Embed Size (px)
Citation preview

1 | P a g e
Supplier Agreement for the Provision of Support
to the North West Coast Patient Safety Collaborative
Lot 1 – Board Level Patient Safety and Culture Development
July 2015
2 | P a g e
Supplier Agreement for the Provision of Support to the North West Coast Patient Safety Collaborative
1. Introduction and Background Page 3 2. Purpose and Scope of this Document Page 3 3. Agreement Process Page 4 4. Agreement Conditions Page 4 5. Instructions to Applicants Page 4 6. Appendices
6a Evaluation Criteria Page 5
6b Format of Agreement Page 5
6c Conditions of Contract Page 6
6d Statement of Requirements – General Page 6
6e Specific Requirements Page 7
Appendix 1 - National Patient Safety Collaborative Programme Page 9 Guiding Principles for Local Patient Safety Collaboratives Appendix 2- Criteria Weighting Page 16 Appendix 3- About the NWC AHSN Page 17
3 | P a g e
1. Introduction and Background
The Francis and Berwick reports dealt with high profile failings in safety and quality within the NHS. Working as part of the National Patient Safety Collaborative Programme, 15 Patient Safety Collaboratives (PSCs) were established during 2014/15, each led by an AHSN to deliver a system-wide, locally owned and delivered improvement programme in response to national concerns about safety and quality. The aim of the PSC is to bring together patients and carers, national and international safety expertise with practical experience, in partnership with NHS England, NHS Improving Quality, and other national, international and local bodies interested in improving safety. This work will closely align with and complement the ambitions of the recently launched ‘Sign up to Safety’ campaign. The NWC AHSN has worked with its colleague organisations and national level bodies to identify a number of key priorities for the NWC PSC. The NWC PSC’s clinical priorities are:-
Medicines Optimisation
Management of Sepsis
Transition between paediatric and adult care
Hydration- including acute kidney injury It has also identified the following priorities for action:-
Providing Board level development in safety
Providing safety training and development to staff working at patient care level
Setting up learning networks around safety improvement themes
Developing safety champions or leads in each organisation
Technology reviews to identify solutions to safety issues
2. Purpose and Scope of this Document This document describes, at 6e one Patient Safety Collaborative function – Board level Patient Safety and
Culture Development against which the NWC AHSN seeks proposals. Applicants are invited to submit fully - costed proposals for an assumed level of activity so that the AHSN can determine the volume of service it seeks to purchase. 3. Agreement Process Proposals should be submitted by email, to
Dr Liz Mear Chief Executive North West Coast Academic Health Science Network c/o [email protected]
The applicant is responsible for ensuring that their proposal is received in the AHSN by 17:00 on Monday 17 August 2015. [email protected]
4 | P a g e
4. Agreement Conditions The contract between the NWC AHSN and the successful applicant(s) will commence following appointment and to be completed before May 2016. The NWC AHSN reserves the right to issue additional conditions to the contract extension if performance in the first period is not wholly satisfactory but the AHSN wishes to retain the services of the provider concerned. 5. Instructions to Applicants
Applicants are, within the conditions described below, free to submit their proposals against the Statement of Requirements at 6e in any format which conforms to usual public sector business practice. The following conditions must be observed:-
Submit a single copy of any proposal by email.
Submit the proposal in accordance with part 3 above.
Submit a single document detailing the proposal – do not include attachments or appendices, and do no refer the reader to separate or external sources of reference.
Indicate your recommended response to the function(s) in terms of volume and cost (e.g. provide 3 days “Safety insight” training for 150 clinical staff at band 7 or below at a cost of £175 per attendee).
State clearly which elements of the provider’s costs are subject to VAT or other charges and whether VAT or other charges have been added to the stated costs. For the avoidance of doubt, any costs without such clarity will be assumed to include any and all VAT charges at the prevailing rate.
Include all associated charges and resource requirements in any submitted costing. This might include, but is not limited to travel expenses; venue hire; speaker fees; validation costs; and so on. It will not be possible to reimburse such commitments retrospectively if they were not included in the original proposal.
Any queries about the Agreement should be addressed to the AHSN via the following email address: – [email protected], with “Patient Safety Collaborative” as the subject heading. In the interests of transparency and probity, all such queries, and the response of the AHSN to them, will be shared with all relevant applicants (i.e. generic queries with all applicants, function specific queries with any other applicant producing a proposal against the same function).
