Embed Size (px)
DESCRIPTION
First Annual Minnesota Pediatric Obesity Conference Practical Approaches for Managing and Preventing Pediatric Obesity . Surgery: Considerations and Research . Sayeed Ikramuddin, MD. Aldolescent obesity. Disclosures. Fellowship support: Ethicon, Covidien R esearch grant support: Covidien - PowerPoint PPT Presentation
Citation preview

Surgery: Considerations and Research
Sayeed Ikramuddin, MD
First Annual Minnesota Pediatric Obesity Conference Practical Approaches for Managing and Preventing Pediatric Obesity
Aldolescent obesity

Disclosures
•Fellowship support: Ethicon, Covidien•Research grant support: Covidien•Proctorship: Ethicon•I will discuss off label use of the gastric band system

Pories, W.J., et al., Who would have thought it? An operation proves to be the most effective therapy for adult-onset diabetes mellitus. Ann Surg, 1995. 222(3): p. 339-50; discussion 350-2.
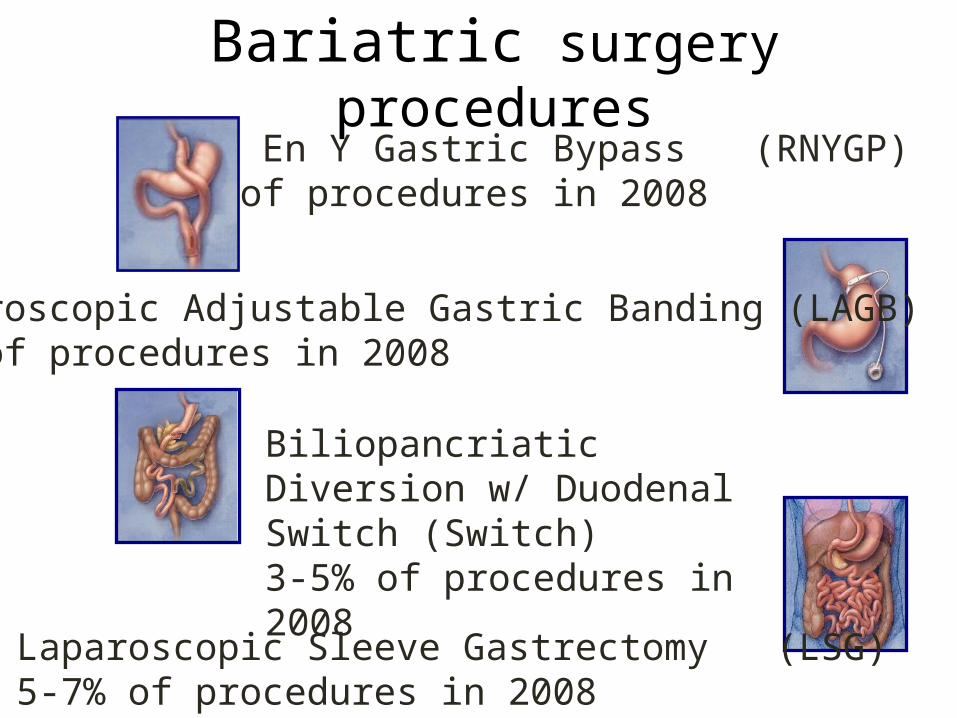
Bariatric surgery procedures
Laparoscopic Adjustable Gastric Banding (LAGB)40% of procedures in 2008
Biliopancriatic Diversion w/ Duodenal Switch (Switch) 3-5% of procedures in 2008
Laparoscopic Sleeve Gastrectomy (LSG)5-7% of procedures in 2008
Roux En Y Gastric Bypass (RNYGP)50% of procedures in 2008
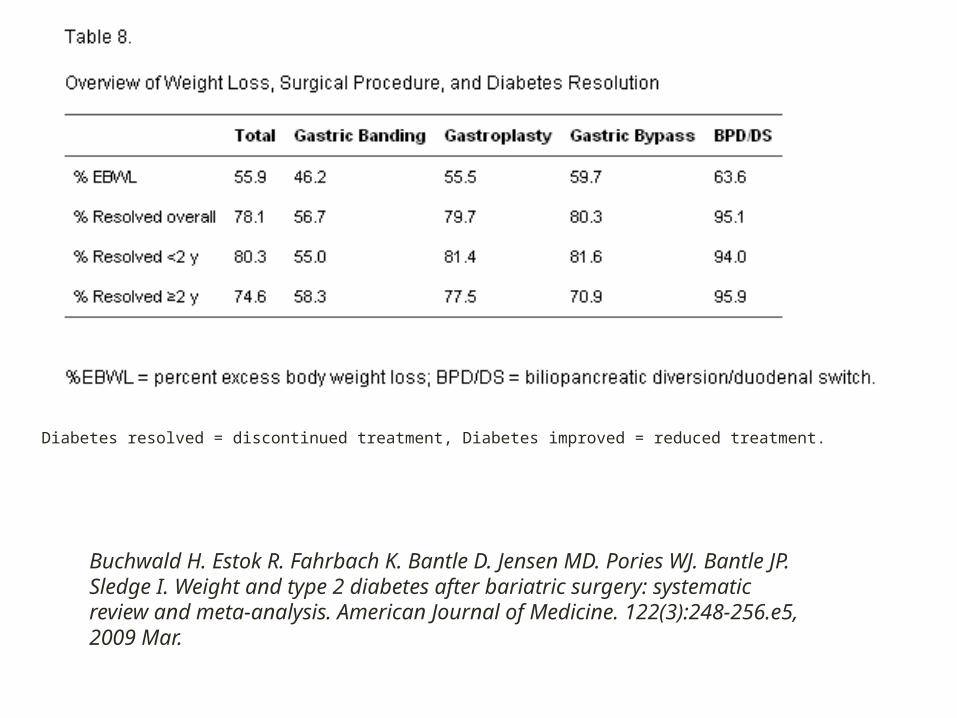
Buchwald H. Estok R. Fahrbach K. Bantle D. Jensen MD. Pories WJ. Bantle JP. Sledge I. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. American Journal of Medicine. 122(3):248-256.e5, 2009 Mar.
Diabetes resolved = discontinued treatment, Diabetes improved = reduced treatment.

