Embed Size (px)
Citation preview

SURGICAL TREATMENT()['“—
NASO-PHARYNGEAL CATARRH.UY
I). H. GOOD WILLIE, M.D, D.D.S.,
NEWYORK CITY:
(Read before the American Medical Association.)
LATE CLINICAL ASSISTANT TO- TUB METROPOLITAN THROAT HOSPITALPERMANENT MEMBER OP THE AMERICAN MEDICAL ASSOCIATION ;
MEMBER OP N. Y. NEUROLOGICAL SOCIETY; OU" THE MEDICAL
SOCIETY OP THE COUNTY OP N. Y.; ETC.
FIRST EDITION.
KEI’RINTBD FROM THE MEDICAL GAZETTE, JULY SI, 1880

TO THE MEDICAL PROFESSION.
LACTOPEPTINE.We take pleasure in calling the attention of the Profession to Lactopeptine.
After a long series of careful experiments, we are able to produce its variouscomponents in an absolutely pure state, thus removing all unpleasant odor andtaste, (also slightly changing the color). We can confidently claim, that itsdigestive 'properties are largely increased thereby, and can assert withouthesitation that it is as perfect a digestive as can be produced.
Lactopetine is the most important remedial agent ever presented to theProfession for Indigestion, Dyspepsia,Vomiting in Pregnancy, Cholera Infantum,Constipation, and all diseases arising from imperfect nutrition. It contains thefive active agents of digestion, viz: Pepsin, Pancreatine, Diastase, or Veg.Ptyalin, Lactic and Hydrochloric Acids, in combination with Sugar of Milk.
Formula of Lactopeptine.Sugar of Milk 40 ounces.Pepsin 8 ounces.Pancreatine 6 ounces.
Yeg. Ptyalin or Diastase 4 drachms.Lactic Acid ,5 fl. drachms.Hydrochloric Acid.... 5 fl. drachms.
Lactopeptine is sold entirely by Physicians’ Prescriptions, and its almostuniversal adoption by physicians is the strongest guarantee we can give that itstherapeutic value has been most thoroughly established.
The undersigned haviug tested LACTOPEPTINE, recommend it to the profession.'ALFRED L. LOOMIS, M. D.,
Prof, of Pathology and Practice of Medicine, University of the City of New YorkSAMUEL R. PERCY, M. !).,
Prof. Materia Medica, New York Medical College.F. LE ROY SATTERLEE, M. D., Ph. D.,
Prof Chem .Mat. Med.and Therap. in N.Y Col.of Deni.; Prof.Chem.and Hyg. in Am. Vet.Col etcJAS. AITKIN MEIGS, M.D., Philadelphia, Pa.
Prof of the Institutes of Med. and Med. Juris., Jeff. Medical College; Phy. to Penn. Hoe.W. W. DAWSON, M. D., Cincinnati, Ohio,
Prof. Prin. and Prac. Surg.. Med. Col. of Ohio; Surg. to Good Samaritan Hospital.ALFRED F. A. KING, M. D., Washington, D. C.r
Prof, of Obstetrics, Univer ity of Vermont.D. W. VAN DELL. M. D„
Prof of the Science and Art of Surg. and Clinical Surg., University of Louisville, Kv.L. P. YANDELL, M.D.,
Prof, of Clin. Med., Diseases of Children, and Dermatology, University of Louisville, Ky.ROBT. BATTEY, M. D., Rome, Ga.,
Emeritus Prof, of Obstetrics. Atlanta Med. College, Ex. Pres. Med. Association of G iCLAUDE H. MASTIN, M. D., LL. D., Mobile, Ala.
Prof. H. C. BARTLETT, Ph. D., F. C. S., London, England.
THE NEW YORK PHARMACAL ASSOCIATIONNos. !0 & 12 COLLEGE PLACE, NEW YORK.
P.O. BOX 1574.

