Embed Size (px)
Citation preview

Peripheral neuropathy marked by reduced nerve conduction velocities was found in four unrelated children, between the ages of 15 months and 9 years, whose autopsies revealed Leigh's subacute necrotizing encephalomyelopathy. Sural nerve biopsies disclosed primary demye- lination and remyelination, as well as loss of myelinated and unmy- elinated axons. The use of morphometric and electron microscopic studies shows that these techniques may reveal peripheral neuropathy in Leigh's disease more often than light microscopic methods alone.
MUSCLE & NERVE 9~165-173 1986
SURAL NERVE BIOPSY STUDIES IN LEIGH'S SUBACUTE NECROTIZING ENCEPHALOMYELOPATHY
HANS H. GOEBEL, MD, AlTILA BARDOSI, MD, REINHARD L. FRIEDE, MD, ALFRIED KOHLSCHUlTER, MD, MICHAEL ALBANI, MD, and HARTMUT SIEMES, MD
F o r many years after Leigh" reported subacute necrotizing encephalomyelopathy in a 7-month- old boy, interest in this disease focused on the clini- cal and morphological aspects of the central ner- vous system. Biochemical s t ~ d i e s ~ , ~ ~ later enlarged the nosologic aspects of this disease. Recently, en- zyme deficiencies, such as those of cytochrome ox- idase," pyruvate decarboxylase' or pyruvate dehy- drogenase (PDH) complex5*' and pyruvate
From the Department of Neuropathology, University of Mainz, FRG (Dr. Goebel), the Department of Neuropathology, University of Gottingen, FRG (Drs. Bardosi and Friede), the Department of Pediatrics, University of Hamburg, FRG (Drs. Kohlschutter and Albani), and the Department of Pediatrics, University of Bochum, FRG (Dr. Siemes)
Acknowledgments: We are grateful to Dr. Rusing. Stadtkrankenhaus KassellFRG, for providing the brain of patient 1, to Dr. Klein, Department of Clinical Neuropathology, Zentralkrankenhaus Bremen-OstlFRG, for providing histologic preparations of the brain of patient 2, and to Profes- sor Colmant. Department of Neuropathology. University of Hamburg/ FRG, for conveying neuropathologic data of Leigh's disease in patient 4. We also appreciate the enzyme determinations of hepatic PDH complex in patient 3 by Dr. J. M. F. Trijebels, Department of Pediatrlcs, University of NijrnegenlNetherlands, and of cultured fibroblast cytochrome oxidase in patient 4 by Dr. Sengers, Department of Pediatrics, University of NijrnegeniNetherlands. We also thank Mrs. I . Warlo and Ms. R. Kosswig for the electron microscopic work and Mr. W. Meffert for the photographic preparation.
Address reprint requests to Dr. Goebel at the Department of Neuropathology, University of Mainz, Langenbeckstr. 1, D-6500 Mainz, FRG.
Received for publication April 12, 1985; revised manuscript accepted for publication July 26, 1985.
@ 1986 John Wiley &Sons, Inc. 01 48-639)(/0902/0165 $04 00
carboxylase" have been documented. Leigh's dis- ease is therefore a syndrome of separate entities, or a multisystem disorder not confined to the cen- tral nervous system, an observation that had previ- ously been emphasized by the demonstration of "ragged red fibers" in skeletal muscle in these cases.4 In view of these findings, it is not surprising that involvement of peripheral nerves has been oc- casionally documented ' electrophysio- logically20921 and morphologically6 (Table 1) .
T o our knowledge, no systematic ultrastruc- tural and morphometric studies of peripheral nerves in Leigh's disease have been recorded. We report such studies for sural nerve biopsies in four unrelated children in whom the diagnosis of Leigh's disease was verified at autopsy.