7 |
Glycemia as an Endpoint
Year Author N Level Therapy Control Outcome
2008 Dixon J 60 ALAGB (BMI
30-40 kg/m2)Medical
management 72% Resolution of Type 2 DM
2007 Sjostrom L 4047 A
Surgery (GBP, GB,
VBG)Medical
management 24% reduction in mortality with surgery
2006 O’Brien PE 79 ALAGB (BMI 30-34 kg/m2)
Medical management
Reduction in metabolic syndrome 93%- surgery vs.
46%- medical management
2004 Buchwald H 22,094 BBariatric Surgery Meta Analysis 77% Resolution of Type 2 DM
2007 Adams TD 15,850 B RYGBPConventional
treatment 92% reduction in diabetes related death
2006 le Roux CW 39 BRYGBP/LAGB
Lean and obese patients
improved insulin, GLP-1 response after RYGBP
2008 Lee WJ 158 CRYGBP < 35
kg/m2RYGBP >35
kg/m276.5% success in BMI<35 kg/m2; 88.9%
success in BMI 35–45 kg/m2,
2006 Cohen R 37 CRYGBP < 35
kg/m2 97% Resolution of Type 2 DM
2005 Torquati A 107 C RYGBP 72% Resolution of Type 2 DM
2005Wickremesekera
K 31 C RYGBP Insulin resistance decrease at 6 days post surgery maintained after 12 months;
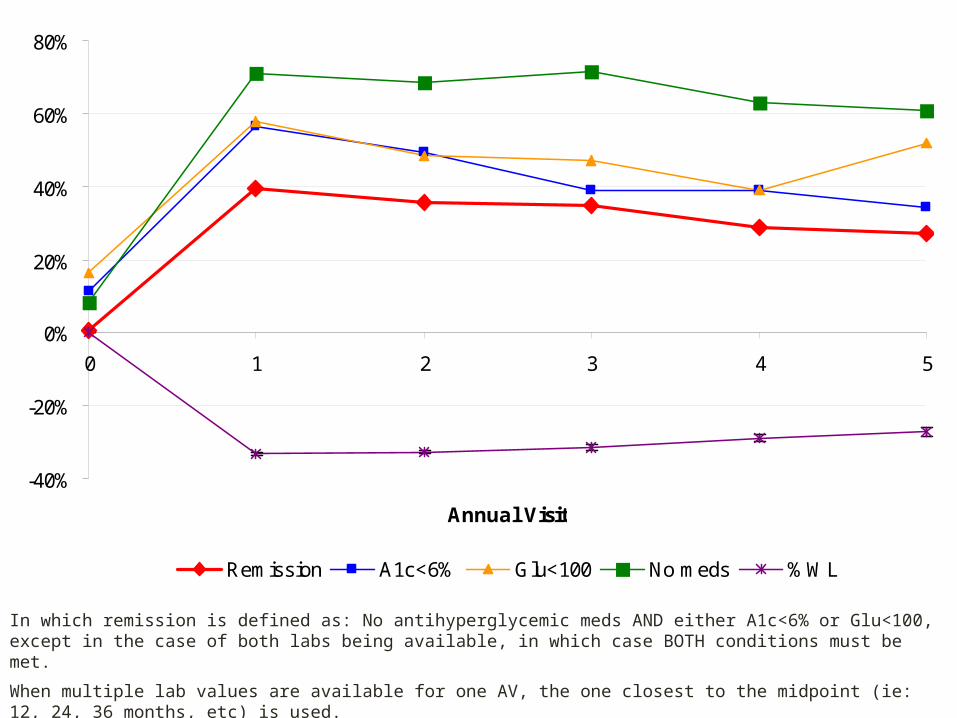
In which remission is defined as: No antihyperglycemic meds AND either A1c<6% or Glu<100, except in the case of both labs being available, in which case BOTH conditions must be met.
When multiple lab values are available for one AV, the one closest to the midpoint (ie: 12, 24, 36 months, etc) is used.
%Weight Loss (%WL) = [ (Weight Preop – Weight Postop) / Weight Preop ] *100
-40%
-20%
0%
20%
40%
60%
80%
0 1 2 3 4 5
Annual Visit
Remission A1c<6% Glu<100 No meds %WL

Gastric bypass
Small divided gastric pouch (30 cc)Roux limb 75cm-150cm Biliopancreatic limb 20cm-100cmantecolic or retrocolic roux“Gold Standard”

