Embed Size (px)
Citation preview

Introduction
Coronary artery disease remains the leading cause of death in the United States, and remains the largest contributor to the nation’s morbidity and health-
care expenditures.1 Although deaths from heart disease are declining in both women and men in recent years, more women have died from heart disease than men since 1984.1 In addition, the prevalence of heart disease is increasing, to the point where 1 of every 3 female adults has some form of heart disease.1 Given these facts, there is increased atten-tion on prevention of heart disease in women,2 particularly the impact of therapeutic lifestyle changes on reducing the risk of cardiovascular disease. One such area given atten-tion within the Guidelines for Heart Disease Prevention in Women is the role of cardiorespiratory fitness (CRF) on heart disease and mortality in women.2
Physical Fitness versus Physical ActivityCRF is also known as physical fitness, and there is an
extensive body of literature showing the powerful and inverse relationship between one’s fitness level and the risk of death.3–8 Similarly, there is a strong and inverse relation-ship between physical activity and the risk of death and cardiac events in both men and women,9–14 but physical activity is not the same as physical fitness. Physical activity is defined as any body movement produced by contraction of skeletal muscle. Unlike CRF, which can be objectively measured, physical activity is a self-reported behavior and how well it correlates with exercise capacity has not been
extensively vali-dated.15–19 None-theless, attempts have been made to develop and validate question-naires of assess-ment of physical activity, as a sur-rogate measure of physical fitness in women.19 The Women’s Ischemia Syndrome Evalua-tion (WISE) Study compared the CRF level as measured on a symptom-limited exercise stress test in symptomatic women to two questionnaires of physical activity, in which physical activity estimates were compared to measured physical fitness. Physical activity was measured by the Postmenopausal Estrogen and Progesterone Intervention physical activity questionnaire (PEPI-Q) and the Duke Activity Status Index (DASI) questionnaire. Both were well correlated with CRF levels measured during the symp-tom-limited exercise treadmill testing, but the DASI was a significant independent predictor of functional capacity even after adjustment for cardiac risk factors, whereas the PEPI-Q was not.19
Three studies of physical activity that focused on women were studies from the Framingham Heart Study,13 the Women’s Health Initiative (WHI) Observational Study,12 and the Women’s Health Study.20 The Framingham Heart Study demonstrated a relationship between physical activ-
Survival of the Fittest: Impact of Cardiorespiratory Fitness on Mortality, Cardiac Risk, and its Relationship with Body Mass Index in WomenMartha Gulati, M.D., M.S.1,2 and Dina M. Sparano, M.D.1
Departments of 1Medicine, 2Preventive Medicine, Northwestern University, Chicago, IL
222 Obesity Management October 2008 © Mary Ann Liebert, Inc. DOI: 10.1089/obe.2008.0223
Dina M. Sparano, M.D.Martha Gulati, M.D., M.S.

ity and all-cause mortality. The WHI Observational Study was able to show an association between physical activity and cardiac events, but concluded that both walking and vigorous activity for at least 2.5 hours per week carried a similar risk reduction of cardiac events compared to less active women. The Women’s Health Study (WHS) recently reported the protective role of physical activity in more than 39,000 women in terms of incident cardiac events in the following 11 years. Interestingly, this study showed physical activity attenuated risk of cardiac events from elevated BMI in women, but physical activity was not able to entirely eliminate the excess risk of cardiac events associated with being overweight or obese.20 In all these studies, physical activity was assessed by a questionnaire and was essentially an estimate of activity status.
Physical activity is one component that influences an individual’s CRF level (Table 1). It has been shown that increasing a woman’s physical activity is associated with an improvement in her CRF level,21 despite the fact that CRF levels are expected to decline with age.8 Certainly, physical activity is inversely associated with the presence of cardiac risk factors, and is ultimately associated with reduced cardiac events and mortality.12,14,22 It is a practical measure that is easy to use in a clinical setting, in order to estimate a woman’s functional capacity (or CRF level) if measurements of CRF are not available.
Cardiorespiratory Fitness CRF is a quantitative measurement, also known as exer-
cise capacity or physical fitness. It is a measure of amount of work completed before exhaustion. CRF is measured as a function of maximal oxygen uptake (VO2max) at peak exercise, and is measured in units of metabolic equivalents (METs), where 1 MET is the amount of oxy-
gen consumed at a resting state and equals 3.5 mL/kg per minute of oxygen consumption.23
CRF has been shown in numerous studies of men and women to be strongly and inversely associated with cardiovascular risk and mortality.3,4,6,7,24–26 The precise mechanism by which CRF protects against cardiovascular events in not clearly established. It is certainly influenced
by gender and age.8 In addition, there are other biologic determinants that can influence CRF, beyond just the physiologic effects of physical exercise (Table 1).
