Embed Size (px)
Citation preview

surgery as primary treatmentsurgery as primary treatment in prostate cancer
Donata VillariSod Urologia IISod Urologia IIAzienda Ospedaliera Universitaria CareggiFirenze
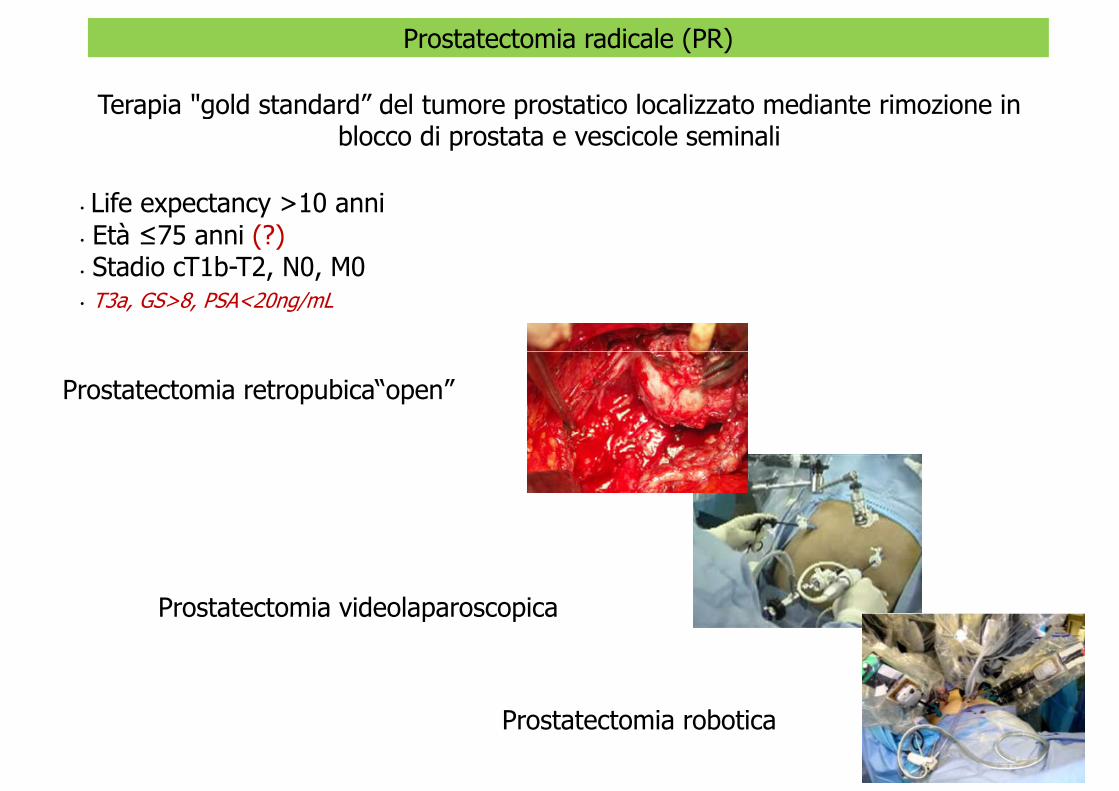
Prostatectomia radicale (PR)
Terapia "gold standard” del tumore prostatico localizzato mediante rimozione in blocco di prostata e vescicole seminali
• Life expectancy >10 anni• Età ≤75 anni (?)Stadio cT1b T2 N0 M0• Stadio cT1b-T2, N0, M0
• T3a, GS>8, PSA<20ng/mL
Prostatectomia retropubica“open”
Prostatectomia videolaparoscopicaProstatectomia videolaparoscopica
Prostatectomia robotica
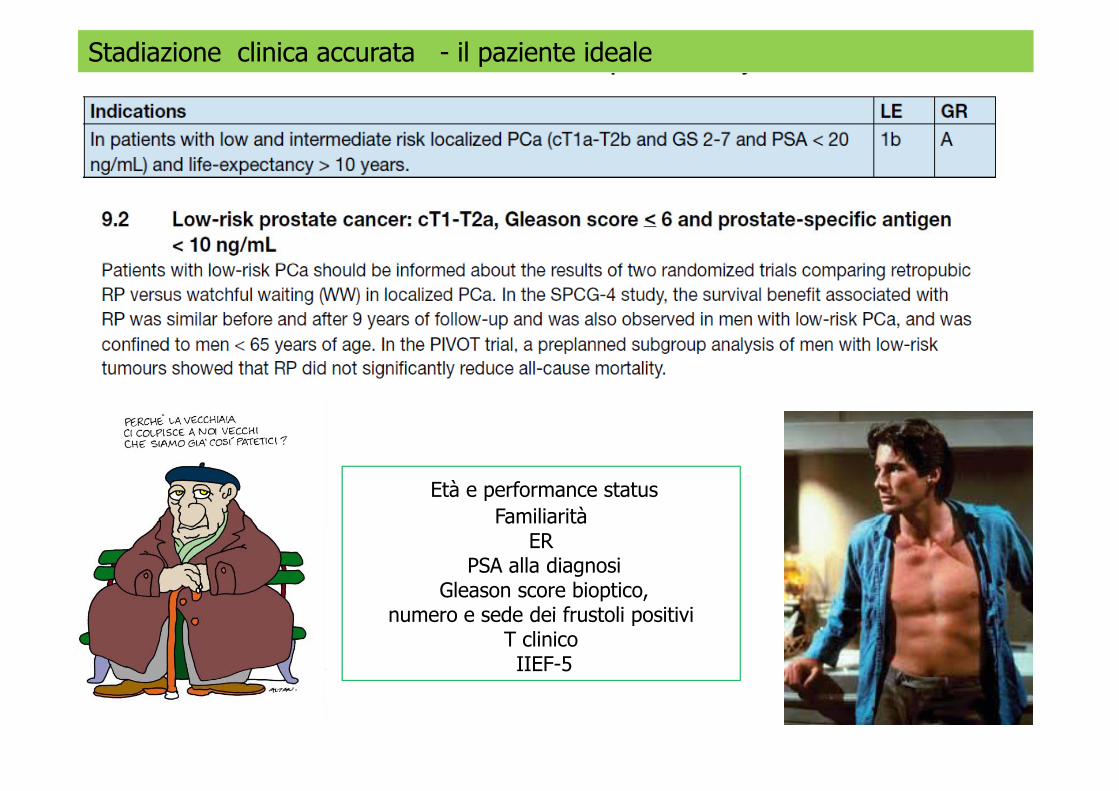
Stadiazione clinica accurata - il paziente ideale
Età e performance statusFamiliarità
ERPSA alla diagnosi
Gleason score bioptico, numero e sede dei frustoli positivinumero e sede dei frustoli positivi
T clinicoIIEF-5
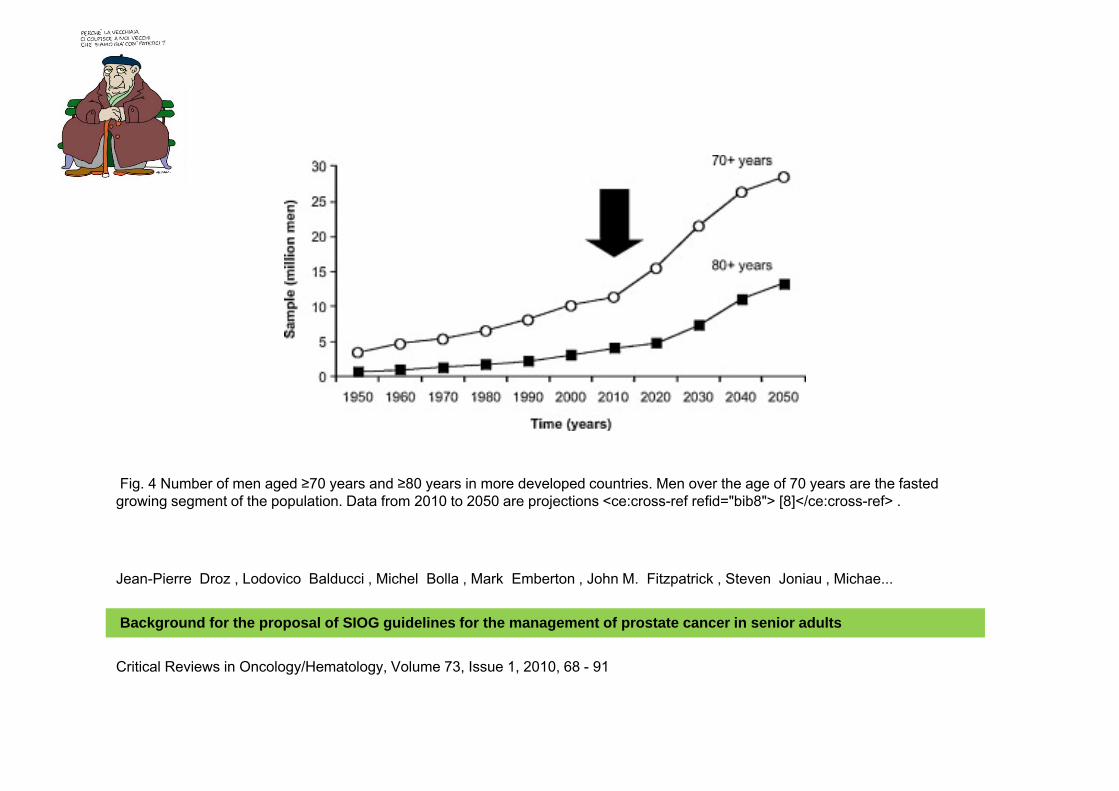
Fig. 4 Number of men aged ≥70 years and ≥80 years in more developed countries. Men over the age of 70 years are the fasted growing segment of the population. Data from 2010 to 2050 are projections <ce:cross-ref refid="bib8"> [8]</ce:cross-ref> .
Jean-Pierre Droz , Lodovico Balducci , Michel Bolla , Mark Emberton , John M. Fitzpatrick , Steven Joniau , Michae...
Background for the proposal of SIOG guidelines for the management of prostate cancer in senior adults
Critical Reviews in Oncology/Hematology, Volume 73, Issue 1, 2010, 68 - 91
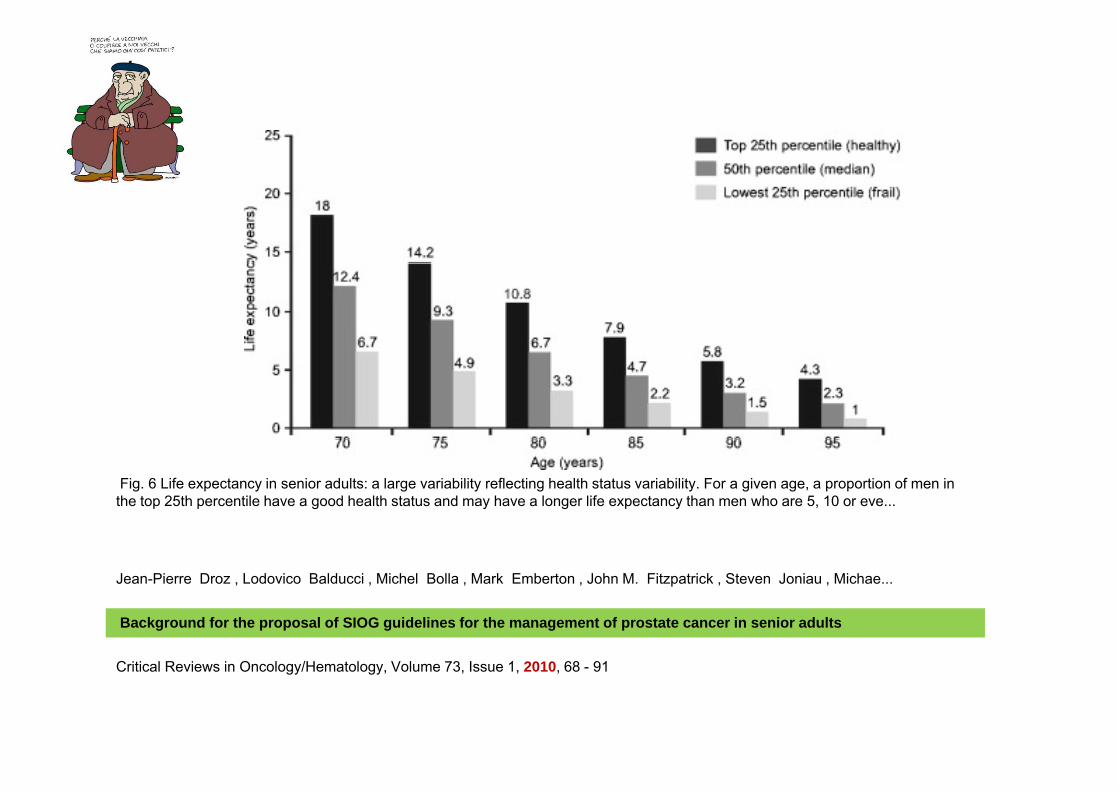
Fig. 6 Life expectancy in senior adults: a large variability reflecting health status variability. For a given age, a proportion of men in the top 25th percentile have a good health status and may have a longer life expectancy than men who are 5, 10 or eve...
