Embed Size (px)
Citation preview
Project CARE
Surgery and Diet for Epilepsy
Elia M Pestana Knight, MD
Topic today
• Surgery treatment for epilepsy
• Diet treatment for epilepsy
SURGERY FOR EPILEPSY
What is Refractory or Intractable
Epilepsy?
Definition of Refractory Epilepsy:
- Lack of acceptable seizure control
despite of
- adequate trials of appropriate drugs
- at doses or levels appropriate to
produce seizure control
- with minimal side effects
Impact of Intractable Epilepsy
• Quality of life (psychological, social,
occupational)
• SUDEP (sudden unexpected death in
epilepsy)
• Interictal Dysfunction
- (learning, memory, attention, etc.)
• Progressive neurological dysfunction
- Epileptic encephalopathy
• Neuropsychiatric comorbidities
Epilepsy Surgery
• Epilepsy surgery is a highly effective and safe alternative for selected patients with intractable focal epilepsy.
• Epilepsy surgeries have been performed for more than five decades.
• Estimate of the number of appropriate candidates far exceeds the actual referrals to epilepsy centers.
Goal of epilepsy surgery
• 1. Seizure freedom
• 2. Improved quality of life for patients
and family
Presurgical Evaluation
• Tests and evaluations that need to be done before the patient have epilepsy surgery