CASE REPORTS
Patient 1. This girl was born after an uneventful pregnancy. Birth and early development were nor- mal. Difficulties in walking and frequent falls de- veloped at 2 years of age, followed by bilateral ptosis, nystagmus, dysarthric speech, and tremor of her hands about 1 year later. She had dysplastic stigmata, including an antimongoloid slant, a low hairline, and hypertrichosis of her back. Nerve conduction velocities at the age of 3 years showed 37 and 41 mlsec for the peroneal nerves, 38 mlsec for the right peroneal nerve, 45 and 48 mlsec for the ulnar nerves, and 30 mlsec with a latency of 5.9 msec for the fibular nerve. No additional elec-
Neuropathy in Leigh 's Disease MUSCLE & NERVE February 1986 165

Table 1. Perinheral neurooathv in Leiah’s disease. -~
Agehex; Electro- Morphology: sporadic (s) Clinical physi- biopsy (bx), autopsy (ax), Diagnosis of
References No. familial (f) symptoms ology electron microscopy (EM) Leigh’s disease
Clayton et a1.2 1 2 yr, 7 molM; f 1 yr, 2 molF; f
Guazzi et aI.l3 1 3 rno1F; f Nam i ki22 1 15 yrlF; f?
2
ReyeZ4 1 2 3 4
1 yr, 4 molF; f? 3 yr, 4 mo1M; s 2 yr, 1 mo1M; s 2 yr, 3 molM; s
Robinson et 1 2 yr, 7 molM; s 1 yr, 3 molF; s 2
Kolkmann and V o l ~ k e ’ ~ 2 1 yr, 10 molM; f
Evans et a ~ . ~ 1 8yrlM; s Dunn and Dolman‘ 1 8 yr, 3 moIM; s
Moosa‘O 1 1 yr, 2 molM; s
Moosa” 1 1 yr, 2 rnolM; s (same patient as previous one) 3 yr, 6 mo1M; f 2
3 9 rnolM; f
Jellinger et al.’5 1 7 yr/M; s
Kohlschijtter et 1 10 moiF; f
Seitz et 1 8 w k f F s
This paper 1 2 yr1F; s
2 6 rno1F; s 3 6mo/M;f? 4 6moIM; s
0 0 0 0
0 0 0 0
0 +
0
+ + +
+
0 ?
?
+
0
0
0 0 0
29
0 0
0
+ +
.8 mlsec +
-t
0 0
ax: Sciatic n. ax: PNS; demyelination
ax: PNS; demyelination ax: PNS; demyelination ax: PNS; demyelination ax: Vagus n.; mild seg-
mental demyelination ax: PNS; normal bx: Sural n.; ax: PNS; focal
demyelination ax: Sciatic n.; demyelina-
tion
+ axonal degeneration
0 ax: PNS; demyelination,
bx, EM: Sural n.; myelin rernyel inat ion
breakdown +
Autopsy of sibling Autopsy of sibling Autopsy Autopsy
Autopsy Autopsy Autopsy Autopsy
Autopsy Autopsy
Autopsy
PDH deficiency Autopsy
Autopsy
Autopsy
+ +
0
0
0
+
+ + +
0 Clinical and biochem- 0 ical
Clinical and biochem- ical
ax: PNS; segmental demy- Autopsy
ax: PNS; diffuse and focal elination
dernyelination decarboxylase activity Autopsy; low pyruvate
(116) in cultured fibroblasts
ax: Sciatic n.; primary de- Autopsy
ax: Sural n.; loss of demy- Autopsy
bx: Sural n.; demyelination Autopsy bx: Sural n.; demyelination Autopsy bx: Sural n.; demyelination Autopsy
myel i nation
linated fibers
PNS, peripheral nervous system; M, maie; F, femaie
troneurographic data were available. These values were in the low normal range for her age. A sural nerve biopsy was obtained at the age of 3 years. Contact was lost with her and she died at the age of 9 years. Autopsy showed spongiform lesions in her brain stem and diencephalon with preservation of neurons, proliferation of capillaries, and astrocy- tosis compatible with Leigh’s disease.
Patient 2. This girl was the second child of healthy parents, the older sibling being normal. She devel-
oped normally after an uneventful pregnancy and delivery until the age of 6 months, when she started to vomit and to have feeding difficulties, muscle hypotonia, and sleepiness. At the age of 15 months, she developed respiratory distress, optic atrophy, motor retardation, and was found to have a reduced peroneal nerve conduction velocity of 27 mhec (normal 48 & 12 m/sec). No additional electroneurographic data were recorded. A sural nerve biopsy was taken at this time. She died at the age of 17 months. Autopsy showed gross sym-
166 Neuropathy in Leigh’s Disease MUSCLE & NERVE February 1986

metric necrotizing spongiform lesions in the putamina, dentate nuclei, and in the brain stem, which were histologically marked by rarefaction of the gray matter tissue, proliferation of capillaries, preservation of neurons, astrocytosis, and reduced numbers of oligodendrocytes, compatible with Leigh’s disease.
