Embed Size (px)
Citation preview

Scaphoid Nonunion
Scaphoid nonunion is challengingto manage because of the geom-
etry of the scaphoid, the directionand type of fracture, and the vascularpattern of the blood supply to thescaphoid. Fracture proximal to theperforating vessels on the dorsora-dial surface of the scaphoid cancause significant bone ischemia ofthe proximal pole. Delayed diagno-sis, inadequate initial management,proximal fracture location, osteone-crosis, and associated carpal instabil-ity with acute scaphoid fracture canlead to nonunion of the scaphoidwaist or the proximal pole.1 Non-union can exist with or without os-teonecrosis of the proximal frag-ment. Osteonecrosis of the proximalpole can occur with a scaphoid waistnonunion, but there is almost al-ways loss of blood supply in proxi-mal pole scaphoid nonunion. Non-union involving the scaphoid waistoften has significant bone loss andcarpal collapse, along with volar ro-tation of the distal pole, which pro-duces an apex dorsal humpback de-formity.
Left untreated, scaphoid non-union can progress to carpal collapseand a predictable pattern of radiocar-pal arthrosis.2 The goals of surgeryfor scaphoid nonunion include unit-ing the fracture and restoring carpalalignment (ie, correcting carpal in-stability). Evidence suggests that sur-gical results are better when care istaken to correct deformity and to ad-dress the vascularity of the scaphoid.
Indications
Cast immobilization, with or with-out adjunctive treatment (eg, pulsedelectromagnetic fields), is not as ef-fective as surgical intervention andtypically is not recommended formanaging scaphoid nonunion.3 Im-mobilization with a long arm cast
for prolonged periods (>6 months)can have a significant impact onwrist and elbow motion, as well ason quality of life. Because unionrates with pulsed electromagneticfields are inferior to those with sur-gery, electromagnetic fields shouldbe used only as an adjunct to surgeryor when surgery is not possible. Sev-eral reports indicate that few non-unions remain stable or nondis-placed and free of arthritis after10 years.2,4 Because of the evidencelinking nonunion with osteoarthri-tis, surgery is recommended formost young, healthy patients evenwhen they are symptom-free andhave normal wrist mobility. Mosthand surgeons recommend open re-duction and internal fixation com-bined with bone graft.5-8
Contraindications
Surgery to correct scaphoid non-union with bone grafting and inter-nal fixation is contraindicated in thepatient with progressive arthrosis(eg, scaphoid nonunion advancedcollapse [SNAC] wrist).9 Relativecontraindications include chronici-ty, location, size and vascularity ofthe nonunion,10 smoking,11,12 and pa-tient age,13 all of which are impor-tant to consider when evaluating thepotential for postoperative success.
Surgical Technique
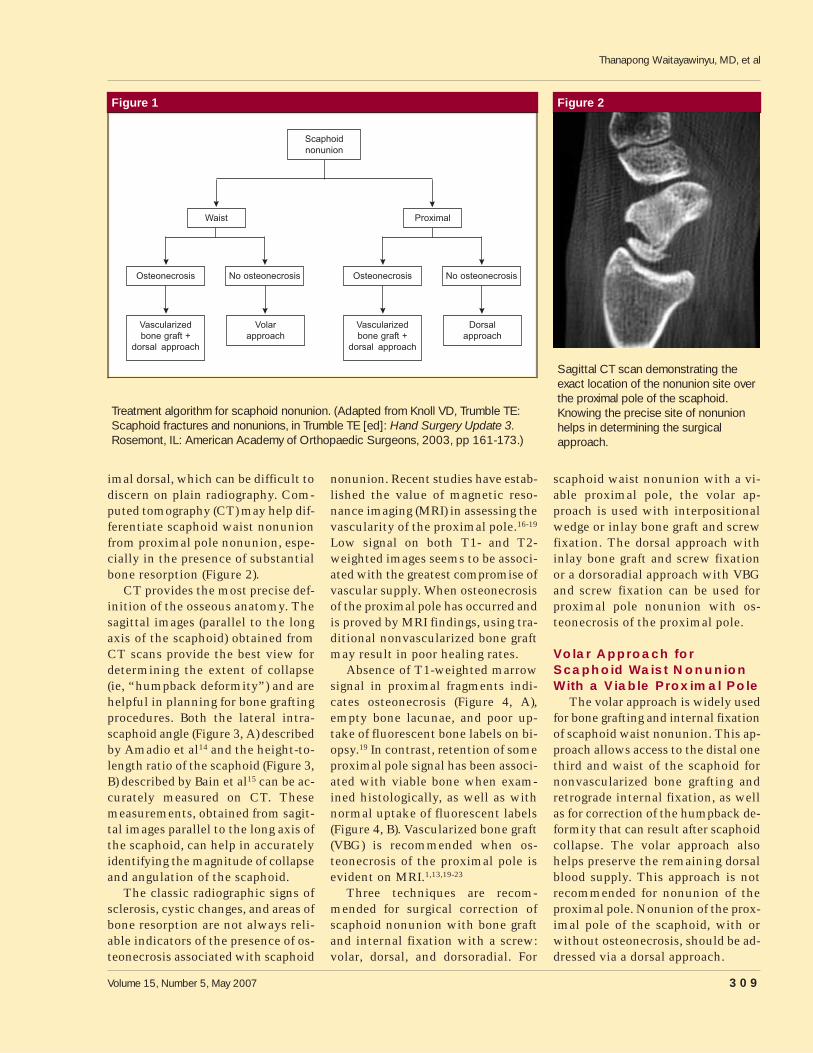
Determining the location of thescaphoid nonunion, degree of carpalcollapse, and viability of the proxi-mal fragment is important in devel-oping a treatment algorithm forscaphoid nonunion (Figure 1).
Plain radiographs are helpful, butnot foolproof, in determining whetherthe scaphoid fracture involves theproximal pole. The scaphoid fractureoften angles from distal volar to prox-
Thanapong Waitayawinyu, MD
Wren V. McCallister, MD
Nicholas M. Nemechek
Thomas E. Trumble, MD
Dr. Waitayawinyu is Research Fellow,Hand and Microvascular Surgery,Department of Orthopaedics & SportsMedicine, University of Washington,Seattle, WA. Dr. McCallister is Fellow,Hand and Microvascular Surgery,Department of Orthopaedics & SportsMedicine, University of Washington. Mr.Nemechek is Research Assistant, Handand Microvascular Surgery, Departmentof Orthopaedics & Sports Medicine,University of Washington. Dr. Trumble isProfessor and Chief, Hand andMicrovascular Surgery Service,Department of Orthopaedics & SportsMedicine, University of Washington.
None of the following authors or thedepartments with which they areaffiliated has received anything of valuefrom or owns stock in a commercialcompany or institution related directly orindirectly to the subject of this article:Dr. Waitayawinyu, Dr. McCallister,Mr. Nemechek, and Dr. Trumble.
Reprint requests: Dr. Trumble,Department of Orthopaedics & SportsMedicine, University of Washington,4245 Roosevelt Way NE, Box 354743,Seattle, WA 98195-4743.
J Am Acad Orthop Surg 2007;15:308-320
Copyright 2007 by the AmericanAcademy of Orthopaedic Surgeons.
