Embed Size (px)
Citation preview

World J. Surg. 12, 676-684, 1988
World Journal of Surgery �9 1988 by the Soci~t~
lnternationale de Chirurgie
Surgical Lessons from the Intergroup Rhabdomyosarcoma Study (IRS) Pertaining to Extremity Tumors
Walter Lawrence, Jr., M.D., Daniel M. Hays, M.D., Ruth Heyn, M.D., Mohan Beltangady, Ph.D., Harold M. Maurer, M.D. (for the Intergroup Rhabdomyosarcoma Study Committee), and others*
Representing Children's Cancer Study Group, Pediatric Oncology Group, United Kingdom Children's Cancer Study Group, and Pediatric Intergroup Statistical Center
The large number of patients entered into the Intergroup Rhabdo- myosarcoma Study (IRS) has allowed a study of prognostic factors and clinical management decisions for a specific primary site---the extremities. A retrospective review of IRS I (1972-1978) and IRS II (1978-1984) included 217 patients with sarcomas of the extremities of 1,415 patients without distant metastases. Disease-free survival and survival data from this subgroup of patients demonstrated that: (a) the UICC clinical staging system has clear-cut validity, (b) total gross resection of sarcomas of the extremities is an optimal therapeutic approach in spite of proven benefits from nonoperative therapies, (c) results of treatment are improved by reexcision of the initial resection site if the histologic margin is involved o r
the initial resection was an unplanned procedure for diagnosis, (d) regional lymph node biopsy or dissection is an important procedure for planning and conduct of the treatment program, and (e) vigorous and thorough surgical procedures are required for optimal end results of treatment of extremity sarcomas despite the proven value of nonoperative therapies.
Patients with childhood rhabdomyosarcoma demonstrate marked variations in presentation, nature of clinical manage- ment decisions and prognosis depending on the anatomic site of origin of the sarcoma. Whereas radical surgical approaches are not feasible for many of the anatomic sites of origin, the extremity sites are often amenable to radical surgery (including amputation). This factor makes this site a particularly important one from the standpoint of surgical management decisions.
The large number of patients entered into the Intergroup Rhabdomyosarcoma Study (IRS) since its initiation in 1972 has allowed us to utilize data obtained for extremity sites to assist in answering some questions regarding the importance of potential
*William Crist, M.D., Edmund A. Gehan, Ph.D., Denman Ham- mond, M.D., Pat Morris Jones, M.D., William Newton, Jr., M.D., A.H. Ragab, M.D., R. Beverly Raney, Jr., M.D., Frederick B. Ruymann, M.D., Melvin Tefft, M.D,, Bruce Webber, M.D., and Moody Wharam, M.D.
Presented at the Soci6t6 Internationale de Chirurgie in Sydney, Australia, September, 1987.
Supported by grants CA-24507, CA-30138, CA-30969, CA-29139, and CA-13539 from the National Cancer Institute.
Reprint requests: Dr. Walter Lawrence, Jr., Division of Surgical Oncology, Medical College of Virginia, P.O. Box 11, MCV Station, Richmond, Virginia 23298-0001, U.S.A.
prognostic factors and surgical decisions in their management. These are pertinent questions in view of the significant impact of nonsurgical approaches to soft tissue sarcomas in childhood, a situation quite dissimilar to that seen with adult soft tissue sarcomas. Specific questions regarding the surgical approach to extremity sarcomas in childhood included the potential impor- tance of various staging factors and histologic subtype on the surgical treatment and outcome, the need for total gross resec- tion of the sarcoma (even if major physical disability is a result), the relative need for achieving pathologically clear margins under the same circumstances, and the optimal management approach to the regional lymph nodes.
Background
Rhabdomyosarcoma is the most frequent soft tissue sarcoma in children. Prior to the mid-1960's, less than 20% of children with rhabdomyosarcoma enjoyed long-term survival, a time when surgical resection and/or radiation were the only true effective therapies [1, 2]. The development of effective chemotherapy and the demonstration by Heyn et al. [3] that an adjuvant chemotherapy program was effective, led to a major improve- ment in end results of treatment. With almost 70% of children with these sarcomas surviving after multidisciplinary treatment programs including surgery, radiation, and intensive chemo- therapy, a new era began in the early 1970's. The national cooperative effort, the Intergroup Rhabdomyosarcoma Study (IRS) was initiated to further refine the therapy for this disease [4].
The IRS was initiated in 1972 and patient entry into the multiple protocols, depending on surgical-pathologic group (clinical group), totaled 1,626 eligible patients after the first 2 major protocols were completed in 1984. Of these, 1,415 patients had no distant metastases (group I-III) . All patients in the first study (IRS I), entered in the years 1972-1978, have a potential follow-up interval of at least 9 years. The minimum follow-up time is 3 years for the second study (IRS II), from 1978 to 1984.
This national cooperative clinical trial, which included pa- tients from the United Kingdom, has utilized a surgical-
W. Lawrence, Jr. et al.: Rhabdomyosarcoma 677
Table 1. Surgical-pathologic grouping system used in trials I and II of the Intergroup Rhabdomyosarcoma Study.
Group I: Localized disease, completely resccted. A. Confined to organ or muscle of origin, B. Infiltration outside organ or muscle of origin; regional
nodes not involved. Group II: Compromised or regional resection of 3 types including:
A. Grossly resected tumors with "microscopic residual," B. Regional disease, completely resected, in which nodes
may be involved and/or extension of tumor into an adjacent organ present%
C. Regional disease with involved nodes, grossly resected, but with evidence of "microscopic residual."
Group III: Incomplete resection o r biopsy with gross residual disease. Group IV: Distant metastases, present at onset.
~In IRS III, this category (II B) is limited to patients with microscopically-proven regional lymph node metastasis.
Z 0
ry
o 0 o~ (I.
