Embed Size (px)
Citation preview


Surgery of the Esophagus
Textbook and Atlas of Surgical Practice

Editors
Surgeryof the EsophagusTextbook and Atlasof Surgical Practice
With 394 Drawings in 564 Separate Illustrations
� �
J.R. Izbicki
D.C. Broering
E.F. Yekebas
A. Kutup
A.F. Chernousov
Y. I. Gallinger
P.M. Bogopolski
N. Soehendra

Drawings
Franziska von Aspern
Peter von Aspern
Alfons Eugen Drews
Katharina Schumacher
S. Stämpfli
M. Lück
ISBN 978-3-7985-1309-9 Steinkopff Verlag
Bibliographic information published by Die Deutsche NationalbibliothekDie Deutsche Bibliothek lists this publication in the Deutsche Nationalbibliografie;detailed bibliographic data is available in the Internet at http://dnb.d-nb.de.
This work is subject to copyright. All rights are reserved, whether the whole or part of the material is concerned,specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on mi-crofilm or in any other way, and storage in data banks. Duplication of this publication or parts thereof is permittedonly under the provisions of the German Copyright Law of September 9, 1965, in its current version, and permis-sion for use must always be obtained from Steinkopff Verlag. Violations are liable for prosecution under the GermanCopyright Law.
Steinkopff Verlaga member of Springer Science+Business Media
www.steinkopff.com
© Steinkopff Verlag 2009Printed in Germany
The use of general descriptive names, registered names, trademarks, etc. in this publication does not imply, even inthe absence of a specific statement, that such names are exempt from the relevant protective laws and regulationsand therefore free for general use.
Product liability: The publishers cannot guarantee the accuracy of any information about the application of operativetechniques and medications contained in this book. In every individual case the user must check such informationby consulting the relevant literature.
Medical Editors: Dr. med. Gertrud Volkert, Petra ElsterProduction Editor: Klemens SchwindCover design: Erich Kirchner, HeidelbergTypesetting: K+V Fotosatz GmbH, BeerfeldenPrinting and binding: Stürtz GmbH, Würzburg
SPIN 10783278 105/7231-5 4 3 2 1 0 – Printed on acid-free paper

Dedicated to
Prof. Dr. med. Dr. h.c.Hans-Wilhelm Schreiber (1924–2004)
pioneer in upper gastrointestinal surgery

Preface
While a surgeon many decades ago treated diseases from head to toe, this concepthas evolved, and today some degree of specialization is the rule worldwide. Inmany countries various boards for sub-specializations are designed, and after abroad training in general surgery, many young surgeons move on further into aspecific field.
Knowledge of anatomy and precise surgical technique remain the foundation ofhigh quality surgery. A knowledgeable surgeon, equipped with excellent theoreti-cal and clinical skills, will only be accomplished when he or she masters the op-erative techniques of the practice of surgery. The legacy of an academic surgeonor a surgical teacher relies in great part on the transmission of his or her surgicalabilities. Significant influence on the development in esophageal surgery arisesfrom the surgical understanding of the anatomical and functional structures ofthe esophagus as well as the ongoing developments in the multidisciplinary man-agement in this challenging field of surgery.
In bringing forth this atlas, we were motivated by the desire to create a compre-hensive and educational atlas on esophageal diseases, emphasizing all details ofpathophysiologies, diagnostic strategies, pre- and postoperative management, andoperative techniques covering minimally invasive and open procedures rangingfrom straightforward to more complex procedures.
This Textbook and Atlas is intended for residents in surgery and for fellows spe-cializing in esophageal surgery preparing themselves for the operation, and willbe useful for specialists and general surgeons, who may compare their techniqueswith the one described herein or find some additional help or tricks when per-forming rare procedures.
In summary, we hope that specialists as well as surgeons at various levels oftraining will benefit from this huge effort, combining the work of many experts,gifted artists, and the publisher.
The Editors

Contents
Basic Principles of Esophageal Surgery
1 Surgical Anatomy of the Esophagus . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3D.C. Broering, J. Walter, Z. Halata
� Topography of the esophagus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
� Development of the esophagus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
� Structure of the esophagus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2 The EsophagusDiagnostic Methods of Examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11G. Krupski, V. Nicolas
� Conventional methods of examination . . . . . . . . . . . . . . . . . . . . . . . . . . 11
� Diverticula . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
� Achalasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
� Gastroesophageal reflux and hernias . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
� Varices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
� Foreign bodies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
� Esophageal tumors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
� CT and MRI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
3 Endoscopic Examination of the Esophagus . . . . . . . . . . . . . . . . . . . . . . . 19K.F. Binmoeller, B. Brand, N. Soehendra
� Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
� Equipment and normal anatomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
� Malignant tumors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
� Benign tumors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
� Esophagitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
� Complications of esophagitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
� Varices and other sources of upper gastrointestinal bleeding . . . . . . . . . 22
� Diverticula . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
� Achalasia and other motor disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
� References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24

� ContentsX
4 Role of Endoscopic Ultrasound for Diagnosis and Stagingof Esophageal Cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25A. Fritscher-Ravens, M.X. Pelling
� Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
� Principles of EUS tumor staging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
� Examination technique and instrumentation . . . . . . . . . . . . . . . . . . . . . 27
� EUS compared to other imaging techniques . . . . . . . . . . . . . . . . . . . . . 29
� EUS and tumor stenosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
� EUS and re-staging of esophageal cancer . . . . . . . . . . . . . . . . . . . . . . . 31
� Endoscopic ultrasound in early tumor stages . . . . . . . . . . . . . . . . . . . . 31
� Endoscopic ultrasound guided fine needle aspiration . . . . . . . . . . . . . . 32
� Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
� References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
5 Preoperative Evaluation of the Operative Risk Profile . . . . . . . . . . . . . 39K.A. Gawad, C. Busch, D.C. Broering, E.F. Yekebas
� Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
� Definition of “risk” . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
� Methods of risk ascertainment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
� Measures for preoperative risk minimization . . . . . . . . . . . . . . . . . . . . 40
� References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
6 Perioperative and Postoperative Management . . . . . . . . . . . . . . . . . . . 43J. Scholz, P.H. Tonner, G. von Knobelsdorff
� Preoperative evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
� Postoperative phase . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
� References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
7 Pathophysiology of Gastroesophageal Reflux Diseaseand Indication for Surgical Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51K.-H. Fuchs
� Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
� Definition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
� The antireflux barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
� Esophageal peristalsis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
� Mucosal resistance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
� Duodeno-gastroesophageal reflux . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
� Gastroduodenal disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
� Indication for surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
� Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
� References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55

Contents � XI
8 Gastroesophageal Reflux and its Surgical Management . . . . . . . . . . . . 59G.G. Jamieson, D. I. Watson
� Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
� Which patients should be considered for antireflux surgery? . . . . . . . . . 59
� What are the advantages and disadvantages of antireflux surgery? . . . . . 60
� Operations available . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
� Traditional open fundoplication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
� Laparoscopic fundoplication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
� Laparoscopic versus open surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
� Randomzied trials of laparoscopic antireflux surgery . . . . . . . . . . . . . . . 65
� Controversies and questions in regard to laparoscopic antireflux surgery 65
� Why do antireflux operations sometimes fail . . . . . . . . . . . . . . . . . . . . . 66
� When do antireflux operations fail? . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
� Re-operative surgery for failed antireflux procedures . . . . . . . . . . . . . . . 67
� References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
9 Pathologic Classification of the Esophageal Carcinoma . . . . . . . . . . . . . 71P. Hermanek
� Tumor classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
� Tumor site . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
� Typing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72
� Grading . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72
� TNM/pTNM classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
� Requirement for pTNM classification of esophageal carcinoma(UICC 2002, 2003) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
� Additional descriptors and optional categories of the TNM system . . . . 76
� Residual tumor (R) classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77
� Grading of histological regression after neoadjuvant treatment . . . . . . . 78
� Preconditions for adequate histopathological tumor classification . . . . . 79
� References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79
10 Lymphatic Dissemination and Principles of Lymph Node Dissection . . . 81J.R. Izbicki, A. Rehders, A. Kutup, C. Busch
� Anatomy of the lymphatic system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
� Operative procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85
� References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86

� ContentsXII
11 Rationale for Type of Resection in Cancer of the Esophagusand Gastroesophageal Junction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89W.T. Knoefel, I. Alldinger, J.R. Izbicki
� Tumor typing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89
� Anatomic location . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
� Cervical esophagus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
� Upper thoracic esophagus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
� Lower thoracic esophagus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91
� Tumors of the gastroesophageal junction . . . . . . . . . . . . . . . . . . . . . . . 91
� Limited resections . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
� Palliative esophageal resection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
� Recurrences . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
� Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
� References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
12 Results of Extended en bloc Esophagectomy in Treatmentof Patients with Esophageal Cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97D. I. Watson, G.G. Jamieson
� Rationale for extended en bloc esophagectomy . . . . . . . . . . . . . . . . . . . 97
� Proposed advantages and disadvantages for extendeden bloc esophagectomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
� Results of standard esophagectomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
� Results of 2 field (en bloc) esophagectomy . . . . . . . . . . . . . . . . . . . . . . 99
� Results of extended 3 field esophagectomy . . . . . . . . . . . . . . . . . . . . . . 100
� Case selection and peri-operative outcomes for 3 field esophagectomy . 100
� Complications following 3 field esophagectomy . . . . . . . . . . . . . . . . . . . 101
� Lymph node metastases to the cervical nodes foundby 3 field lymphadenectomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101
� Survival following esophagectomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101
� Randomized trials of extended 3 field esophagectomyversus 2 field en bloc esophagectomy . . . . . . . . . . . . . . . . . . . . . . . . . . 102
� Use of 3 field en bloc esophagectomy for adenocarcinomaof the esophagus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104
� Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104
� References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104

Contents � XIII
Surgical Techniques
13 Blunt Transhiatal Subtotal Esophagectomywith Gastroplasty and Cervical Anastomosis . . . . . . . . . . . . . . . . . . . . . . 109E.F. Yekebas, A.F. Chernousov, D.C. Broering, P.M. Bogopolski,
C.F. Eisenberger, A. Kutup, J.R. Izbicki
� Blunt transhiatal esophagectomy and substitution by gastric tube . . . . . 109
� Complications of transhiatal blunt esophageal dissectionand gastric pull-up . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155
14 Partial Abdominothoracic Resection of the Esophaguswith Gastroplasty and Intrathoracic Anastomosis . . . . . . . . . . . . . . . . . 157A.F. Chernousov, A. Kutup, P.M. Bogopolski, D.C. Broering
� Indications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 157
15 Abdominothoracic Subtotal en bloc Esophagectomyand Reconstruction with Gastric Tube Transposition . . . . . . . . . . . . . . . 171J.R. Izbicki, D.C. Broering, P. Kaudel, A. Kutup, E.F. Yekebas
16 Fundus Rotation Gastroplasty . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181M.K. Schilling, M.W. Buechler
17 Proximal Gastrectomy with Distal Esophagectomy(Proximal Resection) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 185A.F. Chernousov, O. Zehler, P.M. Bogopolski, D.C. Broering,
H.W. Schreiber�
18 Transhiatal Esophagogastrectomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 199J.R. Izbicki, D.C. Broering, A. Kutup, E.F. Yekebas
19 Colon Interposition after Total and Subtotal Esophagectomy . . . . . . . . 205J.R. Izbicki, K. Steffani, A.F. Chernousov, P.M. Bogopolski,
D.C. Broering, H.W. Schreiber�
� Complications after subtotal or total esophagectomywith colonic interposition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 222
20 Intrathoracic Esophagoplasty by Colon Interposition . . . . . . . . . . . . . . . 223A.F. Chernousov, P.M. Bogopolski, H.W. Schreiber�, D.C. Broering
21 Reconstruction of Gastrointestinal Continuity by JejunalInterposition following Total and Subtotal Esophagectomy . . . . . . . . . 233A.F. Chernousov, P. Schurr, P.M. Bogopolski, D.C. Broering,
H.W. Schreiber�

� ContentsXIV
22 Limited en bloc Resection of the Gastroesophageal Junctionwith Isoperistaltic Jejunal Interposition . . . . . . . . . . . . . . . . . . . . . . . . . 247J.R. Izbicki, W.T. Knoefel, D.C. Broering
23 Conventional Cardiomyotomy in Achalasia . . . . . . . . . . . . . . . . . . . . . . 253K.A. Gawad, D.C. Broering, C. Busch
24 Surgical Technique in Gastroesophageal Reflux Disease –Conventional Approach . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 259
� Introduction and Techniques in gastroesophageal reflux . . . . . . . . . . . . 259K.A. Gawad, D.C. Broering, C. Bloechle, C. Busch
� Techniques in peptic stricture and hiatal hernia . . . . . . . . . . . . . . . . . . 264A.F. Chernousov, P.M. Bogopolski, K.A. Gawad
25 Conventional Resection of Esophageal Diverticula . . . . . . . . . . . . . . . . 275A.F. Chernousov, C.F. Eisenberger, P.M. Bogopolski, J.R. Izbicki,
H.W. Schreiber�
� Epiphrenic diverticulum . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 278
� Preparation of a diaphragmatic flap for enforcementof the esophageal wall after resection of an epiphrenic diverticulum . . . 280
26 Local Excision of Benign Esophageal Tumors . . . . . . . . . . . . . . . . . . . . . 281A.F. Chernousov, A. Kutup, P.M. Bogopolski, H.W. Schreiber�
27 Surgical Treatment of Esophageal Fistula and Perforation . . . . . . . . . . 283A.F. Chernousov, N. Roch, P.M. Bogopolski, D.C. Broering,
H.W. Schreiber�
� Fistulas of the esophagus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 284
� Cervical fistulas of the esophagus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 284
� Intrathoracic esophago-tracheal fistula . . . . . . . . . . . . . . . . . . . . . . . . . 286
� Intrathoracic fistulas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 287
� Intraabdominal fistulas of the esophagus . . . . . . . . . . . . . . . . . . . . . . . 288
� Esophagopleural fistulas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 289
28 Techniques of Local Esophagoplasty . . . . . . . . . . . . . . . . . . . . . . . . . . . 293A.F. Chernousov, A. Kutup, P.M. Bogopolski, H.W. Schreiber�

Contents � XV
29 Minimal Invasive Surgery of the Esophagus . . . . . . . . . . . . . . . . . . . . . . 297H. Feussner, R. Bumm, T. Olah
� Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 297
� Diverticula of the esophagus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 297
� Minimal invasive treatment of esophageal motility disorders . . . . . . . . . 301
� Antireflux surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 303
� Excision of benign tumors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 307
� Minimally invasive procedures in esophageal carcinoma . . . . . . . . . . . . 308
30 Endoscopic Technique in the Treatment of Esophageal Diseases . . . . . 315Y. I. Gallinger, M. Rehner, F.M. Steichen, N. Soehendra
� Hemorrhage and esophageal varices . . . . . . . . . . . . . . . . . . . . . . . . . . . . 315
� Foreign bodies and bolus obstruction . . . . . . . . . . . . . . . . . . . . . . . . . . 324
� Resection of tumors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327
� Photodynamic therapy of tumors (PDT) . . . . . . . . . . . . . . . . . . . . . . . . 333
� Obstructions by malignant tumors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 335
� Esophageal fistula . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 341
� Dilatation of benign stenoses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 345
� Stenotic esophageal anastomoses and membranes (webs) . . . . . . . . . . . 348
� Achalasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 351
� Diverticula . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 355
� References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 357
31 Post-operative Complications of the Esophagusand Esophagus Bridge Graft . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 361D.C. Broering, J.R. Izbicki, Y. Vashist, A.F. Chernousov,
P.M. Bogopolski, E.F. Yekebas
� Early post-operative complications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 361
� Late post-operative complications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 367
Subject Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 373

Editors and Authors
Ingo Alldinger, MDDepartment of General-,Visceral- and Pediatric SurgeryHeinrich-Heine-University of DüsseldorfMoorenstrasse 540225 Düsseldorf, Germany
Kenneth F. Binmoeller, MDCenter for Complex Digestive2333 Buchanan StreetSan Francisco, CA 94115, USA
Christian Bloechle, MDDepartment of Generaland Visceral SurgerySana Kliniken Lübeck GmbHKronsforder Allee 71-7323560 Lübeck, Germany
Pavel M. Bogopolski, MDDepartment for Thoracic& Abdominal SurgeryNational Research Centre of SurgeryAbrikosovski pereulok 2Moscow, 119992, Russia
Boris Brand, MDMedical Center HammoniabadLerchenfeld 1422081 Hamburg, Germany
Dieter C. Broering, MDDepartment of Generaland Thoracic SurgeryChristian-Albrechts-University KielOlshausenstrasse 4024118 Kiel, Germany
Markus W. Buechler, MDDepartment of General,Visceral and Transplantation SurgeryUniversitätsklinikum HeidelbergIm Neuenheimer Feld 67269120 Heidelberg, Germany
Rudolf Bumm, MDDepartment of SurgeryKlinikum rechts der IsarTU MünchenIsmaninger Strasse 2281675 München, Germany
Christoph Busch, MDDepartment of General,Visceral and Thoracic SurgeryUniversity Hospital Hamburg EppendorfMartinistrasse 5220246 Hamburg, Germany
Alexandr F. Chernousov, MDDepartment for Thoracic& Abdominal SurgeryNational Research Centre of SurgeryAbrikosovski pereulok 2Moscow, 119992, Russia
Claus F. Eisenberger, MDDepartment of General-,Visceral- and Pediatric SurgeryHeinrich-Heine-University of DüsseldorfMoorenstrasse 540225 Düsseldorf, Germany
Hubertus Feussner, MDDepartment of SurgeryKlinikum rechts der IsarTU MünchenIsmaninger Strasse 2281675 München, Germany
Annette Fritscher-Ravens, MDSt. Mary’s HospitalImperial CollegePraed StreetLondon W2 1NY, UK
Karl-Hermann Fuchs, MDDepartment of SurgeryMarkus-KrankenhausFrankfurter Diakonie-KlinikenWilhelm-Epstein-Straße 260431 Frankfurt am Main, Germany

� Editors and AuthorsXVIII
Yury I. Gallinger, MDDepartment for Endosopic SurgeryNational Research Centre of SurgeryAbrikosovsky pereulok 2Moscow, 119992, Russia
Karim A. Gawad, MDDepartment of General,Visceral and Thoracic SurgeryUniversity Hospital Hamburg EppendorfMartinistrasse 5220246 Hamburg, Germany
Zdenek Halata, MDInstitute of AnatomyFirst Medical FacultyCharles University in PragueU Nemocnice 3128 00 Praha 2, Czech Republic
Paul Hermanek, MDDepartment of SurgeryUniversity Hospital ErlangenKrankenhausstrasse 1291054 Erlangen, Germany
Jakob R. Izbicki, MDDepartment of General,Visceral and Thoracic SurgeryUniversity Hospital Hamburg EppendorfMartinistrasse 5220246 Hamburg, Germany
Glyn G. Jamieson, MDDiscipline of SurgeryUniversity of AdelaideRoyal Adelaide HospitalNorth TerraceAdelaide, S.A. 5000 Australia
Philipp Kaudel, MDDepartment of General,Abdominal and Transplant SurgeryHannover Medical SchoolCarl-Neuberg-Strasse 130625 Hannover, Germany
Georg von Knobelsdorff, MDDepartment of AnaesthesiologySt. Bernward KrankenhausTreibestrasse 931134 Hildesheim, Germany
Wolfram T. Knoefel, MDDepartment of General-,Visceral- and Pediatric SurgeryHeinrich-Heine-University of DüsseldorfMoorenstrasse 540225 Düsseldorf, Germany
Gerrit Krupski-Berdien, MDDepartment of RadiologyHospital Reinbek St. Adolph-StiftHamburgerstrasse 4121465 Reinbek, Germany
Asad Kutup, MDDepartment of General,Visceral and Thoracic SurgeryUniversity Hospital Hamburg EppendorfMartinistrasse 5220246 Hamburg, Germany
Volkmar Nicolas, MDDepartment of Radiologyand Nuclear MedicineUniversity BochumBürkle de la Camp-Platz 144789 Bochum, Germany
Tiborné Olah, MDDepartment of SurgeryUniversity SzegedKalvaria sgt. 576725 Szeged, Hungary
Mark X. Pelling, MDSt. Mary‘s HospitalImperial CollegePraed StreetLondon W2 1NY, UK
Alexander Rehders, MDDepartment of General-,Visceral- and Pediatric SurgeryHeinrich-Heine-University of DüsseldorfMoorenstrasse 540225 Düsseldorf, Germany
Manfred Rehner, MDRehmkoppel 39b22391 Hamburg, Germany
Nadine Roch, MDDepartment of General,Visceral and Thoracic SurgeryUniversity Hospital Hamburg EppendorfMartinistrasse 5220246 Hamburg, Germany
Martin K. Schilling, MDDepartment of General Surgery,Abdominal and Vascular Surgeryand Paediatric SurgerySaarland University HospitalKirrberger Straße66421 Homburg/Saar, Germany

Editors and Authors � XIX
Jens Scholz, MDDepartment of Anaesthesiologyand Operative MedicineUniversity Hospital Schleswig-Holstein,Campus KielSchwanenweg 2124105 Kiel, Germany
Hans-Wilhelm Schreiber�, MDDepartment of General,Visceral and Thoracic SurgeryUniversity Hospital Hamburg EppendorfMartinistrasse 5220246 Hamburg, Germany
Paulus Schurr, MDDepartment of General,Visceral and Thoracic SurgeryUniversity Hospital Hamburg EppendorfMartinistrasse 5220246 Hamburg, Germany
Nib Soehendra, MDDepartment of Interdisciplinary EndoscopyUniversity Hospital Hamburg EppendorfMartinistrasse 5220246 Hamburg, Germany
Katharina Steffani, MDDepartment of General,Visceral and Thoracic SurgeryUniversity Hospital Hamburg EppendorfMartinistrasse 5220246 Hamburg, Germany
Felicien M. Steichen, MDInstitute for Minimally Invasive Surgery303 North Street, Suite 103White PlainsNew York, 10605, USA
Peter H. Tonner, MDDepartment of AnaesthesiologyHerzzentrum BremenKlinikum Links der WeserSenator-Weßling-Straße 128277 Bremen, Germany
Yogesh Vashist, MDDepartment of General,Visceral and Thoracic SurgeryUniversity Hospital Hamburg EppendorfMartinistrasse 5220246 Hamburg, Germany
Jessica Walter, MDDepartment of General and Thoracic SurgeryChristian-Albrechts-University KielOlshausenstrasse 4024118 Kiel, Germany
David I. Watson, MDDiscipline of SurgeryUniversity of AdelaideRoyal Adelaide HospitalNorth TerraceAdelaide, S.A. 5000 Australia
Emre F. Yekebas, MDDepartment of General,Visceral and Thoracic SurgeryUniversity Hospital Hamburg EppendorfMartinistrasse 5220246 Hamburg, Germany
Oliver Zehler, MDDepartment of General,Visceral and Thoracic SurgeryUniversity Hospital Hamburg EppendorfMartinistrasse 5220246 Hamburg, Germany

Basic Principlesof Esophageal Surgery

The esophagus is a part of the alimentarytract. It is a muscular tube approximately25 cm long extending from the pharynx to thestomach. The esophagus begins at the lowermargin of the cricoid cartilage opposite thesixth cervical vertebra and enters the gastricorifice at the level of the twelfth thoracic verte-bra.There are some morphological and physio-
logical differences between the esophagus andthe remaining parts of the gastrointestinaltract. The esophagus is the narrowest of thedigestive tubes and is collapsed under restingconditions. The main function is to provide aproper transit of the food bolus from the phar-ynx into the stomach. Positioned in the poste-rior mediastinum, the esophagus is surround-ed only by adventitial tissue. The musculartube remains under permanent tension and isproximally secured by the upper esophagealsphincter and distally by the lower esophagealsphincter. These sphincters create a high-pres-sure zone of 2 to 4 cm in length. The uppersphincter prevents any continous air flow intothe digestive tube. The lower sphincter func-tions as a barrier against reflux of gastric juiceinto the esophagus. The closure of the upperand the lower sphincter is optimized by a sub-mucous venous plexus. Both sphincters andadditionally the passage through the musculardiaphragm describe 3 narrowings. Above thesenarrowings diverticula may occur due to areasof weakness in the muscular wall.After deglutition starts with a pharyngeal
phase, the esophageal phase of swallowing con-tinues with a progressing peristaltic wave. Thecontraction is initiated in the external longitu-dinal muscle layer and results in shorteningand dilating the esophagus simultaneously.Secondly, the circular muscle layer narrows thediameter of the esophagus. The peristaltic con-
traction moves down from oral to aboral at 2to 4 cm per second. The transit time dependson the consistence of the food. The passage ofliquids lasts for at least 1 to 2 seconds, mashedfood for at least 5 seconds, and solid foodneeds a transit time of about 9 seconds toreach the cardiac orifice of the stomach.
Topography of the esophagus
The esophagus passes through three compart-ments: the neck, the chest, and the abdomen.Therefore, it can be divided into a cervical,thoracic and abdominal segment.
� The cervical segment (C6–Th1) of the esopha-gus begins as a continuation of the pharynxabout 15 cm from the incisors. Lying preverte-bral between the deep and the middle cervicalfascia and anteriorly attached to the trachea,the course of the esophagus deviates slightly tothe left.
� Relations. Anteriorly, the trachea passes thecervical esophagus. The esophageal adventitiais attached to connective tissue of the membra-nous wall of the trachea and anchored to thetrachea and the pleura by fibromuscular tissuebands. Posteriorly, the cervical esophagus is re-lated to the longissimus cervicis muscles underthe prevertebral fascia. Bilaterally, there are thecommon carotid arteries, the internal jugularveins, and the vagal nerves. The left side of theesophagus lies somewhat closer to the carotidbundle than the right. The dorsal parts of thethyroid gland are located bilaterally betweenthe esophagus and the carotid arteries. Thethoracic duct ascends for a short distance
Surgical Anatomy of the EsophagusD.C. Broering, J. Walter, Z. Halata
1

along the left side of the esophagus before ar-riving to the left venous confluence. In agroove between the trachea and the esophagus,the recurrent nerves ascend on each side tothe larynx.
� The thoracic segment (Th1–Th10) of the eso-phagus descends from the superior mediasti-num to the lower posterior mediastinum andturns slightly to the right of the spine. Itcourses behind the trachea from the superiormediastinum downward, where it is attachedto the left main bronchus. The aortic archwhich becomes the descending thoracic aortaruns on the left side of the esophagus. Thethoracic aorta gives rise to branches fromwhich this portion of the esophagus directlyreceives its blood supply.
� Relations. The ventral thoracic esophagus iscovered by the trachea and the left main stembronchus. While descending, it passes the rightpulmonary artery and touches the pericardiumof the adjacent left atrium. Below the trachealbifurcation a vagal plexus surrounds the eso-phageal wall. At the level of the diaphragmhiatus, the plexus gives rise to an anterior anda posterior vagal trunk. The anterior trunkpasses downward on the ventral surface of thetube, and the posterior trunk runs on the dor-sal esophageal wall.In the superior mediastinum, the last part
of the aortic arch with the left subclavian ar-tery lies left of the esophagus. Further to theleft, there are the thoracic duct and the leftmediastinal pleura.The thoracic aorta descends on the left side
of the esophagus in the lower dorsal mediasti-num. On the right side there is the mediastinalpleura and the azygos vein ascending fromdorsal right to the upper mediastinum anddraining into the superior vena cava.The vertebral column, the thoracic duct, and
the intercostal arteries are located dorsally. Di-rectly above the diaphragm, the last part of thethoracic aorta crosses behind the esophagus.
� The abdominal segment (Th10–Th11) is about1.2–2.5 cm in length, it takes a conical coursewhile running below the diaphragm from theesophageal hiatus to enter the cardiac part ofthe stomach. This abdominal portion lies in-
traperitoneal and is surrounded by a serosacoat.
� Relations. Ventrally runs the anterior vagaltrunk, the posterior vagal trunk is placed onthe dorsal muscular wall. To its right, the eso-phagus lies in close contact to the left lobe ofthe liver, which forms an esophageal groove.While running through the diaphragm, the
esophagus is surrounded and attached by thephrenoesophageal membrane. This ligamentconsists endothoracically of the pleura, thesubpleural fascia, and the phrenoesophagealfascia of Laimer. The subdiaphragmatic por-tion of the membrane consists of peritoneumand the transversalis fascia, blending into theadventitial coat of the abdominal esophagus.This membranous arrangement allows elasticmobility of the distal esophagus.
Development of the esophagus
The esophagus is derived from the caudal partof the foregut just below the germ of the phar-ynx. In the fourth week of development, thecaudal portion of the foregut builds a fusiformenlargement to mark the site of the futurestomach. Above this dilatation, the tracheo-bronchial diverticula develop ventrally. In laterperiods, the development of a tracheoesopha-geal septum partitions the future trachea fromthe future esophagus. The trachea originatesfrom the ventral part, the esophagus from thedorsal part of the membranous septum.The endoderm of the primitive gut gives
rise to the mucosal epithelium. The remaininglayers are derived from mesenchyme of thecaudal branchial arches and from the segmen-tal splanchnic mesenchyme. Two thirds of themuscular esophageal wall contains striatedmuscle fibers. In the middle third both smoothand striated muscle fibers are represented. Thelower third of the muscle coat is dominated bysmooth muscle fibers only.The arterial blood supply (Fig. 1.1) repre-
sents the complicated development and seg-mentation of the esophagus. The cervical eso-phagus receives its blood supply mainly fromthe inferior thyroidal artery of the thyrocervi-
� D. C. Broering et al.4

cal trunk and from the superior thyroidal ar-tery. Together with branches of the tracheoeso-phageal artery, the vessels build a dense net-work of collateral anastomoses on both theanterior and posterior esophageal wall. In rarecases, the subclavian artery may give rise to anesophageal branch. The thoracic esophagealsegment is proximally supplied by two to threebronchial arteries originating from the archand the upper descending aorta. Distally, oneor two esophageal arteries arise directly fromthe thoracic aorta. These vessels divide intoone ascending and one descending branchsome distance before entering the esophagealwall. The abdominal esophagus receives its ar-terial blood from the ascending branches ofthe left gastric and inferior phrenic arteries.The branches of the left gastric artery run onthe lateral side of the cardia following thelongitudinal axis of the esophagus. The dorsalwall of the distal esophagus is supplied bybranches of the inferior phrenic arteries and
by branches of the splenic artery. All of themain esophageal arterial branches follow thelongitudinal course of the esophagus afterentering the submucosal layer. They form alongitudinal network and give rise to minutebranches at right angles which surround thecircumference to communicate with the oppo-site side. Altogether, the cervical, thoracic, andabdominal esophageal arterial branches areconnected by a dense anastomosing submuco-sal network of small vessels. This network pro-vides an adequate circulation during surgicalmobilization.The venous drainage continues the division
into three segments. The veins of the cervicalportion drain into the inferior thyroid vein. Inthe thoracic region, the blood empties into theazygos, hemiazygos, and the accessory hemi-azygos veins. Caudally, the venous plexi of theabdominal esophagus return blood into the leftgastric vein, and into the coronary vein. Thiscommunication belongs to the portocaval anas-tomoses. In case of portal venous obstruction,collaterization through the venous plexus mayoccur and result in esophageal varices.For clinical aspects and especially for thera-
py of malignant tumors, knowledge of the lym-phatic vessels (Figs. 1.2–1.5, Table 1.1 and 1.2)and the regional lymph nodes is of immenseimportance. The lymphatic capillary vesselsform a plexus in the submucosal layer of theesophageal wall. The flow of lymph runsmainly in a longitudinal direction. During con-traction of the muscular tube, the lymph canflow bidirectionally, cranial and caudal. Therecan be a direct connection from lymphaticcapillary vessels to the thoracic duct in themiddle part of the esophagus.Lymph ducts of the cervical esophagus drain
mainly into the paraesophageal lymph nodes,lying laterally to the esophagus, and into theretropharyngeal lymph nodes, which are posi-tioned behind the pharynx on the prevertebralfascia. These lymph nodes drain into the cervi-cal lymph nodes, running with the externaland internal jugular veins.Lymph flow from the upper third of the me-
diastinal compartment enters the superiorparaesophageal lymph nodes which are later-ally attached to the esophagus, and the prever-tebral lymph nodes, located caudally. In com-mon, lymphatic drainage of the mid-third
1 Surgical Anatomy of the Esophagus � 5
Fig. 1.1. Arterial supply of the esophagus. 1 Thoracic aorta;2 trachea; 3 left and right subclavian artery; 4 inferior thy-roid artery with (5) esophageal branches; 6 bronchial artery;7 aortic esophageal arteries; 8 left gastric artery; 9 ascendingbranches of the left gastric artery; 10 ascending branches ofthe phrenic artery.

� D. C. Broering et al.6
Fig. 1.2. Mediastinum – ventral view including esophagus (1),thoracic aorta (2) and trachea (3). 4 Right principal bronchus;5 left principal bronchus; 6 nodi lymphatici bronchopulmo-nales; 7 nodi lymphatici juxtaesophageales pulmonales; 8 nodilymphatici tracheobronchiales inferiores; 9 nodi lymphatici tra-cheobronchiales superiores; 10 nodi lymphatici mediastinalesanteriores; 11 thoracic duct.
Fig. 1.3. Mediastinum – ventral view including esophagus(1) and thoracic aorta (2). 3 Brachiocephalic trunk; 4 leftcommon carotid artery; 5 left subclavian artery; 6 nodi lym-phatici mediastinales anteriores; 7 nodi lymphatici juxtaeso-phageales pulmonales; 8 nodi lymphatici prevertebrales;9 anterior facies of the stomach; 10 celiac trunk with nodilymphatici coeliaci; 11 nodi lymphatici gastrici sinistri; 12 nodilymphatici pancreaticolienales; 13 nodi lymphatici gastroomen-tales.

1 Surgical Anatomy of the Esophagus � 7
Fig. 1.4. Mediastinum – ventral view including thoracic aor-ta (2) and thoracic duct (8). 1 Esophagus; 2 thoracic aorta;3 superior vena cava; 4 brachiocephalic veins; 5 externaljugular veins; 6 subclavian veins; 7 azygos vein; 8 thoracicduct; 9 nodi lymphatici prevertebrales (UICC-108 – nodi lym-phatici paraesophageales mediales); 10 (nodi lymphatici in-tercostales – not constantly); 11 nodi lymphatici aortici;12 nodi lymphatici phrenici.
Fig. 1.5. Mediastinum – dorsal view. 1 Esophagus; 2 des-cending aorta; 3 internal jugular vein; 4 pharynx; 5 commoncarotid artery; 6 trachea; 7 right principal bronchus; 8 leftprincipal bronchus; 9 left vagus nerve; 10 right vagus nerve;11 left pulmonary artery; 12 left and right lung; 13 nodilymphatici retropharyngeales and nodi lymphatici paraeso-phageales; 14 nodi lymphatici tracheobronchiales inferiores;15 nodi lymphatici juxtaesophageales pulmonales; 16 thorac-ic duct.

courses into the medial paraesophageal lymphnodes and into the paratracheal, tracheobron-chial and bronchopulmonary lymph nodes.However, it can also enter the thoracic duct di-rectly in rare cases. Another course for thelymphatic pathway can be to the lymph nodesof the cranial or caudal compartment. Thelymphatic flow from the lower mediastinalthird runs to the inferior paraesophageal andprevertebral lymph nodes. Additionally, the su-perior diaphragmatic lymph nodes have to bementioned. They rest on the diaphragm alongthe dorsal connection between the pericardiumand the diaphragm.
Lymphatic flow from the abdominal segmentempties into the left and right gastric lymphnodes along the lesser curvature and into thegastroomental, pyloric, and/or coeliacal lymphnodes along the greater curvature. The lym-phatic pathways, the UICC and the anatomicalnomenclature are summarized in a table.The innervation of the esophagus is pro-
vided by both sympathetic and parasympa-thetic fibers. The sympathetic nerve supply isthrough the cervical and thoracic sympatheticchain. Commonly, the branches run with thearterial vessels. The parasympathetic nerve isprimarily through the recurrent laryngeal
� D. C. Broering et al.8
Table 1.1. Lymph nodes of the esophagus
Draining region UICC Anatomical nomenclature Position
� Cervical 100 Nodi lymphatici cervicales laterales:compartment 100 – superficiales along the external jugular vein
102 – profundi along the internal jugular vein
101 (Nodi lymphatici paraesophageales) beside the esophagusNodi lymphatici retropharyngeales inbetween the dorsal aspect of the
pharynx and the prevertebral fascia
103
104 Nodi lymphatici supraclaviculares the lowest of the deep cervical lymph nodes
� Mediastinal 105, 108, 110 Nodi lymphatici prevertebrales beside andcompartment 105 (Nodi lymphatici paraesophageales
superiores)above
108 (Nodi lymphatici paraesophagealesmediales)
beside and behind the esophagusin the middle
110 (Nodi lymphatici paraesophagealesinferiores)
beside and behind the esophagus below
106 Nodi lymphatici paratracheales along the trachea
107 Nodi lymphatici tracheobronchiales inbetween the bifurcation of trachea alongthe principal bronchi
109 Nodi lymphatici bronchopulmonalesand hilares
at the pulmonary hilum
111 Nodi lymphatici diaphragmatici superiores along the attachment of the pericardiumwith the diaphragm
112 Nodi lymphatici prevertebrales along the caudal thoracic aorta
� Perigastrical 1 and 2 Nodi lymphatici gastrici sinistri right and left to the cardiacompartment 3 Nodi lymphatici gastrici dextri along the lesser curvature
4 Nodi lymphatici gastroomentales along the greater curvature
5 and 6 Nodi lymphatici pylorici above and below the pylorus
7 Nodi lymphatici preaortici (coeliaci) along the left gastric artery

nerve and the esophageal plexus arising fromthe vagus nerve.Due to the close relationship to the respira-
tory tract and an extending increase of muco-sal epithelium, malformations can occur in sev-eral cases. Most common are esophageal steno-sis, atresia, fistula, and diverticula.
Structure of the esophagus
The esophageal wall consists of four layers. Itis comprised of a characteristic tissue textureof the mucosa – the internal mucous coat (tu-nica mucosa), the submucosal (tela submuco-sa), and the muscular layer (tunica muscu-laris). The external layer is an adventitial coat(tunica adventitia) composed of loose connec-tive tissue.
The mucous layer consists of three layers:� the lamina epithelialis, characterized bystratified, non-keratinizing squamous epithe-lium
� the lamina propia mucosae, and� the lamina muscularis mucosae, containinga small layer of smooth muscle fibers.
The submucosa consists of loose fibrous con-nective tissue and contains mucous and tubu-lar glands, arterial and venous blood vessels aswell as lymphatic vessels. The fine lymph cap-illaries run in a longitudinal direction. Conse-quently, lymph flow may empty both craniallyand caudally into regional lymph nodes. In theupper two thirds of the esophagus, the lymphflow courses mainly cephalad and caudad inthe lower third. Lymph from the middle partmay directly drain into the thoracic duct. Inrare cases, lymphatic follicles can be found inthe submucosal layer.
1 Surgical Anatomy of the Esophagus � 9
Table 1.2. Lymph nodes of the mediastinum
Anatomical nomenclature Position Draining region
� Nodi lymphatici parasternales along the internal thoracic vessels Thoracic wall, mamma, diaphragm,pericardium, prepericardial lymph nodes
� Nodi lymphatici mediastinalesanteriores
aortic arch, brachiocephalic vein Pericardium, thymus, parasternal lymphnodes
� Nodi lymphatici prepericardiales inbetween the sternumand the pericardium
Pericardium
� Nodi lymphatici mediastinalesposteriores:
� Nodi lymphatici juxtaesophagealespulmonales
along the esophagus Esophagus, lung
� Nodi lymphatici bronchopulmonales pulmonary hilum Lung and bronchi
� Nodi lymphatici tracheobronchialesinferiores
inbetween the bifurcation of trachea Lung, bronchi, trachea
� Nodi lymphatici tracheobronchialessuperiores
in the angle between the tracheaand the principal bronchi
Lung, bronchi, trachea
� Nodi lymphatici paratracheales along the trachea Trachea, esophagus
� Nodi lymphatici prevertebrales posterior mediastinum betweenthe thoracic spine and the esophagus
Dorsal thoracic wall, esophagus
� Nodi lymphatici phrenici right and left on the diaphragminbetween the tendinous centerand the costalic part
Diaphragm, pericardium, right sideof the liver, left side of the pericardium
� Nodi lymphatici gastrici around the gastric vessels along thelesser curvature of the stomach
Esophagus, liver, gall bladder, stomach

The submucosal layer also contains a networkof nerves, representing parasympathetic inner-vation through the vagus nerve and sympatheticinnervation. Innervation of glands, smooth andstriated muscle fibers is given through vegetativeneural branches of this network.The muscular coat can be divided into an in-
ternal circular-oriented muscle layer and an ex-ternal muscle layer of longitudinal orientation.In the superior third of the esophagus, theselayers are exclusively composed of striated mus-cle fibers. In the middle third the striated musclefibers dominate, but smooth muscle fibers areintermingled. In the lower third, smooth musclefibers predominate. Most likely, the striatedmuscle originates from the mesenchyme of thecaudal branchial arches, and the smooth muscledevelops from the surrounding segmental mes-
enchyme. A somewhat helical direction of themuscular layer has been described. This obser-vation together with the longitudinal course ofthe lymphatic vessels in the submucous layercould explain the spreading of carcinoma cellsover a long distance before entering the regionallymph nodes both superiorly and inferiorly.The nerve supply of the esophageal muscles
is through both vagus nerves and theirbranches and the sympathetic nervous system.There are no muscle spindles in between thestriated muscle fibers. Stretching of the muscu-lar wall is detected by specific mechanorecep-tors which are similar to the Riffini bodies ofthe locomotor apparatus.The esophagus is enveloped and connected
with its surrounding structures by loose con-nective tissue, the tunica adventitia.
10 � D. C. Broering et al.: 1 Surgical Anatomy of the Esophagus

Conventional methods of examination
To judge the anatomy, the function, as well aspathologic findings in the esophagus, contrastesophagographies are needed. Applied contrastmedia are the barium swallow and water solu-ble contrast media. For the diagnostic routineexamination, viscous barium suspensions arerequired in order to judge motor disorders, themucous membrane, and lateral boundaries. Ifperforation, rupture or postoperative suturedehiscence is suspected, water soluble contrastmedia or contrast media used in bronchogra-phy should be taken. These contrast mediashould also be used in case of suspected eso-phago-tracheal fistula and where risk of aspira-tion is present. The double contrast of the eso-phagus can be improved by mixing the usualcontrast medium with gas, or if necessary withintravenous application of anticholinergic sub-stances.For the investigation of dysphagia, a 100 mm
camera should be applied or cinefluorography isrequired; with the use of these techniques, espe-cially proximal tumors can be demonstrated anddocumented. The patient can be examined in anupright or a lying position. The latter is used toslow down the passage of contrast media. To getan impression of the organs of the thorax, aroentgenoscopy should be performed first. Ab-normalities of the lungs, the diaphragm, andthe heart can be seen with the use of this tech-nique.The standard projections are frontal, right
oblique and lateral positions, as well as targetradiography in two planes of pathological or-gan regions. The esophagogram is the methodof first choice to detect diverticula, hernias,varices, and achalasia.
Diverticula
Depending on their origin pulsion-, traction-and mixed diverticula can be detected as wellas cervical, thoracic and epiphrenic diverticula.
� Cervical diverticula show a progression incomplaints with increasing size of the diverti-culum during the course of the disorder. Ini-tially the patients complain of a sensation of aforeign body and difficulty in swallowing.Congestion, regurgitation, and the linked dan-ger of aspiration take place only with progres-sion of disease. In the beginning the com-plaints may be misinterpreted as of cardiacorigin. Depending on its size, a diverticulumusually lies on the left side of the neck. Occa-sionally distension of the neck or even a palp-able tumor is evident. A diverticulum may becompressed in order to limit further filling.Posterior pharyngeal diverticula (Zenker’s di-
verticulum), in most cases, lie on the left handside. With progression of the disease, it mayreach such a size that the esophagus may becompressed and displaced. In this case, we referto a false diverticulum created by pulsation inthe region of Killian’s triangle. This is a regionwith a scarce amount of muscle above the M.cricopharyngeus, but it is more likely due to afailure of opening of the M. cricopharyngeus.It may occur as a result of an error in the coor-dination between the closure of the sphincterand the emptying of the pharynx. Piriform di-verticula fill during swallowing earlier than theesophagus and usually show a neck.These characteristically show retention of
food. Since the neck of the diverticulum is sit-uated quite cranially, the diverticulum is oftenseen as a mass lesion within air fluid levels inplain radiographs.
The Esophagus
Diagnostic Methods of Examination
G. Krupski, V. Nicolas
2

� Traction diverticula are usually found arisingfrom the anterior or lateral wall of the esopha-gus, at the level of the tracheal bifurcation.The cause is thought to be inflammatory,lymph nodes as a result of e.g. tuberculosis.This infiltrates the wall of the esophagus and,with remission of disease, a cricatricial retrac-tion of the esophagus wall occurs. The x-rayfindings tend to show clearly defined 0.5–1 cmdeep extrusions of the esophagus wall, usuallywith a pointed above and a broad basic. Trac-tion diverticula generally are incidental find-ings, since the patient usually has no symp-toms or suffers from non-specific symptomsonly. They can be missed on x-ray, if the ex-amination is performed in an upright positionwith a minimal filling of the diverticulum, orif a patient has not been examined in theoblique or lateral position especially if the di-verticulum is the anterior extrusions of theesophagus.
� Epiphrenic diverticula, as their name implies,are situated near the diaphragm arriving fromthe right posterolateral aspect of the esopha-gus. They develop due to mal- or dysfunctionof the esophagus. If the diverticula is in com-bination with achalasia, diffuse spasm of the
esophagus or hypertonic sphincter may be as-sociated findings. Dysphagia, nocturnal heart-burn due to emptying of the diverticulum inthe horizontal position, and epigastric abdom-inal pain are the resulting symptoms. The ab-sence of gastric mucosa in the diverticulum aswell as the connection to the esophagus allowsthe diverticulum to be differentiated from aprolapsed part of the stomach.
Achalasia
Dysfunction in the esophageal body and loweresophageal sphincter serve as a guide to theclinical picture of achalasia. The causativeagent of achalasia (cardio spasm, mega esopha-gus) is unknown. The rare mega esophaguscongenitus must be separated from the megaesophagus of achalasia. The predominant guid-ing symptom of achalasia is difficulty in swal-lowing. The sensation of food sticking orcramping pain is often projected retrosternallyor around the xiphoid process. As the diseaseprogresses the patients present with regurgita-tion and weight loss. There is a risk of aspira-tion and bronchopulmonary complications.
� G. Krupski, V. Nicolas12
Fig. 2.1. Typical depiction of a cervical esophageal diverticu-lum (Zenker) in a.p. and lateral projection after barium swal-low. On the lateral film the esophagus is compressed and
shows ventral displacement (�). Therefore, it can be classi-fied as stage II according to Brombard.

Depending on the severity of the disease, onplain chest x-rays broadening of the mediasti-nal silhouette located on the right side due toa distended esophagus may be visible. On thelateral view, the retrocardial space is often opa-cified and the trachea is anteriorly displaced.After the swallow there is a slow filling of thedilated esophagus and the barium contrast me-dium mixes with retained food resulting in aninhomogenous image. The esophageal wall ap-pears smooth. With varying prestenotic dilata-tion of the esophagus in its distal part, there isa smooth narrowing in the gastroesophagealjunction. To rule out a malignant stenosis, theproof of the continuity of the longitudinal eso-phageal fold is essential. Suction of remainingfood and additional application of glucagonsmay help to distinguish achalasia from otherconditions.
Gastroesophageal reflux and hernias
The term reflux disease summarizes clinicalfindings resulting from reflux of gastric acidand aggressive duodenal secretors into the eso-phagus. In association with food intake andposition of the body, the leading symptoms ofretrosternal pain or burning sensations as wellas projected pain in the epigastrium or throatare reported. The diagnosis of gastroesophagealreflux is primarily made from the typical clinicalfindings with proof of either reflux of inflamma-tory mucosal reactions being achieved by endo-scopy or radiology.The radiological examination of gastroeso-
phageal reflux or hiatus hernia is performedwith the patient head down or prone. Valsalvamaneuver followed by deep inspiration andcoughing can provoke gastroesophageal con-trast media reflux and herniation. The earlystage of the disease often lacks clear signs. Ad-ditional findings are disturbed motility (tertia1 contractions) and swollen folds. Evidence ofa short esophagus or hiatus hernia supportsthe diagnosis. Minor ulceration is not normallydetectable radiologically but is seen by endo-scopy. However more extensive ulceration is
seen as contour irregularities or a niche partic-ularly using a double contrast technique. Pep-tic stenosis resulting in a shortened esophagusand post-inflammatory scarring of the eso-phageal wall is the final stage of the disease.The involvement of the esophageal musculaturein the disease becomes obvious by spasticchanges in stenotic areas and disturbed motil-ity in prestenotic dilatation proximal to tubularstenoses. These causes reduce contrast mediaoutflow on x-rays.There are no specific clinical findings in hia-
tus hernia. Most of the patients are completelyfree of symptoms, and the hernia is detectedas an incidental finding in gastrointestinal ex-aminations for other reasons. Large herniasmay already have been diagnosed from a plainchest x-ray as translucencies in the right peri-cardial angle or retrocardial and paravertebralspace, respectively. The surrounding margin isformed by the gastric wall and shows varyingair fluid levels. Using oral contrast media, hia-tus hernias can be classified and clearly differ-entiated from hernias of the diaphragm. For asliding hiatus hernia the level of pretubularesophagus, gastroesophageal vestibulum, andSchatzki-ring (mucosal border of esophagusand stomach) (if present) as well as an intra-thoracic and infradiaphragmal stomach have tobe described. For all types of hernias (sliding,paraesophageal, mixed, upside-down-stomach)primary or acquired brachyesophagus has tobe ruled out prior to surgery.
Varices
The examination for the detection of esopha-geal varices is performed in a supine positionin expiration. Submucosal varices present withlinear, nodular, and pearly thickenings in thelower third of the esophagus. In the same ex-amination fundal varices in the stomachshould be ruled out as well. If varices are lim-ited to the upper third of the esophagus,thrombosis or stenosis of the SVC should beconsidered and further investigations such asCT or angiography are necessary.
2 The Esophagus � 13

Foreign bodies
The localization of ingested foreign bodies isan important radiological examination. Re-tained foreign bodies in the esophagus orthroat cause vomiting and coughing and maydisturb swallowing. Before using contrastagents plain x-rays should be taken from theneck and chest region in at least two planes.One has to look for air trapping in soft tissues,frontal positioning of the pharyngoesophagealsegment, broadening of the mediastinum, dis-turbed motility of the diaphragm, atelectasis,pleural effusion, or free intraperitoneal air asmarkers for complications of foreign body in-gestion. Most foreign bodies are trapped in theupper third of the esophagus by its strongmusculature. The esophageal lumen is flattenedat this level by the cricoid cartilage anteriorlyand at the 6th cervical vertebra posteriorly.Flat foreign bodies tend to become positionedin a frontal plane which plays an importantrole for the differentiation from tracheal for-
eign bodies because these tend to be posi-tioned in a sagittal plane. The precise localiza-tion of either endotracheal or esophageal for-eign bodies needs a lateral view. After oral ap-plication of water soluble contrast media, theforeign body becomes smoothly covered. Largeforeign bodies, such as a bit of meat, mightblock the contrast passage completely. Swal-lowing of a cotton pad previously dipped intocontrast media can enable visualization of pre-viously invisible foreign bodies. Apart fromthe direct demonstration of foreign bodies, theoral contrast application facilitates the detec-tion of associated mucosal ulceration, fistulas,or perforations which determine further thera-peutic approaches.
Esophageal tumors
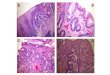
Dysphagia is the first und most common clini-cal sign of an esophageal carcinoma. Quiteoften the disease starts with uncharacteristicburning sensations or retrosternal pressurewhile swallowing. Surprisingly, patients can pre-cisely localize the level of obstruction. In con-trast to esophagitis or esophageal spasm, painsensations are well described and localized.The diagnosis of an esophageal carcinoma ismade by radiology, endoscopy, and biopsy.Characteristic findings in the esophagogram of-ten enable the differentiation between malignantand benign lesions. Depending on the extentand growth, the appearance may vary. Basedon x-ray morphology there are three maintypes:� Scirrhous carcinoma with intramural growthand early stenosis
� the ulcerated or medullary carcinoma withulceration
� the exophytic, polypoid carcinoma with intra-luminal growth and filling defect with irregu-lar surface at the periphery.
Plaque-like lesions are an early sign of an in-filtrating growth. For the detection of smalllesions, a multiplanar examination using dou-ble contrast is obligatory. Mucosal folds tendto be only slightly thickened and can be dis-rupted. There might be remaining contrast de-pots in lesions. In the early stages motility and
� G. Krupski, V. Nicolas14
Fig. 2.2. Esophageal varices: round-shaped filling defectslined up like pearls.

flexibility of the esophagus are normal. De-pending on their growth, advanced tumors re-sult in rigidity of the esophagus wall, destruc-tion of the normal fold architecture, intralum-inal filling defects, and stenoses with presteno-tic dilatation. Due to ulceration and loss ofsmall tumor parts, the radiological aspect canvary from examination to examination. Fibroustypes of the esophageal carcinoma are very dif-ficult to detect in the early stage because mini-mal wall deformities are easily missed. In theadvanced stages hourglass-like circular ste-noses develop which primarily have smoothmargins (increasing infiltration and ulcerationfinally leads to irregular contours).
� Benign esophageal tumors (0.6%) are rarecompared with malignant tumors. The presen-tation of symptoms and signs depend on thesite, extent, configuration, and growth direc-tion of the tumor. Most benign tumors areasymptomatic. Dysphagia is the leading symp-
tom for submucosal and intraluminal growthwhen the lumen becomes obliterated. Intra-mural and extraesophageal growth can lead tovery large tumor size before symptoms becomeclinically apparent (dysphagia, vomiting, retro-sternal pain). Depending on their growth pat-tern, benign esophageal tumors can be classi-fied as intraluminal (papilloma, adenoma, car-cinoid, hemangioma, fibrovascular polyp, gran-ular cell myoblastoma), intramural (leiomyoma)and cysts. After histological examination 50–70% of benign tumors are found to be leiomyo-mas which are located in the mid and lowerthird in 90% of cases. Radiologically they pres-ent with well defined round filling defects with-out disruption of the mucosa. Compared withthe normal esophagus there might be a slightflattening of the folds in the neoplastic area.Peristalsis is normal. With circular growth pre-stenotic dilatation and a mega esophagus canresult in rare cases. Sometimes, there is ulcera-tion which can be difficult to differentiate from
2 The Esophagus � 15
Fig. 2.3. Platelet-cell carcinoma of the thoracic esophagusdemonstrated in double-contrast technique. Apple-coreshaped filling defect of the otherwise adequately distendedesophagus with an irregular and ulcerated surface (�).
Fig. 2.4. Distal adenocarcinoma of the esophagus (Barrettcarcinoma) positioned in the esophagogastric junction. Asmall rim of the distal esophagus in the hiatus shows residu-al normal epithelial folds (�).

malignant lesions such as carcinomas or sarco-mas or polyps (a short course of the disease,weight loss and rapid deterioration with diffuseleiomyomatosis, diverticula, gastric carcinomaand a synchronous malignant lesion in benignesophageal tumors. Hence on barium swallowonly intraluminal growth can be observed. Peri-esophageal growth has to be demonstrated usingcross sectional imaging techniques: CT, MRI,and endosonography.
CT and MRI
Indications for a CT examination in esophagealdisease are: diagnosis of lymphatic and hema-togenous metastatic spread, periesophageal tu-mor extent, and tumor localization for irradia-tion. For the detection of the longitudinal ex-tent of a tumor the esophagogram is superior.The application of water soluble oral contrastmedia for the demonstration of the esophageallumen has shown to be of value. In the CT in-filtrative or medullary growing scirrhous carci-nomas might present with a thickening anddemarcation of the periesophageal tissues.Proximal to a stenotic tumor a fluid-air levelcan be seen. In polyploidy growing tumors theintraluminal tumor or an eccentric wall thick-ening might strike ones eyes. Wrong estima-tion of tumor size and lymph node staging arecommon in cachectic patients or after surgeryand irradiation, respectively. In cachectic pa-tients the differentiation of the esophagus fromsurrounding tissues might be almost impossi-ble due to reduction of mediastinal fatty tissue.In this situation the missing fat pad does notnecessarily suggest an infiltration of the adja-cent structures or vessels. The 90� rule is helpfulto decide whether there is a vascular infiltration:if the contact area of tumor and aorta lies above1/4 of the circumference of the vessel (whichequals an angle of 90�) there is an infiltrationof the aorta in 80% of the cases. However, withan area less than 45� (1/8 of the circumference)there is no infiltration to be expected. Preopera-tive irradiation leads to increased fatty tissuedensities and therefore impossibility to differ-entiate such changes from infiltration.
With the introduction of multislice CT-imag-ing slight improvements in the imaging of eso-phageal tumors could be achieved for primaryand secondary staging as well as detection ofdistant metastasis (Figs. 2.1–2.3). Neverthelessthis still cannot be called a true breakthrough.Indications for MRI are equal to CT, but cor-
onal and sagittal image planes allow sufficientdifferentiation for longitudinal tumor extent de-finition. Nevertheless, in all publications to date,there is no evidence that MRI is superior to CTin the imaging of malignant esophageal disease.Since the T1 and T2 weighted images, esopha-geal musculature is equal to skeletal muscle ora good differentiation from tumor can be ex-pected in T2 weighted sequences. However,due to low signal to noise ratios and motion ar-tifacts in long acquisitions, the anatomical spa-tial resolution is worse. To enhance the differ-ences in relaxation of tumor and surroundingtissue the application of i.v. Gadolinium DTPAcan be advantageous. Because of diaphragmaticmotion, particularly the inferior part of the eso-phagus and the esophagogastric junction aredifficult to image on MRI (Figs. 2.4–2.6).The lymphatic spread of malignant esopha-
geal tumors follows the esophageal wall to lo-coregional paraesophageal lymph nodes. De-pending on the localization of the tumor, low,cervical and supraclavicular lymph node sta-
� G. Krupski, V. Nicolas16
Fig. 2.5. Cross-sectional CT-image of the thorax in a patientwith esophageal platelet-cell carcinoma (same case as in Fig.2.3.). After barium swallow, a narrowed residual lumen isvisible (�) surrounded by tumor mass.

tions have to be included in CT examinations.They can be visualized from 5–10 mm depend-ing on slice thickness. Normal lymph nodesmay reach a diameter of up to 10 mm. Diame-ters above 15 mm are suspect for metastatic
infiltration but cannot be differentiated fromreactive lymph node enlargement in e.g. asso-ciated pulmonary diseases.In the literature the accuracy for the T-stag-
ing in CT is 60% and 47–74% for the N-stag-
2 The Esophagus � 17
Fig. 2.6. T1-weighted axial and sagittal MR images of themid esophagus in a patient with platelet-cell carcinoma
(same patient as in Figs. 2.3 and 2.5). In both planes the tu-mor extent can clearly be outlined (�).
Fig. 2.7. Axial T2-weighted MR image in a patient withproximal platelet-cell carcinoma of the esophagus presentingwith suspicious paratracheal lymphoma. In addition, there isan infiltration of the pars membranacea of the trachea (proven
by tracheoscopy and biopsy) best seen on the left image(disruption of the low signal intensity outer margin of thetrachea). The tumor has to be staged as T4 N2.

ing, whereas endosonography is doubtlessly bet-ter with an accuracy of 73–95% and 73–80%, re-spectively. Although the accuracy of CTand MRIis insufficient for N- and T-staging, in esopha-geal malignant disease both are obligate for de-tection of hepatic and pulmonary metastases.
� Perspectives in imaging
New imaging techniques are subsequently in-troduced and applied in the diagnosis of eso-phageal disease. Promising first results werepresented using e.g. intraluminal MRI probesand PET (Figs. 2.7, 2.8). The latter seems tobear a certain impact on early detection ofnon-responding tumors undergoing neoadju-vant treatment regimes.
18
� Fig. 2.8. Sagittal T1-weighted image of a large esopha-geal carcinoma from a modern 1.5 T MRI: both proximaland distal tumor borders are visible.
Fig. 2.9. Sagittal T1-weighted MR images in advanced eso-phageal carcinoma of the middle third. Both tumor massand pulmonary metastases of the left apical lung lobe aswell as multiple suspicious lymph nodes are displayed with asolitary sequence.�
� G. Krupski, V. Nicolas: 2 The Esophagus

Introduction
Endoscopy is well established in the evaluationof esophageal disease. With the widespreadavailability of endoscopy in nearly every hospi-tal around the world, it has largely supplantedradiological examination as the primary inves-tigation of choice. The major advantage overradiological examination is that the endo-scopist can directly visualize the mucosa andobtain targeted biopsy specimens. Further-more, endoscopic treatment (e.g., balloon dila-tation for achalasia or stent inception for eso-phageal carcinoma) can often be performedimmediately after the diagnostic examination.Conventional endoscopy has most recentlybeen complemented by endoscopic ultrasonog-raphy, which adds a new dimension to endo-scopic diagnostic capability. Using an endo-scope equipped with a miniaturized ultrasoundtransducer at its tip (echoendoscope), or cathe-ter ultrasound probes (‘miniprobes’) that canbe inserted through the working channel of astandard endoscope, the endoscopist is able tosonographically “look” into and beyond theesophageal wall.
Equipment and normal anatomy
Videoendoscopes that use an electronic CCD(charge-coupled device) or chip for generationof an image are rapidly replacing the older fi-beroptic endoscopes. The videoendoscopesproduce clear high-resolution color images ofthe luminal wall lining that are displayed on atelevision monitor. Since videoendoscopicimages can be viewed by multiple observers, ithas improved coordination between endosco-
pist and assistant, such as the timely openingand closing of biopsy forceps. Videoendoscopyhas also significantly improved the teaching ofendoscopy.The normal color of the wall is a pale sal-
mon pink. On close inspection, tiny vesselscan be seen shimmering through the mucosa.Small whitish papules are commonly some-times seen along the mucosa and represent abenign entity without clinical significance (gly-cogenic acanthoses). In the proximal esopha-gus an isolated patch of reddish mucosa maybe seen, which histologically represents hetero-topic gastric (columnar) mucosa. The upperand lower esophageal sphincters (at approxi-mately 15 cm and 40 cm from the incisors, re-spectively) can be recognized endoscopically asregions of luminal constriction that can be eas-ily passed with gentle advancement of the en-doscope. Occasionally, neighboring organssuch as the aorta can impinge on the esopha-gus and cause mild luminal narrowing. Thismay mimic a submucosal tumor. In this caseendosonography is helpful.The transition of the squamous epithelium
of the esophagus to the columnar epitheliumof the stomach is always sharp and readilyidentified by an abrupt change in the colorand appearance of the mucosa from a glossypale pink (squamous epithelium) to a velvetydeep red (columnar epithelium). This transi-tion is referred to as the Z-line, derived fromits irregular zig-zag appearance.
Malignant tumors
Because esophageal carcinoma originates fromthe mucosal layer, it is easily recognized onendoscopic examination. Patients usually pre-
Endoscopic Examination of the EsophagusK.F. Binmoeller, B. Brand, N. Soehendra
3

sent at an advanced stage of disease when ste-nosis has resulted in dysphagia and weightloss. Most esophageal malignancies are squa-mous cell carcinoma, but the incidence of ade-nocarcinoma has been steadily rising. The en-doscopic appearance may vary, but typicallypresents as a lumen-occluding ulcerating poly-poid lesion. There is often increased vascular-ity and contact friability. The sudden onset ofa coughing spell or respiratory distress duringendoscopy should alert the endoscopist to thepossibility of an esophago-tracheal fistula,which can be confirmed by a radiographic gas-trograffin study or bronchoscopy. Stenosing tu-mors that cannot be traversed with a thin-cali-ber endoscope (e.g., pediatric gastroscope) willrequire preliminary bougienage, which shouldbe done cautiously in graduated steps. Rarely,a diffusely infiltrating scirrhous cancer maypresent as thickening and rigidity of the eso-phageal wall of variable length. This may befalsely interpreted to represent fibrosis ofchronic esophageal reflux disease. It is impor-tant to recognize that the visible tumor maynot represent its true extent. A tumor mayspread submucosally and even establish satel-lite lesions far removed from the primary le-sion.Although carcinomas are easily accessible to
endoscopic biopsy and brushings for histocy-tological confirmation, the diagnosis may bemissed if faulty biopsy technique is used. Mul-tiple biopsies and brushings should be takenfrom different sites of the tumor, avoidingareas of obvious necrosis. When 6 to 10 biopsyspecimens are obtained, the diagnostic accu-racy has been reported to be around 80%. Thetype of forceps selected may improve the tissueyield; if possible, large-cupped biopsy forcepswith a needle should be used. Forceps thatopen laterally are preferable for flat lesions thatare approached tangentially.Endoscopic detection of early or superficial
cancer in the esophagus is difficult to diagnoseand is often overlooked in the asymptomaticpatient. Their detection requires mass screen-ing programs, as have been established in Ja-pan where the incidence is around 40% (com-pared to <5% in Europe and the United Stateswhere screening is absent). In line with the Ja-panese experience, early malignancy is subdi-vided into three main macroscopic types ac-
cording to the tumor’s height in relation to theneighboring normal epithelial surface:� Type I, elevated or protruded type� Type II, superficial flat type� Type III, depressed or excavated type.
Type II is divided into three subtypes:� Type IIa, flat with elevation� Type IIb, flat without elevationor depression
� Type IIc, flat with depression.
The typical appearance of an early cancer is acircumscribed polypoid lesion (Type I), butthe lesion may appear as a patch of mucosaldiscoloration (Type II).Chromoscopy using dye stains such as Lu-
gol’s solution and methylene blue may be usedto facilitate the detection of early carcinomasor Barrett’s epithelium. Lugol’s solution stainsglycogen components of normal nonkeratin-ized squamous epithelium and will fail to stainseverely dypsplastic and carcinomatous tissue(“negative staining”). Methylene blue stains ab-sorptive epithelium and will identify regions ofintestinal metaplasia or dysplasia [3].
Benign tumors
Benign non-epithelial tumors include leiomyo-mas, lipomas, granular cell tumors, neurofibro-mas and fibrovascular tumors. All of these typ-ically appear on endoscopic examination as a“submucosal” tumor, i.e., a rounded, raisedmass with normal appearing overlying mucosa.The most common benign tumor of the eso-
phagus is a leiomyoma, which arises fromsmooth muscle cells in the mucularis propriaor less commonly the muscularis mucosa. Pal-pation of this solid mesenchymal tumor withan endoscopic accessory (e.g., closed biopsyforceps) reveals the submuscosal lesion to befirm in consistency. The overlying mucosa isnormal and can be moved against the underly-ing tumor. Forceps biopsies are usually toosuperficial to establish a diagnosis.Hemangiomas, composed of numerous cap-
illary or cavernous channels lined with endo-thelial cells within the mucosa or submucosa,
� K. F. Binmoeller et al.20

typically appear as a nodular mass with a blueor plum hue. In contrast to leiomyomas andother mesenchymal tumors, they are soft to in-strumental palpation. Endoscopic biopsies ofthese lesions have been reported without sig-nificant bleeding.EUS is the procedure of choice to evaluate
submucosal lesions. EUS is capable of definingthe origin of the lesion relative to the histolog-ic layers of the gastrointestinal tract and theextent of its spread. Genuine submucosal tu-mors can be distinguished from extramuralstructures that can compress the esophagealwall and thereby mimic a submucosal tumor(e.g., aorta, bronchogenic cyst, lymph node).Although EUS cannot provide a histologic di-agnosis, the layer of origin and the echogeni-city of the lesion are often highly suggestive ofthe diagnosis. Leiomyomas present characteris-tically as a well demarcated hypoechoic massoriginating from the muscularis propria ormuscularis mucosae layer (Fig. 3.1). A leiomyo-ma can be differentiated from a leiomyosarco-ma with reasonable certainty by assessing so-nographic features such as size, homogenicity,and margins, and following these featureslongitudinally over time. Lipomas are typicallywell demarcated hyperechoic structures origi-nating from the submucosal layer.
Esophagitis
Gastroesophageal reflux disease (GERD) leadsto inflammation of the esophageal mucosa thatcan be detected on endoscopy. The most reli-able endoscopic markers of inflammation areerosions and ulcers. Erythema alone is often anonspecific finding and poorly reproducibleamong examiners. Numerous classificationschemes have been proposed to grade the sev-erity of esophagitis, but the most commonlyused is that of Savary Miller:
0 normal1 Erythema or edema2 noncircumferential erosions3 Circumferential erosions4 Ulcerations
Savary Miller stage ‘0’ is GERD without endo-scopic evidence of esophagitis. The diagnosisof GERD is established by histologic evidenceof esophagitis or 24-hour pH manometry. Re-flux is usually acid in nature, but may be alka-line, such as after a partial Billroth-II gastrec-tomy.Complications of GERD include ulcerations,
peptic stenosis, and Barrett’s esophagus.GERD is often associated with a hiatal her-
nia, which may contribute to incompetency ofthe lower esophageal sphincter. The axial slid-ing hernia is the most common type, but occa-sionally a paraesophageal hernia (stomach fun-dus herniated into the thorax alongside theesophagus) is encountered, of which the “up-side-down” stomach is an extreme variant.Endoscopy is the method of choice for the
detection of nonreflux-induced esophagitis.The most common cause of infectious esopha-gitis is Candida. The diagnosis is usually sug-gested by the typical endoscopic appearanceshowing multiple isolated or confluent yellow-whitish plaques. The proximal esophagus ispreferentially involved. At an advanced stage,these plaques become circumferential and mayresult in luminal narrowing. The diagnosis isestablished by brush cytology.Viral esophagitis due to cytomegalovirus
(CMV) and herpes simplex virus (HSV) causemucosal ulcerations. The appearance can varyconsiderably depending on the cause of immu-nodeficiency and severity of disease. The ear-
3 Endoscopic Examination of the Esophagus � 21
Fig. 3.1. Benign leiomyoma; hypoechoic mass originating fromthe muscularis propria or muscularis mucosae layer.

liest lesion of HSV is the vesicle, usually seenin the oropharynx, but occasionally encoun-tered in the esophagus. HSV ulcers are superfi-cial and often scattered throughout the esopha-gus. By contrast, CMV ulcers tend to be largeand more well-circumscribed with sparing ofintervening mucosa. Brushings of HMV lesionsfor cytology are usually diagnostic, whereasthe diagnosis of HMV requires large forcepsbiopsies taken from the ulcer base.
Complications of esophagitis
� Peptic strictures. Peptic strictures may occurin as many as 10–20% of patients with chronicGERD. The endoscopic appearance is typicallythat of a concentrically fixed narrowing thatdoes not distend with air insufflation at orslightly above the level of the cardia. The lengthof the stricture is rarely greater than 1–2 cm,and the mucosa appears scarred. Inflammatorymucosal changes are usually present.Tissue sampling is mandatory to exclude
malignancy.
� Barrett‘s esophagus. Barrett’s esophagus isdefined as metaplastic change of squamousepithelium to columnar lined epithelium causedby chronic GERD. The diagnosis is a histologicalone and requires the identification of gobletcells on histopathology to establish the presenceof intestinal metaplasia. The entity is more com-mon in men than women, and the frequency ofBarrett’s esophagus in patients undergoingendoscopy for clinical indications approaches1% for men [1, 2]. The entity is widely regardedas pre-malignant owing to a risk of developingcancer that is 30- to 100-fold higher than healthycontrols. However, the actual likelihood of an in-dividual with Barrett’s esophagus over a lifetimeis difficult to define. Prospective series define anincidence of adenocarcinoma ranging from 1 in52 patient years of follow-up to 1 in 278 patientyears. The prognostic significance of Barrett’sesophagus will depend on whether dysplasia ispresent and what the estimated life expectancyis (patient’s biological age and comorbid condi-tion). Barrett‘s esophagus has received greaterattention in recent years due to the rising inci-
dence of adenocarcinoma relative to squamouscell carcinoma of the esophagus.Barrett’s esophagus should be suspected
when the squamocolumnar junction (Z-line) isproximally displaced from the gastroesopha-geal (GE) junction. This may be difficult to di-agnose when the Z-line is obscured – as maybe the case with accompanying inflammation –or the GE junction is obscured – as may bethe case with an accompanying hiatal herniaor tortuous anatomy. Barrett’s epithelium typi-cally appears as “tongues” of velvety red muco-sa that extends into the tubular esophagus.However, a long circumferential segment ofBarrett’s can mimic normal squamous epithe-lium.Barrett’s esophagus has been defined in the
past as metaplastic tissue extending 3 cm intothe tubular esophagus. However, recently “shortsegment” (<3 cm) and “ultrashort segment” (atthe gastric cardia) Barrett’s esophagus have beenfound to have malignant potential. Endo-scopically inapparent but histologically con-firmed Barrett’s metaplasia has received greaterappreciation as endoscopists have begun to sys-tematically evaluate for Barrett’s with biopsies.The use of vital dyes such as methylene or tolui-dine blue, which specifically stain intestinalizedepithelium, can help to identify Barrett’s change.
Varices and other sourcesof upper gastrointestinal bleeding
In the patient with upper gastrointestinal bleed-ing, endoscopy is indicated as a first-line proce-dure to localize the bleeding source. Vomiting offresh blood suggests variceal bleeding as themost likely source. Other less frequent sourcesmay be hemorrhagic esophagitis or a Mallory-Weiss tear, the latter a linear mucosal tear atthe cardia caused by violent retching. A deeptear may result in perforation (Boerhaave’s syn-drome) with signs of mediastinitis or media-stinal emphysema. Hematemesis may also becaused by swallowed blood from the nose or hy-popharynx, mimicking gastrointestinal bleed-ing.Dilated esophageal veins may be seen in pa-
tients with portal hypertension and do not
� K. F. Binmoeller et al.22

pose any risk for bleeding. By contrast, visiblevarices may rupture and bleed, as they are lo-cated in the mucosa (lamina propria mucosa).Varices are typically seen in the lower third ofthe esophagus and are categorized accordingto their risk of bleeding in 3 grades:� Grade 1: discretely protruding into the lumen� Grade 2: protruding into the lumen and per-sisting even after maximal insufflation of air
� Grade 3: filling the variceal lumen with nonormal mucosa between columns.
Additional signs that correlate with an in-creased risk of bleeding are red spots overvarices (‘red color signs’) and small venulesover varices (‘blue wale sign’).
Esophageal varices are usually a complicationof portal hypertension (pre-, intra- and posthe-patic block). Rarely, varices may complicatemediastinal compression with obstruction ofvenous emptying (‘down-hill’ varices in theupper third of the esophagus). In northernEurope portal hypertension is most commonlycaused by alcoholic liver cirrhosis and in south-ern Europe by posthepatic cirrhosis (especiallyhepatitis B and C). Portal hypertension causedby a liver tumor is characterized by recurrentbleeding.Endoscopic hemostasis is the procedure of
choice for acute variceal bleeding. The injec-tion of Histoacryl (Braun-Melsungen) to oblit-erate the bleeding varix is the best endoscopictreatment [4]. After hemostasis is achieved, en-doscopic ligation with rubber bands and para-variceal sclerotherapy are well established aseffective treatments to prevent variceal rebleed-ing, the risk of which is very high and asso-ciated with significant mortality. After varicealeradication, endoscopic follow-up examinationsare indicated to treat new varices. Varices thathave not previously bled are generally treatedby beta-blockers to prevent first-time bleeding.Variceal band ligation is undergoing investiga-tion as a possible treatment for the primaryprevention of variceal bleeding.
Diverticula
Diverticula are outpouchings of the esophagealwall. True diverticula comprise all layers of theesophageal wall (e.g., the typically asympto-matic mid-esophageal traction diverticula),whereas pseudodiverticula are herniations ofthe mucosa through the muscle layer (e.g.,Zenker diverticula of the proximal esophagus,whereby the diverticulum protrudes posteriorlythrough the muscle fibers of the Kilian triangleand can cause severe symptoms of dysphagiaand regurgitation of food). Epiphrenic divertic-ula are often found in association with eso-phageal motility disorders (see below).
Achalasia and other motor disorders
Endoscopy is a relatively insensitive method forassessing esophageal motility disorders, as theanatomy and mucosal lining of the esophagusdo not show pathognomonic changes. However,the diagnosis may be suggested in advancedcases. Achalasia, an acquired neurodegenerativedisease of the esophagus, in which there is a se-lective loss of inhibitory neurons to the ganglioncells of the Auerbachs plexus, has several char-acteristic findings. Firstly, the esophagus proxi-mal to the gastroesophageal (GE) junction maybe dilated and filled with food or secretions.Stasis may result in varying degrees of inflam-matory changes. Secondly, the GE junctionmay show a puckered appearance without evi-dence of fibrosis or tumor. Characteristically,the endoscope will “pop” through the tightopening with pressure. It is imperative to distin-guish primary achalasia from secondary achala-sia due to malignancy involving the cardia. Thecareful examination of the cardia region, includ-ing a retroflexed view from the stomach, is re-quired, and biopsies should be liberally takenfrom any suspicious area.
3 Endoscopic Examination of the Esophagus � 23

