Embed Size (px)
Citation preview

Sponsored by
AAGLAdvancing Minimally Invasive Gynecology Worldwide
Surgical Tutorial 6: Surgical Management of Fibroids
PROGRAM CHAIR
Malcolm G. Munro, MD
Keith B. Isaacson, MD Olav Istre, MD, PhD Charles E. Miller, MD

Professional Education Information Target Audience This educational activity is developed to meet the needs of residents, fellows and new minimally invasive specialists in the field of gynecology. Accreditation AAGL is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The AAGL designates this live activity for a maximum of 1.0 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. DISCLOSURE OF RELEVANT FINANCIAL RELATIONSHIPS As a provider accredited by the Accreditation Council for Continuing Medical Education, AAGL must ensure balance, independence, and objectivity in all CME activities to promote improvements in health care and not proprietary interests of a commercial interest. The provider controls all decisions related to identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the activity. Course chairs, planning committee members, presenters, authors, moderators, panel members, and others in a position to control the content of this activity are required to disclose relevant financial relationships with commercial interests related to the subject matter of this educational activity. Learners are able to assess the potential for commercial bias in information when complete disclosure, resolution of conflicts of interest, and acknowledgment of commercial support are provided prior to the activity. Informed learners are the final safeguards in assuring that a CME activity is independent from commercial support. We believe this mechanism contributes to the transparency and accountability of CME.

Table of Contents
Course Description ........................................................................................................................................ 1 Disclosure ...................................................................................................................................................... 2 Conserving the Uterus: Options, Evaluation, and Patient Selection M.G. Munro .................................................................................................................................................. 3 Hysteroscopic Management – The Most Minimally Invasive Surgical Approach K.B. Isaacson ................................................................................................................................................. 9 Abdominal Management – Laparoscopic Management Techniques C.E. Miller ................................................................................................................................................... 14 Abdominal Management – The Very Large Uterus O. Istre ........................................................................................................................................................ 17 Cultural and Linguistics Competency ......................................................................................................... 21

Surgical Tutorial 6: Surgical Management of Fibroids
Malcolm G. Munro, Chair
Faculty: Keith B. Isaacson, Olav Istre, Charles E. Miller This session provides an opportunity for attendees to gain insight into the contemporary issues around myomectomy and to discover “pearls” that will help them provide safer, more effective surgical management of women afflicted with leiomyomas. The faculty participating in this surgical tutorial all have extensive experience with such patients and their operative management via the hysteroscopic, laparoscopic, and laparotomic approaches. The essential steps in patient assessment will be reviewed, with a particular emphasis on uterine imaging and the features that help determine the most appropriate route of removal. Hysteroscopic morcellators have been positioned as replacements for the uterine resectoscope – the advantages and limitations of each of these devices will be discussed and demonstrated. The preferred abdominal approach to myomectomy is laparoscopic, but there are a number of instances where laparotomy still has a major role. Identification of which patients are most appropriate for which technique will be covered, and, for each approach, key surgical techniques will be covered by the faculty using presentation graphics and videos. Such techniques include laparoscopic port selection, management of multiple leiomyomas, and laparoscopic extraction options. Attendees will have an opportunity to ask questions at the end of the session. Learning Objectives: At the conclusion of this course, the clinician will be able to: 1) Evaluate patients for the appropriate route of myomectomy, and describe key elements in the performance of hysteroscopic, laparoscopic, and laparotomic removal of uterine leiomyomas.
Course Outline 2:15 Welcome, Introductions and Course Overview M.G. Munro
2:20 Conserving the Uterus: Options, Evaluation, and Patient Selection M.G. Munro • Description of the Spectrum of Options • Identification of Patient Goals • Evaluation – Imaging, Imaging, Imaging (FIGO-‐based Evaluation) • Creating the Menu of Options
2:30 Hysteroscopic Management – The Most Minimally Invasive K.B. Isaacson Surgical Approach • Resectoscope or Electromechanical Morcellator?
2:40 Abdominal Management – Laparoscopic Management Techniques C.E. Miller • Port Placement • Techniques for Enucleation and Multiple Myomectomy • Uterine Wound Closure • Extraction of Leiomyomas from the Peritoneal Cavity
2:50 Abdominal Management – The Very Large Uterus O. Istre • Factors That Make Laparotomy the Preferred Approach • Ancillary Techniques to Facilitate Surgery on the Very Large Uterus • Techniques for Laparoscopic Approach to the Very Large Uterus
3:00 Questions & Answers All Faculty
3:15 Adjourn
1

