Embed Size (px)
Citation preview
Turkis/i Neurosiirgery 7: 1 - 4, 1997
CLINICAL RE SEARCH
Baysefer: Sel/ar Neoplasnis
Surgical Treatment of Sellar Region Neoplasms
Sella Bölgesi Neoplazmlannin Cerrahi Tedavisi
ALPER BAYSEFER, ERSIN ERDOGAN, FERRUH GEZEN,
ERDENER TIMURKA YNAK, NACI SEBER
Gülhane Military Medical SchooL,Department of Neurosurgery, Ankara, Turkey
Abstract: The result of surgical therapy of sellar regionneoplasms in 107 patients treated between 1986-1995 isreviewed. In this series there were 89 pituitary adenomas,8 meningiomas, 9 craniopharyngiomas, and one mucocele.Transcranial, transphenoidal, and combined transcranialtranssphenoidal approaches were used for surgicaltherapy. Three patients died postoperatively. Ten patientshad complications related to surgery; CSF leak in threepatients, diabetes insipidus in four, meningitis in two, andabscess in one. Radiation therapy was administered to fourpatients postoperatively.
Key Words: Craniopharyngioma, meningioma, pituitaryadenoma, sellar region
INTRODUCTION
The close relationship of ne ural, endocrine,vascular, meningeal, and skeletal tissues in the sellarand parasellar region s poses special surgicalproblems in a smaIl anatomical area (21). Most ofthe pathological entities encountered in this area arepituitary adenomas, meningiomas, andcraniopharyngiomas. Clinical manifestations of thesetumors may be similar (18,20). Introduction ofmicrosurgical techniques to the surgical treatmentof sellar tumors increased successful outcome. In this
study, we reviewed the result of surgical treatmentin 107 sellar region neoplasms.
Özet : Bu çalismada 1986-1995 yillari arasinda, sellabölgesi neoplazmi nedeni ile cerrahi tedavi uygulanan107 olgu incelendi. Olgularin 89'u hipofiz adenomu, 8'imeningioma, dokuzu kraniofaringioma ve biri mukoselidi. Tümör çikarilmasi için transkranial, transsfenoidal vetranssfenoidal-transkranial bilesik yaklasimlar kullanildi.Üç hasta ameliyat sonrasi dönemde öldü. On hastadacerrahiye bagli komplikasyon gelisti; üç hastada rinore,dört hastada diabetes insipitus, iki hastada menenjit, birhastada abse. Ameliyat sonrasinda dört hastayaradyoterapi uygulandi.
Anahtar Sözcükler: Hipofiz adenomu, kraniofaringioma,meningioma, sella bölgesi
PATIENTS AND METHOD S
Between 1986 and 1995, 107 pa tien ts wi th sellarregion neoplasm were treated surgically. Fifty-fivepatients were female and 52 were male, ranging inage from 8 to 67 years. Initial medical records of thepatients were reviewed in detail and the clinical,laboratory, and radiographic data were collected.
Pituitary adenomas were classified accordingto radiological findings as proposed by HardyandVesina (7).
In 89 patients with pituitary adenomas 79
1

Tiirkish Neiirosiirgenj 7: 1 - 4, 1997
patients had hormonally funetioning adenomas,with high blood levels of prolaetin (PRL) in 48cases, growth hormone (GH) in 20,both GH and PRLin 7, and adrenocorticotropic hormone (ACTH) in 4.In 10 patients pituitary adenomas were hormon einaetive.
All 9 craniopharyngiomas were eystic and fiveof them had cakification.
Of 8 meningiomas 4 were clinoidal, 2 weretuberculum sellae meningioma, and two werecavernous.
Presenting symptoms are given in Table i.
Table i. Clinical findings in 107 patients.
Finding Number of patientsHeadache63Amenorrhea 33Loss of vision 24
Acromegaly 19Galactorrhea 11
Cranial nerve palsy(3,4,5,6) 8Polydipsy 7Polyuria 7Impotence 4Obesity 4Exophthalmos 3Seizure 3
The patient with mucocele, and 68 pituitaryadenomas (including 47 PRL-secreting adenomas, 14GH-secreting adenomas, 3 PRL-GH secretingadenomas, 1 ACTH-secreting adenoma, and 3 nonsecreting adenomas) underwent transsphenoidalsurgery.
30 patients with 13 pituitary adenomas(including 1 PRL-secreting adenoma, 2 GH-secretingadenomas, 3 PRL-GH-secreting adenomas, 2 ACTHsecreting adenomas, and 5 non-secreting adenomas),9 craniopharyngiomas, and 8 meningiomasunderwent transcranial surgery. Eight pituitaryadenomas (inciuding 4 GH-secreting adenomas, 1PRL-GH-secreting adenoma,I ACTH-secretingadenoma and 2 non-secreting adenomas) weretreated by transcranial-transsphenoidal approach(multiple procedures).
