Embed Size (px)
Citation preview

University of Birmingham
Surgery in the era of the 'omics revolutionBeggs, A. D.; Dilworth, M. P.
DOI:10.1002/bjs.9722
License:Creative Commons: Attribution (CC BY)
Document VersionPublisher's PDF, also known as Version of record
Citation for published version (Harvard):Beggs, AD & Dilworth, MP 2015, 'Surgery in the era of the 'omics revolution', British Journal of Surgery, vol. 102,no. 2, pp. e29-e40. https://doi.org/10.1002/bjs.9722
Link to publication on Research at Birmingham portal
Publisher Rights Statement:Eligibility for repository : checked 03/02/2015
General rightsUnless a licence is specified above, all rights (including copyright and moral rights) in this document are retained by the authors and/or thecopyright holders. The express permission of the copyright holder must be obtained for any use of this material other than for purposespermitted by law.
•Users may freely distribute the URL that is used to identify this publication.•Users may download and/or print one copy of the publication from the University of Birmingham research portal for the purpose of privatestudy or non-commercial research.•User may use extracts from the document in line with the concept of ‘fair dealing’ under the Copyright, Designs and Patents Act 1988 (?)•Users may not further distribute the material nor use it for the purposes of commercial gain.
Where a licence is displayed above, please note the terms and conditions of the licence govern your use of this document.
When citing, please reference the published version.
Take down policyWhile the University of Birmingham exercises care and attention in making items available there are rare occasions when an item has beenuploaded in error or has been deemed to be commercially or otherwise sensitive.
If you believe that this is the case for this document, please contact [email protected] providing details and we will remove access tothe work immediately and investigate.
Download date: 30. Apr. 2020

Review
Surgery in the era of the ’omics revolution
A. D. Beggs and M. P. Dilworth
Translational Surgical Biology Laboratory, School of Cancer Sciences, University of Birmingham, Vincent Drive, Birmingham B15 2TT, UKCorrespondence to: Mr A. D. Beggs (e-mail: [email protected])
Background: Surgery is entering a new phase with the revolution in genomic technology. Cheap, massaccess to next-generation sequencing is now allowing the analysis of entire human genomes at the DNAand RNA level. These data sets are being used increasingly to identify the molecular differences thatunderlie common surgical diseases, and enable them to be stratified for patient benefit.Methods: This article reviews the recent developments in the molecular biology of colorectal, oesopha-gogastric and breast cancer.Results: The review specifically covers developments in genetic predisposition, next-generationsequencing studies, biomarkers for stratification, prognosis and treatment, and other ’omics technologiessuch as metabolomics and proteomics.Conclusion: There are unique opportunities over the next decade to change the management of surgicaldisease radically, using these technologies. The directions that this may take are highlighted, includingfuture advances such as the 100 000 Genomes Project.
Click here to listen to the author discuss the contents of this article.
Paper accepted 20 October 2014Published online in Wiley Online Library (www.bjs.co.uk). DOI: 10.1002/bjs.9722
Introduction
The field of molecular biology has undergone rapidadvancement in the past 5 years, with exciting conse-quences for the diagnosis, treatment and follow-up ofsurgical patients.
A series of enabling technologies and projects haveexpanded the knowledge of how basic molecular biol-ogy can assist in the management of surgical disease.The first, and most important, was the Human GenomeProject, established in 1990 by the US National Insti-tutes of Health and the UK Sanger Centre1. Thisestablished the reference human genome by carryingout sequencing of multiple fragments of a referencehuman genome using the dye-terminator techniquedescribed by Sanger and colleagues2. A consequence ofthis technology is that the project took 10 years to pro-duce a single genome and cost over US $3 billion tocomplete.
The development of microarray technology andnext-generation sequencing (NGS) within the past 5 yearshas led to a step-change in the implementation of genomictechnologies; before this, the bulk of genetic research wascarried out on DNA microarrays.
Genome-wide association studies
DNA microarrays are available from a variety ofmanufacturers (Illumina, Affymetrix and Agilent) andconsist of silicon or glass slides with oligonucleotidescomplementary to the DNA sequence being studied,which are annealed to their surface. This allows cheap,mass production of microarrays that can be used for largepopulation-based studies. Typically these microarrayshave between 500 000 and 1⋅5 million genomic mark-ers, usually single-nucleotide polymorphisms (SNPs).SNPs are single-nucleotide changes within a gene thatlead to protein change and subsequent change in thefunction of that gene. When scanned with a laser,each individual oligonucleotide fluoresces a specificcolour, depending on the bound oligonucleotide fragment(Figs 1 and 2).
A variety of projects have been undertaken usingDNA microarrays, typically taking the form of thegenome-wide association study (GWAS). These areusually case–control studies with cases enriched for thedisease of interest. SNPs of interest are identified andtaken forward to validation in larger cohorts, givinginsights into the disease process being studied. Examples
© 2015 The Authors. BJS published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.This is an open access article under the terms of the Creative Commons Attribution License, which permits use, distribution and reproduction in any medium,provided the original work is properly cited.

e30 A. D. Beggs and M. P. Dilworth
Fig. 1 Image of scanned oligonucleotide array (from WikimediaCommons)
of GWASs include the COGENT (COlorectal cancerGENeTics) Consortium, and the Wellcome Trust CaseControl Consortium 1/2 (WTCCC 1/2) examiningcolorectal cancer, Crohn’s disease, diabetes, ischaemicheart disease, and several other common diseases andpathologies.
Next-generation sequencing
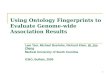
The most widely used NGS technology, sequencing bysynthesis (Illumina, San Diego, California, USA) allowsentire human genomes to be sequenced within 24 h atlow cost, with the sub $1000 genome barrier (X-prize)being achieved earlier this year. Other innovative tech-nologies include single molecular real-time sequencing(PacBio® SMRT™; Pacific Biosciences, Menlo Park, Cal-ifornia, USA), semiconductor sequencing (Ion Torrent™;Life Technologies, Paisley, UK) and nanopore sequenc-ing (Oxford Nanopore, Oxford, UK). Until recently,NGS was limited to small studies on a few samplesowing to cost constraints, but because of the rapid fallin price-per-sample (Fig. 3), large studies are now inprogress. The Cancer Genome Atlas (TCGA) projectis sequencing the cancer genome of 33 different cancertypes in the US population; the 100 000 Genomes Projectin the UK is undertaking to sequence 50 000 cancergenomes and 50 000 rare disease genomes over the next5 years.
Fig. 2 Affymetrix microarray chip from Wikimedia Commons
To carry out NGS, an inherently massively parallel tech-nique, several steps are required. All technologies requirecapture of DNA or RNA into sequencing libraries. Illu-mina Solexa™ then uses this captured DNA/RNA to gen-erate clusters, which are amplified. Cluster amplificationis the process whereby target DNA is immobilized onto spatially separated template sites, allowing sequencingreactions to occur in parallel. Sequencing is then carriedout on the clusters present on the glass slide. The slide isportioned into eight channels, enabling independent sam-ples to be run simultaneously. Typically, reads of between75 and 100 base pairs are possible, and the nucleotide incor-poration cycle is repeated until sufficient depth is coveredfor all targeted regions. Data generated are then alignedwith a reference sequence, and variants are called aftercomparing the sequencing data to a reference. This allowsa tumour specimen to be compared with its paired normaltissue sample.