Jean-Pierre Droz , Lodovico Balducci , Michel Bolla , Mark Emberton , John M. Fitzpatrick , Steven Joniau , Michae...
Background for the proposal of SIOG guidelines for the management of prostate cancer in senior adults
Critical Reviews in Oncology/Hematology, Volume 73, Issue 1, 2010, 68 - 91
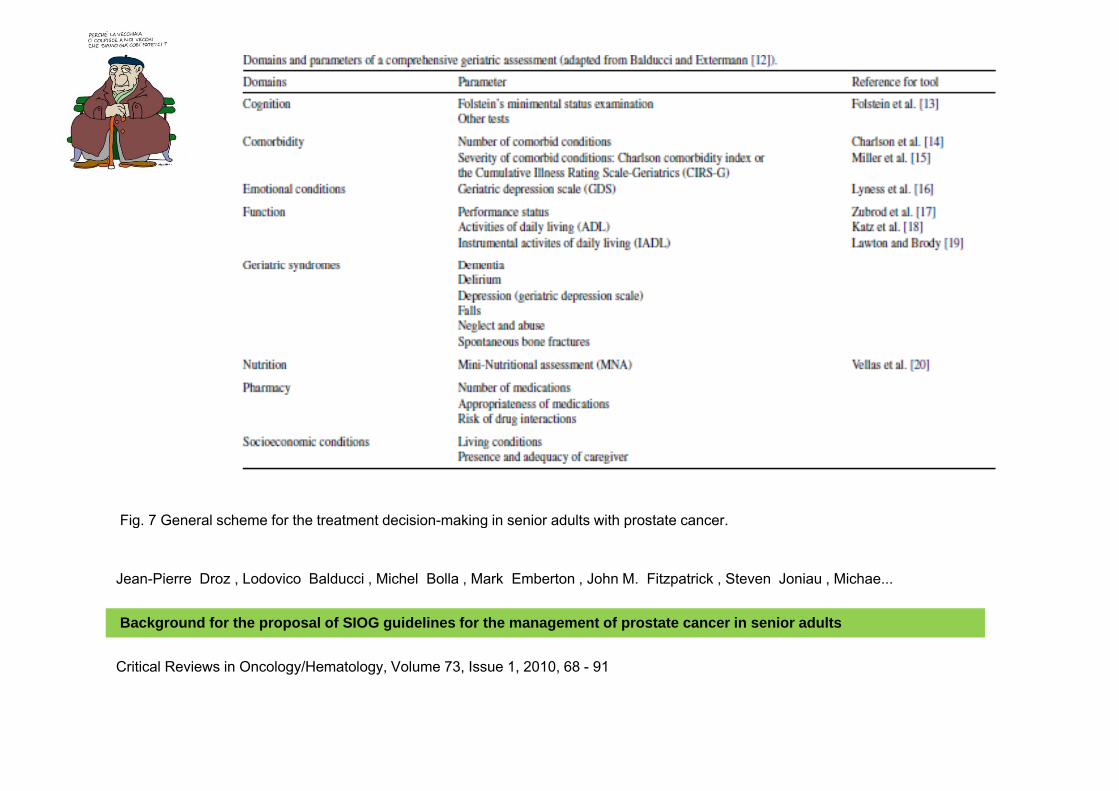
Fig. 7 General scheme for the treatment decision-making in senior adults with prostate cancer.g g p
Jean-Pierre Droz , Lodovico Balducci , Michel Bolla , Mark Emberton , John M. Fitzpatrick , Steven Joniau , Michae...
Background for the proposal of SIOG guidelines for the management of prostate cancer in senior adults
Critical Reviews in Oncology/Hematology, Volume 73, Issue 1, 2010, 68 - 91
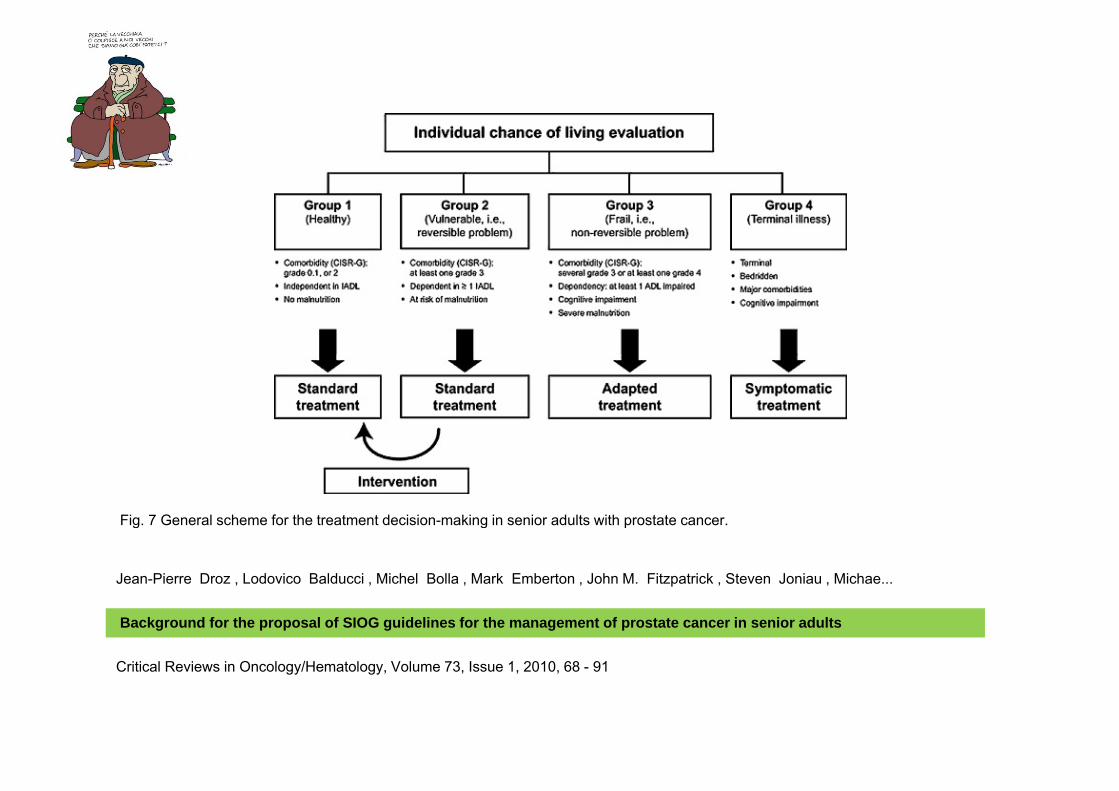
Fig. 7 General scheme for the treatment decision-making in senior adults with prostate cancer.g g p
Jean-Pierre Droz , Lodovico Balducci , Michel Bolla , Mark Emberton , John M. Fitzpatrick , Steven Joniau , Michae...
Background for the proposal of SIOG guidelines for the management of prostate cancer in senior adults
Critical Reviews in Oncology/Hematology, Volume 73, Issue 1, 2010, 68 - 91
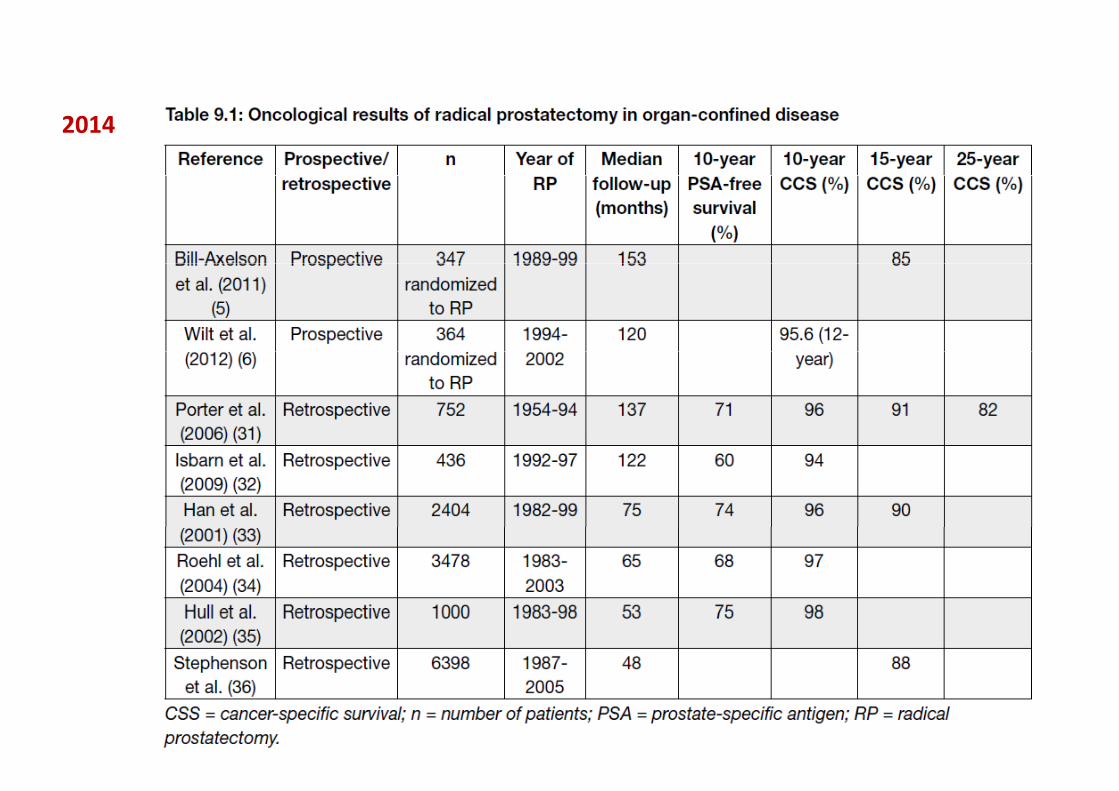
2014
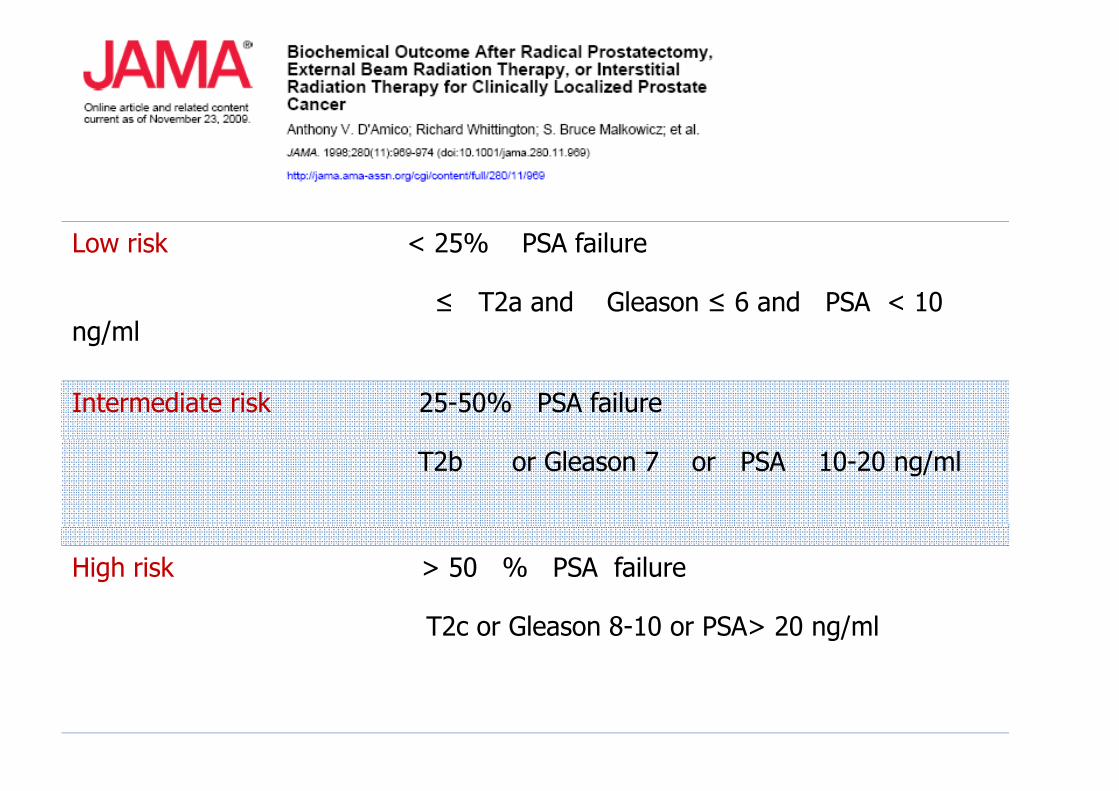
Low risk < 25% PSA failure
