Embed Size (px)
Citation preview

Suspected Cauda-EquinaSyndrome: Moving the
Physiotherapy Consultation from Capability to
Competency
Elaine Buchanan, MSc MCSP
Consultant [email protected]

A Sad Story
Persisting:
• Low Back Pain
• Ankle instability
• Perineal sensory loss:
• major sexual difficulties
Self- catheterises several times a day:
• Which she finds humiliating
• Recurrent urinary tract infections
• Attends continence service
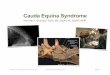
Cauda Equina Syndrome
Depression:
• Feels inadequate as a wife and a woman
• Profound impact on relationship
• Medication
• Intense psychological support.
No longer participates in sport
Works part time

Cauda Equina Syndrome
Variable manifestation of:• Back pain with unilateral or bilateral leg pain
And one or more of the following
• Perianal/perineal sensory loss
• Bladder disturbance
• Rectal sphincter dysfunction
• Sexual impotence
and may also have lower limb weakness or sensory loss
Due to a number of conditions:
• Most commonly degenerative (disc herniation, canal stenosis)
• Other causes: neoplastic, infective, traumatic, vascular, iatrogenic, endocrine, biochemical, inflammatory, idiopathic, thrombotic, haemorrhagic.

Medico-Legal
One of the most commonly litigated diagnoses
– Failure to identify
– Failure to escalate
– Delay in management
Substantial costs are a reflection of the damaging and distressing nature of the condition.

The Solution
All clinicians across the back pain pathway are competent in the recognition and assessment of suspected Cauda-Equina Syndrome and that they make timely referral to a spinal surgical service who have the competency to provide timely investigation and decompression of the lumbar spine.

Relevance to Physiotherapy
Failure to identify
• Lack of knowledge of Cauda Equina Syndrome
• Failure to identify bladder, bowel dysfunction and perianal/saddle sensation
• Reliance on subjective information only
• Few MSK physiotherapists carry out objective assessment for suspected CES
• Symptoms and signs associated with CES change but are not always reviewed following the initial assessment
• Reliance of previous clinicians evaluation
Failure to escalate
• Lack of objective findings increases the risk of
• Missed diagnosis (CES:I)
• Emergency referral for CES:I not being accepted
Delay in management
• Referral to another medical clinician for objective assessment.
• End of day/Friday presentations

Physiotherapists Are Capable of:
Competency can be developed
Examination and assessment of the pelvic floor complexis within the scope of physiotherapy practice
•Taking a history
•Testing neurology
•Testing a muscle

Oxfordshire Musculoskeletal Triage Service2012 Training
Cauda Equina Syndrome
• Cause, clinical presentation
• Diagnostic groups: – CES: Retention– CES: Incomplete
• Prognostic significance of:– complete versus incomplete CES– sphincter involvement– sensory deficit
• Management of CES-R and CES-I
Significance of delays in diagnosis and surgical referral

Oxfordshire Musculoskeletal Triage Service2012 Training
Objective assessment skills:
• Informed consent for objective CES examination
• Chaperone policy
Testing: • Perianal sensation• Resting anal tone• Anal sphincter squeeze

Oxfordshire Musculoskeletal Triage Service2012 Training
Patient explanation:• CES
– Symptoms
– Prevalence
• Examination
– what needs to be tested
– why it is important
– consequences of lack of information and delay
Communication
Warning patients:
– What to do should symptoms develop
– Consequences of delayed management
– Immediate emergency visit
Patient information booklet
Concise case presentation

Oxfordshire Musculoskeletal Triage Service2012 Training
Paperwork:
• Patient completed screening form
• Suspected CES checklist
Skills to:
• Complete paperwork
• Interpret information
Support for clinical reasoning/advice
• Spinal Consultant Physiotherapist
• Spinal Extended Scope Practitioner
• On-Call clinicians

Trust Policies
• Consent policy
• Chaperone policy
• On-Call referral protocol
• Core competency for all MSK Physiotherapists in department
Trust Meetings:
Spinal Team Clinical Governance
Physiotherapy Clinical Governance
On-Call doctors Training

648
105
No CES Checklist
CES Checklist
MSK Triage: Case Note Review 2013
• 4/12 retrospective review of electronic case notes
• 753 back pain assessments
735
18
No on-Call referral
On Call referral
Volume of suspected CES consultations varies between clinicians
• CES Checklist used 14%
• 2.5% referred to spinal on-call service

Self Rated Competence
Competence
• Use of the CES checklist
• Diagnosis of CES
• Significance of delayed management
• Testing:
– Peri-anal sensation
– Anal tone
– Anal squeeze
• Making emergency on-call referral
Lacks competence/confidence
• Pelvic floor anatomy
• Prevalence of bladder/bowel disturbance in general population.
• Differentiating CES: incomplete from CES: retention
• What to do with a patient who does not wish to consent to objective examination

Conclusion
• Delays in management are a significant contributor to poor outcome in Cauda-Equina Syndrome
• Physiotherapists are capable doing a Cauda-Equina Syndrome assessment
• Competency can be developed










![23...nerve root involvement; all symptoms and signs of the surgical emergency Cauda Equina syndrome (CES) [3]. 2. Vertebral column The vertebral column consists of 33 [4] individual](https://img.pdfslide.us/doc/110x75/5f278361982179088e4471c4/23-nerve-root-involvement-all-symptoms-and-signs-of-the-surgical-emergency.jpg)