The video that accompaniesthis article is “ScaphoidNonunion,” available on the
Orthopaedic Knowledge Online Website,at http://www5.aaos.org/oko/jaaos/surgical.cfm
Surgical Techniques
308 Journal of the American Academy of Orthopaedic Surgeons
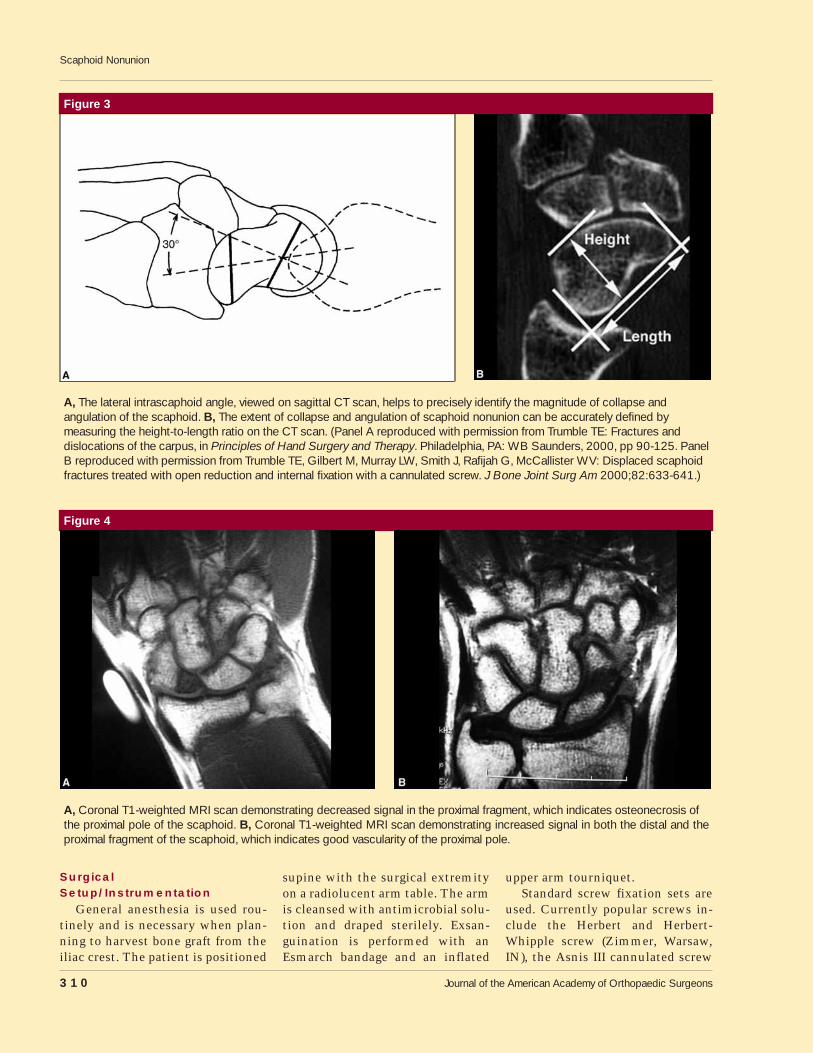
imal dorsal, which can be difficult todiscern on plain radiography. Com-puted tomography (CT) may help dif-ferentiate scaphoid waist nonunionfrom proximal pole nonunion, espe-cially in the presence of substantialbone resorption (Figure 2).
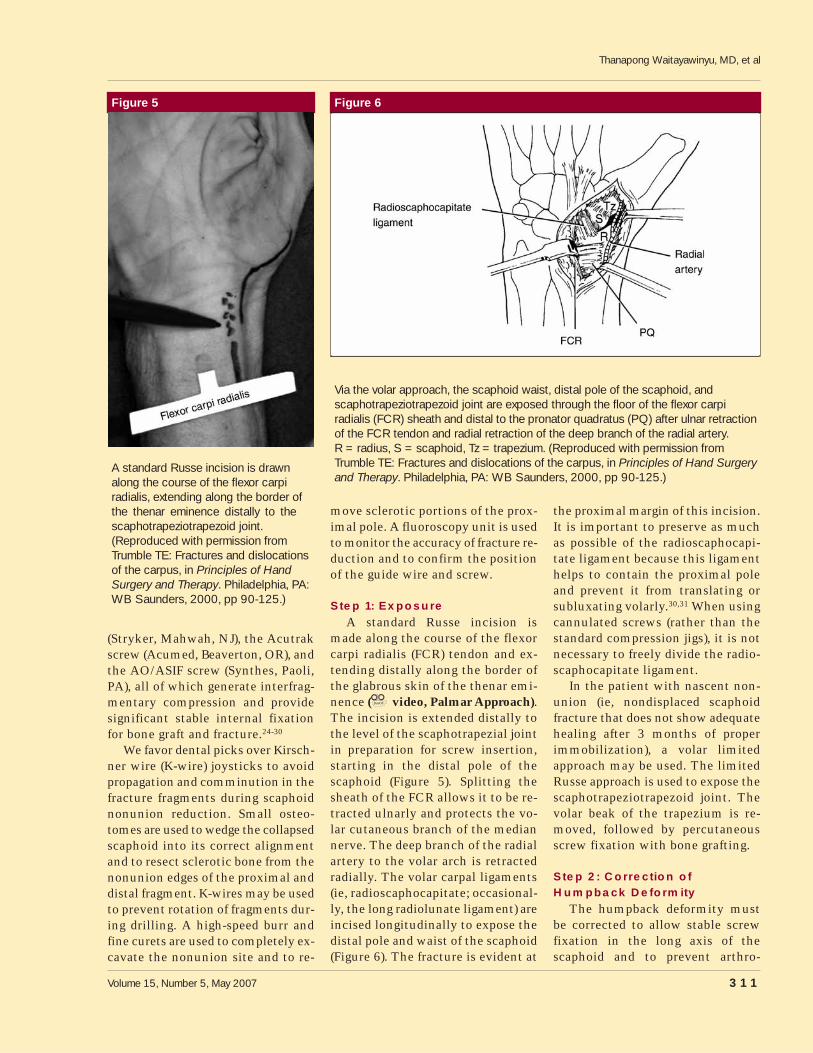
CT provides the most precise def-inition of the osseous anatomy. Thesagittal images (parallel to the longaxis of the scaphoid) obtained fromCT scans provide the best view fordetermining the extent of collapse(ie, “humpback deformity”) and arehelpful in planning for bone graftingprocedures. Both the lateral intra-scaphoid angle (Figure 3, A) describedby Amadio et al14 and the height-to-length ratio of the scaphoid (Figure 3,B) described by Bain et al15 can be ac-curately measured on CT. Thesemeasurements, obtained from sagit-tal images parallel to the long axis ofthe scaphoid, can help in accuratelyidentifying the magnitude of collapseand angulation of the scaphoid.
The classic radiographic signs ofsclerosis, cystic changes, and areas ofbone resorption are not always reli-able indicators of the presence of os-teonecrosis associated with scaphoid
nonunion. Recent studies have estab-lished the value of magnetic reso-nance imaging (MRI) in assessing thevascularity of the proximal pole.16-19
Low signal on both T1- and T2-weighted images seems to be associ-ated with the greatest compromise ofvascular supply. When osteonecrosisof the proximal pole has occurred andis proved by MRI findings, using tra-ditional nonvascularized bone graftmay result in poor healing rates.
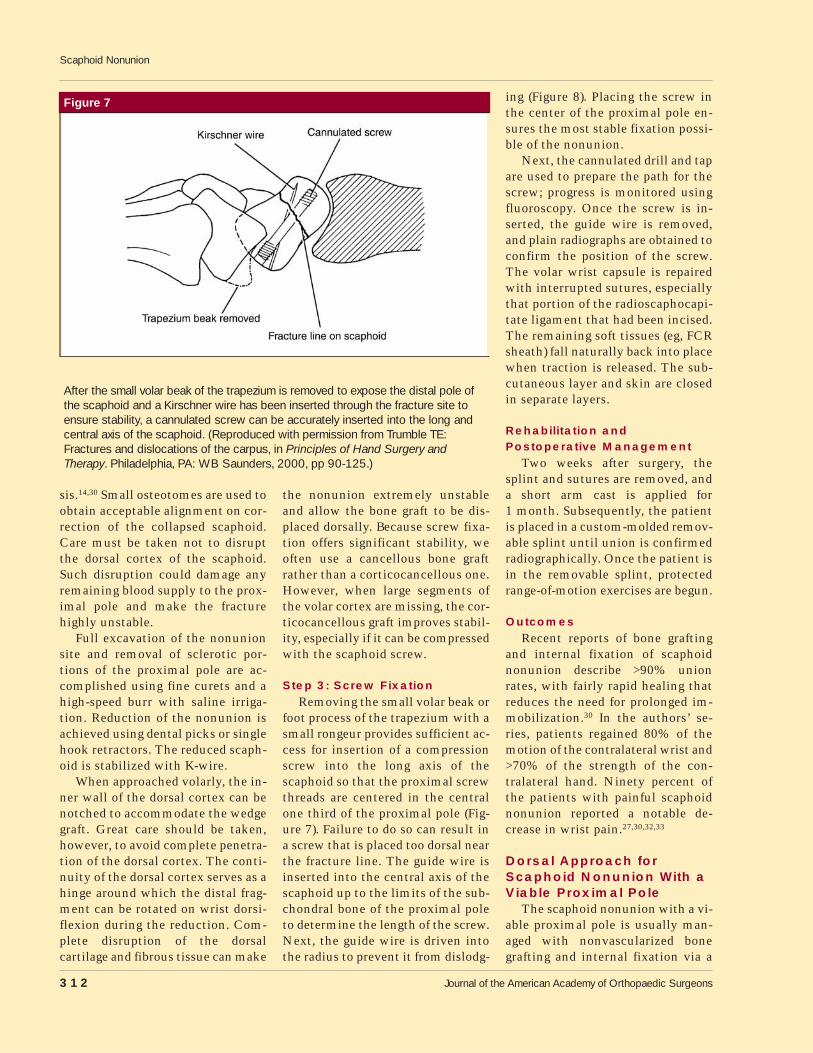
Absence of T1-weighted marrowsignal in proximal fragments indi-cates osteonecrosis (Figure 4, A),empty bone lacunae, and poor up-take of fluorescent bone labels on bi-opsy.19 In contrast, retention of someproximal pole signal has been associ-ated with viable bone when exam-ined histologically, as well as withnormal uptake of fluorescent labels(Figure 4, B). Vascularized bone graft(VBG) is recommended when os-teonecrosis of the proximal pole isevident on MRI.1,13,19-23
Three techniques are recom-mended for surgical correction ofscaphoid nonunion with bone graftand internal fixation with a screw:volar, dorsal, and dorsoradial. For
scaphoid waist nonunion with a vi-able proximal pole, the volar ap-proach is used with interpositionalwedge or inlay bone graft and screwfixation. The dorsal approach withinlay bone graft and screw fixationor a dorsoradial approach with VBGand screw fixation can be used forproximal pole nonunion with os-teonecrosis of the proximal pole.
