Embed Size (px)
Citation preview

Surgical Treatment of Thyroid-related Upper Eyelid Retraction
Graded Muller's Muscle Excision and Levator Recession
ALLEN M. PUTTERMAN, MD
Abstract: A graded, controlled excision of MUlier's muscle with or without recession of the levator aponeurosis using sensory without motor anesthesia is an excellent technique for releasing thyroid-related upper eyelid retraction. The procedure has provided statistically significant success rates in the first 53 upper eyelids treated by this technique that were carefully analyzed postoperatively. It has continued to provide consistently good results in an additional 49 upper eyelids. The six complications in the first 53 cases included nasal ptosis (4), diffuse ptosis (1), and residual eyelid retraction (1). These were easily rectified with a second simple surgical procedure. The operation described is considered superior to other techniques in treating thyroid-related upper eyelid retraction because other procedures have not been analyzed in large enough numbers to demonstrate as high a degree of success as this operation. The procedure is simple, based on anatomic and physiologic principles, tailored to the individual patient intraoperatively, and yields consistently good results. [Key words: levator recession, MUlier's muscle, retraction, thyroid.] Ophthalmology 88:507 -512, 1981
Eyelid retraction, a manifestation of thyroid ophthalmopathy, often continues after the underlying systemic disease has been successfully treated. Upper lid retraction is not only cosmetically deforming because the amount of exophthalmos is exaggerated, but
it also contributes to corneal and conjunctival exposure.!
From the University of Illinois Hospital Eye and Ear Infirmary, Department of Ophthalmology, Chicago.
Presented at the Eighty-Fifth Annual Meeting of the American Academy of Ophthalmology, Chicago, November 2 - 7, 1980.
Supported in part by grant EY 1792 from the National Institutes of Health, Bethesda.
Reprint requests to Allen M. Putterman, MD, 111 North Wabash, Chicago, IL 60602.
0161-6420/8110600/0507/$00.80 © American Academy of Ophthalmology
Upper lid retraction is generally thought to be caused by increased innervation of the sympathetically innervated Muller's muscle. 2,3 Activity of the levator palpebrae superioris muscle is also increased in association with the increased tone ofthe superior rectus muscle to compensate for a contracted inferior rectus muscle. 2- 4
Many surgical methods have been proposed to treat upper eyelid retraction. Blaskovic5 severed the levator and, presumably Muller's muscle, from the superior tarsal border and retracted them with sutures. Goldstein6 recessed the levator aponeurosis and Muller's muscle with either a skin or conjunctival approach.
507

OPHTHALMOLOGY. JUNE 1981 • VOLUME 88 • NUMBER 6
Moran 7 made a horizontal incision via a skin approach through the levator aponeurosis and MOller's muscle just above the tarsus, and had the patient open and close the eyelids during the procedure to determine the length of the incision. Henderson l made a conjunctival- MOller's muscle incision along the entire superior tarsal border and then excised the levator aponeurosis for different lengths, depending on the severity of retraction. Baylis et alB recessed the levator aponeurosis and MOller's muscle twice the distance of the measured retraction and sutured them to conjunctiva. Dryden and So1l9 placed donor sclera in the upper eyelid to relieve the retraction.
In 1972, Urist and 14 described a procedure for excising MOller's muscle with or without recessiori ofthe levator aponeurosis. The patient is awake during the procedure and is brought to the sitting position at various times either to match the level of the affected lid to the unaffected lid in unilateral cases or to achieve a functionally and cosmetically acceptable level in bilateral cases. In 1979, Chalfin and po reported results of the first 53 consecutive upper eyelids that were treated by this procedure. The cosmetic results were excellent in 47, four months to six years postoperatively. Six had minor complications that were rectified with additional surgery. The latter report stressed the use of subcutaneous and subconjunctival local anesthesia rather than frontal nerve block advocated originally. Also stressed were the dissection of MOller's muscle and levator aponeurosis only over the temporal two thirds of the lid during the initial steps of the procedure to avoid a postoperative nasal ptosis. Since then, another 49 upper lids have been treated by this technique with equally good results. The follow-up period of this group ranged from two months to three years. Only one of the patients required additional surgery for residual retraction.
