Embed Size (px)
Citation preview
CLINICAL ARTICLEJ Neurosurg Pediatr 21:563–573, 2018
The presence of disease dissemination has been iden-tified as an adverse prognostic factor in several pe-diatric tumors of the CNS, and it presents specific
management challenges over and above isolated focal le-sions.1,2,4,7,8,10,12 It is unusual for pediatric CNS tumors to be disseminated at the time of initial clinical presentation, and dissemination at initial presentation has only previ-ously been reported in small series.5 The optimal surgical management of patients with disseminated CNS tumors is contentious in terms of both aggressiveness of tumor
resection and optimal strategy for CSF diversion. There is little evidence to guide the decision-making process in this regard.
The aim of the present study was to review our center’s surgical experience in treating children with CNS tumors disseminated at presentation, with a focus on the manage-ment of hydrocephalus. In addition, we collected data from patients with focal (i.e., nondisseminated) disease and used the combined data to review hydrocephalus management practices more generally in the pediatric CNS tumor popu-
ABBREVIATIONS ATRT = atypical teratoid rhabdoid tumor; ETV = endoscopic third ventriculostomy; EVD = external ventricular drain; GTR = gross-total resection; PNET = primitive neuroectodermal tumor; VP = ventriculoperitoneal; VPS = VP shunt.SUBMITTED August 12, 2017. ACCEPTED January 2, 2018.INCLUDE WHEN CITING Published online April 6, 2018; DOI: 10.3171/2018.1.PEDS17456.
Surgical decision-making in the management of childhood tumors of the CNS disseminated at presentationMatthew A. Kirkman, MEd, MRCS, Richard Hayward, FRCS, Kim Phipps, BSc, and Kristian Aquilina, MD, FRCS(SN)
Department of Neurosurgery, Great Ormond Street Hospital, London, United Kingdom
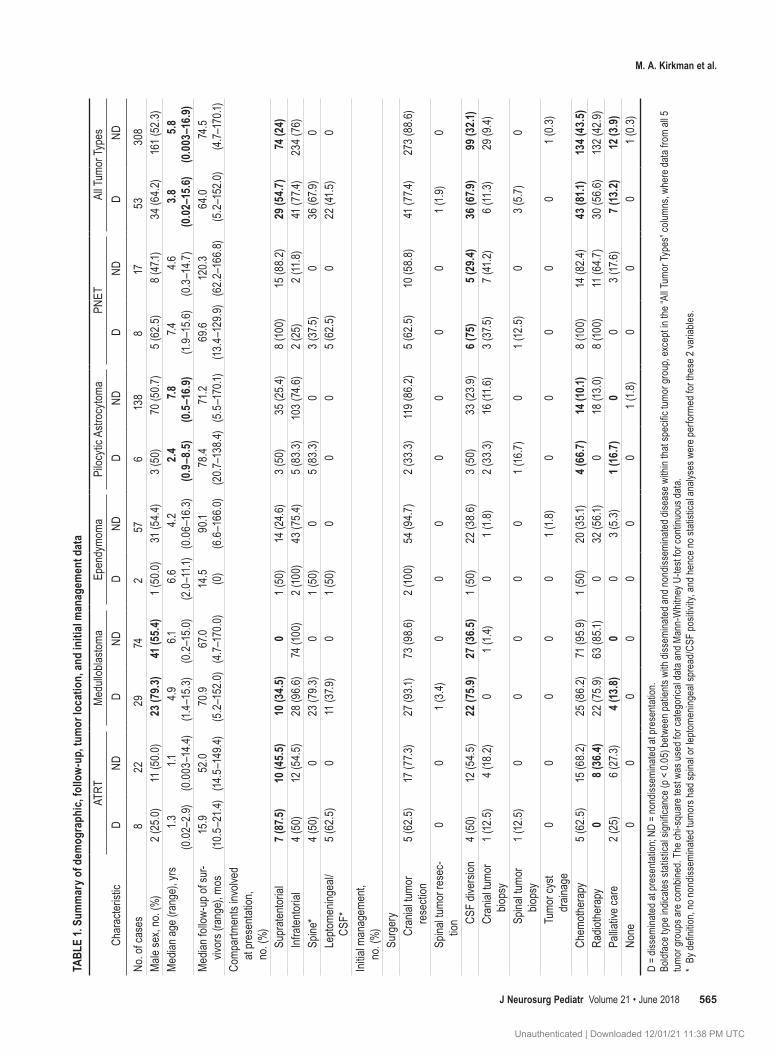
OBJECTIVE It is relatively unusual for pediatric CNS tumors to be disseminated at presentation, and the literature on the clinical features, management, and outcomes of this specific group is scarce. Surgical management in this popula-tion is often challenging, particularly in the presence of hydrocephalus. The authors present their recent experience of treating pediatric CNS tumors that were disseminated at presentation, and they compare these lesions with focal tumors.METHODS The authors performed a retrospective review of prospectively collected data on children presenting to a tertiary center between 2003 and 2016 inclusive.RESULTS Of 361 children with CNS tumors, the authors identified 53 patients with disease dissemination at presenta-tion (male/female ratio 34:19, median age 3.8 years, age range 7 days to 15.6 years) and 308 without dissemination at presentation (male/female ratio 161:147, median age 5.8 years, age range 1 day to 16.9 years). Five tumor groups were studied: medulloblastoma (disseminated n = 29, focal n = 74), other primitive neuroectodermal tumor (n = 8, n = 17), atypical teratoid rhabdoid tumor (n = 8, n = 22), pilocytic astrocytoma (n = 6, n = 138), and ependymoma (n = 2, n = 57). The median follow-up duration in survivors was not significantly different between those with disease dissemination at presentation (64.0 months, range 5.2–152.0 months) and those without it (74.5 months, range 4.7–170.1 months) (p > 0.05). When combining data from all 5 tumor groups, dissemination status at presentation was significantly associated with a higher risk of requiring CSF diversion, a higher surgical complication rate, and a reduced likelihood of achieving gross-total resection of the targeted lesion (all variables p < 0.05). Differences between the 5 tumor groups were evident. No factors that predicted the need for permanent CSF diversion following temporary external ventricular drainage were identified on multivariate analysis, and there was no clear superiority of either ventriculoperitoneal shunt surgery or en-doscopic third ventriculostomy as a permanent CSF diversion procedure.CONCLUSIONS Tumor type and dissemination status at initial presentation significantly affect outcomes across a range of measures. The management of hydrocephalus in patients with CNS tumors is challenging, and further prospec-tive studies are required to identify the optimal CSF diversion strategy in this population.https://thejns.org/doi/abs/10.3171/2018.1.PEDS17456KEYWORDS CSF diversion; disseminated CNS tumors; endoscopic third ventriculostomy; external ventricular drain; hydrocephalus; multidisciplinary treatment; ventriculoperitoneal shunt; surgery; oncology
J Neurosurg Pediatr Volume 21 • June 2018 563©AANS 2018, except where prohibited by US copyright law
Unauthenticated | Downloaded 12/01/21 11:38 PM UTC

M. A. Kirkman et al.
J Neurosurg Pediatr Volume 21 • June 2018564
lation. This allowed us to consider questions about factors influencing the conversion of external ventricular drainage to permanent CSF diversion and to compare the durability and efficacy of ventriculoperitoneal (VP) shunting to en-doscopic third ventriculostomy (ETV) in this setting.