• Why do a presurgical evaluation?
- Select the cases for surgery
- Determine the impact of the surgical brain resection on the cognitive, emotional state, and social situation of the patient
What are some of the test done
during the presurgical evaluation?
Most important tests
• EEG and video-EEG
• Brain MRI
Additional tests
• PET scan
• Ictal SPECT
• Neuropsychological Testing
• Tests to localize spikes and some specific functions: memory, motor and language
- MEG
- fMRI
- WADA Test
What is an EEG?
• A diagnostic study
• Records spontaneous electrical activity fired by the neurons in the brain
• From electrodes places in the skull or the cranial cavity
- Surface electrodes
- Intracranial electrodes
• Subdural electrodes
• Depth electrodes
Who recorded the first human
EEG?
• Hans Burger (1873–
1941)
• German psychiatrist
• Recorded the first
human EEG in 1924
• Discovered the
alpha rhythm
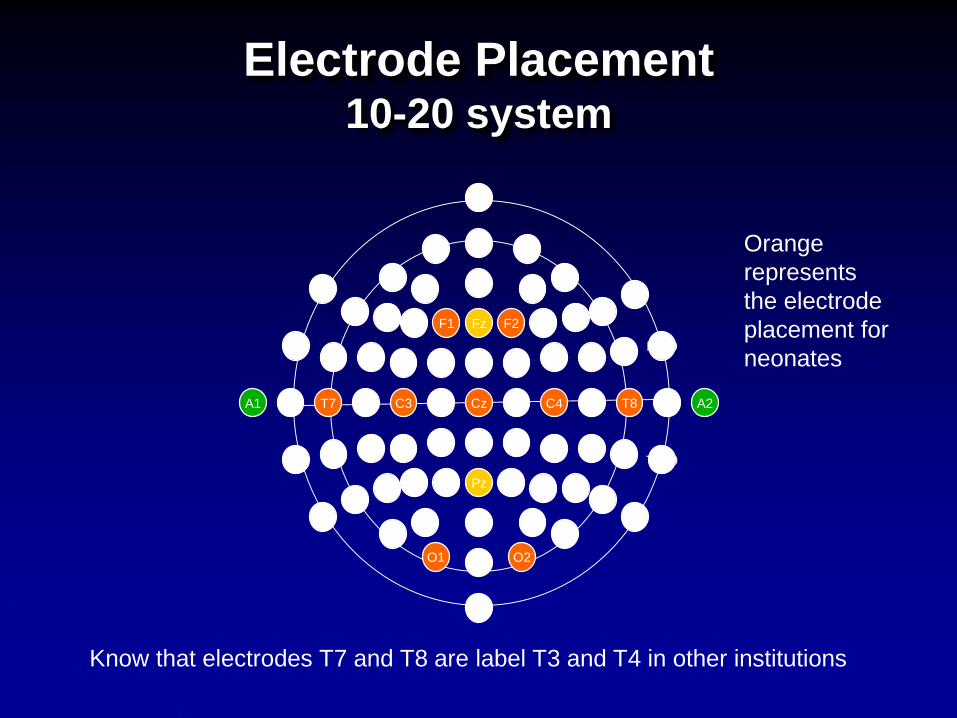
Electrode Placement10-20 system
Nz
FPz
AFz
Fz
FCz
Cz
CPz
Pz
FC3
F3
AF3
Fp1
Iz
Oz
POz
FC1
F1
O1
PO3
P3
CP3
C3
P2 P4
PO4
O2
C1
CP1
P1
AF4
Fp2
F2
FC2
C2
CP2 CP4
C4
FC4
F4
CP6 TP8 TP10
P10
P8P6
PO8
FC6
C6 T8 A2T10
FT8
F10
F8F6
FT10
PO7
AF8
P7P5
CP5
C5
FC5
AF7
F5
T9A1 T7
TP9 TP7
P9
F7
F9
FT9FT7