≤ T2a and Gleason ≤ 6 and PSA < 10 ng/ml
Intermediate risk 25-50% PSA failure
T2b or Gleason 7 or PSA 10-20 ng/ml
High risk > 50 % PSA failure
T2c or Gleason 8-10 or PSA> 20 ng/ml
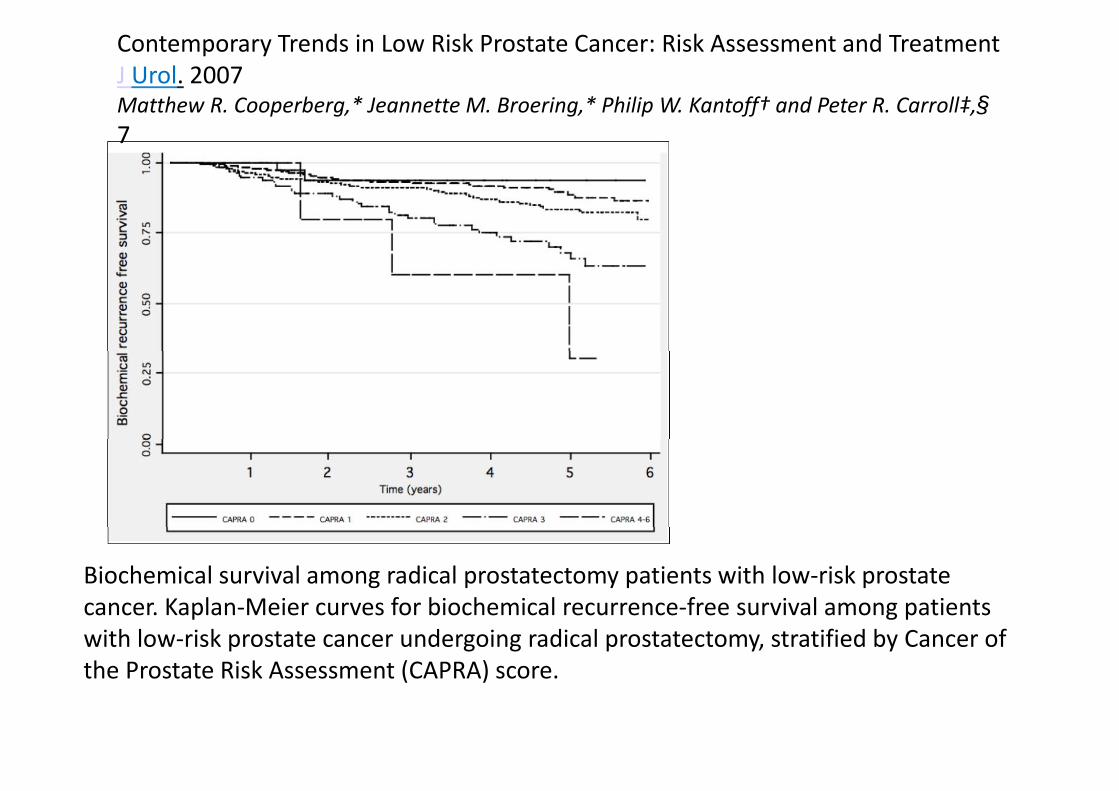
Contemporary Trends in Low Risk Prostate Cancer: Risk Assessment and TreatmentJ Urol. 2007Matthew R. Cooperberg,* Jeannette M. Broering,* Philip W. Kantoff† and Peter R. Carroll‡,§7
Biochemical survival among radical prostatectomy patients with low‐risk prostate cancer. Kaplan‐Meier curves for biochemical recurrence‐free survival among patientscancer. Kaplan Meier curves for biochemical recurrence free survival among patients with low‐risk prostate cancer undergoing radical prostatectomy, stratified by Cancer of the Prostate Risk Assessment (CAPRA) score.
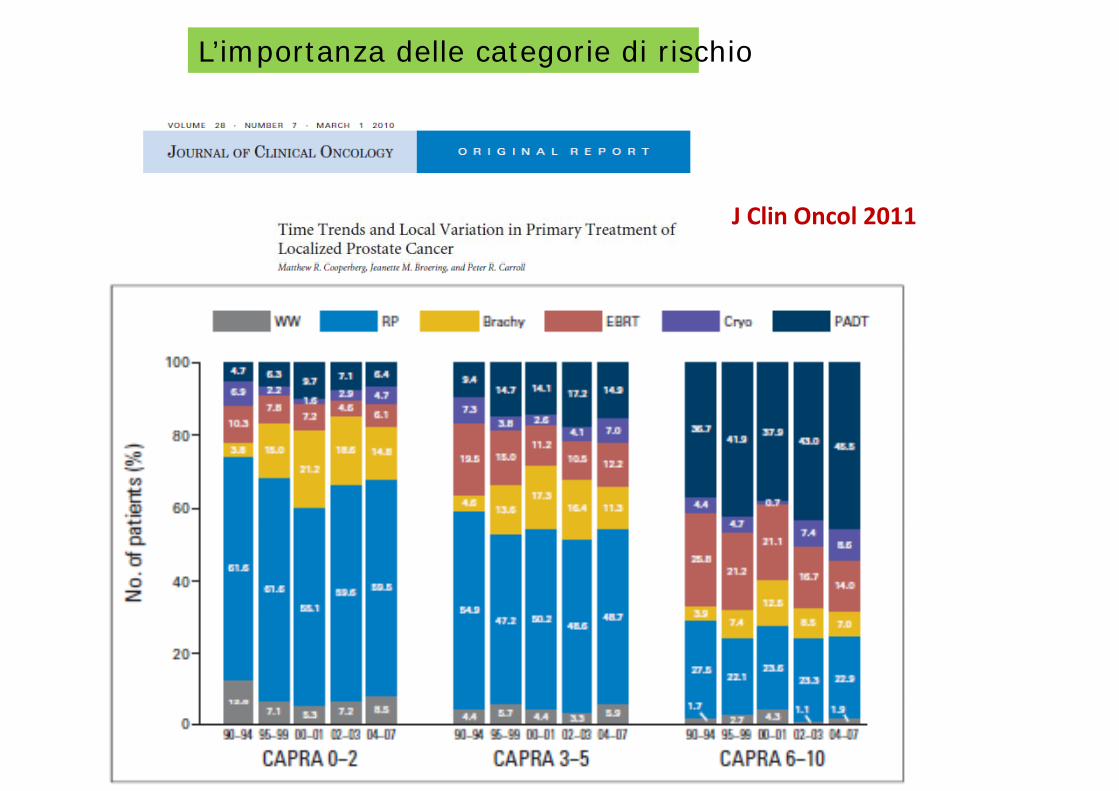
L’importanza delle categorie di rischio
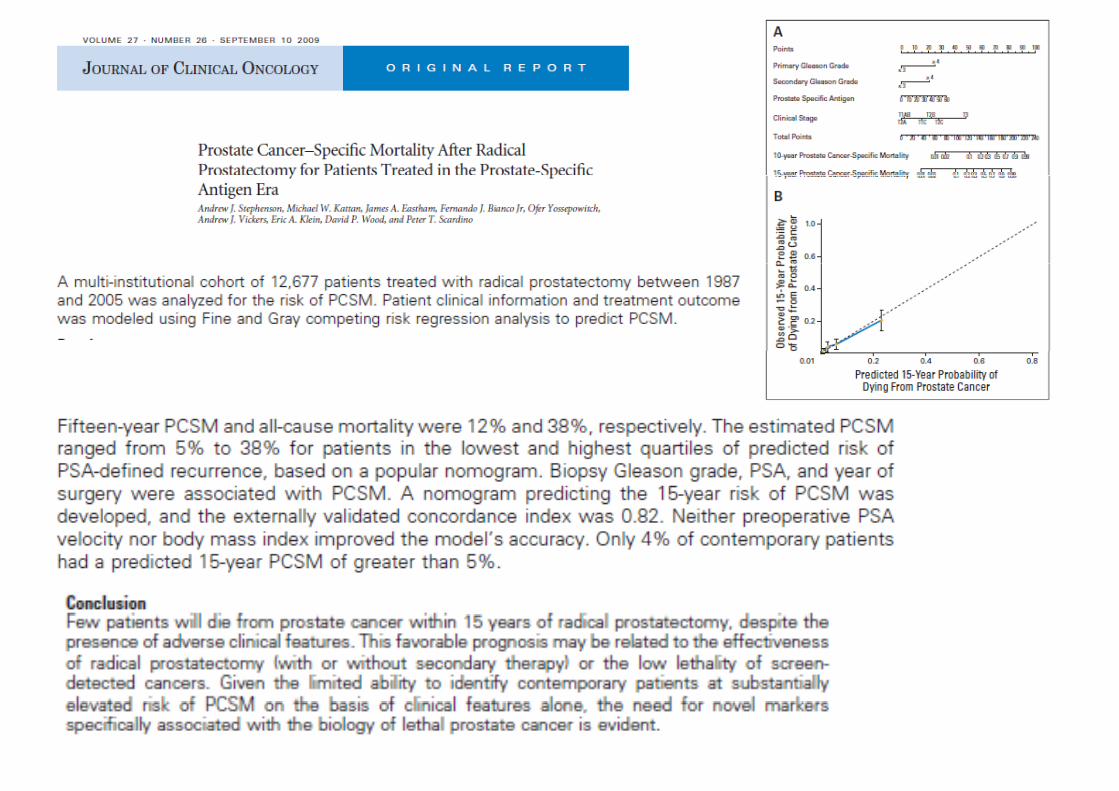
J Clin Oncol 2011
Click to edit the outline text format
Second Outline Level
− Third Outline Level
Fourth Outline LevelFourth Outline Level−Fifth Outline Level
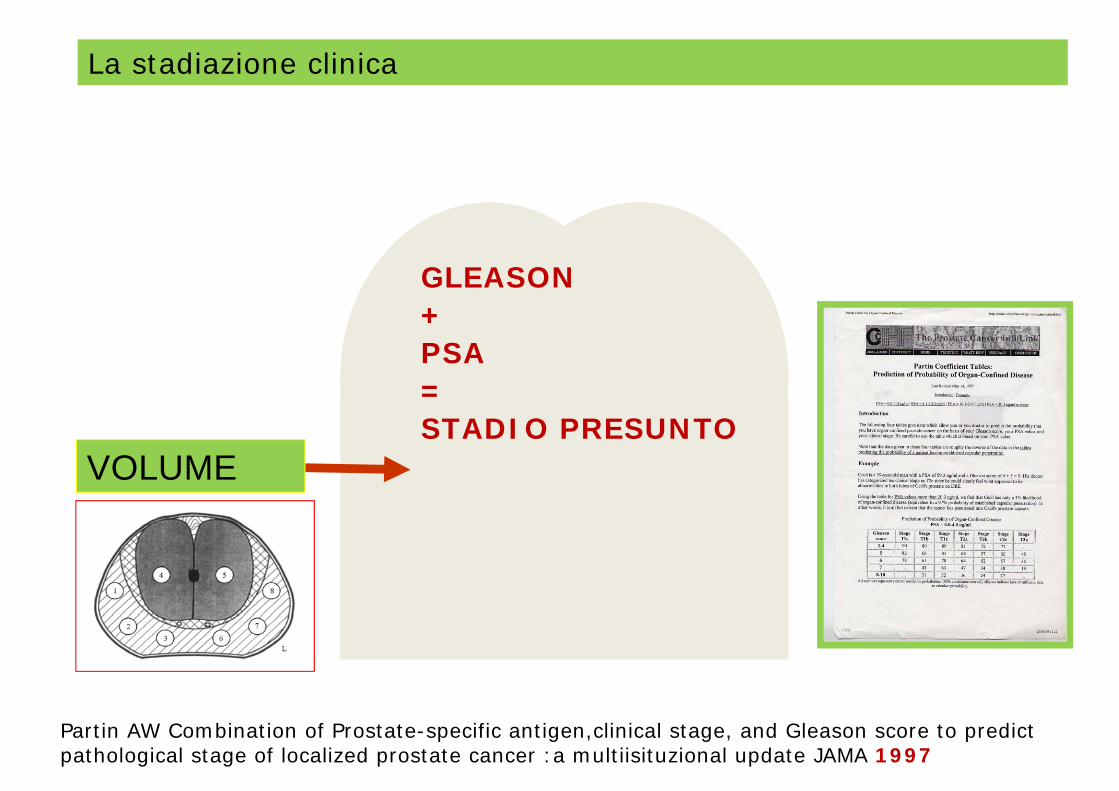
La stadiazione clinica
GLEASON+PSAPSA=STADIO PRESUNTO
VOLUME
Partin AW Combination of Prostate-specific antigen,clinical stage, and Gleason score to predict pathological stage of localized prostate cancer :a multiisituzional update JAMA 1997