As a rule, manometric studies should beobtained to confirm the diagnosis of primaryachalasia. Manometric studies may also sug-gest other motility disorders such as diffuseesophagospasm, nutcracker esophagus, orsclerodermia, all of which can mimic achalasia.It must be emphasized that motility disordersare a diagnosis of exclusion, and that all pa-tients should undergo an endoscopy to excludemalignancy and GERD. The diagnosis of refluxdisease is of importance, as this can be easilyand effectively treated.
References
1. Cameron AJ, Zinsmeister AR, Ballard DJ, Carnen JA(1990) Prevalence of columnar-lined (Barrett’s) eso-phagus. Comparison of population-based clinicaland autopsy findings. Gastroenterology 99:918–922
2. Eloubeidi MA, Provenzale D (2001) Clinical and de-mographic predictors of Barrett’s esophagus amongpatients with gastroesophageal reflux disease: a mul-tivariable analysis in veterans. J Clin Gastroenterol33(4):306–309
3. Shim CS (1999) Staining in gastrointestinal endo-scopy: clinical applications and limitations. Endo-scopy 31:487–496
4. Soehendra N, Grimm H, Nam VC, Berger B (1987)N-butyl-2-cycinoacerylate: a supplement to endo-scopic sclerotherapy. Endoscopy 19:221–224
24 � K. F. Binmoeller et al.: 3 Endoscopic Examination of the Esophagus

Introduction
Despite radical and aggressive combination che-motherapy, the prognosis for esophageal cancerremains poor.Any decision about the best and/or most
suitable treatment with curative or palliativeintent is dependent on the depth of penetrationof the primary tumor and on the presence orabsence of local or distant lymph node meta-stases.Computer tomography remains the “gold
standard” for pre-operative staging of esopha-geal cancer. Measurements of wall thicknessserve as criteria for depth of invasion by theprimary tumor. A wall thickness of less than1 cm is classified as T1–T2 and a wall thicknessgreater than 1 cm as T3. The limited spatial re-solution of CT and its inability to visualize thelayers of the esophageal wall make it unreliablefor detection and staging of early cancers,although the accuracy of CT improves in ad-vanced disease.To improve preoperative staging, including
evaluation of depth of invasion and involve-ment of local nodes, it is necessary to use animaging technique that is able to resolve thedifferent layers of the esophageal wall, as wellas the surrounding tissues. Over the past 20years endoscopic ultrasound (EUS) has devel-oped and become established as a high-resolu-tion technique for the evaluation of upper gas-trointestinal lesions. At present it is the onlyimaging modality able to demonstrate the de-tailed anatomy and layers of the esophagealwall. This allows correct tumor staging, whichcan be correlated with the post-operative his-tology.In many centers it is now standard practice
to perform precise staging with endoscopic ul-
trasound after CT has been obtained. Also, en-doscopic ultrasound has emerged as the mostimportant new tool for pre-operative treatmentdecision.
Principles of EUS tumor staging
Endoscopic ultrasound with 5–10 MHz probesenables visualization of 5 different layers of thewall of the upper gastrointestinal tract, whichmakes tumor staging (T-staging) according tothe UICC TNM classification possible [4, 5, 82](Table 4.1, Fig. 4.1). The T-staging is based onthe definition of “normal” and “destroyed or ab-normal” wall structures [6]. The normal ana-tomical wall structures consist of two mucosallayers (echorich and echopoor), an echorichsubmucosal layer and an echopoor muscle layer.Sometimes the echorich adventitial layer can bevisualized (Fig. 4.2 a,b). Malignant T1 or T2 tu-mors appear as echopoor lesions within the nor-mal mucosal layer leaving the submucosal and/or muscle layers intact. Once the echopoor le-sion extends through the muscle layer the tumor
Role of Endoscopic Ultrasound for Diagnosisand Staging of Esophageal CancerA. Fritscher-Ravens, M.X. Pelling
4
Table 4.1. TNM classification and stage grouping of esopha-geal carcinoma
� Tx – Primary tumor cannot be assessed
� T0 – No evidence of primary tumor
� Tis – Carcinoma in situ
� T1 – Tumor invades lamina propria or submucosa
� T2 – Tumor invades muscularis propria
� T3 – Tumor invades adventitia
� T4 – Tumor invades adjacent structures

� A. Fritscher-Ravens, M. X. Pelling26
Fig. 4.1. a T1 sm; b T2; c T3; d T4.
Fig. 4.2. a Echo rich submucosal layer and echo poor musclelayer; b configuration of the layers.
a
b
a b
c d
L. muscularis mucosaeL. submucosa
L. muscularis propriaAdventitia
Echoendoscope
Water-filledballon

is defined as T3 (Fig. 4.1). If there is invasion ofadjacent organs, such as the trachea or dia-phragm, it is defined as T4.Although usually well visualized these tu-
mors can be difficult to stage correctly. Thereis often edema around the lesion, which hassimilar echogenicity as the tumor itself andcan lead to overstaging. Tumor understagingwith endoscopic ultrasound is rather rare[7, 8].Endoscopic ultrasound can penetrate about
5–7 cm, allowing visualization of the posteriormediastinum, celiac axis, part of the liver, thespleen and the body of the pancreas. Conse-quently in addition to T-staging it is possibleto stage local nodes larger than 3–5 mm (N-staging) [9, 10] as well as some distant meta-static nodes (M-staging), in particular celiacaxis nodes. Assessment of these distant nodesis most important if primary surgery withcurative intent has been planned.Tytgat and Tio [11] attempted to define EUS
criteria for “normal” and “metastatic” lymphnodes in the presence of malignant disease.Criteria such as size, echogenicity, roundshape, and smooth borders were used to classi-fy nodes. Published data show an accuracy ofup to 80% using this classification. However,this does not allow reliable differentiation ofbenign and malignant involvement [12, 13],and CT or EUS guided needle aspiration of de-tected nodes is required if these would changethe treatment plan. This applies particularly toceliac axis nodes.
Examination techniqueand instrumentation
Esophageal cancers are generally examinedwith mechanical or electronic radial echoendo-scopes with shaft diameter of 11.5–13 mm andprobes switchable from 5 to 10 MHz (Fig. 4.3,left). The mechanical echoendoscopes are side-viewing and have a 360� ultrasound image(Olympus Optical Inc, Tokyo, Japan). Newerelectronic radial echoendoscopes are forwardviewing and have color Doppler ultrasound.
A water filled balloon is mounted on the tipof the scope for better acoustic coupling to thebowel wall, which is sometimes needed to ob-tain optimal ultrasound images. Radial echoen-doscopes have a scanning plane perpendicularto the endoscope and create images of the eso-phagus and surrounding structures in thesame projection as axial CT. As a consequencethe structures seen on EUS are moderatelyeasy to recognize even for examiners notexperienced in interpretation of ultrasoundimages. Consequently, evaluation and inter-pretation of pathologies is quite easily learnt(Fig. 4.4).Unfortunately at the time of presentation
many esophageal tumors are already quite ad-vanced in the lumen, preventing passage of themain echoendoscopes. A special tapered echo-endoscope, “the esophagoprobe”, with a shaftdiameter of only 7.9 mm has been developedfor these patients (GF MH 908, Olympus OpticalCo., Tokyo, Japan) (Fig. 4.3, centre) [14, 15].For very small and superficial or highly ste-
notic tumors, miniprobes are available. Theseare mechanical catheter-like 2.4 mm probeswith a 360� view. They cannot be used inde-pendently but are operated through the acces-sory channel of a gastroscope (Fig. 4.3, right).The depth of penetration of these catheterprobes varies from a maximum of 1.8 cm for
4 Role of Endoscopic Ultrasound for Diagnosis and Staging of Esophageal Cancer � 27
Fig. 4.3. Echoendoscopes.

the 20 MHz probe (UM 3R, Olympus OpticalCo., Tokyo, Japan) to 2.9 cm for the 12 MHzprobe (UM 2R, Olympus Optical Co., Tokyo,Japan). If necessary an additional water filledcatheter sleeve can be used for better acousticcoupling. The higher resolution of these highfrequency probes allows up to 7–9 layers to beseen in the wall of the bowel [16]. For endo-scopic ultrasound guided fine needle aspiration(EUS-FNA) electronic linear array echoendo-scopes with a 100–180 degree sector parallel tothe long axis of the endoscope are available(Pentax GmbH, Hamburg, Germany; OlympusOptical Co., Tokyo, Japan; Toshiba, Tokyo, Ja-pan) (Fig. 4.5).The anatomical views seen with linear endo-
scopic ultrasound are quite different to thosewith radial echoendoscopes. Reliable identifica-tion of anatomical landmarks and pathologytakes some time, and there is a rather longerlearning curve [17]. A major advantage of thelinear system over the radial is the ability tovisualize the entire length of a biopsy needleadvanced through the accessory channel. Theneedle can be seen endoscopically as itemerges from the channel and can then be fol-lowed on ultrasound in real time as it ispushed through the bowel wall into the targettissue. The needle can be advanced and re-tracted under direct ultrasound visual control.For fine needle aspiration 170 cm long 19–
22 gauge needle systems are commercially
available. These can be securely screwed ontothe accessory channel of the endoscope [18].Color Doppler ultrasound can be used to iden-tify and avoid vessels in the path of the needle.With this technique it is possible to samplenodes as small as 5 mm adjacent to large ves-sels or the heart. The fine needle aspiration isperformed through the esophageal or gastricwall and does not leave any visible mark in thegut wall. Generally 22 gauge needles are usedto obtain cytology. If histology is necessary,particularly for suspected GIST tumors ornon-Hodgkin’s lymphoma, a 19 gauge needle isavailable. These are similar to the smaller nee-dles but are more rigid and slightly more diffi-cult to handle, so they should be reserved forcases where cytology might not be sufficient.
� A. Fritscher-Ravens, M. X. Pelling28
Fig. 4.4. a Evaluation of pathologies and structures; b interpretation of pathologies and structures.
Fig. 4.5. EUS-FNA echoendoscopes.
a b
Echoendoscope LN
Lymph node (LN)
Water-filledballon
azygos vein Thoracic duct
Aorta

The complication rate with these larger needleshas not been established but is likely to behigher [19].
EUS compared to other imaging techniques
Several earlier studies compared the accuracyof CT and EUS in the staging of esophagealcancer. EUS correctly staged the primary tu-mor in 76–88% and nodes in 70–86%. CT inthe same patients was significantly less accu-rate correctly staging the primary tumor andnodes in 43–59% and 46–58% respectively [2,8, 20, 24, 26, 27].Newer studies using helical or multi-slice CT
showed slightly improved results. Of 60 patientswith esophageal cancer who underwent pre-op-erative CT and EUS, sensitivities for T and Nstaging were 58% and 79% for CT and 72%and 91% for EUS, respectively (Figs. 4.6, 4.7).Specificity for both T and N stages was 80%and 84% for CT and 85% and 68% for EUS, re-spectively [28]. The impact of the tumor stageon final therapy was assessed in 125 patients.CT was less accurate (51%) than EUS (74%)for nodal staging. EUS-FNA further improvedthese results [29].In recent years Positron Emission Tomogra-
phy (PET), a new imaging technique, has beenintroduced to overcome some of the shortcom-ings of CT for staging. This technique relies onincreased uptake of the positron emitting glu-cose analogue by neoplastic tissue and has the
advantage over conventional imaging of not re-lying only on anatomic imaging. Recent studiescomparing CT, PET and EUS showed sensitiv-ity for T staging of 83–95% for PET, which wassimilar to EUS but higher than for CT (67%).Sensitivity for local N staging was 33–37–55%for PET compared to 69–81–89% for EUS.However the specificity for local node involve-ment was 89–100% with PET and only 54–67%for EUS, while accuracy was 63% for PET, 66%for CT and 75% for EUS [30–32]. These dataclearly suggest EUS is superior to PET forstaging local nodes. The relatively low specific-ity of EUS imaging alone can be improved byperforming FNA during the procedure. PETdetected distant metastases in 47% and CT in33%, while EUS cannot be used for distant dis-ease other than celiac nodes [30].CT and PET add important information
about possible distant metastases, and particu-larly CT remains an important imaging tech-nique for the staging of esophageal cancer. Itis readily available, relatively inexpensive, andfees are usually reimbursed. PET has a highspecificity for nodal involvement and thereforemay be indicated in selected cases. Wallace etal. compared the health care cost and effective-ness of all three imaging techniques for stagingesophageal cancer in the USA. CT and EUS-FNA was the most inexpensive strategy andoffered more quality-adjusted life-years thanother strategies. PET+EUS-FNA were slightlymore effective but also more expensive [33].All in all CT and EUS are complimentary tech-niques for the staging of esophageal tumors,
4 Role of Endoscopic Ultrasound for Diagnosis and Staging of Esophageal Cancer � 29
a b
Fig. 4.6. a T2-tumor, N1-status; b schematic demonstration of the pathologies and structures.
LNL. musc. propria
Tumor Aorta
Thoracicduct
azygos vein

and PET may add additional useful informa-tion in certain cases where there is uncertaintyabout nodal involvement.
EUS and tumor stenosis
A prerequisite of a complete EUS examinationis that the esophageal tumor allows the scopeto pass into the stomach. If there is a tight ma-lignant stenosis it may be impossible to passthe echoendoscope. Stenoses are present in 25–36% of tumors at the time of diagnosis [2, 34–36], and in most of these cases EUS evaluationis limited and incomplete. Images exclusivelyobtained from the proximal part of the tumorare not representative of the entire tumor, andcorrect T staging is possible in only 32% com-pared to 81% if the scope can pass (34%).In general patients with tight strictures due
to esophageal cancer have a higher tumorstage (T3–T4) and a less favorable prognosis.To be able to identify at EUS those strictureswith a lower T stage suitable for curative sur-gery, endoscopic dilatation would be required.Despite controversial results such dilatation isnot recommended only for imaging as the riskof perforation is as high as up to 25% [35, 36].To reduce the risk of perforation in tight
strictures a small calibre tapered echoendo-
scope has been developed, the esophagoprobe,which has a shaft of only 7.9 mm and a slip-pery tapered metal tip (Fig. 4.3, middle) [14,15, 37]. As it has no optics it has to be intro-duced over a guide wire, which is advancedinto the stomach via a small calibre gastro-scope prior to the EUS examination. Guidedby the wire the echoendoscope can passblindly through even the narrowest stenosis asthe tapered tip serves as a dilator. A minor en-doscopic dilatation is only rarely necessary[15]. Using this probe correct T staging is pos-sible in up to 89% and N staging in 79%. Theevaluation of nodes at the celiac axis can beachieved in 91%. There have been no reportedcomplications using this scope [14, 15, 37].In addition to the esophagoprobe ultra-thin
miniprobes with 12, 20 and 30 MHz are avail-able, which can be advanced via the accessorychannel of a standard gastroscope throughtight strictures. With these catheters T stagingis possible in 87–90% of cases [38, 39]although evaluation of celiac nodes is moredifficult because of the limited depth of pene-tration.Results using either the esophagoprobe or
the miniprobes for evaluation of strictures dueto esophageal cancer show that 12–19% ofthese patients have T2 stage disease and maybe eligible for surgery [15, 37]. In these casesEUS can significantly change further manage-ment of these patients.
� A. Fritscher-Ravens, M. X. Pelling30
Fig. 4.7. a T3-tumor; b schematic demonstration.
a b
Tumor behind theL. muscularis propria
Tumor
Aorta

EUS and re-staging of esophageal cancer
For patients with advanced tumors not suitablefor surgery, combined chemoradiotherapy is anoption. Post therapy follow-up and re-stagingis necessary, at least in patients receiving neoad-juvant therapy, to evaluate whether the patienthas become eligible for surgery. Imaging tech-niques used for this purpose include EUS.Extent of the tumor, wall thickness, and
number and size of locoregional nodes areused to evaluate therapeutic response. A num-ber of studies have shown that EUS is not ableto differentiate true extent of residual tumorfrom fibrosis and peripheral edema followingtherapy. These appear hypoechoic similar tothe tumor and may result in over-staging. As aresult T staging correlates with surgical stagingin only 27–43% following neoadjuvant chemo-radiotherapy [41–47]. This is also true if thepatient receives radiotherapy alone [48].Patients who have had an R0 resection re-
quire regular follow-up. Nearly 50% of patientsdevelop local recurrence or distant metastases.In these cases EUS can help detect irregulari-ties of the wall and echopoor areas [49, 50].The sensitivity is over 75% [49, 50]. Howeverbecause of the surgery the normal wall layersare destroyed in the area of the anastomosisand early recurrence might be missed. Falsepositive results also occur so special care hasto be taken not to over-interpret the alteredanatomy.However in the presence of focal wall thick-
ening or tumor near the esophageal or gastricwall EUS achieved a positive predictive valueof 100% for recurrence.EUS may provide satisfactory results for the
detection of involved local nodes, but echo-genicity and altered node shape and size alonedoes not prove malignancy as the specificity ofEUS is low [13]. In these cases EUS-FNA isnecessary for definitive tissue diagnosis.
Endoscopic ultrasoundin early tumor stages
Since endoscopic mucosal resection (EMR) andother endoscopic methods such as photody-namic therapy and argon plasma therapy wereintroduced for the treatment of early esopha-geal cancer, accurate staging of these cancershas become even more important [52].Early esophageal cancer can only be de-
tected endoscopically as most imaging tech-niques are not sensitive enough to detect thesesubtle changes. Once proven histologically, ac-curate selection of patients for mucosectomy isvital. This includes the ability to differentiateT1m (tumors which are limited to the mucosa)from T1sm tumors (those which invade thesubmucosa). T1m tumors metastasise rarely tolymph nodes (<5%) and EMR may be cura-tive. T1sm tumors behave like more advancedtumors and node metastases are more likely.Therefore these may better be treated with sur-gery, depending on the general condition ofthe patient [53–55].Although EUS performed with 5–10 MHz
probes can differentiate between T1 and T2 ma-lignancies, their resolution is not sufficient toreliably diagnose and differentiate betweenT1m and T1sm tumors. Although correct diag-nosis may be possible in up to 71% (Fig. 4.8 a,b)the evaluation of these lesions is best per-formed with miniprobes at 12–30 MHz. Theseprobes enable up to nine wall layers to be visu-alized resulting in easier differentiation be-tween mucosal and submucosal spread. Thisdifferential diagnosis is possible in up to 86%of cases (Fig. 4.9) [56]. Failure to correctlystage these tumors is mainly due to the knownsurrounding edema, resulting in overstaging ofa mucosal lesion into a T1sm or T2 stage tu-mor [57]. 30 MHz probes provide the best re-solution but have poor penetration. Recentlythree dimensional probes have been developed,which transform two dimensional images intovirtual three dimensional images and allowmeasurement of tumor volume [58].With T1 tumors intended for endoscopic
therapy it is especially important to evaluatelymph node status. In general local lymphnodes are correctly described in 67–91% withEUS [28, 30–32, 56, 59].
4 Role of Endoscopic Ultrasound for Diagnosis and Staging of Esophageal Cancer � 31

Miniprobes have limited depth of penetra-tion and therefore limited potential for the ex-amination of local nodes. This is reflected bythe lower accuracy of only 56% for N stagingT1 tumors using miniprobes [56].In general lymph node metastases are only
to be expected with T1sm tumors. If fit en-ough, those patients with T1m tumor wouldundergo surgery, and it is hardly ever neces-sary to exchange a miniprobe for an echoen-doscope to complete nodal staging in thesecases. There may be some critical cases wheretherapy would be altered, in which case stagingwith both EUS probes is required. If nodes are
detected tissue proof is necessary to confirmmetastatic involvement, as specificity of EUSalone is not sufficient for final diagnosis.
Endoscopic ultrasound guidedfine needle aspiration
CT evaluation of mediastinal and celiac nodesand their differentiation into benign and meta-static lacks precision [61, 62]. EUS is able todetect up to 90% of involved nodes, but theimaging alone using criteria such as echogeni-
� A. Fritscher-Ravens, M. X. Pelling32
Fig. 4.8. a T1 sm-tumor; b schematic demonstration.
Fig. 4.9. a T1 m-tumor; b schematic demonstration.
a b
a b
Aorta
Tumor withinsubmucosallayer
L. musc. mucosae
L. musc. propria2nd layer L. musc.mucosaetotally seen
Submucosa
L. musc. propria

city, clear margins and small size (>1 cm) isnot able to define their aetiology with suffi-cient specificity [2, 7, 8, 12, 13, 20, 25, 28, 30–32, 63].The required tissue diagnosis of detected
nodes can be provided by EUS guided fineneedle aspiration (EUS-FNA) of the mediasti-num, performed at the same time as the EUSstaging. Potentially this method is comparableto CT guided transthoracic biopsy, but this isburdened with a complication rate of 9%; 7.7%pneumothorax, which needs drainage in 1.6%;1.3% bleeding [65–67]. In addition the accu-racy of transthoracic needle biopsy of nodessmaller than 1 cm is low and cannot be per-formed in close proximity to large vessels.EUS-FNA represents a fairly new and alterna-tive modality for tissue diagnosis. This can beused for all nodes within 5 cm of the GI tractas long as vision is not inhibited by air(Fig. 4.10). For esophageal cancer all lesions lo-cated within the posterior mediastinum 3 mmor larger, as well as celiac nodes can be visual-ized and punctured in real time under directvision [10].The pretracheal area and the anterior me-
diastinum are not accessible due to interferingair from the trachea. Nodes proximal or distalto the tumor are easily accessible. Nodes visi-ble directly behind the primary tumor mass,which can only be approached through thetumor are to be avoided. The needle may becontaminated by malignant cells from the pri-mary tumor giving rise to a false positive nodecytology (68%). Around 20% of patients withesophageal cancer have celiac metastases, whichare easily assessed (Fig. 4.11).Technically EUS-FNA of mediastinal and ce-
liac nodes is not demanding, especially whencompared with fine needle aspiration of pan-creatic masses or peri-pancreatic lymph nodes.The echoendoscope is straight, and the nodesare in close proximity to the gastrointestinalwall. Color Doppler allows the identification ofnearby or interfering vessels allowing saferpuncture. Advancement of the needle can beseen endoscopically as well as on ultrasoundin real time. Complications of EUS-FNA forlymph node puncture are extremely rare. Oneesophageal perforation was reported when theechoendoscope was forced to pass a malignantesophageal stricture [62]. In general EUS-FNA
provides cytology. It is able to verify the etiol-ogy of the tumor as well as metastases fromother primaries such as breast, kidney, or lungcancer. False positive results are rare [69].The technical success rate of EUS-FNA for
mediastinal nodes is 89–96% [70–74] and is inthe same range for the staging of lymph nodesin esophageal cancer [29, 75–78]. In a largeprospective study of 125 patients EUS-FNAwith lymph node involvement was significantlymore sensitive (83% vs 29%) and more accu-rate (87% vs 51%) than CT, and also more ac-curate than EUS alone (87% vs 74%), resultingin a change in management in 77% of patients[29].EUS and EUS-FNA of celiac nodes may re-
quire esophageal dilatation because stenosismay be seen in patients with advanced disease.No complications were observed from esopha-geal dilatation in a study using EUS. 18 (90%)of 20 nodes biopsied were positive for malig-nancy. CT detected only 6 (30%) of 20 cases ofsuspicious celiac lymph nodes, of which 83%were positive for malignancy by FNA [79]. Inanother study helical CT achieved a sensitivityand specificity for celiac nodes of 53%, and86% of those nodes were detected and provento contain malignancy by EUS-FNA [80]. An-other group performed EUS-FNA in 94% [51,54] of patients with celiac lymph nodes. Theaccuracy of EUS-FNA in detecting malignantnodes was 98% [78].
4 Role of Endoscopic Ultrasound for Diagnosis and Staging of Esophageal Cancer � 33
Fig. 4.10. Scheme of EUS-FNA.
Aorta
Lymphnodes
Celiac trunk

In recent studies comparing the health carecost and effectiveness of multiple staging strat-egies EUS-FNA and/or CT+EUS-FNA were themost inexpensive options and offered the mostquality-adjusted life-years. EUS-FNA±CT cantherefore be considered the preferred strategy[33, 81].
Conclusion
EUS represents a highly sensitive and accuratemethod for the staging of esophageal cancer,which is not achieved by any other imagingmodality to date. Simultaneously performedEUS guided FNA adds cytology for regionaland celiac node staging, thus providing valu-able information for the management of eso-phageal cancer patients.
References
1. Moss A, Schnyder P, Thoeni RF et al (1981) Eso-phageal carcinoma: pretherapy staging by com-puted tomography. AJR 136:1051–1056
2. Tio TL, Cohen P, Coene PP et al (1989)Endosonography and computed tomography ofesophageal carcinoma: preoperative classificationcompared to the new 1987 TNM staging system.Gastroenterology 96: 1478–1486
3. Halvorsen RA, Magruder-Habib K, Foster WL et al(1986) Esophageal cancer staging by CT: Longterm follow up study. Radiology 161:17–151
4. Hutter VP (1987) At last – worldwide agreementon the staging of cancer. Arch Surg 122:1235–1239
5. Hermanek P, Sobin LH (eds) (1987) TNM classifi-cation of malignant tumors, 4th ed. Springer, Ber-lin
6. Kimmey MB, Martin RW, Haggit RC et al (1989)Histologic correlations of gastrointestinal ultra-sound images. Gastroenterology 96:433–441
7. Nattermann CH, Dancygier H (1993) Endoscopicultrasound in the preoperative TN-staging of eso-phageal carcinoma. A comparative study betweenendosonography and computed tomography. Ultra-schall in Med 14:100–105
8. Grimm H, Binmöller KF, Hamper K et al (1993)Endosonography for preoperative locoregional stag-ing of esophageal and gastric cancer. Endoscopy25:224–230
9. Tio TL, Coene PP, den Hartog Jager et al (1990)Preoperative TNM classification of esophageal car-cinoma by endosonography. Hepatogastroenterol-ogy 37:376–381
10. Vilmann P (1996) Endoscopic ultrasonography-guided fine-needle aspiration biopsy of lymphnodes. Gastrointest Endosc 43:24–29
11. Tio T, Tytgat GNJ (1986) Endoscopic ultrasonogra-phy in analyzing peri-intestinal lymph node ab-normality. Preliminary results of studies in vitroand in vivo. Scand J Gastroenterol 21 (suppl 123):158–163
12. Catalano MF, Sivak MV, Rice TW et al (1994) En-dosonographic features predictive of lymph nodemetastasis. Gastrointest Endosc 40:442–446
13. Bhutani MS, Hawes RH, Hoffmann BJ (1997) Acomparison of the accuracy of echo features dur-ing endoscopic ultrasound (EUS) and EUS-guidedfine-needle aspiration for diagnosis of malignantlymph node invasion. Gastrointest Endosc 45:474–479
14. Grimm H, Binmöller KF, Soehendra N (1992) Ul-trasonic esophagoprobe (prototype I). GastrointestEndosc 38:490–493
15. Binmöller KF, Seifert H, Seitz U et al (1995) Ultra-sonic esophagoprobe for TNM staging of highlystenosing esophageal carcinoma. Gastrointest En-dosc 41:547–552
16. Takemoto T, Yanai H, Hada M (1992) Applicationof ultrasonic probes prior to endoscopic resectionof early gastric cancer. Endosc 24(suppl 1):329–333
� A. Fritscher-Ravens, M. X. Pelling34
Fig. 4.11a,b. Schematic demonstration of EUS-FNA at theceliac trunk.
a
b
Needle
Lymph node
Celiactrunk
Aorta

17. Consensus conference (1993) Clinical applicationsof endoscopic ultrasonography in gastroenterology– State of the art 1993. Endosc 25:358–366
18. Vilmann P, Hancke S (1996) A new biopsy handleinstrument for endoscopic ultrasound guided fine-needle aspiration biopsy. Gastrointest Endosc 43:238–243
19. Fritscher-Ravens A, Brand B, Bohnacker S, SriRam PVJ, Soehendra N (2000) Techniques in EUS-guided FNA of lymph nodes. Techniques in Endo-scopy 2:142–248
20. Rösch T (1995) Endosonographic staging of eso-phageal cancer. A review of literature results. Gas-trointest Endosc Clin North Am 5:537–547
21. Chak A, Canto M, Gerdes H et al (1995) Prognosisof esophageal cancers preoperatively staged to belocally invasive (T4) by endoscopic ultrasound(EUS): a multicenter retrospective cohort study.Gastrointest Endosc 42:501–506
22. Gertsch P, Vauthey JN, Lustenberger AA et al(1993) Long-term results of transhiatal esophagec-tomy for esophageal carcinoma. Cancer 72:231–239
23. Müller JM, Erasmi H, Stelner M (1990) Surgicaltherapy of esophageal carcinoma. Br J Surg 77:845–857
24. Rösch T, Classen M (1992) Gastroenterologic endo-sonography. Thieme, Stuttgart
25. Dittler HJ, Siewert RJ (1993) Role of endoscopicultrasonography in esophageal carcinoma. Endosc25:156–161
26. Hordijk ML, Zander H, Van Blankenstein M et al(1993) Influence of tumor stenosis on the accuracyof endosonography in preoperative T-staging ofesophageal cancer. Endosc 25:171–175
27. Souquet JC, Napoleon B, Pujol B et al (1992) En-dosonography guided treatment of esophageal car-cinoma. Endosc 24 (suppl 1):324–328
28. Weaver SR, Blackshaw GR, Lewis WG, Edwards P,Roberts SA, Thomas GV, Allison MC (2004) Com-parison of special interest computed tomography,endosonography and histopathological stage of oe-sophageal cancer. Clin Radiol 59:499–504
29. Vazquez-Sequeiros E, Wiersema MJ, Clain JE, Nor-ton ID, Levy MJ, Romero Y, Salomao D, Dierkhi-sing R, Zinsmeister AR (2003) Impact of lymphnode staging on therapy of esophageal carcinomaGastroenterology 125:1626–1635
30. Rasanen JV, Sihvo EI, Knuuti MJ, Minn HR, Luos-tarinen ME, Laippala P, Viljanen T, Salo JA (2003)Prospective analysis of accuracy of positron emis-sion tomography, computed tomography, and en-doscopic ultrasonography in staging of adenocar-cinoma of the esophagus and the esophagogastricjunction. Ann Surg Oncol 10:954–960
31. Flamen P, Lerut A, Van Cutsem E, De Wever W,Peeters M, Stroobants S, Dupont P, Bormans G,Hiele M, De Leyn P, Van Raemdonck D, Coose-mans W, Ectors N, Haustermans K, Mortelmans L(2000) Utility of positron emission tomographyfor the staging of patients with potentially oper-able esophageal carcinoma. J Clin Oncol 18:3199–3201
32. Heeren PA, Jager PL, Bongaerts F, van DullemenH, Sluiter W, Plukker JT (2004) Detection of dis-tant metastases in esophageal cancer with (18)F-FDG PET. J Nucl Med 45:980–987
33. Wallace MB, Nietert PJ, Earle C, Krasna MJ, HawesRH, Hoffman BJ, Reed CE (2002) An analysis ofmultiple staging management strategies for carci-noma of the esophagus: computed tomography, en-doscopic ultrasound, positron emission tomogra-phy, and thoracoscopy/laparoscopy. Ann ThoracSurg 74:1026–1032
34. Catalano MF, Van Dam J, Sivak MV (1995) Malig-nant esophageal strictures. Staging accuracy of en-doscopic ultrasonography. Gastrointest Endosc41:535–539
35. Van Dam J, Rice TW, Catalano MF et al (1993)High grade malignant stricture is predictive ofesophageal tumor stage. Risks of endosonographicevaluation. Cancer 71:2910–2917
36. Kallimanis GE, Gupta PK, Al-Kawas FH et al (1996)Endoscopic ultrasound for staging esophageal can-cer, with or without dilatation, is clinically impor-tant and safe. Gastrointest Endosc 41:540–546
37. Mallery S, Van Dam J (1999) Increased rate ofcomplete EUS staging of patients with esophagealcancer using the nonoptical, wire-guided echoen-doscope. Gastrointest Endosc 50:53–57
38. Menzel J, Höpffner N, Nottberg H et al (1999) Pre-operative staging of esophageal carcinoma: Minip-robe sonography versus conventional endoscopicultrasound in a prospective histopathologicallyverified study. Endoscopy 31:291–297
39. Hünerbein M, Ghadimi BM, Hänsch W et al (1998)Transendoscopic ultrasound of esophageal and gas-tric cancer using miniaturized ultrasound catheterprobes. Gastrointest Endosc 48:371–375
40. Chak A, Canto M, Stevens PD et al (1997) Clinicalapplications of a new through the scope ultra-sound probe. Prospective comparison with an ul-trasound endoscope. Gastrointest Endosc 45:291–295
41. Isenberg G, Chak A, Canto MI et al (1998) Endo-scopic ultrasound in restaging of esophageal can-cer after neoadjuvant chemoradiation. GastrointestEndosc 48:158–163
42. Hordijk ML, Kok TC, Wilson JH et al (1993) As-sessment of response of esophageal carcinoma toinduction chemotherapy. Endosc 25:592–596
43. Dittler HJ, Fink U, Siewert GR (1994) Response tochemotherapy in esophageal cancer. Endoscopy26:769–771
44. Zuccaro G, Rice TW, Goldblum J et al (1999) En-doscopic ultrasound cannot determine suitabilityfor esophagectomy after aggressive chemoradio-therapy for esophageal cancer. Am J Gastroenterol94:906–912
45. Laterza E, Manzoni G, Guglielmi A et al (1999) En-doscopic ultrasonography in the staging of esopha-geal carcinoma after preoperative radiotherapy andchemotherapy. Ann Thorac Surg 67:1466–1469
46. Kalha I, Kaw M, Fukami N, Patel M, Singh S, Gag-neja H, Cohen D, Morris J (2004) The accuracy of
4 Role of Endoscopic Ultrasound for Diagnosis and Staging of Esophageal Cancer � 35

endoscopic ultrasound for restaging esophagealcarcinoma after chemoradiation therapy. Cancer101:940–947
47. Beseth BD, Bedford R, Isacoff WH, Holmes EC,Cameron RB (2000) Endoscopic ultrasound doesnot accurately assess pathologic stage of esopha-geal cancer after neoadjuvant chemoradiotherapy.Am Surg 66:827–831
48. Tio LT, Blank LEC, Wijers OB et al (1994) Stagingand prognosis using endosonography in patientswith inoperable esophageal carcinoma treated withcombined intraluminal and external irradiation.Gastrointest Endosc 40:304–310
49. Lightdale CJ, Botet JF, Kelsen DP et al (1989) Diag-nosis of recurrent upper gastrointestinal cancer atthe surgical anastomosis by endoscopic ultra-sound. Gastrointest Endosc 35:407–412
50. Catalano MF, Sivak MV, Rice TW et al (1995) Post-operative screening for anastomotic recurrence ofesophageal carcinoma by endoscopic endosonogra-phy. Gastrointest Endosc 42:540–544
51. Fockens P, Manshanden CG, van Landschot JB etal (1997) Prospective study on the value of endoso-nographic follow-up after surgery for esophagealcarcinoma. Gastrointest Endosc 46:487–491
52. Soehendra N, Binmöller KF, Bohnacker S et al(1997) Endoscopic snare mucosectomy in the eso-phagus without any additional equipment: A sim-ple technique for resection of flat early cancer. En-dosc 29:380–383
53. Goseki N, Koike M, Yoshida M (1992) Histopatho-logic characteristics of early stage esophageal car-cinoma. A comparative study with gastric carcino-ma. Cancer 69:1088–1093
54. Bogomoletz WV, Molas G, Gayet B et al (1989)Superficial squamous cell carcinoma of the eso-phagus. Am J Pathol 13:535–546
55. Tio TL (1998) Diagnosis and staging of esophagealcarcinoma by endoscopic ultrasonography. Endo-scopy 30 (suppl 1):A33–A40
56. Hasegawa N, Niwa Y, Arisawa T et al (1996) Pre-operative staging of superficial esophageal carcino-ma: comparison of an ultrasound probe and stan-dard endoscopic ultrasonography. Gastrointest En-dosc 44:388–393
57. Yanai H, Yoshida T, Harada T et al (1996) Endo-scopic ultrasonography of superficial esophagealcancers using a thin ultrasound probe systemequipped with switchable radial and linear scan-ning modes. Gastrointest Endosc 44:578–582
58. Yasuda K, Kamaguchi M, Morikawa J, Honda M,Nakajima M (2005) Role of endoscopic ultrasonog-raphy in the diagnosis of early esophageal cancer.Gastrointest Endosc Clin N Am 15:93–99
59. Natsugoe S, Yoshinaka H, Morinaga T et al (1996)Ultrasonographic detection of lymph node meta-stases in superficial carcinoma of the esophagus.Endoscopy 28:674–679
60. McLoud TC, Bourgouin PM, Greenberg RW (1992)Bronchogenic carcinoma: Analysis of staging in themediastinum with CT by correlative lymph-nodemapping and sampling. Radiology 182:319–323
62. Izbicki JR, Thetter O, Karg et al (1992) Accuracy ofcomputed tomographic scan and surgical assess-ment for staging of bronchial carcinoma. J ThorCardiovasc Surg 104:413–420
63. Kondo D, Imaizumi M, Abe T et al (1990) Endo-scopic ultrasound examination for mediastinallymph node metastases of lung cancer. Chest 98:586–593
64. Ikenberry S, Bilderback S, Hawes R (1997) Endo-scopic ultrasonography, fine-needle aspirationbiopsy guided by endoscopic ultrasonography, andcomputed tomography in the preoperative stagingof non-small-cell lung cancer: A comparison study.Ann Int Med 127:604–612
65. Salazar AM, Westcott JL (1993) The role of trans-thoracic needle biopsy for the diagnosis and stag-ing of lung cancer. Clin Chest Med 14:99–110
66. Belfiore G, Camera L, Vetrani A, Fraioli G, Salva-tore M (1997) Middle mediastinum lesions: Pre-liminary experience with CT guided fine-needleaspiration biopsy with a suprasternal approach.Radiology 202:870–873
67. Schneider CP, Pröschild A, Mäder I et al (1999)CT-guided transthoracic biopsy of intrapulmonaryand mediastinal lesions. A retrospective study in300 patients. Pneumologie 53:71–76
68. Ciccia D (1999) Endoscopic ultrasound-fine needleaspiration in esophageal cancer. Techniques inGastrointest Endosc 1:60–62
69. Fritscher-Ravens A, SriRam PVJ, Schröder S, Topa-lidis T, Bohnacker S, Soehendra N (2000) Stromaltumor as a pitfall in endosonography-guided fine-needle aspiration cytology. Gastrointest Endosc 51:746–749
70. Silvestri GA, Hoffmann BJ, Bhutani MS et al(1996) Endoscopic ultrasound with fine needle as-piration in the diagnosis and staging of lung can-cer. Ann Thorac Surg 61:1441–1446
71. Gress F, Savides T, Sandler A et al (1997) Endo-scopic ultrasonography, fine-needle aspirationbiopsy guided by endoscopic ultrasonography, andcomputed tomography in the preoperative stagingof non small-cell lung cancer: A comparison study.Ann Int Med 127:604–612
72. Fritscher-Ravens A, SriRam PVJ, Bobrowski B,Pforte A, Topalidis T, Thonke F, Jäckle S, Soehen-dra N (2000) Mediastinal lymphadenopathy in pa-tients with and without previous malignancy –EUS-FNA based cytodiagnosis in 153 patients. AmJ Gastroenterol 95:2278–2284
73. Wiersema MJ, Vilmann P, Giovannini M et al(1997) Endosonography guided fine-needle aspira-tion biopsy: diagnostic accuracy and complicationassessment. Gastroenterology 112:1087–1095
74. Williams DB, Sahai AV, Aabakken L et al (1999)Endoscopic ultrasound guided fine-needle aspira-tion biopsy: a large single center experience. GUT44:720–726
75. Giovannini M, Monges G, Seitz JF et al (1999) Dis-tant lymph node metastases in esophageal cancer.Impact of endoscopic ultrasound-guided biopsy.Endosc 31:536–540
� A. Fritscher-Ravens, M. X. Pelling36

76. Reed CE, Mishra G, Sahai A (1999) Esophagealcancer staging: Improved accuracy by endoscopicultrasound of celiac lymph nodes. Ann ThoracSurg 67:319–322
77. Chang KJ, Soetikno RM, Bastas D, Tu C, Nguyen PT(2003) Impact of endoscopic ultrasound combinedwith fine-needle aspiration biopsy in the manage-ment of esophageal cancer. Endosc 35:962–966
78. Eloubeidi MA, Wallace MB, Reed CE, HadzijahicN, Lewin DN, Van Velse A, Leveen MB, Etemad B,Matsuda K, Patel RS, Hawes RH, Hoffman BJ(2001) The utility of EUS and EUS-guided fineneedle aspiration in detecting celiac lymph nodemetastasis in patients with esophageal cancer: a sin-gle-center experience. Gastrointest Endosc 54(6):714–719
79. Parmar KS, Zwischenberger JB, Reeves AL, WaxmanI (2002) Clinical impact of endoscopic ultrasound-
guided fine needle aspiration of celiac axis lymphnodes (M1a disease) in esophageal cancer. AnnThorac Surg 73(3):916–920, discussion 920–921
80. Romagnuolo J, Scott J, Hawes RH, Hoffman BJ,Reed CE, Aithal GP, Breslin NP, Chen RY, Gumu-stop B, Hennessey W, Van Velse A, Wallace MB(2002) Helical CT versus EUS with fine needle as-piration for celiac nodal assessment in patientswith esophageal cancer. Gastrointest Endosc 55:648–654
81. Harewood GC, Wiersema MJ (2002) A cost analysisof endoscopic ultrasound in the evaluation of eso-phageal. Am J Gastroenterol 97(2):452–458
82. Greene FL, Page DL, Fleming ID et al (eds) (2002)TNM classification and stage grouping of esopha-geal carcinoma. American joint committee on can-cer. Cancer staging manual, 6th edn. Springer, NewYork, pp 91–98
4 Role of Endoscopic Ultrasound for Diagnosis and Staging of Esophageal Cancer � 37

Introduction
The primary goal of a preoperative risk analy-sis is the reduction of perioperative morbidityand mortality. The latter is still ranging up to10% for esophageal cancer despite all progressin intensive care therapy and the refinement ofsurgical technique. The morbidity, in particu-lar the incidence of pulmonary complications,is by far higher and amounts to approximately50%.To reduce this high morbidity, insufficient
organ systems are to be recognized and theirfunction should be improved by suitablemeans, preoperatively.
Definition of “risk”
Mortality and morbidity are affected by tumor-related and patient-related factors, which haveto be differentiated.Tumor-related factors of risk such as tumor
size, infiltration of neighboring organs, lym-phatic spread, or possible distant metastasisare evaluated by preoperative staging.The patient-related risk is characterized by
pre-existing diseases leading to dysfunctions ofcertain organ systems not related to the malig-nant disease, thus accounting for the individu-al risk of the patient.Methods for the ascertainment and objectifi-
cation of this risk will be described in the fol-lowing.
Methods of risk ascertainment
Traditionally risk assessment is a subjectiveappraisal of the patient by the surgeon sup-ported by objective findings such as routineblood chemistry, chest x-ray, and ECG. Byquestions evaluating physical performancesuch as “How many floors can you walk upwithout shortness of breath or chest pain?”,the surgeon tries to objectify his appraisal.This procedure assumes extensive clinical
experience and is not suitable for a standard-ized, objective patient evaluation and selection.Different instruments for the objective esti-
mation of the risk are established. The ASAclassification predominantly applied in anes-thesia. It combines objective findings, the sub-jective impression, and the clinical findings ofthe examiner into a 5-step classification. It isdesigned, however, for the application to abroad spectrum of surgical patients and is notsuitable for the individual risk assessment be-fore esophagectomy.Different analyses described in the literature
could isolate a multiplicity of independent riskfactors, which significantly affect postoperativemortality and the incidence of postoperativecomplications. However, none of these investi-gations lead to the establishment of a simple,practicable scoring system allowing a generalevaluation.
Preoperative Evaluationof the Operative Risk ProfileK.A. Gawad, C. Busch, D.C. Broering, E.F. Yekebas
5

An instrument for preoperative risk analysis,particularly in esophageal cancer patients, wasrecently established on the basis of an analysisof 553 patients [1]. It seems to allow the iden-tification of patients with a clearly increasedrisk who may have to be admitted to a non-surgical treatment. The factors shown in Table1 are multiplied with a priority factor (generalstate �4, cardiac function �3, hepatic function�2 and respiratory function �2), and a totalscore is calculated allowing the assignment to
one of a total of 3 risk groups (small risk (11–15 points), moderate risk (16–21 points), highrisk (22–33 points)).In our own patient collective the use of
scores established in thoracic surgery [2] hasbeen shown to be effective for the assessmentof pulmonary and cardiac risk. Based on ourexperience, these are the limiting factors thatsubstantially affect postoperative morbidityand mortality. In particular a preoperative op-timization of the patient condition can beachieved in a suitable manner. The function ofother organ systems is assessed by means oflaboratory analyses and, if necessary, functiontests.
Measures for preoperativerisk minimization
We are in favor of an interdisciplinaryapproach with participation of surgeons, cardi-ologists, and pulmonologists. Patients in whoma restriction of the pulmonary or cardiac func-tion is evitable by the preoperative analysiscan possibly be brought into a lower riskgroup by suitable measures. To achieve an im-provement of cardiac function above all, theoptimization of the medication for hyperten-sion, cardiac insufficiency or arrhythmia ismandatory. In coronary obstruction, stenting
� K.A. Gawad et al.40
Table 5.1. Classification of organ dysfunction
� Pulmonary function 1 – normal VC>90% and PaO2 >70 mmHg2 – restricted VC<90% or PaO2 <70 mmHg3 – highly restricted VC<90% and PaO2 <70 mmHg
� Hepatic function 1 – normal ABT>0.42 – restricted ABT<0.4; cirrhosis3 – highly restricted cirrhosis
� Cardiac function 1 – normal normal risk(cardiological appraisal) 2 – restricted increased risk
3 – highly restricted high risk
� General status 1 – normal Karnofsky Index >80% and good cooperation2 – restricted Karnofsky Index � 80% or bad cooperation3 – highly restricted Karnofsky Index �80% and bad cooperation
ABT: Aminopyrine breath test; VC: vital capacity; PaO2: arterial O2 partial pressure; Karnofsky Index, see Table 5.2
Table 5.2. Karnofsky Index
100% Normal activity, no complaints
90% Marginally reduced activity and capacity
80% Normal activity only with exertion,clearly reduced activity
70% Unable for normal activity, autonomousmaintenance
60% Occasional help, largely autonomousmaintenance
50% Continuous support and care, regular medicalhelp needed
40% Mostly bedridden, professional nurse needed
30% Continuously bedridden, professional nurseneeded
20% Badly ill, hospitalized, active supportive therapy
10% Moribund

or even bypass procedures should be per-formed to improve the cardiac risk of the pa-tient. To improve pulmonary function the sen-sible use of mucolytic agents, bronchodilatorsas well as effective respiratory therapy (drain-age, percussion, vibration, and breathing exer-cises) under physiotherapeutic guidance ormachine measures (incentive spirometry, “Con-tinuous positive airway pressure” (CPAP), “in-termittent positive pressure breathing” (IPPB))have to be considered. In patients with cachex-ia, a high caloric enteral nutrition should besupported by infusion therapy.Patients with esophageal cancer represent a
difficult patient group, usually afflicted withmultiple pre-existing diseases. An exact historyprovides initial information on possible riskfactors. It is especially necessary to ask aboutactive alcoholism or other intoxicant consump-tion. For the minimization of the perioperativemorbidity and mortality, an exact analysis ofthe organ systems is necessary by appropriatefunction tests. These should cover an examina-tion of the cardiac function by means ofechocardiography and ergometry. If necessary,further investigations have to be conducted aftercardiological evaluation. If an improvement offunction by respective treatment is possible, thishas to be documented by repeat assessment afteran appropriate interval. Pulmonary functiontesting should include plethysmography and ar-
terial blood gas analysis. Following appropriatepretreatment, a new analysis is also necessary.In patients with pathological creatinin val-
ues, a determination of the creatinin clearanceis mandatory.After the execution of the investigations spe-
cified above, the operative risk for the patientcan be objectified by assigning the findingsinto a scoring system. The following patientsshould be excluded from an operation: patientsassigned to a high risk group according to thescoring system previously described, patientswith a severe dysfunction of individual organsystems, or those with an accumulation of lesssevere but still serious dysfunctions. However,surgery can be indicated as an individualapproach and only after an intensive consentdiscussion.
References
1. Bartels H, Stein HJ, Siewert JR (1998) Preoperativerisk analysis and postoperative mortality of oeso-phagectomy for resectable oesophageal cancer. Br JSurg 85(6):840–844
2. Izbicki JR, Knöfel WT, Passlick B, Habekost M, KargO, Thetter O (1995) Risk analysis and long-termsurvival in patients undergoing extended resectionof locally advanced lung cancer. J Thorac CardiovascSurg 110(2):386–395
5 Preoperative Evaluation of the Operative Risk Profile � 41

Developments in surgical as well as anestheticmanagement have meant that the morbidityand the mortality of esophageal surgery havesubstantially reduced during the last decade.Modern anesthetic management allows tar-geted risk stratification, especially of cardiacand pulmonary risk factors, thus providing arationale for intraoperative monitoring andchoice of anesthetic technique as well as post-operative pain and intensive care therapy. It isessential for the attending anesthesiologist tounderstand the underlying principles of thepathophysiology and surgery of esophagealdiseases and to cooperate closely with the sur-geon in order to provide the best care possiblefor the patient.
Preoperative evaluation
Depending on the pathologic condition of theesophagus, chronic, subacute or acute aspira-tion may occur. Aspiration often results in apoor preoperative respiratory status with re-curring pneumonia. Furthermore, during in-duction of anesthesia the risk of regurgitationand aspiration is increased [1]. Patients withmalignancies of the esophagus often present ahistory of smoking with resulting complica-tions of chronic obstructive lung diseases.Treatment of malignant esophageal tumors
with bleomycin may cause further deteriora-tion in the respiratory status especially afterperiods of ventilation with high oxygen tension[2]. Dyspnea due to obstruction of the airwaysby large mediastinal masses is a rare finding.Initial screening of the severity of esopha-
geal diseases with respect to tumor mass, oc-currence of dyselectasis or atelectasis and
pleural effusions may be achieved by basicclinical techniques such as inspection, palpa-tion, auscultation, and percussion. The preop-erative chest X-ray in anterior-posterior andlateral position allows diagnosis of emphyse-ma, pneumonia or intrapulmonary metastases.Displacements or obstructions of the tracheamay indicate a difficult endotracheal intuba-tion. The computed tomogram of the lung al-lows an even more detailed analysis of pulmo-nary and mediastinal pathologies. Forced ex-pired volume in one second (FEV1) and func-tional vital capacity are the most importantparameters determined by specialized lungfunction tests indicating obstructive or restric-tive lung disease often accompanied by an in-creased risk of postoperative morbidity andmortality. Preoperative hypoxia and/or hyper-capnia may indicate a postoperative need formechanical ventilation as well as difficultweaning phase with a prolonged stay on theintensive care unit (ICU) [3].Patients with obstructive diseases of the eso-
phagus often have a poor nutritional status.Depending on the severity of the dysphagiasolids and sometimes even fluids cannot passthe esophagus. Improving the nutritional sta-tus prior to surgery can lead to lowered mor-bidity and mortality. If the intake of fluids isrestricted thus leading to hypovolemia, fluidsneed to be replaced by parenteral therapy.Many patients with malignancies of the eso-phagus are older than 40 years and have a his-tory of hypertension, smoking, diabetes melli-tus, claudication, and hyperlipoproteinemia.Further evaluation is necessary if history andexamination reveal symptoms of coronary ar-tery disease, a previous myocardial infarction,or congestive heart failure. The routine preop-erative ECG does not exhibit signs of myocar-dial ischemia in 15–50% of patients with coro-
Perioperative and Postoperative ManagementJ. Scholz, P.H. Tonner, G. von Knobelsdorff
6

nary artery disease. Another 25% of the pa-tients present with dysrhythmias that prohibitthe use of ECG as a marker for myocardialischemia. In addition to routine testing, exami-nations such as a stress ECG, echocardiograhywith and without stress, pharmalogical stresstests, or diagnostic coronary angiography mayreveal evidence of the severity of cardiac dis-ease [4]. Depending on the results of the pre-operative evaluation, a cardiologic or cardio-surgical intervention may be necessary be-fore the planned operation. Chemotherapeuticagents such as daunorubicin and adriamycinas well as chronic alcohol abuse, which areoften present in these patients, may also leadto cardiomyopathies.The extent of preoperative laboratory testing
depends on the history and physical examina-tion of the patient. Basic testing includes he-matologic parameters, electrolytes, glucose, se-rum creatinine, blood urea nitrogen, transami-nases, alkaline phosphatases, and serum albu-min. If the coagulation status exhibits abnor-malities, factors and platelets should be admin-istered as needed. A preoperative autologousblood donation should be considered if the un-derlying disease is not of malign nature, hemo-globin concentration is in the normal range,and the planned operation is not urgent.The goal of premedication is sedation, anxio-
lysis and amnesia. This profile is best achievedby administration of short acting benzodiaze-pines. Additionally, if the patient is in pain orif preemptive analgesia is desired an opioidcan be given. If signs of gastric reflux are pres-ent, H2-receptor antagonists may reduce gastricsecretions and gastric pH. However, these agentsrequire a sufficient interval between administra-tion and anesthesia in order to provide adequateeffects. Cimetidine and the more potent raniti-dine are currently the preferred agents. Admin-istration is usually orally. However in the pres-ence of severe dysphagia they may be givencarefully intravenously. Increased rates of bac-terial pneumonia have been reported after ad-ministration of H2-antagonists. However, thesignificance of these findings is still being dis-cussed. Metoclopramide increases the loweresophageal sphincter pressure and may thusreduce the risk of aspiration. In contrast, anti-cholinergic drugs may reduce the lower esopha-geal sphincter tone (Table 6.1).
In addition to routine monitoring, a centralvenous line and an arterial catheter are neces-sary to continuously monitor hemodynamicsand to perform frequent analyses of the bloodgas status. The intraoperative manipulation ofthe mediastinum and the accompanying com-pression of the heart or major vessels as wellas the induction of cardiac arrhythmias to-gether with massive blood loss often lead tosevere intraoperative cardiocirculatory depres-sion that makes continuous online monitoringof arterial and venous blood pressure manda-tory. Depending on the preoperative status ofthe patient, the use of a pulmonary arterycatheter should be considered [5]. Pulse oxime-try is imperative for monitoring of oxygen de-livery, especially during one-lung ventilation.Anesthesia in esophageal surgery is per-
formed as balanced anesthesia or as a total in-travenous anesthesia (TIVA). Additionally athoracic epidural catheter may be applied forintra- and postoperative pain therapy. Epiduralanalgesia has been demonstrated to providebetter postoperative lung function, better spon-taneous ventilation, and higher arterial oxygentensions than systemic administration of anal-gesics [6]. In patients with coronary artery dis-ease and myocardial infarction epidural analge-sia has been demonstrated to be beneficial.Due to a favorable effect on the ratio betweenoxygen demand and oxygen delivery sym-patholysis may improve stress-induced leftventricular function [7]. Placement of the epi-
� J. Scholz et al.44
Table 6.1. Preoperative minimal diagnostic requirements forpatients undergoing major esophageal surgery
Laboratory tests Apparative tests
� Hemoglobin, hematocrit � plain chest x-ray
� Serum electrolytes � electrocardiogram (ECG)(sodium, potassium)
� pulmonary function test� Serum creatinine and urea
� Blood glucose
� Liver enzymes
� Blood group
� Coagulation status
Further investigations might be necessary depending ontest results

dural catheter is best performed before induc-tion of general anesthesia because of the betterpositioning of the patient, early detection ofcomplications such as hematoma or neural in-juries, and more rapid detection of catheterdisplacements [8]. The injection of local anes-thetics via an epidural catheter under generalanesthesia is currently under discussion.Although analgesia, good surgical exposuredue to a small and contracted gastrointestinaltract, and muscle relaxation are benefits of thisapproach, one has to consider increased risk ofintraoperative hypotension and blood loss dueto peripheral vasodilatation.The role of the new volatile anesthetics sevo-
flurane and desflurane in anesthesia for eso-phageal surgery has not yet been determined.The rapid pharmacokinetics of these agents al-lows achievement of spontaneous ventilationand extubation of the patient shortly after skinclosure. However, the use of TIVA may improveoutcome with respect to postoperative shiver-ing as well as nausea and vomiting. The opioidremifentanil possesses an extremely short con-text-sensitive half-time, thus allowing a betteradaptation to surgical stress. Nitrous oxidemay diffuse into preformed gaseous bubbles,for example in the gastrointestinal tract, thusleading to bowel distention. Furthermore, one-lung ventilation requires the administration ofhigh fractions of oxygen (FiO2), thus prohibit-ing the use of nitrous oxide.Aspiration during induction of anesthesia is
a frequent complication in patients with eso-
phageal diseases. Therefore the trachea shouldbe intubated after rapid-sequence inductionwith cricoid pressure. The introduction of ro-curonium as a muscle relaxant allows perform-ing a modified rapid-sequence induction with-out using succinyl choline and may thus re-duce the risk of a massive release of potassiumor the triggering of a malignant hyperthermia(MH) episode. Tumors of the esophagus ormediastinal lymph nodes may lead to a com-plete collapse and obstruction of the upper air-ways after loss of muscle tone due to adminis-tration of muscle relaxants [9]. Ventilation ofthe patient may be impossible unless an endo-tracheal tube is placed distally to the obstruc-tion. However, placement of an endotrachealtube may be extremely difficult leading to a“cannot ventilate, cannot intubate” situation. Ifa difficult intubation is expected preoperatively,a fiberoptic intubation is performed in theawake, spontaneously breathing patient. In or-der to facilitate intubation, lidocaine is adminis-tered topically in nose and larynx. Additionally,parasympatholytics, sedatives, and analgesicsmay be administered systemically. Transcricoi-dal administration of lidocaine is often usefulto suppress coughing, thus aiding endotrachealintubation. After identification of the trachea,the endotracheal tube, which is placed on thefiberscope prior to starting the procedure, ispushed forward. Before securing the tube, a fi-nal fiberoptic check of placement is performed.An awake nasal intubation should only be per-formed in emergency situations.
6 Perioperative and Postoperative Management � 45
Table 6.2. Influence of various drugs on pressure of the lower esophageal sphincter
Reduction Increase No change
� Atropine � Metoclopramide � Propranolol
� Glycopyrrolate � Droperidol � Cimetidine
� Dopamine � Edrophonium � Ranitidine
� Nitroprusside � Neostigmine � Atracurium
� Ganglionic blocking agent � Histamine
� Thiopentone � Succinylcholine
� Tricyclic antidepressant � Pancuronium
� Beta-adrenoceptor agonist � Metoprolol
� Volatile anesthetics � Alpha-adrenoceptor agonist
� Opioids � Antacida

If preoperative hypovolemia is not treatedaccordingly, hypotension is a common findingafter induction of anesthesia. Thus adequatefluid therapy is mandatory before induction ofanesthesia. Administration of anesthetics forinduction is dependent on their effect. Etomi-date has been demonstrated to exert the leastcardiocirculatory depression and is thus thepreferred induction agent at many hospitals.During surgery of the lower esophagus via a
left thoraco-abdominal incision or during bluntesophagectomy, it is not necessary to collapseone lung using a double lumen endotrachealtube. A single lumen endotracheal tube can beplaced, and surgical exposure may be obtainedby retraction of the left lung. For esophagealsurgery via a thoracotomy, it is usually neces-sary to place a double lumen endobronchialtube to collapse the ipsilateral lung. Double lu-men tubes allow selective intubation of theright or left main stem bronchus (Fig. 6.1).Although some investigators have advocatedthe placement of a double lumen tube accord-ing to the side of surgery, a right-sided doublelumen tube carries the risk of a collapse of theright upper lobe due to obstruction of theupper right bronchus. Thus left side double lu-men tubes have been demonstrated to be morebeneficial, independent of the side of operationif the operation does not involve the left mainbronchus [10]. However, a right-sided doublelumen tube is technically easier to place in thecorrect bronchus because of the steep anglebetween trachea and left main bronchus. Place-ment of a double lumen tube is checked byclamping and auscultation. However, additionalfiberoptic control is indispensable [11] (Fig.6.1). As an alternative to the double lumentube a Univent tube may be placed (Fig. 6.2).This endotracheal tube consists of a one-lumentube with a small lumen for insertion of abronchus blocker. The patient is intubated inthe usual fashion following in which a cuffedcatheter is introduced under fiberoptic surveil-lance. Collapse of the lung is achieved via de-flation through a small lumen in the bronchusblocker. The disadvantages of the Univent tubecomprise frequently inadequate differentialventilation, especially if blocking the rightlung, the lack of suction through the blockerlumen, and the often insufficient inflation anddeflation of the lungs.
� J. Scholz et al.46
a b
Fig. 6.1. Schematic depiction of placement of a left-sideddouble-lumen tube in a patient in the supine position. a Ini-tially the tube is inserted by holding its end to one side.After passage of the laryngeal cords the tube is rotated by90� to the left while it is gently pushed forward into the leftmain bronchus. b After placement of the tube positioning ischecked by clamping and auscultation. However, fiberopticcontrol of the tube position is mandatory. Modified from Be-numof and Alfery [11].
a b
Fig. 6.2. Schematic depiction of a Univent tube. The pa-tient’s trachea is intubated in the usual fashion as for a sin-gle-lumen tube. Under fiberoptic surveillance the bronchusblocker is promoted through a thin working channel. Theblocker is positioned by turning the attached catheter untilthe chosen left or right main stem bronchus is clearly shutoff. Care has to be taken that the right upper lobe bronchus,which is close to the carina, is not obstructed by the cuff ofthe blocker. Modified from Benumof and Alfery [11].

If the trachea is injured during the course ofoperation, only the endobronchial lung shouldbe ventilated until definite repair is achieved.If the patient has been intubated with a one lu-men tube, the tube is advanced until an endo-bronchial position is obtained. During one-lung ventilation for esophageal surgery hypoxiamay occur more often than during one-lung-ventilation for lung surgery (Fig. 6.3). This isbecause the patient presenting for lung surgerymay already have limitations of blood flow tothe diseased lung and, thus, less ventilation/perfusion mismatching during one-lung anes-thesia. Frequently, parts of the pulmonary ves-sels are ligated during lung surgery, thus de-creasing the shunt.Should hypoxia occur during one-lung ven-
tilation, the FiO2 is increased to 1.0 and theposition of the double-lumen tube should bechecked using a fiberoptic bronchoscope. Thus,the immediate availability of a fiberopticbronchoscope is mandatory during one lung
ventilation. Another method to increase the ar-terial oxygen saturation is the administrationof positive endexpiratory pressure (PEEP) tothe ventilated lung [12]. However, becausePEEP increases the pulmonary vascular resis-tance, perfusion of the unventilated lung mayincrease, thus increasing the shunt volume andincreasing the ventilation/perfusion mismatch.Administration of a continuous positive airwaypressure (CPAP) to the unventilated lung po-tentially increases arterial oxygenation, in thiscase. Finally, clamping of the pulmonary arteryto reduce the shunt volume may be consideredas a last resort. If none of these measures issuccessful in restoring oxygenation, conven-tional ventilation of both lungs has to be rein-stituted [10].Patients who require postoperative ventila-
tion on the intensive care unit should have thedouble-lumen tube replaced by a single-lumenendotracheal tube. However, an inadvertentintubation of the esophagus must be strictlyavoided not only because of the catastrophicconsequences of the hypoxia, but because thedistension by ventilated air may lead to an in-sufficiency of the anastomosis. If a Univenttube has been used, simple retraction of thebronchus blocker allows this tube to be usedas a single-lumen tube.In patients who do not present with esopha-
geal perforation, a nasogastric tube is placedby the anesthesiologist preoperatively. Thistube will be accurately positioned by the sur-geon intraoperatively. In some cases the distalend of the tube is placed close to the anasto-mosis in order to test for leaks by administra-tion of methylene blue. After esophagectomyand gastric or colon replacement, the tube isneeded to remove secretions. In order to avoidan accidental removal of the nasogastric tubesecuring by a suture has been suggested.The patient is positioned intraoperatively by
the surgeon. Especially in a lateral positioncare has to be taken to support the patientwithout exerting too much pressure and tocushion exposed body parts. At risk are espe-cially the brachialis plexus, peroneal nerves, aswell as soft tissues such as ears, eyes, and gen-itals. Peripheral pulses have to be checked inorder to prevent obstruction of the arterialblood supply. The intraoperative control ofbody temperature is mandatory because it has
6 Perioperative and Postoperative Management � 47
Fig. 6.3. Schematic depiction of the relation between venti-lation and perfusion during operations in a lateral position.The upper lung is well ventilated until clamped. Howeverdue to gravitation, perfusion is preferentially directed to-wards the dependent lung. Ventilation of the dependentlung is reduced because of suboptimal positioning, high ab-dominal pressure, and surgical manipulation. Some parts ofthe lung may even be atelectatic. However, oxygenation ofthe blood is improved by hypoxic pulmonary vasoconstriction(HPV), leading to a reduced perfusion of non-ventilated partsof the lung by reflex mechanism. Examples of factors reduc-ing the positive influence of HPV are high pressures in pul-monary artery, hyperventilation, vasodilators, and volatile an-esthetics. Modified from Benumof and Alfery [11].
Open thoraciccavity
Upper lung(not insufflated)
Abdominalpressure
Relaxateddiaphragm
Abdominalpressure
Mediastinum
Lower insufflatedlung
Suboptimalpositioning

been demonstrated that even mild hypothermiaresults in an increased frequency of wound in-fections and prolonged hospital stay [13]. Ef-fective measures of temperature maintenanceare increase of room temperature, warm waterblankets, convective warming devices, wrap-ping of exposed extremities in metallic foil,warming of fluids, as well as warming of venti-lated air.The decision to extubate the patient at the
end of the surgical procedure depends on thepreoperative status, the cardiac status, the tem-perature, and the extent of surgery. Weaningfrom mechanical ventilation should beginwhen the patient is awake and cooperative,able to protect the airway, have adequate re-turn of pulmonary function, and when the pa-tient is hemodynamically stable. Muscle relaxa-tion should have faded or been antagonized.Usually this condition will only be achieved inthe intensive care unit. Basically the patientshould be weaned and extubated as soon aspossible to reduce the risks due to prolongedmechanical ventilation. The use of a thoracicepidural catheter may facilitate this goal. How-ever, patients with esophageal perforation oftendevelop mediastinal infection and should beventilated during the immediate postoperativeperiod.
Postoperative phase
Only after short surgical procedures on theesophagus (such as esophageal dilatation inachalasia) will postoperative care in the recov-ery room and consecutive transfer to the wardbe possible. In all other cases a transfer to theintensive care unit offering the option of me-chanical ventilation is necessary. Complicationsin the postoperative period comprise: first im-mediate problems such as pain, respiratory in-sufficiency and blood loss, second problemsdue to preexisting conditions, and third prob-lems caused by insufficiencies of anastomosesand consequent infection.Postoperative hypotension is most likely due
to hypovolemia caused by hemorrhage or fluidimbalances. In case of hemorrhage, the sur-
geon should be notified immediately and a sur-gical revision be performed. The coagulationstatus should be optimized by substitution ofcoagulation factors or platelet concentrates.Respiratory insufficiency is frequent after
esophageal surgery especially if the patient isobese or presents with lung disease [14]. Paindue to the surgical incision leads to hypoventila-tion and that is often complicated by retentionof secretions and dystelectasis. Pneumonia is afrequent complication under these circum-stances. Postoperative pain therapy via a thorac-ic epidural catheter can reduce these complica-tions and may facilitate postoperative mobiliza-tion of the patient. The prophylactic use ofbroad spectrum antibiotics is still a matter ofdiscussion. A pneumothorax may lead to dete-rioration of the respiratory function of the pa-tient. An immediate diagnosis by chest X-rayis necessary unless the patient is hypoxic and re-quires urgent chest decompression. Therapeuti-cally an additional chest drainage is inserted.Care has to be taken that the laryngeal nerveson both sides are not injured during surgery.However, if the patient develops inspiratory stri-dor after extubation this possibility has to beconsidered. A reintubation and then tracheoto-my is necessary in such circumstances.Depending on the existence and the nature
of preexisting diseases, a rapid or prolongedpostoperative course can be expected. Cardiacand pulmonary diseases may exacerbate prob-lems and lead to decompensation after the sur-gical procedure. In patients with malignantdiseases of the esophagus pulmonary compli-cations including the adult respiratory distresssyndrome (ARDS) have been reported after apreoperative combination of chemotherapy andradiation [15]. Furthermore patients with ma-lignancies frequently have a history of alcoholabuse. These patients often develop a deliriumdue to withdrawal that can considerably in-fluence the postoperative course. Recently theadministration of �2-adrenergic agonists hasshown to be successful in the therapy of theseconditions [16]. In rare cases the administra-tion of alcohol cannot be avoided in order tokeep the patient cooperative.Leakage from anastomoses can occur from
the third to the twelfth postoperative day. Thediagnosis is confirmed if acidic fluids (pH<6)with a high concentration of amylase issue
� J. Scholz et al.48

from a thoracic drain. Endoscopy, X-ray (pos-sibly with contrast medium) and computed to-mography will further confirm the diagnosis.Consequences are mediastinitis and sepsis witha high rate of mortality. The therapy includesthe administration of broad spectrum antibiot-ics and surgical revision with additional place-ment of drainage tubes.
References
1. Greenhow D (1988) Esophageal surgery. In: Mar-shall B, Longnecker D, Fairley H (eds) Anesthesiafor thoracic procedures. Blackwell Scientific Publi-cations, Boston
2. Allen S, Riddell G, Butchart E (1981) Bleomycintherapy and anesthesia: the possible hazards ofoxygen administration to patients after treatmentwith bleomycin. Anaesthesia 36:60–63
3. Hickling K (1990) Ventilatory management ofARDS. Can it affect the outcome? Intensive CareMed 16:219–226
4. Tonner PH, Scholz J, Schulte am Esch J (1996) An-esthesia for non-cardiac surgery in patients at highcardiac risk. Anaesthesiol Intensivmed 37:373–385
5. Izbicki JR, Knöfel WT, Passlick B, Habekost M, KargO, Thetter O (1995) Risk analysis and longterm sur-vival in patients undergoing extended resection oflocally advanced lung cancer. J Thorac CardiovascSurg 110:386–395
6. Connors A, Speroff T, Dawson N, Thomas C, Har-rell F, Wagner D, Desbiens N, Goldman L, Wu A,Califf R, Fulkerson W, Vidaillet H, Broste S, Bella-my P, Lynn J, Knaus W for the SUPPORT investi-gators (1996) The effectiveness of right heart cath-
eterization in the initial care of critically ill pa-tients. JAMA 276:889–897
7. Fratacci M, Kimball W, Wain J et al (1993) Dia-phragmatic shortening after thoracic surgery in hu-mans: effects of mechanical ventilation and thoracicepidural anesthesia. Anesthesiology 79:654–665
8. Blomberg S, Emanuelsson H, Kvist H et al (1990)Effects of thoracic epidural anesthesia on coronaryartery disease. Anesthesiology 73:840–847
9. Norlander O (1988) Combined epidural and gener-al anesthesia for abdominal operations – a goodtechnique. Acta Anaesth Belg 39:203–208
10. Mackie A, Watson C (1984) Anaesthesia and media-stinal masses. Anaesthesia 39:899–903
11. Benumof J, Alfery D (1995) Anesthesia for thoracicsurgery. In: Miller R (ed) Anesthesia. Churchill Li-vingstone, New York
12. Smith G, Hirsch N, Ehrenwerth J (1986) Sight andsound. Can double-lumen endotracheal tubes beplaced accurately without fiberoptic bronchoscopy?Anesth Analg 65:S 1
13. Campos JH, Reasoner DK, Moyers JR (1996) Com-parison of a modified double-lumen endotrachealtube with a single-lumen tube with enclosed bron-chial blocker. Anesth Analg 83:1268–1272
14. Hedenstierna G, Baehrendtz S, Klingstedt C, San-tesson J, Söderborg B, Dahlborn M, Bindslev L(1984) Ventilation and perfusion of each lung dur-ing differential ventilation with selective PEEP. An-esthesiology 61:369–376
15. Kurz A, Sessler D, Lenhardt R for the Study ofWound Infection and Temperature Group (1996)Perioperative normothermia to reduce the inci-dence of surgical wound infection and shortenhospitalization. N Engl J Med 334:1209–1215
16. Kido Y, Ogawa Y, Kawasaki K, Shiozaki H, Mori-moto S, Mori T (1988) Pulmonary complicationsfollowing surgery for esophageal cancer. In: Sie-wert H, Hölscher A (eds) Diseases of the esopha-gus. Springer, Berlin Heidelberg New York
6 Perioperative and Postoperative Management � 49