Volar Approach forScaphoid Waist NonunionWith a Viable Proximal Pole
The volar approach is widely usedfor bone grafting and internal fixationof scaphoid waist nonunion. This ap-proach allows access to the distal onethird and waist of the scaphoid fornonvascularized bone grafting andretrograde internal fixation, as wellas for correction of the humpback de-formity that can result after scaphoidcollapse. The volar approach alsohelps preserve the remaining dorsalblood supply. This approach is notrecommended for nonunion of theproximal pole. Nonunion of the prox-imal pole of the scaphoid, with orwithout osteonecrosis, should be ad-dressed via a dorsal approach.
Figure 1
Osteonecrosis No osteonecrosis
Vascularizedbone graft +
dorsal approach
Dorsalapproach
Waist
Scaphoidnonunion
Proximal
Osteonecrosis No osteonecrosis
Vascularizedbone graft +
dorsal approach
Volar approach
Treatment algorithm for scaphoid nonunion. (Adapted from Knoll VD, Trumble TE:Scaphoid fractures and nonunions, in Trumble TE [ed]: Hand Surgery Update 3.Rosemont, IL: American Academy of Orthopaedic Surgeons, 2003, pp 161-173.)
Figure 2
Sagittal CT scan demonstrating theexact location of the nonunion site overthe proximal pole of the scaphoid.Knowing the precise site of nonunionhelps in determining the surgicalapproach.
Thanapong Waitayawinyu, MD, et al
Volume 15, Number 5, May 2007 309
SurgicalSetup/Instrumentation
General anesthesia is used rou-tinely and is necessary when plan-ning to harvest bone graft from theiliac crest. The patient is positioned
supine with the surgical extremityon a radiolucent arm table. The armis cleansed with antimicrobial solu-tion and draped sterilely. Exsan-guination is performed with anEsmarch bandage and an inflated
upper arm tourniquet.Standard screw fixation sets are
used. Currently popular screws in-clude the Herbert and Herbert-Whipple screw (Zimmer, Warsaw,IN), the Asnis III cannulated screw
Figure 3
A, The lateral intrascaphoid angle, viewed on sagittal CT scan, helps to precisely identify the magnitude of collapse andangulation of the scaphoid. B, The extent of collapse and angulation of scaphoid nonunion can be accurately defined bymeasuring the height-to-length ratio on the CT scan. (Panel A reproduced with permission from Trumble TE: Fractures anddislocations of the carpus, in Principles of Hand Surgery and Therapy. Philadelphia, PA: WB Saunders, 2000, pp 90-125. PanelB reproduced with permission from Trumble TE, Gilbert M, Murray LW, Smith J, Rafijah G, McCallister WV: Displaced scaphoidfractures treated with open reduction and internal fixation with a cannulated screw. J Bone Joint Surg Am 2000;82:633-641.)
Figure 4
A, Coronal T1-weighted MRI scan demonstrating decreased signal in the proximal fragment, which indicates osteonecrosis ofthe proximal pole of the scaphoid. B, Coronal T1-weighted MRI scan demonstrating increased signal in both the distal and theproximal fragment of the scaphoid, which indicates good vascularity of the proximal pole.
Scaphoid Nonunion
310 Journal of the American Academy of Orthopaedic Surgeons
(Stryker, Mahwah, NJ), the Acutrakscrew (Acumed, Beaverton, OR), andthe AO/ASIF screw (Synthes, Paoli,PA), all of which generate interfrag-mentary compression and providesignificant stable internal fixationfor bone graft and fracture.24-30
We favor dental picks over Kirsch-ner wire (K-wire) joysticks to avoidpropagation and comminution in thefracture fragments during scaphoidnonunion reduction. Small osteo-tomes are used to wedge the collapsedscaphoid into its correct alignmentand to resect sclerotic bone from thenonunion edges of the proximal anddistal fragment. K-wires may be usedto prevent rotation of fragments dur-ing drilling. A high-speed burr andfine curets are used to completely ex-cavate the nonunion site and to re-
move sclerotic portions of the prox-imal pole. A fluoroscopy unit is usedto monitor the accuracy of fracture re-duction and to confirm the positionof the guide wire and screw.
Step 1: ExposureA standard Russe incision is
made along the course of the flexorcarpi radialis (FCR) tendon and ex-tending distally along the border ofthe glabrous skin of the thenar emi-nence ( video, Palmar Approach).The incision is extended distally tothe level of the scaphotrapezial jointin preparation for screw insertion,starting in the distal pole of thescaphoid (Figure 5). Splitting thesheath of the FCR allows it to be re-tracted ulnarly and protects the vo-lar cutaneous branch of the mediannerve. The deep branch of the radialartery to the volar arch is retractedradially. The volar carpal ligaments(ie, radioscaphocapitate; occasional-ly, the long radiolunate ligament) areincised longitudinally to expose thedistal pole and waist of the scaphoid(Figure 6). The fracture is evident at
the proximal margin of this incision.It is important to preserve as muchas possible of the radioscaphocapi-tate ligament because this ligamenthelps to contain the proximal poleand prevent it from translating orsubluxating volarly.30,31 When usingcannulated screws (rather than thestandard compression jigs), it is notnecessary to freely divide the radio-scaphocapitate ligament.
In the patient with nascent non-union (ie, nondisplaced scaphoidfracture that does not show adequatehealing after 3 months of properimmobilization), a volar limitedapproach may be used. The limitedRusse approach is used to expose thescaphotrapeziotrapezoid joint. Thevolar beak of the trapezium is re-moved, followed by percutaneousscrew fixation with bone grafting.
Step 2: Correction ofHumpback Deformity
The humpback deformity mustbe corrected to allow stable screwfixation in the long axis of thescaphoid and to prevent arthro-
Figure 5
A standard Russe incision is drawnalong the course of the flexor carpiradialis, extending along the border ofthe thenar eminence distally to thescaphotrapeziotrapezoid joint.(Reproduced with permission fromTrumble TE: Fractures and dislocationsof the carpus, in Principles of HandSurgery and Therapy. Philadelphia, PA:WB Saunders, 2000, pp 90-125.)
Figure 6
Via the volar approach, the scaphoid waist, distal pole of the scaphoid, andscaphotrapeziotrapezoid joint are exposed through the floor of the flexor carpiradialis (FCR) sheath and distal to the pronator quadratus (PQ) after ulnar retractionof the FCR tendon and radial retraction of the deep branch of the radial artery.R = radius, S = scaphoid, Tz = trapezium. (Reproduced with permission fromTrumble TE: Fractures and dislocations of the carpus, in Principles of Hand Surgeryand Therapy. Philadelphia, PA: WB Saunders, 2000, pp 90-125.)
Thanapong Waitayawinyu, MD, et al
Volume 15, Number 5, May 2007 311
sis.14,30 Small osteotomes are used toobtain acceptable alignment on cor-rection of the collapsed scaphoid.Care must be taken not to disruptthe dorsal cortex of the scaphoid.Such disruption could damage anyremaining blood supply to the prox-imal pole and make the fracturehighly unstable.
