Embed Size (px)
Citation preview
34
OrthopedicDisorders
Orthopedic injuries are common in pet bird practice.Some of the more common causes are falling, an impactwith a window or ceiling fan, a crushing incident such asbeing stepped on, or an encounter with a dog or cat.
Definitive fixation of a fracture is rarely an emergency.Due to the traumatic nature of most of these injuries,first priority must be given to stabilizing the patient.Emergency treatment of shock, hemorrhage and sepsisare covered elsewhere. It is important to assess thepatient holistically, including diet, husbandry and con-current medical conditions, without focusing solely onthe obvious injuries.
Prior to examination, obtain a thorough history from theowner. Upon initial examination of the patient, orthope-dic problems may manifest as lameness, a wing droop,paresis, a swelling or an open wound. Following initialstabilization of the patient, further investigation of theseabnormalities is warranted.
The initial orthopedic exam is generally performed withthe bird awake. Prior to handling the bird, visually assessit in its cage:• Does the bird bear weight equally on each leg?• Are the wings held symmetrically and in the
proper position?• Does the bird grip a perch?• Is the overall body posture correct?
CHAPTER
Surgical Resolution of
PPEETTEERR HHEELLMMEERR,, DDVVMM,, DD iippll AABBVVPP--AAvviiaann;;PPAATTRRIICCKK TT.. RREEDDIIGG,, DDVVMM,, PPhhDD
34_Orthopedic.qxd 8/23/2005 4:55 PM Page 761

Cl inica l Avian Medic ine - Volume I I762
Following the initial visual examination, restrain the ani-mal and systematically assess the skeletal system. Theskull is palpated and the feathers covering the headparted to examine the head for hemorrhage or otherinjuries. In small birds, transillumination of the skullmay identify intracranial bleeding. The keel is palpatedfor evidence of a fracture. Palpation and visualization ofthe entire length of the vertebral column may revealdeviations or swellings. Wings and legs are examinedbeginning at the proximal aspect and progressing dis-tally. Long bones are assessed for fractures, deviationsand swellings, and joints are assessed for appropriaterange of motion. The contralateral appendage may beused as a normal for comparison. Be careful examiningextended wings, as iatrogenic fractures may result fromthe bird trying to flap while improperly restrained.
Suspicion or identification of orthopedic injury requiresfurther examination under anesthesia. Isoflurane orsevoflurane are the agents of choice. While under anes-thesia, a more complete evaluation of suspicious areasmay be performed, including investigation of masses,minor wound debridement and investigation, wetting orplucking of feathers for closer inspection (Fig 34.1), andradiographs may be made.
Radiographic technique and positioning are coveredelsewhere. At a minimum, two orthogonal views arerequired for evaluation of a particular area. Radiographsof the non-affected contralateral limb are often helpfulfor comparison, especially as anatomy is quite variablebetween genera of birds.
Following identification of an orthopedic problem, atreatment plan must be formulated. Fractures should betemporarily immobilized with splints or bandages untilthe patient is otherwise stable enough to undergo sur-gery for repair.
One must keep in mind that splints and bandages are
usually meant for temporary fixation only.
The selection of an appropriate technique for definitiverepair will depend on several variables, including thesize of the patient, the degree of postoperative return tofunction required, cost, the skill of the surgeon and con-current medical conditions.
The importance of the first of these conditions, the size ofthe patient, is often underestimated. Many avian ortho-pedic techniques were developed for use in raptorsweighing approximately 1 kg. While it is true that “tie-in”fixators (TIF) was developed on birds around 1 kg inweight, available hardware is such that it can be readilyapplied to birds 65-100 grams. These techniques may notbe feasible in the 20-g canary. The reduction of load asso-ciated with smaller size and higher surgical morbidity andmortality of small patients often contribute to a decisionto manage fractures more conservatively in small patients.
The goal of every surgeon should be to return eachpatient to the pre-injury level of activity; however, this isnot always possible. Consideration must be given to thequality of life of a non-releasable wild bird postsurgically.Given the same circumstance, a pet parrot may have anexcellent quality of life.
The ideal method of fixation must always be offered andrecommended, but lower cost alternatives may have tobe considered. A lower cost option may sacrifice post-operative return to function, but in a pet this may be anacceptable compromise. Preoperative communicationwith owners may be as important as the surgical fixationtechnique.
Finally, all surgeons do not possess the same skill andexperience with avian fracture repair. Referral of ortho-pedic cases to a more experienced surgeon should beconsidered.
PPrriinncciipplleess ooff OOrrtthhooppeeddiicc RReeppaaiirrThe basic fundamental principles of orthopedic repairare similar to other species. The repair technique shouldpromote a functional union of the fragments, share theload on the bone during healing, allow early return tofunction and have a low morbidity. The ideal hardwarefor use in this repair would be versatile, effective,adjustable, lightweight, inexpensive and associated withminimal complications.
Although the principles of repair are the same as in otherveterinary patients, some important differences exist:• Bone cortices are thinner and more brittle, resulting in
Fig 34.1 | Wetting with alcohol or removing feathers over afracture site often reveals the contusion.
Gre
g J.
Har
riso
n
34_Orthopedic.qxd 8/23/2005 4:55 PM Page 762
Chapter 34 | S U R G I C A L R E S O L U T I O N O F O R T H O P E D I C D I S O R D E R S 763
less holding power for hardware.• There is less soft tissue covering the bones. As a result,
blood and nerve supplies are commonly injured.Fracture segments tend to be unstable and commonlypenetrate the skin, with bacterial contamination acommon sequela. These fragments of exposed boneare non-viable and commonly form sequestra if incor-porated into the repair.
• Bone grafting is not common, as there is little cancel-lous bone to harvest.
• Load bearing must be rapidly restored to the legs, aslocomotion is bipedal.
The healing patterns of avian bone have been exam-ined.8,19 In adult birds, the amount of time needed forradiographic and histologic union of unilateral radiusand ulna fractures in an experimental setting was 5weeks with internal fixation and 8 weeks with externalcoaptation.8 The majority of the callus tissue duringhealing is derived from the periosteal surface, and theblood supply to the periosteum from surrounding softtissues is very important. The intramedullary circulationappears to be of less significance in avian bone healingthan in mammals.19
GGeenneerraall MMeetthhooddss ooff FFrraaccttuurree FFiixxaattiioonn
CCAAGGEE RREESSTTVery few avian fractures are satisfactorily treated with thismethod of repair. Fractures of the digits as well as green-stick fractures of young birds may be managed in this way.Cage rest also may be appropriate in the management offractures of non-weight-bearing bones in very small birdssuch as canaries and finches. Consider decreasing lightlevels to decrease activity; however, adequate light mustbe provided at least twice daily for feeding. Also considerthe use of smooth-sided cages without perches (eg, aquar-ium or plastic carrier) to prevent climbing.
EEXXTTEERRNNAALL CCOOAAPPTTAATTIIOONNThe use of splints and bandages for fracture repair inthe avian patient is limited. Bandages tend to be bulkyand cumbersome. They require prolonged immobiliza-tion of joints and usually result in poor alignment offracture fragments. Though this type of repair may beinitially less expensive, return to function is typicallyprolonged and may not be as complete as with internalfixation. Coaptation may be considered if:• Full return to function is not required.• Fractures are pathologic as a result of metabolic
bone diseases.
• Bones are too soft to hold hardware.
• The patient is too small for internal fixation alternatives.
• The surgical or anesthetic risk is judged to be too great.
Commonly used splints include the “figure-8” wrap,which may or may not include a body wrap, the Altmansplint, and Robert-Jones bandages with the incorpora-tion of splinting material. The application of the figure-8wrap and the Robert-Jones bandage are covered in othertexts.7 A description of the application of the Altmansplint is found below in Managing Fractures of theSpecific Bones, Tibiotarsus.
