Embed Size (px)
Citation preview
2/1/2017
1
Sheila Lopez, MSN,CNM
DON’T HOLD YOUR BREATH-
EVIDENCED BASED PUSHING
No conflict of interest
• I have no financial or other conflicts of interests related to this presentation.
Objectives: At the end of the course participants will be able to:
• Identify benefits to un-directed, open-glottis pushing for both mother and fetus.
• Identify strategies to facilitate patient education of open-glottis pushing techniques for the RN or other care provider at the bedside.
• Define labor dystocia and factors that contribute to slowed labor progress.
• Identify techniques, including optimal positioning, that promote labor progress and prevent or treat labor dystocia.
2/1/2017
2
Supporting Physiologic Birth
“Nature does not hurry, yet everything is accomplished.”
~Lao Tzu
Normal Physiology of Second Stage of Labor:
• Latent phase:
• “Resting phase”
• Lull in contractions for 20-30 minutes
• Not experienced by all laboring women
• Active phase:
• Contractions resume
• Often more intense
• Involuntary urge to push
• Fetal descent
(Simkin & Ancheta, 2011)
Ferguson Reflex • Involuntary pushing
• Caused by positive feedback loop: • Cervical and vaginal stretching
• Increased oxytocin release
• Occurs when fetal head is at 0 to +1 station
http://intranet.tdmu.edu.ua/data/kafedra/internal/ginecology2/classes_stud/en/nurse/bsn/ptn/4/Nursing%20Care%20of%20Childbearing%20Family_Practicum/16.%20Labor%20and%20birth%20process..files/image006.gif
2/1/2017
3
Physiology of closed-glottis (Valsalva) pushing
• Venous return and CO decreases
• Maternal arterial BP decreases then elevates suddenly
• Maternal O2 saturation and placental blood flow decreases
• Maternal CO2 increases
• Lactic acidosis begins to develop
• Vaginal canal and pelvic musculature is distended rapidly
• Oxygen available to the fetus is decreased
Maternal-
• Increased perineal trauma
• Structural and/or neurologic injury to the pelvic floor
Fetal-
• Increased non-reassuring fetal heart rate patterns
• Lower APGAR scores
• Fetal acidemia
With prolonged breath holding and straining: May lead to:
(Roberts & Hanson, 2007; Simkin & Ancheta, 2011)
Spontaneous Undirected Pushing
• AWHONN Perinatal Nursing Quality Measure B:
• Goal: 100%
• Documentation
Definition:
• AWHONN defines spontaneous pushing as “a mother’s response to a natural urge to push or a bearing down effort that comes and goes several times during each contraction. It does not involve timed breath holding or counting to 10.”
(AWHONN,2014)
Spontaneous Undirected Pushing • Woman experiences several urges
to bear down, that last for 5-7 seconds each and breathes several times between pushes.
Benefits:
• Duration, force, and timing of bearing down efforts are directed by the mother.
• Decreases maternal fatigue, active pushing time, and operative delivery, and perineal trauma
Potential Risks:
• Increases second stage total length
2/1/2017
4
EBP Pushing
LITERATURE REVIEW
Pushing/ Bearing down methods for the second stage of labour by Lemos et al, 2015. • Cochrane review:
• 20 studies with total N= 815 of spontaneous vs directed pushing
• 13 studies with total N= 2879 comparing delayed pushing vs immediate pushing with epidural anesthesia.
• Spontaneous vs. Directed:
• No difference in second stage length
• No difference in perineal lacerations and episiotomy
• No difference in neonatal outcomes- APGAR scores, NICU admissions
• Active pushing time lessened by 5 mins for spontaneous pushing group
• Delayed vs. Immediate pushing:
• Second stage increased by 54 min for delayed pushing
• Active pushing decreased by 20 min in delayed pushing group
• Increased intrapartum care cost
• Neonatal outcomes similar except one study reported increased risk of low umbilical cord pH in delayed pushing group
A randomized trial of the effects of coached vs uncoached maternal pushing during the second stage of labor on postpartum pelvic floor structure and function; Schaffer et al, 2004 • Coached N= 67 nulliparous women
• Uncoached N=61 nulliparous women
• Urodynamic indices were negatively affected in the coached group
• First urge to void significantly decreased
• Bladder capacity decreased
• Trend towards detrusor over-activity
2/1/2017
5
A randomized controlled trial comparing the physiological and directed pushing on the duration of the second stage of labor, the mode of delivery and Apgar score; Jahdi et al, 2011
• Spontaneous and undirected N=100
• Second stage was shortened 10 min for nulliparas and 7 mins for multiparas
• Closed-glottis, supine, coached immediate pushing (Control) N=91
• No differences in mode of delivery or Apgar scores
Evidence Based Pushing
NURSING IMPLICATIONS
How should we teach pushing?