5 | P a g e
6. Appendices
6a. Evaluation Criteria The NWC AHSN will apply “best-fit” criteria to each proposal, awarding weighted marks against
- Degree to which the proposal reflects the stated requirements (6e) and the ethos of the Patient Safety Collaboratives
- Evidence that the applicant organisation can scale up to deliver against the selected function(s)
- Evidence that the proposal has the capacity to deliver specific, tangible and
meaningful outcomes at a scale and level of impact consistent with the level of resource allocated
- The extent to which the proposal exploits proven, evidence based approaches to change, improvement etc.
- The extent to which the proposal provides a model which will lead to measurable
outcome evaluation and replication in other contexts. A table summarising how the AHSN will weight each criterion is attached and Appendix 2. 6b. Format of Agreement As noted at section 5, applicants are, within the conditions described there, free to submit their proposals against the Statement of Requirements at 6e electronically in any style or format which conforms to usual public sector business practice. The Agreement will take the form of a formal contract with an agreed pricing structure. The contract will be formally let by NWC AHSN’s host organisation, Lancashire Care NHS Foundation Trust. Applicants may submit a proposal for one, two or three functions, and/or specific parts of individual functions so long as the proposal makes clear which combination has been selected. Applications can come from single or combined organisations, though in the case of combined organisations, the NWC AHSN will wish to have a lead organisation identified to it. This will be the organisation with which the NWC AHSN will conduct discussions about performance, finance and any other aspect of the contract. Single or combined organisations are also at liberty to source provision from third party providers. NWC AHSN does not expect to be directly involved in the selection of such parties, but will seek an assurance that they are reputable, solvent, fit for purpose, appropriately constituted and governed and, as far as can be determined will not bring the AHSN or its partners into disrepute.
6 | P a g e
6c. Conditions of Contract The contract will be formally let by NWC AHSN’s host organisation, Lancashire Care NHS Foundation Trust and will conform to NHS Business Standards. Any special considerations or variations agreed between the NWC AHSN and any of its providers will, as far as possible, be incorporated into the main contract. If this is not possible, any variations will be agreed and documented separately. Representatives of the AHSN will meet with all providers to agree the content of the contract. 6d. Statement of Requirements
General
6di Proposals are invited for the provision of specific items of support to the North West Coast AHSN in relation to developing leadership capability programme for Patient Safety and
Culture Development.
6dii The AHSN invites proposals against the specific element identified below from individual or collaborating bodies.
6diii It is essential that submitted proposals are consistent with both the current “Guiding Principles for Local Patient Safety Collaboratives” (see Appendix 1) and the philosophy, working methods, and wider priorities and objectives of the NWC AHSN (see NWC AHSN Business Plan, 2015 at www.nwcahsn.nhs.uk).
6div Recognising that the support provided will be at least in part organisational and practical in nature, it is also essential that all proposals reflect the need to build and develop a positive safety culture within organisations and across the North West Coast region as a whole. 6dv The Appended “Guiding Principles” identify the importance of “ensuring patients and carers play a fundamental and active part in planning”. The AHSN will expect all applicants to reflect this requirement in their proposal(s) and for the successful applicants to work collaboratively with the AHSN/PSC’s structures for patient, carer and community engagement, as well as with its partners in the academic sector, as appropriate. 6dvi In their proposals, applicants should also give a firm cost of the services they will provide to meet the NWC AHSN’s requirements, including VAT and all other charges, where appropriate. This can be expressed as a unit cost, on a cost and volume or sliding scale basis, and so on – it should enable the AHSN to determine what volume of service it may commission from the applicant.
7 | P a g e
6e Specific Requirements Building Safety Leadership Capacity and Capability -Board1 Level Patient Safety and Culture Development
The NWC AHSN seeks support in developing the capacity and capability for safety improvement and leadership at Board/senior level. The aim is to build and develop a positive safety culture within organisations and across the North West Coast region through collaboratives.
The NWC AHSN’s specific requirements are as follows:- - Provide a Board development programme – to include:
I. A whole system approach to develop individuals working at Board Level to create several patient safety collaboratives across individual localities. The collaboratives to include Commissioners (e.g. CCGs, Local Authority, NHS England) Providers (e.g. Ambulance Services, Mental Health & Learning Disabilities, Acute, Community, Primary Care, Social and Adult Care) and patient representative organisations (e.g. CEO HealthWatch). Collaboratives to be aligned with commissioning and strategic plans to represent the whole health and care delivery system.