PLANNER DISCLOSURE The following members of AAGL have been involved in the educational planning of this workshop and have no conflict of interest to disclose (in alphabetical order by last name). Art Arellano, Professional Education Manager, AAGL* Amber Bradshaw Speakers Bureau: Myriad Genetics Lab Other: Proctor: Intuitive Surgical Erica Dun* Frank D. Loffer, Medical Director, AAGL* Linda Michels, Executive Director, AAGL* Johnny Yi* SCIENTIFIC PROGRAM COMMITTEE Arnold P. Advincula Consultant: Intuitive Royalty: CooperSurgical Sarah L. Cohen* Jon I. Einarsson* Stuart Hart Consultant: Covidien Speakers Bureau: Boston Scientific, Covidien Kimberly A. Kho Contracted/Research: Applied Medical Other: Pivotal Protocol Advisor: Actamax Matthew T. Siedhoff Other: Payment for Training Sales Representatives: Teleflex M. Jonathon Solnik Consultant: Z Microsystems Other: Faculty for PACE Surgical Courses: Covidien FACULTY DISCLOSURE The following have agreed to provide verbal disclosure of their relationships prior to their presentations. They have also agreed to support their presentations and clinical recommendations with the “best available evidence” from medical literature (in alphabetical order by last name). Keith B. Isaacson* Olav Istre* Charles E. Miller Contracted/Research: AbbVie, Actavis, Aegea Medical, Bayer Healthcare Corp., Covidien, Gynesonics, Intuitive Surgical Consultant: AbbVie, Covidien, Ethicon Endo-‐Surgery, Gynesonics, Halt Medical, Intuitive Surgical, Pacira Pharrmaceuticals Speakers Bureau: Ethicon Endo-‐Surgery, intuitive Surgical, Smith & Nephew Endoscopy Royalty: Thomas Medical Malcolm G. Munro Consultant: Aegea Medical, Bayer Healthcare Corp., Boston Scientific, Gynesonics, Hologic, Idoman Teoranta Asterisk (*) denotes no financial relationships to disclose.
2

Malcolm G. Munro MD, FRCS(c), FACOGProfessor, Department of Obstetrics & Gynecology
David Geffen School of Medicine at UCLADirector of Gynecologic Services
Kaiser Permanente, Los Angeles Medical CenterLos Angeles, CA, USA
Malcolm G. Munro MDDisclosures
Consultant:Aegea MedicalBayer Healthcare Corp.Boston ScientificGynesonicsHologicIdoman Teoranta
Conserving the Uterus with Fibroids:Options, Evaluation & Patient Selection
Objectives
• Describe the surgical alternatives to hysterectomy for symptoms associated with uterine leiomyomas
• Discuss the approach to evaluation of patients with uterine leiomyomas
• Counsel women with symptoms thought to be related to leiomyomas considering their reproductive, cosmetic and economic goals
• Leiomyoma manifestations
• The spectrum of options
• Identification of patient goals
• Evaluation
• Creating the menu of options
Conserving the Uterus with Fibroids:Options, Evaluation & Patient Selection
Agenda
• Leiomyoma manifestations
• The spectrum of options
• Identification of patient goals
• Evaluation
• Creating the menu of options
Conserving the Uterus with Fibroids:Options, Evaluation & Patient Selection
Agenda
Manifestation
• Asymptomatic
• Abnormal Uterine Bleeding
• Bulk/pressure symptoms
• Infertility
• Recurrent Pregnancy Loss
• Other
Conserving the Uterus: Options, Evaluation & Patient Selection-Leiomyoma Manifestations
00
22
33
11
44
5566
77
00
2-52-5
0
2
3
1
4
56
7
0
2-5
3

• Leiomyoma manifestations
• The spectrum of surgical options
• Identification of patient goals
• Evaluation
• Creating the menu of options
Conserving the Uterus with Fibroids:Options, Evaluation & Patient Selection
Agenda
00
22
33
11
44
5566
77
00
2-52-5
0
2
3
1
4
56
7
0
2-5
Conserving the Uterus: Options, Evaluation & Patient Selection
Options for Leiomyoma-Associated Symptoms
• AUB
• Bulk Symptoms
Medical Therapy
• AUB
• Bulk Symptoms
• Infertility
• Recurrent Pregnancy Loss
Myomectomy
• AUB
• Bulk Symptoms
• Infertility?
• Recurrent Pregnancy Loss?
Image Guided Therapy
• AUB
Endometrial Ablation
00
22
33
11
44
5566
77
00
2-52-5
0
2
3
1
4
56
7
0
2-5
Conserving the Uterus: Options, Evaluation & Patient Selection
Options for Leiomyoma-Associated Symptoms
• AUB
• Bulk Symptoms
Medical Therapy
• AUB
• Bulk Symptoms
• Infertility
• Recurrent Pregnancy Loss
Myomectomy
• AUB
• Bulk Symptoms
• Infertility?
• Recurrent Pregnancy Loss?
Image Guided Therapy
• AUB
Endometrial Ablation
Procedural Options00
22
33
11
44
55
66
77
00
2-52-5
0
2
3
1
4
5
6
7
0
2-5
Conserving the Uterus: Options, Evaluation & Patient Selection
Procedural Options
• Myomectomy
• Leiomyoma ablation
• Endometrial ablation
• Myomectomy– Laparoscopic
– Laparotomic
• Uterine Artery Occlusion
• Leiomyoma Ablation
• Uterine Artery Embolization
• MR-guided Focused Ultrasound
Intrauterine
Abdominal
Interventional Radiology
00
22
33
11
44
55
66
77
00
2-52-5
0
2
3
1
4
5
6
7
0
2-5
• Myomectomy
• Leiomyoma ablation
• Endometrial ablation
• Myomectomy– Laparoscopic
– Laparotomic
• Uterine Artery Occlusion
• Leiomyoma Ablation
• Uterine Artery Embolization
• MR-guided Focused Ultrasound
Intrauterine
Abdominal
Interventional Radiology
Conserving the Uterus: Options, Evaluation & Patient Selection
Procedural Options
00
22
33
11
44
55
66
77
00
2-52-5
0
2
3
1
4
5
6
7
0
2-5
• Myomectomy
• Leiomyoma ablation
• Endometrial ablation
• Myomectomy– Laparoscopic
– Laparotomic
• Uterine Artery Occlusion
• Leiomyoma Ablation
• Uterine Artery Embolization
• MR-guided Focused Ultrasound
Intrauterine
Abdominal
Interventional Radiology
Conserving the Uterus: Options, Evaluation & Patient Selection
Procedural Options
4

