Embed Size (px)
Citation preview
Surgical Options in Young Adultswith Aortic Valve Disease
Lars G. Svensson, MD, PhD, Eugene H. Blackstone, MD,and Delos M. Cosgrove III, MD
As the United States’ and first-world populations age, valve surgery hascome to represent an increasingly large share of cardiac operations.Furthermore, in the younger adult population between the ages of 20 and60 years, valve surgery is among the most common cardiac operations.An ideal aortic valve prosthesis for these patients would be easilyimplanted, durable, and have few late complications. Unfortunately, sucha valve does not exist. Therefore, the choice of valve procedure in thisyoung patient population is difficult, because valve durability has to beweighed against risk of long-term morbidity from anticoagulation. Valveselection in young adults is a dilemma we frequently face and that we willaddress in this review, which is based on our experience and reportedliterature.
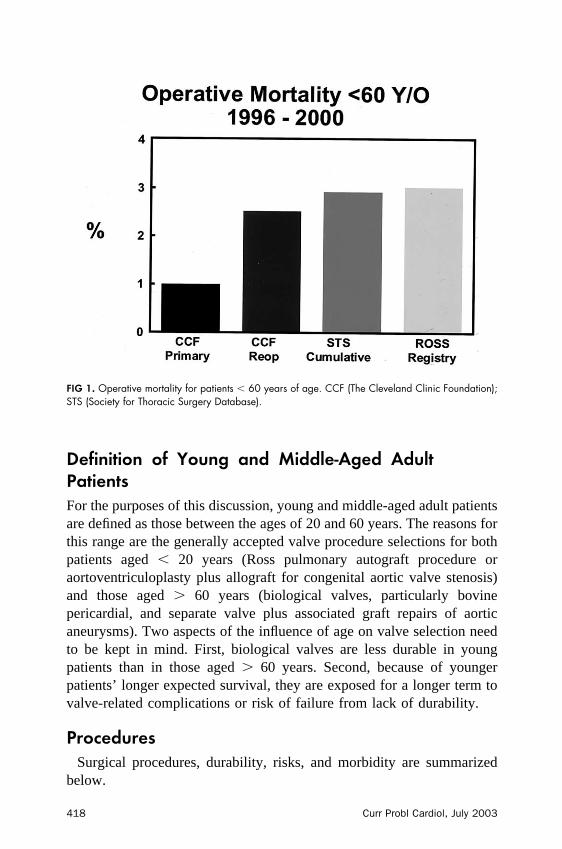
In 2001, our department at The Cleveland Clinic Foundation performed3,791 surgical procedures, 2,001 (53%) of them valve related. Of these,1,050 were aortic valve procedures (964 replacements, 86 repairs), with2% mortality. Of the 964 valve replacements, 76% were bioprostheses,13% allografts, and 11% mechanical valves. For isolated aortic valves,including reoperations (51% of which were done using a minimallyinvasive approach), mortality was 0.75%. Fig 1 shows operative mortalityfrom 1996 to 2000 for patients� 60 years of age.
Herein we present the merits and drawbacks of valve types andprocedures and offer some guidelines for a more informed choice foryoung adults, based on patient comorbid disease.
From the Department of Thoracic and Cardiovascular Surgery, The Cleveland Clinic Foundation, Cleveland,Ohio, USA.*Reprint requests: Lars G. Svenson, MD, PhD, The Cleveland Clinic Foundation, Department of Thoracic andCardiovascular Surgery, 9500 Euclid Avenue/Desk F25, Cleveland, OH 44195.E-mail: [email protected] Probl Cardiol 2003;28:417-479.0146-2806/2003/$30.00 � 0doi:10.1016/j.cpcardiol.2003.08.002
Curr Probl Cardiol, July 2003 417
Definition of Young and Middle-Aged AdultPatientsFor the purposes of this discussion, young and middle-aged adult patientsare defined as those between the ages of 20 and 60 years. The reasons forthis range are the generally accepted valve procedure selections for bothpatients aged � 20 years (Ross pulmonary autograft procedure oraortoventriculoplasty plus allograft for congenital aortic valve stenosis)and those aged � 60 years (biological valves, particularly bovinepericardial, and separate valve plus associated graft repairs of aorticaneurysms). Two aspects of the influence of age on valve selection needto be kept in mind. First, biological valves are less durable in youngpatients than in those aged � 60 years. Second, because of youngerpatients’ longer expected survival, they are exposed for a longer term tovalve-related complications or risk of failure from lack of durability.
ProceduresSurgical procedures, durability, risks, and morbidity are summarized
below.
FIG 1. Operative mortality for patients � 60 years of age. CCF (The Cleveland Clinic Foundation);STS (Society for Thoracic Surgery Database).
418 Curr Probl Cardiol, July 2003
Mechanical Valve ProsthesesMost currently used mechanical valve prostheses can be divided into 2
categories: unileaflet tilting disc and bileaflet. Unileaflet and ball valvesare less commonly used because of the greater excursion of the leafletabove the anulus, additional care needed to insert them, embolization risk,and greater noise compared to bileaflet valves. They will not be discussedfurther.
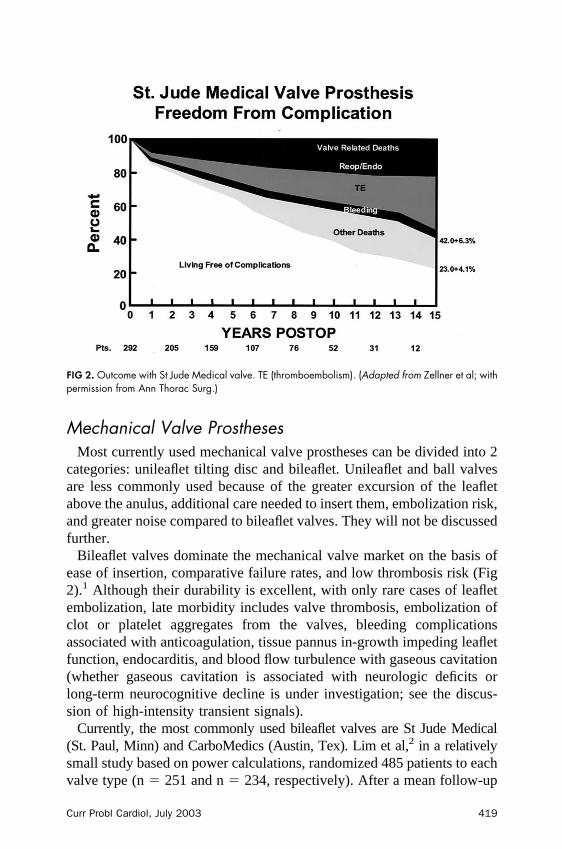
Bileaflet valves dominate the mechanical valve market on the basis ofease of insertion, comparative failure rates, and low thrombosis risk (Fig2).1 Although their durability is excellent, with only rare cases of leafletembolization, late morbidity includes valve thrombosis, embolization ofclot or platelet aggregates from the valves, bleeding complicationsassociated with anticoagulation, tissue pannus in-growth impeding leafletfunction, endocarditis, and blood flow turbulence with gaseous cavitation(whether gaseous cavitation is associated with neurologic deficits orlong-term neurocognitive decline is under investigation; see the discus-sion of high-intensity transient signals).
Currently, the most commonly used bileaflet valves are St Jude Medical(St. Paul, Minn) and CarboMedics (Austin, Tex). Lim et al,2 in a relativelysmall study based on power calculations, randomized 485 patients to eachvalve type (n � 251 and n � 234, respectively). After a mean follow-up
FIG 2. Outcome with St Jude Medical valve. TE (thromboembolism). (Adapted from Zellner et al; withpermission from Ann Thorac Surg.)
Curr Probl Cardiol, July 2003 419

of 50 � 22 months and 47 � 20 months, respectively, 5-year survival was80% � 2.8% and 82% � 2.6% (P � .7). The valves were also similarwith respect to freedom from valve-related mortality (95.9% vs 96.7%),major thromboembolism (92.5% vs 90.9%), hemorrhage (83% vs 87%),nonstructural valve dysfunction (96.0% vs 96.1%), and prosthetic aorticvalve endocarditis at 5 years. Emery et al3 recently presented 20-year dataon 269 aortic valve replacements in patients aged � 50 years (mean 40years); operative mortality was 1.5%, and there were 21 late deaths, 4valve related. The events are summarized below:
● Endocarditis: 0.15% per patient-year, 98.9% freedom at 20 years● Perivalvular leak: 0.3% per patient-year, 96% freedom at 20 years● Thromboembolic events: 0.3% per patient-year, 94% freedom at 20
years● Valve thrombosis: 0.1% per patient-year, 99% freedom at 20 years● Hemorrhage: 0.16% per patient-year, 98.9% freedom at 20 years
Although these valves are considerably better than older devices, they stillrequire anticoagulation—the bane of mechanical valves.
Newer bileaflet valves have also been marketed, both because the earlierbileaflet patent has expired and because companies are attempting toproduce improved mechanical valves that may require lower levels ofanticoagulation. These include the St Jude Regent, Sorin, Duromedics,ATS, Medtronic-Hall, and On-X. Currently, most of these are not readilyavailable in the United States, or long-term follow-up is still needed. Datafrom the US Food and Drug Administration (FDA) application for theATS valve, reported by Emery et al,4 show that the valve has similaroutcomes to other bileaflet valves, although the thromboembolic rate was3.8% per patient-year. The On-X valve is made of pure carbon rather thanpyrolytic carbon, resulting in what is claimed to be a less thrombogenicsurface. The thromboembolic event rate has been reported as 1.7% perpatient-year.5 Whether these newer valves will have lower transvalvargradients, less hemolysis, fewer perceived valve-related clicks, and lowerthrombogeneity than the older St Jude Medical and CarboMedics pros-theses remains to be established. Ideally, a mechanical valve will bedeveloped that does not require warfarin anticoagulation.
In an extensive review of mechanical valve complication rates, Akins6
concluded that there were no major advantages for any single valve,although he noted that long-term results favored St Jude Medical andMedtronic-Hall.
CarboMedics, Inc, asked David et al7 to evaluate outcomes aftermechanical valve insertions in North America. They likewise found no
420 Curr Probl Cardiol, July 2003

major differences among valves. They questioned the methodology usedin Akins’ study, particularly how 30-day events were analyzed in thecalculated linearized rates. Akins responded that early events wereincluded in the calculations.
Based on David et al’s report,7 the mean aortic valve thrombosis riskwas as follows (Fig 3): CarboMedics valve based on accumulated series,0.2% per patient-year; Medtronic-Hall, 0.2% per patient-year; and St JudeMedical, 0.1% per patient-year (P � .37). The mean linearized rates forthromboembolism, both major and minor, were as follows: CarboMedics,0.8% per patient-year; Medtronic-Hall, 1.5% per patient-year; and St JudeMedical, 1.9% per patient-year (P � .14). Mean rates of major valvehemorrhage were as follows: CarboMedics, 1.25% per patient-year;Medtronic-Hall, 0.6% per patient-year; and St Jude Medical, 1.3% perpatient-year (P � .37).
Intensity of Anticoagulation. Intensity of anticoagulation influences thepresumed inverse relationship between hemorrhagic events and thrombo-embolic events for these valves. Chang et al8 found no long-termdifference between St Jude Medical (n � 641) and CarboMedics (n �601) valves in this regard. Nonetheless, when they intensified anticoag-ulation follow-up by seeing patients more frequently and more carefullyadjusting anticoagulation, 5-year freedom from bleeding fell from 99.3%to 96.1% (P � .0004), and thromboembolism improved from 96.7% to
FIG 3. Rates of mechanical valve thrombosis according to FDA data. (Adapted from David et al; withpermission from Ann Thorac Surg.)
Curr Probl Cardiol, July 2003 421
99.0% (P � .031). Although it is generally held that there is an inverserelationship between risk of thromboembolism and risk of bleedingaccording to anticoagulation, this has recently been challenged byButchart et al,9 who stressed that anticoagulation variability is a moreimportant factor in long-term survival.
Echocardiographically and by Doppler analysis, mechanical bileafletvalves have flow characteristics associated with the particular valvedynamics. Thus, bileaflet valves require a degree of regurgitation toensure washing of the leaflets and hinges to thus prevent clot formation inareas of reduced flow or turbulence. Intraoperatively perivalvular jets alsoappear to be more common after replacement;10 however, in more thanhalf of patients, these jets resolve with administration of protamine andrequire no further treatment.
High-Intensity Transient Signals. There appear to be differences in theprevalence of Doppler microembolic signals that are intriguing yet remainto be fully explained. Whether these signals have any neurologicconsequences is unclear. For example, in healthy volunteers, high-intensity transient Doppler signals (HITS) are not detected, whereas theyoccur in most patients after mechanical valve replacement (P � .05) andoccasionally after the Ross procedure.11 Similarly, HITS occur afterallograft replacement, although less frequently than after mechanicalvalve replacement (P � .02). Nevertheless, allografts have a greaternumber of HITS than do controls (P � .02). Mechanical valves are alsoassociated with a greater number (P � .05) and amplitude (P � .0001) ofHITS, although there is no association or difference in the occurrence offocal neurologic deficits.12 Biological valves appear to have fewer HITSthan mechanical valves.
In a study of 580 valve replacements, Sliwka and Georgiadis13 foundthe prevalence of HITS for mechanical valves to be 92% for theBjork-Shiley Monostrut valve, 81% for CarboMedics valves, 72% for StJude Medical, 71% for Tekna Duromedics, 52% for ATS, and 47% forMedtronic-Hall tilting disc valves; and for biological valves to be 39% forCarpentier-Edwards Supraannular, and 9% for Sorin biological valves.There was no relationship to valve size, degree of anticoagulation, patientage, implantation duration, or neurologic symptoms. This lack of clinicalcorrelation has been reported by others as well,14 although no largelongitudinal study has looked at long-term neurocognitive function;however Deklunder et al14a did report cognitive changes. Orientation ofthe valve in the aortic anulus influences HITS counts per minute,particularly for the Medtronic-Hall valve,15 and optimal orientationreduces the incidence for the latter valve.
422 Curr Probl Cardiol, July 2003
HITS appear to be nitrogen bubbles created by cavitation in thebloodstream from turbulence and high shear stress areas. One study foundthat 100% inhaled oxygen reduced the incidence of HITS, whereasmanipulation of pressure in a hyperbaric chamber increased it, confirminga gaseous etiology.16 The bubbles disintegrate within milliseconds and donot appear to obstruct brain circulation.
In our analysis (see Statistical section) of 3,583 mechanical prosthesesby multivariable analysis, there were no early postoperative, constant, orlate hazard phase differences in mortality for various mechanical valvereplacements.
Summary. Although bileaflet valves have excellent durability, latemorbidity is of concern, particularly because patients with normal leftventricular function and without coronary artery disease or hypertensionare expected to have a life expectancy commensurate with the age-matched population.17
Xenograft Biological Valve ProsthesesXenograft biological valves can be divided into 2 categories: bovine
pericardial and porcine native aortic. These can each be further subdi-vided into the categories of stented and stentless mounting.
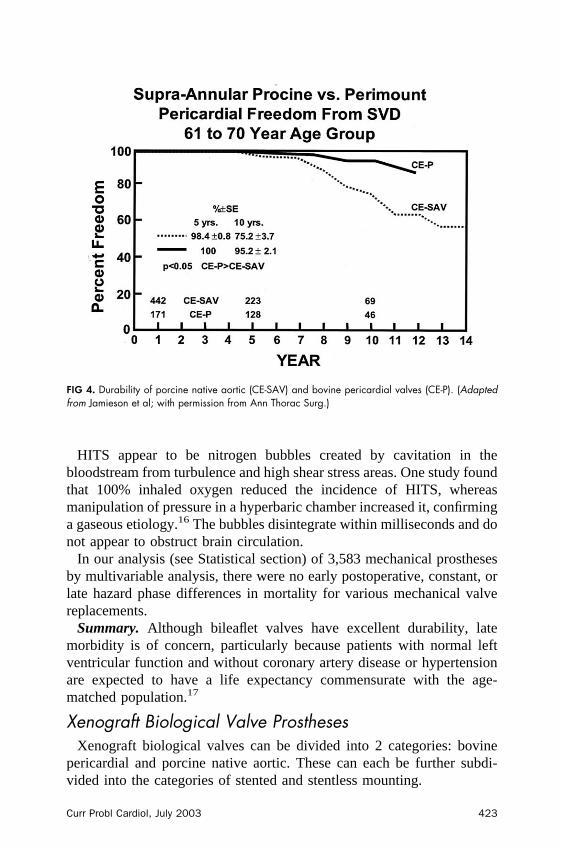
FIG 4. Durability of porcine native aortic (CE-SAV) and bovine pericardial valves (CE-P). (Adaptedfrom Jamieson et al; with permission from Ann Thorac Surg.)
Curr Probl Cardiol, July 2003 423
The problem with xenograft bovine pericardial valves or porcine nativevalves is limited durability (Fig 4).18 Deterioration in leaflets is progres-sive, and therefore definitions of structural valve deterioration vary.Explantation of valves for deterioration, however, is a “hard” end point.Nonetheless, because of these definition problems, results of long-termoutcome reported by various authors cannot easily be compared. It shouldbe noted that in our experience, only two thirds of explanted valves are forstructural valve deterioration.
Porcine Xenografts: Stented. Currently, the most used stented porcinexenografts are the Hancock II (and its derivatives) and the Carpentier-Edwards valve. Stented porcine valves have not been reported to be asdurable in young patients. Ten-year freedom from structural deteriorationfor stented porcine xenografts is between 76%19 and 91%.6,20,21 David etal22 reported a 12-year follow-up of 723 patients with a Hancock IIporcine valve. Prevalence of primary tissue failure was greater in patientsaged � 65 years (n � 9, 84% freedom).22,23 Subsequently, David et alreported that the Hancock II valve was associated with worse survival and50% 8-year freedom from all valve events, compared with 81% for theToronto stentless valve.24 These findings, however, may be influenced byselection bias, because stentless valves are avoided in patients withcalcified roots and extensive coronary artery disease and are frequentlyused in younger patients.
Porcine Xenografts: Stentless. With the exception of the Torontoexperience,24 stentless valves have been associated with unreasonablyhigh perioperative mortality, particularly for aortic root replacements.Doty et al25 report that mortality for 1,163 patients in the FDA trial was5.0% for subcoronary implants and 11.7% for root replacements. Simi-larly, in the report by Dagenais et al26 it was 6.2% overall and 20.3% for69 root replacements. It should be noted that perioperative mortality isoften excluded from long-term survival curve calculations based on STSguidelines. Mortality has been reduced by both increased experience andbetter patient selection.27
Reoperation because of root calcification of stentless porcine valves isexpected to be more complicated than with stented xenografts ormechanical prostheses, and possibly will be associated with greatermortality. Indeed, in a recent report by Luciani et al,27a stentless valveswere found to be less durable. Freedom from reoperation was lower in 5types of stentless valves when compared to Hancock II (Medtronic Inc,Minneapolis, Minn) stented porcine valves (at 8 years 90% vs 99%, P �.0009). Similarly, on multivariable analysis, stentless valves had a greater
424 Curr Probl Cardiol, July 2003
risk of reoperation (P � .05). Furthermore, mortality for reoperation forstentless valves was 17.6% versus none for stented valves (3/17 vs 0/2).
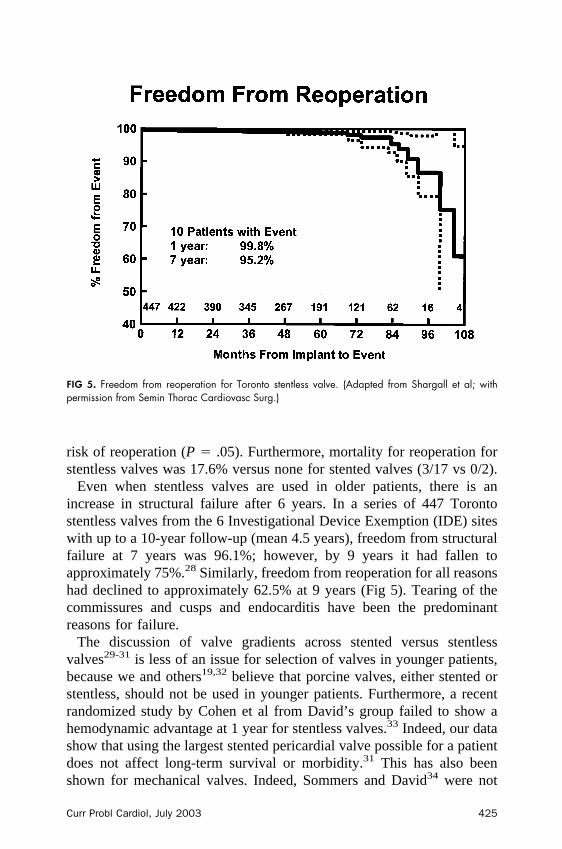
Even when stentless valves are used in older patients, there is anincrease in structural failure after 6 years. In a series of 447 Torontostentless valves from the 6 Investigational Device Exemption (IDE) siteswith up to a 10-year follow-up (mean 4.5 years), freedom from structuralfailure at 7 years was 96.1%; however, by 9 years it had fallen toapproximately 75%.28 Similarly, freedom from reoperation for all reasonshad declined to approximately 62.5% at 9 years (Fig 5). Tearing of thecommissures and cusps and endocarditis have been the predominantreasons for failure.
The discussion of valve gradients across stented versus stentlessvalves29-31 is less of an issue for selection of valves in younger patients,because we and others19,32 believe that porcine valves, either stented orstentless, should not be used in younger patients. Furthermore, a recentrandomized study by Cohen et al from David’s group failed to show ahemodynamic advantage at 1 year for stentless valves.33 Indeed, our datashow that using the largest stented pericardial valve possible for a patientdoes not affect long-term survival or morbidity.31 This has also beenshown for mechanical valves. Indeed, Sommers and David34 were not
FIG 5. Freedom from reoperation for Toronto stentless valve. (Adapted from Shargall et al; withpermission from Semin Thorac Cardiovasc Surg.)
