Embed Size (px)
Citation preview
O R I G I N A L A R T I C L E
Supportive counseling for postpartum depression in Asianmothers
Johnson Fam MBBS MMed (Psych), Helen Chen MBBS MMed (Psych) Dip Psychotherapy &Jemie Wang BPsych (Hons)
Mental Wellness Service, KK Women’s and Children’s Hospital, Singapore
Keywords
counseling, depression, postpartum
Correspondence
Johnson Fam, Mental Wellness Service, KK
Women’s and Children’s Hospital, Singapore,
100 Bukit Timah Road, 229899 Singapore.
Tel: 163 94 2205
Fax: 163 948 087
Email: [email protected]
Received 5 September 2010
Accepted 19 January 2011
DOI:10.1111/j.1758-5872.2011.00122.x
AbstractIntroduction: The aim of the present study was to describe the role of
supportive counseling for postpartum depression (PPD) in an Asian popu-
lation and explore the treatment outcomes of supportive counseling with
and without antidepressants. Oral antidepressants remain the mainstay
treatment in depression. However in postpartum depression, mothers are
often concerned about breastfeeding and the effects of medication on the
developing child. For mothers willing to take antidepressants, the class of
antidepressant more efficacious for postpartum depression still remains
unclear. Non-pharmacological treatments appear to have an important role
in recent studies.
Methods: In this naturalistic prospective cohort study, patients were iden-
tified from a postpartum depression screening program in a maternity
hospital. Patients diagnosed with PPD were treated with antidepressant and
counseling, or counseling alone. Outcomes were assessed using the Edin-
burgh Postnatal Depression Scale (EPDS) and Global Assessment of Func-
tioning Scale (GAF). Statistical Package for the Social Sciences (SPSS) was
used for statistical analyses (SPSS Inc., Chicago, IL, USA).
Results: Between April 2008 and December 2009, 87 patients were re-
cruited in this study. Sixty-nine percent of all patients achieved remission
at 6 months. Combining antidepressants and counseling did not appear to
significantly improve outcome compared to counseling alone.
Discussion: The majority of all depressed mothers with supportive coun-
seling had remission of symptoms by 6 months. The benefit of combining
antidepressants and counseling needs to be further studied.
Introduction
Maternal depression can have deleterious effects on
new mothers, their infants, and their family. Postpar-
tum mood disorders represent the most frequent form
of maternal morbidity following delivery (Stocky &
Lynch, 2000). A meta-analysis reported that approxi-
mately 13% of new mothers experience PPD in the
first year after childbirth (O’Hara & Swain, 1996). In
Singapore, a study of 559 women at 6 weeks postpar-
tum reported a point prevalence of 6.8% for depres-
sion (Chee et al., 2005).
Postpartum depression is not uncommon and
consequences can be grave, yet there remains a pau-
city of evidence for effective treatment, particularly of
randomized clinical trials on antidepressants use (Hoff-
brand et al., 2001). Mothers who breastfeed may be
apprehensive towards taking antidepressants, result-
ing in delayed treatment and illness progression. Anti-
depressants prescribed in reduced doses can also lead
to potentially ineffective treatment.
Psychosocial factors are important in the etiology
of postpartum depression, especially risk factors such
as stressful life events, marital conflict and the lack of
social support (O’Hara & Swain, 1996; Bernazzani
et al., 1997). Treatment by social and psychological
interventions appeared effective in a recent systematic
review and meta-analysis (Dennis & Hodnett, 2007).
In this study, we primarily aimed to examine the role
of supportive counseling for postpartum depression by
describing the characteristics of postpartum depressed
mothers, the treatment received and the longitudinal
Asia-Pacific Psychiatry 3 (2011) 61–66 Copyright c� 2011 Blackwell Publishing Asia Pty Ltd 61
Asia-Pacific Psychiatry ISSN 1758-5864
Offi cial journal of thePacifi c Rim College of Psychiatrists

outcome, and secondarily to explore if adding antide-
pressants affected treatment outcome.
Methods
Study design
Naturalistic prospective cohort study.