00
22
33
11
44
55
66
77
00
2-52-5
0
2
3
1
4
5
6
7
0
2-5
• Myomectomy
• Leiomyoma ablation
• Endometrial ablation
• Myomectomy– Laparoscopic
– Laparotomic
• Uterine Artery Occlusion
• Leiomyoma Ablation
• Uterine Artery Embolization
• MR-guided Focused Ultrasound
Intrauterine
Abdominal
Interventional Radiology
Conserving the Uterus: Options, Evaluation & Patient Selection
Procedural Options
• Leiomyoma manifestations
• The spectrum of surgical options
• Identification of patient goals
• Evaluation
• Creating the menu of options
Conserving the Uterus:Options, Evaluation & Patient Selection
Agenda
Manifestation
• AUB
• Bulk/pressure symptoms
• Infertility
• Recurrent Pregnancy Loss
• Other
Goal(s)
• Symptom control
• Fertility– Preserve or enhance
– No desire for future fertility
• Cosmetic result
• Minimizing economic impact of intervention
Conserving the Uterus: Options, Evaluation & Patient Selection-Identification of Patient Goals
00
22
33
11
44
5566
77
00
2-52-5
0
2
3
1
4
56
7
0
2-5
• Leiomyoma manifestations
• The spectrum of surgical options
• Identification of patient goals
• Evaluation
• Creating the menu of options
Conserving the Uterus:Options, Evaluation & Patient Selection
Agenda
• Are the symptoms related to the leiomyomas?
• Is surgery the most appropriate intervention?
• Determination of: – FIGO Type(s)
– Location (anterior, posterior, fundal, lower segment)
– Size or volume
– Number
• List of options compatible with patient goals
Conserving the Uterus: Options, Evaluation & Patient Selection-Evaluation of Patients with Leiomyomas
00
22
33
11
44
5566
77
00
2-52-5
0
2
3
1
4
56
7
0
2-5
Polyp
Adenomyosis
Leiomyoma
Malignancy & Hyperplasia
Coagulopathy
Ovulatory Dysfunction
Endometrial
Iatrogenic
Not Yet Classified
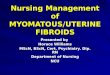
FIGO Classification System for Causes of Abnormal Uterine Bleeding in the Reproductive Years
Munro et al Int J Gynaecol Obstet. 2011;113:3-13.
5
Leiomyoma Subclassification System
S M‐ Submucous 0 Pedunculated Intracavitary
1 <50% Intramural
2 ≥ 50% Intramural
O ‐ Other 3 Contacts endometrium; 100% Intramural
4 Intramural
5 Subserous ≥50% Intramural
6 Subserous < 50% Intramural
7 Subserous Pedunculated
8 Other (specify eg. cervical, parasitic)
Hybrid
Leiomyomas (impact both
endometrium and
serosa)
Two numbers are listed separated by a dash. By convention, the first
refers to the relationship with the endometrium while the second refers to
the relationship to the serosa. One example is below
2‐5 Submucosal and subserosal, each with less
than half the diameter in the endometrial
and peritoneal cavities respectively.
00
22
33
11
44
5566
77
00
2-52-5
0
2
3
1
4
56
7
0
2-5
Polyp
Adenomyosis
Leiomyoma
Malignancy & Hyperplasia
Coagulopathy
Ovulatory Dysfunction
Endometrial
Iatrogenic
Not Otherwise Classified
Submucous
Other
00
22
33
11
44
5566
77
00
2-52-5
0
2
3
1
4
56
7
0
2-5
Leiomyoma Subclassification System
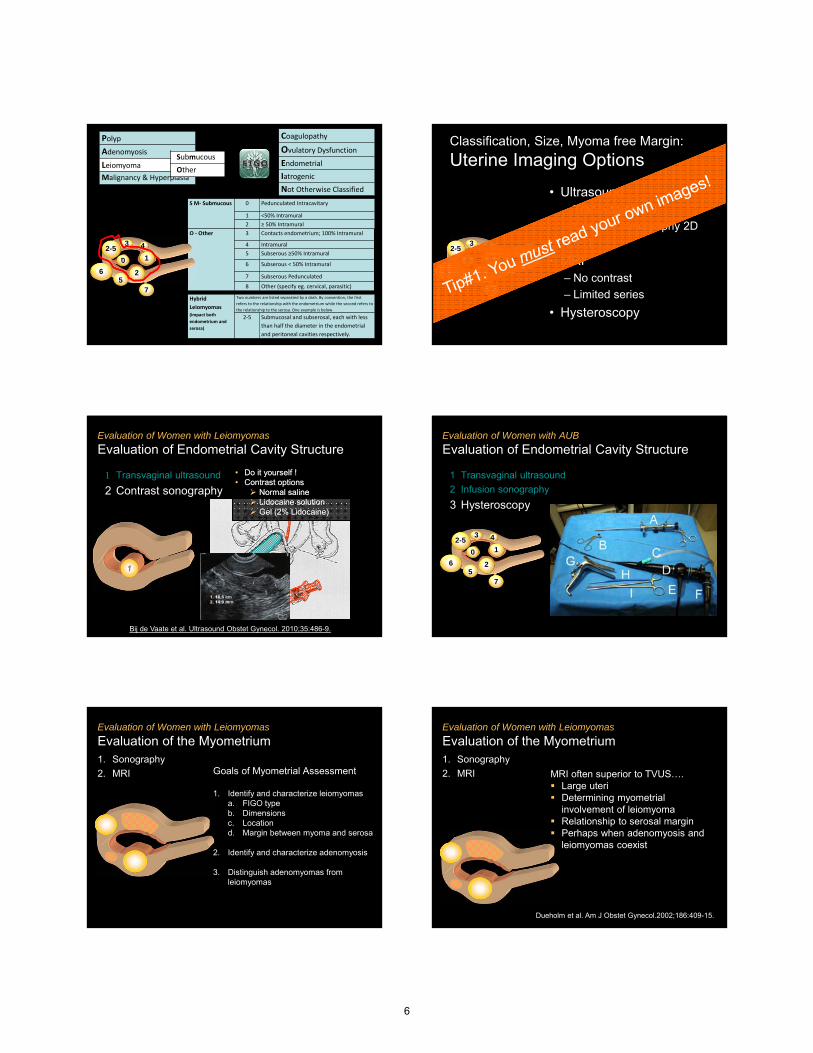
Classification, Size, Myoma free Margin:
Uterine Imaging Options
• Ultrasound– Transvaginal 2D
– Contrast sonography 2D
– 3-D
• MRI– No contrast
– Limited series
• Hysteroscopy
1 Transvaginal ultrasound
2 Contrast sonography
Evaluation of Women with Leiomyomas
Evaluation of Endometrial Cavity Structure
• Do it yourself !• Contrast options
Normal saline Lidocaine solution Gel (2% Lidocaine)
• Do it yourself !• Contrast options
Normal saline Lidocaine solution Gel (2% Lidocaine)
Bij de Vaate et al. Ultrasound Obstet Gynecol. 2010;35:486-9.
Evaluation of Women with AUB
Evaluation of Endometrial Cavity Structure
1 Transvaginal ultrasound
2 Infusion sonography
3 Hysteroscopy
00
22
33
11
44
5566
77
00
2-52-5
0
2
3
1
4
56
7
0
2-5
Evaluation of Women with Leiomyomas
Evaluation of the Myometrium1. Sonography
2. MRI Goals of Myometrial Assessment
1. Identify and characterize leiomyomasa. FIGO typeb. Dimensionsc. Locationd. Margin between myoma and serosa
2. Identify and characterize adenomyosis
3. Distinguish adenomyomas from leiomyomas
Evaluation of Women with Leiomyomas
Evaluation of the Myometrium1. Sonography
2. MRI MRI often superior to TVUS…. Large uteri Determining myometrial
involvement of leiomyoma Relationship to serosal margin Perhaps when adenomyosis and
leiomyomas coexist
Dueholm et al. Am J Obstet Gynecol.2002;186:409-15.
6

