Embed Size (px)
Citation preview

Survivors of Motor Vehicle Trauma:
An Analysis of Seat Belt Use and Health Care Utilization
DONALD A. REDELMEIER, MD, MS(HSR), PA TRICIA J. BLAIR, MD
Objective: To determine whether the protective effects of seat belt use on acute injury are followed by corresponding reductions in outpatient health care utilization. Design: Retrospective cohort analysis. Setting: Northern California Region Kaiser Health Plan hospitals and medical offices. Patients: All Kaiser Foundation Health Plan members injured in motor vehicle crashes in Santa Clara County during one year (total number of patients = 246). Measurements and main results: 54% of the study participants had been wearing seat belts at the time of injury, and 46% had not been. The belted patients had fewer head injuries (30% vs 50%, p < 0.05), better mean Injury Severity Scale scores (4.3 vs 7.4, p < 0.05), and smaller mean hospital charges ($8,580 vs $16,209, p < 0.05). How- ever, the effects of injury did not end upon discharge from the trauma center; the patients averaged about eight outpatient visits during the subsequent year, a rate almost double their prior use. In contrast to inpatient measures of utilization, the patients who had been wearing seat belts at the time of injury had more outpatient visits during the year after injury than had their unbelted counterparts (9.0 vs 7.1, p < 0.05). This discrepancy was not explained by differences in amounts of utilization during the year before injury, which were similar in the two groups (4.4 vs 4.8, p = NS). Overall, general inter- nists provided the most follow-up care and accounted for the largest discrepancy in utilization between the belted and unbelted patients. Conclusions: Seat belt use does not result in lower utilization of follow-up outpatient services in the year following injury. However, the beneficial effects on acute care utilization more than offset the marginal effects on subsequent medical services utilization. Key words: abbreviated injury scale; motor vehicle crashes; automo- bile driving; Injury Severity Scale; hospital outpatient clinics; seat belts; utilization. J GEN INTERN MED 1993;8:199-203.
TRAUMATIC INJURY is a l ead ing cause of death , yet mos t i n ju r ed p e o p l e do no t die. ~ Dur ing a l i f e t ime of dr iv ing, for example , the average pe r son has a b o u t a 2% c h a n c e of dy ing f rom a fatal traffic-related even t b u t a 33% chance of e x p e r i e n c i n g a s ignif icant traffic-related in- jury.2, 3 What h a p p e n s to these survivors? Author i ta t ive texts on i n t e rna l m e d i c i n e p rov ide l i t t le d i scuss ion abou t the long- te rm courses of pa t i en t s w h o survive injury. ~'6 Specialists in i n ju ry con t ro l t e n d to focus on p r e v e n t i o n and have i n c o m p l e t e i n f o r m a t i o n a b o u t de-
Received from the Trauma Management Program, Department of Emergency Medicine Service, Kaiser Permanente Medical Center, San Jose, California. Dr. Redelmeier is currently with the Division of Clinical Epidemiology of the Wellesley Hospital Research Institute and the Department of Medicine of the University of Toronto, Tor- onto, Ontario, Canada.
Presented at the R. Adams Cowley 13th National Trauma Sym- posium, Baltimore, Maryland, March 21 -23, 1991.
The Trauma Management Program was supported by a grant from the Garfield Fund.
Address correspondence and reprint requests to Dr. Redel- meier: Clinical Epidemiology Division, Department of Medicine, The Wellesley Hospital Research Institute, 160 Wellesley Street East, Jones Building, Room 123, Toronto, Ontario, Canada M4Y IJ3.
