Embed Size (px)
Citation preview
Surgery for cervical spine disease
Patrick Statham,
Consultant Neurosurgeon,
Western General Hospital, Edinburgh
Format
• Anatomy and load bearing• Spectrum of Pathology• Clinical examination and assessment• Differential diagnosis• Special tests• Approaches • Instrumentation and prosthesies• Specific pathology• The future
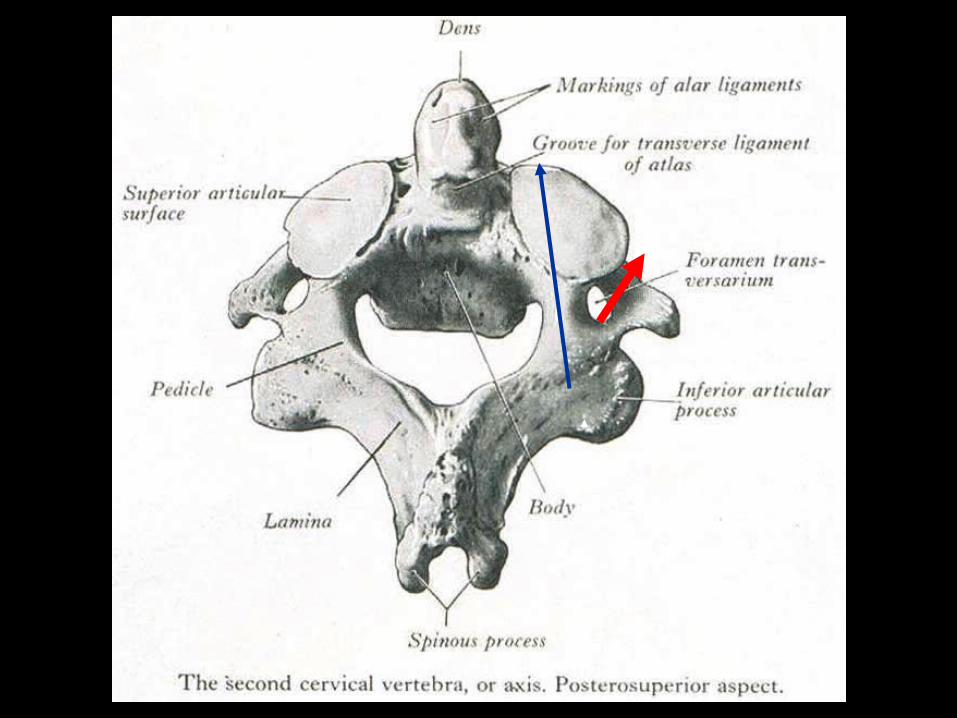
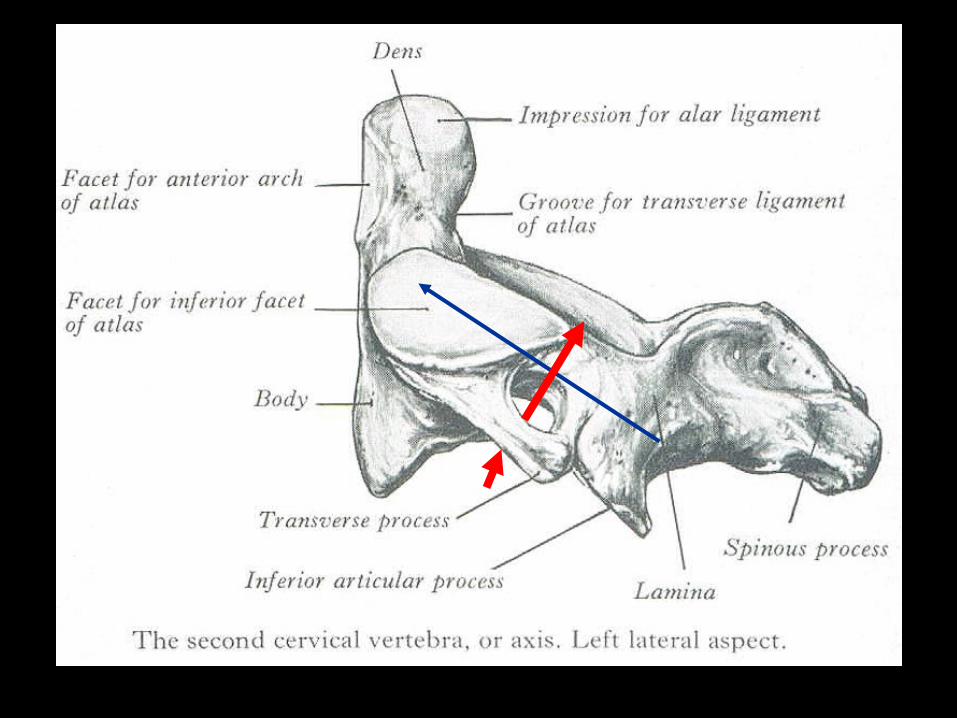
Functional units: anatomy and pathology
• Occiput C1 and C2
• C3 to C7
• Cervicothoracic junction
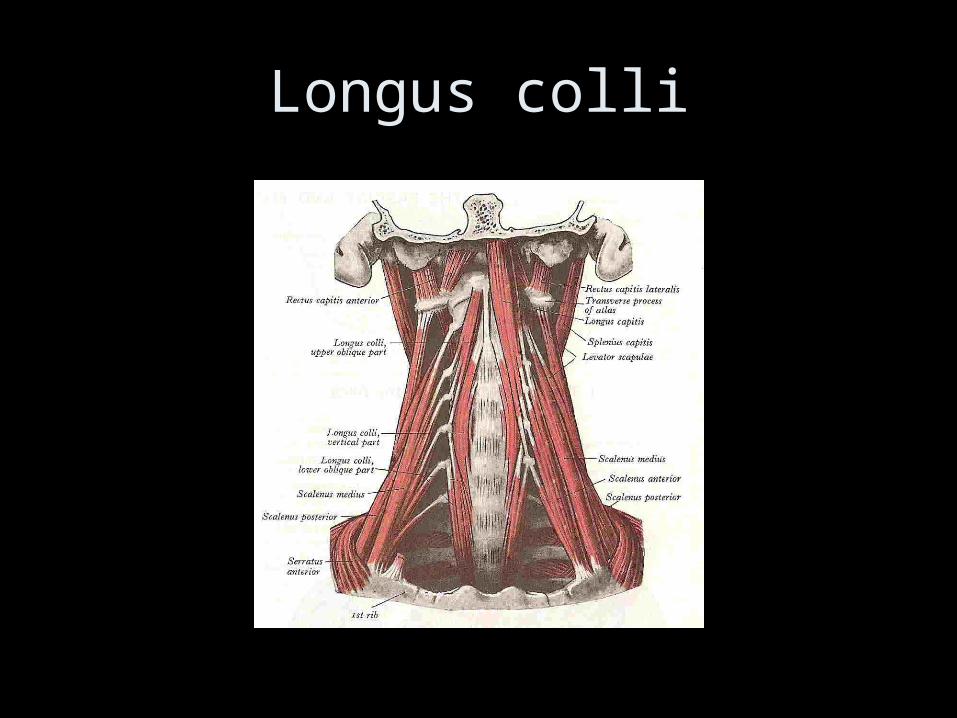
Longus colli
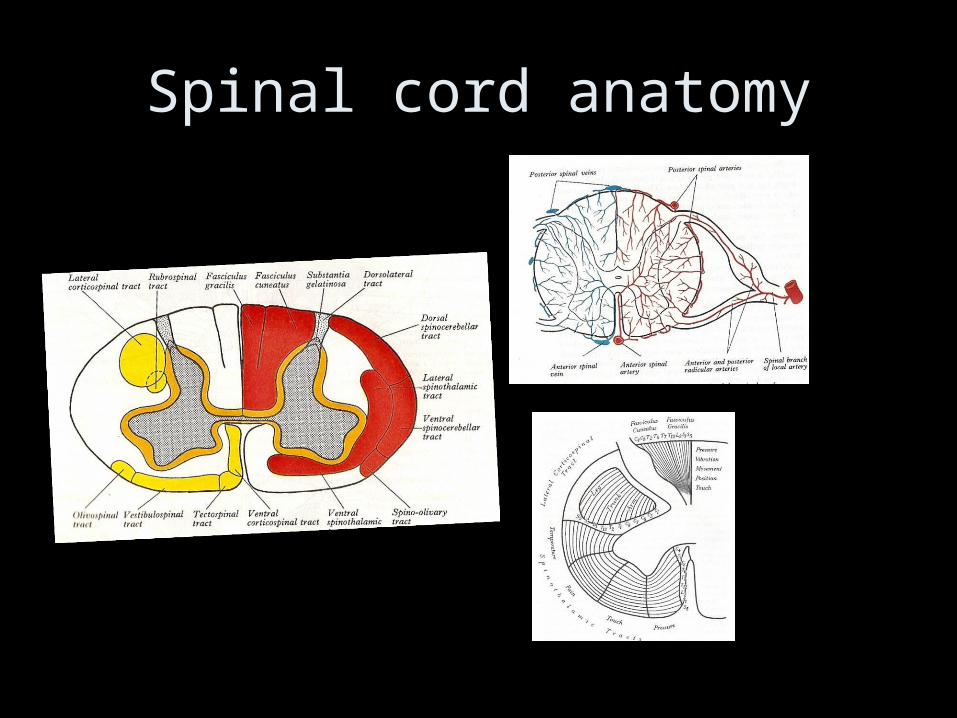
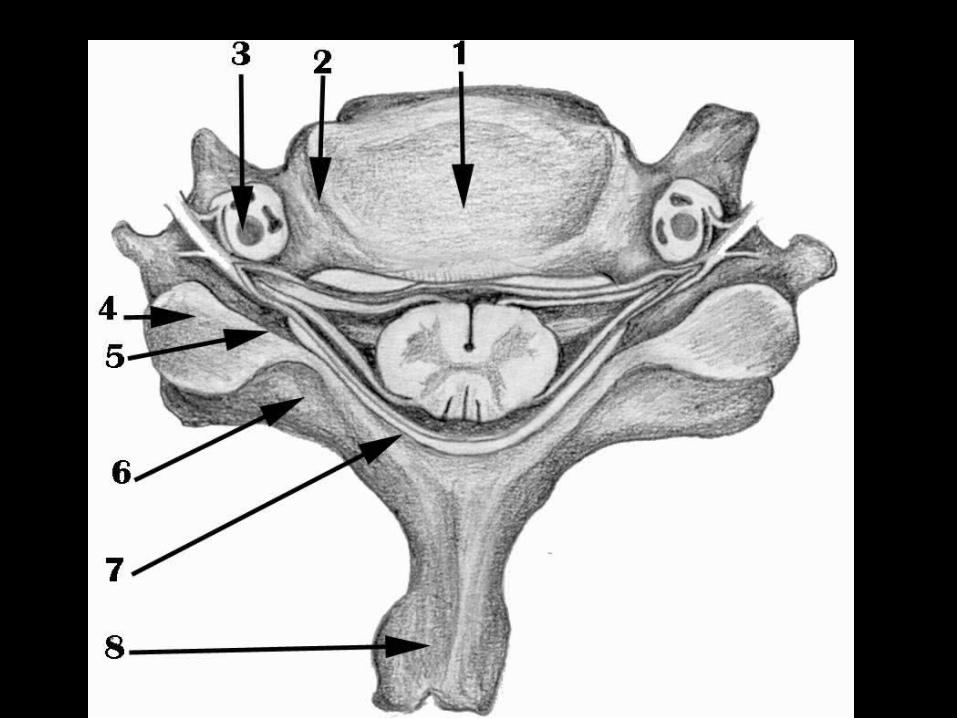
Spinal cord anatomy
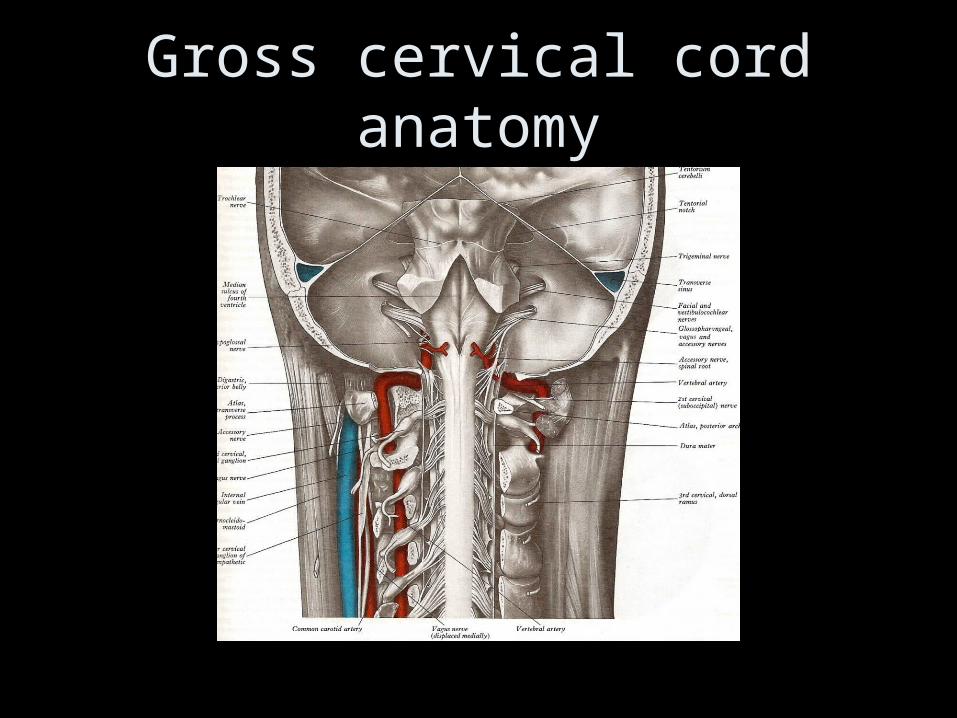