00
22
11000
2
10
Submucous Myomectomy: Issues to Consider
FIGO Myoma
Type
Diameter/Volume
Location NumberMyoma
Free Margin
0 − − −
1 −
2
Myoma Free Margin
Leiomyoma Subclassification System
Classification, Size, Myoma free Margin:
Myomectomy Route
22
00
22
33
11
44
5566
77
00
2-52-5
0
2
3
1
4
56
7
0
2-5
Superficial Type 2Superficial Type 2 Deep Type 2Deep Type 2 Type 2-5Type 2-5
Hysteroscopic/Resectoscopic
Hysteroscopic/Resectoscopic
Hysteroscopic/Resectoscopic or
Laparoscopic/Laparotomic
Hysteroscopic/Resectoscopic or
Laparoscopic/Laparotomic
Laparoscopic or Laparotomic
Laparoscopic or Laparotomic
Leiomyoma Subclassification System
00
22
110002
10
Classification, Size, Myoma free Margin:
Uterine Imaging
11
• Leiomyoma manifestations
• The spectrum of surgical options
• Identification of patient goals
• Evaluation
• Creating the menu of options
Conserving the Uterus:Options, Evaluation & Patient Selection
Agenda
Manifestation
• AUB
• Bulk symptoms
• Infertility
• Recurrent Pregnancy Loss
• Other
Goal(s)
• Symptom control
• Fertility– Preserve or enhance
– No desire for future fertility
• Cosmetic result
• Minimizing economic impact of intervention
Conserving the Uterus: Options, Evaluation & Patient Selection-Counseling Considering Patient Goals
00
22
33
11
44
5566
77
00
2-52-5
0
2
3
1
4
56
7
0
2-5
0011
55
000 1
5
0
11
442-52-5
1
42-5
2-52-5
33 44
66
2-62-6
2-5
3 4
6
2-6
2244
66
24
6
Submucous LeiomyomasInfertility, RPL or wishes to retain fertility
Resectoscopicc
Laparoscopic OR LaparotomiccLaparoscopic OR Laparotomic
AND Resectoscopicc
Laparoscopic OR Resectoscopicc
Myomectomy
7

