Embed Size (px)
Citation preview

Supporting Patient Transitions to Improve Client and Health System Outcomes: CCAC Rapid Response Nursing Program
Dilys Haughton RN(EC), BScN, PHC-NP, GNC(C), MHSc, CHE Director Client Services Operations and Professional Practice Lead Colleen Lackey RN, BScN Manager Client Services
Outstanding care – every person, every day
National Health Leadership Conference June 11, 2013

Overview
Objective
Learn about the provincial CCAC Rapid Response Nurse Program
• facilitates safe transitions from acute care to home, primary care provider, and community supports;
• Reduce hospital readmission rates
• Review lessons learned and key success factors
1. Project Background and Evidence
2. Overview of Provincial Rapid Response Nurse Program
3. Local Experience
4. Summary
2

Background
3
• Effective transitions between hospital and home are recognized as critical to achieving better patient outcomes and avoiding rehospitalisation.
• Many patients have sub-optimal experiences in care transition
between hospital and home/community care. Problems include: • Medication discrepancies • Confusion about post discharge care plans
• Hospital readmission rates for COPD / HF ~30%
• Risk of readmission is significantly lower when:
• 1st home care visit take place within 24 hours of discharge • Primary care visit occurs within 7 days of discharge
1Nurses in CCACs: Providing Care and Creating Connections Across Sectors, P. 4

RRNP -The Journey Ahead
4
March 2013
RRNP Go LIVE
January 2013
Communication Plan Confirmed
Policy/Procedures Gaps Addressed
Documentation Processes Set
Training/Orientation Plan
RRNP Role Defined
Scheduling Model Set
Relationships Clarified
Common Equipment Determined
Intake/Screening Processes Defined
Stakeholder Engagement Planned
December 2012
November 2012
Goal & Objectives Refined
RRNP Model Developed
Target Pop/Eligibility Clarified
Recruitment Process Occurring
Work Streams Established
Provincial RRNP
Working Group Initiated
October 2012
Clinical Supervision Processes Set
Alignment with CCM Determined
February 2012
Ongoing Refinement of
RRNP Model
June 2013 & Onward
TBD
Funding Accountabilities Capabilities
Measurement & Reporting Processes Confirmed
BTS in Place

RRN Allocation by LHIN
5
LHIN/CCAC RRN (Minimum # for Care of Complex Children)
Erie St. Clair 8 (1)
Southwest 13 (3)
Waterloo-Wellington 6 (1)
Hamilton Niagara Haldimand Brant
14 (2)
Central West 6 (1)
Mississauga Halton 7 (1)
Toronto Central 10 (2)
Central 10 (2)
Central East 11 (2)
South East 7 (1)
Champlain 11 (2)
North Simcoe Muskoka 5 (1)
North East 13 (3)
North West 5 (1)
126

Evidence: Effective Transitions
Evidence to support care transitions and prevent hospital readmission (models and for specific diagnoses)
• Common elements from the literature include:
• In-home follow-up care (24-72 hours)
• Care coordination across transitions
• Medication management/reconciliation
• Patient education/empowerment (Coleman) or care management (Naylor)
• Patient-centered care
• Patient enabled with personal health record
• Follow-up with primary care provider
(Rich et al, 1995; Naylor et al., 1995; Coleman et al., 2006)
6

Program Goals
• Reduce rehospitalization and avoidable emergency department visits by improving the quality of transition from acute care to home care for two population groups:
• Frail adults and seniors who are medically complex or have chronic diseases that tend towards frequent hospitalization, unstable health and costly treatments.
• Medically complex/vulnerable children, and their families
7

Rapid Response Nurses
8
Home
Hospital
24 hours 7 days
Care
Coordinator
Rapid
Response
Nurse
Primary Care
Home/Community Care

Care Coordinators
Hospital
-Case finding
-Screening for eligibility
-Identify RRN involvement Pre D/C
-Collection of D/C information
-Overall Service Planning
-Service Ordering of RRN
-Consent for Tx
-Problem-based assessment using common tool
-Teach back approach to education
-Medication Reconciliation
-Confirm medical tests
-Update In-Home Health Record
-Linking with PCP
- Ongoing problem- based assessment to ensure client stable & safe
-Address ongoing medication issues
-Linking with PCP
-Contribute to Service Planning
-Joint visit/phone with CC and SP to transition care
Emergency Dept.
-
-Arrange PCP appointment if needed
-Update PCP about acute care event/ post D/C plan
-Share contact information
-Share problem based assessment & medication reconciliation
-Discharge from RRN Program
9
Referral
Source Intake by Hospital CC
RRN
Visit
Follow-up
Care
Transition to
PCP/SP/Community CC
Target Population - Complex and Chronic Using CCM: • * Frail adults and seniors that are medically complex or have chronic diseases that tend
towards frequent hospitalization, unstable health and costly treatments, including: CHF,
COPD, Diabetes, Other Ambulatory Sensitive Conditions
• Medically complex/vulnerable children, and their families
Model of Care Discharge from
Hospital
24 Hours
7 Days
Integrated Care Transitioning from Hospital to PCP/Community Providers
LOS 2-3 weeks

RRN Role – Transitional Care • First visit within 24 hours at a time when caregiver
available
• Conduct clinical problem-based assessment
• Use “teach back” techniques to provide education about care plan, treatment, symptom management, and when/who to ask for help
• Perform medication reconciliation
• Confirm and arrange for follow-up tests
• Follow-up visit/phone call to provide further assessment or address ongoing medication issues
• Arrange follow-up appointment with primary care within 7 days of hospital discharge
10