layed ou t c ome s . 2, 7 Physic ians t r a ined in t r auma to logy
c o n c e n t r a t e d o n acu te t r e a t me n t and have less con tac t w i t h the d iverse aspects of s u b s e q u e n t hea l th care. G i v e n the p a u c i t y of avai lable in fo rma t ion , in te rn is t s i n t e re s t ed in the genera l hea l th of pa t i en t s may have diff iculty a n t i c i p a t i n g the f o l l ow - up care for survivors
of m o t o r v e h i c l e t rauma. P l a n n i n g f o l l ow - up care r equ i r e s d i s t i ngu i sh ing
b e t w e e n i n p a t i e n t a nd o u t p a t i e n t set t ings, s In i t ia l t r auma care r equ i r e s a br isk assessment of ten fo l l owed
by a t e c h n o l o g i c p r o c e d u r e , whereas o u t p a t i e n t care enta i ls m a n a g e m e n t over t ime w i t h less in t ens ive use of tests a nd in t e rven t ions . 9 I n p a t i e n t care focuses on re- s to r ing a n a t o m i c integr i ty , c o n t r o l l i n g b l e e d ing , and m a n a g i n g infec t ions , whereas o u t p a t i e n t m a n a g e m e n t c o n c e n t r a t e s o n f u n c t i o n a l recovery, c h r o n i c p a i n man- agemen t , a nd psychosoc ia l r e in tegra t ion , t°. t l Dur ing
acu te care, pa t i en t s may be u n a b l e to pa r t i c ipa te in dec i s ion mak ing , whereas o u t p a t i e n t m a n a g e m e n t de- p e n d s o n good co l l abo ra t i on and c o m p l i a n c e , t2, 13 Thus , acu te t r auma m a n a g e m e n t may be an impe r f ec t
m o d e l for the genera l in te rn i s t p r o v i d i n g fo l l ow-up
care to t r auma pat ients . To h igh l igh t the d i f ference b e t w e e n the i n p a t i e n t
a nd o u t p a t i e n t set t ings, w e e x a m i n e d the effect of seat be l t use o n hea l th care u t i l i za t ion . Seat be l t use r educes fatal i t ies caused by mo t o r ve h i c l e crashes; however , the long- t e rm c o n s e q u e n c e s for survivors r e m a i n un- k n o w n . 14"t9 Is a pa t i en t ' s use of seat be l t s associa ted
w i t h lower u t i l i z a t i on of f o l l ow - up care? W e c o n d u c t e d a r e t rospec t ive cohor t s tudy of hea l th care u t i l i z a t i on by survivors of mo t o r ve h i c l e crashes, c o m p a r i n g pa- t ien ts w h o had b e e n w e a r i n g seat be l t s at the t ime of in ju ry w i t h those w h o had not . In so doing , w e invest i- gated w h e t h e r a factor that p red ic t s a favorable cour se in the hosp i ta l impar t s a c o r r e s p o n d i n g l y pos i t ive
p rognos i s in the o u t p a t i e n t set t ing.
METHODS
We s t ud i e d all Kaiser F o u n d a t i o n Heal th Plan m e m b e r s i n j u r e d in Santa Clara County , Cal i fornia , be-
t w e e n Ju ly 1, 1988 , a nd Ju ly 1, 1989 . We i n c l u d e d o n l y pa t i en t s w hose in ju r ies we re caused by mo t o r v e h i c l e crashes and w hose in i t ia l sever i t ies of i n ju ry me t the cr i ter ia for t r iage to a l eve l -one t r auma center . 2° The cohor t was spec ia l in two re t rospects . First, the Kaiser t r auma m a n a g e m e n t t eam d i rec t ly eva lua ted all pa- t ients , assessed the i r in jur ies , a nd a r ranged fo l low-up care. Second, all the pa t i en t s had the same hea l th insur-
199
200 Redelmeier, Blair, SEAT BELTS AND RESOURCE UTIUZATION
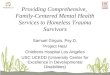
TABLE 1
Characteristics and Severity of Injury of Patients Who Survived Motor Vehicle Trauma
Unbelted Group Belted Group (n = 114) (n = 132)
Characteristics Age--mean 27.8 years 32.5 years* Gender-- male 62% 48%* Pregnant (% of women) 5% 4%o Marital status--single 74% 62%* Seating position (% driving) 68% 73% Excessive speed--> 55 mph 19% 23% Positive blood alcohol
level - - > 0 mg/dL 36% 150/0 * Toxic blood alcohol l eve l -
> BO mg/dL 280/o 13%* Positive drug screen 3% 0%0
Severity of Injury Abnormal vital signs 1 t % 10% Head injuries 50% 30%* Facial injuries 46% 20%* Thoracic injuries 3% 6%* Abdominal injuries 6% 6% Musculoskeletal injuries 39%0 32% Injury Severity Scale--meant 7.4 units 4.3 units*
Severe injuries-- ISS> 9 25% 15%* Very severe injuries-- ISS> 15 12% 3%*
*p < 0.05 by chi-square test or Student's t-test, as appropriate. tRange from 0 to 75: higher values denote more severe injuries.