SURGICAL TREATMENT-OF
NASO-PHARYNGEAL CATARRH.BY
D. H. GOODWILLIE, M.D., D.D.S.,
NEWYORK CITY;
(Read before the American Medical Association.)
LATE CLINICAL ASSISTANT TO THE METROPOLITAN THROAT HOSPITAL;PERMANENT MEMBER OP THE AMERICAN MEDICAL ASSOCIATION ;
MEMBER OP N. T. NEUROLOGICAL SOCIETY; OP THE ?.IEDXCAJ,
SOCIETY OP THE COUNTY OP N. Y.; ETC.
REPRINTED FROM THE MEDICAL GAZETTE, JULY 31. 1880.
NEWYORK :
CHAS. L. BERMINGHAM & CO.1260 Broadway.


SURGICAL TREATMENT OF NASO-PHARYNGEAL CATARRH.BY
D. H. GOOmVILLIE, M.D., D.D.S.New York City.
(Read before the American Medical Association, June 3, 1S80.)
Of the etiology of naso-pharyngeal catarrh,I desire only to say in reference to those casesthat shall occupy our attention at this time,that their history, in many instances, com-mences in early life—even in infancy. Par-ticularly is this the case in deviations and ex-ostosis of the nasal septum.
The sides of each nasal fossae contain thethree turbinated bones and throw the mucousmembrane that covers them into folds, so thatin a small space a large amount of mucoussurface is exposed. A wise provision for tem-pering and cleansing the air that passes overit to the lungs. Experiments have shownthat air respired through the nose is raisedmore than two degrees in temperature thanwhen respired by the mouth.
Respired air must pass through both thenostrils alike to producea healthyrespiration.
In the same proportion that respiration isprevented through the nose , the gate way to thelungs . will there be catanhal conditions of the■upper airpassages, and in many casesreachingthe lungs ultimately.
Of the passages through the nostrils the in-ferior meatus is the most important, as it isthe chief respiratory passage for air, and forthe carrying off, in a great measure, the nasalsecretions.
For the latter purpose it is lined with coll-ated columna epithelium. The mucous mem-brane is quite vascular, and consequentlysub-ject to very sudden engorgement.
I do not propose to say anyth rug respectingcatarrhal conditions that require medical treat-ment only, but to such cases as have passedthat point and can only be relieved by sur-gical interference.
Some of the pathological conditions towhich I desire at this time to call your atten-tion requiring surgical treatment are the fol-lowing, viz;
1. Exostosis. 2. Deviated nasal septum.3. Hypertrophy of the erectile cavernoustissue on the turbinated bones. 4. Polypi.5. Necrosis from struma or syphilis. 6.Chronic antrum disease. 7. Chronic maxil-lary abscess from tooth disease.
The time allotted me will only suffice forthe consideration of some of these which Iwill endeavor to illustrate by a few cases bymeans of diagrams and wax models.
Exostosis of the turbinated bones is not sofrequent an occurrence as it is in the vomerwhen it is associated with deviated septum.
Their growth is attended usually by painsof a neuralgic character. They prevent res-piration, and by pressure causes sloughing andnecrosis of adjacent parts. Exostosis withdeviation of septum is of more commonoccurrence.
Whenever the vomer takes a sharp deflec-tion there is often found an exostosis on theconvex side, just at the greatest part of thecurve.
When this occurs along the line and intothe inferior meatus, as it more often does, itgives a great deal of catarrhal trouble by pre-venting free respiration and the passage outof the nasal secretions, which not beingchanged by a free respiration, becomes fetidby decomposition.
Deviations of cartilaginous septum are quitenumerous—curves in between the bony sep-tum and the columna in many directions.Dislocation of the lower end of the septumwith displacement of the nasal spina, alsoproduce abnormal respiration. .
HYPERTROPHY OF THE ERECTILE CAVERN-OUS TISSUE COVERING THE INFERIOR TUR-
*
BINATED BONES.