• Best practices show that we actually shouldn’t “teach” it at all.
“Do what comes naturally.”
• Best maternal and fetal outcomes occur when pushing efforts are:
• Spontaneous
• Un-Directed
• Open-glottis
(AWHONN, 2014;Roberts & Hanson, 2007; Simkin & Ancheta, 2011)
2/1/2017
6
Nursing Implications • Wait for woman’s report of sensation of pressure or need to push
prior to initiation of active pushing
• Assist woman to remain up-right, gravity-neutral positions
• Encourage grunting, groaning, or vocalization during pushing
• Provide information and feedback as encouragement
• “ You’re moving the baby.”
• “That’s it. That’s the right spot.”
• “Good job.”
• “I see her/his head.”
• Avoid directing pushing efforts if fetal descent is evident
• Do not say:
• “Harder.” “Longer.” “Mas forte” or “Forte”
• “Hold your breath and bear down.”
• “Push here.” (AWHONN, 2014;Roberts & Hanson, 2007; Simkin & Ancheta, 2011)
ACOG Recommendations to Reduce Intervention • When not coached to breathe in a
specific way, women push with an open glottis. In consideration of the limited data regarding outcomes of spontaneous versus Valsalva pushing, each woman should be encouraged to use the technique that she prefers and is most effective for her.
• In the absence of an indication for expeditious delivery, women (particularly those who are nulliparous with epidural analgesia) may be offered a period of rest of 1–2 hours (unless the woman has an urge to bear down sooner) at the onset of the second stage of labor.
https://www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Obstetric-Practice/Approaches-to-Limit-Intervention-During-Labor-and-Birth
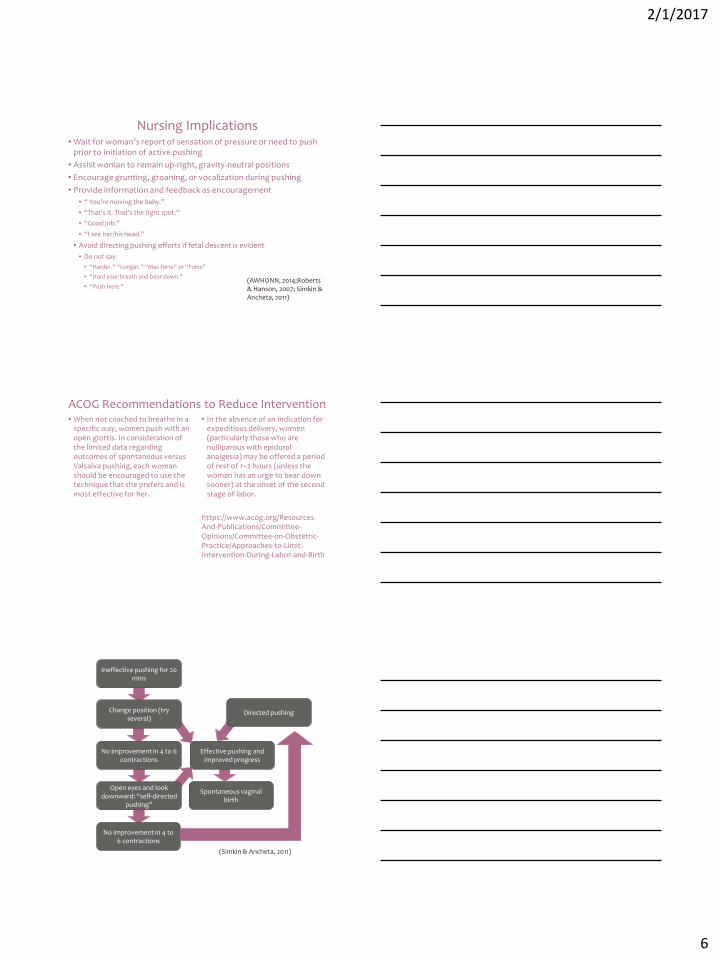
Spontaneous vaginal birth
Effective pushing and improved progress
Directed pushing