1.0~
0.9-
0.8-
0.7-
o%
0.6 - " ........ o
0 . 5 "
0.4 -
0 , 3 -
0 . 2 "
0o l ~
0.0
%
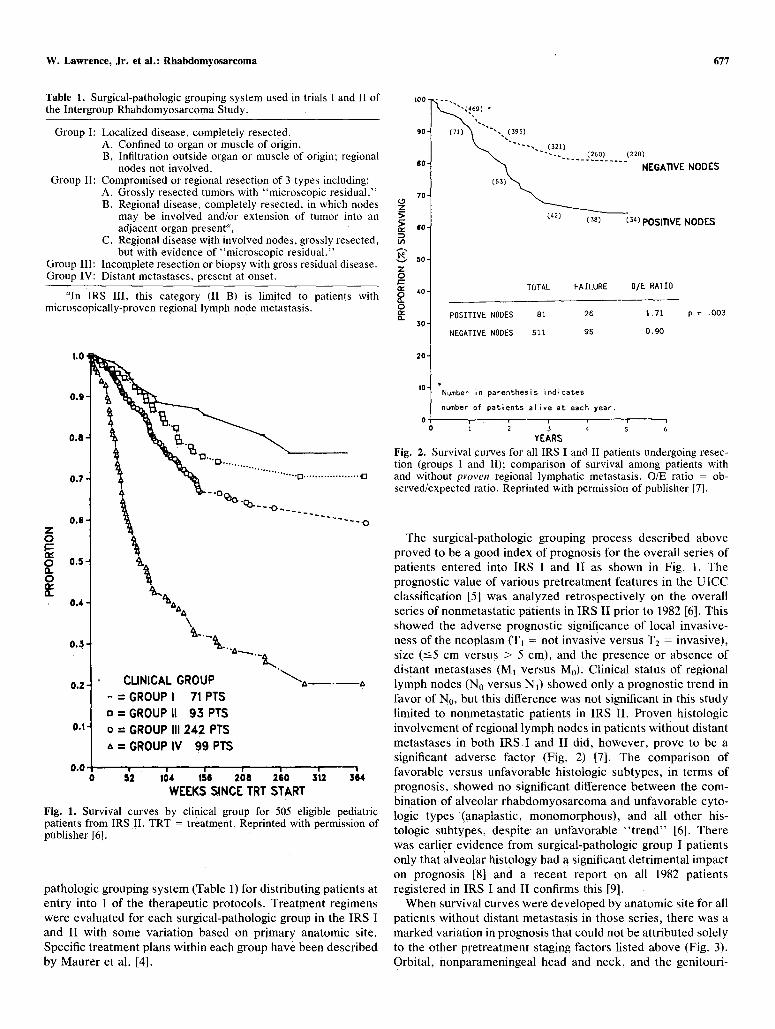
CUNICAL GROUP - = G R O U P I 71PTS o=GROUPI I 93PTS o = GROUP III 242 PTS A=GROUPIV 99PTS
WEEKS SINCE TRT START
Fig. 1. Survival curves by clinical group for 505 eligible pediatric patients from IRS II. TRT = treatment. Reprinted with permission of publisher [6].
pathologic grouping system (Table 1) for distributing patients at entry into 1 of the therapeutic protocols. Treatment regimens were evaluated for each surgical-pathologic group in the IRS I and II with some variation based on primary anatomic site. Specific treatment plans within each group have been described by Maurer et al. [4].
>_ > t~
t/%
v Z 0
0 rv r~
100-
9 0 -
60-
70-
60-
50-
4 0 -
30-
20-
10-
0
69 ) *
. . . . . . . . . _(260) . . . . . (22~ NODES
(42) (38) (34) POSITIVE NODES
TOTAL FAILURE D/E RATIO
POSITIVE NODES 81 26 1.71
NEGATIVE NODES 511 95 0,90
p = .003
'Number in parenthesis indicates
number of patients alive at each year.
YEARS
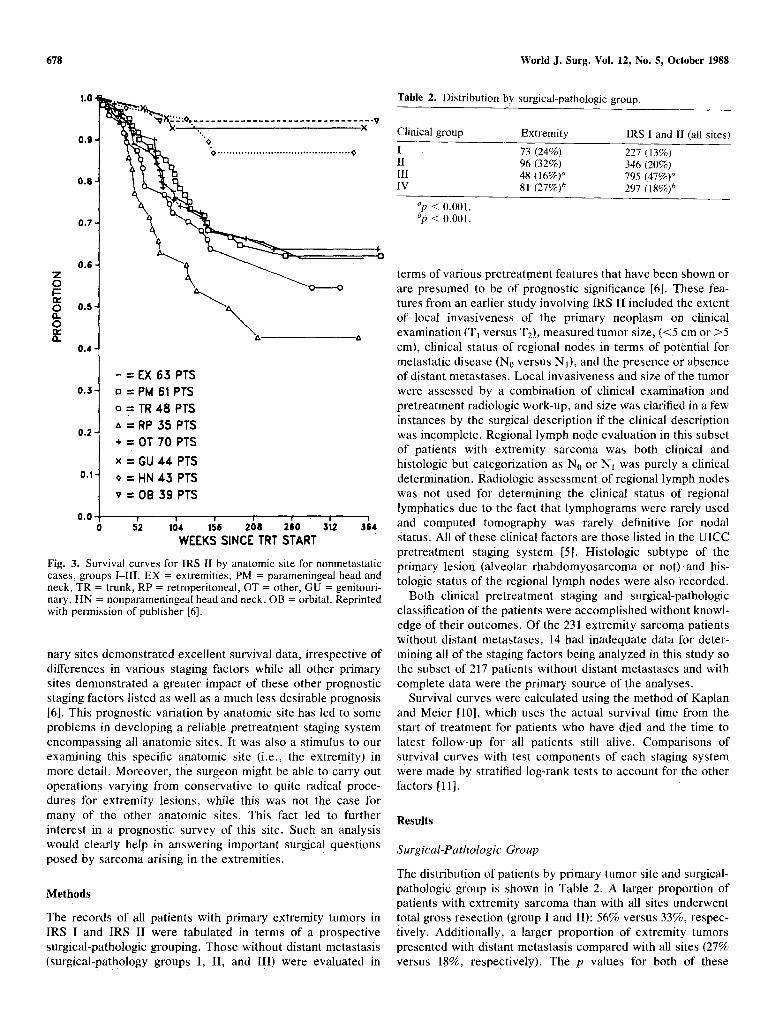
Fig. 2. Survival curves for all IRS I and II patients undergoing resec- tion (groups I and lI); comparison of survival among patients with and without proven regional lymphatic metastasis. O/E ratio = ob- served/expected ratio. Reprinted with permission of publisher [7].
The surgical-pathologic grouping process described above proved to be a good index of prognosis for the overall series of patients entered into IRS I and II as shown in Fig. I. The prognostic value of various pretreatment features in the UICC classification [5] was analyzed retrospectively on the overall series of nonmetastatic patients in IRS II prior to 1982 [6]. This showed the adverse prognostic significance of local invasive- hess of the neoplasm (T] = not invasive versus T2 : invasive), size (-<5 cm versus > 5 cm), and the presence or absence of distant metastases (MI versus M0). Clinical status of regional lymph nodes (No versus N1) showed only a prognostic trend in favor of No, but this difference was not significant in this study limited to nonmetastatic patients in IRS II. Proven histologic involvement of regional lymph nodes in patients without distant metastases in both IRS I and II did, however, prove to be a significant adverse factor (Fig. 2) [7]. The comparison of favorable versus unfavorable histologic subtypes, in terms of prognosis, showed no significant difference between the com- bination of alveolar rhabdomyosarcoma and unfavorable cyto- logic types (anaplastic, monomorphous), and all other his- tologic subtypes, despite ~ an unfavorable " t rend" [6]. There was earlier evidence from surgical-pathologic group I patients only that alveolar histology had a significant detrimental impact on prognosis [8] and a recent report on all 1982 patients registered in IRS I and II confirms this [9].