Some years ago Dr. Henry J. Bigelow, ofBoston, in an article foundin the Boston Medi-cal and Surgical Journal for April 29. 1875,states that he has found ‘
‘ a remarkable andwell-formed cavernous structure at least uponthe middle and inferior turbinated bones.The difference in size of the distended andcollapsed cavernous bodies is quite strikingand is best seen upon the inferior turbinated.Collapsed, the outline and dimensions arenearly those of its attenuated, bony frame-work. Distended, it becomes an angry, tur-gid mass of uneven surface and livid color,completely closing the lower nostril. Apouch-like dilatation projects from the rear ofthe bone, increasing its length and with theaid of a blow-pipe readily showing, on sec-tion, to the naked eye cavernous cells. Itis this reticulated pouch that is seen with themirror at the back of the nares. Above isseen the middle turbinated mass similarly dis-tended, and if the injection of the wholemembrane is considerable, the nasal septumalso swells to nearly the thickness of one-quarter of an inch. If inflated and dried,the cells project upon the surface. A sectiongives further evidence of a cavernous struct-ure with juxtaposed cavities, tolerably uni-

4
form in size and equally distributed; ap-proaching quite nearly, both the mucous sur-face and the bone. They communicate byirregular apertures while minute bands andsepta traverse and connect their commonwalls.
A wet microscopic section exhibits thintrabeculae and walls composed mainly of con-nective tissue, presenting cavities of unequaldimensions and closely resembling the cavernous structure of the penis, although thesmooth muscular element, as also the tunicaalbuginea of the latter, are somewhat morepronounced, as-raight be anticipated from thecomparative erectile tension of this organ.”
I pass around for your inspection two waxmodels of cleft palates,showing the extensivehypertrophy of the tissue covering thesebones. When fully erected they entirely fillthe cleft. In one will be observed this con-dition, while in the other it is in a state ofnon-erection.
By experiment made on them I found thatanything that would excite the salivary andmuciparous glands to increased action causedan erection of this hypertrophied erectile tis-sue. When the exciting cause was removed,after a short time it receded.
engine, when it may be removed with thenasal forceps. (See Fig. x, cutting drills.)
The exostosis on the vomer is removed bythe revolving multiple knife (Fig. 2) carriedthrough the nostrils to the pharnyx enclosedwithin a sheath, so as not to cut any tissueexcept the exostosis. The small exostosisof the turbinated bones are removed in thesame way.
For the treatment of the deviated cartila-ginous septum I have found no operation sosuccessful as removing a section containingthe bend by means of the excising nasal for-ceps (Fig. 3) devised some years, ago. Oneblade contains the circular or oval knife anathe other is flat, against which the knifecomes when it has cut its way through theseptum.
My attention lias been called to a some-what similar instrument described in Diet.Encycloped des sciences med. et chirurg;article nez.
It requires some half a dozen forceps ofdifferent sizes and shapes to meet everycase.
In dislocation of lower end of cartilagin ■ous septum make an incision over the end ofthe dislocated and protruding cartilage down
Fig. 1.
This erection and collapse is a physiologi-cal fact in the normal condition and is in-tended to purify the tidal air passing in res-piration from all impurities and soprotect thepulmonary organs against disease. The hairsin the vestibule of the nostrils and this erect-ile tissue are faithful sentinels to arrest im-purities in the respired air.
By a constant irritation of this erectile tis-sue by impurities in the respired air, by amechanical irritation caused by a constantand forcible blowing of the nose in chroniccatarrh, the effect of which is felt on theanterior part of the inferior turbinated bonejust within the vestibule, a hyperplasia is
to the cartilage, denude it of the periosteum,push, it back and then amputate the protrud-ing cartilage (and nasalspine also, if it is dis-placed), replace the denuded soft tissue andhold them together by small sutures.