0011
55
000 1
5
0
11
44
66
2-52-5
1
4
6
2-5
2-52-5
33 44
66
2-62-6
2-5
3 4
6
2-6
2244
66
24
6
Submucous LeiomyomasDoes not wish to retain fertility
Resectoscopicc
Laparoscopic OR LaparotomiccLaparoscopic OR Laparotomic
AND Resectoscopicc
Laparoscopic OR Resectoscopicc
Endometrial Ablation ± Myoma ResectionEndometrial Ablation ± Myoma Resection
…provided endometrial cavity within limitsHachman – Nielsen et al. J. Min Invasive Gynecol 2012;19:212-6Loffer FD. J. Min Invasive Gynecol 2012;12:254-60
Multiple and/or Large LeiomyomasInfertility, RPL or wishes to retain fertility
2-52-5
33 44
55
2-52-5
2-5
3 4
5
2-5
4
6 • Myomectomy• Laparotomic• Laparoscopic?
• UAE?
• Myomectomy• Laparotomic• Laparoscopic?
• UAE?
Multiple and/or Large LeiomyomasDoes NOT wish to retain fertility
2-52-5
33 44
55
2-52-5
2-5
3 4
5
2-5
4
6 • Myomectomy• Laparotomic• Laparoscopic?
• UAE• RF Laparoscopic
Leiomyoma Ablation
• Hysterectomy
• Myomectomy• Laparotomic• Laparoscopic?
• UAE• RF Laparoscopic
Leiomyoma Ablation
• Hysterectomy
• Gupta JK, et al. Uterine artery embolization for symptomatic uterine fibroids. CochraneDatabase of Systematic Reviews 2012, Issue 5.
• Berman et al. J Minim Invasive Gynecol. 2014;21:767-74
Berman et al. J Minim Invasive Gynecol. 2014;21:767-74.
Hachman – Nielsen et al. J. Min Invasive Gynecol 2012;19:212-6
Loffer FD. J. Min Invasive Gynecol 2012;12:254-60
Dueholm et al. Am J Obstet Gynecol.2002;186:409-15.
Munro et al Int J Gynaecol Obstet. 2011;113:3-13.
Bij de Vaate et al. Ultrasound Obstet Gynecol. 2010;35:486-9.
Gupta JK, et al. Uterine artery embolization for symptomatic uterine fibroids. CochraneDatabase of Systematic Reviews 2012, Issue 5.
References
Malcolm G. Munro MD, FRCS(c), FACOGProfessor, Department of Obstetrics & Gynecology
David Geffen School of Medicine at UCLADirector of Gynecologic Services
Kaiser Permanente, Los Angeles Medical CenterLos Angeles, CA, USA
8

Hysteroscopic Management – The Most Minimally Invasive
Keith Isaacson MD
Associate Professor OB/GYN
Harvard Medical School
Boston, MA
Disclosures
• I have no financial relationships to disclose
Objective
Discuss Hysteroscopic Management – The Most Minimally Invasive
Hysteroscopic Energy
• Laser
• Radiofrequency– Monopolar
– Bipolar
• Morcellation
• Morcellation with bipolar energy
1970 – 1995Monopolar Hysteroscopy
Electrosurgery =Secondary Thermodynamic Change
Na+ Cl-
Na+
Na+ Cl-Cl-
9

Non-conductive media Ω = ∞
TissueTissue Impedance = 100
Conventional Monopolar Electrosurgeryrequires non-conductive media and adequate current density
Current flows through
the tissue
concentrated
• 3% Sorbitol
• 1.5% Glycine
• 5% Mannitol
• 3% Sorbitol
• 1.5% Glycine
• 5% Mannitol
Non-Electrolyte, Non-Conductive Solutions for Monopolar Resectoscopic Surgery
Non-Electrolyte, Non-Conductive Solutions for Monopolar Resectoscopic Surgery
Changes in amino acids, ammonium, and coagulation factors after transcervical resection of the endometrium with a glycine solution used for uterine irrigation.Istre O, Jellum E, Skajaa K, Forman A.Am J Obstet Gynecol. 1995 Mar;172
Potential Risks of Monopolar Electrosurgery
• Direct Coupling
• Capacitive Coupling
• Insulation Failure
• Surgical Fires
• Alternate Site Burn (Injury)
• Grounding / Return Pad Failure
Saline Impedance = 25
TissueTissue Impedance = 100
Conventional Monopolar Electrosurgery- In Normal Saline -
Current flows through saline
following path of least resistance to return electrode
10

Current HysteroscopicBipolar Technology
Myoma Resection With VERSAPOINT ElectrodeMyoma Resection With VERSAPOINT Electrode
VideoTo view, click on picture with left mouse button.
Bipolar resection type II
Monitoring Venous Air Embolism
• Doppler, TE echo 0.1 - 0.25
• End title CO2 or 025-0.5
• Nitrogen tension
• CVP and Pulmonary 05-0.75artery P increase
• Mean Art P decrease 0.75 - 1.25
• Ventricular dysrhythmias 1.25
• Mill-wheel murmur 1.5
• Cardiovascular collapse 2.0
Sensitivity
mL/Kg/min air entrapment Hysteroscopic Mechanical
Morcellation
11