Bypass considerations
Longest followupmoderate malabsorption (Iron, B12, Thiamine)hypoglycemiamarginal ulcersexcluded stomachinternal herniaHigher perioperative complications
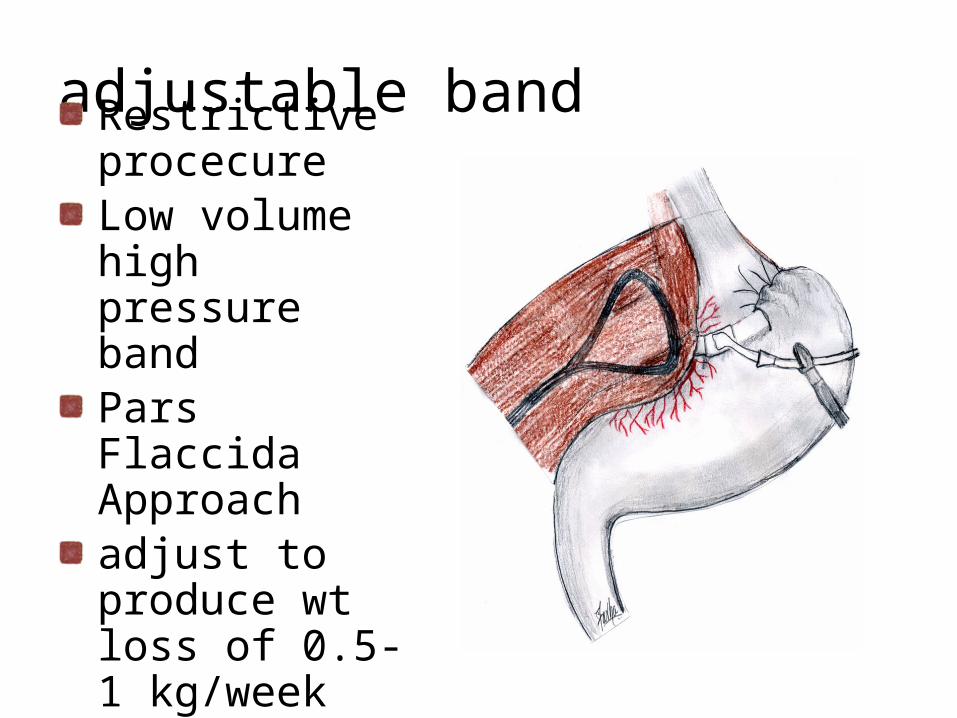
adjustable band
Restrictive procecureLow volume high pressure bandPars Flaccida Approachadjust to produce wt loss of 0.5-1 kg/week
Band considerations
Not FDA approved for < 18very low short term morbidity and mortalitypoor results in the superobese explantation 10%long-term risk of slippagelong-term risk of erosionneed for adjustments

Procedures
• Band
• Sleeve• Gastric bypass• Duodenal switch

Sleeve considerationslittle long term datapotential for leak insurance coverage an issueIncreased incidence of GERDNo nutritional complicationsease of conversion to DS or to RNY

Duodenal switch
Malabsorbtive and restrictive proceduremost durable weight loss4% incidence of revision for nutritional problems42F sleeve (32-60)100 cm common channel (50-125)

Effectiveness of Weight Management Programs inChildren and Adolescents
http://www.ahrq.gov/downloads/pub/evidence/pdf/childweight/chweight.pdf
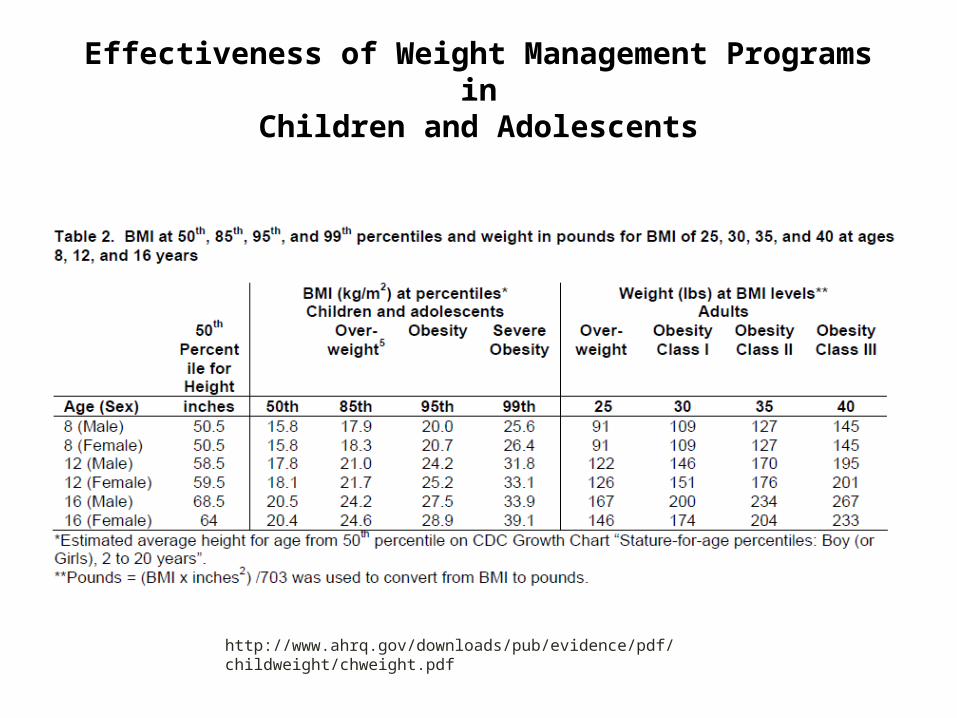
Effectiveness of Weight Management Programs inChildren and Adolescents
http://www.ahrq.gov/downloads/pub/evidence/pdf/childweight/chweight.pdf
Introduction Weight Loss Surgery in Adolescents
The treatment of the morbidly obese adolescent patient is controversial.No clear consensus on best treatment of the morbidly obese adolescent.Contention between bariatric surgeons and pediatricians.