A critical difference in analysis of human cancers is theconcept of germline and somatic mutations. Germlinemutations are the constitutive DNA that the patient isborn with, and variation within the germline confers anincreased (or decreased) risk of cancer. Somatic mutationsoccur as a consequence of tumour development, althoughthey may initiate tumour development by occurring
© 2015 The Authors. BJS published by John Wiley & Sons Ltd www.bjs.co.uk BJS 2015; 102: e29–e40on behalf of BJS Society Ltd.

Surgery in the era of the ’omics revolution e31
100
Sept 2
001
Dec 2
002
Oct 20
03
Aug 2
004
Nov 2
005
Sept 2
006
Dec 2
007
Oct 20
08
Aug 2
009
Nov 2
010
Sept 2
011
Dec 2
012
Oct 20
13
Mar
201
4
1000
10 000
100 000
Cos
t per
gen
ome
(US
$)
1 000 000
10 000 000
100 000 000
Fig. 3 Cost in US dollars per genome sequenced in 2001–2014, at 5-month intervals (data from http://www.genome.gov/sequencingcosts/)
spontaneously as a result of external factors such asionizing radiation or carcinogens.
Microarray and sequencing technologies also allowanalysis of other types of genetic information, such asDNA methylation (epigenetics), which acts as a switchin the regulation of gene expression. NGS also allowsanalysis of gene expression by NGS of mRNA (RNA-seq)and other genetic modifications, such as sequencingof chromatin-immunoprecipitated DNA (ChIP-seq).Non-coding small RNAs that may affect gene function,such as long non-coding RNA (lncRNA), small interferingRNA (siRNA) and small nucleolar RNA (snoRNA), canalso be analysed by NGS.
Other ’omics technologies
Other technologies are emerging as potential methods forthe downstream analysis and stratification of patient sam-ples in surgical disease. Two examples of these technolo-gies are metabolomics and proteomics. Metabolomics useseither nuclear magnetic resonance or mass spectrometryto ascertain the presence of metabolites in surgical speci-mens. The patterns and relative abundances of the metabo-lites observed can give clues as to the underlying biologicalprocesses at work in the tissues studied3.
Proteomics uses mass spectrometry to understand thestructure of proteins. Several methods exist to allowproteins to be studied in the ionized form without
fragmentation or damage including matrix-assistedlaser desorption ionization (MALDI)4 and electrosprayionization5. Because proteins are modified after they areproduced by transcription (post-translational modifica-tion), study of both the protein and RNA involved intissues allows a fuller appreciation of the changes that maybe occurring in a particular disease.
These technologies have allowed advances in under-standing of the initiation and progression of multiplesurgical diseases, and in adjuvant therapies for surgicaldisease such as chemotherapy and radiotherapy. Theyalso allow the possibility of population screening ofasymptomatic carriers.
Lower gastrointestinal tract: colorectal cancerand inflammatory bowel disease
Genetic predisposition
The predominant surgically relevant disease types stud-ied in the lower gastrointestinal (GI) tract have been col-orectal cancer, Crohn’s disease and ulcerative colitis. TheCOGENT Consortium6 has undertaken multiple GWASsof patients with colorectal cancer associated with a strongfamily history or extreme phenotype (such as young age ofonset), identifying ten SNPs associated with colorectal can-cer at population-wide significance. Although inheritanceof one disease association SNP confers a population risk ofodds ratio approximately 1⋅05 (Table 1, taken from Tenesa
© 2015 The Authors. BJS published by John Wiley & Sons Ltd www.bjs.co.uk BJS 2015; 102: e29–e40on behalf of BJS Society Ltd.

e32 A. D. Beggs and M. P. Dilworth
Table 1 Frequency of identified single-nucleotide polymorphisms in colorectal cancer, and their effect sizes (from Tenesa and Dunlop7)
Gene/locus Chromosome SNP Effect size (odds ratio) Allele frequency Population attributable risk (%)
– 8q24 rs6983267 1⋅21 (1⋅15, 1⋅27) 0⋅51 9⋅7GREM1 15q13 rs4779584 1⋅26 (1⋅19, 1⋅34) 0⋅18 4⋅5SMAD7 18q21 rs4939827 1⋅18 (1⋅12, 1⋅23) 0⋅52 8⋅6– 11q23 rs3802842 1⋅12 (1⋅07, 1⋅17) 0⋅29 3⋅4EIF3H 8q23 rs16892766 1⋅25 (1⋅19, 1⋅32) 0⋅07 1⋅7– 10p14 rs10795668 1⋅12 (1⋅10, 1⋅16) 0⋅67 7⋅4
BMP4 14q21 rs4444235 1⋅11 (1⋅08, 1⋅15) 0⋅46 4⋅8CDH1 16q22 rs9929218 1⋅10 (1⋅06, 1⋅12) 0⋅71 6⋅6RHPN2 19q13 rs10411210 1⋅15 (1⋅10, 1⋅20) 0⋅90 11⋅9BMP2 20q12 rs961253 1⋅12 (1⋅08, 1⋅16) 0⋅35 4⋅0
Values in parentheses are 95 per cent c.i. SNP, single-nucleotide polymorphism.
and Dunlop7), inheritance of multiple SNPs (more than10) confers a cumulative threefold risk of cancer. Othersuccesses from the GWAS/NGS approach have been iden-tification of the GREM-associated duplication in heredi-tary mixed polyposis syndrome8 and mutations in the DNApolymerase genes POLE and POLD as a cause of hereditarypolyposis9. Identification of these mutations allows familialtesting, enhanced surveillance and reduction in the risk ofdeveloping colorectal cancer.
In Crohn’s disease, multiple large-population GWASstudies10 have been undertaken identifying multiple SNPsof predisposition, suggesting that Crohn’s disease has astrong heritable component. In total, more than 73 SNPshave been identified, with the strongest association in theNOD2 gene, which plays an important role in immunity. Intotal, these loci make up about 20 per cent of the observedinheritability of Crohn’s disease.
Comparatively less research has been undertaken ingermline susceptibility to ulcerative colitis; several largepopulation GWAS studies11–13 have demonstrated over 30associated SNPs. These SNPs are in a variety of genes,but are associated predominantly with immune system andimmunity-related genes. In addition, approximately 50 percent of identified loci overlap with those of Crohn’s disease.
