Embed Size (px)
DESCRIPTION
Scottish Surveillance of Healthcare Associated Infection Programme. SURGICAL SITE INFECTION SURVEILLANCE Training to ensure valid and reliable surveillance data. Why are we here?. National SSI surveillance in Scotland Establishing the impact of HAI in Scotland HDL (2001) 57 - PowerPoint PPT Presentation
Citation preview

SURGICAL SITE INFECTION SURVEILLANCE
Training to ensure valid and reliable surveillance data
Scottish Surveillance of HealthcareAssociated Infection Programme
Why are we here?
• National SSI surveillance in Scotland– Establishing the impact of HAI in
Scotland
– HDL (2001) 57
•All acute Divisions must do surveillance of 2 surgical procedures, 1 of which should be orthopaedic
HDL (2006)38• Hip arthroplasty surveillance mandatory from
Jan 2007 if procedure performed within hospital
• Readmission surveillance must be undertaken for this category until day 30 post op
• Caesarean section surveillance mandatory from Jan 2007
• PDS must be undertaken to day 30 post all for all c section procedures
Surveillance is:
• Policing!
• A survey
–Research–Audit
HPS’s Role
• To co-ordinate, facilitate and support the implementation of SSI surveillance
• To prepare Protocols• To prepare data collection tools• To support on-going data
management and ensure quality data
• To collate and report the national data set
Scottish Surveillance of HealthcareAssociated Infection Programme
Today’s climate and demands!• Public awareness!• Quality is at the
heart of everyone’s agenda– Clinical
Governance– Clinical Standards– Accountability
Reviews– Performance
Assessment Framework
HAI - Extent of the problem
• 100, 000 patients affected per year
• 5000 deaths per year
The Cost of HAI
AIM
• To promote accurate completion of surgical site infection surveillance forms
Scottish Surveillance of HealthcareAssociated Infection Programme
Learning Objectives• To recognise the benefits of
surveillance in relation to surgical site infection (SSI)
• To describe the background to SSI surveillance
• To discuss the importance of data definitions
• To evaluate the variety of processes that can be utilised to carry out SSI surveillance
Scottish Surveillance of HealthcareAssociated Infection Programme
Introduction to Surveillance• Surveillance is the ongoing systematic Surveillance is the ongoing systematic
collection, analysis, and interpretation collection, analysis, and interpretation of health data essential to the planning, of health data essential to the planning, implementation, and evaluation of implementation, and evaluation of public health practice, closely integrated public health practice, closely integrated with the timely dissemination of these with the timely dissemination of these data to those who need to know. The data to those who need to know. The final link of the surveillance chain is the final link of the surveillance chain is the application of these data to prevention application of these data to prevention and control. and control.
(Centers for Disease Control and Prevention 1988)(Centers for Disease Control and Prevention 1988)
Introduction to Surveillance
• The objectives of healthcare associated infection (HAI) surveillance are to:– Monitor the incidence of HAI, including SSI
– Provide early warning and investigation of problems and subsequent planning and intervention to control
– Monitor trends, including the detection of outbreaks
– Examine and share the impact of interventions
– Gain information on the quality of care
– Prioritise the allocation of resources
Introduction to Surveillance
• Surveillance is a multidisciplinary activity and local ownership is crucial
• National surveillance should be a by-product of local surveillance
• Local feedback is essential
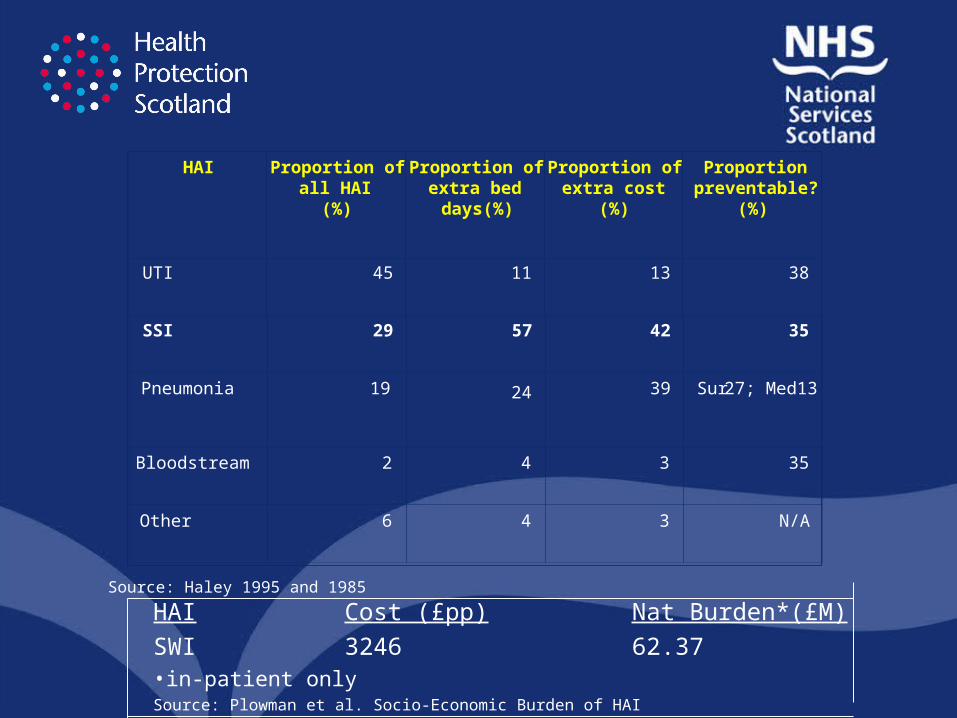
HAI Proportion of all HAI
(%)
Proportion of extra bed days(%)
Proportion of extra cost
(%)
Proportionpreventable?