The TRUCLEAR ™ 5.0 System* offers many benefits
19
205mm working length provides access to entire uterus
J-snap locking mechanism for one handed control of sheath
Patented dual outflow allows clear visualization
2.9 mm close cutting edge resects pathology down to base
Distal marking ideal for blade orientation
Proximal marking indicates blade has reached distal end of scope
5.0 Scope and 5.6 Sheath allows procedure with limited to no dilation
Inflow from Fluid Mgmt.Systemor Pressurized Saline Bag
Gravity Outflow
3.1mm diameter working channel allows 9 Frinstruments
* Pending FDA clearance
MyoSure® Tissue Removal System
FDA Clearance October-2009; Commercial Launch- November 2009
Pathology Removal with MyoSure®
Tissue Removal System is Fast and Effective
Historical perspective
1869
Pantaleoni credited with 1st
hysteroscopic procedure in uterine
cavity
Rubin utilized C02 to distend the uterine
cavity
1925
Source(s): Valle, R, Glob. libr. women's med., (ISSN: 1756-2228) 2008; DOI 10.3843/GLOWM.10087Cohen, S. et. al., Hysteroscopic Morcellation for Treating Intrauterine Pathology, Obstet Gynecol. 2011 Summer; 4(2): 73-80
Von Mikulicz-Radecki & Freund introduced electro-
coagulation of intramural portion of
tubes
1927
Silander introduced a hysteroscope with a latex balloon for
distention
1962
Edstrom & Fernstrom used
dextran for distention
1970
Distention & Visualization Visualization & Intervention
Neuwirth & Amin first resectoscope
hysteroscpic resection of
submucous myoma
1976
Smith & Nephew’s Truclear™ System
Introduced(mechanical cutting)
2005
Hologic’s MyoSure™ System
Introduced(mechanical cutting)
2009
Boston Scientific’s Symphion™ System
Introduced(closed-loop, RF bipolar resection)
2014
Monopolar and Bipolar resection
RF Bi-Polar Resection Process
• Tissue hydraulically drawninto resecting window
• Reciprocating RF electrode delivers bipolar plasma
• Minimal collateral effect
• Bipolar current switches to internal path
• Vaporized tissue & fluid trapped in the tip of the device
Phase I
• Vaporized tissue & fluid help to remove resected fragments
• Cleans electrodes surface to eliminate tissue sticking to electrode surface
Phase II Phase III
Hysteroscopic Morcellation Patient Selection
12

Follow-up after incomplete hysteroscopicremoval of uterine fibroids
Van Dongen H, Emanuel MH, Smeets J, Trimbos, B and Jansen FW
• 528 Hysteroscopic myomectomies• 91 Incomplete resections (17%)
• 37 repeated immediately for fertility• 41 observed for menorrhagia
Incomplete myomaresection
55% required additional surgery within 3 years
13

Abdominal Management – Laparoscopic Management Techniques
Charles E. Miller, MD, FACOG
Past President, AAGL (2007 – 2008)
Past President, International Society for Gynecologic Endoscopy – ISGE (2011 – 2013)
Treasurer, International Society for Gynecologic Endoscopy (ISGE)
Clinical Associate Professor, Department OB/GYN, University of IL at Chicago, Chicago, IL USA
Director of Minimally Invasive Gynecologic Surgery, Advocate Lutheran General Hospital, Park Ridge, IL USA
Director, AAGL/SRS Fellowship in Minimally Invasive Gynecologic Surgery, Advocate LutheranGeneral Hospital, Park Ridge, IL USA
Contracted/Research:AbbVie, Actavis, Aegea Medical, Bayer Healthcare Corp., Covidien, Gynesonics, IntuitiveSurgical
Consultant: AbbVie, Covidien, Ethicon Endo--‐Surgery, Gynesonics, Halt Medical, IntuitiveSurgical, Pacira Pharrmaceuticals
Speakers Bureau: Ethicon Endo--‐Surgery, intuitive Surgical, Smith & Nephew Endoscopy
Royalty: Thomas Medical
Abdominal Management – Laparoscopic Management Techniques
At the end of this discussion, the physician will be able to:
1. List two different energy sources for fibroid enucleation.
2. List two advantages of barbed vs. monofilament suture.
3. Explain how morcellation in a bag minimizes the risk of tissue spread at time of myomectomy.
• Parker, WH, 2010. Risk factors for uterine rupture after laparoscopic myomectomy. J Minim Invasive Gynecol, Sep-Oct;17(5), 551-4.
• Pelosi, MA, 1997. Spontaneous uterine rupture at thirty-three weeks subsequent to previous superficial laparoscopic myomectomy. Am J Obstet Gynecol, Dec;177(6), 1547-9.
• Dubuisson, JB, 1995. Uterine rupture during pregnancy after laparoscopic myomectomy. Hum Reprod, Jun;10(6), 1475-7
Abdominal Management – Laparoscopic Management Techniques
Strategies in the Laparoscopic Management of the Large Myomatous Uterus
Surgery Preparation
• Cycle timing – early follicular phase– Day# 6-12
• OCP’s– Anytime
• GNRH agonists– Anytime
– Fibroid degeneration can cause loss of myoma planes
– Try to avoid unless severely anemic
Abdominal Management – Laparoscopic Management Techniques
Strategies in the Laparoscopic Management of the Large Myomatous Uterus
Surgery Preparation
• General endotracheal anesthesia
• Place Foley catheter
• Perform hysteroscopy to identify and treat submucosal fibroids, polyps, intrauterine adhesions
• Place uterine manipulator that enables anterior-posterior and lateral mobility— Valchev
— Pelosi
— Rumi
— Jarcho
— V-Care
— Fornisee
14