II. Defining and aligning the programme in relation to “Seven Steps to Patient Safety” (NPSA 2004, 2008, 2009) undertaking a gap analysis against each step and developing a plan for improvement.
III. Defining and understanding risk, harms, safety, safety management systems including human factors and error, open and transparent care, quality and improvement methodology.
IV. Exploring safety and innovation– learning from industry and the use of technology to improve safety.
V. Interpreting and triangulating data from multiple sources to understand how safe the organisation is. Aligning with the NWC AHSN PSC patient safety measurement strategy, supporting organisations to develop their own safety measurement strategy , dashboard and surveillance.
VI. Aligning with NWC AHSN PSC business plan in relation to, capability building, staff health and wellbeing, care home safety and the four clinical safety priorities.
VII. Undertaking safety culture baseline assessment, developing an action plan and building in systems for monitoring progression.
VIII. Developing, implementing and monitoring safety improvement plans using improvement methodology to improve safety across systems and aligned to “Sign up to Safety”. Plans should address workforce factors e.g. health and wellbeing.
IX. Site visits to support and coach participants. X. Agreeing a model of resilience and sustainability within the collaborative including
working with the NWC AHSN PSC and signing up to a joint pledge for safety across the NWC footprint.
- Work with the NWC AHSN PSC to agree timelines, - deliverables and programme outcomes. - Work with the NWC AHSN PSC to promote and publish specific programme outcomes
which includes baseline line assessment to demonstrate programme impact and improvement.
- Co-ordinate local work with the NHS Leadership Academy who will continue to deliver their national safety programmes.
- Ensure the appropriate links are made and maintained with national initiatives including the Q initiative.
1 Board level to include equivalent level for CCGs and Local Authority

8 | P a g e
- Work with the NWC AHSN PSC to focus on organisations who have not been involved in similar programmes or where the proposal can add value and impact across the system.
- Work with AHSNs who will be delivering national work across patient safety topic ‘clusters’ and NHS IQ who will be delivering improvement training and development to each of AHSN’s footprint.
- Demonstrate evidence-based methods of safety improvement science using relevant methodology to develop outcomes and evaluation for the above programme.
~~ END ~~
9 | P a g e
Appendix 1
National Patient Safety Collaborative Programme
Guiding Principles for Local Patient Safety Collaboratives
Purpose of this paper
1. This document describes the proposed principles upon which the Patient Safety Collaborative Programme will be based and in particular the proposed principles against which each Academic Health Science Networks (AHSNs) will establish and support the local Patient Safety Collaborative in their area. This draft is a document for discussion between NHS England, NHS Improving Quality and the AHSNs. If necessary it will be amended before a final version, acceptable to all, will be produced to guide the establishment of the Patient Safety Collaboratives
Background to the Programme
2. The NHS has recently been named the safest healthcare system in the world by the influential Washington-based Commonwealth Fund. This is something everyone in the NHS and beyond can be proud of, but the only reason this is the case is because the NHS strives continuously to do the best that it can for the population it serves. The NHS must continue to improve and learn. The need for this is illustrated by the series of challenges the system has faced over the past five years; financial pressures, organisational changes and, most damagingly, repeated reports of failures in the quality and particularly the safety, of care.
3. The NHS should provide people who work across the healthcare system the opportunity to work together in a collaborative way in their own healthcare communities to address and prevent the most significant sources of harm in their services. The NHS should enable them to engage with all levels of the organisations within which they work and help them to connect with widespread support outside their organisations to underpin their systematic improvement efforts to prevent and learn from errors, reduce avoidable harm and create safer systems of care.
4. Working as part of the National Patient Safety Collaborative Programme, the Patient Safety Collaboratives each established and supported by an AHSN will deliver a system-wide, locally owned and led, improvement programme. This will bring together patients and carers, national and international safety expertise with practical experience, in partnership with NHS England, NHS Improving Quality, and other national, international and local bodies interested in improving safety. This work will align with and complement the ambitions of the recently launched ‘Sign up to Safety’ campaign.