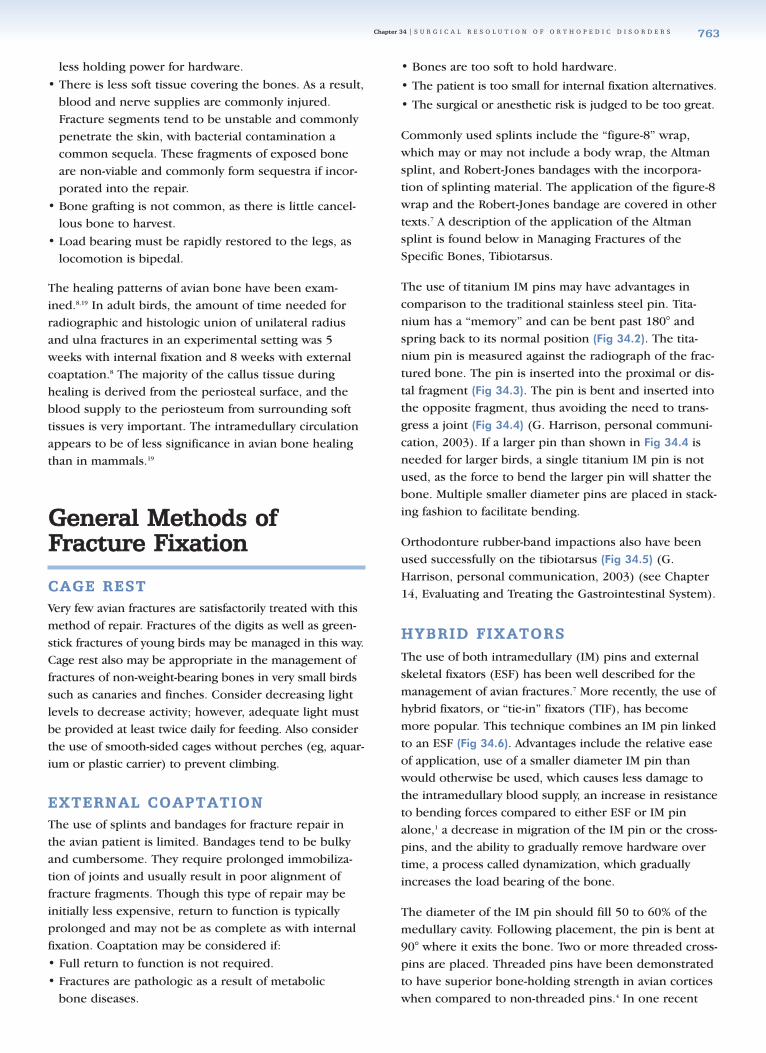
The use of titanium IM pins may have advantages incomparison to the traditional stainless steel pin. Tita-nium has a “memory” and can be bent past 180° andspring back to its normal position (Fig 34.2). The tita-nium pin is measured against the radiograph of the frac-tured bone. The pin is inserted into the proximal or dis-tal fragment (Fig 34.3). The pin is bent and inserted intothe opposite fragment, thus avoiding the need to trans-gress a joint (Fig 34.4) (G. Harrison, personal communi-cation, 2003). If a larger pin than shown in Fig 34.4 isneeded for larger birds, a single titanium IM pin is notused, as the force to bend the larger pin will shatter thebone. Multiple smaller diameter pins are placed in stack-ing fashion to facilitate bending.
Orthodonture rubber-band impactions also have beenused successfully on the tibiotarsus (Fig 34.5) (G.Harrison, personal communication, 2003) (see Chapter14, Evaluating and Treating the Gastrointestinal System).
HHYYBBRRIIDD FFIIXXAATTOORRSSThe use of both intramedullary (IM) pins and externalskeletal fixators (ESF) has been well described for themanagement of avian fractures.7 More recently, the use ofhybrid fixators, or “tie-in” fixators (TIF), has becomemore popular. This technique combines an IM pin linkedto an ESF (Fig 34.6). Advantages include the relative easeof application, use of a smaller diameter IM pin thanwould otherwise be used, which causes less damage tothe intramedullary blood supply, an increase in resistanceto bending forces compared to either ESF or IM pinalone,1 a decrease in migration of the IM pin or the cross-pins, and the ability to gradually remove hardware overtime, a process called dynamization, which graduallyincreases the load bearing of the bone.
The diameter of the IM pin should fill 50 to 60% of themedullary cavity. Following placement, the pin is bent at90° where it exits the bone. Two or more threaded cross-pins are placed. Threaded pins have been demonstratedto have superior bone-holding strength in avian corticeswhen compared to non-threaded pins.4 In one recent
34_Orthopedic.qxd 8/23/2005 4:55 PM Page 763
Cl inica l Avian Medic ine - Volume I I764
study, a significant difference in pull-out strength wasnot demonstrated when comparing positive profilethreaded pins vs. negative profile threaded pins.4 How-ever, positive profile pins have a higher locking strengthat the pin-bone interface and may be considered advan-tageous in larger bones. The cross-pins are linked to theIM pin with either a metal or acrylic bar. Several wayshave been described for linking the pins including rub-ber tubing (ie, Penrose drain, IV tubing, PVC tubing)that is filled with methylmethacrylate (ie, hoof repairmateriala) or car body filler. Also available is a methyl-methacrylate puttyb that is semi-solid. This material iskneaded and applied without the need for any tubing.The fumes emitted from this product are significantlyless than the hoof repair material.
Fig 34.3 | Titanium pin, precut and placed in the distal frag-ment via the fracture site.
Fig 34.4 | Radiograph of a titanium pin in the marrow cavity,having never transversed a joint surface.
Fig 34.5 | Bending a hook shape into the distal end of a stain-less steel transverse pin and the distal end of the distal fragmentpin can allow a periodontal rubber band to be used to applytraction to a fracture. A topical bandage covering helps preventthe rubber band from being removed inadvertently.
Gre
g J.
Har
riso
nG
reg
J. H
arri
son
Gre
g J.
Har
riso
n
Fig 34.2 | Titanium pin bent past 180º.
Gre
g J.
Har
riso
n
Fig 34.6 | Schematic of a tie-in fixa-tor (TIF) comprising an IM pin linkedto two cross-pins.
34_Orthopedic.qxd 8/23/2005 4:55 PM Page 764

Chapter 34 | S U R G I C A L R E S O L U T I O N O F O R T H O P E D I C D I S O R D E R S 765
MMaannaaggiinngg FFrraaccttuurreess ooff SSppeecciiffiicc BBoonneess
TTHHOORRAACCIICC LLIIMMBBFractures of the scapula, coracoid and clavicle are man-aged conservatively in all sizes of birds. Figure-8 band-ages with body wraps are left in place for approximately3 weeks, then radiographs are made for reevaluation.Previous recommendations for internal fixation of cora-coid fractures, compared to bandaging, resulted in lowersuccess rates in birds of prey, even when severe displace-ment of fragments existed.16
Luxations of the elements of the shoulder girdle also aremanaged conservatively, with the exception of subluxa-tion of the proximal end of the coracoid from the cranialaspect of the sternum. Open reduction of these subluxa-tions is performed via a standard approach to the cora-coid. The musculature of the keel is detached andreflected laterally to expose the proximal coracoid. Anelevator or osteotome is used for reduction. Transar-ticular cerclage wire or pins may be placed if instabilitypersists. The wing is bandaged for 3 weeks postopera-tively with physical therapy beginning about 10 dayspostoperatively.
Patagium
The patagium is a soft tissue structure comprising muscu-lar, elastic and tendinous tissues that extends from theshoulder to the metacarpus. This structure forms the lead-ing edge of the wing during flight. Injury to the patagiummay result in perforation or tearing. Healing of theseinjuries often results in contraction of the web, alteringthe conformation and restricting extension of the wing.
Sutures do not hold well in patagial tissue. This can beovercome by suturing a piece of cardboard slightlylarger than the defect over the area. The splint shouldbe replaced every 7 to 10 days until the defect is healed.The support of the cardboard allows extension of thewing during healing.
Humerus
Fractures of the humerus are classified anatomically intoone of three zones: (1) The proximal zone, which extendsfrom the tubercles to the pectoral crest, (2) the diaphysealzone extending from just distal to the pectoral crest to theapex of the distal curvature of the bone, and (3) the distalzone, which is the curved portion of the bone adjacent tothe elbow.
Proximal humeral fractures that are minimally displacedoften heal well with a figure-8 wrap combined with awrap to immobilize the wing against the body wall.
However, in order to maximize postoperative flightchances, or in cases of displacement, internal fixation isrequired. Generally the proximal fragment is too smallto drive two cross-pins for external fixation, and there isinsufficient purchase for an IM pin. A tension bandmethod of fixation has been described as the most effec-tive technique in the management of these fractures.16
The proximal humerus is approached from the dorsalaspect. The major pectoral muscle and the deltoid mus-cle are elevated from their attachments to the pectoralcrest. Two small-diameter pins are driven to exit at thedorsal and ventral aspects of the pectoral crest. Follow-ing fracture reduction, the pins are driven into the distalfragment, which results in tension exerted against themedullary cavity. This advancement can be difficult, asthe pins bend against the bone and each other. The pinsshould be driven in an alternating fashion, advancingeach only a small amount at a time. The wires are leftprojecting from the head of the humerus for futureremoval. This fixation, in addition to wrapping the wingto the body for approximately 1 week, is sufficient inbirds under 300 g.