Introduction
Gastroesophageal reflux disease is one of themost common diseases in western societies.The prevalence is estimated to be around 10%in those populations, if the presence of the dis-ease is based on weekly or daily reflux symp-toms [1–3]. The disease has been diagnosedmore often due to increased and improved di-agnostic activities, but there is also a true in-crease in incidence of the problem. Since it isrelated to western lifestyle, eating habits andenvironmental factors are discussed. In addi-tion in recent years, detection of extraesopha-geal problems, especially respiratory symptomsand problems, is increasing, often related to re-flux [4, 5]. A special interest in this disorderhas emerged in the past 15 years since studieshave shown the possible connection betweenreflux, the development of intestinal metaplasiain the esophagus, and the increase in the inci-dence of adenocarcinoma in Barrett’s esopha-gus [6–10].The pathophysiologic background of the
disease is multifactorial, as has been shown inrecent years [11, 16]. The main reason forpathologic reflux is a malfunction of the anti-reflux barrier at the level of the gastroesopha-geal junction. This antireflux barrier consistsof the high pressure zone of the lower esopha-geal sphincter as well as the hiatus or thephrenico-esophageal ligament, also causing apinching effect at the level of the lower esopha-geal sphincter [13, 14]. The lower esophagealsphincter has been assessed quantitatively bymechanical parameters such as the lower eso-phageal sphincter pressure, the overall length,and the intraabdominal length. On the otherhand, a functional description of transient low-er esophageal sphincter relaxations described
by many gastroenterologists brings up moredynamic facts on the antireflux barrier [13,16].
Definition
An important issue when discussing patho-physiology is the appropriate definition of thedisease. Several definitions have been dis-cussed in the past decades. Currently, the defi-nition of the GENVAL-consensus conference isbeing widely used [1]. Based on the latter, gas-troesophageal reflux disease is present whenthe person/patient has a risk of complicationsdue to excessive reflux and/or a significant re-duction of her/his quality of life and well-being. Of course, the definition of gastroeso-phageal reflux disease can be discussed contro-versially since there is no diagnostic test thatproves the presence of this disease in all casesand is able to exclude the disease at the sametime [11, 12]. Endoscopy has a high specificityand can show the presence of esophagitis.However, its sensitivity is not sufficient sinceonly about 60% of patients with gastroesopha-geal reflux disease have developed an endosco-pically-visible esophagitis at the time of theinitial investigation. Similar circumstances canbe discussed for 24-hour-esophageal pH moni-toring, which is often called the gold standardin the objective assessment of gastroesophagealreflux disease [13]. It quantitatively measuresgastroesophageal acid exposure in the esopha-geal lumen. Negative results may be caused bytechnical failures, a “good day” in borderlinereflux cases, the combination of mixed refluxwith high proportion of duodenal juice, or anon-acidic stomach under PPI therapy. More-
Pathophysiology of Gastroesophageal RefluxDisease and Indication for Surgical TherapyK.-H. Fuchs
7

over, typical symptoms such as heartburn andregurgitation are of course present in manybut not in all reflux patients. As a conse-quence, symptoms cannot be a reliable guidefor a definitive diagnosis. Therefore the detec-tion of the disease must be based on a spec-trum of diagnostic investigations in order toprove its presence [14].The most accurate definition for the disease
is a pathophysiologic explanation: The diseaseis present when pathologic exposure of theesophageal lumen to gastric juice occurs, andthis can be a pathologic amount of acid and/ora pathologic amount of duodenal componentssuch as bile [12]. The most frequent conditionin gastroesophageal reflux disease is pathologicacid exposure, and therefore this is often usedsynonymously. Nevertheless, the role of duode-nogastroesophageal reflux has been investi-gated recently, and its importance in complica-tions of the disease such as Barrett’s esophagushas been shown [15].In order to obtain more information about
the definition of gastroesophageal reflux dis-ease used in clinical practice, the definitions ofthe disease used in randomized trials for anti-reflux therapy can be reviewed. It is surprisingwhat a variety of definitions have been usedfor the disease by several authors performingrandomized trials in the past decades. In 25randomized trials focusing on surgical therapyof the disease, the definition used by the ma-jority of the studies was the presence of symp-toms and esophagitis [17–40]. Only in aboutone-third of the studies was positive pH-moni-toring as a more specific tool to verify patho-logical esophageal acid exposure used as thedefinition. Only a few studies relied on symp-toms only, since symptoms can be an unreli-able guide for the presence of gastroesophagealreflux disease.It must be emphasized that the presence of
typical symptoms such as heartburn and acidor fluid regurgitation have been shown to bevery specific symptoms with a positive predic-tive value for therapeutic success [41]. Theauthors of this study have shown that a goodresult of laparoscopic antireflux surgery ismore probable in patients with preoperativepresence of typical symptoms of reflux such asheartburn and regurgitation, a preoperativepositive test in 24-hour-esophageal pH moni-
toring showing a pathological acid exposure inthe esophagus, and a positive response to pro-ton-pump inhibitors, indicating that medicalacid reduction will also reduce at least some ofthe heartburn of the patient.Regarding the diagnostic requirements, pH
monitoring and endoscopy are necessary forthe objective documentation of the disease[11–13]. With manometry other esophagealfunctional disorders can be excluded, whichpotentially cause a postoperative failure, espe-cially spastic disorders [11]. Since a weak low-er esophageal sphincter has been shown to bea poor prognostic sign regarding the futureprognosis of GERD, one could use this criteri-on for the indication [42]. In addition, selec-tion of patients with preoperative normal loweresophageal sphincter parameters can be indica-tive for worse postoperative results [43]. How-ever, several studies have shown that its predic-tive value for the postoperative results remainscontroversial and is therefore not recommend-ed by gastroenterologists [44, 45].Currently gastroesophageal reflux disease has
been redefined in three subgroups [1]. Thesesubgroups are nonerosive reflux disease, erosivereflux disease, and Barrett’s esophagus. This is areasonable division. However, it must be kept inmind that there is some overlapping especiallybetween patients with Barrett’s esophagus anderosive gastroesophageal reflux disease, since ithas been shown that this overlapping is presentin at least 30% of the Barrett’s patients in severalseries [11, 12, 15, 46, 47].
The antireflux barrier
The lower esophageal sphincter has been as-sessed quantitatively by mechanical parameterssuch as the lower esophageal sphincter pres-sure, the overall length, and the intraabdom-inal length [11, 13]. Since reflux can be causedby different factors such as elevation of intra-gastric pressure, elevation of intraabdominalpressure and loss of gravity when persons laydown. In persons in a supine position, thesphincter system must prevent reflux in severalways. The intraabdominal portion of the loweresophageal sphincter is involved in preventing
� K.-H. Fuchs52

reflux during the swallowing of the patient.Both the intraabdominal sphincter length andthe pinching effect of the diaphragm help toclose the sphincter during elevation of intraab-dominal pressure. The high pressure zone onitself at rest prevents reflux in a person’s su-pine position. Transient sphincter relaxationhas been described by many gastroenterolo-gists as the most important causes of refluxdisease [13, 16]. This is supported by a num-ber of studies showing abnormal acid exposurein the esophagus correlating with sphincter re-laxation on simultaneous pH and motility re-cordings. In healthy volunteers the majority ofreflux episodes occur during transient sphinc-ter relaxations [1]. In reflux patients, especiallyin the postprandial phase, these relaxationsoccur more often. However, it is somewhatcontroversial that in patients with severe refluxdisease, reflux episodes occur also withouttransient sphincter relaxations.The mechanical incompetence of the lower
esophageal sphincter has been described byDeMeester, using the overall length of thesphincter which is in the physiologic situation3–4 cm long at the distal end of the esophagusas relevant criteria [11]. The resting tone ofthe sphincter characterized by the lower eso-phageal sphincter pressure varies in healthyvolunteers in relation to the intragastric pres-sure between 10 and 30 mmHg. There are cir-cadian changes with a low level in the post-prandial phase and a high level at night. Thesphincter tone is regulated by intrinsic and ex-ternal factors and is influenced by intraabdom-inal pressure changes, gastric dilatation as wellas composition of food and medication. Asmentioned above, the intraabdominal length ofthe sphincter characterizing the segment of thesphincter which is exposed to the intraabdom-inal pressure is important for the optimalfunctioning of the antireflux barrier. Stress re-flux occurs if an elevation of the intraabdom-inal pressure causes an overriding of the pres-sure level of the lower esophageal sphincter.Free reflux occurs without any changes ofintragastric pressure and the pressure of thesphincter. Quantification of the lower esopha-geal sphincter and its mechanical componentsis expressed by manometric assessment ofsphincter length, the intraabdominal length,and the sphincter pressure.
The role of a hiatal hernia has been inter-preted controversially over the years [13, 48].In the past decades hiatal hernia often ob-served with the presence of the reflux disease.Currently it has been shown that 80% of pa-tients with GERD have a hiatal hernia, thusloosening the pinching effect of the dia-phragm. It is also true that hiatal hernia is apromoter of gastroesophageal reflux. In thephysiologic situation a substantial part of thelower esophageal sphincter is kept tight in theabdominal cavity and to the hiatal crura by anarrow fixation of the phrenico-esophagealligament. The area of the lower esophagealsphincter is integrated in the architecture ofthe hiatus and the hiatal crura, causing thepinching effect mentioned above. In case of ahiatal hernia which usually develops in a per-son older than 50 years, the loosening of thephrenico-esophageal ligament fixation and thetissue of the GE junction allows gliding andcauses temporary to permanent incompetenceof the lower esophageal sphincter system.
Esophageal peristalsis
Esophageal clearance and peristaltic functionof the esophageal body is also involved in pro-ducing increased esophageal exposure to gas-tric juice [11, 12]. The physiologic swallowingfunction is involved in neutralizing the refluxof gastric acid through the swallowing ofsaliva. Another reason is impaired esophagealperistalsis either by a pre-existing motility dis-order resulting often in simultaneous and in-terrupted contractions or weak peristalsis dueto inflammation of the esophageal wall causedby esophagitis. Impaired esophageal peristalsiscan be defined as more than 30% of non-effec-tive contractions such as weak amplitude lowerthan 30 mmHg or non-propulsive peristalsis.Impaired esophageal peristalsis can lead to in-creased exposure of gastric juice to the esopha-geal mucosa by delayed esophageal emptying.This can cause a vicious cycle, since pre-exist-ing esophageal motility disorders will cause anincrease in acid exposure which again willcause inflammation and further loss of peri-staltic activity. This, in turn, causes more eso-
7 Pathophysiology of Gastroesophageal Reflux Disease and Indication for Surgical Therapy � 53

phagitis. So far it is not exactly known whichlevel of physiological motor activity is neces-sary to keep a sufficient peristalsis for suffi-cient esophageal emptying. In healthy volun-teer studies up to 30% of peristaltic action isnon-effective. Severe motility disorders becomeclinically relevant probably only when 70–80%of the peristaltic actions are non-effective,since gravity compensates a lot [43–45, 49].Recent studies with impedance manometryhave provided more insights [50].
Mucosal resistance
Mucosal resistance is not investigated on aroutine basis in patients with the disease. It is,however, an important factor in assessing theability of gastric juice to cause toxic effects inthe esophageal wall [51, 52]. Few investigationshave been reported to describe this process. Ithas been shown that toxic activity of gastricjuice containing acid and bile as well as pan-creatic components is a major factor in eso-phageal injury.
Duodeno-gastroesophageal reflux
Gastroduodenal dysfunctions in reflux diseasehave been neglected for decades [11, 12]. Eversince new pathophysiologic understandingsemerged that Barrett’s esophagus is significant-ly associated with duodeno-gastroesophagealreflux, more attention and research activitieshave been focussed on this matter [15, 46]. Ithas been shown that acid production can beelevated in Barrett’s esophagus. It has alsobeen shown duodeno-gastroesophageal refluxcan be detected in 10–15% of patients with re-flux disease. Only recently it has been provenby many centers that Barrett’s esophagus is as-sociated with an increased exposure to bileand pancreatic components. Even though duo-deno-gastric reflux is a physiologic phenome-non, once present it is obviously involved inthe development of more serious esophagealmucosal injury together with acid.
Gastroduodenal disorders
The backup of gastric contents in the intraduo-denal segment due to delayed gastric emptyingcan cause pathologic acid reflux and bile refluxinto the esophagus. In some patients delayedgastric emptying can be the only cause ofpathologic reflux through a normal physiologicsphincter mechanism [53]. Transient sphincterrelaxations are very important in these patientsfor deflation of the stomach. This is of majorimportance in patients who are candidates forantireflux surgery since after a fundoplicationthis deflation mechanism is not possible any-more and can cause severe gas bloat syndromeif the stomach cannot deflate air neither in aproximal direction nor in the distal direction.
Indication for surgery
There is very little evidence-based informationto justify certain factors for the indication ofantireflux surgery. With the introduction ofminimal invasive technique, antireflux surgeryhas boomed in the past ten years. In most wes-tern countries the number of antireflux opera-tions have more than tripled as compared withthe time before the introduction of minimalaccess techniques. This happened at a timewhen the most potent antisecretory drugs wereon the market, which stimulates the controver-sial discussion between gastroenterologists andsurgeons regarding the indication for surgery.The presence of severe esophagitis was for
many surgeons an indication for surgery. To-day many authors are convinced that the onlycriteria for therapeutic success is the removalof symptoms, may it occur by healing of eso-phagitis or not [1]. In surgical literature, bothremoval of symptoms and healing of esophagi-tis are necessary to determine a successful sur-gical therapy [54, 55].In summary, for the establishment of the in-
dication of a surgical procedure, gastroenterol-ogists and surgeons should use more than onecriteria for the definition and the verificationof gastroesophageal reflux disease. In severalconsensus projects it was documented that en-doscopic signs of esophagitis should have been
� K.-H. Fuchs54

documented at present or in the past at leastonce. In addition, a positive 24-hour pH moni-toring together with typical symptoms of thedisease such as heartburn and/or regurgitationare important criteria for the presence of dis-ease, which are needed for indication.
Conclusions
Gastroesophageal reflux disease is a multifac-torial process. The most frequent pathophysio-logic cause is a functional incompetence of thegastroesophageal junction as antireflux barrier.In a substantial part of patients other factorsare also involved isolated or in combinationwhich usually aggravate the disease and alsoimplicate a special therapeutic consideration.Prior to any decision for a long term therapeu-tic management or especially prior to anti-reflux surgery these pathologic componentsshould be assessed and documented. The indi-cation for antireflux surgery, which should beperformed by minimal access technique, mustbe based on multiple factors such as severesymptoms for a long time, documented pres-ence of the disease and documented morpho-logic and functional defects.
References
1. Dent J, Brun J, Fendrick AM, Fennerry MB, Jans-sens J et al (1999) Genval Workshop Group: Anevidence-based appraisal of reflux disease manage-ment. Gut 44:S1–16
2. Locke G, Talley NJ, Fett SL (1997) Prevalence andclinical spectrum of gastroesophageal reflux: apopulation based study in Olmsted-County, Min-nesota. Gastroenterology 112:1448–1456
3. Louis E, DeLooze D, Deprez P (2002) Heartburn inBelgium: prevalence, impact on daily life, and uti-lization of medical resources. Eur J GastroenterolHepatol 14:279–284
4. Jaspersen D, Weber R, Hammer LH (1996) Effectof omeprazole on the course of associated esopha-gitis and laryngitis. J Gastroenterol 31:765–767
5. Micklefield GH, Radu HJ, Grewing I (1998) Acidesophago-pharyngeal reflux as etiology of hoars-ness. Laryngorhinootologie 77:496–499
6. Haggit RC, Tryzelaar J, Ellis FH, Colcher H (1978)Adenocarcinoma complicating columnar-epitheli-
um-lined (Barrett’s) esophagus. Am J Clin Pathol70:1
7. Hameeteman W, Tytgat GNJ, Houthoff HJ, Van denTweel JG (1989) Barrett’s esophagus: developmentof dysplasia and adenocarcinoma. Gastroenterolo-gy 96:1249–1256
8. Pera M, Cameron AJ, Trastek VF, Carpenter HA,Zinsmeister AR (1993) Increasing incidence ofadenocarcinoma of the esophagus and esophago-gastric junction. Gastroenterology 104:510–513
9. Lagergren J, Bergström R, Lindgren A, Nyrén O(1999) Symptomatic gastroesophageal reflux as arisk factor for esophageal adenocarcinoma. NewEngl J Med 340:825–831
10. DeMeester SR, DeMeester TR (2000) Columnarmucosa and intestinal metaplasia of the esophagus:fifty year controversy. Ann Surg 231(2):303–321
11. DeMeester TR (1987) Definition, detection andpathophysiology of gastroesophageal reflux disease.In: DeMeester TR, Matthews HR (eds) Internationaltrends in general thoracic surgery, vol 3. Benignesophageal disease. Mosby, St. Louis, pp 99–127
12. Fuchs KH, Freys SM, Heimbucher J, Fein M,Thiede A (1995) Pathophysiologic spectrum in pa-tients with gastroesophageal reflux disease in asurgical GI function laboratory. Diseases of theEsophagus 8:211–217
13. Zaninotto G, DeMeester TR, Schwizer W, Johans-son KE, Cheng SC (1988) The lower esophagealsphincter in health and disease. Am J Surg 155:104–111
14. Costantini M, Crookes PF, Bremner RM, Hoeft SF,Ehsan A, Peters JH, Bremner CG, DeMeester TR(1993) Value of physiologic assessment of foregutsymptoms in a surgical practice. Surgery 114(4):780–786
15. Fein M, Ireland AP, Ritter MP, Peters JH, HagenJA, Bremner CG, DeMeester TR (1997) Duodeno-gastric reflux potentiates the injurious effects ofgastroesophageal reflux. J Gastrointest Surg 1:27–33
16. Mittal RK, Holloway RH, Penagini R, Blackshaw A,Dent J (1995) Transient lower esophageal sphincterrelaxation. Gastroenterology 109:601–610
17. Behar J, Sheahan DG, Biancani P, Spiro HM, StorerEH (1975) Medical and surgical management of re-flux esophagitis. N Engl J Med 293(6):263–268
18. Thor KBA, Silander T (1989) A long-term random-ized prospective trial of the Nissen procedure ver-sus a modified Toupet technique. Ann Surg 210:719–724
19. Kmiot WA, Kirby RM, Akinola D, Temple JG(1991) Prospective randomized trial of Nissen fun-doplication and Angelchik prosthesis in the surgi-cal treatment of medically refractory gastro-oeso-phageal reflux disease. Br J Surg 78:1181–1184
20. Lundell L, Abrahamsson H, Ruth M, Sandberg L,Olbe L (1991) Lower esophageal sphincter charac-teristics and esophageal acid exposure followingpartial or 360� fundoplication: Results of a pro-spective, randomized, clinical study. World J Surg15:115–121
7 Pathophysiology of Gastroesophageal Reflux Disease and Indication for Surgical Therapy � 55

21. Spechler SJ and the Department of Veterans AffairsGastroesophageal Reflux Disease Study Group(1992) Comparison of medical and surgical thera-py for complicated gastroesophageal reflux diseasein veterans. N Engl J of Med 12:786–792
22. Eyre-Brook IA, Codling BW, Gear MWL (1993) Re-sults of a prospective randomized trial of the An-gelchik prosthesis and of a consecutive series of119 patients. Br J Surg 80:602–604
23. Janssen IMC, Gouma DJ, Klementschitsch P, van derHeyde MN, Obertop H (1993) Prospective random-ized comparison of teres cardiopexy and Nissenfundoplication in the surgical therapy of gastro-oe-sophageal reflux disease. Br J Surg 80:875–878
24. Hill ADK, Walsh TN, Bolger CM, Byrne PJ, Hen-nessy TPJ (1994) Randomized controlled trial com-paring Nissen fundoplication and the Angelchikprosthesis. Br J Surg 81:72–74
25. Ortiz EA, Martinez de Haro LF, Parrilla P, MoralesG, Molina J, Bermejo J, Liron R, Aguilar J (1996)Conservative treatment versus antireflux surgeryin Barrett’s oesophagus: long-term results of a pro-spective study. Br J Surg 83(2):274–278
26. Lundell L, Abrahamsson H, Ruth M, Rydberg L,Lonroth H, Olbe L (1996) Long-term results of aprospective randomized comparison of total fundicwrap (Nissen-Rossetti) or semifundoplication(Toupet) for gastro-oesophageal reflux. Br J Surg83(6):830–835
27. Rydberg L, Ruth M, Lundell L (1997) Does oeso-phageal motor function improve with time aftersuccessful antireflux surgery? Results of a prospec-tive, randomized clinical study. Gut 41:82–86
28. Watson DI, Pike GK, Baigrie RJ, Mathew G, DevittPG, Britten-Jones R, Jamieson GG (1997) Prospec-tive double-blind randomized trial of laparoscopicNissen fundoplication with division and withoutdivision of short gastric vessels. Ann Surg 226(5):642–652
29. Laws HL, Clements RH, Swillie CM (1997) A ran-domized, prospective comparison of the Nissenfundoplication versus the Toupet fundoplicationfor gastroesophageal reflux disease. Ann Surg225(6):647–653, discussion 654
30. Anderson JA, Myers JC, Watson DI, Gabb M,Mathew G, Jamieson GG (1998) Concurrent fluoro-scopy and manometry reveal differences in laparo-scopic Nissen and anterior fundoplication. Dig DisSci 43(4):847–853
31. Lundell L, Dalenbäck J, Hattlebakk J et al (1998)Outcome of open antireflux surgery as assessed ina nordic multicentre, prospective clinical trial. EurJ Surg 164:751–757
32. Rydberg L, Ruth M, Abrahamsson H, Lundell L(1999) Tailoring antireflux surgery: a randomizedclinical trial. World J Surg 23:612–618
33. Watson DI, Jamieson GG, Pike GK, Davies N, Ri-chardson M, Devitt PG (1999) Prospective ran-domized double-blind trial between laparoscopicNissen fundoplication and anterior partial fundo-plication. Br J Surg 86:123–130
34. Luostarinen MES, Isolauri JO (1999) Randomizedtrial to study the effect of fundic mobilization onlong-term results of Nissen fundoplication. Br JSurg 86:614–618
35. Csendes A, Burdiles P, Korn O, Braghetto I, Huer-tas C, Rojas J (2000) Late results of a randomizedclinical trial comparing total fundoplication versuscalibration of the cardia with posterior gastropexy.Br J Surg 87:289–297
36. Bais JE, Bartelsman JF, Bonjer HJ, Cuesta MA, GoPM, Klinkenberg-Knol EC, van Lanschot JJB, Na-dorp JH, Smout AJ, van der Graaf Y (The Nether-lands Antireflux Surgery Study Group) (2000) Lap-aroscopic or conventional Nissen fundoplicationfor gstroesophageal reflux disease: randomizedclinical trial. Lancet 355:170–174
37. Nilsson G, Larsson S, Johnsson F (2000) Random-ized clinical trial of laparoscopic versus open fun-doplication: blind evaluation of recovery and dis-charge period. Br J Surg 87:873–878
38. Lundell L, Miettinen P, Myrvold HE, Pedersen SA,Liedman B, Hatlebakk JG, Julkonen R, Levander K,Carlsson J, Lamm M, Wiklund I (2001) Continued(5-year) followup of a randomized clinical studycomparing antireflux surgery and omeprazole ingastroesophageal reflux disease. J Am Coll Surg192(2):172–179, discussion 179–181
39. Luostarinen M, Virtanen J, Koskinen M, Matikai-nen M, Isolauri J (2001) Dysphagia and oesopha-geal clearance after laparoscopic versus open Nis-sen fundoplication. A randomized, prospectivetrial. Scand J Gastroenterol 6:565–571
40. Spechler SJ, Lee E, Ahnen D, Goyal RK, Hirano I,Williford WO (2001) Long-term outcome of medi-cal and surgical therapies for gastroesophageal re-flux disease. JAMA 285:2331–2338
41. Campos GM, Peters JH, DeMeester TR, Oberg S,Crookes PF, Tan S, DeMeester SR, Hagen JA, Brem-ner CG (1999) Multivariate analysis of factors pre-dicting outcome after laparoscopic Nissen fundo-plication. J Gastrointest Surg 3(3):292–300
42. Kuster E, Ros E, Toledo-Pimentel V, Pujol A, Bor-das JM, Grande IC (1994) Predictive factors of thelong term outcome in gastro-oesophageal refluxdisease: six year follow up of 107 patients. Gut35(1):8–14
43. Blom D, Peters JH, DeMeester TR, Crookes P, Ha-gen JA, DeMeester SR, Bremner CG (2002) Physio-logic mechanism and preoperative prediction ofnew-onset dysphagia after laparoscopic Nissenfundoplication. J Gastrointest Surg 6(1):22–27
44. Fang J, Bjorkman D (2002) Prefundoplication test-ing: is manometry needed? Am J Gastroenterol97(4):1056–1058
45. Fibbe C, Layer P, Keller J et al (2001) Esophagealmotility in reflux disease before and after fundo-plication: a prospective, randomized, clinical andmanometric study. Gastroenterology 121:5–14
46. Vaezi MF, Richter JE (1995) Synergism of acid andduodeno-gastro-esophageal reflux in complicatedBarrett’s esophagus. Surgery 117:699–704
� K.-H. Fuchs56

47. Tack J, Koek G, Demedts I, Sifrim D, Janssens J(2004) Gastroesophageal Reflux Disease Poorly Re-sponsive to Single-Dose Proton Pump Inhibitors inPatients without Barrett’s Esophagus: Acid Reflux,Bile Reflux, or Both? Am J Gastroenterol 99:981–988
48. Fein M, Ritter MP, DeMeester TR, Oberg S, PetersJH, Hagen JA, Bremner CG (1999) Role of the low-er esophageal sphincter and hiatal hernia in thepathogenesis of gastroesophageal reflux disease. JGastrointest Surg 3(4):405–410
49. Timmer R, Breumelhof R, Nadorp JH, Smout AJ(1994) Oesophageal motility and gastro-oesopha-geal reflux before and after healing of reflux oeso-phagitis. A study using 24 hour ambulatory pHand pressure monitoring. Gut 35:1519–1522
50. Sifrim D, Castell D, Dent J, Kahrilas PJ (2004) Gas-tro-oesophageal reflux monitoring: review and con-sensus report on detection and definitions of acid,non-acid and gas reflux. Gut 53(7):1024–1031
51. Orlando RC (1996) Why is the high grade inhibi-tion of gastric acid secretion afforded by proton
pump inhibitors often required for healing of re-flux esophagitis? An epithelial perspective. Am JGastroenterol 91:1692–1696
52. Orlando RC (2000) Pathophysiology of gastroeso-phageal reflux disease: offensive factors and tissueresistance. In: Orlando RC (eds) Gastroesophagealreflux disease. Dekker, New York, pp 164–192
53. Schwizer W, Hinder RA, DeMeester TR (1989)Does delayed gastric emptying contribute to gas-troesophageal reflux disease? Am J Surg 157:74–81
54. Eypasch E, Neugebauer E, Fischer F, Troidl H(1997) Laparoscopic antireflux surgery for gastro-esophageal reflux disease (GERD). Results of aconsensus development conference. Surg Endo-scopy 11:413–426
55. Fuchs KH, Feussner H, Bonavina L, Collard JM,Coosemans W for the European Study Group forAntireflux Surgery (1997) Current status andtrends in laparoscopic antireflux surgery: results ofa consensus meeting. Endoscopy 29:298–308
7 Pathophysiology of Gastroesophageal Reflux Disease and Indication for Surgical Therapy � 57

Introduction
In Western societies, gastroesophageal refluxhas assumed importance for two reasons. Firstit is a common disorder with as many as 40%of the adult population having heartburn atleast once a month and 7% experiencing it dai-ly. Secondly, it is associated with adenocarci-noma of the cardia. Because the incidence ofthis is rising at a considerable rate (particular-ly in white Western males), cure of reflux mayassume an important role in preventing thiscancer in the future.In the past, surgical treatment of gastroeso-
phageal reflux disease has tended to be limitedto those patients with complicated reflux diseaseor those with very severe symptoms of reflux.Recently the surgical role has changed some-what, and although varying from country tocountry, there is now an increasing tendencyto utilize surgery at earlier stages in the courseof reflux disease. This is because of changes insurgical technique (most notably the introduc-tion of laparoscopic surgery), the previouslymentioned rising incidence of adenocarcinomaof the cardia associated with uncontrolled refluxdisease and, paradoxically, because of improve-ments in medical therapy (see later).
Which patients should be consideredfor antireflux surgery?
Patients with gastroesophageal reflux diseasecan be divided broadly into 2 groups:� first are patients who have complicated re-flux disease, and
� second are patients who have straight for-ward symptoms without complications.
� Patients with complicated reflux disease
� Reflux with stricture formation. With extreme-ly dense and undilatable fibrotic strictures, re-section is the only effective treatment, but for-tunately it is unusual today to see patients withsuch advanced strictures. Dilatable stricturesin young and fit patients are best treated byfundoplication and dilatation [2]. However,many patients who develop strictures are el-derly or infirm and the use of proton pump in-hibitors with dilatation has proven very effec-tive treatment and thus has lessened the needfor operation in high risk patients [3].
� Reflux with respiratory complications. Whengastro-esophageal regurgitation leads to spill-over into the respiratory tree, this can causechronic respiratory illness, such as recurrentpneumonia and asthma [4]. This is a firm in-dication for antireflux surgery, as proton pumpinhibitors’ predominant action is to block acidsecretion rather than alter gastroesophageal re-gurgitation.Such problems as halitosis, acid taste in the
mouth, chronic laryngitis, chronic pharyngitis,and loss of enamel on teeth are sometimes at-tributed to gastroesophageal reflux. There is alittle doubt that on occasions such problemsdo arise in refluxing patients, but acid isusually the damaging agent in these situations,and antireflux surgery should not be consid-ered unless proton pump inhibition has shownunequivocally that it ameliorates the problem.
� Reflux with columnar lined esophagus (Barrett’s
esophagus). At the present time it remains anopen question whether Barrett’s esophagus perse is an indication for antireflux surgery. Thereis experimental evidence to suggest that con-
Gastroesophageal Refluxand its Surgical ManagementG.G. Jamieson, D. I. Watson
8

tinuing reflux may be deleterious in regard tomalignant change in esophagus mucosa [5],and one prospective randomized trial has sug-gested that antireflux surgery gives superiorresults to drug therapy [6]. However protonpump inhibitors were only introduced into themedical arm of that trial in its later years.Therefore, one recommendation which might
be given at present is that the indications forsurgery are related to the reflux symptoms andnot to the presence of columnar lined esophagusper se. However, as most observers regard co-lumnar lined esophagus as being at the severeend of the reflux spectrum, it seems reasonableto factor it in as a further reason for givingstrong consideration to antireflux surgery. Onemust also keep an open mind in regard to thelink between reflux and intestinal metaplasia atthe lower end of the esophagus. If this linkand the progression to adenocarcinoma becomefirmly established, then the role of antirefluxsurgery will almost certainly be expanded.
� Patients with uncomplicated reflux disease
In the past, it was easy to make the recommen-dation for antireflux surgery on the basis whenthe disorder was spoiling the patients’ enjoy-ment of living, in spite of the best that medicaltherapy has to offer. This indication remainsvalid, but medical therapy in the form of pro-ton pump inhibitors is so effective today thatit is only a small minority of patients who donot get substantial or complete relief to theirsymptoms with the use of such agents [7].Why then does there appear to be a trend forpatients to present for antireflux surgery ingreater numbers than ever? There are severalreasons for this.First, if patients will stop taking their proton
pump inhibitors, symptoms of reflux recurvery rapidly, and sometimes the symptoms areworse than they were prior to taking protonpump inhibitors. This may relate to parietalcell hyperplasia which has been reported inpatients taking proton pump inhibitors [8].The importance of this finding remains to beelucidated. Regardless, many patients do notlike to be dependent on drugs to be symptomfree. Thus, the second and related reason isthat many patients with reflux potentially have
years of life remaining, and they do not wishto take drugs in the long term when the drugshave not been established as safe if taken formany years. It must be said, however, thatthere is no particular reason to think they willnot establish such a record of safety.The cost of proton pump inhibitors to the
patients varies from country to country, but itis an additional factor, as is the cost of thedrugs to society as a whole.An additional factor, already mentioned, is
the rising incidence of adenocarcinoma of thecardia associated with gastroesophageal refluxdisease [9, 10]. However, whether antirefluxsurgery is more effective at preventing thedevelopment of columnar lined esophagus andcarcinoma of the cardia than long term protonpump inhibition remains a controversial issue.But perhaps none of these reasons, even
taken together, would have convinced patientsto take the operative alternative, if open sur-gery had remained the standard. There seemslittle doubt that the advent of laparoscopic fun-doplication [11, 12] with its greatly reducedmorbidity has also been a major factor in theswing to operation in the treatment to reflux.
What are the advantages anddisadvantages of antireflux surgery?
� Advantages
The advantages are fairly clear. The operationis the only treatment which actually cures theproblem, i.e. stops gastric contents from reflux-ing into the esophagus. So in terms of their re-flux, patients can eat whatever foods theychoose, they can lie down flat, bend over etc.,without reflux occurring; importantly, they donot have to take any tablets.
� Disadvantages
The first disadvantage is the morbidity asso-ciated with the operation (see later in regard tocomplications). It is true that the advent oflaparoscopic surgery has meant that the painof the open operation has abolished. Neverthe-
� G.G. Jamieson, D. I. Watson60

less, most patients have some difficulty inswallowing in the immediate postoperative per-iod. Fortunately, in the great majority of casesthis is only a temporary problem, but the timeit takes to get better is widely variable and oc-casionally takes several months [12].Furthermore, the great majority of patients
feel very full after eating even small meals,which often leads to some postoperative weightloss. In the patients who are overweight at thetime of surgery (the majority!) this is some-times seen as an advantage of the operation,rather than a disadvantage. This restriction onmeal size also usually disappears over a fewmonths. Because fundoplication, along with allother effective antireflux operations, producesa one way valve, swallowed air, which haspassed into the stomach, usually cannot passback through the valve. Thus, patients have tobe forwarned that they will not be able tobelch effectively after the operation and soshould be cautious about taking gassy drinks.As swallowed gas cannot be belched either, thegreat majority of patients are aware of in-creased flatulence with increased borborygmiand increased passage of wind after the proce-dure. For similar reasons, patients will be un-able to vomit after the procedure, and shouldbe informed of this. This is not of importancewith such conditions as gastroenteritis, whenpatients will dry retch only. In fact, it only as-sumes importance if the patient should developgastrointestinal obstruction. As vomiting cannotoccur in such circumstance, the patient has aunique, large, closed loop obstruction (whichcan be decompressed by passing a nasogastrictube).An overwhelming majority of patients state
that the disadvantage of the procedure is faroutweighed by the advantages of the operation,but occasionally this is not the case. Perhaps itmay prove possible, by the use of preoperativepsychological questioning, to predict thosepatients who will be troubled by what to themajority of patients are minor nuisances,although this remains to be proven [13].
Operations available
There is no doubt that the fundoplication in-troduced by Rudolf Nissen in 1956, or somevariant of it, is overwhelmingly the most popu-lar operation in the world today. Total fundo-plications such as the Nissen or partial fundo-plications, whether anterior or posterior, prob-ably all work in similar fashion. And the fash-ion may be as much mechanical as physiologi-cal, as it has been demonstrated that these pro-cedures are effective, not only when placed inthe chest in vivo [14] but also on the benchtop,i.e. ex vivo [15].The principles of fundoplication are to mo-
bilize the lower esophagus and to wrap thefundus of the stomach, either partially ortotally, around the esophagus. When the eso-phageal hiatus is enlarged, it is narrowed bysutures to prevent paraesophageal herniationpostoperatively, and also prevent the wrapbeing pulled up into the chest (although thefundoplication will work in the chest, othercomplications such as gastric ulceration some-times occur in this situation).These operations can be undertaken either
transthoracically or transabdominally. Althoughthe latter seems a simpler approach, the choicetends to depend on whether the surgeon ispredominantly a thoracic or predominantly anabdominal surgeon.Operations which are limited to one or the
other approach (e.g. thoracic-Belsey and ab-dominal-Hill) have never gained the wide-spread popularity of the Nissen fundoplicationoperation.
Traditional open fundoplication
Fundoplication was first described by Nissen1956 [16] following the serendipitous discoverythat a fundal patch, used to reinforce an eso-phageal suture line, also prevented gastroeso-phageal reflux. Whilst achieving good controlof pathological reflux in the majority of pa-tients [17], an incidence of adverse sequelaehas led to the subsequent modification of Nis-sen’s original technique. Shortening the fundo-
8 Gastroesophageal Reflux and its Surgical Management � 61

plication length to 1 to 2 cm, dividing theshort gastric vessels to achieve full mobiliza-tion of the gastric fundus, calibration of aloose fundoplication over a large intra-esopha-geal bougie, and modification of the completefundoplication to one of a number of partialfundoplication variants, have all been advo-cated. Few of these modifications, however,have been evaluated within the context of pro-spective randomized trials.Following four decades of experience with
antireflux procedures, long term outcomes fol-lowing open surgery have been well described.The postoperative hospital stay following opensurgery ranges from 7 to 14 days, and shortterm morbidity is acceptable. Long-term suc-cess is achieved in the majority of patients[18, 19].Adverse outcomes following open Nissen
fundoplication include persistent dysphagiaand the gas bloat symptoms. Although lesscommon in late follow-up, many patients re-port troublesome early dysphagia [21]. The as-sessment of dysphagia symptoms, however, canbe difficult because variable methods of clini-cal assessment and scoring are used in the var-ious reported studies. There is also the poten-tial for the introduction of assessment bias byclinician investigators, particularly if follow-upis performed by the operating surgeon. Despitethese difficulties, it is likely that the incidenceof persistent long-term troublesome dysphagiais less than 5% following Nissen fundoplica-tion. Uncontrolled reports suggest that the per-formance of a partial fundoplication variantmay reduce this incidence [22]. However, todate, this proposal has not been proven by ran-domized trials.Despite the large number of publications de-
scribing fundoplication outcomes in the era ofopen surgery, few randomized trials have beenconducted. Three trials have compared a Nis-sen fundoplication with a posterior partial fun-doplication [23, 24], and one has compared aNissen fundoplication with a Hill and a Belseyprocedure [25]. None of these studies describeany significant increase in the likelihood or se-verity of dysphagia following Nissen fundopli-cation, compared to a posterior partial fundo-plication procedure. However, with the excep-tion of the study reported by Lundell et al.[21] which enrolled 137 patients, all of the
studies assessing the partial fundoplicationvariants enrolled small numbers of patients,which were inadequate to allow one to drawstatistically valid conclusions. Other smallstudies have compared Nissen fundoplicationwith the Angelchik prosthesis and with the Li-gamentum teres cardiopexy, demonstrating ad-vantages for Nissen fundoplication [26, 27].Another compared the Nissen procedure withand without division of short gastric vesselsshowing no difference [28], and a recent largerstudy compared medication with surgical treat-ment therapy [29]. Although findings were infavor of operation, neither the medical nor thesurgical therapy used would now be regardedas optimal.
Laparoscopic fundoplication
Initial reports of small case series of laparo-scopic Nissen fundoplication with follow-up of3 months or less first appeared in the pub-lished literature in 1991 [11, 30]. Althoughthese studies confirmed the technical feasibilityof laparoscopic antireflux surgery, the lack ofadequate follow-up data and the small patientnumbers precluded any adequate assessment ofthe merits of the procedures described. Thefirst large study was published by Cuschieri etal. in 1993, who reported promising resultsfrom a multicenter series of 116 patients [31].Further large single center experiences describ-ing series of more than 100 patients have beenpublished since, with follow-up intervals of 2to 3 years described in some later studies [32].Mean or median operating times vary from 30to 185 minutes in these studies. Some of thereported variation in operating may be due todifferences in laparoscopic technique, as wellas possible increased operation times in somecenters involved in teaching surgical trainees[33, 34]. Reported complication rates rangefrom 2 to 26%, and surgical revision has beenneeded in a small group of patients in most se-ries. Variation in these rates may be influencedby the effect of the institutional learning curve,technical factors associated with the choice ofsurgical technique, and different criteria usedfor the recognition and classification of com-
� G.G. Jamieson, D. I. Watson62

plications in different reports. For exampledysphagia rates may depend on the choice ofclinical measure used to determine post-opera-tive dysphagia, and who applies the measurechosen. The operating surgeon may elicit a dif-ferent response from an independent investiga-tor.Laparoscopic Nissen fundoplication is re-
ported to control reflux symptoms in 91 to100% of patients followed for up to two years,results which mirror previous experience withopen antireflux surgery. Post-operative hospitalstays have been short in all published reports,with mean/median stays ranging from 2 to 5days. Overall results from these initial case se-ries suggest that laparoscopic antireflux sur-gery is effective, and that it results in an over-all reduction in the short term morbidity asso-ciated with surgery for reflux. However, severalcomplications, some of which may be uniqueto the laparoscopic approach, have now beendescribed.
� Pneumothorax. This and accompanying pneu-momediastinum is not an infrequent occurrencein more difficult cases, such as reoperative sur-gery. However, they are of no particular concern,and the CO2 is rapidly absorbed.
� Vascular injury. Vascular injury to the inferiorvena cava, the left hepatic vein, the abdominalaorta, and the inferior phrenic vessels has allbeen reported [35]. It is possible that this com-plication is associated with a combination ofaberrant anatomy, inexperience, and the exces-sive use of monopolar diathermy dissection.Intraoperative bleeding more commonly fol-lows inadvertent laceration of the left lobe ofthe liver by a laparoscopic liver retractor orother instrument, or hemorrhage from shortgastric vessels during fundal mobilization. Arare complication is cardiac tamponade due tolaceration of the right ventricle by a liver re-tractor [36].The overall risk of perioperative hemorrhage
associated with antireflux surgery, however,may well be reduced by the laparoscopicapproach. The risk of splenectomy due to inad-vertent splenic injury during Nissen fundopli-cation is dramatically reduced by the laparo-scopic approach [37]. Whilst splenectomy ratesof 1 to 3% have been reported in association
with open fundoplication, splenectomy is arare event following laparoscopic fundal mobi-lization. It is likely that the more precise dis-section and better anatomical exposure af-forded by the laparoscopic approach minimizesthe likelihood of inadvertent splenic trauma.
� Para-esophageal hiatus herniation. Althoughpara-esophagus hiatus herniation may occa-sionally present in the late follow-up periodfollowing open fundoplication, most large caseseries of the laparoscopic procedure report anincidence of paraesophagus herniation, partic-ularly in the immediate post-operative period.The incidence of this has ranged up to 7% inpublished reports [38]. This problem may bemore likely following laparoscopic surgery forseveral reasons. First is the tendency to extendlaparoscopic esophagus dissection well intothe thorax, second is the increased risk ofbreaching the left pleural membrane, and thirdis the effect of reduced post-operative pain. Re-duced pain may permit more abdominal forceto be transmitted to the hiatal area duringcoughing, vomiting or other forms of early ex-ertion, thereby pushing the stomach into thethorax. It is likely routine hiatal repair will re-duce the risk of this problem [38, 39]. It is alsopossible that some of the apparent variation inthe incidence of this problem reflects the stepstaken to actively look for this complication.Also, the incidence following open fundoplica-tion may be greater than previously recognized[21].
� Dysphagia. Early severe dysphagia requiringsurgical revision has been reported in a num-ber of series. Conversion of a Nissen fundopli-cation to a posterior partial fundoplication hasbeen performed for troublesome dysphagia byboth open and laparoscopic techniques, usuallywith success. Over narrowing of the esophagushiatus, another potential cause of early dyspha-gia may be difficult to assess intraoperativelybecause of reduced tactile feedback duringlaparoscopic surgery. This can be corrected byearly laparoscopic re-intervention to releaseone or two hiatal sutures. Late narrowing ofthe esophagus hiatus due to the post-operativescarring, even in patient’s not undergoing hia-tal repair, has also been reported [40]. It ispossible that this complication is due to an
8 Gastroesophageal Reflux and its Surgical Management � 63

idiosyncratic response to dissection which oc-curs in certain patients. Correction requireswidening of the diaphragmatic hiatus by eitheropen surgical or laparoscopic techniques.
� Pulmonary embolism. Pulmonary embolismhas been reported following laparoscopic anti-reflux surgery. This is likely to result from acombination of primarily mechanical factors.The combination of head up tilt of the operat-ing table, intraabdominal insufflation of gasunder pressure, and placement of the legs ofpatients in stirrups may greatly reduce venous-flow in leg veins [41]. Coagulation changes as-sociated with surgery are not altered by theapplication of laparoscopic techniques [42]. Toprevent this problem it is mandatory that anti-thromboembolism prophylaxis is routinely ap-plied.
� Perforation of the gastrointestinal tract. Per-foration of the esophagus, stomach, duode-num, or bowel has all been described followinglaparoscopic antireflux surgery. Whilst perfora-tion of the small bowel and the colon may berelated to laparoscopic access in general, eso-phagus and gastric perforations are specificrisks of laparoscopic antireflux surgery, withan incidence of approximately 1% reported bymost series. Perforation of the back wall of theesophagus can occur when dissecting the pos-terior aspect of the esophagus with laparo-scopic instruments. The anterior esophaguswall is at risk when a bougie is passed to cali-brate the tightness of the Nissen wrap. Gastricperforation is usually an avulsion injury of thegastric cardia due to rough handling by thesurgical assistant, or the use of inappropriategrasping instruments to retract the stomach.These injuries can be repaired by sutures,applied either laparoscopically or by an opentechnique. Awareness of the potential for theseinjuries is likely to reduce their occurrence[43].
� Mortality. Three deaths have been describedfollowing laparoscopic antireflux procedures[33, 44, 45]. The first was a patient who diedsecondary to peritonitis and sepsis from aduodenal perforation, presumably due to aninstrumental injury occurring outside of therestricted field of view provided by the laparo-
scope [43]. Another was an instance of throm-bosis of both the superior mesenteric arteryand the coeliac axis [44]. This rare complica-tion has also been seen following laparoscopiccholecystectomy, suggesting that it may be re-lated to the use of positive pressure insuffla-tion. A third was a case of infarction of the liverfollowing laparoscopic fundoplication [45].
Laparoscopic versus open surgery
Although laparoscopic approaches may reduceshort term surgical morbidity, on a prioriground, it does not seem likely that long-termoutcomes will be different from equivalentopen procedures. It is even possible that tech-nical modifications introduced to facilitate var-ious laparoscopic approaches will result inpoorer long term outcomes. Equally the supe-rior view of the operative field in laparoscopicsurgery might lead to better outcomes. Untilthe results of long term studies are availablethe true outcome of laparoscopic antirefluxsurgery, and its status as compared with openantireflux surgery will remain unknown.Few direct comparisons of clinical outcome,
surgical morbidity, and cost effectiveness havebeen attempted between early series of laparo-scopic Nissen fundoplication and open surgicalexperience (historical or otherwise) withinsingle institutions. Of the cost comparisonsattempted, all are within the context of theAmerican health system. Given the constraintsof the non-randomized research methodologyfor almost all of these studies, and the differentcost structure of the American health care, afair comparison of laparoscopic and open tech-niques is difficult. All published studies reportthat laparoscopic antireflux surgery reduceshospital treatment costs and early surgicalmorbidity. Similar advantages were identifiedby non-randomized studies which comparedlaparoscopic inguinal hernia repair, appendec-tomy, and cholecystectomy with their equiva-lent open procedures. However, these advan-tages have not always been supported whenprospective randomized trials were reportedsubsequently. Three randomized controlledtrials which compare a laparoscopic Nissen
� G.G. Jamieson, D. I. Watson64

fundoplication with its open surgical equiva-lent have been reported [46–48], two in ab-stract only. Nevertheless, the results of all ofthese early trials confirm advantages for the la-paroscopic approach, albeit less dramatic thanthe advantages expected from the results ofnon-randomized studies.
Randomzied trials of laparoscopicantireflux surgery
Apart from the above three randomized trials,which compare laparoscopic with open Nissenfundoplication, five other randomized trials ex-amining laparoscopic antireflux surgery havebeen reported. Two of these studies compareddifferent techniques for dividing the short gas-tric vessels during laparoscopic Nissen fundo-plication. Laycock et al. [49] randomized 20patients to have these vessels divided betweenmetal clips or by the Ultracision UltrasonicShears (Ultracision, Smithfield, Rhode Island,USA). A time saving was demonstrated for theUltrasonic Shears. Swanstrom and Pennings[50] randomized 31 patients in a similar studywhich also demonstrated a time saving of 10minutes for the Ultrasonic Shear technique.Neither of these studies enrolled a large groupof patients, or attempted to assess outcome dif-ferences between different antireflux proce-dures.A third study, reported by Laws et al. [51],
randomized 39 patients to undergo either alaparoscopic Nissen fundoplication or a laparo-scopic Toupet fundoplication. No significantshort term outcome differences were demon-strated between the two procedures.The first of our own studies enrolled 103 pa-
tients to undergo either a total fundoplicationwithout division of short gastrics vs a totalfundoplication with division of short gastricvessels. At six months there were no significantor indeed appreciable differences between thetwo operations with regard to dysphagia, re-current reflux, gas bloat, or patient satisfaction[52]. The second of our studies randomized105 patients to undergo either a total fundo-plication or an anterior fundoplication bothwithout division of short gastric vessels. At six
months significant differences had emergedbetween the groups with the anterior grouphaving less dysphagia, gas bloat, and a higherpatient satisfaction rate [53]. Both of thesetrials are continuing in order to look at theimportant question of rates of recurrent re-flux.
Controversies and questions in regardto laparoscopic antireflux surgery
The advent of laparoscopic antireflux surgeryhas focused debate between protagonists ofvarious antireflux surgical techniques. Whilstthe Nissen fundoplication remains the tech-nique advocated by the majority of surgeons, anumber of variants such as posterior fundopli-cation, anterior partial fundoplication, andother techniques have been advocated to re-duce the likelihood of post-operative dysphagiaand gas bloat. Some surgeons advocate selec-tive use of partial fundoplication variants forpatients with esophagus dysmotility. Othersadvocate routine application of a particularpartial fundoplication variant. Surgeons havenot reached agreement on these questionswhich still require randomized studies for theirresolution.Even the incidence of disease induced by fi-
brotic shortening of the esophagus remains indoubt. Most surgeons report a very low inci-dence of shortened esophagus during laparo-scopic antireflux surgery, with the incidence ofconversion to an open procedure of this prob-lem being less than 1% [54]. Although thissuggests that the problem is infrequent, theability of surgeons to determine adequate eso-phagus length at the time of laparoscopic anti-reflux surgery has been questioned with thesuggestion that the problem is more commonthan usually appreciated [55, 56]. Because ofthis Kauer et al. [55] have advocated an opentransthoracic approach to perform a Collis gas-troplasty in patients with a hiatal hernia lengthof more than 5 cm. Swanstom et al. [56] havedescribed a method for the laparoscopic con-struction of a Collis gastroplasty if the surgeonconsiders the gastroesophageal junction cannotbe brought down beyond the narrowed hiatus.
8 Gastroesophageal Reflux and its Surgical Management � 65

Why do antireflux operationssometimes fail
� Inappropriate surgery. If a patient does nothave reflux, operation will cure whatever iscausing the patient’s symptoms. Perhaps thesingle most common non-reflux disorder,sometimes treated as reflux, is achalasia. In acollective review, the incidence of this occur-ring was 8% of cases presenting for re-opera-tion [57].The situation with adynamic (scleroderma)
esophagus is not quite so clear cut although inthe collective review was seen as the reason forreoperative surgery in 8% of cases also. Thereis little doubt that the potential for creating arelatively tight wrap in a patient with ady-namic esophagus is quite high. Nevertheless,authorities are divided as to whether the pre-operative demonstration of an adynamic eso-phagus should preclude the construction of atotal wrap. It seems not unreasonable to acceptthat a very floppy complete wrap as advocatedby Siewert [53] should not prove obstructive,although Skinner has stated that a partial fun-doplication is preferred in these circumstances[58]. Duranceau et al. have demonstrated thata loose, short fundoplication can be con-structed in patients with scleroderma esopha-gus, but significant acid exposure persisted in50% of 12 patients [60]. Our own preferencewhen an adynamic esophagus has been dem-onstrated on manometry is to carry out ananterior fundoplication.As a general rule, it can be stated that if
reflux cannot be demonstrated then antirefluxsurgery should not be undertaken.
� Obstructive problems. The usual problem isthe construction of wrap which is too tightand therefore produces obstruction even to anormally contracting esophagus. As mentionedabove, if the esophagus is adynamic, this prob-lem is potentially more likely to occur. Shiraziet al. compared 250 patients who had a shorttotal fundoplication carried out around a 60 Frbougie with 200 patients who had a long totalfundoplication carried out around a bougie of<40 Fr, and found the incidence of dysphagiain the latter group to be approximately doublethat in the former group [61].
In the collective review about 12% of pa-tients had this indication for their reoperation[57].Extrinsic obstruction can also occur by
three other means. First is when the esophagushiatus is narrowed too much in the placementof crural sutures, and sedond is when an An-gelchik prosthesis is inserted. Although thisdevice is effective in preventing reflux, it cancause severe dysphagia, leading to a need forearly removal of the device in up to 20% ofpatients [62]. The third mechanism has onlybeen described after laparoscopic fundoplica-tion and consists of an excessive fibrous tissuereaction in the hiatus leading to extrinsic ob-struction [40].
� Gastric pullthrough (slipped Nissen)
In the presence of a shortened esophagus andfixed sliding hiatus hernia, it is sometimes dif-ficult to be certain where the stomach finishesand the esophagus begins, when operatingfrom the abdomen, or vice versa, when operat-ing from the chest. Under these circumstances,it is possible that the inexperienced surgeonmay mobilize the herniated stomach, believingit to be esophagus and then wrap the moredistal stomach around this mobilized stomach– a so called gastric Nissen fundoplication. Itis impossible to glean from the literature howoften this occurs, as the end result is similar tothe gastric pullthrough problem. The gastricpullthrough (slipped Nissen) is a moderatelycommon form of failure reported. It is usuallyimpossible to know if a gastric Nissen wasfashioned in the first place, or if the fundopli-cation has slipped down from around the eso-phagus to lie around the stomach (which isprobably unlikely), or if the longitudinal mus-cle of the esophagus has pulled the distalstomach through the fundoplication, which, apriori, seems inherently the most likely cause.This problem accounted for 29% of cases un-dergoing re-operative surgery in the collectivereview [57].
� G.G. Jamieson, D. I. Watson66

� Breakdown of the repair
All patients who present with recurrent refluxprobably have breakdown of their repair tosome degree. Anatomical breakdown of the re-pair is the most common cause for re-opera-tion (46% in the collective review [57]). Thereasons why a repair should break down withtime are conjectural. It might be expected thata loose wrap would be less likely to breakdown than a wrap constructed under sometension. There is no doubt that a floppy Nissenis associated with almost no tension, and aNissen Rossetti repair (where only the anteriorwall of the stomach is used) is often underquite a degree of tension. However, there is noevidence from the literature that the one typeof repair is more likely to break down than theother. The fact that many of the repairs seemto break down early in the post-operativecourse suggests that precipitating factors suchas straining coming out of anaesthesia, post-operative vomiting, or just post-operative gas-tric distension, may play a role. In the longerterm it is not difficult to imagine gastric dis-tension with eating chipping away at the repair,a factor which may explain why delayed gastricemptying seems to have a strong associationwith recurrent reflux [63].
When do antireflux operations fail?
� Open operations. If an inappropriate opera-tion has been carried out, or if a total wraphas been constructed too tightly, either in rela-tive or absolute terms, or if the hiatus has beenmade too narrow, or if an Angelchik prosthesisis going to cause problems, then the failure ofthe surgery should be evident from the outset.The fact that, often, problems only become ap-parent some months after the surgery probablyrelates to the fact that many patients will takeliquid diets initially and only slowly progressto solid food. It may also relate to the strongplacebo effect of a major abdominal operation.However, it is surprising that many repairsbreak down early after surgery, as mentionedpreviously, with some even appearing to breakdown in the immediate post-operative period.
Leonardi et al. found that the mean time to re-flux recurrence was 19 months [64], and a sim-ilar finding was reported in 29 children [65].Furthermore, Varron et al. stated that 19 oftheir 37 patients who came to re-operation de-veloped recurrent reflux within 12 months oftheir surgery [66]. Collected data from someolder series similarly showed that the majorityof reflux recurrences occurred within the first2 years after surgery [67].
� Laparoscopic operations. Most large series oflaparoscopic antireflux surgery describe an in-cidence of adverse outcomes requiring subse-quent surgical revision [32, 65]. The incidencevaries with the length of post-operative follow-up and the criteria used for reporting. An inci-dence of 2 to 6% at short term follow-up isusual with many of the reoperations requiredto correct unique complications of the laparo-scopic approach. Early identification of theseproblems may facilitate early laparoscopic re-pair. However, later identification, beyond thefirst post-operative week, often necessitates amore difficult open surgical procedure due toadhesion formation and fibrosis rendering thelaparoscopic option in many instances moredifficult.Laparoscopic revision procedures performed
more than 3 months after the original fundo-plication have also been described [37, 68].However, these are often technically demand-ing operations. On the other hand, laparo-scopic revision within a few days of the origi-nal procedure for complications such as post-operative paraesophagus herniation or early se-vere dysphagia are technically less demanding,and may not add greatly to the overall morbid-ity of the laparoscopic approach [33, 37]. Tofacilitate this, we recommend routine earlypost-operative barium swallow x-rays to enableearly identification of problems and laparo-scopic correction.
Re-operative surgeryfor failed antireflux procedures
In general terms, the indications for secondtime around surgery are similar to indicationsfor primary surgery, i.e. intractability of symp-
8 Gastroesophageal Reflux and its Surgical Management � 67

toms in spite of the best that conservative mea-sures have to offer. However, it must be re-membered that operative mortality has to beconsidered here (unlike with primary surgery).For this reason it seems prudent to resort onlywhen symptoms are making a patient’s lifemiserable.It is extremely difficult to determine from
the literature what proportion of patients withrecurrent (or new) symptoms come to re-op-erative surgery. In O’Hanrahan et al.’s seriesthe number was 7 of 12 patients, with demon-strated recurrent reflux [69]. However, what-ever the proportion has been in the past, it isreasonable to expect that, for recurrent refluxat least, the figure will be somewhat less in thefuture, since the introduction of proton pumpinhibitors.The incidence of patients overall who come
to re-operation is also not known for certain,as no series has achieved 100% follow-up oftheir patients. Nevertheless, the figure is prob-ably of the order of 4–6%.As the esophagus hiatus can be approached
either from the thorax or from the abdomen,theoretically it seems attractive to advocate anapproach for reoperative surgery via the pre-viously unoperated route. In practice, however,it seems that surgeons operate through theroute with which they are most familiar. Someform of total fundoplication remains the mostpopular re-operation, but equally a fundoplica-tion constructed around an esophagus exten-sion procedure may need to be performed.Perhaps somewhat surprisingly, the results
of re-do antireflux surgery are not that muchdifferent from the primary surgery [57], withthe one important exception being operativemortality. Most series of patients having pri-mary antireflux surgery show no or very lowmortality rates. Thus, Siewert et al. report acollected series of 1240 patients with a 0.34%mortality rate [70]. However, series of re-docases show operative mortality rates whichvary from 0 to 18%, underlining the fact thatthis surgery can be technically extremely chal-lenging [57].The results of surgery worsen with the num-
ber of previous operations a patient has under-gone for the problem. For example, Little et al.found that 85% of 34 patients who had under-gone one previous operation had a good result,
66% of 19 who had undergone two previousoperations obtained a good result, and only42% of 8 patients who had undergone three ormore operations had a good result [71].
References
1. Nebel OT, Fornes MF, Castell DO (1976) Symptom-atic gastro esophageal reflux: incidence and preci-pitating factors. Am J Dig Dis 21:953–956
2. Condon RE (1988) Intraoperative dilatation andfundoplication for benign peptic oesophageal stric-ture. In: Jamieson GG (ed) Surgery of the Oeso-phagus. Churchill Livingstone, London
3. Smith PM, Kerr CD, Cockel R et al (1994) A com-parison of omeprazole and ranitidine in the pre-vention of recurrence of benign oesophageal stric-ture. Gastroenterology 107:1312–1318
4. Allen CJ, Newhouse MT (1984) Gastroesophagealreflux and chronic respiratory disease. Am Rev Re-spir Dis 129:646–647
5. Attwood SE, Smyrk TC, DeMeester TR et al (1992)Duodenoesophageal reflux and the development ofadenocarcinoma in rats. Surgery 111:503–510
6. Ortiz A, Martinex LF, Parrilla P et al (1996) Con-servative treatment vs antireflux surgery in Bar-rett’s oesophagus: long term results of a prospec-tive study. Br J Surg 83:274–278
7. Hardhan KD (1995) The role of the proton pumpinhibitors in the treatment of gastroesophagealreflux disease. Aliment Pharmacol Ther 9 (suppl):15–25
8. Druman D, Wright C, Tougas C et al (1995) Ome-prazole produces parietal cell hypertrophy and hy-perplasia in humans. Gastroenterology 108 (suppl):A85
9. Pera AM, Cameron AJ, Trastec VF (1993) Increas-ing incidence in adenocarcinoma of the oesopha-gus and esophagastric junction. Gastroenterology104:510–513
10. Peters JH, Clarke GWV, DeMeester TR (1994) Doall adenocarcinomas of the esophagus arise in Bar-rett’s mucosa. In: Giuli RR, Tytgat GNJ, DeMeesterTR, Calmiech E (eds) The esophageal mucosa.Elsevier, Amsterdam, pp 1009–1115
11. Dallemagne B, Weerts JN, Jehaes C et al (1992)Laparoscopic Nissen fundoplication: preliminaryreport. Surg Laparosc Endosc 1:138–143
12. Jamieson GG, Watson DJ, Britten-Jones R et al(1994) Laparoscopic Nissen fundoplication. AnnSurg 220:137–145
13. Watson DI, Chan ASL, Myers JC et al (1997) Illnessbehaviour influences the outcome of laparoscopicantireflux surgery. J Am Coll Surg 184:44–48
14. Maher JW, Hocking MP, Woodward ER (1981)Long term follow-up of the combined fundoplica-tion for treatment of longitudinal peptic stricturesof the oesophagus. Ann Surg 194:64–69
� G.G. Jamieson, D. I. Watson68

15. Watson DI, Mathew G, Pike GK et al (1997) Com-parison of anterior, posterior and total fundoplica-tion using a viscera model. Dis Esophagus 10:110–114
16. Nissen R (1956) Eine einfache Operation zur Beein-flussung der Refluxoesophagitis. Schweiz Med Wo-chenschr 86:590–592
17. Rossetti M, Hell K (1997) Fundoplication for thetreatment of gastroesophageal reflux in hiatal her-nia. World J Surg 1:439–444
18. DeMeester TR, Bonavina L, Albertucci M (1986)Nissen fundoplication for gastroesophageal refluxdisease. Evaluation of primary repair in 100 con-secutive patients. Ann Surg 204:9–20
19. Luostarinen M, Isolauri J, Laitinen J, Koskinen M,Keyrilainen O, Markkula H, Lehtinen E, Uusitalo A(1993) Fate of Nissen fundoplication after 20 years.A clinical endoscopical and functional analysis.Gut 34:1015–1020
20. Pope CE (1992) The quality of life following anti-reflux surgery. World J Surg 16:355–358
21. Lundell L, Abrahamsson H, Ruth M, Rydberg L,Lonroth H, Olbe L (1991) Long-term results of aprospective randomized comparison of total fundicwrap (Nissen-Rossetti) or semifundoplication(Toupet) for gastro-oesophageal reflux. Br J Surg78:1088–1094
22. Watson A, Jenkinson LR, Ball CS, Norris TL(1991) A more physiological alternative to totalfundoplication for the surgical correction of resis-tant gastro-oesophageal reflux. Br J Surg 78:1088–1094
23. Thor KBA, Silander T (1989) A long-term random-ized prospective trial of the Nissen procedure ver-sus a modified Toupet technique. Ann Surg 210:719–724
24. Walker SJ, Holt S, Sanderson CJ, Stoddard CJ (1992)Comparison of Nissen total and Lind partial trans-abdominal fundoplication in the treatment of gas-trooesophageal reflux. Br J Surg 79: 410–414
25. DeMeester TR, Johnson LF, Kent AH (1974) Evalu-ation of current operations for the prevention ofgastroesophageal reflux. Ann Surg 180:511–525
26. Hill ADK, Walsh TN, Bolger CM, Byrne PJ, Hen-nessy TPJ (1994) Randomized controlled trialcomparing Nissen fundoplication and the Angel-chik prosthesis. Br J Surg 81:72–74
27. Janssen IM, Gouma DJ, Klementschitsch P, van derHeyde MN, Obertop H (1993) Prospective random-ised comparison of teres cardiopexy and Nissenfundoplication in the surgical therapy of gastro-oesophageal reflux disease. Br J Surg 80:875–878
28. Luostarinen MES, Koskinen MO, Isolauri JO(1996) Effect of fundal mobilisation in Nissen-Ros-setti fundoplication on oesophageal transit anddysphagia. Eur J Surg 162:37–42
29. Spechler SJ (1992) Comparison of medical andsurgical therapy for complicated gastroesophagealreflux disease in veterans. NEJM 326:786–792
30. Geagea T (1991) Laparoscopic Nissen’s fundoplica-tion: preliminary report on ten cases. Surg Endosc5:170–173
31. Cuschieri A, Hunter J, Wolfe B, Swanström LL,Hutson W (1993) Multicentre evaluation of laparo-scopic antireflux surgery. Preliminary report. SurgEndosc 7:505–510
32. Watson DI, Jamieson GG (2008) Antireflux surgeryin the laparoscopic era. Br J Surg (in press)
33. Hinder RA, Filipi CJ, Wetscher G, Neary P,DeMeester TR, Perdikis G (1994) LaparoscopicNissen fundoplication is an effective treatment forgastroesophageal reflux disease. Ann Surg 220:472–483
34. Watson DI, Baigrie RJ, Jamieson GG (1996) Alearning curve for laparoscopic fundoplication. De-finable, avoidable, or a waste of time? Ann Surg224:198–203
35. Baigrie RJ, Watson DI, Game PA, Jamieson GG(1997) Vascular perils during laparoscopic dissec-tion of the oesophageal hiatus. Br J Surg 84:556–557
36. Firoozmand E, Ritter M, Cohen R, Peters J (1996)Ventricular laceration and cardiac tamponade dur-ing laparoscopic Nissen fundoplication. Surg LaparEndosc 6:394–397
37. Watson DI, Jamieson GG, Devitt PG, Mathew G,Britten-Jones RE, Game PA, Williams RS (1995)Changing strategies in the performance of laparo-scopic Nissen fundoplication as a result of experi-ence with 230 operations. Surg Endosc 9:962–966
38. Watson DI, Jamieson GG, Devitt PG, Mitchell PC,Game PA (1995) Paraoesophageal hiatus hernia; animportant complication of laparoscopic Nissenfundoplication. Br J Surg 82:521–523
39. Gotley DC, Smithers BM, Rhodes M, Menzies B,Branicki FJ, Nathanson L (1996) Laparoscopic Nis-sen fundoplication 200 consecutive cases. Gut 38:487–491
40. Watson DI, Jamieson GG, Mitchell PC, Devitt PG,Britten-Jones R (1995) Stenosis of the oesophagealhiatus following laparoscopic fundoplication. ArchSurg 130:1014–1016
41. Jorgensen JO, Gilles RB, Lalak NJ, Hunt DR (1994)Lower limb venous hemodynamics during laparo-scopy: An animal study. Surg Lapar Endosc 4:32–35
42. Pike GK, Bessell JR, Mathew G, Watson DI, MitchellPC, Jamieson GG (1996) Changes in fibrinogenlevels in patients undergoing open and laparoscopicNissen fundoplication. Aust NZ J Surg 66:94–96
43. Cadiere GB, Himpens J, Bruyns J (1995) How toavoid esophageal performation while performinglaparoscopic dissection of the hiatus. Surg Endosc9:450–452
44. Mitchell PC, Jamieson GG (1994) Coeliac axis andmesenteric arterial thrombosis following laparo-scopic Nissen fundoplication. Aust NZ J Surg 64:728–730
45. Medina LT, Vientimilla R, Williams MD, FenoglioE (1996) Laparoscopic fundoplication. J Laparoen-dosc Surg 6:219–226
46. Franzen T, Anderberg B, Tibbling L, Johansson KE(1996) A report from a randomized study of openand laparoscopic 360 fundoplication. Surg Endosc10:582 (Abstract)
8 Gastroesophageal Reflux and its Surgical Management � 69

47. Laine S, Rantala A, Gullichsen R, Ovaska J (1997)Laparoscopic vs conventional Nissen fundoplica-tion. A prospective randomized study. Surg Endosc11:441–444
48. Watson DI, Gourlay R, Globe J, Reed MWR, John-son AG, Stoddard CJ (1994) Prospective random-ised trial of laparoscopic versus open Nissen fun-doplication. Gut 35 (suppl 2):15 (Abstract)
49. Laycock WS, Trus TL, Hunter JG (1996) New tech-nology for the division of short gastric vesselsduring laparoscopic Nissen fundoplication. SurgEndosc 10:71–73
50. Swanström LL, Pennings JL (1995) Laparoscopiccontrol of short gastric vessels. J Am Coll Surg181:347–351
51. Laws HL, Clements RH, Swillies CM (1997) A ran-domized, prospective comparison of the Nissenversus the Toupet fundoplication for gastroesopha-geal reflux disease. Ann Surg 225:647–654
52. Watson DI, Pike GK, Baigrie RJ, Mathew G, DevittPG, Britten-Jones R, Jamieson GG (1997) Prospec-tive double blind randomized trial of laparoscopicNissen fundoplication with division and withoutdivision of short gastric vessels. Ann Surg 226:642–652
53. Watson DI, Pike GK, Davies N, Mathew G, DevittPG, Britten-Jones R, Jamieson GG (2008) Prospec-tive double blind randomized trial of laparoscopicNissen fundoplication versus an anterior partialfundoplication. Br J Surg (in press)
54. Jamieson GG, Watson DI, Britten-Jones R, MitchellPC, Anvari M (1994) Laparoscopic Nissen fundo-plication. Ann Surg 220:137–145
55. Kauer WKH, Peters JH, DeMeester TR, Heim-bucher J, Ireland AP, Brenner CG (1995) A tailoredapproach to antireflux surgery. J Thorac Cardio-vasc Surg 110:141–147
56. Swanstrom LL, Marcus DR, Galloway GQ (1996)Laparoscopic Collis gastroplasty is the treatmentof choice for the shortened esophagus. Am J Surg171:477–481
57. Jamieson GG (1993) The results of antireflux sur-gery and reoperative antireflux surgery. Gullett 3:41–45
58. Siewert JR, Feussner J (1988) Collagen diseases,Chapter 54. In: Jamieson GG (ed) Surgery of theoesophagus. Churchill Livingston, Edinburgh
59. Skinner DB (1992) Surgical management after failedantireflux operations. World J Surg 16:359–363
60. Durancequ A, Topart P, Deschamps C (1992) Tail-lerfer reflux control in operated scleroderma pa-tients. Abstract SP-080, 5th World Congress of In-ternational Society of Diseases of the Esophagus
61. Stirling MC, Orringer MB (1989) Continued assess-ment of the Collis-Nissen operation. Ann ThoracSurg 47:224–230
62. Maddern GJ, Myers J, McIntosh N, Bridgewater F,Jamieson GG (1992) The effect of the Angelchickprosthesis on oesophageal and gastric function.Arch Surg 126:14–17
63. Maddern GJ, Jamieson GG, Chatterton BE, CollinsPJ (1985) Is there an association between failedantireflux procedures and delayed gastric empty-ing? Ann Surg 202:162–165
64. Leonard HK, Crozier RE, Ellis FH (1989) Reopera-tion for complications of the Nissen fundoplica-tion. J Thorac Cardiovasc Surg 81:50–56
65. Dedinsky GK, Vane DE, Black CT, Turner MK,West KW, Grosfeld JL (1987) Complications andreoperation after Nissen fundoplication in child-hood. Am J Surg 153:177–183
66. Varron F, Siksik JM, Tiret E, Parc R (1989) Re-operation for oesophagitis following failed anti-reflux procedure. Abstract 156, European DigestiveDiseases Week, Amsterdam
67. Jamieson GG, Durandequ A, Deschamps C (1988)Surgical treatment of gastroesophageal reflux dis-ease. In: Jamieson GG, Durandequ A (eds) Gastro-esophageal reflux, chap 10. WB Saunders, Philadel-phia
68. Depaula AL, Hashiba K, Bafutto M, Machado CA(1995) Laparoscopic reoperations after failed andcomplicated antireflux operations. Surg Endosc 9:681–686
69. O’Hanrahan T, Marples M, Bancewicz J (1990) Re-current reflux and wrap disruption after Nissenfundoplication: detection incidence and timing. BrJ Surg 77:545–547
70. Siewert JR, Feussner H, Walker SJ (1992) Fundo-plication: how to do it? Periesophageal wrappingas a therapeutic principle in gastro esophageal re-flux prevention. World J Surg 16:326–334
71. Little AG, Ferguson MK, Skinner DB (1986) Re-operation for failed antireflux operations. J ThoracCardiovasc Surg 91:511–517
70 � G.G. Jamieson, D. I. Watson: 8 Gastroesophageal Reflux and its Surgical Management

In esophageal carcinoma as well as in othermalignant tumors, present-day oncology re-quires a standardized classification for� planning treatment procedures,� estimation of prognosis and� evaluation of treatment results and, thus,quality assurance.
As in other malignant tumors the tumor classi-fication of esophageal carcinoma is based onfour pillars and follows uniform internationalrecommendations by the World Health Organi-zation (WHO) [4] and the International UnionAgainst Cancer (UICC) (2002, 2005) [16, 18].
Tumor classification
1. Tumor site UICC2. Histomorphology– Typing WHO– Grading
3. Anatomical extent UICCbefore treatment=TNM/pTNM
4. Anatomical extent after treatment UICC=Residual tumor (R) classification
Tumor site
The esophagus commences at the lower borderof the cricoid cartilage. The UICC (2002, 2005)distinguishes between the cervical and the in-trathoracic esophagus. The latter is subdividedinto the upper thoracic, mid-thoracic, and low-er thoracic portion (including the abdominalesophagus) (Fig. 9.1). The upper thoracic por-tion extends from the thoracic inlet to the level
of the tracheal bifurcation. The mid-thoracicportion is the proximal half, the lower thoracicportion the distal half of the esophagus be-tween the tracheal bifurcation and the esopha-gogastric junction.From a clinical point of view subdivision
into an infrabifurcational portion (=mid-tho-racic and lower thoracic), a suprabifurcationalportion (including the region at the trachealbifurcation) (=upper thoracic portion) and acervical portion is important.For the classification of tumors involving
the distal esophagus as well as the cardiac areaof the stomach the following rules of the UICC(2003) [17] should be applied (Fig 9.2):� If more than 50% of the tumor involves theesophagus, the tumor is classified as eso-phageal, if less than 50%, as gastric;
Pathologic Classificationof the Esophageal CarcinomaP. Hermanek
9
Fig. 9.1. Anatomic subdivision of the esophagus. Modifiedfrom UICC 2005.
18 cm
24 cm
32 cm
40 cm
Cervical esophagusC15.0
Thoracic inletUpper thoracic esophagus
C15.3
Tracheal bifurcationMid-thoracic esophagus
C15.4
Lower thoracic esophagusC15.5
esophagogastricjunction

� if the tumor is equally located above and be-low the esophagogastric junction or is desig-nated as being at the junction, squamous cell,small cell and undifferentiated carcinomasare classified as esophageal, adenocarcinomaand signet ring cell carcinoma as gastric.
Typing
The main histological types are the squamouscell carcinoma and the adenocarcinoma. In sta-tistics from the 1980s from Western countriesabout 85–90% squamous cell carcinomas and5–19% adenocarcinomas are reported. In the Er-langen Cancer Registry 1978–1991 (n=581)83.3% squamous cell carcinomas, 10.2% adeno-carcinomas and 6.5% other or unclassified car-cinomas were observed. While adenocarcino-mas in Japan are very uncommon, in the Wes-tern countries a considerable increase of adeno-carcinomas during the last 10–20 years was reg-istered: National Cancer Data base of USA: 1988:33.2%, 1993: 43.1% adenocarcinomas [21]. How-ever sometimes in such statistics carcinomas ofthe cardia are included, and in these cases theproportion of adenocarcinomas is considerablyhigher than in statistics of carcinomas of theesophagus only.
� Squamous cell carcinomas show intercellularbridges and variable amounts of keratin.Variants are:
� the verrucous carcinoma with papillary pat-tern and well differentiated,
� the spindle cell (pseudosarcomatous) carci-noma, a poorly differentiated carcinoma thatmay be misinterpreted as sarcoma or carci-nosarcoma,
� the basaloid squamous cell carcinoma, inprognosis similar to the common squamouscell carcinoma, with difficulties in differen-tial diagnosis to small cell and adenoid cys-tic carcinoma.
� The adenocarcinoma of the esophagus arisesas a rule from a Barrett syndrome (endobra-chyesophagus, columnar epithelial-lined loweresophagus, CELLO). Very uncommon are ade-nocarcinomas arising from congenital foci ofheterotopic gastric mucosa, mostly in the upperthoracic portion, or from esophageal glands.Adenocarcinoma show papillary, tubular, ortubulo-papillary pattern and may includecircumscribed areas with squamous meta-plasia.
� Uncommon carcinomas (less than 5%) include
– mucinous adenocarcinoma– adenosquamous carcinoma– mucoepidermoid carcinoma– adenoid cystic carcinoma– lymphoepithelioma-like carcinoma– small cell carcinoma (to be distinguishedfrom extension of a primary small cellcarcinoma of the lung)
– undifferentiated carcinoma– choriocarcinoma.
Grading
Squamous cell carcinomas and adenocarcino-mas are graded by considering the degree ofcytological and architectural similarity to thetissue of origin as well as nuclear abnormali-ties and mitotic activity:� G1 Well Low gradedifferentiated of malignancy
� G2 Moderately Low gradedifferentiated of malignancy
� G3 Poorly High gradedifferentiated of malignancy
� P. Hermanek72
Fig. 9.2. Distal esophageal carcinoma versus proximal gastriccarcinoma/adenocarcinoma of the gastroesophageal junction.
Esophageal carcinoma Gastric carcinoma

The small cell and the undifferentiated carci-nomas are always G4 (Undifferentiated) andhigh grade.An independent prognostic influence of the
grade of differentiation could not be shown inmost multivariate analyses. Recently, for squa-mous cell carcinoma a grading system (prog-nostic score) considering only the pattern ofinvasion and the inflammatory response wasproposed by [14]:
� Pattern of invasion
– Pushing well-delineated 1 pointstumor margins
– Infiltrating, solid cords 2 pointsand bands
– Small groups of dissociated 3 pointscells (n>15)
– Marked cellular dissociation 4 points
� Inflammatory response
– Marked 1 point– Moderate 2 points– Slight 3 points– None 4 points
– Sum of Prognosticpoints group2.3 1 Favorable prognosis4 2 Favorable prognosis5.6 3 Favorable prognosis7.8 4 Poor prognosis
TNM/pTNM classification
The anatomic extent of esophageal carcinomais classified according to the TNM/pTNM clas-sification of UICC (2002, 2005). It is applied tothe squamous cell carcinoma as well as to ade-nocarcinoma and other uncommon carcino-mas.The clinical TNM Classification is based on
evidence from pre-therapeutic clinical exami-nation, endoscopy, imaging, and from surgicalexploration. The pathological pTNM classifica-tion entails relevant histopathological examina-tion.
Requirement for pTNM classificationof esophageal carcinoma (UICC 2002, 2003)
pT1–3 Pathological examination of the pri-mary carcinoma with no gross tumor atthe deep (radial, lateral), proximal anddistal margins of the resection (with orwithout microscopic involvement)
pT4 Microscopic confirmation of invasionof adjacent structures
pN0 Histological examination of a mediasti-nal lymphadenectomy specimen whichwill ordinarily include 6 or more lymphnodes
pN1 Microscopic confirmation of at leastone regional lymph node metastasis
pM1 Microscopic (histologic or cytologic)confirmation of distant metastasis
� Primary tumor: T/pT classification. The deci-sive parameter for the classification of the pri-mary tumor is the depth of invasion (Fig. 9.3).In addition to the categories presented in Fig.9.3 the categories T/pTX: Primary tumor can-not be assessed and T/pT0: No evidence of pri-mary tumor is available.In Japan, frequently the term “superficial
esophageal carcinoma” is used to summarizeTis and T1 tumors [11]. In contrast, in Japanthe term “early carcinoma of the esophagus”characterizes a pT1 carcinoma without meta-stasis in most publications.
� Regional lymph nodes. According to the UICCrules the regional lymph nodes for the cervicaland the intrathoracic esophagus are different:
� Cervical esophagus. Cervical lymph nodes in-cluding supraclavicular lymph nodes
� Intrathoracic esophagus
– Mediastinal lymph nodes– Perigastric lymph nodes along the lesserand greater curvatures (including rightand left cardial, supra- and infrapyloricalnodes) and along the left gastric artery
(Attention: The celiac lymph nodes are non-re-gional, involvement is classified as distant me-tastasis!)
9 Pathologic Classification of the Esophageal Carcinoma � 73

From surgical point of view and for describingthe extent of lymphadenectomy, the regionallymph nodes are subdivided into compart-ments or fields (cervical, mediastinal, and peri-gastric).Thus, a two field and three field lymphade-
nectomy can be distinguished:� Cervicalcompartment
� Mediastinalcompartment Two field
� Perigastriccompartment Two field
��������
�������
Three field (allcompartments)
Within the 3 compartments various lymphnodes stations are included and numbered bythe Japanese Society for Esophageal Diseases[8] (Fig. 9.4).
� Regional lymph nodes for the cervical
esophagus (cervical compartment)
(100) Lateral cervical nodes bilateral(101) Cervical paraesophageal nodes(102) Deep cervical nodes (bilateral)(103) Retropharyngeal nodes(104) Supraclavicular nodes (bilateral), includ-
ing the so-called scalenus nodes
� P. Hermanek74
Fig. 9.3. T/pT classification (UICC 2002). Modified from UICC 2005.
112
112
104
102100
103
102100
104
109
108
110
111
2
1
7
5
3
4
4
6
107
106
105
101
Fig. 9.4. Regional lymph nodes of the esophagus. Subdivi-sion into lymph node compartments and stations accordingto the Japanese Society for Esophageal Diseases (1992).
T/pTisCarcinoma in situ
T/pT1a *)Mucosa (Lamina propria,
Muscularis mucosae)
T/pT1b *)Submucosa
Epthelium
Lamina propriaMuscularis mucosaeSubmucosa
MucosaSubmucosa
Muscularispropria
Adventitia
T/pT2Muscularis propria
T/pT3Adventitia
T/pT4Neighbored structures
*) Facultative classification: TNM Supplement (UICC 2001)
Cervicalcompartment
Mediastinalcompartment
Perigastriccompartment