Curr Probl Cardiol, July 2003 425
able to show a survival advantage with the frequent use of patchenlargements of the aortic anulus.34-36 In our analysis of 13,258 aorticvalve replacements, prosthesis patient size down to at least 1.1 cm2/m2 or�3z did not adversely affect intermediate or long-term survival (P � .2;see Statistics section).
Although there appears to be no convincing studies showing a benefitfor stentless valves compared to stented valves, it is possible that withvigorous exercise or echocardiographic stress testing there may be abenefit.
In a patient with severe congenital aortic valve stenosis with a small leftventricular outflow tract, we, however, would consider an allograft as anoption without having to resort to a root enlargement procedure in mostpatients. However, if the stenosis is particularly severe, usually congen-ital, an aortoventriculoplasty using an allograft with a right ventricularoutflow tract enlargement with a patch is an excellent operation to relievethis problem, as we have described previously. Use of the Ross procedurein this situation is also an option.37
Thus, the hemodynamic performance of biological valves appears to begood. In addition, compared to mechanical valves, HITS are lesscommon.
Bovine Pericardial Valves: Stented. Bovine pericardial valves, specif-ically the Carpentier-Edwards valve, have been reported to be reasonablydurable in young patients. The Carpentier-Edwards pericardial aorticvalve was designed to minimize cusp stress and reduce abrasion wear onthe leaflets.38 This was achieved by placing the cusp between 2 pillars atthe flexible valve struts rather than over the struts. The Carpentier-Edwards valve also has better hemodynamic performance than stentedporcine valves of equivalent outflow diameter. In an intraoperative studyby Cosgrove et al,21 the bovine pericardial valve was found to have agreater functional orifice area, higher performance indices, and lowergradients than porcine valves.
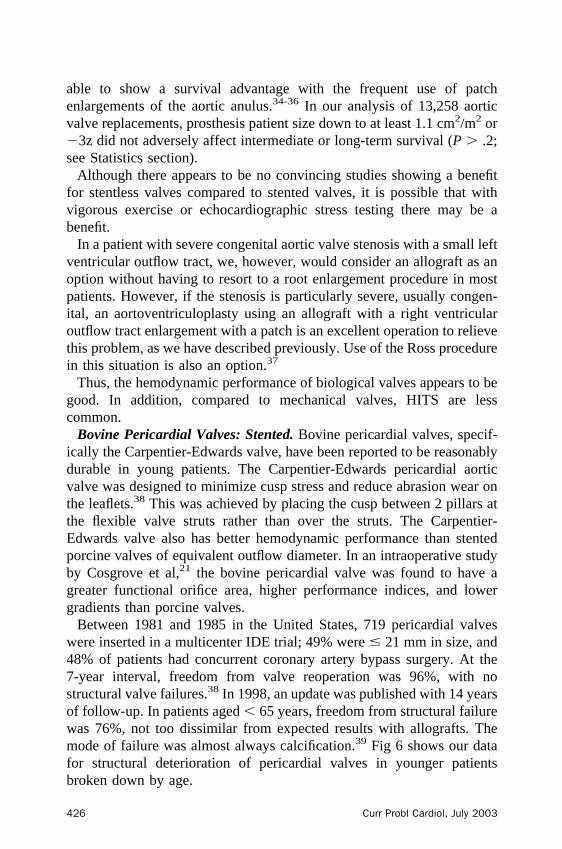
Between 1981 and 1985 in the United States, 719 pericardial valveswere inserted in a multicenter IDE trial; 49% were � 21 mm in size, and48% of patients had concurrent coronary artery bypass surgery. At the7-year interval, freedom from valve reoperation was 96%, with nostructural valve failures.38 In 1998, an update was published with 14 yearsof follow-up. In patients aged � 65 years, freedom from structural failurewas 76%, not too dissimilar from expected results with allografts. Themode of failure was almost always calcification.39 Fig 6 shows our datafor structural deterioration of pericardial valves in younger patientsbroken down by age.
426 Curr Probl Cardiol, July 2003
In a subanalysis of 310 of the above patients, Cosgrove et al40 foundsimilar results, with 96% freedom from explantation at 10 years and 89%for patients aged � 65 years. Of the 12 failures, 11 were fromcalcification causing stenosis and 1 was from wear-related leaflet tear.When analyzed for actual freedom from deterioration for patients aged �65 years, freedom from explantation was 94%. With the actual method ofanalysis, patient deaths are censored because they would not obviously beat risk for developing valve failure. Interestingly, by Cox proportionalhazard analysis, age was not a risk factor for structural valve failure,although more recent data show this to be the case (see Statistics section).
It should be noted that in most studies, 14- or 15-year survival has beenbetween 35% and 40%. Thus, because of patients’ comorbid disease, theiraortic valves outperformed their life expectancy, and only about 10%required reoperation for valve failure. Banbury et al41 examined in greaterdetail the influence of age and valve size at the time of implantation onlate outcome. Freedom from explantation for valve structural dysfunctionat 15 years had declined to 77%, and younger age of initial implantationwas a predictor, although implanted valve prosthetic size was not.
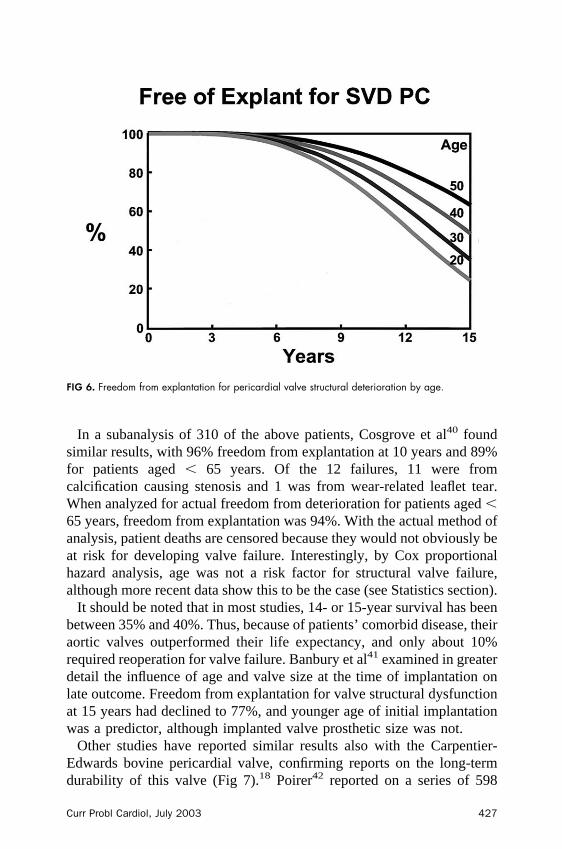
Other studies have reported similar results also with the Carpentier-Edwards bovine pericardial valve, confirming reports on the long-termdurability of this valve (Fig 7).18 Poirer42 reported on a series of 598
FIG 6. Freedom from explantation for pericardial valve structural deterioration by age.
Curr Probl Cardiol, July 2003 427
aortic valve replacements between 1981 and 1996, with 24% of patientsaged � 60 years. The respective 10- and 14-year freedom from aorticstructural dysfunction was 93% and 80%. Marchand et al43 reported 435patients operated on between 1984 and 1989 at 7 institutions, with anactual freedom from explantation for valve failure of 83.4% at 14 years.Nakajima et al44 examined their experience with 19-mm pericardialvalves used in small aortic roots and found that at 12 years, freedom fromreoperation for valve failure was 92%.
In our recent analysis of 3,819 pericardial valves (see Statistics section),the 15-year survival was 30%; however, when adjusted for age ofimplantation and comorbid disease, survival was no different than othervalves—namely, 68% for patients aged � 50 years, 35% for patients aged50 to 75 years, and 2% for patients aged � 75 years. Our data show that,particularly for young patients aged � 50 years, but less so for elderlypatients (aged � 75 years), long-term survival is reduced when comparedto the general population, largely because of comorbid disease (seeStatistical section). Clearly, comorbid disease in young patients mustinfluence valve selection.
Data collected by Edward Lifesciences Corporation on the original 267aortic PERIMOUNT valves inserted between September 1981 and
FIG 7. Structural valve deterioration by age. (Adapted from Jamieson et al; with permission from AnnThorac Surg.)
428 Curr Probl Cardiol, July 2003
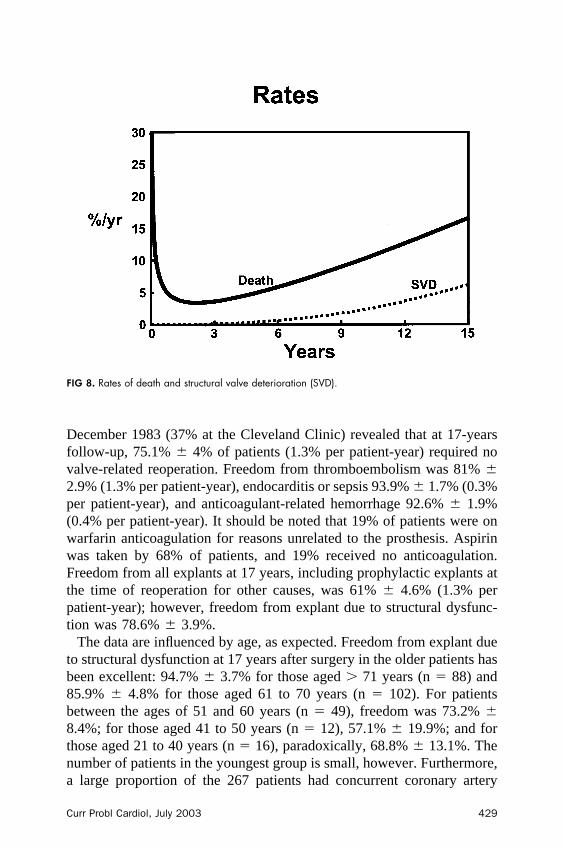
December 1983 (37% at the Cleveland Clinic) revealed that at 17-yearsfollow-up, 75.1% � 4% of patients (1.3% per patient-year) required novalve-related reoperation. Freedom from thromboembolism was 81% �2.9% (1.3% per patient-year), endocarditis or sepsis 93.9% � 1.7% (0.3%per patient-year), and anticoagulant-related hemorrhage 92.6% � 1.9%(0.4% per patient-year). It should be noted that 19% of patients were onwarfarin anticoagulation for reasons unrelated to the prosthesis. Aspirinwas taken by 68% of patients, and 19% received no anticoagulation.Freedom from all explants at 17 years, including prophylactic explants atthe time of reoperation for other causes, was 61% � 4.6% (1.3% perpatient-year); however, freedom from explant due to structural dysfunc-tion was 78.6% � 3.9%.
The data are influenced by age, as expected. Freedom from explant dueto structural dysfunction at 17 years after surgery in the older patients hasbeen excellent: 94.7% � 3.7% for those aged � 71 years (n � 88) and85.9% � 4.8% for those aged 61 to 70 years (n � 102). For patientsbetween the ages of 51 and 60 years (n � 49), freedom was 73.2% �8.4%; for those aged 41 to 50 years (n � 12), 57.1% � 19.9%; and forthose aged 21 to 40 years (n � 16), paradoxically, 68.8% � 13.1%. Thenumber of patients in the youngest group is small, however. Furthermore,a large proportion of the 267 patients had concurrent coronary artery
FIG 8. Rates of death and structural valve deterioration (SVD).
Curr Probl Cardiol, July 2003 429
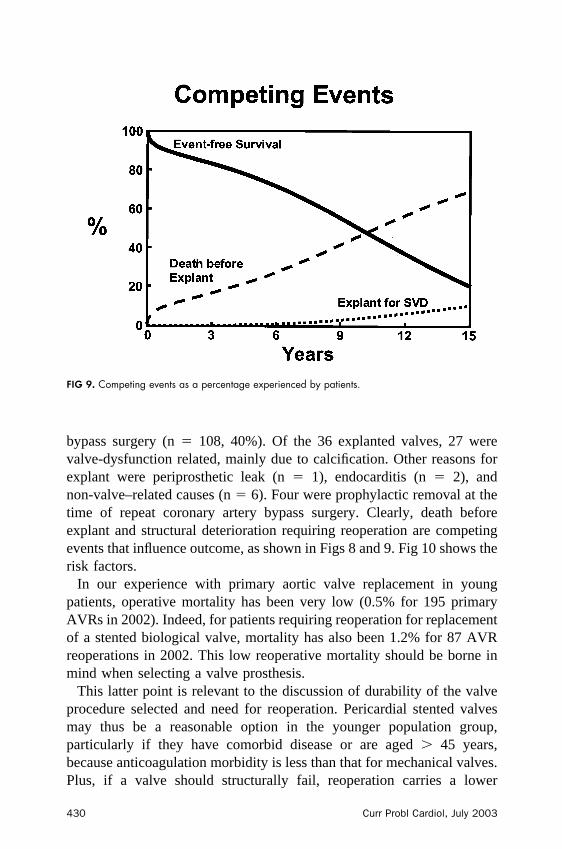
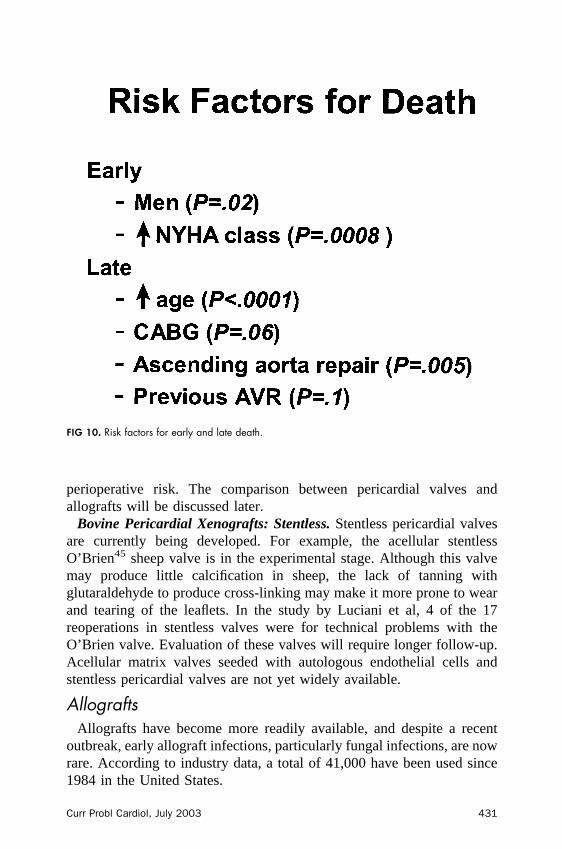
bypass surgery (n � 108, 40%). Of the 36 explanted valves, 27 werevalve-dysfunction related, mainly due to calcification. Other reasons forexplant were periprosthetic leak (n � 1), endocarditis (n � 2), andnon-valve–related causes (n � 6). Four were prophylactic removal at thetime of repeat coronary artery bypass surgery. Clearly, death beforeexplant and structural deterioration requiring reoperation are competingevents that influence outcome, as shown in Figs 8 and 9. Fig 10 shows therisk factors.
In our experience with primary aortic valve replacement in youngpatients, operative mortality has been very low (0.5% for 195 primaryAVRs in 2002). Indeed, for patients requiring reoperation for replacementof a stented biological valve, mortality has also been 1.2% for 87 AVRreoperations in 2002. This low reoperative mortality should be borne inmind when selecting a valve prosthesis.
This latter point is relevant to the discussion of durability of the valveprocedure selected and need for reoperation. Pericardial stented valvesmay thus be a reasonable option in the younger population group,particularly if they have comorbid disease or are aged � 45 years,because anticoagulation morbidity is less than that for mechanical valves.Plus, if a valve should structurally fail, reoperation carries a lower
FIG 9. Competing events as a percentage experienced by patients.
430 Curr Probl Cardiol, July 2003
perioperative risk. The comparison between pericardial valves andallografts will be discussed later.
Bovine Pericardial Xenografts: Stentless. Stentless pericardial valvesare currently being developed. For example, the acellular stentlessO’Brien45 sheep valve is in the experimental stage. Although this valvemay produce little calcification in sheep, the lack of tanning withglutaraldehyde to produce cross-linking may make it more prone to wearand tearing of the leaflets. In the study by Luciani et al, 4 of the 17reoperations in stentless valves were for technical problems with theO’Brien valve. Evaluation of these valves will require longer follow-up.Acellular matrix valves seeded with autologous endothelial cells andstentless pericardial valves are not yet widely available.
AllograftsAllografts have become more readily available, and despite a recent
outbreak, early allograft infections, particularly fungal infections, are nowrare. According to industry data, a total of 41,000 have been used since1984 in the United States.
FIG 10. Risk factors for early and late death.
Curr Probl Cardiol, July 2003 431
Theoretically, allografts are the ideal valve replacements for thefollowing reasons:
● They are human tissue and are known to function well after hearttransplantation with immune suppresion in the long term, withoutdeterioration.46
● They have a central blood flow with low transvalvar gradients, evenwith vigorous exercise in patients with an active lifestyle.
● They appear to resist bacterial endocarditis, although not entirely, andeven when the indication for insertion is native valve endocarditis, riskof recurrent endocarditis is low.
● Risk of thromboembolic events is very low.
The disadvantage of allografts is the immunologic response they mayelicit, particularly in young adults and children, including prolongedfevers and resultant limited durability, often resulting in calcification anddegeneration of the leaflets and aortic wall. Fever may be related tolow-grade rejection47-50 and occurs in up to 26% of patients, according toShapira.51 This has resulted in some surgeons instituting low-doseimmunosuppression or administration of anti-inflammatory medications,
FIG 11. Freedom from structural valve deterioration of aortic allografts according to preservationmethod: viable cryopreserved versus 4°C storage. (Adapted from O’Brien et al; with permission fromJ Heart Valve Dis.)
432 Curr Probl Cardiol, July 2003
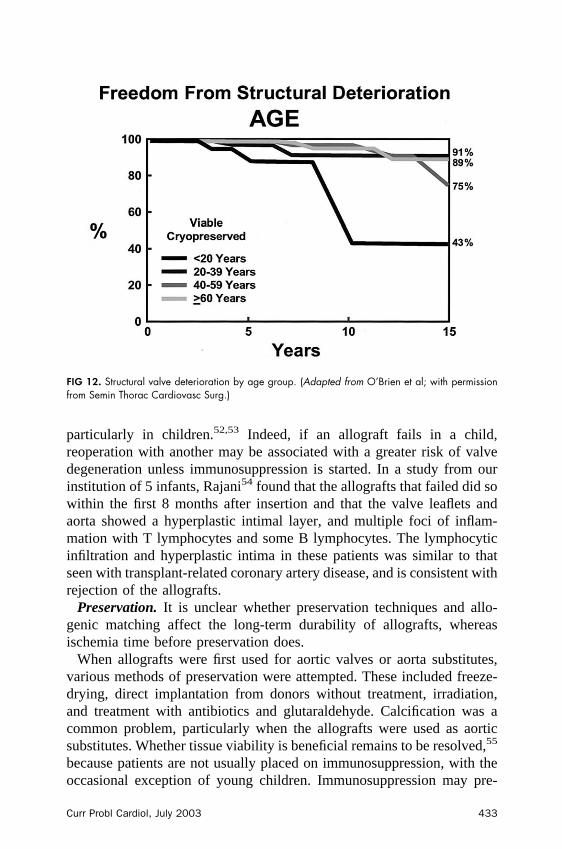
particularly in children.52,53 Indeed, if an allograft fails in a child,reoperation with another may be associated with a greater risk of valvedegeneration unless immunosuppression is started. In a study from ourinstitution of 5 infants, Rajani54 found that the allografts that failed did sowithin the first 8 months after insertion and that the valve leaflets andaorta showed a hyperplastic intimal layer, and multiple foci of inflam-mation with T lymphocytes and some B lymphocytes. The lymphocyticinfiltration and hyperplastic intima in these patients was similar to thatseen with transplant-related coronary artery disease, and is consistent withrejection of the allografts.
Preservation. It is unclear whether preservation techniques and allo-genic matching affect the long-term durability of allografts, whereasischemia time before preservation does.
When allografts were first used for aortic valves or aorta substitutes,various methods of preservation were attempted. These included freeze-drying, direct implantation from donors without treatment, irradiation,and treatment with antibiotics and glutaraldehyde. Calcification was acommon problem, particularly when the allografts were used as aorticsubstitutes. Whether tissue viability is beneficial remains to be resolved,55
because patients are not usually placed on immunosuppression, with theoccasional exception of young children. Immunosuppression may pre-
FIG 12. Structural valve deterioration by age group. (Adapted from O’Brien et al; with permissionfrom Semin Thorac Cardiovasc Surg.)
Curr Probl Cardiol, July 2003 433
serve and protect viable donor cells from the hosts and immunologicattack.