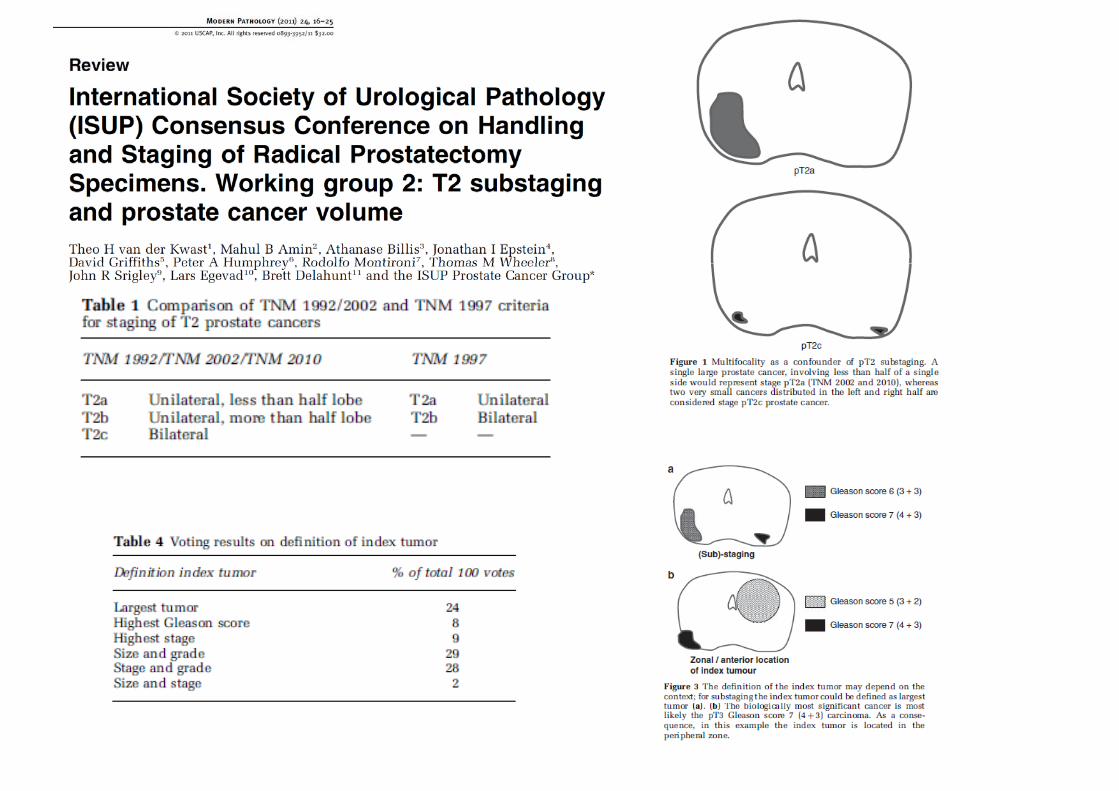
VOLUME DELLA NEOPLASIAVOLUME DELLA NEOPLASIA
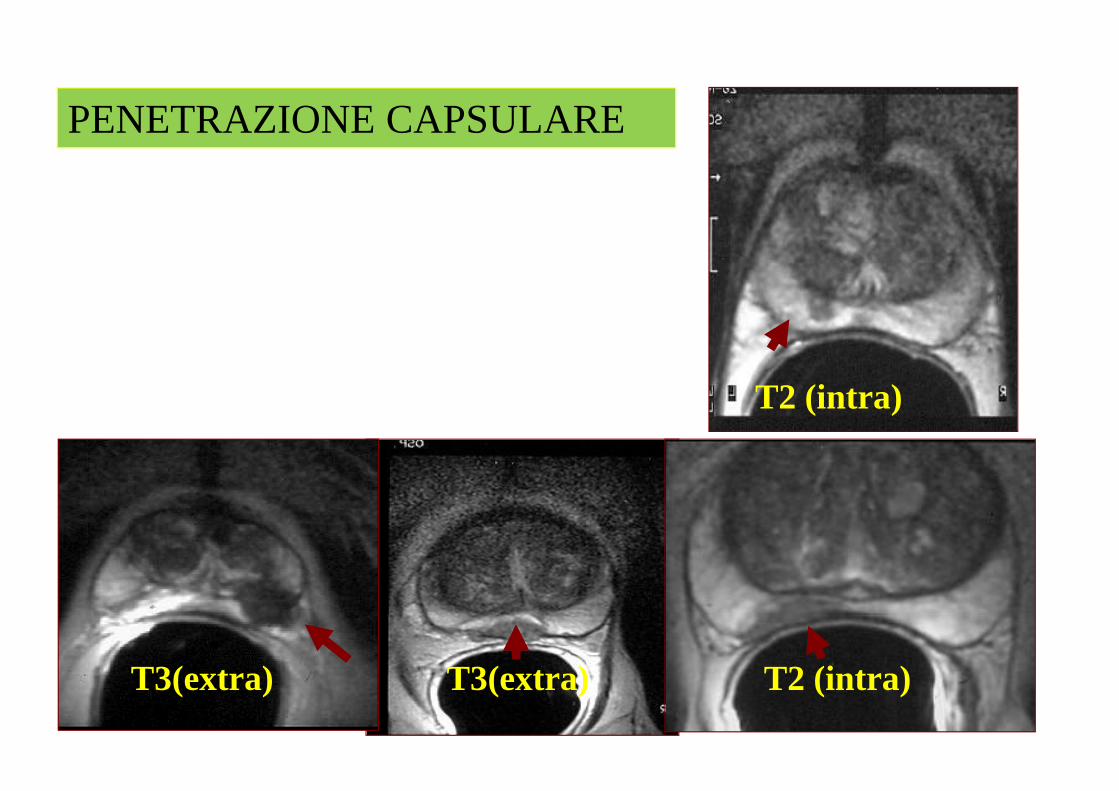
PENETRAZIONE CAPSULARE
T2 (intra)
T2 (intra)T3(extra) T3(extra)
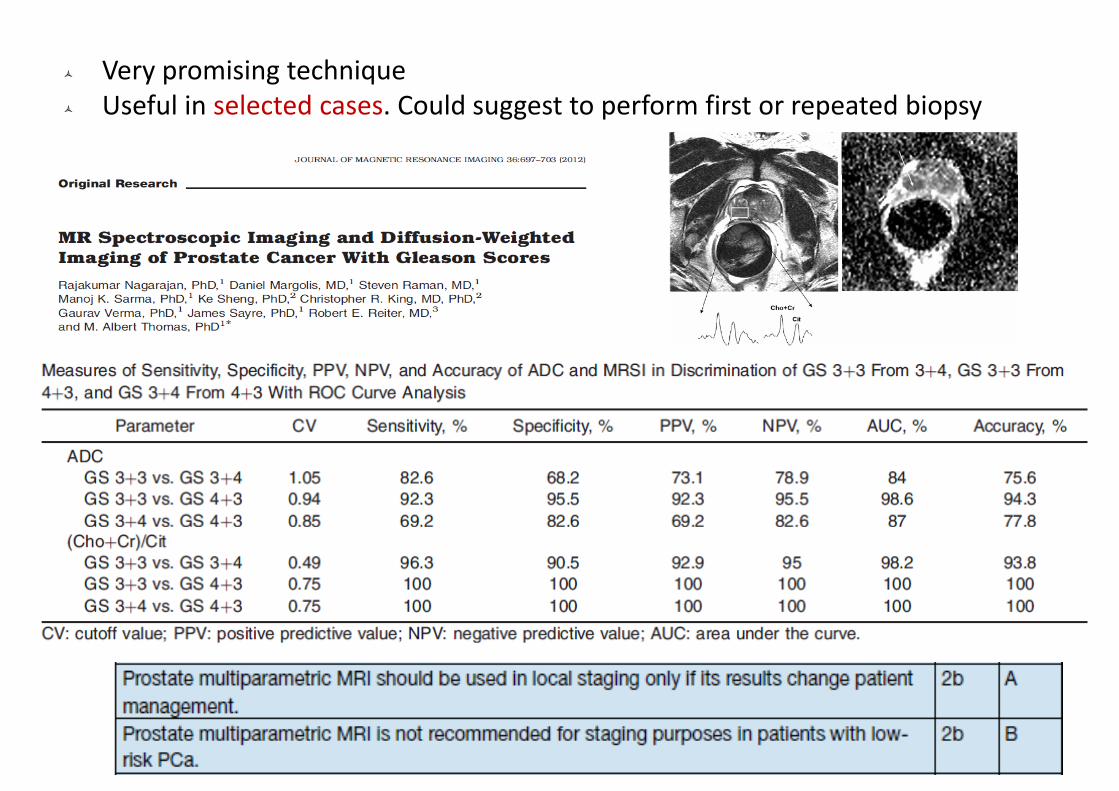
Very promising techniqueUseful in selected cases. Could suggest to perform first or repeated biopsy
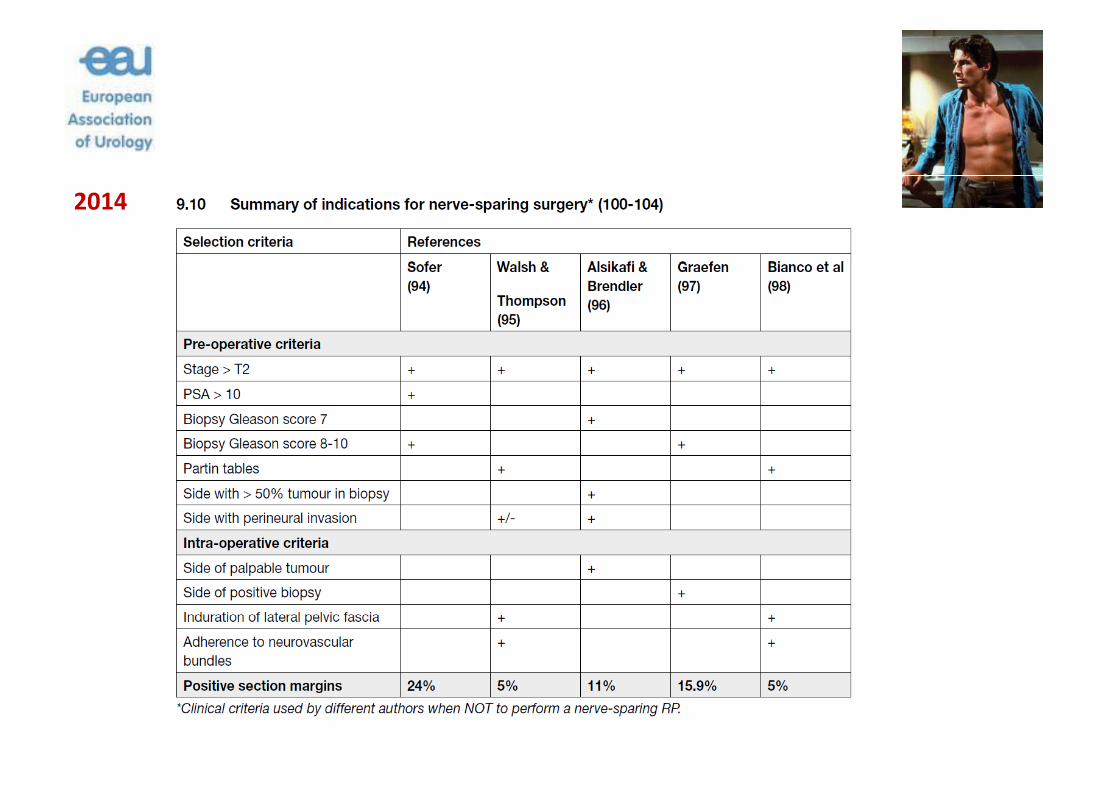
2014
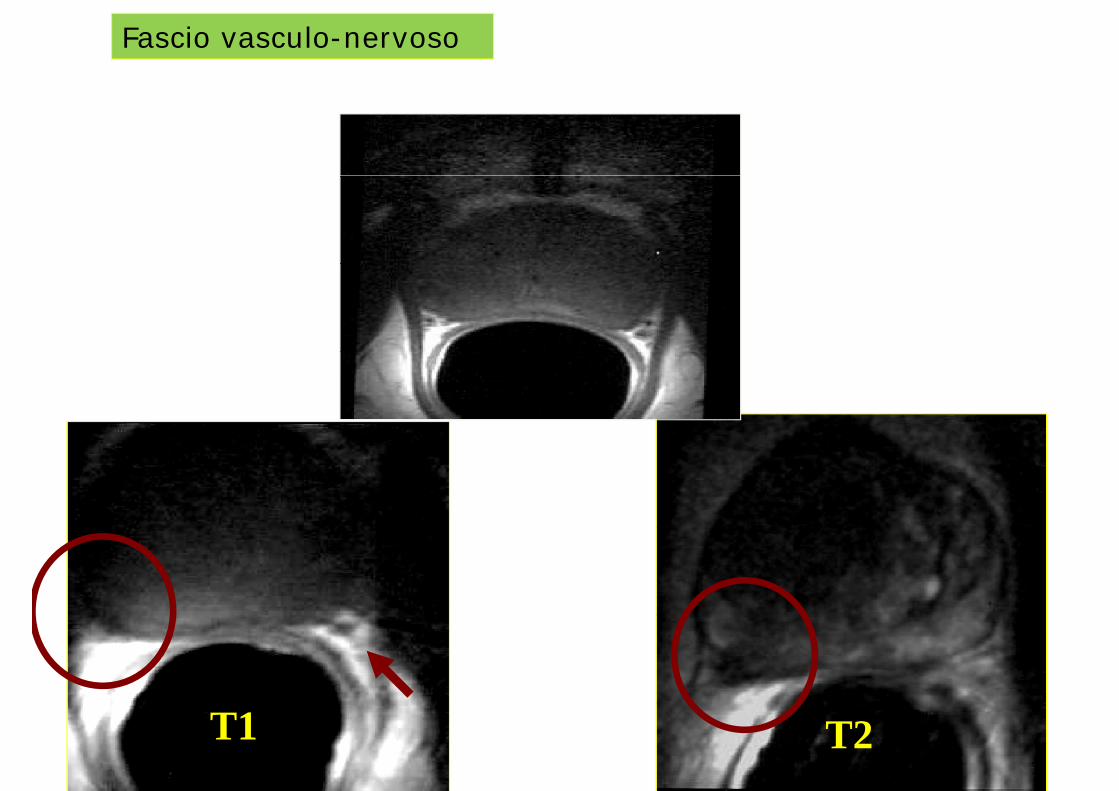
Fascio vasculo-nervoso
T1 T2
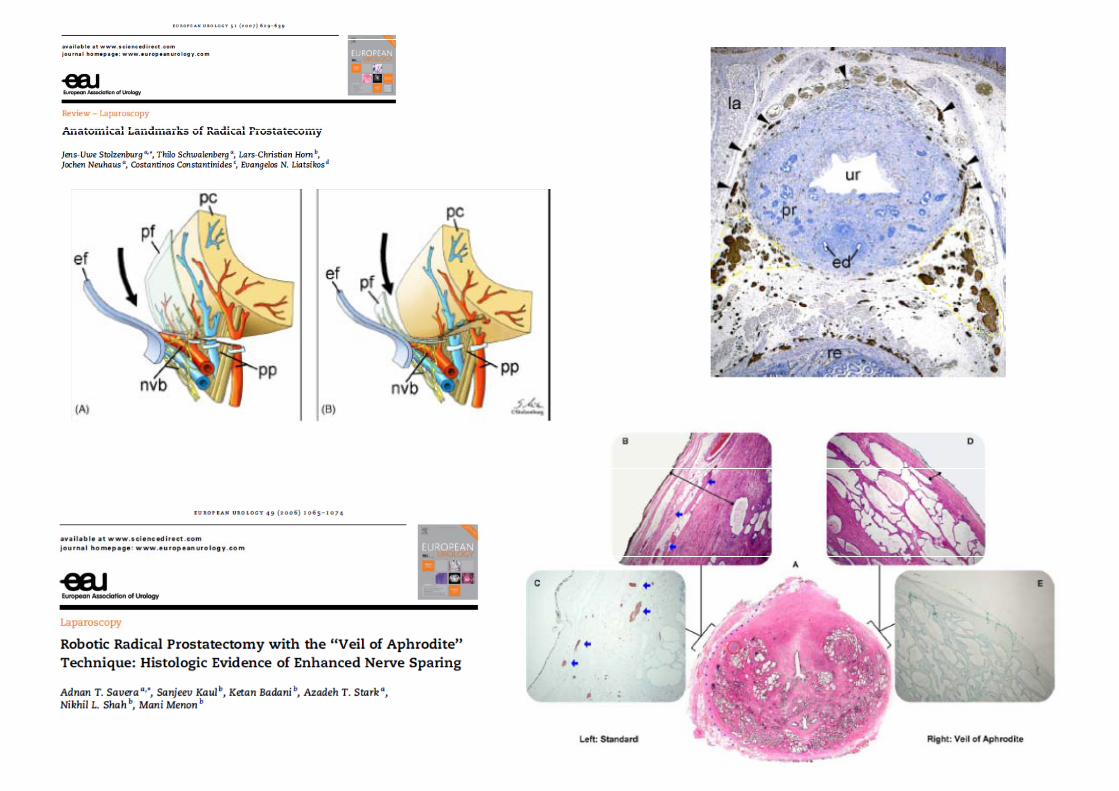
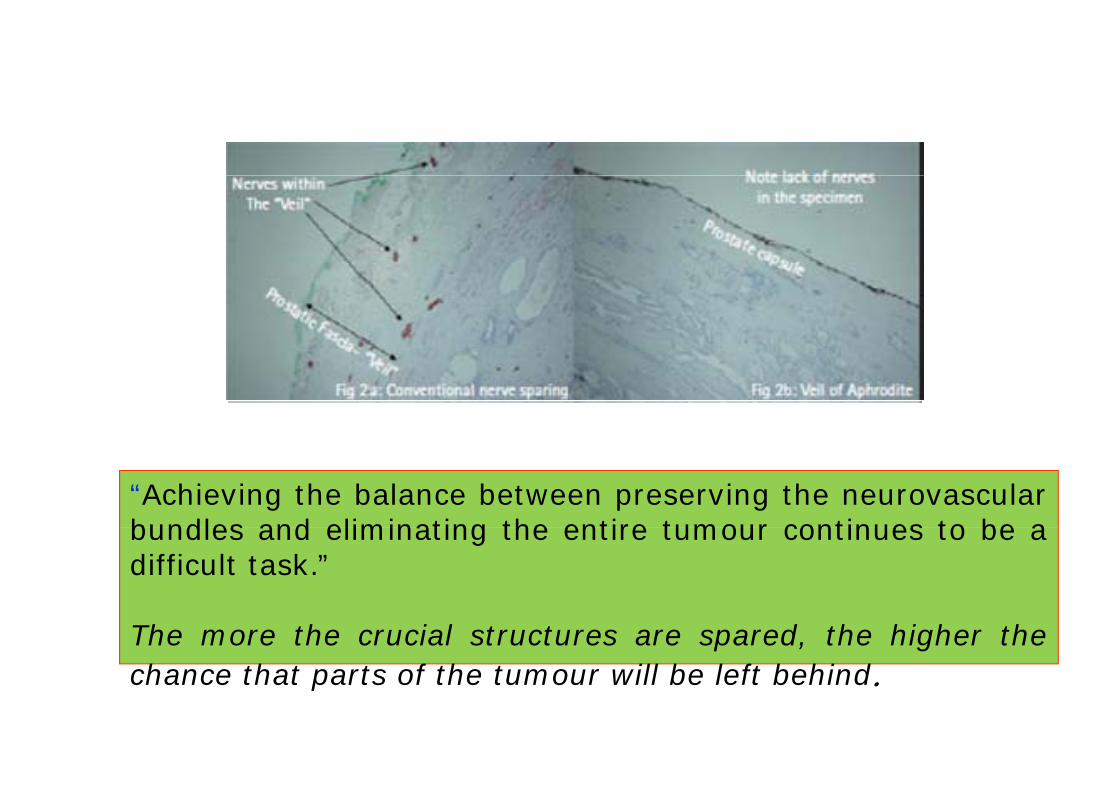
“Achieving the balance between preserving the neurovascularbundles and eliminating the entire tumour continues to be abundles and eliminating the entire tumour continues to be adifficult task.”
The more the crucial structures are spared, the higher thechance that parts of the tumour will be left behind.
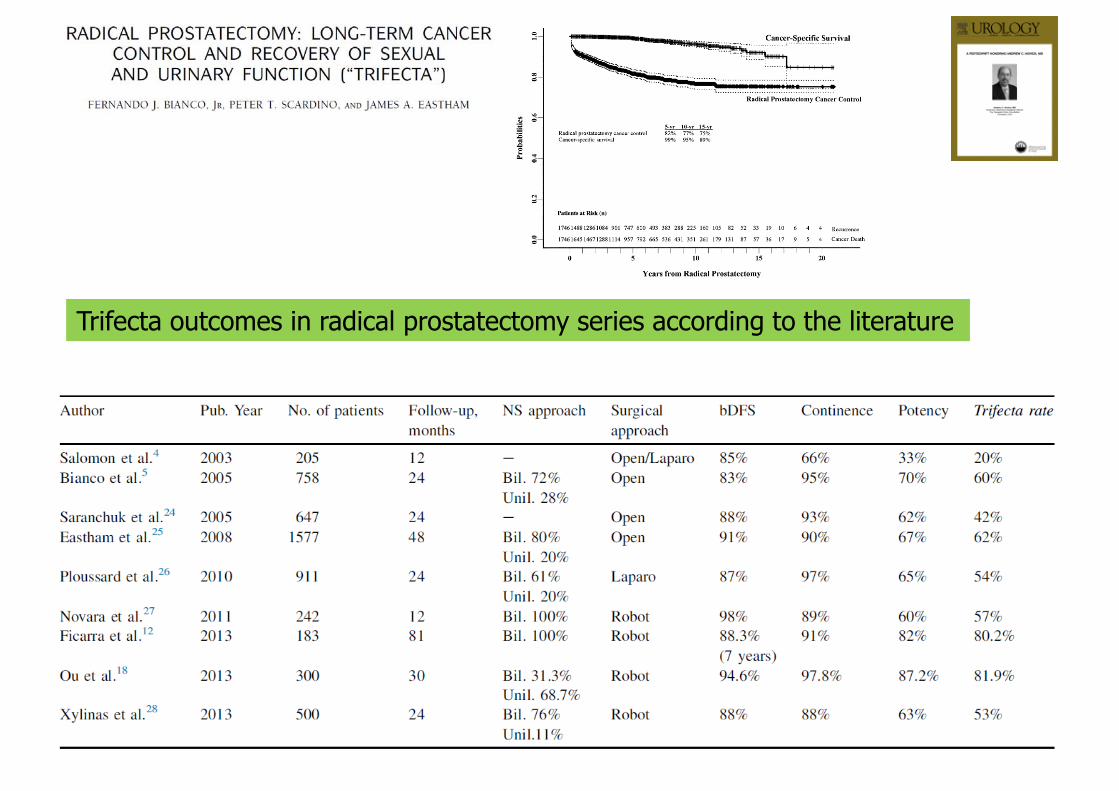
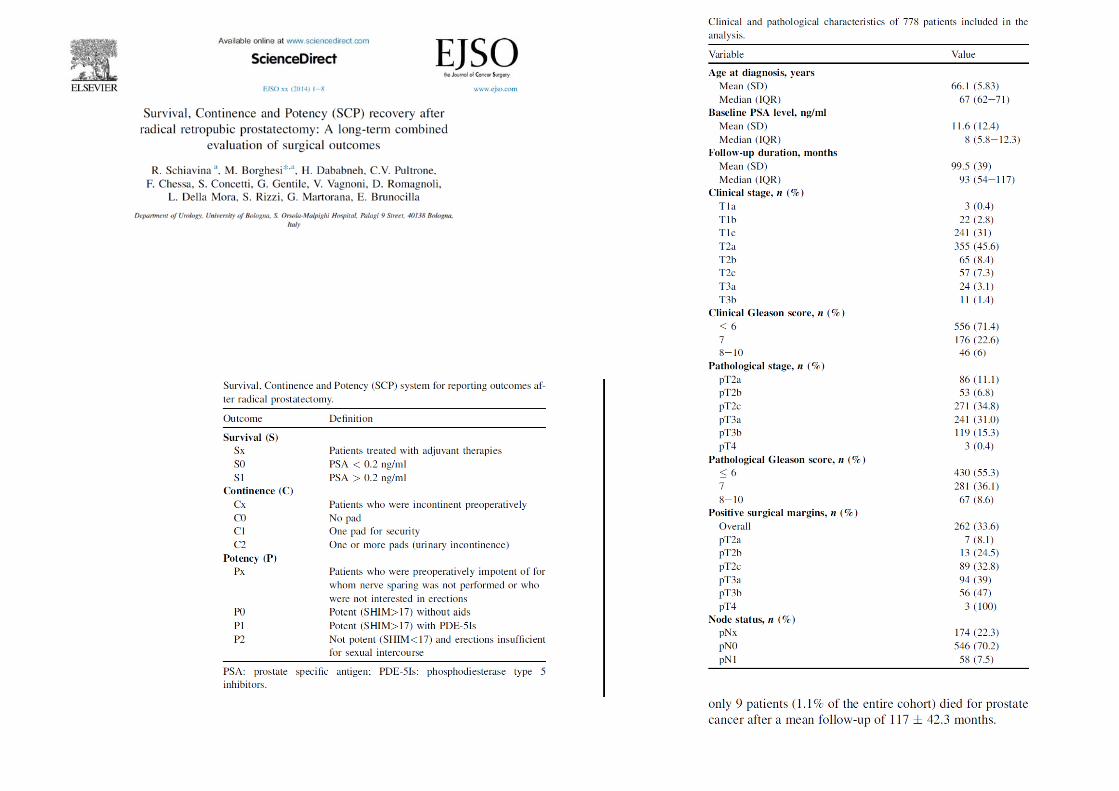
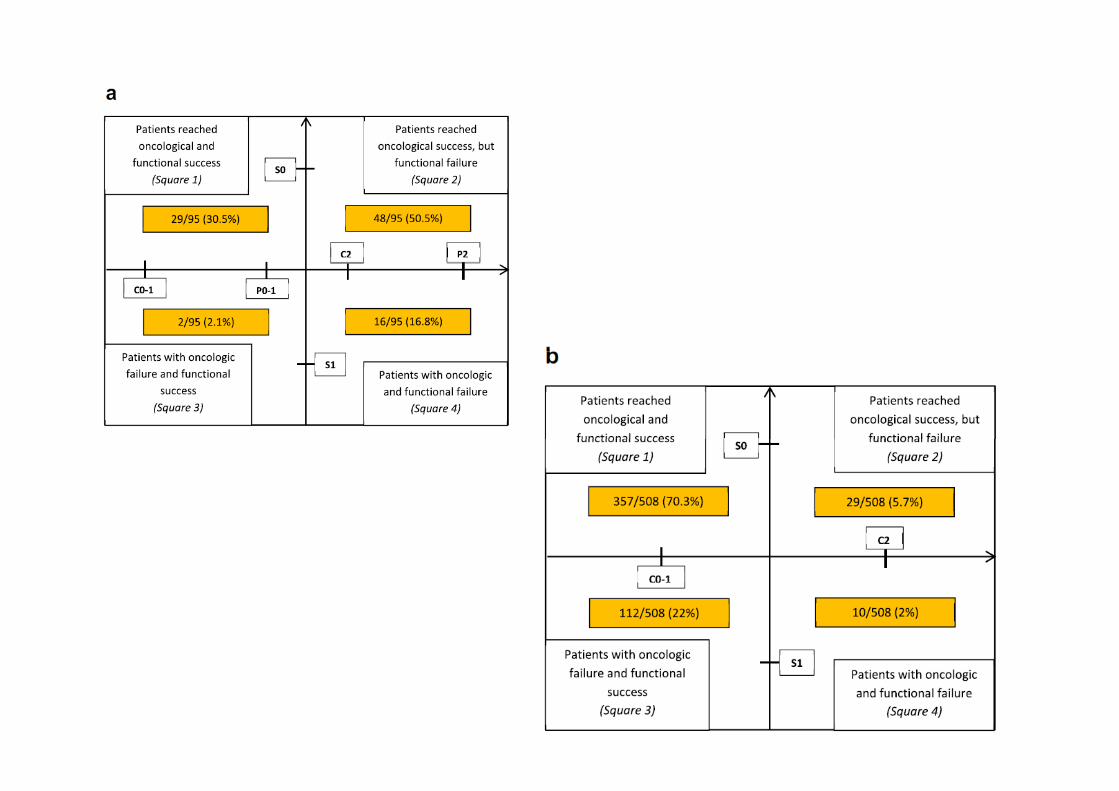
Trifecta outcomes in radical prostatectomy series according to the literature
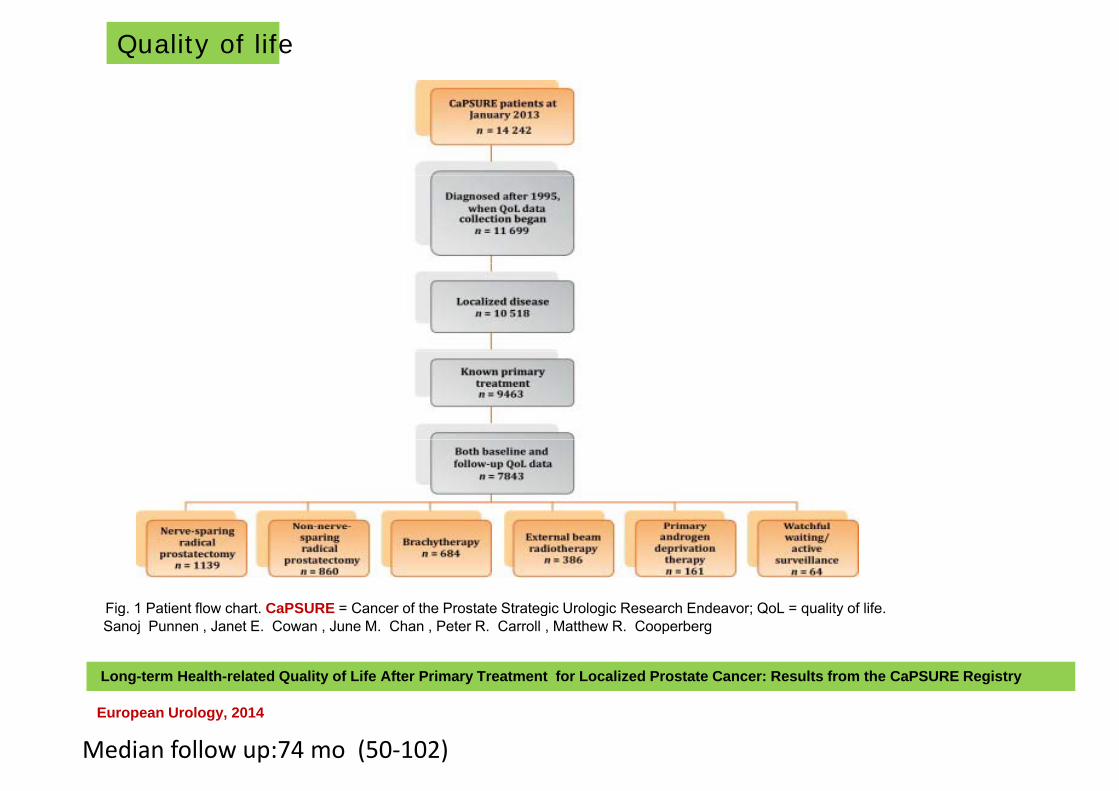
Quality of life