Patient 3. This Turkish boy’s parents were first cousins. Several children in both parental families had died in infancy of unknown causes. His deliv- ery and early development were normal until the age of 6 months, when muscle weakness and hy- potonia became apparent. He had bilateral ptosis, difficulties in swallowing and chewing, nystagmus, and tremor. Conduction velocities of the tibia1 and peroneal nerves were reduced to 20 and 27 m/sec, respectively, and the evoked muscle action poten- tials were reduced to 2 mV and 1.8 mV, respec- tively. No further electroneurographic data were recorded. He had elevated cerebrospinal fluid (CSF) protein, elevated serum alanine, pyruvate and lactate levels, and a partial deficiency of he- patic PDH (22.6 nmol/hr/mg protein; normal 68 %
9). A gastrocnemius muscle biopsy showed type 2 fiber atrophy and normal mitochondria by elec- tron microscopy. A sural nerve biopsy was ob- tained a few months before he died at the age of 3 years. His brain showed gross symmetric spon- giform lesions in the cerebral and cerebellar white matter, the substantia nigra, and the brain stem. These were histologically characterized by mul- tifocal loss of myelinated nerve fibers and astrocy- tosis in the white matter and sponginess of the neuropil, preservation of nerve cells, proliferation of capillaries and astrocytosis in the gray matter regions, compatible with Leigh’s disease.
Patient 4. This firstborn child had hemimelia. His parents were healthy and not related. Pregnancy, birth, and postnatal development were unremark- able except for mild muscle hypotonia associated with normal movements. He stopped gaining weight and growing when 6 months old and hy- potonia increased, followed by loss of deep tendon reflexes and feeding problems. Nerve conduction velocities of peroneal nerve were 24 m/sec at 12 months (normal 47 f 12 m/sec), and 29 m/sec at 18 months (normal 50 % 12 m/sec). He had consis- tent serum lactic acidosis and elevated alanine. Cultured fibroblasts revealed cytochrome oxidase deficiency (4.4 mU/mg protein, normal 23-43). He died at the age of 2 years. Autopsy revealed gross bilateral lesions in the cerebral white matter, the
basal ganglia and the brain stem. These were histo- logically characterized by spongiform necrosis of the neuropil, proliferation of capillaries, mac- rophages, and partial loss and partial preservation of neurons, and severe demyelination of the spinal posterior tracts, compatible with Leigh’s disease.
MATERIALS AND METHODS
Sural nerve biopsies of these four patients were immediately fixed in buffered glutaraldehyde for 3-4 hours, washed in the same buffer, and dehy- drated in increasing concentrations of ethanol. For light microsopy, 1 +m longitudinal and transverse sections were cut of plastic-embedded nerves and stained with toluidine blue and paraphenylene- diamine. For electron microscopy, ultrathin sec- tions were cut and stained with uranyl acetate and lead citrate. Morphometry was performed on elec- tron micrographs according to established pro- cedures.”
The entire transverse section of the sural nerve was examined with electron micrographs taken of every grid opening at a magnification of 3400 x , using a Zeiss EM10 electron microscope (Carl Zeiss, Inc., Thomwood, NY). The inner and outer surfaces of the sheaths were traced manually with a cursor and were measured using Kontron video- plan (Kontron Electronics, Inc., Redwood City, CA). The g-ratio (ratio axon diametedfiber diame- ter), based on the circular profile of the fibers and determined by axon circumference and sheath cir- cumference, was calculated by a special computer program specified by Friede and Beuche. lo Scatter diagrams showing the g-ratio versus circular axon diameter were printed for control nerves and nerves from children with Leigh’s disease. The un- myelinated fibers were counted, and the density of unmyelinated fibers/lOO sq +m area of nerve was calculated.
Light Microscopy Patient I . Only a single fascicle was available for
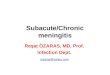
study, which revealed an even distribution of large and small myelinated fibers without evidence of myelin or axonal lesions. No onion bulb formation or macrophages were seen (Fig. la).
