physiol. 299, L816. 10.1152/ajplung.00188.2010
139. Wells, S M,Buford, M C,Migliaccio, C T & Holian, A(2009) Elevated asymmetric
dimethylarginine alters lung function and induces collagen deposition in mice.
Am. J. Resp. Cell Mol. Biol. 6, 332. 10.1165/rcmb.2008-0148OC
140. Grasemann H., Al-Saleh S., Scott J. A., Shehnaz D., Mehl A., Amin R., Rafii M.,
Pencharz P., Belik J. & Ratjen F. (2011) Asymmetric dimethylarginine contributes to
airway nitric oxide deficiency in patients with cystic fibrosis. Am. J. Respir. Crit. Care
Med. 201012-1995OCv1. 10.1164/rccm.201012-1995OC
141. Scott J. A., North M. L., Rafii M., Huang H., Pencharz P., Subbarao P., Belik J. &
Grasemann H. (2011) Asymmetric dimethylarginine is increased in asthma. Am. J.
Respir. Crit. Care Med. 201011-1810OCv1. 10.1164/rccm.201011-1810OC
142. Bedford M. T. (2007) Arginine methylation at a glance. J. Cell. Sci. 120, 4243-4246.
10.1242/jcs.019885
143. Vallance P., Leone A., Calver A., Collier J. & Moncada S. (1992) Accumulation of an
endogenous inhibitor of nitric oxide synthesis in chronic renal failure. Lancet 339, 572-
575. 10.1016/0140-6736(92)90865-Z
144. Bode-Boger S. M., Scalera F. & Ignarro L. J. (2007) The L-arginine paradox: Importance
of the L-arginine/asymmetrical dimethylarginine ratio. Pharmacol. Ther. 114, 295-306.
10.1016/j.pharmthera.2007.03.002

126
145. Achan V., Broadhead M., Malaki M., Whitley G., Leiper J., MacAllister R. & Vallance
P. (2003) Asymmetric dimethylarginine causes hypertension and cardiac dysfunction in
humans and is actively metabolized by dimethylarginine dimethylaminohydrolase.
Arterioscler. Thromb. Vasc. Biol. 23, 1455-1459.
10.1161/01.ATV.0000081742.92006.59
146. Sasaki A., Doi S., Mizutani S. & Azuma H. (2007) Roles of accumulated endogenous
nitric oxide synthase inhibitors, enhanced arginase activity, and attenuated nitric oxide
synthase activity in endothelial cells for pulmonary hypertension in rats.
Am. J. Physiol. Lung Cell. Mol. Physiol. 36, 10.1152/ajplung.00360.2006
147. Reid K. M., Tsung A., Kaizu T., Jeyabalan G., Ikeda A., Shao L., Wu G., Murase N. &
Geller D. A. (2007) Liver I/R injury is improved by the arginase inhibitor, NΩ-hydroxy-
nor-L-arginine (nor-NOHA). Am. J. Physiol. Gastrointest. Liver Physiol. 292, G512.
10.1152/ajpgi.00227.2006
148. Rhoden E. L., Rhoden C. R., Lucas M. L., Pereira-Lima L., Zettler C. & Bello-Klein A.
(2002) The role of nitric oxide pathway in the renal ischemia-reperfusion injury in rats.
Transpl. Immunol. 10, 277-284. 10.1016/S0966-3274(02)00079-5
149. Gao X., Xu X., Belmadani S., Park Y., Tang Z., Feldman A. M., Chilian W. M. & Zhang
C. (2007) TNF-α contributes to endothelial dysfunction by upregulating arginase in
ischemia/reperfusion injury. Arterioscler. Thromb. Vasc. Biol. 27, 1269. 10.1161/
ATVBAHA.107.142521
150. Tennyson A. G., Lippard S. J. (2011) Generation, translocation, and action of nitric oxide
in living systems. Chem. Biol. 18, 1211-1220. 10.1016/j.chembiol.2011.09.009
151. Gomez C. B., del Valle H. F., Bertolotti A., Negroni J. A., Cuniberti L., Martinez V.,
Osses J., Laguens R. P. & Favaloro R. R. (2005) Effects of short-term inhaled nitric
oxide on interleukin-8 release after single-lung transplantation in pigs. J. Heart Lung
Transplant. 24, 714-722. 10.1016/j.healun.2004.03.017
152. Marczin N., Riedel B., Gal J., Polak J. & Yacoub M. (1997) Exhaled nitric oxide during
lung transplantation. Lancet 350, 1681-1682. 10.1016/S0140-6736(05)64281-X
153. Shiraishi Y., Lee J. R., Laks H., Waters P. F., Meneshian A., Blitz A., Johnson K., Lam
L. & Chang P. A. (1996) L-arginine administration during reperfusion improves
pulmonary function. Ann. Thorac. Surg. 62, 1580-6; discussion 1586-7. 10.1016/S0003-
4975(96)00884-3
154. Hein T. W., Zhang C., Wang W., Chang C. I., Thengchaisri N. & Kuo L. (2003)
Ischemia-reperfusion selectively impairs nitric oxide-mediated dilation in coronary
arterioles: counteracting role of arginase. FASEB J. 17, 2328-2330. 10.1096/fj.03-0115fje