The hypertrophy of the erectile tissue on theturbinated bones is removed by means of thegalvano or thermo-cautery. To the parquelincautery I have devised a new handle, whichis held between the two fingers and thumb.(Fig. 4.) In the office use the condensed airinstead of forcing the air by the hand-balls.The cautery is very efficiently held and theforce of the air easily controlled by the thumb.The thermo-cautery can only be used in the
Fig. 2. —Knife (a) within the sheath.thereby set up which results in so thickeningthis tissue that normal respiration is verymuch interfered with and in some cases en-tirely prevented. To the above causes maybe added in many cases a constitutional pre-disposition to catarrhal conditions.
Treatment of exostosis of the turbinatedbones, when large, consists in drilling the en-largement at its base by means of the surgical
anterior nares.Dotted lines represent the shield through
which the cautery passes.The part of the cautery within the shield
is covered over with asbestos to protect thevestibule from the heat.
The galvano-cautery is by far the most effi-cient cautery to be used in the nose. Bv theuse of properly constructed electrodes it can

5
be used anywhere in the nose, pharynx orlarynx.
The vestibule of the nostrils isprotected fromthe heat by a shield made of glass and asbestos.(Fig. 5.) The lower part of the shield isflanged so as to be easily held between thefingers. The top of it embraces the part tobe cauterized. The electrode when heatedto a high heat is passed through the shield onto the parts to be removed.
ferior turbinated bone will be necrosed. Suc-cessful treatment requires a large opening inthe nasal wall so that it may give free exit tothe discharge and proper cleansing of thecavity. It must be faithfully dressed bywashing it out with thymol or carbolic acidand water.
Chronic maxillary abscesses of thesecond orthird molars occasionally discharge into thepharynx and produce catarrhal conditions.
Fig- 3-Extract the tooth and open well into the
abscess and keep it open until it granulatesfrom the bottom to the surface.
Chronic antrum disease is a frequent sourceofnaso-pharyngeal catarrh. This commencesalmost always by a decomposed dental pulpopening into and setting up trouble in theantrum. With this there is more or lessfacial neuralgia. Ido not think this is oftenrecognized except perhaps in extreme caseswhere extensive necrosis exists.
After all surgical operations the patient ispositively forbidden to blow the nose for thefirst twenty-four hours as a preventativemeasure against hemorrhage. After thattime the nose is freed of clot and mucus bymeans of the nasal dressing forceps and thenasal douche. Then the powder of iodoformand camphor is blown in, covering the en-tire mucous surface of the nose or antrumwhen that cavity has been opened.
In cases where an anaesthetic is given Ialways commence with nitrous oxide, and, ifthe operation is to be prolonged, continuewith some other anaesthetic. The head ofthe patient is securely fixed in a head-rest,preventing any motion during the operation.
Fig. 5.
The following cases were all severelytroubled with naso-pharyngeal catarrh. Therebeing stenosis of the nostrils, the dischargeswere either expectorated or swallowed.HYPERTROPHY OF THE ERECTILE TISSUE OF
Fig. 4- BOTH INFERIOR TURBINATED BONES.
The proper treatment is to extract themolar and trefine through the alveolar pro-cess into the lower part of the antrum.
If the disease has existed for any length oftime the naso-antrum foramen will be enlargedand occasionally the entire nasal wall and in-
Case I.—G. G. (sent to me by Dr. D.Monro, Ontario, Canada,), aged 29 years, ofOntario, Canada. Single. Has had catarrh for many years. Formerly had muchblowing of the nose, but now has so muchstenosis of anterior nares that the discharges

are now expectorated; respires through thenose very little; voice in consequence quitenasal in tone; slight curve in the cartilagin-ous septum to the left; soft tissue over bothinferior turbinated bones hypertrophied, theright one the largest as it fills up the curvein the septum.
Rhynoscopic appearance reveals enlarge-ment of tissues on inferior turbinated bones,and also on each side of the septum. In-ferior meatus nearly filled up by the hyper-trophy.