In larger birds, following placement of the cross-pins, ahole is drilled approximately 1 cm distal to the fracturesite and another just caudal to the exit point of thewires. A wire is passed through these holes and tight-ened in a figure-8 pattern to complete the tension band.
Fractures of the humeral diaphysis tend to be obliqueand are best managed with a TIF device. The radialnerve, which must be identified and preserved, crossesthe dorsal aspect of the humerus at approximately onehalf of its length.
There are two methods of placing the IM pin in thehumerus: 1) the retrograde (ie, away from the fracturesite) method that is generally used for fixation of openfractures, and 2) the normograde (ie, toward the frac-ture site) method for closed fractures.
For retrograde IM pin insertion, the patient is placed inventral recumbency and the humerus is approachedfrom the dorsal aspect. The diameter of the IM pinshould be slightly larger than 50% of the diameter of themarrow cavity. The pin is introduced at the fracture siteand driven retrograde, exiting the proximal humerusjust distal to the shoulder. The bone chuck is thenattached to the free end of the pin and the pin with-drawn until the interval end is flush with the fracturesite. The fracture is reduced and the pin driven into thedistal fragment. Care must be taken not to penetrate thedistal end of the humerus, as damage to the triceps ten-don and joint damage are common sequelae.
34_Orthopedic.qxd 8/23/2005 4:55 PM Page 765
Cl inica l Avian Medic ine - Volume I I766
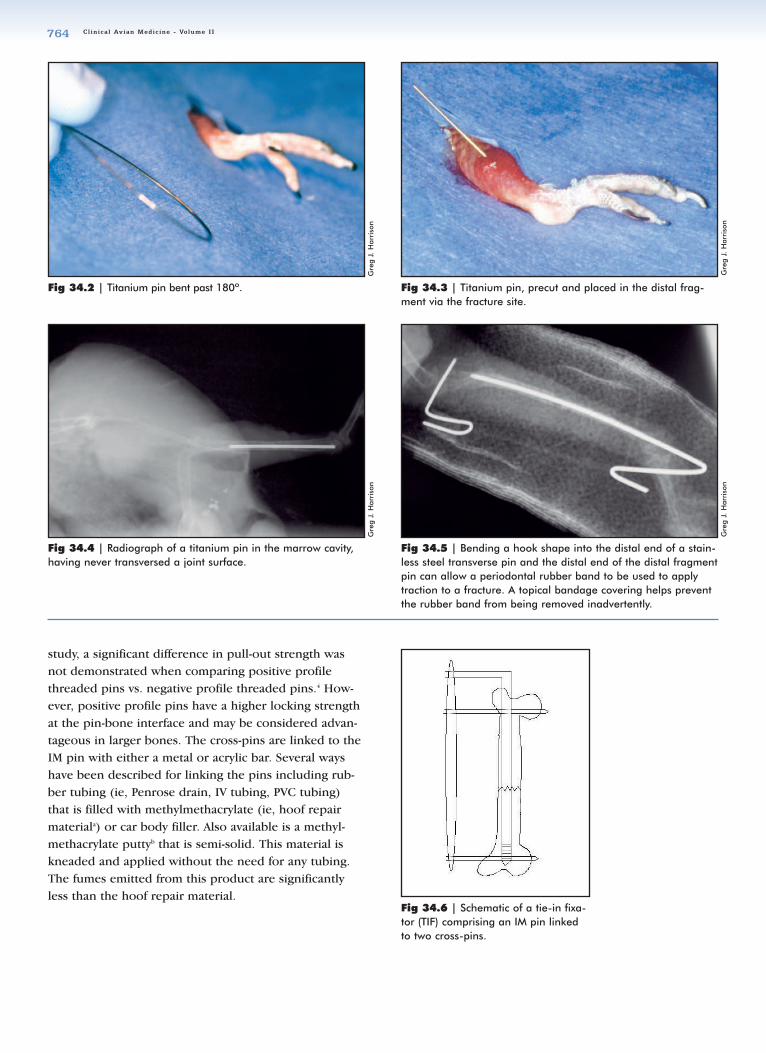
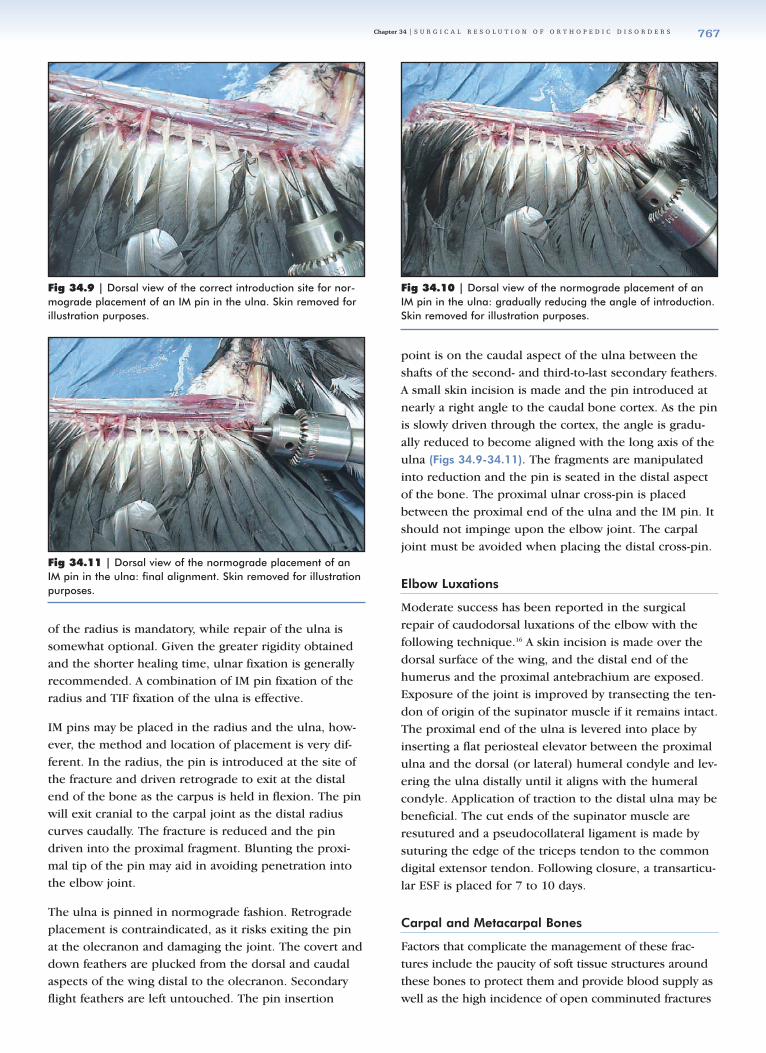
Fig 34.7 | Dorsal view of the correct introduction site for nor-mograde placement of an IM pin in the humerus. Skin has beenremoved for illustration purposes.
Fig 34.8 | Dorsal view of the correct sites for placement ofcross-pins in the humerus. Skin has been removed for illustra-tion purposes.
Normograde pin insertion is often possible in closed dia-physeal fractures (Fig 34.7). A small skin incision is madeon the dorsal aspect of the distal humerus just proximalto the lateral (or dorsal) humeral condyle. Following cau-dal retraction of the triceps tendon, a non-threaded pin isintroduced. The fracture is reduced and the pin is drivenproximally to engage the cortex of the proximal humerusin the midsection of the pectoral crest.
Regardless of the manner of IM pin insertion, positiveprofile interface K-wires are placed at the proximal anddistal aspects of the humerus to link externally to the IMpin (Fig 34.8). The distal pin is placed first. A small skinincision is made just proximal to the highest point of thelateral (or dorsal) condyle and aimed toward the ventralcondyle. The pin is driven until a full thread extendsthrough the opposite cortex. Prior to placing the proxi-mal pin, the wing is folded against the body to properlyalign the rotation of the fragments. The midsection of thefree edge of the pectoral crest is palpated and fingerswalked along it until the high point is reached. The pin isdriven, parallel to the distal one, until both cortices areengaged. The free end of the IM pin is bent at 90°approximately 2 cm from the skin. The three pins areattached as previously described. It is not recommendedto place the distal ESF pin directly through the condylesin fractures of either the distal humerus or the distaltibiotarsus. In many species the intercondylar sulcus issufficiently deep that the pin will skewer the tendon (tri-ceps or gastrocneumius) that rides in that sulcus. The pinis placed in a slightly proximal position: at the humeralepicondyle to which the tendon of the common digitalextensor and supinator muscle arise and in the tibiotar-sus, proximal to the supratendinal ridge.
Fractures of the distal humerus (ie, those that occurwithin 2 to 3 bone diameters of the distal humeralcondyles) are problematic, as there is insufficient spacefor an IM pin to gain purchase in the distal fragment.