Genomic analysis of colorectal cancer
The colorectal cancer TCGA project14 has carried outexome sequencing (sequencing of the protein codingregions of the genome), RNA-seq, genome-wide methyla-tion analysis and protein expression (via reverse-phase pro-tein arrays; RPPAs) of, at the time of writing, 461 colorectaltumours. This group has confirmed recurrent driver muta-tions in APC, TP53, SMAD4, PIK3CA and KRAS, butalso found novel therapeutic targets in ARID1A, SOX9and FAM123B. Another study15 observed gene fusions(merging of two genes, which causes abnormal function)in R-spondin. The mutations observed in ARID1A are
Table 2 The Colorectal Cancer Subtyping Consortiumclassification of colorectal cancer
Classifier Frequency (%) Characteristics
CMS1 14 MSI, immune pathwayactivation/expression, right-sidetumours, older age at diagnosis,females, hypermutation, BRAFmutation, intermediate survival
CMS2 41 High CIN, MSS, strong Wnt/Mycpathway activation, left-sidetumours, TP53 mutation, EGFRamplification/overexpression, bettersurvival
CMS3 8 Low CIN, moderate Wnt/Myc pathwayactivation, KRAS mutation, PIK3CAmutation, IGFBP2 overexpression,intermediate survival
CMS4 20 CIN/MSI heterogeneous,mesenchymal/TGF-β activation,younger age at diagnosis,NOTCH3/VEGFR2 overexpression,worse survival
CMS, Colorectal cancer Molecular Subtype; MSI, microsatelliteinstability; CIN, chromosomal instability; MSS, microsatellite stable;TGF, transforming growth factor.
particularly exciting as they present a potential therapeutictarget16. These data sets provide a wealth of informationabout colorectal cancer, and linkage to a clinical data setprovides opportunities for future biomarker studies.
Recent work has examined the role of integration of mul-tiple ’omics data sets to produce classifiers of disease17, alsoknown as endotypes. These are based on mutation, expres-sion and immunological data sets. The Colorectal CancerSubtyping Consortium found four distinct Colorectalcancer Molecular Subtypes (CMSs) (Table 2). The clas-sifiers identified provide insight into the biology of thedistinct types. CMS1 consisted of microsatellite-unstable,immunologically active tumours occurring mainly onthe right side in the elderly, whereas CMS2 (the mostfrequent endotype) consisted of chromosomally unstable,microsatellite-stable tumours. Further study of these
© 2015 The Authors. BJS published by John Wiley & Sons Ltd www.bjs.co.uk BJS 2015; 102: e29–e40on behalf of BJS Society Ltd.

Surgery in the era of the ’omics revolution e33
classifiers may permit finer stratification, allowing preciselytargeted therapy.
Screening biomarkers
A wide variety of biomarkers have been examined18 incolorectal cancer, as both markers of screening and ofprognosis. The ideal biomarker would be easily detectablein either stool or blood, cheap and highly accurate.Unfortunately, no current biomarker fits these criteriaprecisely owing to the molecular heterogeneity associatedwith colorectal cancer. The most promising markers seemto be associated with abnormal DNA methylation. Forexample, in colorectal cancer, differential methylation ofthe septin 9 gene has been shown to have 72 per centsensitivity and 90 per cent specificity for the detection ofmalignancy. However, many biomarker studies across allcancer types are plagued by poor study design, insuffi-cient power and non-hypothesis-driven marker selection.Currently, a well designed, UK-based trial of methylatedbiomarkers, the ENDCaP-C study (Enhanced NeoplasiaDetection and Cancer Prevention in Chronic Colitis)is under way19, examining their value in the detectionof dysplasia in a screened population of patients withulcerative colitis.
Another rich field of developing interest in colorectalcancer is sequencing of the microbial genomes that existwithin the colon. Experimental murine models seem toindicate that the microbiome within the colon alters therisk of colorectal cancer by modulating inflammation20.This has also been demonstrated to be the case in patientswith inflammatory bowel disease, for both ulcerative colitisand Crohn’s disease21.
Metabolomic techniques also show promise in acting asscreening biomarkers. Mirnezami and co-workers22 under-took high-resolution magic-angle spinning nuclear mag-netic resonance spectroscopy in 44 tumour–normal pairs,finding cancer-specific metabolite patterns allowing differ-entiation of cancer from normal tissues, in addition to find-ing changes in the metabolome as the tumour progressed.A number of proteomic studies have also been carried outin colorectal cancer23, although these all suffer from lack ofvalidation, and the variety of different markers identifiedundoubtedly reflects the varying populations from whichthey were sampled.
Targeted therapies, prognostic and predictivebiomarkers
The discovery that the epidermal growth factor (EGF)pathway in colorectal cancer was sensitive to inhibition by
anti-EGF receptor (EGFR) monoclonal antibodies (mAbs)led to the rapid development of panitumumab and cetux-imab. However, it was found in initial trials that theantibodies seemed to have no clinical effect against col-orectal cancer; although a proportion of patients seemedto benefit from therapy, the majority did not24. It wasfound subsequently that mutations in the EGFR path-way genes (KRAS, BRAF, NRAS and PIK3CA) conferredresistance to anti-EGFR mAbs due to hyperactivation ofthe pathway independent of the EGFR25. The CRYSTALtrial26 compared patients with a KRAS mutation and thosewithout, finding a clear response and survival benefit foranti-EGFR mAbs in patients without mutation. A num-ber of other pathway-specific inhibitors exist for colorectalcancer, including the antivascular endothelial growth fac-tor (VEGF) mAb bevacizumab, MEK inhibitors that tar-get EGF pathway mutated cancers and cancer vaccines.The FOCUS4 trial27 is currently recruiting patients for amolecularly stratified trial of metastatic colorectal cancertherapy: patients are selected for a specific therapy whenthey possess a mutation specific to that cancer. This raisesthe intriguing possibility of molecular-targeted therapy forprimary, non-metastatic tumours as neoadjuvant therapybefore surgery.
A commercially available test exists for prediction ofrecurrence and benefit for 5-fluorouracil chemother-apy (Oncotype DX®; Genomic Health, RedwoodCity, California, USA), based on a multigene panel ofRNA expression from formalin-fixed paraffin-embeddedtissues28. This was developed by screening 761 candidategenes against a large cohort of 1851 patients undergoingsurgery for colorectal cancer, with or without adjuvant5-fluorouracil therapy. Validation was carried out on theQUASAR study29, which could stratify prognosis, but didnot correlate with benefit from chemotherapy.
Another intriguing possibility is the use of immune-basedstratification to estimate colorectal cancer prognosis. Lalet al.30 used the TCGA expression data set to identifyfour different immune classifiers based on the expres-sion of immune system-related genes. Immunogenicity isthought to be related to survival, as tumours that aremore visible to the immune system are more likely toundergo destruction by the immune system. One of themechanisms that may occur in highly mutated tumours,such as tumours with a POLE mutation or those withmicrosatellite instability, is where the large number ofmutations causes a variety of frameshift mutations. Theseframeshift mutations drive the production of neoantigens31
caused by the alternative splicing of multiple genes, whichincreases the visibility of the tumour to the immunesystem.
© 2015 The Authors. BJS published by John Wiley & Sons Ltd www.bjs.co.uk BJS 2015; 102: e29–e40on behalf of BJS Society Ltd.

e34 A. D. Beggs and M. P. Dilworth
Upper gastrointestinal tract: oesophagogastriccancer
Genetic predisposition
Research into predisposition to gastro-oesophageal canceris complicated by the fact that it can arise in two histolog-ically different epithelial types: squamous cell carcinoma(SCC) and adenocarcinoma. A significant proportion of therisk is likely to comprise lifestyle factors such as smoking,gastro-oesophageal reflux and diet.