Uvula very much hypertrophied and elon-gated; slightly deaf in both ears; pharyngio-eustachian opening much enlarged, with two
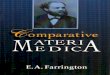
Fig. 6.
on one and three on the other of fibrousbands, attaching it to the pharyngeal folds.(See Figs. 6 and 7.)
Fig. 6 represents hypertrophy of inferiorturbinated within the vestible.
opening without an anaesthetic. Twenty-four hours after each operation the nostrils arecleaned out by the forceps, and the nasaldouche cautiously used and the powder ap-plied. For a short time after the operationthis dressing is made twice a day.
Not much benefit in respiration is experi-enced by the patient during and for sometime after the operation, as the cauterizingexcites a free discharge from all the mucipar-ous glands of the nose and pharynx, and inconsequence the nostrils are quite stuffy.But as the parts heal and contract, and theair (the natural element) passes over it, therecomes a great sense of relief.
This patient being a large manufacturer, hecould only remain under treatment sixweeks, but much was accomplished in thattime; thanks to the patience of my patient.His respiration was fully restored and voicemuch improved. Small scabs over the lastplaces cauterized,some nasal secretion, as thesmall scabs kept up an irritation in the nose;but as they heal the secretion becomes nor-mal.LOSS OF SINGING VOICE FROM HYPERTROPHY
OF ERECTILE TISSUE ON INFERIOR TURBIN-
ATED BONES.
Case II.—The following letter from thefamily physician gives the history, diagnosisand result of treatment, in the next case, of aprominent singer:
Fig. 7. (a) Hypertrophy on inferior turb-inated filling the inferior meatus, (3) andseen also behind the posterior septum atc. Dotted lines represent the normal size ofinferior turbinated bones, d represents anenlargement on the septum, f. Pharyngio-eustachian opening with three fibrous bands.
Treatment.—Amputated uvula. Removedthe anterior part of the hypertrophy on in-ferior turbinated bones by the thermo - cau-tery, and the posterior part by the galvano-cautery under anaesthesia produced by nitrousoxide. Cut the adhesions at the eustachian
New York, May 28, ’BO.
To D. IT Goodwillie, M.D. :
My Dear Doctor—On the 26th of Octo-ber, 1879. I sent you for treatment Mrs. A.B. ael. 26. The following is the history ofthe case. The patient was one of our bestcontralto singers; when suddenly she noticeda difficulty in emitting her head notes andlittle by little lost her singing voice almostcompletely.
Being the family physician I was consultedand after a laryngoscopic and rhinoscopic ex

7
amination, I was convinced that all thetrouble was in the nasal cavities. I found oneach side a thickening of the mucous mem-brane and hypertrophyof the soft tissues overthe turbinated bones. The occlusion wasnearly complete, havingvery little respirationthrough the nose. Your diagnosis confirmedmine and putting the patient in your handsyou began the treatment that terminated sosuccessfully.
Now I am happy to state that the resultwas very gratifying to my patient.
After the first operation her voice began toreturn and after the last operation she wasable to appear in public on April 22, 1880,and sang four times with encores.
Receive, my dear doctor, with my congrat-ulations, for such a success, the expression ofkindest regards.
Yours very truly,L. de Bremont, M.D.
From the shock from the loss of her voiceshe had become amende and suffered from in-digestion, constipation, headaches and in-somnia.
Treatment. —Prohibited the use of wine,tea, or coffee, and recommended milk dietwith farinaceous food. The milk to be takenwarm, a teacupful at a time with a very littlelime water. Give also elix. gentian and tine,of chlo. of iron. The body to be spongednight and morning with salt water and bayrum.
Flannel to be worn next the skin whichshe had never done before.
The hypertrophy was removed by means ofthe cautery in three operations under N. O.She now looks hale and hearty; no indigestionor constipation; has gained more than twentylbs in weight; no insomnia, and voice re-gaining its strength after having lost it forsome three years.