MethodsStudy Population
Patients were identified for inclusion into this study through retrospective review of a prospectively recorded, dedicated neurooncology database. We identified all pa-tients, 0–18 years of age, with tissue diagnosis–confirmed CNS tumors treated at our tertiary pediatric neurosurgery center between January 1, 2003, and December 31, 2016, inclusive. We then searched this data set to identify pa-tients with tumors that had disease dissemination at pre-sentation. Dissemination was defined as the spread of tu-mor cells along CSF pathways, confirmed with the pres-ence of multiple (more than one) spatially distinct tumor masses located within, adjacent to, or in close proximity to a CSF space, with or without the presence of tumor cells in the CSF and/or leptomeningeal enhancement anywhere in the neural axis (i.e. brain and/or spine) on MRI. By this definition, if patients had a negative CSF cytological re-sult but a positive MRI scan, or vice versa, they were con-sidered to have disseminated disease for the purposes of this study. We excluded patients with high-grade gliomas because these tumors generally disseminate through the parenchyma rather than through the CSF. This resulted in a group of patients with 5 different tumor types: atypi-cal teratoid rhabdoid tumors (ATRTs), medulloblastomas, ependymomas, pilocytic astrocytomas, and primitive neu-roectodermal tumors (PNETs); we considered medullo-blastoma to be a distinct form of PNET in our analyses due to the relative frequency of the tumor relative to other PNETs and its accepted definition based on location. As a result, hereon the term PNET refers specifically to non-medulloblastoma PNETs. In part due to their anatomical location, optic pathway pilocytic astrocytomas present specific challenges, and features, that are distinct from those of other pilocytic astrocytomas; only optic pathway pilocytic astrocytomas treated surgically were included in this study. Where relevant, they are discussed as a specific group.
For a comparison population, we also collected the same data from patients who had focal disease at presen-tation and who harbored the same 5 tumor types.
Data CollectionThe following information was collected from the data-
base: age at diagnosis; sex; date of admission for surgery; tumor location(s); type(s) and date(s) of surgery/surgeries performed, including CSF diversion and revision proce-dures; surgical morbidities; adjuvant treatment (chemo-therapy, radiotherapy, both); palliative care; presence, tim-ing, and management of CNS and distant recurrence/dis-ease progression; and occurrence and timing of deaths. For the purpose of this study, “recurrence/disease progression” was defined as the development of new tumor in a new or previously treated site, or an increase in volume of exist-
ing tumor in a new or previously treated site. This applied equally to those with and without disseminated disease at presentation. We reviewed imaging studies, medical notes, and laboratory investigation reports of all identified pa-tients to confirm these details. The radiology reports were reviewed, along with the original imaging studies, by one of the authors (M.A.K.), who was blinded to the clinical information of the patient at the time of imaging review. Original pathology reports for all patients were reviewed to confirm the histological diagnosis. As standard of care, all patients underwent MRI of the entire neural axis at presentation to allow disease staging. All patients had the following studies performed as a minimum. Imaging of the head included T1-weighted axial and sagittal precon-trast; T1-weighted axial and coronal postcontrast; and T2-weighted axial, coronal FLAIR, axial diffusion-weighted, and susceptibility-weighted axial images. Imaging of the spine included T1-weighted sagittal pre- and postcontrast images, with axial images acquired if abnormalities were detected on the sagittal scan. Some but not all patients had CSF samples acquired during the course of their admis-sion; there were no specific criteria for this, and there were differences in the timing and method of collection (e.g., via lumbar puncture or at the time of surgery for ventricu-lostomy).
The classification of pediatric CNS tumors changed over the study period; detailed molecular subtyping of tu-mors, particularly medulloblastomas, was not available for the patients treated earlier in the series and has therefore not been included in this study.
Statistical AnalysisAll data were analyzed using SPSS Statistics version
24.0 (IBM). Data are presented for the individual tumor groups and for the 5 tumor groups combined. To compare frequencies of categorical data, we used chi-square tests, and to compare continuous data, we used the nonparamet-ric Mann-Whitney U-tests. Binary logistic regression anal-yses were performed to evaluate risk factors for conversion of temporary external ventricular drainage to permanent CSF diversion. Survival analyses were performed using Kaplan-Meier analysis initially, followed by Cox regres-sion controlling for selected variables.
For the purposes of statistical analyses, a variable named “tumor type/dissemination status” was created and consists of 10 groups of patients—namely, the 5 tu-mor types each with a subcategory of either disseminated or nondisseminated (focal) at presentation. The reference category for this variable was nondisseminated pilocytic astrocytoma. A p value of < 0.05 was considered statisti-cally significant.
ResultsOverall, between 2003 and 2016, 1385 patients with
CNS tumors were treated at our center (including those with isolated spinal tumors). Across the 5 tumor groups of interest in this study, 361 patients were identified: 30 with ATRTs, 103 with medulloblastomas, 59 with epen-dymomas, 144 with pilocytic astrocytomas, and 25 with PNETs. Table 1 provides an overview of the demograph-ic features of our cohort. Of the pilocytic astrocytomas,
Unauthenticated | Downloaded 12/01/21 11:38 PM UTC
J Neurosurg Pediatr Volume 21 • June 2018 565
M. A. Kirkman et al.TA
BLE
1. Su
mm
ary o
f dem
ogra
phic
, fol
low-
up, t
umor
loca
tion,
and
initi
al m
anag
emen
t dat
a
Char
acter
istic
ATRT
Med
ullob
lastom
aEp
endy
moma
Piloc
ytic A
stroc
ytoma
PNET
All T
umor
Type
sD
NDD
NDD
NDD
NDD
NDD
ND
No. o
f cas
es8
2229
742
576
138
817
5330
8M
ale se
x, no
. (%)
2 (25
.0)11
(50.0
)23
(79.3
)41
(55.
4)1 (
50.0)
31 (5
4.4)
3 (50
)70
(50.7
)5 (
62.5
)8 (
47.1)
34 (6
4.2)
161 (
52.3)
Med
ian ag
e (ra
nge),
yrs
1.3
(0.0
2–2.
9)1.1
(0
.003
–14.4
)4.9
(1.
4–15
.3)6.1
(0
.2–1
5.0)
6.6
(2.0
–11.1
)4.
2 (0
.06–
16.3)
2.4
(0.9
–8.5)
7.8
(0.5
–16.
9)7.4
(1.
9–15
.6)4.6
(0
.3–1
4.7)
3.8
(0.02
–15.6
)5.
8 (0
.003
–16.
9)M
edian
follo
w-up
of su
r-viv
ors (
rang
e), m
os15
.9 (10
.5–2
1.4)
52.0
(14.5
–149
.4)70
.9 (5
.2–1
52.0)
67.0
(4.7–
170.0
)14
.5
(0)
90.1
(6.6
–166
.0)78
.4 (2
0.7–1
38.4)
71.2
(5
.5–1
70.1)
69.6
(13.4
–129
.9)12
0.3
(62.
2–16
6.8)
64.0
(5.2
–152
.0) 7
4.5
(4.7–
170.1
)Co
mpar
tmen
ts inv
olved
at
pres
enta
tion,
no. (
%)
Su
prate
ntoria
l7 (
87.5)
10 (4
5.5)
10 (3
4.5)
01 (
50)
14 (2
4.6)
3 (50
)35
(25.4
)8 (
100)
15 (8
8.2)
29 (5
4.7)
74 (2
4)
Inf
raten
torial
4 (50
)12
(54.5
)28
(96.