2
Bnysefer: Sellnr Neoplnsl11s
RESULTS
In eight transsphenoidal approaches, thetumors were subtotally excised not to damage theoptic nerve and vascular stmctures. Because of thisproblem, in cas es with lateral extension anddumbbell shape tumors, we preferred transcranialapproach in second surgery in the following 6-12months.
Forty-seven of 48 patients with PRL-secretingpituitary tumors underwent transsphenoidalsurgery. In 45 patients, PRL values were in normalrange «20ng/ml) by the 8th week of surgery.Thirteen patients who were in remission reportedreturn of normal menstmal cycle and 8 patients nolonger had galactorrhea. In three cases with subtotalremoval the adenomas had significant extrasellarextension.
Fourteen of 20 patients with GH-secretingadenomas underwent transsphenoidal surgery.Twelve of 14 patients had remission in this groupand GH values were in nonnal range «10ng/ml).
Thirteen of 89 pituitary tumors (1 PRL, 2 GH,3PRL-GH, 2 ACTH secreting, 5 non-secretingadenomas) were removed by transcranial surgery.In two patients with subtotal removal radiationtherapy was administered postoperatively. Thesepatients are in remission.
Five of 9 patients with craniopharyngioma whounderwent transcranial surgery had solid-cakifiedportions and eysts, and 4 of them showed extensionto the third ventricle. In 7 cases total removal was
performed. Postoperative radiotherapy wasadministered to a patient after subtotal removaL. Onepatient underwent secondary surgery due torecurrence .
Of 8 transcranially operated meningiomas allwere excised totally except one cavernousmeningioma.
Although three patients developedcerebrospinal fluid leak after surgery, all resolvedwith conservative therapy. Four patients developedpermanent diabetes insipidus. Three patientsdeveloped infeetion, meningitis in two, abscess inone. Three patients died after surgery; one frommeningitis and the others from cerebral infarction.
The histopathological findings, postoperativetreatment, complication and mortality are
Turkish Neuyosiirgeri; 7: i - 4, 1997
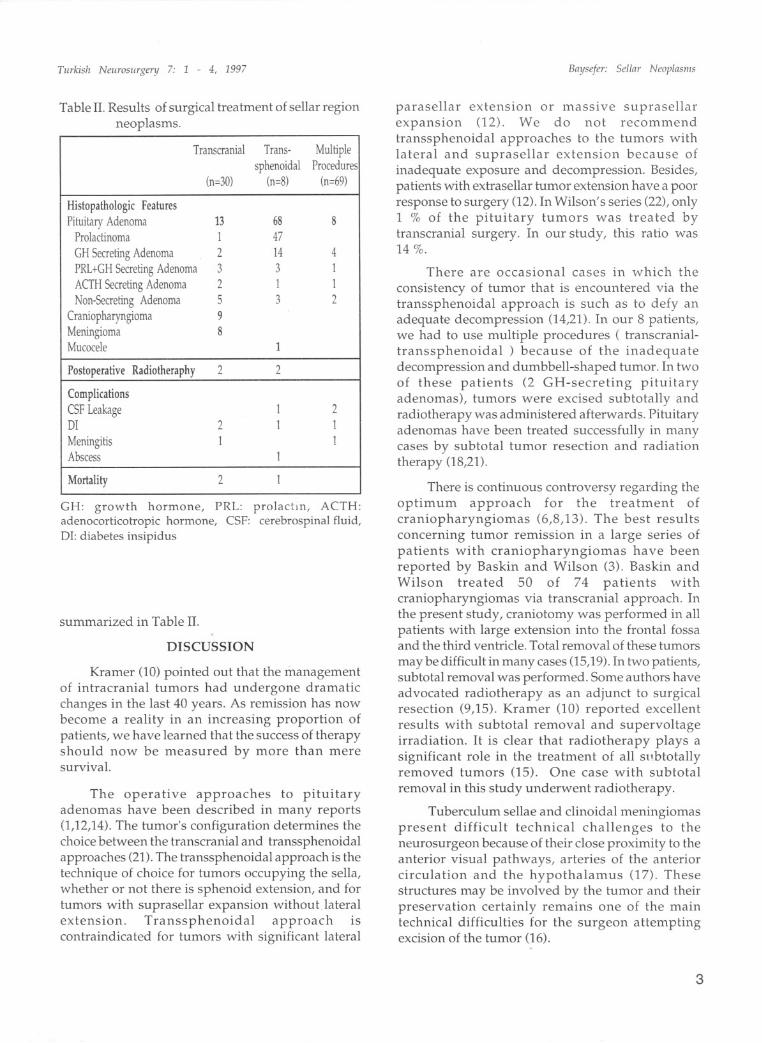
Table II. Results of surgical treatment of sel1ar regionneoplasms.