In adenocarcinoma, a GWAS of the premalignant stageof oesophageal cancer32, Barrett’s oesophagus, demon-strated associations between the major histocompatibilitylocus and a gene associated with oesophageal development(FOXF1). It was also found that the predisposition to Bar-rett’s oesophagus was made up of multiple common vari-ants of small effect, rather than a single genetic driver. Afurther GWAS of oesophageal adenocarcinoma32 demon-strated associations with transcription factors (CRTC1,FOXP1, BARX1). In light of these results it is difficult tohighlight SNPs that may act as markers for increased dis-ease risk or act as molecular targets for therapy.
Several GWAS studies have been undertaken, predomi-nantly in Chinese populations at high risk of oesophagealSCC33,34. They highlighted SNPs in the riboflavin trans-porter C20orf54, and a cell growth and differentiationgene, PLCE1. Riboflavin deficiency was identified beforethis study as a risk factor35 for oesophageal SCC. ThePLCE1 variant was further found to interact specificallywith tobacco smoke exposure36.
Genomic analysis of oesophagogastric cancer
Both the Broad Institute (Cambridge, Massachusetts,USA) and the OCCAMS (Oesophageal Cancer Clinicaland Molecular Stratification) Consortium have stud-ied oesophageal adenocarcinoma. The Broad Instituteproject37 undertook whole-exome and whole-genomesequencing in 149 tumour–normal pairs, verifying previ-ously identified mutations in TP53, CDKN2A, SMAD4,ARID1A and PIK3CA. Previously unidentified mutationsin SPG20, TLR4, ELMO1 and DOCK2 were also found,and a possible role for the RAC1 pathway (a modulator ofepithelial–mesenchymal transition) was identified.
The OCCAMS Consortium38 examined whole-genomesequencing of oesophageal adenocarcinoma, as well as tar-geted sequencing of never-dysplastic Barrett’s oesophagus(which did not progress to malignancy) and high-gradedysplasia. They found that TP53 was the dominant muta-tion seen in adenocarcinoma, in over 80 per cent ofsamples, but that these mutations were also present in
biopsies from never-dysplastic patients, contrary to whatwas expected based on the known oncological progressionof these lesions. The only stage-specific mutations seen inhigh-grade dysplasia and adenocarcinoma were in TP53and SMAD4.
Whole-genome and whole-exome sequencing ofoesophageal SCC has also been performed39. Whole-genome sequencing of 17 tumour–normal pairs andwhole-exome sequencing in a further 71 tumour–normalpairs identified recurrent mutations in TP53, RB1,CDKN2A, PIK3CA, NOTCH1 and NFE2L2, as well asADAM29 and FAM135B. The genomic landscape ofoesophageal SCC was significantly different from that ofoesophageal adenocarcinoma, highlighting the differenttherapeutic strategies that are needed in this disease.
Biomarkers of predisposition/sensitivityand screening
Given the above OCCAMS findings, it is difficult to useTP53 mutation as a biomarker of adenocarcinoma, as ithas also been identified in biopsies from never-dysplasticpatients, who should not progress to adenocarcinoma. Asa precursor to the OCCAMS study38, the same groupundertook combined-array CGH (comparative genomichybridization, a type of microarray analysis looking atchromosomal abnormalities) in tumour samples and geneexpression via microarray40. They found a pattern ofcopy number alterations and associated expression changethat could identify poor-prognosis oesophageal adenocar-cinoma. The OCCAMS group also examined gene expres-sion changes in adenocarcinoma using RNA microarrays41,finding a four-gene expression panel of DCK , PAPSS2,SIRT2 and TRIM44 that were independently predictive ofsurvival.
There have been a number of attempts at developingmethylated biomarkers in oesophageal adenocarcinoma,both as screening biomarkers and to identify high-risk Bar-rett’s oesophagus. The genes studied include CDKN2A,vimentin, P14ARF, CDX2, SOCS1/3, SFRP1/2/4/5 andWIF142–44. Unfortunately no consistent marker can beidentified that successfully differentiates adenocarcinomafrom normal oesophagus and high-grade Barrett’s dyspla-sia. These types of focused biomarker will become increas-ingly important to stratify therapy.
Attempts have been made using proteomics45 to dis-tinguish oesophagogastric cancer from benign disease, toallow screening. MALDI mass spectrometry was used tocompare the differences between oesophageal cancer andnormal mucosa, and gastric cancer and normal mucosa.It was found that, although there were clear differences
© 2015 The Authors. BJS published by John Wiley & Sons Ltd www.bjs.co.uk BJS 2015; 102: e29–e40on behalf of BJS Society Ltd.

Surgery in the era of the ’omics revolution e35
between cancer and normal tissue, there was a wide varietyof changes that varied between different tumours, makingdetermination of a specific biomarker difficult.
Targeted therapies
Despite the recent advances in discovery science ingastro-oesophageal cancer, few therapeutic targets cur-rently exist. A small proportion of cancers overexpress thehuman EGFR 2 (HER2) protein46, and clinical trials oftrastuzumab, a mAb against the HER–receptor complexare ongoing. The ToGA (Trastuzumab for Gastric Can-cer) study47 investigated the addition of trastuzumab tostandard chemotherapy, and demonstrated a small survivalbenefit in HER2-positive cancer. Targeting by anti-VEGFtherapy is also undergoing clinical trials48; however, resultshave been mixed with no improvement in overall survival,but improvements in response rates and progression-freesurvival.
Breast cancer
Genetic predisposition
The role of inherited variability in breast cancer hasbeen investigated extensively. A very strong signal forvariants in the fibroblast growth factor receptor 2 gene(FGFR2) have been found in GWAS studies across mul-tiple populations49–51. Carriers of the two low-risk allelesat FGFR2 (frequency 38 per cent of the population) have arelative risk of breast cancer of 0⋅83 compared with the gen-eral population52; carriers of one high-risk and one low-riskallele (47 per cent) have a relative risk of 1⋅05; and car-riers of two high-risk alleles (14 per cent) have a relativerisk of 1⋅2653. FGFR2 mutations are of particular inter-est as they may represent a therapeutic target in breastcancer54.
A recent GWAS55 in oestrogen receptor (ER)-negativebreast cancer demonstrated four variants that reachedgenome-wide significance in MDM4, LGR6, FTO and aSNP within the 2p24⋅1 region. These SNPs were presentonly in ER-negative breast cancers, in contrast to the find-ings in a combined ER-positive/ER-negative GWAS56.This found variants located with PTHLH, known to havea role in breast development, and NRIP1, a co-factor ofthe ER.