A cross-pinning technique for these supracondylar fractures has been described.16
A skin incision is made dorsally to approach the fracture.The distal fragment is isolated and elevated while pro-tecting the soft tissues and avoiding the separation ofcomminuted fragments from their soft tissue attach-ments. Two K-wires are placed in retrograde manner, atan angle such that they exit the fragment on the oppo-site side of the marrow cavity. When pin ends are flushwith the fracture line, the fracture is reduced and thepins are driven into the proximal fragment. Movement isalternated between the pins, advancing about 0.5 cm ata time until properly seated. Pins are placed in the prox-imal and distal humerus as previously described and theelements attached to form a hybrid fixator device.
Radius and Ulna
The method of repair of fractures of the radius and ulnawill depend upon the integrity of the other bone of thepair. External coaptation is a viable option in small com-panion birds when either the radius or the ulna is frac-tured and the displacement of fragments is minimal.Potential complications include patagial contraction as aresult of prolonged immobilization and the formation ofsynostosis between any displaced fragments and theother bone. This significantly affects the bird’s ability tofly, as both lift and descent require the radius to rotateabout the ulna.
Internal fixation of the radius and/or ulna may beaccomplished with ESF, IM pins, or a combination form-ing a TIF. The prognosis for diaphyseal fractures is good;however, some very proximal radius and ulna fracturesmay be managed only by transarticular ESF, with a verypoor prognosis for return to flight. Repair of avulsionfractures of the olecranon has not been reported.
In cases of fracture of both the radius and ulna, fixation
34_Orthopedic.qxd 8/23/2005 4:55 PM Page 766
Chapter 34 | S U R G I C A L R E S O L U T I O N O F O R T H O P E D I C D I S O R D E R S 767
of the radius is mandatory, while repair of the ulna issomewhat optional. Given the greater rigidity obtainedand the shorter healing time, ulnar fixation is generallyrecommended. A combination of IM pin fixation of theradius and TIF fixation of the ulna is effective.
IM pins may be placed in the radius and the ulna, how-ever, the method and location of placement is very dif-ferent. In the radius, the pin is introduced at the site ofthe fracture and driven retrograde to exit at the distalend of the bone as the carpus is held in flexion. The pinwill exit cranial to the carpal joint as the distal radiuscurves caudally. The fracture is reduced and the pindriven into the proximal fragment. Blunting the proxi-mal tip of the pin may aid in avoiding penetration intothe elbow joint.
The ulna is pinned in normograde fashion. Retrogradeplacement is contraindicated, as it risks exiting the pinat the olecranon and damaging the joint. The covert anddown feathers are plucked from the dorsal and caudalaspects of the wing distal to the olecranon. Secondaryflight feathers are left untouched. The pin insertion
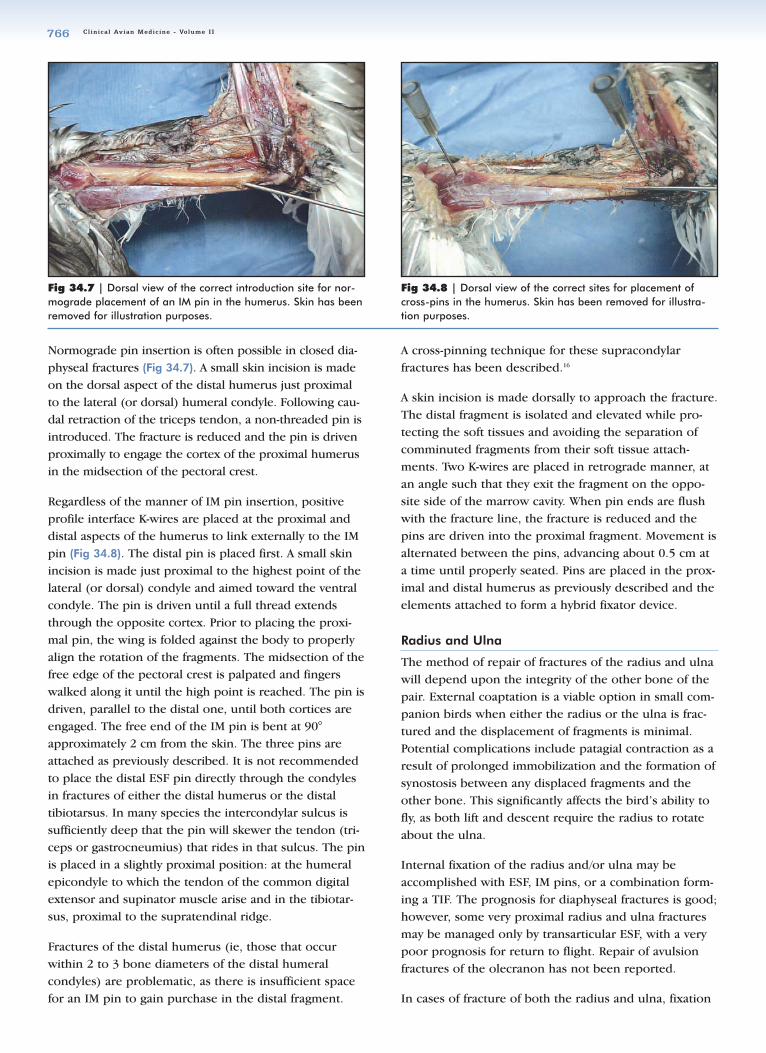
point is on the caudal aspect of the ulna between theshafts of the second- and third-to-last secondary feathers.A small skin incision is made and the pin introduced atnearly a right angle to the caudal bone cortex. As the pinis slowly driven through the cortex, the angle is gradu-ally reduced to become aligned with the long axis of theulna (Figs 34.9-34.11). The fragments are manipulatedinto reduction and the pin is seated in the distal aspectof the bone. The proximal ulnar cross-pin is placedbetween the proximal end of the ulna and the IM pin. Itshould not impinge upon the elbow joint. The carpaljoint must be avoided when placing the distal cross-pin.
Elbow Luxations
Moderate success has been reported in the surgicalrepair of caudodorsal luxations of the elbow with thefollowing technique.16 A skin incision is made over thedorsal surface of the wing, and the distal end of thehumerus and the proximal antebrachium are exposed.Exposure of the joint is improved by transecting the ten-don of origin of the supinator muscle if it remains intact.The proximal end of the ulna is levered into place byinserting a flat periosteal elevator between the proximalulna and the dorsal (or lateral) humeral condyle and lev-ering the ulna distally until it aligns with the humeralcondyle. Application of traction to the distal ulna may bebeneficial. The cut ends of the supinator muscle areresutured and a pseudocollateral ligament is made bysuturing the edge of the triceps tendon to the commondigital extensor tendon. Following closure, a transarticu-lar ESF is placed for 7 to 10 days.
Carpal and Metacarpal Bones
Factors that complicate the management of these frac-tures include the paucity of soft tissue structures aroundthese bones to protect them and provide blood supply aswell as the high incidence of open comminuted fractures
Fig 34.9 | Dorsal view of the correct introduction site for nor-mograde placement of an IM pin in the ulna. Skin removed forillustration purposes.
Fig 34.11 | Dorsal view of the normograde placement of anIM pin in the ulna: final alignment. Skin removed for illustrationpurposes.
Fig 34.10 | Dorsal view of the normograde placement of anIM pin in the ulna: gradually reducing the angle of introduction.Skin removed for illustration purposes.