When survival curves were developed by anatomic site for all patients without distant metastasis in those series, there was a marked variation in prognosis that could not be attributed solely to the other pretreatment staging factors listed above (Fig. 3). Orbital, nonparameningeal head and neck, and the genitouri-
678 World J. Surg. Vol. 12, No. 5, October 1988
0.9 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ~
0,7
,
g o.s o
0 0.5 n. 0
0.4
- = FaX 6 3 PTS
o.z D = PM 61 PTS
o = TR 48 PTS
= RP 35 PTS 0.2
= OT 70 PTS
x = GU 44 PTS
0.1 o = HN 4~ PTS
v = OB 39 PTS
o.o 5'2 ' ' ; ' ' ' 0 104 158 2 8 260 312 ,364
WEEKS SINCE TRT START
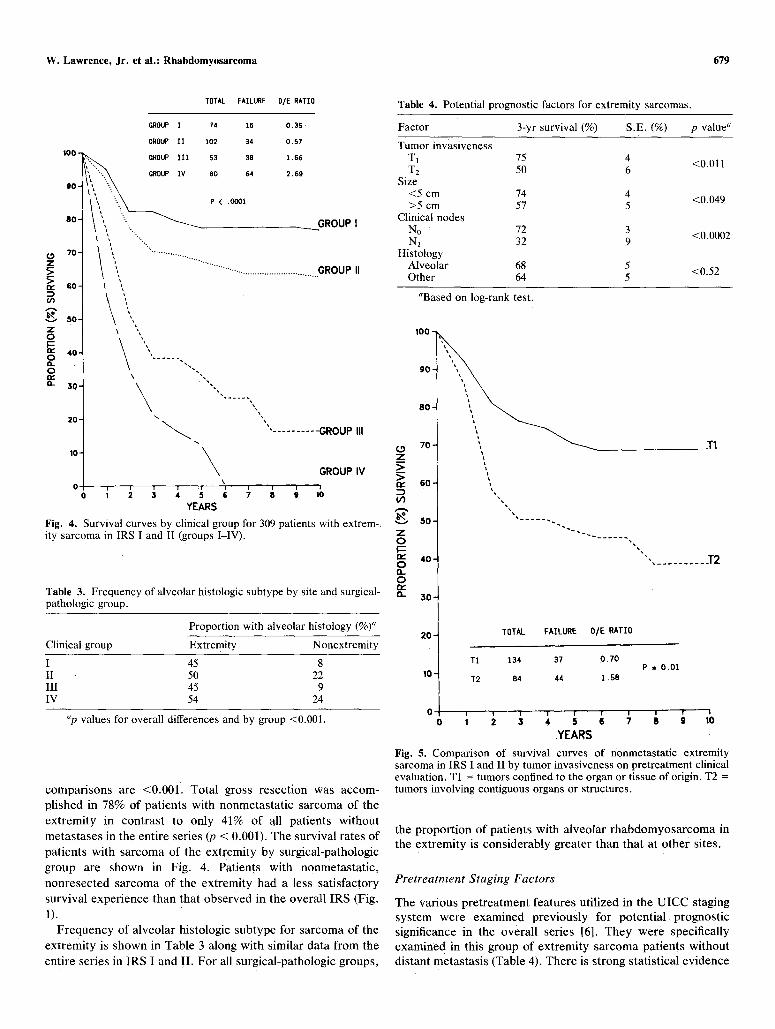
Fig. 3. Survival curves for IRS II by anatomic site for nonmetastatic cases, groups I-III. EX = extremities, PM = parameningeal head and neck, TR = trunk, RP = retroperitoneal, OT = other, GU = genitouri- nary, HN = nonparameningeal head and neck, OB = orbital. Reprinted with permission of publisher [6].
nary sites demonstrated excellent survival data, irrespective of differences in various staging factors while all other primary sites demonstrated a greater impact of these other prognostic staging factors listed as well as a much less desirable prognosis [6]. This prognostic variation by anatomic site has led to some problems in developing a reliable pretreatment staging system encompassing all anatomic sites. It was also a stimulus to our examining this specific anatomic site (i.e., the extremity) in more detail. Moreover, the surgeon might be able to carry out operations varying from conservative to quite radical proce- dures for extremity lesions, while this was not the case for many of the other anatomic sites. This fact led to further interest in a prognostic survey of this site. Such an analysis would clearly help in answering important surgical questions posed by sarcoma arising in the extremities.
Methods
The records of all patients with primary extremity tumors in IRS I and IRS II were tabulated in terms of a prospective surgical-pathologic grouping. Those without distant metastasis (surgical-pathology groups I, II, and I!I) were evaluated in
Table 2. Distribution by surgical-pathologic group.
Clinical group Extremity IRS I and II (all sites)
I 73 (24%) 227 (13%) II 96 (32%) 346 (20%) III 48 (16%) a 795 (47%) ~ IV 81 (27%) ~ 297 (18%) b
~p < 0.001. ~p < 0.001.
terms of various pretreatment features that have been shown or are presumed to be of prognostic significance [6]. These fea- tures from an earlier study involving 1RS I1 included the extent of local invasiveness of the primary neoplasm on clinical examination (T] versus T2), measured tumor size, (<5 cm or >5 cm), clinical status of regional nodes in terms of potential for metastatic disease (No versus N1), and the presence or absence of distant metastases. Local invasiveness and size of the tumor were assessed by a combination of clinical examination and pretreatment radiologic work-up, and size was clarified in a few instances by the surgical description if the clinical description was incomplete. Regional lymph node evaluation in this subset of patients with extremity sarcoma was both clinical and histologic but categorization as No or N~ was purely a clinical determination. Radiologic assessment of regional lymph nodes was not used for determining the clinical status of regional lymphatics due to the fact that lymphograms were rarely used and computed tomography was rarely definitive for nodal status. All of these clinical factors are those listed in the UICC pretreatment staging system [5]. Histologic subtype of the primary lesion (alveolar rhabdomyosarcoma or not) and his- tologic status of the regional lymph nodes were also recorded.
Both clinical pretreatment staging and surgical-pathologic classification of the patients were accomplished without knowl- edge of their outcomes. Of the 231 extremity sarcoma patients without distant metastases. 14 had inadequate data for deter- mining all of the staging factors being analyzed in this study so the subset of 217 patients without distant metastases and with complete data were the primary source of the analyses.