ance, access to fol low-up care, and comprehensive doc- umentat ion of health care utilization. Together, these unique condit ions provided a rare oppor tuni ty to ex- amine the relation be tween seat belt use and health care utilization.
We evaluated all the patients within 48 hours of injury, by direct contact for the patients who were still hospitalized and by t e lephone interview for the pa- tients wh o had been discharged. We determined whe ther the patient had been wearing a seat bel t at the t ime of injury by reviewing the paramedic report , ex- amining the patient 's pat tern of injuries, and direct ly quest ioning the patient. In cases in which the three sources did not all agree, we coded the patient 's use of seat belts at the t ime of injury as "uncer ta in . " For the patients who were still in hospital, we sought confir- mation of seat bel t use by direct conversation with the attending physicians: in no circumstances did they dis- agree with our final assessment.
Emergency room reports, hospital records, and subsequent financial billings provided information about each patient 's severity of injury, hospital care, and final charges. Vehicle speeds at the t ime of the crash that were estimated by paramedics as more than 55 miles per hour were classified as "excess ive ." Toxi- cology evaluations of urine and b lood document ing any illicit drug use were considered "posi t ive ." Similarly, b lood alcohol assays that revealed any detectable amount were classified as "pos i t ive ," and those with levels above 80 mg/dL as " t ox i c . " We characterized
any of the fol lowing as abnormal vital signs: respiratory rate higher than 25 or lower than 10 per minute, sys- tolic b lood pressure less than 90 mm Hg, or a Glasgow Coma Scale score less than 14. We classified concus- sions, intracranial hemorrhages, and spinal cord dam- age as "serious head injuries"; facial lacerations, dental avulsions, mandibular fractures, and orbit injuries as "serious facial injuries"; hemopneumothoraces , rib fractures, and cardiopulmonary contusions as "serious thoracic injuries"; abdominoperi toneal organ lacera- tions, perforations, and hemorrhages as "serious ab- dominal injuries"; and fractures, dislocations, and cer- vical strains as "serious musculoskeletal injuries." Ambulance fees and hospital charges excluded physi- cians' billings and referred to the financial bills issued by the paramedic company and the trauma center, respectively.
To summarize each patient 's initial injury, we used the Injury Severity Scale (ISS), an established index for quantifying the degrees of anatomic trauma to different parts of the body. 2t Scores range from 0 to 75; the higher the number, the more extensive the damage. Bull 22 showed that a score of 9 provides a convenient threshold for separating patients at low risk for disabil- ity after discharge from the hospital (1 in 90) from those at high risk (1 in 7) for severe disability after discharge. Alternatively, Copes et al. 23 showed that for young patients with blunt injuries, an ISS score of 15 separates patients who are not l ikely to die (1 in 112) from those at substantial risk for dying in the hospital(1 in 5). We used these two thresholds to provide clinical interpretations for statistically significant differences in ISS scores.
To evaluate each patient 's outpat ient health care utilization, we accessed the Registration Plus Kaiser Permanente appoin tment report ing system.Z4 Although the principal purpose of the system was to organize daily scheduling activities, it provided a record of all outpat ient visits occurr ing at the 14 hospitals affiliated with the Kaiser Permanent Medical Care Program in the Northern California Region. We linked each patient 's hospital course to his or her outpat ient care by match- ing records according to name, birthday, and Kiaser Foundation Health Plan number. By indexing each pa- tient 's date of injury, we analyzed outpatient utilization both before and after the event; that is, all visits made during the year before injury and all visits made during the year after injury.