Next-generation sequencing
A number of NGS projects have examined the muta-tion spectrum in breast cancer. The most comprehensiveof these is from the TCGA project57, which carried out
exome sequencing, RNA-seq, methylation array analysisand RPPA of 463 patients. Recurrent mutations were foundin TP53, PIK3CA and GATA3 at frequencies of over 10 percent, reinforcing their role as driver mutations in breastcancer, as well as mutations in several dozen genes pre-viously identified in breast cancer. Study of the role ofexpression subtypes in breast cancer demonstrated fourseparate subtypes (luminal A/B, basal and HER2E), withthe mutational burden and spectrum varying in each. TheHER2E subtype demonstrated a relatively low mutationalfrequency, whereas the luminal A subtype demonstratedlarge numbers of significantly mutated genes, the most fre-quent mutation being in PIK3CA.
In common with colorectal cancer, methylation arrayanalysis of breast cancer revealed a hypermethylator phe-notype, associated with the luminal B expression subtype,and a hypomethylated phenotype associated with a basalexpression subtype and comparatively higher frequency ofTP53 mutation. Copy number analysis was also performed,with the previously identified amplifications in HER2 andEGFR being identified, as well as novel amplifications inPIK3CA and FOXA1 and deletions in RB1 and PTEN .A striking finding throughout the study was the detectionof genetic heterogeneity both within tumours and betweensamples, highlighting the diverse nature of this disease.
Shah and colleagues58 examined the mutational spec-trum in triple-negative breast cancer (ER/progesteronereceptor/HER-negative), again finding that TP53 andPIK3CA mutations were clonally dominant, but also find-ing a wide variety of mutation spectra, including tumourswith few driving mutations and tumours with extremelycomplex mutational spectra (the hypermutated pheno-type). A separate study59 identified recurrent mutations inthe transcription factor genes CBFB and RUNX1, as wellas a gene fusion seen only in triple-negative breast cancers,the MAGI3–AKT3 fusion transcript. An exome sequenc-ing study60 of 100 breast cancers at the Wellcome TrustSanger Institute (Cambridge, UK) identified more than 40driver mutations in a breast cancer cohort, including genesnow known to be important therapeutic targets, such asAKT1/2, ARID1B, CASP8 and MAP3K1.
NGS also has applications in the monitoring ofmetastatic disease or in recurrence. Dawson et al.61
used a combination of targeted NGS, digital PCR andwhole-genome sequencing to examine DNA circulatingin the bloodstream that is shed from metastatic tumours.They found that increasing amounts of circulating DNAcorrelated with poorer overall survival, but also that,by comparing mutations in the primary tumour with thecell-free DNA obtained, recurrence of the primary tumourcould be detected by the presence of the same somatic
© 2015 The Authors. BJS published by John Wiley & Sons Ltd www.bjs.co.uk BJS 2015; 102: e29–e40on behalf of BJS Society Ltd.

e36 A. D. Beggs and M. P. Dilworth
mutations in the circulating DNA. This technology hasapplications for the detection of recurrence in multipletumour types across the disease spectrum.
Biomarkers of predisposition/sensitivityand screening
One-step nucleic acid amplification (OSNA) is an exampleof the use of genetic technologies to stratify patients. Itworks by the detection of raised copy number of the cytok-eratin 19 gene (CK19) as a surrogate marker of the presenceof breast cancer within sentinel lymph nodes62, and is usedas a proxy marker for axillary lymph node positivity inbreast cancer. OSNA has been approved as a technolog-ical solution to determine sentinel lymph node positivityby the UK National Institute for Health and Care Excel-lence (NICE), and has been shown to be equivalent toboth radioisotope- and dye-based technologies for map-ping lymph nodes63.
Another recent development is the DNA dam-age response assay for the prediction of response toanthracycline/cyclophosphamide-based chemotherapy inbreast cancer64. The study examined RNA expressionin patients with a DNA damage response deficiency anddeveloped a 44-gene RNA expression panel that could pre-dict response to chemotherapy in sporadic breast cancer.
Targeted therapies
A rich variety of targeted therapies exist for breast can-cer, based on the underlying biology of the tumour, gainedby the extensive molecular research carried out on breastcancer. Aromatase inhibitors (such as anastrazole) and tar-geted ER modulators (such as tamoxifen) have been usedextensively for many years, based on the observation thata proportion of breast cancers are ER-positive. Identifi-cation of the overexpression of HER2 in breast cancerhas allowed targeting with both mAbs (trastuzumab) andsmall-molecule tyrosine kinase inhibitors such as lapatanib,with appreciable survival benefits.
More recently, several novel pathways have beenidentified as being dysregulated in breast cancer:the insulin-like growth factor (IGF) 1 pathway; theBRCA-associated double-strand break repair pro-tein, poly(ADP-ribose) polymerase (PARP) 1; and thephosphatidylinositol-3-kinase (PIK3)–Akt–mammaliantarget of rapamycin (mTOR) pathway. Immunohisto-chemistry of IGF-1 has revealed that it is overexpressedin more than 50 per cent of breast cancers, and a mAb(cixutumumab) that targets these pathways is currently inphase 1 studies65.
PARP inhibitors were identified from work targetingBRCA mutant breast cancer66 as a therapeutic strategy totreat patients with BRCA mutations. A small molecularPARP inhibitor, olaparib, has been used to treat germlineBRCA mutant breast cancer67, with a clinical trial (theOlympiAD trial) currently under way. PARP inhibitorsalso show promise in triple-negative breast cancer, asstudies have shown that a proportion of these womenpossess BRCA mutations68,69 and may respond to PARPinhibitors. mTOR pathway inhibitors, such as everolimus,should theoretically be of benefit in breast cancer as aresult of the dysregulation of this pathway demonstratedby molecular studies, although initial results have beendisappointing70.
The future
The union of basic biological research with surgeryhas allowed the field of translational surgical biologyto develop, utilizing modern molecular technologies tostratify surgical disease based on therapeutic and outcomeresponse.
A number of possibilities exist for future research.First, whole-genome studies using NGS technologies ofprospectively collected samples will allow identificationof biomarkers for response (such as radiotherapy in rectalcancer) and treatment (for instance, molecularly targetedtherapies). An example of current clinical issues that couldbe answered using this technology is the response ofrectal cancer to radiotherapy. Around 5–10 per cent ofpatients with advanced rectal cancer given preoperativeradiotherapy have a complete response71. Research is cur-rently under way to understand what makes these tumoursparticularly sensitive (the so-called extreme responders) toradiation, and it is likely that a highly focused approachusing NGS will identify responsible pathways.
Stratification of premalignant lesions is also an importantfocus of research. In colorectal, upper GI and breast cancer,few biomarkers exist to predict which premalignant lesionswill progress to invasive cancer. Typically less than 1 percent of patients with Barrett’s oesophagus will progressto invasive oesophageal cancer, but no markers reliablypredict this. The use of retrospective cohorts of patientswith progressive Barrett’s oesophagus and NGS analysismight identify genetic markers.
The concept of disease classifiers will play an increas-ingly important role and, as more NGS data sets becomeavailable, the granularity of classifiers will improve tothe extent whereby a more precise understanding of thebiology underlying a tumour will be available. This willbe enhanced by the integration of multiplatform (NGS,
© 2015 The Authors. BJS published by John Wiley & Sons Ltd www.bjs.co.uk BJS 2015; 102: e29–e40on behalf of BJS Society Ltd.