(%)
UTI 45 11 13 38
SSI 29 57 42 35
Pneumonia 19 24 39 Sur 27; Med13
Bloodstream 2 4 3 35
Other 6 4 3 N/A
Source: Haley 1995 and 1985
HAI Cost (£pp) Nat Burden*(£M)
SWI 3246 62.37•in-patient onlySource: Plowman et al. Socio-Economic Burden of HAI
Background to SSI surveillance – What is the problem?
• Specific operation categories known to have unacceptably high infection rates
• Many factors have been recognised that influence the occurrence of SSI
– Pre operative
– Intra operative
– Post operative
• Surveillance can result in a reduced infection rates but is unlikely to be the only factor:– ICTs– Commitment of all staff– Education on risk
factors/evidence based practice
– Adequate staffing, resources, equipment
– Is there a Hawthorne effect?
Background to SSI Surveillance• SSI is therefore important as it continues to be a key
complication of surgery, with high human and financial costs
• The potential to improve infection rates through surveillance has been proven
• A number of other programmes are already in place:
– NNIS
– SSISS
– PAN CELTIC
– Local projects
• In Scotland: SSHAIP
Scottish SSI Surveillance Programme – the way forward……
• SSI Surveillance Protocol and Resource Pack
• HAI Surveillance newsletter to share good practice
• Communications and visits with all divisions
• Updates to National Steering Group
• Training for those involved…………
Operation Categories for SSI Surveillance
• Orthopaedic: hip replacement, knee replacement, operations for fractured neck of femur
• Cardiac: CABG, other cardiac surgery
• General: breast, major vascular
• Obs/Gyn: abdo hysterectomy, c.section
• Cranial Surgery
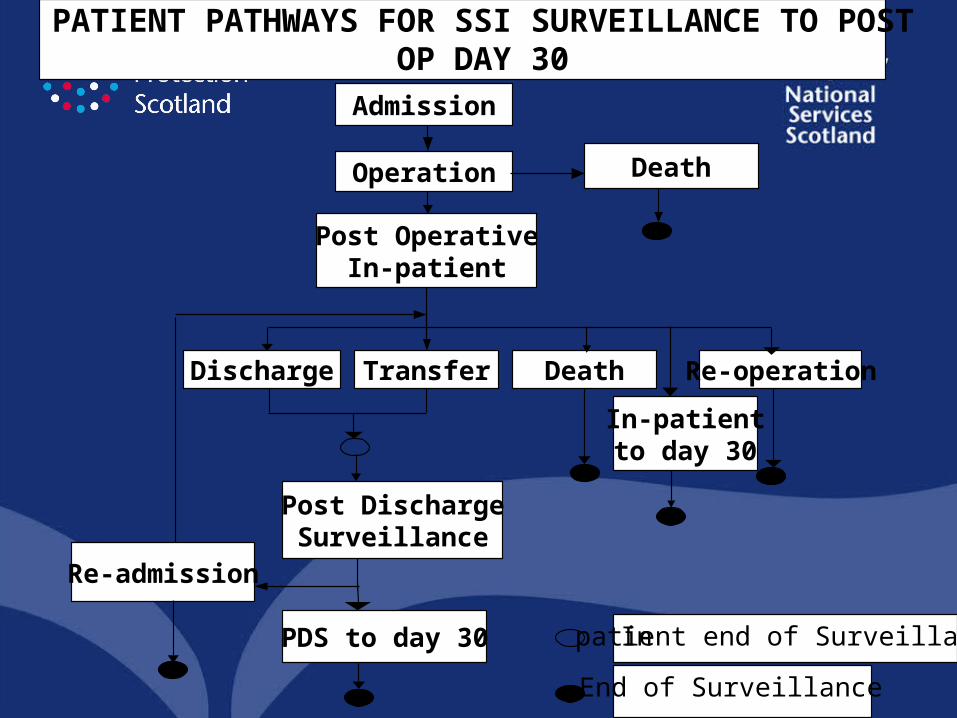
Admission
Operation
Discharge Transfer
Post DischargeSurveillance
Death Re-operation
In-patientto day 30
Post OperativeIn-patient
Death
In-patient end of Surveillance
End of Surveillance
PATIENT PATHWAYS FOR SSI SURVEILLANCE TO POST OP DAY 30
PDS to day 30
Re-admission
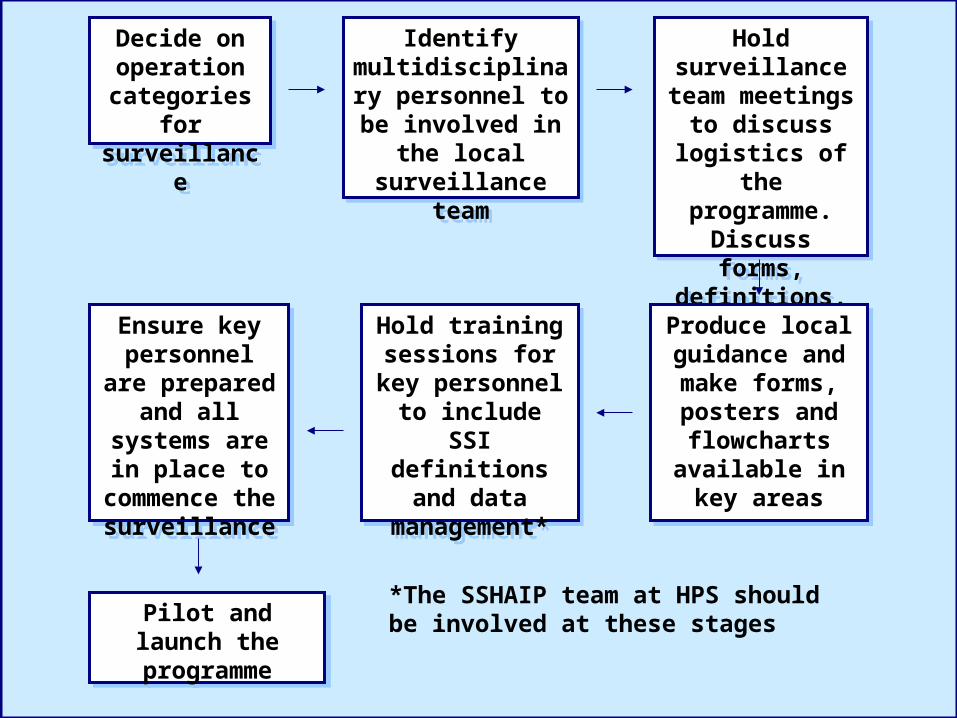
Decide on operation
categories for surveillance
Decide on operation
categories for surveillance
Identify multidisciplinary personnel to be
involved in the local surveillance team
Identify multidisciplinary personnel to be
involved in the local surveillance team
Hold surveillance team meetings to discuss logistics of the programme. Discuss forms,
definitions, dataset, start date
etc.*
Hold surveillance team meetings to discuss logistics of the programme. Discuss forms,
definitions, dataset, start date
etc.*
Produce local guidance and make forms, posters and flowcharts
available in key areas
Produce local guidance and make forms, posters and flowcharts
available in key areas
Hold training sessions for key
personnel to include SSI