Survival curves were calculated using the method of Kaplan and Meier [10], which uses the actual survival time from the start of treatment for patients who have died and the time to latest follow-up for all patients still alive. Comparisons of survival curves with test components of each staging system were made by stratified log-rank tests to account for the other factors [11].
Results
Surgical-Pathologic Group
The distribution of patients by primary tumor site and surgical- pathologic group is shown in Table 2. A larger proportion of patients with extremity sarcoma than with all sites underwent total gross resection (group I and II): 56% versus 33%. respec- tively. Additionally, a larger proportion of extremity tumors presented with distant metastasis compared with all sites (27% versus 18%. respectively). The p values for both of these
W. Lawrence, Jr. et al.: Rhabdomyosarcoma 679
TOTAL FAILURE O/E RATIO
o z > > r 60-
O3
50- 7" o
I!~ 4 0 - o o
a_ 30-
GROUP I 74 16
GROUP ii 102 34
IO0-~>.. GROUP I I I 53 38
lb. ' ~ \
so-, \~ ", ~''.
7 0 - I ~ i
\',
\
20- "
10-
O- 1 r i r ' ; , 0 I 3 4 5 6
YEARS
0.35
0.57
1.66
2.69
GROUP I
. . . . . . . . . . . . . . . . . . . . . . . . . . . . .
.............................................. GROUP II
" . . . . . . . . . . GROUP lU
GROUP IV
'1 ; s ; .... ' I0
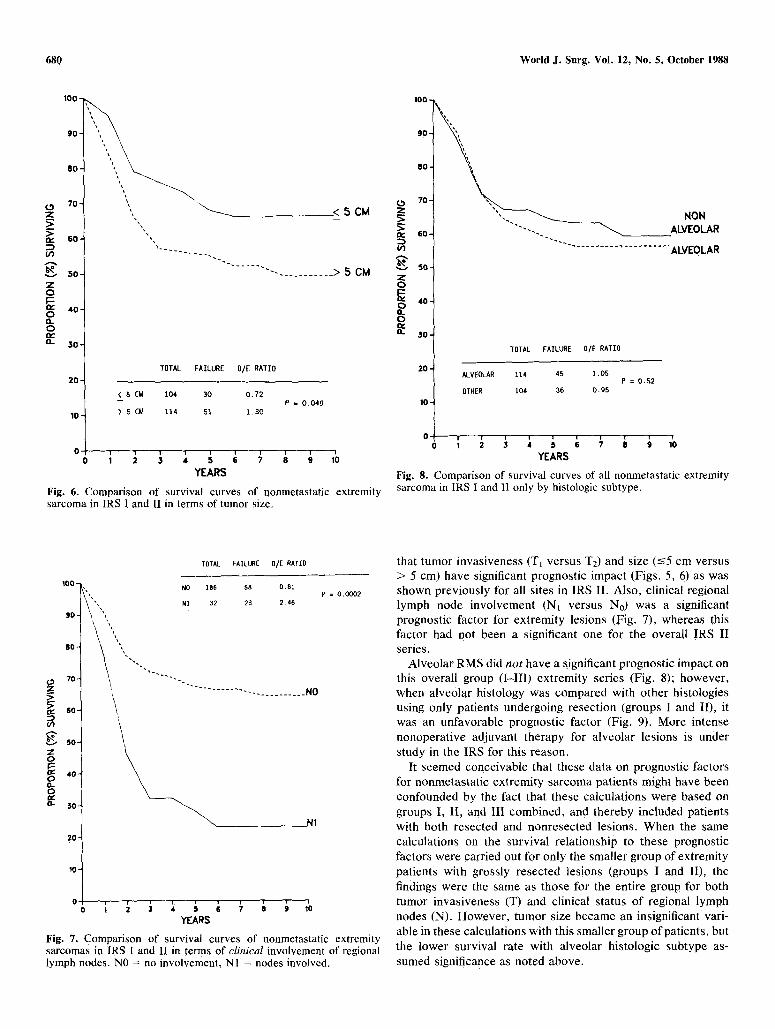
Fig. 4. Survival curves by clinical group for 309 patients with extrem-. ity sarcoma in IRS I and II (groups I-IV).
Table 3. Frequency of alveolar histologic subtype by site and surgical- pathologic group.
Proportion with alveolar histology (%)a
Clinical group Extremity Nonextremity
I 45 8 II 50 22 lII 45 9 IV 54 24
Up values for overall differences and by group <0.001.
comparisons are <0.001. Total gross resection was accom- plished in 78% of patients with nonmetastatic sarcoma of the
extremity in contrast to only 41% of all patients without
metastases in the entire series ~p < 0.001). The survival rates of
patients with sarcoma of the extremity by surgical-pathologic
group are shown in Fig. 4. Patients with nonmetastatic,
nonresected sarcoma of the extremity had a less satisfactory
survival experience than that observed in the overall IRS (Fig.
1). Frequency of alveolar histologic subtype for sarcoma of the
extremity is shown in Table 3 along with similar data from the
entire series in IRS I and II. For all surgical-pathologic groups,
Table 4. Potential prognostic factors for extremity sarcomas.
Factor 3-yr survival (%) S.E. (%) p value ~
Tumor invasiveness T1 75 4 <0.011 T2 50 6
Size <5 cm 74 4 <0.049 >5 cm 57 5
Clinical nodes No 72 3 <0.0002 N1 32 9
Histology Alveolar 68 5 <0.52 Other 64 5
r~ z
aBased on log-rank test.
s-%
V z o
o O_ o i,Y
1 0 0 ~
70- ~ i
6 0 -
5 0 -
40 -
30 -
20-
10-
.T1
", . . . . . . . . . . .T2
TOTAL FAILURE O/E RATIO
T1 134 37 0 .70 P = 0.01
T2 84 44 1.58
YEARS
Fig. 5. Comparison os survival curves o f nonmetastat ic ext remi ty sarcoma in IRS I and I I by tumor invasiveness on pretreatment cl inical evaluation. T1 = tumors confined to the organ or tissue of origin~ T2 = tumors involving contiguous organs or structures.
the proportion of patients with alveolar rhabdomyosarcoma in the extremity is considerably greater than that at other sites.