Patient 2. Several cross-sectioned fascicles con- tained almost evenly distributed small and large myelinated nerve fibers. Fibers of larger caliber of- ten showed rather thin myelin sheaths compared to their axon diameters. There was neither myelin nor axonal damage, nor onion bulb formation or macrophages (Fig. lb).
Patient 3 . Several fascicles contained large and
Neuropathy in Leigh’s Disease MUSCLE & NERVE February 1986 167

FIGURE 1. Semithin sections of sural nerve biopsies, 1 pm thick, stained with toluidine blue. (a) case 1, (b) case 2, (c) case 3, (d) case 4. Bars (a-d) = 100 pm.
small myelinated fibers evenly scattered through- out the nerve’s profile. Several large myelinated axons had rather thin myelin sheaths compared to the caliber of their axons. There was no myelin or axonal damage, nor onion bulb formation or mac- rophages (Fig. lc).
Patient 4. Several cross-sectioned fascicles con- tained large and small myelinated nerve fibers. Many large myelinated fibers had thin myelin sheaths when compared to their axon caliber. There was no damage of myelin or axoplasma, on- ion bulb formation, or macrophages (Fig. Id).
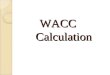
Morphometric Data. The scattergram of g-ratio of the 15-month-old child with Leigh’s disease [number of analyzed fibers (n) = 3511 did not dif-
fer from the control (n = 268) (Fig. 2, a and b), as the two populations of fibers found in normal adult sural nerves are not yet separable at this age. The possible occurrence of pathologic fibers may be concealed by the overlap of normal fiber populations.
In the other three children, aged 2-3 years, we observed a difference between the scattergrams of the control and the pathologic nerves (Fig. 2, c and d). The clear-cut separation of two fiber classes found in the controls (n = 1218) was lost in the pathologic nerves (case 1, n = 950; case 3, n = 430; case 4, n = 930) by a new population of fibers having a higher g-ratio and positioned between the two normal populations, suggesting the presence of regenerating or remyelinating fibers (see Dis-
168 Neuropathy in Leigh’s Disease MUSCLE & NERVE February 1986

b
8 Re0 3 0 0 0 h Baa 9 eee I2 UU 15 90 8 0 8 8 3 R O O 6 BBLl 9 00s I : 0 8 35 08
I 2aeL n e e RYOW DIRIElCL.CIRCULRC ::l *WON B l R i n E T E i . C I P C l i l R R . . ,
'
FIGURE 2. Scatter diagrams of sheath thickness. Sheath thickness is shown in terms of the g-ratio (ratio axon diametedfiber diameter) plotted for circular fiber profiles, based on circumference. (a) Fiber population of sural nerve of a 15-month-old child with Leigh's disease shows no differences in the g-ratio to those of the normal control (b). (c) Three children with Leigh's disease aged 2-3 years do not show the typical separation of fibers into the groups of fiber populations, in contrast to the controls (d). A new group of fibers (arrow), having higher than normal g-ratios (which means thinner than normal sheaths), may indicate regeneration or remyelination.
cussion). The mean g-ratio for the three patients was 0.82 ? 0.06 SD compared with 0.76 ? 0.06 for the controls.
Upon subjective assessment, there appeared to be a decrease in the density of nonmyelinated fibers, but the morphometric analysis of the con- trol and pathologic nerves showed no significant difference. The number of nonmyelinated fibers
in controls was 3.1/100 sq pm and in the pathologic nerves 2.5/100 km.
Electron Microscopy Patient 1. Ultrastructural changes consisted of
remnants (Fig. 3a) of degenerated single myelin- ated fibers, some Biingner's bands, and Schwann cell processes devoid of myelinated or nonmy-
FIGURE 3. Case 1. (a) Remnant of a myelinated axon. Bar = 1 pm. (b) A mitochondrion contains a paracrystalline inclusion. Bar = 0.1 pm.
Neuropathy in Leigh's Disease MUSCLE & NERVE February 1986 169

elinated axons. My elin ovoids were occasionally seen in the Schwann cell cytoplasm of myelinated nerve fibers. Rarely, a large process, apparently of axonal origin, contained glycogen and a few other unidentified structures surrounded by Schwann cell processes or a finely dense, granular matrix. Large mitochondria were sometimes seen, one of which had a paracrystalline inclusion (Fig. 3B). These subtle abnormalities pointed to a break- down of myelinated nerve fibers without evidence of unequivocal preceding demyelination.