(In the wax model of this case you can seejust within the vestibule the passage nearlyclosed up. It looks very much like a half ofa red cherry. The other model exhibits thenostril after the operation for its removal.)HYPERTROPHY OF TISSUE ON INFERIOR TUR-
BINATED BONES WITH DEVIATION OF CAR-
TILAGINOUS SEPTUM.Case 111. —S. M. of Alabama, sent me by
Dr. L. B. Bangs. In early life was troubledwith running from the nose, but in adult agethe anterior nares became partially closed,then expectoration increased. Went abroadand in Germany received treatment by cauter-izing the enlargedpharyngeal follicles withoutany benefit. On examination found lungshealthy, a severe naso-pharyngeal catarrhgiving him great trouble. Thick mucus runningdown on each side of the vertebral ridge fromthe nares. Pharynx granular with patchesof a dry smooth surface where the follicleshad suppurated or been destroyed by thecautery.
Cartilaginous nasal septum deviated into
right nostril with hypertrophy of soft tissueon both inferior turbinated bones; very im-perfect respiration. Smelling much impaired.
Treatment.—Removed oval section l/ 2 by£i inch of bend of septum with the excisingnasal forceps; this operation opened up rightnostril and improved his respiration.
Six months after this first operation re-moved small pedunculated polypus fromright nostril posterior to the section; also bythe cautery the hypertrophy on left inferiorturbinated bone without an anaesthetic.
Two months after his return home hewrites that his respiration is good, and ca-tarrhal discharge very little, and graduallydecreasing.
DEVIATED SEPTUM.
Case IV.—Dr. Herman Knapp sends meI. E. C., a law student with the cartilaginousnasal septum deviated into the left nostrilpreventing respiration, causing catarrhaltrouble, with some defect in his sight.
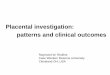
On Oct. 22d, 1879, the presence of Drs.Knapp, Farnham, Robinson and Bozeman,removed with the excising nasal forceps thebent part of the septum. This restored res-piration and gave him great relief. Fig. 8&9,
BEFORE.
Fig. 3.DISLOCATION OF CARTILAGINOUS SEPTUM.*
Case V.—E. G. was referred to me byDr. C. R. Agnew, who has been sufferingfor many years with catarrh. While it was
AFTER.
Fig. 9.at first nasal, he was in the habit of placinghis right thumb against the right side of hisnose when he blew it (the catarrh being in a* Canada Medical Record, Dec. ’79-

8
great measure from the left nostril), dislocatedthe septum and nasal spine into the vestibuleof the left nostril, and protruded outside,pushing to the right the colurnna nasi. Res-piration was entirely prevented from the leftnostril, and not perfect in the right. Hasdeafness of left ear.
Treatment consisted in making an incisionover the protruding end of the septum andspine, denuding the soft parts, pushing themback and amputating the septum with one ofthe excising nasal forceps. Soft parts werebrought together again and united by sutures.This restored respiration, the good effect ofwhich was seen by great improvement in ca-tarrh and also in the hearing.HYPERTROPHY OF ERECTILE TISSUE AND
DEVIATION, WITH EXOSTOSIS OF NASALSEPTUM.Case VI.—F. P. from Westchester Co.,
N. Y., has had nasal catarrh for many years.Now air and the mucous discharge does notpass freely out the anterior nares in conse-
quence of an enlargement on the inferiorturbinated bones, and a deviation with exos-tosis of the septum, into the inferior meatus.Has also chronic follicular pharyngitis. Hesuffers now from post-nasal trouble. Snoresin his sleep from imperfect nasal respiration.Takes cold readily, and has sore throat.Hawks and expectorates to relieve himself ofthe naso-pharyngeal discharge.
Operated under an anesthetic, and re-moved hypertrophied erectile tissue with thegalvano-cautery. The deviation and exosto-sis was removed by means of the revolvingknives (Fig. 2) and surgical engine. The in-ferior meatus is now quite free, and hebreathes, sleeps and eats well, or, as he ex-presses it, has a “wonderful amount of com-fort now.”