Pretreatment Staging Factors
The various pretreatment feature s utilized in the UICC staging sYstem were examined previously for potential prognostic significance in the overall series [6]. They were specifically examined in this group o f extremity sarcoma patients without distant metastasis (Table 4). There is strong statistical evidence
680 World J. Surg. Vol. 12, No. 5, October 1988
0 Z
I v 6 0 -
U')
5 0 - Z 0
4 0 . 0 0 . 0
n
80
70 ~"~ \
30-
20-
< 5 CM 104
1 0 - ) 5 s 114
0 r
~- - -__ < 5 CM
- - . . . . . . . . . . . > 5 CM
TOTAL FAILURE O/E RATIO
30 O, 72 P = 0.049
51 1.30
�9 F Y 4 5 6 7 8 9 1(}
YEARS
Fig. 6. Comparison of survival curves of nonmetastatic extremity sarcoma in IRS I and II in terms of tumor size.
Z
r v
O3
Z 0 n- O o.
0 m, o
100 -
9 0 -
8 0 -
70-
6 0 -
5 0 -
4 0 -
3 0 -
2 0 -
10-
O-
~,~~~ NON "'-. ~ ALVEOLAR
. . . . . . . . . . . . . . . . . . . . . . ALVEOLAR
TOTAL FAILURE O/E RATIO
ALVEOLAR 114 45 1.05 P = 0.52
OTHER 104 36 0.95
! ~ i- i i i 1' i , s , n s 7 ~ ; 10
YEARS
Fig. 8. Comparison of survival curves of all nonmetastatic extremity sarcoma in IRS I and 11 only by histologic subtype.
100 -
9 0 -
8 0 -
70-
60-
50-
0
OC) ~ 40- 0- o r,,, o.- 50-
20"
TOTAL FAILURE O/E RATIO
~ NO 186 88 0.81
" ' , N1 32 23 2.46
. . . . . . . . . . . . . NO
2
p=0.0002
0 " l "~ q- 1 0 ~ = ~ �9 ; 6 ~ ~ ~ ,b
YEARS
Fig. 7. Comparison of survival curves of nonmetastatic extremity sarcomas in IRS I and II in terms of clinical involvement of regional lymph nodes. NO = no involvement, NI = nodes involved.
that tumor invasiveness (T 1 versus T2) and size (-<5 cm versus > 5 cm) have significant prognostic impact (Figs. 5, 6) as was shown previously for all sites in IRS II. Also, clinical regional lymph node involvement (Nt versus No) was a significant prognostic factor for extremity lesions (Fig. 7), whereas this factor had not been a significant one for the overall !RS II series.
Alveolar RMS did n o t have a significant prognostic impact on this overall group ( I - l iD extremity series (Fig. 8); however, when alveolar histology was compared with other histologies using only patients undergoing resection (groups I and II), it was an unfavorable prognostic factor (Fig. 9). More intense nonoperative adjuvant therapy for alveolar lesions is under study in the IRS for this reason.
It seemed conceivable that these data on prognostic factors for nonmetastatic extremity sarcoma patients might have been confounded by the fact that these calculations were based on groups I, II, and III combined, and thereby included patients with both resected and nonresected lesions. When the same calculations on the survival relationship to these prognostic factors were carried out for only the smaller group of extremity patients with grossly resected lesions (groups I and II), the findings were the same as those for the entire group for both tumor invasiveness (T) and clinical status of regional lymph nodes (N). However, tumor size became an insignificant vari- able in these calculations with this smaller group of patients, but the lower survival rate with alveolar histologic subtype as- sumed significance as noted above,

W. Lawrence, Jr. et al.: Rhabdomyosarcoma 681
z >
~,- 6 0 -
Oq
v 5 0 -
Z O
r162 4 0 - O D- O ew
O_ 3 0 -
1OO-
gO - ~
8 0 - ~
i
7 0 - " . .
2 0 -
ALVEOLAR
I O - OTHER
0
NON ALVEOLAR
"" . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ALVEOLAR
TOTAL FAILURE OrE RATIO
94 33 1,26 P = 0,05
75 15 0.69
t t t i
YEARS
Fig. 9. Comparison of survival curves of grossly resected extremity sarcoma (groups I and lI only) in IRS and I and II by histologic subtype.
Total Gross Resection
The prognostic impact of total gross resection of extremity lesions versus incomplete resection and primary nonoperative treatment was shown in the survival curves using surgical- pathologic grouping (Fig. 4). Patients with extremity lesions in groups I and II (complete gross resection) had significantly better survival curves than those patients in group III (all patients with nonmetastatic sarcomas that were not resected). However, the latter group had both patients who appeared to be clearly unresectable on clinical grounds, by even radical resec- tion or amputation, and patients who were clinically resectable but not treated by resection due to either the resulting potential disability or the possibility of local control by nonoperative means. The records of the 55 patients in group III who did not undergo total gross resection were reviewed in order to distin- guish those patients in whom it might have been anatomically feasible to carry out a radical resection or amputation, but such a procedure was not done for one of the reasons listed above.
In 35 of the 55 patients it appeared that total gross resection of the sarcoma could have been accomplished if the surgical decision had been to do so. Twenty patients had lesions that seemed completely unsuitable for resection, even by amputa- tion. The 3-year survival data calculated for these 2 retrospec- tively classified groups of patients in group III are shown in Table 5 compared with survival data from the grossly resected group II patients. Although the group III patients considered potentially resectable in this retrospective evaluation had a superior 3-year survival compared to those that were consid- ered nonresectable: 48% versus 28% (p = 0.001), it was of
Table 5. Effect of resection and resectability on survival of patients with extremity sarcomas.
Clinical group No. of patients 3-yr survival (%)" S.E. (%)
Group 11 101 70 4.6 Group II1 55
Resectable 35 48 8.6 Nonresectable 20 28 10
Up value for group ll versus both resectable and nonresectable group III and resectable versus nonresectable group III is <0.001.
Table 6. Primary reexcision for microscopically involved surgical margin in extremity patients without lymphatic spread.
No. of Relapse Deaths Surgical margin patients (%) (%)
Clear at initial operation 56 17 (30%) 16 (29%) (group I)
Margin involved (group IIA) 73 26 (36%) 18 (25%)" Converted to clear margin by 22 5 (23%) 1 (5%) ~
reexcision (group IIA to group I)
"p = 0.04.
interest that these 3-year results for potentially resectable group III patients were clearly inferior to those for patients in group II (70%, p = 0.001). The range and median of tumor size was similar in these 2 groups. Also, the nonoperative therapy in IRS protocol was even more aggressive for the nonresected group than the resected one. This comparison was a retrospective nonrandomized one, but it does strongly suggest an overall survival benefit from carrying out total gross resection, if feasible, even if a "radical" operation with physical disability would be required.