Patient 2. Several myelinated fibers had rather thin myelin sheaths compared to their axon diame- ters. My elinated axons were occasionally encom- passed by Schwann cell processes, some of which contained nonmyelinated axons, representing an incipient onion bulb formation (Fig. 4). A few Bungner’s bands were present. Schwann cell pro- cesses devoid of myelinated or nonmyelinated ax- ons were also encountered, occasionally forming stacks surrounded by a common basal lamina. In other instances, basal lamina derived from Schwann cell surfaces formed multiple loops de- void of Schwann cell cytoplasm or axoplasm. Mitochondria often appeared in aggregates within Schwann cell processes or as rather large inclu- sions.
FIGURE 4. A myelinated axon is surrounded by Schwann cell processes, forming an incipient onion bulb. Bar = 1 pm.
Patient 3 . Large axons without myelin sheaths were encountered, the Schwann cells of which oc- casionally contained myelin debris. In longitudinal sections, rather wide nodes of Ranvier and demy- elinated and remyelinated internodes were present (Fig. 5) . Myelinated axons were frequently sur- rounded by Schwann cell processes with incipient onion bulb formation, whereby the circular Schwann cell processes were densely plated, sur- rounded by a common basal lamina. In other in- stances, circular or isolated loops of basal lamina were derived from Schwann cell surfaces of my- elinated and nonmyelinated axons. Occasionally, a rather large mitochondrion was encountered within the Schwann cell cytoplasm. A few lipid- laden macrophages were also present. Stacks of Schwann cell processes without myelinated or non- myelinated axons were occasionally seen.
Patient 4 . Myelinated nerve fibers often had thin myelin sheaths compared to their axon diame- ter. Other large single axons were entirely devoid of a myelin sheath; the adjoining Schwann cell cy- toplasm contained fragments of myelin sheath. Segments were encountered in longitudinal sec- tions, which represented paranodal demyelination (Fig. 6a) and wide nodes of Ranvier (Fig. 6,b and c). Schwann cell cytoplasm contained elec- tron-lucent or electron-dense membranous lipid material, even when also harboring a small, nonmyelinated axon. Membranous profiles were scattered in several myelinated axons. Myelin de- bris was present in the Schwann cell cytoplasm of other myelinated axons next to a myelin sheath having a normal structure. Occasionally, a large mitochondrion was seen. Schwann cell processes of various size were found without axons forming Bungner’s bands (Fig. 6d).
In summary, in the electron microscopic changes there was primary demyelination and re- myelination, as well as loss of nerve fibers, shown by the presence of Bungner’s bands. There also seemed to be a variable loss of unmyelinated axons evidenced by flat-plated Schwann cell processes surrounded by a common basal lamina. Break- down of myelinated nerve fibers resulted in ac- cumulation of myelin debris in Schwann cells and lipid material in macrophages.
DISCUSSION
Each of the four patients reported here had Leigh’s subacute necrotizing encephalomyelopathy identified by characteristic histologic lesions in the brain stem and other areas of the brain. Involve- ment of peripheral nerves was clearly evident from
170 Neuropathy in Leigh’s Disease MUSCLE & NERVE February 1986

FIGURE 5. Case 3. Differences in myelin sheath thickness of two adjacent internodes indicate remyelination (R), whereas the vacuolization between myelin sheath and axon in the right lower internode represents a preparative artifact. Bar = 1 Krn.
reduced conduction velocities, and this involve- ment was further documented by morphological studies of sural nerves. Pathology of the sural nerves was less obvious by light microscopic inspec- tion than by morphometry, especially when cal- culating the g-ratio (axon diameterhotal fiber di- ameter).