11
Client Care Model

Key Performance Indicators Client Information
• Number / % of patients served (by type/profile children, adults, seniors; by ambulatory sensitive condition*)
Access • # of visits; average number of visits per patient • Average Length of Stay • Number / % of in-home visits within 24 hours of hospital discharge* • Reason for not receiving service
Health System Impact / Cost Effectiveness • Number / % of emergency visits within 30 days* • Number / % of hospital re-admissions in 30 days* • Number / % of primary care appointments within 1 week of hospital discharge*
Quality Measures
• Patient / informal caregiver experience & Provider Experience –overall satisfied with transition care, perception of care connections and integration(TBD)*
Health System Outcomes
• Measure of physician engagement - contacts between RRN and PCP*
12

Learnings from Local Implementation

HNHB CCAC: Overview
HNHB CCAC
• Hamilton, Niagara, Haldimand Norfolk, Brant, Burlington
• HNHB LHIN has 11% of Ontario population
• Older than average population
• CCAC70,000 patients / year
• 10 hospital corporations, 21 hospital sites
14

Implementation
15
January to March 2012: Design and implementation in 2 branches (Hamilton and Burlington) April to June 2012: Implemented a consultant pharmacy programme July to September 2012: Spread programme across the LHIN (Haldimand Norfolk, Brant and Niagara) October to December 2012: Full implementation of Adult Rapid Response Programme Consolidated clinical programme infrastructure (e.g. P and Ps) January 2013 ongoing: Partnered with hospital Bundled Transitions Project test of change Developing Paediatric focus of intervention Knowledge transfer

Patient Story: Improving the Transition
Mr. J. was in hospital for 9 months following a stoke and was discharged home. He requiring total care and was awaiting a move into Long Term Care.
PMHx: Longstanding epilepsy, osteoarthritis, osteoporosis - experiencing fracture of the hip and wrist, depression, non insulin dependent diabetes, indwelling by catheter. Recent UTI x 3 with the onset of delirium.
• No primary care provider visits in the last 6 years.
Issue: Patient is sleeping 23 hours / day. Why: Drug toxicity? Infection? Blood sugars? Pneumonia? UTI? Narcotic influence? Depression?
Key success factors: Access to hospital information (clinical connect); collaboration with primary care (blood work / CXR); consultation with pharmacist
Outcome: The patient woke up! Up in the chair 5 – 6 hours / day. Socializing with others. Able to moving successfully to Long Term Care.
16


Patient Characteristics: Diagnoses
• ~25% HF / heart related disorders
• ~25% COPD
• ~25% geriatric giants (e.g. pain, cognition, continence, mobility, falls)
• Most patients have multiple conditions, and multiple physicians involved
18

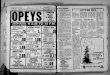
Patient Characteristics: Care Requirements
19
0
50
100
150
200
250
300
MAPLe 1 MAPLe 2 MAPLe 3 MAPLe 4 MAPLe 5
MAPLe Score by Age Group
75+
0 - 74
• MAPLe is a subset of the RAI HC instrument
• Measures ability to care for self / care requirements
• 47% patients could move into LTC (MAPLe 4,5)
• Another 35% are at the “tipping point”
• 18% of RRTT patients have an active placement file

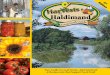
Patient Characteristics: Medical Complexity
20
0
50
100
150
200
250
300
350
400
450
CHESS 0 CHESS 1 CHESS 2 CHESS 3 CHESS 4 CHESS 5
Patients by CHESS Score (N=1315) • CHESS is a subscale of the RAI HC instrument
• Measures medical frailty
• Higher CHESS, lower life expectancy
• 66% patients have CHESS >2
• 30.4% patients >3

Performance Metrics: 2012 – 2013
Performance Output Indicator Actuals
# of new hospital patients discharged home to CCAC RRTT program
911 (60.9%)
# of existing CCAC patients referred to CCAC RRTT program
584 (39.1%)
% of high risk patients from hospital that require readmission within 7 days of discharge (81 of 911 patients)
8.9
21

Hospital Readmissions
22
0
0.02
0.04
0.06
0.08
0.1
0.12
0.14
0.16
May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
% R
ead
mis
sio
n
RRTT 7 Day Readmission Rate
Avg hospital readmission rate 8.9%

Hospital Readmissions
Hospital readmissions within 7 days
• N = 81 (8.9%)
• 82% > age 70
• 63% patients have CHESS >2
• 72% patients have MAPLe >3
23
0
5
10
15
20
25
30
<50 51-60 61-70 71-80 81-90 91-100 >100
Patients Readmitted to Hospital by Age (N=81)

Key Learnings
• Bridging the patient to home is an effective strategy to reduce hospital readmission rate
• Programme supports integration of patient care across sectors (hospital / home care / primary care)
• Hospital engagement is required at the front line, middle and upper management levels
• Identification / hospital screening for risk is important: need appropriate hospital risk screening process
• Local test of change showed all medical patients at risk of readmission using LACE screening tool. Hospitals across the LHIN will implement a Bundled Transitions Project using teach back techniques to further screen patients
• Timely transfer of accurate information such as medication lists and in-hospital record of care is important
• Medication lists, in-hospital record of care.
24

Key Learnings
• Focus on specific populations will focus efforts and help reduce hospital readmission (e.g. HF)
• About half of all patients have diagnosis of COPD or HF.
• Many patients have multiple diagnoses and multiple physicians involved – who is ‘in charge’?
• Patients often become disconnected from their primary care physicians: making the connection is important but can be challenging (physicians away, may not know the patients well). Number of orphaned patients is small
• Medication management is a key strategy
• Data collection across sectors is important to determine impact of programme on readmission rate
25

Outstanding care – every person, every day