Adolescent Obesity and DiabetesWhat is Known
A steep rise in the prevalence of T2DM parallels the rise in obesity .Young patients with T2DM have rapidly progressive disease.5 fold increase in the incidence of obesity since 1970’sProgressive retinopathy and ASHD noted within 5yrs of diagnosis of T2DM in young adults.Health-related QOL 5.5x more likely to be impaired compared to healthy kids. similar to those diagnosed as having cancer.
# Kohn M and Booth M. Adol Med 2003 *Schwimmer JB, Burwinkle TM, Varni JW. JAMA 2003

Adolescent ObesityWhat is Unknown
When is the best time in the course of development (physical and emotional) for surgical intervention?How is compliance in this patient population?What are the long-term nutritional sequelae?What are the multi-generational sequelae?What are the long-term outcomes and recidivism rates?

Author (year) N Procedure (n) Age range
Mean follow-
up
Mean %EWL
Compl.rate Deaths
Lawson MLet al. (3 centers;
2006)39 LRYGB (34)
ORYGB (5) 13 to 21 1 year(n=30) 63% 39%
(n=15)1
(9 mos.)
Sugerman, et al. (2003) 33
LRYGB (2)ORYGB (28)
Open gastroplasty (3)12 to 17 Up to
14 years 58% 40% (n=13) 2 (late)
Stanford et al.(2003) 4 LRYGB (4) 17 to 19 17 mos. 87% 0% 0
Strauss et al. (2001) 10 ORYGB (10) 15 to 17 > 1 year 55% 50% late
(n=5) 0
Rand et al.(1994) 34 ORYGB (30)
Open gastroplasty (4) 11 to 19 6 years 66% NR 0
Barnett et al.(2005) 15
Open gastroplasty (7)ORYGB (5)
JIB (3)13 to 17
6 years(>9 mos.)
(n=9)64% 33%
(n=5) 0
Bariatric surgery Outcomes
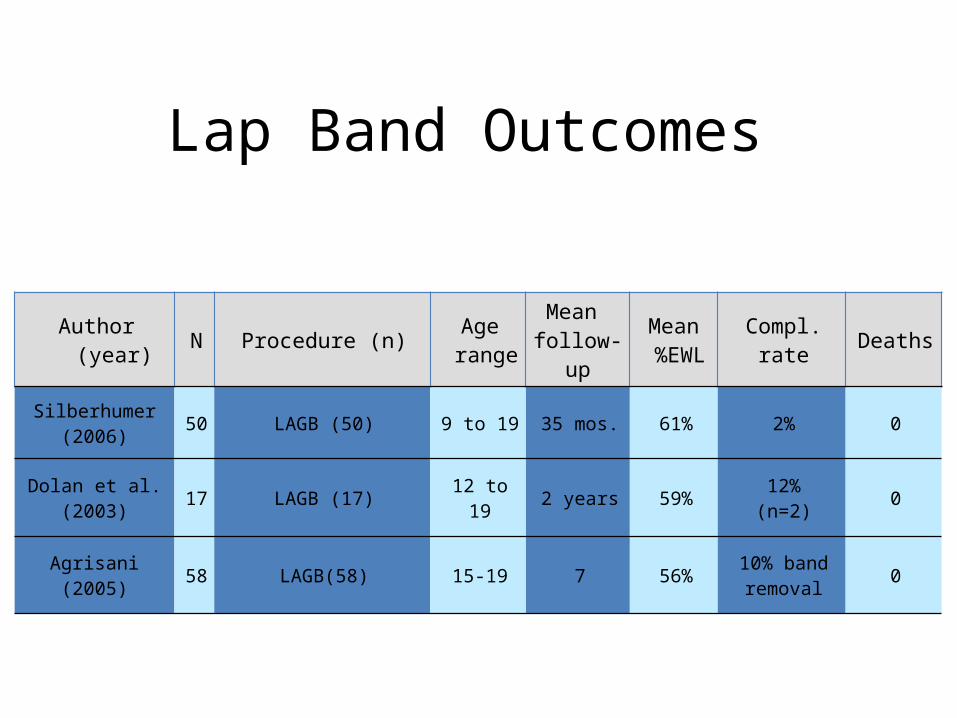
Author (year) N Procedure (n) Age range
Mean follow-
up
Mean %EWL
Compl.rate Deaths
Silberhumer(2006) 50 LAGB (50) 9 to 19 35 mos. 61% 2% 0
Dolan et al.(2003) 17 LAGB (17) 12 to 19 2 years 59% 12%
(n=2) 0
Agrisani (2005) 58 LAGB(58) 15-19 7 56% 10% band removal 0
Lap Band Outcomes

Current Management of the Morbidly Obese Adolescent at the University of Minnesota
Evaluation by multidisciplinary team(statewide).Pediatric gastroenterologist / weight loss specialistPediatric psychologistBariatric surgeon with > 50 cases adolescentDietician: minimum of 6 months
Intensive medical weight loss programOutpatient / inpatient treatment
Bariatric surgery candidateDemonstrated compliance with medical weight lossSerious medical comorbidities