6)74
(100
)2 (
100)
43 (7
5.4)
5 (83
.3)10
3 (74
.6)2 (
25)
2 (11
.8)41
(77.4
)23
4 (76
)
Sp
ine*
4 (50
)0
23 (7
9.3)
01 (
50)
05 (
83.3)
03 (
37.5
)0
36 (6
7.9)
0
Le
ptome
ninge
al/CS
F*5 (
62.5
)0
11 (3
7.9)
01 (
50)
00
05 (
62.5
)0
22 (4
1.5)
0
Initia
l man
agem
ent,
no. (
%)
Su
rger
y
Cran
ial tu
mor
rese
ction
5 (62
.5)
17 (7
7.3)
27 (9
3.1)
73 (9
8.6)
2 (10
0)54
(94.7
)2 (
33.3)
119 (
86.2)
5 (62
.5)
10 (5
8.8)
41 (7
7.4)
273 (
88.6)
Spina
l tumo
r res
ec-
tion
00
1 (3.
4)0
00
00
00
1 (1.9
)0
CSF
diver
sion
4 (50
)12
(54.5
)22
(75.
9)27
(36.
5)1 (
50)
22 (3
8.6)
3 (50
)33
(23.
9)6 (
75)
5 (29
.4)36
(67.9
)99
(32.1
)
Cr
anial
tumo
r bio
psy
1 (12
.5)
4 (18
.2)0
1 (1.4
)0
1 (1.8
)2 (
33.3)
16 (1
1.6)
3 (37
.5)
7 (41
.2)6 (
11.3)
29 (9
.4)
Spina
l tumo
r bio
psy
1 (12
.5)
00
00
01 (
16.7)
01 (
12.5
)0
3 (5.7
)0
Tumo
r cys
t dr
ainag
e0
00
00
1 (1.8
)0
00
00
1 (0.
3)
Chem
other
apy
5 (62
.5)
15 (6
8.2)
25 (8
6.2)
71 (9
5.9)
1 (50
)20
(35.1
)4 (
66.7)
14 (1
0.1)
8 (10
0)14
(82.4
)43
(81.1
)13
4 (43
.5)
Ra
dioth
erap
y0
8 (36
.4)22
(75.
9)63
(85.1
)0
32 (5
6.1)
018
(13.
0)8 (
100)
11 (6
4.7)
30 (5
6.6)
132 (
42.9)
Pallia
tive c
are
2 (25
)6 (
27.3)
4 (13
.8)0
03 (
5.3)
1 (16
.7)0
03 (
17.6)
7 (13
.2)12
(3.9)
None
00
00
00
01 (
1.8)
00
01 (
0.3)
D =
disse
mina
ted a
t pre
sent
ation
; ND
= no
ndiss
emina
ted a
t pre
sent
ation
.Bo
ldfac
e typ
e ind
icate
s sta
tistic
al sig
nifica
nce (
p < 0.
05) b
etwe
en pa
tient
s with
diss
emina
ted a
nd no
ndiss
emina
ted d
iseas
e with
in th
at sp
ecific
tum
or gr
oup,
exce
pt in
the “
All T
umor
Type
s” co
lumns
, whe
re da
ta fr
om al
l 5
tum
or gr
oups
are c
ombin
ed. T
he ch
i-squ
are t
est w
as us
ed fo
r cate
goric
al da
ta an
d Man
n-W
hitne
y U-te
st fo
r con
tinuo
us da
ta.
* By
defin
ition,
no no
ndiss
emina
ted t
umor
s had
spina
l or le
ptome
ninge
al sp
read
/CSF
pos
itivity
, and
henc
e no s
tatis
tical
analy
ses w
ere p
erfo
rmed
for t
hese
2 va
riable
s.
Unauthenticated | Downloaded 12/01/21 11:38 PM UTC

M. A. Kirkman et al.
J Neurosurg Pediatr Volume 21 • June 2018566
11 (7.6%) were optic pathway lesions. Overall, 53 tumors (14.7%) were disseminated at presentation. The proportion of patients with disease dissemination at presentation was highest for PNET (n = 8 [32%]), medulloblastoma (n = 29 [28.2%]), and ATRT (n = 8 [26.7%]), and it was lowest for ependymoma (n = 2 [3.4%]) and pilocytic astrocytoma (n = 6 [4.2%]). Only one of the 11 patients with optic pathway pilocytic astrocytomas requiring surgical management had disseminated disease at presentation. There was no significant difference in follow-up durations for survivors with disseminated versus nondisseminated disease at pre-sentation (Table 1).
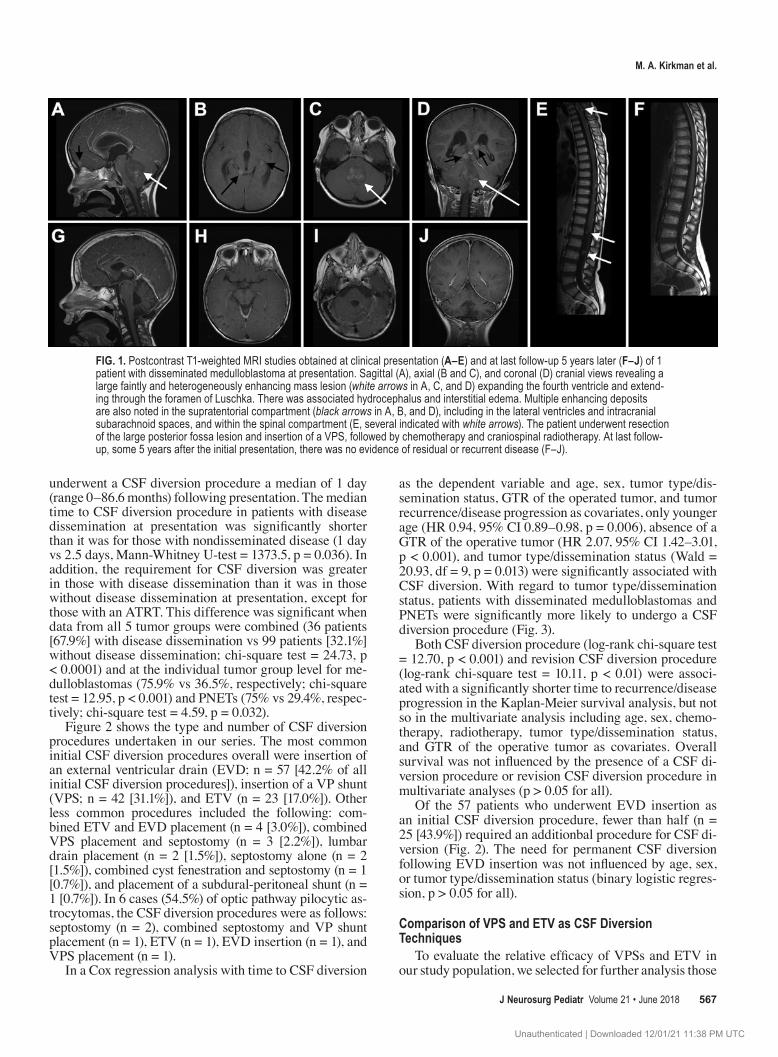
Tumor LocationThe majority of tumors in the disseminated and nondis-
seminated groups were infratentorial (n = 41 [77.4%] and n = 234 [76%], respectively). In the nondisseminated group, the remainder (n = 74, 24%) were supratentorial. In the disseminated group, the majority also had spinal (n = 36, 67.9%) and/or supratentorial (n = 29, 54.7%) tumors (Fig. 1). In total, 72 patients (19.9%) had CSF samples taken for cytology prior to or at the time of initial surgery. Thirteen patients (24.5%) with disease dissemination at presenta-tion had MRI evidence of tumor burden in all 3 CNS com-partments (supratentorial, infratentorial, and spinal), and 22 (41.5%) had tumor cells in their CSF.
