Embed Size (px)
Citation preview

a report by
Pierre J Hoffmeyer
Professor and Chairman, Department of Orthopaedic Surgery, University Hospitals of Geneva
Displaced proximal humerus fractures are on the rise and, in many
cases, are still the source of painful loss of function if not adequately
treated. Many treatment options exist depending on the fracture
pattern, the bone stock and the vascular status of the fractured
fragments. Recently, many fixation techniques using various implants
have been introduced; some implants have been successful, others less
so. The indications for the newer plates with locking screws or locked
nails have yet to be evaluated. Arthroplasty remains a useful option
when the fracture is not reconstructible due to extensive comminution
or inadequate osteoporotic bone. Whether the fracture is
reconstructed or a prosthesis inserted, the rehabilitation protocol is a
very important part of the treatment plan and must be strictly adhered
to if good results are to be expected.
Introduction
Displaced fractures of the proximal humerus are frequent articular injuries
that are a source of pain, functional loss and disability. These articular
fractures are complex injuries involving the glenohumeral space, the
subacromial space, the rotator cuff and the capsule. Furthermore,
adjacent neurological and vascular structures are also at risk when these
fractures occur.
Definition of ‘Displaced’
A fracture is said to be displaced when the morphologic disruption of the
fragments hampers normally smooth and painless articular function. This
concerns about 20% of all proximal humerus fractures. In the past,
authors have used measurements (1cm translation and/or 45° angular
displacement) to define the fragment displacement necessary for surgical
intervention.1 Today, any displacement presumably leading to poor
function may qualify for surgical fixation. However, surgical indication is
obviously not related solely to fracture displacement and must be
associated with patient expectations and activity.
Pathophysiology
These fractures are essentially related to osteoporosis, which accounts for
many of the difficulties encountered when performing internal fixation.2,3
This signifies that the bone fragments will be of a low mineral content and
that the holding power of the implants will be compromised. This implies
using techniques or implants designed for fragility fractures. The
vascularisation of the proximal humerus is of a terminal type, similar to
other epiphyses such as the femoral head or talus. The main sources of
blood supply are the anterior circumflex and posterior circumflex arteries,
the vessels of the rotator cuff and the intraosseous metaphyseal artery. If
the main nutrient arteries to the humeral head are interrupted, avascular
necrosis with subsequent collapse of the articular surface will occur.4 Neer
has contributed to establishing an estimation of prognosis with the
fragment classification of proximal humeral fractures, which other authors
have refined.5 Other factors affecting outcome are the complexity of the
surgical approach, the obligatory use of indirect reduction techniques
because the articular surfaces cannot be visualised intra-operatively and
the lack of perfect fixation techniques. Once the purely surgical hurdles
have been passed, there remains the rehabilitative process, which is also a
cause for controversy. All these problems have led some authors to refer
to this fracture as being still ‘unsolved’.6
Imaging
Accurate imaging is mandatory for precise classification, a strategically
essential step for establishing the operative tactics. Strict anteroposterior
(AP) and axillary views with a clear view of the glenohumeral space will
show fragment displacement, allowing pre-operative planning. Spiral
3-D computed tomography (CT) scanning is an ideal imaging modality
showing from all perspectives the exact relationships and positions
between all involved fragments. Surgical planning is enhanced by these
techniques and hopefully a better outcome will be achieved in these
difficult injuries.
Patient Positioning for the Intervention
In most cases the patient is operated on in a beach chair position under
a general anaesthetic and the question arises as to whether an
interscalene bloc is indicated. This is only possible after a careful
neurological examination has ruled out any pre-existing neurological
Surgical Management of Displaced Fractures of the Proximal Humerus
© T O U C H B R I E F I N G S 2 0 0 7
Pierre J Hoffmeyer is Professor of Orthopaedics, Head of theOrthopaedic and Trauma Service and Chairman of theDepartment of Surgery of the University Hospital of Geneva,Switzerland. He is a member of many national andinternational societies, including the European Shoulder andElbow Society, and is active in the Swiss Association forOsteosynthesis. Professor Hoffmeyer is the author of over200 scientific publications and book chapters. He wastrained in Geneva, Vancouver and Rochester, MN.
Orthopaedic Surgery Shoulder
78
In case of an isolated greater
tuberosity fracture or an impacted
three fragment necessitating little
reduction a deltoid split rotator cuff
approach can be performed.