127
155. Boehler A. (2002) The role of interleukin-10 in lung transplantation. Transpl. Immunol.
9, 121-124. 10.1016/S0966-3274(02)00045-X
156. Kling K. M., Kirby L., Kwan K. Y., Kim F. & McFadden D. W. (1999) Interleukin-10
inhibits inducible nitric oxide synthase in an animal model of necrotizing enterocolitis.
Int. J. Surg. Investig. 1, 337-342.
157. Ogando D., Cella M., Ribeiro M. L., Weissmann C., Aisemberg J. & Franchi A. (2004)
IL-10 inhibits nitric oxide synthesis in murine uterus. Neuroimmunomodulation 11, 127-
132. 10.1159/000075322
158. Maru A., Jackson S. K. (1996) Opposite effects of interleukin-4 and interleukin-10 on
nitric oxide production in murine macrophages. Mediators Inflamm. 5, 110-112.
10.1155/S096293519600018X
159. Martins S., De Perrot M., Imai Y., Yamane M., Quadri S., Segall L., Dutly A., Sakiyama
S., Chaparro A. & Davidson B. (2004) Transbronchial administration of adenoviral-
mediated interleukin-10 gene to the donor improves function in a pig lung transplant
model. Gene Ther. 11, 1786-1796. 10.1038/sj.gt.3302357
160. Novitzky D., Horak A., Cooper D. K. & Rose A. G. (1989) Electrocardiographic and
histopathologic changes developing during experimental brain death in the baboon.
Transplant. Proc. 21, 2567-2569.
161. Huttemann E., Schelenz C., Sakka S. G. & Reinhart K. (2000) Atropine test and
circulatory arrest in the fossa posterior assessed by transcranial Doppler. Intensive Care
Med. 26, 422-425. 10.1007/s001340051176
162. Pierre A. F., Xavier A. M., Liu M., Cassivi S. D., Lindsay T. F., Marsh H. C., Slutsky A.
S. & Keshavjee S. H. (1998) Effect of complement inhibition with soluble complement
receptor 1 on pig allotransplant lung function. Transplantation 66, 723-732.
10.1097/00007890-199809270-00006
163. Steen S., Sjoberg T., Pierre L., Liao Q., Eriksson L. & Algotsson L. (2001)
Transplantation of lungs from a non-heart-beating donor. Lancet 357, 825-829.
10.1016/S0140-6736(00)04195-7
164. Bio-Rad Laboratories U. Bio-Rad protein assay.
Http://Labs.Fhcrc.Org/Fero/Protocols/BioRad_Bradford.Pdf
165. Bradford M. M. (1976) A rapid and sensitive method for the quantitation of microgram
quantities of protein utilizing the principle of protein-dye binding. Anal. Biochem. 72,
248-254. 10.1006/abio.1976.9999; 10.1016/0003-2697(76)90527-3