Know that electrodes T7 and T8 are label T3 and T4 in other institutions
Orange
represents
the electrode
placement for
neonates

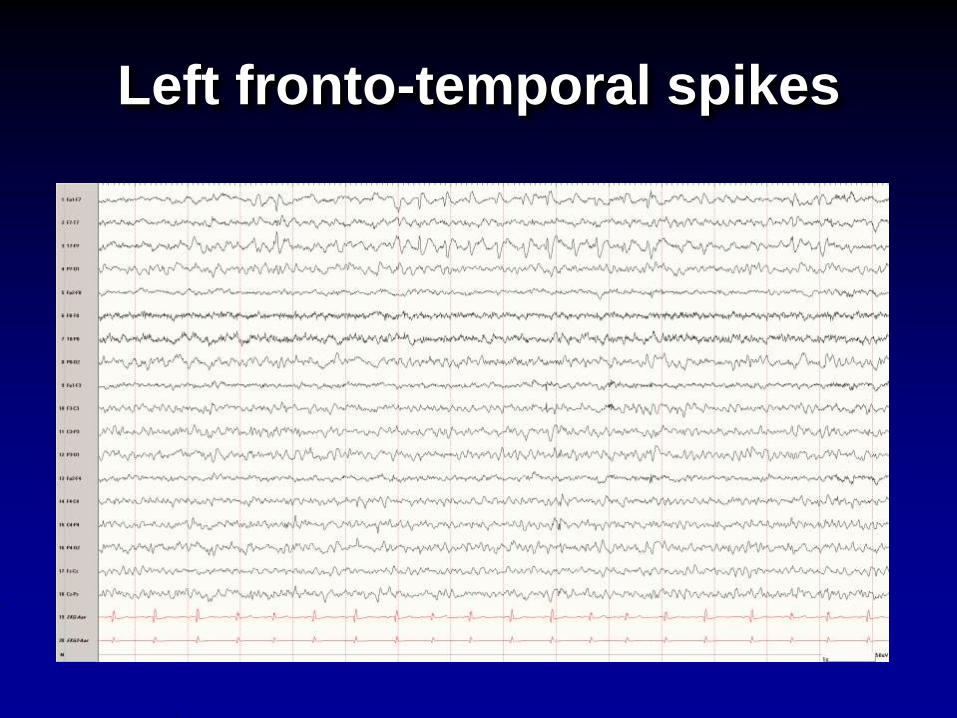
Left fronto-temporal spikes
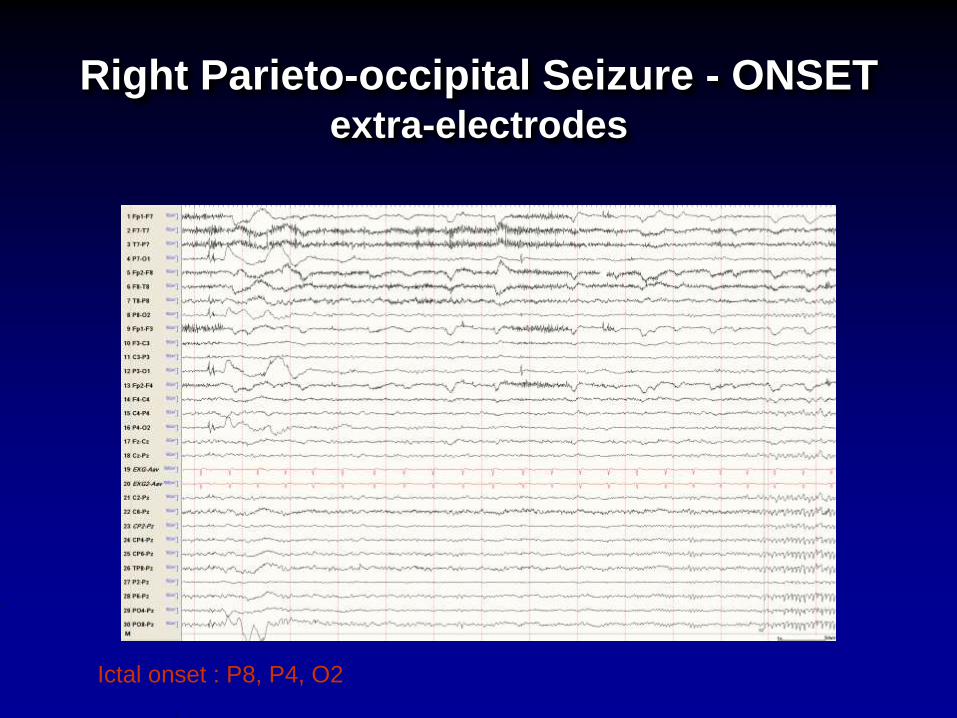
Right Parieto-occipital Seizure - ONSETextra-electrodes
Ictal onset : P8, P4, O2
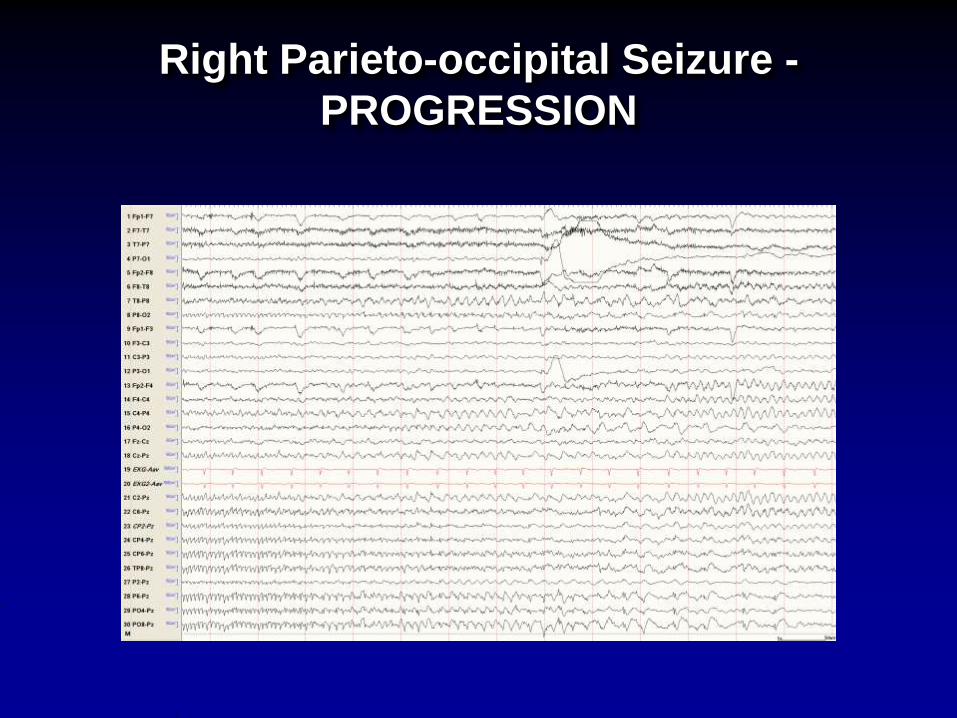
Right Parieto-occipital Seizure -
PROGRESSION
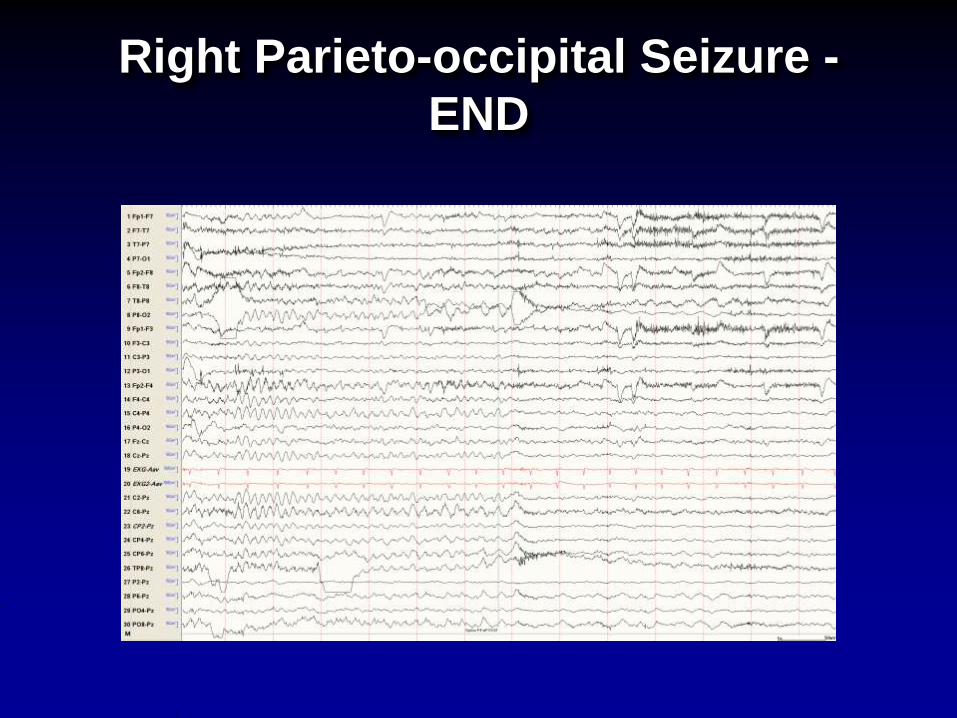
Right Parieto-occipital Seizure -
END
Brain MRI
• Recommended to be done in all patients with new onset seizures in a non-urgent setting
• Shows abnormalities that can potentially produce epilepsy such as:
- Mesial Temporal Sclerosis also known as hippocampal sclerosis
- Tumors
- Vascular malformation and strokes
- Malformation of the cortical development
09/08/06 University Hospitals Neurological Institute 19
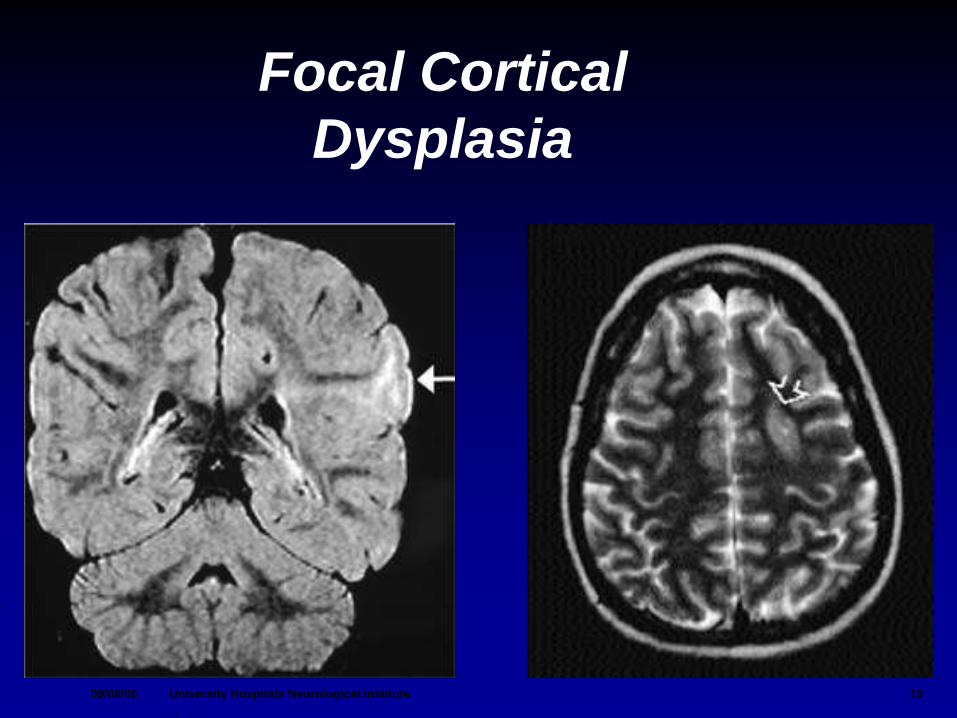
Focal Cortical
Dysplasia
PET Scan
Positron Emission Tomography
• Shows how the brain functions, specifically how various regions of the brain utilize (metabolize) glucose (sugar)
• It is helpful in providing additional information for accurately locating epilepsy in a specific region of the brain
• Requires the injection of a radiotracer (substance that has been radiolabeled so it can be identified when the patient is in the scan)
