Embed Size (px)
Citation preview
Supplementary appendixThis appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors.
Supplement to: Varenne O, Cook S, Sideris G, et al. Drug-eluting stents in elderly patients with coronary artery disease (SENIOR): a randomised single-blind trial. Lancet 2017; published online Nov 1. http://dx.doi.org/10.1016/S0140-6736(17)32713-7.
1
SUPPLEMENTARY APPENDIX 1
2
Table of content: 3
A:SENIORStudyorganisation..................................................................................................................................34
B:Inclusionandexclusioncriteria.......................................................................................................................45
C:Studydevices................................................................................................................................................................56
D:Endpointdefinitions..............................................................................................................................................67
E:Randomisation.........................................................................................................................................................108
F:SupplementaryTablesandFigures..............................................................................................................109
TableS1:Sensitivityanalysesfortheprimaryendpoint(intention-to-treat)........................1110
TableS2:Sensitivityanalysesfortheprimaryendpoint(perprotocol)....................................1211
TableS3:MedicaltreatmentimmediatelyafterbaselinePCI(intention-to-treat)...............1312
TableS4:Targetvesselrevascularisationandnon-targetvesselrevascularisationatone13year(intention-to-treat)..........................................................................................................................................1414
TableS5:Qualityoflife(intention-to-treat)................................................................................................1615
TableS6:DepressionevaluationinelderlypatientsundergoingPCI...........................................1716
FigureS1:KaplanMeierComponentsoftheprimaryendpoint(all-causemortality,17myocardialinfarction,strokeandischemia-driventargetlesionrevascularisation)........1818
FigureS3:Primaryendpointbysubgroups:RelativeRiskwith95%ConfidenceIntervals19(Intention-to-treat).....................................................................................................................................................2020
FigureS4:Primaryendpointbysubgroups:RelativeRiskwith95%ConfidenceIntervals21(Intention-to-treat).....................................................................................................................................................2122
FigureS5:BleedingComplicationsbysubgroups:RelativeRiskwith95%Confidence23Intervals(Intention-to-treat)...............................................................................................................................2224
FigureS6:BleedingComplicationsbysubgroups(cont):RelativeRiskwith95%25ConfidenceIntervals(Intention-to-treat).....................................................................................................2326
FigureS7.MACCEatoneyearaccordingtoage(post-hocanalysis)..............................................2427
FigureS8.Bleedingevents(BARC2-5)accordingtoageat1year(post-hocanalysis)......2528
FigureS9:Timelineofstentthrombosisduringandafterdiscontinuationof29thienopyridinetreatment.......................................................................................................................................2630
FigureS10:IschemiadrivenTLRatoneyearbysubgroups:RelativeRiskwith95%31ConfidenceIntervals(FS)........................................................................................................................................2732
FigureS11:IschemiadrivenTLRatoneyearbysubgroups:RelativeRiskwith95%33ConfidenceIntervals(FS)........................................................................................................................................2834
FigureS12:Durationofdualantiplatelettherapyinpatientswithacutecoronary35syndrome..........................................................................................................................................................................2936
2
FigureS13:Durationofdualantiplatelettherapyinpatientswithstable/silentischemia1.................................................................................................................................................................................................302