Participants
Participants were recruited consecutively from general
obstetric outpatient clinics from the largest hospital
providing specialized obstetric and care in Singapore,
under a postpartum depression screening and inter-
vention program.
Inclusion criteria
(i) All women screened within 6 months after a live
birth.
(ii) Baseline Edinburgh Postnatal Depression Scale
(EPDS) score Z13, and with follow-up score.
(iii) Clinically assessed to have major or minor depres-
sion according to Diagnostic and Statistical Manual of
Mental Diseases Fourth Edition (DSM-IV) Research
Criteria.
Exclusion criteria
(i) Young mothers aged below 18, as they are already
provided care from an established medical social work
program that includes emotional support.
(ii) Mothers who were already engaged in psychiatric
care during the antepartum period.
Screening procedure
Participants were screened by trained perinatal mental
health case managers, in a private setting, using the
EPDS (Cox et al., 1987). We made a minor modification
to the EPDS, to include the qualifier of symptoms ‘‘in
the past 1 week’’, as in a pilot run we noted that local
women tended to misinterpret the questions to refer-
ring to the general past. We used a threshold of 13 to
identify women likely to suffer from major depression,
as recommended (Cox et al., 1987; Murray & Car-
others, 1990). Those with EPDS scores of 13 or more
were clinically reviewed to confirm diagnosis accord-
ing to DSM-IV.
Intervention
Treatment was provided to cases identified to have
postpartum depression after initial screening and clin-
ical assessment by a psychiatrist. Clinical intervention
included supportive counseling and antidepressants,
or supportive counseling alone. Supportive counseling
is given to all patients by both clinicians and case
managers, addressing the immediate stressors, particu-
larly those relating to the adjustment to motherhood
and the newborn. It is given during follow-up visits
and telephone contact. A supportive counseling frame-
work, detailing areas to address during initial, follow-
up and concluding sessions, was in place to provide
both guidance and consistency.
Antidepressants were given to patients who were
agreeable to take medications. The type of antidepres-
sant used was in accordance with UK guidelines
(National Institute for Health and Clinical Excellence,
2007), and by considering individual patient risk
and their informed choice of either tricyclic antide-
pressants (TCAs) or selective serotonin reuptake inhi-
bitors (SSRIs).
Case management was provided by trained case
managers, providing integrated and individualized
care for our patients together with the psychiatrist,
thus ensuring continuity of care through the different
phases of the illness. To enhance the level of social
support, participation in facilitated support groups was
encouraged. Those with significant social problems
(e.g. domestic violence, marital conflicts, and financial
difficulties) were referred to our medical social work-
ers or appropriate community resources.
Outcome measurement
The EPDS and Global Assessment of Functioning
Scale (GAF) scores were measured at baseline, and
subsequently measured again upon discharge, or by
6 months follow-up if not discharged. The EPDS
is validated in many Asian populations (Lee et al.,
1998; Rushidi et al., 2002; Benjamin et al., 2005)
and has been used to measure change in postnatal
depression. The reliable change index (RCI) using
12/13 as the cutoff for depression was calculated to be
4 points for 95% confidence in detecting real change
(Matthey, 2004). Remission was defined as o9 points
on follow-up EPDS score. Time to remission was
measured in weeks.
Data analysis
Statistical Package for the Social Sciences (SPSS) ver-
sion 14 (SPSS Inc., Chicago, IL, USA) was used for data
analysis unless otherwise stated. The t-test, w2 and
analysis of variance (ANOVA) were used where appro-
priate for univariate analysis. Regression methods
were used for covariate analysis.
62 Asia-Pacific Psychiatry 3 (2011) 61–66 Copyright c� 2011 Blackwell Publishing Asia Pty Ltd
J. Fam et al.Counseling for postpartum depression in Asian mothers
Results
From April 2008 to December 2009, 87 subjects who
met the study criteria received psychiatric treatment at
KK Hospital. Of the 12 lost to follow-up, nine were not
contactable, one refused for no reason, one refused for
financial reason and one returned overseas. The over-
all drop-out rate in this study was low at 13.8%.