TranscranialTrans-Multiple
sphenoidal
Pmcedures
(n=30)
(n=8)(n=69)
Histopathologic FeaturesPituitary Adenoma
13688
Prolactinoma
147
CH Secreting Adenoma
2144
PRL+CH Secreting Adenoma
331
ACTH Secreting Adenoma
211
Non-Secreting Adenoma
532
Craniopharyngioma
9
Meningioma
8
Mucocele
1
Postoperalive
Radiotheraphy22
CompIicationsCSF Leakage
12
DI
211
Meningitis
11
Abscess
1
MortaIity
21
CH: growth harrnone, PRL: prolactm, ACTH:adenocorticotropic harrnone, CSF: cerebrospinal fluid,DI: diabetes insipidus
summarized in Table II.
DISCUSSION
Kramer (10) pointed out that the managementof intracranial tumors had undergone dramaticchanges in the last 40 years. As remission has nowbecome a reality in an increasing proportion ofpatients, we have learned that the success of therapyshould now be measured by more than meresurvival.
The operative approaches to pituitaryadenomas have been described in many reports(1,12,14). The tumor's configuration determines thechoice between the transcranial and transsphenoidalapproaches (21).The transsphenoidal approach is thetechnique of choice for tumors occupying the sel1a,whether or not there is sphenoid extension, and fortumors with suprasellar expansion without lateralextension. Transsphenoidal approach iscontraindicated for tumors with significant lateral
Baysefer: Sel/ar Neoplasnis
parasellar extension or massiye suprasellarexpansion (l2). We do not recommendtranssphenoidal approaches to the tum or s withlateral and suprasellar extension because ofinadequate exposure and decompression. Besides,patients with extrasel1ar tumor extension have a poorresponse to surgery (12). In Wilson' s series (22), only1 % of the pituitary tumors was treated bytranscranial surgery. In our study, this ratio was14 %.
There are occasional cases in which the
consistency of tumor that is encountered via thetranssphenoidal approach is such as to defy anadequate decompression (14,21). In our 8 patients,we had to use multiple procedures ( transcranialtranssphenoidal ) because of the inadequatedecompression and dumbbell-shaped tumor. In twoof these patients (2 GH-secreting pituitaryadenomas), tumors were excised subtotally andradiotherapy was administered afterwards. Pituitaryadenomas have been treated successful1y in manycases by subtotal tumor resection and radiationtherapy (18,21).
There is continuous controversy regarding theoptimum approach for the treatment ofcraniopharyngiomas (6,8,13). The best resultsconcerning tumor remission in a large series ofpatients with craniopharyngiomas have beenreported by Baskin and Wilson (3). Baskin andWilson treated 50 of 74 patients withcraniopharyngiomas via transcranial approach. Inthe present study, crani otomy was performed in allpatients with large extension into the frontal fossaand the third ventride. Total removal of these tumors
may be difficult in many cases (15,19). In two patients,subtotal removal was performed. Some authors haveadvocated radiotherapy as an adjunct to surgicalresection (9,15). Kramer (10) reported excellentresults with subtotal removal and supervoltageirradiation. it is dear that radiotherapy plays asignificant role in the treatment of all sllbtotallyremoved tumors (LS). One case with subtotalremoval in this study underwent radiotherapy.
Tuberculum sellae and dinoidal meningiomaspresent difficult technical challenges to theneurosurgeon because of their dose proximity to theanterior visual pathways, arteries of the anteriorcirculation and the hypothalamus (l7). Thesestructures may be involved by the tumor and theirpreservation certainly remains one of the maintechnical difficulties for the surgeon attemptingexcision of the tumor (16).
3
Turkish Neurosiirgenj 7: 1 - 4, 1997
Cavernous meningiomas were technically themost difficult tumors to excise (2). The difficultieswere related to internal carotid artery encasementand narrowing, and the involvement of the adjacentstructures (4). In our patient with cavernousmeningioma, tumor was removed subtotally. Thepresence of a mass in the cavernous sinus does notitself constitute an indication for operation. Onerecent report have demonstrated that stereotacticradiosurgery presented a viable alternatiye inpatients with small cavernous meningiomas (5).
Complications in the surgery of sellar regionincludes cerebral edema, damage to important bloodvessels, injury to cranial nerves, and injury to thehypothalamus (11).Minimizing these complicationsrequires attention to detail and a few simpleprinciples.