Surgery in the era of the ’omics revolution e37
metabolomics, proteomics) data into these classifiers, andwill allow tailoring of therapy to the underlying disease.
The availability of NGS data sets for the surgicalpopulation will be enhanced by the commissioningof the UK 100 000 Genomes Project72. This excitingproject will carry out whole-genome sequencing of 50 000tumour–normal pairs from patients with a range of can-cers, but concentrating primarily on colorectal, breast,lung and prostate cancer. The data made available by thisproject will allow a highly detailed examination of thedrivers in these cancer types; this is the largest project ofits type in the world.
Although the technological advances are numerous, theyare not without their own challenges. The recent iden-tification of intratumoral heterogeneity, long hypothe-sized but only recently identified definitively in renal cellcancer73 and in preneoplastic lesions74, provides uniquechallenges for stratification. It is likely that multiple sub-clones of tumour exist within a primary tumour, each withdiffering characteristics. These will dictate prognosis andresponse to therapy, and further investigation is neededto understand the extent and consequences of this phe-nomenon.
Technological leaps in molecular biology will enableselection of the right therapy for the right patient at theright time, and further build on the surgical and anaestheticimprovements achieved in the past century to providemaximal benefit for the patient.
Acknowledgements
A.D.B. is supported by a Wellcome Trust Post-DoctoralFellowship for Clinician Scientists (102732/Z/13/Z).A.D.B. undertakes collaborative research with IlluminaUK into colorectal cancer; sequencing was provided freeof charge by Illumina UK as part of the research project.Disclosure: The authors declare no other conflict of interest.
References
1 Dulbecco R. A turning point in cancer research: sequencingthe human genome. Science 1986; 231: 1055–1056.
2 Sanger F, Nicklen S, Coulson AR. DNA sequencing withchain-terminating inhibitors. Proc Natl Acad Sci U S A 1977;74: 5463–5467.
3 Patti GJ, Yanes O, Siuzdak G. Innovation: Metabolomics: theapogee of the omics trilogy. Nat Rev Mol Cell Biol 2012; 13:263–269.
4 Lattová E, Chen VC, Varma S, Bezabeh T, Perreault H.Matrix-assisted laser desorption/ionization on-target methodfor the investigation of oligosaccharides and glycosylationsites in glycopeptides and glycoproteins. Rapid Commun MassSpectrom 2007; 21: 1644–1650.
5 Ho CS, Lam CW, Chan MH, Cheung RC, Law LK, Lit LCet al. Electrospray ionisation mass spectrometry: principlesand clinical applications. Clin Biochem Rev 2003; 24: 3–12.
6 Tomlinson IP, Dunlop M, Campbell H, Zanke B, GallingerS, Hudson T et al. COGENT (COlorectal cancerGENeTics): an international consortium to study the role ofpolymorphic variation on the risk of colorectal cancer. Br JCancer 2010; 102: 447–454.
7 Tenesa A, Dunlop MG. New insights into the aetiology ofcolorectal cancer from genome-wide association studies. NatRev Genet 2009; 10: 353–358.
8 Jaeger E, Leedham S, Lewis A, Segditsas S, Becker M,Cuadrado PR et al. Hereditary mixed polyposis syndrome iscaused by a 40-kb upstream duplication that leads toincreased and ectopic expression of the BMP antagonistGREM1. Nat Genet 2012; 44: 699–703.
9 Palles C, Cazier JB, Howarth KM, Domingo E, Jones AM,Broderick P et al. Germline mutations affecting theproofreading domains of POLE and POLD1 predispose tocolorectal adenomas and carcinomas. Nat Genet 2013; 4ac5:136–144.
10 Franke A, McGovern DP, Barrett JC, Wang K,Radford-Smith GL, Ahmad T et al. Genome-widemeta-analysis increases to 71 the number of confirmedCrohn’s disease susceptibility loci. Nat Genet 2010; 42:1118–1125.
11 UK IBD Genetics Consortium, Barrett JC, Lee JC, LeesCW, Prescott NJ, Anderson CA et al. Genome-wideassociation study of ulcerative colitis identifies three newsusceptibility loci, including the HNF4A region. Nat Genet2009; 41: 1330–1334.
12 Franke A, Balschun T, Sina C, Ellinghaus D, Hasler R, MayrG et al. Genome-wide association study for ulcerative colitisidentifies risk loci at 7q22 and 22q13 (IL17REL). Nat Genet2010; 42: 292–294.
13 McGovern DP, Gardet A, Torkvist L, Goyette P, Essers J,Taylor KD et al. Genome-wide association identifies multipleulcerative colitis susceptibility loci. Nat Genet 2010; 42:332–337.
14 Cancer Genome Atlas Network. Comprehensive molecularcharacterization of human colon and rectal cancer. Nature2012; 487: 330–337.
15 Seshagiri S, Stawiski EW, Durinck S, Modrusan Z, StormEE, Conboy CB et al. Recurrent R-spondin fusions in coloncancer. Nature 2012; 488: 660–664.
16 Sayegh J, Cao J, Zou MR, Morales A, Blair LP, Norcia Met al. Identification of small molecule inhibitors of JumonjiAT-rich interactive domain 1B (JARID1B) histonedemethylase by a sensitive high throughput screen. J BiolChem 2013; 288: 9408–9417.
17 Dienstmann R, Guinney J, Delorenzi M, De Reynies A,Roepman P, Sadanandam A et al. Colorectal CancerSubtyping Consortium (CRCSC) identification of aconsensus of molecular subtypes. J Clin Oncol 2014;32(Suppl): 5s (Abstract).
© 2015 The Authors. BJS published by John Wiley & Sons Ltd www.bjs.co.uk BJS 2015; 102: e29–e40on behalf of BJS Society Ltd.

e38 A. D. Beggs and M. P. Dilworth
18 Newton KF, Newman W, Hill J. Review of biomarkers incolorectal cancer. Colorectal Dis 2012; 14: 3–17.
19 National Institute for Health Research. EME - 11/100/29:Enhanced Neoplasia Detection and Cancer Prevention in ChronicColitis (ENDCaP-C). http://www.nets.nihr.ac.uk/projects/eme/1110029 [accessed 1 October 2014].
20 Zackular JP, Baxter NT, Iverson KD, Sadler WD, PetrosinoJF, Chen GY et al. The gut microbiome modulates colontumorigenesis. mBio 2013; 4: e00692–e00613.
21 Morgan XC, Tickle TL, Sokol H, Gevers D, Devaney KL,Ward DV et al. Dysfunction of the intestinal microbiome ininflammatory bowel disease and treatment. Genome Biol2012; 13: R79.
22 Mirnezami R, Jiménez B, Li JV, Kinross JM, Veselkov K,Goldin RD et al. Rapid diagnosis and staging of colorectalcancer via high-resolution magic angle spinning nuclearmagnetic resonance (HR-MAS NMR) spectroscopy of intacttissue biopsies. Ann Surg 2014; 259: 1138–1149.