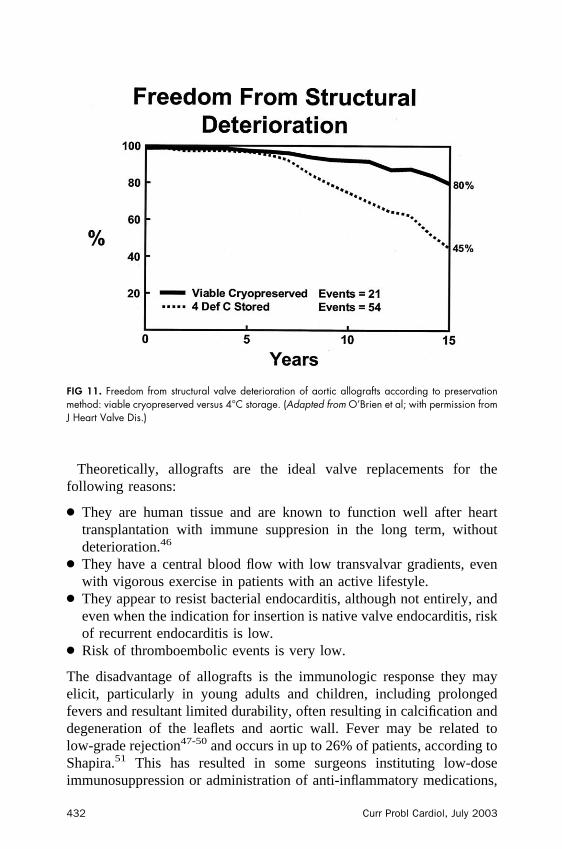
Current methods of preservation concentrate on either cold storage at4°C with antibiotic-impregnated growth media to preserve viability(homovital valves) and implantation within 3 days,55,56 or freezing inliquid nitrogen to �196°C in a solution with antibiotics and 10%dimethyl sulfoxide (DMSO). The latter approach was pioneered byO’Brien and is the method most commonly used by companies thatsupply allografts in the United States.57,58 Whether these valves showevidence of being viable after rewarming and thawing is controver-sial.55,57-61 The critical factor appears to be the warm ischemia timebefore harvesting.
Results from centers using different preservation techniques havegenerally been similar. Yacoub’s group,56 using antibiotic sterilizedhomovital allografts inserted mostly � 3 days after harvesting, reported97% 10-year freedom from valve degeneration in patients aged � 30years. O’Brien et al,57,58 using valves cryopreserved in liquid nitrogen forpatients aged � 20 years, reported freedom from valve degeneration ofapproximately 90% at 10 years.
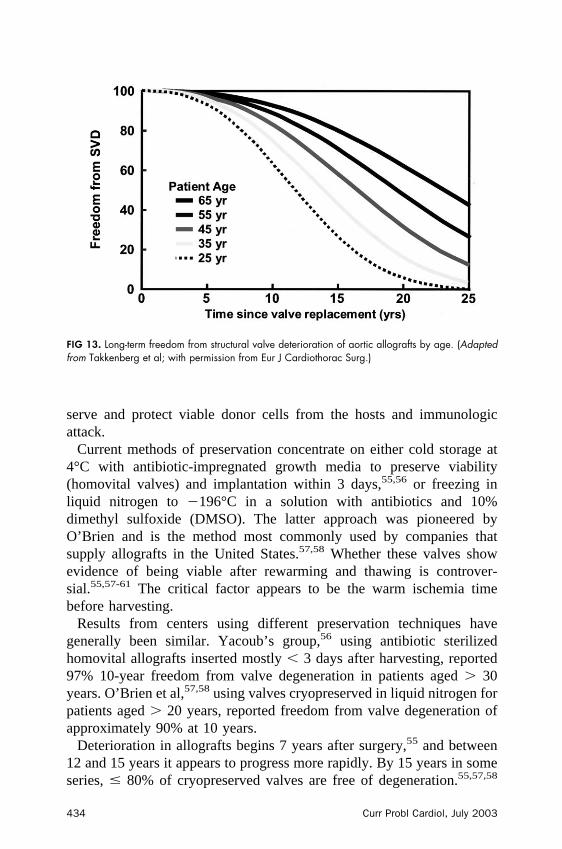
Deterioration in allografts begins 7 years after surgery,55 and between12 and 15 years it appears to progress more rapidly. By 15 years in someseries, � 80% of cryopreserved valves are free of degeneration.55,57,58
FIG 13. Long-term freedom from structural valve deterioration of aortic allografts by age. (Adaptedfrom Takkenberg et al; with permission from Eur J Cardiothorac Surg.)
434 Curr Probl Cardiol, July 2003
Once deterioration begins, replacement of allografts is usually neededwithin 4 to 5 years.55
Durability of allografts beyond 15 years has been a concern. It appearsthat in the large series of O’Brien,57,58 durability declined sharplyapproximately 7 years after insertion (Figs 11 and 12). This increasingrisk of failure after 7 years results in a larger proportion of patientsundergoing reoperation. In a recent analysis by O’Brien58 of 418 patientswith � 1% mortality and eradication of preoperative endocarditis,structural valve deterioration started approximately 6-and-a-half yearsafter implantation in the group aged 21 to 40 years, with similar cures inpatients aged 40 to 59 years and � 60 years (Fig 12). By 12 years,freedom from deterioration had declined to 80%. These experiencedauthors concluded that “ this lack of durability may outweigh all the otheradvantages,” although “active endocarditis may still remain its strongestindication.” A recent study by Takkenberg et al62 confirmed thesedisappointing long-term results, particularly in young patients (Fig 13).
In a 20-year experience and follow-up of 1,022 allograft replacementsimplanted as a root, O’Brien et al57 found there was a difference in20-year survival (19%), endocarditis, thromboembolism, and structuraldeterioration according to the preservation method (4°C or cryopreserva-
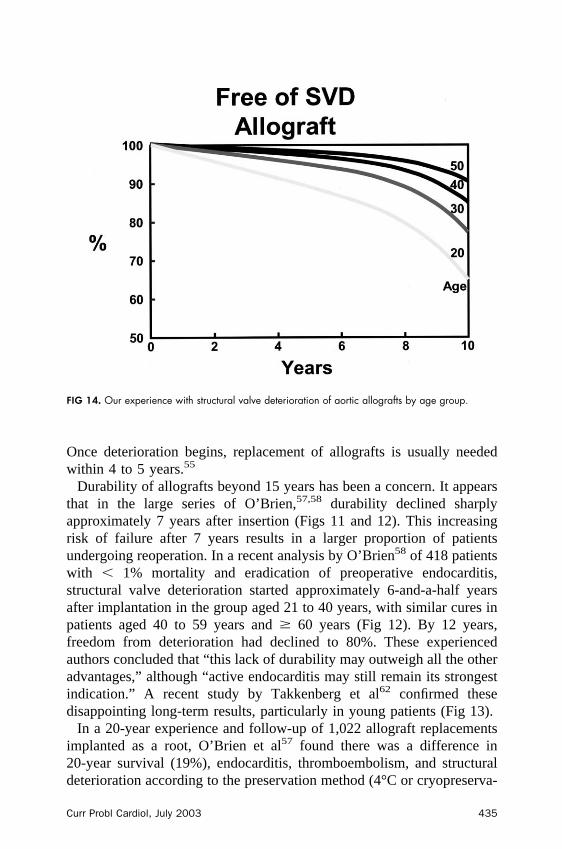
FIG 14. Our experience with structural valve deterioration of aortic allografts by age group.
Curr Probl Cardiol, July 2003 435
tion) (Fig 11). In their experience, antibiotic preserved valves at 4°C didpoorly in contradistinction to the results obtained by Yacoub’s group.56
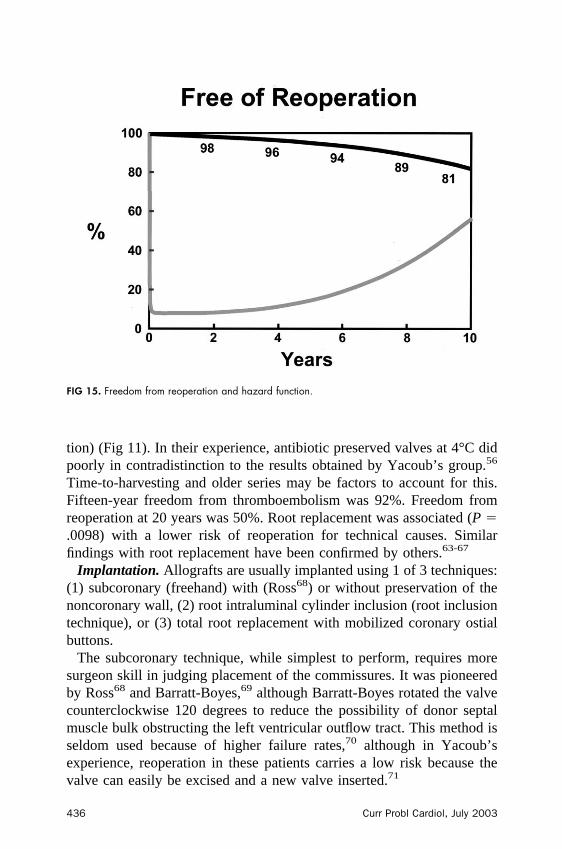
Time-to-harvesting and older series may be factors to account for this.Fifteen-year freedom from thromboembolism was 92%. Freedom fromreoperation at 20 years was 50%. Root replacement was associated (P �.0098) with a lower risk of reoperation for technical causes. Similarfindings with root replacement have been confirmed by others.63-67
Implantation. Allografts are usually implanted using 1 of 3 techniques:(1) subcoronary (freehand) with (Ross68) or without preservation of thenoncoronary wall, (2) root intraluminal cylinder inclusion (root inclusiontechnique), or (3) total root replacement with mobilized coronary ostialbuttons.
The subcoronary technique, while simplest to perform, requires moresurgeon skill in judging placement of the commissures. It was pioneeredby Ross68 and Barratt-Boyes,69 although Barratt-Boyes rotated the valvecounterclockwise 120 degrees to reduce the possibility of donor septalmuscle bulk obstructing the left ventricular outflow tract. This method isseldom used because of higher failure rates,70 although in Yacoub’sexperience, reoperation in these patients carries a low risk because thevalve can easily be excised and a new valve inserted.71
FIG 15. Freedom from reoperation and hazard function.
436 Curr Probl Cardiol, July 2003
The root intraluminal cylinder technique maintains the native geometryof the commissures, an advantage when replacing distorted native valves,and hemostatis can easily be obtained. The allograft valve anulus is sewninto position with a running suture, the coronary arteries attached to thevalve without mobilizing the ostia, and the native wall closed andwrapped around the allograft. This method may have some advantage inpatients with extensive root destruction from bacterial endocarditis, whenthere is little tissue to hemostatically anchor an allograft to the leftventricular outflow tract. The disadvantages are that the gradient may begreater across the valve and regurgitation appears to be more frequent,especially if blood between the allograft wall and the native aortatamponades the allograft. Paradoxically, absorption of the blood in thewall may result in less regurgitation with time. Alternatively, the trappedblood may cause dehiscence of the coronary artery anastomoses or anularsuture line.
Total root replacement with mobilization of the coronary artery ostialbuttons is now the most popular technique. The reasons are 4 fold:
1. Valve sizing is not critical, because the native valve tissue does notconstrict the allograft. If the native anulus is considerably enlarged itcan be narrowed either by placing horizontal plegeted sutures at thecommissures (each suture at the commissures reduces the size byapproximately 3 mm in diameter) or by placing a subanular circum-ferential left ventricular outflow tract suture.
2. Native valve distortion, particularly congenital valve deformities, canbe largely ignored because the allograft root maintains its shape.
3. Insertion does not require as much skill as freehand insertion injudging valve leaflet apposition and commissure placement.
4. Insertion technique is similar to that for a composite valve graft withmobilized buttons.72
Disadvantages are that hemostasis may be more difficult to obtain thanwith the other techniques, reoperations are more difficult if the entireallograft root has to be replaced, and risk of coronary artery injury or latestenosis may be greater.
If the valve fails, however, a new valve can be reinserted within theallograft root in approximately half of patients. Sundt et al73 reportedreoperating on 22 patients, with no early deaths but 5 late deaths inpatients who had previously undergone allograft insertions.
Events. It should be noted that there is an unfavorable bias againstallografts in statistical analyses. The reasons are 2 fold. First, earlymortality is relatively higher than for other valve replacements because a
Curr Probl Cardiol, July 2003 437
higher proportion of patients are operated on for endocarditis. Second,these endocarditis patients are more prone to late valve failures, problems,or death. Thus, the data presented below do not include them. Neverthe-less, we have previously used allografts successfully to treat endocarditisin this higher-risk group, including prosthetic endocarditis, with a lowrisk of early and late complications, including composite graft reopera-tions.74,75 Event rates related to endocarditis, bleeding, thrombosis, andstroke are generally favorable on late follow-up in patients who have hadallografts inserted. Nevertheless, some surgeons have reported higherearly mortality with allografts. Also, in our analysis of 13,258 aortic valvereplacements (see Statistics section), of which 720 were allografts, anddespite exclusion of patients with documented endocarditis, the earlypostoperative 30-day mortality rate was increased (P � .03). In 1 olderstudy, mortality for root replacements for root endocarditis approached50%.76
In the 25-year experience of primary valve replacement with 618 allograftsin Yacoub’s group,64 20-year survival was 18% and freedom from endocar-ditis 89%, primary tissue failure 18%, and valve replacement 35%. For apatient aged 70 years with a 30-year-old allograft, freedom from tissue failurewas 91% at 10 years but only 64% at 20 years—namely, less than theapproximate prevalence for a pericardial xenograft valve. For a patient aged
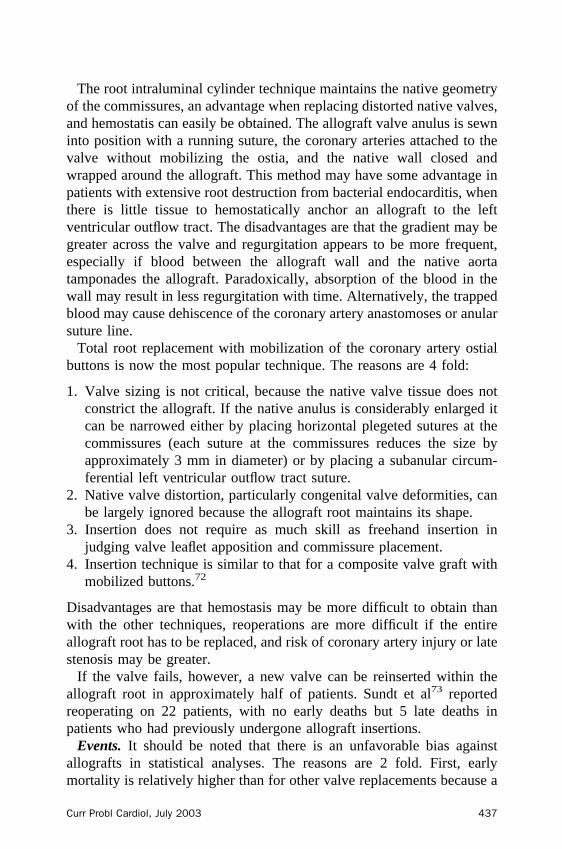
FIG 16. Modes of structural valve deterioration over time.
438 Curr Probl Cardiol, July 2003
30 years with a 30-year-old valve donor, 10- and 20-year freedom fromfailure was 82% and 39%, respectively.
In patients who had previously had allografts inserted, Yacoub’sgroup71 reported 3.4% reoperative mortality, although the majority ofthese patients had earlier subcoronary allograft insertions. Freedom froma repeat (third) operation was 97% and 82%, respectively, at 5 and 10years.
Sundt,73 when with the same group, reported that in 21 reoperations, thevalve alone was replaced within the root in 13 patients (9 mechanicalvalves, 4 subcoronary allografts). With extensive root calcification, theentire root may need to be replaced. Subcoronary reoperations do notcarry a particularly increased risk of reoperation because the valve isusually excised and a new valve inserted. However, in patients with rootreplacements, if the allograft aortic valve cannot be replaced and if theentire root has to be again replaced, the risk is not inconsequential. Insome surgeons’ experience, mortality is as high as 20%.
Figs 14 to 16 show our experience with structural valve deterioration byage, freedom from reoperation, and modes of structural valve deterioration.
Pulmonary Autografts (Ross Procedure)Despite the 3-plus decades that have passed since Ross performed the
first pulmonary autograft transfer to the aortic valve position and replaced
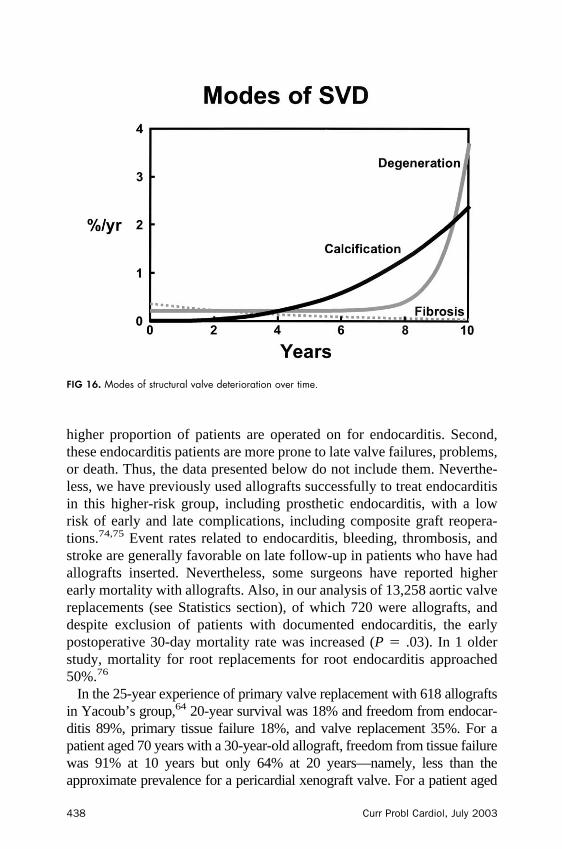
FIG 17. Freedom from aortic autograft reoperation for patients � 60 years of age.
Curr Probl Cardiol, July 2003 439

the pulmonary valve with an allograft, debate continues on the virtues ofthis procedure.
Current consensus appears to favor its use in children, particularlybecause the autograft enlarges as the patient grows. In the young adultpopulation, there is concern that the surgeon is creating 2 potentiallydiseased valves for a patient who has an expected long-term survival ofmany decades. Although early operative mortality has been reduced fromas high as 30% to � 5%, the failure rate for pulmonary-positionedallografts and aortic-positioned autografts continues to be a problem (Figs17 and 18).
Pulmonary Position. Pulmonary-positioned allograft failure requiringreoperation is an unsolved problem (see Allografts section). Patientsdevelop stenosis, with high right ventricular outflow tract gradients fromfunctional obstruction or failure of the valve, including calcification.Ross55 and others have postulated that inflammation around the allograftdue to the immunologic reaction to the viable cell-rich cryopreservedallografts is one mechanism of failure. Thus, he favors developingnonreactive, nonviable grafts.55,77 Recently developed treated allograftsor xenografts may reduce the incidence of this problem, includingglutaraldehyde-treated bovine jugular veins.
FIG 18. Freedom from pulmonary allograft reoperation in the right ventricular outflow tract (RVOT) forpatients � 60 years of age.
440 Curr Probl Cardiol, July 2003
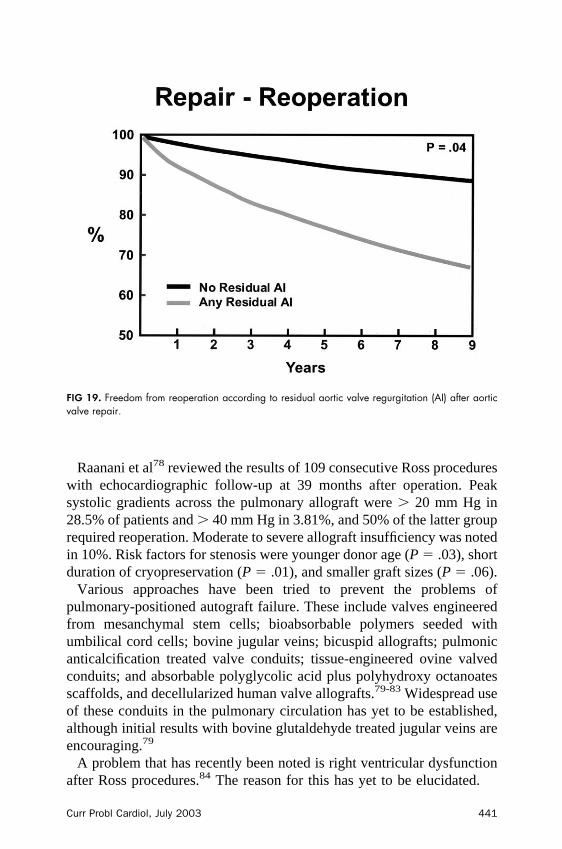
Raanani et al78 reviewed the results of 109 consecutive Ross procedureswith echocardiographic follow-up at 39 months after operation. Peaksystolic gradients across the pulmonary allograft were � 20 mm Hg in28.5% of patients and � 40 mm Hg in 3.81%, and 50% of the latter grouprequired reoperation. Moderate to severe allograft insufficiency was notedin 10%. Risk factors for stenosis were younger donor age (P � .03), shortduration of cryopreservation (P � .01), and smaller graft sizes (P � .06).
Various approaches have been tried to prevent the problems ofpulmonary-positioned autograft failure. These include valves engineeredfrom mesanchymal stem cells; bioabsorbable polymers seeded withumbilical cord cells; bovine jugular veins; bicuspid allografts; pulmonicanticalcification treated valve conduits; tissue-engineered ovine valvedconduits; and absorbable polyglycolic acid plus polyhydroxy octanoatesscaffolds, and decellularized human valve allografts.79-83 Widespread useof these conduits in the pulmonary circulation has yet to be established,although initial results with bovine glutaldehyde treated jugular veins areencouraging.79
A problem that has recently been noted is right ventricular dysfunctionafter Ross procedures.84 The reason for this has yet to be elucidated.