� Regional lymph nodes for the intrathoracic
esophagus
Mediastinal compartment
(105) Upper thoracic para-esophageal nodes Upper region
(106) Thoracic paratrachealnodes (bilateral)
(107) Nodes at the trachealbifurcation
(108) Middle thoracic Middle regionparaesophageal nodes
(109) Pulmonal hilar nodes (bilateral)
(110) Lower thoracicparaesophageal nodes Lower region
(111) Diaphragmatic nodes
(112) Posterior mediastinal Middle andnodes lower region
Perigastric compartment
(1) Right cardiac nodes(2) Left cardiac nodes(3) Nodes along the lesser curvature(4) Nodes along the greater curvature(5) Suprapyloric nodes(6) Infrapyloric nodes(7) Nodes along the left gastric artery
The number of regional lymph nodes removedby a systemic two-field lymphadenectomy is 25to 40 nodes in the Western countries [3, 7].With increasing number of nodes histologicallyexamined the number of node-positive cases isincreasing [3].
Number of nodesexamined per tumorsresection specimen
Frequency of nodepositive resectionspecimen
1–5 1/10=10%
6–20 15/53=28%
>20 55/93=59%
� N/pN classification. The obligatory categoriesof the UICC classification are:N/pNX Regional lymph nodes cannot be as-
sessedN/pN0 No regional lymph node metastasisN/pN1 Regional lymph node metastasis
Cases with micrometastasis only, i.e., no me-tastasis larger than 2 mm, can be identified bythe addition of “(mi)”, e.g., pN1(mi) (UICC2002).In the TNM Supplement (UICC 2003) an op-tional ramification of N/pN1 is proposed:N/pN1a 1 to 3 regional lymph nodes
involvedN/pN1b 4 to 7 regional lymph nodes
involvedN/pN1c More than 7 lymph nodes involved
Because the tumor length appears to be an in-dependent indicator of mortality [2], in the lastedition of the TMN Supplement (UICC 2003)an additional optional ramification of the T cat-egories according to the tumor length is pro-posed:T1a-T1b Tumor length <3 cmT1b-T4b Tumor length >3 cm
� Classification of isolated tumor cells in the
regional lymph nodes [6] (UICC 2002, 2003)Isolated tumor cells (ITC) are single tumorcells or small clusters of cell not more than 0.2mm in greatest dimension that are usually de-tected by immunocytochemistry or molecularmethods (flow cytometry, DNA analysis), butwhich may be verified H and E stains. Theirclassification is as follows:pN0 (i–) No regional lymph node metasta-
sis histologically, negative mor-phological findings for ITC
pN0 (i+) No regional lymph node metasta-sis histologically, positive morpho-logical findings for ITC
pN0 (mol–) No regional lymph node metasta-sis histologically, negative non-morphological findings for ITC
pN0 (mol+) No regional lymph node metasta-sis histologically, positive non-morphological findings for ITC
9 Pathologic Classification of the Esophageal Carcinoma � 75

� Distant metastasis: M/pM. The categories are:M/pMX Distant metastasis cannot be as-
sessedM/pM0 No distant metastasisM/pM1 Distant metastasis
For carcinomas of the intrathoracic esophagusthe category M/pM1 is subdivided intoM/pM1a and M/pM1b:
Tumors of the upper intrathoracic esophagusM/pM1a Metastasis in cervical lymph nodesM/pM1b Other distant metastasis
Tumors of the mid-thoracic esophagusAll distant metastasis (including those in non-regional lymph nodes) are classified asM/pM1b
Tumors of the lower intrathoracic esophagusM/pM1a Metastasis in celiac lymph nodesM/pM1b Other distant metastasis
The not uncommon so-called skip metastasis(intramural metastasis, predominant in themucosa and submucosa) should not be classi-fied as distant metastasis, their occurrence isnot considered in the present TNM system.If all distant metastases are not larger than
2 mm in dimension, i.e. micrometastasis, thismay be indicated by the suffix “(mi)”, e.g.pM1b(mi).
� Classification of isolated tumor cells in non-re-
gional lymph nodes or bone marrow. Such find-ings are classified according to the same sche-ma as for regional lymph nodes (see above),e.g., isolated tumor cells identified by morpho-logic techniques M0(i+) and non-morphologicfindings as M0(mol+).
For specification of the site of distant metasta-sis the following notations may be used:PUL Lung(s)OSS Bone(s)HEP LiverBRA BrainLYM Lymph node(s) (non-regional)MAR Bone marrowPLE Pleura
PER PeritoneumADR AdrenalsSKI SkinOTH OthersGEN Generalized metastasis
� Stage grouping
By considering of T, N and M and pT, pN andpM categories respectively so-calledstages may be defined:Stage 0 Tis N0 M0Stage I T1 N0 M0Stage IIA T2,3 N0 M0Stage IIB T1,2 N1 M0Stage III T3 N1 M0Stage IV Any T Any N Any M
Additional descriptors andoptional categories of the TNM system
For identification of special cases in the TNMor pTNM classification, the following symbolsare used:
� m symbol. Addition to T and pT to indicatethe presence of multiple synchronous primarytumors in the esophagus. In this case, the tu-mor with the highest T category should beclassified and the multiplicity or the numberof tumors should be indicated in parentheses.Example: The pathological examination
shows a pT2 tumor and an additional primarypT1 carcinoma. The classification is pT2(m) orpT2 [2].
� y symbol. In those cases in which classifica-tion is performed following preoperative che-mo- and/or radiotherapy, the TNM or pTNMcategories are identified by the y prefix, e. g.yT2N0M0 or ypT2pN1M0.
� r symbol. Recurrent tumors, when stagedafter a disease-free interval, are identified bythe prefix r, e. g. rT2N0M0.
� a symbol. The prefix “a” indicates that classi-fication is first determined at autopsy.
� P. Hermanek76

� Lymphatic invasion. For description of lym-phatic invasion the following categories areused:LX Lymphatic invasion cannot be assessedL0 No lymphatic invasionL1 Lymphatic invasion
� The C-factor (certainly factor) reflects the va-lidity of clinical classification according to thediagnostic methods employed. The C-factor isadded to the T, N, and M categories, e.g. T2C2N1C3 M0C1. The definitions for the esophagus[19] are:
� Primary tumorC1 Physical examination, esophagogastroduo-
denoscopy, esophagography, bronchoscopyC2 Chromoendoscopy, radiographs with spe-
cial projections, endoluminal ultrasonog-raphy, CT, MRI, laparoscopy, biopsy, cy-tology
C3 Surgical exploration including biopsy andcytology
� Regional lymph nodesC1 Physical examination (cervical lymph
nodes)C2 Endoluminal ultrasonography, CT, MRI,
PET, laparoscopyC3 Surgical exploration including biopsy and
cytology
� Distant metastasisC1 Physical examination, standard radiogra-
phyC2 Tomography, CT, external ultrasonography,
MRI, scintigraphy, laparoscopy, biopsy,cytology
C3 Surgical exploration including biopsy andcytology
For pTNM the C-factor is not important andmay be omitted because the requirements forpT, pN, and pM are defined in the generalrules of the TNM system and in the TNM Sup-plement (UICC 2003).
Residual tumor (R) classification
While TNM and pTNM describe the anatomicextent of tumor before treatment, the R classi-fication deals with tumor status after treat-ment. It reflects the effects of therapy, influ-ences further therapeutic procedures, and isthe strongest predictor of prognosis.
The categories of the R classification are:RX Presence of residual tumor cannot be as-
sessedR0 No residual tumorR1 Microscopic residual tumorR2 Macroscopic residual tumor
The Working Group of German Cancer Centers[1] proposed a subdivision of the R2 category:R2a Macroscopic residual tumor without mi-
croscopic confirmationR2b Macroscopic residual tumor with micro-
scopic confirmation
In the R classification the loco-regional tumorstatus (primary tumor and regional lymphdrainage area) as well as distant residual tu-mor in the form of remaining distant metasta-sis are taken into consideration. Thus the Rclassification following surgical treatment re-quires the co-operation of the surgeon and thepathologist (Fig. 9.5).In esophageal carcinoma loco-regional resid-
ual tumor is found most frequently in the medi-astinal (circumferential, lateral, radial) resectionmargins, more rarely on the oral, and very sel-dom on the aboral margin: In 107 locally-re-gionally incomplete esophageal resections themediastinal margin was tumor positive in82%, the oral margin in 15%, and the aboralmargin in 3% [20]. Thus, the histological exam-ination has to focus on the mediastinal resectionmargins in the region of the deepest invasion ofthe primary carcinoma. Transverse sections aretaken for histology after marking the marginwith India ink or white latex-emulsion (Tipp-Ex). Because of the relatively frequent histologictumor extension beyond the gross tumor mar-gins and microscopic skip metastasis, the addi-tional histologic examination of the oral andaboral resection margin is obligatory [5].
9 Pathologic Classification of the Esophageal Carcinoma � 77

Grading of histological regressionafter neoadjuvant treatment
Following preoperative radio- and/or chemo-therapy, a variable histologic regression of tu-mor tissue is seen. For grading these changes,two methods may be used [9].
� Assessment of “effectivity” (Ef) according tothe proposals of the Japanese Society for Eso-phageal Diseases [8]:Ef1 (no slight regression)
vital tumor cells with absent or slight de-generative changes in more than 1/3 ofthe tumor
Ef2 (moderate regression)neither Ef1 nor Ef3
Ef3 (severe regression)no vital tumor cells
� Assessment of tumor regression grade(TRG) according to Mandard et al. [10];TRG1 No identifiable residual cancer, only fi-
brosis with or without granulomas(complete regression)
TRG2 Rare residual cancer cells scatteredthrough fibrosis
TRG3 Increased number of residual cancercells, fibrosis still predominant
TRG4 Residual cancer outgrowing fibrosisTRG5 No regressive changes
� Further prognostic factors (for more informa-tion and references see Roder et al. [12] andStein et al. [5]).
The anatomic extent of tumor, assessed by theTNM defined stage and after treatment, by theR classification are the most important indica-tors of outcome. For all other possible tumor-,patient- and treatment-related prognostic fac-tors is the independent significance by multi-variate analysis not yet proven and only forsome patient subgroups probable [13]. This ap-plies to the histologic type which influencesprognosis probably only in pT1 tumors. An in-dependent prognostic influence has beenshown for the so-called lymph node ratio, i.e.the ratio of involved and removed nodes, by asingle study from Munich [12]. This ratio re-flects the extent of lymphatic metastasis as wellas the extent of lymphadenectomy. Followingneoadjuvant therapy the grade of histologicaltumor regression is of prognostic importance[10]. For all biological and molecular markers,it has to be stated that their significance fortreatment decisions as well as for prognosis re-mains to be proven.
� P. Hermanek78
Fig. 9.5 Assessment of the residualtumor (R) classification. From Wagnerand Hermanek 1995 [19].
Preoperatively/intraoperatively:residual tumor/distant metastasis?
No
Resection marginstumor free?
Yes No
R0 R1
No
No residual tumormicroscopically?
No Yes
R2a R2b

Preconditions for adequatehistopathological tumor classification
An optimal histopathological tumor classifica-tion requires the close co-operation betweenclinicians and pathologists. Optimal methodsin the histopathological laboratories must besupplemented by three preconditions to be metby clinicians:� Adequate sampling for pretherapeutic diag-nostics,
� careful handling of specimen during thetransport into the histopathological labora-tories,
� sufficient information on the clinical situa-tion for the pathologist.
� Sampling for pre-therapeutic diagnostics. Fromany grossly recognizable lesion multiple biop-sies (at least 5 particles) have to be taken. Inulcerous lesions, not only the ulceration itselfbut also the margins should be biopsied. Poly-poid lesions up to 1 cm in dimension shouldbe completely removed by diathermy snare asprimary diagnostic step (total biopsy). Diag-nostic difficulties arise in case of tumor steno-sis and oral submucous extension. If stenosiscannot be passed by a baby endoscope, biop-sies may be possible after dilatation. In suchcases, material for cytological examinationmay be obtained by washing, brushing or bal-loon sampling. The assessment requires specialexperiences with esophageal cytology. Duringesophagoscopy, biopsies should be taken notonly from the visible tumor, but also from theadjacent grossly normal mucosa to detect anassociated in situ component. Synchronousmultiple primary tumors of the category Tisand T1 sometimes can be detected only bychromoendoscopy (with lugol solution).
� Handling of specimens during the transport to
the histological laboratories. Biopsies and ecto-mized polyps should be immersed in fixative assoon as possible. The type of fixative shouldbe chosen in agreement with the pathologist.Mucosal resection specimens should bemounted on cardboard or corkboard, mucosalside up, and attached to it with pins (avoidstretching!). If possible, esophagectomy speci-mens should be transported to the pathologist
immediately after resection. Areas suspiciousof locally incomplete resection should bemarked by the surgeon. In addition the level oftracheal bifurcation should be marked to en-able a topographic assignment of the paraeso-phageal lymph nodes. All lymph nodes sepa-rately removed should be carefully labelled in-dicating their localisation. If resection speci-mens have to be sent to the pathologist bymail, the specimens have to be opened longi-tudinally, trying to cut on the side opposite tothe tumor, in circular tumors on the anteriorsite and along the greater curvature of thestomach. The specimens are pinned up onstyropore or corkboards (avoid stretching!)and then immersed in sufficient fixative (ac-cording to agreement with the pathologist).
� Information for the pathologist. An optimalhistological examination of incision and totalbiopsies and resection specimens requires ade-quate information for the pathologist on theclinical situation including history.
References
1. Dudeck J, Wagner G, Grundmann E, Hermanek P(eds) (1994) Basisdokumentation für Tumor-kranke, 4. Aufl. Springer, Berlin Heidelberg NewYork Tokyo
2. Eloubeidi MA, Desmond R, Arguedas MR et al.(2002) Prognostic factors in the survival of pa-tients with esophageal carcinoma in the US. Can-cer 95:1434–1444
3. Fraunberger L, Kraus B, Dworak O (1996) Verteilungvon Lymphknoten und Lymphknotenmetastasenbeim Esophaguskarzinom. Zbl Chir 121:102–105
4. Hamilton SR, Aaltonen LA (eds) (2000) Pathologyand genetics of tumors of the digestive system.World Health Organisation Classification of tu-mors. IARC Press, Lyon
5. Hermanek P, Wittekind Ch (1994) Diagnosticseminar: The pathologist and the residual tumor(R) classification. Path Pract Res 190:115–123
6. Hermanek P, Hutter RVP, Sobin LH, Wittekind Ch(1999) Classification of isolated tumor cells andmicrometastasis. Cancer 86:2668–2673
7. Jacobi CA, Zieren HU, Müller JM, Pichlmaier H(1996) Systematische Lymphadenektomie beim Öso-phaguskarzinom – Vorläufige Ergebnisse einer pro-spektiven randomisierten Studie. Zbl Chir 121:110–115
8. Japanese Society for Esophageal Diseases (1990)Guidelines for the clinical pathologic studies on car-cinoma of the esophagus, 8th ed. Kanehara, Tokyo
9 Pathologic Classification of the Esophageal Carcinoma � 79

9. Junginger T, Hermanek P, Klimpfinger M (2002)Klassifikation maligner Tumoren des Gastrointesti-naltraktes I. Springer, Berlin Heidelberg New York
10. Mandard A-M, Dalibard F, Mandard J-C, Marnay J,Henry-Amar M, Petiot J-F, Roussel A et al. (1994)Pathologic assessment of tumor regression afterpreoperative chemoradiotherapy of esophageal car-cinoma. Cancer 73:2680–2686
11. Nagawa H, Kaizaki S, Seto Y, Tominaga O, Muto T(1995) The relationship of macroscopic shape ofsuperficial esophageal carcinoma to depth of inva-sion and regional lymph node metastasis. Cancer75:1061–1064
12. Roder JD, Busch R, Stein HJ, Fink U, Siewert JR(1994) Ratio of invaded and removed lymph nodesas a predictor of survival in squamous cell carci-noma of the esophagus. Br J Surg 81:410–413
13. Roder JD, Stein HJ, Siewert JR (1995) Esophagealcarcinoma. In: Hermanek P, Gospodarowicz MK,Henson DE, Hutter RVP, Sobin LH (eds) UICCPrognostic factors in cancer. Springer, Berlin Hei-delberg New York Tokyo
14. Sarbia M, Bittinger F, Porschen R, Dutkowski P,Willers R, Gabbert HE (1995) Prognostic value ofhistopathologic parameters of esophageal squa-mous cell carcinoma. Cancer 76:922–927
15. Stein HJ, Feith M (2001) Prognostic factors in thecancer of the esophagus. In: Gospodarowicz MK,Henson DE, Hutter RVP, O’Sullivan B, Sobin LH,Wittekind Ch (eds) Prognostic factors in cancer,2nd ed. Wiley-liss, New York
16. UICC (2002) TNM Classification of malignant tu-mours, 6th ed (Sobin LH, Wittekind Ch, eds). Wi-ley-Liss, New York
17. UICC (2003) TNM Supplement. A commentary onthe uniform use, 3rd ed (Wittekind Ch, Greene FL,Henson DE, Hutter RVP, Sobin LH, eds). Wiley,New York
18. UICC (2005) TNM Atlas. Illustrated guide to theTNM/pTNM classification of malignant tumours,5th ed (Wittekind Ch, Greene FL, Hutter RVP,Klimpfinger M, Sobin LH, eds). Springer, BerlinHeidelberg New York
19. Wagner G, Hermanek P (1995) OrganspezifischeTumordokumentation. Springer, Berlin HeidelbergNew York Tokyo
20. Wittekind Ch (1993) Bedeutung von Tumorwachs-tum und -ausbreitung für die chirurgische Radika-lität. Zbl Chir 1118:500–597
21. Daly JM, Karnell LH, Menck HR (1996) NationalCancer Data Base report on esophageal carcinoma.Cancer 78(8):1820–1828
80 � P. Hermanek: 9 Pathologic Classification of the Esophageal Carcinoma

Throughout the last decades the results of sur-gical treatment on esophageal cancer have im-proved continuously. Before 1980 Isono [1] re-ported a 5-year survival rate of 12.4%. In thisstudy he describes the mode of recurrenceafter esophagectomy: 13.0% of patients had lo-cal recurrence, 8.7% had recurrence in the re-sidual esophagus, 43.5% had evidence oflymph node metastasis, 28.3% had recurrencein other organs, and 6.5% had pleural or peri-toneal tumor dissemination. The relapse pat-tern in lymph nodes showed recurrence in cer-vical nodes in 21.7%, mediastinal nodes in19.6%, and abdominal nodes in 2.2%. Theseresults suggest that extensive surgery with rad-ical lymph node dissection could bear achance of cure for these patients.Meanwhile the more radical en bloc esopha-
gectomy has found widespread approval. In Ja-pan three field lymph node dissection, includ-ing systematic lymphadenectomy of cervical,mediastinal, and abdominal nodes has beenproposed to improve survival rates. However,there is evidence that significantly improved 5-year survival rates can not be achieved as com-pared with two-field dissection [3, 27, 28].The overall frequency of positive lymph
nodes according to all tumor sites is shown inTable 10.1. Improvements in preoperative stag-ing, with the introduction of CT, EUS, andEUS plus FNA (fine needle aspiration) havecontributed to an improved treatment of pa-tients with esophageal cancer. EUS has anoverall staging accuracy for N-status of about60–70% [34], and CT is the appropriate meansto detect distant metastasis in secondary or-gans such as liver or lung. An improvement ofstaging accuracy may be achieved by comple-mentarily supplementing FNA to EUS becauseFNA improves N-stage accuracy, but has nobearing on T-stage accuracy [35]. Thus, unre-
sectable cases can be excluded in most casespreoperatively and can be treated with pallia-tive modalities. This better selection of pa-tients could amount for the improved survivalrates observed over the decades, rather thanthe introduction of lymphadenectomy. The is-sue of radical lymphadenectomy is discussedvery controversially in surgical oncology. Afterinitial enthusiasm a more realistic approach tothis issue has now been advocated, for examplein gastric cancer [4, 5, 29] and non small celllung cancer [6, 30]. It seems that only a limitednumber of patients will experience a benefitfrom this procedure. Patients with advancedtumors (T4) and lymph node involvementshould undergo preoperative radiochemother-apy and should only be operated in case of re-sponse [7]. This better selection of patientscould account for the improved survival ratesobserved over the decades, rather than the in-troduction of lymphadenectomy.Thus, prognosis of patients with esophageal
cancer still remains unsatisfying. Tumor recur-rence occurs frequently even despite the ab-sence of residual tumor detectable at primary
Lymphatic Dissemination and Principlesof Lymph Node DissectionJ.R. Izbicki, A. Rehders, A. Kutup, C. Busch
10
Table 10.1. Frequency of lymph node metastasis
Author Numberof patients
Overall rate oflymph nodemetastasis
Akiyama 1991 236 73.7%
Isono 1991 4590 72.9%
Ide 1994 403 58.0%
Nishihira 1995 171 58.5%
Izbicki 1995 67 55.2%
Altorki 2002 80 69.0%
Lerut 2004 174 70.1%

surgery and by current clinico-pathologicalstaging procedures. This observation suggeststhat a substantial fraction of these patientspresent initially with occult micrometastases.This is confirmed by our own results, with50% of patients with tumor stage pT1 havingimmunhistochemically detected individual tu-mor cells in their lymph nodes. Histopatholog-ically proven lymph node metastases are evi-dent in about 30% of patients with small tu-mors (pT1), which also underlines the earlymetastatic potential of esophageal cancer [26].This is of great clinical importance as lymphnode involvement is regarded as one of thestrongest prognostic factors for tumor recur-rence [9–15]. Therefore, extensive lymph nodesampling is essential to facilitate correct post-operative staging. Hence patients with an in-creased risk for tumor recurrence may be se-lected for adjuvant multimodal treatment.
Anatomy of the lymphatic system
Lymph nodes draining the esophagus arewidely distributed due to two different embry-ologic origins of the esophagus. Throughoutembryologic development the branchial archesand the yolk sac grow together in the area ofthe tracheal bifurcation, forming the origin ofthe esophagus. Thus, the organ has two mainlymphatic collection areas, in the abdomenaround the celiac trunk and at the neck. Pio-neering work on the lymphatics of the esopha-gus was done in 1903 by Sakata, who revealedthat the submucosal lymphatics do not drainsegmentally, but in a longitudinal fashion. Thelymphatic pathway of the middle and superioresophagus goes to the neck before passingthrough the muscular layer to finally reach thedeep cervical nodes and the nodes locatedalong the recurrent laryngeal nerve. The lym-phatics of the lower esophagus drain down-wards to the cardiac nodes and the nodesaround the celiac trunk. These results are alsoreflected by the frequency of lymph node me-tastasis according to tumor location (Table10.2). To assess which lymph nodes have to bedissected for correct staging, analysis of dataconcerning the frequency of lymph node in-volvement is necessary.
� Cervical nodes
The deep cervical node group is often affectedby metastasis, while superficial nodes usuallyare not involved except in very advanced pri-maries. The deep nodes consist of the deeplateral nodes or “the accessory nerve chaingroup” in the lateral part of the neck. The deepexternal nodes include those of the internaljugular chain and the supraclavicular nodes,and the deep internal nodes are located medialto the jugular chain. The lower part of thedeep internal nodes is also known as the “re-current laryngeal nerve chain”. However, thedeep internal nodes bear a very high risk ofmetastasis (Table 10.3).
� Superior mediastinal nodes
At the right side of the superior mediastinum,the lymph node chain along the right recurrentnerve winds around the subclavian artery. Onthe left side of the superior mediastinum,some smaller nodes are located along the leftrecurrent laryngeal nerve. Since these nodes liealong the left laryngeal border, they are alsocalled the “left paratracheal nodes”. Both rightand left laryngeal nerve chain groups bear ahigh risk of metastasis.
� Middle mediastinal nodes
The nodes located at the tracheal bifurcationare also known as the carinal nodes. They arelocated closely to the mid-esophagus and are a
� J. R. Izbicki et al.82
Table 10.2. Frequency of involvement of lymph node groupsassessed by three-field lymphadenectomy
Author No. ofpatients
Cervicalnodes
Media-stinalnodes
Abdomi-nal nodes
Akiyama 1991 236 33.1% 58.1% 49.2%
Isono 1991 1740 27.4% 55.8% 49.2%
Kato 1991 79 36.7% 59.5% 41.8%
Altorki 2002 80 36.25% – –
Lerut 2004 174 23.6% – –

frequent site of metastasis. The posterior medi-astinal nodes, paraaortic nodes, and nodesalong the thoracic duct can also be grouped to-gether as “paraesophageal nodes”. Because oftheir vicinity to the esophagus, they are partic-ularly often involved in tumors located at thelevel of the tracheal bifurcation, which is themost frequent site of tumor occurrence.
� Lower mediastinal nodes
The description of the paraesophageal nodesof the mid-esophagus also applies here.
� Superior gastric nodes
The paracardiac nodes are essential, as theyare frequently involved in esophageal cancer,regardless of tumor location. They are locatedalong the highest branch of the left gastric ar-tery. The nodes of the lesser gastric curvatureare an important route for tumor spread fromthe esophagus to the celiac trunk. The major-ity of the nodes affected by tumor dissemina-tion are situated along the upper half of thelesser curvature in the left gastric area. As amatter of fact, positive nodes hardly ever occuralong the fifth branch of the left gastric artery.Nevertheless, the lesser curvature should be re-moved. The left gastric artery nodes are inter-
10 Lymphatic Dissemination and Principles of Lymph Node Dissection � 83
Table 10.3. Lymph node metastases mapping and localization of the primary tumor
Lymph node Lymph nodes Kato 1991 Akiyama 1991 Nishira 1995field
Rate of involvement Rate of involvement Rate of involvement
� Cervical Accessory nerve chain (right/left)Cervical paraesophagealSupraclavicular rightSupraclavicular leftDeep cervical nodes rightDeep cervical nodes left
�21.5%6.3%6.3%
15.2%21.5%
5%���10.6%8.9%
�21.9%9.4%6.3%9.4%3.1%
� Superiormediastinal
Right recurrent nerveParatracheal (right/left)BrachiocephalicUpper periesophageal
34.2%38.0%�19.0%
37.3%21.2%6.8%9.8%
17.5%12.3%�8.8%
� Middlemediastinal
Infraaortic archTracheobronchialPulmonaryHilar (right/left) infracarinalMiddle periesophagealPosterior mediastinal
2.5%��17.7%20.3%�
6.8%�14.8%14.8%25.4%�
1.8%0.6%4.6%
12.3%12.2%9.4%
� Lowermediastinal
Lower mediastinalLower periesophagealDiaphragmatic (hiatal region)
�13.9%�
25.8%�2.1%
�9.4%0.6%
� Superiorgastric
Paracardiac (right/left)Left gastric arteryLesser curvature
38.0%21.5%11.4%
32.6%23.7%18.2%
25.2%10.5%8.2%
� Distantabdominal
Celiac trunkSplenic arteryCommon hepatic artery
8.9%�2.5%
16.1%�5.1%
3.5%4.7%1.2%

posed between the route of the artery and less-er gastric curvature. This is one of the mainroutes of lymphatic spread from the primarytumor.
� Distant abdominal nodes
The nodes along the short trunk of the celiacartery, the root of the left gastric, the commonhepatic, and the splenic artery belong to thegroup of the celiac nodes. Lymph node meta-stasis occurring at this point indicates systemicdissemination of the tumor. The common he-patic artery nodes lie along the course of thecommon hepatic artery, and metastasis in thisarea also indicates distant tumor spread. Nodesof the hepatoduodenal ligament, distal splenicartery, or splenic hilum are very rare sites oflymphatic tumor spread. Therefore thesegroups are not discussed here.The frequency of metastasis in certain
lymph node groups is influenced by the loca-tion of the primary tumor. Akiyama publisheddata on 236 patients about this aspect of meta-static spread [31]. All patients underwent cer-vico-thoraco-abdominal lymph node dissec-tion. Patients with carcinoma of the upper eso-phagus had metastasis in the neck lymphnodes in 44.1%, upper mediastinum in 50.0%,middle mediastinum in 20.6%, and lower me-diastinum in 5.9%. Remarkably 14.7% of thecases presented with metastasis in the uppergastric area.Carcinoma of the mid-esophagus was asso-
ciated with metastasis in 32.9% in the neck,38.1% in the upper mediastinum, 41.0% in themid-mediastinum, 20.2% in the lower media-stinum, and 42.5% in the upper gastric region.Carcinoma of the lower esophagus was asso-ciated with 29.4% positive lymph nodes in theneck and 30.9% in the upper mediastinum,48.5% bad metastasis in the middle mediasti-num, 35.3% in the lower mediastinum, and69.1% in the upper gastric area.
In summary the incidence of metastases in thesuperior mediastinum and the neck is high,even in patients with primary tumors locatedin the lower esophagus. These data underlinethe importance of extensive lymph node sam-pling for correct staging.
Since the present 5-year survival rates ofradical three-field lymph node dissection donot seem to improve 5-year survival rates sig-nificantly, a minimal tumor spread in seem-ingly localized disease has to be assumed [26],which is confirmed by our own data. 50% ofour pN0 patients had single immuno-stainedtumor cells in their lymph nodes (Table 10.4).The presence of these cells was an independentfactor for a significantly reduced relapse-freesurvival. The demonstrated prevalence for de-veloping distant metastases in our patientswith tumor cells in lymph nodes suggests thatthe presence of these cells is an expression of ageneralized tumor disease rather than an indi-cator of the site of subsequent metastasis. Thusthe majority of patients with esophageal cancercannot be cured by surgery alone. Therefore,the benefit of radical systematic three-fieldlymphadenectomy on relapse-free survival, andoverall survival, remains unclear. Therefore, werecommend extensive lymph node samplingfor correct pathological staging to identify thegroup of patients who may benefit from adju-vant therapeutic regimes because of a minimalresidual tumor load.Since lymph node spread remains an ex-
tremely rare event in patients with early cancerconfined to the lamina propria (Tis), new ther-apeutic concepts of local treatment have beenadvocated as an adequate therapy. Strip biopsyof the mucosa and photodynamic therapy or
� J. R. Izbicki et al.84
Table 10.4. Frequency and location of lymph node groupsaffected by micrometastasis *
Lymph node field Lymph nodes Rate ofinvolvement(%)
� Superior mediastinal periesophageal 3.0paratracheal 4.5
� Middle and lower carinal 8.9mediastinal tracheobronchial 3.0
� Abdominal paracardiac 7.5hepatic artery 7.5celiac trunk 14.9
� Periesophageal nodesnext to primary lesion
8.9
* Data from micrometastasis in 393 lymph nodes of 67 pa-tients with esophageal cancer [26]

laser therapy for local intraluminal treatment,and minimally invasive surgery for resectionof the esophagus are applied to patients, inwhom endoluminal ultrasound suggests a limi-tation of the tumor to the mucosa.
Operative procedure
� Abdomino-thoracic en bloc esophagectomy
The operation starts with the patient in a leftsided position with the thorax slightly angu-lated, opening the right sided intercostal spacesand a right anterolateral thoracotomy in thefifth intercostal space is performed. After tho-racotomy, a rib retractor is inserted, and de-compression of the right lung is commenced.Incision of the mediastinal pleura starts by di-viding the hilum of the right lung along theright pulmonary ligament, and then proceedsat the back of the lateral side of the tracheaand the V. cava superior up to the thoracicaperture. At this point the incision turns lateralto the V. azygos and descends at its lateral sidedown to the diaphragm and then medial tocomplete the pleural incision. Care must betaken not to compromise the phrenic nerve.The azygos vein is now divided between
ligatures at the confluens to the V. cava supe-rior. Lymphadenectomy starts along the venacava superior up to the laryngeal nerve, whichis identified properly. Lymphadenectomy ex-tends now along the dorsal wall of the venacava to the pre- and paratracheal lymph nodes,including the tracheobronchial, upper paraeso-phageal, and retrotracheal node groups. Thevagus nerve is divided caudal to the laryngealnerve.The intercostal branches of the azygos vein
are ligated and divided. Lymph node dissectionis carried out along the dorsal pericardium ex-tending from the main carina down to the veinof the right lower lobe including dissectionalong the bronchus intermedius and thebronchus of the right lower lobe paraaortal tothe left hilum. Lymphadenectomy continuesalong the ascending aorta including the para-aortal node groups, the subcarinal nodes, andthe lymph nodes of the left hilum.
Dissection continues at the anterior wall ofthe descending thoracic aorta to the anteriorligament of the spine up to the right brachio-cephalic vein and the confluence of the anony-mous veins, turning then to the left side of theaorta.While dissecting along the aortic arch,
branches supplying the esophagus are dividedand ligated. Lymphadenectomy now is directedversus caudal on the adventitia of the aortadescendens. At the tracheal bifurcation, thethoracic duct is ligated cranially.Dissection is completed down to the aortal
and esophageal hiatus where the thoracic ductis ligated caudally.The abdominal part of the lymphadenec-
tomy starts after changing the patient to thesupine position, with a bilateral subcostal inci-sion combined with an upper median laparo-tomy.Lymphadenectomy starts at the hepatoduo-
denal ligament. The right gastric artery is di-vided at the bifurcation from the gastroduode-nal artery. Lymphadenectomy continues alongthe common hepatic artery up to the celiactrunk.Next, the left gastric artery is divided at the
celiac trunk and lymphadenectomy is per-formed along the upper margin of the pan-creas along the splenic artery and down to theorigin of the celiac trunk at the aorta. Fromthere lymphadenectomy is performed alongthe aorta up to the aortic hiatus of the dia-phragm. Abdominal lymphadenectomy is com-pleted by lifting up the lesser curvature anddissecting the node groups at the cardia afterincision of the esophageal hiatus.
� Lymphadenectomyin transhiatal esophagectomy
Operation starts in supine position with a bi-lateral subcostal incision combined with anupper median laparotomy, as it is done in theabdominal part of the radical en bloc esopha-gectomy.Abdominal lymphadenectomy is performed
exactly as described for the abdominal part ofthe en bloc esophagectomy.After incision of the esophageal hiatus, lym-
phadenectomy is performed along the ventral
10 Lymphatic Dissemination and Principles of Lymph Node Dissection � 85

side of the aorta up to the carina including theparaaortal and paraesophageal lymph nodegroups under direct vision. Both pulmonary li-gaments are divided and the lymph nodes re-moved.Starting at the level of the pulmonary hilum
or the main carina, the dissection plane ap-proaches the esophageal wall.
� Three-field lymphadenectomy
Two-field lymphadenectomy is conducted asdescribed earlier, except for the lymph nodedissection of the anterior mediastinum. Inci-sion of the median laparotomy is now ex-tended up to the neck, and a Kocher’s collarincision is made subsequently.After partial or complete sternotomy is per-
formed, cervico-mediastinal lymphadenectomybegins with dissection of the paratracheal nodegroups on both sides in the upper anterior andupper posterior mediastinum. It starts fromthe carina up to the node groups betweenanonymous vein and clavicula, dissecting theright and left laryngeal nerves from the originto the larynx. Lymph node dissection also in-cludes the thymus in the anterior mediasti-num.Lymphadenectomy goes up to the central
cervical compartment between the carotid ar-teries including the paratracheal, infra- and su-prathyroidal and submandibular node groups.Three-field lymphadenectomy ends with dis-
section of the lateral cervical compartments in-cluding lymph nodes between the carotid ar-tery and the trapezius muscle starting fromthe subclavian vein up to the hypoglossusnerve on the ventral and dorsal side of the cer-vical plexus.Sometimes the term three-field lymphade-
nectomy applies just to the combination of thetwo-field lymphadenectomy with a bilateralmodified neck-dissection encompassing cervicalthymectomy without using a median sterno-tomy.
References
1. Isono K, Onoda S, Ishikawa T, Sato H, NakayamaK (1982) Studies on the causes of deaths from eso-phageal carcinoma. Cancer 49:2173–2179
2. Byrne J, Waldron R, McAvinchey D, Dervan P(1987) The use of monoclonal antibodies for thehistopathological detection of mammary axillarymicrometastases. J Surg Oncol 13:409–411
3. Watanabe H (1992) Plattenepithelcarcinom desOesophagus. Chirurg 63:689–692
4. Van de Velde CJH, Bohnenkamp HJ, Sasako M(1995) The value of extended lymphadenectomyfor gastric cancer will become clear in a prospec-tive randomized trial in the Netherlands. Int J SurgSci 2:11–16
5. Siewert JR, Böttcher K, Roder JD, Busch R, Her-manek P, Meyer HJ (1993) Prognostic relevance ofsystematic lymph node dissection in gastric carci-noma. Br J Surg 80:1015–1018
6. Izbicki JR, Thetter O, Habekost M et al (1994)Radical systematic mediastinal lymphadenectomyin non-small cell lung cancer: a randomized con-trolled trial. Br J Surg 81:229–235
7. Shields TW (1990) The significance of ipsilateralmediastinal lymph node metastasis (N2 disease) innon-small cell carcinoma of the lung. A commen-tary. J Thorac Cardiovasc Surg 99:48–53
8. Watanabe Y, Shimizu J, Tsubota M, Iwa T (1990)Mediastinal spread of metastatic lymph nodes inbronchogenic carcinoma. Mediastinal nodal meta-stases in lung cancer. Chest 97:1059–1065
9. Siewert JR, Bartels H, Bollschweiler E et al (1992)Plattenepithelcarzinom des Ösophagus. Chirurg 63:693–700
10. Vogel SB, Mendenhall WM, Sombeck MD, MarshR, Woodward ER (1995) Downstaging of esopha-geal cancer after preoperative radiation and chemo-therapy. Ann Surg 221:685–695
11. Becker HD (1994) Esophageal cancer, early disease:diagnosis and current treatment. World J Surg 18:331–338
12. Hennessy TPJ (1994) Lymph node dissection.World J Surg 18:367–372
13. Lerut T, de Leyn P, Coosemans W, van RaemdonckD, Cuypers P, Van Cleynenbreughel B (1994) Ad-vanced esophageal carcinoma. World J Surg 18:379–387
14. Scholz J, Steinhöfel U, Dürig M et al (1993) Post-operative pulmonary complications in patientswith esophageal cancer. Clin Investig 71:294–298
15. Martini N, Flehinger BJ (1987) The rote of surgeryin N2 lung cancer. Surg Clin North Am 67:1037–1049
16. Izbicki JR, Passlick B, Karg O et al (1995) Impactof radical systematic mediastinal lymphadenec-tomy on tumor staging in lung cancer. Ann ThoracSurg 59:209–214
� J. R. Izbicki et al.86

17. Shields TW, Yee J, Conn JH, Robinette CD (1975)Relationship of cell type and lymph node metasta-sis to survival after resection of bronchial carcino-ma. Ann Thorac Surg 20:501–510
18. Pearson FG, DeLarne NC, Ilves R, Todd TR, Coop-er JD (1982) Significance of positive superior me-diastinal nodes identified at mediastinoscopy inpatients with resectable cancer of the lung. J Tho-rac Cardiovasc Surg 83:1–11
19. The Lung Cancer Study Group (1988) Should sub-carinal lymph nodes be routinely examined in pa-tients with non-small cell lung cancer? J ThoracCardiovasc Surg 95:883–887
20. Raymond WA, Leong AS (1989) Immunoper-oxidase staining in the detection of lymph nodemetastases in stage I breast cancer. Pathology 21:11–15
21. Martini N, Flehinger BJ, Zaman MB, Beattie EJ Jr(1983) Results of resection in non-oat cell carcino-ma of the lung with mediastinal lymph node me-tastases. Ann Surg 198:386–397
22. Naruke T, Suemasu K, Ishikawa S (1978) Lymphnode mapping and curability at various levels ofmetastasis in resected lung cancer. J Thorac Car-diovasc Surg 76:832–839
23. Lerut T, DeLeyn P, Coosemans W, van RaemdonckD, Schers I, LeSaffre E (1992) Surgical strategies inesophageal carcinoma with emphasis on radicallymphadenectomy. Ann Surg 216:583–590
24. Siewert JR, Dittler H-J (1993) Esophageal carcino-ma: impact of staging on treatment. Endoscopy25:28–32
25. Marcon NE (1994) The endoscopic management ofesophageal cancer. Acta Gastro-Enterol Belg 57:143–154
26. Izbicki JR, Hosch SB, Pichlmeier U, Rehders A,Busch C, Niendorf A, Passlick B, Broelsch CE, Pan-tel K (1997) Prognostic value of immunohisto-chemically identifiable tumor cells in lymph nodesof patients with completely resected esophagealcancer. New Engl J Med 337:1188–1194
27. Law S, Wong J (2007) Lymph node dissection insurgical treatment of esophageal neoplasms. SurgOncol Clin N Am 16 (1):115–131
28. Nozoe T, Kakeji Y, Bab H, Maehara Y (2007) Two-field lymph-node dissection may be enough totreat patients with submucosal squamous cell car-cinoma of the thoracic esophagus. Dis Esophagus18(4):226–229
29. Danielson H, Kokkola A, Kiviluoto T, Siren J, Lou-himo J, Kivilaakso E, Puolakkainen P (2007) Clini-cal outcome after D1 vs D2-3 gastrectomy fortreatment of gastric cancer. Scand J Surg 96(1):35–40
30. Doddoli C, Aragon A, Barlesi F, Chetaille B, Robi-tail S, Giudicelli R, Fuentes P, Thomas P (2005)Does the extent of lymph node dissection influenceoutcome in patients with stage I non-small-celllung cancer? Eur J Cardiothorac Surg 27(4):680–685
31. Akiyama H, Tsurumaru M, Udagawa H, KajiyamaY (1994) Radical lymph node dissection for cancerof the thoracic esophagus. Ann Surg 220(3):364–372, discussion 372–373
32. Lerut T, Nafteux P, Moons J et al (2004) Three-fieldlymphadenectomy for carcinoma of the esophagusand gastroesophageal junction in 174 R0 resec-tions: impact on staging, disease-free survival, andoutcome. Ann Surg 240(6):962–974
33. Altorki N, Kent M, Ferrara C, Port J (2002) Three-field lymph node dissection for squamous cell andadenocarcinoma of the esophagus. Ann Surg236(2):177–183
34. Kutup A, Link BC, Schurr PG et al (2007) Qualitycontrol of endoscopic ultrasound in preoperativestaging of oesophageal cancer. Endoscopy 39(8):715–719
35. Vazquez-Sequeiros E, Wiersema MJ, Clain JE et al(2003) Impact of lymph node staging on therapyof esophageal carcinoma. Gastroenterology 125(6):1626–1635
10 Lymphatic Dissemination and Principles of Lymph Node Dissection � 87

Despite new insights into its molecular basisand various treatment options evaluated in nu-merous trials, therapy of esophageal cancer re-mains a challenge. In the past, surgery was theonly treatment option. A patient qualified forsurgery when he presented in stable conditionand when the tumor was believed to be resec-table. Today a vast number of treatment strate-gies, including induction chemotherapy, radio-chemotherapy with or without combinationwith surgery, administered in an adjuvant or aneoadjuvant setting, are added to the tradi-tional therapy of surgery alone. Even the ques-tion, whether surgery after effective chemora-diation does have any impact on prognosis atall or is no more than a “big biopsy” is dis-cussed today. There is increasing evidence thatpatients may benefit from induction chemo-therapy.However, on the basis of the results of the
trials performed, complete resection of the tu-mor currently remains the gold standard oftherapy and surgery by far offers the bestchance for cure. Ongoing trials concentrate onan improvement of the chemotherapy andradiotherapy regimens as well as on an im-provement of the drugs used.Adequate treatment for patients with eso-
phageal carcinoma and carcinoma of the car-dia is based on tumor typing, anatomic loca-tion, and tumor staging.Resection usually entails subtotal esopha-
gectomy and radical lymphadenectomy. Insome cases, as discussed below, gastrectomy orextended resections may be necessary. How-ever, in order to give the patient the chance tobe cured, an R0 resection is imperative.Esophageal carcinoma, if untreated, leads to
death after diagnosis within 3–6 months. Ra-diotherapy alone can achieve two-year survivalrates with a maximum of 20%. Results for che-
motherapy alone are even worse. The value ofchemotherapy lies in neoadjuvant protocols orin combination with radiation, especially inadenocarcinomas.
Tumor typing
In the past the majority of malignant esopha-geal tumors were squamous cell carcinomas.However, the frequency of adenocarcinomas isrising, accounting for up to 60% of all malig-nant esophageal tumors.Due to the high potential of squamous cell
carcinomas to metastasize into the peri-eso-phageal lymphatics, radical removal withoutresidual disease will usually require transtho-racic en bloc esophagectomy. This includesremoval of the lymph nodes of the lower andupper mediastinum, and the abdominal lymphnodes. The value of removal of unsuspiciouscervical lymph nodes is still discussed contro-versially. So far this three-field lymphadenec-tomy has not been evaluated in a prospectiverandomized fashion. Retrospective data collec-tions of personal experiences favor three-fieldlymphadenectomy over two-field lymphade-nectomy with comparable morbidity and mor-tality, while other large personal data collec-tions advocate transhiatal esophagectomy. Thetranshiatal approach enables removal of thelymph nodes of the entire lower mediastinumdorsal to the pericardium. However, lymphaticclearance around and above the main carina isdangerous and unreliable.In contrast, adenocarcinomas, if localized at
the cardia (type II according to Siewert’s clas-sification), metastasize mainly to the abdom-inal or inferior mediastinal lymph nodes. Since
Rationale for Type of Resection in Cancer ofthe Esophagus and Gastroesophageal JunctionW.T. Knoefel, I. Alldinger, J.R. Izbicki
11

these fields can be reached via a transhiatalapproach, this procedure is warranted, espe-cially in patients who are not fit for a trans-thoracic procedure. On the one hand some fa-vor the transthoracic procedure in case of T2tumors because of the probability of a high in-cidence of positive lymph nodes in the uppermediastinum. On the other hand, there aresome who favor the extended gastrectomy forthe true cardia carcinoma. According to Sie-werts’ classification, for type III carcinoma theextended gastrectomy is the standard proce-dure.Adenocarcinomas that arise more than 1 cm
proximal to the muscular border between eso-phagus and stomach (type I according to Sie-wert’s classification) may metastasize like squa-mous cell carcinomas. The value of lymphade-nectomy of the upper mediastinum in thesepatients, however, is under discussion. Positiveupper mediastinal lymph nodes are found inapproximately 20% of patients with early ade-nocarcinomas (T1b), and lymph node recur-rence of adenocarcinoma above the carina hasbeen reported in over 20% of patients afterlymph node clearance of the inferior mediasti-num only. Lymph node metastases in the uppermediastinum are mainly present in T2 and T3.Therefore transthoracic resection with radicallymph node clearance of the lower and uppermediastinum is indicated.If all histological typings, including adeno-
carcinomas and squamous cell carcinomas, aregrouped together, a survival benefit has beenshown for transthoracic en bloc esophagec-tomy. Consequently, if in doubt, this operationshould be performed if the patient is deemedfit for the procedure.
Anatomic location
The esophagus can be divided into 4 regions:� The cervical esophagus extends from theupper esophageal sphincter to the entranceof the esophagus into the thorax. This corre-sponds to a distance between approximately15 and 20 cm from the incisors.
� The upper thoracic part of the esophagusextends down to the bifurcation of the tra-
chea. This anatomical structure is best visu-alized on a barium swallow.
� The lower thoracic esophagus extends fromthe main carina down to the hiatus of theesophagus which corresponds to approxi-mately 38–44 cm from the incisors.
� The gastroesophageal junction comprisesthe area of the esophagus 5 cm proximal to5 cm distal to the anatomical cardia. Sincethe epithelial border moves during the indi-vidual’s life and especially in disease, it can-not be used as a landmark for location.
Cervical esophagus
Tumors of the cervical esophagus have theirlymphatic drainage mainly to the neck andinto the thoracic duct. These tumors usuallyarise from squamous epithelium. Due to theirclose anatomic relationship to the larynx andupper trachea these tumors are often primarilyirresectable. Therefore large T3 and especiallyT4 tumors may benefit from preoperative com-bined radiochemotherapy to downstage thetumor. This enables transthoracic en bloc eso-phagectomy, bilateral modified neck dissection,and a reconstruction either with a gastric tubeor colon interposition. Occasionally a localresection with free jejunal interposition maybe indicated. However, even in these cervicallesions, lymphatic metastases to the mediasti-num are frequent. These very high lesions arerare and account for only about 5% of esopha-geal cancers.
Upper thoracic esophagus
The majority of tumors of the upper esopha-gus are squamous cell carcinomas with a tre-mendous increase in the proportion of adeno-carcinomas over the last years.Lymphatic drainage of squamous cell carci-
nomas of the upper thoracic esophagus ismainly towards the neck with 15–30% positivelymph nodes in surgical specimens. If these tu-
� W. T. Knoefel et al.90

mors metastasize to the lymph nodes belowthe carina, the location of these metastases isinfracarinal (15%), in the lower mediastinum(15%), or directly adjacent to the cardia (23%).The comparable data for adenocarcinomas arenot yet available, but there is no reason to be-lieve they would be different. Accordingly radi-cal removal of the tumor entails thoraco-ab-dominal en bloc esophagectomy and resectionof the corresponding lymph node regions [39].These tumors are more likely to be resec-
table than tumors of the cervical esophagus.However, infiltration of the aorta, trachea, andthe main bronchi should be ruled out beforeproceeding to surgery. If there is a strong sus-picion of a T4 tumor involving the above men-tioned structures, a preoperative radiochemo-therapy might help to downstage the tumorand enable radical resection.Unfortunately, the randomized studies per-
formed included both adenocarcinomas andsquamous cell carcinomas, although epidemiol-ogy, etiology, biology of metastases, and prog-nosis differ markedly [23]. Available data indi-cate that neoadjuvant chemoradiation is mosteffective in patients with advanced squamouscell carcinomas with a close topographicalrelationship to the tracheo-bronchial system[32]. The most effective adjuvant therapy inadvanced adenocarcinomas is preoperativechemotherapy [32]. However, due to the weakevidence provided in the trials performed, aprospective randomized trial to assess the opti-mal subgroups of patients that benefit fromthis strategy is badly needed.
Lower thoracic esophagus
Tumors of the esophagus below the carina oc-cur in an approximately equivalent frequencyas adenocarcinomas and as squamous cell car-cinomas [8, 9]. Squamous cell carcinomas ofthis location metastasize in about 15% [10] tothe lymph nodes above the carina and also inmore than 10% to the lymph nodes in the he-pato-duodenal ligament. Again, these data arenot available for adenocarcinomas, but upper
thoracic lymphatic metastases are frequent alsoin patients with adenocarcinomas [21]. Thebest chance for cure therefore lies in a thora-co-abdominal en bloc esophagectomy with rad-ical systematic lymph node clearance in thethorax and the abdomen [31]. These tumorsare more frequently initially resectable withoutresidual tumor than those of the higher eso-phagus. Only T4 tumors with infiltration ofthe heart, the aortic wall, or vertebrae are gen-erally considered non-resectable. Neoadjuvanttherapy is recommended according to the cri-teria for the upper thoracic esophagus. T4 ex-tension into the lung or the diaphragm is not acontraindication for surgery since prognosis ofthese tumors does not so much depend onT stage, but on N stage [33]. Unfortunately,these tumors metastasize in about 20% to thelymph nodes in the celiac trunk (M1 lymph).These M1 stages are currently considered acontraindication for radical surgery, although,for many surgeons, the difference between alymph node at the left gastric artery or one atthe celiac trunk is not striking. Convincingdata to support a nihilistic approach for M1(lymph) stages at the celiac trunk in compari-son to N1 stages at the left gastric artery arelacking. However, detection of this stage bypreoperative imaging is unreliable. Also, dur-ing the course of a routine thoraco-abdominalesophagectomy the thoracic part is alreadycompleted when the M1 stage is surprisinglydetected. Hence, occasionally in these tumors a‘palliative’ thoraco-abdominal esophagectomyensues.
Tumors of the gastroesophageal junction
Most tumors that are summarized under thisdefinition are adenocarcinomas. In fact theyare defined as adenocarcinomas in the region5 cm proximal to 5 cm distal of the muscularlimit between esophagus and stomach. Themucosal limit is unreliable since it moves dueto disease and age of the patient. Three tumorentities are summarized under this definitionand require specific treatment.
11 Rationale for Type of Resection in Cancer of the Esophagus and Gastroesophageal Junction � 91

� The first entity, type I according to Siewert’sclassification [38], is a distal esophageal adeno-carcinoma in the region between 5 cm proxi-mal to 1 cm proximal of the muscular limit be-tween esophagus and stomach. They accountfor 30–35% of the tumors of the gastroesopha-geal junction [35].These tumors tend to spread longitudinally
in the submucosal lymphatic vessels of the eso-phageal wall. Data about the ideal surgicalapproach are inconsistent. It is obvious thatradical lymphadenectomy of the lower media-stinum is compulsory. No confident data areavailable to decide whether this procedureshould be combined with thoraco-abdominalesophagectomy or if transhiatal esophagectomywith lymphadenectomy of the lower mediasti-num and the periaortic compartment only issufficient or should be reserved for high riskpatients. The potentially higher oncologicalsafety of the extended operation comes with anincreased morbidity and mortality. Removal ofall lymph nodes in the area of the lesser curva-ture, and especially around the celiac trunkand probably also in the hepatoduodenal liga-ment, remains advisable. After wide excisionof the diaphragm, the lower mediastinum upto the carina can be cleared satisfactorily bythis route. Aortic branches to the esophagusendanger the route above the carina duringblunt dissection. Therefore the esophageal wallis reached at this level during dissection.
� Type II of these entities is the so-called car-cinoma of the cardia. It is defined as an ade-nocarcinoma between 1 cm proximal to 2 cmdistal of the muscular border between esopha-gus and stomach. Although most of these tu-mors are truly adenocarcinomas, a certain per-centage of up to 15% can occur as adeno-squa-mous carcinomas. It is speculated that this isdue to an instable differentiation of thesetumor cell lines [36]. These tumors should betreated just like the true adenocarcinomas.For type II carcinomas of the gastroesopha-
geal junction staging becomes important to se-lect adequate treatment. All of these tumorsexcept T1 N0 carcinomas will require total gas-trectomy with lymphadenectomy as performed
in patients with gastric carcinoma. In patientswith stage I or II carcinomas of the cardia,total gastrectomy with distal esophageal resec-tion and transmediastinal reconstruction witha jejunal loop is sufficient. General experiencenot based on large studies so far is that thelymphatic spread into the periesophageallymph nodes as well as in the esophageal wallis not extensive enough to justify an esophago-gastrectomy. However, perigastric and lowerperiesophageal lymphatic clearance is impor-tant. It is also imperative to obtain negative re-section margins on frozen section. In contrastpatients with stage III and IV carcinoma of thecardia may benefit from esophagogastrectomywith consecutive colon interposition. No ran-domized prospective studies have shown abenefit for this procedure so far. Therefore thisapproach should be limited to low operativerisk patients with a high risk of recurrence, toprospective studies, and eventually to patientswith a simultaneously occurring very long Bar-rett’s segment in the thoracic esophagus. Inthese tumors a transhiatal approach with re-moval of the lymph nodes in the lower medias-tinum is preferred to avoid excessive morbidityand since no data exist so far showing a pre-dominance for lymphatic relapse in the upperthorax.
� Type III carcinoma of the gastroesophagealjunction is defined as a tumor between 2 cmbelow the muscular gastroesophageal limit and5 cm below this limit. These tumors accountfor 40–45% of all tumors of the gastroesopha-geal junction. Treatment of these tumors issimilar to early type II carcinomas with ab-dominal transhiatal total gastrectomy includingdistal esophagectomy. However, since these tu-mors have not reached the longitudinal lym-phatic vessels of the esophageal wall, subtotalesophagectomy is not necessary unless nega-tive margins on frozen section cannot bereached. A subtotal proximal gastric resectionis, however, not recommended. Functional re-sults are, due to a high incidence of alkalinereflux, poor [37], and lymphatic clearance isless sufficient than with total gastrectomy.
� W. T. Knoefel et al.92

Limited resections
Limited resection of the gastroesophageal junc-tion with reconstruction by jejunal interposi-tion (Merendino procedure) between distalesophagus and gastric fundus seems to be suf-ficient in early stages of tumors of the gastro-esophageal junction. A short Barrett’s segment,ending below the carina and a T1a (T1b) N0stage has to be confirmed before embarkingon this less invasive procedure.
Palliative esophageal resection
Palliative esophageal resection for esophagealcarcinoma is extremely rare. It can be indi-cated if the palliative character becomes ob-vious only after the point of no return hasbeen reached in the course of the operation.For example, after completion of the thoracicpart of a thoraco-abdominal esophageal resec-tion, a liver metastasis that eluded preoperativestaging is detected after opening the abdomen.Another example is the postoperative detectionof tumor spread in a celiac trunk lymph node.These palliative resections are incidental andcannot be compared to intended palliative re-sections. In extremely rare cases a palliativeesophagectomy may be planned ahead as anindividualized intent to treat or palliate. It isstill unclear whether the patient will gainsomething in terms of quality of life or even insurvival in comparison to palliative radioche-motherapy and stent placement [38]. Morbidityand mortality, however, are high in these pa-tients. Palliative resections should ideally belimited resections, like cervical resection or aMerendino operation.So far, reliable assessment of quality of life
in these two patient groups is imperfect but isbecoming standardized [39]. It will deliverguidelines for the treatment of this desperategroup of patients. So far, valuable data compar-ing stent placement with surgical removal ofthe esophagus are not yet available. An in-dividualized decision, based on the generaland tumor specific condition of the patient aswell as on the experience of the surgeon, is sofar the only option.
Recurrences
Distant relapse of esophageal cancer such asliver metastases, pulmonary metastases, etc.are usually no indication for operative treat-ment. In contrast, a localized relapse such as arelapse after transhiatal gastrectomy for anearly type II carcinoma of the cardia may re-quire surgery. The success depends very muchon the early diagnosis of this recurrence. If thetumor has not spread to vital structures a radi-cal surgical approach with consecutive colon-interposition or free jejunal interposition maybe promising. For these recurrences, however,an individualized approach is necessary.
Summary
Since current medical treatment has no otherpromising therapeutic alternative to an R0 re-section, an aggressive surgical approach seemsto be warranted. Subgroups of patients mightqualify for different therapeutic approaches,but definition of these subgroups remains un-certain. Available data show that the parame-ters histology, tumor location, and tumor stageare not sufficient to define a tailored therapeu-tic concept. The goal for the next years lies inthe development of tools to define these sub-groups in order to avoid overtreatment andundertreatment. Gene expression and genomicprofiling might help in the individualization oftherapy.
References
1. Munro AJ (2004) Oesophageal cancer: a view overoverviews. Lancet 364:566–568
2. Bedenne L, Michel P, Bouche O et al (2002) Ran-domized phase III trial in locally advanced esopha-geal cancer: radiochemotherapy followed by surgeryversus radiochemotherapy alone (FFCD 9102). AmSoc Clin Oncol Proc, p 519 (abstract)
3. Medical Research Council Oesophageal Cancer Work-ing Group (2002) Surgical resection with or withoutpreoperative chemotherapy in oesophageal cancer:a randomised controlled trial. Lancet 359:1727–1733
11 Rationale for Type of Resection in Cancer of the Esophagus and Gastroesophageal Junction � 93

4. Stein HJ, Feith M, Müller J, Werner M, Siewert JR(2000) Limited resection for early adenocarcinomain Barrett’s esophagus. Ann Surg 232(6):733–742
5. Beatty JD, DeBoer G, Rider WD (1979) Carcinomaof the esophagus: pretreatment assessment, corre-lation of radiation treatment parameters with sur-vival, and identification and management of radia-tion treatment failure. Cancer 43:2254-2267
6. Earlam R, Cunha-Melo JR (1980) Oesophageal squa-mous cell carcinoma: I. A critical review of surgery.Br J Surgery 67:381–390
7. Newaishy GA, Read GA, Duncan W, Kerr GR(1982) Results of radical radiotherapy of squamouscell carcinoma of the oesophagus. Clin Radiol 33:347–352
8. Lund O, Hasenkam JM, Aagaard MT, Kimose HH(1989) Time-related changes in characteristics ofprognostic significance in carcinomas of the oeso-phagus and cardia. Br J Surg 76:1301–1307
9. Blot WJ, Devesa SS, Kneller RW, Fraumeni JF Jr(1991) Rising incidence of adenocarcinoma of theesophagus and gastric cardia. JAMA 265:1287–1289
10. Akiyama H (1980) Surgery for carcinoma of theesophagus. Curr Probl Surg 17:53–120
11. Baba M, Aikou T, Yoshinaka H, Natsugoe S, Fuku-moto T, Shimazu H, Akazawa K (1994) Long-termresults of subtotal esophagectomy with three-fieldlymphadenectomy for carcinoma of the thoracicesophagus. Ann Surg 219:310–316
12. Hennessy TP (1994) Lymph node dissection. WorldJ Surg 18:367–372
13. Lerut TE, de Leyn P, Coosemans W, Van Raem-donck D, Cuypers P, Van Cleynenbreughel B(1994) Advanced esophageal carcinoma. World JSurg 18:379–387
14. Akiyama H, Tsurumaru M, Udagawa H, KajiyamaY (1994) Radical lymph node dissection for cancerof the thoracic esophagus. Ann Surg 220:364–373
15. Fujita H, Kakegawa T, Yamana H, Shima I, Toh Y,Tomita Y, Fujii T, Yamasaki K, Higaki K, Noake Tet al (1995) Mortality and morbidity rates, postop-erative course, quality of life, and prognosis afterextended radical lymphadenectomy for esophagealcancer. Comparison of three-field lymphadenec-tomy with two-field lymphadenectomy. Ann Surg222:654–662
16. Kato H, Tachimori Y, Watanabe H, Igaki H, Naka-nishi Y, Ochiai A (1996) Recurrent esophagealcarcinoma after esophagectomy with three-fieldlymph node dissection. J Surg Oncol 61:267–272
17. Altorki NK, Skinner DB (1997) Occult cervicalnodal metastasis in esophageal cancer: preliminaryresults of three-field lymphadenectomy. J ThoracCardiovasc Surg 113:540–544
18. Lerut T, Nafteux P, Moons J, Coosemans W, DeckerG, De Leyn P, Van Raemdonck D, Ectors N (2004)Three-field lymphadenectomy for carcinoma of theesophagus and gastroesophageal junction in 174R0 resections: impact on staging, disease-free sur-vival, and outcome: a plea for adaptation of TNM
classification in upper-half esophageal carcinoma.Ann Surg 240:962–974
19. Orringer MB, Marshall B, Iannettoni MD (1999)Transhiatal esophagectomy: clinical experience andrefinements. Ann Surg 230:392–403
20. Tachimori Y, Kato H, Watanabe H, Sasako M,Kinoshita T, Maruyama K (1996) Difference be-tween carcinoma of the lower esophagus and thecardia. World J Surg 20:507–511
21. Hoelscher AH, Bollschweiler E, Bumm R, BartelsH, Hoefler H, Siewert JR (1995) Prognostic factorsof resected adenocarcinoma of the esophagus. Sur-gery 118:845–855
22. Clark GW, Peters JH, Ireland AP, Ehsan A, HagenJA, Kiyabu MT, Bremner CG, DeMeester TR (1994)Nodal metastasis and sites of recurrence after enbloc esophagectomy for adenocarcinoma. AnnThorac Surg 58:646–653
23. Siewert JR, Stein HJ, Feith M (2003) Surgicalapproach to invasive adenocarcinoma of the distalesophagus (Barrett’s cancer). World J Surg 27(9):1058–1061
24. Skinner DB, Little AG, Ferguson MK, Soriano A,Staszak VM (1986) Selection of operation for eso-phageal cancer based on staging. Ann Surg 204:391–401
25. Lerut T, De Leyn P, Coosemans W, Van Raem-donck D, Scheys I, LeSaffre E (1992) Surgical strat-egies in esophageal carcinoma with emphasis onradical lymphadenectomy. Ann Surg 216:583–590
26. Hagen JA, Peters JH, DeMeester TR (1993) Supe-riority of extended en bloc esophagogastrectomyfor carcinoma of the lower esophagus and cardia. JThorac Cardiovasc Surg 106:850–859
27. Junginger T, Dutkowski P (1996) Selectiveapproach to the treatment of oesophageal cancer.Br J Surg 83:1473–1477
28. Doggett RLS, Guernsey JM, Bagshaw MA (1970)Combined radiation and surgical treatment of car-cinoma of the thoracic esophagus. Front RadiatTher Oncol 5:147–154
29. Parker EF, Gregorie HB (1976) Carcinoma of theesophagus. Long-term results. JAMA 235:1018–1020
30. Siewert JR, Hölscher AH (eds) Diseases of the Eso-phagus. Springer, Berlin Heidelberg New York To-kyo
31. Hulscher JB, van Sandick JW, de Boer AG, Wijnho-ven BP, Tijssen JG, Fockens P, Stalmeier PF, tenKate FJ, van Dekken H, Obertop H, Tilanus HW,van Lanschot JJ (2002) Extended transthoracic re-section compared with limited transhiatal resec-tion for adenocarcinoma of the esophagus. N EnglJ Med 347(21):1662–1669
32. Lordick F, Stein HJ, Peschel C, Siewert JR (2004)Neoadjuvant therapy for oesophagogastric cancer.Br J Surg 91(5):540–551
33. Izbicki JR, Hosch SB, Pichlmeier U, Rehders A,Busch C, Niendorf A, Passlick B, Broelsch CE, Pan-tel K (1997) Prognostic value of immunohisto-chemically identifiable tumor cells in lymph nodes
� W. T. Knoefel et al.94

of patients with completely resected esophagealcancer. New Engl J Med 337:1188–1194
34. Siewert JR, Stein HJ (1998) Classification of adeno-carcinoma of the oesophagogastric junction. Br JSurg 85(11):1457–1459
35. Siewert JR, Hoelscher AH, Becker K, Goessner W(1987) Kardiacarcinom: Versuch einer therapeu-tisch relevanten Klassifikation (Cardia cancer: at-tempt at a therapeutically relevant classification).Chirurg 58:25–32
36. Steele VE, Nettesheim P (1981) Unstable cellulardifferentiation in adenosquamous cell carcinoma.JNCI 67:149–154
37. Hsu CP, Chen CY, Hsieh YH, Hsia JY, Shai SE, KaoCH (1997) Esophageal reflux after total or proxi-mal gastrectomy in patients with adenocarcinomaof the gastric cardia. Am J Gastroenterol 92:1347–1350
38. Wang LS, Chi KH, Hu MH, Fahn HJ, Huang MH(1996) Management for patients with advanced T4epidermoid carcinoma of the esophagus. J SurgOncol 62:22–29
39. Blazeby JM, Williams MH, Brookes ST, AldersonD, Farndon JR (1995) Quality of life measurementin patients with oesophageal cancer. Gut 37:505–508
11 Rationale for Type of Resection in Cancer of the Esophagus and Gastroesophageal Junction � 95

Rationale for extendeden bloc esophagectomy
Unlike some other malignancies, such as colonand breast carcinoma, recent progress in themanagement of esophageal carcinoma has beenlimited. The overall prognosis for this diseaseremains dismal, having improved only margin-ally over recent decades. Because most patientspresent with advanced stage carcinomas, treat-ment is usually palliative, and only a minorityof patients are cured by surgery. Even whenthe disease is confined to the esophagus, thereis only about a 50% chance of 5-year survivalafter surgical resection.Opinions are divided as to the way forward.
Many Western surgeons believe that increas-ingly radical surgical approaches are unlikelyto improve long-term outcomes, and indeedcould create further problems due to additionalcomplications which follow radical resection.This body of opinion has supported the evalua-tion of adjuvant treatment strategies, with evi-dence now emerging that combined treatmentwith synchronous chemotherapy and radio-therapy improves overall survival [25]. On theother hand, an opposing body of opinion, ledprincipally by the Japanese surgical commu-nity, has advocated more radical lymph noderesection as the way forward, citing improvedoutcomes in uncontrolled studies to supportthis approach.The concept of extensive lymph node resec-
tion combination with esophagectomy, i.e. enbloc esophagectomy, was proposed by Logan in1963 [17]. Originally this entailed the removalof abdominal and thoracic lymph nodes up tolevel of the aortic arch. A more extensive re-section which included lymph nodes in the su-perior mediastinum was the next step, whilst
recently the concept of 3 field (extended)lymph node dissection has emerged. This in-corporates the additional removal of lymphnodes from both sides of the neck, as well asmediastinal and upper abdominal lymphnodes. This radical approach was devised fol-lowing analysis of Japanese data which docu-mented that recurrence of squamous cell carci-noma (SCC) can occur initially in the cervicallymph nodes. Therefore it was proposed thatremoving the cervical lymph nodes might im-prove the overall success rate following esopha-gectomy.The procedure of extended (3 field) esopha-
gectomy has been applied in Japan principallyin patients with potentially curable, i.e. earlierstage SCC of the esophagus. Few Western stud-ies have been reported, in part due to the lackof enthusiasm for this approach, and also be-cause of a lower incidence of curable esopha-geal cancer. There has also been a generalskepticism that extensive lymph node resectionwill achieve better surgical outcomes. In part asurgeon’s acceptance of the concept of patternsof metastatic spread of esophageal cancer. Sup-port for extended resection depends on the hy-pothesis that esophageal cancer spreads se-quentially from the esophageal wall to locallymph nodes initially, and that metastases arearrested at this stage for a period of time be-fore metastasis by hematogenous spread finallyoccurs to distant organs. This concept oftumor spread is often held to be correct for co-lonic malignancy although even here there isno universal acceptance of the concept, andanyway it is unlikely to be applicable to allmalignancies. For example, radical lymph noderesection was proposed by Halsted for carcino-ma of the breast, and it was universally ac-cepted as correct treatment until approximately20 years ago. Breast carcinoma, however, ap-
Results of Extended en bloc Esophagectomy inTreatment of Patients with Esophageal CancerD. I. Watson, G.G. Jamieson
12

pears to metastasize via both lymphatic andhematogenous routes at the same stage in thetumor development cycle. The understandingof this process has led to the development ofconservative surgical approaches to breast can-cer, and a greater emphasis on the role of sys-temic management therapies. It was not untilthe results of randomized trials of radicalmastectomy versus less radical surgery were re-ported and their results widely disseminatedthat it was agreed that survival following sur-gery was not improved by radical lymph noderesection.As current opinion about the role of lymph
node resection during esophagectomy is di-vided, it is likely that only well conducted pro-spective randomized trials will resolve the cur-rent controversy surrounding this question.However, as trials have not yet provided ade-quate information which can resolve this, it isimportant to closely examine outcomes follow-ing esophageal resection with and without ex-tended lymph node resection to determine thelevel of support for radical lymph node resec-tion during esophagectomy for cancer.
Proposed advantages and disadvantagesfor extended en bloc esophagectomy
The proponents of 3 field lymph node resec-tion claim improved survival following thisprocedure, as well as improved local diseasecontrol and reduced local recurrence rates,particularly in the neck. In addition, staging isfacilitated by more accurate assessment oflymph node status because more lymph nodesare removed for pathological examination,thereby providing information which may helpsome surgeons to tailor post-operative adju-vant therapies. These advantages may be offsetby disadvantages associated with more exten-sive dissection. The upper mediastinal andneck dissection requires the identification andremoval of nodes around both recurrent laryn-geal nerves, maneuvers which increase the riskof transient or permanent damage to thesenerves. Of particular concern is the potentialfor bilateral nerve palsies which can compro-mise airway protection mechanisms and the
ability to cough, as well as cause breathing dif-ficulties if both vocal cords cannot be ab-ducted. This might be expected to lead to pro-longed assisted ventilation following surgery insome patients, and possibly an increased re-quirement for tracheostomy. In addition, thereis the potential for a higher rate of post-opera-tive pneumonia and adult respiratory distresssyndrome associated with this procedure.Operating times are lengthened significantly
due to the increased complexity of the surgery,and the suitability of the approach in Westernpatients who are often larger and heavier thanJapanese patients has been questioned. The lat-ter issue, however, has been partly resolved byAltorki and Skinner [4], who reported an ex-perience with 30 American patients who un-derwent extended en bloc esophagectomy withacceptable results, thus confirming it’s feasibil-ity in the non-Japanese.
Results of standard esophagectomy
Before considering the possible advantages forextended lymphadenectomy during esophagec-tomy, it is necessary to review outcomes fol-lowing esophagectomy using less radicaltechniques. Standard esophagectomy involvesesophageal resection without formal en bloclymph node dissection. Variants of thisapproach are commonly performed world-wide. In our own experience the majority ofpatients die from disseminated disease follow-ing esophagectomy, rather than lymph noderecurrence. Hence, we have applied neoadju-vant preoperative combination chemotherapy/radiotherapy with the less radical surgicalapproach (usually a standard Ivor-Lewis proce-dure). The results of this approach for SCC ofthe esophagus at our hospital have been re-cently reported [5]. Despite a liberal selectionpolicy, in which advanced preoperative stagealone was rarely considered to be a contraindi-cation to resection, an overall 7-year survivalof 27% was achieved from an experience of 53patients. In addition, a subgroup of 14 patientswho were down staged to T0 N0 by neo-adju-vant preoperative treatment achieved a 69%7-year survival rate. These long term results
� D. I. Watson, G. G. Jamieson98

compare favorably with outcomes following ex-tended lymphadenectomy.Good outcomes have also been achieved by
other surgeons. Bolten et al. [8] reported a37% year survival rate following transhiatalblunt esophagectomy and an associated lowperioperative mortality rate of 0% in the latterhalf of their experience. Similarly Orringer[20] described a mortality rate of approxi-mately 1% with acceptable survival outcomesfrom a series of more than 1000 patients. Elliset al. [9] highlighted the influence of tumorstage at the time of presentation on the subse-quent outcome of surgery. Using a liberal se-lection policy for esophagectomy, a 19% over-all 5-year survival was achieved. However, thisimproved significantly to 37% in patients withstage I disease. A similar outcome was reportedby Watson [26] who described a 23% 5-yearoverall survival following Ivor Lewis esopha-gectomy. However, survival was much betterfor patients without cancer in lymph nodes(47% alive at 5 years) and even better if the tu-mor was confined to the esophageal wall mus-cle layer (71% alive at 5 years).A much poorer outcome has been reported
from South Africa by Mannell and Becker [18].They described a 13% 5-year survival following108 esophagectomies. However, in their series,82% of patients undergoing surgery had ad-vanced (T3) tumors, again highlighting the factthat overall outcome varies widely between dif-ferent centers, depending on whether patientstend to present with early or late stage esopha-geal cancer. This must be constantly kept inmind when comparing outcomes from uncon-trolled series of patients who have undergoneesophagectomy for cancer.
Results of 2 field (en bloc)esophagectomy
The techniques of 2 field (en bloc) esophagect-omy has been advocated as a more applicableoperation for esophageal cancer, as it entailsthe removal of the esophagus in continuitywith a margin of surrounding tissues includingdraining thoracic and abdominal lymph nodes.The proponents of the 3 field technique, how-
ever, argue that this procedure is not oncologi-cally adequate, as it fails to address cervicalnode metastases. Nevertheless it is importantto consider the results for this procedure as Ja-panese surgeons who advocate the 3 field tech-nique invariably compare their results withhistorical controls who underwent the ex-tended 2 field lymphadenectomy technique.Wong et al. described their experience with
this technique in two publications [16, 24]. Intheir experience, 52% of patients developed re-current cancer at a median follow-up intervalof 20 months. 26% developed recurrence insystemic organs, 25% within the thoracic cavi-ty, and 11% in cervical lymph nodes. In addi-tion, cervical node recurrence tended to occurconcurrently with recurrence elsewhere, and itdid not precede systemic recurrence, i.e. thepattern of recurrence did not support the con-cept of more radical surgery which includes re-section of cervical lymph nodes. Overall 5-yearsurvival was 32%.Skinner’s experience with en bloc esopha-
gectomy confirmed its relative safety. His ini-tial report in 1983 [23] was associated with a30 day operative mortality of 11%. Subsequentexperience [3] described a 30 day mortality of8%. Initial experience [23] resulted in an 18%5-year survival rate, although only 44% of theoverall esophageal cancer group underwentradical surgery. Subsequent experience [3] wasassociated with a 50% surgical explorationrate, and 33% resection rate. This highlightsthe possibility of selection bias which must beconsidered when evaluating outcomes follow-ing more radical esophagectomy procedures.Unlike the standard esophagectomy experiencewhere the majority of patients underwent astandard surgical approach, less than half ofpatients presenting with esophageal cancer arelikely to be offered en bloc esophagectomy,with patients with more advanced stage diseasemore likely to be excluded. This will improvethe outcome following the more radical proce-dure due to the effect of selecting better prog-nosis patients only for this option.Experience with 186 patients from Roder et
al. [22] who all underwent en bloc resectionwas associated with a 30 day mortality of12.4%. 61% of patients had stage T3 or T4 le-sions, and 61% also had tumor in the lymphnodes. The most important prognostic variable
12 Results of Extended en bloc Esophagectomy in Treatment of Patients with Esophageal Cancer � 99

in their experience was not lymph node in-volvement, but presence of residual tumor atthe completion of surgery. An overall 5-yearsurvival rate of 31% was achieved, althoughthis was better in patients with early stage tu-mors. Analysis of lymph node involvement ver-sus survival suggested that lymph node dissec-tion might improve prognosis if less than 20%of the nodes removed contained tumor. Moreextensive disease did not benefit.Horstmann et al. [12] compared transhiatal
with en bloc transthoracic esophagectomy in anon-randomized study of 87 patients. Hospitalmortality, as well as the incidence of post-operative pulmonary and cardiac complicationswere similar for the two groups. Anastomoticleakage was more common following transhia-tal esophagectomy (50 vs 24%). However, sur-vival similar following the two procedures at 1,2, and 3 follow-up, demonstrating no overalladvantage for more radical lymph node dissec-tion, perhaps with the exception of an im-proved ability to accurately stage the disease.Hagen et al. [11] compared two groups of pa-tients, one group of 30 patients undergoing aradical lymphadenectomy below the carinaand the other group of 16 patients undergoinga transhiatal esophagectomy (because theywere deemed medically unfit to undergo themore radical procedure). Although both groupshad similar numbers of equivalent stage dis-ease, survival was greater at 5 years in thegroup undergoing en bloc lymphadenectomy(41 vs 14%). However, apart from the non-ran-domized nature of the study, the possible, andeven likely, influence of comorbidity on thecancer was not addressed by the authors.
Results of extended 3 field esophagectomy
Three field lymphadenectomy results havebeen reported predominantly by Japanese sur-gical groups, with Western surgeons who sup-port the concept of radical lymph node dissec-tion usually confining lymph node dissectionto the thorax and abdomen. However, Skinnerand his colleagues have recently decided to fol-low the Japanese lead (see later). Consequentlythe results for this procedure are heavily
weighted by Japanese practice, which becauseof endoscopic screening programs have agreater proportion of patients presenting withearly stage disease. Western experience is char-acterized by late stage presentation, whichmakes direct comparison with the Japanese ex-perience difficult.
Case selection and peri-operativeoutcomes for 3 field esophagectomy
Most advocates of 3 field lymph node dissec-tion recommend the application of this proce-dure wherever possible. However, it is not ap-propriate for advanced tumors in which residu-al tumor is likely to be left behind despite ex-tensive lymph node resection. Furthermore,analysis of patterns of metastasis to cervicallymph nodes suggests that lymph node meta-stasis to the neck is less likely in patients withtumors involving the lowermost esophagus, inparticular the abdominal esophagus [2]. In ad-dition, superficial tumors confined to the mu-cosa and submucosa have a low risk of lym-phatic metastases. Therefore, selection of casesbest suited to 3 field lymphadenectomy hasbeen recommended [2].Short term outcomes may be affected by more
extensive lymph node dissection. Operatingtimes are generally prolonged. Kato et al. [14]describe a mean operating time of 484 minutesfor 3 field dissection compared to 331 minutesfor the two field procedure, i.e. operating timewas prolonged by approximately 2.5 hours. Sim-ilar outcomes were reported by Nishihira et al.[19], 487 versus 396 minutes. Hospital stays ofapproximately 3 months are usual for these pro-cedures in Japan [15]. However, this is influ-enced by the Japanese health system which en-courages patients to remain in hospital for allpreoperative work up and postoperative adju-vant treatment, rather than only for the time re-quired to safely recover from surgery. No datafor post-operative stay following this procedureare available from Western hospitals. Neverthe-less, it is unlikely to be shorter than conven-tional experience of 2 to 3 weeks, and it maybe prolonged if complications occur more oftenthan following standard procedures.
� D. I. Watson, G. G. Jamieson100