PET scan
Ictal SPECT ScanSingle Photon Emission Computed
Tomography
• Shows how the brain functions before (interictal) and during the seizure (ictal)
• Useful for the detection of the focus that generates the seizures
• Measures the relative blood flow in various regions of the brain at a specific moment in time.
• Requires the injection of a radiotracer (substance that has been radiolabeled so it can be identified when the patient is in the scan)
Ictal SPECT
Neuropsychological Testing
• Identifies cognitive weakness correlating it with areas of brain dysfunction or seizure onset
• Identifies the functional capacity of patients
• Predicts neurosurgical outcomes, risk for changes after the surgery, i.e. memory dysfunction, cognitive changes, etc.
TESTS TO LOCALIZE SPIKES AND
SOME SPECIFIC FUNCTIONS:
MEMORY, MOTOR AND
LANGUAGE
Other complementary tests
MEG
Magnetoencephalography
• Measures the magnetic field generated
by electric current within the brain
neurons
• EEG and MEG are complementary and
can be recorded simultaneously
• useful mainly for interictal recording
• not available in all centers
• requires patient cooperation
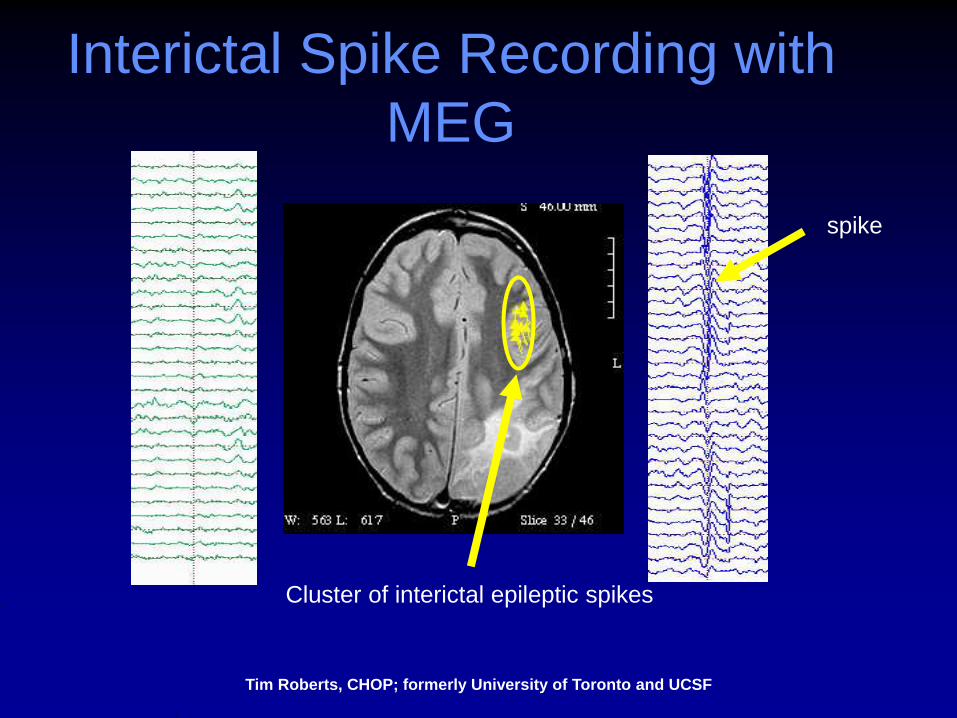
Cluster of interictal epileptic spikes
spike