Gross cervical cord anatomy
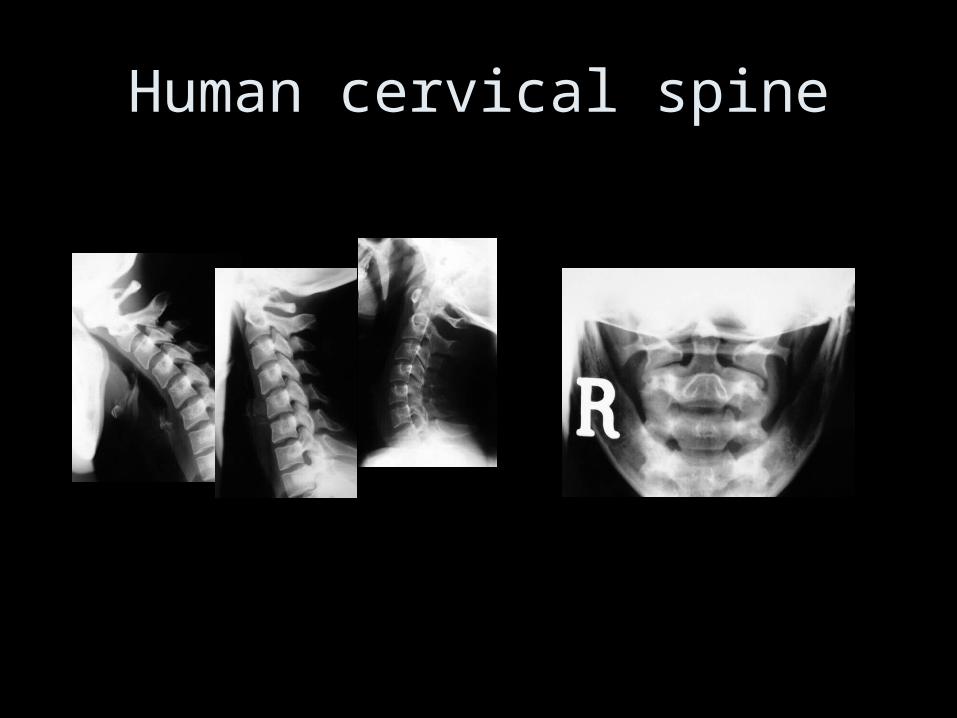
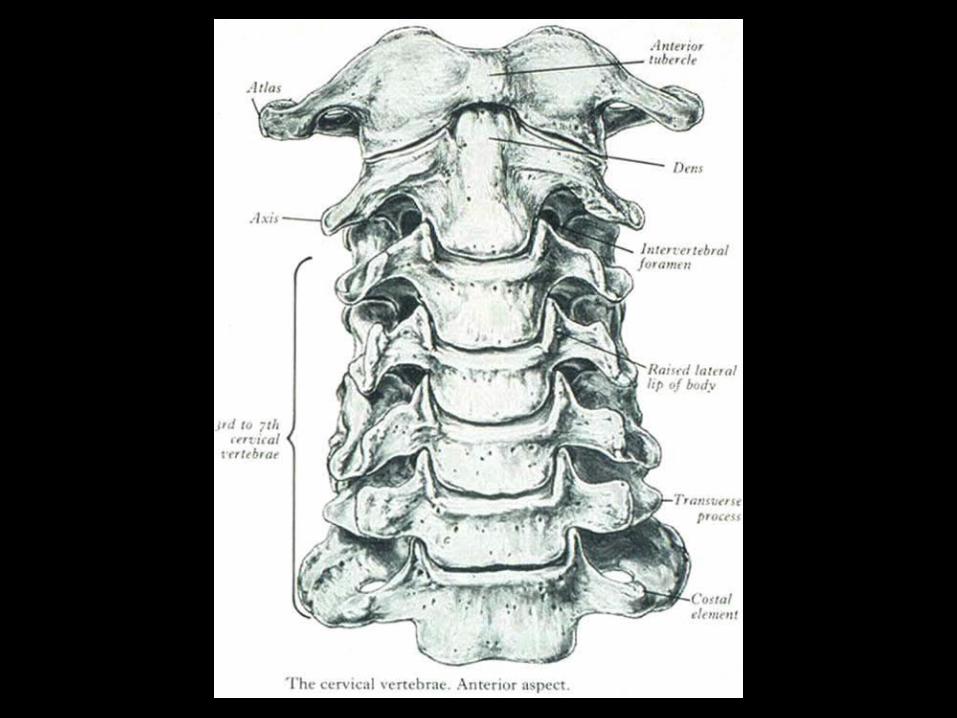
Human cervical spine
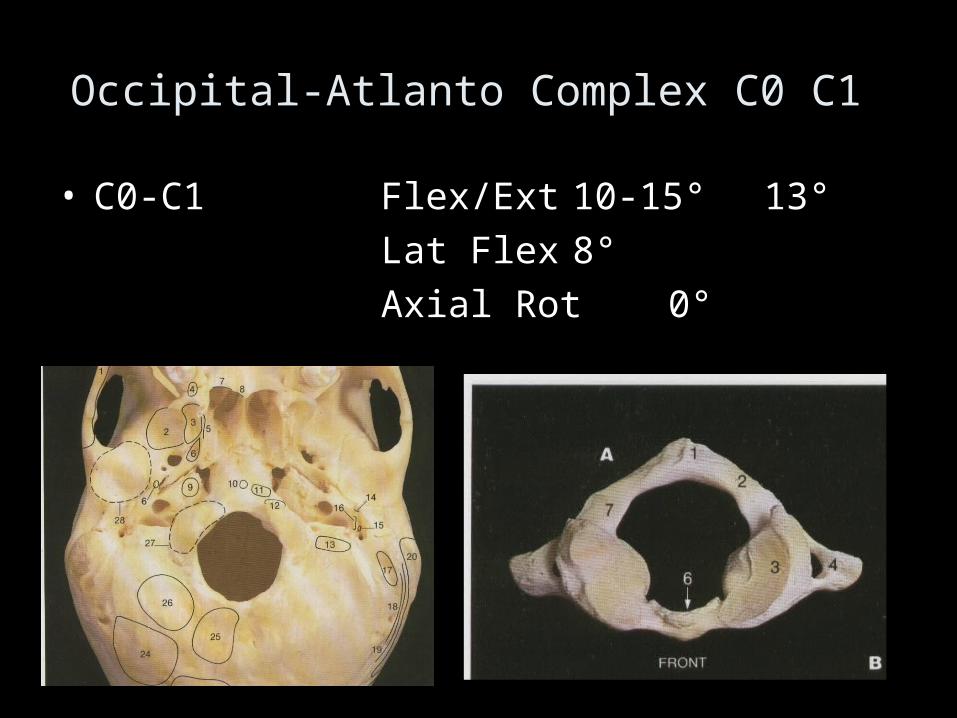
Occipital-Atlanto Complex C0 C1
• C0-C1 Flex/Ext 10-15° 13°
Lat Flex 8°
Axial Rot 0°
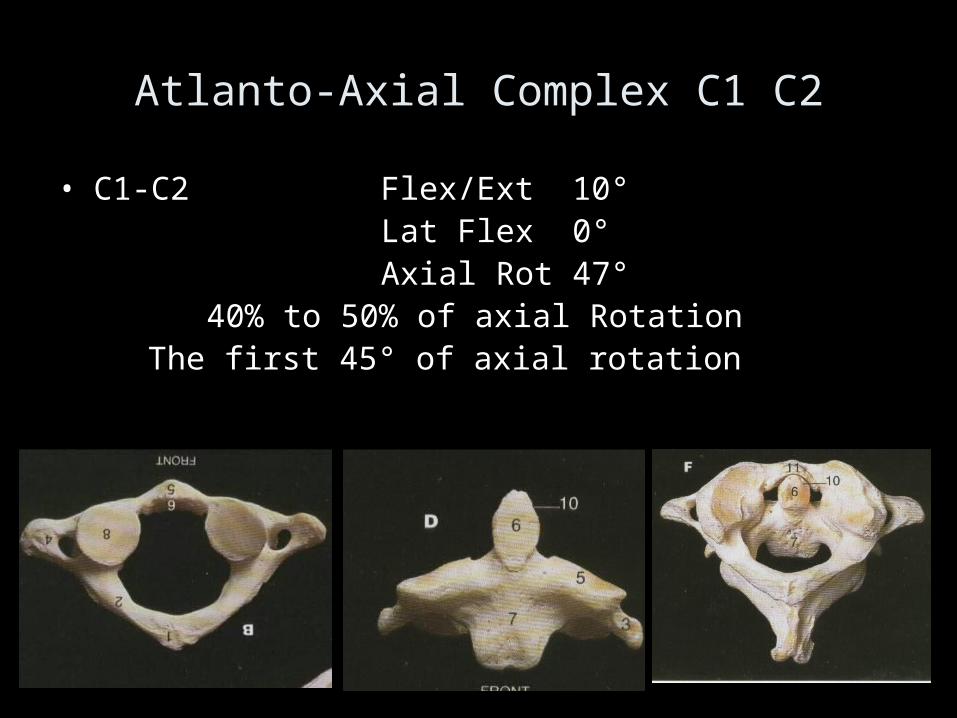
Atlanto-Axial Complex C1 C2
• C1-C2 Flex/Ext 10°Lat Flex 0°Axial Rot 47°
40% to 50% of axial RotationThe first 45° of axial rotation
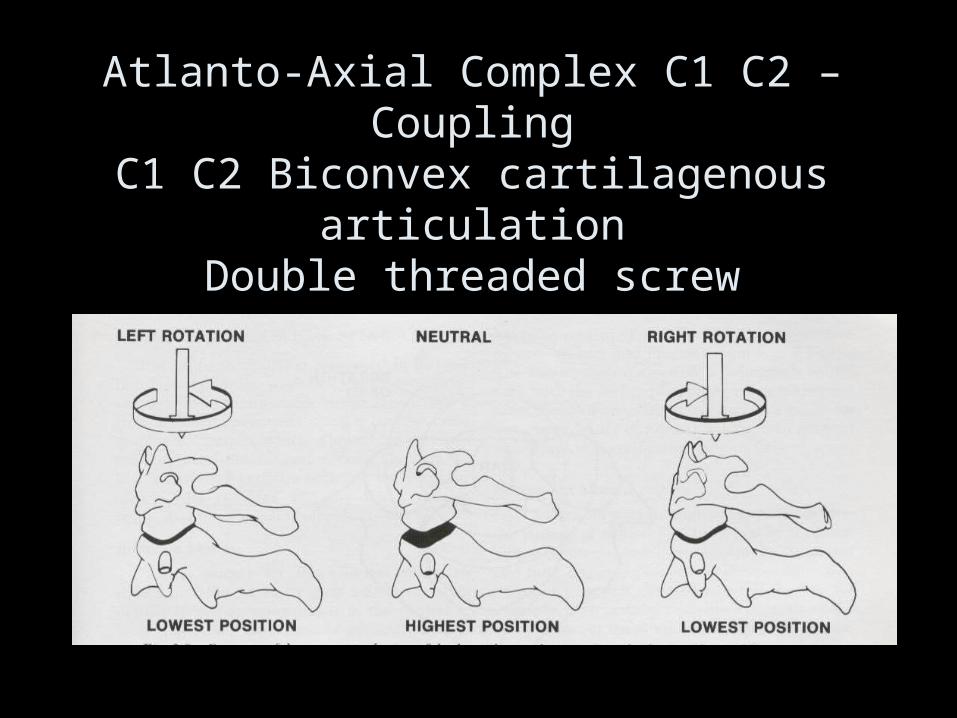
Atlanto-Axial Complex C1 C2 – CouplingC1 C2 Biconvex cartilagenous articulation
Double threaded screw
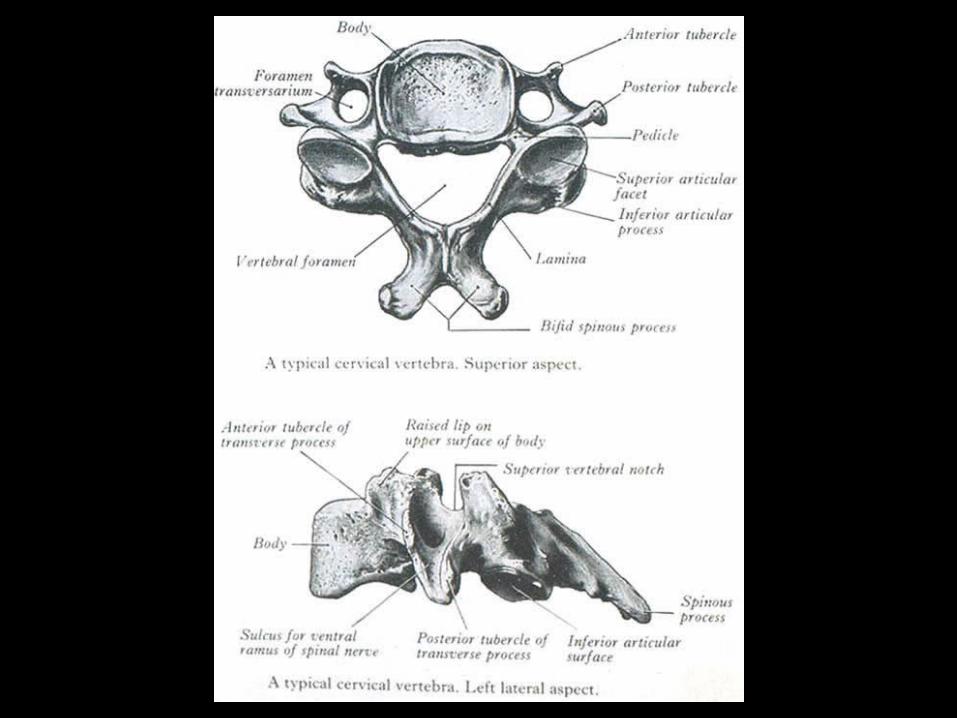
Cervical Spine Kinematics & Anatomy
• Flexion/Extension 145°
• Axial rotation 180°
• Lateral flexion 90°