10 | P a g e
Overarching principles and scope of the Programme
5. In order to work towards significant cultural change and to create a continuous learning system across health and social care, the overarching principles of the work will include:
Local engagement through structured quality improvement initiatives leading towards transformational change
Building system-wide capability for both staff and patients in quality and safety improvement
Local systematic spread of quality improvement outcomes across health and social care
Networking between the AHSNs and their partner organisations and stakeholders to ensure the optimal spread of locally developed solutions & interventions
Active contribution to national sharing and learning
6. Patient safety as a concept needs to be clearly defined in order to understand the scope and remit of
the Patient Safety Collaboratives work. Patient safety is the avoidance or prevention of unintended or
unexpected harm during the provision of healthcare. It is concerned with preventing errors of
commission (doing the wrong thing) and errors of omission (failure to do the right thing). ‘Harm’ in this
context means injury, suffering, disability or death of a patient where that is not an expected part of the
process of the disease the patient has or the expected consequence of the healthcare they are being
provided with. While some patient safety incidents involve individual and clearly defined errors that lead
directly to harm, we know that most of the harm caused by healthcare is a consequence of multiple,
relatively minor errors that accumulate to have significant consequences. The work of the patient safety
collaboratives will encompass both these scenarios in order to support the creation of the conditions
that prevent patient safety incidents from occurring in the first place and that support the development
of a safety culture in the NHS.
7. The Patient Safety Collaboratives themselves will be encouraged to be innovative about the methods
they use to drive improvement and prevention of harm, although they will be expected to demonstrate
that their chosen methods of safety improvement and harm prevention are evidence-based. Local
Collaboratives will be encouraged to build upon existing initiatives or instigate new areas of work. It is
anticipated that work will take a practical approach to pathway redesign, employing a range of quality
improvement tools and techniques currently available – and importantly, explore in detail what ‘really’
works, and what does not, for the benefit of others, building a measurable and sustainable system for
the spread of good practice across health and social care that prevents things from going wrong.
8. However, in order to aspire to the level of change required for a cultural shift in how care is delivered,
the national programme will be drawing on expertise around ‘operational excellence’ that will underpin
this work, and surpasses primary pathway redesign that has been seen within traditional quality
improvement. As outlined in the Berwick Report, (August 2013) capability will need to be built around
the following areas:
Transparency
Continuous learning
Prevention
Reliability
Leadership for culture change
Improvement and measurement
Accountability
Teamwork and communication
Negotiation
11 | P a g e
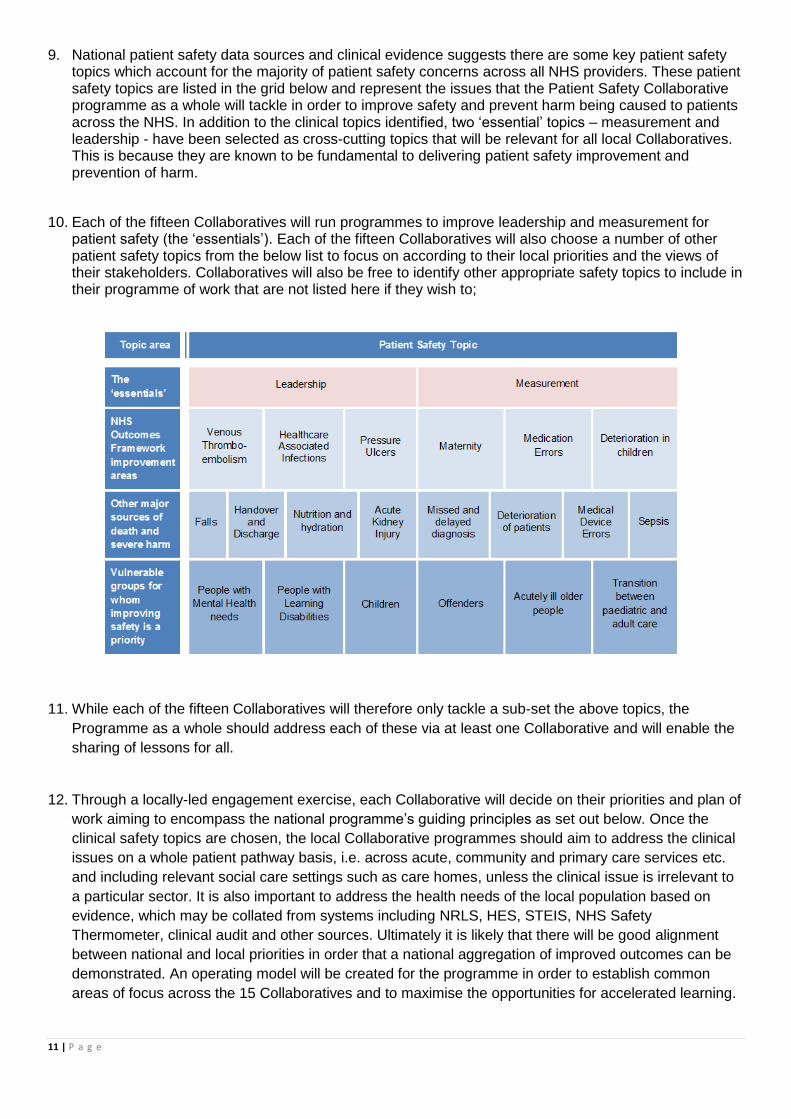
9. National patient safety data sources and clinical evidence suggests there are some key patient safety topics which account for the majority of patient safety concerns across all NHS providers. These patient safety topics are listed in the grid below and represent the issues that the Patient Safety Collaborative programme as a whole will tackle in order to improve safety and prevent harm being caused to patients across the NHS. In addition to the clinical topics identified, two ‘essential’ topics – measurement and leadership - have been selected as cross-cutting topics that will be relevant for all local Collaboratives. This is because they are known to be fundamental to delivering patient safety improvement and prevention of harm.