Fig. 1 Patient flow chart. CaPSURE = Cancer of the Prostate Strategic Urologic Research Endeavor; QoL = quality of life.g g g ; q ySanoj Punnen , Janet E. Cowan , June M. Chan , Peter R. Carroll , Matthew R. Cooperberg
Long-term Health-related Quality of Life After Primary Treatment for Localized Prostate Cancer: Results from the CaPSURE Registry
European Urology, 2014
Median follow up:74 mo (50‐102)

Adjusted mean summary scores for theAdjusted mean summary scores for the Medical Outcomes Studies 36-item Short Form (a) physical function and (b) mental health, and for the University of California, Los Angeles, Prostate Cancer Index (c) sexual function, (d) sexual bother, (e) urinary function (f) urinary bother (g) bowelfunction, (f) urinary bother, (g) bowel function, and (h) bowel bother are displayed over time by primary treatment type among 3294 men in the study cohort.
BT = brachytherapy; EBRT = external beam radiotherapy; NSRP = nerve-sparing
di l t t t N NSRPradicalprostatectomy;NonNSRP=non nerve sparing radical prostatectomy PADT = primary androgen deprivation therapy; PRE = before treatment; py; ;WW/AS = watchful waiting/active surveillance.
Sanoj Punnen , Janet E. Cowan , June M. Chan , Peter R. Carroll , Matthew R. Cooperberg Eur Urol 2014
Long-term Health-related Quality of Life After Primary Treatment for Localized Prostate Cancer: Results from the CaPSURE Registry