128
166. Mateos-Corral D., Coombs R., Grasemann H., Ratjen F. & Dell S. D. (2011) Diagnostic
value of nasal nitric oxide measured with non-velum closure techniques for children with
primary ciliary dyskinesia. J. Pediatr. 10.1016/j.jpeds.2011.03.007
167. Belik J., Stevens D., Pan J., Shehnaz D., Ibrahim C., Kantores C., Ivanovska J.,
Grasemann H. & Jankov R. P. (2009) Chronic hypercapnia downregulates arginase
expression and activity and increases pulmonary arterial smooth muscle relaxation in the
newborn rat. Am. J. Physiol. Lung Cell. Mol. Physiol. 297, L777.
10.1152/ajplung.00047.2009
168. Pinder A. G., Rogers S. C., Khalatbari A., Ingram T. E. & James P. E. (2008) The
measurement of nitric oxide and its metabolites in biological samples by ozone-based
chemiluminescence. Methods Mol. Biol. 476, 11-28. 10.1007/978-1-59745-129-1_2
169. ECO PHYSICS I. <br />. Available from:www.ecophysics-us.com/wp-
content/uploads//2012/03/Liquid-NO-Application-V10-US.pdf. Accessed September 25,
2013.-Homepage/Web site:http://www.ecophysics-us.com/.
170. Li X., Hanson C., Cmarik J. L. & Ruscetti S. (2009) Neurodegeneration induced by PVC-
211 murine leukemia virus is associated with increased levels of vascular endothelial
growth factor and macrophage inflammatory protein 1 alpha and is inhibited by blocking
activation of microglia. J. Virol. 83, 4912-4922. 10.1128/JVI.02343-08
171. Kurien B. T., Scofield R. H. (2006) Western blotting. Methods 38, 283-293.
172. Corraliza I., Campo M., Soler G. & Modolell M. (1994) Determination of arginase
activity in macrophages: a micromethod. J. Immunol. Methods 174, 231-235.
10.1016/0022-1759(94)90027-2
173. Armbruster D. A., Pry T. (2008) Limit of blank, limit of detection and limit of
quantitation. Clin. Biochem. Rev. 29 Suppl 1, S49-52.
174. Pinsky D. J., Naka Y., Chowdhury N. C., Liao H., Oz M. C., Michler R. E., Kubaszewski
E., Malinski T. & Stern D. M. (1994) The nitric oxide/cyclic GMP pathway in organ
transplantation: critical role in successful lung preservation.
PROC. NATL. ACAD. SCI. U. S. A. 91, 12086.
175. Rossaint R., Falke K. J., Lopez F., Slama K., Pison U. & Zapol W. M. (1993) Inhaled
nitric oxide for the adult respiratory distress syndrome. N. Engl. J. Med. 328, 399-405.
10.1056/NEJM199302113280605
176. Rich G. F., Lowson S. M., Johns R. A., Daugherty M. O. & Uncles D. R. (1994) Inhaled
nitric oxide selectively decreases pulmonary vascular resistance without impairing
oxygenation during one-lung ventilation in patients undergoing cardiac surgery.
Anesthesiology 80, 57-62; discussion 27A. 10.1097/00000542-199401000-00012