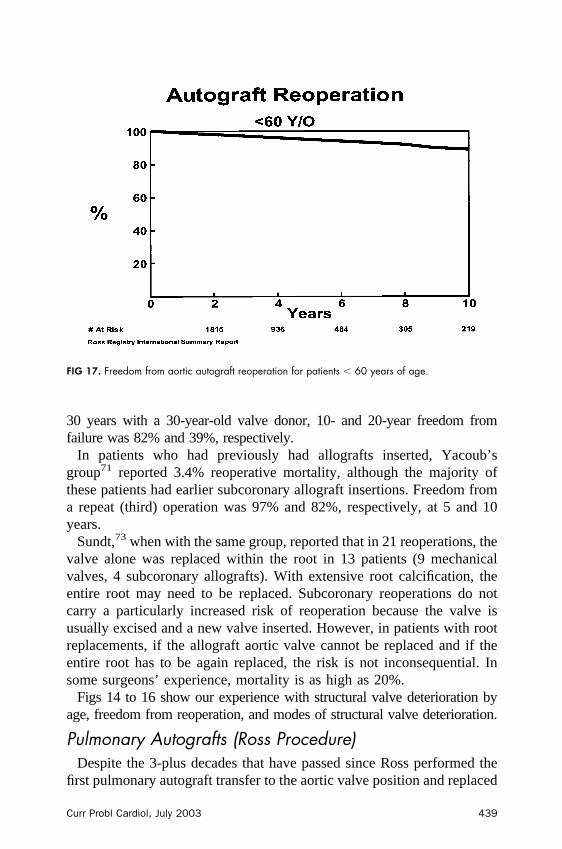
FIG 19. Freedom from reoperation according to residual aortic valve regurgitation (AI) after aorticvalve repair.
Curr Probl Cardiol, July 2003 441
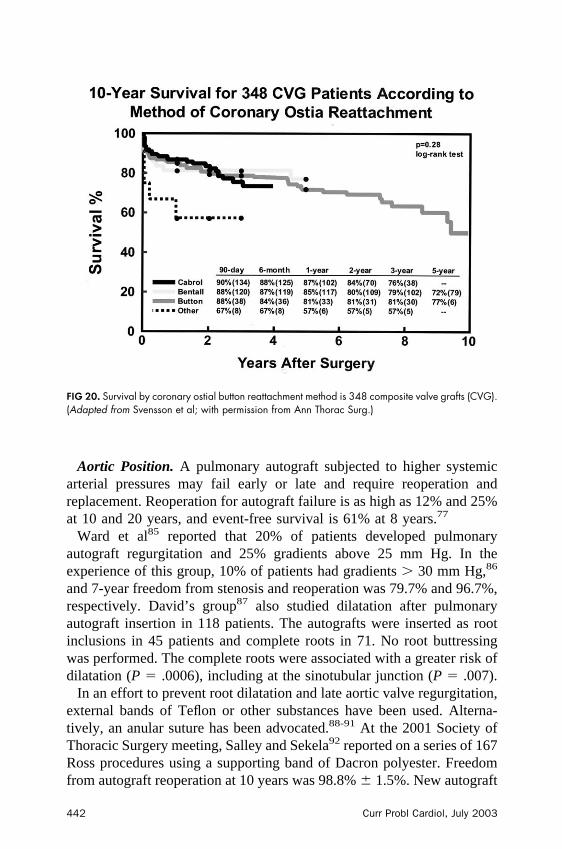
Aortic Position. A pulmonary autograft subjected to higher systemicarterial pressures may fail early or late and require reoperation andreplacement. Reoperation for autograft failure is as high as 12% and 25%at 10 and 20 years, and event-free survival is 61% at 8 years.77
Ward et al85 reported that 20% of patients developed pulmonaryautograft regurgitation and 25% gradients above 25 mm Hg. In theexperience of this group, 10% of patients had gradients � 30 mm Hg,86
and 7-year freedom from stenosis and reoperation was 79.7% and 96.7%,respectively. David’s group87 also studied dilatation after pulmonaryautograft insertion in 118 patients. The autografts were inserted as rootinclusions in 45 patients and complete roots in 71. No root buttressingwas performed. The complete roots were associated with a greater risk ofdilatation (P � .0006), including at the sinotubular junction (P � .007).
In an effort to prevent root dilatation and late aortic valve regurgitation,external bands of Teflon or other substances have been used. Alterna-tively, an anular suture has been advocated.88-91 At the 2001 Society ofThoracic Surgery meeting, Salley and Sekela92 reported on a series of 167Ross procedures using a supporting band of Dacron polyester. Freedomfrom autograft reoperation at 10 years was 98.8% � 1.5%. New autograft
FIG 20. Survival by coronary ostial button reattachment method is 348 composite valve grafts (CVG).(Adapted from Svensson et al; with permission from Ann Thorac Surg.)
442 Curr Probl Cardiol, July 2003
valve regurgitation occurred in 16%, with none greater than 2�. Opera-tive mortality was 1.8% and late mortality 3.7%.
It should be noted that in this series, the pulmonary valve was rejectedfor the Ross procedure in 7 patients because of leakage or congenitalvalve abnormalities. This has also been our experience. Despite trans-esophageal or transthoracic (usually more accurate) echocardiographyappearing to show a good valve, at the time of surgical inspection thevalve is sometimes not usable. Furthermore, de Sa et al93 advised cautionin using the Ross procedure in patients with bicuspid aortic valvesbecause of the high prevalence of concurrent abnormal pulmonary valves.
In the invited commentary on the paper by Salley and Sekela,92 wenoted that mortality for the Ross procedure is 3% and reoperation at 10years is 19%; similarly, for the series by Ross it was 16%, Elkins 17%,and at the Cleveland Clinic 20%. Thus, the calculated risk of a patientaged 35 years requiring a reoperation during a normal life expectancy is50%.
Outcomes. Use of the Ross procedure in young adults has beenanalyzed by several groups. Ross’ group77 reported in 1997 on 131hospital survivors operated on between 1967 and 1984, mostly using thesubcoronary technique. Ten- and 20-year survival was 85% and 61%;freedom from autograft replacement was 88% and 75%, freedom from
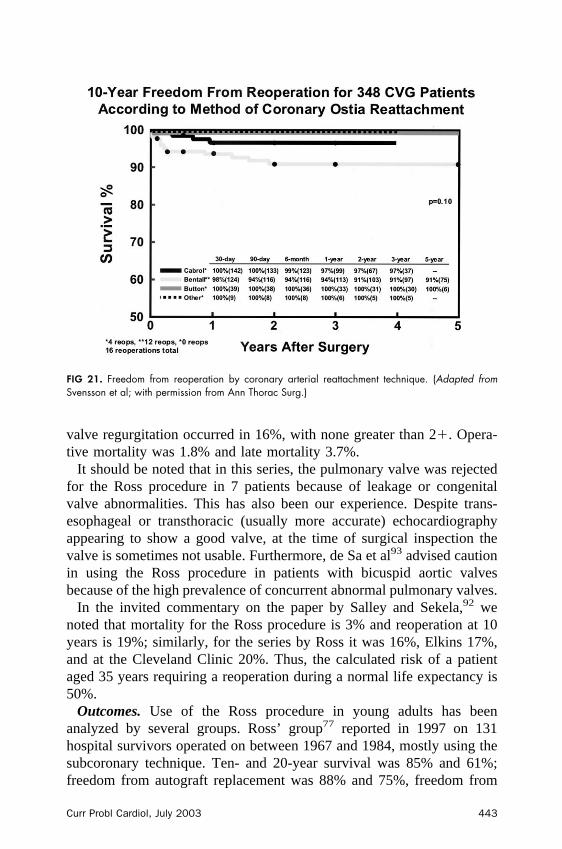
FIG 21. Freedom from reoperation by coronary arterial reattachment technique. (Adapted fromSvensson et al; with permission from Ann Thorac Surg.)
Curr Probl Cardiol, July 2003 443

reoperation on the pulmonary allograft was 89% and 80%, and freedomfrom all reoperations was 76% and 62%, respectively. Of note, thesubcoronary technique is generally no longer used for the Ross procedurebecause of its higher failure rate.
Of interest, endocarditis occurred in 9.2% (3 autograft, 4 pulmonaryallograft, 5 other sites). Thromboembolism was also uncommon (12.2%,11 systemic, 5 pulmonary). Unfortunately, 23% developed arrhythmias,mostly atrial (two thirds). With a shorter follow-up, Elkins88 reported, ina series of 328 patients, 5% operative mortality, 89% 5-year survival,94% freedom from pulmonary allograft reoperation, and 83% freedomfrom autograft reoperation or failure. Thus, by 8 years, it would appearthat an important proportion of approximately 75% of patients whounderwent surgery were not event-free survivors, even excluding com-plications related to bacterial endocarditis, hemorrhage, or embolism.88 Ina report also in 1999, Elkins et al90 reported on 244 operative survivors(excluding early deaths), with a freedom from autograft degeneration of83% at 10 years. However, they excluded endocarditis, allograft reopera-tion, and valve-related deaths from the analysis.
In 1998, Oury et al94 published the results of 2,523 patients enrolled inthe Ross International Registry. Operative mortality was 2.5%, and withonly 70% follow-up, 5.4% of patients had reoperations for valve-relatedproblems. Of interest, based on the Ross Registry, no relationship wasapparent between patient age and either pulmonary allograft or aorticautograft failure.
Bicuspid Aortic Valve RepairIn selected patients and with experience, a bicuspid aortic valve
associated with aortic valve regurgitation can be successfully repairedwith excellent long-term durability and results (Fig 19). Casselman95
from our group reported on 94 patients who had repairs with no operativedeaths, and at 7 years after surgery, 84% had not required a reopera-tion.96,97
Technique of Repair. The technique of repair of a regurgitant bicuspidvalve is based on its pathophysiology. If a bicuspid valve is competent,the 2 cusps are usually symmetrical and of equal length, and thecircumference of the anulus for each cusp is equal. However, if the oneconjoined cusp is longer, prolapse and regurgitation occurs.98,99 Further-more, in patients with bicuspid valves, the inter-commissural angle at theapex of the triangle is greater, resulting in a greater inter-commissuraldistance. This, in turn, reduces the area of coaptation between the leaflets,known as the lunula.98,99
444 Curr Probl Cardiol, July 2003
Repair of a regurgitant bicuspid valve is a 2-step process. First,leaflet symmetry is restored by excising a triangular wedge of theprolapsing cusp and repairing it with a continuous running stitch.Alternatively— our current preferred method—the wedge can beplicated or imbricated without excision. Second, valve coaptation atthe lunula is increased by placing subcommissural horizontalpledgeted sutures as first described by Cabrol.100 It is important thatthese sutures are fairly low on the commissures to substantially narrowthe inter-commissural triangle apex. In addition, a suture is placedacross the top of the leaflets at the commissures to reapproximate theleaflets at their edges. If needed, a subanular left ventricular outflowtract circumferential stitch can also be added to improve coaptation,especially if the anulus is enlarged. We do not recommend leafletextension with pericardial strips, because this appears to be associatedwith a greater risk of thromboembolic complications. These tech-niques of leaflet repair have also been used in conjunction withtricuspid aortic valves and combined aortic aneurysm procedures,particularly valve-preserving operations or remodeling or modifiedDavid reimplantation, with excellent long-term results.
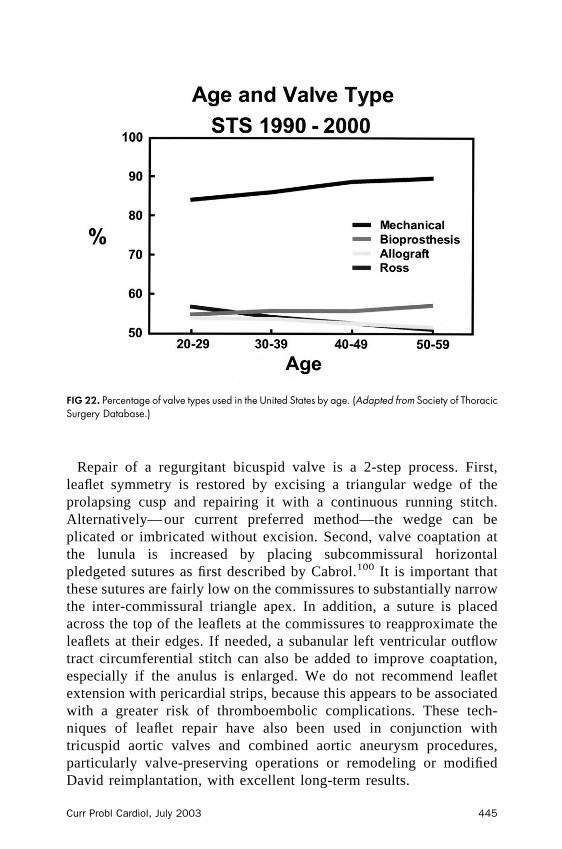
FIG 22. Percentage of valve types used in the United States by age. (Adapted from Society of ThoracicSurgery Database.)
Curr Probl Cardiol, July 2003 445
Outcomes. From 1988 to 2002, 288 patients underwent aortic valverepair, 75% with bicuspid valves. Triangular resection was done in 61%,plication in 26%, and commissuroplasty in 97%. Freedom from reopera-tion was 79% at 10 years. At 10 years, 71% had 0 to 1� regurgitation (Fig19). Bicuspid valve repairs are nearly as durable as mitral valve repairs,particularly if they are performed before extensive calcification hasdistorted the valves to the point where they are no longer repairable.
Special Situations
Aortic Valve Disease Associated with Coronary ArteryDisease
Clearly, one of the most common and important variables in selectinga valve prosthesis is presence of concurrent coronary artery disease.Patients with coronary artery disease and who need concurrent valvereplacement have reduced long-term survival.101-103,103a
There are 2 relevant arguments that can be debated. The first is that useof a mechanical valve, with warfarin for anticoagulation, may reduce therisk of subsequent reoperation from progression of coronary disease.However, there is no convincing evidence that warfarin prevents progres-sion of coronary artery disease. The second argument, and the antithesisof the first, is that because of coronary artery disease, left ventricularfunction is reduced in most patients, their life expectancy is limited, andtherefore a pericardial valve is unlikely to need replacement during apatient’s lifetime.
Of relevance in choosing a valve in young patients with coronary arterydisease is the study by Lytle from our group.101 For those patients whounderwent aortic valve replacements combined with coronary arterybypass surgery at our institution, 10-year survival was 52%. Theindependent determinants of decreased late survival were advanced age,cardiothoracic ratio � 50% on the chest radiograph, higher preoperativeNew York Heart Association class, and moderate or severe left ventric-ular dysfunction. Of particular relevance, patients receiving bioprostheses(P � .001) had better long-term survival and event-free survival (P �.01) than did those receiving mechanical valves. Patients receivingmechanical valves who were not taking warfarin had the worst survivaland event-free survival, whereas those with bioprostheses and not takingwarfarin had the best. Of note, Lytle et al102 also showed that apart frompatients having coronary artery disease, long-term survival was alsoreduced with severe left ventricular function impairment and renaldysfunction.
446 Curr Probl Cardiol, July 2003
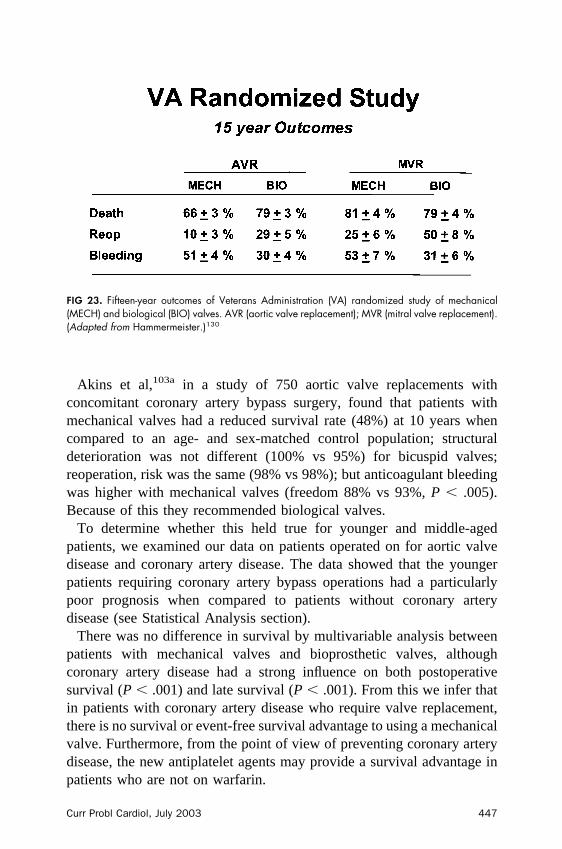
Akins et al,103a in a study of 750 aortic valve replacements withconcomitant coronary artery bypass surgery, found that patients withmechanical valves had a reduced survival rate (48%) at 10 years whencompared to an age- and sex-matched control population; structuraldeterioration was not different (100% vs 95%) for bicuspid valves;reoperation, risk was the same (98% vs 98%); but anticoagulant bleedingwas higher with mechanical valves (freedom 88% vs 93%, P � .005).Because of this they recommended biological valves.
To determine whether this held true for younger and middle-agedpatients, we examined our data on patients operated on for aortic valvedisease and coronary artery disease. The data showed that the youngerpatients requiring coronary artery bypass operations had a particularlypoor prognosis when compared to patients without coronary arterydisease (see Statistical Analysis section).
There was no difference in survival by multivariable analysis betweenpatients with mechanical valves and bioprosthetic valves, althoughcoronary artery disease had a strong influence on both postoperativesurvival (P � .001) and late survival (P � .001). From this we infer thatin patients with coronary artery disease who require valve replacement,there is no survival or event-free survival advantage to using a mechanicalvalve. Furthermore, from the point of view of preventing coronary arterydisease, the new antiplatelet agents may provide a survival advantage inpatients who are not on warfarin.
FIG 23. Fifteen-year outcomes of Veterans Administration (VA) randomized study of mechanical(MECH) and biological (BIO) valves. AVR (aortic valve replacement); MVR (mitral valve replacement).(Adapted from Hammermeister.)130
Curr Probl Cardiol, July 2003 447
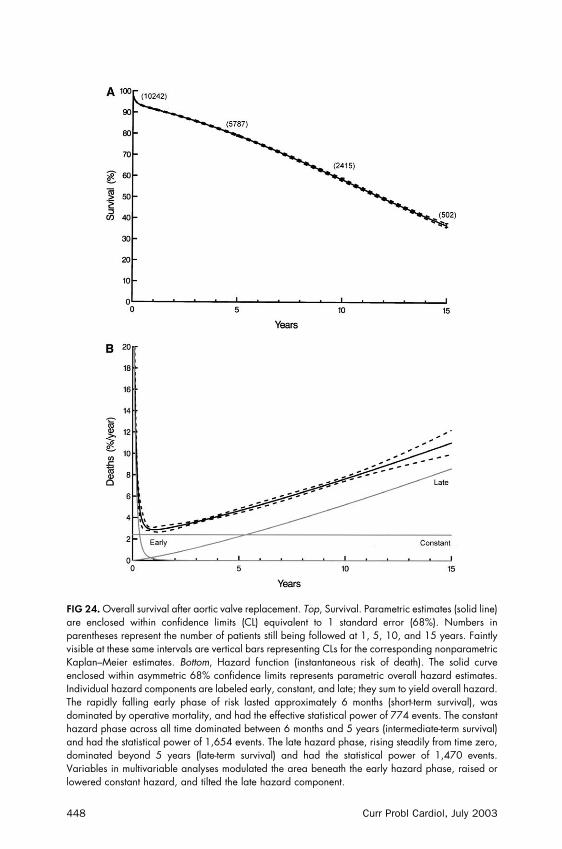
FIG 24. Overall survival after aortic valve replacement. Top, Survival. Parametric estimates (solid line)are enclosed within confidence limits (CL) equivalent to 1 standard error (68%). Numbers inparentheses represent the number of patients still being followed at 1, 5, 10, and 15 years. Faintlyvisible at these same intervals are vertical bars representing CLs for the corresponding nonparametricKaplan–Meier estimates. Bottom, Hazard function (instantaneous risk of death). The solid curveenclosed within asymmetric 68% confidence limits represents parametric overall hazard estimates.Individual hazard components are labeled early, constant, and late; they sum to yield overall hazard.The rapidly falling early phase of risk lasted approximately 6 months (short-term survival), wasdominated by operative mortality, and had the effective statistical power of 774 events. The constanthazard phase across all time dominated between 6 months and 5 years (intermediate-term survival)and had the statistical power of 1,654 events. The late hazard phase, rising steadily from time zero,dominated beyond 5 years (late-term survival) and had the statistical power of 1,470 events.Variables in multivariable analyses modulated the area beneath the early hazard phase, raised orlowered constant hazard, and tilted the late hazard component.
448 Curr Probl Cardiol, July 2003

Minimal Access (“Keyhole”) Aortic Valve SurgeryCosgrove and Navia104,105 pioneered minimally invasive aortic valve
surgery using a parasternal incision. Subsequently, we have tailored theminimally invasive incision for specific sites.106-109 Thus, we use the 7-to 8-cm (3-in) “ j” or “J” incision we described for aortic valve or aorticvalve plus aorta operations, including reoperations, and a left-sided “J” or“L” incision for mitral valve repair or replacements.106-109
Using these minimally invasive approaches in 1,427 mitral valveoperations, 90% of them repairs, mortality was 0.3%; for 607 minimallyinvasive aortic valve replacements, including 158 allografts, it was 0.8%.With the minimally invasive approach we have shown that patients haveless postoperative pain and a better cosmetic result, require fewer bloodtransfusions, are extubated earlier, and are discharged earlier fromhospital; it is also our impression that they return to work earlier,particularly manual labor, and also to sports.
Similarly, aortic valve reoperations and aorta reoperations, an increas-ing problem, have been simplified by this approach, with no patientsdying from aorta reoperation in our last report.109 We have no evidencethat late results have been adversely affected by minimally invasivesurgery, nor is valve selection affected by using the minimally invasiveapproach; however, we have not used it for the Ross procedure.