CRF is measured either directly (by a direct measurement of oxygen exchange) or indirectly (by estimations of oxygen exchange based on the grade and speed of treadmill) by a maximal exercise stress test. Of all the information obtained from an exercise stress test, CRF appears to be the most important prognostic marker.27 CRF has been shown to be an independent predictor of mortality and cardiovascular mor-tality in asymptomatic women, beyond traditional cardiac risk factors (Fig. 1).6,7 The largest of these studies is the St. James Women Take Heart (WTH) Project. In this study of 5721 asymptomatic women who were free of known heart disease, we found that for every MET increase in fitness, there was a 17% reduction in all-cause mortality. In addition, this study showed that performance of less than 5 METS was associated with approximately 3 times the risk of death from any-cause in women, compared with women achieving greater than 8 METs. Those achieving 5–8 METs had twice the risk of death compared to the most fit category.6 To put this into practical terms, 5 METs is considered moderately
October 2008 Obesity Management 223
Table 1. Possible Biologic Links between Cardiorespiratory Fitness and Cardiovascular Outcomes34
TYPE OF LINK LINKS
Determinants of cardiorespiratory fitness
Greater regularity of exerciseGreater intensity of exerciseGeneticsLower body weightHealthy dietNo cigarette smokingIncreased total blood volumeDecreased arterial stiffnessMedications
Standard cardiovascular risk factors
Lower blood pressureLower blood glucoseLower LDL cholesterol and triglycerides
Biologic markers of atherosclerosis
Quantitative coronary angiographyCarotid intimal thickness by ultrasound
Physiologic effects of exercise
Increased HDL cholesterolImproved autonomic balanceIncreased parasymptathetic toneDecreased sympathetic toneImproved endothelial functionDecreased oxidative stressDecreased heart rate
LDL, low-density lipoprotein; HDL, high-density lipoprotein. Modified and adapted from "Functional Capacity and Activities on Daily Living in Women," In: Shaw LJ, Redberg RF (eds.) Coronary Disease in Women. Totowa, NJ: Humana Press Inc., 2004: Ch. 8; pg. 110.
One of every three female adults has some form
of heart disease.

224 Obesity Management October 2008
vigorous activity. Examples include brisk walking (walking 1 mile in 15 minutes), slow swimming, golfing without a cart, doubles tennis, or dancing. Eight METs would be con-sidered vigorous activity, and examples of this include jog-ging (running 1 mile in 12 minutes), rowing, fast swimming in laps, aerobic calisthenics, or downhill skiing.28
Despite its strong prognostic power, the use of CRF in routine care has been problematic because of a lack of standardization, particularly relating to the functions of age and gender. CRF deceases with age and is also lower for women at any given age compared to their male counterparts. The continuous nature of CRF has recently been described and validated in women by our group.8 A nomogram has been derived in asymptomatic women, but validated in symptomatic women, showing that achieving a CRF level of less than 85% of predicted for age would characterize a substantial increase risk of all-cause and cardiovascular mortality in women.8
Although measurements of CRF may not be avail-able clinically in all patients, since current stress testing guidelines do not advocate routine exercise stress testing in asymptomatic persons, when this information is avail-able, it should be translated to patients for its prognostic significance when available.
Fit versus Fat: Impact of Fitness on BMI and Prognosis
Both CRF level and BMI are predictive of mortality and cardiac events. But there is growing evidence that a person’s CRF level may be more important than the
effect of BMI, when determining future risk. This is the basis of the “fit versus fat” theory, meaning that a per-son’s physically fitness level would be more predictive of future cardiovascular risk, and a high level of CRF would attenuate the effects of BMI. This finding means that fitness is far more important in determining cardio-vascular risk, compared to BMI.