Full excavation of the nonunionsite and removal of sclerotic por-tions of the proximal pole are ac-complished using fine curets and ahigh-speed burr with saline irriga-tion. Reduction of the nonunion isachieved using dental picks or singlehook retractors. The reduced scaph-oid is stabilized with K-wire.
When approached volarly, the in-ner wall of the dorsal cortex can benotched to accommodate the wedgegraft. Great care should be taken,however, to avoid complete penetra-tion of the dorsal cortex. The conti-nuity of the dorsal cortex serves as ahinge around which the distal frag-ment can be rotated on wrist dorsi-flexion during the reduction. Com-plete disruption of the dorsalcartilage and fibrous tissue can make
the nonunion extremely unstableand allow the bone graft to be dis-placed dorsally. Because screw fixa-tion offers significant stability, weoften use a cancellous bone graftrather than a corticocancellous one.However, when large segments ofthe volar cortex are missing, the cor-ticocancellous graft improves stabil-ity, especially if it can be compressedwith the scaphoid screw.
Step 3: Screw FixationRemoving the small volar beak or
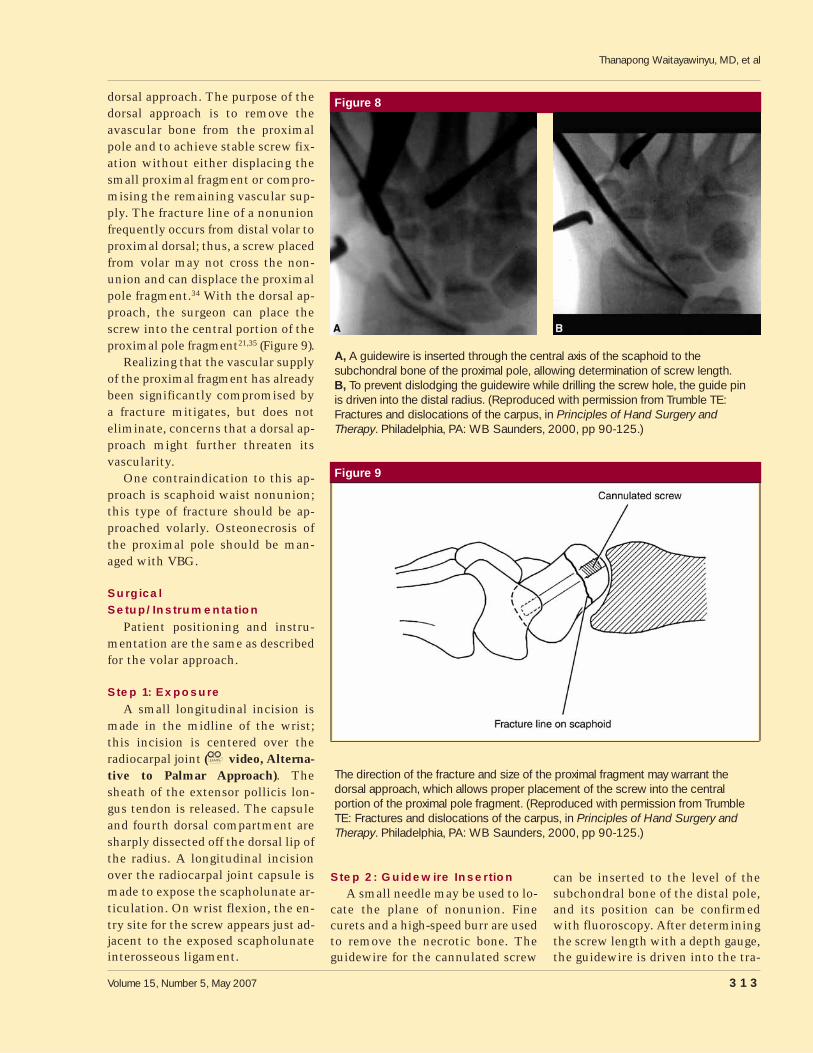
foot process of the trapezium with asmall rongeur provides sufficient ac-cess for insertion of a compressionscrew into the long axis of thescaphoid so that the proximal screwthreads are centered in the centralone third of the proximal pole (Fig-ure 7). Failure to do so can result ina screw that is placed too dorsal nearthe fracture line. The guide wire isinserted into the central axis of thescaphoid up to the limits of the sub-chondral bone of the proximal poleto determine the length of the screw.Next, the guide wire is driven intothe radius to prevent it from dislodg-
ing (Figure 8). Placing the screw inthe center of the proximal pole en-sures the most stable fixation possi-ble of the nonunion.
Next, the cannulated drill and tapare used to prepare the path for thescrew; progress is monitored usingfluoroscopy. Once the screw is in-serted, the guide wire is removed,and plain radiographs are obtained toconfirm the position of the screw.The volar wrist capsule is repairedwith interrupted sutures, especiallythat portion of the radioscaphocapi-tate ligament that had been incised.The remaining soft tissues (eg, FCRsheath) fall naturally back into placewhen traction is released. The sub-cutaneous layer and skin are closedin separate layers.
Rehabilitation andPostoperative Management
Two weeks after surgery, thesplint and sutures are removed, anda short arm cast is applied for1 month. Subsequently, the patientis placed in a custom-molded remov-able splint until union is confirmedradiographically. Once the patient isin the removable splint, protectedrange-of-motion exercises are begun.
OutcomesRecent reports of bone grafting
and internal fixation of scaphoidnonunion describe >90% unionrates, with fairly rapid healing thatreduces the need for prolonged im-mobilization.30 In the authors’ se-ries, patients regained 80% of themotion of the contralateral wrist and>70% of the strength of the con-tralateral hand. Ninety percent ofthe patients with painful scaphoidnonunion reported a notable de-crease in wrist pain.27,30,32,33
Dorsal Approach forScaphoid Nonunion With aViable Proximal Pole
The scaphoid nonunion with a vi-able proximal pole is usually man-aged with nonvascularized bonegrafting and internal fixation via a
Figure 7
After the small volar beak of the trapezium is removed to expose the distal pole ofthe scaphoid and a Kirschner wire has been inserted through the fracture site toensure stability, a cannulated screw can be accurately inserted into the long andcentral axis of the scaphoid. (Reproduced with permission from Trumble TE:Fractures and dislocations of the carpus, in Principles of Hand Surgery andTherapy. Philadelphia, PA: WB Saunders, 2000, pp 90-125.)
Scaphoid Nonunion
312 Journal of the American Academy of Orthopaedic Surgeons
dorsal approach. The purpose of thedorsal approach is to remove theavascular bone from the proximalpole and to achieve stable screw fix-ation without either displacing thesmall proximal fragment or compro-mising the remaining vascular sup-ply. The fracture line of a nonunionfrequently occurs from distal volar toproximal dorsal; thus, a screw placedfrom volar may not cross the non-union and can displace the proximalpole fragment.34 With the dorsal ap-proach, the surgeon can place thescrew into the central portion of theproximal pole fragment21,35 (Figure 9).
Realizing that the vascular supplyof the proximal fragment has alreadybeen significantly compromised bya fracture mitigates, but does noteliminate, concerns that a dorsal ap-proach might further threaten itsvascularity.
One contraindication to this ap-proach is scaphoid waist nonunion;this type of fracture should be ap-proached volarly. Osteonecrosis ofthe proximal pole should be man-aged with VBG.
SurgicalSetup/Instrumentation
Patient positioning and instru-mentation are the same as describedfor the volar approach.
Step 1: Exposure
A small longitudinal incision ismade in the midline of the wrist;this incision is centered over theradiocarpal joint ( video, Alterna-tive to Palmar Approach). Thesheath of the extensor pollicis lon-gus tendon is released. The capsuleand fourth dorsal compartment aresharply dissected off the dorsal lip ofthe radius. A longitudinal incisionover the radiocarpal joint capsule ismade to expose the scapholunate ar-ticulation. On wrist flexion, the en-try site for the screw appears just ad-jacent to the exposed scapholunateinterosseous ligament.