Interictal Spike Recording with
MEG
Tim Roberts, CHOP; formerly University of Toronto and UCSF
fMRI (functional MRI)
• Used to map language, motor function,
and interictal spikes
• Localizes those areas by looking at the
difference oxygenated and
deoxygenated hemoglobin before and
during specific activation task
• Requires active cooperation of the
patient
• Not available in all center
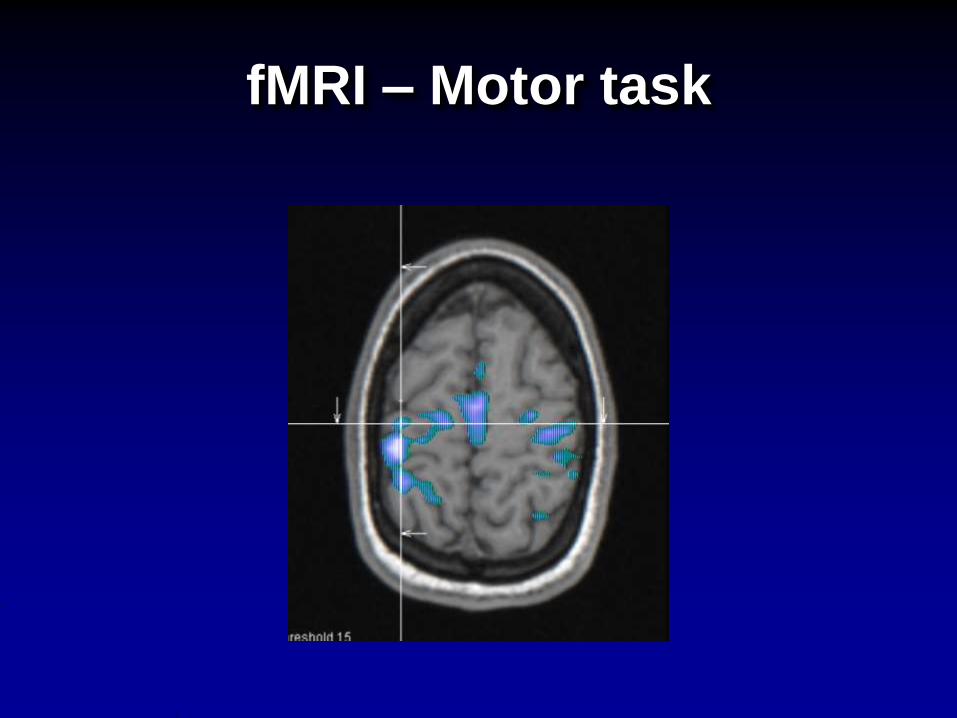
fMRI – Motor task
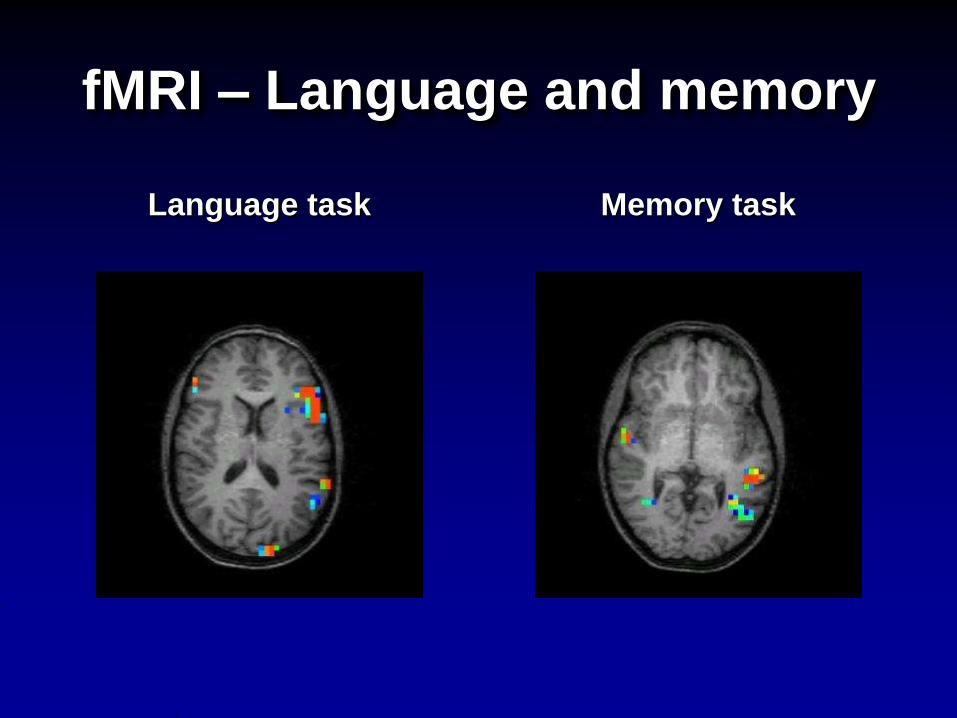
fMRI – Language and memory
Language task Memory task
The Wada Test
Intracarotid Amobarbital
Procedure
• is named after the Japanese physician
who first performed it, Dr. Jun Wada
• used to localize language and memory
• it is an invasive procedure meaning
that patient will need anesthesia and
femoral artery access to reach the
internal carotid artery
• requires patient cooperation
DIET FOR EPILEPSY
When do we use ketogenic diet:
• Patient has failed more than 2 antiepileptic medications
• Patient is not a surgical candidate
• Patient has generalized epilepsy, in particular myoclonic
• Patient has epileptic encephalopathy
• Don’t Miss –
- Glut 1 deficiency
- Pyruvate dehydrogenase deficiency
Livingston S. et al. Ketogenic diet in the treatment of childhood epilepsy.