Complications following 3 fieldesophagectomy
Isono et al. [13] collected outcome data foresophageal resections performed between 1983and 1989 in 96 Japanese institutions, 35 whichperformed 3 field and 61 performed 2 fielddissections. Whilst this is the largest overviewof outcomes following extended lymphadenect-omy, the data must be interpreted cautiously asthe authors obtained their results from a postalsurvey of Japanese hospitals, and the responserate was only 45%. Whilst post-operative pneu-monia was equally common following 3 fieldesophagectomy compared to two field dissec-tion (18.1 vs 16.6 %), the incidence of recur-rent laryngeal nerve injury was increased by 3field dissection; 20.3 versus 14.0%. This shouldalso be compared to the standard Ivor Lewistechnique during which the risk of this injuryis nearly 0% [10]. Additional morbidity canoccur due to phrenic nerve injury and a highrequirement for tracheostomy. A 13% inci-dence of phrenic nerve injury, 56% incidenceof recurrent laryngeal nerve injury, and 53%requirement for tracheostomy was recently re-ported by Nishihira et al. [19]. Similarly Bhan-sali and Fujita et al. [6] describe an incidenceof recurrent laryngeal nerve injury of 74% (ofwhich 34% of patients overall had a permanentparesis), an anastomotic leak rate of 34%, anda 33% incidence of pneumonia.Perioperative mortality in the Japanese ex-
perience with 3 field esophagectomy is prob-ably similar to other esophagectomy tech-niques. Isono et al. [13] described a 30 daymortality rate of 2.8% from data collected bypostal survey from 1.791 3 field esophagectomyprocedures. Akiyama et al. [1] report a 2.2%30 day mortality rate. Importantly, the hospitaldeath rate was 2.5 times higher than this(5.2%), demonstrating how 30 day mortalityrates can provide misleading informationabout the real mortality risk patients facewhen they undergo esophagectomy. Initial re-sults have been reported from North Americaby Altorki and Skinner [3] who describe a 30day mortality rate of 3.3%. This suggests thatthe relative safety of extended lymphadenec-tomy demonstrated by Japanese experience can
be replicated in selected Western patients, butof course the experience does not establish thenecessity for the radicality.
Lymph node metastases to the cervicalnodes found by 3 field lymphadenectomy
Isono et al. [13] reported an incidence of cer-vical nodal metastases following cervical nodedissection of 42% for upper thoracic esopha-geal cancer, 28% for middle thoracic esopha-geal cancer, and 11% when the tumor was lo-cated in the abdominal esophagus. Metastaseswere more likely as the T stage of the esopha-geal tumor advanced. Similar outcomes weredescribed by Akiyama et al. [1], with cervicallymph node metastases present in 46% of pa-tients with upper esophageal cancer, 29% withmiddle esophageal cancer, and 27% for loweresophageal cancer. Altorki and Skinner [3]report single field involvement for the cervicallymph nodes alone in 7% of procedures.Whilst the incidence of cervical node metasta-ses is unequivocal, the important questions tobe answered are: does removal of cervicalnodes improve prognosis, and is involvementof cervical nodes really just a marker for ‘in-curable’ disease?
Survival following esophagectomy
Survival data for 3 field esophagectomy hasbeen drawn principally from uncontrolleddata. This data must be treated with caution assurvival can be influenced by tumor stage dif-ferences between different series, and possibleselection bias due to selection of potentiallycurable patients for the extended lymphade-nectomy procedure. These factors may contrib-ute to some of the good survival data reportedin various case series. In addition it is difficultto directly compare series of different proce-dures as staging is more accurate following 3-field dissection, up-staging patients withlymph node metastases which would not have
12 Results of Extended en bloc Esophagectomy in Treatment of Patients with Esophageal Cancer � 101

been detected if a less radical lymph node dis-section had been performed. This phenomenoncan lead to improved outcomes following 3field dissection in both early and late stagegroups. The outcome of the early stage groupis improved by removing patients’ otherwiseoccult lymph node metastases from the group,and the outcome of the late stage group is im-proved by the addition of the patients with theoccult lymph node metastases. Late stagegroups of patients having less radical proce-dures will contain a larger proportion of pa-tients with gross macroscopic nodal disease.The sub-group with occult lymph node meta-stases may have a better survival outcome thanpatients with gross lymph node involvement. Itis possible that this effect accounts for at leastpart of the survival improvement seen in eachstage following extended lymph node resec-tion. In the group, as a whole however, overallprognosis should not be altered by the effectof restaging, unless different selection criteriafor surgery are applied for the different opera-tive procedures.Isono et al. [13] describe a 34% year sur-
vival rate following extended lymph node dis-ssection. Similarly Bhansali and Fujita [6] de-scribed 39% survival at 5 years following ex-tended lymphadenectomy in 90 patients. Thesesurvival figures are reasonably consistent. Thesurvival data should also be considered along-side good results reported by surgeons per-forming less radical procedures. For exampleOrringer et al. [21] reported a 27% 5-year sur-vival following transhiatal esophagectomywithout radical lymph node dissection, andour own experience with less radical surgerycombined with adjuvant preoperative chemo-therapy and radiotherapy was associated withan overall 27% 7-year survival [5]. Theseresults might appear to be associated with a10% reduction in survival. However, they wereachieved following surgery in patients havingadvanced disease. When one compares out-come following extended lymphadenectomywith 2 field esophagectomy, most surgeonshave relied on historical controls to providecomparative data. Isono et al. [13] describe animprovement in 5-year survival from 27 to35%. Akiyama et al. [1] reported an evengreater improvement from 38.3 to 55%. Inter-estingly Akiyama et al. achieved a better 5-year
survival following 2 field esophagectomy thanthe survival following extended 3 field lympha-denectomy reported by Isono et al., suggestingthat the two groups of patients were different.
Randomized trials of extended 3 fieldesophagectomy versus 2 field en blocesophagectomy
Comparison of new procedures with historicalexperience can result in significant bias in fa-vor of newer techniques. This issue has beenelegantly highlighted by Bhansali and Patil etal. [6], who compared outcomes for esophagealcarcinoma following adjuvant chemotherapy.They demonstated that the benefits of adjuvantchemotherapy demonstrated in studies whichused historical controls disappeared when datawas re-analyzed after correcting for the year ofentry into their study. They concluded that his-torical controls are unreliable for studies thatseek to detect modest treatment benefits. Po-tential advantages for 3 field lymph node dis-section are of a similar order of magnitude tothose advocated for adjuvant chemotherapy,highlighting the importance of randomizedtrials to assess extended lymph node dissec-tion.Two randomized trials have been reported.
Kato et al. [15] entered 150 patients with tho-racic esophageal carcinoma into a comparativestudy of esophagectomy with 2 field versus 3field lymph node resection. This group repre-sented less than half of the patients presentingto their institution with esophageal carcinoma,and approximately 60% of all esophagectomies.Only patients with “good surgical status”, i.e.predominantly earlier stage tumors, were en-tered. Patients were randomly allocated to oneof two groups of surgeons. One group per-formed a 2 field procedure for the duration ofthe trial, and the other a 3 field procedure.This trial should be commended for enrollingan appropriate number of patients to enable avalid comparison between the two techniques.However, because different surgeons performedthe different procedures, two variables werecompared, i.e. the type of procedure and theskill of the surgeon. The study groups were
� D. I. Watson, G. G. Jamieson102

generally comparable, although the average ageof patients undergoing 3 field resection was 4years less than for the 2 field procedure (60.5vs 64.5 years). The number of lymph nodesdissected was greater in the extended lymphnode dissection group (69 vs 36), and 26% ofpatients had tumors in the cervical lymphnodes when these were dissected. Operatingtime was prolonged from 379 to 483 minutesby cervical lymph node dissection, and post-operative hospital stay was approximately 3months for both groups.No significant differences in the incidence of
complications were demonstrated between the2 groups, with vocal cord paralysis occurringin 11 (14%) of patients undergoing extendedlymph node dissection versus 15 (21%) follow-ing 2 field dissection. Anastomotic leakage washigher in the 3 field group: 34% versus 23%.Hospital mortality was 2.6% (1 patient) in the3 field group as compared with 12.3% (9 pa-tients) in the 2 field group. this difference washighly significant (P=0.008, Fisher’s exact test)and raised the problem of the study design ofthis trial as clearly there is no a priori reasonwhy the 3 field lymphadenectomy should besafer than the 2 field techniques. Post-operativesurvival rates favored 3 field extended lymphnode resection, with 49% of patients alive 5years after 3 field resection versus 34% follow-ing 2 field resection. These survival rates,when compared with Western series indicatethe early pathological stage in the Japanese se-ries. The authors concluded that extended 3field dissection resulted in improved 5-yearsurvival following esophagectomy of thoracicesophageal carcinoma. However, the 13% sur-vival advantage for the extended lymph nodedissection was largely due to the 10% differ-ences in the operative mortality rates. Whenpatients who survived surgery are considered,then the survival advantage is no longer signif-icant.More recently Nishihira et al. [19] reported
the outcome of a smaller randomized trial of 3field versus 2 field lymphadenectomy duringesophagectomy. 73 patients, 28% of the overallesophageal cancer caseload were entered intothe trial and 11 (15%) were withdrawn afterbeing randomized, leaving the study withgroups of 32 and 30 patients. Whilst not spe-cifically stated in their paper, one can probably
assume that the same surgeons performed sur-gery in both study groups. Post-operativelymost patients received either adjuvant radio-therapy or combination treatment with che-motherapy and radiotherapy. Both groups weredemographically similar, and most patientshad middle third SCC’s. The vast majoritywere T2 stage lesions, with more advancedcancers comprising only a small part of thetrial.Mean operating times were 487 versus 396
minutes, and the mean number of lymphnodes resected was 82 versus 43. Interestinglyin this study only one patient in the 3 fieldlymphadenectomy group actually had metasta-ses to the cervical nodes. Pathological exami-nation in all other patients demonstrated nocervical lymph node involvement. Postopera-tive pulmonary complications were similar forthe 2 procedures, although recurrent laryngealnerve palsy (56 vs 30%), phrenic nerve palsy(13 vs 0%) and the need for tracheostomy (53vs 10%) all occurred more frequently following3 field lymphadenectomy. Anastomotic leakage,however, was less common following the moreextensive procedure (6 vs 20%). In hospitalmortality was 3% (1 patient) following 3 fielddissection and 7% (2 patients) following 2 fielddissection. There was a trend to improved sur-vival following 3 field lymphadenectomy,although the survival difference was not signif-icant (P=0.19). At 5 years, the survival was66% following 3 field lymphadenectomy ascompared with 48% following 2 field lympha-denectomy. However, it is unclear from the re-port whether follow-up was complete for allpatients, or whether the survival data was cal-culated by actuarial analysis.The results of these trials allow us to con-
clude that 3 field lymphadenectomy is asso-ciated with a higher risk of complications suchas injury to the recurrent laryngeal nerves,and phrenic nerve, and operation times aresignificantly lengthened. However, peri-opera-tive mortality is not increased when this pro-cedure is performed by experienced Japanesesurgeons. The trials have only addressed thisprocedure for patients with early stage squa-mous cell carcinomas (i.e. not invadingthrough the full thickness of the esophagealwall muscle), and a significant improvement inlong term survival has yet to be demonstrated.
12 Results of Extended en bloc Esophagectomy in Treatment of Patients with Esophageal Cancer � 103

However, it is unlikely that the results of thesestudies can be extrapolated to Western experi-ence, as the majority of patients undergoingsurgery outside Japan have advanced tumorswhich penetrate the full thickness of the eso-phageal wall. In recent years the majority ofpatients presenting with esophageal carcinomain the West have an adenocarcinoma involvingthe lower third of the esophagus and/or thegastroesophageal junction. Extended lympha-denectomy in the latter group of patients hasbeen largely untested.
Use of 3 field en bloc esophagectomyfor adenocarcinoma of the esophagus
The application of this procedure for adenocar-cinoma has only been reported in the study ofAltorki and Skinner [3] of 30 patients under-going 3 field lymphadenectomy. Fifteen of theirpatients had adenocarcinoma of the distal eso-phagus. Interestingly, 4 of these patients hadcervical nodal metastases, although each ofthese 4 patients also had metastases in othernodal groups. The number of patients in thisstudy is not sufficient to allow us to draw con-clusions about the role of 3 field lymphade-nectomy for adenocarcinoma of the distal eso-phagus.
Conclusions
The role of 3 field lymphadenectomy remainscontroversial outside of Japan. Whilst good re-sults have been reported from many Japaneseinstitutions, data has been largely uncontrolledor compared to historical controls limiting theconclusions which can be drawn from thesestudies. Nevertheless, the relative safety of theprocedure has now been demonstrated in bothJapanese and Western experience. However, theprocedure is associated with significant mor-bidity, including a high incidence of perma-nent recurrent laryngeal nerve and phrenicnerve injury, as well as possibly higher anasto-motic leakage rates and a greater requirement
for assisted ventilation and tracheostomy fol-lowing the more radical procedure. Theseproblems may be acceptable if a long term out-come benefit can be demonstrated. For now,however, only data from well conducted pro-spective randomized trials is likely to convincethe majority of surgeons that extended lym-phadenectomy is beneficial. The 2 trials re-ported to date either had numbers too small todraw significant conclusions or were difficultto interpret because of potential problems as-sociated with the randomization process usedduring the trial.So far there is a lack of comparative data
between 3 field lymphadenectomy and con-ventional resection combined with adjuvantchemotherapy and radiotherapy. These adju-vant approaches have achieved similar out-comes to radical surgery in uncontrolled trials.As patients usually die with distant metastasesfollowing esophagectomy, in the future it seemsmore likely that improvements in outcome foresophageal cancer will be achieved by im-provements in systemic therapies rather thanthrough the development of progressively moreradical surgical techniques.
References
1. Akiyama H, Tsurumaru M, Udgawa H, Kajiyama Y(1994) Radical lymph node dissection for cancer ofthe thoracic esophagus. Ann Surg 220:364–373
2. Akiyama H, Tsurumaru M, Udgawa H, Kajiyama Y(1997) Esophageal cancer. Curr Probs in Surg 10:765–834
3. Altorki NK, Girardi L, Skinner DB (1994) Squamouscell carcinoma of the esophagus: therapeutic dilem-ma. World J Surg 18:308–311
4. Altorki NK, Skinner DB (1997) Occult cervical nodalmetastases in esophageal cancer: preliminary resultsof 3-field lymphadenectomy. J Thorac CardiovascSurg 113:540–544
5. Bessell JR, Devitt PG, Gill PG, Goyal S, JamiessonGG (1996) Prolonged survival follows resection ofesophageal SCC downstaged by prior chemoradio-therapy. Aust NZ J Surg 66:214–217
6. Bhansali MS, Fujita H, Kakegawa T, Yamana H, OnoT, Hikita S, Toh Y, Fujii T, Tou U, Shirouzu K (1997)Pattern of recurrence after extended radical esopha-gectomy with 3-field lymph node dissection forsquamous cell carcinoma in the thoracic esophagus.World J Surg 21:275–281
� D. I. Watson, G. G. Jamieson104

7. Bhansali MS, Patil PK, Badwe RA, Havaldar R,Desai PB (1997) Historical control bias: adjuvantchemotherapy in esophageal cancer. Dis Esoph10:51–54
8. Bolton JS, Ochsner JL, Abdoh AA (1994) Surgicalmanagement of esophageal cancer. A decade ofchange. Ann Surg 219:475–480
9. Ellis FH, Gibb SP, Watkins E (1985) Overview ofthe current management of carcinoma of the eso-phagus and cardia. Can J Surg 28:493–496
10. Goldmine M, Maddern GJ, LePrise W, Meunier B,Campion JP, Launois B (1993) Esophagectomy by atranshiatal approach or thoracotomy: a prospectiverandomised trial. Br J Surg 80:367–370
11. Hagen JA, Peters JH, DeMeester TR (1993) Superi-ority of extended en bloc esophagectomy for carci-noma of the lower esophagus and cardia. J ThorCardiovasc Surg 106:850–859
12. Horstmann O, Verreet PR, Becker H, Ohmann C,Roher H-D (1995) Transhiatal esophagectomy com-pared with transthoracic resection and systemiclymphadenectomy for the treatment of esophagealcancer. Eur J Surg 161:557–567
13. Isono K, Sato H, Nakayama K (1991) Results of anationwide study on the 3-field lymph node dis-section of esophageal cancer. Oncology 48:411–420
14. Kato H, Tachimori Y, Watanabe H, Kikuchi S,Umemura A (1996) Recurrent disease after esopha-gectomy with 3-field lymph node dissection forthoracic esophageal carcinoma. In: Peraccia A, Ro-sati R, Bonavina L, Bona S, Chella B (eds) RecentAdvances in Diseases of the Esophagus. MonduzziEditore, Bologna, Italy, pp 405–410
15. Kato H, Watanabe H, Tachimori Y, Iizuka T (1991)Evaluation of neck lymph node dissection forthoracic esophageal carcinoma. Ann Thor Surg 51:931–935
16. Law SYK, Fok M, Wong J (1996) Pattern of recur-rence after resection for cancer: clinical implica-tions. Br J Surg 83:107–111
17. Logan A (1963) The surgical treatment of carcino-ma of the esophagus and cardia. J Cardiovasc Surg46:150–163
18. Mannell A, Becker PJ (1991) Evaluation of the re-sults of esophagectomy for esophageal cancer. Br JSurg 78:36–40
19. Nishihira T, Hirayama K, Mori S (1998) A prospec-tive randomized trial of extended cervical andsuperior mediastinal lymphadenectomy for carci-noma of the thoracic esophagus. Am J Surg 175:47–51
20. Orringer MB (1997) Editorial on Occult cervicalnodal metastases in esophageal cancer: prelimi-nary results of 3-field lymphadenectomy. J ThoracCardiovasc Surg 113:538–539
21. Orringer MB, Marshall B, Stirling MC (1993)Transhiatal esophagectomy for benign and malig-nant disease. J Thorac Cardiovasc Surg 105:265–276
22. Roder JD, Busch R, Stein HJ, Fink U, Siewert JR(1994) Ratio of invaded to removed lymph nodesas a predictor of survival in squamous cell carci-noma of the esophagus. Br J Surg 81:410–413
23. Skinner DB (1983) En bloc resection for neo-plasms of the esophagus and cardia. J CardiovascSurg 85:59–71
24. Tam PC, Cheung HC, Ma L, Siu KF, Wong J (1987)Local recurrences after subtotal esophagectomy forsquamous cell carcinoma. Ann Surg 205:189–194
25. Walsh TN, Noonan N, Hollywood D, Kelly A, Keel-ing, Hennessy TP (1996) A comparison of multi-modal therapy and surgery for esophageal adeno-carcinoma. N Engl J Med 335:462–467
26. Watson A (1994) Operable esophageal cancer: Re-sults from the West. World J Surg 18:361–366
12 Results of Extended en bloc Esophagectomy in Treatment of Patients with Esophageal Cancer � 105

Surgical Techniques

Blunt transhiatal esophagectomyand substitution by gastric tube
� Indications
– Adenocarcinoma localized distal to thetracheal bifurcation
– Squamous cell carcinoma or severe dys-plasia localized distal to the tracheal bi-furcation
– Primarily palliative resection– Extensive stricture* (stenosis) due to ero-sion (chemical burns) unresponsive tononsurgical treatment including bougie-nage
– Extensive peptic stricture* (stenosis)– Relapse of megaesophagus* after surgicalrepair of cardiospasm combined withpeptic strictures and failure of dilatation
– Extensive benign esophageal tumors*– Extensive intraluminal injury with per-foration* (one- or two-stage procedure)
� Contraindications
– Florid duodenal ulcer– Gastric stricture due to erosion(chemical burns)
– Status post distal gastrectomy or other op-erations in the epigastric region with in-complete gastroepiploic vascular anatomy
– Irreversible cardio-respiratory disorders
� Operative risk and patient information
– High morbidity (~40%) and mortality(~5%)
– Prolonged monitoring in intensive careunit due to pulmonary complications
– Pulmonary complications(ARDS, pneumonia)
– Injury to recurrent laryngeal nerve uni-or bilateral
– Horner’s syndrome– Injury to phrenic nerve with diaphrag-matic paralysis
– Necrosis of the gastric tube– Injury to arteries of the gastric tube in-traoperatively followed by immediate co-lon interposition
– Dehiscence of cervical suture line– Mediastinitis– Pancreatitis– Peritonitis– Pleural empyema– Intraoperative emergency thoracotomy– Tracheobronchial fistula
Blunt Transhiatal Subtotal Esophagectomywith Gastroplasty and Cervical AnastomosisE.F. Yekebas, A.F. Chernousov, D.C. Broering, P.M. Bogopolski, C.F. Eisenberger,
A. Kutup, J.R. Izbicki
13
* These indications do not need a lymphadenectomy(see chapter 10)

� Specific preoperative management
Preoperative investigations (staging) include:– Esophagogastroduodenoscopy incl. histo-logic diagnosis
– CT scanning of the thorax and abdomen– Abdominal sonography– Esophageal endosonography– Bronchoscopy if the tumor is localized inthe mid-third
– Pulmonary function tests and blood gasanalysis
– Echocardiography– Ergometry and other cardiac investiga-tions if necessary
One day prior to the operation the esophagusand intestinal washout should be performed bymeans of orthograde irrigations with e.g. 3–4liters cleansing solutions. Electrolyte, clotting,and hemoglobin imbalances (depletion) shouldbe corrected preoperatively. Breathing exercisesand physiotherapy must be explained andshould be started preoperatively.
� Anesthesia. Endotracheal intubation. Postop-eratively, thoracic-epidural anesthesia is appro-priate. Perioperative antibiotic therapy 30 minprior to operation.
� Technique
� Positioning. Supine position with hyperlordo-sis and bending of the lower thoracic spine.Abduction of the right arm. Adduction of
the left arm. The head is turned to the rightand slightly extended. This results in exposureof the cervical esophagus for performing theneck anastomosis.
� Approach. Upper transverse incision withmedian T-shaped extension (inverted T-inci-sion) for best overall view of the epigastric re-gion, especially the diaphragmatic esophagealhiatus. Alternatively upper midline laparotomywith left periumbilical incision.
� E. F. Yekebas et al.110
Fig. 13.1. Approach and positioning. The patient is placed insupine position with spinal hyperlordosis for better exposureof the epigastric region.

� Operative procedure
– Laparotomy and inspection of the stom-ach, distal esophagus, liver, and regionallymph nodes. Mobilization of left laterallobe of the liver.
– Preparation and mobilization of the stom-ach with epigastric lymphadenectomy in-cluding paraaortic lymphatic tissue.
– Mobilization of abdominal portion of theesophagus and sagittal incision of theesophageal hiatus.
– Transhiatal esophageal dissection in theposterior mediastinum including paraaor-tic lymphadenectomy.
– Construction of a gastric tube.– Mobilization and dissection of cervicalesophagus. Resection of the esophagus.
– Transposition of the gastric tube throughthe anterior/posterior mediastinal tunnelafter mobilization of the duodenum (ex-tensive Kocher maneuver) and performingthe cervical anastomosis.
� Special instruments. Performing the invertedT-shape incision, insertion of Rochard retrac-tors is useful to elevate the costal margin. Dur-ing mobilization of the esophagus in the poste-rior mediastinum the use of very long Mikuliczretractors has been proved to be very worth-while.
� Special technique. Example: Resection of car-cinoma of distal third of the thoracic esopha-gus.
13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 111
Fig. 13.2. Upper transverse laparotomy with median exten-sion (inverted T-shaped incision).

� E. F. Yekebas et al.112
Fig. 13.3. Placement of Rochard self-retaining retractor system for exposureof the epigastric region. Alternativelyuse of the Sial retraction system.
Fig. 13.4. Mobilization of the left lateral liver lobe for opti-mal visualization of the diaphragmatic esophageal hiatus.Transection of the left triangular ligament with diathermy. To
prevent injury of adjacent structures, a pack is placed overthe stomach.

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 113
Fig. 13.5. To prevent the risk of a bile leak from an irregularbile duct, the tip of the left triangular ligament must beoversewn with a suture ligation.

� Mobilization of the duodenum by an extensive
Kocher maneuver. This maneuver is always nec-essary in case of a very small stomach to allowa tension free gastric tube transposition to the
neck. In the situation of a normal anatomy, atension free gastric tube transposition to theneck is also possible without mobilization ofthe duodenum.
� E. F. Yekebas et al.114
Fig. 13.6. Mobilization of the duodenum by the Kochermaneuver. While the duodenum is being retracted medially,the peritoneum is incised close to the border of the duode-num. 1 Duodenum; 2 Peritoneum.
Fig. 13.7. Blunt dissection of the avascular plane betweenthe duodenum, the head of the pancreas, and the retroperi-toneal vessels until the anterior wall of the inferior venacava is exposed. 1 Duodenum; 2 Peritoneum; 3 retroperito-neal vessels.
1
2
1
2
3

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 115
1
2
3
Fig. 13.8. Skeletonization of the greater curvature is com-menced from below, care being taken to spare the left andright gastro-epiploic vessels up to the level of the splenichilum. Moderate traction on the transverse colon and coun-tertraction at the stomach results in proper exposure of thegastrocolic ligament. The skeletonization of the gastrocolicligament should be performed away from the greater curva-
ture, thus avoiding any possible damage to the gastroepi-ploic vessels. 1 A. and V. gastroepiploica dextra; 2 Lig. gas-trocolicum; 3 Colon transversum. Alternatively the skeletoni-zation of the gastric tube can be performed using an auto-matic clip-applicator and cutter (multifire). Direction right toleft and afterwards left to right.

� E. F. Yekebas et al.116
Fig. 13.9. Skeletonization of the greater curvature iscontinued towards the spleen. For preservation ofthe blood supply, the dissection must be performedwell away from the stomach wall. Next the left gas-troepiploic artery is transected directly at its originat the splenic artery. In this way, an existing anasto-mosis between the left and right gastroepiploic ar-teries will be preserved, thus ensuring that the bloodsupply of the upper part of the gastric tube is main-tained. 1 Gastrosplenic lig.; 2 splenic artery; 3 leftgastroepiploic vessels; 4 phrenicocolic lig.
Fig. 13.10. a Lymphadenectomy in the area of the hepato-duodenal ligament. 1 Portal vein; 2 A. hepatica propria;3 bile duct; 4 Lymphatic tissue.
a
1
2
3
4
1
2
3
4

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 117
Fig. 13.10. b Dissection of the lymph nodes of thehepatic artery up to the celiac trunk, of the portalvein as well as the lymphatic tissue around the com-mon bile duct is removed. c Division of the gastro-duodenal artery. 1 A. gastrica dextra.
1
b
c

� E. F. Yekebas et al.118
Fig. 13.11a–c. Dissection of flaccidal part of the lesseromentum. The cranial part of the hepatogastric ligament(hepatoesophageal lig.) is tunneled with the finger and dis-sected from the diaphragm with electrocautery. Check for an
existing relevant accessory left hepatic liver artery whichshould be preserved. 1 Hepatoesophageal lig.; 2 accessoryleft hepatic artery.
a
1
2

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 119
Fig. 13.11b
Fig. 13.11 c

� E. F. Yekebas et al.120
Fig. 13.12. a After transection and ligature of short gastricvessels, the greater curvature can be positioned cranially andanteriorly, the parietal peritoneum is incised at the upperpancreatic margin. b Transection of left gastric vein is donebetween suture ligations. c, d In case the left gastric veinruns behind the left gastric artery, attention is focused
not to ensure this structure during the dissection of the leftgastric artery.All lymph nodes along the left gastric artery, the splenic ar-tery, the common hepatic artery, the celiac trunk, and para-aortic lymph nodes are removed. This phase of the operationends with the ligation of the left gastric artery.
a
b

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 121
Fig. 13.12 c
Fig. 13.12d

In case of a blunt transhiatal esophageal dis-section for benign reasons, lymphadenectomyshould be omitted.
� E. F. Yekebas et al.122
Fig. 13.13. After lymphadenectomy of the celiac trunk,splenic artery, and common hepatic artery, the lymphatic dis-section is continued along the celiac trunk to the paraaorticregion. Lymphatic tissue thus remains adherent en bloc withthe lesser curvature and is later resected en bloc with thetumor. For better exposure of the esophageal hiatus and the
paraaortic region, the diaphragmatic crura are incised withdiathermia and the stumps are ligated (see belowFig. 13.15). 1 Left diaphragmatic crus; 2 Left gastric artery;3 Lymph nodes; 4 Splenic artery; 5 Hepatic artery; 6 Celiactrunk; 7 Incision of the right diaphragmatic crus (interuptedline on both sides).
1
2
3
4
7
6
5

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 123
Fig. 13.14. Sharp transection of the phrenicoesophageal li-gament at the margin of the esophageal hiatus. This step isfacilitated by transection to the cardia caudally with an ab-dominal pad. Thus the diaphragmatic crura become exposed
to the left and right side of the esophagus. Next, transectionand ligature of the gastrophrenic ligament between clampsat the esophagogastric angle of His is undertaken.

� E. F. Yekebas et al.124
Fig. 13.15. Blunt mobilization of the esophagus with the in-dex finger. During this maneuver connective tissue fibers be-tween esophagus, diaphragmatic crus, and abdominal aortamust be removed carefully. The esophagus is armed with arubber tube using a curved clamp.

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 125
1
2
Fig. 13.16. The abdominal esophagus is mobilized and cau-dal traction is applied with the rubber tube. Identification ofanterior and posterior vagus nerve. 1 Vagus nerve withbranches; 2 paraaortic and paraceliac lymphatic tissue.

� E. F. Yekebas et al.126
1
2
Fig. 13.17. For a better exposure of the distal esophagus, itis incised up to the inferior left phrenic vein with scissors ordiathermy. Continuous traction should be applied during thispart of the procedure. 1 Phrenic vein; 2 Diaphragm.

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 127
a
b
Fig. 13.18a, b. The esophagus is mobilized anteriorly byblunt dissection of the plane. The fingers are used to sepa-rate the diaphragm and pericardium from the esophagus.

� E. F. Yekebas et al.128
Fig. 13.19a, b. Transection of the leftinferior phrenic vein is suture ligatedand transected and the diaphragm isincised up to the central portion. Expo-sure of the pericardium. Insertion ofMikulicz retractors, which are pulledupward to the left and to the right.
a
b

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 129
Fig. 13.20. Dissection of the distal esophagus starts withsharp dissection of the anteriorly esophageal surface fromthe pericardium. As a rule the dissection can be continuedanteriorly under vision up to the tracheal bifurcation withtwo fingers initially and finally using the whole hand.
Injury to the pleural cavity should be avoided. Above thetracheal bifurcation the dissection is done bluntly with twofingers, with the dissection plane directly along the esopha-gus. The trachea and the brachiocephalic trunk are palpableanteriorly.

� E. F. Yekebas et al.130
Fig. 13.21. Now we have reached the most critical stage ofthe procedure where complications can be lethal. If extensivelocal tumor growth has not been recognized during preoper-ative investigations, serious damage of the pars membrana-cea of the trachea, the azygos vein, the pulmonary vessels,or the aorta is possible. Extensive involvement of lymphatictissue makes the blunt dissection more difficult, and also
makes complications more likely. In the same way mobiliza-tion of the region posterior to the esophagus including para-esophageal lymphatic tissue from aorta and prevertebral fas-cia up to the tracheal bifurcation is done sharply and undervision. Above the tracheal bifurcation the dissection is con-tinued bluntly using digital dissection and staying close tothe esophageal wall.

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 131
Fig. 13.22. Great care must be taken to avoid damage tothe lateral esophageal wall and the parietal pleura. Aftercomplete anterior and posterior mobilization, the esophagusis pulled caudally. This causes the lateral ligament like struc-tures to tighten. These so called lateral esophageal ligamentsconsisting of branches of the vagal nerves, pulmonary liga-
ments and esophageal branches should be transected sharplybetween clamps. Alternatively clips can be used for this step.The left lobe of the liver is moved to the right using Mikuliczretractors. Strong retraction of the esophagus to the leftusing a rubber tape facilitates transection of the right lateralesophageal ligament. 1 Right lateral esophageal ligament.
1

� E. F. Yekebas et al.132
Fig. 13.23. a Dissection of the left lateral esophageal wallincluding all lymph nodes and surrounding tissue is carriedout under direct vision. This step should be performed usingmediastinal retractors. For better exposure optimal light fromceiling lights or from lights directly attached to the mediasti-nal retractors should be used. b The left lateral esophagealligament should be ligated carefully. During this step it is im-portant to proceed close to the aorta and under direct divi-sion. This ensures that all esophageal branches from the des-
cending aorta are divided without bleeding. It is importantto ligate the left lateral esophageal ligament very carefully atthe level of the eighth vertebral body (T8), since the largestesophageal branches of the aorta originate from there. Anybleeding from esophageal branches is controlled by suture li-gation close to the aorta using resorbable or nonresorbablemonofilament suture. 1 Pericardium; 2 left esophageal liga-ment; 3 mediastinal pleura.
1
2
3

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 133
Fig. 13.23b

� E. F. Yekebas et al.134
Fig. 13.24. In case of suspected pericardial infiltration, theadherent portion of the pericardium should be resected enbloc. 1 Pericardium; 2 pericardial resection margin.
1
2

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 135
Fig. 13.25. In case of tumor infiltration of the parietal pleura,the adherent part should be excised with a clear margin. Thesame applies for tumor infiltration of the mediastinal pleura
and lung. The diaphragmatic incision is enlarged and an en-bloc resection of the adherent lung segment using either aclamp resection or a linear stapler is performed.

� E. F. Yekebas et al.136
Fig. 13.26a, b. Ligation and dissection of the lateral liga-ment under direct vision up to a point directly proximal tothe tracheal bifurcation. This step includes lymphadenectomyof the posterior mediastinum. 1 Light retractor; 2 Lymphnodes.
a
1

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 137
Fig. 13.26b
2

� E. F. Yekebas et al.138
Fig. 13.27. After blunt dissection of the esophagus up tothe thoracic inlet, pack gauze into the posterior mediasti-num. This provides excellent hemostasis. In cases of scarringresulting from caustic burns, when multiple dilations with abougie or even perforation may have occurred, the blunt dis-
section of the esophagus may prove impossible. In thesecases sharp dissection of the esophagus under direct visionshould be performed. Preparation close to the esophagealwall is mandatory to avoid injury of the adjacent structures.

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 139
Fig. 13.28a, b. There is no special order for the gastric liga-ture – starting with the left gastric artery is possible. Theblood supply of the gastric tube after preparation is exclu-
sively provided by the right gastroepiploic artery. 1 Esopha-gus; 2 trachea; 3 superior vena cava; 4 azygos vein; 5 rightbronchus; 6 pericardium; 7 diaphragm.
a b
1
2
3
5
6
7
4

� E. F. Yekebas et al.140
Fig. 13.29. Insert alternative: Transhiatal blunt esophagealdissection. Formation of the gastric tube. In case of a smallstomach the first step in constructing an isoperistaltic gastrictube is to perform a transverse incision of the antrum 2.5–3.5 cm proximal to the pylorus. The incision starts at the
lesser curvature and is made for a distance of about half ofthe antral diameter. By doing the incision longitudinally a 3–4 cm elongation of gastric tube, which sometimes has apoor blood supply, can be resected if necessary during theperformance of the cervical anastomosis.
Fig. 13.30. Insert alternative: Transhiatal blunt esophagealdissection. Formation of a gastric tube. Stretch the transverseantrotomy and close longitudinally using a two-layer inter-
rupted suture. The optimal diameter of the gastric tube is2.5–3 cm. Gastric tubes with a greater or lesser diametermay be associated with ischemia of the gastric wall.

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 141
Fig. 13.31. Formation of an isoperistaltic gastric tube startsat the fundus. It follows the direction of the pylorus and ismost easily performed with a stapler. The longer the staplerthe less steps are needed. During the use of the stapler it isimportant to stretch the stomach longitudinally to avoid
shortening of the gastric tube caused by the stapler. Toavoid gaps between the staple lines place the next staplerexactly behind the previous row of staples. 1 Gastroepiploicvessels.
1

� E. F. Yekebas et al.142
Fig. 13.32. A seromuscular suture is placed between tworows of staples to avoid leakage. Leave sutures long to keepthe gastric tube stretched. Invert the stapled sutures byusing seromuscular interrupted sutures. As mentioned above,
the diameter of the gastric tube should be 2.5–3 cm afterinversion of the stapled sutures. The sutures at the top ofthe gastric tube are left long for the transthoracic transposi-tion performed later on.

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 143
Fig. 13.33. A pylorotomy is necessary only when the wholestomach is used to avoid gastric outlet obstruction. By usingthe described procedure resulting in a gastric tube, a pyloro-tomy is not necessary.

� E. F. Yekebas et al.144
Fig. 13.34. Cervical stage. For better exposition of the opera-tive field, the patient is placed with an extended neck andhead turned to the right. Oblique incision of the skin extendingfrom the jugular notch to the level of the thyroid cartilagealong the anterior rim of the sternocleidomastoid muscle.
Fig. 13.35. Cervical stage. Sharp dissection of the subcuta-neous fatty tissue and the platysma muscle along the ante-rior rim of the sternocleidomastoid muscle.
Fig. 13.36. Cervical stage. Blunt dissection of the space be-tween the straight muscles and the sternocleidomastoidmuscle. Retract the sternocleidomastoid muscle laterally.Sharp transection of the omohyoid muscle exposes thelateral edge of the thyroid, the jugular vein, and the carotidartery, when the straight muscles are pulled medially.The straight muscles may be transected in case of insufficientexposure of the esophagus. 1 Omohyoid muscle; 2 sterno-cleidomastoid muscle.
1
2

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 145
Fig. 13.37. Transection of the median venter of the sterno-cleidomastoid muscle near the clavicle with electrocauteryfor a better exposure.
Fig. 13.38. Blunt dissection of the layer between the thyroidand the carotid sheath. Insertion of retractors for exposure ofthe left recurrent laryngeal nerve and inferior thyroid arteryby retracting the thyroid medially and the neurovascularbundle laterally. Identification of the left laryngeal recurrentnerve in the tracheoesophageal groove. Medial retraction ofthe trachea together with the recurrent laryngeal nerve andpartial blunt and sharp dissection of the cervical esophagus.1 Recurrent laryngeal nerve.
1

� E. F. Yekebas et al.146
Fig. 13.39. 1 Superficial fascia of the neck; 2 prevertebralfascia; 3 pretracheal fascia; 4 omohyoid muscle; 5 sternoclei-domastoid muscle; 6 platysma muscle; 7 neurovascular bun-dle; 8 sternohyoid muscle; 9 sternothyroid muscle.
12
3
5
6
7
4
8
9
Fig. 13.40a

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 147
Fig. 13.40a–c. The cervical esophagus is dissected withcurved instrument (right angle clamp) and armed with arubber tube. Completion of the dissection of the cervicalesophagus and upper thoracic esophagus by blunt dissectionwith the finger or dissector (c). Careful protection of the re-current laryngeal nerve is mandatory. After removal of thenaso-gastric tube, the esophagus is divided with a stapler(b) or with scissors (a), after ligation of the aboral part ofthe esophagus has been ligated (a). A strong thread or arubber band is fixed to the aboral stump of the esophagusbefore the esophagus is transposed into the abdominal cavi-ty. This facilitates easy transposition of the gastric tube tothe neck later on.
Fig. 13.40b
Fig. 13.40 c

� E. F. Yekebas et al.148
Fig. 13.41a–c. Options for a gastric pull-up. The above men-tioned formation of the gastric tube is useful for all forms ofreconstruction because it provides sufficient length of the tube.
a Gastric tube pull-up in the original esophageal bed.b Retrosternal gastric tube pull-up.c Presternal gastric pull-up.
Fig. 13.42. The gastric tube is pulled up in the original eso-phageal bed into the cervical position and is fixed to theadjacent cervical tissue by 6 interrupted sutures. In this waythe anastomosis is walled off from the posterior mediastinum
in order to prevent mediastinitis. Dislocation of the anasto-mosis into an intrathoracic position is prevented. The firststitches are placed in the prevertebral fascia.
a b c

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 149
Fig. 13.43. Finally the gastric tube is fixed to the fasciaand to the muscles of the caudal part of the wound.
Fig. 13.44. Esophagogastrostomy can be performed as aone-layer or two-layer anastomosis. Two seromuscular suturesare placed, and the protruding parts of the gastric tube andthe esophagus are resected. We prefer a full thickness extra-mucosal interrupted suture technique. The stitches should be9–10 mm from the edge of the esophagus and the gastrictube, respectively. The knots should be just tight enough tobring them snugly into contact with the tissue. The sutures
always tighten later from the postoperative edema which oc-curs in the area of the anastomosis. After completion of theposterior wall a naso-gastric tube is inserted through theanastomosis and into the duodenum. The esophageal stumpshould not be longer than 2.0–2.5 cm. Thus, blood supply isimproved reducing the probability of anastomotic leakage. Inaddition this means that the operation is more radical incases of malignancy.
Posterior wall Anterior wall
Esophagus
Stomach

� E. F. Yekebas et al.150
Fig. 13.45a–d. Technique of the two-layer anastomosis ofthe gastric tube and the esophageal stump. The first sero-muscular suture-line is performed in an interrupted fashion(a). Resection of the protruding parts of the esophagus andthe gastric tube using electrocautery (b). The second innersuture of the posterior wall has to be done strictly extra-
mucosally and can be performed as an interrupted or arunning suture (c). Having finished the posterior wall a naso-gastric tube is inserted over the anastomosis and into theduodenum (d). The naso-gastric feeding tube should not beremoved before the 5th postoperative day.
a b
c d
5 mm

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 151
Fig. 13.46a, b. Two-layer technique of the neck anastomosisbetween the gastric tube and the esophageal stump. The in-ner suture of the anterior wall is performed using inter-rupted sutures to prevent postoperative stenosis. The secondsuture of the anterior wall is performed in a U-shaped fash-
ion (a). The transverse suture is done at the esophagus. Ty-ing of the knots after all three U-shaped sutures are placed.This guarantees an inversion of the anastomosis into thegastric tube (b).
Fig. 13.47. Figure of the completedesophagogastrostomy.
a b

� E. F. Yekebas et al.152
Fig. 13.48a,b. Technique of pharyngogastrostomy in case ofcomplete extirpation of the esophagus. The pharynx istrimmed diagonally through the piriform fossa (a). A one-layer anastomosis should be performed. All interrupted su-
tures at the posterior wall are first placed and then tied con-secutively (b). After insertion of the naso-gastric tube com-pletion of the anastomosis of the anteriorly wall is underta-ken using the same technique.
Fig. 13.49. Alternative methods of neck anastomosis between the gastrictube and the esophagus. Anastomosis using an end to end stapler.
Fig. 13.50. Situation after havingcompleted pharyngogastrostomy.
a b

13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 153
Fig. 13.51. One penrose drain is placed be-side the cervical anastomosis (a). The woundis closed with cursory platysma sutures andskin closure (b). The mediastinum is drainedtransabdominally with two drains (c), addi-tionally drains are placed in the right and leftsubphrenic space. A chest tube is used if thepleural cavity has been opened accidentally.
a
b c

� E. F. Yekebas et al.154
Fig. 13.52. Alternative methods of neck anastomosis be-tween the gastric tube and the esophagus. Anastomosisusing an end-to-side stapler.

Complications of transhiatal bluntesophageal dissection and gastric pull-up
� Intraoperative complications
� Injury of mediastinal visceral pleura. Duringblunt esophageal dissection injury of the medi-astinal visceral pleura with opening of the pleu-ral cavity is a frequent event. In these cases pos-terior basal drainage with chest tube is neces-sary to prevent a pneumothorax or pleural effu-sion arising which might lead to postponingearly extubation.
� Hemorrhage from esophageal branches of the
aorta. Slipped ligatures or retracted vesselstumps are the main causes of mediastinalhemorrhage from esophageal branches of theaorta. Bleeding from these branches can be re-solved with sutures using a non-absorbablemonofilament suture. If exact localization ofthe bleeding is not possible tamponade of themediastinum with dry sponges or gauze isindicated. If the bleeding continues, a rightthoracotomy has to be performed to stop thehemorrhage.
� Laceration of the thoracic duct. If the thoracicduct has been damaged then ligation should beperformed both above and below the damagedarea. To avoid this complication, preparationand ligation of the lateral esophageal ligamentsshould be performed under direct vision.
� Injury of the azygos vein. During blunt dis-section of the esophagus injury of this vein ispossible. If sudden hypotension caused by loss
of intravascular volume occurs during this op-erative step this complication has to be kept inmind. Mostly the blood loss is realized first bythe anesthesiologist, because a considerablebleeding into the right thoracic cavity is pos-sible before bleeding is recognized by the sur-geon in the mediastinum. Injury to the azygosvein should be anticipated when the tumor islocated in the middle third of the esophagusand with locally advanced and/or metastaticlymph node involvement close to the azygosvein. Transmediastinal dissection of the veinfollowed for ligation under direct vision shouldbe undertaken to stop the bleeding. Time con-suming trials of direct transhiatal dissectionshould be avoided if direct access cannot beachieved. In these cases tamponade of the pos-terior mediastinum is indicated and hemosta-sis is then achieved via a right anterolateralthoracotomy through the 5th intercostal space.To avoid hemorrhage in cases of a close re-
lation between the tumor and the azygos vein,ligation of the azygos vein should be per-formed before blunt dissection is carried out.If not possible then a thoracic approach shouldbe undertaken.
� Injury of the aorta. This severe complicationusually is only a potential problem in caseswhere there is a tumor infiltration of the aorta.If there is a suspicion that tumor infiltration ofthe aorta has occurred, then a right thoraco-tomy is performed and the tumor is excised enbloc with an aortic cuff. Transhiatal sharp dis-section of the esophagus from the esophagealbed is undertaken in cases where the tumorgrowth has occurred adjacent to the aorta.
13 Blunt Transhiatal Subtotal Esophagectomy with Gastroplasty and Cervical Anastomosis � 155

Indications
– Short distance peptic stenosis of the distalesophagus
– Boerhaave syndrome– Short distance ruptures of the distal eso-phagus
– Carcinoma of the esophageal-gastric junc-tion with tumor extension above the dia-phragm
– Squamous cell carcinoma of the distalesophagus.
� Contraindications, operative risksand patient information
See chapter 13.
� Specific preoperative management
� Anesthesia. Orotracheal intubation with adouble-lumen tube for single lung ventilation.
� Patient’s position
– Supine position with intraoperative rear-rangement on the left side
– Alternatively 45� spiral-positioning is pos-sible, in this case intraoperative changesof the position are not necessary.
� Surgical approach. Upper transverse incisionwith median T-shaped extension for the ab-dominal part.Anterolateral thoracotomy through 5th ICR
for the thoracic part.
� Operative procedure
The most frequent techniques of reconstruc-tion after partial abdominothoracic esophagec-tomy with intrathoracic anastomosis by gastricpull-up. For carcinoma of the esophageal junc-tion, preparation and construction of the gas-tric tube should be performed following theoncological radical excision (Fig. 14.1 a). Incase of benign diseases, e.g. strictures, a radi-cal oncological construction of the gastric tubeshould be avoided (Fig. 14.1b).In benign disease the abdominal and distal-
thoracic esophagus is mobilized after diaphrag-motomy. Then transection of the esophagusabove the tumor in the pericardial area using asurgical stapler. The oral end is fixated andmarked using strong sutures (Fig. 14.2 a, b).The greater omentum is divided along the
great curvature of the stomach respecting theright gastroepiploic artery and vein. The stom-ach is mobilized gradually. According to therequired length of the gastric tube and dignityof the lesion, transection of the left gastric ar-tery and the short gastric veins is necessary.The required length of the gastric tube is sig-nificantly shorter for an intrathoracic anasto-mosis than for cervical anastomosis. Thereusually is no need for Kocher’s maneuver.After completion of the lymphadenectomy
in carcinomatous disease, the sutures whichwere left long for serosa suture of the surgicalstaples at the proximal end of the gastric tubewill be tied with the long suture at the distalesophageal end (Fig. 14.5).After drainage of the left subphrenic area
and epigastric region, which is the major loca-tion of lymphadenectomy, the abdomen isclosed.
Partial Abdominothoracic Resectionof the Esophagus with Gastroplastyand Intrathoracic AnastomosisA.F. Chernousov, A. Kutup, P.M. Bogopolski, D.C. Broering
14

� A. F. Chernousov et al.158
a
b
Fig. 14.1. a Oncological extent; b extent in benign diseases.

14 Partial Abdominothoracic Resection of the Esophagus with Gastroplasty and Intrathoracic Anastomosis � 159
Fig. 14.2. a Transection of theesophagus with a stapler device;b fixation of the oral and of theesophagus with strong sutures.
a
b

� A. F. Chernousov et al.160
Fig. 14.3. Skeletonization of the greater curvature (see Fig. 13.8).

The patient is positioned to the left for thethoracic part of surgery by turning the table(initially helical-positioning of the patient with45� elevation of the right thorax and elevatedarm).The optimal access regarding the overall
view is the right anterolateral thoracotomy inthe fifth intercostal space. The gastric tube willbe placed into the pleural cavity by traction onthe distal esophagus. It follows the en bloc-re-section of the thoracic esophagus includingmediastinal pleura, the periesophageal fat tis-sue, and the mediastinal lymph nodes. It isrecommended to ligate all adhesions with thesurrounding tissue. The esophagus will be di-vided as cranial as possible (interrupted line)(Fig. 14.6).The diameter of the esophagus is clearly
smaller than that of the gastric tube if not pre-stenotically dilated. This incongruence of the
lumens can be equalized using a conic reduc-tion plastic of the proximal gastric tube (Fig.14.7).After incomplete transverse incision and di-
agonally aboral completion of division of thegastric tube at the oral end, the 2.5–3 cm longdiagonal incision will be closed using extramu-cous simple interrupted stitches (Vicryl/Dex-on/PDS 3/0). Length and angle of the diagonalincision determine the resulting diameter ofthe lumen (Figs. 14.8, 14.9).This procedure simplifies the inserting of
the esophageal end into the gastric tube andcreates a staple-free zone for anastomosis.If the intestinal walls of the esophagus and
gastric tube are strong, a double rowed anasto-mosis should be performed.In case of a very thin esophageal wall, a sin-
gle rowed all-layer anastomosis of esophaguswith the gastric tube is favored.
14 Partial Abdominothoracic Resection of the Esophagus with Gastroplasty and Intrathoracic Anastomosis � 161
Fig. 14.4. Skeletonization of the greater curvature (see Fig. 13.9).

Extramucous placed simple interrupted su-tures should be laid out loosely in the poste-rior anastomotic area. The risk of anastomoticstenosis is higher in the running suture tech-nique. If all posterior wall sutures are placed,they are tied gradually avoiding strong tissuetension. A slightly adaptation should beachieved, squeezing should be avoided.The single rowed anastomosis is covered
with mediastinal pleura to secure the suturesand lessen the tension at the esophagogastros-tomy, and consecutively the rate of insuffi-ciency (Fig. 14.10).The lesser curvature of the stomach will be
not resected if there are strictures of the distalesophagus or the esophagogastric region.Therefore, the entire stomach can be used for
pull-up. As blood supply of cardia and distalparts of the fundus are insecure, both shouldbe resected (Fig. 14.11 a, b).The esophagus is being anastomosed with
the anterior stomach wall in double row suturetechnique. The esophagus is fixated initiallywith the gastric tube using six seromusculoussutures. After incision of the gastric tube withthe electrocautery the posterior wall is anasto-mosed with extramucous all-layer sutures insimple interrupted stitching technique. Thedistance between the sutures should be 5 mm(Fig. 14.12 a, b). A naso-gastric feeding tube isgenerally inserted over the anastomosis andplaced into the duodenum for decompressionand postoperative enteral feeding.
� A. F. Chernousov et al.162
Fig. 14.5. Connecting the proximal end ofthe gastric tube with the distal esophagealend before closure the abdomen.

14 Partial Abdominothoracic Resection of the Esophagus with Gastroplasty and Intrathoracic Anastomosis � 163
Fig. 14.6. Transection of the esophagus as cranial as possi-ble (interrupted line).
Fig. 14.7. Conic reduction plastic of the proximal gastrictube to equalize incongruences.

� A. F. Chernousov et al.164
Fig. 14.8. Length and angle of the diagonal incision deter-mine the diameter of the lumen.
Fig. 14.9. Extramucous placed simple interrupted sutures.
�2.5–3 cm
�

After completion of the anterior wall anasto-mosis using the same technique as for the pos-terior wall, the anastomosis should be invertedtelescopically by placing seromuscular U-su-tures grasping the mediastinal pleura (Fig.14.13 a). The tie of the U-suture should cometo lie in the area of the gastric tube, as the ser-osa of the stomach gives the knots morestrength. The base of the U-suture should bepositioned 1.5 cm proximal to the anastomosis(Fig. 14.13b). The distance between the suturesshould be 6 mm (Fig. 14.13 a).After completion of the esophagogastros-
tomy, the anastomosis is inserted into thestomach telescopically (Fig. 14.14). Drainagetubes are placed into the mediastinum. Thesupraphrenic region is drained by a furtherdrainage tube.Alternatively the anastomosis can be made
transthoracically or transhiatally using a circu-lar stapler.Introduction of the stapler into the gastric
tube and perforation of the wall at the pro-spective site of the anastomosis with the pike.Removal of the pike and connection with theanvil. Firing of the instrument. Check for com-pleteness of the anastomotic rings. Removalof the stapler and closure of the gastric tubewith extramucous all-layer sutures (Fig. 14.15).
14 Partial Abdominothoracic Resection of the Esophagus with Gastroplasty and Intrathoracic Anastomosis � 165
Fig. 14.10. Mediastinal pleura to secure the anastomosis.

� A. F. Chernousov et al.166
Fig. 14.11. a The entire stomach is used for pull-up.b Extent of the resection (interrupted line).
a
b

14 Partial Abdominothoracic Resection of the Esophagus with Gastroplasty and Intrathoracic Anastomosis � 167
Fig. 14.12. a Fixation of the gastric tube with six seromus-culous sutures; b the posterior wall is anastomosed. The dis-tance between the sutures should be 5 mm.
a
b
5mm

� A. F. Chernousov et al.168
b
1,5 cm
6 mm
a
Fig. 14.13. a Inversion of the anastomosis with mediastinalpleura (U-sutures) (distance 6 mm); b Positioning of the U-sutures (1,5 cm proximal to the anastomosis).

14 Partial Abdominothoracic Resection of the Esophagus with Gastroplasty and Intrathoracic Anastomosis � 169
Fig. 14.14. Telescopically inserted esophagogastrostomy. Fig. 14.15. Introduction of the stapler.Final situation before fixing.

� Indication
– Mid thoracic esophageal carcinoma– Esophageal squamous-cell carcinomain the lower third of the esophagus
– Long peptic stricture, if transhiatalresection is not possible.
� Contraindication
– Severe cardio-pulmonary insufficiency.
� Risks and patient’s informed consent
– Refer to chapter 13 blunt dissection. Ad-ditionally, the patient should be informedabout bilateral pareses of the recurrentlaryngeal nerve, pareses of the phrenicnerve, and chylothorax.
� Special preoperative preparations
Anesthesia: Orotracheal intubation with a dou-ble-lumen tube for single lung ventilation.
� Patient’s position
– Position of the patient on his left side forthe thoracal part of surgery
– Supine position, comparable to blunttranshiatal dissection
– Alternatively 45� positioning is possible,in this case intraoperative changes of theposition are not necessary.
� Surgical approach
– Anterolateral thoracotomy through 5th ICR– Transverse laparotomy with cranial med-ian enlargement (inversed T-incision).
� Operative procedure
1. Right-sided anterolateral thoracotomythrough 5th ICR
2. Incision of the mediastinal pleura along thehilum of the right lung and the superiorcaval vein
3. Dissection and ligation of the azygos vein4. Preparation of the vena cava by resection ofthe accompanying adipose and lymphatictissue
5. Dissection of the vagus nerve distal to therecurrent laryngeal nerve
6. Dissection of intercostal veins, sparing thearteries
7. Dissection between esophagus, aorta, andtrachea and resection of paratracheal, para-bronchial, paracarinal, and infracarinallymph nodes
8. Thoracic drainage and closure of the thora-cotomy
9. Abdominal and cervical part(see chapter 13).
Abdominothoracic Subtotal en blocEsophagectomy and Reconstructionwith Gastric Tube TranspositionJ.R. Izbicki, D.C. Broering, P. Kaudel, A. Kutup, E.F. Yekebas
15
Fig. 15.1. Left-sided positioning of the patient with thoracickinking. Skin incision from the apex of the scapula in thesubmammarian fold in the 5th ICR.

� J. R. Izbicki et al.172
Fig. 15.2. After thoracotomy in 5th ICR, two retractors areplaced to spread the incision and to retract the ribs. Singleleft lung ventilation. Incision of the mediastinal pleura alongthe marked line for the en bloc esophagectomy. It startsfrom the pulmonary ligament, runs along the dorsal part ofthe right hilum of the lung to the lateral margin of the
superior caval vein up to the upper thoracic aperture. Inci-sion direction is changed to the right lateral margin of thespine, down to the diaphragm along the azygos vein. Themost important part of this step is the recognition of theright recurrent laryngeal nerve and the right phrenic nerve.

15 Abdominothoracic Subtotal en bloc Esophagectomy and Reconstruction with Gastric Tube Transposition � 173
Fig. 15.3. The first step is the incision of the pulmonary li-gament. For exposition of the pulmonary ligament the sur-geon’s left hand pushes the lung cranially and laterally. Thelymphatic tissue of the pulmonary ligament should be dis-
sected towards the esophagus. The cranial margin of thepulmonary ligament – the veins of the lower lobe of theright lung – should not be injured during this procedure.
Fig. 15.4. Dissection of the junction of the azygos vein andsuperior caval vein with a right angle clamp. Double sutureligation of the vein adjacent to the caval vein.

� J. R. Izbicki et al.174
Fig. 15.5. The lymphadenectomy starts from the superiorvena cava upwards to the confluence of the two V. anon-yma. Preparation of the origin of the recurrent laryngealnerve from the vagus nerve. Caudal to its origin the vagus
nerve is severed and pushed towards the en bloc specimen.The lymphadenectomy is performed along the dorsal wall ofthe superior caval vein.

15 Abdominothoracic Subtotal en bloc Esophagectomy and Reconstruction with Gastric Tube Transposition � 175
Fig. 15.6. After complete preparation of the superior cavalvein, the trachea and the right- and left-sided main bronchusshould be exposed from lymphatic tissue. The paratracheally
situated fat and lymphatic tissue is dissected towards theesophagus by sharp dissection or electrocautery and later re-sected en bloc with the esophagus.

� J. R. Izbicki et al.176
Fig. 15.7. Dissection of the retrotracheal lymph nodes. Theyshould be dissected towards the esophagus. Care has to betaken to avoid injury to the membranaceous part of the tra-chea.

15 Abdominothoracic Subtotal en bloc Esophagectomy and Reconstruction with Gastric Tube Transposition � 177
Fig. 15.8. Dissection of the cranial paraesophageal lymph nodes.

� J. R. Izbicki et al.178
Fig. 15.9a,b. Dissection and ligation of all intercostalveins, which drain into the azygos vein for en bloc resec-tion with the azygos vein. Lymphadenectomy of the sub-carinal lymph nodes (a): For a better exposition of thisarea the esophagus should be held aside with a sponge(b): Alternatively the esophagus can be held with rubberbands.
a
b

15 Abdominothoracic Subtotal en bloc Esophagectomy and Reconstruction with Gastric Tube Transposition � 179
Fig. 15.10. Paraaortic lymphadenectomy. With continuoustraction on the esophagus the paraaortic lymphadenectomycan be performed. The esophageal branches of the thoracicaorta have to be dissected very carefully and should be li-gated with suture ligation.

180
Fig. 15.11. Transection of the thoracic duct with double ligations caudal to the tracheal bifurcationand directly above the diaphragm.
Fig. 15.12. Completion of the mediastinal lymphadenectomywith removal of the left sided paraaortic and retropericardiallymph nodes down to the esophageal hiatus. After complet-ed mobilization of the en bloc esophageal specimen, thoracic
drains are placed in the right thoracic cavity. The thoracic in-cision is closed and the patient‘s position is changed for theabdominal part to a supine position.
� J. R. Izbicki et al.: 15 Abdominothoracic Subtotal en bloc Esophagectomy and Reconstruction with Gastric Tube Transposition

The use of the stomach is still the preferredsubstitute for the esophagus requiring only theanastomosis to reestablish food passage.Furthermore the gastric substitute acquiresspontaneous propulsive contractility and is as-sociated with good long-term functional re-sults. In Western populations, tubular transfor-mation of the stomach following lesser curva-ture resection, as described by Akiyama occa-sionally results in a short gastric tube withperfusion deficiencies at the cranial part of thetube.Gastric tube formation utilizing the gastric
fundus and maintaining the arterial arcadealong the lesser gastric curvature results in alonger and better perfused gastric tube.
� Anesthesia. A combination between regionalanesthesia and balanced intravenous and inha-lation anesthesia is used. Epidural anesthesiaat the level of TH 5–7 reduces perioperativeopioid application and postoperative pain.
� Positioning. For transhiatal esophagectomies,the patient is placed in a supine position withan 80� abduction of both arms. The head isflexed to the right side, to gain access to thecervical esophagus.For a thoraco-abdominal approach, patients
are placed in a spiral position with rotation ofthe torso to the left and abduction of the rightarm. The head is flexed to the right side togain access to the cervical esophagus.
� Incision. An upper median laparotomy withextension to the left of the xyphoid is used togain access to the abdominal portion of theesophagus and the stomach (Fig. 16.1). The ab-dominal cavity is kept open by two retractors(three in obese patients) (Fig. 16.2).
� Gastric mobilization. The first step in gastricmobilization is dissection of the greater omen-tum. The dissection is performed at a 3–4 cmdistance from the greater curvature to avoidinjury to the gastroepiploic arteries and theextramural connections between the right andleft gastroepiploic arteries.
Fundus Rotation GastroplastyM.K. Schilling, M.W. Buechler
16
Fig. 16.1. Approach; upper mid-line incision.

The short gastric arteries are divided closeto the spleen to avoid injury to the gastricwall.In a second step the lesser omentum is dis-
sected close to the liver. Care is taken not tosevere accessory left hepatic arteries from theceliac trunk or the left gastric artery. Thestomach is dissected and the gastroesophagealjunction is divided with a TA stapler.After gastric mobilization, the stomach is
placed on warm packs (Fig. 16.3).
� Fundus rotation gastroplasty. For oncologicalprocedures, all connective, adipose, and lym-phoid tissue is carefully dissected from the leftgastric artery. The left gastric artery and theconcomitant vein are ligated close to thestomach.
� M. Schilling, M.W. Buechler182
Fig. 16.2. Open cavity with inserted retractors. Fig. 16.3. Mobilized stomach on warm packs.
Fig. 16.4. Skeletonization starting at the proximal small cur-vature.

The gastric tube is formed by stepwisestapling along the gastric fundus with a linearstapler as depicted in Figures 16.4 and 16.5.Careful traction is applied to the edges with Allisclamps (Fig. 16.6). The stapler line is invertedwith 4/0 interrupted absorbable sutures.Gastric tube formed by the fundus rotation
gastroplasty technique are usually long enough
to perform tension-free anastomosis even withthe mid pharynx.The vascular supply of the tube in its distal
part consists of direct vessels running from theleft gastroepiploic artery, and the more oralpart of the tube is supplied by an intramuralvascular plexus, fed by the gastric and gastro-epiploic arterial arcade.
16 Fundus Rotation Gastroplasty � 183
Fig. 16.5. Last steps of the fundus rotation gastroplasty. Fig. 16.6. Completed fundus rotation gastroplasty.

� Indications
Indications for this surgical procedure are rare.– Carcinoma of the cardia in the abdominalesophagus (below the diaphragm) in pati-ents with high comorbidity
– Long strictures of the abdominal esopha-gus.
� Contraindication
Severe cardiopulmonary insufficiency.
� Risks and patient’s informed consent
See chapter 13.
� Special preoperative preparation
See chapter 13.
� Patient position and surgical incision
See chapter 13.
� Operative procedure
1. Mobilization of the abdominal part of theesophagus
2. Sagittal diaphragmotomy3. Truncal vagotomy4. Mobilization of the stomach with preserva-tion of the right gastric omental vein andartery
5. Extensive lymphadenectomy in the area of thehepatic artery, splenic artery, celiac trunk,and paraaortal
6. Optional: splenectomy in patients with sus-picious lymph nodes
7. Tube reconstruction using the distal stom-ach
8. Intrathoracic esophagogastrostomy.
Proximal Gastrectomywith Distal Esophagectomy (Proximal Resection)A.F. Chernousov, O. Zehler, P.M. Bogopolski, D.C. Broering, H.W. Schreiber�
17

� A. F. Chernousov et al.186
Fig. 17.1. Mobilization of the stomach and the distal eso-phagus, resection lines during the procedure of proximal gas-trectomy, and distal esophagectomy.
Fig. 17.2. Technique of blunt dissection of the esophagus atthe diaphragm. After incision of the peritoneum on bothsides of the esophagus, the forefinger of the right hand isbluntly inserted behind the esophagus. The esophagus andthe vagal nerves are mobilized stepwise.
Fig. 17.3. The left lobe of the liv-er is dissected by the incision ofthe left triangular ligament. Thediaphragm is retracted to theright side. Sagittal incision of thediaphragm is performed after su-ture ligation of the diaphragmaticvein. The retropericardial and intra-abdominal esophagus is mobilized.Slight traction is applied to theesophagus to the left and caudally.The vagal nerves are transected.

17 Proximal Gastrectomy with Distal Esophagectomy (Proximal Resection) � 187
Fig. 17.4. Anatomy of the lesser omentum in cross-section.1 Greater omentum; 2 celiac trunk; 3 pancreas; 4 superiormesenteric artery; 5 duodenum; 6 transverse colon.
Fig. 17.5. During the mobilization of thegreater curvature, the greater omentumwith the anterior peritoneal aspect of thecolon is dissected. Lymphadenectomy inthe area of the middle colic vessels.
1
2
3
4
5
6

� A. F. Chernousov et al.188
Fig. 17.6. The fat and lymphatic tissue alongthe lower pancreatic edge is removed. Theperitoneum covering the body and the tail ofthe pancreas is dissected. The peritoneum ofthe frontal surface of the pancreas is pre-served.
Fig. 17.7. In cases with enlarged pathologiclymph nodes at the hilar region of the spleen,en bloc splenectomy is indicated. Care shouldbe taken to avoid any damage to the pan-creatic tail. Dissection of the splenic arteryand vein.

17 Proximal Gastrectomy with Distal Esophagectomy (Proximal Resection) � 189
Fig. 17.8. Transection of the splenicvessels between clamps. The vessels aresuture-ligated separately. The fatty tissuearound the pancreatic tail is resectedwith the spleen.
Fig. 17.9. The splenic artery is freedfrom the surrounding lymphatic tissue tothe pancreatic head. Lymphadenectomyis completed along the left gastric ar-tery, celiac trunk, and in the paraaorticarea.

� A. F. Chernousov et al.190
Fig. 17.10. Fat tissue and lymph nodes along the commonhepatic artery, hepatic artery, portal vein, and the bile ductis resected. The right gastric artery is dissected and ligatedclose to the hepatic artery.

17 Proximal Gastrectomy with Distal Esophagectomy (Proximal Resection) � 191
Fig. 17.11. Peritoneal incision line for the Kocher maneuver.
Fig. 17.12. After completion of the Kocher maneuver theretropancreatic, paracaval, and right paraaortic lymphade-nectomy may be performed. The dorsal surface of the pan-
creatic head, the caval vein, the renal vein and the aorta arecompletely dissected. 1 Right renal vein; 2 right renal artery;3 right ovarian or spermatic vein.
1
2
3

� A. F. Chernousov et al.192
Fig. 17.13. A supraradically lymphadenectomy encompassesthe continuation of the paracaval and paraaortal lymphade-nectomy caudally to the bifurcation of the aorta. All lymph
nodes along the caval vein, the aorta, and the renal vein areremoved (compartment-3 resection). 1 Superior mesentericartery; 2 inferior mesenteric artery.
1
2

17 Proximal Gastrectomy with Distal Esophagectomy (Proximal Resection) � 193
Fig. 17.14. Completion of the extensive lymphadenectomyin compartment 3. Dissection of the pancreatic corpus andtail. The remaining fatty tissue and lymph nodes along thesuperior mesenteric artery, the abdominal aorta, the left
renal artery, and suprarenal arteries are removed. 1 Splenicvein; 2 left suprarenal gland; 3 left suprarenal vein; 4 left re-nal vein; 5 superior mesenteric artery.
1
2
3
4
5

� A. F. Chernousov et al.194
Fig. 17.15. Preparation of a distal stomach tube.
Fig. 17.16. Preparation of the distal stomach tube is per-formed in the same way as in the description of the bluntdissection excluding the transverse antrotomy. The esophagushas to be resected with at least 5 cm tumor-free esophagealmargin. After resection of the stomach including the tumor,a right-angle clamp is placed at the esophagus. The eso-phagus is incised. The anastomosis starts at the backsideof termino-terminal esophagogastrostomy with extramucosal
all layer stitches in a single stitch technique. First, all stitchesare armed with clamps and are then tied after completion ofthe dorsal wall. The distance between the single stitches is5 mm. The external stitch is performed 1 cm from the edgeof the anastomosis. After tying the sutures are cut. The cor-ner stitches are not cut and ventral wall of the anastomosisis sewn in the same way.
5 mm
1 cm

17 Proximal Gastrectomy with Distal Esophagectomy (Proximal Resection) � 195
Fig. 17.17. The sutures of the dorsal wall are finished andtied (a). A naso-gastric tube is to be placed beyond the ana-stomosis (b). Finally, the ventral part of the anastomosis isperformed.
a b

� A. F. Chernousov et al.196
Fig. 17.18. The dorsal and ventral suture line is doubled byusing sero-muscular U-stitches. The distance between thesestitches is 5 mm. The sutures should be 1 cm from the ana-stomosis (a). During tying of the knots, the index finger may
be helpful inverting the anastomosis. Principle of the anti-refluxive esophagogastrostomy (b). If the esophageal wall isvery thin, the esophagogastrostomy should be performed ina single row anastomosis.
a b
1 cm
0.5 cm

17 Proximal Gastrectomy with Distal Esophagectomy (Proximal Resection) � 197
Fig. 17.19. Alternatively, the esophagogastrostomy may beperformed using a circular stapler. The transverse gastros-tomy for the introduction of the stapler is closed using alllayer sutures. The stapled anastomosis is inverted as de-scribed above.

� Indications
– Adenocarcinoma of the distal esophaguswith involvement of the proximal stomach
– Locally advanced carcinoma of the cardia– Adenocarcinoma of the proximal stomachwith infiltration of the distal esophagus.
� Contraindications
– Active duodenal ulcer– Severe cardiopulmonary insufficiency.
� Risks and informed consent
– See chapter 13– Necrosis of the colon– Risk of pancreatitis and injury of thespleen.
� Special preoperative preparations
� Anesthesia, patient position and surgical inci-
sion. See chapter 13.Laparotomy is performed as demonstrated
in chapter 13 by transverse abdominal incisionextended by an upper abdominal midline inci-sion (inverse T-incision). After mobilization ofthe left lateral liver lobe and dissection of thelesser sac close to the liver, the greater omen-tum is detached from the transverse colon.Lymphadenectomy begins at the basis of theright gastroepiploic vessels.
Transhiatal EsophagogastrectomyJ.R. Izbicki, D.C. Broering, A. Kutup, E.F. Yekebas
18

� J. R. Izbicki et al.200
Fig. 18.1. Incision of the peritonealsheath above the right gastroepi-ploic vessels. The right epiploic ves-sels are suture ligated as close aspossible to the pancreas without in-juring the pancreatic capsule.
Fig. 18.2. Dissection of the sur-rounding lymph nodes is performed.For better exposure of these nodes,the stomach is held upwards usingventral traction. The lymph nodes atthe upper margin of the pancreasare dissected towards the duodenumto facilitate the en bloc resectionlater. Injury of the serosa of theduodenum and of the capsule ofthe pancreas has to be avoided.

18 Transhiatal Esophagogastrectomy � 201
Fig. 18.3. The lymphadenectomy of the hepatoduodenal li-gament is performed as described in chapter 13. In addition,the lymph nodes around the origin of the right gastric arteryare dissected towards the stomach. The right gastric artery is
then ligated at its origin. After circular dissection of the gas-troduodenal junction, the duodenum is transsected 2–3 cmbehind the pylorus with a linear stapler device, and the sta-pler suture line is inverted with single sutures.

� J. R. Izbicki et al.202
Fig. 18.4. The upper margin of the pancreas is now exposedby applying traction upwards to the distal stomach. Lympha-denectomy continues from the hepatoduodenal ligament
along the common hepatic artery down to the celiac trunk.Lymphadenectomy at the splenic artery, the celiac trunk, andthe paraaortal space is performed as described in chapter 13.
Fig. 18.5. Traction is applied to the stomach towards theright upper abdomen to expose the origin of the left gastro-epiploic artery and the short gastric vessels. These vesselsare transsected and ligated between clamps. Mobilization of
the greater curvature of the stomach is performed up to thegastroesophageal junction. During this step the phrenicogas-tric ligament has to be transsected with electrocautery.

18 Transhiatal Esophagogastrectomy � 203
Fig. 18.6. Operative site after dissection of the stomach withcompleted lymphadenectomy at the hepatoduodenal liga-ment with exposure of the hepatic artery, the splenic artery,the celiac trunk, and the paraaortal region. The stapledsuture line of the duodenal stump is oversewn. Median inci-
sion of the diaphragm in combination with incision of bothdiaphragmatic crura allows exposure of the esophageal hia-tus. This is the first step of the transhiatal dissection of theesophagus.