The myelinated fibers of the normal human sural nerve can be separated, after the age of about 2 years, into two populations, using the g-ratio cal- culation. l l A population of fibers of thin caliber is characterized by relatively thin myelin sheaths, having high g-ratios. The rest of the fibers of larger caliber show a regression of sheath thickness with fiber caliber. These fiber classes cannot be separated between the ages of 1 and 6 months. Infants between the 6 and 12 months of age showed an initial separation of fiber classes with much overlap between the caliber ranges of the two populations. In children aged 2-4 years, the two classes are completely separated. The fibers of larger diameter show an increase both in caliber and in sheath thickness, with a change in their po- sition in the scattergram. Regenerated, and proba- bly also remyelinated, fibers have permanently thinner sheaths than normal fibers. They showed typical scattergrams of higher g-ratios, sensitively detecting the changes in the regenerated fiber populations.' l 1
In the present study, the youngest child (pa- tient 2) did not show an abnormal g-ratio, whereas the three older ones did. This seems to indicate that an abnormal g-ratio may have developed after 20 months of age. However, only one child with
Leigh's disease among our four patients fell into the category of under 2 years; her normal g-ratio must be compared with findings in other patients of the same age class. The elevated g-ratio in the sural nerves of three older children affected by Leigh's disease indicated the existence of a popula- tion of myelinated nerve fibers having abnormally thin myelin sheaths. Morphometric data of a higher g-ratio may not distinguish whether abnor- mally thin myelin sheaths are due to remyelination or regeneration. Electron microscopy clarified that remyelination was at least one factor contributing to the elevated g-ratio.
Demyelination was also clearly evident in sural nerves with evidence of paranodal demyelination, and it seemed to occur early in the course of the disease, as it has been shown in congenital Leigh's disease.26 A widened node of Ranvier between two myelinated internodes, where the axon is covered only by a basal lamina but not by Schwann cell cytoplasm (Fig. 6b and c), may be a subtle sign of the demyelination-remyelination process.
Thus, peripheral, and also ~ e n t r a l , ' ~ . ' ~ myelin is primarily damaged in Leigh's disease. Myelin dam- age is independent of the type of underlying en- zyme defect, as morphometric as well as electron microscopic features were identical in our patients afflicted by PDH complex (patient 3) as well as cytochrome oxidase deficiency (patient 4).
Proliferation of Schwann cell processes form- ing densely packed plates surrounded by a com- mon basal lamina also suggested a primary loss of unmyelinated fibers, without giving convincing evidence of whether this loss of unmyelinated
Neuropathy in Leigh's Disease MUSCLE & NERVE February 1986 171

FIGURE 6. Case 4. (a) A small demyelinated axon with its Schwann cell (S) is located between two adjacent myelinated internodes representing paranodal demyelination. (b) A single axon devoid of ensheathing Schwann cell cytoplasm is sur- rounded only by a basal lamina. This probably indicates a cross-section through a widened Ranvier’s node, as illustrated (c) in a longitudinally sectioned Ranvier’s node below. (d) Biinger’s band: Schwann cell processes without axons. Bars = 1 pm.
nerve fibers was due to direct axonal damage or secondary damage to the respective neuronal perikarya.
REFERENCES Beuche W, Friede RL: A new approach toward analyzing peripheral nerve fiber populations. 11. Foreshortening of regenerated internodes corresponds to reduced sheath thickness. J Neuropathol Ejsp Neurol44:73-84, 1985. Clayton BE, Dobbs RH, Patrick AD: Leigh‘s subacute nec- rotizing encephalopathy: clinical and biochemical study, with special reference to therapy with lipoate. Arch Dis Child
Cooper JR, Pincus JH, Itokawa Y, Piros K: Experience with phosphoryl transferase inhibition in subacute necrotizing encephalomyelopathy. N Engl J Med 283:793-795, 1970.
42~467-478, 1967.
4.
5.
6.
7.
8.
9.
10.
Crosby TW, Chou SM: “Ragged-red” fibers in Leigh’s dis- ease. Neurology (Minneap) 24:49-54, 1974. De Vivo DC, Haymond MW, Obert KA, Nelson JS, Pagliara AS: Defective activation of the pyruvate dehydrogenase complex in subacute necrotizing encephalomyelopathy (Leigh disease). Ann Neurol6:483-494, 1979. Dunn HG, Dolman CL: Necrotizing encephalomyelopathy. Neurology (Minneap) 19:538-550, 1969. Evans OB: Polyneuropathy in childhood. Pediutncs 64:96- 105, 1979. Evans OB: Pyruvate decarboxylase deficiency in subacute necrotizing encephalomyelopathy. Arch Neurol 38:5 15- 519, 1981. Evans OB, Kilroy AW, Fenichel GM: Acetazolamide in the treatment of pyruvate dysmetabolism syndromes. Arch Neurol35:302-305, 1978. Friede RL, Beuche W: A new approach toward analyzing peripheral nerve fiber populations. I. Variance in sheath thickness corresponds to different geometric proportions of the internodes. J Neuropathol Exp Neurol 44:60-72, 1985.