Data analysis inc luded both quantitative and quali- tative components . We used the chi-square test, Stu- dent 's t-test, and the Mann-Whitney U statistic, as appro- priate, to compare the demographic characteristics, severities of injury, and acute care treatments of pa- tients who had been wearing seat belts at the t ime of injury and those who had not been. We summarized outpat ient util ization before and after injury by calcu- lating for each patient the total visits to the correspond-

JOURNAL OF GENERAL INTERNAL MEDICINE, Volume 8 (April), 1993 201
ing office or cl inic and by using the Mann-Whitney sta- tistic to test for differences in utilization by the two groups. Finally, to gain supplemental information about outpat ient management, we conduc ted a chart review of patient records at one facility.
RESULTS
Overall, 265 health plan members were injured in motor vehicle crashes during the study period. We ex- c luded 14 patients because of their use of seat belts at the time of injury was uncertain and five patients be- cause they died of acute injuries. The remaining 246 patients composed our study cohor t (Table 1). The typical patient in each group was young, unmarried, and driving the vehicle at the t ime of injury: few indi- viduals had been sitting in the front passenger posit ion (21%) or the back seat (8%). The incidence of trauma fol lowed a circadian pattern: 10% during the day (8:00 AM-12:00 noon) , 10% during the afternoon (12:00 n o o n - 4 : 0 0 PM), 20% during the evening (4:00 PM-- 8:00 PM), 26% during the night (8:00 PM- 12:00 mid- night), 24% during the late night (12:00 m i d n i g h t - 4:00 AM), and 10% during the dawn (4:00 AM-8:00 AM). At the t ime of injury, 20% had been traveling at excessive speeds, 20% had had toxic b lood alcohol levels, and 5% of the women had been pregnant.
About half had been wearing seat belts at the t ime of injury, and half had been unbel ted. The two groups were similar with regard to the individual 's seating po- sition, the t ime of the incident, and the propor t ion traveling at excessive speed. The patients who had been wearing seat belts tended to be older than the patients who had been unbel ted, and were less likely to be men, less likely to be single, and less likely to have had de- tectable b lood alcohol levels. Overall, 33% of the sin- gle men with positive b lood alcohol levels had been wearing seat belts (95% confidence interval: 17% to 49%), whereas 81% of the married women with nega- tive blood alcohol levels had been wearing seat belts (95% confidence interval: 68% to 94%).
As expected, the patients who had been wearing seat belts had less severe injuries than did their un- bel ted counterparts. The patients who had been wear- ing seat belts were 40% less likely to sustain serious head injuries and 57% less likely to have serious facial injuries. Rates of thoracic, abdominal, and musculo- skeletal injuries were similar in the two groups. Ac- cording to the criteria of Bull 22 and of Copes et ai.,23 the patients who had been wearing seat belts were 40% less likely to have disabling injuries and 75% less likely to have life-threatening injuries than were their unbe l ted counterparts.