129
177. Moreno I., Vicente R., Mir A., Leon I., Ramos F., Vicente J. L. & Barbera M. (2009)
Effects of inhaled nitric oxide on primary graft dysfunction in lung transplantation.
Transplant. Proc. 41, 2210-2212. 10.1016/j.transproceed.2009.05.019
178. Pasero D., Martin E. L., Davi A., Mascia L., Rinaldi M. & Ranieri V. M. (2010) The
effects of inhaled nitric oxide after lung transplantation. Minerva Anestesiol. 76, 353-361.
179. Sedoris K. C., Ovechkin A. V., Gozal E. & Roberts A. M. (2009) Differential effects of
nitric oxide synthesis on pulmonary vascular function during lung ischemia-reperfusion
injury. Arch. Physiol. Biochem. 115, 34-46. 10.1080/13813450902785267
180. Normandin L., Herve P., Brink C., Chapelier A. R., Dartevelle P. G. & Mazmanian G. M.
(1995) L-arginine and pentoxifylline attenuate endothelial dysfunction after lung
reperfusion injury in the rabbit. The Paris-Sud University Lung Transplant Group. Ann.
Thorac. Surg. 60, 646-650. 10.1016/0003-4975(95)00484-3
181. Novitzky D. (1997) Detrimental effects of brain death on the potential organ donor.
Transplant. Proc. 29, 3770-3772. 10.1016/S0041-1345(97)01149-4
182. Gall W. E., Beebe K., Lawton K. A., Adam K. P., Mitchell M. W., Nakhle P. J., Ryals J.
A., Milburn M. V., Nannipieri M., Camastra S., Natali A., Ferrannini E. & RISC Study
Group. (2010) Alpha-Hydroxybutyrate is an Early Biomarker of Insulin Resistance and
Glucose Intolerance in a Nondiabetic Population. PLoS One 5, e10883.
10.1371/journal.pone.0010883
183. Redondo J., Manso A. M., Pacheco M. E., Hernandez L., Salaices M. & Marin J. (2000)
Hypothermic storage of coronary endothelial cells reduces nitric oxide synthase activity
and expression. Cryobiology 41, 292-300. 10.1006/cryo.2000.2285
184. Venturini G., Colasanti M., Fioravanti E., Bianchini A. & Ascenzi P. (1999) Direct effect
of temperature on the catalytic activity of nitric oxide synthases types I, II, and III. Nitric
Oxide 3, 375-382. 10.1006/niox.1999.0250
185. Lehmann S., Barten M. J., Topf C., Garbade J., Dhein S., Mohr F. W. & Bittner H. B.
(2012) Donor type impact on ischemia-reperfusion injury after lung transplantation. Ann.
Thorac. Surg. 93, 913-9; discussion 919-20. 10.1016/j.athoracsur.2011.11.033
186. Weyker P. D., Webb C. A., Kiamanesh D. & Flynn B. C. (2013) Lung ischemia
reperfusion injury: a bench-to-bedside review. Semin. Cardiothorac. Vasc. Anesth. 17,
28-43. 10.1177/1089253212458329
187. Kokko J. P. (1987) The role of the collecting duct in urinary concentration. Kidney Int.
31, 606-610. 10.1038/ki.1987.41
188. Rocha P. N., Rocha A. T., Palmer S. M., Davis R. D. & Smith S. R. (2005) Acute renal
failure after lung transplantation: incidence, predictors and impact on perioperative