Ineffective pushing for 20 mins
Change position (try several)
No improvement in 4 to 6 contractions
No improvement in 4 to 6 contractions
Open eyes and look downward: “self-directed
pushing”
(Simkin & Ancheta, 2011)
2/1/2017
7
Additional Learning: • Labor Progress Handbook by Penny Simkin
• ACOG Committee Opinion 687 Approaches to Limit Intervention During Labor and Birth
• www.evidencebasedbirth.org
To resolve or prevent labor dystocia
POSITIONING TECHNIQUES
Labor Progress
• 6 ways to progress in labor:
• Cervix moves from posterior to anterior
• Ripening
• Effacement
• Dilation
• Fetal rotation, and molding
• Fetal descent
• 4 “Ps” that affect labor:
• Passageway
• Passenger
• Powers
• Psyche
(Simkin & Ancheta, 2011)
2/1/2017
8
Causes of prolonged labor • Passenger: • CPD/ macrosomia
• Malpositioning
• Asynclitism
• OP
• Deflexed head
• Passageway: • CPD
• Powers: • Inadequate uterine intensity or
frequency
• Psyche: • Fear
• Exhaustion
• Iatrogenic:
• Dehydration
• Restriction of movement
• Epidural anesthesia
• Relaxation of pelvic floor
• Inhibition of Ferguson Reflex
(Simkin & Ancheta, 2011)
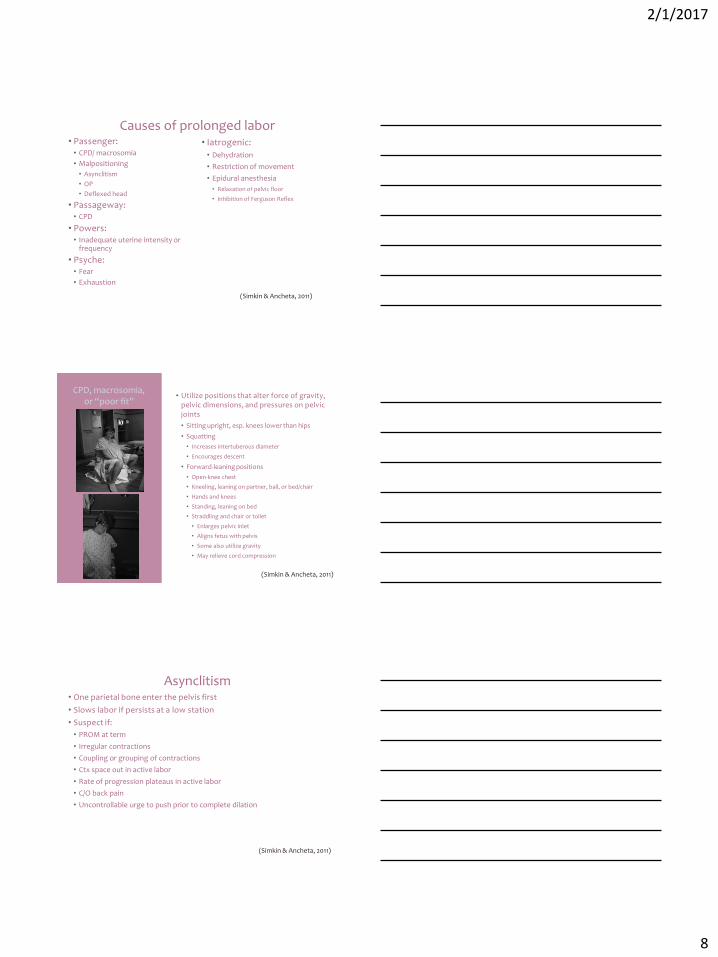
CPD, macrosomia, or “poor fit”
• Utilize positions that alter force of gravity, pelvic dimensions, and pressures on pelvic joints
• Sitting upright, esp. knees lower than hips
• Squatting
• Increases intertuberous diameter
• Encourages descent
• Forward-leaning positions
• Open-knee chest
• Kneeling, leaning on partner, ball, or bed/chair
• Hands and knees
• Standing, leaning on bed
• Straddling and chair or toilet
• Enlarges pelvic inlet
• Aligns fetus with pelvis
• Some also utilize gravity
• May relieve cord compression
(Simkin & Ancheta, 2011)
Asynclitism • One parietal bone enter the pelvis first
• Slows labor if persists at a low station