� Indications
– Patients with esophageal carcinoma aftersubtotal gastrectomy
– Locally advanced carcinoma of the cardiawith infiltration of the lower esophagus
– Peptic stricture of the total esophagus, in-cluding strictures with extension to phar-ynx or stomach
– Long peptic stricture of the esophaguswith severe esophagitis and esophagealfistula
– Extensive peptic stricture of the esopha-gus in patients after subtotal gastrectomy
– Any affection of the “neo-esophagus”after transpleural esophagectomy, gastrictube reconstruction with cervical esopha-gostomy (secondary reconstruction aftergastric tube necrosis)
– Necrosis or inadequate length of the gas-tric or jejunal interposition for recon-struction.
� Contraindications
– Severe cardiopulmonary insufficiency– Pathology of the colon (e.g. carcinomas,adenomas, inflammatory bowel disease,strictures).
� Risks and informed consent
– See chapter 13– Insufficiency of the colo-colonic anasto-mosis with subsequent peritonitis
– Local ischemia with subsequent total orsubtotal necrosis of the colon, leading tototal or subtotal colon resection.
� Special preoperative preparations
– See chapter 13– Total colonoscopy– Entire orthograde bowel preparation withhyperosmolar solution. In case of dyspha-gia, application through a stomach tube isrecommended. Retrograde bowel lavageor application through a gastrostomyshould be performed in patients with totalesophageal stenosis. Patients sufferingfrom catabolic metabolism are to be sup-ported by hyperalimentation (parenteralor enteral) for several days prior to opera-tion.
� Anesthesia. See chapter 13.
� Position. The patient should be in the supineposition with hyperlordosis in the lower tho-racic spine. The left arm is fixed to the bodyallowing better access to perform the collaranastomosis. The patients head is reclined andturned to the right (Fig. 19.1).
� Surgical approach. Transverse lower abdom-inal laparotomy below the umbilicus with ex-tension as midline upper laparotomy (low in-verted T-incision). Alternatively a median lapa-rotomy from symphysis up to the xiphoid pro-cess can be performed (Fig. 19.2).
Colon Interposition after Total and SubtotalEsophagectomyJ.R. Izbicki, K. Steffani, A.F. Chernousov, P.M. Bogopolski,
D.C. Broering, H.W. Schreiber�
19

� Operative procedure
1. Mobilization of the large bowel beginning atthe cecum up to the sigmoid colon
2. Gross examination of the vascular supply ofthe colon
3. Examination of the colonic segment, intendedfor interposition for adequate length and vas-cular supply by intermittent clamping
4. Preparation of the colonic segment, which issuitable for interposition
5. Establishment of a substernal tunnel (for ret-rosternal reconstruction route). Alternativelythe posterior mediastinal route for orthotopicreconstruction is used
6. Exposure of the cervical esophagus or phar-ynx, transposition of colon interponate andperformance of the esophago-colic or phar-yngo-colic anastomosis
7. Performance of the cologastrostomy, alterna-tively anastomosis to the duodenum or jeju-num
8. Colonic anastomosis for reconstruction ofthe lower gastrointestinal tract
9. Drainage of the mediastinum, abdomen, andneck.
� J. R. Izbicki et al.206
Fig. 19.1. Perioprative positioning.
Fig. 19.2. Low inverted T-incision, or alternatively median la-parotomy.

19 Colon Interposition after Total and Subtotal Esophagectomy � 207
Fig. 19.3. Incision of the peritoneum using electrocautery orfine scissors and mobilization of the ascending colon and theright colonic flexure beginning at the cecum. The right ureterand the kidney should be preserved carefully. Care has to betaken not to injure the duodenum accidentally.1 Duodenum; 2 cecum; 3 right iliac vessels; 4 right ureter;5 right kidney.
1
23
4
5

� J. R. Izbicki et al.208
Fig. 19.4. For mobilization of the right colonic flexure,the right phrenico-colic ligament has to be divided and sutureligated.
Fig. 19.5. Mobilization of the transverse colon by sharp dis-section of the greater omentum. Preparation of the avasculartissue plane, assisted by antero-caudal traction of the trans-
verse colon (assistant) and ventro-cranial traction of theomentum and stomach, thus leaving the greater omentumat the stomach.

19 Colon Interposition after Total and Subtotal Esophagectomy � 209
Fig. 19.6. Mobilization of the sigmoid colon, which is facili-tated by performing medio-cranial traction to expose theembryonic adhesions between the colon and retroperitone-um. Further dissection between mesosigmoid and retroperi-toneal fat, taking care of the left ureter and gonadal vessels.
Fig. 19.7. The left lateral peritoneal reflection is finally mobi-lized by dissection of the peritoneum in cranial direction.The colico-splenic ligament and the phrenico-colic ligamentare ligated and divided using cautery or scissors. Thus, the
whole splenic flexure of the colon is mobilized. A prophylac-tic appendectomy after total mobilization of the colon is rec-ommended.

� J. R. Izbicki et al.210
Fig. 19.8
Fig. 19.8 and 19.9. Selection of a colonic segment suitablefor interposition. Determination of the essential length bythe following procedure: Elevation of the colon in front ofthe abdominal wall, measurement of the distance betweenthe abdomen and the angle of the mandible by a suture,fixed at the root of the strongest vessel of the colonic mes-entery (see Fig. 19.9: middle colic artery). The length of thesuture is finally transferred to the colon and the resectionmargin is marked.1 Anastomosis between the left and the middle colonic ar-tery (Riolan); 2 left colonic artery; 3 root of the middle colo-nic artery.
Fig. 19.9
1
2
3

19 Colon Interposition after Total and Subtotal Esophagectomy � 211
Fig. 19.10. Preparation of an anisoperistaltic colonic seg-ment begins with incision of the peritoneum far from thecolon and stepwise preparation of the mesocolon maintain-ing the paracolic arcades and the middle and left colic ves-sels. A vascular clamp is provisionally applied across the leftcolic artery and the sigmoid artery across the provisional co-
lonic transection plane to prove a sufficient arcade of Riolan.If no ischemia occurs after 3 minutes, the colon interpositioncan be performed.1 Middle colic artery; 2 left colic artery; 3 paracolic anasto-mosis between left colic artery and sigmoid artery.
Fig. 19.11. Construction of an anisoperistaltic colon interpo-sition. 1 Middle colonic artery; 2 superior mesenteric artery;3 inferior mesenteric artery; 4 left colonic artery; 5 sigmoidartery.
1
2
3
4
5
1
2
3

The transparent arrows show alternative linesfor transection of the colon. Resection of blu-ish margins on the right flexure of the trans-verse colon between the middle and the rightcolic artery should be performed under preser-vation of the paracolic arcades. Following thisprocedure a better mobilization of the colonicsegment can be obtained. To perform the phar-yngo-colostomy in carcinomas of the upperthird of the esophagus, a fairly long colonicsegment is required. Therefore, parts of thesigmoid colon have to be used and the first(and probably the second) sigmoid artery hasto be ligated close to the inferior mesentericartery. Prior to dissection of the vessels, aclamp is provisionally applied to prove the suf-ficiency of the vascular supply. Dark arrowspoint to the vascular resection margins. Theanastomosis between the right and middle co-
lonic artery should be preserved for a bettervascular supply of the colonic segment chosenfor interposition.
Advantages of using the left colonic segmentare the following:� the more predictably longer length and thesmaller diameter of the left colon
� adequacy of the vascular pattern due to ar-teries with bigger diameter, instead of vascu-lar supply via several arcades like in theright colon
� using an anisoperistaltic colonic segmenthas no clinical relevance, because the nutri-tional transport follows gravity.
The essential advantage of the left colon is theopportunity to obtain a longer colonic seg-ment.
� J. R. Izbicki et al.212
1
2
3
Fig. 19.12. A frequently employed alternative is a left-sidedisoperistaltic colonic interposition.The middle colonic artery is divided and the vascular supplyis through the left colonic artery, if a sufficient Riolan’s ar-cade exists.1 Superior mesenteric artery; 2 inferior mesenteric artery;3 left colonic artery.This approach ensures an isoperistaltic reconstruction. Care hasto be taken not to injure the left colic vessels. Therefore, trans-ection of the descending colon is always done without exten-sive dissection of the colon using a linear stapler device.
Fig. 19.13. An anisoperistaltic colon interposition supplied bythe left colonic artery can be performed, if the Riolan’s anasto-mosis is either not present or insufficient due to former surgicalprocedures.1 Left colonic artery.
1

19 Colon Interposition after Total and Subtotal Esophagectomy � 213
Fig. 19.14. In case of an inadequate vascular supply by theleft and middle colonic artery, reconstruction of an isoperis-taltic colon interposition supplied by the sigmoid artery ispossible.1 First sigmoid artery.
Fig. 19.15. In very rare cases no anastomosis is found be-tween the left colonic artery and the first sigmoid artery. Inthose cases the main branch of the inferior mesenteric arterycan be used as an anastomosis between the two areas ofblood supply. This can only be accomplished when the distalparts of the sigmoid colon are adequately perfused by themedial and inferior rectal artery. This has to be checked bytemporary clamping.1 Isolated segment of the inferior mesenteric artery with thebranches of the left colic artery and the sigmoid artery.
1
1

� J. R. Izbicki et al.214
Fig. 19.16. Even after right hemicolectomy (e.g. followingcomplicated right colonic interposition) construction of ananisoperistaltic interposition is possible, if the middle colonicartery has been spared during the first operation. The leftcolonic artery and the first sigmoid artery are dissected. Vas-cular supply of the interposition comes from the middle colo-nic artery. Reconstruction is performed with an ileo-sigmoid-ostomy.
Fig. 19.17. Alternatively, an interposition after right hemico-lectomy and after former transection of the middle colonicartery can be performed using the left colon. The blood sup-ply comes from the left colonic artery. The entire sigmoid co-lon is needed for the purpose of receiving sufficient lengthfor the interposition and all sigmoid arteries have to be dis-sected. The proximal colon segment with poor vascular sup-ply is resected.

19 Colon Interposition after Total and Subtotal Esophagectomy � 215
Fig. 19.18. After former surgical procedures (e.g. right co-lectomy) with transection of the middle colonic artery andpresence of a small left colonic artery, a strong arcade be-tween the left colonic artery and the first sigmoid artery isnecessary to perform an isoperistaltic transplant, only sup-ported by the first sigmoid artery. For that procedure, theleft colonic artery has to be dissected.
Fig. 19.19. If it is impossible to use the left hemicolon forinterposition, the right hemicolon can be used to performthe transposition graft.Scheme of construction of an isoperistaltic colonic interposi-tion using the right hemicolon and the terminal part of theileum. The vascular supply comes from the middle colonic ar-tery.1 Right colonic artery; 2 ileocolic artery.Using the right hemicolon for interposition is burdened byfrequent complications leading to poorer postoperative func-tional results.
1
2

� J. R. Izbicki et al.216
Fig. 19.20. Preparation of an anisoperistaltic colonic interpo-sition using the right hemicolon, with vascular supply fromthe ileocolic artery.
Fig. 19.21. Adequate length of the right hemicolon enablesconstruction of an isoperistaltic interposition without usingthe ileocolic portion of the intestine. This technique offersseveral advantages:� omittance of the terminal ileum, which is prone to necro-
sis� omittance of the ileocecal region which is prone for poor
functional results.
Fig. 19.22. Preparation of a substernal tunnel. Blunt openingof the substernal cavity by spreading the scissors, while pull-ing the xiphoid ventrally with a sharp retractor.

19 Colon Interposition after Total and Subtotal Esophagectomy � 217
Fig. 19.23
Fig. 19.24 Fig. 19.25
Fig. 19.23–19.25. After opening the substernal cavity, asubsternal tunnel is constructed with an atraumatic clamp.The sternum has to be pulled continuously and the endo-thoracic membrane is to be separated from the sternum.A longitudinal incision along the anterior border of the left
sternocleidomastoid muscle is made to expose the cervicalesophagus. Blunt preparation with the hand through thesubsternal tunnel usually leads to rupture of the mediastinalpleura.

� J. R. Izbicki et al.218
Fig. 19.26. Completed preparation of the retrosternal tunnel.In case of tight adhesions to the sternum, these adhesionsare dissected sharply by scissors.1 Thyroid gland; 2 esophagus; 3 trachea.Between corpus and manubrium sterni the substernal fasciais very tightly connected to the sternum. Furthermore, the
visceral and parietal pleura are tightly connected in this re-gion. For this reason, very careful, stepwise preparation witha long atraumatic clamp has to be performed and the prepa-ration has to be manually controlled by the substernally in-troduced finger of the surgeon.
Fig. 19.27 Fig. 19.28
Fig. 19.27–19.29. For the substernal reconstruction a longstrong suture fixed to a drainage tube can be used for thepull-through procedure. The suture is tied to the oral end ofthe colonic interposition. The colon is transposed in the sub-
sternal tunnel to the cervical incision under continuous andgentle pull, and the sternum is to be pulled upwards with asharp retractor during the procedure.
1
2
3

19 Colon Interposition after Total and Subtotal Esophagectomy � 219
Fig. 19.29
1
2
Fig. 19.30. Interposition of the colon through the posteriormediastinum, in the bed of the removed esophagus. Theposterior mediastinal route of the interposed colon is favor-able to the substernal or presternal position, because of theshorter distance to the neck. In addition, the posterior medi-astinal route prevents kinking of the colon. The interposedcolon causes hemostasis in the operation field.1 Azygos vein; 2 colonic interposition.

� J. R. Izbicki et al.220
Fig. 19.31. a If possible, the termino-terminal anastomosisshould be performed in a double row suture technique. b Incase of different lumen diameter, single stitches and a termi-no-lateral anastomosis can be performed close to the taenialibera.
Fig. 19.32a, b. After total esophageal resection in patientswith carcinomas of the upper third of the esophagus or aftercorrosive injuries of the esophagus followed by cicatricialstrictures, a latero-lateral pharyngo-colostomy close to theleft recessus piriformis has to be performed in a double rowsuture technique.
a b
a b

19 Colon Interposition after Total and Subtotal Esophagectomy � 221
Fig. 19.33. Alternative technique for anastomo-sis after colonic interposition: Latero-lateral colo-esophageal anastomosis performed by a linearstapler.
Fig. 19.34. Operative site after transposition of the coloninto the upper abdomen and after the transverso-sigmoidos-tomy has been performed. The mesenteric incision has beenclosed. To avoid tension to the mesocolon, the mesenteric in-cision has to be placed dorsally.
Fig. 19.35. Drainage of the substernal tunnel, the lateralcolonic segments, and the colonic anastomosis.

Complications after subtotal or totalesophagectomy with colonic interposition
� Intraoperative complications
– Wrong selection of the transposed colonicsegment with insufficient length.Most likely the vessels are not clampedprior to dissection, so that the vascularsupply of the oral part of the colonic seg-ment can not be visualized and the totallength of the colon is not sufficient, causingnecrosis of the interpositional graft.To avoid this complication, the entire dis-section and mobilization as well as screen-ing of the vascular supply of the colonicsegment is done prior to the choice of theinterpositional graft.
– Wrong selection of the way to the neck.The subcutaneous way is much longer,but in special cases of a short interposi-tion or an interposition with insufficientvascular supply, the colon should beplaced subcutaneously to have a simpleaccess in case of necrosis.
– Destruction of the main vessels of the in-terposed colon.This complication is mostly due to trau-matic surgical technique or enhanced ten-sion to the vascular trunk, often due toinadequate length of the chosen interposi-tion.
– Opening of the pleura during preparationof the substernal tunnel.This can be followed by pleural herniaswith decreased circulation of the interpo-sition. Therefore the mediastinal pleurashould be incised widely in case of local-ized defects.
– Paresis of the recurrent laryngeal nerve.Gentle surgical technique and clear identi-fication of the nerve prevents paresis.
� Complications duringearly postoperative course
– Pulmonary infections: Tracheobronchitisand pneumonia
– Septic complications: Subphrenic or in-traabdominal abscess; cervical wound in-fection (depending on contamination dur-ing surgery). Prevention: Aseptic surgicaltechnique, sufficient drainage and antibio-tic prophylaxis.
– Cervical anastomotic leak.– Reasons for necrosis of the interposition:Decrease of circulation due to kinking orcompression of the main vessels, hypovo-lemia, hypercoagulability. Avoidance byinterposition of a long colonic segmentwithout tension. Optimizing of the post-operative hemodynamic and rheologic pa-rameters is necessary.
� Complications duringthe late postoperative course
– Cicatricial strictures of the cervical eso-phago- or pharyngeo-colostomy: Mostlydue to anastomotic leak. Treatment of thestenosis is performed by bougienage orballoon dilatation. Only in single casessurgical intervention is indicated.
– Kinking of the interposition: Rare but dan-gerous complication, which often requiressurgical intervention due to clinical symp-tomatic disturbance of the gastrointestinalpassage by elongation of the interposition.Surgical intervention is performed byshortening of the graft.
– Mechanical trauma to a subcutaneousgraft, which often needs surgical interven-tion.
– Polyposis of the interposition: No specifictreatment, regular screening for dysplasiasand subsequent resection.
– Carcinoma of esophageal strictures aftercorrosive injury.
222 � J. R. Izbicki et al.: 19 Colon Interposition after Total and Subtotal Esophagectomy

� Indications
– Benign esophageal stricture in the middleor distal esophageal third
– Giant irresectable benign tumor of thedistal esophageal third
– Irresectable carcinoma of the lower eso-phageal third
All mentioned indications are given only invery few cases and should only be used, ifstomach or jejunum can not serve as interposi-tion/bridging graft. A total or subtotal esopha-geal resection and interposition to the neckwith a cervical anastomosis should be pre-ferred.
� Contraindications
– Severe cardiopulmonary insufficiency.
� Risks and informed consent
– See chapter 13– High risk of anastomosis insufficiency withfollowing mediastinitis and pleural empye-ma.
� Special preoperative measuresand anesthesia
– The same as for total and subtotal esopha-geal reconstruction/substitute by means ofcolon.
� Positioning. 45 degree right elevated positionor intraoperative repositioning from the supineposition to the left-sided position.
� Access/approach. Median epigastric laparo-tomy below the navel/umbilicus, right antero-lateral thoracotomy in the 4.–5. intercostalspaces.
� Operative procedure
1. Laparotomy and exploration of the abdomen2. Establishing of an interposition, reconstructthe colon continuity via colo-colostomy, ana-stomosing the colon-interposition with thestomach
3. Incise the diaphragm and resect the crura ofthe diaphragm (lateral hiatutomy)
4. Thoracotomy and preparation of the esopha-gus
5. Closure of the abdomen6. Esophageal resection and esophago-colosto-my, in case of a bypass operation esophago-colostomy
7. Drainage of the thorax and closure of thethoracotomy.
Intrathoracic Esophagoplastyby Colon InterpositionA.F. Chernousov, P.M. Bogopolski, H.W. Schreiber�, D.C. Broering
20

� A. F. Chernousov et al.224
Fig. 20.1a,b. Principle variations of intrathoracic bypassforms by means of colon-interposition for long benign esopha-geal strictures. a Bypass (Korbhenkel type) with upper latero-lateral anastomosis and lower termino-lateral anastomosis.
b Alternative bypass-variant with upper intrathoracic latero-lateral colo-esophagostomy and intraabdominal termino-lateralcolo-gastrostomy in the region of the antrum.
a b

20 Intrathoracic Esophagoplasty by Colon Interposition � 225
Fig. 20.2a, b. Rare variations of an intrathoracic bypass bymeans of colon-interposition for long strictures in the upperthoracic or cervical part of esophagus (an additional left orright cervical incision of the sternocleidomastoid muscle is re-quired). a The lower anastomosis as termino-lateral anastomo-sis in the pleural cavity. The upper anastomosis as latero-lateralbetween colon-interposition and the right piriform recess.
b The lower anastomosis also as termino-lateral anastomosiswith the esophagus distal to the stricture in the right pleuralcavity. The upper anastomosis will be made with the leftpiriform recess also as latero-lateral anastomosis. The prepa-ration of a colon segment with a special long vascular pedi-cle is required for these variations of thoracic esophageal by-pass.
a
b

� A. F. Chernousov et al.226
Fig. 20.3. Preparation of an isoperistaltic colon-interpositionfrom parts of the transverse colon and the ascending colonwith a long vascular pedicle. The feeding vessel will be theleft colic artery. The parts of colon which are colored asdark-grey will be rejected. The light-grey colored part of co-lon serves as interposition.
Fig. 20.4. Preparation of an isoperistaltic colon-interpositionfrom parts of the descending colon with a long vascularpedicle. The feeding vessel will be the middle colic artery.The dark-grey colored parts of colon will be rejected. Thechoice of both described methods to construct a short colo-nic interposition with a long vascular pedicle depends onthe individual vascular anatomy. Adequate blood supply ischecked by intermittent clamping of each vessel which hasto be transected (black arrows).

20 Intrathoracic Esophagoplasty by Colon Interposition � 227
Fig. 20.5a–d. Important steps to create an intrathoracic by-pass in the region of the distal esophagus. a The colon-inter-position is transposed in a cranial direction in a retrogastralposition. The termino-lateral anastomosis between colon andgastric antrum will be established by means of interruptedsutures (vicryl 3/0) in two rows with a distance of 0.5 cm.
b The esophageal hiatus is now opened after longitudinalmedian incision of the diaphragm and its right crus. The in-terposition is transposed to the right pleural cavity. c, d Thelatero-lateral colo-esophagostomy will be established straightabove the esophageal stricture. A transnasal tube will be in-serted for decompression.
a b
c d

� A. F. Chernousov et al.228
Fig. 20.6. Transverse colo-gastrostomyin the region of the antrum. The vascu-lar pedicle of the colon-interposition isnow located behind the stomach. Theline of incision of the antrum is markedwhere the anastomosis between an-trum and colonic interposition is done.
Fig. 20.7. Colo-gastrostomy is finished.1 Diaphragmoid crurotomy; 2 gastros-tomy.
1
2

20 Intrathoracic Esophagoplasty by Colon Interposition � 229
Fig. 20.8a, b. Operative site after finishing the right intra-thoracic colo-esophagostomy. 1 Stump of ligated azygos vein.A transnasal tube is inserted into the interposition for de-compression. The pleural cavity is drained by thoracic drain-age, which will be placed near the anastomosis.
1
1
a
b

� A. F. Chernousov et al.230
Fig. 20.9a–d. Establishment of a Korbhenkel-type bypass tobridge a short distance benign esophageal stricture bymeans of a colon interposition. a, b Upper anastomosis:Longitudinal incision of the lamina muscularis of the esopha-gus of about 5 cm. Sero-muscular adaptation of colon to
esophagus will be established by vicryl 3/0 single sutureswith a distance about 0.5 cm. Afterwards longitudinal inci-sion of the esophageal mucosa and the colon in the regionof the colonic taenia of about 3.5 cm. The interior row ofsutures will be also made by single sutures.
a
b
0.5 cm
3.5 cm5 cm

20 Intrathoracic Esophagoplasty by Colon Interposition � 231
Fig. 20.9 c,d. Performance of the lower anastomosisand decompression of the interposition.
c
d
0.5 cm

� Indications
Benign strictures and malignant tumors of theesophagus, when the stomach or colon cannotbe used as a substitute.The peculiarity of blood supply and conduct
of vessels of the jejunum carries notable disad-vantages in using it as a substitute for the eso-phagus. The anatomy of the jejunal vesselsrarely allows for preparing a jejunal graft ofsufficient length.
� Contraindications
– Previous partial resections of the jejunum– Billroth II anastomosis.
� Risks and informed consent
See chapter 13.Moreover the patient has to be informed of
the fact that often the jejunal bridging graftdoes not have sufficient length, which mightrequire a temporary stoma and a multi-stageprocedure.
� Special preoperative measures
See chapter 13.
� Anesthesia. General anesthesia; when thoraco-tomy is required: use of a double lumen tube.
� Positioning. See chapter 13.
� Approach. See chapter 13.
� Operative procedure
1. Laparotomy and inspection of the jejunalvascular architecture with particular atten-tion to the anastomoses between the jejunalarteries
2. Temporary clamping of the jejunal arteriesof the first loop starting with the second ra-dial artery and vein
3. Provided a sufficient blood flow to the prox-imal jejunum, an isoperistaltic jejunal bridg-ing graft can be fashioned that is suppliedby the third or fourth jejunal radial artery.
4. Establishing esophagojejunostomy. In casethe jejunal bridge is not long enough, the je-junum is transposed to the anterior chestwall via a subcutaneous tunnel and a jejunalstoma is constructed.
5. Jejunojejunostomy6. If the upper thoracic esophagus can be pre-served alternatively, continuity can be re-es-tablished by an intrathoracic esophagojeju-nostomy.
Reconstruction of Gastrointestinal Continuityby Jejunal Interposition followingTotal and Subtotal EsophagectomyA.F. Chernousov, P. Schurr, P.M. Bogopolski, D.C. Broering, H.W. Schreiber�
21

� A. F. Chernousov et al.234
Fig. 21.1. Gross anatomy of the jejunal arteries and veins.1 Superior mesenteric artery; 2 superior mesenteric vein;3 fourth jejunal artery and vein; 4 ileocolic artery and vein;5 right colic artery and vein; 6 middle colic artery and vein.
Fig. 21.2. Temporary clamping of the second and third jeju-nal artery and vein.
1
2
3
6
5
4

21 Reconstruction of Gastrointestinal Continuity by Jejunal Interposition following Total and Subtotal Esophagectomy � 235
Fig. 21.3. In a combined stricture of esophagus and stomachafter caustic injury and in the event that colon cannot beused as a bridging graft, interposition of jejunum must beestablished by several steps. The jejunal bridge, which is tooshort, is brought to the anterior chest wall via a subcuta-neous tunnel and a jejunal stoma is positioned as high aspossible.
Fig. 21.4 and 21.5. Transposition of thesubcutaneously placed jejunal bridginggraft through the hiatus into the rightthoracic cavity and intrathoracic anasto-mosis of esophagus and jejunum. Fig. 21.4 Fig. 21.5

� A. F. Chernousov et al.236
Fig. 21.6 and 21.7. Remobilization of thesubcutaneous jejunal segment and lengthen-ing of the bridging graft subcutaneously tothe neck with collar anastomosis of esopha-gus and jejunum.
Fig. 21.6. Fig. 21.7
Fig. 21.8 and 21.9. Resection of the jejuno-jejunostomy that was positioned too highlyand re-establishment of the continuity ofthe distal jejunal branch by a terminoterm-inal jejunojejunostomy. Mobilization of thedistal jejunal branch and pull-up to the neckfor esophagojejunostomy. Again a termino-lateral Roux-en-Y jejunostomy is performed.Fig. 21.8 Fig. 21.9
� Combined stricture of esophagus and stomach: different variations of reconstruction(jejunum interposition)

21 Reconstruction of Gastrointestinal Continuity by Jejunal Interposition following Total and Subtotal Esophagectomy � 237
Fig. 21.10 and 21.11. Resection of theRoux-en-Y jejunojejunostomy that was posi-tioned too highly and reconstruction of thecontinuity of the jejunum. Transposition ofthe distal jejunal branch through the hiatusto the right thoracic cavity and establishmentof an intrathoracic termino-lateral esophago-jejunostomy. Fig. 21.10 Fig. 21.11
Fig. 21.12. Technique of remobilization ofthe subcutaneously placed jejunal branch in-cluding the jejunal stoma. If the subcuta-neously located jejunal segment after freeingfrom the subcutaneous presternal tunnel isnot long enough, one further radial arteryand vein has to be cut and ligated after proba-tory clamping. 1 Skin defect after detachedjejunostomy.
1

� A. F. Chernousov et al.238
Fig. 21.13. a Incision for mobilization of the jejunal bridgelocated presternally. b Remobilization of the jejunal bridginggraft that has been placed presternally earlier in this multi-stage procedure, by an incision from the left side of the necktowards the middle near, the jugulum, and another one
along the midline going beyond the umbilicus. The jejunumand the depending mesentery are freed from the surround-ing tissue. The procedure is carried out 3–6 months after thefirst attempt to transpose the jejunum to the neck. By thistime approximately 10 cm can be usually gained.
a
b

21 Reconstruction of Gastrointestinal Continuity by Jejunal Interposition following Total and Subtotal Esophagectomy � 239
Fig. 21.14. Termino-terminal esophagojejunostomy. Fig. 21.15. Termino-lateral esophagojejunostomy.
Fig. 21.16. Resection of an abundant bowel loop in order tostraighten the graft and re-establishment of the continuityby termino-terminal jejunojejunostomy.
� Alternative operations for collar esophagojejunal anastomosis

� A. F. Chernousov et al.240
Fig. 21.17. Resection of the abundant loops of the bridginggraft has to be done without compromising the parajejunalvessel arcade. Therefore skeletonization must be carried out
very closely to the wall of the bowel loop that is about tobe removed (dotted line).
Fig. 21.18 and 21.19. Termino-terminal jejunostomy for re-constructing the jejunal continuity carefully sparing the ves-sel arcades.
Fig. 21.18 Fig. 21.19

21 Reconstruction of Gastrointestinal Continuity by Jejunal Interposition following Total and Subtotal Esophagectomy � 241
Fig. 21.20a,b. Fashioning of a short jejunal bridging graftwith a long vascular pedicle to serve as a substitute for thecervical esophagus. Blood supply is provided by the third ra-dial jejunal artery. The clamped-off jejunal segment is dis-carded.
a
b

� A. F. Chernousov et al.242
Fig. 21.21
Fig. 21.22
1
2

21 Reconstruction of Gastrointestinal Continuity by Jejunal Interposition following Total and Subtotal Esophagectomy � 243
Fig. 21.21–21.23. The free jejunal graft replacing the cervi-cal esophagus (Fig. 21.21). A jejunal segment that has alength of 18–20 cm and that is supplied via the fourth jeju-nal radial arterial branch is freed including the fourth radialvein (Fig. 21.22). After collection the graft is immediately
perfused with heparinized saline solution until it pours outclear from the venous branch. The collar vascular connectionis performed on the thyroid artery and vein (Fig. 21.23).1 Superior thyroid artery; 2 jugular vein.
Fig. 21.23

� A. F. Chernousov et al.244
Fig. 21.24a–d. The free jejunal graft replacing the cervicalesophagus. The jugular vein is opened after tangentialclamping (a) or clamping distally from the anastomosis (b).The tip of the jejunal vein is incised on a length of 2–3 mm
for distension of the lumen preventing later stenosis (a, b).Before being anastomosed both veins are flushed with hepa-rine solution (a, b). The end to side anastomosis is done witha running suture using a non-absorbable 7-0 material (c, d).
a
b
c
d

21 Reconstruction of Gastrointestinal Continuity by Jejunal Interposition following Total and Subtotal Esophagectomy � 245
Fig. 21.25a,b. The free jejunal graft as a substitute to thecervical esophagus. Dissection of the superior thyroid arteryand transection between clamps. Ligation of the peripheralbranch. Flushing of the proximal stump of the superior thy-roid artery and of the jejunal artery with heparin solution.Establishment of an end-to-end anastomosis under the mi-croscope or at least at 4-fold optical magnification with arunning suture using monofile nonabsorbable 7.0 material.
The jejunal artery can also be connected to the externalcarotid artery, the lingual or facial artery. Care has to betaken that the vascular pedicle and particularly the vein isnot kinked nor compressed when the jejunal graft is broughtto its place of destination in the former esophageal bed.Thrombosis of the connected vein is always associated withnecrosis of the graft.
a b

246
1
2
Fig. 21.26. The graft is shorted to thematching length (interrupted line).
Fig. 21.27. Free jejunal graft as a substitute for the cervicalesophagus. Preparation of the hypopharynx and the esophagusfor anastomosis with the graft. 1 Open hypopharynx; 2 prox-imal esophageal end.
� A. F. Chernousov et al.: 21 Reconstruction of Gastrointestinal Continuity by Jejunal Interposition

� Indications
– Severe dysplasia in the distal esophagus(Barrett’s esophagus)
– distal adenocarcinoma of the esophagusstage pT1a and pT1b (UICC 2005).
� Contraindications
– Advanced adenocarcinoma of the esopha-gus (stage pT2 and above)
– Long Barrett’s segment above the carina.
� Risks and informed consent
– Insufficiency of the esophagojejunostomyor the intraabdominal anastomosis
– Mediastinitis– Pancreatitis– Peritonitis– Pleural empyema– Emergency thoracotomy– Necrosis of the jejunal interposition– Postoperative reflux– Postoperative delayed gastric emptying– Possible extension of the operation in-cluding transhiatal esophagectomy or eso-phagogastrectomy in case an advanced tu-mor stage is encountered.
� Particular preoperative measures
– Esophagogastroscopy with extensive biop-sies
– Computed tomography of the chest andabdomen
– Abdominal ultrasound– Endosonography of the esophagus– Pulmonary function test
� Anesthesia. Postoperative analgesia may beimproved by implantation of a thoracic peri-dual catheter.
� Positioning of the patient. See chapter 13.
� Access. See chapter 13.
� Operative procedure
1. Inversed T-shaped upper abdominal inci-sion
2. Mobilization of the left liver lobe3. Division of the lesser omentum and identi-fication of the diaphragmatic limbs and ofthe vagal nerves
4. Median longitudinal incision of the dia-phragm
5. Intraoperative esophagoscopy and markingof the proximal limit of resection by dia-phanoscopy
6. Lymphadenectomy of the inferior mediasti-num and the upper abdomen
7. Positioning of a purse string clamp justcranial to the proximal resection limit anddivision of the esophagus
8. Resection of the lesser curvature includingthe distal esophagus, formation of a neofundus
9. Isolation of a proximal jejunal segment of15 cm in length and retrocolic transposi-tion to the subdiaphragmatic region
10. Termino-lateral esophago-jejunostomy witha circular stapler
11. Latero-lateral or termino-lateral jejunogas-trostomy and termino-terminal jejunostomy.
� Particular instruments. Intraoperative esopha-goscopy.
Limited en bloc Resectionof the Gastroesophageal Junctionwith Isoperistaltic Jejunal InterpositionJ.R. Izbicki, W.T. Knoefel, D.C. Broering
22

� J. R. Izbicki et al.248
Fig. 22.1. Limited en bloc resection of the gastroesophagealjunction includes complete removal of the esophageal seg-ment with metaplastic mucosa, the lower esophageal sphinc-ter and a part of the lesser gastric curvature, and formationof a neo-fundus. Since even early adenocarcinomas of the
distal esophagus (T1b) seed lymph node metastases in up to20% of the patients, removal of the lymph nodes of the les-ser curvature, of the hepatic and splenic arteries, the celiactrunk, the paraaortal region and the inferior mediastinum isan essential part of the operation.

22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition � 249
Fig. 22.2. The left liver lobe is completely mobilized, andthe lesser omentum is incised just medial to the anteriorand posterior gastric vagal branches. A longitudinal mediandiaphragmal incision enables exposure of the inferior posteri-or mediastinum. The distal esophagus is then mobilized in-cluding the paraesophageal tissue. The vagal nerves are di-vided. Intraoperative esophagoscopy identifies the cranial
limit of the Barrett’s segment by diaphanoscopy. This alsomarks the proximal limit of resection. A lymphadenectomyaround the splenic and hepatic artery is performed, the leftgastric vein is divided, and the left gastric artery divided atthe celiac trunk. Then the celiac trunk and the paraaorticregion above the celiac trunk are cleared from lymphatictissue.

� J. R. Izbicki et al.250
Fig. 22.3. Approximately 1 cm proximal to the cranial limitof the Barrett’s segment, a purse string clamp is placed andthe esophagus is divided. Removal of the cardia and lessercurvature is performed by placing multiple linear staplersdown to the border between antrum and body. Thus, a
neo-fundus is formed. As an exception, the short gastric ves-sels have to be divided in order to allow for a sufficient mo-bilization of the gastric fundus. However, in most cases thegastric fundus is not mobilized. 1 Lesser curvature; 2 Divisionof the esophagus; 3 Linear stapler.

22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition � 251
Fig. 22.4a,b. A 15 to 20 cm long segment of the proximaljejunum is isolated and transposed with its mesenteric rootto the diaphragmatic region through the mesocolon and be-hind the stomach. Care has to be taken to dissect the vascu-lar pedicle of this jejunal interposition carefully to provideadequate length. It is imperative to form an isoperistalticjejunal interposition. The proximal anastomosis is then per-formed by a circular stapling device as a termino-lateral eso-phagojejunostomy (a). The stapler is introduced into the endof the jejunal interponate. After firing of the anastomosis,the blind end of the loop is then resected and closed by asuture or with a linear stapler and then oversewn (b).
a
b

252
Fig. 22.5. Close to the base of the neo-fundus, the gastricstapler line is removed over a distance of 3–4 cm, and a ter-mino-lateral or latero-lateral jejuno-gastrostomy is performed.The remaining gastric suture line is oversewn. A termino-ter-minal jejuno-jejunostomy reconstructs the enteric passage.Finally an anterior and/or posterior hiatal repair is performed
� J. R. Izbicki et al.: 22 Limited en bloc Resection of the Gastroesophageal Junction

� Introduction
Achalasia is characterized manometrically byan incomplete relaxation of the lower esopha-geal sphincter. This “outflow obstruction” re-sults in a motility disorder of the tubularyesophagus, in most cases aperistalsis. However,an appearance as seen in diffuse esophagealspasm can also occur. Medical therapy showsshort-term benefit but no long-term solution.Endoscopic dilatation has been established asprimary therapy. However usually repetitivedilatations even in short intervals are neces-sary. In comparison to surgery dilatation is aless controllable procedure. The risk of per-foration is always given, especially in cases ofrecurrent application. Surgical therapy on theother hand provides the opportunity for a con-trolled myotomy followed by an antireflux pro-cedure with a high rate of permanent success.Recent publications support an early surgicalapproach because cure can be provided and apartial remission of the motility disorder canbe noticed.
� Indication
– Minimally invasive procedure impossible(previous extended upper abdominal sur-gery)
– Early dysphagia recurrence after repetitivedilatation
– (Peptical) Stricture and scaring paraeso-phageal and paracardial tissue after failedprevious surgery.
� Contraindications
– General – severe cardiopulmonary insuffi-ciency etc.
– Nondistinctive dignity of the cardioeso-phageal “tumor”.
� Special surgical preparation
– Parenteral nutrition or high caloric ent-eral nutrition in cachectic patients.
� Positioning on the operation table. As for trans-hiatal blunt dissection (see chapter 13).
� Anesthesia. General anesthesia.
� Special instruments. As for transhiatal bluntdissection.
Conventional Cardiomyotomy in AchalasiaK.A. Gawad, D.C. Broering, C. Busch
23

� K.A. Gawad et al.254
Fig. 23.1. Approach by upper midline incision. Alternativelythe upper abdomen can be exposed by a left costal incisionor an upper abdominal transverse incision.
Fig. 23.2. Cardia, distal esophagus, and gastric fundus aremobilized. The ventral branch of the vagus nerve is thor-oughly preserved. For an extensive dissection of the esopha-gus, a long median incision of the diaphragm is helpful. Dis-section of the scarred tissue around the esophagus.

23 Conventional Cardiomyotomy in Achalasia � 255
Fig. 23.3a,b. Longitudinal myotomy along the left aspect ofthe anterior wall of the esophagus and cardia. The incisionis extended over the entire length of the narrow segment, intotal 7 cm upwards onto the esophagus and 2 cm down-wards onto the cardia. At first only the longitudinal musclesof the esophageal wall is transected.
Fig. 23.4. Now the circular muscle layer is transected care-fully undermining it with a clamp and dividing it with scis-sors or diathermy. It is mandatory that this division is com-plete because just a few remaining muscle fibers can resultin recurrence.
a
b
7 cm
2 cm

� K.A. Gawad et al.256
Fig. 23.5. The margins of the myotomy are bluntly dissectedfrom mucosa and submucosa to at least half of the circum-ference.
Fig. 23.6. At the end of the operation mucosa and submu-cosa must slightly prolapse through the myotomy. All stepsof the operation are performed with a large gastric tube inplace to arm the esophagus.

23 Conventional Cardiomyotomy in Achalasia � 257
Fig. 23.7. The release of the esophagus from the surround-ing tissue – as shown here from the omentum – can bevery difficult. In these cases myotomy alone is ineffective be-cause scarring prevents the blunt dissection in the layer be-tween submucosa and musculature. In these cases a partialresection of the esophageal anterior-wall musculature will benecessary.
Fig. 23.8. After complete resection of the esophageal ante-rior wall, the esophagogastric junction is prepared for cover-age.

258
Fig. 23.9. Partial fundoplication. The fundus wall is sewn tothe left margin of the myotomy with interrupted sutures(Vicryl 3/0)..
Fig. 23.10. Partial fundoplication. The fundus wall is finallyfixed to the right margin of the myotomy for complete cov-erage, maintenance of tension, and spacing of the muscledefect.
Fig. 23.11. Partial fundoplication. The back wall of the fun-dus is slipped around the distal esophagus and fixed to theanterior wall in the region of the cardia with no more thantwo sutures. Cranially the fundus back wall is fixed to theesophageal wall resulting in an acute angle between fundusfront and back wall. This type of fundoplication achieves op-timal reflux prevention with minimal risk of dysphagia.
� K.A. Gawad et al.: 23 Conventional Cardiomyotomy in Achalasia

Introduction and Techniquesin gastroesophageal reflux
K.A. Gawad, D.C. Broering, C. Bloechle,
C. Busch
Gastroesophageal reflux disease is character-ized by unphysiologically long contact of gas-tric content with esophageal mucosa. This iscaused by an insufficiency of the lower esopha-geal sphincter which can be verified by mano-metry and confirmed by 24-h pH metry.The surgical therapy of gastroesophageal re-
flux disease (GERD) has changed many timesduring its development. In 1956 the first surgi-cal procedure to treat reflux esophagitis wasintroduced by Rudolf Nissen. Around the sametime, another technique was described inFrance by Lortat-Jacob (1957). During the fol-lowing years further techniques had beendeveloped and modified, demonstrating thatthere was no consensus on the optimal tech-nique. Worldwide the most frequently usedtechnique is the Nissen fundoplication en-hanced by M. Rossetti. With this technique, ingreat series a good surgical long-term outcomecould be achieved in 80–90% of all cases. Byintroduction of the proton-pump inhibitors atrend to conservative therapy was recognized.However, after the medication was discontin-ued the patients suffered from recurrence. Lap-aroscopic surgery has led to a revival of anti-reflux surgery (laparoscopic techniques are de-scribed in chapter 29), with most patients ac-cessed that way. Although, care has to be takenin patients with recurrent disease or previoussurgery, where the conventional approach stillhas its place.
Reflux disease is associated with sliding hia-tal hernia in almost 90% of all cases. In casesof paraesophageal or combined hernias, indi-cation for surgical therapy is always given.Peptic stenosis is a complication of reflux dis-
ease. Here improvement can be achieved byanti-reflux surgery, especially in cases of “floridstenosis” by elimination of the noxa.In addition an endoscopic dilatation can be
performed. In the case of an irreversiblyscarred stricture this single procedure can beinsufficient, and further action as stricturo-plasty, and/or the parietal cell vagotomy, or fi-nally resection may become necessary.
Three basically different groups of surgicalprocedures have been established in the past aslisted below:
I. Techniques aiming at an anatomical recon-struction of the gastroesophageal junction
1. Herniorrhaphia1.1 Classical column-suture according to Welch
(1967)1.2 Herniorrhaphy according to Harrington
(1955) and Madden (1956)1.3 Surgery according to Allison (1951)1.4 Surgery according to Sweet (1948)
2. Gastropexia2.1 Gastropexia according to Nissen (1955)2.2 Gastropexia anterior geniculata according
to Boerema (1955)
3. Miscellaneous3.1 Ligamentum teres-plasty according to Ram-
pal (1964), according to Narbona, Molina(1972), according to Mahmud, Ulrich, Kre-mer (1979)
3.2 Fundophrenicopexia and anterior hiatoplas-tic according to Höhle, Kümmerle (1972).
Surgical Techniquein Gastroesophageal Reflux Disease –Conventional Approach
24

II. Valvuloplasty
1. Total fundoplication1.1 Fundoplication according to Nissen (1956)1.2 Anterior wall fundoplication according to
Nissen-Rossetti (1968)
2. Partial Fundoplication:2.1 Esophago-fundo-phrenicopexia according
to Lortat-Jacob (1957)2.2 Anterior hemifundoplication according to
Dor (1957)2.3 Posterior hemifundoplication according to
Toupet (1963)2.4 Fundoplasty according to Hill (1967)2.5 Mark IVoperation according to Belsey (1967)
III. Miscellaneous
1. Silicone antireflux prosthesis according toAngelchik (1979)
2. Vagotomy3. Roux-Y anastomosis
The techniques aiming for anatomical recon-struction are always used when the hiatal her-nia has to be treated. The Ligamentum teres-plasty has its constant indication in this in-stance. The lower esophageal sphincter is ac-cepted to be the most important pathogeneticfactor in the development of reflux disease.Thus the Nissen fundoplication and the modi-fied Nissen-Rossetti procedure have becomethe standard surgical procedure par excellence.In the Anglo-American countries the Marc IVprocedure is also widely accepted. Only in thelaparoscopic era, partial fundoplications havebeen increasingly used.
� Indications
� Reflux disease
1. General indication for anti-reflux surgery(cp. chapter 7)
2. Minimally invasive procedure not possible(status post surgery in the upper abdomen)
3. Recurrent disease following previous anti-re-flux surgery (laparoscopic or conventional).
� Hiatal hernia
1. Sliding hernia: only with concurrent refluxdisease
2. Paraesophageal and combined hernia: gener-al indication for surgery, conventional proce-dure when a minimally invasive approach isnot feasible.
� Peptic stenosis
1. Failure of conservative therapy including di-latation
2. Nondistinctive dignity of the stenosis.
� Contraindications
General – serious cardiopulmonary disordersetc.
� Risks and considerationsfor informed consent
1. Cuff-rupture � recurrence2. Cuff too tight � “Gas-bloat” syndrome3. Stomach slips through the cuff = “Telescope-phenomenon”Cave: particularly following combinedapproach with vagotomy
4. Cuff primarily placed too low on the stom-ach� recurrence, gastric depletion disorder
5. Denervation syndrome � gastric depletiondisorder, “Gas-bloat”.
� Positioning on the operation table. As for trans-hiatal blunt dissection (cp. chapter 13).
� Anesthesia. General.
� Special instruments. As for transhiatal bluntdissection (cp. chapter 13).
� Choice of the procedure
� Simple reflux disease (esophagitis up to �III)1. Fundoplication2. Ligamentum teres plasty.
� Complicated reflux disease (esophagitis �IV)
1. Fundoplication + dilatation (of floride eso-phagitis)
2. Fundoplication + parietal cell vagotomy (ingastric hyperacidity) + if necessary bougie-nage (of floride esophagitis)
3. Fundoplication + parietal cell vagotomy +stricturoplasty (of scarred strictures).
� K.A. Gawad et al.260

� Paraesophageal hernia
1. Reposition + hiatoplasty + fundophrenico-and if necessary anterior corpopexia
2. Reposition + hiatoplasty + Lig. teres plasty3. Reposition + hiatoplasty + fundoplication(in presence of concurrent reflux disease)
24 Surgical Technique in Gastroesophageal Reflux Disease – Conventional Approach � 261
Fig. 24.1. Approach by median upper abdominal laparotomy.Alternatively the upper abdomen can be exposed by a leftsubcostal incision or an upper abdominal transverse incision.A Rochard retractor provides excellent exposure of the epi-gastrium.
Fig. 24.2. Fundoplication according to Nissen-Rossetti. Thedistal esophagus is enlaced. The cardia, the distal esophagus,and the gastric fundus are mobilized preserving the vagusnerve and the spleen. Dissection of the greater curvature isnot mandatory, but can facilitate the easy formation of aloose, “floppy” fundoplication.
Fig. 24.3. Fundoplication according toNissen-Rossetti. A retro-esophageal win-dow is created to pass the fundus to theright side. It is transposed so far that theanterior wall can be wrapped aroundthe distal esophagus loosely withoutany signs of tension.

� K.A. Gawad et al.262
Fig. 24.4. Fundoplication according to Nissen-Rossetti. Thefundoplication is formed by unifying the two cuff-folds ofthe anterior fundus wall and fixed by three, maximally four,
non-absorbable sutures. At least one suture should partiallygrab the esophageal wall to prevent a telescope phenome-non.
Fig. 24.5. The stomach encircles the distal esophagus build-ing a loose cuff (“floppy-Nissen”) to avoid postoperative dys-phagia.
Fig. 24.6. Finally the anterior cuff-fold is secured with twosutures to the stomach to prevent slippage.

24 Surgical Technique in Gastroesophageal Reflux Disease – Conventional Approach � 263
Fig. 24.7. Ligamentum teres (round ligament) plasty. Aftercompletion of the dissection of the esophagogastric junctionand enlacement of the esophagus with a rubber band theround ligament is carefully dissected from the abdominal
wall and from the liver, respectively. Special attention has tobe drawn to thoroughly preserving the ligament at laparo-tomy. The free end of the ligament is transposed dorsallyaround the esophagus coming from the right side.
Fig. 24.8. Ligamentum teres plasty. Finally the ligament isattached to the stomach anterior wall under relative tensionusing three or four non-absorbable sutures.

Techniques in peptic stricture and hiatal hernia
A.F. Chernousov, P.M. Bogopolski, K.A. Gawad
Peptic stricture of the esophagus
� Indications
– Treatment failure of conservative therapyincluding endoscopic dilatation
– In the case of suspected carcinoma of thegastroesophageal junction
– Simultaneous occurrence with a diseaseof the upper gastro-intestinal tract asduodenal ulcer or cholecystolithiasis etc.
– Failed previous anti-reflux surgery or car-dioplasty and in cases of poor outcome ofconservative treatment.
� Contraindications
No special contraindications.
� Special surgical preparation
Endoscopic dilatation to achieve a transitorypre-operative remission of the complaints.Conservative anti-reflux therapy.
� Anesthesia. General anesthesia.
� Positioning on the operation table.
See chapter 13.
� Type of incision. Median laparotomy.
� Special instruments. See chapter 13.
264 � A. F. Chernousov et al.

24 Surgical Technique in Gastroesophageal Reflux Disease – Conventional Approach � 265
Fig. 24.9a–d. Peptic stricture of the esophagus. In cases ofa peptic stricture with minor scarred alterations of the eso-phageal wall (“inflammatory stricture”) parietal cell vagotomycombined with a fundoplication is the approved method.a Dissection of the esophagogastric junction with mandatorytransection of the A. polaris ascendens. The abdominal eso-phagus is exposed up to 6 cm cranial to the cardia. The
fundus is mobilized up to the short gastric vessels in thearea of the hilum of the spleen. b A circular myotomy of theabdominal esophagus should be avoided to preserve thecontractility of the esophagogastric junction. Only vagalbranches which encircle the esophagus are dissected.c, d After completion of the parietal cell vagotomy, a modi-fied fundoplication is performed.
a b
c d

266
Fig. 24.10a–d. Peptic stricture of the esophagus. Perfor-mance of the modified fundoplication: During the creation ofthe cuff the esophagogastric junction should be armed witha large bore gastric tube to prevent the cuff from gettingtoo tight. a Along the dashed line the gastric anterior andposterior wall are sewn together. b Beginning of the fundo-
plication at the antrum. The esophagus is drawn caudallyinto the cuff and will be covered by it. c The upper four su-tures are anchored in the esophageal wall to prevent slip-ping of the esophagus within the cuff. d Two final suturesfix the neck of the cuff to the esophagus.
a b
c d
� A. F. Chernousov et al.

24 Surgical Technique in Gastroesophageal Reflux Disease – Conventional Approach � 267
0.3 cm0.5 cm
Fig. 24.11a–d. Peptic strictures of the esophagus. Shortstricture of the esophagogastric junction. a Longitudinal inci-sion of the esophageal muscle (myotomy). b The ends ofthe incision are pulled aside with corner stitches. The stric-tured anterior wall is excised (dashed line). c The resulting
defect is closed with full thickness single stitches (Vicryl 3/0)in a single row. d Following parietal cell vagotomy, the su-ture line is covered again by a fundoplication as mentionedabove.
a b
c d

Hiatal hernia
� Indications
Cardiofundal and paraesophageal hernia be-cause of the risk of incarceration, bleeding, orperforation of the hernia.
� Contraindications
No specific contraindications.
� Special surgical preparation
See chapter 14.
� Anesthesia. General anesthesia.
� Positioning on the operation table.
See chapter 14.
� Type of incision. Median laparotomy.
268 � A. F. Chernousov et al.

24 Surgical Technique in Gastroesophageal Reflux Disease – Conventional Approach � 269
Fig. 24.12a–c. Paraesophageal hernia. Paraesophageal her-nias lead to a partial or total gastric volvulus. a The mostcommon type is the proximal partial gastric volvulus with ro-tation and prolapse of a proximal fundus; b rare type withrotation and prolaps of a distal gastric sector and generationof a functional gastric outlet obstruction; c upside-down stom-ach.
Fig. 24.13. Combined hernia. Combined hiatal hernia withaxial sliding of the cardia and para-esophageal component.In both hernia types, a common hiatus is often seen.
a b c

270
Fig. 24.14a,b. Hiatal hernia. Field after mobilization of theleft-lateral lobe of the liver with visible herniation of thegastric fundus into the esophageal hiatus. a Section line.b Scheme of cardio-fundal herniation.
a
b
� A. F. Chernousov et al.

24 Surgical Technique in Gastroesophageal Reflux Disease – Conventional Approach � 271
Fig. 24.15a,b. Hiatal hernia. Stomach and esophagus afterexcision of the hernia sack. a The stomach is reduced fromthe hiatal hernia sack in the dorsal mediastinum. b The her-nia sack is pulled caudally and excised.
a b

272
Fig. 24.16a, b. Hiatal hernia. Closure of the hiatus behindthe esophagus (posterior hiatoplasty). a The first stitch grabsthe left crus; b the suture is then guided behind the esopha-
gus and the right crus is grabbed subsequently. When tyingthe sutures, the esophagus should be armed with a largetube to avoid a stenosis.
Fig. 24.17a,b. Hiatal hernia. The phrenic crura are adaptedwith three non-absorbable sutures. a The large gastric tubeis pushed forward into the stomach. The first suture is put
to tension to adjust the diameter of the hiatus. b Final viewafter tying all sutures.
a b
a b
� A. F. Chernousov et al.

24 Surgical Technique in Gastroesophageal Reflux Disease – Conventional Approach � 273
Fig. 24.18a–c. Hiatal hernia, bilateral hiatoplasty for verylarge hernias. a If the esophageal hiatus is distinctively wideopen after resection of the hernia sack, a hiatoplasty withtwo suture rows becomes necessary. The first row of suturesis placed to the left and ventral to the esophagus with 3single sutures. b The second row of sutures is placed asmentioned for the posterior hiatoplasty. c Finally a partial
fundoplication is used to re-establish the angle of His. Theformer hernia cavity in the posterior mediastinum is drained.A further drainage can be placed subphrenically. A naso-gas-tric tube should be left in place to decompress the stomachfor the first postoperative days.During this operation neither the esophagus nor the gastriccuff should be fixed to the diaphragm.
a b
c

Esophageal diverticula are rare. They can beeither local or generalized, with local circum-script diverticula being the most commontypes. According to their location they are di-vided into: Cervical/pharyngoesophageal, para-bronchial/mid-thoracic, and epiphrenic diver-ticula.Functional problems with regurgitation of
meals and foetor ex ore are common in thosepatients. Dysphagia is the most common rea-son for surgical treatment. Endoscpopic treat-ment might be possible for cervical diverticula(see chapter 30).
� Indications
– Diverticulitis– Dysphagia– Regurgitation– Perforation– Mediastinitis– Bronchial fistula.
� Contraindications
General.
� Special preoperative preparations
Gastric or duodenal nutrition tube for patientswith large diverticula and severe dysphagia.Systemic intravenous antibiotic therapy for pa-tients with complications as perforation, fistu-la, and mediastinitis.
� Anesthesia
– Endotracheal intubation– Perioperative antibiotic prophylaxis.
� Positioning
– Cervical diverticula: Positioning of thepatient on his back. The head of the pa-tient is to be reclined and turned to theright side.
– Mid-thoracic/mid-esophageal diverticula:Positioning of the patient left sided, posi-tion for right anterolateral thoracotomybetween the 4th and the 5th rib.
– Epiphrenic diverticula: Positioning of thepatient in left-sided position for rightanterolateral thoracotomy between the 5thand the 6th rib. If the diverticulum goesto the left side (very rare), the patient isto be positioned on the right side.
� Zenker’s/cervical diverticulum
The pharyngoesophageal diverticulum occursin about 70% of all cases with esophageal di-verticula (1 : 15000). It was first described byLudlow and Zenker consecutively, initially de-fining and showing the correct anatomical po-sition. The main localization is the Kilian tri-angle (first described in 1908 by Kilian and in1950 by Negus), e.g. the weak muscular regionabove the cricopharyngeal muscle. The Lai-mer’s triangle is a far less common anatomicallocalization of the diverticulum. The diverticu-la are mostly located on the left side of the pa-tients’ neck. Big diverticula appear to be in themidline. One of 60 patients with dysphagiamight have a cervical esophageal diverticulum.Patients normally present in advanced age(male> female).
Conventional Resection of Esophageal DiverticulaA.F. Chernousov, C.F. Eisenberger, P.M. Bogopolski, J.R. Izbicki, H.W. Schreiber�
25

� A. F. Chernousov et al.276
Fig. 25.1. Zenker’s diverticulum. 1 Stump of the ligatedupper thyroid artery; 2 diverticulum in the Kilian’s triangle(between cricopharyngeal muscle and pharyngeal constrictormuscle); 3 pharyngeal constrictor; 4 horizontal part of thecricopharyngeal muscle; 5 Laimer’s triangle (weak muscularportion underneath the cricopharyngeus muscle); 6 recurrentlaryngeal nerve.The access is through an incision along the anterior aspectof the sternocleidomastoid muscle. The left lateral wall ofthe esophagus and of the pharynx is dissected. The esopha-gus is intubated with a large gastric tube. Ligation of theupper thyroid vessels might be necessary, but this is notmandatory. Under continuous tension the diverticulum is dis-sected until the neck is exposed.
Fig. 25.2. Zenker’s diverticulum. The diverticulum is trans-sected with a linear stapler in a transverse direction. No ten-sion is to be brought to the mucosa, otherwise stenosismight result after closing the muscular layer by sutures.
Fig. 25.3. Zenker’s diverticulum. The pharyngoesophagealmuscles are closed by interrupted sutures. Myotomy of the low-er pharyngeal constrictor muscle over 2–3 cm is necessary inall cases. 1 Myotomy of the pharyngeal constrictor muscle.
1
2
3
4
5
6
1

25 Conventional Resection of Esophageal Diverticula � 277
Fig. 25.4. Zenker’s diverticulum. Alternatively the diverticu-lum can also be resected between two clamps at its base.The base of the diverticulum should only be touched with asoft bowel clamp. The mucosa of the esophagus should beclosed with a running suture above the clamp. The sutureshould be finished without tension to avoid stenosis of theesophagus.
Fig. 25.5. Zenker’s diverticulum. The pharyngoesophagealmuscles is to be closed with single interrupted sutures. Myo-tomy over 2.3 cm is obligatory. 1 Myotomy of the pharyngealconstrictor muscle.
Fig. 25.6. Insertion of a soft drain and closure of thewound.
1

Epiphrenic diverticulum
� A. F. Chernousov et al.278
Fig. 25.7. Epiphrenic diverticulum. Line of incision of themediastinal pleura.
Fig. 25.8. Epiphrenic diverticulum. Dissected epiphrenic di-verticulum.
Fig. 25.9. Epiphrenic diverticulum. Transection of the diver-ticulum with a linear stapler. Only slight tension on the baseis to be applied to avoid stenosis.

25 Conventional Resection of Esophageal Diverticula � 279
Fig. 25.10. Epiphrenic diverticulum. Alternatively, the diver-ticulum can be transsected in an open fashion with scissorsafter applying stay sutures to both ends.
Fig. 25.11. Epiphrenic diverticulum. After the resection ofthe diverticulum with a stapler, the muscular layer is closedwith interrupted sutures (Vicryl 3/0).
Fig. 25.12. Epiphrenic diverticulum. After the resection ofthe diverticulum with scissors, the mucosa and submucosa,and afterwards the muscular layer, is closed with interruptedsutures.
Fig. 25.13. Epiphrenic diverticulum. The sutures are coveredwith a pleural flap. The thoracic cavity is drained with adrainage.

Preparation of a diaphragmatic flap for enforcement of the esophageal wallafter resection of an epiphrenic diverticulum
280
a b
� A. F. Chernousov et al.: 25 Conventional Resection of Esophageal Diverticula
c d
Fig. 25.14a–d. For sufficient viability the phrenic flapshould have a vessel at the base of the graft (a). The graftis fixed circularly to the esophagus with interrupted sutures(b, c). View of the graft after fixation (d). The esophageal
wall is enforced by the diaphragmatic flap. The defect onthe diaphragm is closed. Gastric decompression is necessarywith a gastric tube as well as the drainage of the pleuralcavity.

� Indications
– Tumor of unclear dignity– Risk of malignant potential– Ulceration– Dysphagia.
� Contraindications
General.
� Special preoperative preparations
– General– An endoscopic biopsy of the tumor is notrecommended because it prevents the tu-mor resection without incision of the eso-phageal lumen.
� Anesthesia. Endotracheal intubation.
� Positioning and surgical approach. It dependson the tumor’s localization as described inchapter 25.
� Leiomyoma of the thoracic esophagus
Leiomyomas localized at the abdominal eso-phagus were excised analogous to the approachdescribed above.However, a subsequent fundoplication am-
plifies the esophageal sutures. Extremely rarelarge leiomyoma which seizes the whole cir-cumference or ranges from the pharynx to thecardia requires a partial or complete resectionof the esophagus.
Local Excision of Benign Esophageal TumorsA.F. Chernousov, A. Kutup, P.M. Bogopolski, H.W. Schreiber�
26

282
Fig. 26.1. Leiomyoma of the thoracic esophagus. Expositionof the thoracic esophagus over a right-sided anterolateralthoracotomy through the 5th ICR and incision of the medias-tinal pleura and esophageal muscles above the tumor. Circu-lar preparation is not necessary in most cases and should beavoided. In cases of rare circular tumor extension, completemobilization of the esophagus has to be done.
Fig. 26.2. Different steps of tumor nucleation. The musclelayers are separated from the tumor.
Fig. 26.3. To perform an atraumatic pull on the tumor astay suture is placed. Under pull at the stay suture prepara-tion of the esophageal mucosa without injury should be per-formed.
Fig. 26.4. Occlusion of the muscle layer with button sutures(Vicryl 3/0). The gastric tube and the thoracic drainageshould remain for at least two days.
� A. F. Chernousov et al.: 26 Local Excision of Benign Esophageal Tumors

Injuries of the esophagus may be caused by me-chanical, chemical, and actinic damages. Usual-ly, they are the consequence of a blunt trauma.The exceptions are perforations of the esopha-gus. Injuries of the esophagus by ingestion ofa foreign body arise in physiologic narrow pas-sages (pharyngoesophageal passage, in the mid-dle third of the aortic arch, cardioesophagealpassage). A decubitus of the esophagus can beseen if a foreign body remains longer in the eso-phagus. Diagnostic and therapeutic endoscopymeasures may also lead to injuries of the eso-phagus. Esophagoscopy and bougienage of a ci-catricial stricture, especially in an early phaseafter a corrosive injury, are the most frequentreasons for an iatrogenic perforation of the eso-phagus. Dilatation of the cardia with the Stark’sinstrument can cause a laceration and perfora-tion. Complications for pneumatic or hydro-static dilatation are rarely seen.An injury of the esophagus is also possible
through severe vomiting (spontaneous rupture,Boerrhaave’s syndrome), blunt traumas of theneck, the thorax, or the abdomen. Radiationinjury of the esophagus is a complication ofradiation therapy of malignant tumors of themediastinum and may lead to the developmentof esophageal fistulas. Chemical injuries of theesophagus are caused by swallowing acids orlyes. They are divided according to their ser-iousness:� Grade 1: Exclusive destruction of the mu-cous coat.
� Grade 2: Destruction of the mucous coat,the submucosa, and parts of the muscularis.
� Grade 3: Destruction of the complete layersof the esophagus and of the surrounding fattissue as well as related organs.
The grade of the corrosive injury depends onthe quantity and ingredients of the swallowed
chemical substance. After swallowing an acid acoagulation necrosis results, which mostly islimited to the superficial layers of the esopha-gus. After swallowing lye, a dreaded colliqua-tive necrosis develops, involving almost alwaysall layers of the esophageal wall leading to aperforation. The most feared complication ofthe corrosive injury of the esophagus is themediastinitis.For grade 1-corrosive injury, a healing
through epithelization without any conse-quences is expected. In cases of extended cor-rosive injuries, a perforation may occur one ortwo weeks after the ingestion; as late complica-tions a shortening of the esophagus due to ci-catricial contracture and ulcerations are de-scribed.An iatrogenic injury of the esophagus is also
possible during thoracic operations, for exam-ple during a pneumonectomy with a radicallymphadenectomy. In these cases, a perforationof the esophagus by devascularization andconsecutive necrosis develops after a period of1–2 weeks.Superficial injuries of the esophagus mani-
fest themselves in the form of an upper gastro-intestinal bleeding. On the other hand, openor penetrating injuries of the esophagus be-come symptomatic by neck emphysema, med-iastinitis, pleural empyema, or peritonitis. Incase of an extensive, fresh injury of the eso-phagus, a transthoracic or transhiatal esopha-gectomy is the preferential method for surgicalintervention. A direct suture of an intrathor-acic injury of the esophagus with an additionalaugmentation of the suture through a pleuralor diaphragmatic flap is not as safe as the eso-phagectomy. Furthermore, scarred strictures inthe area of the direct suture of the esophagusare common late complications of this proce-dure.
Surgical Treatment of Esophageal Fistulaand PerforationA.F. Chernousov, N. Roch, P.M. Bogopolski, D.C. Broering, H.W. Schreiber�
27

The direct suture of injuries of the intra-ab-dominal part of the esophagus therefore ismuch safer to carry out since the suture canbe covered and protected by a fundoplication.In the collar area of the esophagus, it is advi-sable to close the laceration immediately in or-der to prevent the development of fistulas. Ifthey should form, they should be treated con-servatively since they rarely lead to septic com-plications.
Fistulas of the esophagus
Acquired fistulas of the esophagus may be di-vided into internal and external fistulas. Theycan connect the esophagus with tracheobron-chial structures, the pleural cavity, and the me-diastinum. There is a principle that fistulas ofthe esophagus are the result of mechanical,chemical, and actinic injuries of the esopha-gus, of a decubitus caused by foreign bodies,of a perforation of an esophagus diverticulum,tumors, or ulcers. In rare cases fistulas of theesophagus may be healed by an adequate con-servative therapy. Palliative operations (esopha-gostomy and gastrostomy) can also lead to sat-isfactory results in rare cases. Radical opera-tions such as resection and occlusion of thefistulas mostly require an esophagectomy, a re-section of parts of the lung, and decortication.Therefore, they are associated with a highpostoperative morbidity.The main principle of fistula surgery of the
esophagus is the occlusion of the esophagealdefect of the wall and isolation of surroundingtissue.
Cervical fistulas of the esophagus
� A. F. Chernousov et al.284
Fig. 27.1. Left-lateral approach to the cervical esophagusalong the front edge of the sternocleidomastoid muscle. Thefistula is excised and the resulting esophageal defect isclosed with two rows of interrupted button-hole sutures.

27 Surgical Treatment of Esophageal Fistula and Perforation � 285
a b
Fig. 27.2. To cover the suture of the esophagus, a muscle-flap of the sternocleidomastoid muscle will be prepared.
Fig. 27.3a,b. The muscle-flap of the sternocleidomastoideusis fixed circumferentially to the closed fistula.

Intrathoracic esophago-tracheal fistula
� A. F. Chernousov et al.286
Fig. 27.4. Closure of an esophago-tracheal fistula. The fistulais exposed by right-lateral thoracotomy in the 4th or 5th in-tercostal space. The azygos vein is severed and the ends li-gated with transfixing sutures. The fistula is excised.
Fig. 27.5. Closure of the tracheal defect with one row ofbutton-hole sutures (Vicryl 5/0). The stitches should be2–3 mm apart.
Fig. 27.6. After the excision of the fistula the esophagealdefect is closed with two rows of button-hole sutures (Vicryl4/0).
Fig. 27.7. The esophagus wall is reinforced by a pedicledflap from the pleura, and the fistula is simultaneously iso-lated. These operative steps should be carried out only inthe presence of a wide lumen naso-gastric probe.

Intrathoracic fistulas
27 Surgical Treatment of Esophageal Fistula and Perforation � 287
Fig. 27.8a, b. Perforation in the middle third of the esopha-gus. Mobilization and dissection of the arch of the azygosvein. A patch is obtained by longitudinal incision of the vein.The esophageal perforation is closed with two rows of inter-rupted stitches (Vicryl 4/0).
Fig. 27.9a,b. The vein is sutured on the esophageal wallcircumferentially around the esophageal suture line. The azy-gos vein patch is also closed. It is obligatory to providedrainage of the pleural cavity and to ensure intraluminal de-compression.
a a
b b

Intraabdominal fistulas of the esophagus
� A. F. Chernousov et al.288
Fig. 27.10a, b. The preparation of the venous patch de-pends on the location of the perforation. If the preparationis located in the lower segment of the thoracic esophagus,the venous patch must be prepared from the distal segmentsof the azygos vein. The azygos vein and its tributaries (bro-ken line) are mobilized and dissected; the perforation isclosed by suturing the venous patch.
Fig. 27.11a,b. Closure of a perforation of the abdominalesophagus. The perforation is closed with interrupted suturesin two rows. The stitches should be 5 mm apart, and thestitches of the inner row are taken as plan-layer, extramuco-
sal sutures. The ‘in’ and ‘out’ stitch should be approximately3 mm away from the wound margin. The scheme also showsthe start of the fundoplication for covering the esophagealsuture line.
a
b
a
b

27 Surgical Treatment of Esophageal Fistula and Perforation � 289
Fig. 27.12 and 27.13. The suture line is covered by theanterior wall of the fundus. The suture is fixed in a circlearound the perforation stitch (broken line). The posterior
wall of the fundus is put behind the esophagus for plicationand sutured ventrally to the esophagus with the pre-fixedanterior wall of the fundus.
Fig. 27.12 Fig. 27.13
Fig. 27.14. Schemeof the esophagopleural fistula.
Esophagopleural fistulas
Transhiatal closure of an esophagopleural fistu-la (fistula of the lower esophageal third).

� A. F. Chernousov et al.290
Fig. 27.15. Following sagittal diaphragmatomy and abdom-inal and distal thoracic mobilization, traction is applied tothe esophagus in a caudal direction by a soft rubber tube.The fistula is excised.
Fig. 27.16. The esophageal defect is closed with two rowsof interrupted sutures. The defect in the mediastinal pleurais covered by a diaphragmatic pedicled flap.

27 Surgical Treatment of Esophageal Fistula and Perforation � 291
Fig. 27.17. As described earlier, the esophageal stitch is re-inforced by 360� fundoplication. A drainage is provided forthe pleural cavity and the abdomen.
Fig. 27.18a,b. Transhiatal closure of a fistula located in themiddle third of the esophagus. Diagram shows the localiza-tion of the fistula. The esophagus is mobilized along its rightlateral wall, as described in the case of dissection of thetranshiatal blunt dissection. Sharp excision of the fistula.
a
b

292
Fig. 27.19. The esophageal defect will be closed in tworows with button-hole sutures. The mobilized greater omen-tum will be fixed circumferentially around the defect in themediastinal pleura with 4 mattress sutures. The sutures arefirst inserted and subsequently tied in succession. The pleuraldefect is separated from the esophageal suture line by thegreater omentum flap.
Fig. 27.20. Anterior or posterior hiatoplasty.
� A. F. Chernousov et al.: 27 Surgical Treatment of Esophageal Fistula and Perforation

� Indications
After failure of endoscopic therapies includingballoon dilatation and bougienage in cases of– Short peptic stricture– Short scarred stenosis.
� Contraindications
– Suspicion of malignancy– Severe cardiopulmonary insufficiency.
� Risks and informed consent
See chapter 13.
� Special preparation
No peculiarities to the previously mentionedoperations.
� Anesthesia. Endotracheal anesthesia, in caseof intrathoracic stenosis a tracheal tube withthe possibility of separate ventilation should beused.
� Positioning and approach. It depends on thelocation of the stenosis.– Collar stenosis: Left cervical approach, su-pination
– Intrathoracic stenosis: Right antero-lateralthoracotomy 4–6 ICS
– Stenosis of the abdominal part of the eso-phagus: “inverted T-incision” or medianlaparotomy.
Techniques of Local EsophagoplastyA.F. Chernousov, A. Kutup, P.M. Bogopolski, H.W. Schreiber�
28

� A. F. Chernousov et al.294
Fig. 28.1a, b. Resection of a short stricture (length max.1.5 cm). After resection of the stenotic segment, mobilizationof the proximal and distal end of esophagus restores the ba-sis for reconstruction of the continuity with single layer end-to-end anastomosis in single suture technique. The distanceof each suture should be 5 mm. Each stitch should be placed
5 mm distant to the anastomosis. In stenosis shorter than1 cm stricturoplasty according to Heineke Mikulicz should beperformed. Therefore a longitudinal esophagectomy is per-formed and a single layer transverse closure with mattresssutures.
0.5 cm
0.5 cm
a
0.5 cm
b

28 Techniques of Local Esophagoplasty � 295
Fig. 28.2a–d. In stenosis limited to mucosa and submucosaa transverse transection of the esophageal musculature overthe stenosis suffices (a). The anterior part of the stricture is
resected (b). Reconstruction of the continuity of mucosa andsubmucosa in the posterior wall area (c). Transverse closureof the anterior wall with single layer mattress sutures (d).
a b
c d
0.5 cm

296
Fig. 28.3a–c. In case of a prestenotic dilatation of the eso-phagus a side-to-side esophagostomy of the pre- and post-stenotic esophageal segment should be performed. In all
local esophagoplasties an intraluminal placed tube (for exam-ple a large gastric tube) and an abundant external drainageis obligatory.
a b c
� A. F. Chernousov et al.: 28 Techniques of Local Esophagoplasty
0.5 cm

Introduction
Minimal access surgery appears of particularvalue in the surgical treatment of esophagealdiseases because of the disproportion betweenthe access with its considerable invasivenessand morbidity and the surgical interventionper se which is, in the majority of cases, lesssevere. This obvious discrepancy makes aminimal-invasive approach an attractive alter-native. The aim is to avoid a thoracotomy withits attendant morbidity and replace it with thesmaller incisions used in MIC.Meanwhile, MIC alternatives have been de-
veloped for all surgical interventions for be-nign diseases. MIC operations for malignanciesare feasible as well – at least from the technicalpoint of view. In the following, the details ofclinically important esophageal interventionsare demonstrated. Additionally, an evaluationof these techniques will be attempted in com-parison to corresponding open procedures.
Diverticula of the esophagus
Diverticula of the esophagus may be found inthe cervical part (Zenker’s diverticulum), atthe height of the bronchial bifurcation (para-bronchial) and above the esophagogastric junc-tion (epiphrenic d.). In case of cervical andepiphrenic diverticula, we have to deal with socalled “pulsion” diverticula which arise becauseof a malfunction of the correlated sphincter.Both of them need surgical intervention. Myo-tomy of the respective sphincter is an obligatorypart of the operation.
� Endoscopic treatmentof Zenker’s diverticulum
The decisive step in the surgical treatment iscricopharyngeal myotomy, i.e. a complete divi-sion of the upper esophageal sphincter. Incom-plete opening is the cause for the developmentof a diverticulum. The classical surgical treat-ment is cricopharyngeal myotomy and an exci-sion of the sac using a linear stapler. ManyENT surgeons, however, traditionally preferredtransoral treatment (Mocher 1917). The thera-peutic principle of servering the common wallbetween the esophageal lumen and the diver-
Minimal Invasive Surgery of the EsophagusH. Feussner, R. Bumm, T. Olah
29
Fig. 29.1. Positioning of the patient for endoscopic treat-ment of Zenker’s diverticulum. Extension of the head is es-sential. Woodbridge tube is required for intubation.

ticulum is a reasonable approach, since theupper esophageal sphincter is inevitably di-vided as well. Thus, the leading symptom –dysphagia – will be successfully treated. Gener-al surgeons, however, did not adapt this alter-native technique, probably because a simpledissection of the sac without any securing ofthe line of dissection was considered too risky.Today, linear cutting devices are available
which seal the lind of dissection by staples. Ac-cordingly, this may now be used for the trans-oral treatment of cervical diverticulum. By onesingle movement of the handle, a broad com-munication between the esophagus is createdincluding a complete myotomy of the upperesophageal sphincter.After the adequate expositee of the area by
means of a laryngoscope (both the entrance ofthe esophagus and of the diverticulum must beclearly visible), the operation can be accom-plished within a few minutes by the applica-tion of the linear cutter. Accordingly, it isminimally invasive. In comparison to the openprocedure, the risk of a leakage (which mayoccur in open surgery not only in the area ofthe stapling line but as well in the regionwhere the myotomy has been performed)should be lower as well as the risk of recurrentlaryngeal nerve palsy.
� Thoracoscopic extirpationof an epiphrenic diverticulum
The pathogenesis of an epiphrenic diverticu-lum is identical to that of a cervical diverticu-lum. Due to the impaired opening (incompleteor uncoordinated relaxation) of the lower eso-phageal sphincter, the esophageal wall progres-sively bulges at a point of minor resistance.Myotomy of the lower esophageal sphincter is,therefore, an integral part of the operation aswell as the extirpation of the diverticular sac.Extirpation of the diverticulum is only feasibleby the transthoracic route. Correspondingly,the myotomy is performed by transthoracic ac-cess as well.
� H. Feussner et al.298
Fig. 29.2. Self-retaining laryngoscope. Sufficient exposure ofthe esophageal lumen may be difficult in some cases. Theprocedure can only be performed reliable with a self retain-ing laryngoscope.
Fig. 29.3. Operative principle. The arm of the linear staplercontaining the staples is introduced into the esophagus andthe arm is placed into the diverticulum. Firing of the staplercreates a broad communication between the two lumen. Thedissection line is secured by sutures.