definitions and data management*
Hold training sessions for key
personnel to include SSI
definitions and data management*
Ensure key personnel are
prepared and all systems are in
place to commence the surveillance
Ensure key personnel are
prepared and all systems are in
place to commence the surveillance
Pilot and launch the programme
Pilot and launch the programme
*The SSHAIP team at HPS should be involved at these stages
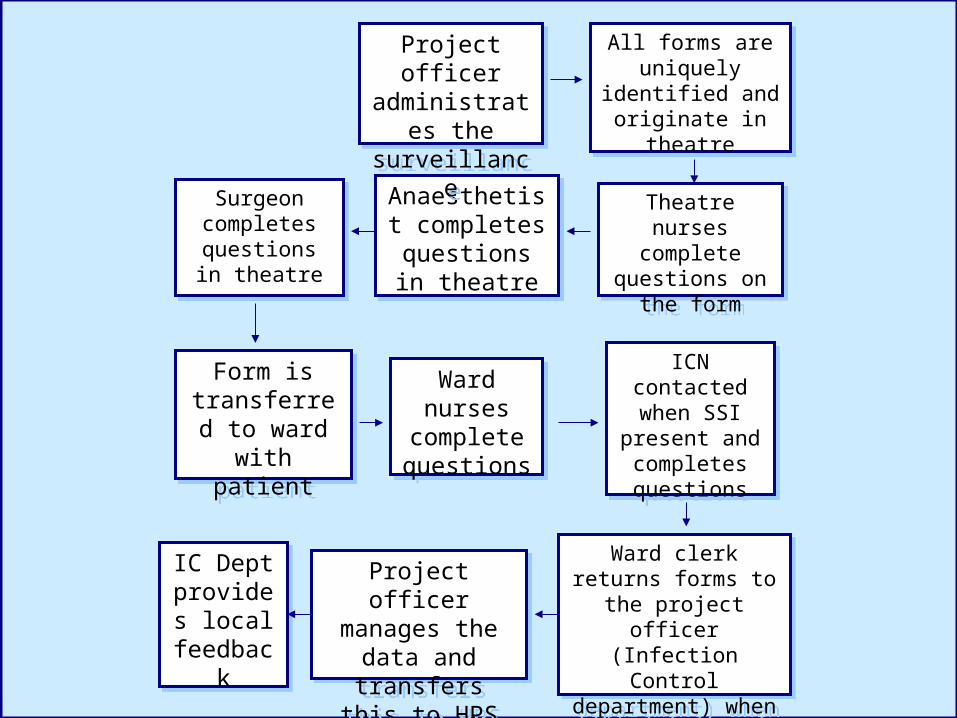
All forms are uniquely identified
and originate in theatre
All forms are uniquely identified
and originate in theatre
Theatre nurses complete questions
on the form
Theatre nurses complete questions
on the form
Anaesthetist completes
questions in theatre
Anaesthetist completes
questions in theatre
Ward clerk returns forms to the project
officer (Infection Control department) when the patient is
discharged
Ward clerk returns forms to the project
officer (Infection Control department) when the patient is
discharged
Project officer manages the data
and transfers this to HPS
Project officer manages the data
and transfers this to HPS
Surgeon completes
questions in theatre
Surgeon completes
questions in theatre
ICN contacted when SSI present
and completes questions
ICN contacted when SSI present
and completes questions
Form is transferred to
ward with patient
Form is transferred to
ward with patient
Ward nurses complete questions
Ward nurses complete questions
Project officer administrates the
surveillance
Project officer administrates the
surveillance
IC Dept provides
local feedback
IC Dept provides
local feedback
Scottish Centre for Infection and Environmental HealthA Division of the Common Services Agency
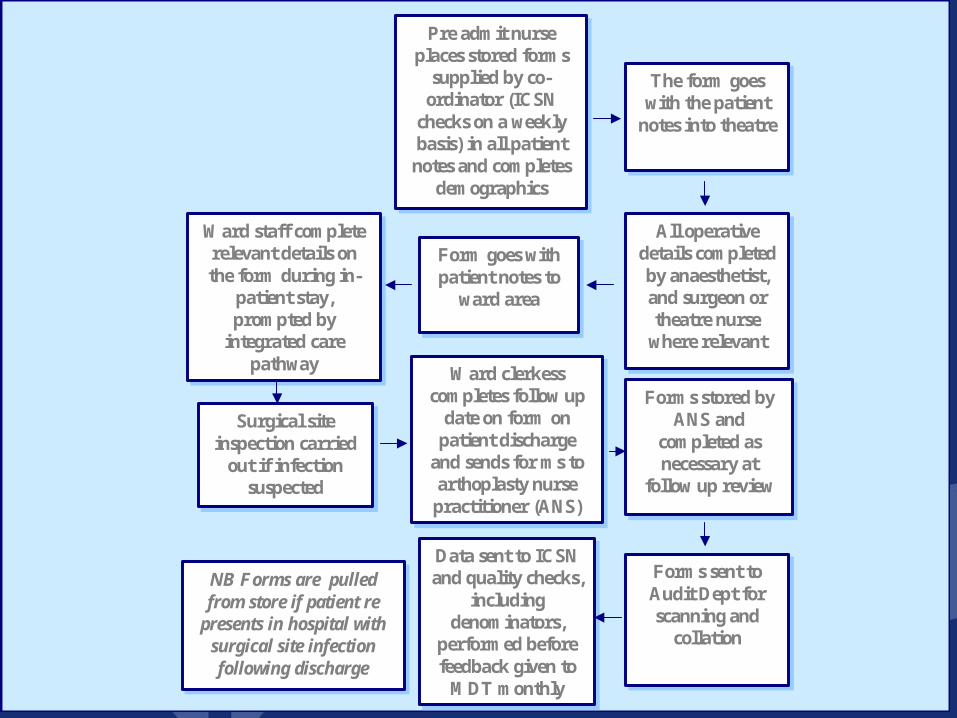
Pre admit nurse places stored forms
supplied by co-ordinator (ICSN
checks on a weekly basis) in all patient
notes and completes demographics
Pre admit nurse places stored forms
supplied by co-ordinator (ICSN
checks on a weekly basis) in all patient notes and completes
demographics
The form goes with the patient
notes into theatre
The form goes with the patient
notes into theatre
All operative details completed by anaesthetist, and surgeon or theatre nurse
where relevant
All operative details completed by anaesthetist, and surgeon or theatre nurse
where relevant
Forms stored by ANS and
completed as necessary at
follow up review
Forms stored by ANS and
completed as necessary at
follow up review
Forms sent to Audit Dept for scanning and
collation
Forms sent to Audit Dept for scanning and
collation
Form goes with patient notes to
ward area
Form goes with patient notes to
ward area
Ward clerkess completes follow up
date on form on patient discharge
and sends for ms to arthoplasty nurse
practitioner (ANS)