130
morbidity and mortality. Am. J. Transplant. 5, 1469-1476. 10.1111/j.1600-
6143.2005.00867.x
189. Moinard C., Cynober L. (2007) Citrulline: a new player in the control of nitrogen
homeostasis. J. Nutr. 137, 1621S-1625S.
190. Liu M., Tremblay L., Cassivi S. D., Bai X. H., Mourgeon E., Pierre A. F., Slutsky A. S.,
Post M. & Keshavjee S. (2000) Alterations of nitric oxide synthase expression and
activity during rat lung transplantation. Am. J. Physiol. Lung Cell. Mol. Physiol. 278,
L1071.
191. Hsin M., Cypel M., Zamel R., Machuca T., Chen M., Liu M. & Keshavjee S. (2013)
Metabolites in human ex vivo lung perfusates are differentially affected in brain death
(BDD) vs. cardiac death donors (DCD) and modified by duration of normothermic
perfusion. J. Heart Lung Transplant. 32, S151-S152. 10.1016/j.healun.2013.01.347
192. Cremona G., Higenbottam T., Takao M., Hall L. & Bower E. A. (1995) Exhaled nitric
oxide in isolated pig lungs. J. Appl. Physiol. (1985) 78, 59-63.
193. Worrall N. K., Boasquevisque C. H., Misko T. P., Sullivan P. M., Ferguson T. B.,Jr &
Patterson G. A. (1997) Inducible nitric oxide synthase is expressed during experimental
acute lung allograft rejection. J. Heart Lung Transplant. 16, 334-339.
194. Adeva M. M., Souto G., Blanco N. & Donapetry C. (2012) Ammonium metabolism in
humans. Metabolism 61, 1495-1511. 10.1016/j.metabol.2012.07.007
195. Curis E., Nicolis I., Moinard C., Osowska S., Zerrouk N., Bénazeth S. & Cynober L.
(2005) Almost all about citrulline in mammals. Amino Acids 29, 177-205.
10.1007/s00726-005-0235-4
196. Taylor S. C., Berkelman T., Yadav G. & Hammond M. (2013) A defined methodology
for reliable quantification of Western blot data. Mol. Biotechnol. 55, 217-226.
10.1007/s12033-013-9672-6
197. Bult H. (1996) Nitric oxide and atherosclerosis: possible implications for therapy. Mol.
Med. Today 2, 510-518. 10.1016/S1357-4310(97)81455-4
198. Soccal P. M., Jani A., Chang S., Leonard C. T., Pavlakis M. & Doyle R. L. (2000)
Inducible nitric oxide synthase transcription in human lung transplantation.
Transplantation 70, 384-385. 10.1097/00007890-200007270-00026
199. Utsumi T., Mizuta T., Fujii Y., Shiono H., Okumura M., Minami M., Takeda S., Miyoshi
S. & Matsuda H. (1999) Nitric oxide production by bronchoalveolar cells during allograft
rejection in the rat. Transplantation 67, 1622-1626. 10.1097/00007890-199906270-
00019

131
200. Worrall N. K., Boasquevisque C. H., Botney M. D., Misko T. P., Sullivan P. M., Ritter J.
H., Ferguson T. B.,Jr & Patterson G. A. (1997) Inhibition of inducible nitric oxide
synthase ameliorates functional and histological changes of acute lung allograft rejection.
Transplantation 63, 1095-1101. 10.1097/00007890-199704270-00008
201. Chu Y., Wu Y. C., Chou Y. C., Chueh H. Y., Liu H. P., Chu J. J. & Lin P. J. (2004)
Endothelium-dependent relaxation of canine pulmonary artery after prolonged lung graft
preservation in University of Wisconsin solution: role of L-arginine supplementation. J.
Heart Lung Transplant. 23, 592-598. 10.1016/S1053-2498(03)00304-8
202. Morris S. M.,Jr. (2002) Regulation of enzymes of the urea cycle and arginine
metabolism. Annu. Rev. Nutr. 22, 87-105. 10.1146/annurev.nutr.22.110801.140547
203. Que L. G., George S. E., Gotoh T., Mori M. & Huang Y. C. (2002) Effects of arginase
isoforms on NO Production by nNOS. Nitric Oxide 6, 1-8. 10.1006/niox.2001.0355
204. Liu H., Drew P., Gaugler A. C., Cheng Y. & Visner G. A. (2005) Pirfenidone Inhibits
Lung Allograft Fibrosis through L‐Arginine–Arginase Pathway. Am J Transplant. 5,
1256-1263. 10.1111/j.1600-6143.2005.00876.x
205. George T. J., Arnaoutakis G. J., Beaty C. A., Jandu S. K., Santhanam L., Berkowitz D. E.
& Shah A. S. (2012) A physiologic and biochemical profile of clinically rejected lungs on
a normothermic ex vivo lung perfusion platform. J. Surg. Res. 10.1016/j.jss.2012.11.012
206. Scott-Burden T. (1995) Regulation of nitric oxide production by tetrahydrobiopterin.
Circulation 91, 248-250. 10.1161/01.CIR.91.1.248
207. Schmid R. A., Hillinger S., Walter R., Zollinger A., Stammberger U., Speich R.,
Schaffner A., Weder W. & Schoedon G. (1999) The nitric oxide synthase cofactor
tetrahydrobiopterin reduces allograft ischemia-reperfusion injury after lung
transplantation. J. Thorac. Cardiovasc. Surg. 118, 726-732. 10.1016/S0022-
5223(99)70019-X
208. Kooy N. W., Royall J. A., Ye Y. Z., Kelly D. R. & Beckman J. S. (1995) Evidence for in
vivo peroxynitrite production in human acute lung injury. Am. J. Respir. Crit. Care Med.
151, 1250-1254. 10.1164/ajrccm.151.4.7697261
209. Andrew P. J., Mayer B. (1999) Enzymatic function of nitric oxide synthases. Cardiovasc.
Res. 43, 521-531. 10.1016/S0008-6363(99)00115-7
210. Bellocq A., Suberville S., Philippe C., Bertrand F., Perez J., Fouqueray B., Cherqui G. &
Baud L. (1998) Low environmental pH is responsible for the induction of nitric-oxide
synthase in macrophages. Evidence for involvement of nuclear factor-kappaB activation.
J. Biol. Chem. 273, 5086-5092. 10.1074/jbc.273.9.5086