� Excision of a parabronchial diverticulum
Surgical resection of a parabronchial diverticu-lum is required in a minority of cases only. If se-vere dysphagia is the leading symptom and canbe explained by retention of food within the di-verticulum, a resection may be justified. In anyinstance, a careful manometric evaluation ofesophageal motility is mandatory. Eventually,the resection has been combined with myotomy.
� Comment
Since esophageal diverticula are comparativelyrare, large series are rare even with conven-tional surgery. This is even more true for mini-mally invasive techniques which have beenavailable for a few years only. An evaluation oftheir role is, therefore, still not possible. Theconventional techniques are still the gold stan-dard. However, MIC procedures may be accept-able, provided that informed consent is givenby the patient. According to our preliminaryexperience, a growing popularity is probable,since the advantages of the minimal invasiveapproach become evident in clinical practice.
29 Minimal Invasive Surgery of the Esophagus � 299
Fig. 29.4. After the application of the linear stapler, the lu-men are in communication. The dissection lines are securedby clamps. Thus, a complete myotomy of the cervical sphinc-ter is undertaken also and dysphagia is relieved.
Fig. 29.5. Positioning of the patient for the excision of anepiphrenic diverticle and myotomy of the lower esophagealsphincter. A 90 degree lateral position is used. Double sidedventilation is required. The monitor is placed to the front ofthe patient and the operation is performed from the posteri-or side. The first trocar is inserted through the 5th or 6th in-tercostal space of the posterior axillary line. The other trocarsare introduced posterior under direct vision.
Fig. 29.6. The pleura is incised just proximal to the divertic-ulum and the esophagus is mobilized circumferentially. It iselevated by means of a rubber sling. A large gastric tubewithin the esophagus facilitates control. Next the divertic-ulum is circumferentially isolated.

� H. Feussner et al.300
Fig. 29.7. The completely isolated sac of the diverticulum isnow fixed with two clamps and put under light traction. Thelinear stapler (preferable with a flexible tip) is now applied.It is essential, during this step of the procedure, to have alarge-bore bougie within the esophagus to avoid any nar-rowing of the lumen.
Fig. 29.8. Finally, the myotomy of the lower esophagealsphincter is performed through the thoracic approach. Itshould be extended sufficiently caudally to reach the stom-ach. The myotomized area can be covered by a mobilizedpatch of the gastric fundus.
Fig. 29.9. The long, extramucosal myotomy of the esopha-geal muscle layer is performed in a similar way to lowermyotomy. With a large bore bougie in place, the esophaguscan be easily palpated. Accordingly, circular mobilization isnot required. The muscle layer, at the border between theupper and the middle third, is laterally elevated and incised.Any perforation of the mucosa is carefully avoided. The planebetween the muscle layer and the mucosa is recognized easi-ly at this level of the esophagus. The tip of a pair scissors iscautiously introduced into this plane. The muscle layer cannow be lifted up and dissected safely. The myotomy is con-tinued down the whole length of the esophagus. The muco-sal layer is not covered by a flap of any sort.

Minimal invasive treatment of esophageal motility disorders
� Long myotomy of the esophagusin diffuse esophageal spasm
The success of operation depends directlyupon the selection of patients. The operativetechnique is less demanding. The approach isthrough the right thoracic wall, the layer be-tween the muscle and the mucosa is identified.Then, the muscle layer has to be split com-pletely over the whole length of the esophagus.
� Cardiomyotomy with Thal (Dor)fundoplasty in achalasia
It is still a matter of debate whether surgicaltreatment of achalasia should be performedtransthoracically or via the abdominal route.Either access is possible. Similarly, the neces-sity of an additional anti-reflux procedure isstill in question. Currently, it appears mostconvincing that it may be superfluous if thetransthoracic approach has been chosen butnecessary if the transabdominal access is pre-ferred. The port sites are demonstrated in Fig-ure 29.10. Usually, 4 trocars are required. Mostinfrequently, a 5th trocar is advisable. Thetherapeutic aim is to relieve dysphagia. Thiscan only be achieved by complete dissection ofall muscle fibers within the esophagogastricjunction. This means complete myotomy of notonly the esophageal muscle layer but also ofthe proximal parts of the so called Willis loopof the gastric fornix.The left lobe of the liver is a retractor for
optimal exposure of the esophagogastric junc-tion. Both pillars of the esophageal hiatus areimportant landmarks. The junction is coveredby a fat pad of varying thickness which has tobe split or resected. Damage to the vagus nervehas to be carefully avoided. Thus, the musclelayer can be exposed. Myotomy is initiatedwithin the area of the proximal gastric wall.The muscle layer is thicker, and the piane be-tween the musculature and the mucosal layeris identified more easily here than at the eso-phagus. Perforation of the mucosa can beclosed here more safely. However there isgreater vascularity in this area. Accordingly, a
few clips may have to be applied. As soon asthe plane has been entered successfully, the re-maining myotomy is usually possible withoutany difficulties. One further critical point hasto be mentioned. At the transition between thethickened muscle layer of the lower esophagealsphincter and the thinner and dilated wall ofthe body of the esophagus, complete myotomyis of particular importance though the risk ofperforation is slightly higher. Having per-formed the myotomy, it should be checked forcompleteness. The most reliable way to do thisis to perform intraoperative endoscopy. Alter-natively, a dilation tube can be inserted and in-
29 Minimal Invasive Surgery of the Esophagus � 301
Fig. 29.10. Port sites for laparoscopic myotomy with fundo-plasty. After having established the pneumoperitoneum, thefirst 10 mm trocar is inserted via a paraumbilical incision.Further trocars are introduced under direct vision. The10 mm trocar for the telescope is positioned below the leftcostal margin medial to the midclavicular line. A trocar isplaced below the right costal margin in order to elevate theleft lobe of the liver. The fourth trocar is used for the inser-tion of the instruments of the right hand of the surgeon.The surgeon is positioned on the right side of the patient.As usual in all procedures in the upper abdomen, a 30 de-gree telescope is preferred.

� H. Feussner et al.302
Fig. 29.11. Myotomy. The cardiomyotomy should extendabout 2 cm onto the gastric fundus and about 4 cm of thedistal esophagus. The plane between the mucosa and themuscle layer is best identified at the lowermost point of themyotomy on the anterior gastric wall. The muscle layer ofthe stomach is quite strong and well vascularized and themucosa is somewhat thicker and stronger than the esopha-geal mucosa. Accordingly, the first critical step of the myo-tomy is performed more easily here than in the esophagealwall. As soon as the plane has been correctly identified,myotomy can now be continued cranially without any diffi-culties. If bleeding occurs from the muscle layer or mucosalvessels, they are usually meaningless. They should not bestopped by electrocautery to avoid mucosal lesions. Some-times, swabs containing POR 8 may be used to stop thebleeding. At any rate, myotomy has to be accomplished com-pletely. In case of doubt, intraoperative endoscopy may behelpful.
a
Fig. 29.12. Fundoplasty. Beginning from the lowermost pointof myotomy, a patch of the gastric fundus is covered eitherwith running or interrupted stitches onto the area of the myot-omy. In the first step, the left edge of the muscle slit is sutured(a). Correspondingly, the right side will be fixed next. It isusually not required to mobilise the great curvature (b).
b

sufflated carefully. This makes muscle fibersvisible if any remain intact.The fundoplasty (Dor, Thal) is created next.
First, the left muscle edge of the myotomy issutured to a corresponding fundic fold. This iscommenced from the lowermost point of myo-tomy using interrupted or continuous stitches.Then, another fold of the fundus, slightly tothe left of the previous one, is taken and su-tured to the right edge of the myotomy. Inmost cases, the gastric fundus does not needto be mobilized. Finally, a nasogastric tube isinserted for 1–2 days.
� Comment
There is rarely a convincing indication for longmyotomy, performed either open or thoraco-scopically. Good results can be expected if theindication is very convincing. Accordingly,myotomy should be considered as an interven-tion which should be performed only in cen-ters with particular expertise. Since the opera-tion, per se, is simple to perform, the minimalaccess technique almost certainly will becomethe standard procedure.This holds true for cardiomyotomy as well.
The surgical option, being significantly less in-vasive now, has become very attractive in com-parison to pneumatic dilation or alternativeconservative treatment.
Antireflux surgery
The positioning of the surgical team and ofthe equipment is identical to cardiomyotomy.After elevation of the left liver lobe, the
greater curvature of the stomach is mobilized.This mobilization also includes the dorsal ad-hesions of the stomach. This facilitates the dis-section of the left pillar of the esophageal hia-tus. Dissection is then continued from theright side. The part of the peritoneum whichcovers the right crus and the anterior aspect ofthe esophagogastric junction is split. The ante-rior branch of the vagus nerve has to be pre-served carefully.
In the line between the right crus and thesmaller curvature of the stomach, a retroeso-phageal tunnel is created. In most cases, thiscan be done bluntly with the use of a swap.Reduction of the hiatal hernia is achieved bypulling the stomach gently into the abdomen.The esophagocardiac junction is elevated by ahook or a rubber band. Thus, the posteriorjunction of the crura is exposed and may nowbe properly prepared for the posterior hiato-plasty.Prior to the shaping of the wrap, the gap in
the hiatus is narrowed (posterior hiatoplasty).A large gastric tube is inserted into the stom-ach via the esophagus. The esophagogastricjunction is elevated to get a good view of theposterior aspect of the hiatus. Depending uponthe size of the hiatus, 1–3 non-absorbable su-
29 Minimal Invasive Surgery of the Esophagus � 303
Fig. 29.13. Port sites for laparoscopic fundoplication. Thefirst trocar is inserted via a paraumbilical incision. The 30 de-gree telescope will now be introduced to position the follow-ing ports under optical control. The second trocar which lateron will be used for the telescope is inserted below the leftrib arch between the medioclavicular line and the xyphoid.The third 10 mm trocar which is required for the elevationof the liver is localized in the medioclavicular line on theright side just below the rib arch. The fourth trocar is usedwithin the left abdomen, laterally to the umbilical trocar. Inmost cases, another 5 mm port is helpful which should beinserted between the right and umbilical trocar.

� H. Feussner et al.304
Fig. 29.14. Mobilization of the greater curvature. A really“floppy” tension free cuff can only be obtained if the greatercurvature has been mobilized generously before. Accordingly,this has to be performed in open as well as in laparoscopicfundoplication. Beginning from the lowermost point (at theborder between left and right gastroepiploic artery), the gas-trosplenic ligament will be opened in an avascular area anddissected up to the fornix of the stomach. The short gastricvessels tend to bleedings which are difficult to control. Bilat-eral ligature with double clips is, therefore, recommended.Prior to the dissection, the vessel should be additionally co-agulated. It is of particular importance to warrant the safeapplication of the clips, since these might easily slip offwhen the cuff is pulled through the retroesophageal tunnellater on. Alternatively, linear staplers (vascular magazine) orthe ultrasound device can be used. Dissection in the upperpart of the fundus has to be performed with particular cau-tion, since branches of the splenic artery supplying the dor-sal gastric wall may occur. Dissection of the left side is com-pleted by the exposition of the whole left crus of the dia-phragm including the posterior commissura.
Fig. 29.15. Exposition of the right crus of the diaphragmand retroesophageal mobilization. The right crus of the dia-phragm is exposed by splitting peritoneal layer and by re-moving the paracardiac fat pad. The peritoneum is split in acurved line from the right crus to the left crus. Mobilizationof the posterior esophageal wall is started from the rightside bluntly by using the scissors. Care has to be taken topreserve the dorsal branch of the vagus which usually is leftout of the wrap.

tures (2-0) are inserted. Any narrowing of theesophagus has to be strictly avoided. Other-wise, persistent dysphagia may occur even ifthe wrap is constructed in a “floppy” way.The wrap is constructed using the anterior
wall of the gastric fundus. From the right side,a suitable instrument is passed behind the eso-phagus to the left side. We use a hook or agrasping forceps with a flexible tip. The instru-ment is fixed to the anterior gastric wall about2 cm to the right of the greater curvature. It ispulled back to the right side, thus moving theanterior fundic wall behind the esophagus tothe other side of the esophagocardiac junction.This movement is supported by pushing thefold gently by a grasping forceps from the leftside. As soon as the fundic fold appears on theright side of the esophagogastric junction, it
should remain in position without fixation. Ifit tends to slip back, this suggests the previousmobilization of the fundus has been insuffi-cient.The wrap is sutured with three non-absorb-
able sutures. The lowermost stitch also incor-porates the anterior gastric wall in order toprevent slippage of the wrap. Finally, the leftedge is secured by two additional sutures.Thus, a so called 3-point support of the wrapis achieved which should prevent “slippage”.
� Comment
Considerable data are available to judge therole of laparoscopic fundoplication. It has beenclearly demonstrated that morbidity and mor-
29 Minimal Invasive Surgery of the Esophagus � 305
Fig. 29.16. Narrowing of the hiatus. With an additional hookor by the means of rubber band, the esophageal junction iselevated, which gives good exposure of the posterior cruraof the diaphragm. The hiatus is now narrowed (posterior hia-toplasty), using several non-absorbable interrupted sutureswhich are knotted extracorporally. It is of utmost importance,to preserve sufficient width of the hiatus, which is achievedby a bougie of at least 50 French. In case of a too narrowhiatoplasty, severe dysphagia may be induced, even if thewrap has been shaped in a floppy way.
Fig. 29.17. Retroesophageal pull-through of the anteriorgastric wall. The very point of the anterior wall of the gastricfundus, which will be pushed during the open operationwith the middle finger to the right side, is now fixed to thetip of the hook. Alternatively it may be fixed by means offlexible grasping forceps. By gentle traction from the rightside, and simultaneous support from the left side, the ante-rior gastric wall is passed through behind the esophagus.

� H. Feussner et al.306
Fig. 29.18. Closure of the cuff. The wrap is now made withthree non-absorbable single sutures. The lowermost suturealso incorporates the anterior gastric wall. Once the wraphas been made, it should be checked to see if it is loose en-ough using a 12 mm device (e.g. the hernia stapler). If the12 mm device can be inserted without difficulties into thespace between the wrap and the anterior gastric wall, it isregarded as floppy enough.
Fig. 29.19. Completed fundoplication. Finally, the left edgeof the fundoplication is secured by two single sutures. Thus,the wrap is protected by a three-point support (lesser omen-tum on the right side, fixation to the anterior gastric wall inthe middle, and the so-called “Flankennähte”) on the leftside against slippage. The large bougie is replaced by a nor-mal naso-gastric tube, which should remain for one or twodays. Optionally, abdominal drainage may be positioned for24 h.

tality are not increased by the use of the newtechnique. On the basis of current follow-ups,the functional results are, at least, equal tothose of open operations. Though controlledstudies are not yet available to demonstrate aclear superiority, there is no doubt that laparo-scopic fundoplication has become the treat-ment of choice in all major centers.
Excision of benign tumors
Most benign tumors of the esophagus are leio-myomas. Provided that no preoperative endo-scopic biopsy has been attempted, they cannearly also be removed easily without openingthe esophageal mucosa. It is advisable to per-form intraoperative endoscopy. This helps toidentify the exact position of the tumor. The
access is identical to that for long myotomy. Ifthe tumor is located anterior or on the right, itis sufficient just to split the covering muscle toexpose the tumor and to dissect it by blunt orsharp dissection. If the tumor is localised pos-teriorly or on the left of the esophagus, theesophagus has to be mobilised before resectionis undertaken. After the removal of the tumor,the muscle layer should be closed by interrupt-ed sutures.
� Comment
Thoracoscopic resection of small benign tu-mors of the esophagus seems to be advanta-geous, at least from the theoretical point ofview. However, it is still too early to give a reli-able statement about its true value.
29 Minimal Invasive Surgery of the Esophagus � 307
Fig. 29.20. Exposure of the esophageal tumor. The leiomyo-ma was localized by intra-operative endoscopy at the levelof the azygos vein. After careful mobilization, the azygos
vein is divided using the vascular stapler. The esophagealmuscle layer grasped directly above the tumor and is incised.

Minimally invasive proceduresin esophageal carcinoma
� Thoracoscopic esophagectomy(squamous cell carcinoma)
This procedure should be carried out by a sur-gical team which is familiar with open thoracicand esophageal surgery. A complete set of in-struments for the open approach should beready for use. The patient is positioned in theleft lateral position, more inclined to the posi-tion than is usual for right-sided thoracotomy.A precondition for successful thoracoscopy isventilation with a double lumen insufflationtube. This allows the right lung to be collapsedand insufflation of CO2 is not required. Thefirst trocar is inserted below the shoulderblade through the 5th intercostal space of theposterior axillary line. Safer insertion is pro-
vided by using an optical trocar. The furthertrocars are then inserted under visual control.Usually, 5 trocars are required.Adhesions of the pleura are dissected, fol-
lowed by a meticulous exploration of the tho-racic cavity. The lung is pushed aside by asuitable retractor, thus exposing the posteriormediastinum.An incision in the mediastinal pleura is
made parallel to the esophagus in two linesalong the right edge of the trachea and thespine. The azygos vein is carefully mobilizedand double-clipped on both sides and divided.However, it is possible to perform the divisionwith a linear stapling device (vascular staples).Right-sided intercostal veins leading to theazygos vein and the thoracic duct are also di-vided between double clips. Careful prepara-tion is of great importance, since bleedingfrom inadequately clipped veins is difficult tocontrol. This makes further dissection more
� H. Feussner et al.308
Fig. 29.21. Extirpation of the tumor. The anterior musclelayer is completely split. The lower edge of the tumor is ele-vated by grasping forceps, which allows us to divide it fromthe mucosal layer.
Fig. 29.22. After removal of the tumor, the muscle layer isclosed, either with interrupted sutures or running sutures(3-0).

29 Minimal Invasive Surgery of the Esophagus � 309
B D
F
A C
TV
E
TV
G
Fig. 29.23. Positioning of the surgicalteam of the equipment for thoraco-scopic mobilization of the esophagus(A: surgeon, B: assistent, C: camera-man, D: scrubnurses, E: anaesthesist,F: instruments for the thoracoscopy,G: instruments for thoracotomy).
Fig. 29.24. Port sites for thoracoscopic mobilization of theesophagus. First trocar in the mid axillary line through the5th intercostal space. A 30 degrees telescope is used. Lungretractors are inserted through the 3rd and 8th intercostal
spaces in the anterior axillary line using 5 mm trocars. Two10 mm operating trocars are introduced through the 5th and7th intercostal space in the posterior axillary line.

� H. Feussner et al.310
difficult. The mobilisation of the esophagus iscontinued stepwise on the aortic aspect usinganother hook. Small tributaries to the esopha-gus are divided between clips. As far as possi-ble from the tumor preferable immediatelyabove the diaphragm, the esophagus is mobi-lized, and gentle traction is exerted using arubber sling. After complete dissection fromthe aorta, the mobilisation is continued alongthe left side of the mediastinal pleura and thepericardium. Lymph nodes below the trachealbifurcation are removed en bloc. The upperthird of the esophagus is then mobilized paral-lel to the membranous part of the trachea. Theleft trunk of the vagus is preserved in itscourse until it reaches the left main bronchus.Thus, the whole intrathoracic segment of theesophagus is isolated including the adjacenttissue and lymph nodes. Thoracic drains areinserted through both of the lower trocar sites.Finally, the trocars are removed and the holeswithin the short wall are closed by sutures.The patient is repositioned and the esophagusis severed via a cervical incision. The specimenis then removed transabdominally. Esophago-intestinal continuity is restored by a gastric in-terposition and esophagogastrostomy.
Fig. 29.25. The mediastinal pleurais incised along the vertebrae, thetrachea and the pericardium. Theazygos vein is divided with a linearstapler. The right-sided intercostalveins are dissected near their junc-tion with the azygos vein and di-vided between clips. In the phreni-cocostal space, the thoracic duct isidentified between the aorta andthe azygos vein. After double clip-ping, it is severed as well.
Fig. 29.26. Dissection of the mediastinum inferior to the bi-furcation of the trachea. The soft periesophageal connectivetissue, fat and lymph nodes are removed en bloc.

� Endodissection of the esophagus(adenocarcinoma)
For this endodissection, the patient is posi-tioned in the supine position. The head isturned to the right side and extended for 40degrees. It is essential to have the patientshead positioned as much as possible to the leftside to create sufficient space for the handlingof the rigid endoscope. The abdominal part ofthe operation is performed from the right sideof the patient. The surgeon performing endo-dissection is positioned behind the leftshoulder of the patient.An oblique cervical incision parallel to the
anterior edge of the sternocleidomastoid mus-cle is made and the omohyoid muscle is cut.After careful dissection of the left recurrentlaryngeal nerve the cervical esophagus is ex-posed and hold by a rubber sling. During thisstep of the operation, the esophagus is intu-bated with a large gastric tube. The posterioresophageal wall and the upper part of esopha-gus are dissected using a blunt technique. Thetip of the endodissector is now introduced intothe anterior mediastinum. The anterior eso-phageal wall is the anatomic landmark used
29 Minimal Invasive Surgery of the Esophagus � 311
Fig. 29.27. After mobilization ofa tumor-free segment of the eso-phagus, further mobilization isachieved using a flexible retractor.Careful preparation is essential inthe region of the pulmonary veinand the left main bronchus. Themembranous part of the mainbronchus is often prominent dueto the cuff of the endotrachealtube.
Fig. 29.28. After complete mobilization, all adjacent organsare easily seen.

� H. Feussner et al.312
Fig. 29.29. Positioning of the surgical team for endodissec-tion of the esophagus. The surgical team for the abdominalpart of the operation are positioned in the conventional way.The endoscopic surgeon stands at the level of the leftshoulder of the patient; the screen is on the opposite side.Left – laterally to him – is his scrubnurse with the instru-ments for the endoscopic dissection (A: endoscopic surgeon,B: abdominal surgeon, C: assistants, D: scrub-nurses, E: an-aesthesist).
Fig. 29.30. Dissection of the anterior esophageal wall. Thecervical esophagus is isolated through an oblique cervical in-cision, according to the conventional technique and con-trolled by a rubber sling. A modified mediastinoscope is in-troduced and placed anterior to the esophagus. Step by step
space between the posterior wall of the trachea and theesophagus is created by means of the tip of the instrument.Strands of connective tissue and small vessels are coagulatedand dissected bluntly or using the scissors (Insert: tip ofmodified mediastinoscope, so called “bulls-head”).
E
A
D
C
C
B
D

since it is identified more easily than adjacentstructures. By the advancement of the thick-ened head of the instrument the paraesopha-geal tissue is put under traction which facili-tates dissection using scissors or electrocau-tery. Proceeding step by step, the trachealbifurcation is identified as another importantanatomical landmark. Lymph nodes of thisarea as well as paratracheal lymph nodes areeasily identified and removed.The left recurrent nerve is easily recognized
to the left of the trachea. Electrocautery shouldbe avoided near the nerve to prevent thermallesions of the nerve. After complete mobiliza-tion of the anterior aspect of the esophagus,the device is drawn back. The tip is rotated180 degrees and inserted again into the medi-astinum, now being positioned between theposterior esophageal aspect and the spine. Dis-section of the posterior wall is easy. But dissec-tion becomes more difficult on the left side,because of close adhesion to the left mainbronchus which requires division as well astissue bridges to the descending aorta. On theright side, the azygos vein has to be handledcarefully. As on the anterior aspect, the poste-
29 Minimal Invasive Surgery of the Esophagus � 313
Fig. 29.31. Dissection of the anterior esophageal wall.Lymph nodes below the tracheal bifurcation are exposed andexcised.
Fig. 29.32. Dissection of the posterior esophageal wall.The tip of the modified mediastinoscope is rotated for180� and is now advanced behind the esophagus.

rior dissection is continued until the abdom-inal surgeon is met at the hiatus. Lesions tothe visceral pleural are difficult to avoid. Thisis why we recommend placing thoracic drainat the end of the procedures.Collection of fluid and blood in front of the
endodissector requires continuous instillationof saline and aspiration.Endodissection is particularly suitable for
the mobilisation of the upper part of the eso-phagus. More distally, it is sometimes difficultto maintain the correct plane of dissection andperforations of the tumor of the esophagusmay occur. Finally, the cervical esophagus isdivided and removed in toto transabdominally.The esophagogastric anastomosis is performedin the usual way.
� Comment
Thoracoscopic esophagectomy for squamouscell cancer of the esophagus – though beingtechnically feasible – is still too time-consum-ing and too invasive to be considered accept-able as alternative to open transthoracic eso-phagectomy (Consensus Conference of the In-ternat. Soc. for Diseases of the Esophagus, Mi-lan 1995). Further evaluation and technical im-
provements are required. For the time being,thoracoscopic esophagectomy should be con-fined to controlled clinical studies. Accordingly,adequate informed consent, documentationand scientific evaluation is necessary in eachcase. The situation is different for distal adeno-carcinoma of the esophagus. Endodissectioncan be considered as a viable alternative toblunt transhiatal dissection, since the overallduration of the operation is shortened. Theincidence of cardiopulmonary complications isreduced significantly. From the oncologicalpoint of view it is of interest that lymph nodeharvesting within the mediastinum is facili-tated which has the potential to improve thesurvival rate.
314
Fig. 29.33. Dissection of the posterior esophagus wall.
Fig. 29.34. Simultaneous abdominal procedure. Through alaparotomy, the hiatus is split, the esophagogastric junctionincluding the crura of the diaphragm are mobilized, and thepericardial fat pad is resected. Complete mobilization of thedistal esophagus is accomplished between the endoscopicand the abdominal surgeon. The cervical esophagus is divid-ed and the esophagus is pulled down into the abdomen.
� H. Feussner et al.: 29 Minimal Invasive Surgery of the Esophagus

Hemorrhage and esophageal varices
� Introduction
Esophageal varices, ulcers due to reflux esopha-gitis, and Mallory Weiss lesions are the mostcommon causes of esophageal hemorrhage.Less common causes include esophageal tu-mors (both benign and malignant) and iatro-genic lesions following endoscopic or surgicalprocedures. In all these cases, endoscopic man-agement is the treatment of choice. To improveclinical outcome, a combination of variousspecialized endoscopic techniques may be re-quired.
� Indications
Endoscopic management is indicated in all in-stances of overt bleeding. In patients with hy-povolemic shock, initial volume resuscitationis important. In order to temporarily stop mas-sive variceal bleeding before endoscopy, phar-macotherapy and balloon tamponade using theSenkstaken Blakemore tube or the Minnesotatube may be needed.
� Contraindications
In the context of emergencies like massive bleed-ing, time consuming diagnostic procedures areunnecessary and only serve to delay definitivetreatment. However, it is necessary to obtaincertain key information such as patient bloodgroup and coagulation status. These can beevaluated simultaneously as the patient isbeing resuscitated.
� Instruments
– Gastroscopes with a large working chan-nel (3.7 or 6 mm) or with 2 channels forsimultaneous suction and treatment
– Two powerful suction pumps with largecontainers
– Water pump for flushing to improve visi-bility
– Injection catheters for sclerotherapy– Loaded clip applicator– Over-tube and guide-wire in the contextof single band ligation (Stiegman-Goff)
– Set for multi-band ligation (e.g. Six-shoo-ter, Speedband)
– Injection solutions: epinephrine dilutedwith normal saline (1 : 20000); N-butyl-2-cyanoacrylate mixed with lipiodol(0.5 ml : 0.8 ml); polidocanol 1% or othersclerosants according to local preferences.
� Patient position. Left lateral position.
� Special techniques
Identification of the actively bleeding site andsource is crucial. With continued bleeding, suf-ficient volumes of washing solutions and ade-quate suction (2 pumps) are necessary to en-sure adequate visibility.
1. Stopping the hemorrhage– Sclerotherapy (Fig. 30.1)– Obliteration of bigger varices (Fig. 30.2)– Clip application (Figs. 30.3–30.6)
2. Eradication of esophageal varices– Perivascular injection of sclerosants(Figs. 30.7–30.9)
– Band ligation (Figs. 30.10–30.14).
Endoscopic Technique in the Treatmentof Esophageal DiseasesY. I. Gallinger, M. Rehner, F.M. Steichen, N. Soehendra
30

� Y. I. Gallinger et al.316
Fig. 30.1. Injection treatment for bleeding esophagealvarices. This technique is also used for other types of hemor-rhage. The injections are made around the lesions; the se-quence of injection is from distal to proximal, so that onehas better visibility. In non-variceal bleeding, 0.05% epi-nephrine solution alone can be injected around the lesion to
create a tamponade effect for initial hemostasis. If the tissueat the bleeding site is indurated due to scars or tumor infil-tration, the injection technique might be more difficult orless effective; one should then try alternative techniquessuch as argon plasma coagulation or clipping.
Fig. 30.2a, b. Intravascular injection of a tissue adhesive issafer than sclerotherapy in the context of severe varicealbleeding. The volume injected each time should be limited
to 0.5 ml to reduce the risk of distal embolizations. An alter-native technique is rubber band ligation.
a b

30 Endoscopic Technique in the Treatment of Esophageal Diseases � 317
Fig. 30.3. Non variceal bleeding such as Mallory-Weiss le-sions and ulcers due to reflux esophagitis can be reliablystopped by application of clips. This technique is performedwith a special delivery system through the working channel
of the endoscope. If several clips are needed, several loadedapplicators should be kept ready as a precaution. Left figure:system in position; right figure: the technique of correctlytightening the clip.
Fig. 30.4a, b. Mallory-Weiss lesion with clipping of a largeartery. Sometimes the bleeding artery itself can be graspedwith a clip (a) and the clip applied directly (b). The necessity
for more clips proximal or distal to the artery should bedecided individually.
a b

� Y. I. Gallinger et al.318
Fig. 30.5a–c. Mallory-Weiss lesion with clip application. Inmost cases, direct occlusion of a bleeding artery is not possi-ble. One could then grasp the mucosa on either sides of thelesion with the clip in order to occlude the vessel (a).
Whether one should grasp both sides of the adjacent muco-sa (b) or only one side (c) depends on the individual situa-tion. The important points are occlusion of the bleeding ves-sel and anchoring the clip securely in the tissue.
a b
c

30 Endoscopic Technique in the Treatment of Esophageal Diseases � 319
Fig. 30.6a,b. Mallory-Weiss lesion with clip-application. The application of a clip isalways more difficult when the bleeding vessel is seen on lower sector of the en-doscopic picture. Because of the technical conditions of the delivery system, a safepositioning is often not possible (a). In these cases the whole endoscope should berotated by 190� to get the bleeding lesion into the upper segment of the picture(b). Thereafter one can commence clip application.
Fig. 30.7a, b. Eradication of esophageal varices. The varices inthe distal esophagus are at risk for hemorrhage because theyrun just beneath the epithelium (a). The aim of the treatmentis to cause tissue fibrosis and perivascular induration usingchemical solutions (e.g. polidocanol 1%). The concentration of
these solutions cannot be too high because otherwise tissuenecrosis with perforation may occur. Injections are made onboth sides of the vessel with volumes of 1–2 ml until tissueswelling is seen (b). The treatment must be repeated atweekly intervals until the varices are completely eradicated.
a
b
a
b

� Y. I. Gallinger et al.320
Fig. 30.8. Eradication of esophageal varices. The treatmentstarts at the distal part of a varix. Using this technique, mi-nor bleeding after injections is common but does not affectthe further treatment of the more proximal segments.
Fig. 30.9. Eradication of esophageal varices. One should en-sure accurate perivascular and subepitheal injections. Intra-vascular injections are not effective because the sclerosant isdiluted by the rapid blood flow and will also predispose tosystemic side-effects. Deeper injections can cause necrosis ofthe wall with possible perforation; stenosis due to scars maydevelop later.

30 Endoscopic Technique in the Treatment of Esophageal Diseases � 321
Fig. 30.10a,b. Eradication of esophageal varices by rubber-band ligation. Instrument for single-band application (Stieg-man-Goff ) (a). Using this technique, over-tubes are necessarybecause each rubber-band must be loaded and tightenedseparately before application (b).
Fig. 30.11a–d. Eradication of varices by rubber-band liga-tion using instruments for multiple-band applications (Six-shooter or Ten-shooter). The endoscope need not be with-drawn prior to each application and hence over-tubes areunnecessary (a, b). By the application of six or more bands
during one session, it is possible to ligate the varices ade-quately. The placement of the rubber-bands is managed by aspecial application set which is fixed to the working channelof the endoscope (c, d).
a
c d
b

� Y. I. Gallinger et al.322
Fig. 30.12. Eradication of esophageal varices by rubber-bandligation. The ligations are performed from distal to proximal,starting with the biggest vessel. Ligations are made in spiralfashion to avoid later strictures.
Fig. 30.13. Eradication of varices by rubber-band ligations.The appearance after treatment.

� Complications
� Intractable hemorrhage. Management: surgicaltreatment. This is associated with high morbid-ity and mortality.
� Recurrent bleeding. Recurrent bleeding oc-curs mainly during the first 3 to 5 days afterinitial successful hemostasis. It is usually ob-served after sclerotherapy of varices. In thiscase, endoscopic obliteration of the varices
using tissue adhesive (e.g. N-butyl-2-cyano-acrylate 0.5 ml with lipiodol 0.8 ml) is usefulin preventing further recurrences.In Mallory-Weiss lesions, recurrent bleeding
may occur with deeper tears. Application ofclips should be used after initial injections ofepinephrine (1 : 20000 dilution).
� Perforations. Prevention: Injections should belimited to the submucosa by selecting the cor-rect needle length and controlling the depth ofneedle insertion. The volume per injectionshould be limited to 1–2 ml.Treatment: Close clinical monitoring is nec-
essary for early detection of mediastinitis. If indoubt, fluoroscopic examination with water-sol-uble contrast may be used. Conservative treat-ment with antibiotics and parenteral nutritionmay be successful. If necessary, surgical treat-ment should be carried out. As an alternativeto surgery, stenting has been used successfullyin selected cases.
� Strictures. Strictures may occur in a smallnumber of cases after sclerotherapy. They re-sult from deep tissue necrosis of the esopha-geal wall due to incorrect injection techniques.Treatment: Endoscopic dilatation.
� Embolic complications. They may occur afterinjections of excessively large volumes of N-bu-tyl-2-cyanoacrylate during obliteration of vari-ces. Prevention: Injection of smaller volumes(per injection: maximum volume of 0.5 ml foresophageal varices and 1 ml for gastric varices).
30 Endoscopic Technique in the Treatment of Esophageal Diseases � 323
Fig. 30.14a,b. Eradication of esophageal varices by rubber-band ligations. After a couple of days, thrombosis andshrinking of the varix occurs. Demarcation of the tissue be-gins after 1–2 weeks, leaving flat lesions (a). A new layer ofepithelium then forms (b). If necessary, additional treatmentscan be started after 4 days. Further sessions of variceal liga-tion may be continued at weekly intervals until the eradica-tion is achieved. For many patients additional treatment withsclerotherapy may be necessary to obtain adequate fibrosisof the esophageal wall.
a b

Foreign bodies and bolus obstruction
� Introduction
This problem arises mainly in children whoswallow toys and other objects. In adults, bonefragments, fish-bones, parts of prostheses, orneedles kept between the lips by tailors may befound. Bigger and bulkier foreign bodies areobserved in psychiatric patients and in thecontext of self-destructive manipulations (e.g.in prisoners). These foreign bodies can befound in the stomach or impacted in the eso-phagus, such as coins in smaller children. Bo-lus obstruction may be a consequence ofasymptomatic disturbances of the esophagealmotility. Bolus obstruction may also occur indeep reflux-related esophageal ulcers or in ste-notic scars. The occlusion of the esophageal lu-men is very often followed by painful spasmsthat cannot be stopped with medications. En-doscopic removal of foreign bodies is the treat-ment of choice. If this is not available, fluoro-scopy guided removal of foreign bodies usingcatheters (e.g. Foley catheters) can be tried.Open or minimally invasive surgery is limitedto rare situations.
� Indications
Every obstructing foreign body should be re-moved as soon as possible. Sometimes it ispossible to push it into the stomach, as in thecase of meatballs. However, it is absolutely nec-essary to extract all objects that might damagethe intestinal wall or block the passage at areaswith a narrow lumen (e.g. pylorus and ileoce-cal valve). Mini-batteries should be removedbecause of possible poisoning.
� Contraindications
Small, non dangerous foreign bodies which areexpected to pass out spontaneously do notneed further treatment. The passage of theseforeign bodies may be monitored using fluoro-scopy if they are radio-opaque.
� Preliminary procedures
– Fluoroscopy is used to identify the diame-ter and configuration of the foreign bodyin order to guide the choice of instru-ments. During fluoroscopy of the thorax,the cervical esophagus must be observedcarefully. The use of contrast such as gas-trografin may be helpful in finding nonradio-opaque objects.
– Premedication: Analgesia-sedation; forchildren and non co-operative patients,general anesthesia.
– Position: Left lateral.– Monitoring and instrument-check.
� Instruments
Gastroscopes with large working channelsshould be favored. Additional equipment: over-tube; collecting sacs or umbrellas to protect theesophageal wall from injuries; different types offorceps and loops; Dormia basket; accessoriesto cut or break bigger boluses or bezoars.
� Special technique
– Extraction with forceps, loop, and Dormiabasket (Fig. 30.15)
– Extraction with protection by cap andumbrella (Figs. 30.16–30.18).
� Y. I. Gallinger et al.324

30 Endoscopic Technique in the Treatment of Esophageal Diseases � 325
Fig. 30.15a–c. Only smooth foreign bodies that do not in-jure the esophageal wall should be extracted without protec-tive accessories. For this purpose a cap fixed to the tip ofthe endoscope is normally sufficient. An over-tube is usedwith protective accessories; the diameter of the protective
accessory is much larger than the foreign body and can helpto extract foreign bodies like prostheses, safety-pins, or forks(a–c) without injuring the proximal parts of the esophagus.Extraction of the foreign body can be performed using for-ceps or snares.
Fig. 30.16a,b. An umbrella fixed to the tip of the endo-scope is a different type of protector. During the insertion ofthe instrument, the umbrella is still folded. After positioningthe instrument in front of the foreign body, the umbrella ismoved forward by grasping a fixed bow (a). The differentumbrella diameters allow the safe extraction of even largerand dangerous foreign bodies (b).
a b c
a b

� Complications
� Perforation. Injury of the esophageal wall withperforation is the most serious complication.Prevention: In all cases with possible inju-
ries and a need for repeated intubations, over-tubes should be used.Treatment: Superficial mucosal injuries do
not require any active treatment. When deeptears occur, perforation with its attendant riskof mediastinitis should be checked for byradiography using water soluble contrast. How-ever, CT is a much more sensitive method fordetecting free air. Most of the smaller perfora-tions can be treated conservatively by clips, pa-renteral nutrition, and antibiotics. Larger per-forations will need surgery.
� Aspiration. To prevent aspiration of foreignbodies during endoscopic extraction, over-tubesand/ or net retriever baskets are used. In casesof high risk for aspiration, especially in chil-dren, general anesthesia should be used.
� Follow-up
In uncomplicated cases, normal diet can bestarted early and no further follow-up is neces-sary.
� Y. I. Gallinger et al.326
Fig. 30.17. For bolus obstructions that are already presentfor a couple of days, one must avoid pushing the bolus dis-tally with the endoscope. There may already be early necro-sis of the esophageal wall, with an attendant risk for per-foration if the bolus is pushed distally without visualizingthe lumen.
Fig. 30.18. Hard meatballs or phytobezoars can often begrasped and extracted with a Dormia basket or with a snare.Rat-tooth forceps or nets are adequate to extract foreignbodies such as coins, mini-batteries, or small toys in children.Soft meatballs sometimes can be removed with suction usinga cap. Very hard big balls or bezoars should be maceratedwith special instruments under endoscopic control (e.g. Bezo-tome, Bezotriptor).

Resection of tumors
� Introduction
The majority of benign tumors arise from thesubmucosal layer. Tumors arising from theepithelium (e.g. adenoma, papilloma) are notfrequent. They are mainly located in the distalesophagus. Smaller submucosal tumors can beresected endoscopically, if the location is con-firmed by endosonography (EUS). One mustconsider the risk of perforation. The endo-scopic resection of malignant tumors of themucosa (EMR or Endoscopic Mucosal Resec-tion) is gaining popularity. Long-term resultsare comparable with surgery. Prior to EMR,precise staging using EUS is necessary. BesidesEMR, different techniques of thermoablationare used (eg. electrocautery, laser ablation, andphotodynamic therapy).
� Indications
– Flat and elevated malignant tumors in allparts of the esophagus limited to the muco-sa [stage T1m, N0, M0]
– Benign mucosal tumors– Selected cases of benign tumors arisingfrom the submucosa or from the muscu-laris mucosa.
� Contraindications
Endoscopic resection should be avoided in alltumors arising or infiltrating beyond the sub-mucosa. Large tumors (diameter greater than3–5 cm) have a higher risk of perforation afterendoscopic resection and should be managedindividually.
� Preliminary examinations
Endoscopy with sufficient number of biopsies;EUS for accurate staging and, if necessary, EUSguided fine needle aspiration biopsy (FNA);coagulation tests.
� Pretreatment preparations
– Monitoring and instrument check– Premedication: Analgesia-sedation– Position: Left lateral.
� Instruments
Gastroscopes with large or dual working chan-nels are helpful; HF generator for electrocau-tery; injection needles with solutions for mu-cosal elevation and treatment of hemorrhage(epinephrine 1 :20000); band ligator and trans-parent cap for suction of the mucosa to the in-strument tip; snares for cutting; forceps; needleknife for 2-channel technique; chromoendosco-py using solutions such as lugol iodine, indigocarmine and methylene blue to stain the tumormay be needed.
� Special technique
– Tumor resection with submucosal injec-tion and loop; mucosa aspiration withcap (Figs. 30.19–30.22)
– Tumor resection with band ligation (Fig.30.23)
– Tumor coagulation with argon plasma co-agulation, laser ablation, or PDT.
30 Endoscopic Technique in the Treatment of Esophageal Diseases � 327

� Y. I. Gallinger et al.328
Fig. 30.19a, b. Endoscopic mucosal resection (EMR). The mu-cosa containing the tumor is elevated by injection of thesubmucosa with 0.05% epinephrine solution. This elevationof the tissue makes it easier to grasp the entire tumor witha snare (a). Simultaneously, the liquid cushion protects thewall from thermal injuries. If needed, the tumor margins canbe demarcated using chromoendoscopy. Lugol’s solution is
used for squamous cell tumors, while an adenocarcinoma isstained with methylene blue or indigocarmine (c). EMR canalso be performed without preliminary injections; with thistechnique, it is helpful to let the wall collapse while suckingthe air, with the intention to grasp a larger area of the mu-cosa within the snare (b). For resections, snares with stiffmonofilament wires should be used (d).
a b
c
d

30 Endoscopic Technique in the Treatment of Esophageal Diseases � 329
Fig. 30.20a,b. Endoscopic mucosal resection (EMR). To pre-vent perforation, the correct technique for cautery should beobserved. The snare must grasp only the mucosal and sub-mucosal layers. The submucosa is expanded by preliminaryinfiltration (a). After resection the muscularis propria may beexposed (b). It should remain unscathed.
a
b
Fig. 30.21. Endoscopic mucosal resection (EMR). Anothertechnique to ensure safe resection is the suction of the tis-sue using a cap. An asymmetrical snare made of braidedwire is preloaded in the inner gutter of the cap and graspsthe tissue layer after suction. For resection pure coagulationcurrent with 60 W power is used.

� Y. I. Gallinger et al.330
Fig. 30.22a,b. Endoscopic mucosal resection (EMR). Submu-cosal infiltration and suction can be combined (a,b). Thistechnique is an additional safety step to prevent perforations(Inoue technique).
Fig. 30.23a,b. Endoscopic mucosal resection (EMR). Rubber-band ligation can be used as an alternative technique to ele-vate the tumor from the surrounding tissue (a). The cut isperformed above the rubber-band. The rubber-band thenslips off, leaving behind an ulcer (b).
ab
a
b

� Complications
The most important complications are hemor-rhage and perforation.
� Hemorrhage. Prevention: Resect slowly stepby step, preferably using coagulation setting;preliminary band ligation of the tumor-bearingmucosa may be performed if feasible.Treatment: Injection of 0.05% epinephrine-
saline solution and clip application. Using co-agulation to stop the hemorrhage should beavoided.Technique of sclerotherapy, see p. 316.Technique of clip application, see p. 317.
� Perforation. Prevention: Infiltration of thesubmucosal layer with isotonic saline solutionand strictly limiting the resection to the sub-mucosa. When resecting benign submucosaltumors, the needle knife can be used to incisethe mucosa, followed by enucleation of the tu-mor.
Treatment: Smaller lesions can be treatedwith endo-clips (Fig. 30.24), parenteral nutri-tion and antibiotics. Close monitoring is cru-cial for the early detection of mediastinitis andpneumothorax. In the case of larger perfora-tions or suspected mediastinitis, open or mini-mally invasive surgery would be required.
� Follow-up
After EMR of larger mucosal lesions, the pa-tient may need to be kept fasted for a few days,depending on the size of the lesion and theclinical situation.Surveillance with biopsies of the scar and
surrounding areas should start 3 months laterin all cases of malignant tumors with R-0 re-sections. Standards for further managementand the value of additional tests such as EUShave not yet been established. In the case ofthermoablation of tumors, surveillance withbiopsies is mandatory after a shorter intervalto confirm complete removal.
30 Endoscopic Technique in the Treatment of Esophageal Diseases � 331

� Y. I. Gallinger et al.332
Fig. 30.24a–c. Endoscopic mucosal resection (EMR). Perfora-tion due to snaring of the muscle layer is a rare complica-tion. If the injury is small and the edges smooth, it can beclosed immediately using clips. In very small lesions whichare not completely transmural, one can grasp the edges ofthe mucosa or mucosa plus muscle layer using just one or
two clips (a). For larger lesions a row of clips is first appliedto the muscle layer (b). In between these clips a second rowis added joining the mucosa and submucosa (c). Careful fol-low-up after endoscopic treatment of perforations is neces-sary to detect early signs of mediastinitis.
a
b
c

Photodynamic therapy of tumors (PDT)
� Introduction
Photodynamic therapy is based on the interac-tion of light with a photosensitizer that is re-tained, preferentially and for longer periods oftime, by cancerous tissue compared with nor-mal tissue. This interaction generates cytotoxicmolecular reactions that result in tissue necro-sis. The photosensitizer is first injected intra-venously, followed 48 hours later by photoacti-vation with use of light that is transmittedthrough an optical fiber coupled to a cylindri-cal light diffuser. The light diffuser is intro-duced directly into the esophagus and posi-tioned according to the measurements of thelength of the lesion as determined during en-doscopy. This technique has been used in se-lected patients for the past couple of years. Ex-act indications and contraindications have notbeen fully evaluated. Small case series have re-ported an acceptable efficacy when PDT isused as palliation for advanced tumors. Com-pared to other forms of thermoablative treat-ment, there are no significant advantages. Amajor adverse effect is the problem of skinphotosensitivity which lasts for several weeksafter the PDT session.
� Indications
There is still a lack of data for appropriate pa-tient selection for PDT. Only preliminary rec-ommendations can be made. There is clinicalexperience with the following situations:– Superficial spreading tumors of the muco-sa [stage T1m]
– High grade dysplasia in Barrett’s esopha-gus, especially for patients at high surgi-cal risk
– Palliation of advanced non-resectable car-cinoma.
� Contraindications
– Resectable tumors arising from the sub-mucosa or those with deeper infiltration(stage T1sm and higher)
– Suspicious involvement of regional lymphnodes in tumors of operable patients.
� Preliminary examinations
Exact diagnosis of the tumor with endoscopicbiopsy; EUS±FNA for T and N staging.
� Special preparations
Injection of the sensitizer (e.g. Porfimer-Sodi-um 2 mg/kg i.v.) 48 hours before treatment;patient should be fasted for 12 hours beforetreatment; premedication and safety proce-dures according to standard recommendations.
� Instruments
A gastroscope with a large working channel,light generator, argon laser (630 nm wave-length), and an optical fiber coupled to a cyl-indrical light diffuser that is adapted to the ex-tent of the tumor, monitoring unit. A dye solu-tion to mark the borders of a spreading tumor(e.g. lugol iodine, indigo carmine, and methy-lene blue) may be required.
� Special technique
The tumor is identified at endoscopy. If it isnecessary to demarcate the tumor margins,chromoendoscopy is used. The light source ispositioned over the tumor and photoradiationperformed.
30 Endoscopic Technique in the Treatment of Esophageal Diseases � 333

� Complications
� Strictures have been reported to occur inaround 30%.Treatment: Endoscopic dilatation.
� Perforations are very uncommon.
� The ineffectiveness of the treatment must betaken into account.Due to the limited experience in small patient
populations, the extent of the risk for complica-tions cannot be accurately determined.
� Alternative therapies in advanced tumors
– Chemical destruction of the tumor by in-jection of concentrated alcohol or otherchemicals
– Laser ablation– Electro-thermocoagulation– Stenting.
� Alternative therapiesfor elective tumor eradications
– In high grade dysplasia of Barrett’s eso-phagus, an extended local eradication byargon plasma coagulation or Nd-YAG la-ser may be performed; this should be fol-lowed by long-term treatment with pro-ton-pump inhibitors (PPI).
– Focal high grade dysplastic areas can becompletely resected by EMR
– Extensive areas of multifocal high gradedysplasia may occasionally require surgery.
� Follow-up
There should be protection from light exposurefor 2 weeks. Surveillance biopsies should beperformed after 4 weeks and then at regularintervals.
� Y. I. Gallinger et al.334

Obstructions by malignant tumors
� Introduction
Endoscopic management is the treatment ofchoice in malignant tumors causing esophagealobstruction. For inoperable patients or unre-sectable tumors, endoscopic techniques are of-ten the definitive treatment. Alternatives forenteral feeding in these situations are percuta-neous endoscopic gastrostomy (PEG) or -jeju-nostomy (PEJ). Relief of obstruction can beachieved by different endoscopic techniquessuch as bougienage and placement of an endo-prosthesis, induction of tissue necrosis by theinjection of solutions such as alcohol, andthermoablation. These techniques are com-monly combined. We prefer the use of bougie-nage with subsequent stent placement. For ob-structive tumors of the cervical esophagus,there is an additional risk of fistulae formation(tracheo-esophageal fistula, esophago-mediasti-nal fistula). If fistulae occur, modified stentsare necessary in order to seal the fistulae.Injection and thermoablative techniques aremainly used for exophytic tumors prior tostent placement.
� Indications
All patients with stenotic tumors of the eso-phagus can be treated. The treatment may bedefinitive or may serve as a temporary mea-sure before surgery.
� Contraindications
The presence of severe cardiac or respiratorydecompensation which precludes the use of en-doscopic procedures and premedication.Advanced tumors without significant steno-
sis.
� Preliminary examinations
– Endoscopy is used to determine the ex-tent of the tumor and degree of stenosis.Biopsy is taken for tumor-typing.
– Screening for fistulae may be required (e.g.with bronchoscopy or radiography withwater soluble contrast).
– Tumor staging by EUS.
� Special preparations
– Premedication: Analgesia-sedation– Monitoring: Based on recommended stan-dards
– Prophylactic antibiotics (e.g. single doseprior to PEG)
– Positioning: left sided.
� Instruments
– Gastroscopes, guidewires, bougies, andballoon dilators as per management of be-nign strictures.
– Injection techniques: the use of needlessimilar to that in the treatment of hemor-rhage; solutions for tissue ablation e.g.absolute alcohol.
– Laser treatment: Nd-YAG laser; gastro-scope with a large working channel or 2-channel endoscopes to allow suctioning ofthe fumes generated during laser ablation.
– Stenting: Celestin-tubes of standard diame-ter (13 mm) or Baby-Celestin tube (11 mm);self expanding metal stents (Fig. 30.34). Forproximal cervical stenoses with fistulae, theuse of modified shortened Baby-Celestintubes (Fig. 30.35).
� Special techniques
– Dilatation (using guidewires and bougie-nage): Figs. 30.25–30.41
– Stenting (Figs. 30.30 a–c, 30.31 a–d, 30.37–30.40)
– Injection treatment– Laser application
Injections of chemical solutions or laser appli-cation generate tissue necrosis after a few days,thus widening the lumen. For injections var-
30 Endoscopic Technique in the Treatment of Esophageal Diseases � 335

ious solutions are used, but there is greater ex-perience with the use of absolute ethanol, iso-propanol, 3% polidocanol, and hypertonic sa-line (10–20%). These solutions are injected asmultiple small deposits (0.5–1 ml) within thetumors. These treatments only have a tempo-rary effect and should be repeated on demandor at short intervals. They are also often usedas preliminary treatment prior to bougienageand stenting. In the palliation of stenotic tu-mors, stenting should be added in order to re-lieve obstruction for a longer time. Varioustechniques in stent placement are available,similar to those used in the treatment of fistu-lae.
� Complications
� Hemorrhage. It can occur during dilatations.Generally it stops spontaneously, but it can betreated by sclerotherapy if necessary.
� Perforation. If perforation is suspected, fluoro-scopic examination using water-soluble contrastshould be performed immediately. Small lesionscan be treated conservatively with parenteralnutrition, antibiotics and, in certain cases,placement of a stent. For larger lesions, surgeryis safer.
� Stent migration. Stent migrations are treatedby endoscopic repositioning. For plastic stentsit is sometimes more effective to place a newstent with a larger diameter (possibly one witha larger funnel and an additional distal stopper).
� Tumor overgrowth. This can occur at boththe proximal and distal ends of the stent. Thetumor overgrowth can be treated by thermo-ablation or sclerotherapy. The treatment mayneed to be repeated depending on the clinicaleffect. Stent exchange is often more appropri-ate.
� Stent intolerance. It is mainly observed afterstenting of the cervical esophagus. Sometimesstent removal cannot be avoided. In that case,it has to be replaced by a nasogastric tube orPEG/PEJ. For uncovered metal stents, removalmay not be easy. The use of removable coveredstent is therefore recommended.
� Bolus obstructions. Bolus obstruction is pos-sible after stent placement. The treatment issimilar to other forms of bolus obstruction. Itmay be prevented by allowing only a liquid orpureed diet.
� Follow-up
After an uncomplicated stent placement, liquidfood is allowed after a few hours. This canthen be followed by pasty and then normalsoft diet. The correct position of stents shouldbe monitored routinely during the first few daysbecause most migrations occur early. Tumorovergrowth occurs only after a few months.Analgesics may need to be given during the firstfew days.
� Y. I. Gallinger et al.336

30 Endoscopic Technique in the Treatment of Esophageal Diseases � 337
Fig. 30.25a,b. For dilatations, a guidewire should be rou-tinely inserted under endoscopic control (a). It is usually pos-sible to insert a pediatric endoscope (7.9 mm diameter) orone with an even smaller diameter (5.3 mm) (b).
Fig. 30.26. To push the instrument through a longer steno-sis, the guidewire should be positioned far into the stomachalong the greater curve. This ensures an additional stiffeningof the flexible tip of the endoscope.
Fig. 30.27. In very narrow stenoses which cannot be passedwith the endoscope, a hydrophilic biliary guidewire with flex-ible tip should be tried first. This technique permits tracingof complicated stenoses under fluoroscopic control.
a b

� Y. I. Gallinger et al.338
Fig. 30.28a,b. In very tight stenoses bougienage over a bili-ary guidewire can be difficult. In these cases a radioopaque9 Fr. catheter is first inserted. Then, under fluoroscopic con-trol, a stiff Savary-Gilliard guidewire is inserted (a). Over thisguidewire the bougienage is performed. One must avoid ex-
cessive pressure to reduce the risk for perforation. For re-peated treatment, bougienage over the Savary-Gilliard guide-wire can be performed without further fluoroscopic or endo-scopic controls (b).
Fig. 30.29. If the stenosis can be passed with a 7.9 mm pe-diatric endoscope the treatment can be started using a bou-gie of 10 mm diameter. Dilatations should only be performedwith increments of 2 mm. After each dilatation the wall mustbe checked carefully for deep ulcers.
a b

30 Endoscopic Technique in the Treatment of Esophageal Diseases � 339
Fig. 30.30a–c. Instruments for stenting: bougie with Savary-Gilliard guidewire, transparent pusher with markings, andthe plastic stent (a). The length of the stent is determinedby measuring the extent of the tumor using the endoscope.An additional funnel and stoppers at the distal end can helpto prevent stent migration (b). The instruments for stenting,when assembled, are from proximal to distal: Savary-Gilliardguidewire in position, prosthesis with pulling thread andpusher. The pulling thread is inserted for repositioning theprosthesis in a proximal direction after the removal of thebougie and the pusher, or for the immediate extraction ofthe stent in cases of intolerability or tracheal compression(c).
a
b
c

� Y. I. Gallinger et al.340
a b
c
d

Esophageal fistula
� Introduction
The majority of fistulae arise from the sites offresh anastomoses after esophagectomy. Spon-taneous fistulae that arise from tumor infiltra-tions or after endoscopic procedures are notthat common. In all these situations, tradi-tional open surgery entails a high risk with un-clear efficacy. Endoscopic procedures, of whichseveral technical modifications have been de-veloped, are now the treatment of choice.
� Indications
All fistulae to the tracheobronchial system andthe mediastinum should be treated. Esophago-bronchial fistulae need urgent management.
� Contraindications
Very large lesions of the wall that cannot besealed by endoscopic means should not betreated endoscopically.
� Preliminary examinations
Radiographic identification of the fistula andits extent is achieved using water-soluble con-trast and/or bronchoscopy.
� Instruments
Pediatric endoscope (diameter 7.9 mm or smal-ler); bougienage for tumor dilatation (e.g. Sa-very-Gilliard dilators); plastic prostheses withvarious diameters; covered metal stents; 7 Frcatheter; hydrophilic guidewires; for esophago-mediastinal fistulae: fibrin glue; fluoroscopy.
� Special preparation
The patient should be fasted for at least 12hours.Premedication and monitoring according to
the recommended standard.
� Special technique
1. Fibrin glue sealing (Fig. 30.31 a–c)2. Sealing with stents (Figs. 30.32–30.35).
� Complications
� Non healing fistulae. Endoscopic and fluoro-scopic monitoring should be planned 2 to 3weeks after initial fibrin application in orderto detect persistent fistulae.Treatment: The whole system or cavity
should be washed out and the surface of thewall curetted before a new series of fibrin ap-plication is started.
� Stent migration. Stent migrations are possi-ble both proximally and distally because of theabsence of stenosis, and may occur with bothplastic as well as metal stents.Treatment: In general, endoscopic reposi-
tioning is effective and sufficient. Sometimes anew stent with a larger diameter may be re-quired. In the absence of esophageal stenosis,such as after anastomotic leakage, a plasticprosthesis can be fixed using a transnasal 7 Frcatheter; alternatively the fistula can be sealedwith fibrin glue.
� Tumor overgrowth. Treatment: Electrocauteryor laser ablation of the tumor tissue. For casesof proximal overgrowth, an additional stent in-serted up to the level of the first stent may bepossible. Alternatively, the old stent is extract-ed and a new stent which is longer is then in-serted.
30 Endoscopic Technique in the Treatment of Esophageal Diseases � 341
Fig. 30.31a–d. Positioning of the prosthesis. When the bou-gienage is finished, the assembled instruments are insertedas a unit. A pulling thread is present which is long enoughfor correction of the stent proximally (a). After preliminarypositioning of the entire set, the bougie and guidewire areremoved and a pediatric endoscope is inserted through theremaining pusher and stent. By retroflexion of the endo-
scope-tip in the stomach, the correct position and length ofthe stent can be confirmed (b, c). As the last step, thepusher and endoscope are removed simultaneously. The pull-ing thread is used for immediate removal of the stent incase of stent intolerability or tracheal compression. Disloca-tions can be safely prevented by using an additional funneland distal stoppers (d).
�

� Y. I. Gallinger et al.342
a b
Fig. 30.32a–d. Esophagomediastinal fistula with fibrin seal-ing. After successful search for the entrance of the fistula anatraumatic hydrophilic guidewire is inserted (a). This guide-wire is necessary for the insertion of a catheter (b). After-wards the guidewire is removed. If there is a larger cavity atthe end of the fistula, flushing can be tried. In narrowfistulas there is often only a small amount of exudates andnecrotic material. Sometimes it is reasonable to curettage
the inner surface of the fistula by means of a cytology brush(c). It is inserted with the catheter in place. After these pro-cedures the components of the fibrin glue are instilled intothe fistula and the cavity until one can see the materialflowing out (d). In most cases repeated applications are nec-essary after short intervals of a couple of days. Most fistulascan be treated successfully in benign diseases.
c d

30 Endoscopic Technique in the Treatment of Esophageal Diseases � 343
Fig. 30.33a,b. Esophagotracheal fistula and endoscopic oc-clusion. In carcinomas of the upper cervical esophagus, com-binations of stenoses and fistulas are common. Generally theocclusion of the fistula is possible by positioning a well fit-ting plastic stent (Celestin) which simultaneously keeps thepassage free (a). According to the topographic position,modifications of the stent design might become necessary,e.g. shortening of the funnel. Only in some cases is the addi-tional stenting of the trachea necessary (b). With one or twoproximal correction threads, repositioning of the stent is pos-sible later. In very high cervical fistulas, these proximal cor-rections are not possible because of patient intolerance.
Fig. 30.34. Esophagotracheal fistula following infiltration ofcarcinoma with endoscopic occlusion. In addition to thecheaper plastic prostheses (e.g. Celestin), self expanding me-tal stents are commonly used in developed countries. For thispurpose silicon- or polyurethane-coated stents are available
(Strecker-, Gianturco- or Wall-stents). The Choo-stent (Koreanstent) has certain advantages for occlusion treatment. Itsconfiguration prevents migration and a special traction loopfacilitates extraction of the stent.
a b

� Y. I. Gallinger et al.344
a b
Fig. 30.35a, b. Very proximal cervical esophagotracheal fistu-las require special modifications of the plastic stent used,e.g. Celestin or Baby-Celestin (a). Patient intolerance is a ma-jor problem. In this position, smaller tubes with 9 or 12 mmdiameter and shortened funnel are necessary (b). Additionaldistal stoppers to prevent proximal dislocations are not nec-essary.

Dilatation of benign stenoses
� Introduction
The majority of benign esophageal stenosesare the result of corrosive injuries due to caus-tic ingestion, reflux esophagitis, and radiother-apy. The historic blind methods of dilatationhave been replaced by endoscopy-based tech-niques. In addition, for very short stenotic seg-ments, local injections of steroids or incisionwith electrocautery can be attempted.
� Indications
All benign stenoses resulting in dysphagiashould be treated.
� Contraindications
Dilatation is contraindicated in the setting ofacute tissue necrosis after caustic ingestion. Itshould be delayed in the context of other acutemedical illnesses such as myocardial infarctionor cerebral infarction. If possible, enteral feed-ing should be secured by placing a thin softnasogastric tube. In patients with concomitantesophagomediastinal or esophagotracheal fistu-lae, the dilatation treatment must be completedby sealing the fistula with an appropriate stent.
� Special preparation
– Liquid food should be given for a coupleof days before treatment. Endoscopy-guided lavage of the prestenotic esopha-gus may be necessary prior to treatment.
– Other preparations are made in accor-dance to the standards of safety and mon-itoring in endoscopic treatment.
– Antibiotic prophylaxis may be needed.– Position: Left lateral.
� Instruments
Gastroscopes with different diameters (includ-ing pediatric endoscopes) and large workingchannels (6.0 mm); Savary-Gilliard dilators with12–42 Fr diameters; double-channel ballooncatheters with diameter up to 30 mm and bal-loon length of 4–10 cm; guidewires with flexibletips. For stenoses that cannot be traversed evenwith a pediatric endoscope, additional 0.032–0.035 inch hydrophilic guidewires.
� Special techniques
– Positioning of guidewires in very narrowstenoses (Figs. 30.36–30.39); bougienage(Fig. 30.40)
– Balloon dilatation (Fig. 30.41).
30 Endoscopic Technique in the Treatment of Esophageal Diseases � 345

� Y. I. Gallinger et al.346
Fig. 30.36. Dilatation of benign stenoses. As first step aguidewire (Savary-Gilliard) is inserted through the stenosis.Under endoscopic control the flexible tip passes through thesmall luminal opening. In short stenoses this technique isnot difficult.
Fig. 30.37. The guidewire is pushed forward into the stom-ach and fluoroscopic monitoring can be helpful. In very nar-row and tortuous stenoses which are difficult to pass, biliaryguidewires should be used first (Terumo, Tracer). With thisassistance a pediatric endoscope (7.9 or 5.3 mm diameter)can usually pass through the narrow segments. The wirehelps to stiffen the flexible tip of the endoscope, facilitatingits passage through the tight stenosis.
Fig. 30.38. The endoscope, assisted by the guidewire, haspassed through the stenosis. The distal esophagus, the eso-phagogastric junction and stomach can then be examined.
Fig. 30.39. Longer and very narrow stenoses are usually tor-tuous and cannot be passed with standard Savary-Gilliardguidewires. To manage these cases, hydrophilic atraumaticbiliary guidewires are essential, which should be inserted un-der fluoroscopic monitoring. Using its flexible tip, tortuousparts of the stenosis can be passed by twisting the wire.After successful passage, the thin guidewire is replaced by astandard Savary-Gilliard wire with the assistance of a 9 Frcatheter.

� Complications
Perforation is the most important complica-tion. It can be caused by inserting either theguidewire or dilator too forcefully or with ex-cessive balloon dilatation.Prevention: Use of guidewires with flexible
tips; insertion of guidewires with endoscopicor fluoroscopic control; use of an atraumatichydrophilic biliary guidewire in very narrow,tortuous stenoses; bougienage in small steps,with not more than 3 attempts per session.Attention: The risk of perforation is always
higher if one does not insert guidewires!If the diameter of the dilator exceeds 42 Fr,
the risk of perforation increases significantly.Treatment: If perforation has happened or is
suspected, fluoroscopic examination with water-soluble contrast should be carried out immedi-
ately. In small lesions, endoscopic clipping andconservative treatment with parenteral nutri-tion and antibiotics is justifiable. The inser-tion of a stent to seal the perforation may behelpful in borderline cases. For all major per-forations, open or minimally invasive surgeryis indicated.
� Follow-up
In all uncomplicated cases, liquid food can bestarted after a few hours, progressing to pastyfood the next day. In stenoses related to refluxesophagitis, long-term treatment with protonpump inhibitors (PPI) is required. Many ste-noses require repeated sessions of dilatation.This should be continued in weekly or fort-nightly intervals up to a diameter of 13–14 mm.
30 Endoscopic Technique in the Treatment of Esophageal Diseases � 347
Fig. 30.40. The bougie is pushed over the guidewire whosetip is situated in the distal stomach. The bougienage is per-formed step by step and care is taken to avoid excessiveforce. For each treatment session, the increase in diametershould be limited to 2 mm diameter in order to reduce therisk of perforation. It is safer to split the whole procedure toseveral sessions once or twice a week.
Fig. 30.41. In some situations, such as in the presence ofpre-existing ulcers or inflammation of the esophageal wall,bougienage should be avoided due to an increased risk ofperforation. In this scenario, a temporary gastric feeding tubecan be used to start enteral feeding. After the inflammationhas resolved in a couple of weeks, the dilatation can be re-attempted.

Stenotic esophageal anastomoses and membranes (webs)
� Introduction
Stenoses as a result of scar formation can beobserved after esophagectomies or resection ofthe gastric cardia. In the treatment of thesecases, conventional surgery has largely been re-placed by endoscopic techniques. Congenitalwebs needing treatment are rare. Endoscopicprocedures used include the following: bougie-nage, balloon dilation, incisions using electro-cautery or laser, injection of steroids. The latterhas been specially approved for children. Veryoften, a combination of techniques is used.
� Indications
All clinically apparent stenoses caused by scarsor webs.
� Contraindications
Endoscopic treatment is contraindicated in thesetting of fresh anastomoses with visible signsof inflammation or in the presence of fistulae.In these situations spontaneous recovery is stillpossible and temporary treatment with feedingtubes can be used to obtain enteral access. Inall cases of recurrent tumors, dilatation per sewould be inadequate; the treatment of choicewould be stent placement or surgery.
� Preliminary examinations
Endoscopy with biopsy in the case of previoustumor resection in order to detect recurrences;EUS±FNA; fluoroscopic examination to detectfistulae; coagulation status.
� Special preparation
Liquid food for a couple of days. If necessary,lavage of the prestenotic area just before endo-scopic treatment. Adherence to conventionalstandards of quality and safety in endoscopicprocedures.
� Instruments
Small caliber or standard gastroscopes; Savary-Gilliard dilators; balloon catheters with fixedfinal diameters; standard guidewires; flexibleatraumatic biliary guidewires for very narrowstenoses; needle papillotome for stricturotomyor partial resection of a scar; argon plasma; in-jection needles for local application of steroidsolutions.
� Special techniques
– Bougienage over a guidewire (Figs. 30.42,30.43)
– Thermal treatment by cutting or excision(Fig. 30.44–30.46).
� Y. I. Gallinger et al.348

30 Endoscopic Technique in the Treatment of Esophageal Diseases � 349
Fig. 30.42. Scars or webs. Bougienage with endoscopic in-spection of the lesion. If the lumen is very narrow, a guide-wire should be inserted to assist the bougie. The dilatationis performed with limited pressure and repeated using dila-tors of different diameters. This technique is adequate mainlyfor webs and very short elastic strictures caused by scars.
Fig. 30.43. The result of the bougienage can be observedimmediately through the endoscope. If a pediatric gastro-scope cannot pass through, the dilatation is usually still in-adequate.
Fig. 30.44. In very hard scars with granular tissue reactionthe dilatation treatment should be supplemented by endo-scopy-controlled incisions. They are performed with a needle-knife papillotome or with the tip of a snare.
Fig. 30.45. Usually 3–6 radial cuts are necessary. The fibrosisof the surrounding tissue protects against perforation. Bou-gienage or balloon-dilatation follows the incisions immedi-ately or after an interval of a few days.

� Complications
– Rupture of the esophageal wall is veryrare. The inner layer of the wall should becarefully inspected after every dilatation.
– Hemorrhage after incision is generally mi-nor. If necessary, it can be stopped bysclerotherapy or endoscopic clip applica-tion.
– In many cases, the first treatment is notfully sufficient. If this is the case, thetreatment should be repeated at weeklyintervals until adequate.
� Follow-up
In uncomplicated cases liquid food is per-mitted 3–4 hours after treatment. Normal softdiet is allowed after a couple of days.The effect of treatment should be monitored
after one week by endoscopy. If necessary, thenext session can start immediately. A normalor near normal diameter of the lumen is theaim of treatment.Re-stenoses are not very common after suc-
cessful dilations. Therefore endoscopic monitor-ing is necessary only with recurrence of clinicalsymptoms, except for patients with previoustumor resections.After injection of steroid solutions, follow-up
endoscopy should be performed after 2 weeksand later on recurrence of symptoms, with re-peated injections if needed.
� Y. I. Gallinger et al.350
Fig. 30.46. Stricturotomy can also be performed with argonplasma coagulation. There are no perceptible advantages ascompared with electrocautery. Personal preferences seem tobe of major importance. Using this technique, the cuts arealso performed by multiple radial incisions, followed by bou-gienage or balloon dilatation.

Achalasia
� Introduction
There is a general consensus that endoscopictreatment should be tried before surgery in allpatients with achalasia. Two endoscopic tech-niques are used: Endoscopy or fluoroscopyguided balloon dilatation and injection of bo-tulinum toxin into the muscle layer. The clini-cal experience with the use of dilatation fortreatment is over 2 decades, while that for bo-tulinum toxin injection spans several years.The clinical outcome after botulinum injectionis more variable. The effects of other forms ofinjection treatment are under clinical review.
� Indications
Balloon dilatation can be used as the initialtreatment. It can also be used after unsuccess-ful botulinum toxin injection or surgery. Thereare 2 technical modifications: high complianceballoons (HCB) and low compliance balloons(LCB), each with different pressures and finaldiameters. Injection with botulinum toxin mayalso be used as initial therapy, but one mustbear in mind the poorer long-term outcomeand higher costs.
� Contraindications
Treatment is contraindicated in the presence ofsevere medical comorbidities such as acutemyocardial infarction, strokes, and respiratoryinsufficiency. One must exclude the possibilityof malignant tumors of the gastroesophagealjunction mimicking achalasia. In the context ofconcomitant epiphrenic diverticula, it is diffi-cult to estimate the risk of complications, andhence the treatment options must be carefullyreviewed.
� Preliminary examinations
Complete diagnostic testing including radiog-raphy, endoscopy with biopsies and manome-try are done prior to treatment. If there is asuspicion of infiltrative tumors, biopsies of thedeeper layers and EUS are imperative.
� Special preparations
– In very narrow stenoses, liquid foodshould be started several days beforetreatment. If necessary, a lavage under en-doscopic control should be performed be-fore commencement of endoscopic treat-ment.
– Other preparations according to the stan-dards for safe endoscopic treatmentshould be adhered to.
– Prophylactic antibiotics may be needed.– Premedication: Analgesia-sedation.
� Instruments
For injection treatment endoscopes with largeworking channels (3.7 mm) or a double chan-nel are preferred in order to facilitate simulta-neous suction. For pre-treatment lavage, endo-scopes with 6 mm working channels are help-ful.For balloon dilatation, endoscopes with a
smaller diameter are more appropriate for easi-er insertion into the stomach.Important accessories: balloon dilators of
different diameters with manometric control;injection catheters with predetermined needlelength to allow safe infiltration of the muscu-laris propria (EUS may be used, if necessary,to guide the exact position of the botulinumdeposits); guidewires for very tight stenoses;botulinum toxin (about 5 ml per session,equivalent to 80–100 U).
30 Endoscopic Technique in the Treatment of Esophageal Diseases � 351

� Special techniques
– Injection treatment (Figs. 30.47, 30.48)– Balloon dilatation (Fig. 30.49)– Endoscopy controlled balloon dilatationover a guidewire (Fig. 30.50).
� Complications
Tears of the esophageal wall, with or withoutperforation, are the most common complica-tions. If only the mucosal layer is involved, nospecific treatment is necessary. Bleeding can bearrested by local infiltration with 0.05% epi-nephrine. In the case of deeper tears, an im-mediate fluoroscopic examination with water-soluble contrast should be performed. Smalltransmural tears can be treated with endo-
scopic clipping, parenteral nutrition, and anti-biotics. However, if mediastinitis or peritonitisdevelops, conventional open or minimally inva-sive surgery is indicated.Botulinum toxin injections may lead to retro-
sternal pain or a burning sensation; sponta-neous relief can be expected within a few days.
� Follow-up
In uncomplicated cases liquid food can be per-mitted 2–3 hours after treatment, followed sub-sequently by normal diet. Treatment may berepeated upon recurrence of symptoms, whichis not uncommon. Based on our experience,the effect of treatment lasts for several months.If the overall outcome is unsatisfactory, surgerymay be indicated.
� Y. I. Gallinger et al.352

30 Endoscopic Technique in the Treatment of Esophageal Diseases � 353
Fig. 30.47. Injection treatment for achalasia. The injectionneedle is placed exactly into the area of the lower esopha-geal sphincter. The tip is pushed forward just to the muscu-lar layer (insert, 3). For each treatment session about 5 ml ofbotulinum toxin is injected in 4–6 deposits (1 mucosae,2 submucosae, 3 muscularis propria, 4 surrounding tissue).
Fig. 30.48. Injection treatment of achalasia. The exact posi-tion of the needle can be identified using endosonographicexamination. The intended muscularis propria is the echo-poor layer just beyond the echo-rich submucosa (double-ar-row). During the injection a widening of the narrow echo-poor muscular layer can be observed.
Fig. 30.49. Achalasia with dilatation treatment. The balloondilator is attached to the distal end of the endoscope nextto the flexible distal end. The major advantage of this tech-nique is that direct observation of the treatment result byretroflexion of the endoscope is possible.