Initial ManagementAll patients with disseminated and nondisseminated
ATRTs, medulloblastomas, ependymomas, PNETs, and pilocytic astrocytomas (except those involving the optic pathway) underwent surgery at the time of initial presen-tation (Table 1). Of the 11 patients with optic pathway pilocytic astrocytomas, 4 patients (1 with disseminated disease and 3 without) did not undergo surgery at initial presentation. In these 4 cases, 3 were scheduled to receive chemotherapy alone as a first-line treatment. In the other case, the patient was a 5-year-old girl with nondissemi-nated disease for whom management was entirely conser-vative at presentation; 7 years after the lesion was identi-fied, a biopsy was performed due to increasing size of the lesion, and this was followed by CSF diversion.
Rates of chemotherapy administration between dis-seminated and nondisseminated tumor groups were simi-lar among all tumor types (Table 1), except for pilocytic astrocytomas, for which, as expected, significantly more patients with disease dissemination at presentation re-ceived chemotherapy (n = 4 [66.7%] vs n = 14 [10.1%]; chi-square test = 16.80, p < 0.0001). Of the 2 patients with disseminated pilocytic astrocytomas who did not receive chemotherapy initially, one presented in extremis and was referred for palliative care, and the other had the optic pathway pilocytic astrocytoma described above that was managed completely conservatively at initial presentation. Administration of radiotherapy at diagnosis varied by tu-mor group, age, and dissemination status, in accordance with established treatment protocols for each tumor. Re-ferral to palliative care was not a frequent initial manage-ment strategy but was more common in patients with dis-ease dissemination at presentation compared to those with
focal disease across all 5 tumor groups (n = 7 [13.2%] vs n = 12 [3.9%], respectively; chi-square test = 7.86, p = 0.005).
Surgical ManagementCranial tumor resection was the most common proce-
dure performed for all tumor types, irrespective of dissemi-nation status at presentation (Table 1). Overall rates of cra-nial tumor biopsy across the 5 tumor groups were similar in the disseminated (11.3%) and nondisseminated (9.4%) groups, although at the individual tumor level almost all patients with medulloblastomas and ependymomas under-went cranial tumor resection, with only 1 patient from each of these 2 tumor groups initially managed with cranial tu-mor biopsy. The child with a medulloblastoma in whom a tumor biopsy was initially performed had focal disease and presented with loss of consciousness secondary to in-tratumoral hemorrhage; he underwent urgent surgery for evacuation of the hematoma, at which point the tumor was biopsied. The patient died the day after surgery. In the case of the child with an ependymoma who underwent initial tumor biopsy, the patient had focal disease and presented with hydrocephalus, and the child proceeded to undergo ETV and biopsy prior to resection. Of the 11 optic pathway pilocytic astrocytomas in this series, 7 (63.6%) were par-tially resected (including the disseminated optic pathway pilocytic astrocytoma) and 4 (36.4%) were biopsied.
Other tumor procedures were performed less com-monly. In 1 case of spinal tumor resection for dissemi-nated medulloblastoma the patient presented with cord compression at T10–11. Of note, this was the only patient in our cohort who presented with cord compression. A pa-tient with focal disease had a large supratentorial cystic ependymoma that was drained through an Ommaya reser-voir inserted prior to craniotomy for resection the follow-ing day, and, in 1 case each, a patient with a disseminated ATRT and a disseminated pilocytic astrocytoma under-went spinal tumor biopsy at presentation.
In evaluating whether dissemination status at pre-sentation influenced the extent of tumor resection of the targeted lesion, we found that patients with disease dis-semination at presentation were significantly less likely to have gross-total resection (GTR) of the operative lesion (14 [26.4%] of 53 cases) than were those without disease dissemination at presentation (178 [57.8%] of 308; chi-square test = 17.88, p < 0.0001). At the individual tumor group level, this difference remained significant only for medulloblastomas (disseminated: GTR in 9 [31%] of 29 cases; nondisseminated: GTR in 53 [71.6%] of 74 cases; chi-square test = 14.32, p < 0.001). Lack of GTR of the op-erative tumor was significantly associated with time to re-currence/disease progression (HR 1.77, 95% CI 1.19–2.64, p < 0.01) in a Cox regression analysis with the additional covariates of age, sex, chemotherapy, radiotherapy, CSF diversion status, revision CSF diversion procedure, and tu-mor type/dissemination status. However, in a separate Cox regression analysis, lack of GTR of the operative tumor did not influence overall survival (p > 0.05).
Hydrocephalus ManagementIn total, 135 patients (37.4%) in our study population
Unauthenticated | Downloaded 12/01/21 11:38 PM UTC
J Neurosurg Pediatr Volume 21 • June 2018 567
M. A. Kirkman et al.
underwent a CSF diversion procedure a median of 1 day (range 0–86.6 months) following presentation. The median time to CSF diversion procedure in patients with disease dissemination at presentation was significantly shorter than it was for those with nondisseminated disease (1 day vs 2.5 days, Mann-Whitney U-test = 1373.5, p = 0.036). In addition, the requirement for CSF diversion was greater in those with disease dissemination than it was in those without disease dissemination at presentation, except for those with an ATRT. This difference was significant when data from all 5 tumor groups were combined (36 patients [67.9%] with disease dissemination vs 99 patients [32.1%] without disease dissemination; chi-square test = 24.73, p < 0.0001) and at the individual tumor group level for me-dulloblastomas (75.9% vs 36.5%, respectively; chi-square test = 12.95, p < 0.001) and PNETs (75% vs 29.4%, respec-tively; chi-square test = 4.59, p = 0.032).