Step 2: Guidewire InsertionA small needle may be used to lo-
cate the plane of nonunion. Finecurets and a high-speed burr are usedto remove the necrotic bone. Theguidewire for the cannulated screw
can be inserted to the level of thesubchondral bone of the distal pole,and its position can be confirmedwith fluoroscopy. After determiningthe screw length with a depth gauge,the guidewire is driven into the tra-
Figure 8
A, A guidewire is inserted through the central axis of the scaphoid to thesubchondral bone of the proximal pole, allowing determination of screw length.B, To prevent dislodging the guidewire while drilling the screw hole, the guide pinis driven into the distal radius. (Reproduced with permission from Trumble TE:Fractures and dislocations of the carpus, in Principles of Hand Surgery andTherapy. Philadelphia, PA: WB Saunders, 2000, pp 90-125.)
Figure 9
The direction of the fracture and size of the proximal fragment may warrant thedorsal approach, which allows proper placement of the screw into the centralportion of the proximal pole fragment. (Reproduced with permission from TrumbleTE: Fractures and dislocations of the carpus, in Principles of Hand Surgery andTherapy. Philadelphia, PA: WB Saunders, 2000, pp 90-125.)
Thanapong Waitayawinyu, MD, et al
Volume 15, Number 5, May 2007 313

pezium to prevent it from being dis-lodged during drilling and tapping(Figure 10). Often, a second K-wire isplaced to prevent rotation or dis-placement of the proximal pole frag-ment during screw insertion.
Step 3: Screw FixationAfter the guidewire is driven up
into the trapezium, the path of thescrew is prepared by drilling and tap-ping. The screw can be inserted ei-ther freehand or by using theguidewire. In small proximal polefragments, we prefer to remove theguide wire and insert a noncannulat-ed Herbert screw (Zimmer) becauseit leaves a smaller defect (footprint)in the cartilage of the proximal pole.The capsule is closed with absorb-able sutures. The third dorsal com-partment is not repaired, and thesubcutaneous tissue and skin areclosed in subsequent layers.
Rehabilitation andPostoperative Management
Generally, we use the same post-operative management protocol aswith the volar approach.
Outcomes
The prognosis for the patient withproximal pole nonunion is moreguarded than for the patient withscaphoid waist nonunion. The timeto union is 2 to 3 months longer forproximal pole nonunion. For the pa-tient with nonunion of the proximalpole, there is a reported union rate of67%, versus a union rate of 87% forscaphoid waist nonunion.36
Dorsal Approach WithVascularized Bone Graftfor Scaphoid NonunionWith Osteonecrosis of theProximal Pole
Evolution of VascularizedGraft
Healing of proximal pole scaphoidnonunion can be achieved with sta-ble internal fixation and bone graft-ing.32,34 The rate of healing correlatesdirectly with the vascularity of theproximal pole.37 Unfortunately, fi-brous union and persistent non-union tend to develop when os-teonecrosis of the proximal pole ispresent. Such conditions are often
refractory to traditional bone graft-ing methods, even when augmentedwith internal fixation. Theoretically,the use of pedicled VBGs, whichhelp revascularize ischemic bone,should improve the union rate andtime to union.22 A recent meta-analysis of treatment of scaphoidnonunion with osteonecrosis of theproximal pole indicated an 88%union rate with a VBG, comparedwith a 47% union rate with non-vascularized bone graft.36
Early vascularized grafts were of-ten based on a pedicle from the pro-nator quadratus insertion on the dis-tal radius.38,39 Recently, several VBGsources have been described, includ-ing the ulnar artery,40 the volar car-pal artery,41,42 vascularized periostealflaps of the distal radius,20,43 thecapsular-based flap vascularizedgraft,23 a combination of inlay corti-cocancellous bone graft with implan-tation of the second dorsal inter-metacarpal artery,44 and even a freevascularized graft from the iliaccrest.45 At present, the most fre-quently used donor sites include thedorsoradial aspect of the distal radius(first described by Zaidemberg et al46)and the second metacarpal graft.21,47
The VBG described by Zaidem-berg, the technique presented in thisarticle, relies on the superior retinac-ular branch of the radial artery,46
which Sheetz et al48 have definedas the 1,2 intercompartmental su-praretinacular artery (1,2 ICSRA).This artery travels in a distal-to-proximal direction along the retinac-ulum between the tendons of thefirst and second dorsal compart-ment. The 2,3 ICSRA may also beused in select patients in whom the1,2 ICSRA is small or absent. Thesevascularized grafts can be harvestedthrough the same dorsal approachused for internal fixation of thescaphoid nonunion.
Indications for the use of VBG in-clude scaphoid waist or proximal polenonunion with associated osteonecro-sis. The primary contraindication isthe presence of a viable proximal pole,
Figure 10
Dorsal approach to the proximal pole of the scaphoid. A, The guidewire for thecannulated screw is inserted to the subchondral bone of the distal pole todetermine screw length. Its position is confirmed with fluoroscopy. B, The guidewireis driven into the trapezium to prevent it from being dislodged during screw holepreparation.
Scaphoid Nonunion
314 Journal of the American Academy of Orthopaedic Surgeons

as demonstrated on MRI. As with thescaphoid waist fracture, the procedureis also contraindicated in the presenceof severe concomitant arthroses(SNAC stage II or greater).
SurgicalSetup/Instrumentation
Surgical setup and patient prepa-ration are the same as described pre-viously. However, microsurgical in-struments, including vessel loopsand special bone tamps, are neededfor harvesting the small vascularpedicle grafts.
Step 1: ExposureThe dorsoradial approach, an ex-
tension of the dorsal approach forthe viable proximal pole, allowsgraft harvesting as well as exposureof the scaphoid nonunion (Figure 11;
video, Vascularized Bone Graft).The midline incision over the dorsalaspect of the wrist curves proximal-ly and radially over the interval be-tween the first and second dorsalcompartments. The third dorsalcompartment is released, and the ex-tensor pollicis longus tendon is re-tracted radially. The sensory branchof the radial nerve is identified exit-ing from between the brachioradialisand the extensor carpi radialis lon-gus muscles. The extensor carpi ra-
dialis longus is retracted ulnarly.The 1,2 ICSRA is visible as a thin redline in the groove between the firstand second dorsal compartments.The vessel takes off distally from theradius and pierces the volar wall ofthe first dorsal compartment. Thefirst dorsal compartment is releasedalong its volar surface, and the ten-dons are retracted. The arterial pedi-cle is mobilized by making parallelincisions in the periosteum betweenthe two compartments, tracing thecourse of the artery from distal toproximal. After preparing a 2.0- to2.5-cm pedicle, the periosteumaround the planned donor site is in-cised as an ellipse or rectangle. Afine oscillating saw, with constantirrigation, is used to cut the threesides of the graft, excluding the sideunder the vascular pedicle. Small os-teotomes are used to complete graftelevation (Figure 12).
Step 2: Graft PlacementPreparation of the scaphoid non-
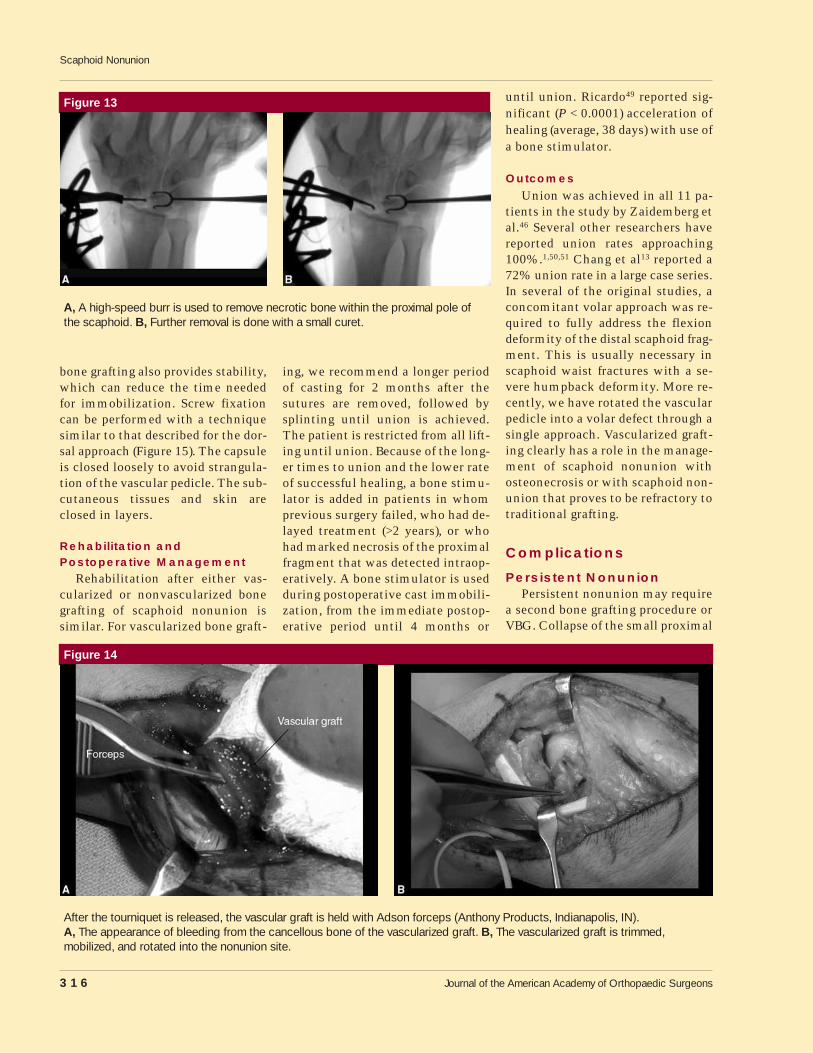
union site and complete removal ofnecrotic bone can be done with finecurets and a high-speed burr, guidedby fluoroscopic imaging (Figure 13).After preparation of the nonunionsite, the tourniquet is released to ob-serve bleeding from the graft. Thevascularized graft is then rotated
into the defect and secured with ei-ther K-wires or a screw (Figure 14).