The WISE study that was discussed above showed that when fitness was estimated from the DASI questionnaire, fitness was an independent predictor of adverse cardio-vascular events in women where obesity was not.29 None-theless, other studies looking at physical activity and BMI have found that activity alone cannot entirely attenuate the effects of BMI on cardiovascular risk.20,30
When CRF was assessed in the Lipid Research Clinic, the effect of CFR did not entirely attenuate the effect of BMI in women or men; both played an independent role on prognosis.31 On the other hand, another study of both men and women over the age of 60 years concluded that CRF was the most important predictor of mortality, and fully attenuated the risk of BMI and percent body fat.32
Regardless of this ongoing debate, the implications to clinical practice are unchanged. We recommend that preservation or improvement of CRF be encouraged by recommending regular physical activity for all adults, normal-weight, overweight, and obese alike.
Current Recommendations for WomenThe current guidelines for recommendations of physical
fitness and physical activity have been recently updated and have been summarized below (Table 2). The cur-rent guidelines from the American Heart Association and the American College of Sports Medicine recommend
Cardiorespiratory fitness has been shown in
numerous studies of men and women to be strongly and inversely associated with cardiovascular risk
and mortality.
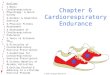
Figure 1. Prognostic value of cardiorespiratory fitness in asymptomatic (N=8715) women as synthesized from the largest published reports.6,7 This figure illustrates the five-year mortality rates for asymptomatic women. METs=achieved metabolic equivalents during exercise stress testing. Reprinted from JACC, Vol 47, Shaw LJ, Merz CNB, Pepine CJ, et al. Insights From the NHLBI-Sponsored Women's Ischemia Syndrome Evaluation (WISE) Study: Part I: Gender Differences in Traditional and Novel Risk Factors, Symptom Evaluation, and Gender-Optimized Diagnostic Strat-egies, S12, 2006, with permission from Elsevier.
8 or higher 7.1 – 8.0 5.5 – 7.0 1.3 – 5.4
6
4
2
0
METs Asymptomatic Women(n = 8,715)
5-Ye
ar D
eath
Rat
e (%
)

October 2008 Obesity Management 225
all healthy adults ages 18–64 should engage in either 30 minutes of moderate-intensity exercise (3–6 METS) at least 5 days per week, or 20 minutes of vigorous-intensity exercise (> 6 METS) 3 days per week.33 The American Heart Association’s Guidelines for cardiovascular disease prevention in women went even further, recommending that for women who need to lose weight or sustain weight loss, a minimum of 60 to 90 minutes of moderate-inten-sity activity should be done on most, and preferably all, days of the week. These guidelines also emphasized the importance of CRF when the measure is available, listing identification of “at-risk” women as women with a poor CRF level.2
ConclusionThe data regarding the role of CRF are quite persuasive
that this measure provides independent prognostic infor-mation in both women and men. When this information is available, translating this information to the person in terms of prognosis will add to the assessment of risk for women. Nonetheless, we do not advocate routine exercise stress testing in asymptomatic women, so when a measure of CRF is not available, estimating CRF from a physical activity inventory is currently recommended when any cardiovascular risk assessment is done, in addition to assessment of tradition cardiovascular risk factors. ■
Author Disclosure StatementNo competing financial interests exist.