Demographics: LRYGB (n=30)Laparoscopic Weight Loss Surgery in Adolescents
Mean age 17.0 (range 12-19)8 patients ≤ 15 years
Mean BMI 55 kg/m2 (range 35-100)Mean weight 156 kg (range 99-275 kg)All > 95th percentile for BMI
Two patients with BMI > 90 kg/m2 were hospitalized ≥ 1 month preoperatively for intensive medical management.
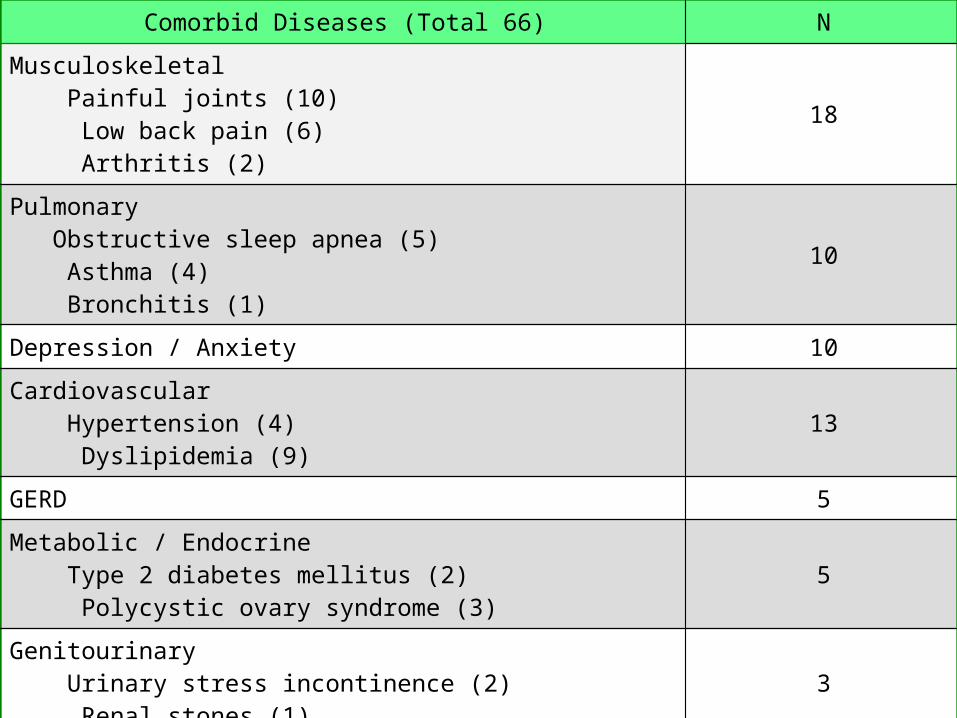
Comorbid DiseaseComorbid Diseases (Total 66) N
Musculoskeletal Painful joints (10) Low back pain (6) Arthritis (2)
18
Pulmonary Obstructive sleep apnea (5) Asthma (4) Bronchitis (1)
10
Depression / Anxiety 10
Cardiovascular Hypertension (4) Dyslipidemia (9)
13
GERD 5
Metabolic / Endocrine Type 2 diabetes mellitus (2) Polycystic ovary syndrome (3)
5
Genitourinary Urinary stress incontinence (2) Renal stones (1)
3
Pseudotumor cerebri 2

