Embed Size (px)
Citation preview

Correspondence
142 www.thelancet.com/neurology Vol 9 February 2010
acute hypertension and lag time from presentation to diagnosis, as suggested by Fei and colleagues, are also worthy of investigation, these data were not collected in the early years of our study, and therefore could not be analysed.
With regard to our choice of predictors, some variables were chosen on the basis of published work: stroke size and age have previously been associated with adverse neurological outcome in childhood-onset stroke.4–6 However, there is a relative paucity of studies of outcome after childhood stroke to guide the selection of predictors. Hence, our analysis was exploratory and intended to generate new predictors in view of the limited research in this area. Stroke subtypes were particularly of interest given the predictive value of the TOAST classifi cation in adults. Indeed, we found that arteriopathy was associated with an increased risk of early adverse outcome.
Further studies of childhood-onset AIS are needed to substantiate our observations of novel prognostic factors such as arteriopathy. The success of future eff orts towards developing risk-stratifi ed therapeutic approaches for childhood-onset AIS depends in
part upon a broader knowledge of prognostic factors of this disease. As part of this eff ort, research is underway by the International Pediatric Stroke Study investigators to evaluate the prognostic usefulness of a paediatric adaptation of the NIHSS, to evaluate the relations between infl ammation, arteriopathy, and outcome, and to develop a consensus-based classifi ca-tion system for childhood-onset AIS.We have no confl icts of interest.
Timothy J Bernard, Neil A Goldenberg, Heather J Fullerton, Anne Gordon, Gabrielle [email protected]
Department of Pediatrics, University of Colorado Denver, Children’s Hospital, and Mountain States Regional Hemophilia and Thrombosis Center, Aurora, CO, USA (TJB, NAG); Section of Hematology, Oncology, and Bone Marrow Transplantation (NAG), Section of Child Neurology (TJB), and Departments of Neurology and Pediatrics (HJF), University of California San Francisco, San Francisco, CA, USA; Children’s Neuroscience Centre, Royal Children’s Hospital and Murdoch Children’s Research Institute, Melbourne, Australia (AG); and Division of Neurology, Hospital for Sick Children, Toronto, Ontario, Canada (GdV)
1 Winbeck K, Poppert H, Etgen T, Conrad B, Sander D. Prognostic relevance of early serial C-reactive protein measurements after fi rst ischemic stroke. Stroke 2002; 33: 2459–64.
2 Potter J, Robinson T, Ford G, et al. CHHIPS (controlling hypertension and hypotension immediately post-stroke) pilot trial: rationale and design. J Hypertens 2005; 23: 649–55.
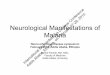
Sex; age (years)
Comorbidities Onset (day of infl uenza-like illness)
Neurological diagnosis
CT scan of brain
MRI scan of brain
EEG CSF analysis Treatment Outcome
1 Female; 43 Myasthenia gravis 4 Exacerbation of myasthenia gravis
·· ·· ·· ·· Intravenous immunoglobulin, oseltamivir
RWS
2 Male; 28 Chronic progressive external ophthalmoplegia
2 First seizure Brain atrophy ·· ·· Increased protein concentrations
Oseltamivir, carbamazepine
RWS
3 Female; 16 None 2 First seizure Normal Normal ·· ·· None RWS
4 Male; 30 Migraine, asthma, gout 7 Migraine exacerbation
Normal ·· ·· ·· Oseltamivir, cafergot RWS
5 Female; 16 Febrile seizures 4 First seizure Brain atrophy Brain atrophy Normal ·· None RWS
6 Male; 19 Previous seizure, asthma 7 Recurrent seizure ·· Normal ·· ·· Oseltamivir, sodium valproate
RWS
7 Male; 18 None 2 First seizure Normal Normal ·· Normal Oseltamivir RWS
8 Male; 15 None 3 First seizure ·· ·· ·· ·· Oseltamivir RWS
9 Male; 57 Diabetes mellitus, hypertension, ischaemic heart disease
4 Acute ischaemic stroke
·· Right corona radiata infarct
·· ·· Aspirin Stroke rehabilitation
EEG=electroencephalogram. RWS=recovered without sequelae. ··=not done.
Table: Patients with infl uenza A H1N1 virus with neurological complications and their clinical features, investigations, treatment, and outcomes
3 Adams HP Jr, Davis PH, Leira EC, et al. Baseline NIH stroke scale score strongly predicts outcome after stroke: a report of the Trial of Org 10172 in Acute Stroke Treatment (TOAST). Neurology 1999; 53: 126–31.