10. Each of the fifteen Collaboratives will run programmes to improve leadership and measurement for patient safety (the ‘essentials’). Each of the fifteen Collaboratives will also choose a number of other patient safety topics from the below list to focus on according to their local priorities and the views of their stakeholders. Collaboratives will also be free to identify other appropriate safety topics to include in their programme of work that are not listed here if they wish to;
11. While each of the fifteen Collaboratives will therefore only tackle a sub-set the above topics, the
Programme as a whole should address each of these via at least one Collaborative and will enable the
sharing of lessons for all.
12. Through a locally-led engagement exercise, each Collaborative will decide on their priorities and plan of
work aiming to encompass the national programme’s guiding principles as set out below. Once the
clinical safety topics are chosen, the local Collaborative programmes should aim to address the clinical
issues on a whole patient pathway basis, i.e. across acute, community and primary care services etc.
and including relevant social care settings such as care homes, unless the clinical issue is irrelevant to
a particular sector. It is also important to address the health needs of the local population based on
evidence, which may be collated from systems including NRLS, HES, STEIS, NHS Safety
Thermometer, clinical audit and other sources. Ultimately it is likely that there will be good alignment
between national and local priorities in order that a national aggregation of improved outcomes can be
demonstrated. An operating model will be created for the programme in order to establish common
areas of focus across the 15 Collaboratives and to maximise the opportunities for accelerated learning.
12 | P a g e
13. The central core team of NHS Improving Quality and the NHS England Patient Safety Domain team
clinical leads will work with the network of AHSNs and individual AHSNs and other safety improvement
experts to provide support, guidance, expertise and resources in relation to these clinical priorities to
support the work of the Patient Safety Collaboratives. The core team will also seek to spread best
practice between Collaboratives where effective solutions are identified and evidenced, both for the
clinical areas on this list and others as identified by local Collaboratives. A centrally accessible web
resource will ensure these resources are made available to each local Collaborative.
The Guiding Principles in detail
14. It is anticipated that each AHSN will lead on the establishment and support a local patient safety
Collaborative within their geographical footprint. While providers remain accountable for the safety of
their patients, accountability for delivering an effective collaborative programme that abides by the
principles in this document and that supports patient safety improvement and prevention of harm will lie
with each respective AHSN’s leadership.
15. The key steps required to establish each local Collaborative will therefore include:
Local engagement across health and social care to scope plans and recruit organisations
Establishment of a local patient safety collaborative and associated governance structure
Local identification of key safety priorities
Development of a locally agreed plan of work
Establishment of a measurement and reporting structure which encompasses prevention and future avoidance of harm.
16. The guiding principles are outlined within two distinct stages of activity. The Stage 1 principles will guide
the ‘work before the work’, in terms of the initial set up phase that will take place in the run up to
October 2014. The stage 2 principles will guide the ongoing operation of the Collaboratives from
October onwards.