Comparing those who accepted treatment and
those lost to follow-up, no significant statistical differ-
ence was found for race, education, marital status,
number of children, baseline EPDS score, percentage
of major depressives and treatment given. However,
subjects lost to follow-up were significantly younger
by an average of 3 years. Post-baseline assessment was
not obtained for those lost to follow-up.
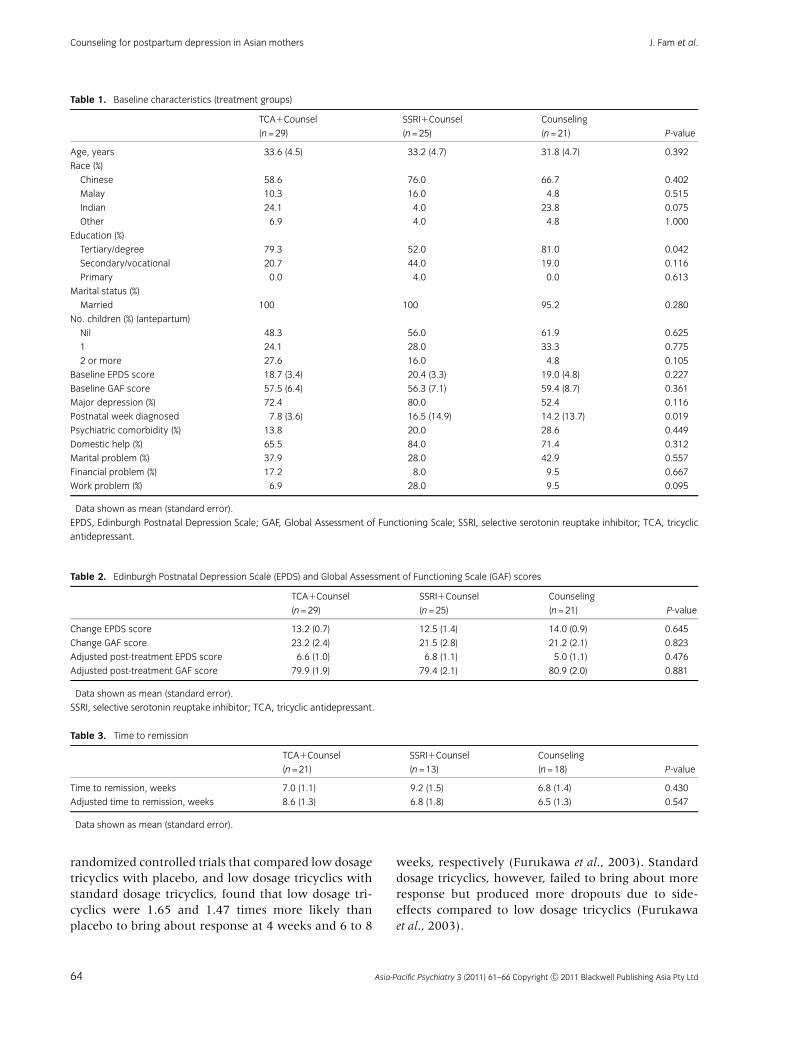
For patients who received antidepressants, 54%
were on TCAs and 46% on SSRIs (Figure 1). TCAs
were used at the lower end of the therapeutic range
compared to the SSRIs (Figure 2), due to the side-effect
tolerability of TCAs.
Baseline depression scores and proportion of sub-
jects with major depression were similar in the three
groups (Table 1). There were significantly fewer In-
dians and tertiary educated subjects in the SSRI group,
and the TCA group subjects were diagnosed earlier.
These variables were adjusted for during outcome
analysis. Twenty percent of all subjects had psychiatric
comorbidities, most frequently an anxiety disorder. Se-
venty-three percent had domestic help in the form of a
live-in maid, relative or some childcare arrangement.
The most prominent psychosocial stressor was marital
problems, affecting 36% of all depressed women.
