Embed Size (px)
Citation preview

Surveillance of AMR in PHE: a multi-disciplinary, integrated approach
Professor Neil Woodford Antimicrobial Resistance & Healthcare Associated Infections (AMRHAI) Reference Unit
© Crown copyright

2 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright
International Consensus: AMR is a Critical Public Health Threat

UK 5-year AMR Strategy 2013-18: Seven key areas for action
PHE Human health
DH – High Level Steering Group
Defra Animal health DH
1. Optimising prescribing practice 2. Improving infection prevention and control 3. Improving professional education, training
and public engagement 4. Better access to and use of surveillance data
• Improving the evidence base through research
• Developing new drugs, vaccines and other diagnostics and treatments
• Strengthening UK and international collaboration
3 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

HCAI & AMR surveillance
4 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

Sources of data on AMR
5 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright
• Hospital laboratories routinely identify bacteria and test antimicrobial susceptibility
• Data stored in LIMS
• GPs do not routinely sample patients microbiologically (except for treatment failures)
• Testing for resistance in fungi and viruses is not yet routine

Surveillance of AMR in England and Wales
6 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright
• Since 1974, hospitals in England & Wales have voluntarily reported infections to the PHLS / HPA / PHE • Data stored in national database (now SGSS)
• Since 1989, laboratories have also voluntarily reported results of susceptibility testing • Originally paper reports, but now electronic
• Huge quantity, but limited control of quality • Cross-validate with other national schemes (e.g. BSAC)

The SGSS Report Menu
7 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

Making Use of AMR Data
• Guide empirical prescribing
• Determine burden of disease • Determine resources
required • Strategic planning
• Measure impact of interventions
• Scope • Local • Regional • National • International
• Focus • Organism • Disease • Patient groups
8 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

Mandatory Reporting of MRSA bacteraemia • From April 2001, it was mandatory
for all acute NHS trusts in England to report:
• All cases of bacteraemia caused by S. aureus
• The proportion of cases due to MRSA
• No of MRSA/1000 bed days • Data made publically
available
9 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

Driving down MRSA bacteraemias • DH Press Release 05/11/04: Hospital
superbug must be halved • Bloodstream infections with the
hospital superbug MRSA must be halved in three years, the government has said.
• Health Secretary John Reid tasked
NHS hospitals with achieving a year on year reduction up to and beyond March 2008.
10 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

Rising numbers of E. coli bacteraemias
-
5,000
10,000
15,000
20,000
25,000
30,000
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Num
ber o
f bac
tera
emia
repo
rts
Escherichia coli Staphylococcus aureus
11 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

Key antibiotic resistance messages
• Reduction, through effective IPC, in proportion of Staphylococcus aureus BSI that caused by MRSA from 12% to 8% over the last 5 years
• 23% reduction in Streptococcus pneumoniae BSI related to pneumococcal vaccination over last 5 years
• The rate of Escherichia coli and Klebsiella pneumoniae bloodstream infections (BSI) increased by 13.5% and 17.2% respectively from 2010 to 2014.
• More individuals have antibiotic-resistant BSI with Gram-negative bacteria
12 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

Carbapenem non-susceptibility, EARS-Net 2013
13 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright
K. pneumoniae E. coli • data risk giving a false sense of security to non-experts • only 9% of UK carbapenemase producers are from blood cultures

Enhancing surveillance with reference microbiology
Pathogen % carbapenem resistance 2008 2009 2010 2011 2012 2013
E. coli 0.08 0.09 0.11 0.18 0.25 0.22 K. pneumoniae 0.7 0.4 0.6 1.2 1.1 1.6
14 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright Data, courtesy Prof Alan Johnson
• Reference laboratory provides specialist microbiology that seeks to explain trends
• Is at the centre of a national / regional laboratory network • Benefits from a ‘spider’s web effect’ • Monitors new and emerging AMR issues, long before they register in surveillance programmes

PHE’s national reference laboratory
The AMRHAI Reference Unit • Susceptibility testing
• for confirmation of exceptional resistances
• Infer resistance mechanisms from antibiograms
• Investigation of priority resistance mechanisms
• Strain typing to aid outbreak investigation
• Treatment advice; infection prevention & control advice
• + Research (externally-funded)
• + Evaluations of new drugs and diagnostics (externally-funded)
15 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

Focus on ‘alert’ resistances: CPOs in the UK
16 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright AMRHAI, Unpublished data

CPE in the UK, 2000-2014
Klebsiella spp. 79%; E. coli 12%, Enterobacter spp., 7%; others 2%
17 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright AMRHAI, Unpublished data
Early cases often imported
Imported & ‘home grown’