Follow-UpLaparoscopic Weight Loss Surgery in Adolescents
Range 0 to 45 months, mean 15.8 months.14 patients had ≥ 12 month follow-up.Poor overall compliance with follow-up.
28.1% (n=9) lost to follow-up.Letters sent, phone calls made.
Of those who didn't follow-up55.6% (n=5) lost within first year44.4% (n=4) lost after 18 months
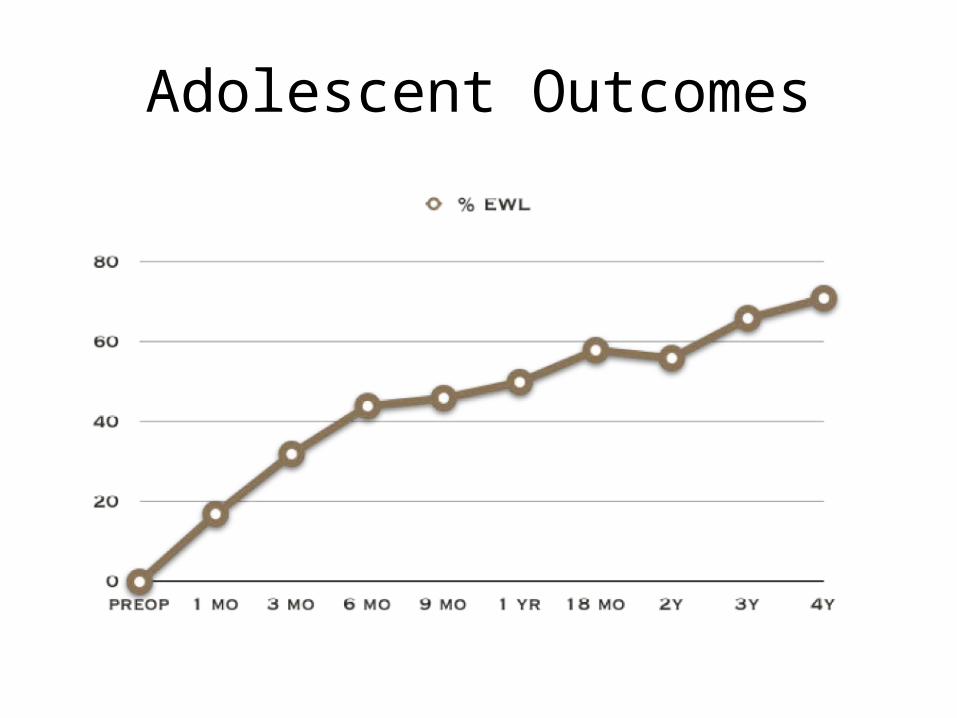
Adolescent Outcomes
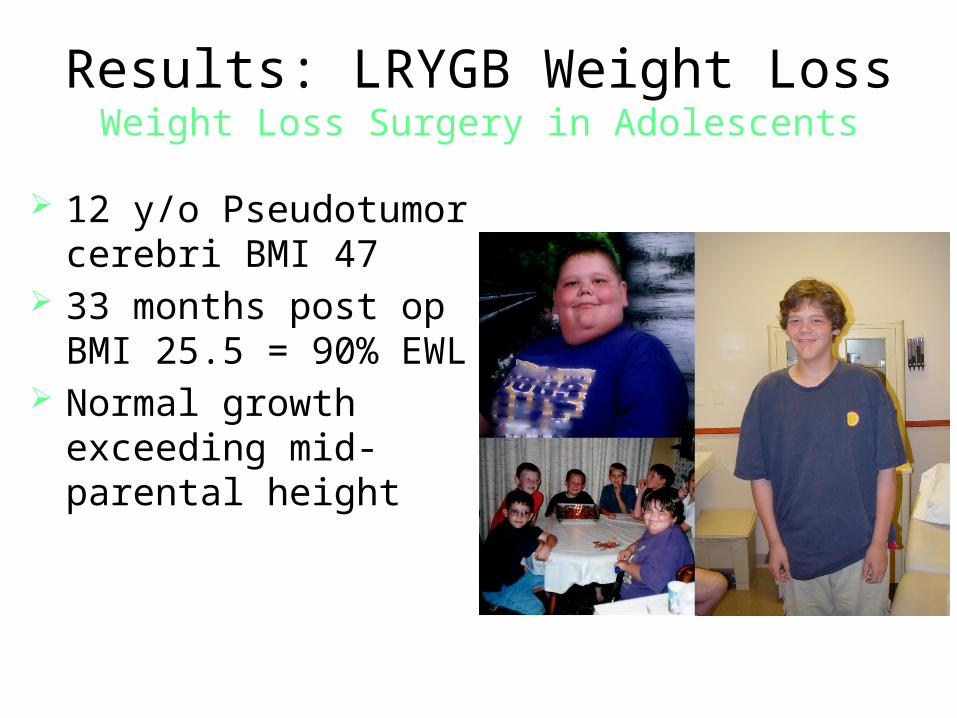
Results: LRYGB Weight LossWeight Loss Surgery in Adolescents
12 y/o Pseudotumor cerebri BMI 47
33 months post op BMI 25.5 = 90% EWL
Normal growth exceeding mid-parental height

Summary of Findings
Adolescent bariatric surgery appears to be similar to adult bariatric surgery in terms of weight loss and complications.surgery safe in short term followup across the age spectrumfollowup can be more difficult than the adult populationAbsolute commitment to post-operative follow-up schedules need to be made pre-operatively with adolescent patients and their parents.evidence for choice of operation mixed
Weight Loss Surgery in Adolescents
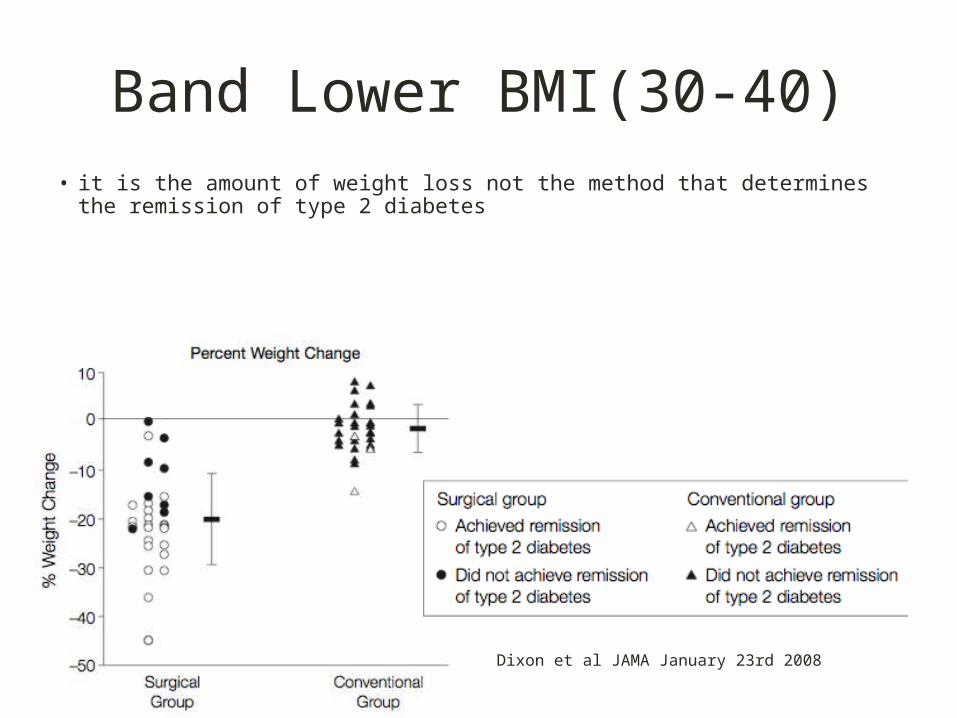
Band Lower BMI(30-40)• it is the amount of weight loss not the method that determines the remission of type 2
diabetes
Dixon et al JAMA January 23rd 2008
The Effects of Bariatric Surgery on Type 2 Diabetes
The Entero-insular Axis
• Glucagon-Like Peptide-1 or GLP-1 (“Enteroglucagon”)– Secreted by ileal “L-cells” in (rapid) response to a meal– Actions
• Potent stimulator of insulin / supresses glucagon• Slows gastric emptying• Reduces appetite• Increases beta cell mass• Increased after gastric bypass (??)
• Peptide YY (PYY)• Gastric Inhibitory Polypeptide (GIP)
Wynne K. J Clin Endo Met, 2004
The Effects of Bariatric Surgery on Type 2 Diabetes
The Entero-insular Axis• Enteral glucose ingestion yields a greater insulin release
than does parenteral glucose infusion *
• Secreted gut hormones effect insulin production, secretion and usage = “incretins” / “anti-incretins”
• Select “known” peptides with various effects
* Elrick H. J Clin Endocrinol Metab. 1964