132
211. North M. L., Grasemann H., Khanna N., Inman M. D., Gauvreau G. M. & Scott J. A.
(2013) Increased ornithine-derived polyamines cause airway hyperresponsiveness in a
mouse model of asthma. Am. J. Respir. Cell Mol. Biol. 48, 694-702. 10.1165/rcmb.2012-
0323OC
212. Becherel P. A., Le Goff L., Ktorza S., Ouaaz F., Mencia-Huerta J. M., Dugas B., Debre
P., Mossalayi M. D. & Arock M. (1995) Interleukin-10 inhibits IgE-mediated nitric oxide
synthase induction and cytokine synthesis in normal human keratinocytes. Eur. J.
Immunol. 25, 2992-2995. 10.1002/eji.1830251042
213. Seyler I., Appel M., Devissaguet J. P., Legrand P. & Barratt G. (1997) Modulation of
nitric oxide production in RAW 264.7 cells by transforming growth factor-beta and
interleukin-10: differential effects on free and encapsulated immunomodulator. J. Leukoc.
Biol. 62, 374-380.
214. Naidu B. V., Fraga C., Salzman A. L., Szabo C., Verrier E. D. & Mulligan M. S. (2003)
Critical role of reactive nitrogen species in lung ischemia-reperfusion injury. J. Heart
Lung Transplant. 22, 784-793. 10.1016/S1053-2498(02)00556-9

133
Appendix

134
Figure A-1: Western blotting; arginase 1 and actin in recipient left lung and in donor lung
tissue in the “no EVLP” group at different time points.
Samples were taken at different time points: 0h CIT, after harvesting the lung from donor and
flushing with Perfadex
; 18h CIT (timed control), 18 hours after cold ischemia; 18h CIT/1h
post rep, 1 hour after transplantation and reperfusion of 18h CIT group; Recipient left lung,
normal lung tissue samples; at some time points same blot for β actin was used for both arginase
1 and 2.

135
Figure A-2: Western blotting; arginase 1 and actin in donor lung tissue in the “EVLP” group at
different time points.
Samples were taken at different time points: 0h CIT, after harvesting the lung from donor and
flushing with Perfadex
; 6h CIT, 6 hours after cold ischemia; 6h CIT+12h EVLP, 6 hours of
cold ischemia followed by 12 hours of EVLP, 6h CIT+12h EVLP+IL-10, 6 hours of cold
ischemia followed by 12 hours of EVLP; EVLP/1h post rep, 1 hour after transplantation and
reperfusion of 6h CIT+12h EVLP group; at some time points same blot for β actin was used for
both arginase 1 and 2.

136
Figure A-3: Western blotting; arginase 1 and actin in donor lung tissue in the “EVLP+IL-10”
group at different time points.
Samples were taken at different time points: Recipient left lung, normal lung tissue samples; 0h
CIT, after harvesting the lung from donor and flushing with Perfadex
; 6h CIT, 6 hours after
cold ischemia; 6h CIT+12h EVLP+IL-10, 6 hours of cold ischemia followed by IL-10 gene
therapy and 12 hours of EVLP; EVLP+IL-10/1h post rep, 1 hour after transplantation and
reperfusion of 6h CIT+12h EVLP+IL-10 group; at some time points same blot for β actin was
used for both arginase 1 and 2.