34_Orthopedic.qxd 8/23/2005 4:55 PM Page 767
Cl inica l Avian Medic ine - Volume I I768
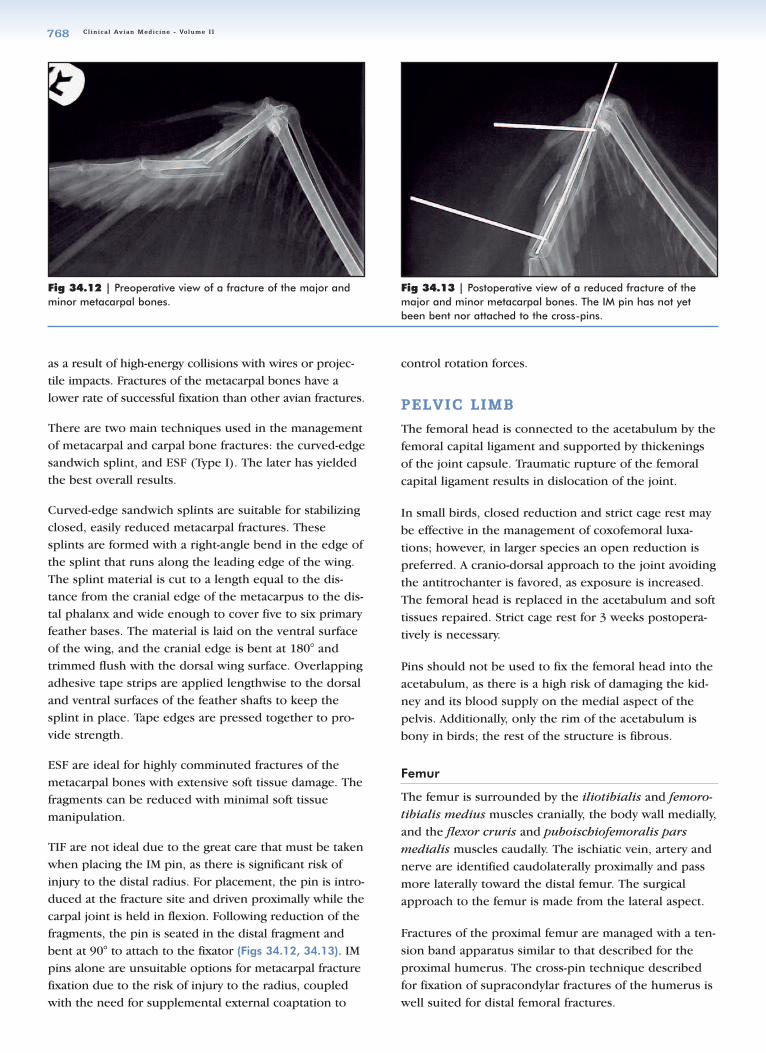
Fig 34.12 | Preoperative view of a fracture of the major andminor metacarpal bones.
Fig 34.13 | Postoperative view of a reduced fracture of themajor and minor metacarpal bones. The IM pin has not yetbeen bent nor attached to the cross-pins.
as a result of high-energy collisions with wires or projec-tile impacts. Fractures of the metacarpal bones have alower rate of successful fixation than other avian fractures.
There are two main techniques used in the managementof metacarpal and carpal bone fractures: the curved-edgesandwich splint, and ESF (Type I). The later has yieldedthe best overall results.
Curved-edge sandwich splints are suitable for stabilizingclosed, easily reduced metacarpal fractures. Thesesplints are formed with a right-angle bend in the edge ofthe splint that runs along the leading edge of the wing.The splint material is cut to a length equal to the dis-tance from the cranial edge of the metacarpus to the dis-tal phalanx and wide enough to cover five to six primaryfeather bases. The material is laid on the ventral surfaceof the wing, and the cranial edge is bent at 180° andtrimmed flush with the dorsal wing surface. Overlappingadhesive tape strips are applied lengthwise to the dorsaland ventral surfaces of the feather shafts to keep thesplint in place. Tape edges are pressed together to pro-vide strength.
ESF are ideal for highly comminuted fractures of themetacarpal bones with extensive soft tissue damage. Thefragments can be reduced with minimal soft tissuemanipulation.
TIF are not ideal due to the great care that must be takenwhen placing the IM pin, as there is significant risk ofinjury to the distal radius. For placement, the pin is intro-duced at the fracture site and driven proximally while thecarpal joint is held in flexion. Following reduction of thefragments, the pin is seated in the distal fragment andbent at 90° to attach to the fixator (Figs 34.12, 34.13). IMpins alone are unsuitable options for metacarpal fracturefixation due to the risk of injury to the radius, coupledwith the need for supplemental external coaptation to
control rotation forces.
PPEELLVVIICC LLIIMMBB
The femoral head is connected to the acetabulum by thefemoral capital ligament and supported by thickeningsof the joint capsule. Traumatic rupture of the femoralcapital ligament results in dislocation of the joint.
In small birds, closed reduction and strict cage rest maybe effective in the management of coxofemoral luxa-tions; however, in larger species an open reduction ispreferred. A cranio-dorsal approach to the joint avoidingthe antitrochanter is favored, as exposure is increased.The femoral head is replaced in the acetabulum and softtissues repaired. Strict cage rest for 3 weeks postopera-tively is necessary.
Pins should not be used to fix the femoral head into theacetabulum, as there is a high risk of damaging the kid-ney and its blood supply on the medial aspect of thepelvis. Additionally, only the rim of the acetabulum isbony in birds; the rest of the structure is fibrous.
Femur
The femur is surrounded by the iliotibialis and femoro-tibialis medius muscles cranially, the body wall medially,and the flexor cruris and puboischiofemoralis parsmedialis muscles caudally. The ischiatic vein, artery andnerve are identified caudolaterally proximally and passmore laterally toward the distal femur. The surgicalapproach to the femur is made from the lateral aspect.
Fractures of the proximal femur are managed with a ten-sion band apparatus similar to that described for theproximal humerus. The cross-pin technique describedfor fixation of supracondylar fractures of the humerus iswell suited for distal femoral fractures.
34_Orthopedic.qxd 8/23/2005 4:56 PM Page 768
Chapter 34 | S U R G I C A L R E S O L U T I O N O F O R T H O P E D I C D I S O R D E R S 769
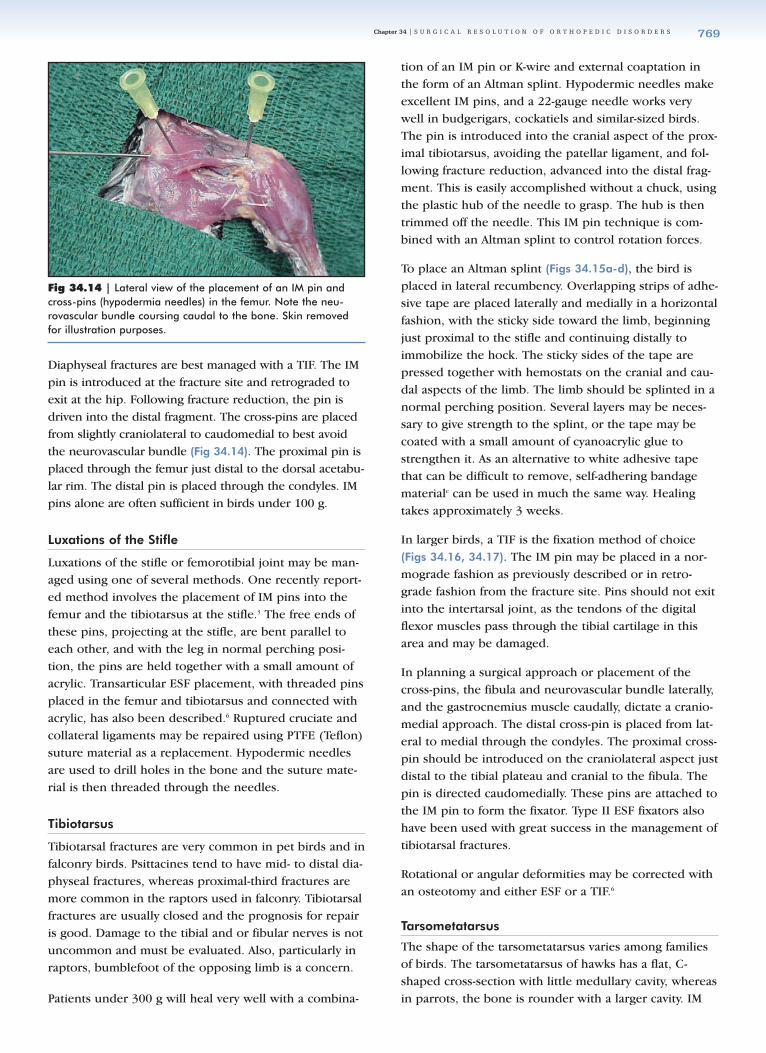
Diaphyseal fractures are best managed with a TIF. The IMpin is introduced at the fracture site and retrograded toexit at the hip. Following fracture reduction, the pin isdriven into the distal fragment. The cross-pins are placedfrom slightly craniolateral to caudomedial to best avoidthe neurovascular bundle (Fig 34.14). The proximal pin isplaced through the femur just distal to the dorsal acetabu-lar rim. The distal pin is placed through the condyles. IMpins alone are often sufficient in birds under 100 g.
Luxations of the Stifle
Luxations of the stifle or femorotibial joint may be man-aged using one of several methods. One recently report-ed method involves the placement of IM pins into thefemur and the tibiotarsus at the stifle.3 The free ends ofthese pins, projecting at the stifle, are bent parallel toeach other, and with the leg in normal perching posi-tion, the pins are held together with a small amount ofacrylic. Transarticular ESF placement, with threaded pinsplaced in the femur and tibiotarsus and connected withacrylic, has also been described.6 Ruptured cruciate andcollateral ligaments may be repaired using PTFE (Teflon)suture material as a replacement. Hypodermic needlesare used to drill holes in the bone and the suture mate-rial is then threaded through the needles.