The goals of surgical treatment of this regioninciude elimination of tumor mass effect and
restoration of normal hormon e physiology. Ourexperience indicates that sellar region neoplasms canbe removed safely with careful preoperativeevaluation and microsurgical technique.
Correspondence: Dr. Alper BayseferGülhane Askeri Tip FakültesiBeyin Cerrahisi ABD06018 Etlik AnkaraPhone: 3251211/1966Fax: 323 49 23
REFERENCES
1. Adams CBT :The management of pituitary tumors andpost-operative visual deterioration. Acta Neurochir(Wien) 94 : 103-107, 1988
2. Al-Mefty O: The supraorbital-pterional approach toskull base lesions. Neurosurgery 21 : 474-477, 1987
3. Baskin DS, Wilson CB: Surgical management ofcraniopharyngiomas. J Neurosurg 65 : 22-27, 1986
4. Bonnal J, Thibaut A, Brotchi J, Bom J: Invadingmeningiomas of the sphenoid ridge. J Neurosurg 53 :587-599,1980
5. Duma CM, Lunsford LD, Kondziolka D: Stereotacticradiosurgery of cavernous sinus meningiomas as anaddition or alternatiye to microsurgery. Neurosurgery32: 699-705, 1993
4
Baysefer: SeHar Neoplasll1s
6. Fischer EG, Welch K, Belli JA: Treatment ofcraniopharyngiomas in children: 1972-1981. JNeurosurg 62: 496-501, 1985
7. Hardy J, Vezina JL: Transsphenoidal neurosurgery ofintracranial neoplasm, in Thompson RA, Green Jr (ed),Neoplasia in the Central Nervous System. Advancesin Neurology, volume 15,New York: Raven Press, 1976:261-274
8. Hoff JT,Patterson RH Jr: Craniopharyngiomas inchildren and adults. J Neurosurg 36: 299-302, 1972
9. Hoffman HJ, Hendrick EB, Humphreys RP:Management of craniopharyngiomas in children. JNeurosurg 47: 218-227, 1977
10. Kramer S: Craniopharyngioma : The best treatment isconservative surgery and postoperative radiationtherapy, in Marley TP(ed), Current Controversies inNeurosurgery,. Philadelphia :WB Saunders, 1976:336343
11. Laws ERJr, Kern EB:Complications of transsphenoidalsurgery. Clin Neurosurg 23: 401-416,1976
12. Mac Kay A, Hosobuchi Y:Treatment of intracavernousextensions of pituitary adenomas. Surg Neurol 10: 377383, 1978
13. Matson DD, Crigler JF Jr: Management oferaniopharyngioma in childhood. J Neurosurg 30: 377390, 1969
14. Nakane T, Kuwayama A, Watanabe M, Kageyama N:Transsphenoidal approaeh to pituitary adenomas withsuprasellar extension. Surg Neurol 16 : 225-229, 1981
15. Richmond IL, Wara WM, Wilson CB: Role of radiationtherapy in the management of eraniopharyngiomas inchildren. Neurosurgery 6: 513-517,1980
16. Sekhor L, Sen C, Jho H, Janeeka I: Surgical treatmentof intraeavernous neoplasms: a four-year experience.Neurosurgery 24: 18-30, 1989
17. Stern WE: Meningiomas in the eranio-orbital junction.J Neurosurg 38: 428-432, 1973
18. Stern WE, Batzdorf u: Intracranial removal of pituitaryadenomas: An evaIuation of varying degrees ofexcision from partial to total. J Neurosurg 33: 564-573,1970
19. Sweet WH: Radical surgieal treatment oferaniopharyngioma. Clin Neurosurg 23: 52-79, 1976
20. Taylor SL, Barakos JA, Harsh GR, Wilson CB: Magneticresonance imaging of tubereulum seiiae meningioma.Neurosurgery 31: 621-627, 1992
21. Tindaii GT, Barrow DL: Tumors of the seiiar andparasellar area in adults, in Youmans JR (ed) ,Neurological Surgery, volume 5, Philadelphia: WBSaunders, 1990, pp 3447-3498
22. Wilson CB, Dempsey LC: Transsphenoidalmicrosurgical removal of 250 pituitary adenomas. J.Neurosurg 48: 13-22, 1978







![Prognostic Value of p53 Expression in Intestinal Neoplasms ... · Small bowel tumours account for 1-2% of all gastrointestinal neoplasms.[3] Surgical resection is the primary treatment](https://img.pdfslide.us/doc/110x75/5fa3d2ecb59fba1af90d8b4a/prognostic-value-of-p53-expression-in-intestinal-neoplasms-small-bowel-tumours.jpg)