• Atypical C1 C2 C7
• Typical C3-C6
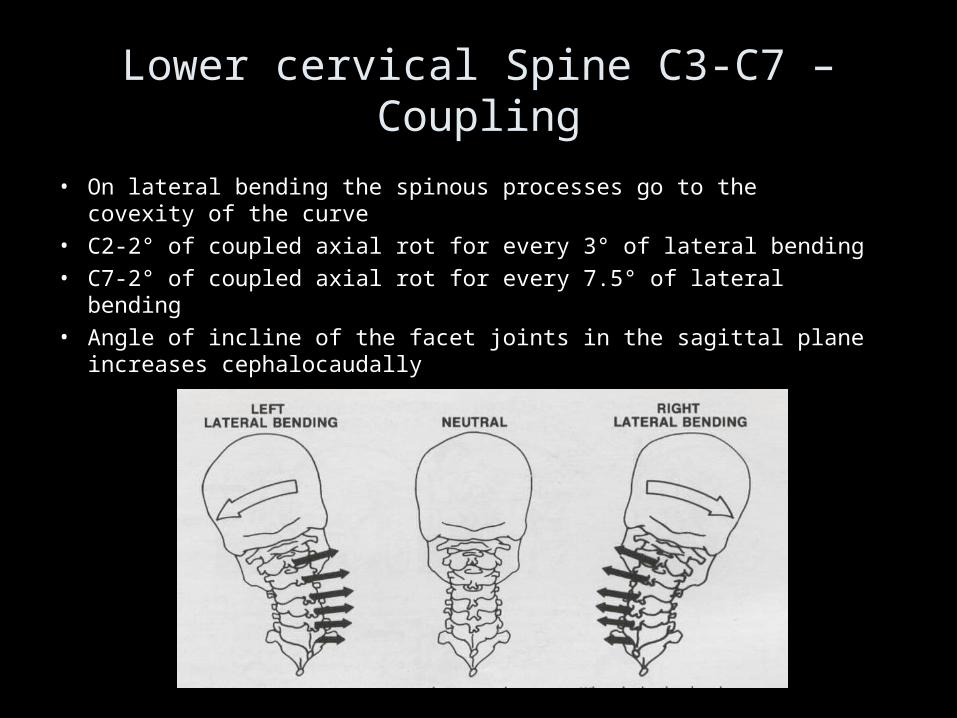
Lower cervical Spine C3-C7 – Coupling
• On lateral bending the spinous processes go to the covexity of the curve
• C2-2° of coupled axial rot for every 3° of lateral bending• C7-2° of coupled axial rot for every 7.5° of lateral bending• Angle of incline of the facet joints in the sagittal plane increases
cephalocaudally
Cervical Spine instability
• Misjudgement – Death or major neurological deficit – Un-necessary surgery with risk of surgical complications
• Definition
“Clinical stability is defined as the ability of the spine to limit its patterns of displacement under physiologic loads so as not to damage the spinal cord or nerve roots.”