Abdominal Management – Laparoscopic Management Techniques
Strategies in the Laparoscopic Management of the Large Myomatous Uterus
Port Placement
10-12mm trocar at umbilicus
— Even if uterine mass is 18+ weeks’ size, generally the umbilicus is the easiest option for insufflation
— Alternatively, consider left upper quadrant access
Place secondary ports lateral and cephalad to uterus/fibroid(s)
— 5-mm lateral ports are advantageous
Cosmetic
Fascia closure not required
Less risk of post-op hernia
Requires morcellation through umbilicus with lateral 5-mm port camera
Abdominal Management – Laparoscopic Management Techniques
Strategies in the Laparoscopic Management of the Large Myomatous Uterus
Large Uterus Port Placement
Abdominal Management – Laparoscopic Management Techniques
Myomectomy (laparoscopic and robotic assisted)
Enucleation
Dilute Vasopressin— 30 units diluted in 100cc normal saline
— Half-life = 10-20 minutes
— 18G spinal needle with controlled syringe Inject into myometrium near fibroid aiming for myoma capsule
• Multiple areas
• “Connect the dots”
Aspirate to avoid injection intravascularly• Notify anesthesia
— Elevates blood pressure
— Loss of pulse oximetry reading
Abdominal Management – Laparoscopic Management Techniques
Myomectomy (laparoscopic and robotic assisted)
Enucleation Instrumentation
Energy options for myomectomy— Monopolar hook or scissors
— Ultrasonic scalpel Maximize cut to minimize tissue desiccation
• Risk of uterine rupture during pregnancy
Instrumentation— Toothed instruments
Single-toothed spoon
Claw
Myoma screw
— Traction/countertraction
• Parker, WH, 2010. Risk factors for uterine rupture after laparoscopic myomectomy. J Minim Invasive Gynecol, Sep-Oct;17(5), 551-4.• Pelosi, MA, 1997. Spontaneous uterine rupture at thirty-three weeks subsequent to previous superficial laparoscopic myomectomy. Am
J Obstet Gynecol, Dec;177(6), 1547-9.• Dubuisson, JB, 1995. Uterine rupture during pregnancy after laparoscopic myomectomy. Hum Reprod, Jun;10(6), 1475-7.
Abdominal Management – Laparoscopic Management Techniques
Myomectomy (laparoscopic and robotic assisted)
Enucleation
Abdominal Management – Laparoscopic Management Techniques
Myomectomy (laparoscopic and robotic assisted)
Tissue Reapproximation
Suture type— Absorbable
— Taper needle
Multi-layer closure— Hemostasis
Avoid use of energy to reduce tissue destruction
— Eliminate “dead” space
— Reduce risk of uterine rupture during pregnancy
• Parker, WH, 2010. Risk factors for uterine rupture after laparoscopic myomectomy. J Minim Invasive Gynecol, Sep-Oct;17(5), 551-4.• Pelosi, MA, 1997. Spontaneous uterine rupture at thirty-three weeks subsequent to previous superficial laparoscopic myomectomy. Am
J Obstet Gynecol, Dec;177(6), 1547-9.• Dubuisson, JB, 1995. Uterine rupture during pregnancy after laparoscopic myomectomy. Hum Reprod, Jun;10(6), 1475-7.
15

Abdominal Management – Laparoscopic Management Techniques
Myomectomy (laparoscopic and robotic assisted)
Barbed Suture
Stratafix™, Quill™, and V-Loc™ wound closure device
— The barbs grasp tissue at numerous points providing distribution of tension across the wound
— Eliminates the need for tying knots
Abdominal Management – Laparoscopic Management Techniques
Traditional Laparoscopic Myomectomy With Covidien V-Loc™ Advanced Wound Closure Device
Abdominal Management – Laparoscopic Management Techniques
Myomectomy (laparoscopic and robotic assisted)
Adhesion Prevention
Minimize energy
Avoid multiple surgical incisions
Serosal closure – minimize suture exposure
Adhesion barriers
Abdominal Management – Laparoscopic Management Techniques
Electromechanical Power Morcellation in a Bag
Abdominal Management – Laparoscopic Management Techniques
GelPOINT Power Morcellation in a Bag
16

Abdominal Management – The Very Large Uterus
Olav Istre, MD. PhDProfessor in MIGS
Aleris private HospitalAnd
University of Southern Denmark
• I have no financial relationships to disclose
To compare surgical approach and technique
• Discuss minimal invasive gynecological tecniques
• Describe pathology that interferes with function
• Improve the quality of life
Complication between abdominal or laparoscopic aproach
• Net difference in the incidences for complications – Adhesions +50.1% (midline double the incidence)
– hernia +10.7%
– surgical site infection +4.8%
– small bowel obstruction +2.8%
– venous thromboembolism +2%
• Audebert AJ, Gomel V. Role of microlaparoscopy in the diagnosis of peritoneal and
• visceral adhesions and in the prevention of bowel injury associated with blind trocar
• insertion. Fertil Steril 2000 Mar;73(3):631‐5.
• Dubuisson J, Botchorishvili R, Perrette S, Bourdel N, Jardon K, Rabischong B, et al.
• Incidence of intraabdominal adhesions in a continuous series of 1000 laparoscopic
• procedures. Am J Obstet Gynecol 2010 Aug;203(2):111 e1‐3.
• Le Huu Nho R, Mege D, Ouaissi M, Sielezneff I, Sastre B. Incidence and prevention of
• ventral incisional hernia. J Visc Surg 2012 Oct;149(5 Suppl):e3‐14.
• Nieboer TE, Johnson N, Lethaby A, Tavender E, Curr E, Garry R, et al. Surgical
• approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev
• 2009(3):CD003677.
• Angenete E, Jacobsson A, Gellerstedt M, Haglind E. Effect of laparoscopy on the risk of
• small‐bowel obstruction: a population‐based register study. Arch. of surg. 2012
Limitation of surgical aproach
• The goal is laparoscopic aproach
• Dependent on
– Number of fibroids
– Size of fibroid
– Previous surgery
– Patients wish
17