The following gantlemen were present atthe operation: Drs. F. N. Otis, J. C. Hutch-inson, H. P. Farnham, and E. D Hud-son, Jr.
160 West 34th street.

MALTINE.Maltine in. Phthisis.
WM. PORTER, A.M., M.D., St. Louis.
Phthisis is pre-eminently a wasting disease, and by exalting failing nutri-tion, cod-liver oil being little more than a given food, a great advance wasmade in therapeutics. It has been found, however, that the oil does not inmany cases meet the indications ; for not only is nourishment needed, but thedigestive power is so reduced that but little use is made of the food that istaken. Hence, a demand both for nutritious material and also for somethingwhich will aid food suitable for assimilation. The clinical starting-point inthe history of the greater number of cases of phthisis is mal-nutrition, andwhen that is guarded against, much is accomplished.
After full trial of the different oils, and extract of malt preparations inboth hospital and private practice, I find Maltine most applicable to the largestnumber of patients, and superior to any other remedy of its class. Theoreti-cally we would expect this preparation , which lias become practicality of-ficinal, to be of great value in chronic conditions of waste and mal-nutrition,especially as exemplified in phthisis Being rich in diastase, albuminoids andphosphates , according to careful analysis, it aids in digesting farinaceous food,while in itself it is a brain, nerve and muscle producer.
In practice, this hypothesis is sustained. A female patient at St. Luke’sHospital, aged 35, with phthisis, signs of deposit in the left upper lobe, losingflesh for six months, poor appetite and night sweats, began taking MaltineMarch 13th, 1880. She now weighs 121 lbs., eats well, no night sweats andthe evidences of local disease are much less marked.
Another case of phthisis: A gentleman from Alabama, with all the phys-ical signs of phthisis, rapidly losing health and strength. His was the re-markable gain of 10 lbs. from, six weeks’ use of Maltine.
Seven pounds increase in as many weeks is the record of the third patient,a lady of 41 years, who has had no other medication than the Maltine. In theseand other cases the increase in strength and mental vigor is in proportion tothe gain in weight.
These instances are sufficient for illustration, and are duplicated manytimes in the experience of physicians everytchere. There is a universal reluc-tance always to testify to results from medicinal preparations, but when, as inthis case, the composition is fully known, and the profession invited to inves-tigate the manner of preparing it, there is no reason why the remedy shouldnot receive general approbation, provided it be worthy.— Quarterly Epitomeof Practical Medicine and Surgery , a supplement to Parithwaite’s Retrospect.
LIST OF MALTINEOTAI/TINE (Plain)JIALTINE with Hops.OTAI/TIN E with Alteratives.MALTIM! with Beef and Iron.-OTA I.TTNB with Cod Liver Oil.OTA L'I'IAE with Cod Liver Oil and lodide Iron.OT ALT INK with Cod Liver Oil and Pancreatine.OTA 4,TIN E with Cod Liver Oil and Phosphates.OT A I/TINE with Cod Inver Oil and Phosphorus.OTAL.TINIS with Hypophosphites.
LABORATORY,TONKEBS-ON-THE-HUDSON(
PREPARATIONS.MALTINE with lodides.OTA I/ITNE with Peptones.OTALTINB with Pepsin and Pancreatine.MALTIN E with Phosphates.MALTINE with Pho-phates Iron and Quinta.MAI/S'INE with Phosphates Iron, Quinia andItIAEXINE Ferrated. [Strychnia.OTALTINE WINE.MALTINE WINE with Pepsin & Pancrea-MALTO- k EUIIINE. [tine.
REED & CARNRICK,Office, 196 FULTON STREET,
NEWYORK.

ESTABLISHED 1876.
THE MEDICAL GAZETTE.PUBLISHED WEEKLY.