Ward clerkess completes follow up
date on form on patient discharge
and sends for ms to arthoplasty nurse practitioner (ANS)
Ward staff complete relevant details on the form during in-
patient stay, prompted by
integrated care pathway
Ward staff complete relevant details on the form during in-
patient stay, prompted by
integrated care pathway
Data sent to ICSN and quality checks,
including denominators,
performed before feedback given to
MDT monthly
Data sent to ICSN and quality checks,
including denominators,
performed before feedback given to
MDT monthly
Surgical site inspection carried
out if infection suspected
Surgical site inspection carried
out if infection suspected
NB Forms are pulled from store if patient re
presents in hospital with surgical site infection following discharge
NB Forms are pulled from store if patient re
presents in hospital with surgical site infection following discharge
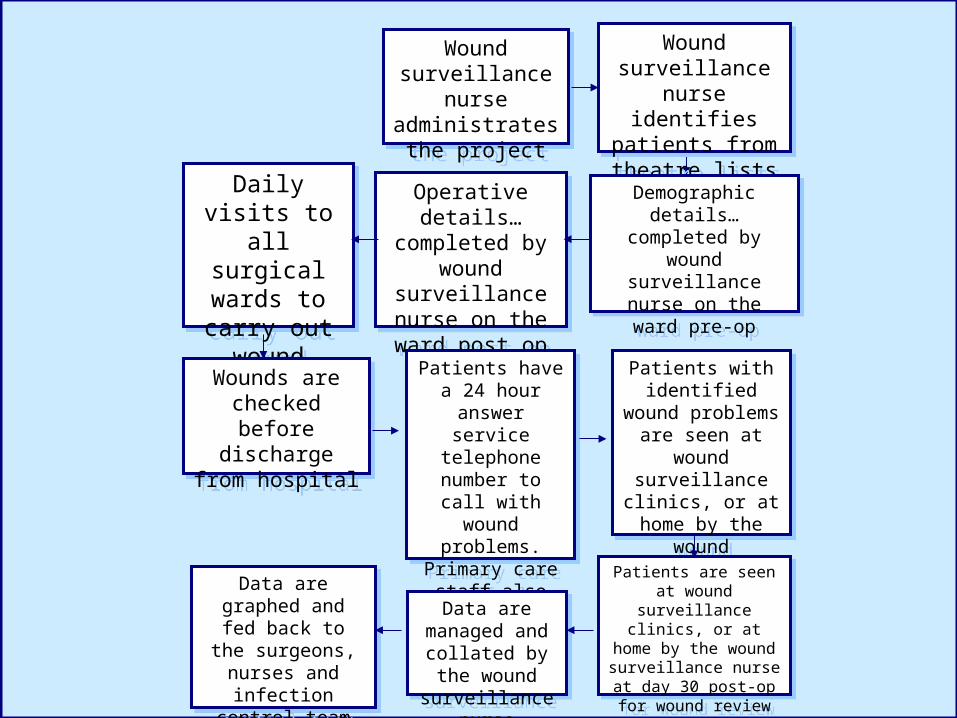
Wound surveillance nurse administrates the
project
Wound surveillance nurse administrates the
project
Wound surveillance nurse identifies patients from theatre lists
Wound surveillance nurse identifies patients from theatre lists
Demographic details…completed by wound
surveillance nurse on the ward pre-op
Demographic details…completed by wound
surveillance nurse on the ward pre-op
Patients with identified wound
problems are seen at wound surveillance clinics, or at home
by the wound surveillance nurse for wound review
Patients with identified wound
problems are seen at wound surveillance clinics, or at home
by the wound surveillance nurse for wound review
Patients are seen at wound surveillance clinics, or at
home by the wound surveillance nurse at day
30 post-op for wound review
Patients are seen at wound surveillance clinics, or at
home by the wound surveillance nurse at day
30 post-op for wound review
Operative details…completed by
wound surveillance nurse on the ward
post op
Operative details…completed by
wound surveillance nurse on the ward
post op
Patients have a 24 hour answer
service telephone number to call with wound problems. Primary care staff
also liaise with wound surveillance
nurse
Patients have a 24 hour answer
service telephone number to call with wound problems. Primary care staff
also liaise with wound surveillance
nurse
Daily visits to all surgical
wards to carry out wound
checks
Daily visits to all surgical
wards to carry out wound
checks
Wounds are checked before discharge from
hospital
Wounds are checked before discharge from
hospital
Data are managed and collated by
the wound surveillance nurse
Data are managed and collated by
the wound surveillance nurse
Data are graphed and fed back to the
surgeons, nurses and infection control