137
Figure A-4: Western blotting; arginase 2 and actin in recipient left lung and in donor lung
tissue in the “no EVLP” group at different time points.
Samples were taken at different time points: 0h CIT, after harvesting the lung from donor and
flushing with Perfadex
; 18h CIT (timed control), 18 hours after cold ischemia; 18h CIT/1h
post rep, 1 hour after transplantation and reperfusion of 18h CIT group; Recipient left lung,
normal lung tissue samples; at some time points same blot for β actin was used for both arginase
1 and 2.

138
Figure A-5: Western blotting; arginase 2 and actin in donor lung tissue in the “EVLP” group at
different time points.
Samples were taken at different time points: 0h CIT, after harvesting the lung from donor and
flushing with Perfadex
; 6h CIT, 6 hours after cold ischemia; 6h CIT+12h EVLP, 6 hours of
cold ischemia followed by 12 hours of EVLP, 6h CIT+12h EVLP+IL-10, 6 hours of cold
ischemia followed by 12 hours of EVLP; EVLP/1h post rep, 1 hour after transplantation and
reperfusion of 6h CIT+12h EVLP group; at some time points same blot for β actin was used for
both arginase 1 and 2.

139
Figure A-6: Western blotting; arginase 2 and actin in donor lung tissue in the “EVLP+IL-10”
group at different time points.
Samples were taken at different time points: Recipient left lung, normal lung tissue samples; 0h
CIT, after harvesting the lung from donor and flushing with Perfadex
; 6h CIT, 6 hours after
cold ischemia; 6h CIT+12h EVLP+IL-10, 6 hours of cold ischemia followed by IL-10 gene
therapy and 12 hours of EVLP; EVLP+IL-10/1h post rep, 1 hour after transplantation and
reperfusion of 6h CIT+12h EVLP+IL-10 group; at some time points same blot for β actin was
used for both arginase 1 and 2.

140
Table A-1: Protein expression in lungs at different time points in “EVLP”, “EVLP+IL-10” and
“no EVLP” groups and in recipient left lungs.
Num
ber o
f
samples
Arg
inase1
/
β actin
Num
ber o
f
samples
Arg
inase2
/
β actin
0h CIT 17 0.70±0.10 17 0.74±0.11
6h CIT 12 0.83±0.09 12 0.78±0.12
18 h CIT (timed control) 4 2.12±0.24 4 1.33±0.22
6h CIT+12h EVLP 6 1.09±0.15 6 0.51±0.16
6h CIT+12h EVLP +IL-10 8 0.84±0.10 9 0.76±0.25
18h CIT/1h post rep 4 1.64±0.15 4 1.33±0.15
EVLP/1h post rep 6 0.85±0.07 6 0.54±0.18
EVLP+IL-10/1h post rep 9 0.74±0.15 9 1.64±0.56
Recipient left lung 12 0.82±0.09 13 1.03±0.09
Protein expressions are shown as meanSEM. Samples were taken at different time points; 0h
CIT, after harvesting the lung from donor and flushing with Perfadex
; 6h CIT, 6 hours after
cold ischemia; 18h CIT (timed control), 18 hours after cold ischemia; 6h CIT+12h EVLP, 6
hours of cold ischemia followed by 12 hours of EVLP, 6h CIT+12h EVLP+IL-10, 6 hours of
cold ischemia followed by IL-10 gene therapy and 12 hours of EVLP; 18h CIT/1h post rep, 1
hour after transplantation and reperfusion of 18h CIT group; EVLP/1h post rep, 1 hour after
transplantation and reperfusion of 6h CIT+12h EVLP group; EVLP+IL-10/1h post rep, 1 hour
after transplantation and reperfusion of 6h CIT+12h EVLP+IL-10 group; Recipient left lung,
normal lung tissue samples.