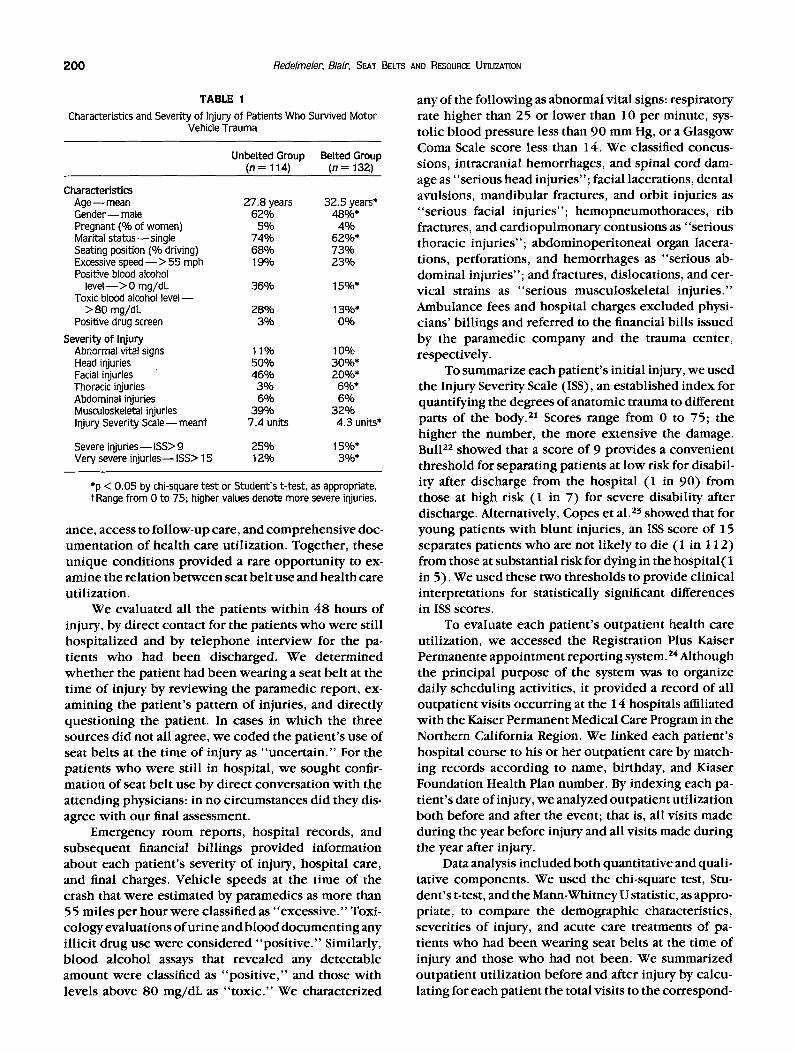
The patients who had been wearing seat belts used fewer acute care services (Table 2). Those who had been wearing seat belts at the t ime of injury were 50% more likely to be treated and released from the emer-
gency department, required shorter lengths of stay when admitted, and were less l ikely to need care in the intensive care unit. Frequency of surgery and pro- tracted length of stay tended to be lower among the bel ted patients, a l though the differences were not sta- tistically significant. Mean hospital charges were about $8,000 lower for the bel ted patients than for the un- bel ted patients.
The consequences of injury did not end upon dis- charge from the hospital. Our patients averaged about eight outpat ient visits in the year after injury compared wi th only about four visits in the year before injury. In contrast to inpatient measures of utilization, patients w h o had been wearing seat belts at the t ime of injury made more, not fewer, visits during the year after injury than did their unbel ted counterparts. This discrepancy could not be expla ined by a difference in amounts of util ization during the year before injury, which were similar for the bel ted and unbel ted patients. The dis- crepancy in fol low-up visit rates appeared among those patients treated and released from the emergency de- par tment (6.5 vs 5.3), those admit ted to the hospital but not treated surgically (9.4 vs 7.1) , and those admit-
TABLE 2
Health Care Utilization among Patients Who Survived Motor Vehicle Trauma
Unbelted Group Belted Group (n = 114) (n = 132)
Inpatient utilization Treated and released from
emergency department 30% 45%* Length of stay if
admi t ted - mean 7.6 days 5.9 days Length of stay > 2 weeks 9% 5% Admitted to intensive care unit 16% 8%* Had surgery 16% 12% Hospital charges - - mean S 16,209 $8,580" Hospital charges-- median $ 4,031 $2,052*
Outpatient utilizationt Year before injury (total) 4.8 4.4
General medicine 1.4 1.4 Physical therapy 0.0 0.2 Urgent care clinic 0.4 0.4 Orthopedics O. 1 O. 1 General surgery 0.2 O. 1 Psychiatry 0.3 O. 1 Othert 2.4 2.1
Year after injury (total) 7.1 9.0* General medicine 1.3 2.0* Physical therapy 0.7 1.3 Urgent care clinic 0.9 0.9 Orthopedics 0.8 0.9 General surgery 0.7 0.7 Psychiatry 0.2 0.3 Othert 2.5 2.9
*p < 0.05 by chi-square. Student'st-test, or Mann-Whitney U test, as appropriate.