18 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright Health Protection Report Vol 9 No. 2 – 16 January 2015
‘CPE’ are multi-resistant, 2014

Monitoring antibiotic usage in England (ESPAUR)
• Established by PHE in 2013 in response to the strategy
• Terms of reference updated in 2015, at year 2 review
• Focuses on bringing together NHS, PHE, Private sector across all prescribers and clinicians to improve • Surveillance data on antibiotic resistance and prescribing • Antimicrobial stewardship activities • Education and training for healthcare professionals • Education and awareness to public
19 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

Carbapenem usage is increasing
• Carbapenems = 0.3% of total antibiotic consumption in 2013
• BUT use increased by 31.3% in England between 2010 and 2013
• Mostly in the hospital sector, <1% in primary care.
• MEM = c. 90% of carbapenem use
20 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright
• ↑ use of carbapenems • new selective pressures, …with consequences

ESPAUR: Key Progress towards objectives • PHE: better surveillance data for non-bacteraemia isolates
• Enhancement of community antibiotic datasets: dentists, out-of-hours and other providers
• Work on Quality Premium
• Measurement of impact of behavioural interventions published by behavioural insights team
• Antibiotic stewardship curriculum (for healthcare professionals) implementation recommendations delivered to HEE
• Updated Antimicrobial stewardship toolkits (SSTF and TARGET)
• Partnerships external to PHE: universities (HPRU), Vets (VMD), ECDC, WHO, O Neill, Longitude Prize
21 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

Summary Antibiotic Use • Total antibiotic prescribing, measured using defined daily doses, a
standardised measure of antibiotic consumption: • continues to increase in the NHS • with a slower rate of increase from 2013 to 2014 than in previous
years.
• Antibiotic prescriptions in primary care, measured as the number of prescriptions dispensed, adjusted for the age and sex distributions in the population: • has declined for the last two years • is now lower than the similar measure in 2011 (1.180 in 2014
compared to 1.233 in 2011), • suggests higher doses or longer course lengths in GP prescriptions.
22 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

Summary Antibiotic Use
• The majority of antibiotic prescribing occurs in primary care but secondary care prescribes more broad-spectrum antibiotics • These antibiotics are effective against a wide range of bacteria,
but are more likely to drive antibiotic resistance than narrow-spectrum antibiotics.
• Early evidence suggests that informing prescribers of their prescribing patterns and comparing them to their peer professionals may be a factor that helps reduce their antibiotic prescribing.
• Continued focus by every individual who prescribes, administers and dispenses antibiotics is essential to continue to reduce antibiotic consumption.
23 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

Limiting the impact of AMR through IPC
• RAPID diagnostics are essential for identifying colonized and infected patients:
1. rapid implementation of infection control procedures
2. Prevent onwards transmission 3. appropriate patient management
• Who are the ‘high risk’ patients; overseas imports vs. within country inter-hospital transfers ?
24 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

Gaps in surveillance
• Reference laboratory characterises increasing numbers of carbapenemase producers, but epidemiological data missing:
• Foreign travel • Previous hospital admissions • Potential contact with other cases infected/colonised with
carbapenemase-producing Gram-negative bacteria • Antibiotic prescribing • Outcomes e.g. mortality
25 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

Electronic Reporting System (ERS)
26 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright
https://cro.phe.nhs.uk/ Manuals available online (see link)
Web-based reporting system
Electronic data capture of surveillance data and microbiology results
Serves two main functions: • Labs can request full
characterisation of Gram-negative bacteria where expression of acquired carbapenemase suspected
• NHS Trusts can submit enhanced surveillance data
Involves prospective and retrospective data submission

Electronic Reporting System (ERS)
Core dataset • Prospective data submission
– Required when isolate referred
• Performed by local microbiology laboratory
• Patient demographic data • Laboratory details • Patient location at time of
specimen collection
27 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright
Enhanced dataset • Retrospective data submission
• Within 7 days of positive result
• Performed by local laboratory and/or trust IPCT
• Travel history (including healthcare abroad)
For admitted patients: • Admission details • Screening results • Potential contact with CPOs

Referral of isolates and data submission
28 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright
Suspected carbapenemase
producer detected at local
microbiology laboratory
Isolate referred by microbiologist for confirmatory
testing
Enhanced (retrospective) data
submitted by microbiologist or infection control
practitioner
Confirmatory testing performed
at regional laboratory
Confirmatory testing
performed at national
laboratory Core
(prospective) data submitted
by microbiologist
Microbiologist releases positive record to infection control practitioner
Test results made available
Data captured by Electronic Reporting System
Data collated and analysed – results fed back to stakeholders