23 de Wit M, Fijneman RJ, Verheul HM, Meijer GA, JimenezCR. Proteomics in colorectal cancer translational research:biomarker discovery for clinical applications. Clin Biochem2013; 46: 466–479.
24 Markman B, Javier Ramos F, Capdevila J, Tabernero J.EGFR and KRAS in colorectal cancer. Adv Clin Chem 2010;51: 71–119.
25 Lièvre A, Bachet JB, Le Corre D, Boige V, Landi B, EmileJF et al. KRAS mutation status is predictive of response tocetuximab therapy in colorectal cancer. Cancer Res 2006; 66:3992–3995.
26 Van Cutsem E, Köhne CH, Hitre E, Zaluski J, Chang ChienCR, Makhson A et al. Cetuximab and chemotherapy as initialtreatment for metastatic colorectal cancer. N Engl J Med2009; 360: 1408–1417.
27 Kaplan R, Maughan T, Crook A, Fisher D, Wilson R, BrownL et al. Evaluating many treatments and biomarkers inoncology: a new design. J Clin Oncol 2013; 31:4562–4568.
28 O’Connell MJ, Lavery I, Yothers G, Paik S, Clark-LangoneKM, Lopatin M et al. Relationship between tumor geneexpression and recurrence in four independent studies ofpatients with stage II/III colon cancer treated with surgeryalone or surgery plus adjuvant fluorouracil plus leucovorin.J Clin Oncol 2010; 28: 3937–3944.
29 Gray RG, Quirke P, Handley K, Lopatin M, Magill L,Baehner FL et al. Validation study of a quantitative multigenereverse transcriptase–polymerase chain reaction assay forassessment of recurrence risk in patients with stage II coloncancer. J Clin Oncol 2011; 29: 4611–4619.
30 Lal N, Beggs AD, Willcox BE, Middleton GW. Animmunogenomic stratification of colorectal cancer:implications for development of targeted immunotherapy.Oncoimmunology 2014; (in press).
31 Maletzki C, Schmidt F, Dirks WG, Schmitt M, LinnebacherM. Frameshift-derived neoantigens constituteimmunotherapeutic targets for patients withmicrosatellite-instable haematological malignancies:
frameshift peptides for treating MSI+ blood cancers. Eur JCancer 2013; 49: 2587–2595.
32 Su Z, Gay LJ, Strange A, Palles C, Band G, Whiteman DCet al.; Esophageal Adenocarcinoma Genetics Consortium;Wellcome Trust Case Control Consortium 2. Commonvariants at the MHC locus and at chromosome 16q24⋅1predispose to Barrett’s esophagus. Nature Genet 2012; 44:1131–1136.
33 Wang LD, Zhou FY, Li XM, Sun LD, Song X, Jin Y et al.Genome-wide association study of esophageal squamous cellcarcinoma in Chinese subjects identifies susceptibility loci atPLCE1 and C20orf54. Nat Genet 2010; 42: 759–763.
34 Wu C, Wang Z, Song X, Feng XS, Abnet CC, He J et al.Joint analysis of three genome-wide association studies ofesophageal squamous cell carcinoma in Chinese populations.Nat Genet 2014; 46: 1001–1006.
35 He Y, Ye L, Shan B, Song G, Meng F, Wang S. Effect ofriboflavin-fortified salt nutrition intervention on esophagealsquamous cell carcinoma in a high incidence area, China.Asian Pac J Cancer Prev 2009; 10: 619–622.
36 Duan F, Xie W, Cui L, Wang P, Song C, Qu H et al. Novelfunctional variants locus in PLCE1 and susceptibility toesophageal squamous cell carcinoma: based on publishedgenome-wide association studies in a central Chinesepopulation. Cancer Epidemiol 2013; 37: 647–652.
37 Dulak AM, Stojanov P, Peng S, Lawrence MS, Fox C,Stewart C et al. Exome and whole-genome sequencing ofesophageal adenocarcinoma identifies recurrent driverevents and mutational complexity. Nat Genet 2013; 45:478–486.
38 Weaver JM, Ross-Innes CS, Shannon N, Lynch AG,Forshew T, Barbera M et al. Ordering of mutations inpreinvasive disease stages of esophageal carcinogenesis. NatGenet 2014; 46: 837–843.
39 Song Y, Li L, Ou Y, Gao Z, Li E, Li X et al. Identification ofgenomic alterations in oesophageal squamous cell cancer.Nature 2014; 509: 91–95.
40 Goh XY, Rees JR, Paterson AL, Chin SF, Marioni JC,Save V et al. Integrative analysis of array-comparativegenomic hybridisation and matched gene expression profilingdata reveals novel genes with prognostic significance inoesophageal adenocarcinoma. Gut 2011; 60: 1317–1326.
41 Peters CJ, Rees JR, Hardwick RH, Hardwick JS, Vowler SL,Ong CA et al.; Oesophageal Cancer Clinical and MolecularStratification (OCCAMS) Study Group. A 4-gene signaturepredicts survival of patients with resected adenocarcinoma ofthe esophagus, junction, and gastric cardia. Gastroenterology2010; 139: 1995–2004.e15.
42 Bian YS, Osterheld MC, Fontolliet C, Bosman FT,Benhattar J. p16 inactivation by methylation of theCDKN2A promoter occurs early during neoplasticprogression in Barrett’s esophagus. Gastroenterology 2002;122: 1113–1121.
43 Moinova H, Leidner RS, Ravi L, Lutterbaugh J,Barnholtz-Sloan JS, Chen Y et al. Aberrant vimentinmethylation is characteristic of upper gastrointestinal
© 2015 The Authors. BJS published by John Wiley & Sons Ltd www.bjs.co.uk BJS 2015; 102: e29–e40on behalf of BJS Society Ltd.

Surgery in the era of the ’omics revolution e39
pathologies. Cancer Epidemiol Biomarkers Prev 2012; 21:594–600.
44 Zou H, Molina JR, Harrington JJ, Osborn NK, Klatt KK,Romero Y et al. Aberrant methylation of secretedfrizzled-related protein genes in esophageal adenocarcinomaand Barrett’s esophagus. Int J Cancer 2005; 116: 584–591.
45 Singhal R, Carrigan JB, Wei W, Taniere P, Hejmadi RK,Forde C. MALDI profiles of proteins and lipids for the rapidcharacterisation of upper GI-tract cancers. J Proteomics 2013;80C: 207–215.
46 Hu Y, Bandla S, Godfrey TE, Tan D, Luketich JD,Pennathur A et al. HER2 amplification, overexpression andscore criteria in esophageal adenocarcinoma. Mod Pathol2011; 24: 899–907.
47 Bang YJ, Van Cutsem E, Feyereislova A, Chung HC, ShenL, Sawaki A et al. Trastuzumab in combination withchemotherapy versus chemotherapy alone for treatment ofHER2-positive advanced gastric or gastro-oesophagealjunction cancer (ToGA): a phase 3, open-label, randomisedcontrolled trial. Lancet 2010; 376: 687–697.