Step 3: Screw Fixationand Closure
Screw fixation in combinationwith bone grafting has significantlybetter union rates (P = 0.004) thanK-wire fixation in combination withbone grafting.13 Screw fixation with
Figure 11
The dorsoradial incision for the dorsalapproach to the nonunion site of thescaphoid is drawn, including harvestingVBG from the distal radius. Proximaland radial extension of the midlineincision over the dorsal aspect of thewrist is demonstrated.
Figure 12
A, Intraoperative photograph demonstrating the parallel incisions in the periosteum between the first and second extensorcompartments, tracing the course of the 1,2 ICSRA from distal to proximal. This incision is used to mobilize the arterial pedicle.B, The three sides of the graft (excluding the side under the vascular pedicle) are cut by a fine oscillating saw. The graft iselevated completely using small osteotomes.
Thanapong Waitayawinyu, MD, et al
Volume 15, Number 5, May 2007 315
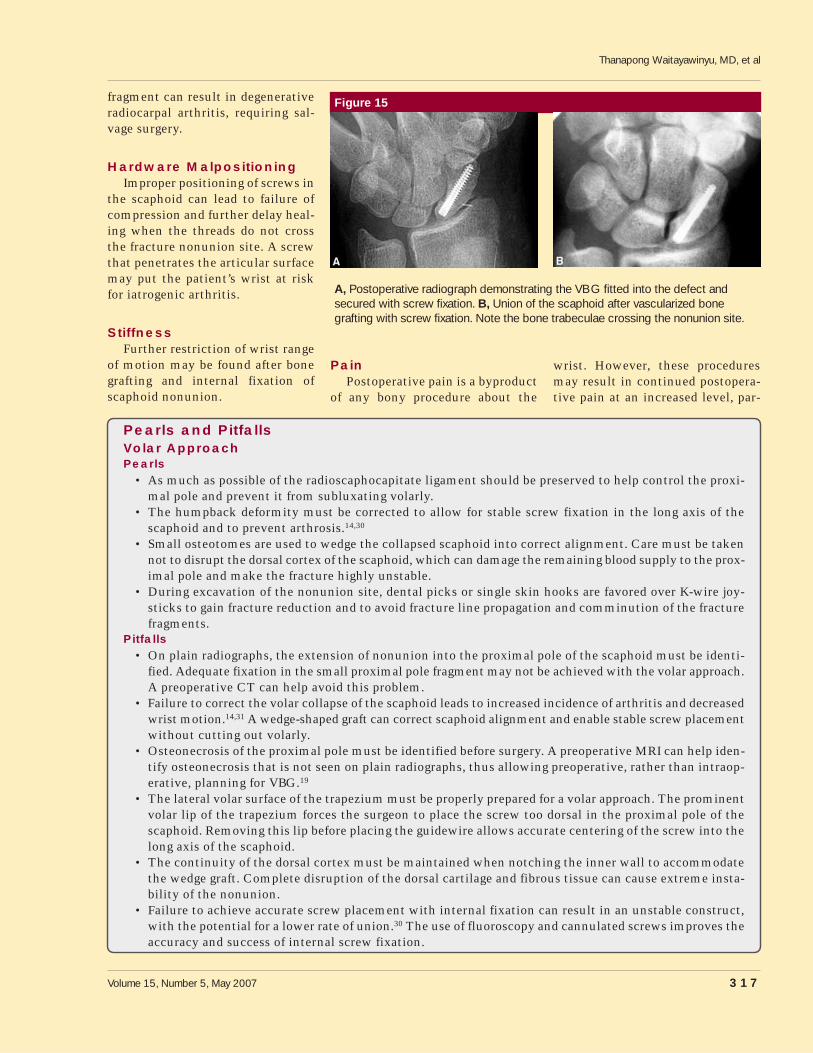
bone grafting also provides stability,which can reduce the time neededfor immobilization. Screw fixationcan be performed with a techniquesimilar to that described for the dor-sal approach (Figure 15). The capsuleis closed loosely to avoid strangula-tion of the vascular pedicle. The sub-cutaneous tissues and skin areclosed in layers.
Rehabilitation andPostoperative Management
Rehabilitation after either vas-cularized or nonvascularized bonegrafting of scaphoid nonunion issimilar. For vascularized bone graft-
ing, we recommend a longer periodof casting for 2 months after thesutures are removed, followed bysplinting until union is achieved.The patient is restricted from all lift-ing until union. Because of the long-er times to union and the lower rateof successful healing, a bone stimu-lator is added in patients in whomprevious surgery failed, who had de-layed treatment (>2 years), or whohad marked necrosis of the proximalfragment that was detected intraop-eratively. A bone stimulator is usedduring postoperative cast immobili-zation, from the immediate postop-erative period until 4 months or
until union. Ricardo49 reported sig-nificant (P < 0.0001) acceleration ofhealing (average, 38 days) with use ofa bone stimulator.
Outcomes
Union was achieved in all 11 pa-tients in the study by Zaidemberg etal.46 Several other researchers havereported union rates approaching100%.1,50,51 Chang et al13 reported a72% union rate in a large case series.In several of the original studies, aconcomitant volar approach was re-quired to fully address the flexiondeformity of the distal scaphoid frag-ment. This is usually necessary inscaphoid waist fractures with a se-vere humpback deformity. More re-cently, we have rotated the vascularpedicle into a volar defect through asingle approach. Vascularized graft-ing clearly has a role in the manage-ment of scaphoid nonunion withosteonecrosis or with scaphoid non-union that proves to be refractory totraditional grafting.
Complications
Persistent NonunionPersistent nonunion may require
a second bone grafting procedure orVBG. Collapse of the small proximal
Figure 13
A, A high-speed burr is used to remove necrotic bone within the proximal pole ofthe scaphoid. B, Further removal is done with a small curet.
Figure 14
After the tourniquet is released, the vascular graft is held with Adson forceps (Anthony Products, Indianapolis, IN).A, The appearance of bleeding from the cancellous bone of the vascularized graft. B, The vascularized graft is trimmed,mobilized, and rotated into the nonunion site.
Scaphoid Nonunion
316 Journal of the American Academy of Orthopaedic Surgeons
fragment can result in degenerativeradiocarpal arthritis, requiring sal-vage surgery.
Hardware MalpositioningImproper positioning of screws in
the scaphoid can lead to failure ofcompression and further delay heal-ing when the threads do not crossthe fracture nonunion site. A screwthat penetrates the articular surfacemay put the patient’s wrist at riskfor iatrogenic arthritis.
StiffnessFurther restriction of wrist range
of motion may be found after bonegrafting and internal fixation ofscaphoid nonunion.
PainPostoperative pain is a byproduct
of any bony procedure about the
wrist. However, these proceduresmay result in continued postopera-tive pain at an increased level, par-
Figure 15
A, Postoperative radiograph demonstrating the VBG fitted into the defect andsecured with screw fixation. B, Union of the scaphoid after vascularized bonegrafting with screw fixation. Note the bone trabeculae crossing the nonunion site.
Pearls and PitfallsVolar ApproachPearls
• As much as possible of the radioscaphocapitate ligament should be preserved to help control the proxi-mal pole and prevent it from subluxating volarly.