172 Neuropathy in Leigh’s Disease MUSCLE & NERVE February 1986

1 1 . Friede RL, Beuche W: Combined scatter diagrams of sheath thickness and fibre calibre in human sural nerves. Changes with age and neuropathy. J Neurol Neurosurg Psy- chiatly 48:749-756, 1985.
12. Gilbert EF, Arya S, Chun R: Leigh’s necrotizing en- cephalomyelopathy with pyruvate carboxylase deficiency. Arch Pathol Lab Med 107:162-166, 1983.
13. Guazzi GC, Martin JJ, Brucher JM, Taper HS, Macken J, Neetens A, Van Haegenborgh J: Sur l’importance de I’at- teinte vasculaire et de la dystrophie gliale dans en- ckphalomyelopathie necrosante de Leigh. J Neurol Scz
14, Jellinger K, Seitelberger F: Subacute necrotizing en- cephalomyelopathy (Leigh). Ergeb Inn Med Kinderheilkd
15. Jellinger K, Zimprich H, Miiller D: Relapsing form of sub- acute necrotizing encephalomyelopathy. Neuropediatrics
16. Kohlschutter A, Kraus-Ruppert R, Rohrer T, Hersch- kowitz NN: Myelin studies in a case of subacute necrotiz- ing encephalopathy (SNE). J Neuropnthol Exp Neurol 37:
17. Kolkmann F-W, Volzke E: Uber die spongiosen Dystro- phien des Nervensystems im fruhen Kindesalter. 11. Fokal- disseminierte Formen mit Bevorzugung des Hirnstammes (infantiles Wernicke-Syndrom und subakute nekrotisier- ende Encephalopathie). 2 Kinderheilk 98:287-306, 1967.
7~357-379, 1968.
29:155-219, 1970.
4:314-321, 1973.
155-164, 1978.
18. Leigh D: Subacute necrotizing encephalomyelopathy in an infant. J Neurol Neurosurg Psychiatry 14:216-221, 1951.
19. Montpetit VJA, Andermann F, Carpenter S, Fawcett JS, Zborowska-Sluis D, Giberson HR: Subacute necrotizing en- cephalomyelopathy. A review and a study of two families. Brain 94:l-30, 1971.
20. Moosa A: Peripheral neuropathy in Leigh’s encephalomy- elopathy. Dev Med Child Neurol 17:621-640, 1975.
21. Moosa A: Motor nerve conduction velocities in Leigh’s en- cephalomyelopathy. Arch Dis Child 53:62-65, 1978.
22 . Namiki H: Subacute necrotizing encephalomyelopathy. Arch Neurol 12:98-107, 1965.
23. Pincus JH, Itokawa Y, Cooper JR: Enzyme-inhibiting factor in subacute necrotizing encephalomyelopathy. Neurology (Minneap) 19:841-845, 1969.
24. Reye RDK: Subacute necrotizing encephalomyelopathy. J Pathol Bacteriol 79:165-173, 1960.
25. Robinson F, Solitare GB, Lamarche JB, Levy LL: Necrotiz- ing encephalomyelopathy of childhood. Neurology (Min- neap) 17:472-484, 1967.
26. Seitz RJ, Langes K, Frenzel H, Kluitmann G, Wechsler W: Congenital Leigh’s disease: panencephalomyelopathy and peripheral neuropathy. Acta Neuropathol (Berl) 64: 167- 171, 1984.
27. Willems JL, Monnens LAH, TrlJbels JMF, Veerkamp JH, Meyer AEFH, van Dam K, van Haelst U: Leigh’s en- cephalomyelopathy in a patient with cytochrome c oxidase deficiency in muscle tissue. Pediatrics 60:850-857, 1977.
Neuropathy in Leigh’s Disease MUSCLE & NERVE February 1986 173