Wigures denote average number of visits per patient per year. *Includes dermatology, gynecology, ophthalmology, and otolar-
yngology.
202 Redelmeier, Blair, SEAT BELTS AND RESOURCE UTILIZATION
ted to the hospital for emergency surgery (16.8 vs 12.0).
The single largest g roup providing outpat ient fol- low-up care was general internists, w h o saw patients about as f requent ly as general surgeons and or thope- dists combined . General medic ine was the largest sin- gle source of d iscrepancy in fo l low-up uti l ization be- tween the bel ted and the unbe l ted patients. Review of individual medical charts suggested that the reasons for visits varied substantially and often inc luded p rob lems not necessari ly direct ly related to t rauma, such as si- nusitis, e levated b lood pressure, and urinary tract in- fections. The pat terns of main compla in ts among the be l ted and the unbe l t ed patients appeared to be simi- lar, a l though the low f requency of any given condi t ion p rec luded formal statistical testing. Regardless of seat bel t use, the single most c o m m o n vexat ion docu- men ted was that the t rauma record of pat ient hospital care was unavailable for the general internist to rev iew dur ing outpat ient fol low-up.
DISCUSSION
We studied the relat ion be tween seat bel t use and health care uti l ization in pat ients surviving motor vehi- cle trauma. Similar to previous studies, our s tudy showed that risk factors for not using seat belts in- c luded age, gender, and marital status. Individuals w h o had been wear ing seat belts at the t ime of injury had a lower chance of serious head injury, a greater likeli- hood of be ing t reated and released f rom the emergency depar tment , and smaller average hospital charges than did those w h o had been unbe l ted at the t ime of injury. Survivors required fo l low-up care: we found that indi- viduals had almost twice as many outpat ient visits in the year fol lowing injury than in the year pr ior to injury. Paradoxically, pat ients w h o had been wear ing seat belts at the t ime of injury used more fo l low-up care than did their unbe l ted counterparts , even though the two groups were similar in their pr ior uses of outpat ient services. Hence, the use of seat belts was associated wi th decreased uti l ization of acute care services but not wi th decreased uti l ization of subsequent outpat ient care.
Several reasons might explain the failure of seat bel t use to reduce uti l ization of outpat ient services. Patients who use seat belts may sustain different pat- terns of injury that have differential requ i rements for outpat ient and inpat ient care; for example , using a seat bel t may prevent a head concussion ( the reby avoiding a hospital admission) but may cause a rib fracture (which necessitates fo l low-up t rea tment) . The o p t i m u m medi- cal fo l low-up for many disorders is unknown, suggest- ing that the similar rates of outpat ient uti l ization may reflect uncertaint ies in decision making and the ab- sence of guidelines. As in other studies of seat be l t ef- fectiveness, we investigated only those patients w h o sought care; an impor tan t benefit of seat belts may be to
obviate the need for medical care, both inpatient and outpatient . The propens i ty to seek fol low-up care may also reflect psychology and not just physiology; for ex- ample , patients who were unbe l ted at the t ime of injury may interpret their survival as meaning that they are "bu l l e tp roof , " whereas bel ted patients who were in- jured may come to bel ieve that life is fragile and re- quires extensive protect ion. Regardless of possible ex- planations, physicians should not expec t that patients discharged f rom the t rauma center who were wearing seat belts at the t ime of injury will use less outpat ient fol low-up care than will their unbel ted counterparts .
Although not the p r imary goal of our study, the results emphas ize that injury behaviors and medical risks tend to cluster together. 2s Overall, 22% of our cohort had visited an emergency depar tment at least once, 5% had seen a psychiatrist at least twice, and I9% had been treated by a general internist at least three t imes dur ing the year pr ior to injury. Past studies indi- cate that physicians ' advice can increase pat ients ' com- pl iance wi th au tomobi le safety, 26 suggesting that more t ime spent counsel ing pat ients might have decreased the incidence of t rauma in our cohort . At the very least, a health maintenance organizat ion needs to be con- cerned w h e n almost half of those injured in motor vehi- cle t rauma were not wear ing seat belts, a fourth were posit ive for b lood alcohol , ~nd a fifth were driving at excessive speeds.