� Y. I. Gallinger et al.354
Fig. 30.50a,b. Achalasia with dilatation treatment. In verynarrow stenoses of the lower esophageal sphincter, a guide-wire is inserted first. Over it, the balloon is pushed until thenarrow segment is just in the middle of the balloon. Fluoro-scopic monitoring is used (a). The markings of the catheter
permit a reliable estimation of the position. Then the pres-sure is slowly increased with manometric control. The selec-tion of an adequate balloon diameter is essential. Duringfluoroscopy one sees the waist of the balloon slowly disap-pearing (b).
a b

Diverticula
� Introduction
Diverticula of the esophagus are herniations ofthe mucosal layer through a gap of the muscu-laris propria (i.e. false diverticula). They aremainly found in the hypopharynx (Zenker’s di-verticulum) or near the diaphragm. Diverticulabecome clinically important when they impedethe normal passage of solid food. Traditionallythe treatment is surgical. The first non-surgicalprocedures for Zenker’s diverticulum were per-formed by ENT surgeons through laryngoscopes(Dohlman and Mattson 1960). The principle ofendoscopic treatment is the incision of the sep-tum between the esophageal wall and the diver-ticulum, thus preventing the retention of foodparticles.
� Indications
All patients with symptomatic Zenker’s diver-ticula with clinical symptoms can be treated.In high risk patients, endoscopic treatment canreplace conventional surgery.
� Contraindications
Treatment is contraindicated in the presence ofinflammation of the diverticular wall.
� Preliminary examinations
Endoscopy and radiography to determine theanatomy of the diverticulum and septum, andto assess the presence of inflammation; coagu-lation status.
� Special preparations
– Liquid food for a few days– Monitoring and safety procedures as perrecommended standards
– Premedication: Analgesia-sedation– Position: Left lateral.
� Instruments
Therapeutic gastroscopes with either a largeworking channel or dual channel.Accessories: Needle knife. Alternative: Argon
plasma coagulation.
� Special technique
Cutting the septum with the assistance of anasogastric tube (Figs. 30.51–30.54).
� Complications
– Hemorrhages are generally minor; ifneeded, they can be stopped by injec-tions.
– Perforation with pneumomediastinum andmediastinitis are very rare complications.
Treatment of perforation in Zenker’s diverticu-lum is mainly conservative with parenteral nu-trition and antibiotics. Small perforations maybe closed by endoscopic clipping.If the clinical response is inadequate, treat-
ment sessions can be repeated at 3 weeks.
� Follow-up
Intravenous fluids should be maintained for afew days, followed by gradual introduction ofpasty and then solid food. When the treatmentis completed, the results should be documentedby radiography.
30 Endoscopic Technique in the Treatment of Esophageal Diseases � 355

� Y. I. Gallinger et al.356
Fig. 30.51a,b. Endoscopic treatment of Zenker’s diverticu-lum basically means the destruction of the septum betweenthe esophagus and the diverticulum to achieve symptomaticrelief from retentions of food (a). The result is a broad con-nection between the diverticulum and esophageal lumenand a flat diverticular cavity (b).
Fig. 30.52. The incision of the septum between the divertic-ulum and the esophageal lumen can be performed usingpure cutting current or argon plasma coagulation. In somecases with larger diverticula, the treatment may need to berepeated at 3 week intervals.
Fig. 30.53. A complete destruction of the septum is notnecessary. Sometimes it is safer to leave a small residual sep-tum in place. It is more important to achieve functional re-sults than perfect anatomy.
a b
Fig. 30.54. A nasogastric tube is inserted to allow correctorientation of the location of the diverticulum. For both theneedle knife and argon plasma coagulation techniques, theincision should not exceed 20 mm in one treatment sessionto avoid perforation. It can be continued at 3 week intervals.

References
Axelrad AM, Fleischer DE, Gomes M (1996) Nitinolcoil esophageal prosthesis: advantages of removableself-expanding metallic stents. Gastrointest Endosc43:155–160
Annese V, Basciani M, Lombardi G, Caruso N, Perri F, Si-mone P, Andriulli A (1996) Perendoscopic injection ofbotulinum toxin is effective in achalasia after failureof myotomy or pneumatic dilation. Gastrointest En-dosc 44:461–465
Berggren PJ, Harrison ME, Sanowski RA, Ingebo K,Noland B, Zierer S (1993) Techniques and complica-tions of esophageal foreign body extraction in chil-dren and adults. Gastrointest Endosc 39:626–630
Bertoni G, Sassatelli R, Conigliaro R, Bedogni G (1996)A simple latex protector hood for safe endoscopicremoval of sharp-pointed gastroesophageal foreignbodies. Gastrointest Endosc 44:458–461
Bethge N, v Kleist D, Vakil N (1996) Treatment of eso-phageal perforation with a covered expandable me-tal stent. Gastrointest Endosc 43:161–163
Bethge N, Somma A, Vakil N (1997) A prospective trialof self-expanding metal stents in the palliation ofmalignant esophageal strictures near the upper eso-phageal sphincter. Gastrointest Endosc 45:300–303
Bigler PC (1966) The use of a Foley catheter for re-moval of blunt foreign bodies from the esophagus. JThorac Cardiovasc Surg 51:477–479
Binmoeller KF, Grimm H, Soehendra N (1993) Endo-scopic closure of a perforation using metallic clipsafter snare excision of a gastric leiomyoma. Gastro-intest Endosc 39:172–174
Binmoeller KF, Thonke F, Soehendra N (1993) Endo-scopic hemoclip treatment for gastrointestinal bleed-ing. Endoscopy 25:167–170
Binmoeller KF, Krug Ch, Rehner M, Seifert H, Soehen-dra N (1997) Endoscopic implantation of endopros-thesis for the palliative treatment of stenoses andfistulas of the proximal cervical esophagus. Zbl Chir122:44–48
Blackard WG, Marks RD, Baron TH (1996) Suctionsclerotherapy for the treatment of esophageal varices.Gastrointest Endosc 44:725–728
Boerke JM, Hope RL, Chu G, Gillespie PE, Bull C,O’Rourke I, Williams SJ (1996) Laser palliation ofinoperable malignant dysphagia: initial and death.Gastrointest Endosc 43:29–32
Brayko CM, Kozarek RA, Sanowski RA (1985) Bacteri-emia during esophageal variceal sclerotherapy: itscause and prevention. Gastrointest Endosc 31:10–12
Broor SL, Lahoti D, Bose PP, Ramsh GN, Raju GS, Ku-mar A (1996) Benign esophageal strictures in chil-dren and adolescents: etiology, clinical profile, andresults of endoscopic dilation. Gastrointest Endosc43:474–477
Burdick JS, Venu RP, Hogan WJ (1993) Cutting the de-fiant lower esophageal ring. Gastrointest Endosc 39:616–619
Celestin LR, Campell WB (1981) A new and safe sys-tem for esophageal dilation. Lancet 1:74–75
30 Endoscopic Technique in the Treatment of Esophageal Diseases � 357
Cellier C, Landi B, Faye A, Wind P, Frileux P, CugnencPN, Barbier JP (1996) Upper gastrointestinal tractfistulae: endoscopic obliteration with fibrin sealing.Gastrointest Endosc 44:731–733
Chung SCS, Leong HA, Choi CYC (1994) Palliation ofmalignant esophageal obstruction by endoscopic al-cohol injection. Endoscopy 26:275–277
Cotton PB (1983) Overtubes (fleeves) for upper gastro-intestinal endoscopy. Gut 24:863–866
Cox J, Buckton GK, Bennett JR (1986) Balloon dilationin achalasia: a new dilator. Gut 27:986–989
De Boer WA, Van Haren F, Driessen WMM (1995)Marking clips for the accurate positioning of self-ex-pandable esophageal stents. Gastrointest Endosc 42:73–76
Den Hartog Jager FCA, Bartelsman JFWM, Tytgat GNJ(1979) Palliative treatment of obstructing esophago-gastric malignancy by endoscopic positioning of aplastic prosthesis. Gastroenterology 77:1008–1014
DePalma GD, DiMatteo E, Romano G, Fimmano A,Rondinone G, Catanzano C (1996) Plastic prosthesisversus expandable metal stents for palliation of in-operable esophageal thoracic carcinoma: a con-trolled prospective study. Gastrointest Endosc 43:478–482
Deviere J, Quarre DP, Love J, Cremer M (1994) Self-ex-pandable stent and injection of tissue adhesive formalignant broncho-esophageal fistula. GastrointestEndosc 40:508–510
D’Imperio N, Piemontese A, Baroncini D, Billi P, Borio-ni D, Dalmonte PP, Borello P (1996) Evaluation ofundiluted N-butyl-2-cyanoacrylate in the endoscopictreatment of upper gastrointestinal tract varices. En-doscopy 28:239–243
Domschke W, Foerster EC, Matek W, Rödl W (1990)Self-expanding mesh stents for esophageal stenosis.Endoscopy 22:134–136
Dumont JF, Meric B, Sivak MV, Fleischer DE (1995) Anew method of esophageal dilation using Savary-Gilliard bougies. Gastrointest Endosc 31:379–382
Ell C, Riemann JF, Demling L (1986) Endoscopic occlu-sion of a neoplastic esophagomediastinal fistula bya fast-hardening aminoacid solution. GastrointestEndosc 32:287–288
Engel JJ, Panje WR (1995) Endoscopic laser Zenker’sdiverticulotomy. Gastrointest Endosc 42:368–370
Fan Z, Dai N, Chen L (1997) Expandable thermal-shaped memory metal esophageal stent: experienceswith a new nitinol stent in 129 patients. GastrointestEndosc 46:352–357
Fleischer DE, Sivak MV (1985) Endoscopic Nd-YAG la-ser therapy as palliation for esophagogastric carci-noma. Gastroenterology 89:827–831
Fleischer DE, Bull-Henry K (1992) A new coated self-expanding metal stent for malignant esophagealstrictures. Gastrointest Endosc 38:494–496
Fleischer DE, Wang GQ, Dawsey S, Tio TL, Newsome J,Kidwell J, Prifti S (1996) Tissue band ligation fol-lowed by snare resection (band and snare): a newtechnique for tissue acquisition in the esophagus.Gastrointest Endosc 44:68–72

Fiorini AB, Goldin E, Valero JL, Bloom A, Beyar M,Pfeffer RP, Goberman O (1995) Expandable metalcoil stent for treatment of broncho-esophageal fistu-la. Gastrointest Endosc 42:81–83
Goldin E, Beyar M, Safra T, Globerman O, Craciun I,Wengrover D, Fich A (1994) A new self-expandablenickel-titanium coil stent for esophageal obstruc-tion: a preliminary report. Gastrointest Endosc 40:64–68
Goldman JH, Goldberg RI (1994) Balloon removal ofan impacted esophageal meat bolus. GastrointestEndosc 40:391
Goldschmiedt M, Haber G, Kandel G, Kortan P, MarconN (1992) A safety maneuver for placing overtubeduring endoscopic variceal ligation. Gastrointest En-dosc 38:399–400
Gossner L, Sroka R, Hahn EG, Ell C (1995) Photody-namic therapy: successful destruction of gastrointes-tinal cancer after oral administration of aminolevu-linic acid. Gastrointest Endosc 41:55–58
Graham DY, Tabibian N, Schwartz JT, Smith JL (1987)Evaluation of the effectiveness of through-the-scopeballoons as dilators of benign and malignant gastro-intestinal strictures. Gastrointest Endosc 33:432–436
Graham DY (1990) Treatment of benign and malignantstrictures of the esophagus. In: Silvwis SE (ed) Ther-apeutical gastrointestinal endoscopy. Igaku-ShoinNew York, pp 1–41
Graham DY (1996) Fluoroscopy or no for esophagealdilation: the passing of an era (Editorial). Gastroin-test Endosc 43:171–173
Hachisu T, Miyazaki S, Hamaguchi K (1989) Endo-scopic clip-marking of lesions using the newly de-veloped HX-3L clip. Surg Endosc 3:142–147
Hashizume M, Sugimachi K, Kishihara F, Kawanaka H,Ohta M, Tomikawa M, Tanoue K, Yamaga H, HigashiH (1995) A serial transparent endoscopic elasticband ligator. Gastrointest Endosc 42:169–170
Healy GB (1988) Removal of esophageal foreign bodieswith a Foley catheter under fluoroscopic control.Can Med Assoc J 138:490–491
Hoffman RJ, Knapple WL, Bhutani MS, Verne GN,Hawes RH (1997) Treatment of achalasia by injec-tion of botulinum toxin under endoscopic ultra-sound guidance. Gastrointest Endosc 45:77–79
Hordijk JL, Dees J, van Blankenstein M (1990) The man-agement of malignant esophago-respiratory fistulaswith a cuffed prosthesis. Endoscopy 22:214–244
Inoue H, Takeshita K, Hori H, Muraoka Y, Yoneshima H,Endo M (1993) Endoscopic mucosal resection with acap-fitted panendoscope for esophagus, stomach andcolon mucosal lesions. Gastrointest Endosc 39:58–62
Inoue H, Endo M, Takeshita K, Kawano T, Yoshino K(1991) Endoscopic resection of early-stage esopha-geal cancer. Surg Endosc 5:59–62
Ishioka S, Sakai P, Maluf Filho F, Melo JM (1995) Endo-scopic incision of Zenker’s diverticula. Endoscopy27:433–437
Jankovic J, Brin MF (1991) Therapeutic use of botuli-num toxin. N Engl J Med 324:1186–1194
Johlin FC, Griglione G (1989) A new technique usinginjectable collagen to promote sealing of an eso-
phagorespiratory fistula. Gastrointest Endosc 35:220–225
Jung M, Manegold BC, Brands W (1989) Endoscopictherapy of gastrointestinal fistulae with fibrin tissuesealant. In: Waclaviczek HW (ed) Progress in fibrinsealing 45–59. Springer, Berlin Heidelberg New York
Kadakia SC, Wang RK (1993) Graded pneumatic dila-tion using Rigiflex achalasia dilators in patients withprimary esophageal achalasia. Am J Gastroenterol88:34–38
Kirsch M, Blue M, Desai RK, Sivak MV (1991) Intrale-sional steroid injections for peptic esophageal stric-tures. Gastrointest Endosc 37:189–192
Kodali VF, Petersen BT, Miller CA, Gostout CJ (1997) Anew jumbo-channel therapeutic gastroscope foracute upper gastrointestinal bleeding. GastrointestEndosc 45:409–411
Kozarek RA, Ball TJ, Brandabur JJ, Patterson DJ, Low D,Hill L, Raltz S (1996) Expandable versus conventionalesophageal prostheses: easier insertion may not pre-clude subsequent stent-related problems. GastrointestEndosc 43:204–208
Lahoti D, Broor SL, Basu PP, Gupta H, Sharma R, PantCS (1995) Corrosive esophageal strictures: predic-tors of response to endoscopic dilation. GastrointestEndosc 41:196–200
Lightdale CJ, Heier SK, Marcon NE, McCaughan JS,Gerdes H, Overholt BF, Sivak MV (1995) Photody-namic therapy with porfimer sodium versus thermalablation therapy with Nd:YAG laser for palliation ofesophageal cancer: a multicenter randomized trial.Gastrointest Endosc 42:507–512
Likier HM, Levine JG, Lightdale C (1991) Photodynamictherapy for completely obstructing esophageal carci-noma. Gastrointest Endosc 37:75–78
Lo GH, Lai KH, Shen MT, Chang CF (1994) A compari-son of the incidence of transient bacteriemia and in-fectious sequelae after sclerotherapy and rubber bandligation of bleeding esophageal varices. GastrointestEndosc 40:675–679
Lux G, Wilson D, Wilson L, Demling L (1987) A cuffedtube for the treatment of esophagobronchial fistula.Endoscopy 19:28–30
Macken E, Gevers A, Hiele M, Rutgeerts P (1996) Treat-ment of esophagorespiratory fistulas with polyure-thane-covered self-expanding metallic mesh stent.Gastrointest Endosc 44:324–326
Malik A, Chitnavis V, Epstein A (1994) Use of a hydro-philic wire for esophageal intubation in Zenker’s di-verticulum. Gastrointest Endosc 40:523–524
Mamel JJ, Weiss D, Pouagare M, Nord HJ (1995) Endo-scopic suction removal of food bolus from the uppergastrointestinal tract using Stiegmann-Goff friction-fit adapter: an improved method for removal offood impaction. Gastrointest Endosc 41:593–596
Mearin F, Armengol JR, Chicharro L, Papo M, BalboaA, Malagelada JR (1994) Forceful dilation under en-doscopic control in the treatment of achalasia: arandomised trial of pneumatic versus metallic dila-tor. Gut 35:1360–1362
McClave SA, Brady PG, Wright RA, Goldschmid S, Min-ocha A (1996) Does fluoroscopic guidance for Malo-
� Y. I. Gallinger et al.358

ney esophageal dilation impact on the clinical end-point of therapy: relief of dysphagia and achievementof luminal patency. Gastrointest Endosc 43:93–97
McCoughan JS, Nims TA, Guy JT, Hicks WJ, WilliamsTE, Laufman LR (1989) Photodynamic therapy foresophageal tumors. Arch Surg 124:74–80
Moreto M, Ojembarrena A, Rodriguez ML (1996) Endo-scopic injection of ethanolamine as a treatment forachalasia: a first report. Endoscopy 28:539–545
Mühldorfer SM, Hahn EG, Ell C (1996) High- and low-compliance balloon dilators in patients with achala-sia: a randomized prospective comparative trial. Gas-trointest Endosc 44:398–403
Neu HC (1989) Recommendations for antibiotic proph-ylaxis before endoscopy. Am J Gastroenterol 84:1488–1489
Neuhaus H, Hoffmann W, Dittler HJ, Niedermeyer HP,Classen M (1992) Implantation of self-expandingesophageal metal stents for palliation of malignantdysphagia. Endoscopy 24:405–410
Neustater B, Barkin JS (1996) Extraction of an esopha-geal food impaction with a Roth retrieval net. Gas-trointest Endosc 43:66–67
Ng TM, Spencer GM, Sargeant IR, Thorpe SM, BrownSG (1996) Management of strictures after radiother-apy for esophageal cancer. Gastrointest Endosc 43:584–590
Overholt BF, Panjehpour M, Tefftellar E, Rose M (1993)Photodynamic therapy for treatment of early adeno-carcinoma in Barrett’s esophagus. Gastrointest En-dosc 39:73–76
Overholt BF, Panjehpour M (1995) Barrett’s esophagus:photodynamic therapy for ablation of dysplastic, re-duction of specialized mucosa, and treatment ofsuperficial esophageal cancer. Gastrointest Endosc42:64–70
Paquet KJ (1983) Endoscopic paravariceal injectionsclerotherapy of the esophagus – indications, tech-nique, complications: results of a period of 14 years.Gastrointest Endosc 29:310–315
Pasricha PJ, Ravich WJ, Kalloo AN (1993) Botulinumtoxin for achalasia. Lancet 341:244–245
Payne-James JJ, Spiller RC, Misiewicz JJ, Silk DB (1990)Use of ethanol-induced tumor necrosis to palliatedysphagia in patients with esophagogastric cancer.Gastrointest Endosc 36:75–78
Perez-Arroyo H, Hunter J, Waring JP (1997) Botulinumtoxin for an esophageal muscular A-Ring. Gastroin-test Endosc 45:193–195
Raijman I, Walden D, Kortan P, Haber GB, Fuchs E,Siemens M, Kandel G, Marcon NE (1994) Expand-able esophageal stents: Initial experience with a newnitinol stent. Gastrointest Endosc 40:614–621
Ramirez FC, Dennert B, Zierer ST, Sanowski RA (1997)Esophageal self-expandable metallic stents – indica-tions, practice, technique, and complications: resultsof a national survey. Gastrointest Endosc 45:360–364
Saeed ZA, Winchester CB, Ferro PS, Michaletz PA,Schwartz JT, Graham DY (1995) Prospective ran-domized comparison of polyvinal bougies andthrough-the-scope balloons for dilation of peptic
strictures of the esophagus. Gastrointest Endosc 41:189–195
Saeed ZA, Ramirez FC, Hepps KS, Cole RA, SchneiderFE, Ferro PS, Graham DY (1997) An objective endpoint for dilation improves outcome of peptic eso-phageal strictures: a prospective randomized trial.Gastrointest Endosc 45:354–359
Sakai P, Filho FM, Iryia K, Moura EGH, Tomishigue T,Scabbia A, Ishioka S (1996) An endoscopic tech-nique for resection of small gastrointestinal carcino-mas. Gastrointest Endosc 44:65–68
Sanowski R (1987) Foreign body extraction in the gas-trointestinal tract. In: Sivak MV (ed) Gastroentero-logic endoscopy, 321–331. Saunders, Philadelphia
Sass NL, Hagenmüller F (1992) First endoscopic im-plantation of memory metal stents in the esophagus.Endoscopy 24:622A
Schulze S, Fischerman K (1990) Palliation of esophago-gastric neoplasms with a Nd-YAG laser treatment.Scand J Gastroenterol 25:1024–1027
Schuman MD, Beckman JW, Tedesco FJ, Griffin JW, As-sad RT (1987) Complications of endoscopic injec-tion sclerotherapy: a review. Am J Gastroenterol82:823–830
Smith JL, Michaletz PE, Tabibian N, Schwartz JT, Gra-ham DY (1987) Improved palliation of a respiratory-esophageal fistula with a cuffed esophageal prosthe-sis. Am J Gastroenterol 82:1175–1176
Soehendra N, Binmoeller KF, Seifert H, Schreiber HW(1997) Praxis der therapeutischen Endoskopie. Thie-me, Stuttgart New York
Stiegmann GV, Cambre T, Sun JH (1986) A new endo-scopic elastic band ligating device. Gastrointest En-dosc 32:230–233
Stiegmann GV, Goff JS (1989) Endoscopic esophagealvarix ligation: preliminary clinical experience. Gas-trointest Endosc 34:113–117
Tajiri H, Daikuzono N, Joffe SN, Oguro Y (1987)Photoradiation therapy in early gastrointestinal can-cer. Gastrointest Endosc 33:88–90
Tsang TK, Buto SK (1992) Catheter guided endoscopicintubation: a new technique for intubating a difficultesophagus. Gastrointest Endosc 38:49–51
Tuan HA, Lam ECS, Fan ST (1989) Endoscopic retrievalof ingested broken glass in the esophagus and stom-ach by end-hood and suction technique. GastrointestEndosc 35:357–358
Tytgat GNJ, Huibregtse K, Bartelsman JWM, Den Har-tog Jager FCA (1986) Endoscopic palliative therapyof gastrointestinal and biliary tumors with prosthe-sis. Clin Gastroenterol 15:249–271
Tytgat GNJ (1989) Dilation therapy of benign esopha-geal stenosis. World J Surg 13:142–148
Tytgat GNJ (1990) Endoscopic therapy of esophagealcancer: possibilities and limitations. Endoscopy 22:263–267
Tytgat GNJ, Classen M (1994) Practice of therapeuticendoscopy. Churchill-Livingstone, Edinburgh
Urita Y, Kondo E, Muto M, Yamada S, Hachiya A, Ishi-hara M, Ozaki M, Nishimo M, Naruki Y, Otsuka S(1996) Combined endoscopic clipping and injection
30 Endoscopic Technique in the Treatment of Esophageal Diseases � 359

sclerotherapy for esophageal varices. GastrointestEndosc 43:140–143
Utts SJ, DiPalma JA, Wytock DH (1995) Tracheobron-chial obstruction complicating peroral prosthesis in-sertion. Gastrointest Endosc 31:383–384
Van den Berg H (1998) On the evolution of some endo-scopic light delivery systems for photodynamic ther-apy. Endoscopy 30:392–407
Vargas-Tank L, Ovalle L, Fernandez C, Mella B, EstayR, De Solar MP, Soto JR (1995) Use of a very flexibleguide wire to permit dilation of complex malignantstrictures of the esophagus. Gastrointest Endosc41:8–10
Wang YG, Seitz U, Li ZL, Soehendra N, Qiao XA (1998)Endoscopic management of huge bezoars. Endoscopy30:371–374
Webb WA (1995) Management of foreign bodies of theupper gastrointestinal tract: update. Gastrointest En-dosc 41:39–51
Wehrmann T, Jacobi V, Jung M, Lembcke B, CasparyWF (1995) Pneumatic dilation in achalasia with alow-compliance balloon: results of a 5-year prospec-tive evaluation. Gastrointest Endosc 42:31–36
Weigert N, Neuhaus H, Rösch T, Hoffmann W, DittlerHJ, Classen M (1995) Treatment of esophagorespira-tory fistulas with silicon-coated self-expanding me-tal stents. Gastrointest Endosc 41:490–496
Wu WC, Katon RM, Saxon RR, Barton RE, Uchida BT,Keller FS, Rösch J (1994) Silicon-covered self-ex-panding metallic stents for the palliation of malig-nant esophageal obstruction and esophagorespira-tory fistulas: experience in 32 patients and a reviewof the literature. Gastrointest Endosc 40:22–23
Zein NN, Gresetz JM, Perrault J (1995) Endoscopic in-tralesional steroid injections in the management ofrefractory esophageal strictures. Gastrointest Endosc41:596–598
360 � Y. I. Gallinger et al.: 30 Endoscopic Technique in the Treatment of Esophageal Diseases

Due to the grave risk of insufficiency of theesophageal anastomosis and considering thesevere operative trauma that is involved, sur-gery of the esophagus is one of the mostdreaded operations in visceral surgery even to-day.The post-operative complications could oc-
cur in the early or in the late post-operativeperiod.
Early post-operative complications
� Necrosis of the gastric tube
The first manifestation of gastric tube necrosisis the insufficiency of collar anastomosis,which presents clinically either as salivary fis-tula with fever as reddening of the skin, or re-sults in a rise in amylase content of the drain-age secretions.In some cases, the first and only manifesta-
tion of gastric tube necrosis is the develop-ment of cardiac arrhythmias with subsequentmediastinitis.Therefore, as soon as the symptoms occur,
an endoscopy may be performed to assess theblood circulation.If a necrosis of the gastric tube is demon-
strated by endoscopy, the collar anastomosis ispromptly released, and the necrotic segment ofthe bridging graft is resected.The operation is concluded by providing
mediastinal drainage, collar esophagostomy,and gastrostomy with the residual stomach.
The residual stomach is left behind for aslong as possible in order to ensure a good lengthof the residual stomach for secondary recon-struction. The proximal esophageal stump isnot shortened for the same reason.
Post-operative Complications of the Esophagusand Esophagus Bridge GraftD.C. Broering, J.R. Izbicki, Y. Vashist, A.F. Chernousov,
P.M. Bogopolski, E.F. Yekebas
31
Fig. 31.1. Necrosis of the gastric tube after esophagealresection and transposition of the stomach in the formeresophageal bed of the collar anastomosis.

� Necrosis of the colonic bridging graft
After interposition of the colon, the bridginggraft can likewise undergo necrosis. A necrosisof the colonic graft is clinically not differentfrom a necrosis of the stomach graft.An immediate discontinuity resection with
intensive drainage of the mediastinum is thepreferred treatment in this case as well. Be-sides collar esophagostomy, a catheter jejunos-tomy is also necessary.
� D. C. Broering et al.362
Fig. 31.2. Situation after discontinuity resection of the gas-tric tube.
Fig. 31.3. Site after esophago-gastrectomy and necrosis ofthe colonic bridging graft.
Esophagostoma
Gastrostoma

31 Post-operative Complications of the Esophagus and Esophagus Bridge Graft � 363
Fig. 31.4a,b. Situation after discontinuity resection of thecolonic bridging graft, collar esophagostomy, and catheter je-junostomy. For catheter jejunostomy, the jejunum is punctu-red, and a nutrient catheter pushed deep into the proxi-
mal jejunum. The site of insertion of the catheter into thesmall intestine is closed with a purse-string suture and addi-tionally reinforced by invaginating sero-muscular sutures.
a
b

� Fistula between the bridging graft(colon, stomach) and the trachea
The development of a fistula between the bridg-ing graft and the trachea is one of the mostdreaded complications. The fistula can be lo-cated in any part of the trachea, the most com-monly affected region being the portion of thetrachea above the tracheal bifurcation. The de-velopment of a fistula is an indication for sur-gery.
� D. C. Broering et al.364
Fig. 31.5. Pedicle pericardial flaps for closing a fistula be-tween the esophageal bridge graft and the trachea. Theapproach is via thoracotomy in the right 5th intercostalspace. The latissimus dorsi muscle should never be incised.The fistula between the esophageal bridge graft (e.g. gastrictube) and the supra-bifurcational trachea is excised and thedefect in the gastric tube is closed with button-hole sutures.The excision of the fistula leaves a defect in the region of
the pars membranacea of the trachea which can be sealedair-tight by a pedicle flap of the pericardium. The phrenicnerve is separated from the pericardium and held ventrallyby using a nerve hook. The pericardiac-phrenic artery andvein form the vascular pedicle of the pericardial flap. To pre-vent necrosis of the flap, it is necessary that the length ofthe pericardial flap does not exceed three times the flapbase.

31 Post-operative Complications of the Esophagus and Esophagus Bridge Graft � 365
Fig. 31.6. Pedicle flap of the pericardium for closing a fistulabetween the esophageal bridge graft and the trachea. Thepericardial flap is transposed below the pulmonary artery be-tween the pulmonary vein and the pulmonary artery to the
pars membranacea of the supra-bifurcational trachea and su-tured circularly with button-hole sutures (Vicryl 4/0) into thedefect in the pars membranacea. The suture should be asair-tight as possible.

� D. C. Broering et al.366
Fig. 31.7a–c. Flap of the latissimus dorsi muscle for muscu-lar covering of a tracheal fistula. Keeping the muscle fasciaintact, the latissimus dorsi muscle is mobilized subcuta-neously up to the iliac crest. Similarly, keeping the vascularbundle intact, the lower surface of the latissimus dorsi mus-cle is also mobilized. The muscle is lifted from the iliac crest(a). After resection of the 4th rib from behind the anterior
axillary line, the muscle is transposed into the thoracic cavitythrough the window thus formed in the thoracic wall (b).The muscle is elevated and placed loosely between the tra-chea and the esophageal bridge graft. The muscle is fixed tothe cartilaginous part of the trachea with a few sutures (c).The muscle should not be fixed to the pars membranacea.
a
b
c

Late post-operative complications
� Esophageal cul-de-sac is a typical change ob-served after shunting operations of the esopha-gus.The following are the indications for correc-
tive surgical intervention in cul-de-sac syn-drome:� Retention of food in the cul-de-sac� Regurgitation of food� Severe esophagitis.
31 Post-operative Complications of the Esophagus and Esophagus Bridge Graft � 367
Fig. 31.8a,b. Dissection of the esophagus below the cervi-cal anastomosis and blind closure of the aboral end of theesophagus. This corrective surgery can be performed only ifa minimum length of the stricture is still patent; otherwise,there could be a risk of retention of the secretions, leadingto bacterial growth. If there is no minimum passage in thestricture, an esophagectomy must be performed right afterthoracotomy.
a b

� D. C. Broering et al.368
a b
a b
Fig. 31.9a,b. A second alternative is to separate the colonicbridge graft from the cervical esophagus and to transpose itinto the right thoracic cavity. Intrathoracic anastomosis ofthe esophagus with the colonic bridge graft directly abovethe stricture. The access is gained via a cervical incision ex-tending below up to the abdomen. Intrathoracic transposi-tion and anastomosis via a right thoracotomy.
Fig. 31.10a, b. The simplest corrective surgery is a closureof the colon-gastrostomy and anastomosis of the distal endof the colonic bridge graft with a Roux-y loop of the jeju-num.

31 Post-operative Complications of the Esophagus and Esophagus Bridge Graft � 369
Fig. 31.11a,b. A trunk vagotomy with pyloroplasty may beperformed as an alternative.
Fig. 31.12a–d. A classical esophageal bridge graft of the je-junum (Roux-Hertzen – Yudin) can lead to severe intestinaldisturbances. A majority of the symptoms can be eliminatedby resection of a jejunum segment directly above the jejuno-jejunostomy, taking care to avoid trauma to the jejunal vas-cular arcade and to the anastomosis of the jejunum with thestomach.
The late post-operative complications of a colonic bridgegraft include an undesirable lengthening of the colon withdifficulty in passage. The preferred corrective surgery in thiscase is a resection of the excessively long colonic segmentand end-to-end anastomosis of the ends of the colon. Atrauma to the colonic vessels can be avoided by skeletoniz-ing the intestine very close to the intestinal wall.
a b c d
a b

� D. C. Broering et al.370
Fig. 31.13a,b. Resection of an excessively long colonic bridgegraft.In principle, the vessels draining the colonic bridge graft shouldnot be traumatized during resection of a colonic segment.
a
b

� Cicatrized stenosis of an esophago-gastrostomy or esophago-colostomy(pharyngeo-gastrostomy or pharyngeo-colostomy)
Surgery is indicated only if conservative therapy fails.
31 Post-operative Complications of the Esophagus and Esophagus Bridge Graft � 371
a b c
Fig. 31.14a–c. Transverse incision of the colon above thestrictured anastomosis. Circular excision of the stricture andadaptation of the mucosal border with interrupted sutures5 mm apart (Vicryl 4/0). The intrathoracic and intraabdomi-nal strictures can be managed similarly.
Fig. 31.15a, b. In some cases, a complete excision of thestrictured segment with end-to-end anastomosis is necessary.Surgery must always be followed by intraluminar decompres-sion and external drainage of the operative area. a b

� Cicatrization and deformationof the pyloric region
The pyloric region can undergo deformationand stenosis many months and even years afteresophageal resection with interposition of thestomach, causing severe dysphagia.
372
Fig. 31.16. Cicatrization and deformation of the pylorus afterinterposition of the stomach (a). The cicatrized stenosis canbe by-passed by gastro-jejunostomy with a Roux-Y loop (b).Alternatively, the stenosis can be subjected to stricturoplastyby a side-to-side jejunostomy with a Roux-Y jejunal loop (c).
a
� D. C. Broering et al.: 31 Post-operative Complications of the Esophagus and Esophagus Bridge Graft
b c

A
abdomen, drainage 291, 306abdominal esophagus, steno-sis 293
abdominal lymphadenect-omy 85
abdominal segment 4abdominal ultrasound 247abdomino-thoracic en bloc eso-phagectomy 85
accessory left hepatic liver ar-tery 118
achalasia 12– cardiomyotomy 253– – with Thal (Dor) fundo-
plasty 301– dilatation treatment 353– endoscopic treatment 351– endoscopy 23– injection treatment 353additional stent, proximal over-growth 341
adenocarcinoma 20, 72, 89, 91,109
– advanced 247– Barrett’s esophagus 22– distal 247– early (T1b) 90, 248– 3 field en bloc esophagect-omy 104
– mucinous 72– mucoepidermoid 72adenoid cystic carcinoma 72adenosquamous carcinoma 72,92
adult respiratory distress syn-drome (ARDS) 48, 98
advanced carcinoma– chemical destruction 334– distant residual 77
– electro-thermocoagula-tion 334
– esophageal, see esophagealtumor
– exophytic, thermoablativetechnique 335
– laser ablation 334– – stenting 334– loco-regional residual 77– mimicking achalasia 351– obstruction– – bougienage 335– – stent placement 335– overgrowth 336, 341– – sclerotherapy 336– – stent exchange 336– – stenting 336– recurrent 348– resection, endoscopic tech-niques 327
– staging, EUS 335– stenosis, EUS 30– unresectable 335aminopyrine breath test 40anastomosis– Billroth II 233– cervical 111, 140, 153– collar– – esophagojejunal 239– – insufficiency 361– colo-colonic, insuffi-ciency 205
– colo-esophageal, latero-lateral 221
– insufficiency 223– 2-layer esophagogastrost-omy 150
– portocaval 5– postoperative edema 149– Roux-Y 260anastomotic leak rate 101
anastomotic leakage 100, 103,104, 149
anastomotic stenosis, risk 162Angelchik prosthesis 62, 67,260
angle of His 123, 273anisoperistaltic colonic inter-position 216
anterior hiatoplastic 259antibiotic prophylaxis 335,345, 351
– perioperative 275antireflux barrier 51, 52anti-reflux surgery 264– advantages 60– breakdown of the repair 67– disadvantages 60– failures 67, 264– Gastric pull through 66– inappropriate surgery 66– MIC 303– obstructions 66– re-operative surgery 67– therapy, conservative 264aorta 191, 310– abdominal 193– bifurcation 192– descending 132– injury 155– thoracic 4– tumor infiltration 155aortic arch 4aortic cuff 155appendectomy, prophylactic 209arcade– of Riolan 211, 212– paracolic 211, 212argon laser 333argon plasma coagulation 316,327, 334, 348, 350, 355, 356,357
Subject Index

arterial blood gas analysis 41arterial blood supply 4arterial catheter 44arterial O2 partial pressure(PeO2) 40
artery– accessory left hepatic 182– carotid 86, 144– – common 3– – external 245– celiac 248– colic left226– colon, middle 226– colonic 214, 216– – left 213, 214, 215– – middle 212, 213, 214, 215– facial 245– gastric 182, 189– – left 5, 85, 120, 139, 157,
182, 249– – right 190, 201– gastroepiploic 182, 304– – left 116, 183, 202– – right 116, 139, 157– hepatic 185, 190, 203, 248– – common 120, 122, 190,
202– – lymphadenectomy 249– jejunal 234, 245– lingual 245– longitudinal network 5– mesenteric– – inferior 212, 213– – superior 193– – pericardiac-phrenic 364– phrenic 5– pulmonary 4, 365– rectal inferior 213– renal, left 193– sigmoid 211, 212, 213, 214– – first 213, 215– splenic 5, 85, 120, 122, 185,188, 189, 203, 248
– lymphadenectomy 249– subclavian 4, 5– suprarenal 193– thyroid 243– – inferior 4, 145– – superior 5, 245ASA classification39ascending colon 207aspiration 43, 45atraumatic hydrophilic guide-wire 342
Auerbach plexus 23axial sliding hernia 21
B
Baby-Celestin-tubes 335, 344balloon dilatation 222, 293,335, 345, 348, 349, 350, 351,352
– over a guidewire 352balloon tamponade 315band ligation 315band ligator 327Barrett’s– esophagus 21, 22, 54, 247– – high grade dysplasia 334– segment 249– – long 247– epithelium 20basaloid squamous cell carcino-ma 72
Belsey procedure 62benign stenoses, dilatation 345,346
benign tumor– endoscopy 20– esophageal 109– excision 307– irresectable 223– leiomyomas 307– thoracoscopic resection 307Bezotome 326Bezotriptor 326big biopsy 89Billroth II anastomosis 233biopsy– diagnostic accuracy 20– endoscopic 20, 333, 348, 351– multiple, pre-therapeutic diag-nostic 79
bleeding, upper gastrointesti-nal 22
– non-variceal 316, 317blood group 315body temperature, intraopera-tive control 47
Boerhaave’s syndrome 22, 157,283
bolus obstruction 324, 326,336
botulinum toxin 351, 352bougienage 293, 335, 338, 341,347, 348, 349, 350
– dilatation 222
– perforation 347– scars or webs 349bougies 335bowel preparation 205brachial fistula 275brachiocephalic trunk 129bronchial bifurcation 297– diverticula 297bronchography 11bronchoscopy 335, 341bronchus, main 175, 311
C
candida 21carcinoma– adenocarcinoma, see adeno-carcinoma
– adenoid cystic 72– adenosquamous 72– cardia 89, 92, 185, 205– – advanced 199– choriocarcinoma 72– early carcinoma of the eso-phagus 73
– esophageal, see esophagealcarcinoma
– esophageal-gastric junc-tion 89, 157
– esophagus– – early 20, 73– – N/pN classification 75– – regional lymph nodes 73,
84– gastric, see gastric carcinoma– gastroesophageal junc-tion 92, 264
– lymphoepithelioma-like 72– mucoepidermoid 72– scirrhous 14– small cell 72– spindle cell 72– squamous cell, see squamouscell carcinoma (SCC)
– total gastrectomy with lym-padenectomy, T1 N0 92
– uncommon 72– undifferentiated 72– verrucous 72cardiac arrhythmia 361cardiac risk 41cardiocirculatory depres-sion 46
cardiomyopathy 44, 302
� Subject Index374

– achalasia 253cardiopulmonary complica-tions 260, 314
cardiopulmonary insuffi-ciency 171, 185, 199, 205,223, 253, 293
catheter jejunostomy 362, 363caustic ingestion 345caustic injury 235cecum 207Celestin -tubes 335celiac trunk 85, 92, 120, 122,182, 185, 189, 202, 203, 249
– dissection of the lymphnodes 117
– lymph nodes 91, 93central venous line 44cervical anastomosis 111, 140,153
cervical anastomotic leak 222cervical approach, left 293cervical diverticula 11, 275– endoscopic treatment 275– transoral treatment 298cervical esophago-colostomy,strictures 222
cervical esophagus 3, 90, 217,284, 336
cervical incision 225, 310– oblique 311cervical lymph nodes 5, 73, 82,97, 100
cervical pharyngeo-colostomy,strictures 222
cervical plexus 86cervical sphincter, completemyotomy 99
cervical stage, transhiatal sub-total esophagectomy 144
cervico-mediastinal lymphade-nectomy 86
C-factor 77chemoradiation, neoadju-vant 91
chemoradiotherapy 31– adjuvant 102, 104– adjuvant preoperative 102– induction 89chemotherapy/radiotherapy,neoadjuvant preoperative 98
chest drainage 48chest tube 155cholecystolithiasis 264choriocarcinoma 72
chromoendoscopy 327, 328,333
chromoscopy 20chylothorax 171cicatrized stenoses– esophago-gastrostomy 371– pharyngeo-colostomy 371– pharyngeo-gastrostomy 371circular myotomy, abdominalesophagus 265
circular stapler 165clamp resection 135clipping 317clips, application 315, 317,318, 319, 331
coagulation status 315, 355coagulation, argon plasma 316collar anastomosis, insuffi-ciency 361
collar esophagostomy 361, 362,363
collar stenosis 293collar vascular connection 243collecting sacs 324Collis gastroplasty 65colo-colonic anastomosis, insuf-ficiency 205
colo-esophageal anastomosis,latero-lateral 221
colo-esophagostomy– intrathoracic, right 229– latero-lateral 227– – left 224colo-gastrostomy 206– intraabdominal termino-lateral 224
– transverse 228colon interposition 90, 92, 93,205, 223, 230
– anisoperistaltic 211– intrathoracic esophago-plasty 223
– Korbhenkel bypass 224– left-sided isoperistaltic 212– posterior mediastinum 219– short 226colon– flexure, splenic 209– kinking 219– necrosis 205colonic bridge graft 367, 369– necrosis 362colonic flexure, right 207,208
colonic interposition, complica-tions 222
colonic segment– anisoperistaltic 211– selection 210colon-interposition 224, 227,228
– intrathoracic bypass 225– isoperistaltic 226colonoscopy, total 205color Doppler ultrasound 28,33
columnar epithelial-lined loweresophagus (CELLO) 72
common bile duct 117compartment -3 resection 192complicated reflux disease 260computed tomography(CT) 16, 247, 326
– accuracy 25– distant metastasis 81– guided transthoracicbiopsy 33
– multislice 16conic reduction plastic 161,163
continuous positive airway(CDPA) 47
contrast esophagographie 11contrast, water soluble 326coronary angiography 44coronary artery disease 44creatinin clearance 41cuff-folds 262cuff-rupture 260cul-de-sac- syndrome 367cytomegalovirus (CMV) 21
D
denervation syndrome 260diagnostic accuracy, biopsy 20diaphanoscopy 247, 249diaphragm– incision 186– – median 254– posterior crura 305– right crus 304diaphragmatic flap 283– preparation 280diaphragmatic perdicledflap 290
diaphragmotomy 157diffuse esophagospasm 24, 253
Subject Index � 375

dilatation 337– achalasia 354, 535– endoscopic 253, 264, 323– fluoroscopic monitoring 354– hemorrhage 336– re-stenoses 350dilation tube 301discontinuity resection 36,3632
dislocation, stents 341dissection of the lymph nodes,hepatic artery 117
disseminated disease 98distal stopper, stent 341, 344distant abdominal lymphnodes 84
distant metastases, esophagealcancer 31
distant metastasis, CT 81distant residual tumor 77diverticula 11– cervical 11, 75, 275– – endoscopic treatment 275,
355– – transoral treatment 298– endoscopy 23– epiphrenic 12, 23, 275, 278,279, 351
– epiphrenic thoracoscopic ex-tirpation 298
– false 355– incision of the septum 355– MIC 297– mid-esophageal 275– parabronchial, excision 299– posterior pharyngeal 11– pulsion 297– resection 274– tracheobronchial 4– traction 12– Zenker 23, 355– – endoscopic treatment 356diverticulitis 275DNA analysis 75Dormia basket 324, 326double lumen endotrachealtube 46
double lumen insufflationstube 308
down-hill varices 23duodenal ulcer 199, 264duodenogastroesophageal re-flux 52
dye solution 333
dysphagia 11, 12, 15, 258, 275,299, 301, 305
– postoperative 262
E
early adenocarcinoma(T1b) 90, 248
early cancer, lymph nodespread 84
early carcinoma of the esopha-gus 73
– classification 20early metastatic potential, eso-phageal cancer 82
early tumor staging, endoscopicultrasound 31
echocardiography 41, 44echoendoscope 19electrocautery 327, 348, 350– short stenoses 345electronic radial echoendo-scopes 27
embolic complications, N-butyl-2-cyanoacrylate 323
emergency thoracotomy 247en bloc transthoracic esopha-gectomy 100
endobrachyesophagus 72endo-clips 331– perforation 331endodissection 314– of the esophagus 311, 312endoprosthesis 335endoscopic biopsy 20, 333,348, 351
endoscopic clipping 352, 357– perforation 347endoscopic dilatation 253, 264,323
– tumor stenosis 30endoscopic examination 19endoscopic hemostasis 23endoscopic mucosal resection(EMR) 327, 328, 329, 330,334
– cap 329– hemorrhage 331– perforation 332– surveillance 331endoscopic occlusion, esophago-tracheal fistula 343
endoscopic removal, foreignbodies 324
endoscopic techniques, esopha-geal diseases 315 f.
endoscopic therapy, stric-tures 293
endoscopic ultrasound(EUS) 19, 21, 25, 27, 351
– accuracy 29– examination technique 27– re-staging of esophageal can-cer 31
– tumor staging 25, 31, 327– tumor stenosis 3– guided fine needle aspiration(EUS ± FNA) 28, 29, 32, 33,81, 327, 333, 348
– – accuracy 33– – complications 33endoscopy 355, 361– intraoperative 301, 302, 307endoscopy-controlled incision,hard scars 349
endosonographic examination,injection treatment 353
endosonography 18, 247endothoracic membrane 217end-to-end stapler 152end-to-side stapler 154epidural catheter 45epigastric lymphadenect-omy 111
epinephrine solution 328, 331epiphrenic diverticula 23, 275,278, 279, 299, 351
– thoracoscopic extirpa-tion 298
eradication, esophagealvarices 319, 320
ergometry 41erosive reflux disease 52esophageal anterior-wall muscu-lature, resection 257
esophageal bridge graft 364,366
– of the jejunum 369esophageal carcinoma– diagnosis 14– distant metastasis (M/pM)
76– early metastatic potential 82– grading 72– indicator of outcome 78– lymphatic invasion 77– MIC 308– stage grouping 76
� Subject Index376

– staging 25– subtotal gastrectomy 205– superficial 73– tumor classification 71– typing 72esophageal cul-de-sac 367esophageal diseases, endoscopictechnique 315 f.
esophageal diverticula, resec-tion 274
esophageal fistula 205– perforation 283– surgical treatment 283esophageal hiatus 270, 273esophageal motility 299esophageal peristalsis,GERD 53
esophageal resection, total 220esophageal spasm, diffuse, longmyotomy 302
esophageal sphincter– lower 3, 51, 52, 248, 259,298, 353
– – myotomy 299, 300– – pressure 45– upper 3– – complete myotomy 298esophageal stricture– benign 230– carcinoma 222– distal esophageal third 223esophageal stump 149esophageal superficial carcino-ma 73
esophageal tumor, benign, localexcision 281
esophageal tumors 14– benign 15– diagnosis 14esophageal varices 13– eradication 315, 319, 320esophageal wall– anterior, dissection 312, 313– structure 9esophageal-gastric junction, car-cinoma 157
esophagectomy– abdomino-thoracic enbloc 85
– abdominothoracic subtotal enbloc 171
– en bloc transthoracic 100– extended– – 3 field 97
– – – en bloc 97– – – – adaenocarcinoma
104– – – – advantages 98– – – – complications 101– – – – disadvantages 98– – – – results 100– – 2 field (en bloc)– – – results 99esophagectomy– radical en bloc 81– randomized trials 102– subtotal 89– – jejunal interposition 233– survival 101– thoracoscopic 314– thransthoracic– – en bloc 89, 90– – open 314– total, jejunal interposi-tion 233
– transhiatal 92, 100, 274– – subtotal 109– – – operative risk 109– transhiatal blunt 109esophagitis 21– complications 22– viral 21esophago-colostomy 223– cicatrized stenoses 371esophago-fundo-phrenicopexia260
esophagogastrectomy 247– transhiatal 199esophagogastric junction 257,301
– diverticula 297esophagogastroscopy 149, 247– cicatrized stenoses 371– circular stapler 197esophagogastrostomy– antirefluxive 196– complete 151– intrathoracic 185– telescopically 169– termino-terminal 194esophagojejunostomy 233,236
– insufficiency 247– intrathoracic 233– termino-lateral 237, 239,247, 251
esophagoplasty, local 293esophagoprobe 30
esophagoscopy, intraopera-tive 247, 249
esophagospasm, diffuse 24esophagostomy, side-to-side 296
esophago-tracheal fistula 20– EUS 27esophagus bridge graft, post-operative complications 361
esophagus carcinoma– early 73– N/pN classification 75– regional lymph nodes 73esophagus– anatomic subdivision 71– cervical, exposure 206– development 4– diagnostic methods 11– distal– – adenocarcinoma 199– – peptic stenosis 157– – ruptures 157– – squamous cell carcino-
ma 157– examination 11– fistula 284– intraabdominal fistula 288– long strictures 185– short 13– topography 3– transhiatal dissection 203esopohagogastrostomy 310examination technique,EUS 27
extended lymph node dissec-tion 97, 102
extensive stricture 109extubation 48
F
feeding tube 348fiberoptic bronchoscope 47fibrin glue sealing 341, 3422-fields lymphadenectomy 893-fields lymph node dissec-tion 84, 102
– extended 973-fields lymphadenectomy 86,89, 98
3-fields esophagectomy, caseselection 100
fine needle aspiration 28fistula 364
Subject Index � 377

– cervical esophagotra-cheal 344
– conservative therapy 284– curettage 342– esophageal 205– esophageal, endoscopic tech-niques 341
– esophago-bronchial 341– esophago-mediastinal 335,342
– esophagopleural, transhiatalclosure 289
– esophago-tracheal 11, 20,286, 335
– external 284– graft metal 364– internal 284– intraabdominal 288– intrathoracic 287– non healing 341– palliative operation 283– radical operation 284– salivary 361– tracheobronchial 4– transhiatal closure 291Flankennähte 306flexible retractor 311floppy, fundoplication 261floppy-Nissen 67, 262flow cytometry 75fluoroscopic examination 352– perforation 336fluoroscopic monitoring, dilata-tion 354
Foley catheters 324foreign bodies 14, 324– aspiration 326– endoscopic removal 324– extraction, perforation 326– fluoroscopy guided removal324
free jejunal interposition 90,93
fundal varices 13fundophrenicopexia 259fundoplasty (Dor, Thal) 260,302, 303
fundoplication 61, 262, 267,288, 291
– 3-fields 306– floppy 261– laparoscopic 62– – complication rate 62– – modified 266
– – Nissen 61– – partial 65, 66, 260, 273– – posterior 65– – total 260fundus rotation gastro-plasty 181, 182
G
Gadolinium DTPA 16gas-bloat syndrome 260gastrectomy 89gastric carcinoma 92gastric decompression 280gastric depletion disorder 260gastric feeding tube, temporary347
gastric interposition 310gastric mobilization 182gastric outlet obstruction 143,269
gastric patch 300gastric pull-up 148– presternal 148gastric tube 90, 256, 266, 272,280, 282, 296, 299, 303, 311
– construction 111– diameter 142– fixation 167– formation 140, 181– isoperistaltic 141– length 157– necrosis 109, 205, 357– pull-up, retrosternal 148– transposition 114, 147, 171gastric vagal branches 249gastric vessels, short 250gastric volvulus 269gastric wall– ischemia 140– retroesophageal pull-through 305
gastrocolic ligament 115gastroepiploic vessels 115– right 199, 200gastroesophageal (GE) junc-tion 23
– anatomical reconstruc-tion 259
– carcinoma 89, 92, 264– en bloc resection 248– isoperistaltic jejunal interposi-tion 247
– tumors 91
gastroesophageal reflux 13, 52gastroesophageal reflux disease(GERD) 21, 51, 259
– Barrett’s syndrome 59– columnar lined esopha-gus 59
– definition 51– diagnostic test 51– duodeno-gastroesophageal re-flux 54
– esophageal peristalsis 53– gastroduodenal disorders 54– hiatal hernia 53– incident of adenocarcino-ma 60
– indication for surgery 54– intestinal metaplasia 51– intraabdominal pressure 53– laparoscopy 259– manometry 52– mucosal resistance 54– prevalence 51– proton pump inhibitors 59– respiratory complications59
– stricture formation 59– surgical management 59– symptoms 52gastrointestinal bleeding,upper 22
gastrointestinal tract, lower,reconstruction 206
gastro-jejunostomy, with Roux-Yloop 372
gastropexia 259gastroplasty 157– fundus rotation 181, 182gastroscopes– large working channels 324,355
– with dual channel 355gastrostomy 361GENEVAL-consensus confer-ence 51
GIST 27glycogenic acanthosis 19grater omentum 157, 187, 199,208
grater omentum flap 292greater curvature– mobilization 304– skeletonization 115, 116, 160guidewire 335, 337, 351– biliary 346
� Subject Index378

– flexible atraumatic biliary348
– hydrophilic 342, 345– hydrophilic biliary 346– atraumatic 342, 346, 347– – with flexible tip 337– standard 348
H
Heineke Mikulicz, stricturo-plasty 294
hemangiomas 20hematogenous spread, metasta-sis 97
hemicolectomy, interposi-tion 214
hemicolon, right, isoperistalticinterposition 216
hemifundoplication– anterior 260– posterior 260hemorrhage 48, 155, 331hemorrhagic esophagitis 22hepatic artery 85hepatoduodenal ligament 85,91, 92
– lymphadenectomy 116hepatogastric ligament 118hernia– axial sliding 21– cardiofundal 268– combined 259– hiatal 260, 268– – combined 269– – reduction 303– – repair 252– – sack 271– – sliding 259– – techniques 264– – GERD 53– hiatus 13– – sliding 13– paraesophageal 21, 259,261, 268, 269
herniorrhaphia 259herpes simplex virus (HSV)21
heterotopic gastric (columnar)mucosa 19
HF generator 327hiatoplasty– anterior 292– bilateral 273
– posterior 272, 273, 292, 303,305
hiatutomy, lateral 223high compliance balloons 351Hill procedure 62histoacryl 23histological regression, neoadju-vant treatment 78
Horner’s syndrome 109hydrophilic guidewire 341hyperalimentation 205hypertonic saline 336hypoglossus nerve 86hypovolemic shock 315hypoxia 47
I
iatrogenic lesions 315ileo-sigmoid ostomy 214iliac crest 366immunocytochemistry 75incision– left costal 254– subcostal 261– upper abdominal trans-verse 254, 261
– upper midline 181, 254– upper transverse 157indigo carmine 327, 328, 333induction chemotherapy 89induction radiochemotherapy89
injection catheter 351injection of steroid 345, 348– stenoses, follow- up 350injection treatment 316, 352– achalasia 353– endosonographic examina-tion 353
injury– direct suture 284– corrosive, grading 283– foreign body 283– grade 1-corrosive 283– penetrating 283– radiation 283– superficial 283innervation, esophagus 8inoperable patients 335Inoue technique 330insufficient length, colonic seg-ment 222
intermittent clamping 206
intestinal metaplasia 22intraluminal decompres-sion 371, 287
intraluminal injury 109intraluminal tube 296intrathoracic anastomosis157
intrathoracic bypass 224– colon-interposition 225– distal esophagus 227intrathoracic esophagoplasty,colon interposition 223
intrathoracic stenosis 293intravenous antibiotic thera-py 275
irresectable benign tumor 223irresectable carcinoma, loweresophageal third 223
isolated tumor cells (ITC) 75– bone marrow 76– non-regional lymphnodes 76
– regional lymph nodes 75isoperistaltic colonic interposi-tion, right hemicolon 215
Ivor-Lewis esophagectomy 98,99, 101
J
jejunal bridging graft 241jejunal graft, free 243, 244,245, 246
jejunal interposition 93– isoperistaltic 251– necrosis 247– total esophagectomy 233jejunal interposition, subtotalesophagectomy 233
jejunal loop 92jejunal stoma 235jejunal vascular arcade 369jejunogastrostomy 233, 247– latero-lateral 252– termino-lateral 252jejuno-jejunostomy 369– terminoterminal 236, 239,252
jejunostomy 362, 363– catheter 362, 363– Roux-en-Y 236, 237– side-to-side, with Roux-Yjejunal loop 372
– termino-terminal 240, 247
Subject Index � 379

K
Killian’s triangle 11, 23, 275,276
kinking of the colon 219kinking of the interposi-tion 222
Kocher maneuver 111, 114,157,191
Kocher’s collar incision 86Korbhenkel type bypass 230
L
Laimer’s triangle 275, 276lamina epithelialis 9lamina muscularis mucosae 9lamina propria mucosae 9laparoscopic antireflux surgery,controversies 65
laparoscopic fundoplication 62,305
– complication rate 62, 63– dysphagia 63– mortality 64– para-esophageal hiatus herni-tation 63
– perforation of the gastrointes-tinal tract 64
– port sites 303– pulmonary embolism 64– splenic injury 63– vascular injury 63laparoscopic Nissen fundoplica-tion 65
laparoscopic operations, fail-ures 67
laparoscopic Toupet fundoplica-tion 65
laparoscopy, GERD 259laparotomy– median 205, 264, 268– – epigastric 223– upper 182– upper abdominal 261– upper midline 110– transverse lower abdom-inal 205
large bowel mobilization 206large working channels, gastro-scopes 324
large-bore bougie 300laryngeal nerve 85– recurrent, paresis 222
laryngoscope, self-retrain-ing 298
laser ablation 327laser treatment 3352-layer anastomosis, esophago-gastrostomy 150
leakage from anastomoses 48left triangle ligament 113, 186left-sided double lumentube 46
leiomyoma 15, 20– EUS 21– nucleation 282– thoracic esophagus 281, 282leiomyosarcoma, EUS 21ligament– colico-phrenic 209– esophageal– – lateral 131, 155– – – right 131– – – left 132– gastrophrenic 123– gastrosplenic 304– hepatoduodenal 202– – lymphadenectomy 201, 203– phrenico-colic 209– – right ligament 208– phrenicoesophageal 123– phrenicogastric 202– pulmonary 131, 172, 173ligamentum teres cardio-pexy 62
ligamentum teres-plasty 259,263
light diffuser 333limited resections 93linear stapler 135, 182, 201,212, 221, 251, 276, 278, 297,298, 299, 300
lipomas, EUS 21liver cirrhosis 23liver metastasis 93liver, left lobe 186, 249, 301– lateral 270local intraluminal treatment,laser 85
local recurrence, esophagealcancer 31
loco-regional residual tumor77
long Barrett’s segment 92, 247long colonic bridge graft, resec-tion 370
longitudinal myotomy 255
Lugol’s solution 20, 327, 328,333
lung function tests 43lung retractors 309lymphadenectomy 85– abdominal 85– abdominothoracic subtotal enbloc esophagectomy 174
– celiac trunk 202– epigastric 111– 2 field 89, 103– – extended 99– 3 field 86, 89, 103– hepatic artery 249– mediastinal 180– – paraaortic 180– – retropericardial lymph
nodes 180– middle colic vessels 187– paraaortal 179, 192, 202– paraaortic, right 191– paracaval 191, 192– posterior mediastinum 136– retropancreatic 191– splenic artery 249– supraradically 192– transhiatal esophagect-omy 85
lymphatic system, anatomy 82lymphatic vessels 5– submucous layer 10lymph-node 8– affected by micrometasta-sis 84
– anatomical nomenclature 8– bronchopulmonary 8– celiac trunk 9, 73, 91, 93– cervical 5, 73, 74, 82, 97, 100– – dissection 103– – esophagus 111– – metastases 101– – recurrence 99– – unsuspicious 89– clearance 91– coeliacal 8– cranial paraesophageal 177– diaphragmatic 8– dissection 117– – 3-fields 84– – hepatic artery 117– – mortality 103– – principles 81– – radical 100– – survival rates 103
� Subject Index380

– distant abdominal 84– gastric 8– gastric superior 83– mediastinal 8,16, 73, 75, 161– – middle 82– – superior 82– metastasis– – frequency 81– – mapping 83– paraaortic 120– paraesophageal 5, 16– perigastric 8, 73– prevertebral 5, 8– recurrence 98– regional 5, 73, 74, 75– – compartments 74– – intrathoracic esophagus 75– – mediastinal compart-
ment 75– – perigastric compart-
ment 75– resection, radical 97– retrotracheal 176– subcarinal, lymphadenec-tomy 178
– supraclavicular 16– tracheal bifurcation 310lymphoepithelioma-like carcino-ma 72
M
malignancy, early, classifica-tion 20
malignant hyperthermia 45Mallory Weiss lesions 315, 317,318, 319
– recurrent bleeding 323Mallory-Weiss tear 22manometry 24, 259, 351– dilatation 354manubrium sterni 218Mark IV operation 260meatballs, obstruction 326mechanical echoendoscopes 27medastinum, dorsal 271median epigastric laparo-tomy 223
mediastinal drainage 361mediastinal lymph nodes,lower 83
mediastinal pleura 165, 278,310
– rupture 217
mediastinal visceral pleura, in-jury 155
mediastinitis 109, 223, 247,275, 283, 323, 326, 331, 332,352, 361
mediastinoscope, modified 312mediastinum– drainage 153, 165– posterior 273– – colon interposition 219– – inferior 249– – lymphadenectomy 136– – tamponade 155– superior 4medullary carcinoma 14megaesophagus 109megaesophagus congenitus 12membranes (webs) 348Merendino procedure 93mesocolon 251mesosigmoid 209metaplastic mucosa 248metastatic potential, early eso-phageal cancer 82
methylene blue 20, 22, 327,328, 333
MIC 297micrometastasis 75– lymph node groups 84– occult 82microscopic skip metastasis 77Mikulicz retractor 111, 128,131
miniprobes 19, 30, 31– EUS 27– N-staging 32Minnesota tube 315mortality rate 101motility disorders, MIC 301MRI 16MRI probes, intraluminal 18M-staging, EUS 27mucinous adenocarcinoma 72mucoepidermoid carcinoma 72multifocal high grade dyspla-sia 334
multiple linear stapler 250multiple-band application 320multi-slice CT accuracy 29– imaging 16multi-stage procedure 233muscle– cricopharyngeal 11, 275, 276– latissimus dorsi 364
– – flap 366– longissimus cervicis 3– lower pharyngeal constrictor,myotomy 276
– omohyoid 144, 311– pharyngeal constrictor 276– – myotomy 277– sternocleidomastoid 144,145, 217, 225, 276, 284, 285,311
– trapezius 86muscle-flap 285myocardial infarction 44myotomy– circular, abdominal esopha-gus 265
– cricoparyngeal 297– extramucosal 300– laparoscopic with fundoplasty,port side 301
– long 307– longitudinal 255– lower esophageal sphincter299
– margins 256– risk of perforation 301
N
narrow stenoses 337, 346nasal intubation 45naso-gastric probe 286naso-gastric feeding tube 162naso-gastric tube 47, 150, 152,195, 273, 303, 306, 336, 355,357
– enteral feeding 345– postoperative edema 149N-butyl-2-cyanoacrylate 323Nd-YAG laser 334, 335neck anastomosis, alternativemethods 154
neck dissection 86, 90, 98neck emphysema 283necrosis of the colon 199, 205necrosis of the interposi-tion 222
needle knife 327, 331, 357needle-knife papillotome 348,349
neoadjuvant chemoradia-tion 91
neoadjuvant preoperative che-motherapy/radiotherapy 98
Subject Index � 381

neoadjuvant treatment, effectiv-ity (Ef) 78
neoadjuvant treatment, histolog-ical regression 78
neoadjuvant treatment, tumorregression grade (TRG) 78
neo-esophagus, affection 205neo-fundus 247, 248, 250, 252nerve supply, esophagus 10nerve– esophageal plexus 9– laryngeal nerves 86– parasympathetic 8– phrenic 85, 364– – right 172– – injury 101, 104, 109– – palsy 103– – pareses 171– reccurent 4– – laryngeal 98, 145, 147, 171,
174– – – injury 101, 104, 109– – – palsy 10– – – pareses 171– – – right 172– – left 313– symphathic nerve 8– vagus 9,10,125,131,171, 174,186, 247, 249, 254, 301,303,304
– – dorsal branch 304net retriever basket 326Nissen fundoplication 61, 259,260
– laparoscopic 65– outcomes 62Nissen– floppy 67– slipped 66Nissen-Rossetti procedure 67,260
nitrous oxide 45nocturnal heartburn 12nonerosive reflux disease 52non-Hodgkin’s lymphoma 28N-staging– CT 17– EUS 27nutcracker esophagus 24nutrition tube 275nutritional status 43
O
obliteration, esophagealvarices 315
obstructions, malignant tu-mors 335
occult micrometastasis 82omentum, lesser 249one-lung ventilation 47operating times 103operation, exclusion 41operative mortality 99operative risk profile, evalua-tion 39
optional categories, TNM sys-tem 76
outflow obstruction 253over-tube 320, 324, 325, 326
P
pain therapy, postoperative 48palliative esophageal resec-tion 93
palliative radiochemother-apy 93
palliative resection 109pancreas 188, 200pancreatic capsule 200pancreatic corpus, dissec-tion 193
pancreatic head 189pancreatic tail 188, 189pancreatitis 109, 199, 247paraaortal region 203parabronchial diverticulum exci-sion 299
paravariceal sclerotherapy 23parental nutrition 253, 336,347, 352
parietal pleura, tumor infiltra-tion 135
partial abdominothoracic resec-tion 157
– parietal cell vagotomy259, 265, 267
partial fundoplication 65, 66,258
pathologic classification, eso-phageal carcinoma 71
pediatric endoscope 20, 337,338, 341, 349
penrose drain 153peptic stenosis 13, 260
peptic stricture 22, 109, 266,267
– techniques 264– total esophagus 205percutaneous endoscopic gastro-stomy (PEG) 336
percutaneous endoscopic jeju-nostomy (PEJ) 335, 336
perforation 11, 275– clipping 332– fluoroscopic examina-tion 336, 347
– foreign bodies extrac-tion 326
– mediastinitis 357– pneumomediastinum 357– sclerotherapy 323– stenting 323pericardial flaps 364, 365pericardial infiltration 134perioperative antibiotic thera-py 110
perioperative ECG 43perioperative opioid applica-tion 181
peritonitis 109, 247, 352perivascular injection 320pH manometry 21pH metry-24-hours 259pharmacotherapy, varicealbleeding 315
pharyngeo-colostomy 212– cicatrized stenoses 371– latero-lateral 220pharyngeo-gastrostomy 152– cicatrized stenoses 371photodynamic therapy 84, 327photodynamic therapy oftumors (PDT) 327, 333
– efficacy 333– high grade dysplasia,Barrett 333
– ineffectiveness 334– non-resectable carcinoma333
– photosensitivity 333– strictures 334– superficial spreading tumor333
– surveillance biopsy 334photosensitizer 333phrenic crura 272phytobezoar 326piriform fossa 152
� Subject Index382

plastic stent 339, 341pletyhsmography 41pleura– empyema 109, 223,247, 283– flap 279, 286– parietal 218– visceral 218pleural cavity, drainage 280,287, 291
pneumatic dilation 303pneumonia 109– post-operative 101pneumothorax 48, 155, 331– laparoscopic fundoplica-tion 63
3-point support, fundoplica-tion 306
polidocanol 319, 336polyposis of the interposi-tion 222
poor nutritional status 43Porfimer-Sodium 333portal hypertension 22, 23portocaval anastomose 5positive endexpiratory pressure(PEP) 47
positron emission tomography(PET) 18, 29
– accuracy 29post operative adjuvant thera-pies 98
posterior fundoplication 65postoperative hemody-namic 222
postoperative hypotension 48postoperative management 43postoperative pain 181postoperative pain therapy 48postoperative parameter 222postoperative pneumonia 98,101
postoperative reflux 247postoperative stenosis, preven-tion 151
postoperative suture dehis-cence 11
postoperative ventilation 47pre treatment lavage 351preliminary treatment– ethanol 336– hypertonic saline 336– isopropanol 336– polidocanol 336premedication 44
preoperative autologous blooddonation 44
preoperative chest X-ray 43preoperative evaluation, risk 43preoperative imaging 91preoperative irradation 16preoperative laboratory test-ing 44
preoperative management 43,110
preoperative radiochemother-apy 81, 91
– combined 90preoperative respiratory status43
pressure, lower esophagealsphincter 45
prestenotic dilatation 296prestenotic esophagus, lavage345, 348
pre-therapeutic diagnostics79
– chromoendoscopy 79– cytological examination 79– multiple biopsies 79– total biopsies 79prophylactic antibiotics 335,351
prosthesis, positioning 341protective accessories 325proton pump inhibitors(PPI) 59, 60, 259, 334, 347
proximal dislocation,stents 344
proximal jejunum 251proximal resection 185proximal stomach, adenocarci-noma 199
pseudodiverticula 23pulling thread 341pull-through procedure 218pulmonary artery catheter 44pulmonary complications 103,109
pulmonary function 41pulmonary function test 247pulmonary infections 222pulmonary ligament 86purse string clamp 250pusher 341pyloric region– cicatrization 372– deformation372pylorotomy 143
R
R2category, subdivision 77radical en bloc esophagect-omy 81
radical lymph node resec-tion 97, 100
radiochemotherapy– adjuvant 104– adjuvant preoperative 102– induction 89– preoperative 81, 91– – combined 90radiography 335, 341, 351, 355rat-tooth forceps 326recess– left piriform 225– right piriform 225recessus piriformis 220reconstruction, trans-mediastinal 92
recurrence rate, en bloc eso-phagectomy 98
recurrences 93– carcinoma of the gastroeso-phageal junction 93
recurrent laryngeal nerve 311recurrent laryngeal nervepalsy 298
red color signs 23reflux disease 260, 315, 317,345
– erosive 52– nonerosive 52reflux prevention 258reflux-related esophageal ulcers324
regurgitation 275re-operative surgery– antireflux operation 67– approach 68– mortality rates 68resection rate, esophageal carci-noma 99
residual tumor (R), classifica-tion 77
respiratory insufficiency 48respiratory therapy 41re-staging of esophageal cancer,EUS 31
retractors, mediastinal 132retroesophageal mobiliza-tion 303
retroesophageal tunnel 303
Subject Index � 383

retroesophageal window 261retrosternal tunnel 218Riffini bodies 10risk ascertainment, meth-ods 39
risk minimization, preopera-tive 40
risk of bleeding, varices 23risk of recurrence, carcinoma ofthe cardiac 92
risk, definition 39Rochard retractor 111, 112,261
Roux-Y anastomosis 260Roux-Y loop 368rubber band ligation 23, 316,321, 322, 323
– EMR 330
S
sagittal diaphragmatomy 185,290
Savary Miller– classification 21– dilator 341, 345, 348– guidewire 338, 339, 346scirrhous carcinoma 14sclerodermia esophagus 24,66
sclerotherapy 315, 336– additional treatment 323– intravascular injection 316– of varices, recurrent bleed-ing 323
– perforation 323– stricture 323self expanding metalstents 335
Senkstaken-Blakemoretube 315
septic complications 222sero-muscular U-stitches196
short Barrett’s segment 93short esophagus 13short gastric vessels 120, 202,304
short peptic stricture 293short scarred stenosis 293Sial retractor system 112Siewert’s classification 90, 92sigmoid colon, mobiliza-tion 209
silicone antireflux prosthe-sis 260
simple reflux disease 260single lung ventilation 157, 171single-band application 320six-shooter 320slippage, prevention 305slipped Nissen 66small cell carcinoma 72spindle cell carcinoma 72spleen, injury 199splenectomy 185, 188splenic transaction 189squamocolumnar junction(Z-line) 22
squamous cell carcino-ma(SCC) 20, 72, 73, 89, 90,91, 109
– prognostic score 73– recurrence 97staging of esophageal cancer25
standard esophagectomy,results 98
stapler 141– introduction 169stenotic esophageal anato-moses 348
stenotic scars 324stent– Choo-stent (Korean) 343– covered 336– covered metal 341– exchange 336– Gianturco-stent 343– insertion 347– instruments 339– intolerance 336, 341, 344– migration 339, 341, 343– placement 93, 335– plastic stent (Celestin) 343– proximal correction 343– sealing 341– self expanding metalstent 343
– Strecker-stent 343– trachea 343– uncovered metal 336– Wall-stent 343sternotomy 86sternum 217Stiegman-Goff 321stomach tube, distal 194stress ECG 44
stricture– cicatricial 220– endoscopic dilatation 259– injection needles 348– intraabdominal 371– intrathoracic 371– of the esophagogastric junc-tion 267
– sclerotherapy 323stricturoplasty 259, 294, 372stricturotomy 350subcutaneous tunnel 235submucosal layer 9submucosal lymphatic vessels10, 92
subphrenic area, drainage 153,157
substernal fascia 218substernal tunnel 206, 216, 217– drainage 221– opening of the pleura 222subtotal esophagectomy 89subtotal proximal gastric resec-tion 92
supra-bifurcational trachea364, 365
supraphrenic region, drainage165
symbol descriptors TNM system– � symbol, TNM system 76– m symbol, TNM system 76– r symbol, TNM system 76– y symbol, TNM system 76sympathic nervous system 10synchronous chemotherapy 97systemic dissemination, esopha-geal carcinoma 84
systemic recurrence, esophagealcarcinoma 99
T
T/pT classification 73T1m tumors 31T1N0 carcinomas, total gastrect-omy with lymphadenect-omy 92
T1sm tumors 31TA stapler 182telescopphenomenon 260, 262temporary clamping 234temporary stoma 233ten-shooter 320terminal ileum 216
� Subject Index384

Terumo 346thermal treatment 348thermoablation 327, 336– surveillance 331thoracic aorta 4thoracic drainage 171, 181,229, 279, 282, 310, 314
thoracic duct 3, 9, 85, 90, 180,308, 310
– laceration 155thoracic epidural catheter 44,48
thoracic esophageal by-pass 225
thoracic esophagus– en bloc-resection 161– leiomyoma 281, 282– lower, 91– upper 90thoracic peridual catheter247
thoraco-abdominal– en bloc esophagectomy 91– esophagectomy 92thoracoscopic mobilizationof the esophagus, port sites309
thoracotomy– anterolateral 85, 157, 171– – right 161, 223, 275, 282,
293– emergency 247– right 155– right-lateral 286thymectomy 86thyroid cartilage 144thyroid gland 3T-incision, inverted 110, 111,171,199, 293
– low 205, 206tissue necrosis 335TMN supplement(UICC 2003) 75
TNM classification, C-factor(certainly factor) 77
TNM/pTNM classification73
TNM system, symbols– � symbol 76– m symbol 76– r symbol 76– y symbol 76toluidine blue 22topography 3
total gastrectomy with lympha-denectomy, T1 N0 carcino-mas 92
total intravenous anesthesia(TIVA) 44
Toupet fundoplication, laparo-scopic 65
trachea 175, 310– membranaceous part 130,176
– supra bifurcation 364, 365tracheal bifurcation 4, 85, 129,136, 180, 313, 364
– lymph nodes 310tracheal compression 339, 341tracheobronchial diverticula 4tracheobronchial fistula 109tracheostomy 101, 103, 104traction diverticula 12transhiatal blunt esophagealdissection, complications155
transhiatal closure, esophago-pleural fistula 289
transhiatal esophageal dissec-tion 111, 121
transhiatal esophagectomy 92,100
– lymphadenectomy 85transit time, esophagus 3transnasal tube 227, 229transthoracic en bloc esopah-gectomy 89, 90
transthoracic resection 90transverse colon 199– mobilization 208transverse-sigmoidostomy 221treacheoesophageal septum 4truncal vagotomy 185– with pyloroplasty 369T-shaped, inversed incision247
T-staging– CT 17– EUS 25
U
UICC TNM classification 25umbrella 324– protector 325uncommon carcinomas 72undifferentiated carcinoma 72univent tube 46
unsuspicious cervical lymphnodes 89
up-side-down stomach 21, 269ureter, left 209U-shaped sutures 151, 168
V
vagal plexus 4, 310vagal trunk– anterior 4– posterior 4vagotomy 260– partial cell 259, 265, 267– truncal 185– truncal with pyloroplasty185
valsalva maneuver 13valvuloplasty 260variceal eradication 23varices 13, 22– bleeding, risk 23– down hill 23– esophageal 13– – eradication 319, 320– – obliteration 315– fundal 13vascular pedicle, long 226vascular stapler 307, 308vein– azygos 5, 85, 130, 172, 173,178, 229, 286, 287, 288, 307,308, 310, 313
– hemiazygos 5– – injury 155– – patch 287– caval 191, 192– – superior 85, 171, 172, 173,
174, 175– coronary 5– gastric– – left 120– – omental 185– – short 157– intercostals 178– jejunal 244– jugular 5, 144– – internal 3– phrenic 126– – inferior 128– portal 117, 190– pulmonary 311, 365– renal 191, 192– splenic 188
Subject Index � 385

– thyroid 243– – inferior 5vena anonyma 174venous drainage 5venous patch 288verrucous carcinoma 72videoendoscopes 19viral esophagitis 21vital capacity (VC)40
W
webs, congenital 348Willis loop 301
X
xiphoid 216
Z
Zenker’s diverticulum 11, 23,275, 276, 277, 297
� Subject Index386












![Color atlas and textbook of human vol 1 [werner platzer]](https://img.pdfslide.us/doc/110x75/545345dfaf7959257f8b50ea/color-atlas-and-textbook-of-human-vol-1-werner-platzer.jpg)