Tibiotarsus
Tibiotarsal fractures are very common in pet birds and infalconry birds. Psittacines tend to have mid- to distal dia-physeal fractures, whereas proximal-third fractures aremore common in the raptors used in falconry. Tibiotarsalfractures are usually closed and the prognosis for repairis good. Damage to the tibial and or fibular nerves is notuncommon and must be evaluated. Also, particularly inraptors, bumblefoot of the opposing limb is a concern.
Patients under 300 g will heal very well with a combina-
tion of an IM pin or K-wire and external coaptation inthe form of an Altman splint. Hypodermic needles makeexcellent IM pins, and a 22-gauge needle works verywell in budgerigars, cockatiels and similar-sized birds.The pin is introduced into the cranial aspect of the prox-imal tibiotarsus, avoiding the patellar ligament, and fol-lowing fracture reduction, advanced into the distal frag-ment. This is easily accomplished without a chuck, usingthe plastic hub of the needle to grasp. The hub is thentrimmed off the needle. This IM pin technique is com-bined with an Altman splint to control rotation forces.
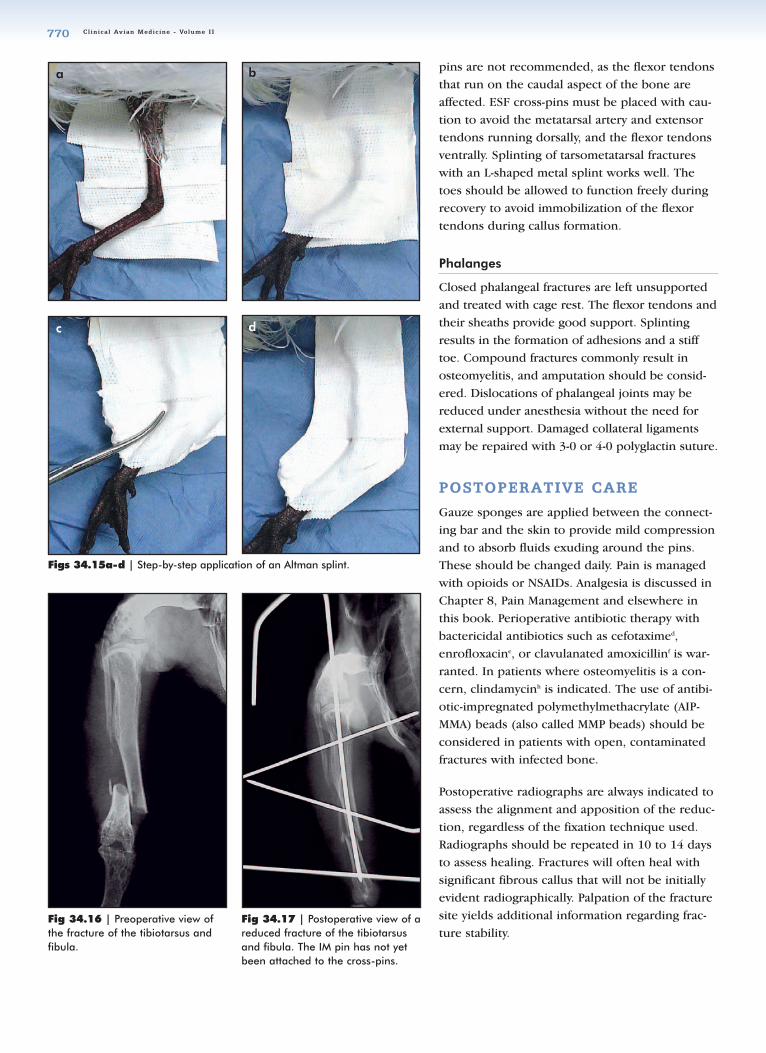
To place an Altman splint (Figs 34.15a-d), the bird isplaced in lateral recumbency. Overlapping strips of adhe-sive tape are placed laterally and medially in a horizontalfashion, with the sticky side toward the limb, beginningjust proximal to the stifle and continuing distally toimmobilize the hock. The sticky sides of the tape arepressed together with hemostats on the cranial and cau-dal aspects of the limb. The limb should be splinted in anormal perching position. Several layers may be neces-sary to give strength to the splint, or the tape may becoated with a small amount of cyanoacrylic glue tostrengthen it. As an alternative to white adhesive tapethat can be difficult to remove, self-adhering bandagematerialc can be used in much the same way. Healingtakes approximately 3 weeks.
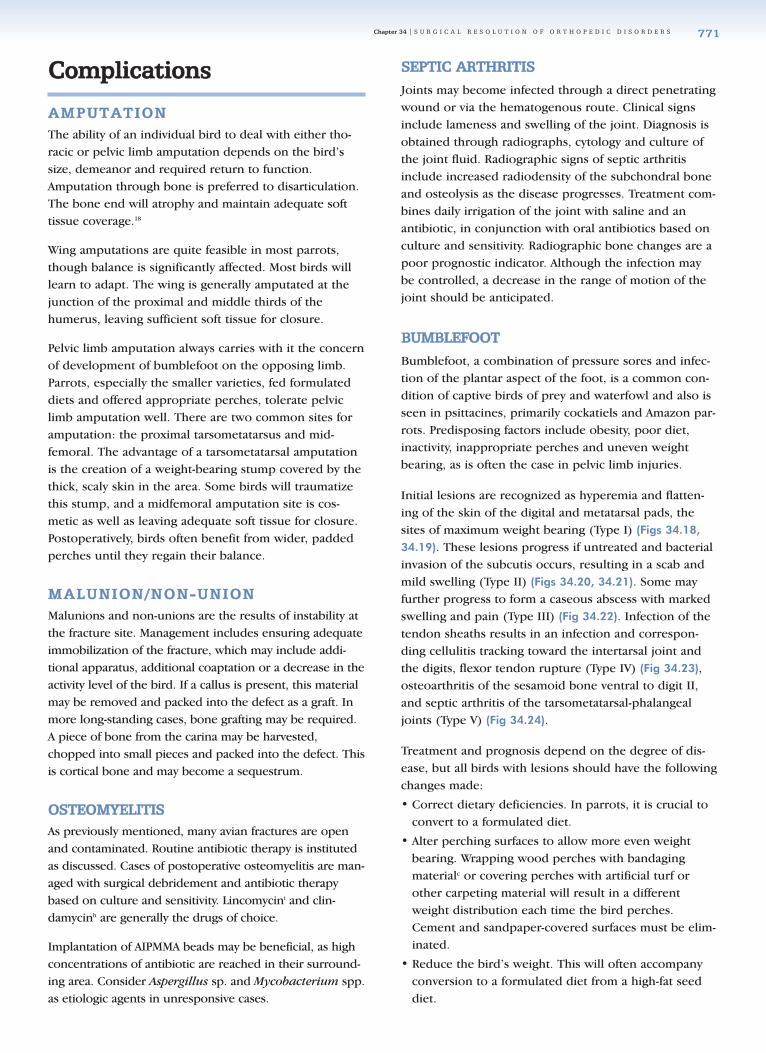
In larger birds, a TIF is the fixation method of choice(Figs 34.16, 34.17). The IM pin may be placed in a nor-mograde fashion as previously described or in retro-grade fashion from the fracture site. Pins should not exitinto the intertarsal joint, as the tendons of the digitalflexor muscles pass through the tibial cartilage in thisarea and may be damaged.
In planning a surgical approach or placement of thecross-pins, the fibula and neurovascular bundle laterally,and the gastrocnemius muscle caudally, dictate a cranio-medial approach. The distal cross-pin is placed from lat-eral to medial through the condyles. The proximal cross-pin should be introduced on the craniolateral aspect justdistal to the tibial plateau and cranial to the fibula. Thepin is directed caudomedially. These pins are attached tothe IM pin to form the fixator. Type II ESF fixators alsohave been used with great success in the management oftibiotarsal fractures.
Rotational or angular deformities may be corrected withan osteotomy and either ESF or a TIF.6
Tarsometatarsus
The shape of the tarsometatarsus varies among familiesof birds. The tarsometatarsus of hawks has a flat, C-shaped cross-section with little medullary cavity, whereasin parrots, the bone is rounder with a larger cavity. IM
Fig 34.14 | Lateral view of the placement of an IM pin andcross-pins (hypodermia needles) in the femur. Note the neu-rovascular bundle coursing caudal to the bone. Skin removedfor illustration purposes.