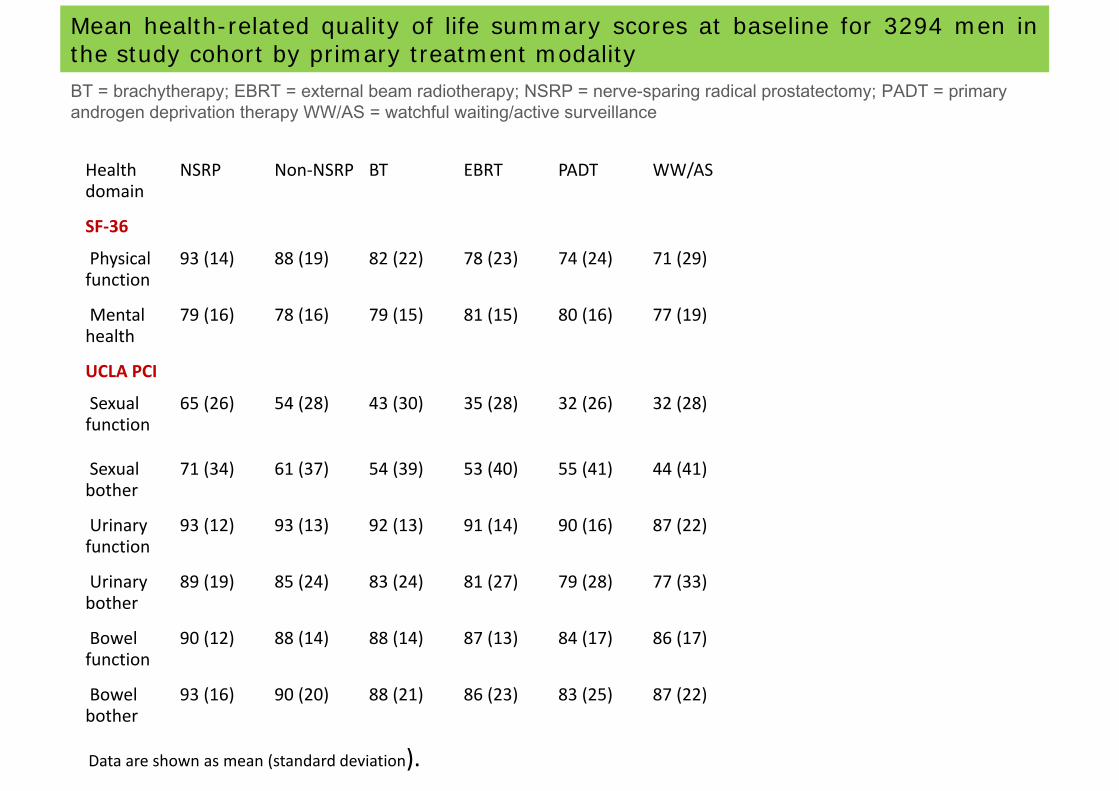
Mean health-related quality of life summary scores at baseline for 3294 men inthe study cohort by primary treatment modalityBT brach therap EBRT e ternal beam radiotherap NSRP ner e sparing radical prostatectom PADT primar
Health NSRP Non‐NSRP BT EBRT PADT WW/AS
BT = brachytherapy; EBRT = external beam radiotherapy; NSRP = nerve-sparing radical prostatectomy; PADT = primary androgen deprivation therapy WW/AS = watchful waiting/active surveillance
Health domain
NSRP Non NSRP BT EBRT PADT WW/AS
SF‐36
Physical 93 (14) 88 (19) 82 (22) 78 (23) 74 (24) 71 (29)Physical function
93 (14) 88 (19) 82 (22) 78 (23) 74 (24) 71 (29)
Mental health
79 (16) 78 (16) 79 (15) 81 (15) 80 (16) 77 (19)
UCLA PCI
Sexual function
65 (26) 54 (28) 43 (30) 35 (28) 32 (26) 32 (28)
Sexual bother
71 (34) 61 (37) 54 (39) 53 (40) 55 (41) 44 (41)
Urinary 93 (12) 93 (13) 92 (13) 91 (14) 90 (16) 87 (22)Urinary function
93 (12) 93 (13) 92 (13) 91 (14) 90 (16) 87 (22)
Urinary bother
89 (19) 85 (24) 83 (24) 81 (27) 79 (28) 77 (33)
Bowel function
90 (12) 88 (14) 88 (14) 87 (13) 84 (17) 86 (17)
Bowel 93 (16) 90 (20) 88 (21) 86 (23) 83 (25) 87 (22)bother
( ) ( ) ( ) ( ) ( ) ( )
Data are shown as mean (standard deviation).