Hoffmeyer_edit.qxp 1/5/07 10:28 am Page 78

79E U R O P E A N M U S C U L O S K E L E T A L R E V I E W 2 0 0 7
Surgical Management of Displaced Fractures of the Proximal Humerus
injury; in cases of doubt one should abstain and use other antalgic
modalities, including patient-controlled antalgia pumps and the generous
use of ice applications (see Figure 1).
Surgical Approaches
As a rule, when reduction manoeuvres must be undertaken it is safest
to use an extensile delto-pectoral approach and the axillary may be
palpated as it lies anteriorly to the subscapularis muscle. The individual
tendons and fragments are then carefully identified using the biceps
tendon as a marker. The tuberosity fragments can then be reduced
around the head. In case of an isolated greater tuberosity fracture or an
impacted three fragment necessitating little reduction a deltoid split
rotator cuff approach can be performed. For intramedullary nailing a
small incision made superiorly over the greater tuberosity may be
sufficient. Very rarely, in cases of an associated posterior dislocation, a
posterior incision might be necessary. In any case the use of an image
intensifier is useful for evaluating fracture reduction.3
Fixation Modalities
Osteosynthesis
See Figure 2. In certain situations, such as two-part fractures at the
surgical neck in strong bone, a standard plate and screw fixation may
be sufficient. With weaker bone, the newer locking plates afford
excellent stability.7 Displaced fractures of the greater tuberosity are
adequately fixed with heavy non-resorbable sutures; displaced lesser
tuberosity fractures are better fixed with isolated compression screws.
Strong fixation will allow stable fixation and immediate mobilisation
of the shoulder.
Osteosuture
See Figure 3. In case of a three-fragment fracture or a four-fragment
valgus-impacted fracture in a patient with porotic or soft bone, it may be
useful to proceed with a supple fixation involving steel wire or heavy non-
resorbable suture.8 The sutures are passed through the bony fragments
at the tendon–bone interface of each main tendon. These are tied around
a screw and washer inserted distally to the fracture into the metaphysis
after the main cephalic fragment has been reduced with a K-wire
manoeuvred as a joystick. In this situation, locking plates can be used to
buttress the fragments. However, care must be taken not to use screws
that are too long in the cephalic fragment with the danger of over-
penetration and breaching into the articular space. The advantage of this
technique is the solid fixation obtained allowing immediate post-
operative mobilisation.
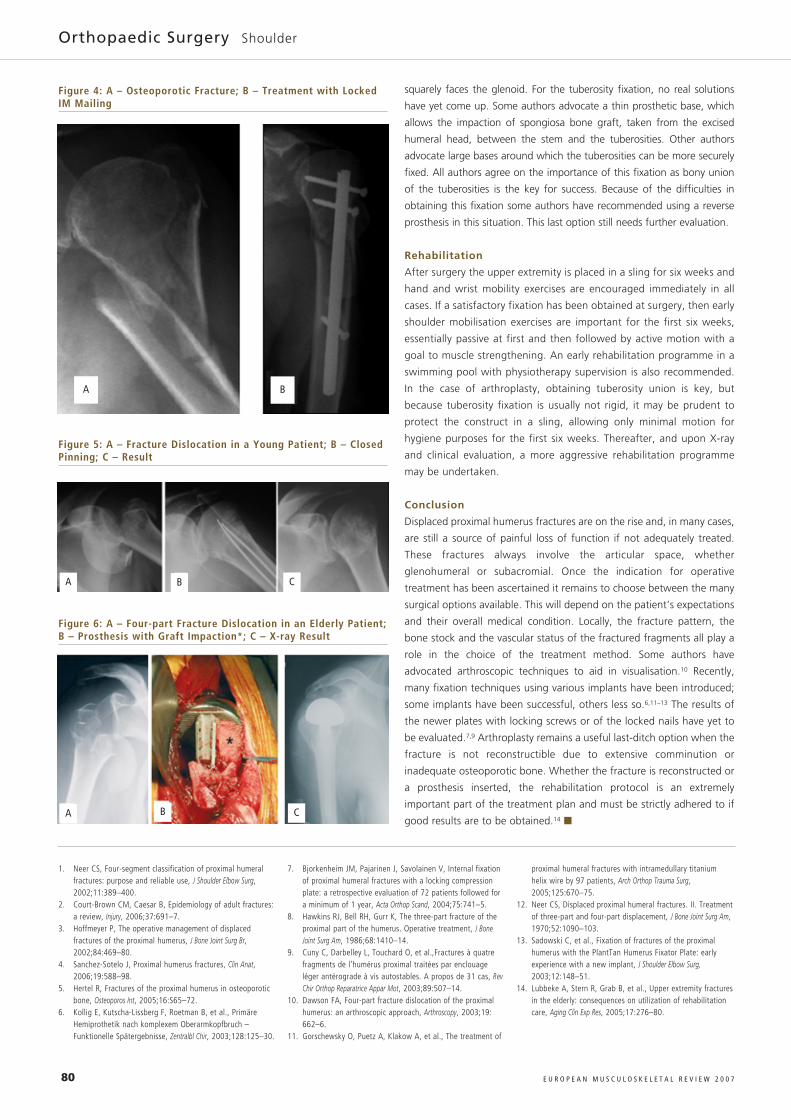
Intramedullary Nailing
See Figure 4. Some authors have advocated the use of closed techniques
such as locked intramedullary nailing to obtain an acceptable reduction
and an adequate fixation of the fracture fragments.9 Further evaluation
of these techniques, applied to articular fractures, is still needed.
Fascicular Pinning
See Figure 5. In an effort to minimise the surgical approach, some