ANATOMY
The levator muscle divides into two parts about 10 to 12 mm above the superior edge of the tarsus. ll
,l2
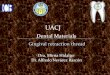
The anterior part is the levator aponeurosis, which inserts onto the lower one third of the anterior tarsus along its entire width (Fig 1). The posterior part is a smooth muscle, called MOller's muscle, which inserts onto the superior edge of the tarsus along its entire width. The levator aponeurosis and MOller's muscle are only loosely attached for their entire lengths. The posterior surface of MOller's muscle is covered by tightly adherent conjunctiva.
SURGICAL PROCEDURE
Only local anesthesia is used in this procedure. Measurements ofthe eyelid levels and excursion ofthe upper lid taken before and after injection of the anesthetic demonstrate no change in the measure-
508
Leva tor muscle
Levator -aponeurosis
'Tarsal plate
Fig 1. Cross section of a normal upper eyelid.
ments after injection. The patient's preoperative regimen consists of 12.5 mg promethazine hydrochloride, administered orally one hour before surgery, and 50 mg intramuscular meperidine hydrochloride, administered in the operating room. This regimen is chosen because it does not affect the eyelid levels at the time of surgery.
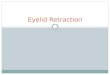
Lidocaine hydrochloride (0.25 ml of 2%) with epinephrine is injected subcutaneously into the center of the upper eyelid just above the eyelid margin (Fig 2A). A 4-0 silk suture is placed in the center of the upper lid 2 mm above the lash line, through skin, orbicularis muscle, and anterior tarsus. A Desmarres retractor everts the upper lid to expose the superior palpebral conjunctiva.
A scleral lens is placed over the globe to protect it during surgery. The upper palpebral conjunctiva is flooded with 0.5% tetracaine hydrochloride drops. Cotton-tipped applicators saturated with tetracaine are also spread over the conjunctiva. Then, 0.25 to 0.5 ml of 2% lidocaine hydrochloride with epinephrine is injected subconjunctivally adjacent to the superior tarsal border over the entire width of the eyelid (Fig. 2B).
The conjunctiva is grasped just over the superior tarsal border at the temporal aspect of the eyelid and severed with Westcott scissors. The surgeon inserts straight, sharp-pointed iris scissors into the plane between the conjunctiva and MOller's muscle, and cuts the conjunctiva from the superior tarsal border (Fig 2C). The conjunctiva is dissected from the muscle by spreading the scissors blades from the superior tarsal border to the superior fornix (Fig 2D). This dissection is facilitated by observing the points of the blades through translucent conjunctiva. Sharp dissection with the iris scissors releases any remaining attachments between conjunctiva and MOller's muscle.
The surgeon grasps MOller's muscle with toothed

PUTIERMAN • EYELID RETRACTION
Fig 2A-D. Muller's muscle excision and levator muscle recession. A. Subcutaneous administration of anesthetic for retraction suture. B. Subconjunctival administration of anesthetic. C. Conjunctival incision along temporal two thirds of superior tarsal border. D. Dissection of conjunctiva from Muller's muscle.
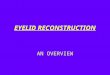
forceps at the temporal aspect of the eyelid just above the superior tarsal border. The muscle is pulled outward, and the Desmarres retractor is pulled simultaneously in the opposite direction. Muller's muscle is cut from the tarsus temporally. The muscle is then undermined from the levator aponeurosis at the level of the superior tarsal border, and all the tissue attached to the top of the tarsus (Muller's muscle anatomically) is severed over the temporal two thirds of the eyelid (Fig 2E). Wet cotton-tipped applicators are used to dissect Muller's muscle bluntly from its loose attachment in the levator aponeurosis for 10 to 12 mm above the superior tarsal border over the temporal two thirds of the eyelid (Fig 2F). The scleral lens is removed from the eye, and the patient is brought to a sitting position by raising the back of the operating table to evaluate the level of the upper eyelid in the primary and up and down positions of gaze, and when the eyelids are opened wide.
If the upper eyelid is at a satisfactory position, the patient lies down, and the section of Muller's muscle that has been detached is clamped with a straight hemostat at its base and excised. If there is still retraction nasally, the nasal one third of Muller's muscle is released. (It is better to be conservative in releasing Muller's muscle nasally, for a nasal ptosis can occur easily.)
If the lid is still retracted, overaction of the levator muscle is implicated, and this muscle must be released. The patient lies down, and the scleral lens and Desmarres retractor are reapplied. With the lid
everted, the fibers of the levator aponeurosis that pass over the anterior surface of the tarsus are exposed. Using two toothed forceps, the surgeon grasps the superficial layers of the levator aponeurosis at the level of the superior tarsus, and they are stripped vertically, layer by layer, along the part of the eyelid that remains retracted (Fig 2G). The patient is brought to a sitting position at various times during the levator stripping procedure until a desirable end point is reached. The gradual, step-by-step lengthening of the aponeurosis allows the f!!traction of the eyelid to be corrected slowly. The detached part of Muller's muscle is then excised as described (Fig 2H).