Effect of Microscopic Involvement of Surgical Margins
A comparison was made of the disease-free survival and overall survival rates of patients with extremity sarcomas in group IIA (margin histologically positive) with those in whom a primary reexcision was accomplished to achieve a microscopically clear margin. This was part of a larger study by Hays et al. [12], which included patients with primary sarcomas both of the trunk and of the extremities. In Table 6 the data from this retrospective assessment of patients with extremity sarcomas only do demonstrate a slightly better local control rate and a much better survival rate in the group undergoing reoperation to achieve clear margins. However, those patients considered to have clear margins at the initial surgery had no better local control or survival rates than those patients with microscopic involvement of the margin but no secondary surgery (group IIA)!
Although these data demonstrate some disease control ben- efit from primary reexcision when the microscopic margins were found to be involved pathologically, they raise questions regarding the validity of pathologic data claiming clear margins in patients who were initially classified as group I in this series. These patients considered to have clear margins on initial pathologic study often had limited sections available from the originating institution for making this determination, suggesting that they may have been Group IIA patients after all.
682 World J. Surg. Vol. 12, No. 5, October 1988
100 . . . . ,
9 0 - "~ . (117)
6 0 "1 ~ " - ~ ~ (74) (62)
w 7~ ( 1 1 ) ~ . . . . " NEGATIVE NODES
z_ >__ > tw- 6O-
50- Z ~ ' ~ 8 } (6) (6) POSITIVE NODES 0
0 4 0 - TOTAL FAILURE D/E RATIO
0 FF 0-
30' POSITIVE NODES 22 11 2 . 1 8 p = .006
NEQATIVE NODES 159 38 O. B7 20-
, 10- Number in parenthesis indicates
number of pat, lents a[ ire at each year.
0 l i i l l i 1 2 3 4 5 6
YEARS
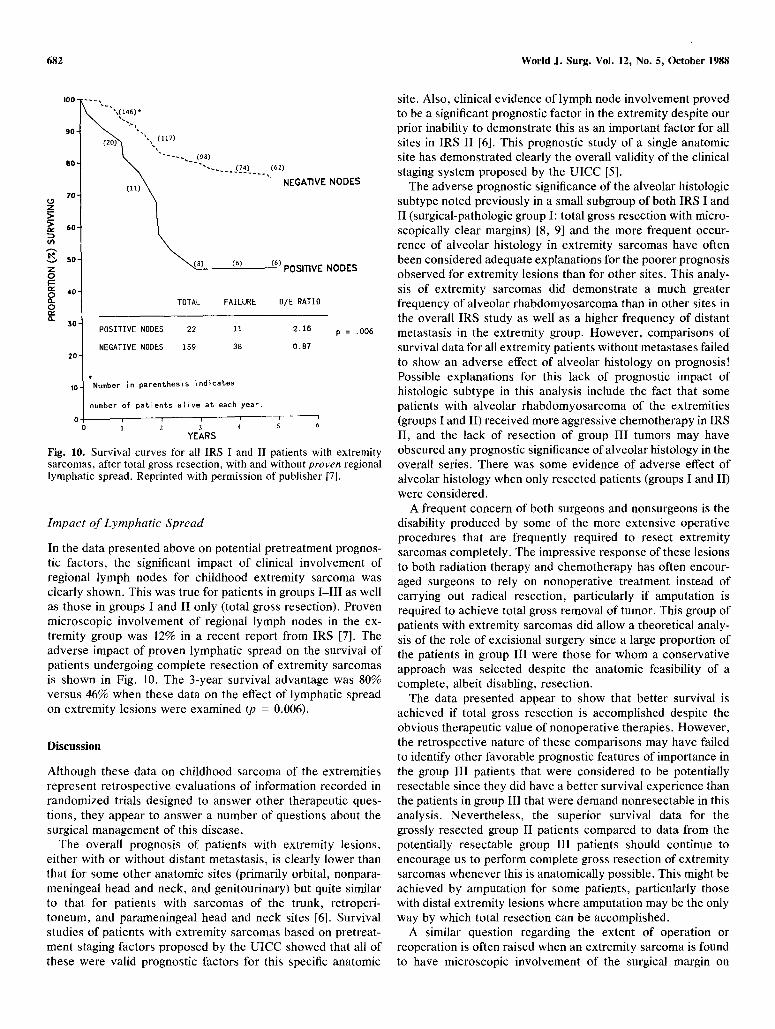
Fig. 10. Survival curves for all IRS I and II patients with extremity sarcomas, after total gross resection, with and without proven regional lymphatic spread. Reprinted with permission of publisher [7].
Impact of Lymphatic Spread
In the data presented above on potential pretreatment prognos- tic factors, the significant impact of clinical involvement of regional lymph nodes for childhood extremity sarcoma was clearly shown. This was true for patients in groups I - I I I as well as those in groups I and II only (total gross resection). Proven microscopic involvement of regional lymph nodes in the ex- tremity group was 12% in a recent report from IRS [7]. The adverse impact of proven lymphatic spread on the survival of patients undergoing complete resection of extremity sarcomas is shown in Fig. 10. The 3-year survival advantage was 80% versus 46% when these data on the effect of lymphatic spread on extremity lesions were examined (p = 0.006).
Discussion
Although these data on childhood sarcoma of the extremities represent retrospective evaluations of information recorded in randomized trials designed to answer other therapeutic ques- tions, they appear to answer a number of questions about the surgical management of this disease.
The overall prognosis of patients with extremity lesions, either with or without distant metastasis, is clearly lower than that for some other anatomic sites (primarily orbital, nonpara- meningeal head and neck, and genitourinary) but quite similar to that for patients with sarcomas of the trunk, retroperi- toneum, and parameningeal head and neck sites [6]. Survival studies of patients with extremity sarcomas based on pretreat- ment staging factors proposed by the UICC showed that all of these were valid prognostic factors for this specific anatomic
site. Also, clinical evidence of lymph node involvement proved to be a significant prognostic factor in the extremity despite our prior inability to demonstrate this as an important factor for all sites in IRS II [6]. This prognostic study of a single anatomic site has demonstrated clearly the overall validity of the clinical staging system proposed by the UICC [5].
The adverse prognostic significance of the alveolar histologic subtype noted previously in a small subgroup of both IRS I and II (surgical-pathologic group I: total gross resection with micro- scopically clear margins) [8, 9] and the more frequent occur- rence of alveolar histology in extremity sarcomas have often been considered adequate explanations for the poorer prognosis observed for extremity lesions than for other sites. This analy- sis of extremity sarcomas did demonstrate a much greater frequency of alveolar rhabdomyosarcoma than in other sites in the overall IRS study as well as a higher frequency of distant metastasis in the extremity group. However, comparisons of survival data for all extremity patients without metastases failed to show an adverse effect of alveolar histology on prognosis! Possible explanations for this lack of prognostic impact of histologic subtype in this analysis include the fact that some patients with alveolar rhabdomyosarcoma of the extremities (groups I and II) received more aggressive chemotherapy in IRS II, and the lack of resection of group III tumors may have obscured any prognostic significance of alveolar histology in the overall series. There was some evidence of adverse effect of alveolar histology when only resected patients (groups I and II) were considered.