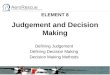
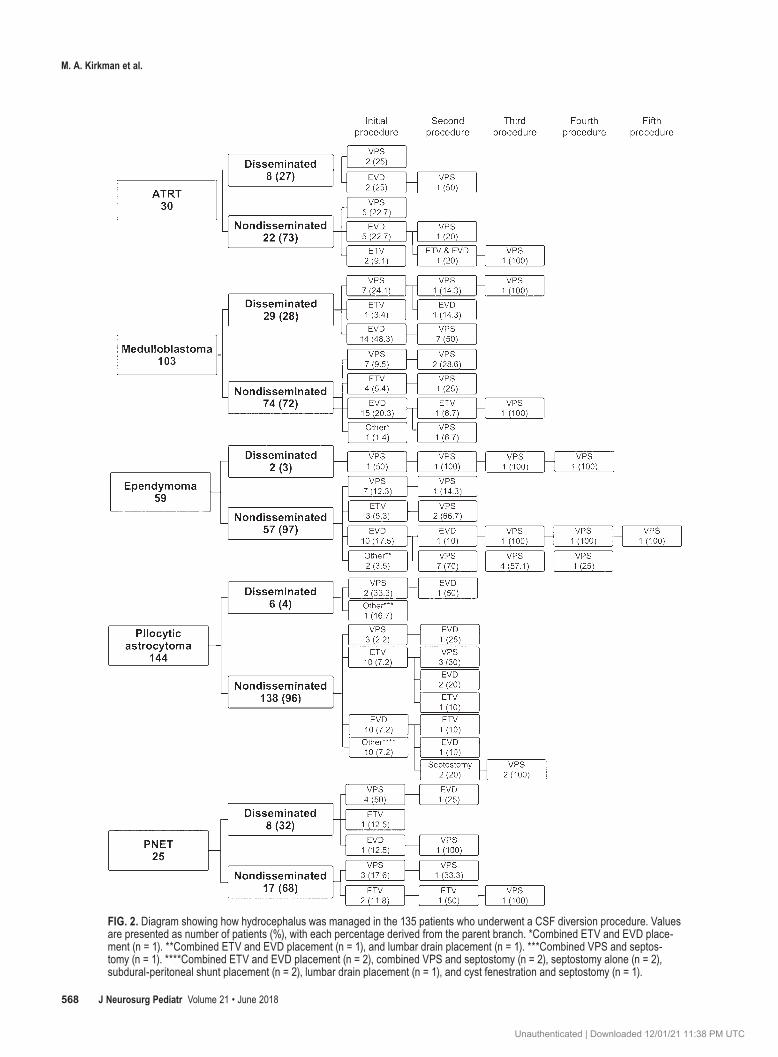
Figure 2 shows the type and number of CSF diversion procedures undertaken in our series. The most common initial CSF diversion procedures overall were insertion of an external ventricular drain (EVD; n = 57 [42.2% of all initial CSF diversion procedures]), insertion of a VP shunt (VPS; n = 42 [31.1%]), and ETV (n = 23 [17.0%]). Other less common procedures included the following: com-bined ETV and EVD placement (n = 4 [3.0%]), combined VPS placement and septostomy (n = 3 [2.2%]), lumbar drain placement (n = 2 [1.5%]), septostomy alone (n = 2 [1.5%]), combined cyst fenestration and septostomy (n = 1 [0.7%]), and placement of a subdural-peritoneal shunt (n = 1 [0.7%]). In 6 cases (54.5%) of optic pathway pilocytic as-trocytomas, the CSF diversion procedures were as follows: septostomy (n = 2), combined septostomy and VP shunt placement (n = 1), ETV (n = 1), EVD insertion (n = 1), and VPS placement (n = 1).
In a Cox regression analysis with time to CSF diversion
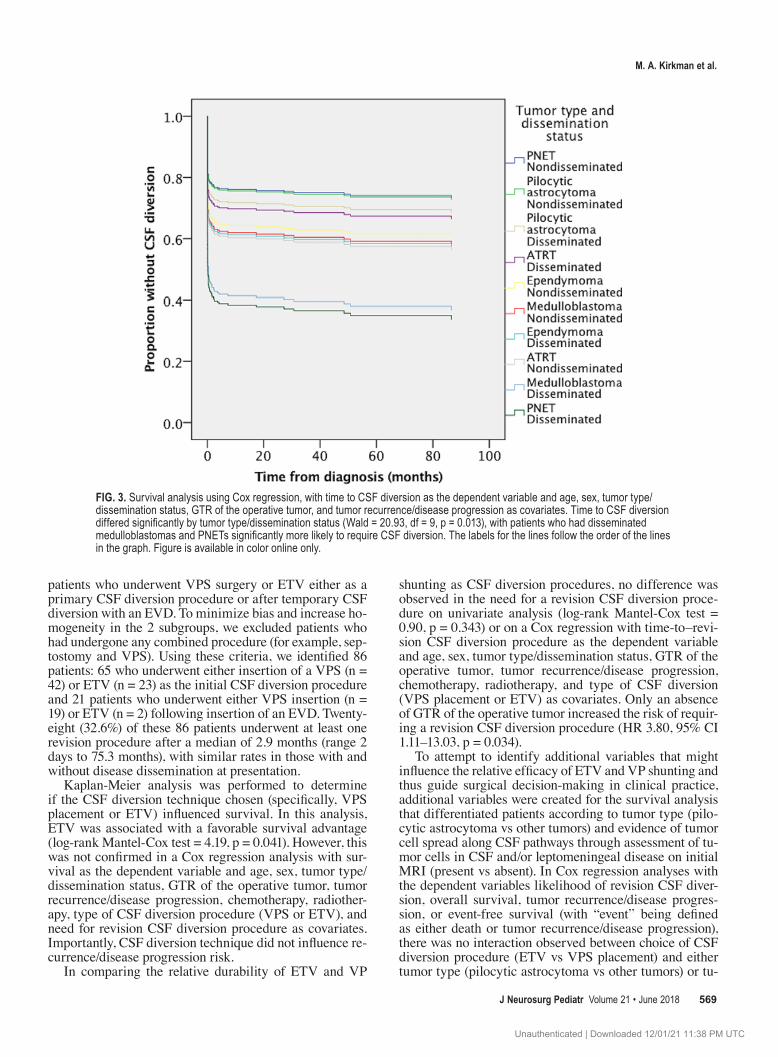
as the dependent variable and age, sex, tumor type/dis-semination status, GTR of the operated tumor, and tumor recurrence/disease progression as covariates, only younger age (HR 0.94, 95% CI 0.89–0.98, p = 0.006), absence of a GTR of the operative tumor (HR 2.07, 95% CI 1.42–3.01, p < 0.001), and tumor type/dissemination status (Wald = 20.93, df = 9, p = 0.013) were significantly associated with CSF diversion. With regard to tumor type/dissemination status, patients with disseminated medulloblastomas and PNETs were significantly more likely to undergo a CSF diversion procedure (Fig. 3).
Both CSF diversion procedure (log-rank chi-square test = 12.70, p < 0.001) and revision CSF diversion procedure (log-rank chi-square test = 10.11, p < 0.01) were associ-ated with a significantly shorter time to recurrence/disease progression in the Kaplan-Meier survival analysis, but not so in the multivariate analysis including age, sex, chemo-therapy, radiotherapy, tumor type/dissemination status, and GTR of the operative tumor as covariates. Overall survival was not influenced by the presence of a CSF di-version procedure or revision CSF diversion procedure in multivariate analyses (p > 0.05 for all).
Of the 57 patients who underwent EVD insertion as an initial CSF diversion procedure, fewer than half (n = 25 [43.9%]) required an additionbal procedure for CSF di-version (Fig. 2). The need for permanent CSF diversion following EVD insertion was not influenced by age, sex, or tumor type/dissemination status (binary logistic regres-sion, p > 0.05 for all).
Comparison of VPS and ETV as CSF Diversion Techniques
To evaluate the relative efficacy of VPSs and ETV in our study population, we selected for further analysis those
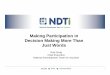
FIG. 1. Postcontrast T1-weighted MRI studies obtained at clinical presentation (A–E) and at last follow-up 5 years later (F–J) of 1 patient with disseminated medulloblastoma at presentation. Sagittal (A), axial (B and C), and coronal (D) cranial views revealing a large faintly and heterogeneously enhancing mass lesion (white arrows in A, C, and D) expanding the fourth ventricle and extend-ing through the foramen of Luschka. There was associated hydrocephalus and interstitial edema. Multiple enhancing deposits are also noted in the supratentorial compartment (black arrows in A, B, and D), including in the lateral ventricles and intracranial subarachnoid spaces, and within the spinal compartment (E, several indicated with white arrows). The patient underwent resection of the large posterior fossa lesion and insertion of a VPS, followed by chemotherapy and craniospinal radiotherapy. At last follow-up, some 5 years after the initial presentation, there was no evidence of residual or recurrent disease (F–J).