• Suspect if:
• PROM at term
• Irregular contractions
• Coupling or grouping of contractions
• Ctx space out in active labor
• Rate of progression plateaus in active labor
• C/O back pain
• Uncontrollable urge to push prior to complete dilation
(Simkin & Ancheta, 2011)
2/1/2017
9
http://intranet.tdmu.edu.ua/data/kafedra/internal/ginecology2/classes_stud/en/nurse/adn/ptn/2/Nursing%20Care%20of%20Childbearing%20Family/02.%20Unit%20test%20II.htm
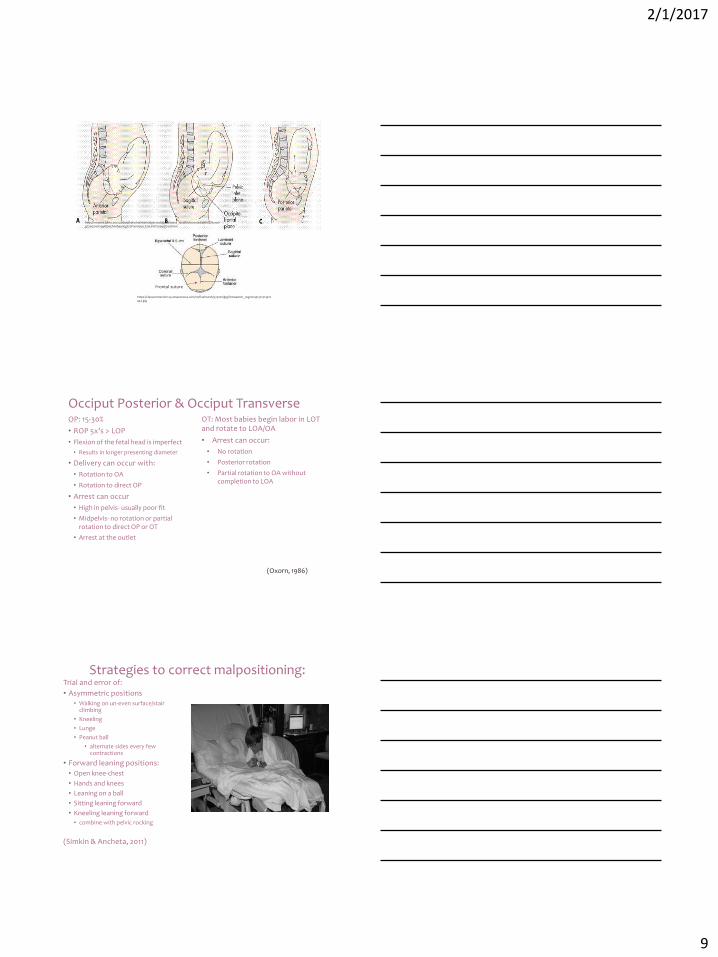
Frontal suture
https://classconnection.s3.amazonaws.com/20/flashcards/573020/jpg/fotosearch_cog120441321414422442.jpg
Occiput Posterior & Occiput Transverse OP: 15-30%
• ROP 5x’s > LOP
• Flexion of the fetal head is imperfect
• Results in longer presenting diameter
• Delivery can occur with:
• Rotation to OA
• Rotation to direct OP
• Arrest can occur
• High in pelvis- usually poor fit
• Midpelvis- no rotation or partial rotation to direct OP or OT
• Arrest at the outlet
OT: Most babies begin labor in LOT and rotate to LOA/OA
• Arrest can occur:
• No rotation
• Posterior rotation
• Partial rotation to OA without completion to LOA
(Oxorn, 1986)
Strategies to correct malpositioning: Trial and error of:
• Asymmetric positions • Walking on un-even surface/stair
climbing
• Kneeling
• Lunge
• Peanut ball
• alternate sides every few contractions
• Forward leaning positions:
• Open knee-chest
• Hands and knees
• Leaning on a ball
• Sitting leaning forward
• Kneeling leaning forward
• combine with pelvic rocking
(Simkin & Ancheta, 2011)
2/1/2017
10
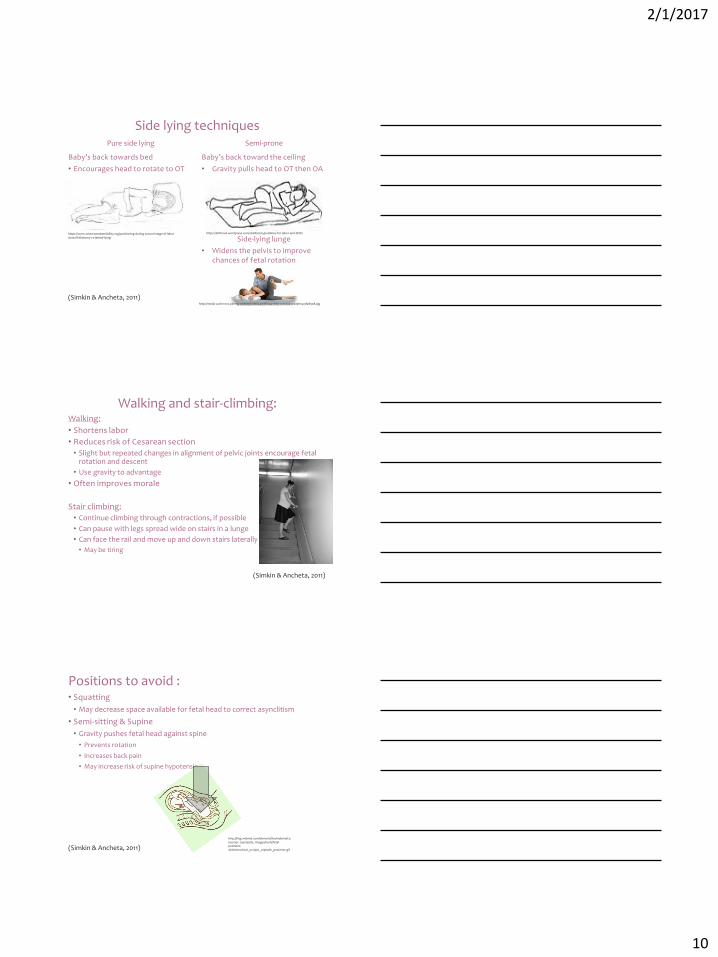
Side lying techniques
Baby’s back towards bed
• Encourages head to rotate to OT
Baby’s back toward the ceiling
• Gravity pulls head to OT then OA
Side-lying lunge
• Widens the pelvis to improve chances of fetal rotation