Open surgery with midline Incision, 1998
Open myomectomy
Multiple (57) Large fiboids >1200 g
Phannenstiel (morcelation with knife in bag, )
Sarcoma issue
• 41 patients leiomyosarcomas morcellated• Prognosis was significantly worse in these patients • 1 of these 41 patients had laparoscopic morcellation.• The other 40 patients had the specimen morcellated using a
cold knife through a minilaparotomy (n=17), transvaginally(n=19), or hysteroscopically (n=4)."
• Park JY, Park SK, Kim DY, et al. The impact of tumor morcellation during surgery on the prognosis of patients with apparently early uterine leiomyosarcoma. Gynecol Oncol. 2011 Aug;122(2):255–259.
• Perri T, Korach J, Sadetzki S, Oberman B, Fridman E, Ben‐Baruch G. Uterine leiomyosarcoma: does the primary surgical procedure matter? Int J Gynecol Cancer. 2009 Feb;19(2):257–260.
The fibroid/Sarcoma debate
• 42 year old women
• Prevoius 5 IVF
• Missed abortion with D&C March 2015
• Ca 125 =280, CEA =1
• Abdominal tumor 11 cm
Fibroid / sarcoma issue
• CT scan suspicion of sarcom
• PET scan = PET positiv (FDG uploading in the periferi of the tumor) with central necrosis
• FDG (deoxyglycose) is obtained in cells with increased metabolisme
18

Fibroid / sarcoma issue
• Rapid Growth
• Recommendation from Gynecology Oncology clinic and sarcoma group ( 12 doctors)
• Recomondation:
• Midline incision, Removal of tumor including Hysterectomy
Fibroid / Sarcoma issue
• She has seen at 3 different University Hospitals
• She wants second opinion
• She wants to be sure
• She wants to keep the uterus
Fibroids natural history
• Composed of smooth muscle and varying amount of fibrous connective tissue
• As leiomyomas enlarge, they may outgrow their blood supply resulting in various types of degeneration: 2/3 shows degeneration
– Hyaline or myxoid degeneration (75%)
– Calcification (10%)
– Cystic degeneration(10%)
– Fatty degeneration
Red degenation
Ueda, Radiographics. 1999 Oct;19 Spec No:S131‐45
19

HISTOLOGY
• Histology:
• Examination number: 15SH1154‐1
• 1. Myometrium
• ‐leiomyoma ‐
• ‐necrosis ‐
• ‐bleeding
20

CULTURAL AND LINGUISTIC COMPETENCY Governor Arnold Schwarzenegger signed into law AB 1195 (eff. 7/1/06) requiring local CME providers, such as
the AAGL, to assist in enhancing the cultural and linguistic competency of California’s physicians
(researchers and doctors without patient contact are exempt). This mandate follows the federal Civil Rights Act of 1964, Executive Order 13166 (2000) and the Dymally-Alatorre Bilingual Services Act (1973), all of which
recognize, as confirmed by the US Census Bureau, that substantial numbers of patients possess limited English proficiency (LEP).
California Business & Professions Code §2190.1(c)(3) requires a review and explanation of the laws
identified above so as to fulfill AAGL’s obligations pursuant to California law. Additional guidance is provided by the Institute for Medical Quality at http://www.imq.org
Title VI of the Civil Rights Act of 1964 prohibits recipients of federal financial assistance from
discriminating against or otherwise excluding individuals on the basis of race, color, or national origin in any of their activities. In 1974, the US Supreme Court recognized LEP individuals as potential victims of national
origin discrimination. In all situations, federal agencies are required to assess the number or proportion of LEP individuals in the eligible service population, the frequency with which they come into contact with the
program, the importance of the services, and the resources available to the recipient, including the mix of oral
and written language services. Additional details may be found in the Department of Justice Policy Guidance Document: Enforcement of Title VI of the Civil Rights Act of 1964 http://www.usdoj.gov/crt/cor/pubs.htm.
Executive Order 13166,”Improving Access to Services for Persons with Limited English
Proficiency”, signed by the President on August 11, 2000 http://www.usdoj.gov/crt/cor/13166.htm was the genesis of the Guidance Document mentioned above. The Executive Order requires all federal agencies,
including those which provide federal financial assistance, to examine the services they provide, identify any
need for services to LEP individuals, and develop and implement a system to provide those services so LEP persons can have meaningful access.
Dymally-Alatorre Bilingual Services Act (California Government Code §7290 et seq.) requires every
California state agency which either provides information to, or has contact with, the public to provide bilingual
interpreters as well as translated materials explaining those services whenever the local agency serves LEP members of a group whose numbers exceed 5% of the general population.
~
If you add staff to assist with LEP patients, confirm their translation skills, not just their language skills.
A 2007 Northern California study from Sutter Health confirmed that being bilingual does not guarantee competence as a medical interpreter. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2078538.
US Population
Language Spoken at Home
English
Spanish
AsianOther
Indo-Euro
California
Language Spoken at Home
Spanish
English
OtherAsian
Indo-Euro
19.7% of the US Population speaks a language other than English at home In California, this number is 42.5%
21