G:Authorsaffiliations...............................................................................................................................................313
I:Listofcentresandinvestigators.....................................................................................................................3245
3
A: SENIOR Study organisation 1
2
SENIOR Excecutive Committee Members: 3Olivier Varenne (Hôpital Cochin, Paris, France), Peter Sinnaeve (University Hospitals 4Leuven, Leuven, Belgium), Thomas Cuisset (Hôpital la Timone, Marseille, France), Manel 5Sabate (Hospital Clinic, Barcelona, Spain), Marie-Claude Morice (CERC, Massy, France). 6 7Data Safety Monitoring Board: 8Chairman: Michel Eugene Bertrand (Institut Cœur Poumon de Lille, Lille, France), Jacques 9Berland (Clinique Saint Hilaire, Rouen, France), Ahmed Waqar (King Fahad Armed Forces 10Hospital, Jeddah, Saudi Arabia). 11 12Clinical Events Committee. 13Alaide Chieffo (San Raffaele Hospital, Milan, Italy), Thierry Royer (Centre Cardiologique du 14Nord, Saint Denis, France), Augusto Pichard (Medstar Washington Hospital Center, 15Washington D.C., USA), Bernard Valeix (Marseille, France), Jacques Machecourt 16(University Hospital, Grenoble, France), Jérôme Garot (Institut Cardiovasculaire Paris Sud, 17Massy, France), Laszlo Levai (Hôpital Pasteur, Colmar, France), Carlos Macaya (Hospital 18Clínico San Carlos, Madrid, Spain), José Ramón Rumoroso (Hospital de Galdakao, 19Galdakao, Spain), Valérie Domigo (Hôpital Sainte Anne, Paris, France), Peter Kearney 20(Cork University Hospital, Cork, Ireland), Roxana Mehran (Mount Sinai Hospital, New York, 21USA), Javier Escaned (Hospital Clínico San Carlos, Madrid, Spain). 22 23Data Management: Cardiovascular European Research Center (CERC), Massy, France 24 25IWRS/eCRF: Clinigrid, Paris, France. 26 27Statisticians: 28Ann Belmans (Interuniversity Institute for Biostatistics and Statistical Bioinformatics, KU 29Leuven, Leuven, and University Hasselt, Hasselt, both in Belgium), Kris Bogaerts 30(Interuniversity Institute for Biostatistics and Statistical Bioinformatics, KU Leuven, Leuven, 31and University Hasselt, Hasselt, both in Belgium) 32 33List of Investigators by Country: 34France: Didier Carrié (CHU Toulouse Rangueil, Toulouse, France), Rami El Mahmoud 35(Hôpital Ambroise Paré, Boulogne-Billancourt, France), Christian Spaulding (Hôpital 36Européen Georges Pompidou, Paris, France), Georgios Sidéris (Hôpital Lariboisière, Paris, 37France), Olivier Varenne (Hôpital Cochin, Paris, France), Thomas Cuisset (Hôpital La 38Timone, Marseille, France), Thomas Hovasse (Hôpital Privé Jacques Cartier, Massy, 39France), Philippe Garot (Hôpital Privé Claude Galien, Quincy-sous-Sénart, France), 40Emmanuel Teiger (CHU Henri Mondor, Créteil, France), Gérard Helft (Hôpital de la 41Salpêtrière, Paris, France), Philippe Commeau (Polyclinique les Fleurs, Ollioules, France). 42 43
4
Switzerland: Stéphane Cook (Université de Fribourg, Fribourg, Switzerland), Eric Eeckhout 1(CHUV, Lausanne, Switzerland), Daniel Weilenmann (Kantonsspital St Gallen, St Gallen, 2Switzerland), Florim Cuculi (Luzerner Kantonsspital, Luzern, Switzerland). 3 4Macedonia: Sasko Kedev (University Clinic of Cardiology, Skopje, Macedonia). 5 6Spain: Javier Zueco (Hospital Universitario Marquès de Valdecilla, Santander, Spain), 7Josepa Mauri Ferre (Hospital Universitari Germans Trias i Pujol, Badalona, Spain), José F. 8Díaz (Juan Ramón Jiménez Hospital, Huelva, Spain), Ramón Lopez Palop (Hospital San 9Juan de Alicante, Alicante, Spain), Eduardo Pinar (Hospital Universitario Virgen de la 10Arrixaca, Murcia, Spain), Salvatore Brugaletta (Hospital Clinic, Barcelona, Spain), Jose 11Antonio Baz Alonso (Hospital Meixoeiro, Vigo, Spain), Ignacio Cruz Gonzalez (University 12Hospital of Salamanca, Salamanca, Spain), Raúl Millán (Hospital del Mar, Barcelona, Spain), 13Ramon Antonio Calviño Santos (Hospital Universitario de A Coruña, A Coruña, Spain), 14Ignacio J. Amat Santos (Hospital Clínico Universitario de Valladolid, Valladolid, Spain), Jose 15Moreu (Hospital Virgen de la Salud, Toledo, Spain), Antonio Serra (Hospital de Sant Pau, 16Barcelona, Spain). 17 18Latvia: Andrejs Erglis (Pauls Stradins Clinical University Hospital, Riga, Latvia). 19 20Belgium: Victor Legrand (CHU Sart-Tilman, Liège, Belgium), Christophe Dubois (UZ Leuven, 21Leuven, Belgium), Claudiu Ungureanu (Centre Hospitalier de Jolimont, La Louvière, 22Belgium), Nadia Debbas (CHU St Pierre, Brussels, Belgium). 23 24United Kingdom: Azfar Zaman (Freeman Hospital - Newcastle Upon Tyne Hospitals NHS 25Foundation trust, Newcastle upon Tyne, UK), Ian Menown (Craigavon Cardiac Center, 26Craigavon, UK), Simon Redwood (Guy’s and St Thomas’ Hospitals, London, UK), Benjamin 27Wrigley (New Cross Hospital, Wolverhampton, UK), Adam de Belder (Brighton and Sussex 28University Hospitals NHS Trust, Brighton, UK), Jonathan Hill (King’s College Hospital, 29London, UK). 30 31Finland: Pasi Karjalainen (Satakunta Central Hospital, Pori, Finland), Kari Kervinen (Oulu 32University Hospital, Oulu, Finland). 33 34Italy: Marco Caruso (ARNAS Civico, Palermo, Italy). 35