2014
CHIRURGIA ROBOT-ASSISTED IN ITALIA
L’Italia è il secondo paese in Europa e il quarto nel mondo per numero di robot «Da Vinci» attualmente in uso:
1.U.S.A. (2000)Gi (138)2.Giappone (138)
3.Francia (69)Italia (64)4.Italia (64)
Oltre 9000 procedure robotiche eseguite in Italia nel 2013
POLO DI CHIRURGIA ROBOTICA
DELLA REGIONE TOSCANA
.1361 procedure a Settembre2014Dept Of Urology AOUC Careggi FlorenceDept. Of Urology, AOUC Careggi, Florence
12
8
10
6
4
2
0
POLO DI CHIRURGIA ROBOTICA
DELLA REGIONE TOSCANA
Stratificazione per tipo di intervento
Dept. Of Urology, AOUC Careggi, Florence
0 2 4 6 8 10 120 2 4 6 8 10 12
POLO DI CHIRURGIA ROBOTICA
DELLA REGIONE TOSCANA
Vantaggi dell’impiego del sistema robotico monodisciplinare in struttura con alto volume operatorio
• Rapida acquisizione di casistica adeguata
Riduzione della curva di apprendimento• Riduzione della curva di apprendimento
• Formazione rapida di una equipe
Miglioramento “outcomes”Miglioramento outcomes oncologici e funzionali e riduzione
dei costidei costi
POLO DI CHIRURGIA ROBOTICA
DELLA REGIONE TOSCANA
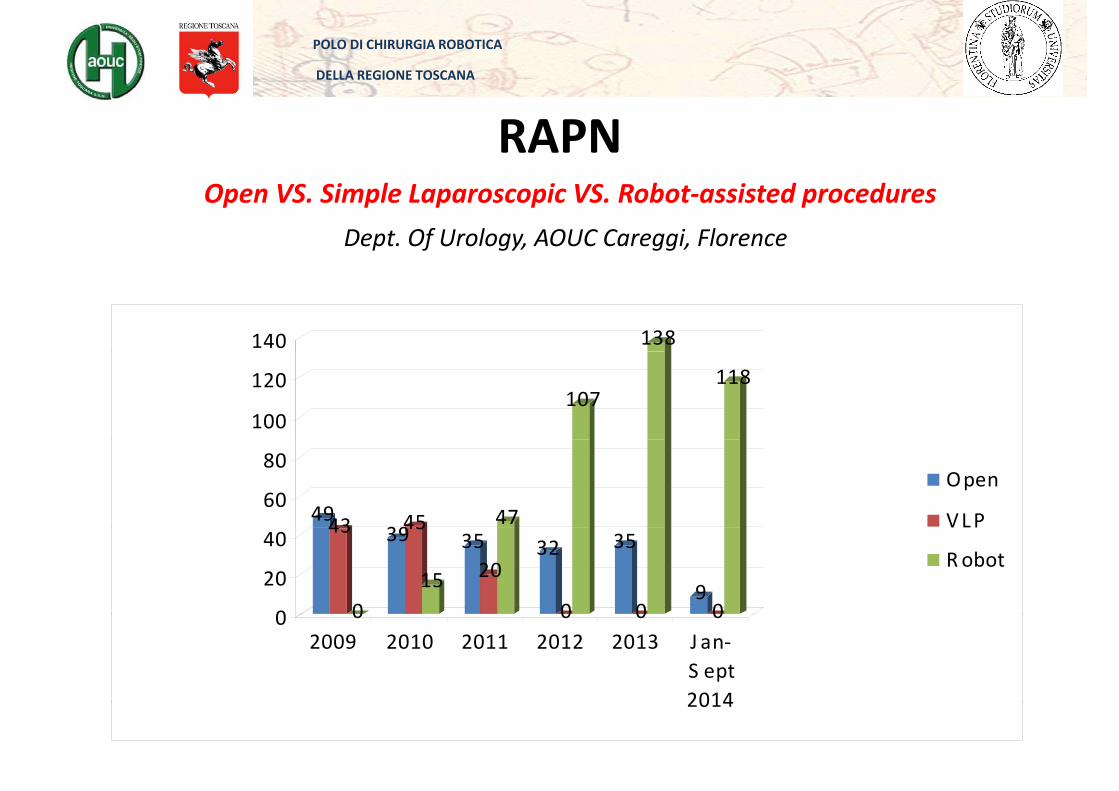
RAPN
Dept. Of Urology, AOUC Careggi, Florence
Open VS. Simple Laparoscopic VS. Robot‐assisted procedures
138140
107118
100
120
4943 394547
60
80Open
VLP43
0
3945
15
3520
32
0
35
0900
20
40VLP
Robot
0 0 0 002009 2010 2011 2012 2013 J an‐
S ept20142014
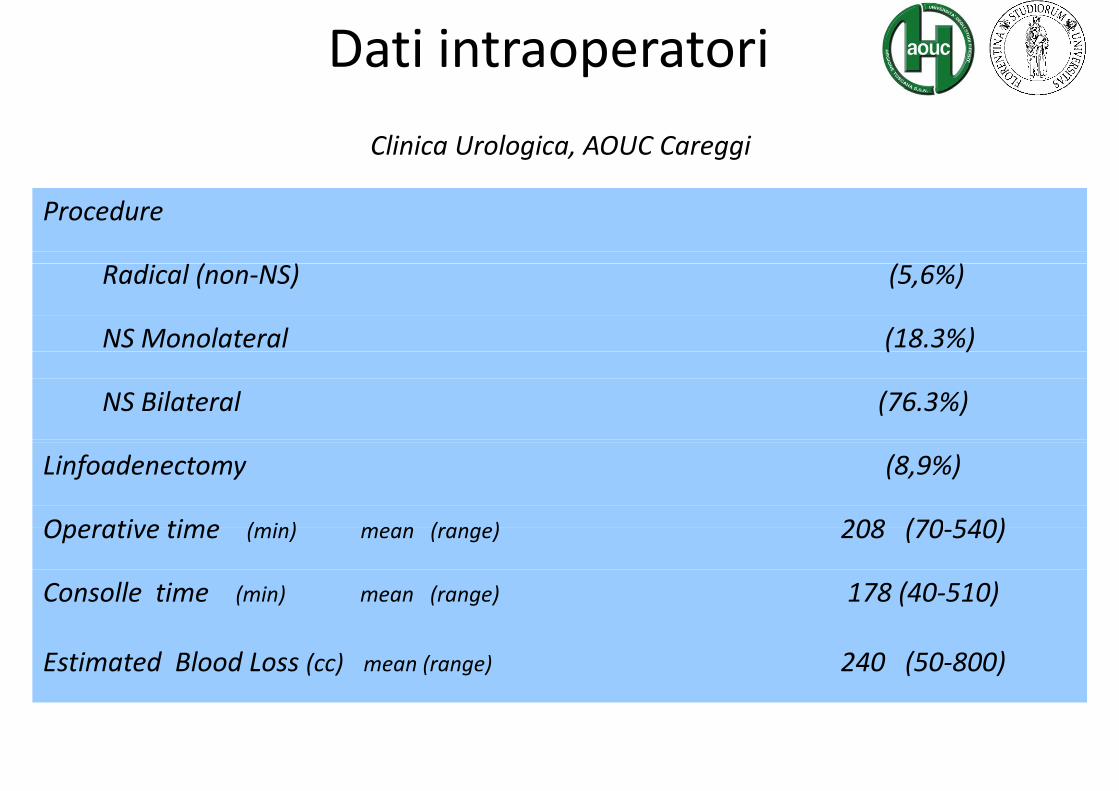
Dati intraoperatori
Clinica Urologica, AOUC Careggi
Procedure
( ) ( )Radical (non‐NS) (5,6%)
NS Monolateral (18.3%)( )
NS Bilateral (76.3%)
Linfoadenectomy (8,9%)
Operative time (min) mean (range) 208 (70 540)Operative time (min) mean (range) 208 (70‐540)
Consolle time (min) mean (range) 178 (40‐510)
Estimated Blood Loss (cc) mean (range) 240 (50‐800)
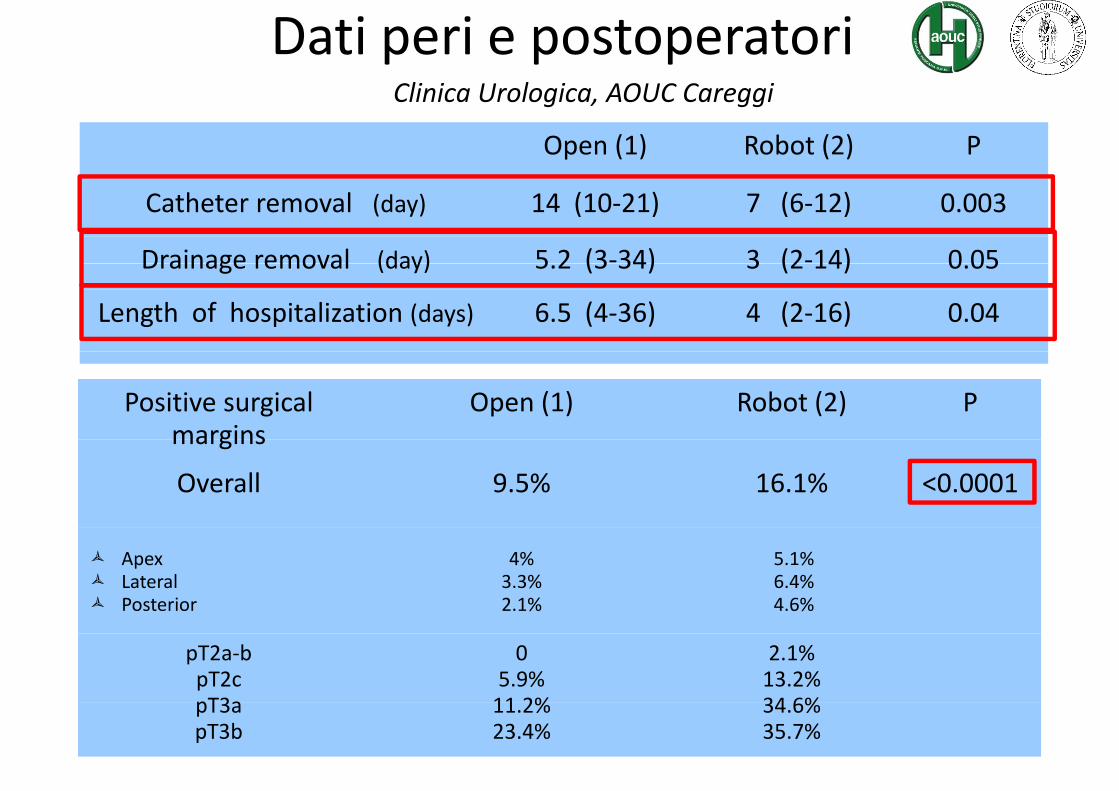
Dati peri e postoperatoriCli i U l i AOUC C i
Open (1) Robot (2) P