Pure side lying Semi-prone
https://www.scienceandsensibility.org/positioning-during-second-stage-of-labor-dorsal-lithotomy-vs-lateral-lying/
http://media-cache-ec0.pinimg.com/236x/66/44/3f/66443fd531c0b49432da9fe4c9fa8908.jpg
https://birthowl.wordpress.com/2008/02/15/positions-for-labor-and-birth/
(Simkin & Ancheta, 2011)
Walking and stair-climbing: Walking:
• Shortens labor
• Reduces risk of Cesarean section
• Slight but repeated changes in alignment of pelvic joints encourage fetal rotation and descent
• Use gravity to advantage
• Often improves morale
Stair climbing:
• Continue climbing through contractions, if possible
• Can pause with legs spread wide on stairs in a lunge
• Can face the rail and move up and down stairs laterally
• May be tiring
(Simkin & Ancheta, 2011)
Positions to avoid : • Squatting
• May decrease space available for fetal head to correct asynclitism
• Semi-sitting & Supine
• Gravity pushes fetal head against spine
• Prevents rotation
• Increases back pain
• May increase risk of supine hypotension
http://img.webmd.com/dtmcms/live/webmd/consumer_assets/site_images/tools/fetal-positions-slideshow/tool_occiput_cephalic_posterior.gif (Simkin & Ancheta, 2011)
2/1/2017
11
Immobility and ineffective contractions: Ineffective contractions: • Walking and upright positions
• Upright positions with knees lower than hips
• Consider exhaustion
Immobility: • Rollover sequence: if no malposition is suspected
• Avoid positions not tolerated by woman or fetus
• Move every 20-30 mins through: • Semi-sitting
• Left side-lying • Left semi-prone
• Hands and knees
• Right semi-prone • Right side-lying
• Repeat (Simkin & Ancheta, 2011)
Exhaustion: • May cause ineffective contractions through lactic acid accumulation
in myometrial cells.