When a desired eyelid level is achieved, either by excision of Muller's muscle alone or in conjunction with the stripping of the levator aponeurosis, the conjunctiva is sutured to the superior tarsal border with a continuous 6-0 plain catgut suture (Fig 21). The silk traction suture placed in the upper eyelid at the beginning of the procedure is taped to the patient's cheek to put a small amount of stretch on the upper eyelid, and a light pressure dressing is applied to the eye. If the lower and upper eyelids are operated on at the same time, a 4-0 silk double-armed suture, placed in the center of the lower eyelid tarsus, enters from the conjunctival side and exits through the skin of the lower eyelid. Each arm of the suture is passed through the central portion of the upper eyelid tarsus from its conjunctival side and exits through the upper eyelid skin. When the suture is tied, the lower lid is elevated simultaneously as the upper eyelid is lowered.
509

OPHTHALMOLOGY. JUNE 1981 • VOLUME 88 • NUMBER 6
H Mul .... '.m.
On the first postoperative day, the traction suture is untaped from the cheek and taped above the eyebrow. The upper lid level is then evaluated as the patient gazes in the primary position. If the upper eyelid is below the mid pupil, the traction suture is released. If the upper eyelid is moderately above the pupil, the traction suture can be taped down to the cheek for several more days. It is expected that the lid will be ptotic initially postoperatively and will gradually raise during the next three to four weeks. If the lid begins to retract, the patient is instructed to massage the lid downward while raising the eyebrow upward. If the lid remains ptotic, elevation can be increased by patching the normal unoperated eyelids. This forces the patient to raise the brow on the treated side and apparently brings the recessed tissues into closer approximation during healing.
COMMENT
In the first 53 upper eyelids (32 patients) operated on for thyroid-related upper eyelid retraction by excision
510
Fig 2E-1. E . Disinsertion of Miiller's muscle from temporal two thirds of superior tarsal border. F. Dissection of Miiller's muscle from levator aponeurosis. O. Stripping levator aponeurosis. H. Excising Miiller' s muscle, also showing recessed levator aponeurosis. 1. Suturing conjunctiva to superior tarsal border.
of Muller's muscle with or without recession of the levator aponeurosis, all had less retraction postoperatively.lo Furthermore, cosmetic symmetry of the upper eyelids was obtained in 26 of the patients by this procedure alone. Four patients required surgical treatment for nasal ptosis in one upper eyelid by a nasal segmental internal vertical shortening operation. 13 One patient had a diffuse ptosis that was also successfully treated with the internal vertical eyelid shortening procedure, in which the clamp was applied to the entire lid rather than just to the nasal segment. Another patient was successfully treated with the described procedure in both upper lids, but retraction in her right upper eyelid subsequently developed and required a simplified levator recession procedure to obtain a lasting good result. 14 (It was not possible to be sure, whether this represented an undercorrection or progression of the underlying disease process, because of the time interval between surgery and the development of the retraction.)
The excision of Muller's muscle and levator recession in the manner described is the procedure of choice for treating thyroid-related retraction of the upper

PUTTERMAN • EYELID RETRACTION
Fig 3A. Preoperative photograph of patient with bilateral upper eyelid retraction.
Fig 38. Postoperative photograph of same patient three years after excision of Miiller's muscle and levator recession.
Fig 4A. Preoperative photograph of patient with bilateral upper eyelid retraction.
Fig 48. Postoperative photograph of same patient eight months after excision of Miiller's muscle and levator recession.
511

OPHTHALMOLOGY • JUNE 1981 • VOLUME 88 • NUMBER 6
eyelid. (Figs 3 and 4). The procedure is based on the theories of the physiologic and anatomic origin of the condition. It is a relatively simple procedure that does not alter the major anatomic relationships in the eyelid by the implantation of foreign material or by distortion of the tissues. With the patient sitting up at various times during the procedure, the technique can be adjusted to the individual by recessing the levator progressively until the desired level and arch are achieved. Overcorrection can be recognized during surgery and dealt with by reattaching the recessed tissues to the tarsus or skin.
It is difficult to make a statistical comparison between this approach and other procedures because of the unavailability of quantitative details in the reports of other authors.