Clinica Urologica, AOUC Careggi
Catheter removal (day) 14 (10‐21) 7 (6‐12) 0.003
Drainage removal (day) 5 2 (3‐34) 3 (2‐14) 0 05Drainage removal (day) 5.2 (3 34) 3 (2 14) 0.05
Length of hospitalization (days) 6.5 (4‐36) 4 (2‐16) 0.04
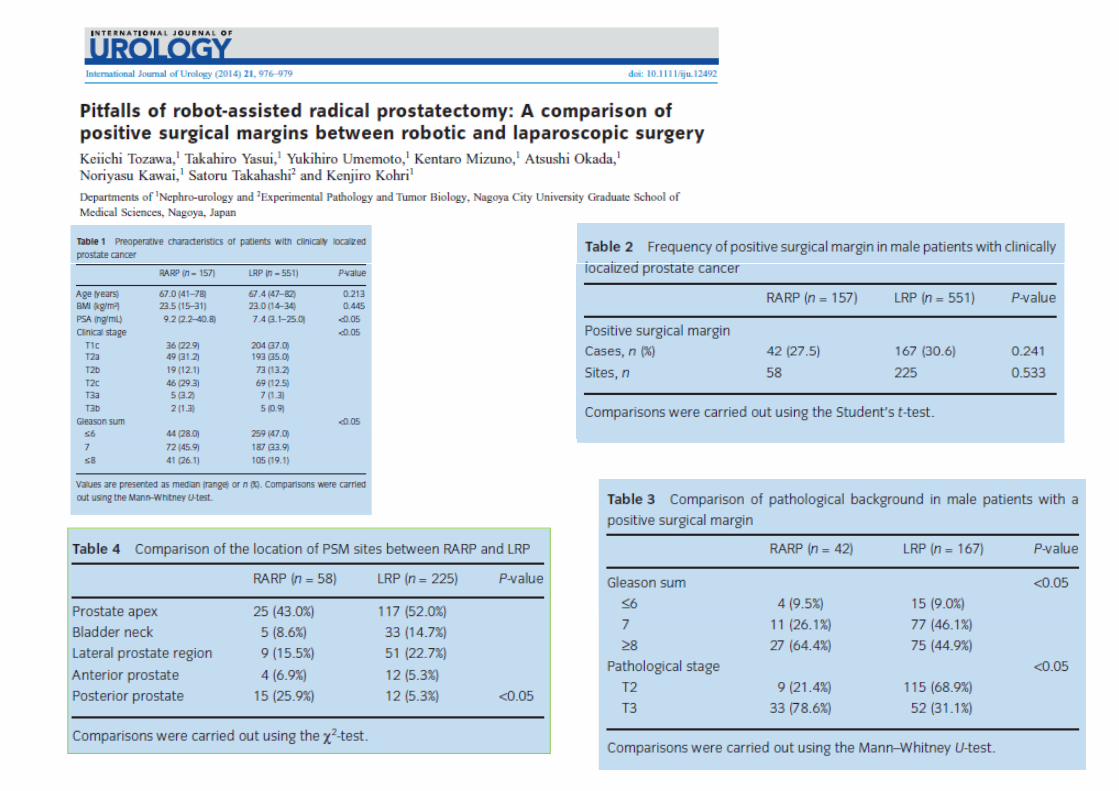
Positive surgical margins
Open (1) Robot (2) Pmargins
Overall 9.5% 16.1% <0.0001
ApexLateralPosterior
4%3.3%2.1%
5.1%6.4%4.6%
pT2a‐bpT2cpT3a
05.9%11 2%
2.1%13.2%34 6%pT3a
pT3b11.2%23.4%
34.6%35.7%
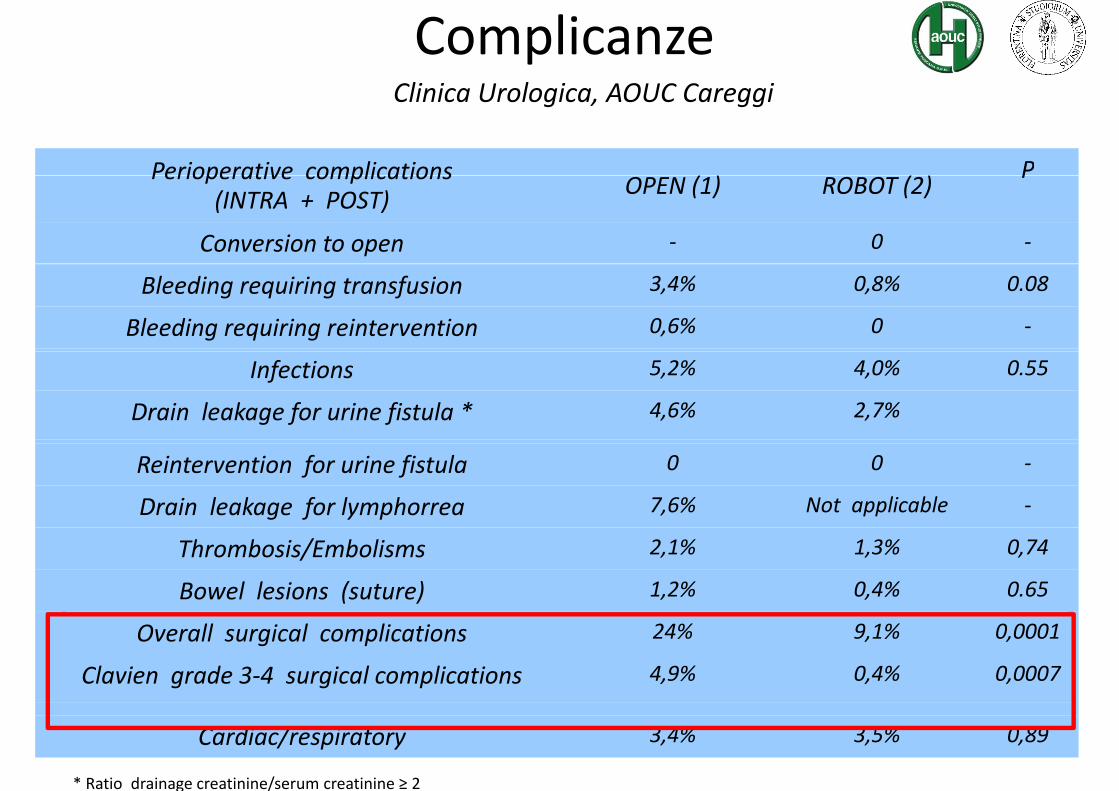
ComplicanzeCli i U l i AOUC C iClinica Urologica, AOUC Careggi
Perioperative complications ( ) ( )PPerioperative complications
(INTRA + POST) OPEN (1) ROBOT (2)P
Conversion to open ‐ 0 ‐
Bleeding requiring transfusion 3,4% 0,8% 0.08
Bleeding requiring reintervention 0,6% 0 ‐
Infections 5,2% 4,0% 0.55
Drain leakage for urine fistula * 4,6% 2,7%
Reintervention for urine fistula 0 0 ‐
Drain leakage for lymphorrea 7,6% Not applicable ‐
Thrombosis/Embolisms 2,1% 1,3% 0,74
Bowel lesions (suture) 1,2% 0,4% 0.65
Overall surgical complications 24% 9,1% 0,0001
Clavien grade 3‐4 surgical complications 4,9% 0,4% 0,0007
* Ratio drainage creatinine/serum creatinine ≥ 2
Cardiac/respiratory 3,4% 3,5% 0,89
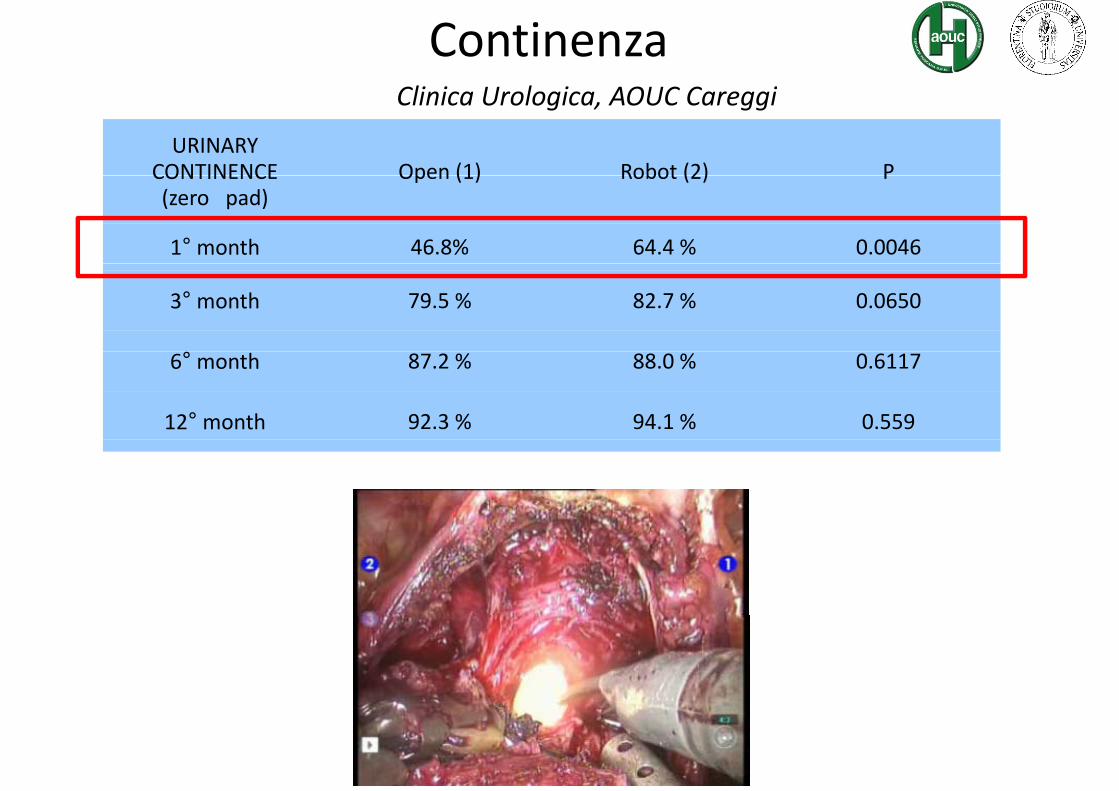
ContinenzaCli i U l i AOUC C i
URINARY CONTINENCE Open (1) Robot (2) P
Clinica Urologica, AOUC Careggi
CONTINENCE(zero pad)
Open (1) Robot (2) P
1° month 46.8% 64.4 % 0.0046
3° month 79.5 % 82.7 % 0.0650
6° month 87.2 % 88.0 % 0.6117
12° month 92.3 % 94.1 % 0.559
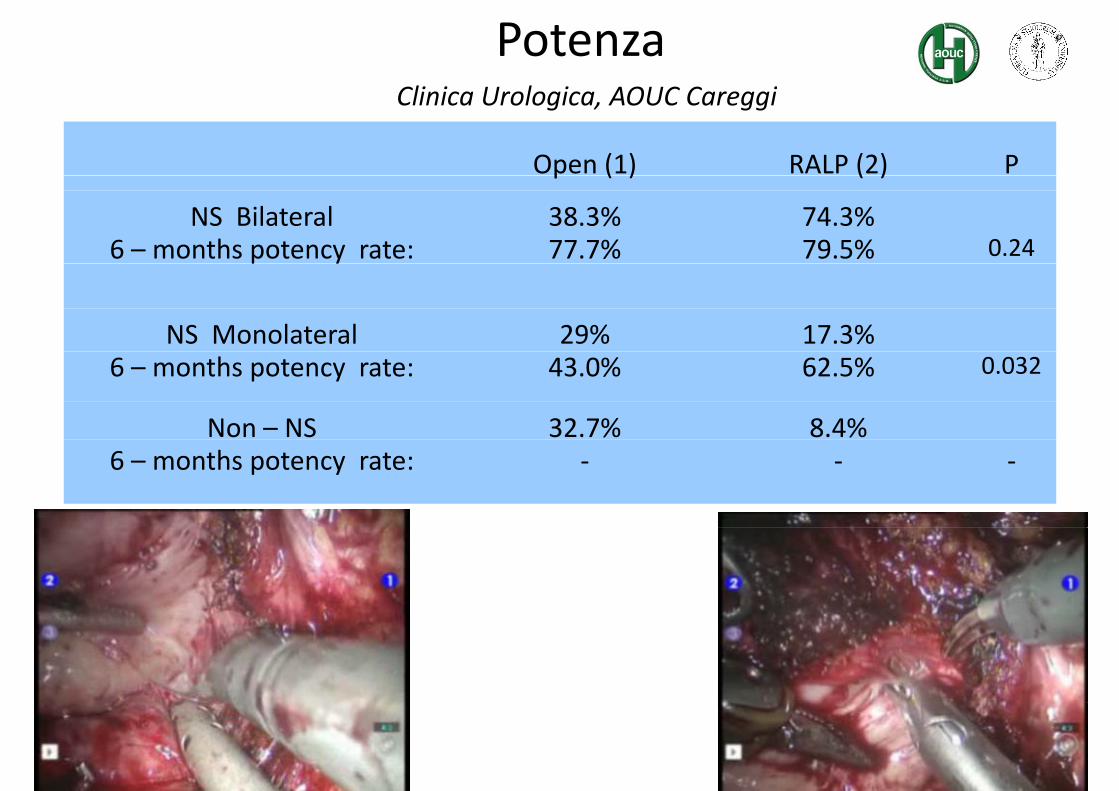
PotenzaCli i U l i AOUC C i
Open (1) RALP (2) P
Clinica Urologica, AOUC Careggi
p ( ) ( )
NS Bilateral6 – months potency rate:
38.3%77.7%
74.3%79.5% 0.24p y
NS Monolateral 29% 17.3%6 – months potency rate: 43.0% 62.5% 0.032
Non – NS 32.7% 8.4%6 – months potency rate: ‐ ‐ ‐

UTILIZZO DEL SISTEMA ROBOTICO «MONODISCIPLINARE»
ANOMALIA??ANOMALIA??