Several features of our s tudy meri t c o m m e n t before the results are appl ied elsewhere. We analyzed only motor vehicle t rauma that occur red in Santa Clara County, a densely popu la t ed urban area wi th a high median family income; the incidence of injury was lower than that in other parts of the United States and the mean ISS score was less severe than in other stud- ies.2~. 23, 27, 2a Our patients were all Kaiser Foundation Health Plan members and may differ from persons in other regions, a l though their demographic features, rates of seat bel t use, mean lengths of stay, and hospital charges were comparab le wi th those repor ted in pre- vious studies of motor vehic le trauma.2933 The Perman- ente Medical Group may have a different pract ice pat- tern than do other health care providers, a l though the rates of outpat ient visit uti l ization in this study were similar to those found in other prepaid group pract ices and fee-for-service systems. 34, 35
We emphas ize that our study does not imply that seat belts are dele ter ious to moto r vehicle passengers. The differences in amounts of outpat ient utilization, whi le statistically significant, were small and overshad- owed by the acute care benefits. Had all the patients in our cohort been wear ing seat belts at the t ime of injury, for example , we est imate that there wou ld have been 23 fewer head injuries, 30 fewer facial injuries, 17 fewer admissions, 237 fewer days in hospital, and a reduct ion of almost $1 mil l ion in total hospital charges. Even if the average cost of an outpat ient visit were $200 and the d iscrepancy in util ization were to
JOURNAL OF GENERAL INTERNAL MEDICINE, Volume 8 (April), 1993 203
p e r s i s t f o r 25 yea r s , t o t a l f i n a n c i a l e x p e n d i t u r e s w o u l d
b e l o w e r in t h e g r o u p w e a r i n g s e a t b e l t s . T h e b e n e f i c i a l
e f f e c t s o f s e a t b e l t u s e o n a c u t e c a r e u t i l i z a t i o n m o r e
t h a n o f f se t t h e m a r g i n a l d i f f e r e n c e s in a m o u n t s o f u t i l i -
z a t i o n o f f o l l o w - u p m e d i c a l s e r v i c e s .
The Medical Editing Department of Kaiser Foundation Hospitals pro- vided editorial assistance. Previous drafts of the manuscript benefit- ted from suggestions from Drs. Douglas Owens, Louise Pilote, Miriam Shuchman, and Elliott Wolfe.
REFERENCES 1. National Center for Health Statistics. Health, United States,
1988. Washington, DC: U.S. Department of Health and Human Services, Public Health Service, CDC, 1989; DHHS publication no. (PHS)89-1232.
2. Rice DP, MacKenzie EJ. Cost of injury in the United States: a report to Congress. San Francisco: Institute for Health and Aging, University of California; and Baltimore: Injury Prevention Center, The Johns Hopkins University, 1989.
3. Sleet DA. Motor vehicle trauma and safety belt use in the context of public health priorities. J Trauma. 1987;27:695-702.
4. WilsonJD, Braunwald E, Isselbacher KJ (eds). Harrison's princi- ples of internal medicine. 12th ed. New York: McGraw-Hill, 1991.
5. Wyngaarden JB, Smith LH Jr (eds). Cecil textbook of medicine. 18th ed. Philadelphia: W. B. Saunders, 1988.
6. Goroll AH, May LA, Mulley AG. Primary care medicine. Philadel- phia: J. B. Lippincott, 1981.
7. Committee onTrauma Research. InjuryinAmerica.Washington, DC: National Academy Press, 1985.
8. TobacmanJK, Zeitler RR, Cilursu AM, Mori M. Variations in phy- sician opinion about scheduling of return visits for common ambulatory care conditions. J Gen Intern Med. 1992;7:312-6.
9. Trunkey DD. Initial treatment of patients with extensive trauma. N EnglJ Med. 1991;324:1259-63.
10. MacKenzie EJ, Siegel JH, Shapiro S, Moody M, Smith RT. Func- tional recovery and medical costs of trauma: an analysis by type and severity of injury. J Trauma. 1988;28:281-95.