White and Panjabi Clin Orthopaedics 1975
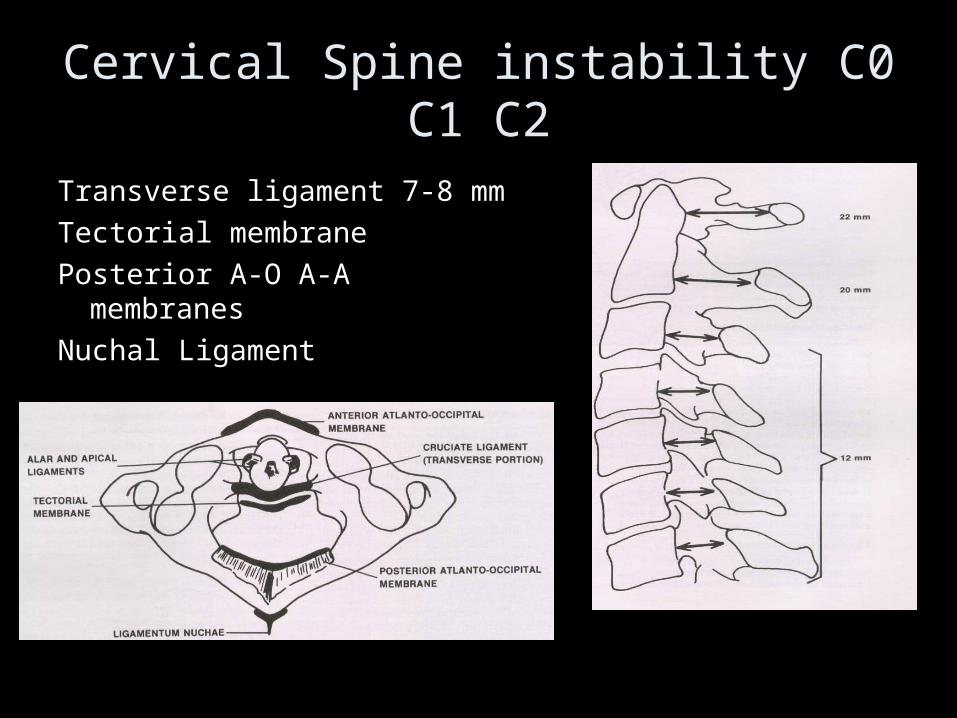
Cervical Spine instability C0 C1 C2
Transverse ligament 7-8 mm
Tectorial membrane
Posterior A-O A-A membranes
Nuchal Ligament
Wolf et al. J Mt Sinai Hosp. NY. 23:283,1956
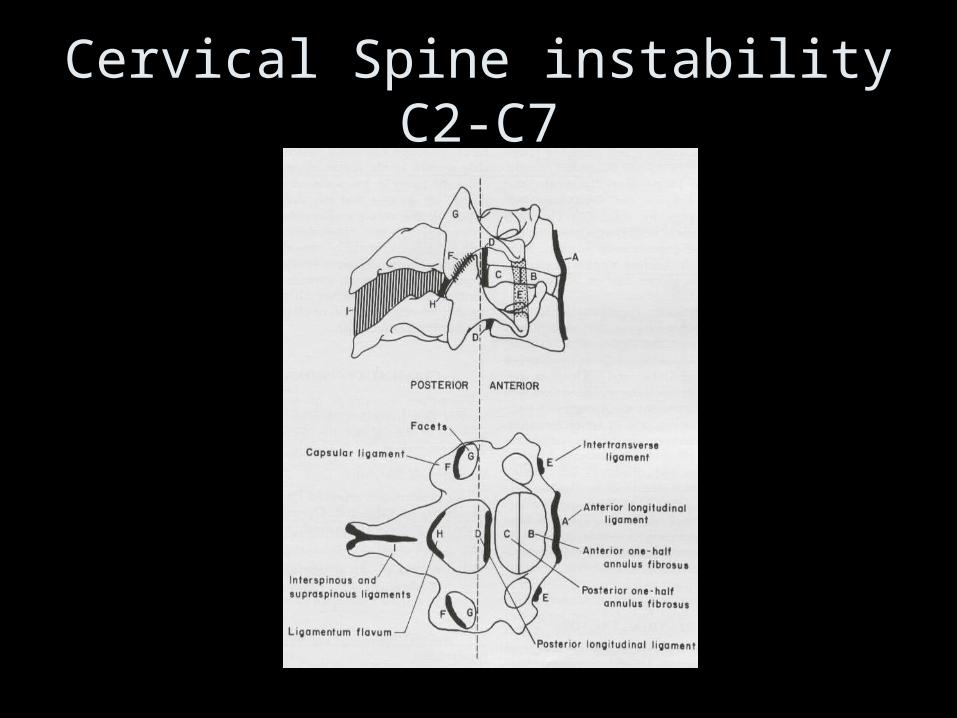
Cervical Spine instability C2-C7
•Flex-Ext All ant structures + 1 post All post structures + ant
Laminectomy
In children - Kyphosis
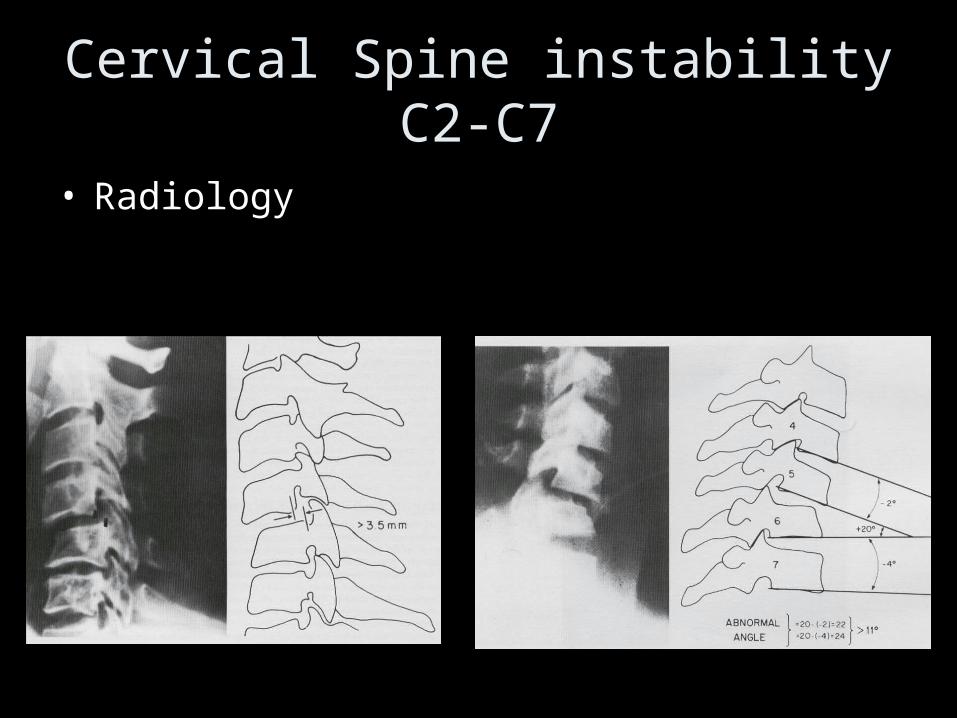
Cervical Spine instability C2-C7
• Radiology
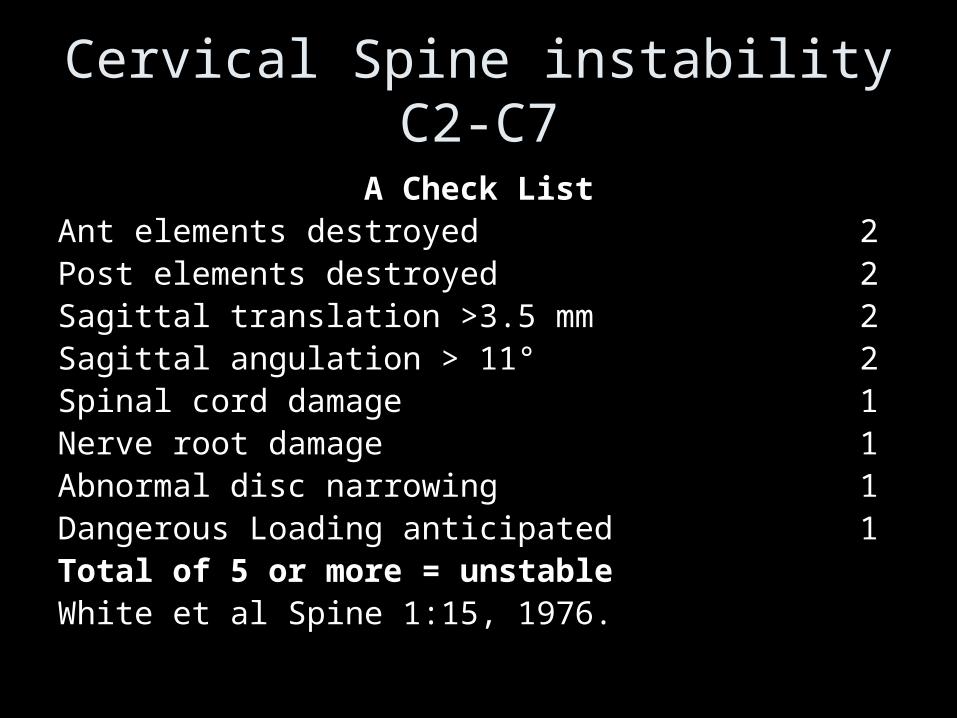
Cervical Spine instability C2-C7
A Check ListAnt elements destroyed 2Post elements destroyed 2Sagittal translation >3.5 mm 2Sagittal angulation > 11° 2Spinal cord damage 1Nerve root damage 1Abnormal disc narrowing 1Dangerous Loading anticipated 1Total of 5 or more = unstableWhite et al Spine 1:15, 1976.