Stage 1 – up to October 2014
i. Agreement of each AHSN to mobilise local engagement across all sectors - providers and
commissioners and including non-acute and social care organisations, to establish a local patient
safety collaborative programme.
ii. Identifying key patient safety challenges and opportunities locally, including gathering evidence of
any work already undertaken to improve patient safety (potentially as part of other local or national
improvement initiatives) and subsequent examples of good practice and using evidence of current
patient safety improvement capability across participating organisations to ensure the Patient Safety
Collaborative will complement rather than compete with existing initiatives.
iii. Ensuring patients and carers play a fundamental and active part in planning.
iv. Baselining relevant data across the whole system
v. Obtaining the explicit engagement of chief executives, boards and other leaders from participating organisations, including their commitment to support and engage in meaningful improvement activity within and between their organisations.
vi. Obtaining agreement that individual leads from member organisations will commit to attend to
relevant learning sessions and national events.
vii. Obtaining data sharing agreements across the Collaboratives and national team.
13 | P a g e
viii. Signalling full support for the process of real time, formative evaluation and commitment to respond to relevant findings in order to ensure timely enhancement of the programme.
ix. Inclusion of both the leadership and measurement topics as cross-cutting themes of work across all Patient Safety Collaboratives.
x. Establishing a local governance structure for local Collaborative oversight on progress, and learning
by October 2014 – from project based steering groups to AHSN Patient Safety Collaborative
boards.
xi. Developing an overarching local Patient Safety Collaborative work plan by October 2014, including
clear aims, objectives and strategic delivery plans, and a set of measurable objectives that align
with the national programme measurement strategy which will be developed with AHSNs:
Stage 2 – after October 2014
i. Demonstrating ongoing patient/carer voice and participation in all Patient Safety Collaboratives and
with any other relevant stakeholders.
ii. Demonstrating improvement in patient safety through systematically addressing causes of harm and
developing preventative approaches to safety thereby demonstrating a return on investment.
iii. Demonstrating real progress in safety culture and learning as evidenced through improved
prevention activities, incident reporting and the use of patient safety culture assessment tools.
iv. Supporting, empowering and including staff of all grades, clinical and otherwise across all
participating organisations to build safety improvement capability, and by supporting exceptional
individuals to take part in relevant development opportunities so that safety becomes everyone’s day
job and not a specialist interest subject.
v. Demonstrating the use of evidence-based methods of safety improvement science to deliver safety
objectives with innovation where appropriate.
vi. Underpin all quality improvement work with a set of principles based on ‘operational excellence’ to
ensure more sustainable culture changes and creation of a continuous learning system – this
includes transparency, team work, communications etc. as outlined on page 2.
vii. Ensuring that clinical interventions introduced for patient safety improvement are grounded in the
evidence base for effectiveness.
viii. Delivering effective communication initiatives to build safety awareness, energy and participation
based upon the wider national programme communications strategy and linking with the ‘Sign up to
Safety’ campaign.
ix. Delivering a cohesive strategy and plans for adoption and spread of the work and learning across all
NHS-funded providers, relevant social care providers and commissioners in the geographical area
within five years.
x. Legitimately reporting the gains where improvement is measurable, and sharing knowledge, case
studies, stories and innovative practice, not just data.
17. It is a fundamental principle of the Programme that we will not dictate to Patient Safety Collaboratives
how they design and implement their programmes of work to fulfil the principles set out above. AHSNs
and their partners will develop a range of approaches and use a number of management models.
There are, however, several core management capabilities that AHSNs and their partners will need to
have at their disposal. These include:
Leadership and networking skills
Programme and project management
Financial planning
Improvement skills and knowledge
Analytical capability to support measurement for improvement and evaluation
Clinical leadership
Administrative capacity
14 | P a g e
Core Team Support and Benefits of the National Programme
18. NHS IQ and NHS England will provide a central core team to support the programme. The core team will work with each Collaborative to develop an individual support and working arrangements plan. The team will collate monthly data on behalf of each AHSN using existing data collections where possible and will keep additional collections to a minimum necessary to support the tracking of improvement.
19. Organisations actively involved in patient safety improvement work will be supported to use a single
national system as a means for their project management, data capture and analysis, and the sharing
of learning nationally. Discussions will be held with AHSNs to understand their requirements from such
a system and ensure these are met as far as possible.
20. The details of the overarching PSC measurement for improvement strategy will be developed further
with and agreed by the AHSNs.
21. AHSNs will be supported to provide more detailed submissions on a quarterly basis covering progress
on improvement in identified priorities, significant learning, and progress on work specific to
measurement and leadership towards culture and learning system change.
22. Collaboratives will be able to actively participate in the design of workshops and events that will include capability building in quality and safety improvement, peer support meetings and other national events in order to share best practice and learning. They will be supported to actively share locally-developed products and resources for the benefit of others and ensure the whole system is able to learn both in terms of success and failures of specific improvement initiatives.