Unauthenticated | Downloaded 12/01/21 11:38 PM UTC
M. A. Kirkman et al.
J Neurosurg Pediatr Volume 21 • June 2018568
FIG. 2. Diagram showing how hydrocephalus was managed in the 135 patients who underwent a CSF diversion procedure. Values are presented as number of patients (%), with each percentage derived from the parent branch. *Combined ETV and EVD place-ment (n = 1). **Combined ETV and EVD placement (n = 1), and lumbar drain placement (n = 1). ***Combined VPS and septos-tomy (n = 1). ****Combined ETV and EVD placement (n = 2), combined VPS and septostomy (n = 2), septostomy alone (n = 2), subdural-peritoneal shunt placement (n = 2), lumbar drain placement (n = 1), and cyst fenestration and septostomy (n = 1).
Unauthenticated | Downloaded 12/01/21 11:38 PM UTC
J Neurosurg Pediatr Volume 21 • June 2018 569
M. A. Kirkman et al.
patients who underwent VPS surgery or ETV either as a primary CSF diversion procedure or after temporary CSF diversion with an EVD. To minimize bias and increase ho-mogeneity in the 2 subgroups, we excluded patients who had undergone any combined procedure (for example, sep-tostomy and VPS). Using these criteria, we identified 86 patients: 65 who underwent either insertion of a VPS (n = 42) or ETV (n = 23) as the initial CSF diversion procedure and 21 patients who underwent either VPS insertion (n = 19) or ETV (n = 2) following insertion of an EVD. Twenty-eight (32.6%) of these 86 patients underwent at least one revision procedure after a median of 2.9 months (range 2 days to 75.3 months), with similar rates in those with and without disease dissemination at presentation.
Kaplan-Meier analysis was performed to determine if the CSF diversion technique chosen (specifically, VPS placement or ETV) influenced survival. In this analysis, ETV was associated with a favorable survival advantage (log-rank Mantel-Cox test = 4.19, p = 0.041). However, this was not confirmed in a Cox regression analysis with sur-vival as the dependent variable and age, sex, tumor type/dissemination status, GTR of the operative tumor, tumor recurrence/disease progression, chemotherapy, radiother-apy, type of CSF diversion procedure (VPS or ETV), and need for revision CSF diversion procedure as covariates. Importantly, CSF diversion technique did not influence re-currence/disease progression risk.
In comparing the relative durability of ETV and VP
shunting as CSF diversion procedures, no difference was observed in the need for a revision CSF diversion proce-dure on univariate analysis (log-rank Mantel-Cox test = 0.90, p = 0.343) or on a Cox regression with time-to–revi-sion CSF diversion procedure as the dependent variable and age, sex, tumor type/dissemination status, GTR of the operative tumor, tumor recurrence/disease progression, chemotherapy, radiotherapy, and type of CSF diversion (VPS placement or ETV) as covariates. Only an absence of GTR of the operative tumor increased the risk of requir-ing a revision CSF diversion procedure (HR 3.80, 95% CI 1.11–13.03, p = 0.034).
To attempt to identify additional variables that might influence the relative efficacy of ETV and VP shunting and thus guide surgical decision-making in clinical practice, additional variables were created for the survival analysis that differentiated patients according to tumor type (pilo-cytic astrocytoma vs other tumors) and evidence of tumor cell spread along CSF pathways through assessment of tu-mor cells in CSF and/or leptomeningeal disease on initial MRI (present vs absent). In Cox regression analyses with the dependent variables likelihood of revision CSF diver-sion, overall survival, tumor recurrence/disease progres-sion, or event-free survival (with “event” being defined as either death or tumor recurrence/disease progression), there was no interaction observed between choice of CSF diversion procedure (ETV vs VPS placement) and either tumor type (pilocytic astrocytoma vs other tumors) or tu-
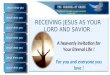
FIG. 3. Survival analysis using Cox regression, with time to CSF diversion as the dependent variable and age, sex, tumor type/dissemination status, GTR of the operative tumor, and tumor recurrence/disease progression as covariates. Time to CSF diversion differed significantly by tumor type/dissemination status (Wald = 20.93, df = 9, p = 0.013), with patients who had disseminated medulloblastomas and PNETs significantly more likely to require CSF diversion. The labels for the lines follow the order of the lines in the graph. Figure is available in color online only.
Unauthenticated | Downloaded 12/01/21 11:38 PM UTC

M. A. Kirkman et al.
J Neurosurg Pediatr Volume 21 • June 2018570
mor cells in CSF/leptomeningeal disease on MRI (pres-ent vs absent; p > 0.05 for all). Although some subgroup numbers were small, the findings suggest that there is no difference in efficacy between the 2 CSF diversion tech-niques among patients with pilocytic astrocytomas com-pared with the other tumors in this study and also between those with and without tumor cells in CSF/leptomeningeal disease on MRI. Furthermore, when comparing the effi-cacy of ETV and VP shunting in only the patients with disseminated disease at presentation, there was no supe-riority of either technique in terms of the likelihood of a revision CSF diversion procedure, overall survival, tumor recurrence/disease progression, or event-free survival (all p > 0.05 for all, log-rank test).
Surgical MorbidityAcross all 5 tumor groups, patients with disease dis-
semination at presentation were more likely to experience a postoperative complication than were those without dis-semination at presentation (Table 2); this difference was significant for ATRTs (n = 4 [50%] vs n = 1 [4.5%], respec-tively; chi-square test = 8.73, p = 0.003), medulloblastoma (n = 12 [41.4%] vs n = 2 [2.7%], respectively; chi-square test = 26.54, p < 0.0001), and in terms of data from all 5 tu-mors combined (n = 20 [37.7%] vs n = 67 [21.8%], respec-tively; chi-square test = 6.32, p = 0.012). Overall, posterior fossa syndrome was the most common complication, ob-served in 8 (15.1%) of the disseminated tumor cases and 21 (6.8%) of the nondisseminated tumor cases; this was followed by a new cranial nerve deficit (n = 5 [9.4%] vs n = 12 [3.9%], respectively), CSF leak (n = 5 [9.4%] vs n = 9 [2.9%], respectively), and meningitis (n = 2 [3.8%] vs n = 12 [3.9%], respectively).
Length of StayThe overall median length of stay for patients with dis-
seminated tumors at presentation was 14 days (range 2–36 days), whereas for those with nondisseminated tumors at presentation overall median length of stay was 11 days (range 1–99 days). There was no significant difference in median length of stay between these 2 groups, either with-in individual tumor groups or when combining data from all 5 tumor groups.
SurvivalAfter a median follow-up of 64.0 months (range 5.2–
152.0 months) in patients with disseminated disease and a median follow-up of 74.5 months (4.7–170.1 months) in those with nondisseminated disease at presentation (Mann-Whitney U-test = 2756.5, p = 0.224), survival was significantly lower in patients with disease dissemination at presentation when combining data from all 5 tumor groups (n = 26 [49.1%] of 53 vs n = 248 of 308 [80.5%], respectively; chi-square test = 24.47, p < 0.0001) (Table 2).
DiscussionOur study of a large cohort of children with CNS tu-
mors presenting to a single institution over a 14-year pe-riod demonstrates that children with disseminated disease at presentation are less likely to have a GTR of their opera-
tive lesion, have a higher risk of requiring CSF diversion, and a have higher surgical complication rate. On multivar-iate analyses, lack of a GTR was associated with a shorter time to disease progression/recurrence but not worse over-all survival. Both having a CSF diversion procedure and having a revision CSF diversion procedure were associ-ated with a shorter time to disease progression/recurrence only on univariate analyses, and these procedures were not associated with overall survival. As expected, individuals with disseminated disease had a worse overall survival.