Spectrum of pathology
• Prolapsed discs, osteophytic compression: ‘wear and repair’
• Inflammatory: rheumatoid, ankylosing spondylitis• Trauma: odontoid, rotatory subluxation• Neoplastic: meningiomas, schwannomas,
metastatic cord compression,intrinsic cord• Congenital Klippel Feil, fused, Down’s,
enterogenous cysts• Infection: discitis, osteomyelitis, epidural
abscess
Clinical examination
• Posture • Tone • Power• Sensation• Deep tendon reflexes• Co ordination• Gait
• Clothing zips, velcro• Aids: stick, wheelchair• Deformity OA,RhA,
AS, klippel feil, Downs
• Other disease; cancer
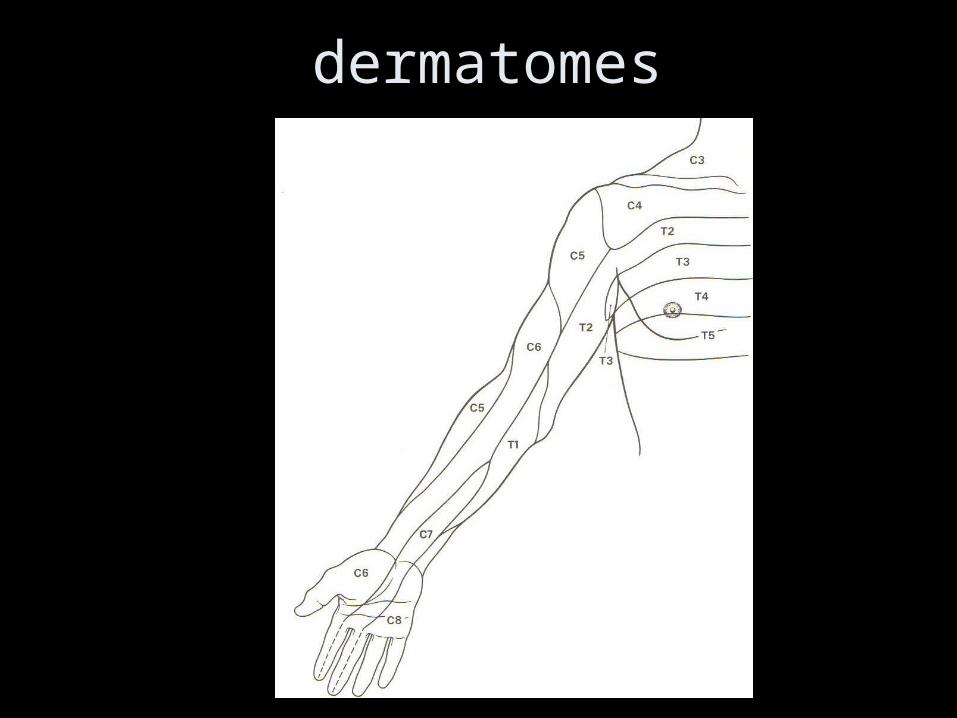
dermatomes
Diagnosis
• MRI• CT or CT myelogram• Nerve conduction
studies• Blood• CSF
• Multiple sclerosis• Mononeuritis
multiplex• Peripheral n
entrapment (median, ulnar)
• SACDC• Brachial amyotrophy
Clinical assessment
• Natural history of condition
• Risks and benefits of the intervention
• Alternatives; collar halo physiotherapy
• Appropriateness for this particular patient
Surgical approaches
• C1/2 anterior: trans oral
• C1/2 posterior: midline sub-occipital
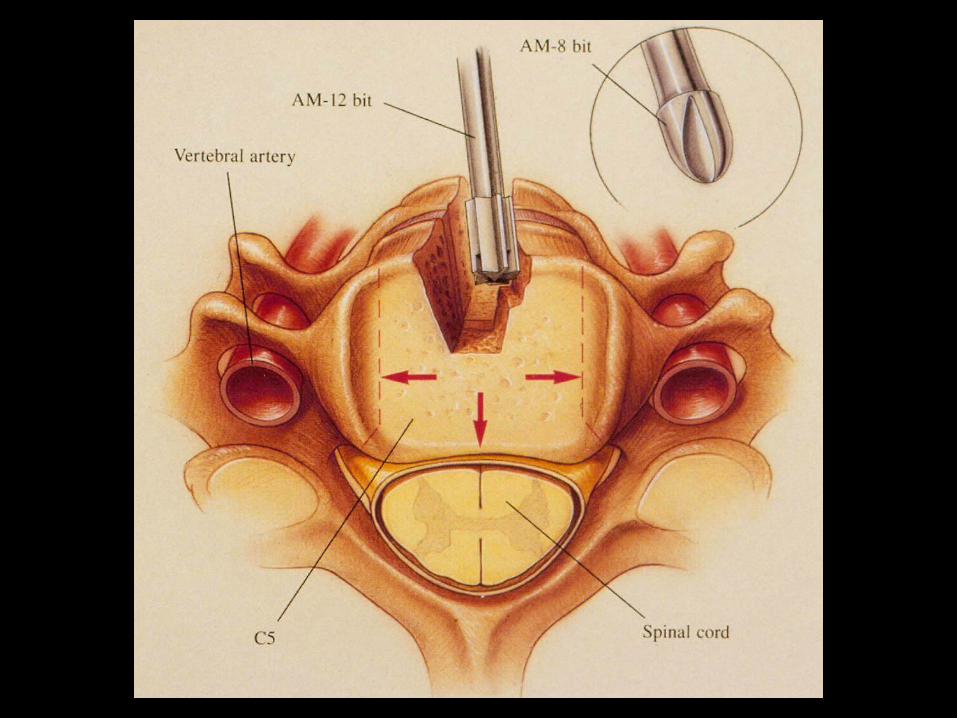