• Positions to allow rest and progression:
• Hydrotherapy
• Hands & knees
• Kneeling
• Side-lying
• Semi-prone
• Supported leaning- sitting, kneeling or standing
• Semi-sitting
(Simkin & Ancheta, 2011)
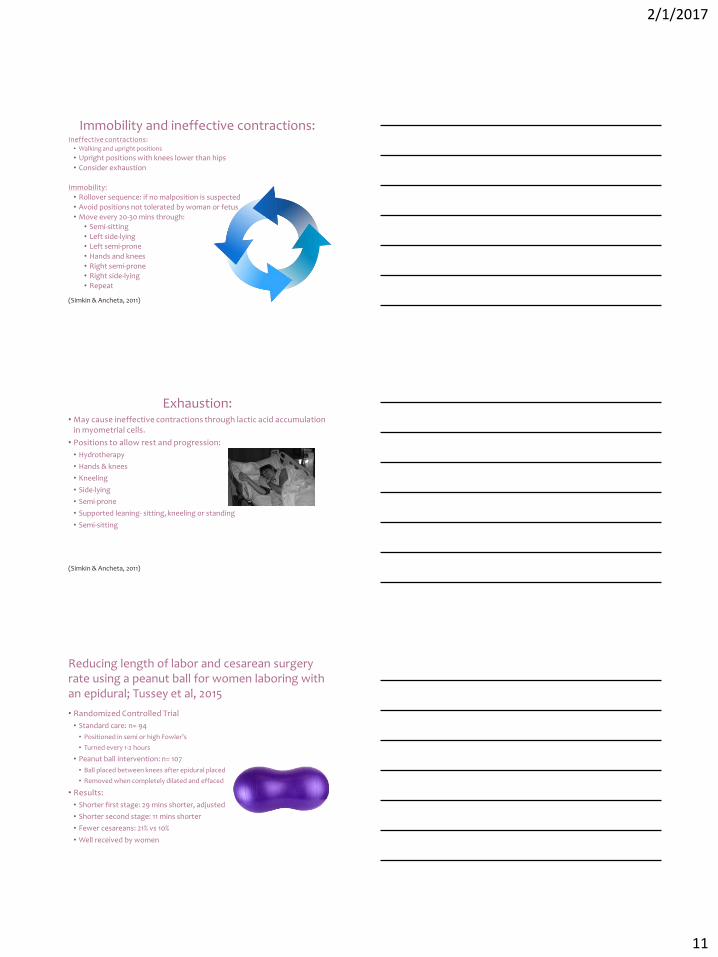
Reducing length of labor and cesarean surgery rate using a peanut ball for women laboring with an epidural; Tussey et al, 2015
• Randomized Controlled Trial
• Standard care: n= 94
• Positioned in semi or high Fowler’s
• Turned every 1-2 hours
• Peanut ball intervention: n= 107
• Ball placed between knees after epidural placed
• Removed when completely dilated and effaced
• Results:
• Shorter first stage: 29 mins shorter, adjusted
• Shorter second stage: 11 mins shorter
• Fewer cesareans: 21% vs 10%
• Well received by women
2/1/2017
12
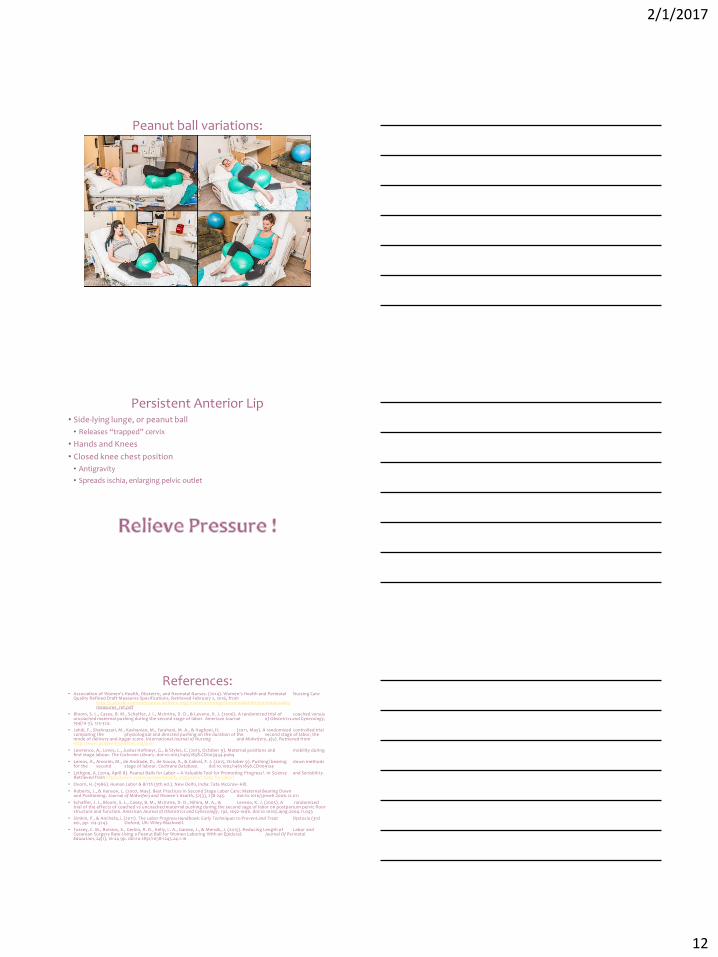
Peanut ball variations:
Persistent Anterior Lip • Side-lying lunge, or peanut ball
• Releases “trapped” cervix
• Hands and Knees
• Closed knee chest position
• Antigravity
• Spreads ischia, enlarging pelvic outlet
References: • Association of Women's Health, Obstetric, and Neonatal Nurses. (2014). Women's Health and Perinatal Nursing Care
Quality Refined Draft Measures Specifications. Retrieved February 2, 2016, from http://c.ymcdn.com/sites/www.awhonn.org/resource/resmgr/Downloadables/perinatalquality measures_ref.pdf
• Bloom, S. L., Casey, B. M., Schaffer, J. I., McIntire, D. D., & Leveno, K. J. (2006). A randomized trial of coached versus uncoached maternal pushing during the second stage of labor. American Journal of Obstetrics and Gynecology, 194(10-3), 124-324.
• Jahdi, F., Shahnazari, M., Kashanian, M., Farahani, M. A., & Haghani, H. (2011, May). A randomized controlled trial comparing the physiological and directed pushing on the duration of the second stage of labor, the mode of delivery and Apgar score. International Journal of Nursing and Midwifery, 3(5). Retrieved from http://www.academicjournals.org/ijnm