The Effects of Bariatric Surgery on Type 2 Diabetes
The Entero-insular Axis
Rehfeld J, 2004
1967 – Gastric Bypass

Peptides in T2DM
• GLP-1 response to mixed meal is blunted compared to non diabetics
• GIP response is blunted• After weight loss GLP-1 response improves
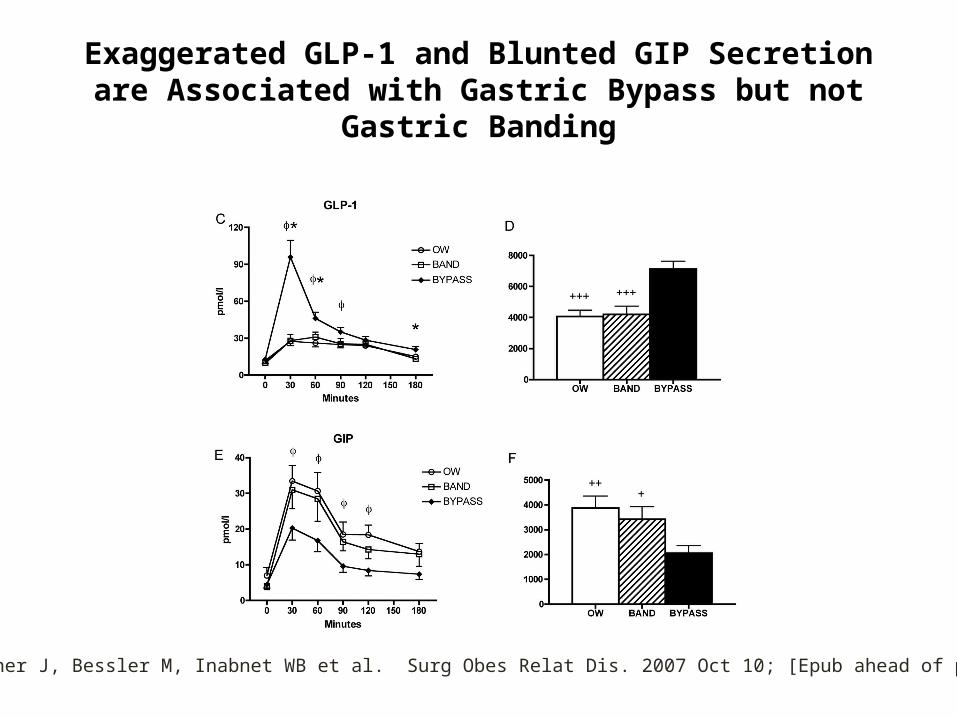
Exaggerated GLP-1 and Blunted GIP Secretion are Associated with Gastric Bypass but not Gastric Banding
Korner J, Bessler M, Inabnet WB et al. Surg Obes Relat Dis. 2007 Oct 10; [Epub ahead of print] .

Insulin response with OGTT RNY
LaFerre et al JCEM 2008
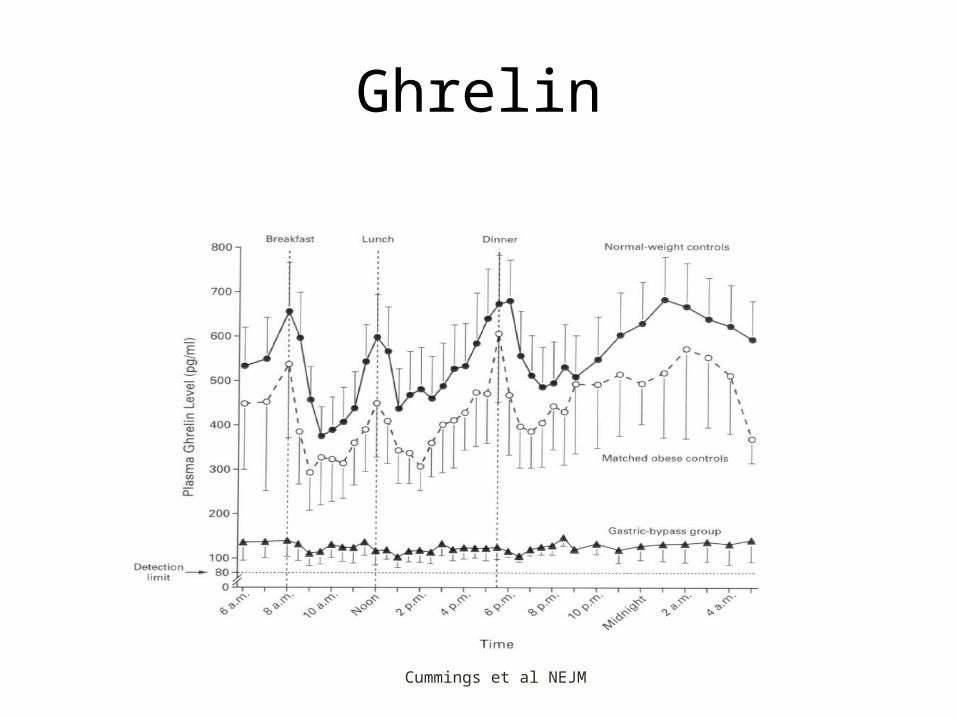
Ghrelin
Cummings et al NEJM