The relationship between disease dissemination and ex-tent of resection may reflect the surgical decision-making process in that more aggressive surgery was pursued in pa-tients without disseminated disease, and/or it might reflect the fact that those with disseminated disease had tumors that were more difficult to completely resect. Differences in management and surgical approaches resulted from the fact that each patient in our study was managed on a case-by-case basis dependent on several factors, including the operating surgeon, of whom there were several treat-ing this cohort. There was a strong preference in some of our surgeons to avoid aggressive resection in the presence of widespread disease dissemination, particularly in cases of posterior fossa tumors, given the risk of posterior fossa syndrome. Similarly, biopsy was sometimes the initial sur-gical procedure performed in the presence of extensive disease dissemination and/or in the presence of a tumor in critical brain structures/eloquent cortex and/or lesions inaccessible for resection.
A particular challenge in patients with tumor dissemi-nation is the decision regarding surgical target(s). There is little evidence to guide decision-making in this matter, and the subgroups in our study were too small to allow us to perform any meaningful analysis on the effect of surgical targets on outcomes. Factors that are often considered in the decision-making process include identification of the largest tumor mass, the most neurologically critical mass, and/or the most surgically accessible mass. This is an area that requires further study.
The optimal management of hydrocephalus in patients with CNS tumors can be challenging, and there is little evidence to guide decision-making in this regard. We performed several analyses to evaluate variations in CSF diversion requirements, efficacy of CSF diversion tech-niques, and associations between CSF diversion surgery and outcomes in our cohort. CSF diversion was required more commonly in children with disease dissemination at presentation—specifically, disseminated PNET and me-dulloblastoma. This finding is not unexpected, as disease dissemination increases the likelihood of the presence of a lesion obstructing CSF flow. In addition, the presence of elevated protein levels and cell count in the CSF also impairs absorption of CSF. Lack of a GTR of the operative tumor also increased the likelihood of requiring CSF di-version, probably because of an increased risk of residual tumor blocking CSF flow.
There has been little investigation into the need for tem-porary versus permanent CSF diversion in patients with CNS tumors. The identification of potential high-risk fac-tors that predict the need for conversion from temporary to permanent CSF diversion could guide early management
Unauthenticated | Downloaded 12/01/21 11:38 PM UTC

J Neurosurg Pediatr Volume 21 • June 2018 571
M. A. Kirkman et al.
TABL
E 2.
Gros
s-to
tal r
esec
tion
rate
s, co
mpl
icat
ions
, leng
th o
f sta
y, an
d su
rviva
l at l
ast f
ollo
w-up
Char
acter
istic
ATRT
Med
ullob
lastom
aEp
endy
moma
Piloc
ytic A
stroc
ytoma
PNET
All T
umor
Type
sD
NDD
NDD
NDD
NDD
NDD
ND
No. o
f cas
es8
2229
742
576
138
817
5330
8GT
R, no
. (%)
1 (12
.5)
6 (27
.3)9 (
31.0)
53 (7
1.6)
1 (50
)38
(66.7
)1 (
16.7)
76 (5
5.1)
2 (25
)5 (
29.4)
14 (2
6.4)
178 (
57.8)
Comp
licati
ons,
no. (
%)
No. w
/ ≥1 c
ompli
catio
n4 (
50)
1 (4.
5)12
(41.4
)2 (
2.7)
1 (50
)28
(49.1
)2 (
33.3)
36 (2
6.1)
1 (12
.5)
020
(37.7
)67
(21.8
)
CSF
leak
1 (12
.5)
04 (
13.8)
00
6 (10
.5)
03 (
2.2)
00
5 (9.4
)9 (
2.9)
He
mipa
resis
1 (12
.5)
05 (
17.2)
00
3 (5.
3)0
3 (2.
2)0
06 (
11.3)
6 (1.9
)
IVH
1 (12
.5)
00
00
00
00
01 (
1.9)
0 (0)
Re
spira
tory/p
neum
onia
1 (12
.5)
01 (
3.4)
00
4 (7)
04 (
2.9)
00
2 (3.
8)8 (
2.6)
Po
sterio
r fos
sa sy
ndro
me0
07 (
24.1)
1 (1.4
)0
8 (14
)1 (
16.7)
12 (8
.7)0
08 (
15.1)
21 (6
.8)
Subd
ural
colle
ction
01 (
4.5)
1 (3.
4)0
01 (
1.8)
04 (
2.9)
00
1 (1.9
)6 (
1.9)
Ne
w cr
anial
nerv
e defi
cit0
04 (
13.8)
1 (1.4
)1 (
50)
4 (7)
07 (
5.1)
00
5 (9.4
)12
(3.9)
Ps
eudo
menin
goce
le0
01 (
3.4)
00
3 (5.
3)0
4 (2.
9)0
01 (
1.9)
7 (2.
3)
Men
ingitis
00
1 (3.
4)0
06 (
10.5
)1 (
16.7)
6 (4.3
)0
02 (
3.8)
12 (3
.9)
Wou
nd in
fectio
n/br
eakd
own
00
1 (3.
4)0
01 (
1.8)
03 (
2.2)
1 (12
.5)
02 (
3.8)
4 (1.3
)
Seizu
res
00
00
02 (
3.5)
00
00
02 (
0.6)
Med
ian le
ngth
of ini
tial in
patie
nt sta
y (ra
nge),
days
10.5
(3
–27)
11.0
(4–9
9)15
(7
–36)
12.5
(1–
54)
16.5
(9
–24)
15
(4–8
5)12
(2
–19)
8 (1–
73)
11.5
(3
–22)
11
(1–81
)14
(2
–36)
11
(1–99
)Al
ive at
last
follo
w-up
, no.
(%)
2 (25)
10
(45.
5)14
(4
8.3)
55
(74.3)
1 (50)
41
(71.9
)4
(66.7
)13
5 (9
7.8)
5 (62.
5)7
(41.2)
26
(49.1
)24
8 (8
0.5)
IVH
= int
rave
ntric
ular h
emor
rhag
e.Bo
ldfac
e typ
e ind
icate
s sta
tistic
al sig
nifica
nce (
p < 0.
05) b
etwe
en pa
tient
s with
diss
emina
ted a
nd no
ndiss
emina
ted d
iseas
e with
in th
at sp
ecific
tum
or gr
oup,
exce
pt in
the “
All T
umor
Type
s” co
lumns
, whe
re da
ta fr
om al
l 5
tum
or gr
oups
are c
ombin
ed. T
he ch
i-squ
are t
est w
as us
ed fo
r cate
goric
al da
ta an
d Man
n-W
hitne
y U-te
st fo
r con
tinuo
us da
ta.
Unauthenticated | Downloaded 12/01/21 11:38 PM UTC

M. A. Kirkman et al.
J Neurosurg Pediatr Volume 21 • June 2018572
and could potentially reduce not only the need for tem-porary CSF diversion but also the risks associated with additional surgical procedures. In our study, over 40% of patients who underwent initial temporary CSF diversion with an EVD required conversion to a means of perma-nent CSF diversion such as ETV or VPS insertion. How-ever, in a comprehensive multivariate logistic regression with a moderate number of patients, we could not identify any risk factors to predict the need for conversion, and this issue requires further study in a larger prospective series.