In Table 2, no significant differences in treatment
outcomes were found among the three groups. Cov-
ariate adjusted post-treatment scores similarly did not
show statistical difference.
The total proportion of remissions at 6 months
were 72% in the TCA and counseling group, 52% in
the SSRI and counseling group and 86% in the coun-
seling alone group. The differences did not reach
statistical difference (P = 0.055), even after adjusting
for covariates. The overall remission for all patients,
regardless of treatment type, was 69% at 6 months.
Among patients who remitted, those on SSRIs and
counseling appeared to take longer to remit compared to
the other two groups, but this was not statistically
significant (Table 3). After adjusting for covariates, there
were still no significant differences in the time to remis-
sion. The mean time to remission was 7.4 weeks.
Discussion
This naturalistic study examined the treatment of post-
natal depression in an outpatient setting of a maternity
hospital. We sought to explore the role of supportive
counseling in a realistic setting and on an Asian popula-
tion, and to examine the treatment outcomes.
In this study, 86% of mothers who received sup-
portive counseling alone had remission, and those
who remitted did so at around 7 weeks. From epide-
miological studies, episodes of postnatal depression last
3 to 6 months (Cooper & Murray, 1995) and up to 50%
of mothers remain depressed at 6 months, and around
25% continue to remain depressed at 1 year postpar-
tum (Kumar & Robson, 1984). From our results, it
appears that supportive counseling was improving
patients’ outcome above that of natural remission.
Whether this benefit is sustained in the long term
requires further study (Cooper et al., 2003).
Seventy-two percent of women diagnosed with
postpartum depression in our study agreed to be on
antidepressant therapy. This perhaps reflects the chan-
ging trend in patient acceptance of medication use in
postpartum depression.
It was striking to observe that antidepressant use
in this study did not result in a larger improvement or a
faster time to remission. The use of lower TCA dosages
compared to SSRIs did not appear to have a differential
effect on treatment outcome. Systematic review of
46%
8%
24%
15%7%
Antidepressants
Dothiepin
Clomipramine
Sertraline
Escitalopram
Fluoxetine
Figure 1 Antidepressants prescribed.
Figure 2 Antidepressant dosages.
Asia-Pacific Psychiatry 3 (2011) 61–66 Copyright c� 2011 Blackwell Publishing Asia Pty Ltd 63
J. Fam et al. Counseling for postpartum depression in Asian mothers
randomized controlled trials that compared low dosage
tricyclics with placebo, and low dosage tricyclics with
standard dosage tricyclics, found that low dosage tri-
cyclics were 1.65 and 1.47 times more likely than
placebo to bring about response at 4 weeks and 6 to 8
weeks, respectively (Furukawa et al., 2003). Standard
dosage tricyclics, however, failed to bring about more
response but produced more dropouts due to side-
effects compared to low dosage tricyclics (Furukawa
et al., 2003).
Table 1. Baseline characteristics (treatment groups)
TCA1Counsel SSRI1Counsel Counseling
P-value(n = 29) (n = 25) (n = 21)
Age, years� 33.6 (4.5)� 33.2 (4.7)� 31.8 (4.7)� 0.392
Race (%)
Chinese 58.6 76.0 66.7 0.402
Malay 10.3 16.0 4.8 0.515
Indian 24.1 4.0 23.8 0.075
Other 6.9 4.0 4.8 1.000
Education (%)
Tertiary/degree 79.3 52.0 81.0 0.042
Secondary/vocational 20.7 44.0 19.0 0.116
Primary 0.0 4.0 0.0 0.613
Marital status (%)
Married 100 100 95.2 0.280
No. children (%) (antepartum)
Nil 48.3 56.0 61.9 0.625
1 24.1 28.0 33.3 0.775
2 or more 27.6 16.0 4.8 0.105
Baseline EPDS score� 18.7 (3.4)� 20.4 (3.3)� 19.0 (4.8)� 0.227
Baseline GAF score� 57.5 (6.4)� 56.3 (7.1)� 59.4 (8.7)� 0.361
Major depression (%) 72.4 80.0 52.4 0.116
Postnatal week diagnosed� 7.8 (3.6)� 16.5 (14.9)� 14.2 (13.7)� 0.019
Psychiatric comorbidity (%) 13.8 20.0 28.6 0.449
Domestic help (%) 65.5 84.0 71.4 0.312
Marital problem (%) 37.9 28.0 42.9 0.557
Financial problem (%) 17.2 8.0 9.5 0.667
Work problem (%) 6.9 28.0 9.5 0.095
�Data shown as mean (standard error).