team on a monthly basis
Data are graphed and fed back to the
surgeons, nurses and infection control
team on a monthly basis
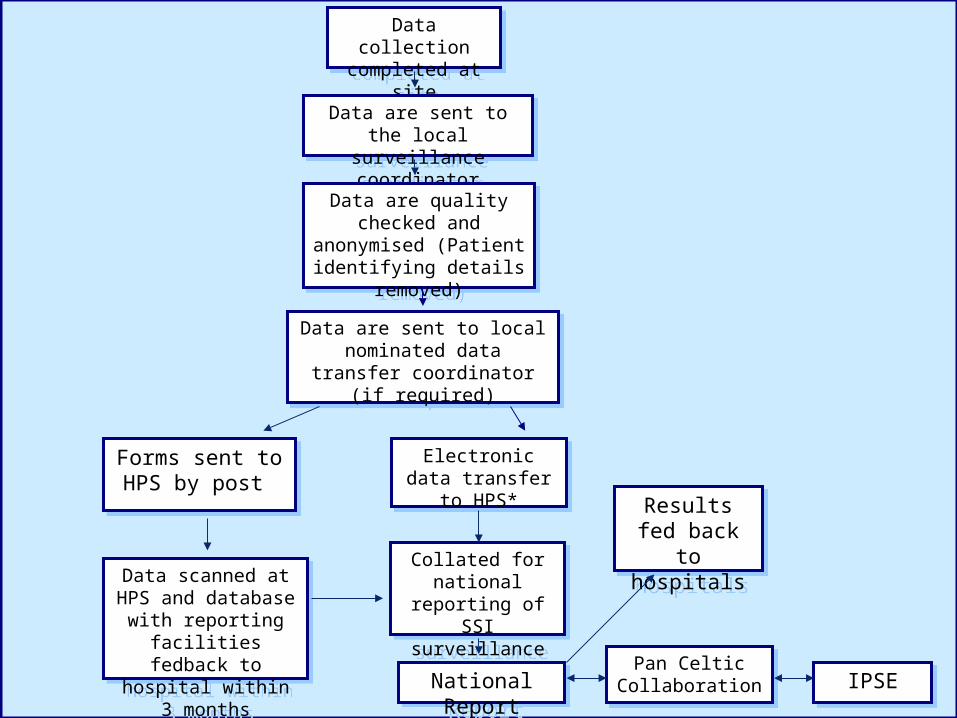
Data collection completed at site
Data collection completed at site
Data are sent to the local surveillance coordinator
Data are sent to the local surveillance coordinator
Data are quality checked and anonymised (Patient
identifying details removed)
Data are quality checked and anonymised (Patient
identifying details removed)
Data are sent to local nominated data transfer coordinator
(if required)
Data are sent to local nominated data transfer coordinator
(if required)
Forms sent to HPS by post
Forms sent to HPS by post
Data scanned at HPS and database with reporting facilities fedback to hospital
within 3 months
Data scanned at HPS and database with reporting facilities fedback to hospital
within 3 months
Electronic data transfer to HPS*
Electronic data transfer to HPS*
Collated for national reporting of
SSI surveillance
Collated for national reporting of
SSI surveillance
National ReportNational Report
Results fed back to
hospitals
Results fed back to
hospitals
Pan Celtic Collaboration
Pan Celtic Collaboration IPSEIPSE
Essential Elements of a Successful HAI surveillance system
• Defining what outcomes to measure
• Ensuring everyone involved is aware of the outcomes
• Reliably collecting the data in a standardised/defined manner
• Analysing data for comparison
• Using the data locally in a timely manner to improve quality of care
Gaynes & Solomon. J Quality Improvement 1996;22:457-67
In Summary
• Recognise the benefits of and the background to conducting SSI Surveillance
• Understand and apply to your setting the various processes that can be utilised to conduct SSI Surveillance
AIM
• To promote accurate completion of surgical site infection surveillance forms
Scottish Surveillance of HealthcareAssociated Infection Programme
Learning outcomes
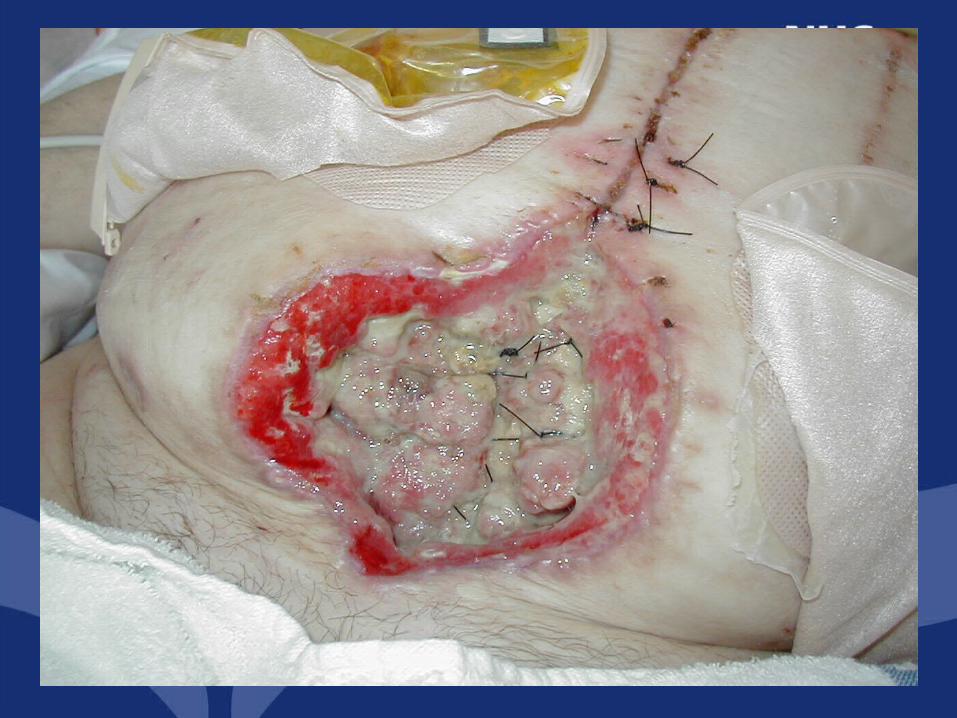
• To define the categories that are included in diagnosing SSIs
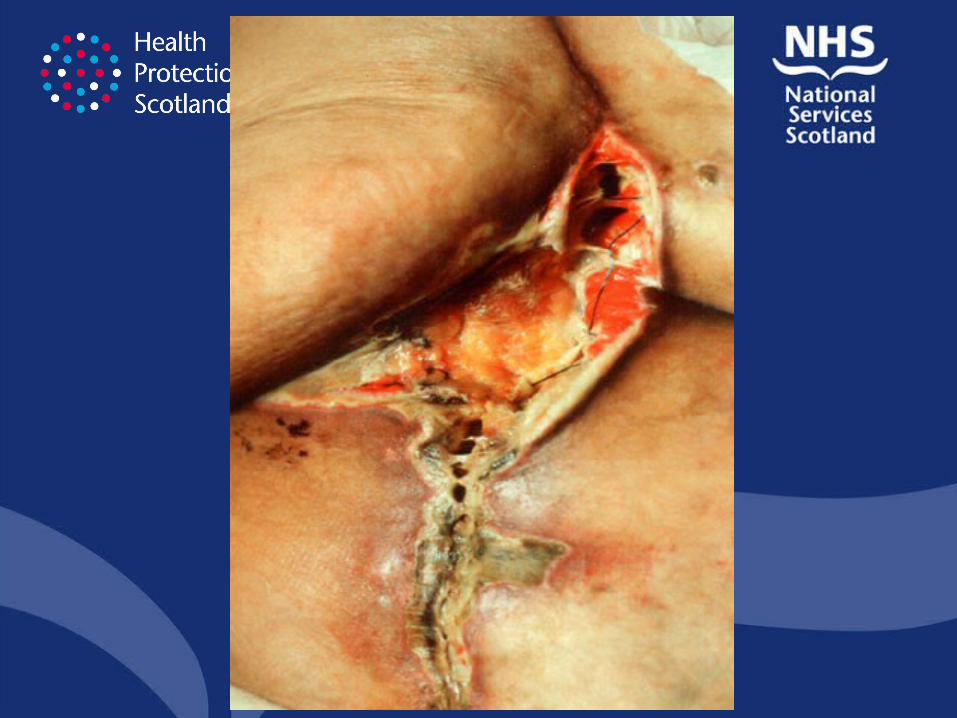
• To describe and discuss the appearance of surgical sites, to include the aforementioned categories
• To explain the surveillance form completion process
Scottish Surveillance of HealthcareAssociated Infection Programme

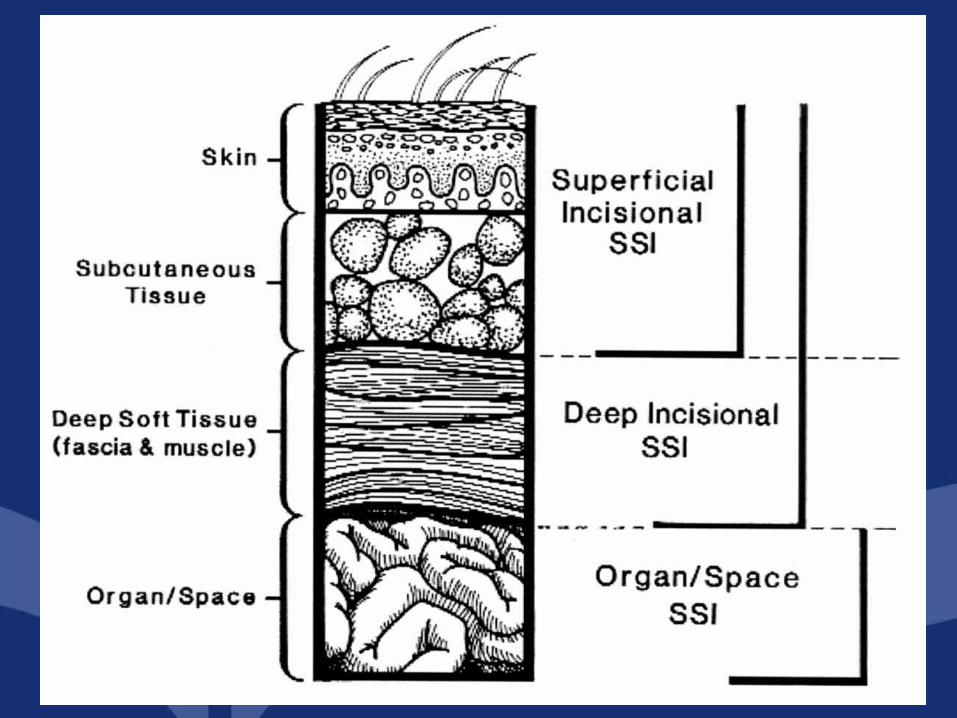
Definitions of SSI
Superficial SSI (Incisional)• A superficial SSI must meet the following criterion:1. Infection occurs within 30 days after the operative procedure2. And involves only skin and subcutaneous tissue of the incision3. And patient has at least one of the following:• Purulent discharge from the superficial incision• Organisms isolated from an aseptically obtained culture of fluid