Dev Med Child Neurol. 1977;19;833-834
KG Diet for some specific
Epilepsy Syndromes
• Early infantile epileptic encephalopathy (Ohtahara Syndrome)
• Early myoclonic epilepsy
• Myoclonic absence epilepsy
• Lennox—Gastaut
• Myoclonic—Astatic Epilepsy (Doose syndrome)
• Severe myoclonic epilepsy in infancy (Dravet syndrome)
• Rett Syndrome
• Tuberous Sclerosis Syndrome
Other benefits of the Ketogenic Diet
• Weight loss
• Potential to reduce medication dosages or
number
• 20% of patients are able to discontinue
medications over time
• Improvements in behavior and development
• Potential for long term
neuroprotective/antiepileptogenic process
• Of those who achieved seizure freedom, up
to 80% remain seizure free once off the diet
(after 2 years) (Marsh EB, et al. Epilepsia. 2006;
47(2):425-430)
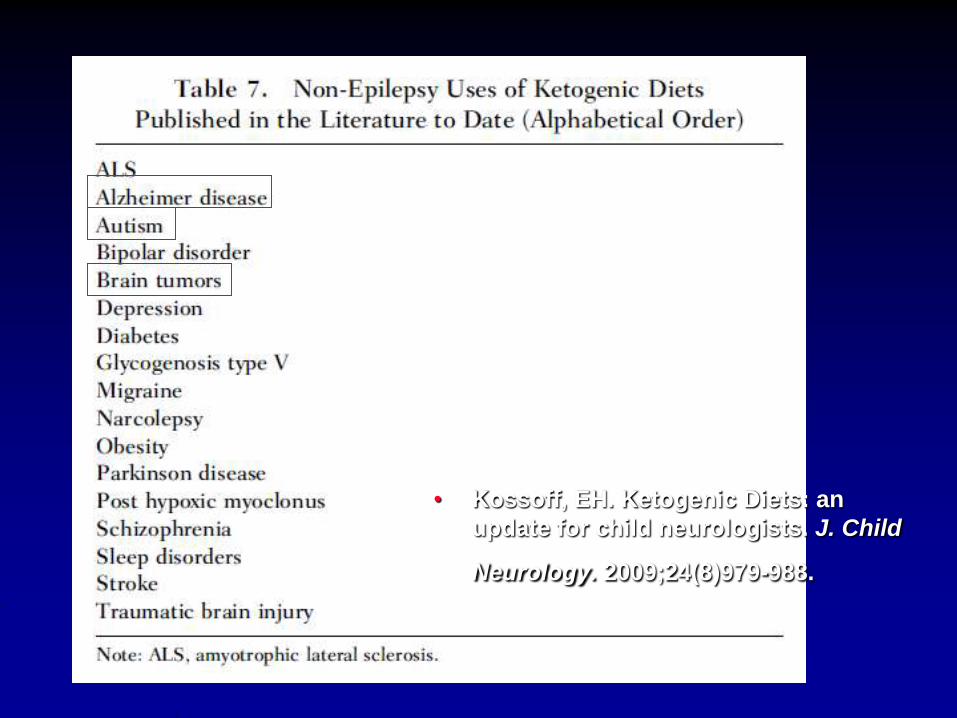
Other uses of ketogenic diet
Kossoff, EH. Ketogenic Diets: an update for child neurologists. J. Child Neurology.
2009;24(8)979-988.
• Kossoff, EH. Ketogenic Diets: an
update for child neurologists. J. Child
Neurology. 2009;24(8)979-988.
Epilepsy and Diet
Historical Aspects
• There are multiple ancient references to starvation or diet alteration in the treatment of epilepsy
- Dating back to 400 BC and include Hippocrates, Galen and Erasistratus
• “One inclining to epilepsy should be made to fast without mercy and be put on short rations”
Epilepsy and Diet
Historical Aspects
• The middle ages: ‘the Falling Sickness’
Possession
Falling Evil
Lunacy
Diets,
Drugs,
Rational <-> Superstitious
Magical <-> Religious
Remedies:
Blood,
bones,
plants,
precious
stones
Amulets,
Observing
the moon,
Prayer to
God
Fasting
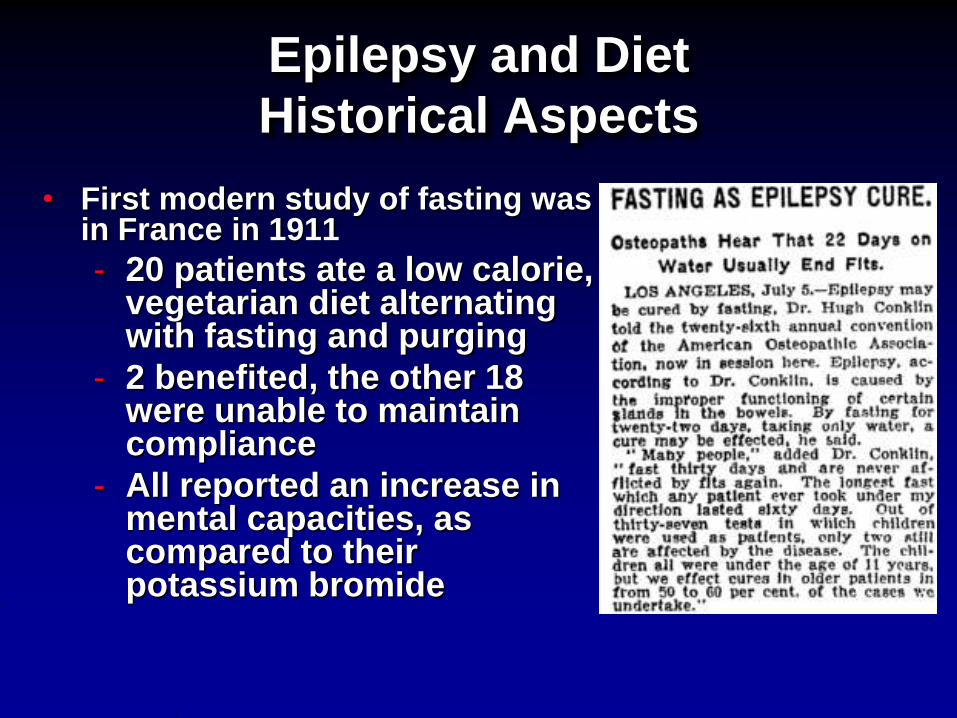
Epilepsy and Diet
Historical Aspects
• First modern study of fasting was in France in 1911
- 20 patients ate a low calorie, vegetarian diet alternating with fasting and purging
- 2 benefited, the other 18 were unable to maintain compliance
- All reported an increase in mental capacities, as compared to their potassium bromide
Epilepsy and Diet
Historical Aspects
• In 1925 Wilder and Peterman released data on children:- 95% of 37 children had improved seizure
control, 60% were seizure free
• By 1930 it had been studied on 100 teens and adults- 56% of 100 improved, 12% were seizure free
- This was the last study of ketogenic diet use in adults with epilepsy until 1999
Epilepsy and Diet
Historical Aspects