Reporting from the ERS Regular national reports will be prepared by AMRHAI and the HCAI & AMR
Department • Act as official reports for PHE
Monthly reports • Numbers of Enterobacteriaceae/non-Enterobacteriaceae by resistance
mechanism
Quarterly reports • Include trend analysis
Annual report • Detailed analysis for peer review publication • Include risk factor analysis • Completeness of enhanced surveillance data
29 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

Working with academia
30 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright
• Health Protection Research Units in HCAI and AMR • Imperial College and PHE (Alison Holmes and Alan Johnson) • University of Oxford and PHE (Derrick Crook and Neil Woodford)
• National research units involving a network of relevant, world class expertise that can comprehensively address the challenges of AMR and HCAI, with the resilience and capacity to respond to emerging issues and public health priorities
• Creating integrated programmes of research to develop new, cost-effective approaches for detection, surveillance, investigation and reduction of HCAI and AMR in the NHS
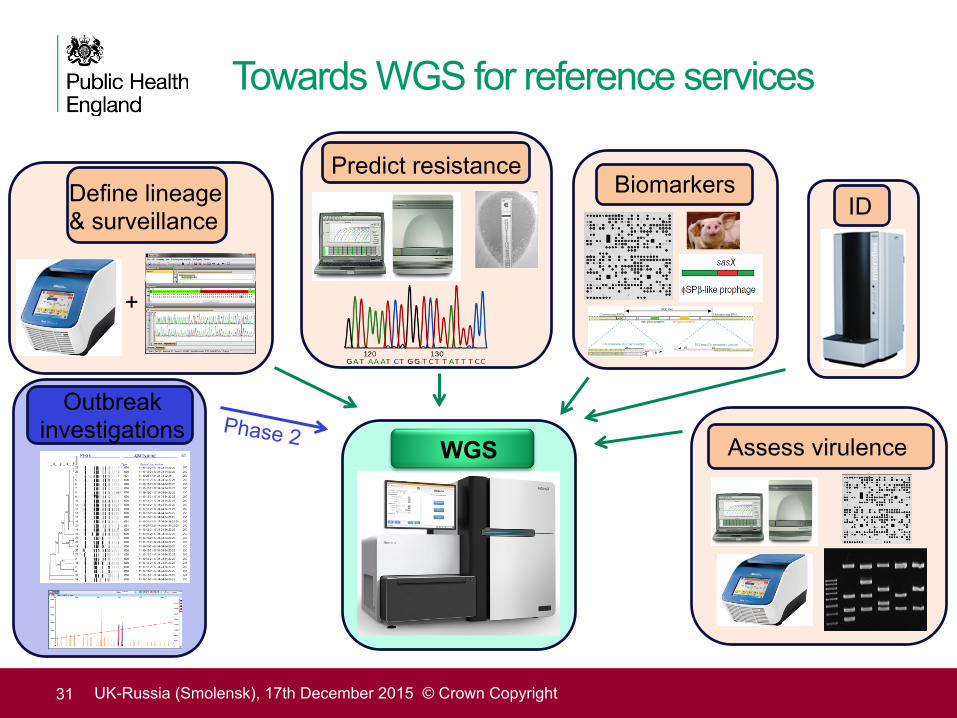
Towards WGS for reference services
31 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright
ID Define lineage & surveillance
Assess virulence
+
Predict resistance
Outbreak investigations
WGS
Biomarkers
Phase 2

Mining WGS data – a new era for AMR surveillance
• Increasing numbers of labs using WGS
• Can rapidly ‘mine’ existing data for to establish national occurrence of new resistance genes
• Analysis can be confirmed if data are public domain
• ‘Straight to WGS’ for settings with poor AMR surveillance ?
32 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright
Petersen et al. Nature Sci Reports 2015; 5, 1-9

Feed into the UK’s integrated surveillance of AMR risks
Colonized residents or visitors
Non-human reservoirs: animals and environment
Victims from conflict zones
Hospital treatment or travel overseas
• Multiple risks to be assessed to minimize damage • We need better intelligence
Inter-hospital transfers (UK)
Non-human reservoirs: foodstuffs (domestic or imported)
33 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright

Summary
• PHE has an AMR surveillance system that captures data nationally • ‘SGSS’ extends data beyond bacteraemias • can combine with patient-level data for e.g. outcomes analysis
• PHE can link resistance rates and prescribing at local level (community and hospital) • Can seek to change behaviours of top prescribers
• The national reference laboratory monitors nationally-rare ‘alert’ resistances • Can be targeted in enhanced surveillance programmes
• Working to link better ‘human-animal’ data to extend One Health analysis
34 UK-Russia (Smolensk), 17th December 2015 © Crown Copyright