authors advocate the use of multiple percutaneous K-wires. This
necessitates accurate reduction, which can be obtained with
percutaneous joystick manoeuvring. This is a demanding technique and
it is not really possible to mobilise the shoulder before sufficient bony
healing has taken place.
Arthroplasty
See Figure 6. In cases of comminuted, displaced four-fragment fractures
in weak bone or if a dislocation has completely detached the cephalic
fragment, arthroplasty is indicated. The surgical difficulties include
obtaining adequate prosthetic head height, suitable torsion or strong
tuberosity fixation. For the head height, a pre-operative plan using the
contra-lateral shoulder as a model can be useful. Concerning prosthetic
retro-torsion, it is imperative that in a resting position the humeral head
Figure 1: A – Patient Under General Anesthetic in Semi-sittingPosition with a Head Rest Allowing Adequate Exposure of theShoulder and Thoracic Quadrant; B – Note the ExtensiveEcchymosis Following the Fracture Dislocation
Figure 2: A – Impacted Three-part Fracture; B – 3-DReconstruction; C – Osteosynthesis Using Locking Plate withSutures Securing the Cuff to the Plate; D – Post-op X-ray
Figure 3: A – Three-part Fracture; B – OsteosutureReconstruction; C – One-year X-Ray Result
A
A B
BA C
B
C D
Hoffmeyer_edit.qxp 1/5/07 10:28 am Page 79
80 E U R O P E A N M U S C U L O S K E L E T A L R E V I E W 2 0 0 7
Orthopaedic Surgery Shoulder
squarely faces the glenoid. For the tuberosity fixation, no real solutions
have yet come up. Some authors advocate a thin prosthetic base, which
allows the impaction of spongiosa bone graft, taken from the excised
humeral head, between the stem and the tuberosities. Other authors
advocate large bases around which the tuberosities can be more securely
fixed. All authors agree on the importance of this fixation as bony union
of the tuberosities is the key for success. Because of the difficulties in
obtaining this fixation some authors have recommended using a reverse
prosthesis in this situation. This last option still needs further evaluation.
Rehabilitation
After surgery the upper extremity is placed in a sling for six weeks and
hand and wrist mobility exercises are encouraged immediately in all
cases. If a satisfactory fixation has been obtained at surgery, then early
shoulder mobilisation exercises are important for the first six weeks,
essentially passive at first and then followed by active motion with a
goal to muscle strengthening. An early rehabilitation programme in a
swimming pool with physiotherapy supervision is also recommended.
In the case of arthroplasty, obtaining tuberosity union is key, but
because tuberosity fixation is usually not rigid, it may be prudent to
protect the construct in a sling, allowing only minimal motion for
hygiene purposes for the first six weeks. Thereafter, and upon X-ray
and clinical evaluation, a more aggressive rehabilitation programme
may be undertaken.
Conclusion
Displaced proximal humerus fractures are on the rise and, in many cases,
are still a source of painful loss of function if not adequately treated.