Aortic Valve Disease in Conjunction with AorticAneurysms or Dissection or Marfan Syndrome
Preservation of Aortic Valve During Aneurysm Repair. In addition tothe potential for bicuspid aortic valve repairs, when a tricuspid aorticvalve is leaking because of distraction of the commissures by ananeurysm, it can be repaired and preserved in combination with the aorticaneurysm or dissection repair. There are 2 current options: (1) remodelingthe aortic root and sewing the valve to the graft by the techniquesdescribed by Yacoub,110,111 David,112 and one of us (LGS113), or (2)mobilizing the entire aortic valve and reimplanting it into a new tube graftas described by David and Feindel.112,114-116
Remodeling Operation. Remodeling operations are best suited fornon-Marfan patients with relatively intact aortic valves and for thoseundergoing reoperations. Remodeling of only 1 sinus of Valsalva is alsoa frequent option, particularly the noncoronary sinus, and is especiallyuseful in acute aortic dissections. When repairing the root for acute aorticdissection, we remodel the noncoronary sinus by suturing the graft to the
Curr Probl Cardiol, July 2003 449
aortic valve anulus rather than doing the anastomosis at the sinotubularridge.
Event rates are low for remodeling operations, although if used forMarfan patients, a higher proportion will require reoperation for valvefailure compared to those undergoing reimplantation.110,117 The risk ofrequiring another operation after reimplantation in Marfan patients hasbeen low.
Yacoub et al110 recently updated their experience since 1979 onvalve-preserving remodeling operations in 158 patients, 68 with Marfansyndrome. Early mortality was 4.6% for chronic aneurysms and 1% forelective repairs. Survival for aneurysm repairs at 10 years was 79%; 82%for elective operations, 53.3% for acute dissection. The risk of reoperationwas 11% � 0.5% at 10 years. No cases of endocarditis or thromboem-bolic events occurred except with leaflet extension, and no anticoagulantswere used. Reduction of left ventricular end-systolic and end-diastolicdimensions were maintained. For a series of 82 Marfan patients, earlymortality was 4.9%; however, risk of reoperation by 10 years was17%.117
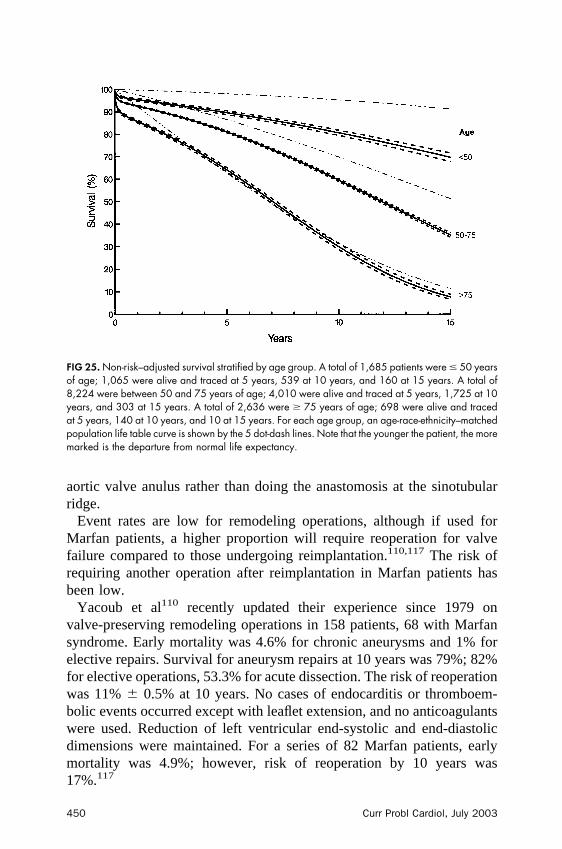
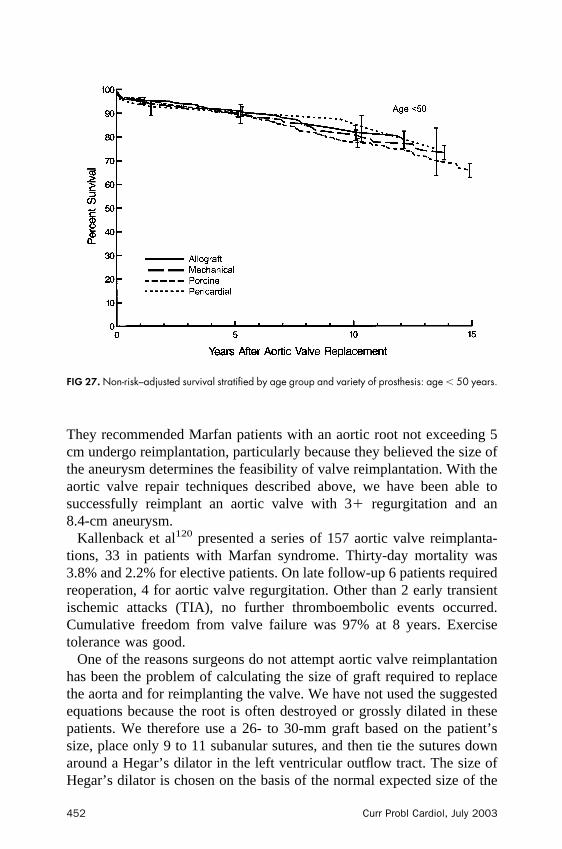
FIG 25. Non-risk–adjusted survival stratified by age group. A total of 1,685 patients were � 50 yearsof age; 1,065 were alive and traced at 5 years, 539 at 10 years, and 160 at 15 years. A total of8,224 were between 50 and 75 years of age; 4,010 were alive and traced at 5 years, 1,725 at 10years, and 303 at 15 years. A total of 2,636 were � 75 years of age; 698 were alive and tracedat 5 years, 140 at 10 years, and 10 at 15 years. For each age group, an age-race-ethnicity–matchedpopulation life table curve is shown by the 5 dot-dash lines. Note that the younger the patient, the moremarked is the departure from normal life expectancy.
450 Curr Probl Cardiol, July 2003
Modified Reimplantation Operation. The reimplantation operation,although more complicated, is best suited for Marfan patients or thosewith severe aortic valve regurgitation or huge aneurysms with intactaortic leaflets. It is also an option if the entire root needs to be repaired foracute aortic dissection.
In 1992, David and Feindel112 described this operation in which thecoronary sinuses were excised from the aortic root, the left ventricularoutflow tract dissected out, the coronary artery ostial buttons mobilized,and the aortic valve, still attached to the left ventricular outflow tract, wasreimplanted into a tube graft. The coronary buttons were also reimplantedwith separate openings in the graft.
Subsequently, an equation was derived for the relationship between rootdiameter and leaflet dimensions. This was proposed as a method forselecting a graft size at the sinotubular junction appropriate for rootdimensions, including remodeling operations.118
Tambeur119 from David’s group compared results of aortic valvereimplantation and composite valve grafts in 78 Marfan patients andfound 5-year survival was better for valve sparing reimplantation (100%vs 88% � 6%, P � .04).
No valve sparing operation required a reoperation. Clearly, these patientgroups were different; nevertheless, the mid-term results are gratifying.
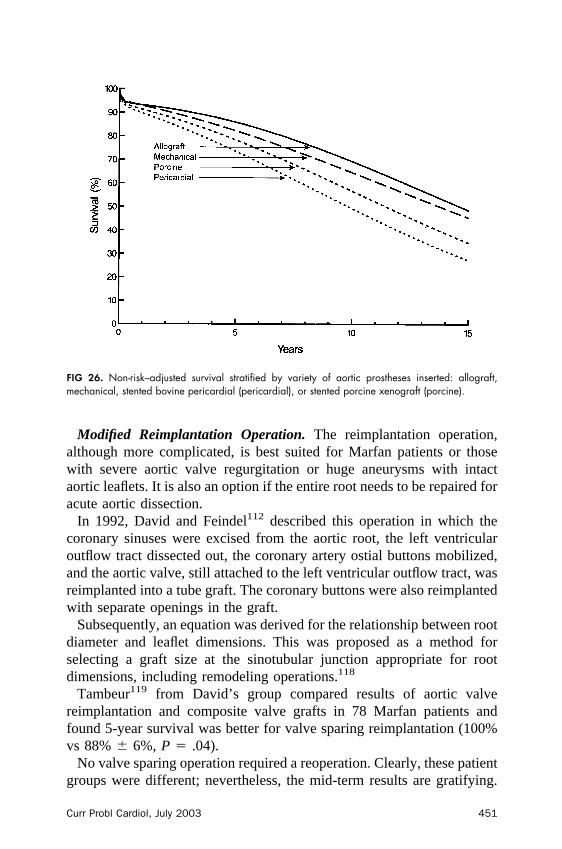
FIG 26. Non-risk–adjusted survival stratified by variety of aortic prostheses inserted: allograft,mechanical, stented bovine pericardial (pericardial), or stented porcine xenograft (porcine).
Curr Probl Cardiol, July 2003 451
They recommended Marfan patients with an aortic root not exceeding 5cm undergo reimplantation, particularly because they believed the size ofthe aneurysm determines the feasibility of valve reimplantation. With theaortic valve repair techniques described above, we have been able tosuccessfully reimplant an aortic valve with 3� regurgitation and an8.4-cm aneurysm.
Kallenback et al120 presented a series of 157 aortic valve reimplanta-tions, 33 in patients with Marfan syndrome. Thirty-day mortality was3.8% and 2.2% for elective patients. On late follow-up 6 patients requiredreoperation, 4 for aortic valve regurgitation. Other than 2 early transientischemic attacks (TIA), no further thromboembolic events occurred.Cumulative freedom from valve failure was 97% at 8 years. Exercisetolerance was good.
One of the reasons surgeons do not attempt aortic valve reimplantationhas been the problem of calculating the size of graft required to replacethe aorta and for reimplanting the valve. We have not used the suggestedequations because the root is often destroyed or grossly dilated in thesepatients. We therefore use a 26- to 30-mm graft based on the patient’ssize, place only 9 to 11 subanular sutures, and then tie the sutures downaround a Hegar’s dilator in the left ventricular outflow tract. The size ofHegar’s dilator is chosen on the basis of the normal expected size of the
FIG 27. Non-risk–adjusted survival stratified by age group and variety of prosthesis: age � 50 years.
452 Curr Probl Cardiol, July 2003
left ventricular outflow tract based on sex and body surface area.121 Thismodification also has the advantage of creating artificial sinuses above thecrimped lower end of the graft.
We have recommended that Marfan patients with an aortic cross-sectional area (cm2) to height (m) ratio � 10 undergo operation andrepair.122 There are 3 important reasons. First, elective surgery in Marfansyndrome patients has become very safe. In 45 recent consecutivepatients, we have not had an early or late death, irrespective of urgencyof operation.122,123 Similarly, in a report on 151 patients, mortality was1% for asymptomatic patients.124 Second, we noted that 15% of ourpatients had developed dissections when the aorta was � 5 cm indiameter.122 Of interest, in our series of 480 patients with bicuspid aorticvalves and concomitant aortic replacement, 41 had aortic dissection, andof these latter patients, 12.5% had a dissected aorta � 5 cm in diameter.Similar to Marfan patients, a ratio � 10 is recommended as an indicationfor aortic repair. For the dissection patients, survival was 95%, and for the380 nondissection patients, survival was 98.7%. Third, apart from the40% risk of immediate death from dissection and approximately 10% to20% risk of death with emergency surgery, the long-term prognosis ismarkedly reduced, and patients require multiple operations. In a study ofMarfans syndrome patients from Stanford, 5-year survival was only 54%after aortic dissection repairs.
In an update of valve-sparing operations, 64 using the valve reimplan-tation technique and 56 aortic remodeling, David et al114,115 reported5-year survival of 88% for root repairs and 68% for root repairs withascending aneurysm replacements (P � .01). Of note, freedom fromreoperation for root repairs was 99% and 97% for those with ascendinganeurysms. At 10 years of follow-up, overall freedom from reoperationfor aortic root repairs was 99%, freedom from thromboembolic eventswas 89% � 5% (n � 3 TIAs), and freedom from moderate aorticregurgitation was 83% � 8% (n � 3). One paraplegic patient developedendocarditis.114,115
One of us (LGS) has performed 58 aortic-valve–preserving remodelingor modified reimplantation operations, and similar to David’s results,none suffered an early event related to the valve. One patient whose valveremodeling operation was combined with a concurrent aortic arch andthoracoabdominal aneurysm repair died after surgery. One patient had alate TIA.
At this time, long-term data (beyond 10 years) are not available forthese valve preserving operations. However, these promising valve-preserving procedures and repair techniques are options in selected
Curr Probl Cardiol, July 2003 453
patients. We have usually not used allografts, nor the Ross procedure, norbiological valves in composite grafts for young patients with ascendingaortic or arch aneurysms or Marfan syndrome. We have thus used valvepreserving procedures preferentially as described above or mechanicalvalve composite grafts if valve preserving operations were not feasible.
Replacement of Aortic Valve During Aneurysm Repair. Compositevalve graft insertion for valvular disease and aortic aneurysm withreimplantation of the coronary arteries is a relatively common andsuccessful operation (Figs 20 and 21).125 With composite valve graftrepairs of aortic aneurysms and replacement of the aortic valve, mechan-ical bileaflet valves appear to be associated with a higher transvalvulargradient, possibly because there is not an elastic sinus of Valsalva rootcomponent to the valve grafts. Although the incidence of late embolicneurologic events is reduced for composite valve grafts compared withsingle aortic valve replacement because the pledgeted valve sutures aretied outside the bloodstream, the risk of endocarditis is increased.113 In aprevious report by one of us on composite valve grafts used for repairingaortic aneurysms, there were no 30-day operative deaths, and 5-yearsurvival was 88%.113 The linearized rate for endocarditis, however, was2.2% per patient-year. Notably, none of these patients required reopera-
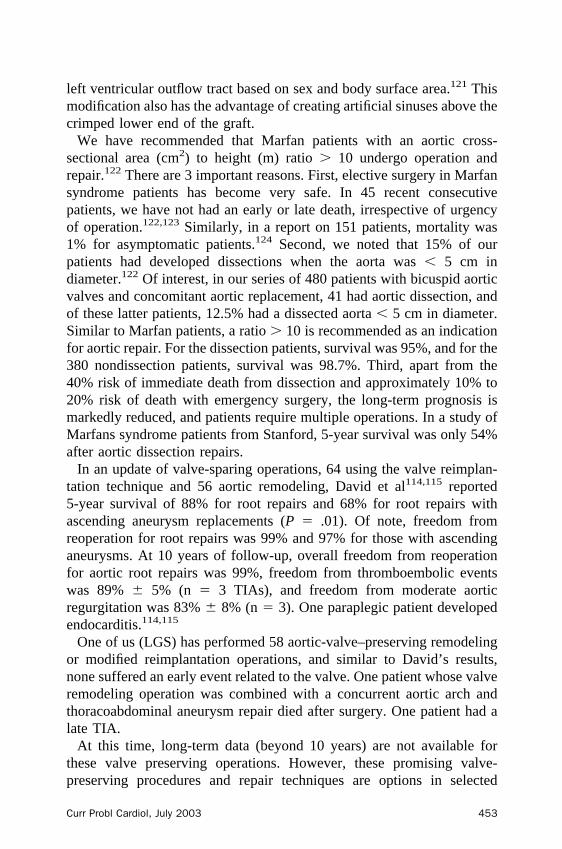
FIG 28. Non-risk–adjusted survival stratified by age group and variety of prosthesis: age 50 to 75years.
454 Curr Probl Cardiol, July 2003

tion for endocarditis (all were successfully treated with antibiotics) or latevalve-related problems.113
Untreated Aneurysms and Valve Replacement. Of relevance to thisdiscussion is the finding that if an aortic valve is replaced and anascending aortic aneurysm � 4 cm is not repaired, patients have worselong-term survival because of developing aortic dissection or rupture. Ina study from our institution,126 30% of female patients who did not havean ascending aortic dilatation � 4 cm repaired at the time of valvereplacement either died from rupture over a 5.7-year period or neededemergency surgery (13%).
Valve Selection in Dialysis PatientsKaplon from our institution compared the results of using pericardial
valves versus mechanical valves in patients on dialysis.127 Previously,porcine valves had been noted to be more prone to calcification in patientson hemodialysis. This study, however, showed no difference in survivalbetween the valve types (P � .3). Because of limited patient lifeexpectancy, pericardial valves were found to be sufficiently durable.Furthermore, other studies have demonstrated that patients with mechan-ical valves—who obviously will need warfarin anticoagulation—developa greater number of bleeding complications in the hospital and afterdischarge, because of the added problem of hemodialysis, than do patientswith a bioprosthesis.
Choice of Procedure
ComparisonsTo better understand which valves are used in young adults in the
United States, Fig 22 shows the types of valve used by age group. Datafrom the STS database show increasing use of allografts, but mechanicalvalves are still most frequently used. With increasing patient age,biological valves are increasingly used. Centers performing the Rossprocedure routinely are few. Selection of the valve procedure thus mustbe predicated on whether the procedure of choice is available where thepatient chooses to have surgery.
The data show that the choice of procedure is influenced largely bylong-term life expectancy and contraindications or indications for anti-coagulation. Two prospective randomized studies, comparing older typesof mechanical valves with biological valves, have failed to show asurvival benefit for mechanical valves (Fig 23).128-130
Gross et al131 compared the use of allografts and mechanical valves in
Curr Probl Cardiol, July 2003 455
patients aged 20 to 50 years (mean 38.6 years), 45 with allografts and 40with mechanical valves. Other than endocarditis in the allograft patients,the groups were comparable. There was a significant difference (P � .05)in perioperative deaths (4 for allografts vs 0 for mechanical valves),reoperation (8 for allografts vs 0 for mechanical valves), and endocarditis(5 for allografts vs 0 for mechanical valves), although embolism andbleeding were more common with mechanical valves. Late mortality wassimilar. The authors concluded that endocarditis and graft failure weremore frequent than expected for allografts in young patients, resulting inunfavorable results. Nevertheless, the risk of embolism and bleeding wascumulative within the mechanical valve group.
In a similar study, Yacoub’s group132 compared outcomes for 518patients who underwent allograft or prosthetic valve insertions. There wasno difference in survival by valve type; however, allografts had lessserious complication, whereas for mechanical valves it was greater.Nevertheless, allografts had more primary tissue failures.
Of interest, in a study of 2,443 patients with valve replacements, ofwhom 3.7% developed late endocarditis, allografts had a constant but lowhazard risk,133 whereas for other devices it peaked 9 weeks afteroperation. Risk factors were xenografts, mechanical valves, renal failure,
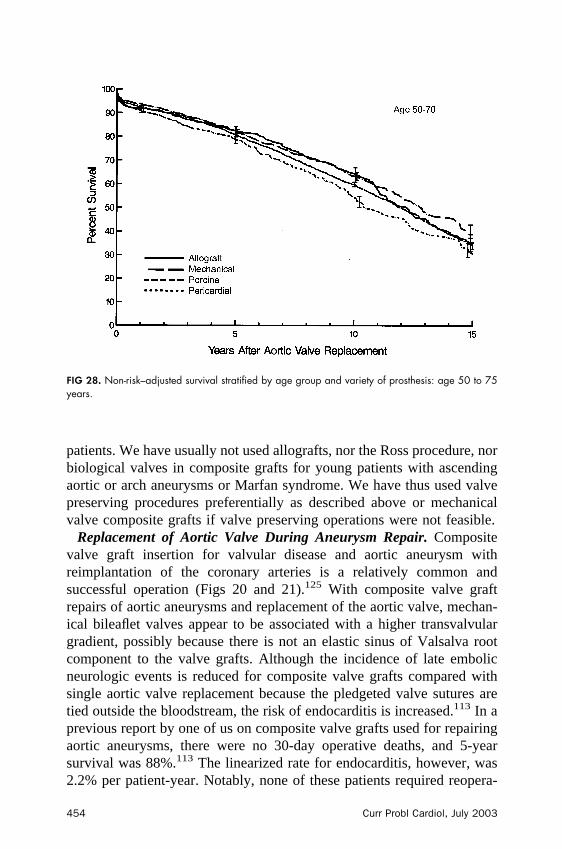
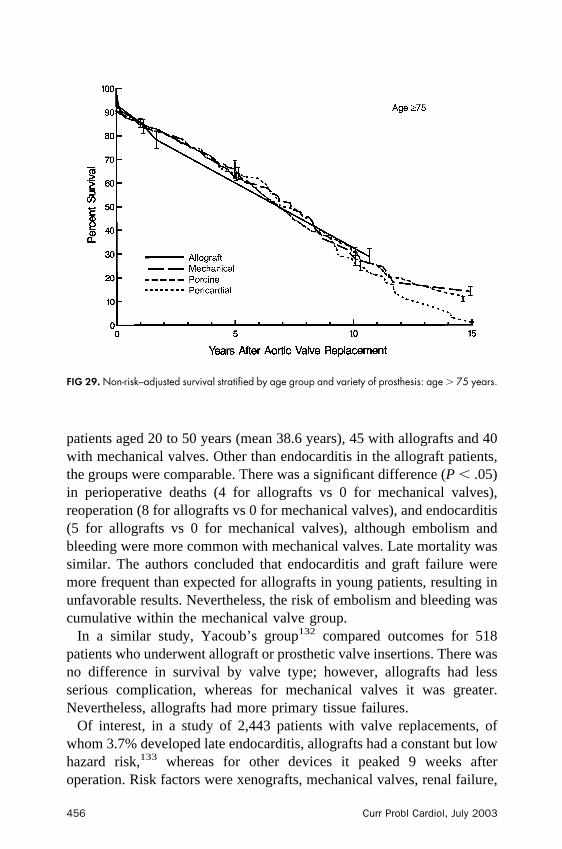
FIG 29. Non-risk–adjusted survival stratified by age group and variety of prosthesis: age � 75 years.
456 Curr Probl Cardiol, July 2003
and younger age. Use of synthetic root material and presence ofpreoperative endocarditis increased the risk of allograft endocarditis.