23. The core team will support the following activities:
i. Working with the AHSN Network of Networks, develop and support the operating model for the national programme.
ii. In partnership with each AHSN, develop and support a system wide capability programme in support of each Patient Safety Collaborative, including measurement capability.
iii. Also in partnership, develop a measurement strategy for the programme in order to demonstrate improvement outcomes and aggregate value.
iv. From the outset and through the diagnostic, implementation and evaluation phases of work, support all Patient Safety Collaboratives through an agreed ‘working arrangements’ plan to meet specific improvement needs.
v. Contribute to the National Patient Safety Programme Board. vi. Work with a variety of stakeholders to ensure access to appropriate expertise within the national
programme. vii. Support all Patient Safety Collaboratives through the use of a single national system that meets the
needs of AHSNs for project management, online collaboration, sharing and local data analysis. viii. Offer a range of patient safety learning opportunities at all levels including leadership, measurement
and operational excellence as core themes. ix. Contribute to the wider NHS England National Patient Safety Plan communications strategy to
promote and support the Patient Safety Collaboratives, and the wider ‘Sign up to Safety’ campaign. x. Support web-based meetings for peer support remote connection and interaction xi. Co-design, organise and deliver workshops and national learning events to support sharing and
learning across the Collaboratives and more widely support the National Patient Safety Programme. xii. Co-produce a range of quality publications and resources using a wide variety of media, in
partnership with stakeholders that focusses on the key evidenced safety improvements principles e.g. ‘how to’, ‘top tips’, guides, e-learning, apps and other resources.
xiii. Build the patient safety evidence base by supporting abstract, peer review and other potential publication submissions.
15 | P a g e
xiv. Provide shared examples of all resources, including policies, procedures and protocols in use in operational settings that are proven to be beneficial.
xv. Provide a quarterly national aggregate report against the agreed programme metrics covering inputs, process, outcomes and balancing measures and demonstrating progress of Patient Safety Collaboratives and provide access to some of the national safety data sources in a format required by AHSNs and associated quality improvement work.
xvi. Commission a programme of research to reflect the wider qualitative aspects of the National Patient Safety Collaborative Programme, in order to capture the aggregate value and the changes in patient and public experience of safety over the lifetime of the Collaboratives.
16 | P a g e
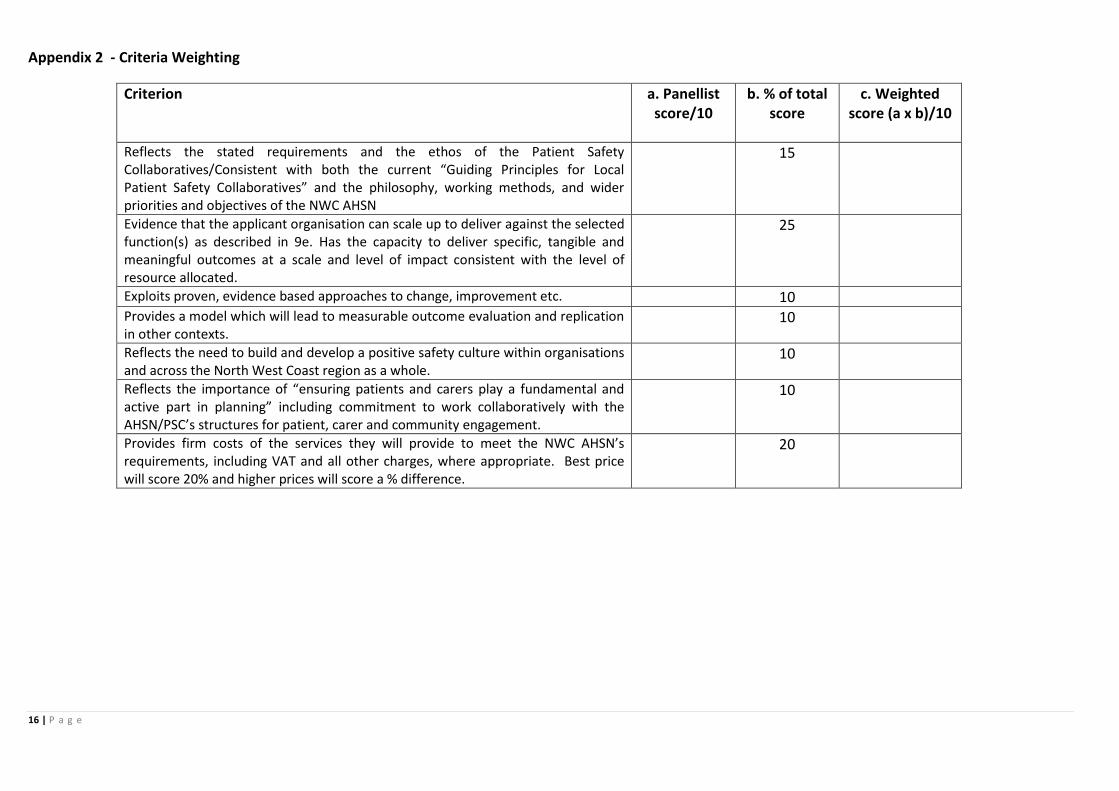
Appendix 2 - Criteria Weighting
Criterion a. Panellist score/10
b. % of total score
c. Weighted score (a x b)/10
Reflects the stated requirements and the ethos of the Patient Safety Collaboratives/Consistent with both the current “Guiding Principles for Local Patient Safety Collaboratives” and the philosophy, working methods, and wider priorities and objectives of the NWC AHSN
15
Evidence that the applicant organisation can scale up to deliver against the selected function(s) as described in 9e. Has the capacity to deliver specific, tangible and meaningful outcomes at a scale and level of impact consistent with the level of resource allocated.