11. Trunkey DD. Trauma. Sci Am. 1983;249(2):28-35. 12. Kaplan SH, Greenfield S, Ware JE Jr. Assessing the effects of
physician-patient interactions on the outcomes of chronic dis- ease. Med Care. 1989;27(3 suppl):S110-S127.
13. Hughes TE, Larson LN. Patient involvement in health care: a procedural justice viewpoint. Med Care. 1991 ;29:297-303.
14. Austin RH. Political risk assessment, from an elected safety belt law advocate's point of view and experience. J Trauma. 1987;27:719-25.
15. Knapper CK, Cropley AJ, Moore RJ. Attitudinal factors in the non-use of seat belts. Accid Anal Prev. 1976;8:241-6.
16. Evans L. Estimating fatality reductions from increased safety belt use. RiskAnal. 1987;7:49-57.
17. U.S. National Highway Traffic Safety Administration. 19 city safety belt and child safety seat use observation study. Washing- ton, DC: National Highway Traffic Safety Administration, 1988.
18. Evans L. The effectiveness of seat belts in preventing fatalities. Accid Anal Prey. 1986; 18:229-41.
19. Houk VN, Thacker SB. The Centers for Disease Control program to prevent primary and secondary disabilities in the United States. Public Health Rep. 1989; 104:226-31.
20. Santa Clara County Health Department. Emergency Medical Ser- vices Division Policy 300.15. Santa Clara, CA: Santa Clara County Health Department, 1991.
21. Baker SP, O'Neill B, Haddon W Jr, Long WB. The Injury Severity Score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma. 1974; 14:187-96.
22. Bull JP. The Injury Severity Score of road traffic casualties in relation to mortality, time of death, hospital treatment time, and disability. Accid Anal Prey. 1975;7:249-55.
23. Copes WS, Champion HR, Sacco WJ, Lawnick MM, Keast SL, Bain LW. The Injury Severity Score revisited. J Trauma. 1988;28:69-77.
24. Carrillo-Vassel R. Registration plus, March 17, 1989. Walnut Creek, CA: Kaiser Permanent Medical Care Program, Information Services, 1989.
25. Lowenstein SR. Injury prevention in primary care. Ann Intern Med. 1990;113:261-3.
26. Logsdon DN, Lazaro CM, Meier RV. The feasibility of behavioral risk reduction in primary medical care. Am J Prev Med. 1989;5:249-56.
27. Baker SP, Whitfield RA, O'Neill B. Geographic variations in mor- tality from motor vehicle crashes. N Engl J Med. 1987; 316:1384-7.
28. Baker SP, Whitfield RA, O'Neill B. County mapping of injury mortality. J Trauma. 1988;28:741-5.
29. OrsayEM, Turnbull TL, Dunne M, BarrettJA, Langenberg P, Orsay CP. Prospective study of the effect of safety belts on morbidity and health care costs in motor vehicle accidents. JAMA. 1988;260:3598-603.
30. Lestina DC, WilliamsAF, LundAK, Zador P, Kuhlmann TP. Motor vehicle crash injury patterns and the Virginia seat belt law. JAMA. 1991;265:1409-13.
31. Reath DB, Kirby J, Lynch M, Maull KI. Injury and cost compari- sons of restrained and unrestrained motor vehicle crash victims.J Trauma. 1989;29:1173-7.
32. Christian MS. Morbidity and mortality in car occupants: compar- ative survey over 24 months. BrJ. 1984;289:1525-6.
33. Petrucelli E. Seat belt laws: the New York experience: prelimi- nary data and some observations. J Trauma. 1987;27:706-10.
34. ManningWG, LeibowitzA, Goldberg GA, RogersWH, Newhouse JP. A controlled trial of the effect of a prepaid group practice on use of services. N EnglJ Med. 1984;310:1505-10.
35. Krieger N. Overcoming the absence of socio-economic data in medical records: validation and application of a census-based methodology. AmJ Public Health. 1992;82:703-10.