• The humpback deformity must be corrected to allow for stable screw fixation in the long axis of thescaphoid and to prevent arthrosis.14,30
• Small osteotomes are used to wedge the collapsed scaphoid into correct alignment. Care must be takennot to disrupt the dorsal cortex of the scaphoid, which can damage the remaining blood supply to the prox-imal pole and make the fracture highly unstable.
• During excavation of the nonunion site, dental picks or single skin hooks are favored over K-wire joy-sticks to gain fracture reduction and to avoid fracture line propagation and comminution of the fracturefragments.
Pitfalls• On plain radiographs, the extension of nonunion into the proximal pole of the scaphoid must be identi-
fied. Adequate fixation in the small proximal pole fragment may not be achieved with the volar approach.A preoperative CT can help avoid this problem.
• Failure to correct the volar collapse of the scaphoid leads to increased incidence of arthritis and decreasedwrist motion.14,31 A wedge-shaped graft can correct scaphoid alignment and enable stable screw placementwithout cutting out volarly.
• Osteonecrosis of the proximal pole must be identified before surgery. A preoperative MRI can help iden-tify osteonecrosis that is not seen on plain radiographs, thus allowing preoperative, rather than intraop-erative, planning for VBG.19
• The lateral volar surface of the trapezium must be properly prepared for a volar approach. The prominentvolar lip of the trapezium forces the surgeon to place the screw too dorsal in the proximal pole of thescaphoid. Removing this lip before placing the guidewire allows accurate centering of the screw into thelong axis of the scaphoid.
• The continuity of the dorsal cortex must be maintained when notching the inner wall to accommodatethe wedge graft. Complete disruption of the dorsal cartilage and fibrous tissue can cause extreme insta-bility of the nonunion.
• Failure to achieve accurate screw placement with internal fixation can result in an unstable construct,with the potential for a lower rate of union.30 The use of fluoroscopy and cannulated screws improves theaccuracy and success of internal screw fixation.
Thanapong Waitayawinyu, MD, et al
Volume 15, Number 5, May 2007 317
ticularly when surgery to correctnonunion is performed in the rela-tively asymptomatic patient.
Nerve InjuryIn the volar surgical approach, the
median nerve and its volar cutane-ous branch are at risk for injury. Inthe dorsal approach, especially when
harvesting a dorsoradial VBG, the ra-dial sensory nerve is at risk.
Summary
Surgical techniques for the manage-ment of scaphoid nonunion aremuch more demanding than thosefor acute fracture because they must
address anatomic changes, such asbone resorption, carpal collapse, andosteonecrosis. The location of thenonunion site and viability of theproximal fragment are the criticalfactors in determining surgical ap-proach.
Scaphoid waist nonunion with-out osteonecrosis warrants the volar
Dorsal Approach for Scaphoid Nonunion With a Viable Proximal PolePearls
• Care should be taken to preserve the tissue on the dorsal ridge of the scaphoid in an attempt to preserveas much as possible of the remaining scaphoid blood supply, which is already significantly compromisedby the fracture.
• The surgeon should use an insertion point that is close to the scapholunate interosseous ligament attach-ment to the scaphoid. The screw should be targeted distally toward the scaphoid tubercle.
• The screw must be adequately countersunk because insertion is performed in the center of the articu-lar surface of the proximal pole. To avoid problems in countersinking the screw, undersize the screw by3 to 4 mm.
Pitfalls• Failure to identify the exact location of the scaphoid nonunion that extends into the proximal pole can
lead to an incorrect surgical approach.• Failure to identify osteonecrosis of the proximal pole during preoperative planning can result in being un-
prepared for VBG at the time of surgery.• Failure to control the proximal fragment during drilling, tapping, or screw insertion can result in further
displacement of the fracture and lead to inaccurate fixation. Using temporary K-wire fixation to controlrotation can stabilize the nonunion during this process.
Dorsal Approach for Vascularized Bone Graft for Scaphoid Nonunion WithOsteonecrosis of the Proximal PolePearls
• The tissue on the dorsal ridge of the scaphoid should be preserved because of its potential for bringingblood supply to the scaphoid. Implants should be adequately countersunk in the proximal pole of thescaphoid.
• We recommend harvesting the VBG before débriding the scaphoid. This allows the surgeon to gauge thesize of the window in the scaphoid that must be prepared.
• We first inspect for the presence of the artery of Zaidemberg;46 the second dorsal metacarpal artery canbe used as an alternative in ≤5% of patients.
• Additional cancellous bone graft is harvested from the bed of the VBG in the distal radius and is packedinto the crevices of the scaphoid defect before tamping in the VBG.
• When the VBG does not fit into the defect in the scaphoid, our first choice is to enlarge the defect of thescaphoid rather than risk damaging the vascular pedicle by resizing the graft.
• To improve exposure and decrease tension in the vascular pedicle, radial styloidectomy is frequently per-formed.
• The patient with significant deformity and collapse from a long-standing scaphoid waist nonunion withosteonecrosis may require a more complex procedure that entails rotating the VBG along the radial andvolar aspects of the scaphoid after radial styloidectomy. A standard volar wedge graft may be required inaddition to the VBG.
Pitfalls• Failure to identify osteonecrosis of the proximal pole before surgery, to correct the humpback deformi-
ty of the scaphoid, and to accurately place screws used for internal fixation of the scaphoid can result indecreased rates of union.
Scaphoid Nonunion
318 Journal of the American Academy of Orthopaedic Surgeons
approach. The dorsal approach isused to enable bone grafting and ac-curate screw placement for non-union of the proximal pole of thescaphoid. When osteonecrosis of theproximal pole is detected on MRI, aVBG from the distal radius (using adorsoradial approach) is recommend-ed. Correction of humpback defor-mity is best achieved by a volar sur-gical approach with bone graftingand internal fixation using supple-mental K-wire or a compressionscrew. Salvage procedures, such asproximal row carpectomy, scaphoid-ectomy with or without limited in-tercarpal arthrodesis, and total wristfusion, are reserved for the patientwith severe carpal collapse and ar-throsis.
References
Citation numbers printed in boldtype indicate references publishedwithin the past 5 years.
1. Steinmann SP, Bishop AT, Berger RA:Use of the 1,2 intercompartmentalsupraretinacular artery as a vascular-ized pedicle bone graft for difficultscaphoid nonunion. J Hand Surg [Am]2002;27:391-401.
2. Ruby LK, Stinson J, Belsky MR: Thenatural history of scaphoid non-union: A review of fifty-five cases.J Bone Joint Surg Am 1985;67:428-432.
3. Adams BD, Frykman GK, Taleisnik J:Treatment of scaphoid nonunion withcasting and pulsed electromagneticfields: A study continuation. J HandSurg [Am] 1992;17:910-914.
4. Mack GR, Bosse MJ, Gelberman RH,Yu E: The natural history of scaphoidnon-union. J Bone Joint Surg Am1984;66:504-509.
5. Cooney WP, Linscheid RL, DobynsJH, Wood MB: Scaphoid nonunion:Role of anterior interpositional bonegrafts. J Hand Surg [Am] 1988;13:635-650.
6. Fernandez DL: Anterior bone graftingand conventional lag screw fixationto treat scaphoid nonunions. J HandSurg [Am] 1990;15:140-147.
7. Nakamura R, Imaeda T, Tsuge S, Wa-tanabe K: Scaphoid non-union withD.I.S.I. deformity: A survey of clinicalcases with special reference to liga-mentous injury. J Hand Surg [Br]
1991;16:156-161.8. Stark A, Brostrom LA, Svartengren G:
Surgical treatment of scaphoid non-union: Review of the literature and rec-ommendations for treatment. ArchOrthop Trauma Surg 1989;108:203-209.
9. Watson HK, Ballet FL: The SLACwrist: Scapholunate advanced col-lapse pattern of degenerative arthritis.J Hand Surg [Am] 1984;9:358-365.
10. Schuind F, Haentjens P, Van Innis F,Vander Maren C, Garcia-Elias M,Sennwald G: Prognostic factors in thetreatment of carpal scaphoid non-unions. J Hand Surg [Am] 1999;24:761-776.
11. Little CP, Burston BJ, Hopkinson-Woolley J, Burge P: Failure of surgeryfor scaphoid non-union is associatedwith smoking. J Hand Surg [Br] 2006;31:252-255.