25
Exploits proven, evidence based approaches to change, improvement etc. 10 Provides a model which will lead to measurable outcome evaluation and replication in other contexts.
10
Reflects the need to build and develop a positive safety culture within organisations and across the North West Coast region as a whole.
10
Reflects the importance of “ensuring patients and carers play a fundamental and active part in planning” including commitment to work collaboratively with the AHSN/PSC’s structures for patient, carer and community engagement.
10
Provides firm costs of the services they will provide to meet the NWC AHSN’s requirements, including VAT and all other charges, where appropriate. Best price will score 20% and higher prices will score a % difference.
20
17 | P a g e
Appendix 3 – About the NWC AHSN
The policy initiative for the development of the AHSNs stems from “Innovation Health and Wealth” (DH 2011). The primary purpose of AHSNs is to implement innovation (which in this context refers to clinically proven healthcare innovations being applied for the first time, or in new clinical settings) at “scale and pace”, that is more quickly, and more widely than is currently the case. This requires AHSNs to broker new working relationships between the NHS, academia, industry and other key players. There are 15 AHSNs across England. AHSNs operate as system integrators, drawing together and capitalising on the extensive skills, resources and facilities in the region to accelerate innovation by aligning the priorities and plans of their partners and members in the most effective and efficient way. The North West Coast Academic Health Sector Network (NWCAHSN) has commenced its integration role by building upon established networks and partnerships across the region, including the NIHR CLAHRC NWC, the NIHR Clinical Research Network, Liverpool Health Partners, Lancaster Health Hub, the North West region’s two Strategic Clinical Networks, and the Northern Health Science Alliance. The core aims of the NWC AHSN are to:-
1. Drive and enable access to safe, effective, evidence-informed healthcare for the entire NWC population 2. Drive the development and delivery of advanced treatments, technologies and clinical practice across the NWC to enhance the quality and efficacy of service provision. 3. Attract global investment and generate jobs for the NWC
The NWC AHSN’s area of cover includes Merseyside, Lancashire, Cheshire and South Cumbria, with a resident population in excess of 4 million. It has a very extensive network of organisations, which includes 25 NHS Trusts and Area Teams, 19 Clinical Commissioning Groups and 9 universities, in addition to a range of support, development, engagement and involvement and third sector bodies, and a huge number of industry and trade contacts, ranging from SMEs employing a handful of people through to multi – nationals. For further information about North West Coast AHSN, please visit http://www.nwcahsn.nhs.uk/

![PRE-QUALIFIED - luc.edu Web viewPRE-QUALIFIED SUPPLIER AGREEMENT . This Pre-Qualified Supplier Agreement (the “Agreement”) is made and entered into as of [_____] (the “Effective](https://img.pdfslide.us/doc/110x75/5a7df6a87f8b9a4d628e0f52/pre-qualified-lucedu-viewpre-qualified-supplier-agreement-this-pre-qualified.jpg)



