or tissue from the superficial incision• At least one of the following signs or symptoms of infection: pain
or tenderness, localised swelling, redness, or heat and superficial incision is deliberately opened by surgeon unless incision is culture negative
• Diagnosis of superficial incisional SSI by surgeon or trained healthcare worker*
(* Trained healthcare worker is defined as a qualified doctor or nurse who has been trained in the national definitions of SSIs.)

Definitions of SSISuperficial SSI (Incisional)
• The following are not reported as superficial incisional SSI:
– Stitch abscess (minimal inflammation and discharge confined to the points of suture penetration)
– Infected burn wound e.g. diathermy
– Incisional SSI that extends into the fascial and muscle layers (deep incisional SSI)

Definitions of SSIDeep SSI (Incisional)
• A deep incisional SSI must meet the following criterion:
1. Infection occurs within 30 days after the operative procedure if no implant is left in place or within one year if implant is in place and the infection appears to be related to the operative procedure
2. And involves deep soft tissues (e.g. fascial and muscle layers) of the incision
Definitions of SSIDeep SSI (Incisional)3. And patient has at least one of the following:• Purulent discharge from the deep incision but not from the
organ/space component of a surgical site• A deep incision spontaneously dehisces or is deliberately
opened by a surgeon when the patient has at least one of the following signs or symptoms: fever (>38oC) or localised pain or tenderness, unless incision is culture negative
• An abscess or other evidence of infection involving the deep incision is found on direct examination, during re-operation, or by histopathological or radiological examination
• Diagnosis of a deep incisional SSI by surgeon or trained healthcare worker
Definitions of SSIOrgan/Space SSI
• An organ/space SSI involves any part of the body, excluding the skin incision, fascia, or muscle layers that is opened or manipulated during the operative procedure. Specific sites are assigned to organ/space SSI to further identify the location of the infection. An example is an appendicectomy with subsequent diaphragmatic abscess, which would be reported as an organ/ space SSI at the intra-abdominal specific site.
Definitions of SSIOrgan/Space SSI
• An organ/space SSI must meet the following criterion:
1. Infection occurs within 30 days after the operative procedure if no implant is left in place or within one year if implant is in place and the infection appears to be related to the operative procedure
2. And infection involves any part of the body, excluding the skin incision, fascia, or muscle layers that is opened or manipulated during the operative procedure