Edited by EDWARD J; BERMINGHAM, A.M., M.D.SUBSCRIPTION, $3.00 PER YEAR, IN ADVANCE.
“Unquestionably the best medical weekly published in this country.”—Wm. A. Hammond , M. D.“A medicalweekly of the highest order.”—/. MarionSims, M. D.
SIXTH YEAR OF PUBLICATION-1 88 IStBSCBIBE NOW
AND GET THE REMAINDER OF THIS YEAR FREE.Any new subscriber remitting the amount ft his subscription for 1881. will receive the journals
regularly from the time of the receipt of his subscription until the close of this year free of charge.Sample copies will be cheerfully furnished.
OHAB. L. BERMINGHAM & CO.. Publishers, 1280 and 1262 Broadway, N. Y,
JUST PUBLISHED.The Hypodermic Injection of Morphia.
Its History, Advantages and Dangers.By H. H. KANE, M.D.
A handsome 12mo. voL of 360 pages. Illustrated.Cloth $2.00
Cuas. L. Bermingham & Co., Publishers.
JUST PUBLISHED.FRACTURE OF THE PATELLA.
A STUDY OE 127 CASES,
By F. 11. Hamilton, A.M., M.D , LL.D.A handsome Byo. vol., pp. 112. Illustrated
Clo h. Bevelled $1.5Chas. L. Bermingham & Co., Publishers.
JUST isstn:i>-
THE MEDICAL GAZETTE MAILING LISTS.MAILING LISTS OF PHYSICIANS.
AX ENTIRELY NEW COMPILATION, REVISED TO JULY, 1880, BY THE EDITOR OP THE MEDICAL GAZETTE. PER-FORATED, GUMMED, AND ON COLORED MAILING PAPER, FOR ADDRESSING CIRCULARS, LETTERS, SAMPLES, AC.
PRICE, $1.25 PER 1,000 NAMES.(A Discount of 20 per cent, allowed where t ie complete set for all the States is ordered.)
The names are arranged alphabetically in each State, and the greatest care has been exercised in thecompilation, to comply with the P. O. regulation, requiring the P. O. Address to be given, where this differ*from the town. y
The complete set numbers about 65.000 names, upwards of 52.000 of which cannot be obtained from anyother source, as they do not appear in Butler’s Directory, or any otherpublished list.
LISTS MAY BE OBTAINED FOR ANY STATE.
THESE LISTS ARE NOW IN USE THE FOLLOWING FIRMS:E. F. Houghton & Co., Phila.Reed & Oarnrick. New York.N. Y. Pharmacal Association, New York.Scott & Bonne, New York.
Keasbey & Mattison Phila.D. Appleton & Co., New York.Houghton, Mifflin & Co., Boston.College of Physicians & Surgeons, New York.Medical Collegeof Indiana.Detroit Medical College.University of Maryland, (Med. Dept.)Columbus (O) Medical College.Long Island Medical College.Purcell, Ladd & Co.. Richmond.Wm.VYood & Co., New York.
A. C. Dung. Now Yoik.J. A. McArthur, Lynn, Mass.Smith's Homoeopathic Pharmacy, New York.G- W. Archer, Rochester, N. Y.G. R. Fuller, Rochester, N. Y.Walter Baker & Co., Boston.J. & W. Horlick & Co., Racine, Wis.Ransom & Raudolpn, Toledo, O.
-A-HsriD uvE.A/isr'sr OTHERS
CHAS. L. BERMINGHAM & CO., Publishers,1260 & 1262 BROADWAY, V. Y.








![Thispaperhasbeenbrokenintotwoparts.Thefirstpartisavailableat ...Corms Stimulant to the secretions in asthma, whooping cough, chronic catarrh, and rheumatism. Green Dragon [Dragon Root]](https://img.pdfslide.us/doc/110x75/5f763701e44bed770578a107/thispaperhasbe-corms-stimulant-to-the-secretions-in-asthma-whooping-cough.jpg)