• In the 1920’s and 30’s the diet was widely
used due to limited drug options:
bromides (1857) and Phenobarbital (1912)
• With the discovery of phenytoin (1938)
and subsequently valproic acid (1970’s),
the use of the diet declined
• The first randomized controlled trial was
published in 2008, 87 years after its
introductionNeal, EG, et al. The ketogenic diet for the treatment of childhood epilepsy:
a randomized controlled trial. Lancet Neurol. 2008;7(6):471-472.
How the ketogenic diet
works?
• The exact mechanism of action is unknown
What is the efficacy of the
ketogenic diet?
• 58% seizure free
• 35% with >50% reduction
Ketogenic Diet
Implementation
• Two approaches:
- Traditional approach: • complete fast for up to two days (historically with
fluid restriction)
- New approach: • immediate initiation of the diet at a reduced
concentration
Ketogenic Diet Prescription
• Ratio 3: 1 or 4:1



Ketocal
Energy Distribution:
Protein 8.2% Carbohydrate 3.1% Fiber1.5% Fat (LCT 100%)90%
Ketogenic Diet—Adverse
Effects
• Patients have reported a consistently reduced quantity of bone mass
- Improves with Vitamin D 5000 IU/day
- Especially significant in those who remain on high risk AED’s
• Kidney stones 6-10%%
• GI symptoms, constipation, nausea, vomiting, abdominal pain
• Elevated lipids (typically transient) and without long term complications
• Thinning of hair and (rarely) alopecia can occur
• Growth retardation
• Carnitine deficiency
• Severe low protein in body
• Elevations in liver function tests (typically with concurrent medication with VPA)
• Bilateral optic neuropathy (improved with Vitamin B supplementation)
Medications to discuss with your
doctor due to Potential Adverse
Drug Reactions
• Medical suspensions: Have sugars added• Children’s Tylenol has 1g per 0.8mls
• Acetazolamide and topiramate
• Valproate: elevated liver enzymes
• Phenobarbital: serum concentration increases in acidotic state
• Carnitine is not contraindicated, but interferes with ketone production
• Others: toothpastes, sunscreens, lotions, shampoo
When to stop the ketogenic
diet?
• Diet has been ineffective after 2-3 months
of trial with documentation of ketosis
• Patient is having undesirable side effects
Think about the ketogenic diet
as another antiseizure
medication
• The diet needs to be stopped gradually
(wean)
• Consumption of glucose or
administration of glucose in fluids can