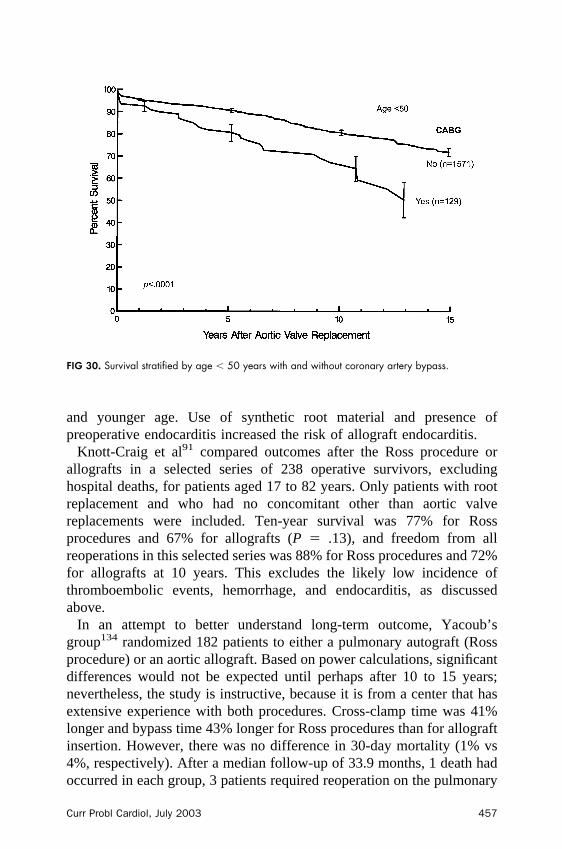
Knott-Craig et al91 compared outcomes after the Ross procedure orallografts in a selected series of 238 operative survivors, excludinghospital deaths, for patients aged 17 to 82 years. Only patients with rootreplacement and who had no concomitant other than aortic valvereplacements were included. Ten-year survival was 77% for Rossprocedures and 67% for allografts (P � .13), and freedom from allreoperations in this selected series was 88% for Ross procedures and 72%for allografts at 10 years. This excludes the likely low incidence ofthromboembolic events, hemorrhage, and endocarditis, as discussedabove.
In an attempt to better understand long-term outcome, Yacoub’sgroup134 randomized 182 patients to either a pulmonary autograft (Rossprocedure) or an aortic allograft. Based on power calculations, significantdifferences would not be expected until perhaps after 10 to 15 years;nevertheless, the study is instructive, because it is from a center that hasextensive experience with both procedures. Cross-clamp time was 41%longer and bypass time 43% longer for Ross procedures than for allograftinsertion. However, there was no difference in 30-day mortality (1% vs4%, respectively). After a median follow-up of 33.9 months, 1 death hadoccurred in each group, 3 patients required reoperation on the pulmonary
FIG 30. Survival stratified by age � 50 years with and without coronary artery bypass.
Curr Probl Cardiol, July 2003 457

autograft after Ross procedure, and 3 required reoperation after allograftaortic valve replacement, 2 of them children.134 Whether this was inpatients with subcoronary implants is not reported. Yacoub’s group71
used to use this technique preferentially, but also has found a higher riskof failure with the subcoronary technique. No adult patient with anallograft required reoperation for valve degeneration. At 4 years, survivaland reoperation-free survival were 97.8% and 94.2% for Ross proceduresand 95.3% and 87.7% for allografts, respectively (P not significant). Nopatient in either group developed endocarditis or had a thromboembolicevent.
Kouchoukos135 published a review of the results of the Ross procedureand allografts. His list of contraindications for allografts included severeventricular dysfunction, severe coronary artery disease, and aortic root �30 mm. For the Ross procedure, he listed these same contraindicationsand added multiple valve disease, Marfan syndrome, and immune-mediated disease such as rheumatic fever, juvenile rheumatic arthritis,systemic lupus, ankylosing spondylitis, Reiter syndrome, and Libman-Sachs endocarditis.135-137 Although we have used a commissural hori-zontal mattress suture to reduce the size of the aortic anulus,138 with orwithout a subanular stitch, long-term durability of this is unknown.Kouchoukos et al135,136 believed the indications for allografts wereendocarditis, women anticipating pregnancy, and young adults withactive lifestyles or contraindications to warfarin. For the Ross procedure,the indications were similar, except the Ross procedure was preferred inchildren.
Thus, the total risk of reoperation for either the allograft or the autograftmay be as high as 22% at 10 years in young patients. In addition, manypatients will develop functional pulmonary allograft valve stenosis ormoderate to severe pulmonary autograft regurgitation that will compro-mise their long-term cardiac function. As with total root allograftreoperations, if the entire neo-aortic pulmonary root graft has to bereplaced again and not just the pulmonary autograft valve leaflets,morbidity will be high.
Clearly, neither allografts nor Ross procedures are panaceas for valvedisease in young patients, particularly taking into account early mortalityand late results. Nevertheless, allografts are preferable to the Rossprocedure for complex endocarditis, particularly if there is a root abscess.Our data indicate that there is not much difference in long-term valvedurability when comparing allografts and pericardial valves if thepatient’s age is adjusted for.
458 Curr Probl Cardiol, July 2003
Statistical Analysis of Our Data
Allografts Versus Pericardial ValvesIn an evaluation of 629 allograft replacements and 267 pericardial valve
replacements with 99% complete follow-up, structural valve deteriorationwas similar for both valve types, although the absolute deterioration wasgreater in patients with pericardial valves at only an age � 45 years (seeFigures below). This suggests that for middle-aged patients withoutendocarditis, a pericardial valve is a reasonable option when avoidinganticoagulation is important.
Multi-Institutional Study of Mortality After Aortic ValveReplacement
In a previous study139,140,141,142 we evaluated the influence of pros-thetic size on survival. This data and additional data we have was used toevaluate the influence of prosthesis type on survival after aortic valvereplacement.
PatientsData from 9 sources142 (Cleveland Clinic Foundation, University of
British Columbia, Northern New England Cardiovascular Disease StudyGroup, Northwest Surgical Association, Stanford University, UniversityHospital, Institute to Chirurgia Cardiovasculore (University of Padova),Hartfield Hospital, Edwards Lifesciences Corporation), for a total of13,258 patients, were analyzed. The data included adults � 18 years of agefor whom prosthesis type, model, and labeled size were recorded. Exclusionswere patients (1) with valve prosthesis in another location, (2) requiringmultiple valve operations, (3) with native or prosthetic valve endocarditis, (4)who had emergency AVR, or (5) required another procedure other thancoronary artery bypass grafting (CABG). Variables included age, sex, height,weight, body surface area, New York Heart Association functional class,valve stenosis or regurgitation, previous aortic valve replacement, need forcoronary bypass, date of operation, institution, valve model, valve type, andprosthetic size.142 Prostheses were of 4 varieties: stented porcine xenografts(n � 5,757), stented bovine pericardial xenografts (n � 3,198), mechanicaldevices (n � 3,583, of which 2,125 were bileaflet and 1,458 monoleaflet),and allografts (n � 720).
End PointThe study end point was mortality due to all causes, including hospital
mortality.140,142 Total follow-up was 69,780 patient-years (mean 5.3 �
Curr Probl Cardiol, July 2003 459
4.7 years); 2,427 patients (18%) were followed-up � 10 years and 498(4%) � 15 years (up to 27 years).139
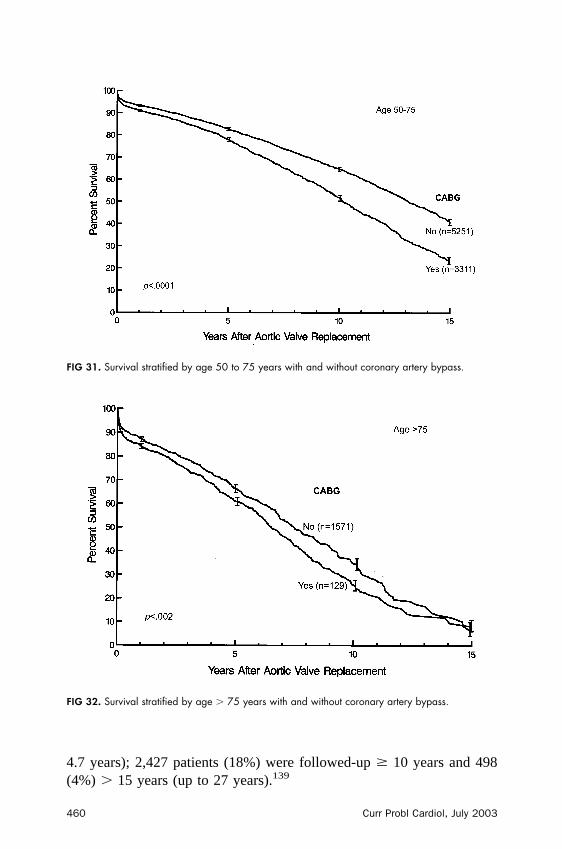
FIG 31. Survival stratified by age 50 to 75 years with and without coronary artery bypass.
FIG 32. Survival stratified by age � 75 years with and without coronary artery bypass.
460 Curr Probl Cardiol, July 2003
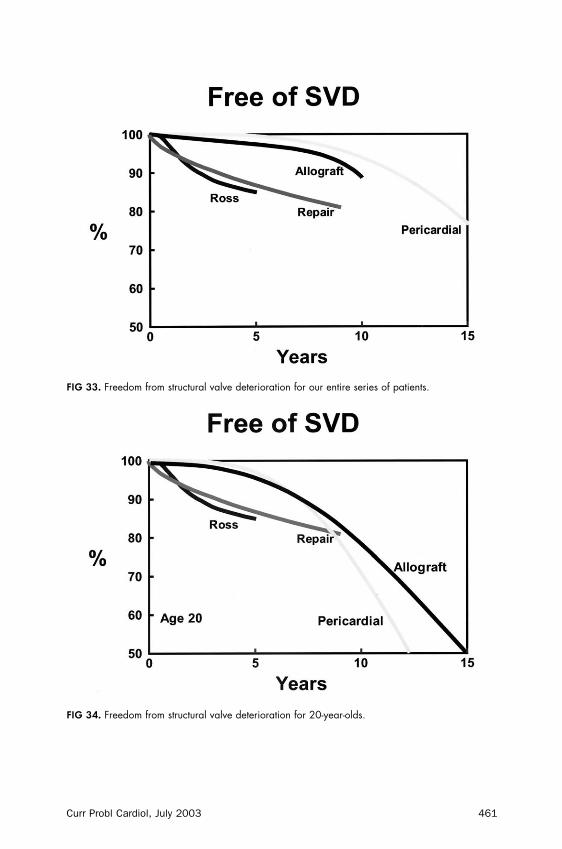
FIG 33. Freedom from structural valve deterioration for our entire series of patients.
FIG 34. Freedom from structural valve deterioration for 20-year-olds.
Curr Probl Cardiol, July 2003 461
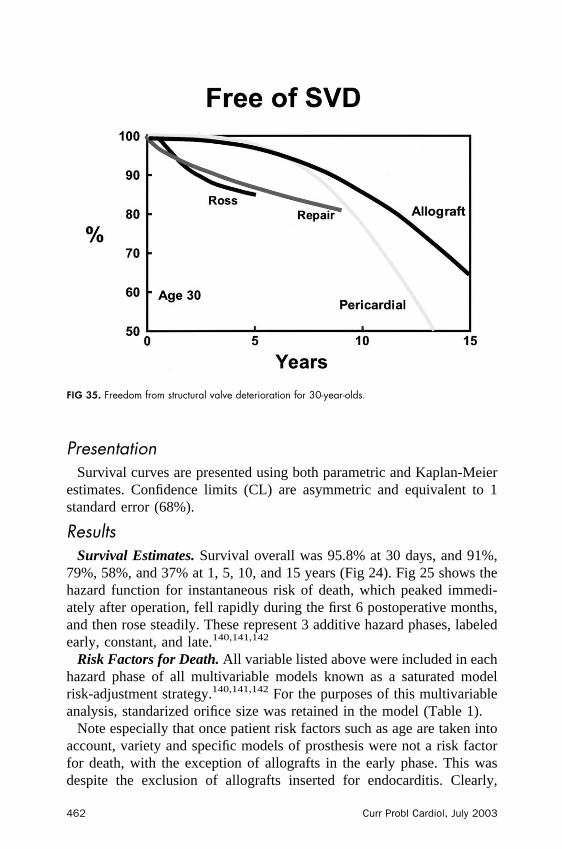
PresentationSurvival curves are presented using both parametric and Kaplan-Meier
estimates. Confidence limits (CL) are asymmetric and equivalent to 1standard error (68%).
ResultsSurvival Estimates. Survival overall was 95.8% at 30 days, and 91%,
79%, 58%, and 37% at 1, 5, 10, and 15 years (Fig 24). Fig 25 shows thehazard function for instantaneous risk of death, which peaked immedi-ately after operation, fell rapidly during the first 6 postoperative months,and then rose steadily. These represent 3 additive hazard phases, labeledearly, constant, and late.140,141,142
Risk Factors for Death. All variable listed above were included in eachhazard phase of all multivariable models known as a saturated modelrisk-adjustment strategy.140,141,142 For the purposes of this multivariableanalysis, standarized orifice size was retained in the model (Table 1).
Note especially that once patient risk factors such as age are taken intoaccount, variety and specific models of prosthesis were not a risk factorfor death, with the exception of allografts in the early phase. This wasdespite the exclusion of allografts inserted for endocarditis. Clearly,
FIG 35. Freedom from structural valve deterioration for 30-year-olds.
462 Curr Probl Cardiol, July 2003
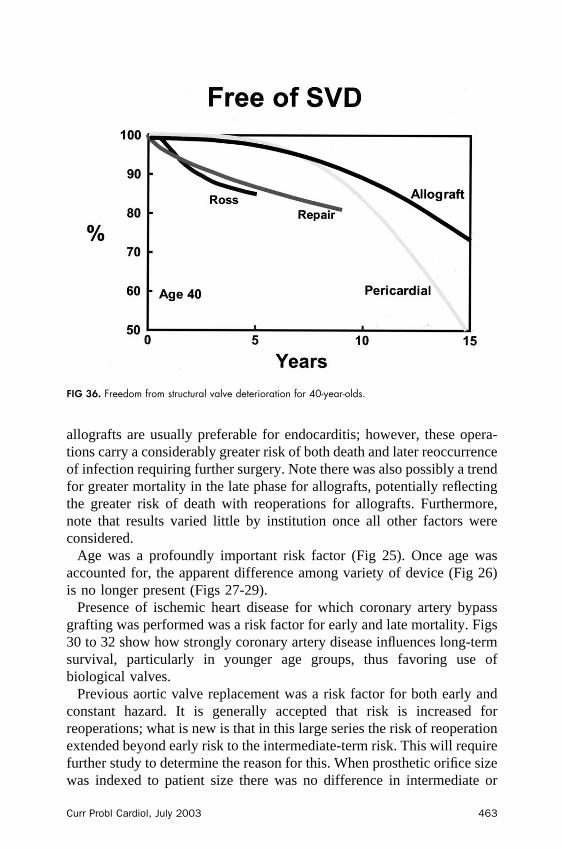
allografts are usually preferable for endocarditis; however, these opera-tions carry a considerably greater risk of both death and later reoccurrenceof infection requiring further surgery. Note there was also possibly a trendfor greater mortality in the late phase for allografts, potentially reflectingthe greater risk of death with reoperations for allografts. Furthermore,note that results varied little by institution once all other factors wereconsidered.
Age was a profoundly important risk factor (Fig 25). Once age wasaccounted for, the apparent difference among variety of device (Fig 26)is no longer present (Figs 27-29).
Presence of ischemic heart disease for which coronary artery bypassgrafting was performed was a risk factor for early and late mortality. Figs30 to 32 show how strongly coronary artery disease influences long-termsurvival, particularly in younger age groups, thus favoring use ofbiological valves.
Previous aortic valve replacement was a risk factor for both early andconstant hazard. It is generally accepted that risk is increased forreoperations; what is new is that in this large series the risk of reoperationextended beyond early risk to the intermediate-term risk. This will requirefurther study to determine the reason for this. When prosthetic orifice sizewas indexed to patient size there was no difference in intermediate or
FIG 36. Freedom from structural valve deterioration for 40-year-olds.
Curr Probl Cardiol, July 2003 463
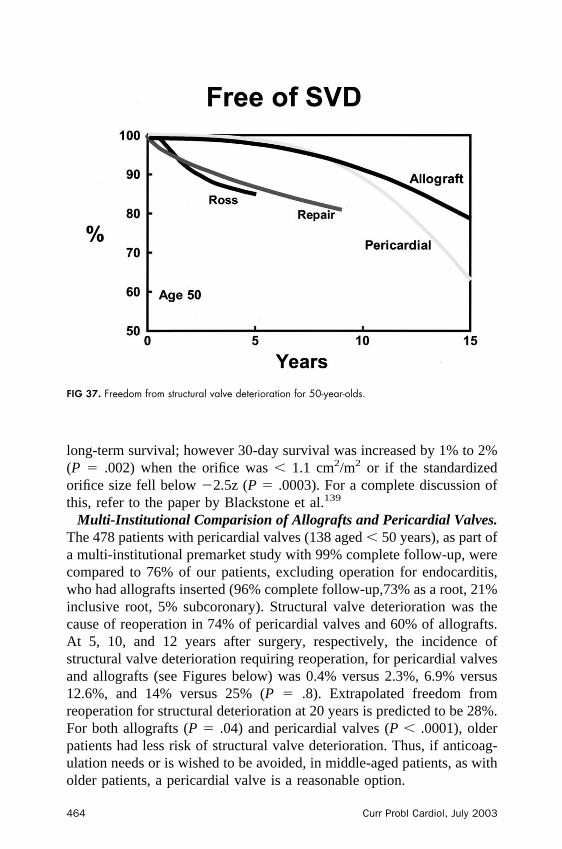
long-term survival; however 30-day survival was increased by 1% to 2%(P � .002) when the orifice was � 1.1 cm2/m2 or if the standardizedorifice size fell below �2.5z (P � .0003). For a complete discussion ofthis, refer to the paper by Blackstone et al.139
Multi-Institutional Comparision of Allografts and Pericardial Valves.The 478 patients with pericardial valves (138 aged � 50 years), as part ofa multi-institutional premarket study with 99% complete follow-up, werecompared to 76% of our patients, excluding operation for endocarditis,who had allografts inserted (96% complete follow-up,73% as a root, 21%inclusive root, 5% subcoronary). Structural valve deterioration was thecause of reoperation in 74% of pericardial valves and 60% of allografts.At 5, 10, and 12 years after surgery, respectively, the incidence ofstructural valve deterioration requiring reoperation, for pericardial valvesand allografts (see Figures below) was 0.4% versus 2.3%, 6.9% versus12.6%, and 14% versus 25% (P � .8). Extrapolated freedom fromreoperation for structural deterioration at 20 years is predicted to be 28%.For both allografts (P � .04) and pericardial valves (P � .0001), olderpatients had less risk of structural valve deterioration. Thus, if anticoag-ulation needs or is wished to be avoided, in middle-aged patients, as witholder patients, a pericardial valve is a reasonable option.
FIG 37. Freedom from structural valve deterioration for 50-year-olds.
464 Curr Probl Cardiol, July 2003
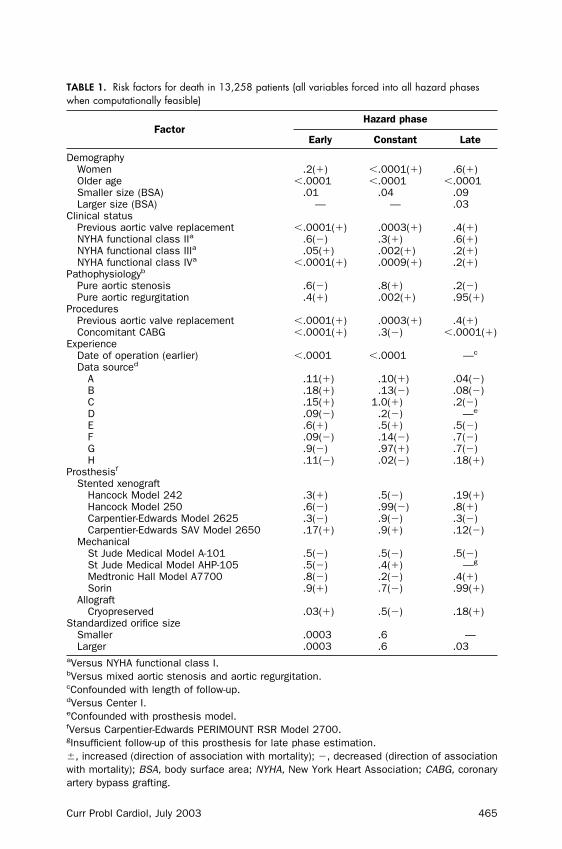
TABLE 1. Risk factors for death in 13,258 patients (all variables forced into all hazard phaseswhen computationally feasible)
FactorHazard phase
Early Constant Late
DemographyWomen .2(�) �.0001(�) .6(�)Older age �.0001 �.0001 �.0001Smaller size (BSA) .01 .04 .09Larger size (BSA) — — .03
Clinical statusPrevious aortic valve replacement �.0001(�) .0003(�) .4(�)NYHA functional class IIa .6(�) .3(�) .6(�)NYHA functional class IIIa .05(�) .002(�) .2(�)NYHA functional class IVa �.0001(�) .0009(�) .2(�)
Pathophysiologyb
Pure aortic stenosis .6(�) .8(�) .2(�)Pure aortic regurgitation .4(�) .002(�) .95(�)
ProceduresPrevious aortic valve replacement �.0001(�) .0003(�) .4(�)Concomitant CABG �.0001(�) .3(�) �.0001(�)
ExperienceDate of operation (earlier) �.0001 �.0001 —c
Data sourced
A .11(�) .10(�) .04(�)B .18(�) .13(�) .08(�)C .15(�) 1.0(�) .2(�)D .09(�) .2(�) —e
E .6(�) .5(�) .5(�)F .09(�) .14(�) .7(�)G .9(�) .97(�) .7(�)H .11(�) .02(�) .18(�)
Prosthesisf
Stented xenograftHancock Model 242 .3(�) .5(�) .19(�)Hancock Model 250 .6(�) .99(�) .8(�)Carpentier-Edwards Model 2625 .3(�) .9(�) .3(�)Carpentier-Edwards SAV Model 2650 .17(�) .9(�) .12(�)
MechanicalSt Jude Medical Model A-101 .5(�) .5(�) .5(�)St Jude Medical Model AHP-105 .5(�) .4(�) —g
Medtronic Hall Model A7700 .8(�) .2(�) .4(�)Sorin .9(�) .7(�) .99(�)
AllograftCryopreserved .03(�) .5(�) .18(�)
Standardized orifice sizeSmaller .0003 .6 —Larger .0003 .6 .03
aVersus NYHA functional class I.bVersus mixed aortic stenosis and aortic regurgitation.cConfounded with length of follow-up.dVersus Center I.eConfounded with prosthesis model.fVersus Carpentier-Edwards PERIMOUNT RSR Model 2700.gInsufficient follow-up of this prosthesis for late phase estimation.�, increased (direction of association with mortality); �, decreased (direction of associationwith mortality); BSA, body surface area; NYHA, New York Heart Association; CABG, coronaryartery bypass grafting.