12. Nolte PA, van der Krans A, Patka P,Janssen IM, Ryaby JP, Albers GH: Low-intensity pulsed ultrasound in thetreatment of nonunions. J Trauma2001;51:693-702.
13. Chang MA, Bishop AT, Moran SL,Shin AY: The outcomes and complica-tions of 1,2-intercompartmental su-praretinacular artery pedicled vascu-larized bone grafting of scaphoidnonunions. J Hand Surg [Am] 2006;31:387-396.
14. Amadio PC, Berquist TH, Smith DK,Ilstrup DM, Cooney WP III, LinscheidRL: Scaphoid malunion. J Hand Surg[Am] 1989;14:679-687.
15. Bain GI, Bennett JD, MacDermid JC,Slethaug GP, Richards RS, Roth JH:Measurement of the scaphoid hump-back deformity using longitudinalcomputed tomography: Intra- and in-terobserver variability using variousmeasurement techniques. J HandSurg [Am] 1998;23:76-81.
16. Morgan WJ, Breen TF, Coumas JM,Schulz LA: Role of magnetic reso-nance imaging in assessing factors af-fecting healing in scaphoid non-unions. Clin Orthop Relat Res 1997;336:240-246.
17. Perlik PC, Guilford WB: Magnetic res-onance imaging to assess vascularityof scaphoid nonunions. J Hand Surg[Am] 1991;16:479-484.
18. Sakuma M, Nakamura R, Imaeda T:Analysis of proximal fragment sclero-sis and surgical outcome of scaphoidnon-union by magnetic resonance im-aging. J Hand Surg [Br] 1995;20:201-205.
19. Trumble TE: Avascular necrosis afterscaphoid fracture: A correlation ofmagnetic resonance imaging and his-
tology. J Hand Surg [Am] 1990;15:557-564.
20. Dailiana ZH, Malizos KN, Zachos V,Varitimidis SE, Hantes M, KarantanasA: Vascularized bone grafts from thepalmar radius for the treatment ofwaist nonunions of the scaphoid.J Hand Surg [Am] 2006;31:397-404.
21. Mathoulin C, Brunelli F: Further ex-perience with the index metacarpalvascularized bone graft. J Hand Surg[Br] 1998;23:311-317.
22. Shin AY, Bishop AT: Pedicled vascu-larized bone grafts for disorders of thecarpus: Scaphoid nonunion and Kien-bock’s disease. J Am Acad OrthopSurg 2002;10:210-216.
23. Sotereanos DG, Darlis NA, DailianaZH, Sarris IK, Malizos KN: Acapsular-based vascularized distal ra-dius graft for proximal pole scaphoidpseudarthrosis. J Hand Surg [Am]2006;31:580-587.
24. Adla DN, Kitsis C, Miles AW: Com-pression forces generated by Minibone screws: A comparative studydone on bone model. Injury 2005;36:65-70.
25. Bailey CA, Kuiper JH, Kelly CP: Bio-mechanical evaluation of a new com-posite bioresorbable screw. J HandSurg [Br] 2006;31:208-212.
26. Beadel GP, Ferreira L, Johnson JA,King GJ: Interfragmentary compres-sion across a simulated scaphoid frac-ture: Analysis of 3 screws. J HandSurg [Am] 2004;29:273-278.
27. Herbert TJ, Fisher WE: Managementof the fractured scaphoid using a newbone screw. J Bone Joint Surg Br1984;66:114-123.
28. Herbert TJ, Fisher WE, Leicester AW:The Herbert bone screw: A ten yearperspective. J Hand Surg [Br] 1992;17:415-419.
29. Toby EB, Butler TE, McCormack TJ,Jayaraman G: A comparison of fixa-tion screws for the scaphoid duringapplication of cyclical bending loads.J Bone Joint Surg Am 1997;79:1190-1197.
30. Trumble TE, Clarke T, Kreder HJ:Non-union of the scaphoid: Treat-ment with cannulated screws com-pared with treatment with Herbertscrews. J Bone Joint Surg Am 1996;78:1829-1837.
31. Trumble TE, Gilbert M, Murray LW,Smith J, Rafijah G, McCallister WV:Displaced scaphoid fractures treatedwith open reduction and internalfixation with a cannulated screw.J Bone Joint Surg Am 2000;82:633-641.
32. Inoue G, Shionoya K: Herbert screw
Thanapong Waitayawinyu, MD, et al
Volume 15, Number 5, May 2007 319
fixation by limited access for acutefractures of the scaphoid. J Bone JointSurg Br 1997;79:418-421.
33. Tsuyuguchi Y, Murase T, Hidaka N,Ohno H, Kawai H: Anterior wedge-shaped bone graft for old scaphoidfractures or non-unions: An analysisof relevant carpal alignment. J HandSurg [Br] 1995;20:194-200.
34. Robbins RR, Ridge O, Carter PR: Iliaccrest bone grafting and Herbert screwfixation of nonunions of the scaphoidwith avascular proximal poles. JHand Surg [Am] 1995;20:818-831.
35. Yuceturk A, Isiklar ZU, Tuncay C,Tandogan R: Treatment of scaphoidnonunions with a vascularized bonegraft based on the first dorsal metacar-pal artery. J Hand Surg [Br] 1997;22:425-427.
36. Merrell GA, Wolfe SW, Slade JF III:Treatment of scaphoid nonunions:Quantitative meta-analysis of the lit-erature. J Hand Surg [Am] 2002;27:685-691.
37. Green DP: The effect of avascular ne-crosis on Russe bone grafting forscaphoid nonunion. J Hand Surg[Am] 1985;10:597-605.
38. Kawai H, Yamamoto K: Pronatorquadratus pedicled bone graft for oldscaphoid fractures. J Bone Joint SurgBr 1988;70:829-831.
39. Leung PC, Hung LK: Use of pronatorquadratus bone flap in bony recon-struction around the wrist. J HandSurg [Am] 1990;15:637-640.
40. Guimberteau JC, Panconi B: Recalci-trant non-union of the scaphoid treat-ed with a vascularized bone graftbased on the ulnar artery. J BoneJoint Surg Am 1990;72:88-97.
41. Kuhlmann JN, Mimoun M, BoabighiA, Baux S: Vascularized bone graftpedicled on the volar carpal artery fornon-union of the scaphoid. J HandSurg [Br] 1987;12:203-210.
42. Mathoulin C, Haerle M: Vascularizedbone graft from the palmar carpal ar-tery for treatment of scaphoid non-union. J Hand Surg [Br] 1998;23:318-323.
43. Dailiana ZH, Malizos KN, UrbaniakJR: Vascularized periosteal flaps ofdistal forearm and hand. J Trauma2005;58:76-82.
44. Fernandez DL, Eggli S: Non-union ofthe scaphoid: Revascularization of theproximal pole with implantation of avascular bundle and bone-grafting.J Bone Joint Surg Am 1995;77:883-893.
45. Gabl M, Reinhart C, Lutz M, et al:Vascularized bone graft from the iliaccrest for the treatment of nonunion ofthe proximal part of the scaphoid with
an avascular fragment. J Bone JointSurg Am 1999;81:1414-1428.
46. Zaidemberg C, Siebert JW, AngrigianiC: A new vascularized bone graft forscaphoid nonunion. J Hand Surg[Am] 1991;16:474-478.
47. Sawaizumi T, Nanno M, Nanbu A, ItoH: Vascularised bone graft from thebase of the second metacarpal for re-fractory nonunion of the scaphoid.J Bone Joint Surg Br 2004;86:1007-1012.
48. Sheetz KK, Bishop AT, Berger RA: Thearterial blood supply of the distal radi-us and ulna and its potential use invascularized pedicled bone grafts.J Hand Surg [Am] 1995;20:902-914.
49. Ricardo M: The effect of ultrasoundon the healing of muscle-pediculatedbone graft in scaphoid non-union. IntOrthop 2006;30:123-127.
50. Malizos KN, Dailiana ZH, Kirou M,Vragalas V, Xenakis TA, Soucacos PN:Longstanding nonunions of scaphoidfractures with bone loss: Successfulreconstruction with vascularizedbone grafts. J Hand Surg [Br] 2001;26:330-334.
51. Uerpairojkit C, Leechavengvongs S,Witoonchart K: Primary vascularizeddistal radius bone graft for nonunionof the scaphoid. J Hand Surg [Br]2000;25:266-270.
Scaphoid Nonunion
320 Journal of the American Academy of Orthopaedic Surgeons





