4 Ganesan V, Hogan A, Shack N, Gordon A, Isaacs E, Kirkham FJ. Outcome after ischaemic stroke in childhood. Dev Med Child Neurol 2000; 42: 455–61.
5 deVeber GA, MacGregor D, Curtis R, Mayank S. Neurologic outcome in survivors of childhood arterial ischemic stroke and sinovenous thrombosis. J Child Neurol 2000; 15: 316–24.
6 Gordon AL, Ganesan V, Towell A, Kirkham FJ. Functional outcome following stroke in children. J Child Neurol 2002; 17: 429–34.
Surveillance of H1N1-related neurological complications
We read with interest the recent editorial urging the neurological community to make plans for coordinated surveillance programmes to estimate the overall burden of pandemic H1N1 infl uenza-related and vaccine-related neurological complications.1 The report by the US Centers for Disease Control and Prevention (CDC) described the fi rst patients who developed neurological complications associated with the 2009 infl uenza A H1N1 virus, the fi rst infl uenza pandemic of the

Correspondence
www.thelancet.com/neurology Vol 9 February 2010 143
21st century.2 These patients were four previously healthy children who presented with infl uenza-like illness and either seizures or encephalopathy but recovered fully without neuro-logical sequelae.
We retrospectively reviewed all patients diagnosed with H1N1 infection in two major hospitals (Tan Tock Seng Hospital and Changi General Hospital) in Singapore from June, 2009, to October, 2009, to determine the burden of neurological complications. Infections were confi rmed with PCR by use of nasal and/or throat swabs. Nine of 826 hospitalised patients with the H1N1 virus were identifi ed to have neurological complications (table 1). The patients, aged 15–57 years, all had onset of neurological complications within 1 week of onset of symptoms of infl uenza (mean 3·8 days; range 2–7 days). These complications included six cases with a seizure (one with a recurrent seizure), one case of myasthenia gravis exacerbation, one case of migraine exacerbation, and one case of ischaemic stroke. Four of these nine patients had no pre-existing neurological or other systemic comorbidities. Neurological examination, neuroimaging, and CSF analysis were normal except in patients with underlying neurological disease. Most patients were treated
with oseltamivir and any underlying neurological disorders were also treated. All individuals recovered fully without any sequelae, except for patient 9 who is undergoing stroke rehabilitation.
In our cohort, neurological complications associated with the H1N1 virus were generally mild but also notably aff ected individuals older than 15 years. First-onset seizure was the most common complication. However, the infection also precipi-tated seizures in patients with previous seizures or with a propensity for seizures (ie, in the patient with chronic progressive external ophthalmoplegia). Although it is not possible to exclude a coincidental association between H1N1 infection and neurological illness, such as in the case of ischaemic stroke, the late-onset fi rst seizures in some of these young adults suggest a possible causal link. Similarly, the infection in some cases might have exacerbated an underlying chronic neurological disorder.
The vaccine against pandemic H1N1 has recently become available.3 Although this strain of H1N1 infl uenza virus has so far been relatively mild in most aff ected people, it has caused neurological complications in 1·1% of our patient cohort. We recommend that all patients with underlying
neurological disease should receive the pandemic H1N1 vaccine as well as seasonal infl uenza vaccination as these individuals are at risk of developing neurological complications from infl uenza infections.
Neurologists, infectious disease physicians, and paediatricians in Singapore are planning coordinated surveillance to estimate the overall national burden of neurological com-plications of H1N1 infection. The Health Sciences Authority in Singapore is also undertaking pharmacovigilance of the new vaccines.4
We have no confl icts of interest.
Kevin Tan, Asha Prerna, Yee-Sin [email protected]
Department of Neurology, National Neuroscience Institute, Singapore (KT, AP); and Department of Infectious Disease, Tan Tock Seng Hospital, Singapore (Y-SL)
1 Pandemic infl uenza: a priority for the neurological community. Lancet Neurol 2009; 8: 869.
2 Neurologic complications associated with novel infl uenza A (H1N1) virus infection in children—Dallas, Texas, May 2009. MMWR Morb Mortal Wkly Rep 2009; 58: 773–78.
3 Zhu FC, Wang H, Fang HH, et al. A novel infl uenza A (H1N1) vaccine in various age groups. N Engl J Med 2009; 361: 2414–23.
4 Health Sciences Authority. About HSA regulatory review on infl uenza A H1N1 vaccines. http://www.hsa.gov.sg/publish/hsaportal/en/for_consumers/infl uenza_a_-_h1n1/h1n1_vaccines/about_hsa_regulatory.html (accessed Dec 3, 2009).