Curr Probl Cardiol, July 2003 465
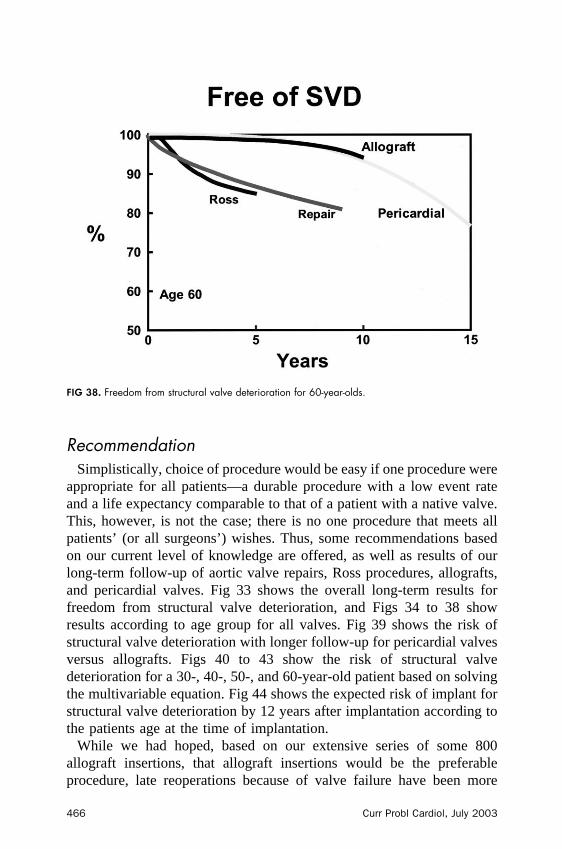
RecommendationSimplistically, choice of procedure would be easy if one procedure were
appropriate for all patients—a durable procedure with a low event rateand a life expectancy comparable to that of a patient with a native valve.This, however, is not the case; there is no one procedure that meets allpatients’ (or all surgeons’ ) wishes. Thus, some recommendations basedon our current level of knowledge are offered, as well as results of ourlong-term follow-up of aortic valve repairs, Ross procedures, allografts,and pericardial valves. Fig 33 shows the overall long-term results forfreedom from structural valve deterioration, and Figs 34 to 38 showresults according to age group for all valves. Fig 39 shows the risk ofstructural valve deterioration with longer follow-up for pericardial valvesversus allografts. Figs 40 to 43 show the risk of structural valvedeterioration for a 30-, 40-, 50-, and 60-year-old patient based on solvingthe multivariable equation. Fig 44 shows the expected risk of implant forstructural valve deterioration by 12 years after implantation according tothe patients age at the time of implantation.
While we had hoped, based on our extensive series of some 800allograft insertions, that allograft insertions would be the preferableprocedure, late reoperations because of valve failure have been more
FIG 38. Freedom from structural valve deterioration for 60-year-olds.
466 Curr Probl Cardiol, July 2003

frequent than expected and than reported in the literature. Nevertheless,allografts are recommended for endocarditis with extensive root destruc-tion. This group of endocarditis patients, however, has a poorer long-term
FIG 39. Risk of structural valve deterioration based on 478 pericardial valves and 756 allografts.
FIG 40. Predicted risk of structural valve deterioration requiring reoperation for a 30-year-old.
Curr Probl Cardiol, July 2003 467
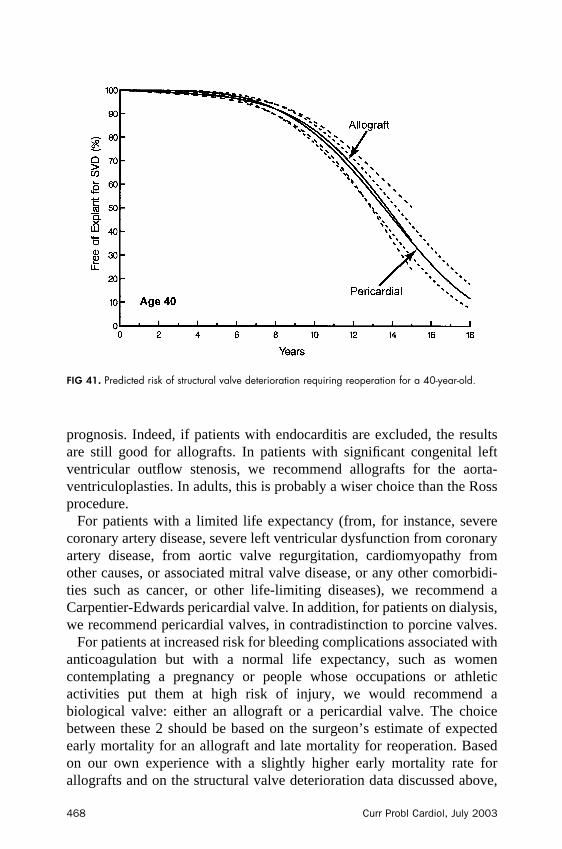
prognosis. Indeed, if patients with endocarditis are excluded, the resultsare still good for allografts. In patients with significant congenital leftventricular outflow stenosis, we recommend allografts for the aorta-ventriculoplasties. In adults, this is probably a wiser choice than the Rossprocedure.
For patients with a limited life expectancy (from, for instance, severecoronary artery disease, severe left ventricular dysfunction from coronaryartery disease, from aortic valve regurgitation, cardiomyopathy fromother causes, or associated mitral valve disease, or any other comorbidi-ties such as cancer, or other life-limiting diseases), we recommend aCarpentier-Edwards pericardial valve. In addition, for patients on dialysis,we recommend pericardial valves, in contradistinction to porcine valves.
For patients at increased risk for bleeding complications associated withanticoagulation but with a normal life expectancy, such as womencontemplating a pregnancy or people whose occupations or athleticactivities put them at high risk of injury, we would recommend abiological valve: either an allograft or a pericardial valve. The choicebetween these 2 should be based on the surgeon’s estimate of expectedearly mortality for an allograft and late mortality for reoperation. Basedon our own experience with a slightly higher early mortality rate forallografts and on the structural valve deterioration data discussed above,
FIG 41. Predicted risk of structural valve deterioration requiring reoperation for a 40-year-old.
468 Curr Probl Cardiol, July 2003
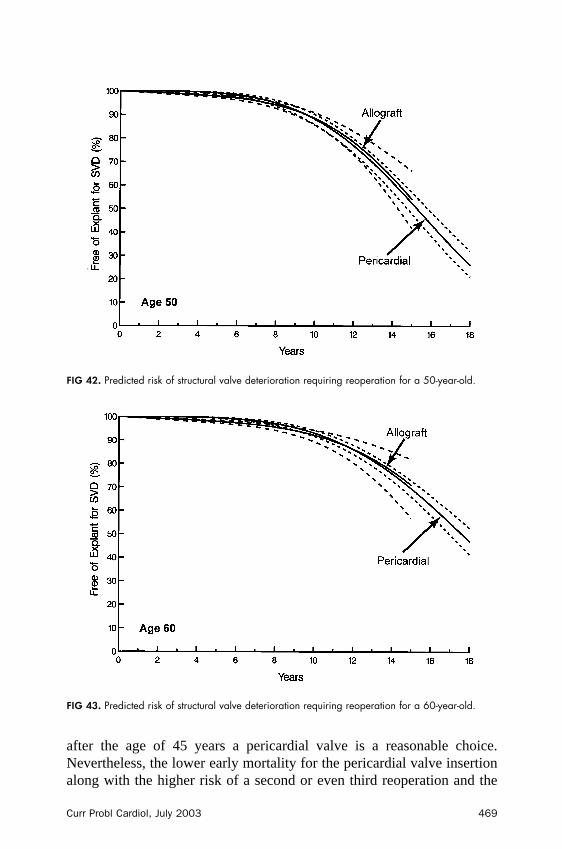
after the age of 45 years a pericardial valve is a reasonable choice.Nevertheless, the lower early mortality for the pericardial valve insertionalong with the higher risk of a second or even third reoperation and the
FIG 42. Predicted risk of structural valve deterioration requiring reoperation for a 50-year-old.
FIG 43. Predicted risk of structural valve deterioration requiring reoperation for a 60-year-old.
Curr Probl Cardiol, July 2003 469

attendant mortality has to be weighed against greater mortality afterreoperation with an allograft. For reoperations for the aortic valve, werecommend replacing mechanical valves with pericardial valves, unlessendocarditis is present or the patient has an associated aneurysm ordissection. If a patient has had a Ross procedure or allograft aortic valvereplacement, the choice is dependent on whether the entire root needs tobe replaced and also on the patient’s age.
For patients in their 20s, the Ross procedure is the choice of manysurgeons. However, approximately 25% to 30% of patients developsignificant problems by 10 years after surgery, and approximately 15% to25% require reoperation. Furthermore, patients may have 2 diseasedvalves, further complicating their care. Based on the multivariableequation for patients in the Ross registry, despite only 70% follow-up, a35-year-old patient undergoing a Ross procedure will have a 50% chanceof needing a reoperation during a normal life expectancy.
For patients with bicuspid aortic valve regurgitation, we recommend anattempted repair and immediate transesophageal echocardiogram to checkthe results. If a patient has � 1� regurgitation after repair, it is replaced.
For patients with Marfan syndrome without aortic dissection, werecommend the modified David reimplantation operation; however,composite valve grafts are the gold standard, particularly for patients with
FIG 44. Risk of replant for structural valve deterioration according to the patients age at the time ofimplantation.
470 Curr Probl Cardiol, July 2003
chronic aortic dissection and requiring extensive aortic arch repairs,including elephant trunk procedures. Similarly in this age group, com-posite mechanical valve conduits have an excellent long-term prognosisand continue to be the technique of choice for patients who require aorticvalve procedures associated with extensive aneurysmal disease repair,particularly reoperation.
What, then, is the role for mechanical valves in the current era oflow-risk surgery for aortic valve pathology, including aortic valvereplacement or repair, or reoperation, and also taking into considerationpatients’ comorbid disease? Clearly, mechanical valve replacement canbe done safely, with � 1% mortality for most patients, and the risk ofreoperation is low. However, a mechanical valve replaces aortic valvedisease and heart failure with the “disease” of anticoagulation pilldependence and associated bleeding morbidity and potential for neuro-cognitive decline.
It was previously argued that atrial fibrillation is an indication for amechanical valve; however, because atrial fibrillation is now treatedaggressively by the Maze procedure or by its newer radiofrequency ormicrowave ablation modifications, which are quicker, this is no longer anindication for mechanical valves in our patients. Our maxim is “no patientleaves the operating room with atrial fibrillation.” Whether a mechanicalvalve can be engineered that does not require anticoagulation remains tobe seen, but that is certainly an admirable goal. Even so, the risk forreoperation would not be zero, because patients may develop tissuepannus ingrowth obstructing the valves, endocarditis, thrombosis of thevalves, or other complications.
SummaryThe ideal valve or ideal procedure for patients requiring aortic valve
surgery has not been developed. It would seem intuitive that an aorticvalve replacement with an allograft—a functioning human valve—wouldbe ideal; however, this is not entirely the case because of the risk of latecalcification, which is probably related to the ischemia time or rejectionof the valve.
Thus, the choice of valve procedure in a young patient should dependon patient preference, pathology, comorbid disease, and the surgeon’sskill with the valve, durability weighed against the disadvantages ofanticoagulation, and risk of insertion and reoperation; until the ideal valveis developed—if ever.
Curr Probl Cardiol, July 2003 471
REFERENCES1. Zellner JL, Kratz JM, Crumbley AJ 3rd, Stroud MR, Bradley SM, Sade RM, et al.
Long-term experience with the St Jude Medical valve prosthesis. Ann Thorac Surg1999;68:1210-8.
2. Lim KH, Caputo M, Ascione R, Wild J, West R, Angelini GD, et al. Prospectiverandomized comparison of CarboMedics and St Jude Medical bileaflet mechanicalheart valve prostheses: an interim report. J Thorac Cardiovasc Surg 2002;123:21-32.
3. Emery R, Arom KV, Kshettry VR, Northrup WF, III, Kersten TE, Von Rueden TJ,et al. Replacement of the aortic valve in patients under 50 years old with the St JudeMedical prosthesis (SJM). In: Annual Meeting, Society of Thoracic Surgeons. FortLauderdale (Fla); Society of Thoracic Surgeons: 2002. p. 208.
4. Emery RW, Petersen RJ, Kersten TE, Stokman P, Harris KM, Knickelbine T, et al.The initial United States experience with the ATS mechanical cardiac valveprosthesis. Heart Surg Forum 2001;4:346-52.
5. Laczkovics A, Heidt M, Oelert H, Laufer G, Greve H, Pomar JL, et al. Earlyclinical experience with the On-X prosthetic heart valve. J Heart Valve Dis2001;10:94-9.
6. Akins CW. Results with mechanical cardiac valvular prostheses. Ann Thorac Surg1995;60:1836-44.
7. David TE, Gott VL, Harker LA, Miller GE Jr, Naftel DC, Turpie AG. Mechanicalvalves. Ann Thorac Surg 1996;62:1567-70.
8. Chang BC, Lim SH, Kim DK, Seo JY, Cho SY, Shim WH, et al. Long-term resultswith St Jude Medical and CarboMedics prosthetic heart valves. J Heart Valve Dis2001;10:185-94.
9. Butchart EG, Payne N, Li HH, Buchan K, Mandana K, Grunkemeier GL. Betteranticoagulation control improves survival after valve replacement. J ThoracCardiovasc Surg 2002;123:715-23.
10. Morehead AJ, Firstenberg MS, Shiota T, Qin J, Armstrong G, Cosgrove DM 3rd,et al. Intraoperative echocardiographic detection of regurgitant jets after valvereplacement. Ann Thorac Surg 2000;69:135-9.
11. Notzold A, Droste DW, Hagedorn G, Berndt S, Kaps M, Graf B, et al. Circulatingmicroemboli in patients after aortic valve replacement with pulmonary autograftsand mechanical valve prostheses. Circulation 1997;96:1843-6.
12. Lievense AM, Bakker SL, Dippel DW, Taams MA, Koudstaal PJ, Bogers AJ.Intracranial high-intensity transient signals after homograft or mechanical aorticvalve replacement. J Cardiovasc Surg (Torino) 1998;39:613-7.
13. Sliwka U, Georgiadis D. Clinical correlations of Doppler microembolic signals inpatients with prosthetic cardiac valves: analysis of 580 cases. Stroke 1998;29:140-3.
14. Kofidis T, Fischer S, Leyh R, Mair H, Deckert M, Haberl R, et al. Clinicalrelevance of intracranial high intensity transient signals in patients followingprosthetic aortic valve replacement. Eur J Cardiothorac Surg 2002;21:22-6.
14a. Deklunder G, Roussel M, Lecroart JL, Prat A, Gautier C. Microemboli in cerebralcirculation and alteration of cognitive abilities in patients with mechanicalprosthetic heart valves. Stroke 1998;29:1821-6.
15. Kleine P, Perthel M, Hasenkam JM, Nygaard H, Hansen SB, Laas J. Downstream
472 Curr Probl Cardiol, July 2003
turbulence and high intensity transient signals (HITS) following aortic valvereplacement with Medtronic Hall or St Jude Medical valve substitutes. EurJ Cardiothorac Surg 2000;17:20-4.
16. Kaps M, Hansen J, Weiher M, Tiffert K, Kayser I, Droste DW. Clinically silentmicroemboli in patients with artificial prosthetic aortic valves are predominantlygaseous and not solid. Stroke 1997;28:322-5.
17. Lund O, Magnussen K, Knudsen M, Pilegaard H, Nielsen TT, Albrechtsen OK. Thepotential for normal long term survival and morbidity rates after valve replacementfor aortic stenosis. J Heart Valve Dis 1996;5:258-67.
18. Jamieson WR, Ling H, Burr LH, Fradet GJ, Miyagishima RT, Janusz MT, et al.Carpentier-Edwards supraannular porcine bioprosthesis evaluation over 15 years.Ann Thorac Surg 1998;66:S49-52.
19. Magilligan DJ Jr, Lewis JW Jr, Stein P, Alam M. The porcine bioprosthetic heartvalve: experience at 15 years. Ann Thorac Surg 1989;48:324-9.
20. Cosgrove DM. Carpentier pericardial valve. Semin Thorac Cardiovasc Surg1996;8:269-75.
21. Cosgrove DM, Lytle BW, Gill CC, Golding LA, Stewart RW, Loop FD, et al. Invivo hemodynamic comparison of porcine and pericardial valves. J ThoracCardiovasc Surg 1985;89:358-68.
22. David TE, Armstrong S, Sun Z. The Hancock II bioprosthesis at 12 years. AnnThorac Surg 1998;66:S95-8.
23. David TE. Aortic valve surgery: where we are and where we shall go. J Heart ValveDis 1999;8:495-8.
24. David TE, Puschmann R, Ivanov J, Bos J, Armstrong S, Feindel CM, et al. Aorticvalve replacement with stentless and stented porcine valves: a case-match study.J Thorac Cardiovasc Surg 1998;116:236-41.
25. Doty DB, Cafferty A, Kon ND, Huysmans HA, Krause AH Jr, Westaby S.Medtronic freestyle aortic root bioprosthesis: implant techniques. J Card Surg1998;13:369-75.
26. Dagenais F, Cartier P, Dumesnil JG, Pibarot P, Lemieux M, Raymond G, et al. Asingle center experience with the freestyle bioprosthesis: midterm results at theQuebec Heart Institute. Semin Thorac Cardiovasc Surg 2001;13:156-62.
27. Westaby S, Jonson A, Payne N, Saito S, Jin XY, Del Rizzo DF, et al. Does the useof a stentless bioprosthesis increase surgical risk? Semin Thorac Cardiovasc Surg2001;13:143-7.
27a. Lucian GB, Casal G, Auriemma S, Santin F, Mazzucco A. Survival after stentlessand stented xenograft antivalve replacement: a concurrent, controlled trial. AThorac Surg 2002;74:1443-9.
28. Shargall Y, Goldman B, Christakis G, David T. Analysis of explants and causes ofmortality during long-term follow-up of the Toronto stentless porcine valve. SeminThorac Cardiovasc Surg 2001;13:106-12.
29. Rao V, Jamieson WR, Ivanov J, Armstrong S, David TE. Prosthesis-patientmismatch affects survival after aortic valve replacement. Circulation 2000;102:III5-9.
30. Medalion B, Lytle BW, McCarthy PM, Stewart RW, Arheart KL, Arnold JH, et al.Aortic valve replacement for octogenarians: are small valves bad? Ann Thorac Surg1998;66:699-705.
31. Medalion B, Blackstone EH, Lytle BW, White J, Arnold JH, Cosgrove DM. Aortic
Curr Probl Cardiol, July 2003 473

valve replacement: is valve size important? J Thorac Cardiovasc Surg 2000;119:963-74.
32. Jin XY, Zhang ZM, Gibson DG, Yacoub MH, Pepper JR. Effects of valve substituteon changes in left ventricular function and hypertrophy after aortic valve replace-ment. Ann Thorac Surg 1996;62:683-90.
33. Cohen G, Christakis GT, Joyner CD, Morgan CD, Tamariz M, Hanayama N, et al.Are stentless valves hemodynamically superior to stented valves? A prospectiverandomized trial. Ann Thorac Surg 2002;73:767-75.
34. Sommers KE, David TE. Aortic valve replacement with patch enlargement of theaortic annulus. Ann Thorac Surg 1997;63:1608-12.
35. David TE, Kuo J, Armstrong S. Aortic and mitral valve replacement withreconstruction of the intervalvular fibrous body. J Thorac Cardiovasc Surg1997;114:766-71.
36. David TE, Uden DE. Aortic valve replacement in adult patients with small aorticannuli. Ann Thorac Surg 1983;36:577-83.
37. Svensson LG, Crawford ES. Cardiovascular and vascular disease of the aorta.Philadelphia: WB Saunders, 1977.
38. Frater RW, Salomon NW, Rainer WG, Cosgrove DM 3rd, Wickham E. TheCarpentier-Edwards pericardial aortic valve: intermediate results. Ann Thorac Surg1992;53:764-71.
39. Frater RW, Furlong P, Cosgrove DM, Okies JE, Colburn LQ, Katz AS, et al.Long-term durability and patient functional status of the Carpentier-EdwardsPerimount pericardial bioprosthesis in the aortic position. J Heart Valve Dis1998;7:48-53.
40. Cosgrove DM, Lytle BW, Taylor PC, Camacho MT, Stewart RW, McCarthy PM,et al. The Carpentier-Edwards pericardial aortic valve: ten-year results. J ThoracCardiovasc Surg 1995;110:651-62.