Definitions of SSIOrgan/Space SSI
3. And at least one of the following:
• Purulent discharge from a drain that is placed through a stab wound into the organ/space
• Organisms isolated from an aseptically obtained culture of fluid or tissue in the organ/space
• An abscess or other evidence of infection involving the organ/space that is found on direct examination, during re operation, or be histopathological or radiological examination
• Diagnosis of an organ/space SSI by surgeon or trained healthcare worker
Organ/Space SSI
• Vascular:– Arterial or
venous• Breast:
– Breast abscess– Mastitis
• Orthopaedic:– Joint or bursa– Osteomylitis
• Abdominal Hysterectomy:– Intraabdominal– Endometritis– Vaginal Cuff– Ovaries, uterus,
pelvic cavity• C. Section:
– Endometritis– Ovaries, uterus,
pelvic cavity
Criteria Used to Determine SSI – Surveillance Form (generic)
• Purulent drainage• Organisms isolated from an aseptically
obtained culture of fluid or tissue• Abscess/other evidence found on direct
examination, during a re-operation or radiology/histopathology
• Incision spontaneously dehisces• Incision is deliberately opened by surgeon• Fever (temperature 38 degrees or more)• Localised pain or tenderness• Localised swelling• Redness• Heat• Diagnosis by surgeon or trained healthcare worker
Extra criteria for organ/ space infection• Vascular:
– Organisms not isolated from blood/ blood culture not done
• Orthopaedic:– Limitation of motion– Evidence of effusion– Organisms and WBC seen on gram stain
of joint fluid– Positive antigen test on blood, urine or
joint fluid– Cellular profile and chemistries of joint
fluid compatible with infection
NB: No extra criteria for breast Various extra criteria for
cardiac/ CABG (See SSI protocol)
• Abdominal Hysterectomy/ C.Section:– Nausea– Dysuria– Vomiting– Organisms seen
on gram stain

Other definitions of wound infections
• Cellulitis• Delayed healing• Discolouration• Friable granulation tissue,
which bleeds easily• Pocketing at the base of
the wound• Bridging within the wound• Odour• 105 colony forming units
per gram of tissue

Surgical site microbiology• Common organisms found to
cause SSIs:– Staphylococcus aureus– Coagulase-negative
staphylococci– Gram negative bacilli– Anaerobes– group B streptococci
• These can be endogenous flora
• Exogenous flora are also common and avoidable
• Surgical site culturing– Why are you sampling?– When are you
sampling?– What are you
sampling?– How are you sampling?– Labelling and lab form
completion– Interpreting results
from the lab
Risk Index for SSI Surveillance
• SSI rates, by surgical procedure/category, which will be stratified by risk index.