A frequent concern of both surgeons and nonsurgeons is the disability produced by some of the more extensive operative procedures that are frequently required to resect extremity sarcomas completely. The impressive response of these lesions to both radiation therapy and chemotherapy has often encour- aged surgeons to rely on nonoperative treatment instead of carrying out radical resection, particularly if amputation is required to achieve total gross removal of tumor. This group of patients with extremity sarcomas did allow a theoretical analy- sis of the role of excisional surgery since a large proportion of the patients in group III were those for whom a conservative approach was selected despite the anatomic feasibility of a complete, albeit disabling, resection.
The data presented appear to show that better survival is achieved if total gross resection is accomplished despite the obvious therapeutic value of nonoperative therapies. However, the retrospective nature of these comparisons may have failed to identify other favorable prognostic features of importance in the group lII patients that were considered to be potentially resectable since they did have a better survival experience than the patients in group III that were demand nonresectable in this analysis. Nevertheless, the superior survival data for the grossly resected group II patients compared to data from the potentially resectable group III patients should continue to encourage us to perform complete gross resection of extremity sarcomas whenever this is anatomically possible. This might be achieved by amputation for some patients, particularly those with distal extremity lesions where amputation may be the only way by which total resection can be accomplished.
A similar question regarding the extent of operation or reoperation is often raised when an extremity sarcoma is found to have microscopic involvement of the surgical margin on

W. Lawrence, Jr. et al.: Rhabdomyosareoma 683
histologic study of the initial surgical specimen. Patients ini- tially found to have such microscopic involvement and then submitted to reoperation to achieve clear margins did have improved disease-free survival and survival over that observed in the group without reoperation. These were the findings observed in the combined study of trunk and extremity lesions reported by Hays et al. [12]. However, the finding that those patients with extremity sarcomas deemed to have clear margins initially (e.g., group I), had local treatment failure and survival data similar to those with microscopic involvement of the resection margin confuses these comparisons somewhat. Pos- sibly, this finding is an indication of the frequent unreliability of pathologic data from an initial resection prior to establishment of the true diagnosis. Whatever the reason, the overall data certainly suggest that secondary surgical resection to achieve convincingly clear margins is a reasonable approach to all extremity sarcomas, even if cursory pathologic study of the margins fails to reveal obvious involvement. This was a con- clusion similar to that reached by Giuliano and Eilber [13] in their study of adult soft tissue sarcomas.
The question of the importance of regional lymph node biopsy for extremity sarcomas was addressed by assessing the frequency of lymph node involvement and the impact of both clinical and histologic evidence of regional lymph node involve- ment on prognosis. The frequencies of clinical involvement and histologic involvement were relatively low but both findings indicated a reduced prognosis for this site. Despite the rela- tively low incidence of regional lymph node involvement ob- served, the knowledge of this route of spread, when it does occur, has a significant effect on treatment planning for these extremity lesions. It has been a general policy in the IRS to treat clinically enlarged regional lymph nodes in extremity sarcoma patients by dissection rather than by excisional biopsy only, but it is impossible to determine from these data whether lymph node dissection is essential if both adjuvant radiation therapy and chemotherapy are employed in the management program. However , knowledge of the presence or absence of regional lymphatic spread clearly affects decisions regarding the poten- tial need for including the primary site and the regional lymph node basin in a radiation portal. Those patients who have adequate resection margins around their primary sarcoma do not require radiation therapy if regional lymph nodes are not involved, as shown by the overall results of group I patients on IRS I [14]. Nevertheless, it is clear that either regional lymph node biopsy or dissection is an important procedure for patients with extremity sarcomas who do not present with distant metastasis, whether these lymph nodes are clinically enlarged or not.
As a result of this retrospective evaluation of extremity sarcoma patients entered into the IRS, some conclusions can be drawn regarding their surgical management:
1. Total gross resection of extremity sarcoma is an optimal therapeutic approach, whether microscopically clear margins can be achieved or not. This appears true, even if a radical and disabling resection is required, since survival data are better with this approach.
2. Those patients with a simple, unplanned excision of an extremity mass, that ultimately proves to be sarcoma, should probably have a formal planned reexcision of the
operative site to achieve truly adequate margins around the tumor site, whether the initial microscopic study of the margin of resection is said to be clear or not.
3. Regional lymph node spread of extremity sarcomas has an impact on prognosis as well as affecting some of the details of the management program. This appears to be ample justification for regional lymph node biopsy or dissection for all patients with extremity lesions despite a relatively low frequency of involvement.
4. Despite the proven value of nonoperative therapies for childhood sarcoma, vigorous and thorough surgical ap- proaches are required to achieve optimal end results with extremity lesions.
5. The potential benefit of reordering the various therapies now used in the multimodal management of extremity sarcomas cannot be assessed from these data. Surgery was always the initial treatment if resection was accom- plished. Use of an established pretreatment staging schema should allow assessment of preoperative adjuvant therapy in future clinical trials.
R6sum6
Grg~ce ~ l 'essai de I ' IRS (Intergroup Rhabdomyosarcome Study), les facteurs de pronostic intervenant dans la d6cision th6rapeutique ont 6t6 6tudi6s chez un grand nombre de patients ayant un rhabdomyosarcome des extr6mit6s. Deux 6tudes r6trospectives IRS I (1972-1978) et IRS II (1978-1984) compor- taient 217 patients ayant un sarcome des extr6mit6s sur 1,415 patients sans m6tastase ~t distance. I1 a 6t6 d6montr6 que: (a) la classification clinique UICC a une grande valeur, (b) la r6sec- tion compl6te des sarcomes des extr6mit6s repr6sente une approche th6rapeutique optimale malgr6 les effets positifs prouv6s des th6rapeutiques non op6ratoires, (c) les r6sultats sont am61ior6s par une nouvelle excision lorsque l 'histologie montre que la section n'6tait pas complete, on lorsque l ' intervention initiale ne visait que le diagnostic, (d) la biopsie ou le curage ganglionnaire est un geste important dans la planification et la conduite du traitement, et (e) une chirurgie active et compl6te est n6cessaire pour obtenir les meilleurs r6sultats pour les sarcomes des extr6mit6s malgr6 la valeur prouv6e des th6rapeutiques non op6ratoires.