From our experience with use of donor sclera to correct lower eyelid retraction, the lower eyelid becomes severely thickened and erythematous, and the eyelid retracts as the sclera absorbs postoperatively. For these reasons, we think that although scleral implants are both necessary and acceptable in the treatment of lower lid retraction, the results are less acceptable cosmetically in the treatment of the upper lid.
In some of the patients with bilateral involvement, the more severely retracted eyelid was operated on first, and the other upper eyelid was operated on several weeks later. It was found that the eyelid not operated on frequently appears to be more retracted after the contralateral upper lid has been surgically treated. This is true of both patients who demonstrated unilateral or bilateral upper lid retraction when their conditions were originally evaluated. Patients with true unilateral retraction often appear to have a slight ptosis of the uninvolved upper eyelid that disappears after correction of the contralateral retraction.
It is thought that the patient keeps the more retracted eyelid at the lowest possible level by decreasing the neural impulse to the levator muscle on that side . This minimizes the irritation of that eye. I believe that the levator muscle obeys Hering's law, whereby there is a decrease in the neural impulse to the uninvolved or less retracted eyelid as well. Possibly, when the tone of the neural impulse returns to normal, the upper eyelid that had appeared normal or slightly ptotic preoperatively appears slightly retracted or in a normal position. Because of these changes postoperatively, I believe that it is important, when performing surgery in a patient with unilateral retraction, to place the affected eyelid at a slightly higher level than that of
512
the unaffected eyelid to ensure symmetry postoperatively.
Similarly, patients with bilateral upper lid retraction appear to have more retraction on the side first operated on after surgery has been performed on the contralateral upper eyelid. I feel that this represents the true amount of retraction of the upper eyelid first operated on. When operating on the second upper eyelid (several weeks after the first procedure), the lid must be placed at the same level to which the other upper lid was placed at the time of surgery. If an attempt is made to match the eyelids so that they are symmetric during the second procedure, the second eyelid will invariably be ptotic.
REFERENCES
1. Henderson JW. Relief of eyelid retraction : a surgical approach. Arch Ophthalmol 1965; 74:205 - 16.
2. Blodi FC. Ophthalmopathy of Graves' disease. In: New Orleans Academy of Ophthalmology. Symposium on Surgery of the Orbit and Adnexa. New Orleans, 1973. St. Louis: CV Mosby. 1974; 101-11 .
3. Adler FH. In: Moses RA, ed . Physiology of the Eye; Clinical Application. 6th ed . St. Louis, CV Mosby, 1975; 15.
4. Putterman AM, Urist M. Surgical treatment of upper eyelid retraction. Arch Ophthalmol 1972; 87:401 -5.
5. Blaskovic L, cited by Berens C, King JH Jr. Atlas of Ophthalmic Surgery. Philadelphia, JB Lippincott, 1961; 76.
6. Goldstein I. Recession of the levator muscle for lagophthalmos in exophthalmic gOiter. Arch Ophthalmol 1934; 11 :389-93.
7. Moran RE. Correction of exophthalmos and levator spasm. Plast Reconstr Surg 1956; 18:411-26.
8. Bayli s HI. Cies WA, Kamin OF. Correction of upper eyelid retraction . Am J Ophthalmol 1976; 82:790-4.
9. Dryden RM, Soil DB. The use of scleral transplantation in cicatricial entropion and eyelid retraction. Trans Am Acad Ophthal mol Otolaryngol 1977; 83:669 - 78.
10. Chalfin J, Putterman AM. Muller's muscle excision and levator recession and retracted upper lid . Treatment of thyroid-related retraction. Arch Ophthalmol 1979; 97:1487 -91.
11 . Putterman AM. Surgical treatment of dysthyroid eyelid retraction and orbital fat hernia. In : Silver B, ed. Ophthalmic Plastic Surgery . Rochester, MN : American Academy of Ophthalmology and Otolarynogology, 1977; 228 - 36.
12. Beard C Ptosis. 2nd ed. St Louis, CV Mosby, 1976; 20 - 2. 13. Putterman AM, Ogura JH. Thyroid disease. Internal vertical
eyelid shortening to treat surgically induced segmental blepharoptosis. Am J Ophthalmol 1976; 82 :122-8.
14. Putterman AM. Urist MJ. A simplified levator palpebrae superioris muscle recession to treat overcorrected blepharoptosis. Am J Ophthalmol 1974; 77358-66.