• The NNIS risk index will be used for this. • This index scores each procedure according to the
presence or absence of three risk factors at the time of surgery and scores range from 0 (none of the factors present) to 3 (all of the factors present). The risk factors are:
– ASA score>=3– Wound classified as contaminated or
dirty– Duration of operation
Background to SSI Surveillance – Wound Classes
• Surgical wounds can be classified according to the likelihood and degree of wound contamination at the time of operation.
• The wound classification used for this surveillance is based on that developed be the National Research Council in the USA.
Wound Classes
• Clean
• Clean contaminated
• Contaminated
• Dirty or infected
Wound Classes
• A minimum wound class is only indicative and may vary according to certain pre operative and intra operative events.
• The final classification of wound contamination must be confirmed in consultation with the surgeon, or by checking the patient’s records.
Wound Classes• Clean wounds: An uninfected operative
wound in which no inflammation is encountered and the respiratory, alimentary, genital or uninfected urinary tracts are not entered. In addition clean wounds are primarily closed and if necessary drained with closed drainage. Operative incisional wounds that follow non-penetrating (blunt) trauma should be included in this category if they meet the criteria.
Wound Classes• Clean contaminated wounds: Operative
wounds in which the respiratory, alimentary, genital or urinary tracts are entered under controlled conditions and without unusual contamination. Specifically, operations involving the biliary tract, appendix, vagina and oropharynx are included in this category, provided no evidence of infection or major break in sterile technique is encountered.
Wound Classes
• Contaminated wounds: Open, fresh, accidental wounds. In addition, operations with major breaks in sterile technique (e.g. open cardiac massage) or gross spillage from the gastrointestinal tract and incisions in which acute, non-purulent inflammation is encountered are included in this category.
Wound Classes
• Dirty or infected wounds: Old traumatic wounds with retained devitalised tissue and those that involve existing clinical infection or perforated viscera. This definition suggests that the organisms causing postoperative infection were present in the field before the operation.
ASA Classification• 1. Normal healthy patient• 2. Patient with mild systemic
disease• 3. Patient with severe systemic
disease that is not incapacitating• 4. Patient with an incapacitating
systemic disease that is a constant threat to life
• 5. Moribund patient who is not expected to survive for 24 hours with or without operation
In Summary• What am I looking for?
– Has an SSI occurred, are there defined signs and symptoms of infection?
– The onset date (signs and symptoms of infection present should be completed on the form when first noticed)
• Complete the form
– With pre, peri and post operative details (see form completion instructions)
Form completion – general points
• Place a cross in the appropriate box
• Use a dark pen or biro
• Correct errors by completely filling the box where the incorrect response is
• Write clearly within the boxes when completing free text and do not write on the line of the boxes
• An empty box does not imply anything!
X
2
Form completion – general points
• DO NOT:– Use light pens– Use a tick – Leave gaps– Staple or tape through/over the four
black cornerstone boxes – Write or draw on the black unique
identifier box in the bottom corner of the forms
– Photocopy forms (you may for your own use however HPS require all originals)
Form completion – general points
• Complete the form:– On discharge– On death– On transfer – On re-operation (at the same surgical site)– At day 30 (if patient is still an in-patient or PDS
in being carried out)• Even if there is an implant complete the form at this time.• In some instances forms will continue to be completed
during the post discharge surveillance period. Procedures should be in place locally for managing this.
• Remember to ensure that the box for ‘no infection present’ is completed when surveillance ends.
Conclusion
• Standardised methodologies for SSI surveillance are essential to allow valid, reliable and comparable data. This includes the use of a common set of understood definitions.
• The local multi-disciplinary team play an essential role in the success of SSI surveillance.
• SSI rates are key quality indicators for surgery
In Summary….
• Understanding the definitions of SSIs and their clinical appearances are essential
• Accurate completion of surveillance forms is key
• Visit our updated SSHAIP Website: www.show.scot.nhs.uk/scieh/ - select HAI& Infection Control.




![Surgical Site Infection (SSI) Surveillance Protocol: Saskatchewan Surveillance Prot… · Surgical Site Infection Surveillance Protocol: Saskatchewan April 2015 1 [Type text] Introduction](https://img.pdfslide.us/doc/110x75/5fb8e047a5f3994f474ed4ac/surgical-site-infection-ssi-surveillance-protocol-saskatchewan-surveillance-prot.jpg)

![Protocol for surveillance of surgical site infection · 2017-07-28 · Protocol for the Surveillance of Surgical Site Infection, version 6 [June 2013] r1 4 4.6 Surveillance committee](https://img.pdfslide.us/doc/110x75/5e6e5d7fd9e9465809191fda/protocol-for-surveillance-of-surgical-site-infection-2017-07-28-protocol-for-the.jpg)






