| April 22, 2023 | Confidential38 |38 |
Bariatric Surgery: Effects on Weight Loss and Mortality
29%
Sjostrom, L, et.al.; N Engl J Med. 2007;357:741-52
Years
Band
VBG
Cha
nge
in W
eigh
t (%
)
Control
80 4 6 15102
-30
0
-20
Gastric Bypass
Years80 4 1612
p = 0.04Cum
ulat
ive
Mor
talit
y (%
)
14
0
2
4
6
8
10
12Control
Surgery
-10
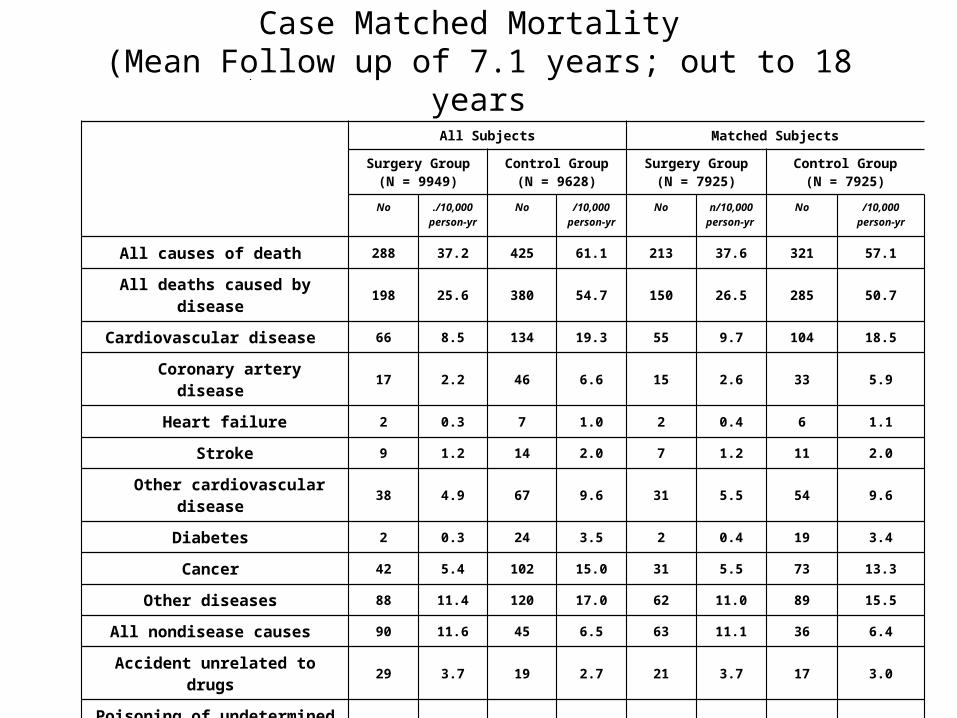
Case Matched Mortality (Mean Follow up of 7.1 years; out to 18 years
All Subjects Matched Subjects
Surgery Group(N = 9949)
Control Group(N = 9628)
Surgery Group(N = 7925)
Control Group(N = 7925)
No ./10,000person-yr
No /10,000person-yr
No n/10,000person-yr
No /10,000person-yr
All causes of death 288 37.2 425 61.1 213 37.6 321 57.1
All deaths caused by disease 198 25.6 380 54.7 150 26.5 285 50.7
Cardiovascular disease 66 8.5 134 19.3 55 9.7 104 18.5
Coronary artery disease 17 2.2 46 6.6 15 2.6 33 5.9
Heart failure 2 0.3 7 1.0 2 0.4 6 1.1
Stroke 9 1.2 14 2.0 7 1.2 11 2.0
Other cardiovascular disease 38 4.9 67 9.6 31 5.5 54 9.6
Diabetes 2 0.3 24 3.5 2 0.4 19 3.4
Cancer 42 5.4 102 15.0 31 5.5 73 13.3
Other diseases 88 11.4 120 17.0 62 11.0 89 15.5
All nondisease causes 90 11.6 45 6.5 63 11.1 36 6.4
Accident unrelated to drugs 29 3.7 19 2.7 21 3.7 17 3.0
Poisoning of undetermined intent 15 1.9 4 0.6 9 1.6 4 0.7
Suicide 21 2.7 8 1.2 15 2.6 5 0.9
Other nondisease cause 25 3.2 14 2.0 18 3.2 10 1.8
Conclusion• Type 2 DM is a complex disease • It is most strongly associated with obesity• Patient and physicians struggle to meet therapeutic goals• Bariatric surgery is established as a treatment of obesity• The effect on diabetes is profound• Clinical trials will allow for treatment of lower BMI
individuals• Adolescents want to look like their peers but they also
want to eat like their peers





