• Lawrence, A., Lewis, L., Justus Hofmeyr, G., & Styles, C. (2013, October 9). Maternal positions and mobility during first stage labour. The Cochrane Library. doi:10.1002/14651858.CD003934.pub4
• Lemos, A., Amorim, M., de Andrade, D., de Souza, A., & Cabral, F. J. (2015, October 9). Pushing/ bearing down methods for the second stage of labour. Cochrane Database. doi:10.1002/14651858.CD009124
• Lythgoe, A. (2014, April 8). Peanut Balls for Labor – A Valuable Tool for Promoting Progress?. In Science and Senisbility. Retrieved from https://www.scienceandsensibility.org/peanut-balls-for-labor/
• Oxorn, H. (1986). Human Labor & Birth (5th ed.). New Delhi, India: Tata McGraw-Hill.
• Roberts, J., & Hanson, L. (2007, May). Best Practices in Second Stage Labor Care: Maternal Bearing Down and Positioning. Journal of Midwifery and Women's Health, 52(3), 238-245. doi:10.1016/j.jmwh.2006.12.011
• Schaffer, J. I., Bloom, S. L., Casey, B. M., McIntire, D. D., Nihira, M. A., & Leveno, K. J. (2005). A randomized trial of the effects of coached vs uncoached maternal pushing during the second sage of labor on postpartum pelvic floor structure and function. American Journal of Obstetrics and Gynecology, 192, 1692-1696. doi:10.1016/j.ajog.2004.11.043
• Simkin, P., & Ancheta, i. (2011). The Labor Progress Handbook: Early Techniques to Prevent and Treat Dystocia (3rd ed., pp. 124-324). Oxford, UK: Wiley-Blackwell.
• Tussey, C. M., Botsios, E., Gerkin, R. D., Kelly, L. A., Gamez, J., & Mensik, J. (2015). Reducing Length of Labor and Cesarean Surgery Rate Using a Peanut Ball for Women Laboring With an Epidural. Journal Of Perinatal Education, 24(1), 16-24 9p. doi:10.1891/1058-1243.24.1.16