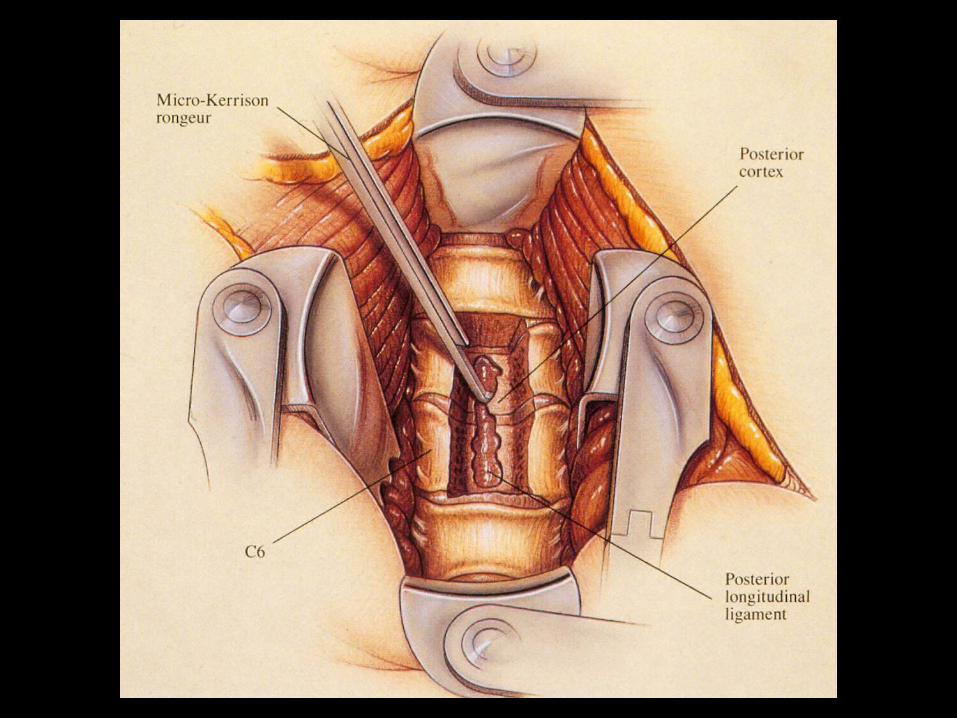
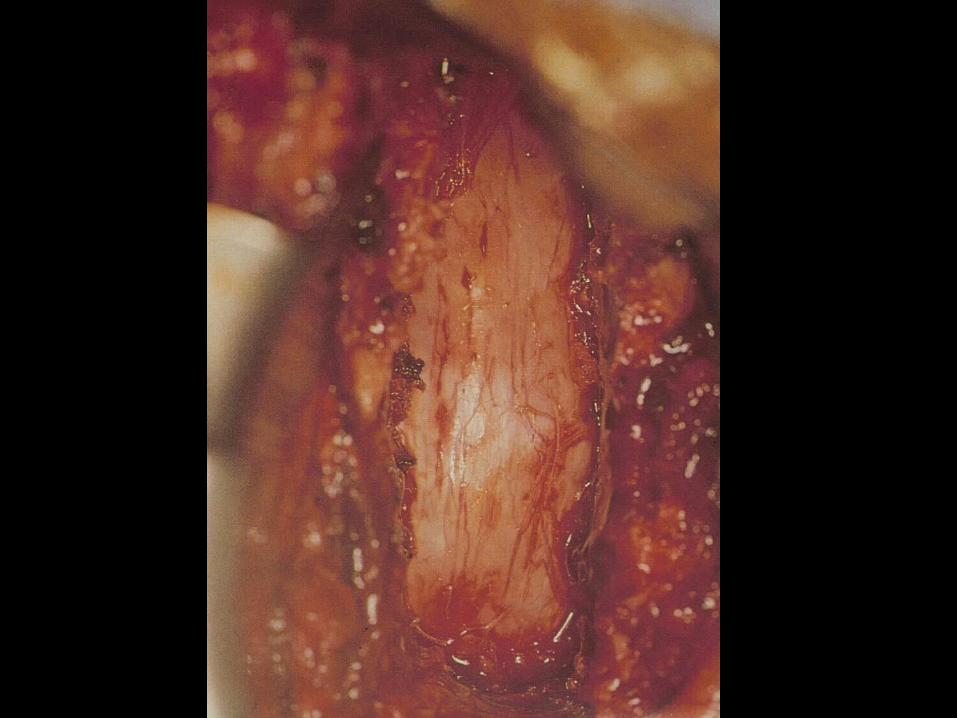
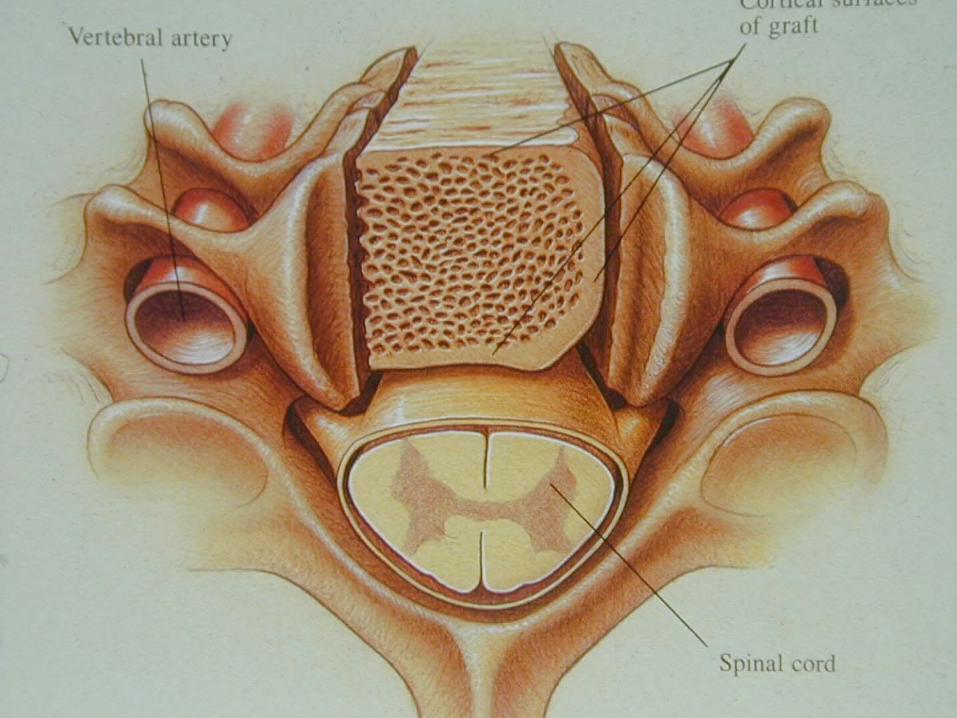
• Sub-axial anterior: anterior cervical decompression
• Sub-axial posterior: cervical laminectomy, laminoplasty, foramenotomy
Results: NASCIS 2
6 weeks: ‘no statistical difference between groups’
6 months: MPSS improved PP (p=0.012), Touch (p=0.042)
1 year:(95%) ‘no significant differences in neurological function by treatment group’
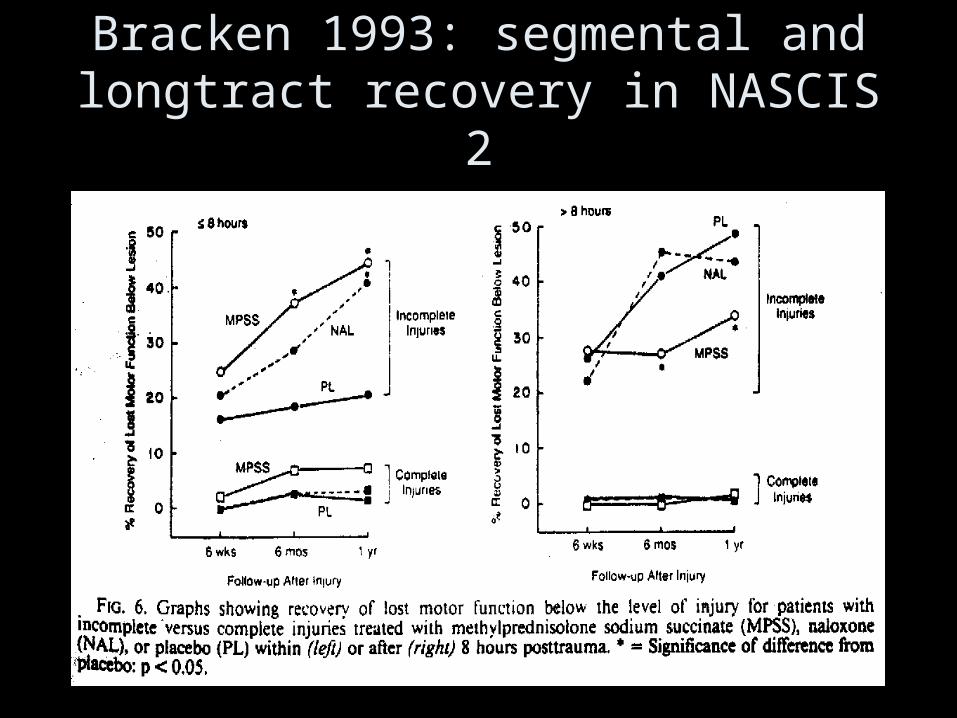
Bracken 1993: segmental and longtract recovery in NASCIS 2