34_Orthopedic.qxd 8/23/2005 4:56 PM Page 769
Cl inica l Avian Medic ine - Volume I I770
pins are not recommended, as the flexor tendonsthat run on the caudal aspect of the bone areaffected. ESF cross-pins must be placed with cau-tion to avoid the metatarsal artery and extensortendons running dorsally, and the flexor tendonsventrally. Splinting of tarsometatarsal fractureswith an L-shaped metal splint works well. Thetoes should be allowed to function freely duringrecovery to avoid immobilization of the flexortendons during callus formation.
Phalanges
Closed phalangeal fractures are left unsupportedand treated with cage rest. The flexor tendons andtheir sheaths provide good support. Splintingresults in the formation of adhesions and a stifftoe. Compound fractures commonly result inosteomyelitis, and amputation should be consid-ered. Dislocations of phalangeal joints may bereduced under anesthesia without the need forexternal support. Damaged collateral ligamentsmay be repaired with 3-0 or 4-0 polyglactin suture.
PPOOSSTTOOPPEERRAATTIIVVEE CCAARREE
Gauze sponges are applied between the connect-ing bar and the skin to provide mild compressionand to absorb fluids exuding around the pins.These should be changed daily. Pain is managedwith opioids or NSAIDs. Analgesia is discussed inChapter 8, Pain Management and elsewhere inthis book. Perioperative antibiotic therapy withbactericidal antibiotics such as cefotaximed,enrofloxacine, or clavulanated amoxicillinf is war-ranted. In patients where osteomyelitis is a con-cern, clindamycinh is indicated. The use of antibi-otic-impregnated polymethylmethacrylate (AIP-MMA) beads (also called MMP beads) should beconsidered in patients with open, contaminatedfractures with infected bone.
Postoperative radiographs are always indicated toassess the alignment and apposition of the reduc-tion, regardless of the fixation technique used.Radiographs should be repeated in 10 to 14 daysto assess healing. Fractures will often heal withsignificant fibrous callus that will not be initiallyevident radiographically. Palpation of the fracturesite yields additional information regarding frac-ture stability.
Fig 34.16 | Preoperative view ofthe fracture of the tibiotarsus andfibula.
Figs 34.15a-d | Step-by-step application of an Altman splint.
Fig 34.17 | Postoperative view of areduced fracture of the tibiotarsusand fibula. The IM pin has not yetbeen attached to the cross-pins.
a b
c d
34_Orthopedic.qxd 8/23/2005 4:56 PM Page 770
Chapter 34 | S U R G I C A L R E S O L U T I O N O F O R T H O P E D I C D I S O R D E R S 771
CCoommpplliiccaattiioonnss
AAMMPPUUTTAATTIIOONNThe ability of an individual bird to deal with either tho-racic or pelvic limb amputation depends on the bird’ssize, demeanor and required return to function.Amputation through bone is preferred to disarticulation.The bone end will atrophy and maintain adequate softtissue coverage.18
Wing amputations are quite feasible in most parrots,though balance is significantly affected. Most birds willlearn to adapt. The wing is generally amputated at thejunction of the proximal and middle thirds of thehumerus, leaving sufficient soft tissue for closure.
Pelvic limb amputation always carries with it the concernof development of bumblefoot on the opposing limb.Parrots, especially the smaller varieties, fed formulateddiets and offered appropriate perches, tolerate pelviclimb amputation well. There are two common sites foramputation: the proximal tarsometatarsus and mid-femoral. The advantage of a tarsometatarsal amputationis the creation of a weight-bearing stump covered by thethick, scaly skin in the area. Some birds will traumatizethis stump, and a midfemoral amputation site is cos-metic as well as leaving adequate soft tissue for closure.Postoperatively, birds often benefit from wider, paddedperches until they regain their balance.
MMAALLUUNNIIOONN//NNOONN--UUNNIIOONNMalunions and non-unions are the results of instability atthe fracture site. Management includes ensuring adequateimmobilization of the fracture, which may include addi-tional apparatus, additional coaptation or a decrease in theactivity level of the bird. If a callus is present, this materialmay be removed and packed into the defect as a graft. Inmore long-standing cases, bone grafting may be required.A piece of bone from the carina may be harvested,chopped into small pieces and packed into the defect. Thisis cortical bone and may become a sequestrum.
OOSSTTEEOOMMYYEELLIITTIISSAs previously mentioned, many avian fractures are openand contaminated. Routine antibiotic therapy is institutedas discussed. Cases of postoperative osteomyelitis are man-aged with surgical debridement and antibiotic therapybased on culture and sensitivity. Lincomycini and clin-damycinh are generally the drugs of choice.
Implantation of AIPMMA beads may be beneficial, as highconcentrations of antibiotic are reached in their surround-ing area. Consider Aspergillus sp. and Mycobacterium spp.as etiologic agents in unresponsive cases.
SSEEPPTTIICC AARRTTHHRRIITTIISSJoints may become infected through a direct penetratingwound or via the hematogenous route. Clinical signsinclude lameness and swelling of the joint. Diagnosis isobtained through radiographs, cytology and culture ofthe joint fluid. Radiographic signs of septic arthritisinclude increased radiodensity of the subchondral boneand osteolysis as the disease progresses. Treatment com-bines daily irrigation of the joint with saline and anantibiotic, in conjunction with oral antibiotics based onculture and sensitivity. Radiographic bone changes are apoor prognostic indicator. Although the infection maybe controlled, a decrease in the range of motion of thejoint should be anticipated.
BBUUMMBBLLEEFFOOOOTTBumblefoot, a combination of pressure sores and infec-tion of the plantar aspect of the foot, is a common con-dition of captive birds of prey and waterfowl and also isseen in psittacines, primarily cockatiels and Amazon par-rots. Predisposing factors include obesity, poor diet,inactivity, inappropriate perches and uneven weightbearing, as is often the case in pelvic limb injuries.
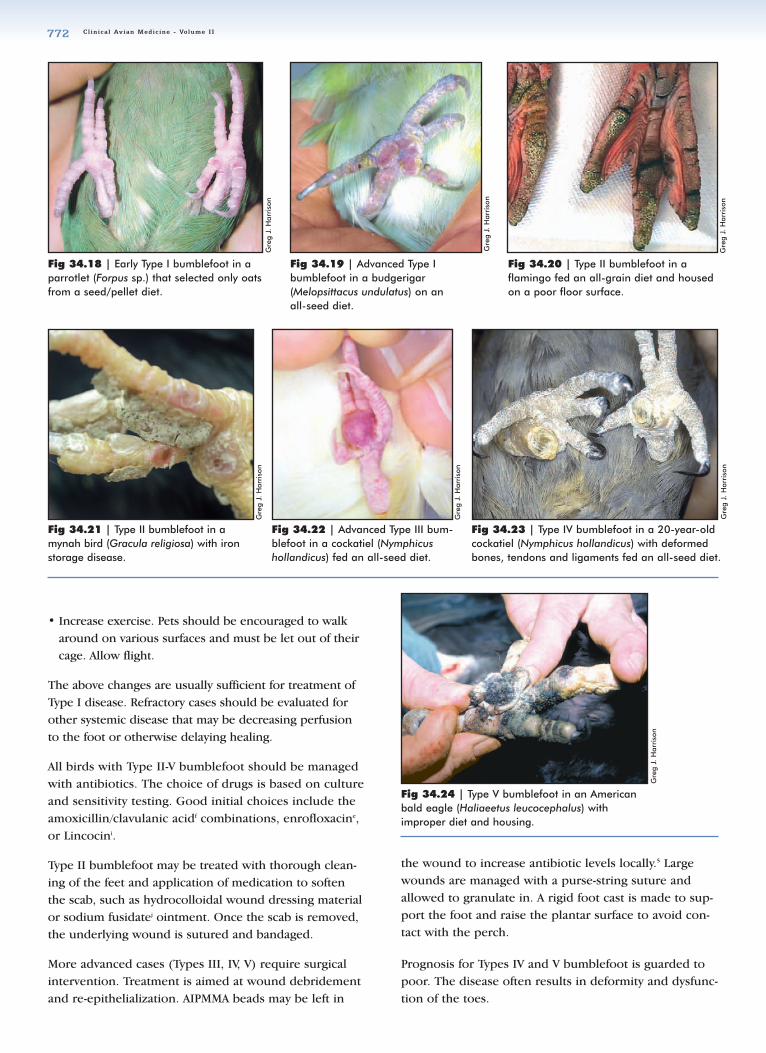
Initial lesions are recognized as hyperemia and flatten-ing of the skin of the digital and metatarsal pads, thesites of maximum weight bearing (Type I) (Figs 34.18,
34.19). These lesions progress if untreated and bacterialinvasion of the subcutis occurs, resulting in a scab andmild swelling (Type II) (Figs 34.20, 34.21). Some mayfurther progress to form a caseous abscess with markedswelling and pain (Type III) (Fig 34.22). Infection of thetendon sheaths results in an infection and correspon-ding cellulitis tracking toward the intertarsal joint andthe digits, flexor tendon rupture (Type IV) (Fig 34.23),osteoarthritis of the sesamoid bone ventral to digit II,and septic arthritis of the tarsometatarsal-phalangealjoints (Type V) (Fig 34.24).