References1. Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, Hailpern SM, Ho M, Howard V, Kissela B, Kittner S, Lloyd-Jones D, McDermott M, Meigs J, Moy C, Nichol G, O’Donnell C, Roger V, Sorlie P, Steinberger J, Thom T, Wilson M, Hong Y; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2008 update: A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117:e25–146.2. Mosca L, Banka CL, Benjamin EJ Berra K, Bushnell C, Dolor RJ, Ganiats TG, Gomes AS, Gornik HL, Gracia C, Gulati M, Haan CK, Judelson DR, Keenan N, Kelepouris E, Michos ED, Newby LK, Oparil S, Ouyang P, Oz MC, Petitti D, Pinn VW, Redberg RF, Scott R, Sherif K, Smith SC Jr, Sopko G, Steinhorn RH, Stone NJ, Taubert KA, Todd BA, Urbina E, Wenger NK; Expert Panel/Writing Group; American Heart Association; American Academy of Family Physi-cians; American College of Obstetricians and Gynecologists; Ameri-can College of Cardiology Foundation; Society of Thoracic Surgeons; American Medical Women’s Association; Centers for Disease Control and Prevention; Office of Research on Women’s Health; Associa-tion of Black Cardiologists; American College of Physicians; World Heart Federation; National Heart, Lung, and Blood Institute; American College of Nurse Practitioners. Evidence-based guidelines for car-diovascular disease prevention in women: 2007 update. Circulation. 2007;115:1481–501.3. Ekelund LG, Haskell WL, Johnson JL, Whaley FS, Criqui MH, Sheps DS. Physical fitness as a predictor of cardiovascular mortality in asymptomatic North American men. The Lipid Research Clinics Mor-tality Follow-up Study. N Engl J Med. 1988;319:1379–1384.4. Wei M, Kampert JB, Barlow CE Nichaman MZ, Gibbons LW, Paffenbarger RS Jr, Blair SN. Relationship between low cardiorespi-ratory fitness and mortality in normal-weight, overweight, and obese men. JAMA. 1999;282:1547–1553.5. Blair SN, Kohl HW, 3rd, Paffenbarger RS, Jr., Clark DG, Cooper KH, Gibbons LW. Physical fitness and all-cause mortality. A prospec-tive study of healthy men and women. JAMA. 1989;262:2395–2401.6. Gulati M, Pandey DK, Arnsdorf MF Lauderdale DS, Thisted RA, Wicklund RH, Al-Hani AJ, Black HR. Exercise capacity and the risk of death in women: The St James Women Take Heart Project. Circula-tion. 2003;108:1554–1559.7. Mora S, Redberg RF, Cui Y Whiteman MK, Flaws JA, Sharrett AR, Blumenthal RS. Ability of exercise testing to predict cardiovascular and all-cause death in asymptomatic women: A 20-year follow-up of the lipid research clinics prevalence study. JAMA. 2003;290:1600–1607.8. Gulati M, Black HR, Shaw LJ Arnsdorf MF, Merz CN, Lauer MS, Marwick TH, Pandey DK, Wicklund RH, Thisted RA. The prognostic value of a nomogram for exercise capacity in women. N Engl J Med. 2005;353:468–475.9. Paffenbarger RS, Jr., Hyde RT, Wing AL, Hsieh CC. Physical activ-ity, all-cause mortality, and longevity of college alumni. N Engl J Med. 1986;314:605–613.10. Kannel WB, Feinleib M, McNamara PM, Garrison RJ, Cas-telli WP. An investigation of coronary heart disease in families. The Framingham offspring study. Am J Epidemiol. 1979;110:281–290.11. Stampfer MJ, Hu FB, Manson JE, Rimm EB, Willett WC. Primary prevention of coronary heart disease in women through diet and life-style. N Engl J Med. 2000;343:16–22.
Table 2. Guidelines for Exercise and Fitness in WomenGUIDELINE RECOMMENDATIONS RECOMMENDATIONS
American Heart Association: Guidelines for Cardiovascular Disease Prevention in Women2
• 30 minutes of moderately intense exercise on most and preferably all days
• 60 to 90 minutes of moderately intense exercise on most days to loose or sustain weight loss
American College of Sports Medicine and the American Heart Association33
• 30 minutes of moderate-intensity exercise (3–6 METS) 5 days/week or 20 minutes of vigorous-intensity exercise (>6 METS) 3 days/week
Centers for Disease Control35/Surgeon General36
• At least 30 minutes of moderate physical activity most days of the week
• Even greater amounts of physical activity may be necessary for the prevention of weight gain, for weight loss, or for sustaining weight loss
METS, metabolic equivalents.