Resumen
El vasto nt~mero de pacientes ingresado al Estudio Intergrupo sobre Rabdomiosarcoma (Intergroup Rhabdomyosarcoma Study, IRS) hace posible el amilisis de los factores de pron6stico y de toma de decisiones en cuanto a manejo clfnico para un lugar especifico de ubicaci6n del tumor primario: las extremidades. La revisi6n retrospectiva del IRS I (1972-1978) y del IRS II (1978-1984) incluy6 217 pacientes con sarcomas de las extremidades, entre 1,415 pacientes sin metfistasis distantes. Los datos sobre supervivencia libre de enfermedad y supervivencia global en este subgrupo de pacientes demostr6 que: (a) la clasificaci6n del estadio clfnico de la Uni6n Internacional contra el C~incer tiene clara validez, (b) la resec- ci6n total de los sarcomas de las extremidades constituye una modalidad terap6utica 6prima, a pesar de los beneficios probados de modalidades terap6uticas no operatorias, (c) los

684 World J. Surg. Vol, 12, No. 5, October 1988
resultados del tratamiento pueden set mejorados con la reoperacidn sobre el lugar de la resecci6n inicial si los mfirgenes aparecen histoldgicamente comprometidos o si la reseccion inicial rue un procedimiento simple no planeado que s61o se realiz6 para diagndstico, asf el estudio microscdpico inicial indique que los mgtrgenes estfin libres o rid, (d) la biopsia o la disecci6n ganglionar regional es un procedimiento de importancia tanto para la planeaci6n como para la ejecuci6n del programa terap6utico, y (e) se requieren vigorosos y completos procedimientos quirfirgicos para el logro de 6ptimos resultados finales en el tratamiento de ins sarcomas de las extremidades a pesar del valor probado de las terapias no operatorias.
References
1. Moore, O., Grossi, D.: Embryonal rhabdomyosarcoma of the head and neck. Cancer 12:69, 1959
2. Lawrence, W., Jr., Jegge, G., Foote, F.W.: Embryonal rhab- domyosarcoma, a clinicopathologic study. Cancer 17:361, 1964
3. Heyn, R.M., Holland, R., Newton, W.A., Tefft, M., Breslow, N., Hartmann, J.R.: The role of combined chemotherapy in the treat- ment of rbabdomyosarcoma in children. Cancer 34:2128, 1974
4. Maurer, H.M., Moon, T., Donaldson, M., Fernandez, C., Gehan, E.A., Hammond, D., Hays, D.M., Lawrence, W., Newton, W., Regab, A., Raney, B., Soule, E.H., Sutow, W.W., Tefft, M.: The Intergroup Rhabdomyosarcoma Study. A preliminary report. Can- cer 40:2015, 1977
5. Harmer, M.H., editor: TNM Classification of Pediatric Tumors, Geneva, UICC International Union Against Cancer, 1982
6. Lawrence, Jr., W., Gehan, E.A., Hays, D.M., Beltangady, M., Mamer, H.M. (For the IRS Committee): Prognostic significance of staging factors of the UICC staging system in childhood rhabdo-
myosarcoma: A report from the Intergroup Rhabdomyosarcoma Study (IRS-II). J. Clin. Oncol. 5:46, 1987
7. Lawrence, Jr., W., Hays, D.M., Heyn, R., Tefft, M., Crist, W., Beltangady, M., Newton, W., Wharam, M.: Lymphatic metastasis with childhood rhabdomyosarcoma sarcoma: A report from the Intergroup Rhabdomyosarcoma Study ORS). Cancer 60:910, 1987
8. Gehan, E.A., Glover, F.N., Maurer, H.M., Sutow, W.W., Hays, D.M., Lawrence, W., Newton, W., Soule, E.H. (For the IRS Committee): Prognostic factors in children with rhabdomyo- sarcoma. Natl. Cancer Inst. Monogr. 56:83, 1981
9. Newton, W.A., Soule, E.H., Hamoudi, A.B., Reiman, H., Shimada, H., Beltangady, M., Maurer, H.M. (For the IRS Com- mittee): Histopathology of childhood sarcomas, Intergroup Rhabdomyosarcoma Studies I & II: Clinicopathologic correlation. J. Clin. Oncol. 6:67, 1988
10. Kaplan, E.L., Meier, P.: Nonparametric estimation from incom- plete observations. J. Am. Stat. Assoc. 53:457, 1958
11. Peto, R., Pike, M.C., Armitage, P., Breslow, N.E., Cox, D.R., Howard, S.V., Mantel, N., McPherson, K., Peto, J., Smith, P.G.: Design and analysis of randomized clinical trials requiring pro- longed observation of each patient II analysis and examples. Br. J. Cancer 35:1, 1977
12. Hays, D.M., Beltangady, M., Lawrence, Jr., W., Wharam, M., Newton, W., Maurer, H.: Early secondary surgery (ESS) in patients with extremity-trunk primaries and microscopic residual (MR) following initial surgery: The Intergroup Rhabdomyosarcoma Study (IRS). (Abstract 852). Proc. Am. Soc. Clin. Oncol. 6:216, 1987
13. Giuliano, A.E., Eilber, F.R.: The rationale for planned reoperation after unplanned total soft tissue excision of soft tissue sarcoma. J. Clin. Oncol. 3:1344, 1985
14. Maurer, H.M., Beltangady, M., Gehan, E.A., Crist, W., Ham- mond, D., Hays, D.M., Heyn, R., Lawrence, W., Newton, W., Ortega, J., Ragab, A.H., Raney, R.B., Ruymann, F.B., Soule, E., Tefft, M., Webber, B., Wharam, M.D., Vietti, T.J.: The Intergroup Rhabdomyosarcoma Study--I: A final report. Cancer 6l:209, 1988
Invited Commentary
E. C a r m a c k Ho lmes , M.D.
Department of Surgery, Division of Oncology, UCLA School of Medicine, Los Angeles, California, U.S.A.
Lawrence and his group have made an important contribution to the understanding and the management of rhabdomyosar- coma of the extremities. They have clearly defined certain important principles, which include the importance of total gross and microscopic resection of the tumor, the importance of regional lymph node involvement, the importance of accurate staging, and the contribution of multimodality therapy. Most of
these principles have also been shown to be important in the treatment of other tumors such as osteosarcoma, Wilms' tumor, Ewing's tumor, and others. This article also points out the importance of the group approach to the study of malignancies, in particular those malignancies which are rare. The Intergroup rhabdomyosarcoma work represents a major contribution to the better understanding of the biology and treatment of this disease. Other major contributions have been provided by other groups such as the Wilms' Tumor Study Group, the Ewing's Tumor Study Group, and the Pediatric Oncology Group with their contribution to the understanding of the importance of surgical adjuvant therapy in osteosarcoma. The success of these groups, and others, clearly demonstrates the importance of multiinstitutional cooperative efforts.





