These fractures always involve the articular space, whether
glenohumeral or subacromial. Once the indication for operative
treatment has been ascertained it remains to choose between the many
surgical options available. This will depend on the patient’s expectations
and their overall medical condition. Locally, the fracture pattern, the
bone stock and the vascular status of the fractured fragments all play a
role in the choice of the treatment method. Some authors have
advocated arthroscopic techniques to aid in visualisation.10 Recently,
many fixation techniques using various implants have been introduced;
some implants have been successful, others less so.6,11–13 The results of
the newer plates with locking screws or of the locked nails have yet to
be evaluated.7,9 Arthroplasty remains a useful last-ditch option when the
fracture is not reconstructible due to extensive comminution or
inadequate osteoporotic bone. Whether the fracture is reconstructed or
a prosthesis inserted, the rehabilitation protocol is an extremely
important part of the treatment plan and must be strictly adhered to if
good results are to be obtained.14 ■
1. Neer CS, Four-segment classification of proximal humeralfractures: purpose and reliable use, J Shoulder Elbow Surg,2002;11:389–400.
2. Court-Brown CM, Caesar B, Epidemiology of adult fractures:a review, Injury, 2006;37:691–7.
3. Hoffmeyer P, The operative management of displacedfractures of the proximal humerus, J Bone Joint Surg Br,2002;84:469–80.
4. Sanchez-Sotelo J, Proximal humerus fractures, Clin Anat,2006;19:588–98.
5. Hertel R, Fractures of the proximal humerus in osteoporoticbone, Osteoporos Int, 2005;16:S65–72.
6. Kollig E, Kutscha-Lissberg F, Roetman B, et al., PrimäreHemiprothetik nach komplexem Oberarmkopfbruch –Funktionelle Spätergebnisse, Zentralbl Chir, 2003;128:125–30.
7. Bjorkenheim JM, Pajarinen J, Savolainen V, Internal fixationof proximal humeral fractures with a locking compressionplate: a retrospective evaluation of 72 patients followed fora minimum of 1 year, Acta Orthop Scand, 2004;75:741–5.
8. Hawkins RJ, Bell RH, Gurr K, The three-part fracture of theproximal part of the humerus. Operative treatment, J BoneJoint Surg Am, 1986;68:1410–14.
9. Cuny C, Darbelley L, Touchard O, et al.,Fractures à quatrefragments de l’humérus proximal traitées par enclouageléger antérograde à vis autostables. A propos de 31 cas, RevChir Orthop Reparatrice Appar Mot, 2003;89:507–14.
10. Dawson FA, Four-part fracture dislocation of the proximalhumerus: an arthroscopic approach, Arthroscopy, 2003;19:662–6.
11. Gorschewsky O, Puetz A, Klakow A, et al., The treatment of
proximal humeral fractures with intramedullary titaniumhelix wire by 97 patients, Arch Orthop Trauma Surg,2005;125:670–75.
12. Neer CS, Displaced proximal humeral fractures. II. Treatmentof three-part and four-part displacement, J Bone Joint Surg Am,1970;52:1090–103.
13. Sadowski C, et al., Fixation of fractures of the proximalhumerus with the PlantTan Humerus Fixator Plate: earlyexperience with a new implant, J Shoulder Elbow Surg,2003;12:148–51.
14. Lubbeke A, Stern R, Grab B, et al., Upper extremity fracturesin the elderly: consequences on utilization of rehabilitationcare, Aging Clin Exp Res, 2005;17:276–80.
Figure 4: A – Osteoporotic Fracture; B – Treatment with LockedIM Mailing
Figure 6: A – Four-part Fracture Dislocation in an Elderly Patient;B – Prosthesis with Graft Impaction*; C – X-ray Result
Figure 5: A – Fracture Dislocation in a Young Patient; B – ClosedPinning; C – Result
A
A
C
C
B
B
A B
Hoffmeyer_edit.qxp 1/5/07 10:29 am Page 80

![Biomechanical Investigation of Locked Plate Fixation with ...duction and internal fixation (ORIF) of displaced proximal humerus fractures is an accepted surgical technique [1]-[6]](https://img.pdfslide.us/doc/110x75/5e32b0b6c428c77b4b67396f/biomechanical-investigation-of-locked-plate-fixation-with-duction-and-internal.jpg)