EPDS, Edinburgh Postnatal Depression Scale; GAF, Global Assessment of Functioning Scale; SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic
antidepressant.
Table 2. Edinburgh Postnatal Depression Scale (EPDS) and Global Assessment of Functioning Scale (GAF) scores�
TCA1Counsel SSRI1Counsel Counseling
P-value(n = 29) (n = 25) (n = 21)
Change EPDS score 13.2 (0.7) 12.5 (1.4) 14.0 (0.9) 0.645
Change GAF score 23.2 (2.4) 21.5 (2.8) 21.2 (2.1) 0.823
Adjusted post-treatment EPDS score 6.6 (1.0) 6.8 (1.1) 5.0 (1.1) 0.476
Adjusted post-treatment GAF score 79.9 (1.9) 79.4 (2.1) 80.9 (2.0) 0.881
�Data shown as mean (standard error).
SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressant.
Table 3. Time to remission�
TCA1Counsel SSRI1Counsel Counseling
P-value(n = 21) (n = 13) (n = 18)
Time to remission, weeks 7.0 (1.1) 9.2 (1.5) 6.8 (1.4) 0.430
Adjusted time to remission, weeks 8.6 (1.3) 6.8 (1.8) 6.5 (1.3) 0.547
�Data shown as mean (standard error).
64 Asia-Pacific Psychiatry 3 (2011) 61–66 Copyright c� 2011 Blackwell Publishing Asia Pty Ltd
J. Fam et al.Counseling for postpartum depression in Asian mothers

In a meta-analysis of randomized controlled trials
of antidepressants in general, using patient-level data,
it was found that the magnitude of benefit from
antidepressant medication compared with placebo in-
creased with severity of depression symptoms, and
may be minimal in patients with mild or moderate
depression symptoms (Fournier et al., 2010). It may be
possible that the antidepressant effect may have failed
to separate from the counseling effect because of the
moderate levels of depression in our cohort. Another
postulation is that the women who opted for counsel-
ing and declined antidepressants were more resilient,
and psychologically minded. Indeed, baseline educa-
tion for the counseling alone group was observed to be
higher than the antidepressant combination groups.
To our knowledge, there are no published controlled
trials comparing supportive counseling with antidepres-
sant treatment in postpartum depression. One rando-
mized controlled trail compared fluoxetine plus cognitive
behavioral counseling (CBC) with placebo plus CBC
(Appleby et al., 1997). Fluoxetine and a full course of
CBC combined had no added advantage over placebo
and a full course CBC. Although this lends some support
to our observation, there is still a need to see if our result
could be replicated in a larger, randomized controlled
trial using supportive counseling in place of CBC.
Considering the study limits, these findings may
not be conclusive and need further verification. Never-
theless, our results do provide useful pilot data to
suggest that supportive counseling alone may be ade-
quate for mothers with depression that is mild to
moderate in severity.
Conclusion
With the coordinated care and close monitoring from
case managers, the overall drop-out from treatment was
low. Sixty-nine percent of all depressed mothers on their
preferred treatment had remission of symptoms by 6
months, within an average time of 7 weeks. Mothers
allowed to express treatment preference may benefit
overall outcome.
Within the limitations of this study, we observed
no additional benefit combining antidepressants with
supportive counseling for mild to moderate levels of
depression. The evidence is inconclusive and more
trials are needed in this area before clinical recommen-
dations can be made.
References
Appleby L., Warner R., Whitton A., Faragher B. (1997) A
controlled study of fluoxetine and cognitive-behavioural
counselling in the treatment of postnatal depression.