226 Obesity Management October 2008
12. Manson JE, Greenland P, LaCroix AZ Stefanick ML, Mouton CP, Oberman A, Perri MG, Sheps DS, Pettinger MB, Siscovick DS. Walk-ing compared with vigorous exercise for the prevention of cardiovas-cular events in women. N Engl J Med. 2002;347:716–725.13. Sherman SE, D’Agostino RB, Cobb JL, Kannel WB. Physical activity and mortality in women in the Framingham Heart Study. Am Heart J. 1994;128:879–884.14. Lee IM, Rexrode KM, Cook NR, Manson JE, Buring JE. Physical activity and coronary heart disease in women: Is “no pain, no gain” passe? JAMA. 2001;285:1447–1454.15. Haskell WL, Leon AS, Caspersen CJ Froelicher VF, Hagberg JM, Harlan W, Holloszy JO, Regensteiner JG, Thompson PD, Washburn RA, et al. Cardiovascular benefits and assessment of physical activity and physical fitness in adults. Med Sci Sports Exerc. 1992;24:S201–220.16. Gotay CC. Patient-reported asessment vesus performance-based tests. In: Spilker B (ed.) Quality of Life and Pharmacoeconomics in Clinical Trials, 2nd ed. Philadelphia: Lippincott-Raven Publishers, 1996:413–420.17. Blair SN, Cheng Y, Holder JS. Is physical activity or physical fit-ness more important in defining health benefits? Med Sci Sports Exerc. 2001;33:S379–399; discussion S419–420.18. Blair SN, Jackson AS. Physical fitness and activity as separate heart disease risk factors: A meta-analysis. Med Sci Sports Exerc. 2001;33:762–764.19. Bairey Merz CN, Olson M, McGorray S Pakstis DL, Zell K, Rick-ens CR, Kelsey SF, Bittner V, Sharaf BL, Sopko G. Physical activity and functional capacity measurement in women: A report from the NHLBI-sponsored WISE study. J Womens Health Gend Based Med. 2000;9:769–777.20. Weinstein AR, Sesso HD, Lee IM Rexrode KM, Cook NR, Man-son JE, Buring JE, Gaziano JM. The Joint Effects of Physical Activity and Bo Effects of different doses of physical activity on cardiorespira-tory fitness among sedentary, overweight or obese postmenopausal women with elevated blood pressure: A randomized controlled trial. JAMA. 2007;297:2081–2091.22. Berlin JA, Colditz GA. A meta-analysis of physical activity in the prevention of coronary heart disease. Am J Epidemiol. 1990;132:612–628.23. Bruce RA, Kusumi F, Hosmer D. Maximal oxygen intake and nomographic assessment of functional aerobic impairment in cardio-vascular disease. Am Heart J. 1973;85:546–562.24. Ellestad MH, Wan MK. Predictive implications of stress testing. Follow-up of 2700 subjects after maximum treadmill stress testing. Circulation. 1975;51:363–369.
25. Carnethon MR, Gulati M, Greenland P. Prevalence and cardiovas-cular disease correlates of low cardiorespiratory fitness in adolescents and adults. JAMA. 2005;294:2981–2988.26. Carnethon MR, Gidding SS, Nehgme R, Sidney S, Jacobs DR, Jr., Liu K. Cardiorespiratory fitness in young adulthood and the development of cardiovascular disease risk factors. JAMA. 2003;290:3092–3100.27. Roger VL, Jacobsen SJ, Pellikka PA, Miller TD, Bailey KR, Gersh BJ. Prognostic value of treadmill exercise testing: A population-based study in Olmsted County, Minnesota. Circulation. 1998;98:2836–2841.28. American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription. 6th ed. Baltimore: Lippincott Wil-liams & Wilkins; 2000.29. Wessel TR, Arant CB, Olson MB Johnson BD, Reis SE, Sharaf BL, Shaw LJ, Handberg E, Sopko G, Kelsey SF, Pepine CJ, Merz NB. Relationship of physical fitness vs body mass index with coronary artery disease and cardiovascular events in women. JAMA. 2004;292:1179–1187.30. Hu FB, Willett WC, Li T, Stampfer MJ, Colditz GA, Manson JE. Adiposity as compared with physical activity in predicting mortality among women. N Engl J Med. 2004;351:2694–2703.31. Stevens J, Cai J, Evenson KR, Thomas R. Fitness and fatness as predictors of mortality from all causes and from cardiovascular disease in men and women in the lipid research clinics study. Am J Epidemiol. 2002;156:832–841.32. Sui X, LaMonte MJ, Laditka JN Hardin JW, Chase N, Hooker SP, Blair SN. Cardiorespiratory Fitness and adiposity as mortality predic-tors in older adults. JAMA. 2007;298:2507–2516.33. Haskell WL, Lee IM, Pate RR Powell KE, Blair SN, Franklin BA, Macera CA, Heath GW, Thompson PD, Bauman A; American College of Sports Medicine; American Heart Association. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Cir-culation. 2007;116:1081–1093.34. Pothier CE, MS L. Functional capacity and activities of daily liv-ing in women. In: Shaw LJ, Redberg RF (eds.) Coronary Disease in Women. Totowa, NJ: Humana Press Inc., 2004:110.35. Pate RR, Pratt M, Blair SN Haskell WL, Macera CA, Bouchard C, Buchner D, Ettinger W, Heath GW, King AC, et al. Physical activity and public health. A recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA. 1995;273:402–407.36. Department of Health and Human Services, Center for Disease Control and Prevention, National Center for Disease Prevention and Health Promotion. Physical Activity and Health: A Report of the Sur-geon General. Atlanta, GA: 1996.