For patients with CNS tumors requiring a procedure for permanent CSF diversion, there has been some debate about whether shunting is superior to ETV. A recent com-bined systematic review and retrospective study including 408 patients with posterior fossa tumors found that ETV failure occurred earlier than VPS failure, but the authors speculated that long-term treatment durability might be higher for ETV and that complications occurred more commonly with a VPS.3 However, the included studies were noted for marked heterogeneity in methodology, tim-ing of CSF diversion, and being subject to surgeon bias. In our study, which included 86 patients who underwent either VPS placement or ETV, we found a significant sur-vival advantage in the Kaplan-Meier analysis for ETV when not controlling for potential confounding variables. However, this advantage did not persist in the multivariate analysis when variables that might independently influ-ence outcome were accounted for, such as patient demo-graphics, the specific tumor type/dissemination status, and adjuvant therapy. Furthermore, there was no difference in CSF diversion procedure failure rates (i.e., time to repeat CSF diversion procedure) or time to tumor recurrence/dis-ease progression between VP shunting and ETV. A repeat CSF diversion procedure in all cases (VPS and ETV) oc-curred earlier in patients with tumor recurrence/disease progression, likely due to an increased risk of the pres-ence of a space-occupying lesion obstructing CSF flow. It was not possible to identify any differential superiority between VPS placement and ETV in terms of need for revision CSF diversion, tumor recurrence/disease progres-sion, or overall survival that was influenced by tumor ag-gressiveness (pilocytic astrocytoma vs the other tumors in this study) or the presence of tumor cells in CSF/lepto-meningeal disease on MRI. Also there was no superiority of a CSF diversion technique found when only individuals with disseminated disease at presentation were taken into consideration. Taking all these results together with those of the systematic review,3 there is no clear superiority of either VPS or ETV in terms of effect on survival or suc-cess of the technical procedure.
There is a theoretical concern that placement of a shunt may facilitate seeding of a CNS tumor outside of the CNS, as demonstrated in a recent case report and literature re-view including 28 cases in which there was evidence of peritoneal seeding from VPS in children with primary brain tumors, including cases of all 5 tumor groups speci-fied in the present study.9 In our study, 2 patients had intraabdominal tumor recurrence during the follow-up period: one with a PNET who had underwent ETV and another with a medulloblastoma with a VPS in situ. There-fore, based on our data, the risk of peritoneal seeding in patients with a VPS is low, and there does not appear to
be a significantly increased risk of peritoneal seeding with VPS placement over ETV.
The higher surgical complication rate in patients with disease dissemination in the present series is driven large-ly by the medulloblastoma and ATRT groups. The spe-cific reasons for this observation remain unclear, but the increased rate of neurological deficits and posterior fossa syndrome, particularly in the context of a more conserva-tive tumor resection, may or may not be related to reduced neurological reserve. Further research may help identify the causative mechanisms of this association as well as methods to reduce the risk of surgical complications in this group.
The main limitations of this study relate to its retrospec-tive nature, which may have limited the quality of data col-lected, the heterogeneous mix of patients and management strategies employed, and the relatively small numbers in some disseminated subgroups, which may have reduced the likelihood of finding statistically significant differenc-es in our results. Not all patients had CSF samples taken to look for malignant cells. In addition, the lack of molecular profiling for the medulloblastoma cohort prevented further analysis by tumor subgrouping; it is known that molecular subtyping of medulloblastomas has more prognostic sig-nificance than looking at the presence of disease dissemi-nation alone.6,11 However, this approach was unavoidable as most patients in this cohort presented prior to the advent of molecular subtyping.
ConclusionsWe present data from a consecutive series of 361
children with CNS tumors treated at a single institution, demonstrating that patients with disease dissemination at presentation are less likely to have a macroscopic GTR of their operative lesion, have a higher surgical compli-cation rate, and are more likely to require CSF diversion, although from our data it was not possible to identify risk factors to predict the need for permanent CSF diversion following temporary external ventricular drainage. Fur-thermore, it was not possible to clearly demonstrate supe-riority of ETV or VPS placement as a permanent CSF di-version procedure. Further studies are required to address this important issue.
References 1. Aryan HE, Meltzer HS, Lu DC, Ozgur BM, Levy ML, Bruce
DA: Management of pilocytic astrocytoma with diffuse lep-tomeningeal spread: two cases and review of the literature. Childs Nerv Syst 21:477–481, 2005
2. Bian SX, McAleer MF, Vats TS, Mahajan A, Grosshans DR: Pilocytic astrocytoma with leptomeningeal dissemination. Childs Nerv Syst 29:441–450, 2013
3. Dewan MC, Lim J, Shannon CN, Wellons JC III: The dura-bility of endoscopic third ventriculostomy and ventriculo-peritoneal shunts in children with hydrocephalus following posterior fossa tumor resection: a systematic review and time-to-failure analysis. J Neurosurg Pediatr 19:578–584, 2017
4. Engelhard HH, Corsten LA: Leptomeningeal metastasis of primary central nervous system (CNS) neoplasms. Cancer Treat Res 125:71–85, 2005
5. Gajjar A, Bhargava R, Jenkins JJ, Heideman R, Sanford RA,
Unauthenticated | Downloaded 12/01/21 11:38 PM UTC

J Neurosurg Pediatr Volume 21 • June 2018 573
M. A. Kirkman et al.
Langston JW, et al: Low-grade astrocytoma with neuraxis dissemination at diagnosis. J Neurosurg 83:67–71, 1995
6. Kool M, Korshunov A, Remke M, Jones DTW, Schlanstein M, Northcott PA, et al: Molecular subgroups of medullo-blastoma: an international meta-analysis of transcriptome, genetic aberrations, and clinical data of WNT, SHH, Group 3, and Group 4 medulloblastomas. Acta Neuropathol 123:473–484, 2012
7. Massimino M, Biassoni V, Gandola L, Garrè ML, Gatta G, Giangaspero F, et al: Childhood medulloblastoma. Crit Rev Oncol Hematol 105:35–51, 2016
8. Mazloom A, Hodges JC, Teh BS, Chintagumpala M, Paulino AC: Outcome of patients with pilocytic astrocytoma and lep-tomeningeal dissemination. Int J Radiat Oncol Biol Phys 84:350–354, 2012
9. Narayan A, Jallo G, Huisman TAGM: Extracranial, perito-neal seeding of primary malignant brain tumors through ven-triculo-peritoneal shunts in children: case report and review of the literature. Neuroradiol J 28:536–539, 2015
10. Raybaud C, Ramaswamy V, Taylor MD, Laughlin S: Poste-rior fossa tumors in children: developmental anatomy and diagnostic imaging. Childs Nerv Syst 31:1661–1676, 2015
11. Taylor MD, Northcott PA, Korshunov A, Remke M, Cho YJ, Clifford SC, et al: Molecular subgroups of medulloblastoma: the current consensus. Acta Neuropathol 123:465–472, 2012
12. Wright KD, Gajjar A: Current treatment options for pediatric and adult patients with ependymoma. Curr Treat Options Oncol 13:465–477, 2012
DisclosuresThe authors report no conflict of interest concerning the materi-als or methods used in this study or the findings specified in this paper.
Author ContributionsConception and design: Aquilina, Kirkman. Acquisition of data: Kirkman, Phipps. Analysis and interpretation of data: Aquilina, Kirkman, Hayward. Drafting the article: Kirkman. Critically revising the article: Aquilina, Kirkman, Hayward. Reviewed sub-mitted version of manuscript: all authors. Approved the final ver-sion of the manuscript on behalf of all authors: Aquilina . Statisti-cal analysis: Kirkman. Administrative/technical/material support: Phipps. Study supervision: Aquilina, Kirkman, Hayward.
CorrespondenceKristian Aquilina: Great Ormond Street Hospital for Children, London, United Kingdom. [email protected].
Unauthenticated | Downloaded 12/01/21 11:38 PM UTC