BMJ. 314, 932–936.
Benjamin D., Chandramohan A., Annie I.K., Prasad J.,
Jacob K.S. (2005) Validation of the Tamil version of
Edinburgh post-partum depression scale. J Obstet
Gynecol India. 55, 241–243.
Bernazzani O., Saucier J., David H., Borgeat F. (1997)
Psychosocial predictors of depressive symptomatology
level in postpartum women. J Affect Disord. 46, 39–49.
Chee C., Lee D., Chong Y., Tan L., Ng T., Fones C. (2005)
Confinement and other psychosocial factors in perinatal
depression: a transcultural study in Singapore. J Affect
Disord. 89(1–3), 157–166.
Cooper P.J., Murray L. (1995) Course and recurrence of
postnatal depression. Evidence for the specificity of the
diagnostic concept. Br J Psychiatry. 166, 191–195.
Cooper P.J., Murray L., Wilson A., Romaniuk H. (2003)
Controlled trial of the short- and long-term effect of
psychological treatment of postpartum depression. I.
Impact on maternal mood. Br J Psychiatry. 182,
412–419.
Cox J.L., Holden J.M., Sagovsky R. (1987) Detection of
postpartum depression. Development of the 10-item
Edinburgh Postnatal Depression Scale. Br J Psychiatry.
150, 782–786.
Dennis C.L., Hodnett E.D. (2007) Psychosocial and
psychological interventions for treating postpartum
depression. Cochrane Database Syst Rev., (4):
CD006116.
Fournier J.C., DeRubeis R.J., Hollon S.D., et al.. (2010)
Antidepressant drug effects and depression severity: a
patient-level meta-analysis. JAMA. 303(1), 47–53.
Furukawa T., McGuire H., Barbui C. (2003) Low dosage
tricyclic antidepressants for depression. Cochrane
Database Syst Rev., (3): CD003197.
Hoffbrand S.E., Howard L., Crawley H. (2001)
Antidepressant treatment for post-natal depression.
Cochrane Database Syst Rev., (2): CD002018.
Kumar R., Robson K.M. (1984) A prospective study of
emotional disorders in childbearing women. Br J
Psychiatry. 144, 35–47.
Lee D.T., Yip S.K., Chiu H.F., et al. (1998) Detecting
postnatal depression in Chinese women. Validation of
the Chinese version of the Edinburgh Postnatal
Depression Scale. Br J Psychiatry. 172, 433–437.
Matthey S. (2004) Calculating clinically significant change
in postnatal depression studies using the Edinburgh
Postnatal Depression Scale. J Affect Disord. 78(3),
269–272.
Murray L., Carothers A.D. (1990) The validation of the
Edinburgh Postnatal Depression Scale on a community
sample. Br J Psychiatry. 157, 288–290.
Asia-Pacific Psychiatry 3 (2011) 61–66 Copyright c� 2011 Blackwell Publishing Asia Pty Ltd 65
J. Fam et al. Counseling for postpartum depression in Asian mothers

National Institute for Health and Clinical Excellence.
(2007) Antenatal and Postnatal Mental Health.
CG45:1.4.8.4-6. London: National Institute for Health
and Clinical Excellence.
O’Hara M.W., Swain A.M. (1996) Rates and risks of
postpartum depression: a meta-analysis. Int Rev
Psychiatry. 8, 37–54.
Rushidi W.M., Azidah A.K., Shaiful Bahari I., Janil M.Y.
(2002) Validation of the Malay version of the Edinburgh
Postnatal Depression Scale (EPDS). Malaysian J
Psychiatry. 10, 44–49.
Stocky A., Lynch J. (2000) Acute psychiatric disturbance in
pregnancy and the puerperium. Baillieres Best Pract Res
Clin Obstet Gynaecol. 14, 73–87.
66 Asia-Pacific Psychiatry 3 (2011) 61–66 Copyright c� 2011 Blackwell Publishing Asia Pty Ltd
J. Fam et al.Counseling for postpartum depression in Asian mothers