Treatment and prognosis depend on the degree of dis-ease, but all birds with lesions should have the followingchanges made:
• Correct dietary deficiencies. In parrots, it is crucial toconvert to a formulated diet.
• Alter perching surfaces to allow more even weightbearing. Wrapping wood perches with bandagingmaterialc or covering perches with artificial turf orother carpeting material will result in a differentweight distribution each time the bird perches.Cement and sandpaper-covered surfaces must be elim-inated.
• Reduce the bird’s weight. This will often accompanyconversion to a formulated diet from a high-fat seeddiet.
34_Orthopedic.qxd 8/23/2005 4:56 PM Page 771
Cl inica l Avian Medic ine - Volume I I772
Gre
g J.
Har
riso
n
Gre
g J.
Har
riso
n
Fig 34.21 | Type II bumblefoot in amynah bird (Gracula religiosa) with ironstorage disease.
Fig 34.22 | Advanced Type III bum-blefoot in a cockatiel (Nymphicushollandicus) fed an all-seed diet.
• Increase exercise. Pets should be encouraged to walkaround on various surfaces and must be let out of theircage. Allow flight.
The above changes are usually sufficient for treatment ofType I disease. Refractory cases should be evaluated forother systemic disease that may be decreasing perfusionto the foot or otherwise delaying healing.
All birds with Type II-V bumblefoot should be managedwith antibiotics. The choice of drugs is based on cultureand sensitivity testing. Good initial choices include theamoxicillin/clavulanic acidf combinations, enrofloxacine,or Lincocini.
Type II bumblefoot may be treated with thorough clean-ing of the feet and application of medication to softenthe scab, such as hydrocolloidal wound dressing materialor sodium fusidatej ointment. Once the scab is removed,the underlying wound is sutured and bandaged.
More advanced cases (Types III, IV, V) require surgicalintervention. Treatment is aimed at wound debridementand re-epithelialization. AIPMMA beads may be left in
the wound to increase antibiotic levels locally.5 Largewounds are managed with a purse-string suture andallowed to granulate in. A rigid foot cast is made to sup-port the foot and raise the plantar surface to avoid con-tact with the perch.
Prognosis for Types IV and V bumblefoot is guarded topoor. The disease often results in deformity and dysfunc-tion of the toes.
Fig 34.23 | Type IV bumblefoot in a 20-year-oldcockatiel (Nymphicus hollandicus) with deformedbones, tendons and ligaments fed an all-seed diet.
Fig 34.24 | Type V bumblefoot in an Americanbald eagle (Haliaeetus leucocephalus) withimproper diet and housing.
Gre
g J.
Har
riso
n
Fig 34.19 | Advanced Type I bumblefoot in a budgerigar (Melopsittacus undulatus) on an all-seed diet.
Gre
g J.
Har
riso
n
Gre
g J.
Har
riso
n
Fig 34.18 | Early Type I bumblefoot in aparrotlet (Forpus sp.) that selected only oatsfrom a seed/pellet diet.
Gre
g J.
Har
riso
n
Fig 34.20 | Type II bumblefoot in aflamingo fed an all-grain diet and housedon a poor floor surface.
Gre
g J.
Har
riso
n
34_Orthopedic.qxd 8/23/2005 4:56 PM Page 772

Chapter 34 | S U R G I C A L R E S O L U T I O N O F O R T H O P E D I C D I S O R D E R S 773
References andSuggested Reading1. Aron DN, et al: Experimental and
clinical experience with an IM pinexternal skeletal fixator tie-in configuration. Vet Comp OrthoTraumatol 4:86-94, 1991.
2. Bennett RA, Harrison GJ: Soft tissue surgery. In Ritchie BW,Harrison GJ, Harrison LR (eds):Avian Medicine: Principles andApplication. Brentwood, TN, HBDInt’l Inc, 1999, pp 1096-1137.
3. Bowles HL, Zantop DW: A noveltechnique for luxation repair ofthe femorotibial joint in a monkparakeet (Myiopsitta monachus). JAvian Med Surg 16(1):34-38, 2002.
4. Degernes L, Roe SC, Abrams CF:Holding power of different pindesigns and pin insertion methods
in avian cortical bone. Vet Surg27:301-306, 1998.
5. Forbes NA: Antibiotic-impregnatedpolymethylmethacrylate beads inthe treatment of bumblefoot,osteomyelitis and other localizedinfections in birds. Proc Assoc AvianVet Aust Com, 2000, pp 82-87.
6. Harcourt-Brown NH: Orthopedicconditions that affect the avianpelvic limb. Vet Clin Nor Am ExotAn Pract 5(1):49-81, 2002.
7. Martin H, Ritchie BW: Orthopedicsurgical techniques. In Ritchie BW,Harrison GJ, Harrison LR (eds):Avian Medicine: Principles andApplication. Brentwood, TN, HBDInt’l Inc, 1999, pp 1137-1169.
8. Newton CD, Zeitlin A: Avian fracture healing. J Am Vet MedAssoc 170(6):620-625, 1977.
9. Orosz SE: Clinical considerations
of the thoracic limb.Vet Clin NorAm Exot An Pract 5(1):31-48,2002.
10. Orosz SE: Surgical anatomy of thepelvic limb. Proc Assoc Avian Vet,1999, pp 389-398.
11. Orosz SE: Avian surgical anatomyof the proximal pelvic limb. ProcAssoc Avian Vet, 2002, pp 317-321.
12. Peirone B, et al: Femoral andhumeral fracture treatment with anintramedullary pin/external fixatortie-in configuration in growingdogs and cats. Vet Comp OrthoTraumatol 15:85-91, 2002.
13. Redig PT: Decision making inavian orthopedics. Proc AssocAvian Vet, 1998, pp 253-263.
14. Redig PT: General aspects of avianorthopedic surgery: The pelviclimb. Proc Assoc Avian Vet, 1999,pp 399-411.
15. Redig PT, Korbel RT, Grimm F:Laboratory procedures for avianorthopedics. Proc European AssocAvian Vet, 2001, pp 323-330.
16. Redig PT: Master class: Anatomicaland surgical considerations of theavian thoracic limb. Proc AssocAvian Vet, 2000, pp 429-438.
17. Redig PT: Orthopedic fixation forlong bone fractures of raptorsand other large birds: Pelvic limb.Proc Assoc Avian Vet, 2002, pp323-335.
18. Weigel, JP: Amputations. In SlatterDS (ed): Textbook of SmallAnimal Surgery 2nd ed.Philadelphia, WB Saunders Co,1993, pp 1901-1910.
19. West PG, et al: Histomorphometricand angiographic analysis of bonehealing in the humerus of pigeons.Am J Vet Res 57(7):1010-1015, 1996.
Products Mentioned in the Texta. Technovit, Jorgensen Laboratories Inc, Loveland, CO, USA www.jorvet.com,
www.3m.com/us/healthcare/professionals/animalcareb. ESF putty, Jorgensen Laboratories Inc, Loveland, CO, USA www.jorvet.comc. Vetrap Bandaging Tape, 3M Animal Care Products, St. Paul, MN, USAd. Claforan, cefotaxime, Hoechst-Roussel Pharmaceuticals, Kansas City, MO,
USA www.aventis- us.com/PIs/claforan_TXT.htmle. Baytril, Bayer, Shawnee Mission, KS, USA www.bayeranimalhealth.com
f. Clavamox, Pfizer Animal Health, Exxon, PA, USA www.pfizer.com/ahg. Suitably sized IM pins are available in the US from IMEX Veterinary Inc,
Longview, TX, USA , www.imexvet.comh. Clindamycin- Antirobe - Upjohn, Kalamazoo, MI. 616-329-8244i. Lincomycin- Lincocin Upjohn, Kalamazoo, MI. 616-329-8244j. Sodium fusidate ointment, Fusidic acid
www.drugs.com/xq/cfm/pageID_0/search_fusidic%20Acid/start_31
34_Orthopedic.qxd 8/23/2005 4:56 PM Page 773

Cl inica l Avian Medic ine - Volume I I774
34_Orthopedic.qxd 8/23/2005 4:56 PM Page 774