result in break though seizures
Other diet modalities used in
epilepsy
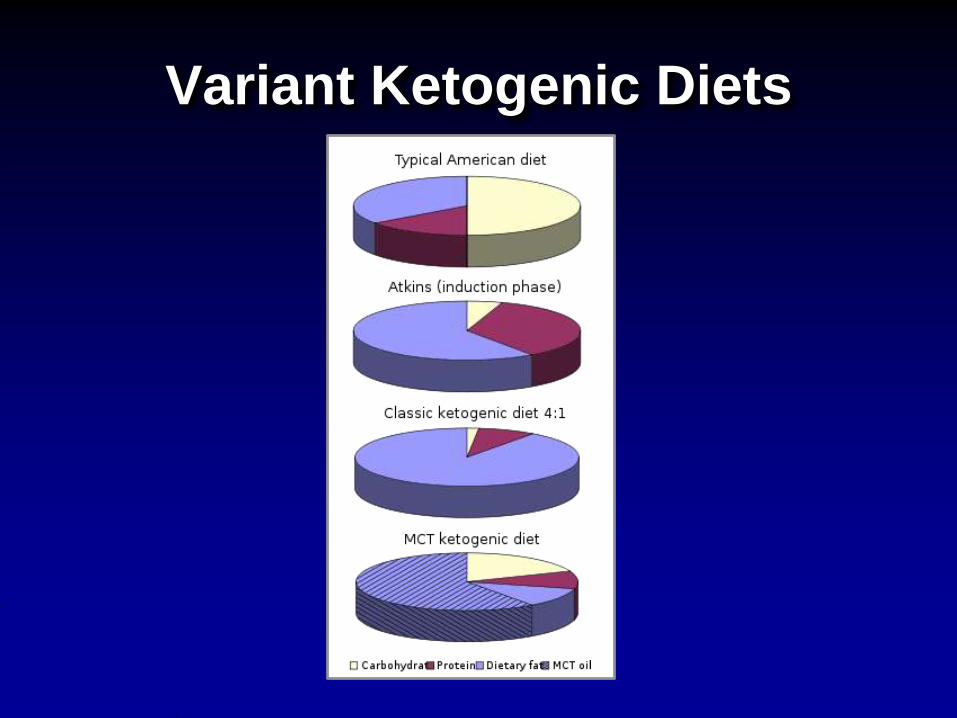
Variant Ketogenic Diets
Dietary Therapies Other than
Classical Ketogenic Diet
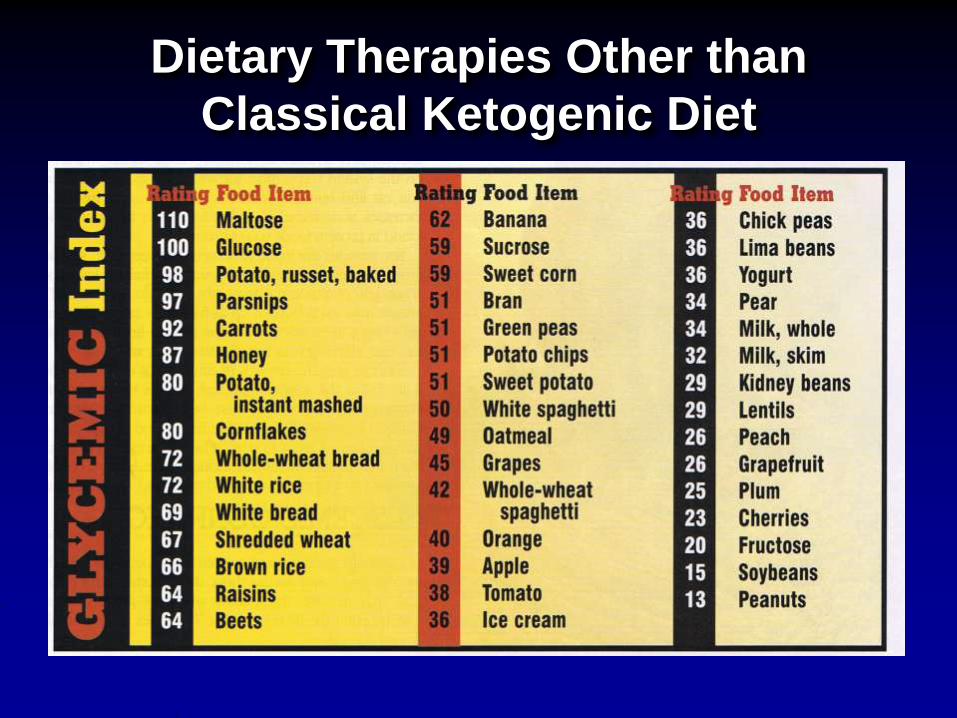
• Low Glycemic Index treatment (Smart Carbohydrate intake)- Works around theory that ketogenic diet may work in part because of
stable, lower serum glucose
- Goal is not ketosis, but chronic stable low glucose
- Remains a high fat diet (60%) but allows most carbohydrates of all the diets (40-60g/d). • Carbs must have a glycemic index under 50
• 1:1 ratio
- Foods are estimated
- Diet is started at home
- Short term results indicate a 50% reduction in seizure frequency with figures approaching the KD.
- Side effect profile is reduced and meals are more palatable and tolerated
- Use of the glycemic index is good for heart health, diabetes
• Modified Atkins (Carbohydrate-only restriction)- Developed at Johns Hopkins after Epilepsy
patients reported in improvement in seizure frequency with induction on Adkins diet
- Modified diet’s goal changed from weight loss to continuous induction phase (prolonged ketosis) and encouraged fat consumption (65% of calories)
- Less severe dietary restrictions, with no limit on calories or protein and a loose ratio of 1:1, foods are “estimated”
Modified Atkins (Carbohydrate-only
restriction)
Modified Atkins (Carbohydrate-only
restriction)
- All carbohydrate types are allowed and can be given all at once
- 10g carbohydrate for children/20g for adults, but may liberalize in 1-3 months to 20-30g/d based on seizure control
- Still require vitamin supplementation
- Few side effects, but cholesterol is increased, and it is a newer diet
- Does not require an hospitalization but routine monitoring is still required
Medium Chain Triglyceride Therapy
- A new spin on the Classic ketogenic diet, which based on Long chain (13-21 carbons) triglyceride therapy
- Produce more ketones than LCT’s
- Allows a reduction in calories from fat, and increment the amount of carbohydrates in diet (approx. 1:1 ratio of F:P+C)
- Some investigators have found this to be less efficacious than the classic ketogenic diet, but this is inconsistent in studies and likely patient dependent
- Side effects: abdominal cramps, diarrhea and vomiting
Questions??
If you have questions, please type
them into the “Viewer questions
and suggestions” box below the
video