48 Ku GY, Ilson DH. Emerging tyrosine kinase inhibitors foresophageal cancer. Expert Opin Emerg Drugs 2013; 18:219–230.
49 Elgazzar S, Zembutsu H, Takahashi A, Kubo M, Aki F,Hirata K et al. A genome-wide association study identifies agenetic variant in the SIAH2 locus associated with hormonalreceptor-positive breast cancer in Japanese. J Hum Genet2012; 57: 766–771.
50 Fletcher O, Johnson N, Orr N, Hosking FJ, Gibson LJ,Walker K et al. Novel breast cancer susceptibility locus at9q31⋅2: results of a genome-wide association study. J NatlCancer Inst 2011; 103: 425–435.
51 Rinella ES, Shao Y, Yackowski L, Pramanik S, Oratz R,Schnabel F et al. Genetic variants associated with breastcancer risk for Ashkenazi Jewish women with strong familyhistories but no identifiable BRCA1/2 mutation. Hum Genet2013; 132: 523–536.
52 Beggs AD, Hodgson SV. Genomics and breast cancer: thedifferent levels of inherited susceptibility. Eur J Hum Genet2009; 17: 855–856.
53 Pharoah PD, Antoniou AC, Easton DF, Ponder BA.Polygenes, risk prediction, and targeted prevention of breastcancer. N Engl J Med 2008; 358: 2796–2803.
54 Dutt A, Salvesen HB, Chen TH, Ramos AH, Onofrio RC,Hatton C et al. Drug-sensitive FGFR2 mutations inendometrial carcinoma. Proc Natl Acad Sci U S A 2008; 105:8713–8717.
55 Garcia-Closas M, Couch FJ, Lindstrom S, Michailidou K,Schmidt MK, Brook MN et al. Genome-wide associationstudies identify four ER negative-specific breast cancer riskloci. Nat Genet 2013; 45: 392–398, 398.e1–e2.
56 Ghoussaini M, Fletcher O, Michailidou K, Turnbull C,Schmidt MK, Dicks E et al. Genome-wide associationanalysis identifies three new breast cancer susceptibility loci.Nat Genet 2012; 44: 312–318.
57 Cancer Genome Atlas Network. Comprehensive molecularportraits of human breast tumours. Nature 2012; 490:61–70.
58 Shah SP, Roth A, Goya R, Oloumi A, Ha G, Zhao Y et al.The clonal and mutational evolution spectrum of primarytriple-negative breast cancers. Nature 2012; 486: 395–399.
59 Banerji S, Cibulskis K, Rangel-Escareno C, Brown KK,Carter SL, Frederick AM et al. Sequence analysis ofmutations and translocations across breast cancer subtypes.Nature 2012; 486: 405–409.
60 Stephens PJ, Tarpey PS, Davies H, Van Loo P, Greenman C,Wedge DC et al. The landscape of cancer genes andmutational processes in breast cancer. Nature 2012; 486:400–404.
61 Dawson SJ, Tsui DW, Murtaza M, Biggs H, Rueda OM,Chin SF et al. Analysis of circulating tumor DNA to monitormetastatic breast cancer. N Engl J Med 2013; 368:1199–1209.
62 Pegolo E, Puppin C, Gerometta A, Damante G, Puglisi F,Di Loreto C. One-step nucleic acid amplification (OSNA)for intraoperative evaluation of sentinel lymph node status inbreast cancer: a comparative study between CK19 proteinexpression and CK19 mRNA level in primary tumorsand lymph node metastasis. Virchows Arch 2013; 463:7–15.
63 Klingler S, Marchal F, Rauch P, Kenouchi O, Chretien AS,Genin P et al. Using one-step nucleic acid amplification(OSNA) for intraoperative detection of lymph nodemetastasis in breast cancer patients avoids second surgeryand accelerates initiation of adjuvant therapy. Ann Oncol2013; 24: 2305–2309.
64 Mulligan JM, Hill LA, Deharo S, Irwin G, Boyle D, KeatingKE et al. Identification and validation of ananthracycline/cyclophosphamide-based chemotherapyresponse assay in breast cancer. J Natl Cancer Inst 2014; 106:djt335.
65 Ma CX, Suman VJ, Goetz M, Haluska P, Moynihan T,Nanda R et al. A phase I trial of the IGF-1R antibodycixutumumab in combination with temsirolimus in patientswith metastatic breast cancer. Breast Cancer Res Treat 2013;139: 145–153.
66 Farmer H, McCabe N, Lord CJ, Tutt AN, Johnson DA,Richardson TB et al. Targeting the DNA repair defect inBRCA mutant cells as a therapeutic strategy. Nature 2005;434: 917–921.
67 Tutt A, Robson M, Garber JE, Domchek SM, Audeh MW,Weitzel JN et al. Oral poly(ADP-ribose) polymeraseinhibitor olaparib in patients with BRCA1 or BRCA2mutations and advanced breast cancer: a proof-of-concepttrial. Lancet 2010; 376: 235–244.
68 Gelmon KA, Tischkowitz M, Mackay H, Swenerton K,Robidoux A, Tonkin K et al. Olaparib in patients withrecurrent high-grade serous or poorly differentiated ovariancarcinoma or triple-negative breast cancer: a phase 2,multicentre, open-label, non-randomised study. Lancet Oncol2011; 12: 852–861.
© 2015 The Authors. BJS published by John Wiley & Sons Ltd www.bjs.co.uk BJS 2015; 102: e29–e40on behalf of BJS Society Ltd.

e40 A. D. Beggs and M. P. Dilworth
69 Greenup R, Buchanan A, Lorizio W, Rhoads K, Chan S,Leedom T et al. Prevalence of BRCA mutations amongwomen with triple-negative breast cancer (TNBC) in agenetic counseling cohort. Ann Surg Oncol 2013; 20:3254–3258.
70 Piccart M, Hortobagyi GN, Campone M, Pritchard KI,Lebrun F, Ito Y et al. Everolimus plus exemestane forhormone-receptor-positive, human epidermal growth factorreceptor-2-negative advanced breast cancer: overall survivalresults from BOLERO-2. Ann Oncol 2014; [Epub ahead ofprint].
71 Habr-Gama A, Perez R, Proscurshim I, Gama-Rodrigues J.Complete clinical response after neoadjuvant chemoradiation
for distal rectal cancer. Surg Oncol Clin N Am 2010; 19:829–845.
72 Genomics England. The 100 000 Genomes Project. http://www.genomicsengland.co.uk/the-100000-genomes-project/[accessed 1 October 2014].
73 Gerlinger M, Rowan AJ, Horswell S, Larkin J, EndesfelderD, Gronroos E et al. Intratumor heterogeneity and branchedevolution revealed by multiregion sequencing. N Engl J Med2012; 366: 883–892.
74 Beggs AD, Domingo E, Abulafi M, Hodgson SV,Tomlinson IP. A study of genomic instability in earlypreneoplastic colonic lesions. Oncogene 2013; 32:5333–5337.
http://olabout.wiley.com/WileyCDA/Section/id-822263.html
© 2015 The Authors. BJS published by John Wiley & Sons Ltd www.bjs.co.uk BJS 2015; 102: e29–e40on behalf of BJS Society Ltd.