41. Banbury MK, Cosgrove DM 3rd, White JA, Blackstone EH, Frater RW, Okies JE.Age and valve size effect on the long-term durability of the Carpentier-Edwardsaortic pericardial bioprosthesis. Ann Thorac Surg 2001;72:753-7.
42. Poirer NC, Pelletier LC, Pellerin M, Carrier M. 15-year experience with theCarpentier-Edwards pericardial bioprosthesis. Ann Thorac Surg 1998;66:S57-61.
43. Marchand MA, Aupart MR, Norton R, Goldsmith IR, Pelletier LC, Pellerin M, etal. Fifteen-year experience with the mitral Carpentier-Edwards PERIMOUNTpericardial bioprosthesis. Ann Thorac Surg 2001;71:S236-9.
44. Nakajima H, Aupart MR, Neville PH, Sirinelli AL, Meurisse YA, Marchand MA.Twelve-year experience with the 19 mm Carpentier-Edwards pericardial aorticvalve. J Heart Valve Dis 1998;7:534-9.
45. O’Brien MF, Goldstein S, Walsh S, Black KS, Elkins R, Clarke D. The SynerGraftvalve: a new acellular (nonglutaraldehyde-fixed) tissue heart valve for autologousrecellularization first experimental studies before clinical implantation. SeminThorac Cardiovasc Surg 1999;11:194-200.
46. Valente M, Faggian G, Billingham ME, Talenti E, Calabrese F, Casula R, et al. Theaortic valve after heart transplantation. Ann Thorac Surg 1995;60:S135-40.
47. Smith JD, Ogino H, Hunt D, Laylor RM, Rose ML, Yacoub MH. Humoral immuneresponse to human aortic valve homografts. Ann Thorac Surg 1995;60:S127-30.
48. Zhao XM, Green M, Frazer IH, Hogan P, O’Brien MF. Donor-specific immune
474 Curr Probl Cardiol, July 2003
response after aortic valve allografting in the rat. Ann Thorac Surg 1994;57:1158-63.
49. Hogan P, Duplock L, Green M, Smith S, Gall KL, Frazer IH, et al. Human aorticvalve allografts elicit a donor-specific immune response. J Thorac Cardiovasc Surg1996;112:1260-6.
50. Hoekstra F, Knoop C, Aghai Z, Jutte N, Mochtar B, Bos E, et al. Stimulation ofimmune-competent cells in vitro by human cardiac valve-derived endothelial cells.Ann Thorac Surg 1995;60:S131-3.
51. Shapira OM, Fonger JD, Reardon K, Shemin RJ. Unexplained fever after aorticvalve replacement with cryopreserved allografts. Ann Thorac Surg 1995;60:S151-5.
52. Clarke DR, Campbell DN, Hayward AR, Bishop DA. Degeneration of aortic valveallografts in young recipients. J Thorac Cardiovasc Surg 1993;105:934-41.
53. Fischlein T, Schutz A, Haushofer M, Frey R, Uhlig A, Detter C, et al. Immunologicreaction and viability of cryopreserved homografts. Ann Thorac Surg 1995;60:S122-5.
54. Rajani B, Mee RB, Ratliff NB. Evidence for rejection of homograft cardiac valvesin infants. J Thorac Cardiovasc Surg 1998;115:111-7.
55. Ross DN. Evolution of the homograft valve. Ann Thorac Surg 1995;59:565-7.56. Yacoub M, Rasmi NR, Sundt TM, Lund O, Boyland E, Radley-Smith R, et al.
Fourteen-year experience with homovital homografts for aortic valve replacement.J Thorac Cardiovasc Surg 1995;110:186-93.
57. O’Brien MF, Harrocks S, Stafford EG, Gardner MA, Pohlner PG, Tesar PJ, et al.The homograft aortic valve: a 29-year, 99.3% follow up of 1,022 valve replace-ments. J Heart Valve Dis 2001;10:334-44.
58. O’Brien MF, Harrocks S, Stafford G, Gardner M, Sparks L, Barnett A. Allograftaortic root replacement in 418 patients over a span of 15 years: 1985 to 2000. SeminThorac Cardiovasc Surg 2001;13:180-5.
59. Mitchell RN, Jonas RA, Schoen FJ. Structure-function correlations in cryopre-served allograft cardiac valves. Ann Thorac Surg 1995;60:S108-12.
60. Armiger LC. Viability studies of human valves prepared for use as allografts. AnnThorac Surg 1995;60:S118-20.
61. Niwaya K, Sakaguchi H, Kawachi K, Kitamura S. Effect of warm ischemia andcryopreservation on cell viability of human allograft valves. Ann Thorac Surg1995;60:S114-7.
62. Takkenberg JJ, van Herwerden LA, Eijkemans MJ, Bekkers JA, Bogers AJ.Evolution of allograft aortic valve replacement over 13 years: results of 275procedures. Eur J Cardiothorac Surg 2002;21:683-91.
63. Knott-Craig CJ, Elkins RC, Stelzer PL, Randolph JD, McCue C, Wright PA, et al.Homograft replacement of the aortic valve and root as a functional unit. AnnThorac Surg 1994;57:1501-5.
64. Lund O, Chandrasekaran V, Grocott-Mason R, Elwidaa H, Mazhar R, Khaghani A,et al. Primary aortic valve replacement with allografts over twenty-five years:valve-related and procedure-related determinants of outcome. J Thorac CardiovascSurg 1999;117:77-90.
65. Matsuki O, Robles A, Gibbs S, Bodnar E, Ross DN. Long-term performance of 555aortic homografts in the aortic position. Ann Thorac Surg 1988;46:187-91.
66. Okita Y, Franciosi G, Matsuki O, Robles A, Ross DN. Early and late results of
Curr Probl Cardiol, July 2003 475
aortic root replacement with antibiotic-sterilized aortic homograft. J ThoracCardiovasc Surg 1988;95:696-704.
67. Bodnar E, Matsuki O, Parker R, Ross DN. Viable and nonviable aortic homograftsin the subcoronary position: a comparative study. Ann Thorac Surg 1989;47:799-805.
68. Ross DN. Homograft replacement of the aortic valve. Lancet 1962;2:487-92.69. Barrett-Boyes BG. A method for preparing and inserting a homograft aortic valve.
Br J Surg 1965;52:847-56.70. Rubay JE, Raphael D, Sluysmans T, Vanoverschelde JL, Robert A, Schoevaerdts
JC, et al. Aortic valve replacement with allograft/autograft: subcoronary versusintraluminal cylinder or root. Ann Thorac Surg 1995;60:S78-82.
71. Hasnat K, Birks EJ, Liddicoat J, Hon JK, Edwards S, Glennon S, et al. Patientoutcome and valve performance following a second aortic valve homograftreplacement. Circulation 1999;100:II42-7.
72. O’Brien MF. Allograft aortic root replacement: standardization and simplificationof technique. Ann Thorac Surg 1995;60:S92-4.
73. Sundt TM 3rd, Rasmi N, Wong K, Radley-Smith R, Khaghani A, Yacoub MH.Reoperative aortic valve operation after homograft root replacement: surgicaloptions and results. Ann Thorac Surg 1995;60:S95-9.
74. Sabik JF, Lytle BW, Blackstone EH, Marullo AG, Pettersson GB, Cosgrove DM.Aortic root replacement with cryopreserved allograft for prosthetic valve endocar-ditis. Ann Thorac Surg 2002;74:650-9.
75. Lytle BW, Sabik JF, Blackstone EH, Svensson LG, Cosgrove DM 3rd. Reoperativecryopreserved root and ascending aorta replacement for acute prosthetic valveendocarditis. Ann Thorac Surg 2002;74:S1754-7.
76. Kirklin JK, Smith D, Novick W, Naftel DC, Kirklin JW, Pacifico AD, et al.Long-term function of cryopreserved aortic homografts: a ten-year study. J ThoracCardiovasc Surg 1993;106:154-65.
77. Chambers JC, Somerville J, Stone S, Ross DN. Pulmonary autograft procedure foraortic valve disease: long-term results of the pioneer series. Circulation 1997;96:2206-14.
78. Raanani E, Yau TM, David TE, Dellgren G, Sonnenberg BD, Omran A. Riskfactors for late pulmonary homograft stenosis after the Ross procedure. Ann ThoracSurg 2000;70:1953-7.
79. Bove T, Demanet H, Wathy P, Goldstein JP, Dessy H, Viart P, et al. In: Earlyresults of bovine jugular vein conduit versus bicuspid homografts for RVOTreconstruction. Fort Lauderdale (Fla): Society of Thoracic Surgeons; 2002. p.152-3.
80. Pearl JM, Cooper DS, Manning PB. Early failure of the Shelhigh pulmonic valveconduit in infants: the Cincinnati experience. In: Annual Meeting, Society of ThoracicSurgeons. Fort Lauderdale (Fla); Society of Thoracic Surgeons: 2002. p. 176.
81. Stock UA, Nagashima M, Khalil PN, Nollert GD, Herden T, Sperling JS, et al.Tissue-engineered valved conduits in the pulmonary circulation. J Thorac Cardio-vasc Surg 2000;119:732-40.
82. Shum-Tim D, Stock U, Hrkach J, Shinoka T, Lien J, Moses MA, et al. Tissueengineering of autologous aorta using a new biodegradable polymer. Ann ThoracSurg 1999;68:2298-304.
476 Curr Probl Cardiol, July 2003
83. Elkins RC, Dawson PE, Goldstein S, Walsh SP, Black KS. Decellularized humanvalve allografts. Ann Thorac Surg 2001;71:S428-32.
84. Carr-White GS, Kon M, Koh TW, Glennan S, Ferdinand FD, De Souza AC, et al.Right ventricular function after pulmonary autograft replacement of the aorticvalve. Circulation 1999;100:II36-41.
85. Ward KE, Elkins RC, Overholt ED, Knott-Craig CJ, Razook JD, Lane MM, et al.Evaluation of cryopreserved homografts in the right ventricular outflow tract afterthe Ross procedure: intermediate-term follow up. J Heart Valve Dis 1997;6:130-3.
86. Carr-White GS, Kilner PJ, Hon JK, Rutledge T, Edwards S, Burman ED, et al.Incidence, location, pathology, and significance of pulmonary homograft stenosisafter the Ross operation. Circulation 2001;104:I16-20.
87. David TE, Omran A, Ivanov J, Armstrong S, de Sa MP, Sonnenberg B, et al.Dilation of the pulmonary autograft after the Ross procedure. J Thorac CardiovascSurg 2000;119:210-20.
88. Elkins RC. The Ross operation: a 12-year experience. Ann Thorac Surg 1999;68:S14-8.
89. Elkins RC, Knott-Craig CJ, Ward KE, Lane MM. The Ross operation in children:10-year experience. Ann Thorac Surg 1998;65:496-502.
90. Elkins RC, Lane MM, McCue C, Ward KE. Pulmonary autograft root replacement:mid-term results. J Heart Valve Dis 1999;8:499-503.
91. Knott-Craig CJ, Elkins RC, Santangelo KL, McCue C, Lane MM. Aortic valvereplacement: comparison of late survival between autografts and homografts. AnnThorac Surg 2000;69:1327-32.
92. Salley RK, Sekela ME. The Ross procedure: a midterm follow-up. In: Annualmeeting, Society of Thoracic Surgeons. Fort Lauderdale (Fla); Society of ThoracicSurgeons: 2002. p. 58.
93. de Sa M, Moshkovitz Y, Butany J, David TE. Histologic abnormalities of the ascendingaorta and pulmonary trunk in patients with bicuspid aortic valve disease: clinicalrelevance to the ross procedure. J Thorac Cardiovasc Surg 1999;118:588-94.
94. Oury JH, Hiro SP, Maxwell JM, Lamberti JJ, Duran CM. The Ross procedure:current registry results. Ann Thorac Surg 1998;66:S162-5.
95. Casselman FP, Gillinov AM, Akhrass R, Kasirajan V, Blackstone EH, CosgroveDM. Intermediate-term durability of bicuspid aortic valve repair for prolapsingleaflet. Eur J Cardiothorac Surg 1999;15:302-8.
96. Cosgrove DM 3rd. Aortic valve repair. Ann Thorac Surg 1992;54:1014-5.97. Cosgrove DM, Rosenkranz ER, Hendren WG, Bartlett JC, Stewart WJ. Valvulo-
plasty for aortic insufficiency. J Thorac Cardiovasc Surg 1991;102:571-6.98. Fraser CD Jr, Wang N, Mee RB, Lytle BW, McCarthy PM, Sapp SK, et al. Repair
of insufficient bicuspid aortic valves. Ann Thorac Surg 1994;58:386-90.99. Fraser CD Jr, Cosgrove DM 3rd. Surgical techniques for aortic valvuloplasty. Tex
Heart Inst J 1994;21:305-9.100. Cabrol C, Cabrol A, Guiraudon G, Bertrand M. Treatment of aortic insufficiency by
means of aortic annuloplasty. Arch Mal Coeur Vaiss 1966;59:1305-12.101. Lytle BW, Cosgrove DM, Gill CC, Taylor PC, Stewart RW, Golding LA, et al.
Aortic valve replacement combined with myocardial revascularization: late resultsand determinants of risk for 471 in-hospital survivors. J Thorac Cardiovasc Surg1988;95:402-14.
102. Lytle BW, Cosgrove DM, Taylor PC, Goormastic M, Stewart RW, Golding LA, et
Curr Probl Cardiol, July 2003 477
al. Primary isolated aortic valve replacement: early and late results. J ThoracCardiovasc Surg 1989;97:675-94.
103. Kay PH, Nunley D, Grunkemeier GL, Garcia C, McKinley CL, Starr A. Ten-yearsurvival following aortic valve replacement: a multivariate analysis of coronarybypass as a risk factor. J Cardiovasc Surg (Torino) 1986;27:494-9.
103a. Akins CW, Hilgenberg AD, Vlahakes GJ, MacGillivray TE, Torchiana DF, MadsenJC. Results of bioprosthetic versus mechanical aortic valve replacement performedwith concomitant coronary bypasss grafting. Ann Thorac Surg 2002;74:1098-106.
104. Cosgrove DM 3rd, Sabik JF, Navia JL. Minimally invasive valve operations. AnnThorac Surg 1998;65:1535-8.
105. Navia JL, Cosgrove DM 3rd. Minimally invasive mitral valve operations. AnnThorac Surg 1996;62:1542-4.
106. Svensson LG. Minimal-access “J” or “ j” sternotomy for valvular, aortic, andcoronary operations or reoperations. Ann Thorac Surg 1997;64:1501-3.
107. Svensson LG, D’Agostino RS. Minimal-access aortic and valvular operations,including the “J/j” incision. Ann Thorac Surg 1998;66:431-5.
108. Svensson LG, D’Agostino RS. “J” incision minimal-access valve operations. AnnThorac Surg 1998;66:1110-2.
109. Svensson LG, Nadolny EM, Kimmel WA. Minimal access aortic surgery includingre-operations. Eur J Cardiothorac Surg 2001;19:30-3.
110. Yacoub MH, Gehle P, Chandrasekaran V, Birks EJ, Child A, Radley-Smith R. Lateresults of a valve-preserving operation in patients with aneurysms of the ascendingaorta and root. J Thorac Cardiovasc Surg 1998;115:1080-90.
111. Sarsam MA, Yacoub M. Remodeling of the aortic valve anulus. J ThoracCardiovasc Surg 1993;105:435-8.
112. David TE, Feindel CM. An aortic valve-sparing operation for patients with aorticincompetence and aneurysm of the ascending aorta. J Thorac Cardiovasc Surg1992;103:617-21.
113. Svensson LG, Longoria J, Kimmel WA, Nadolny E. Management of aortic valvedisease during aortic surgery. Ann Thorac Surg 2000;69:778-83.
114. David TE. Aortic valve-sparing operations for aortic root aneurysm. Semin ThoracCardiovasc Surg 2001;13:291-6.
115. David TE, Armstrong S, Ivanov J, Feindel CM, Omran A, Webb G. Results ofaortic valve-sparing operations. J Thorac Cardiovasc Surg 2001;122:39-46.
116. David TE, Armstrong S, Ivanov J, Webb GD. Aortic valve sparing operations: anupdate. Ann Thorac Surg 1999;67:1840-2.
117. Birks EJ, Webb C, Child A, Radley-Smith R, Yacoub MH. Early and long-termresults of a valve-sparing operation for Marfan syndrome. Circulation 1999;100:II29-35.
118. Kunzelman KS, Grande KJ, David TE, Cochran RP, Verrier ED. Aortic root andvalve relationships: impact on surgical repair. J Thorac Cardiovasc Surg 1994;107:162-70.
119. Tambeur L, David TE, Unger M, Armstrong S, Ivanov J, Webb G. Results ofsurgery for aortic root aneurysm in patients with the Marfan syndrome. EurJ Cardiothorac Surg 2000;17:415-9.
120. Kallenbach K, Hagl C, Walles T, Pethig K, Leyh RG, Haverich A. Results of valvesparing aortic root reconstruction in 157 consecutive patients. In: Annual meeting,
478 Curr Probl Cardiol, July 2003
Society of Thoracic Surgeons. Fort Lauderdale (Fla); Society of Thoracic Surgeons:2002. p. 180-1.
121. Svensson LG. Sizing for modified David reimplantation procedure. Ann ThoracSurg (in press).
122. Svensson LG, Khitin L. Aortic cross-sectional area/height ratio timing of aorticsurgery in asymptomatic patients with Marfan syndrome. J Thorac Cardiovasc Surg2002;123:360-1.
123. Svensson LG, Nadolony E, Kimmel W. Multimodal protocol influence on strokeand neurocognitive deficit prevention after ascending arch operations. Ann ThoracSurg 2002:74:2040-6.
124. Svensson LG, Crawford ES, Coselli JS, Safi HJ, Hess KR. Impact of cardiovascularoperation on survival in the Marfan patient. Circulation 1989;80:I233-42.
125. Svensson LG, Crawford ES, Hess KR, Coselli JS, Safi HJ. Composite valve graftreplacement of the proximal aorta: comparison of techniques in 348 patients. AnnThorac Surg 1992;54:427-37.
126. McDonald ML, Smedira NG, Blackstone EH, Grimm RA, Lytle BW, CosgroveDM. Reduced survival in women after valve surgery for aortic regurgitation: effectof aortic enlargement and late aortic rupture. J Thorac Cardiovasc Surg 2000;119:1205-12.
127. Kaplon RJ, Cosgrove DM 3rd, Gillinov AM, Lytle BW, Blackstone EH, SmediraNG. Cardiac valve replacement in patients on dialysis: influence of prosthesis onsurvival. Ann Thorac Surg 2000;70:438-41.
128. Bloomfield P, Wheatley DJ, Prescott RJ, Miller HC. Twelve-year comparison of aBjork-Shiley mechanical heart valve with porcine bioprostheses. N Engl J Med1991;324:573-9.
129. Hammermeister KE, Henderson WG, Burchfiel CM, Sethi GK, Souchek J, OprianC, et al. Comparison of outcome after valve replacement with a bioprosthesisversus a mechanical prosthesis: initial 5 year results of a randomized trial. J AmColl Cardiol 1987;10:719-32.
130. Hammermeister KE, Sethi GK, Henderson WG, Oprian C, Kim T, Rahimtoola S.A comparison of outcomes in men 11 years after heart-valve replacement with amechanical valve or bioprosthesis: Veterans Affairs Cooperative Study on ValvularHeart Disease. N Engl J Med 1993;328:1289-96.
131. Gross C, Klima U, Mair R, Brucke P. Aortic homografts versus mechanical valvesin aortic valve replacement in young patients: a retrospective study. Ann ThoracSurg 1998;66:S194-7.
132. Grocott-Mason RM, Lund O, Elwidaa H, Mazhar R, Chandrasakeran V, MitchellAG, et al. Long-term results after aortic valve replacement in patients withcongestive heart failure: homografts vs prosthetic valves. Eur Heart J 2000;21:1698-707.
133. Agnihotri AK, McGiffin DC, Galbraith AJ, O’Brien MF. The prevalence ofinfective endocarditis after aortic valve replacement. J Thorac Cardiovasc Surg1995;110:1708-20.
134. Aklog L, Carr-White GS, Birks EJ, Yacoub MH. Pulmonary autograft versus aortichomograft for aortic valve replacement: interim results from a prospectiverandomized trial. J Heart Valve Dis 2000;9:176-88.
135. Kouchoukos NT. Aortic allografts and pulmonary autografts for replacement of theaortic valve and aortic root. Ann Thorac Surg 1999;67:1846-8.
Curr Probl Cardiol, July 2003 479
136. Kouchoukos NT, Davila-Roman VG, Spray TL, Murphy SF, Perrillo JB. Replace-ment of the aortic root with a pulmonary autograft in children and young adultswith aortic-valve disease. N Engl J Med 1994;330:1-6.
137. Kouchoukos NT. Reconstructive surgery of the aortic root. Ann Thorac Surg1995;60:734-5.
138. Svensson LG, Crawford ES. Cardiovascular and vascular disease of the aorta.Philadelphia: WB Saunders, 1997.
139. Lauer MS, Blackstone EH, Young JB, Topol EJ. Casue of death in clinicalresearch: time for a reassessment? J Am Coll Cardiol 1999;34:618-20.
140. Blackstone EH, Naftel DC, Turner ME Jr. The decomposition of time-varyinghazard into phases, each incorporating a separate stream of concomitant informa-tion. J Am Stat Assn 1986;81:615-24.
141. Steyerberg EW, Elijkemans MJ, Harrell FE Jr, Habbema JD. Prognostic modellingwith logistic regression analysis: a comparison of selection and estimation methodsin small data sets. Stat Med 2000;19:1059-70.
142. Blackstone EH, Cosgrove DM, Jamieson WR, Birkmeyer NJ, Lemmer JH Jr, MillerDC, et al. Prosthesis size and long-term survival after aortic valve replacement. JThorac Cardiovasc Surg 2003;126:783-93.
480 Curr Probl Cardiol, July 2003