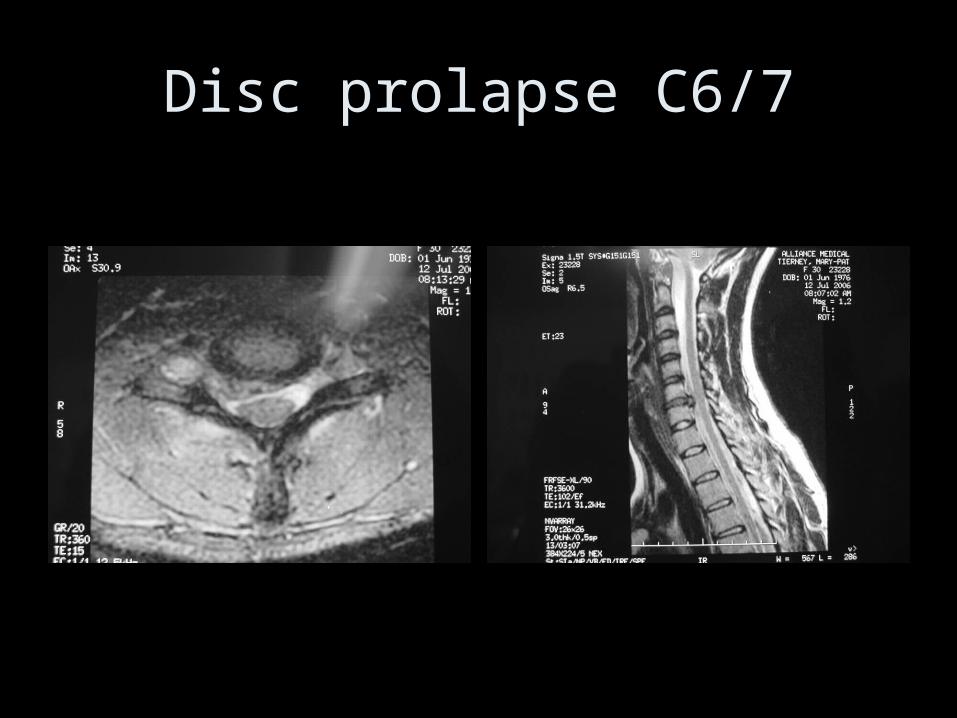
Disc prolapse C6/7
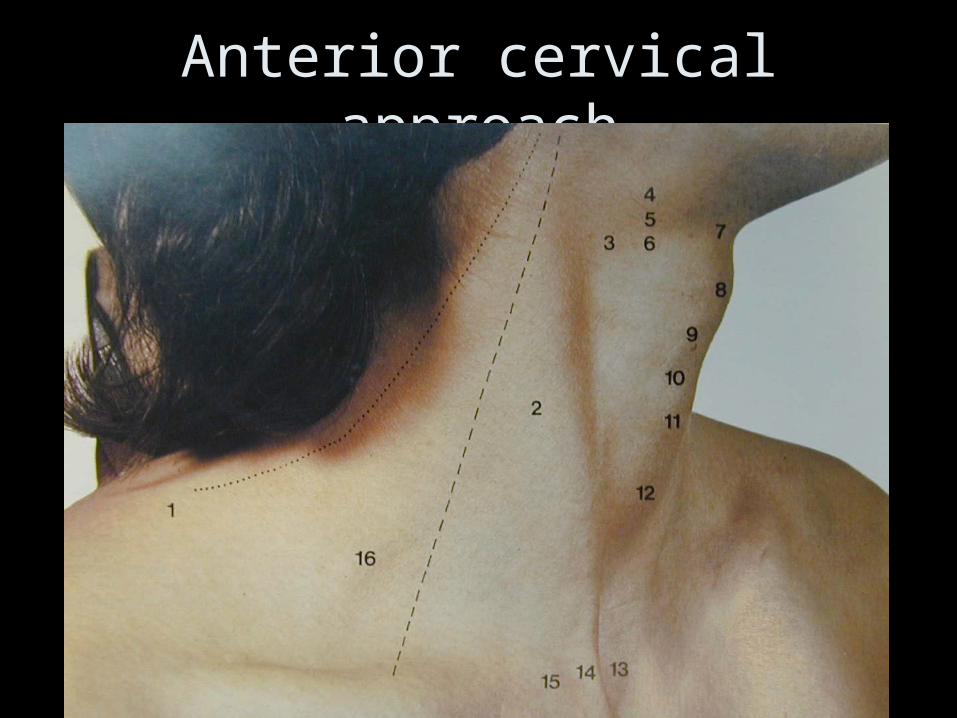
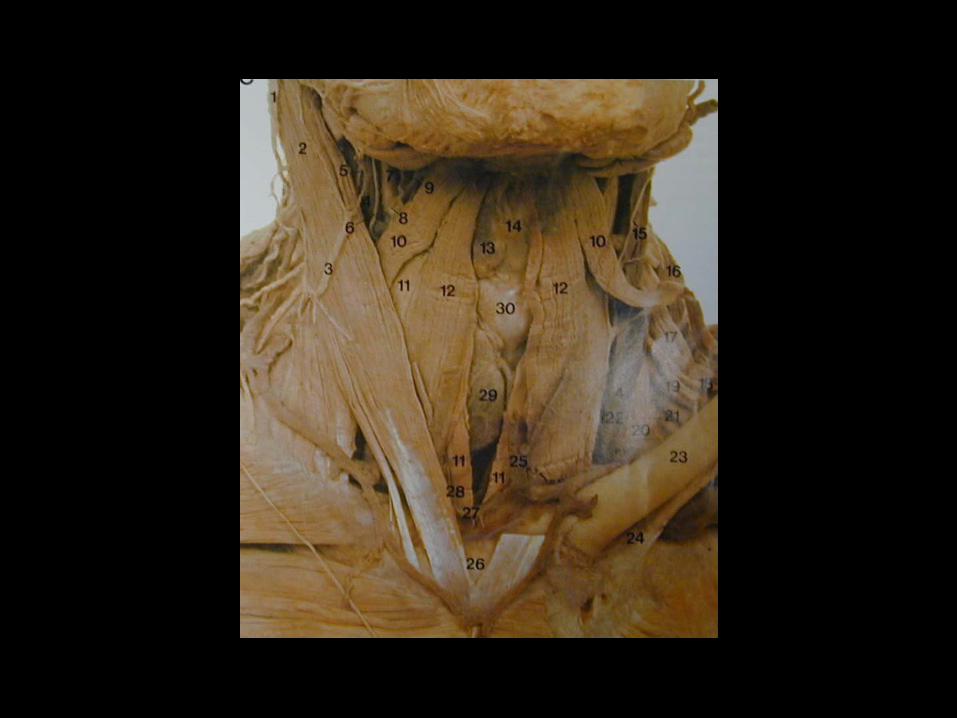
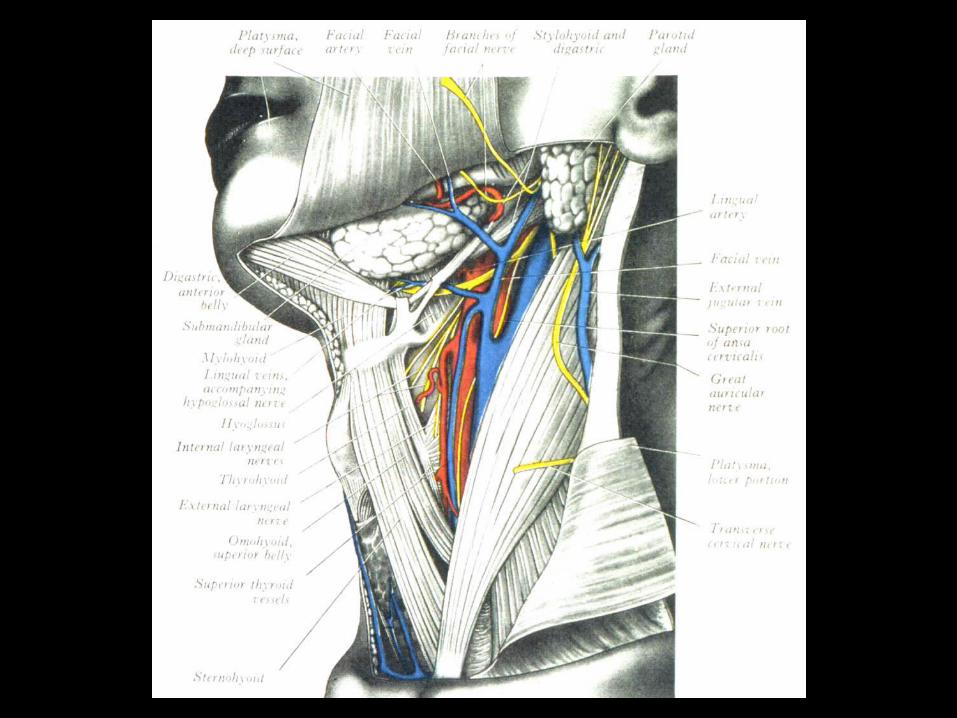
Anterior cervical approach
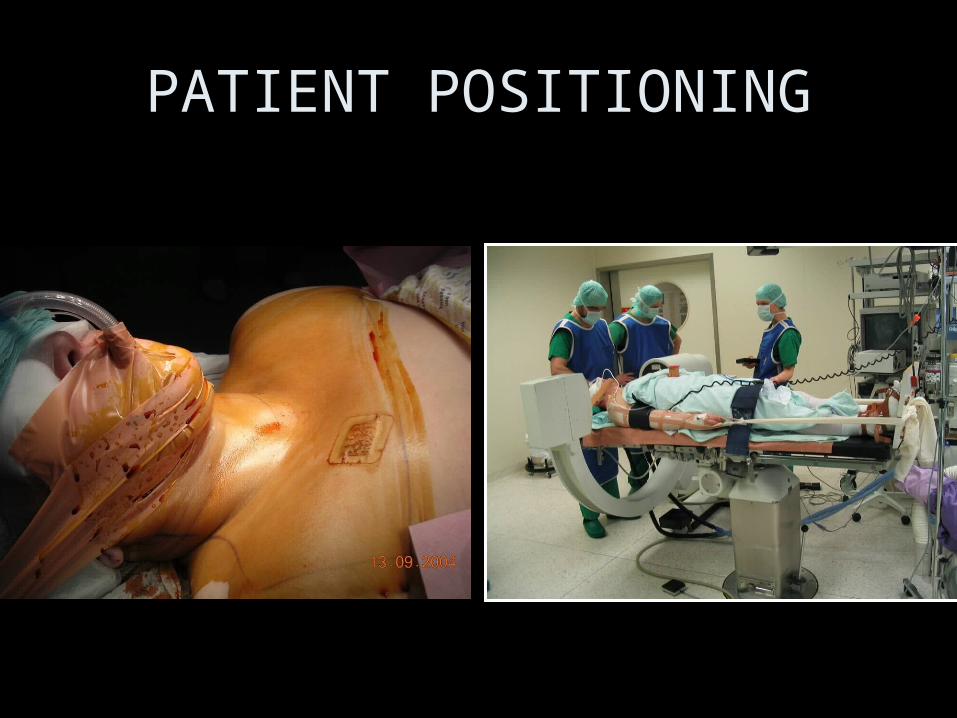
PATIENT POSITIONING
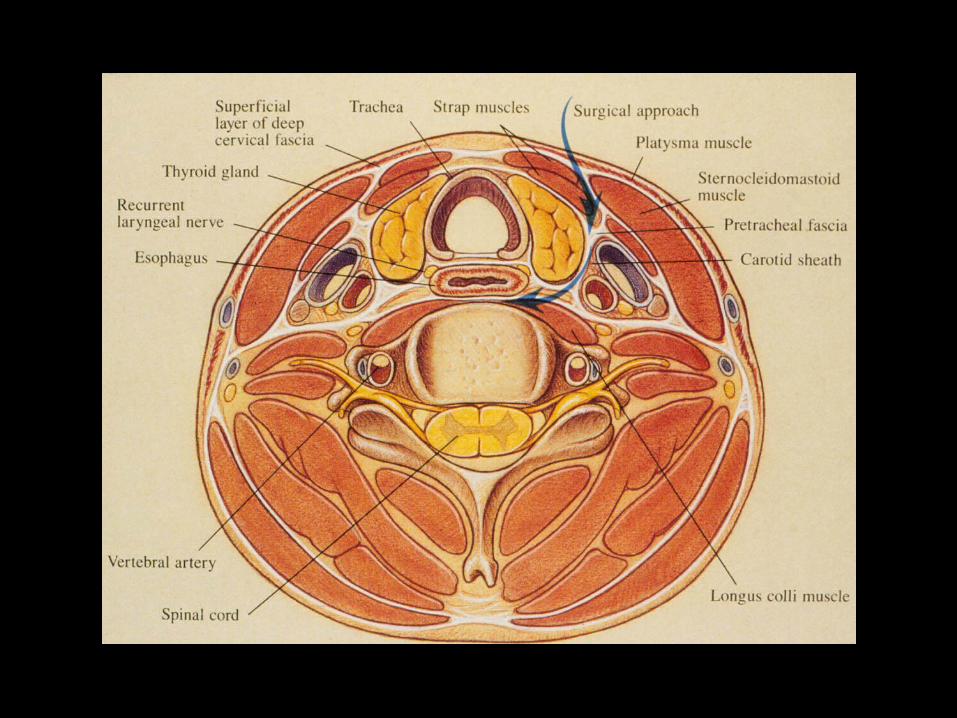
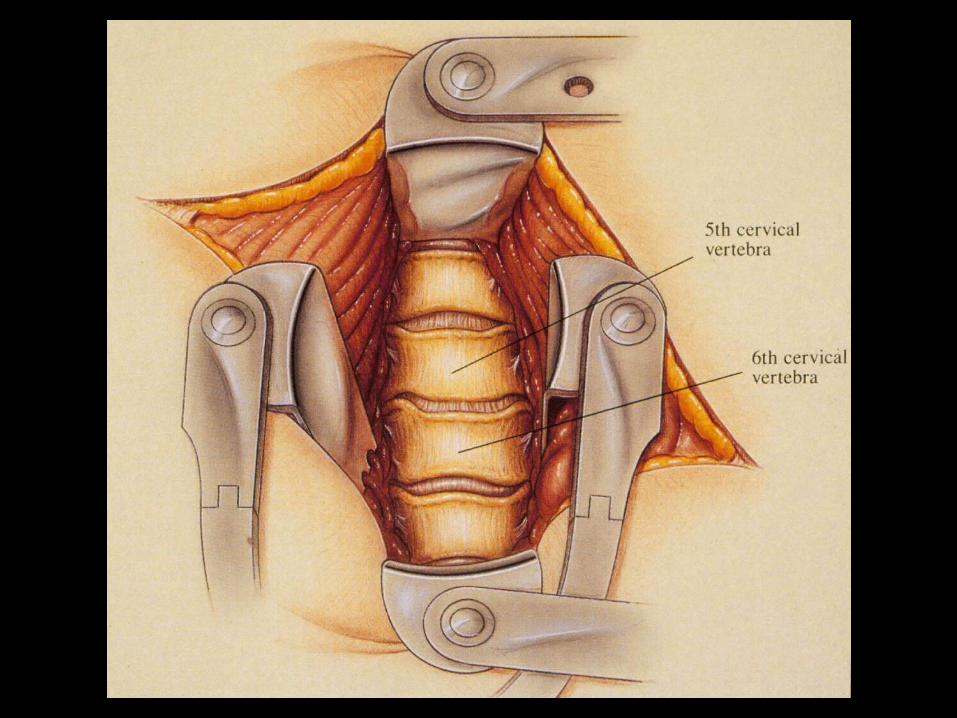
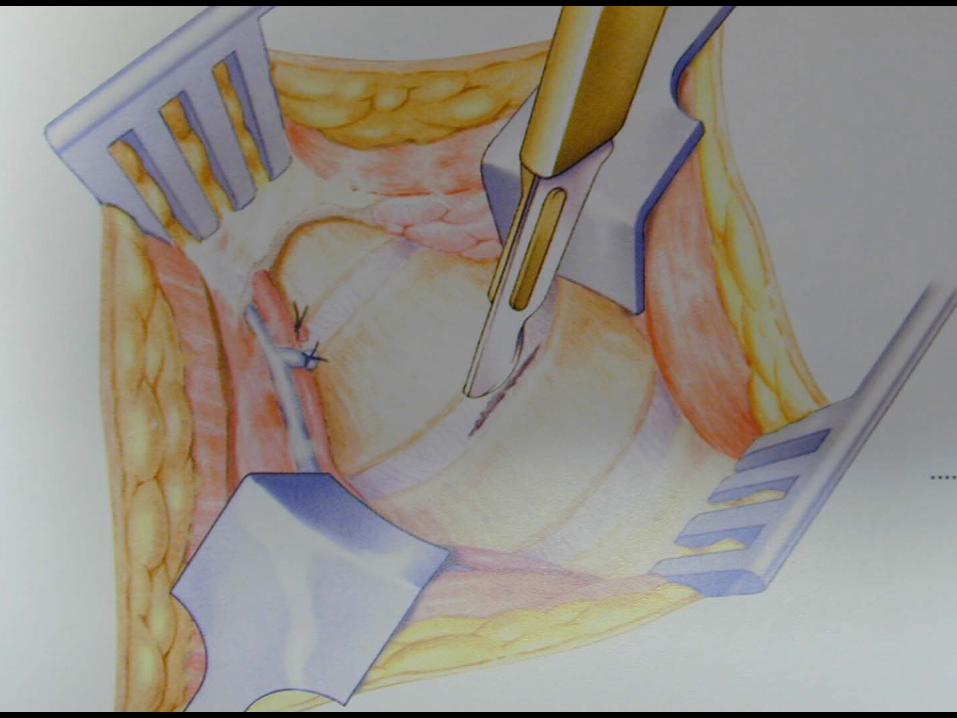
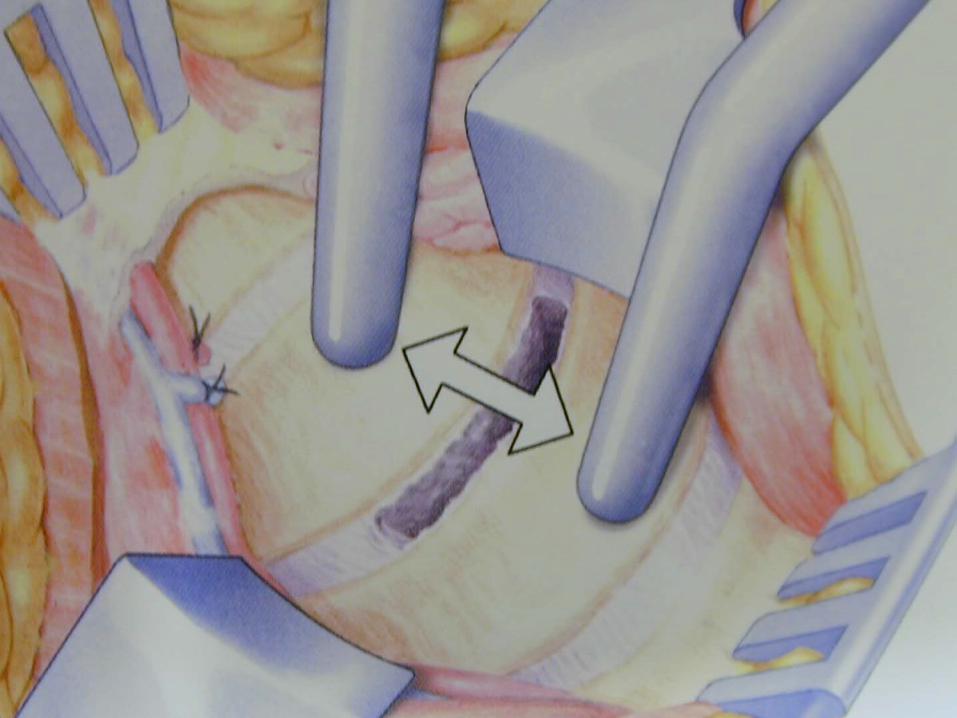

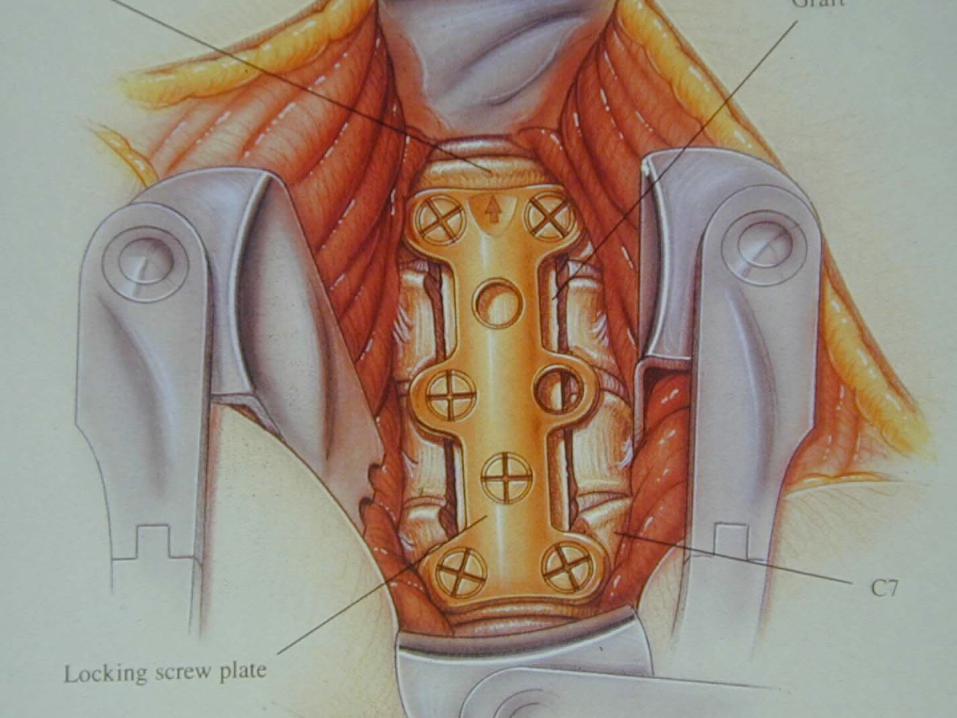
Plate removal, disc decompression, solis cage and graft

Total discectomy, iliac graft, Anterior locking plate