B: Inclusion and exclusion criteria 36
Inclusion criteria: 37Patients with one or more significant coronary artery stenosis (defined as ≥70% by visual 38assessment or ≥50% with Fractional Flow Reserve <0·80) or a left main coronary stenosis 39≥50% by visual assessment, deemed suitable for percutaneous coronary intervention with 40ALL of the following criteria: 41 1. Patient are 75 years old and above 42 2. Patients have acute coronary syndrome, or, stable angina or silent ischemia. 43 - Stable angina, in a patient with myocardial ischemia despite optimal medical therapy 44OR 45 - Acute coronary syndrome including: unstable angina, non ST- or ST-segment 46
5
elevation myocardial infarction. 1OR 2 - Silent ischemia, as defined by: 3 ο Stress-induced myocardial ischemia ≥10% of the myocardium in 4asymptomatic patients. 5 ο Stress-induced myocardial ischemia <10% of myocardium in asymptomatic 6patients AND a Fractional Flow Reserve ≤0·80 7 3. Patients must sign informed consent as per local law and comply with all study 8process during follow up for at least one year. 9 10Exclusion criteria (any criteria) 11 1. Indication for myocardial revascularisation by coronary artery bypass grafting, 12 2. Subjects unable to tolerate, obtain or comply with dual antiplatelet therapy for at 13least six month (acute coronary syndrome) or at least one month (stable angina or silent 14ischemia), 15 3. Subjects requiring additional surgery (cardiac or non-cardiac) within one month, 16 4. Non-cardiac co-morbidities with life expectancy less than 1 year, 17 5. Prior hemorrhagic stroke, 18 6. Known allergy to aspirin, 19 7. At least one contra indication to all the authorized P2Y12 inhibitors at the requested 20dose (in case of contra indication to only one of two of the P2Y12 inhibitors, the investigators 21are allowed to use the P2Y12 inhibitors for which no allergy is known). 22 8. Silent ischemia <10% of the left myocardium with fractional flow reserve ≥0·80. 23 9. Participation in another randomized clinical trial. 24
C: Study devices 25
The Synergy II coronary stent delivery system (Boston Scientific, Marlborough, MA, USA) is 26a device consisting of three components, including 27 1. a thin-strut (74µm) platinum-chromium stent platform 28 2. an ultrathin bioabsorbable poly(DL-lactide-co-glycolide) polymer mixed with the 29drug and only applied to the abluminal surface. 30 3. the drug, everolimus, is a sirolimus derivative, delivered in the vicinity of the vessel 31wall upon stent implantation. 32 33The drug eluting stent is crimped onto a rapid exchange delivery system which includes a 34high pressure, semi-compliant balloon onto the distal tip of of the system. The delivery 35system consists in a balloon with two radiopaque markers nominally 0·4 mm longer than the 36stent at each end, to facilitate proper stent placement. Everolimus is the therapeutic agent, 37rapidly absorbed in vessel wall, and able to reversibly inhibit growth factor-stimulated medial 38smooth muscle cells proliferation. Current data suggest that everolimus, on a molecular 39level, forms a complex with the cytoplasmic proteins that inhibit the cell cycle between the 40G0 and G1 phase. The result is an interruption of the cascade governing cell metabolism, 41growth, and proliferation. The bioabsorbable polymer has totally disappeared at three 42months. For this trial, the Synergy II stent was available in five stent diameters (2·25 – 4·0 43mm), six lengths (8-38mm) and one drug dosage (1�g/mm2). 44 45The control Omega and Rebel bare metal stents ((Boston Scientific, Marlborough, MA, USA) 46
6
consist of a platinum-chromium platforms, similar to the Synergy II stent without the 1abluminal polymer, and are crimped onto the same balloon delivery system. 2The Omega and Rebel stents are balloon expandable platinum chromium alloy, thin strut 3(81µm) stents pre-mounted on a monorail catheter. The delivery system consists in a 4balloon with two radiopaque markers nominally 0·4 mm longer than the stent at each end, to 5facilitate proper stent placement. For this trial, the Rebel stent was available in five stent 6diameters (2·25 – 4·0 mm), and six lengths (8-38mm), identical to the Synergy II stents. 7 8
D: End point definitions 9
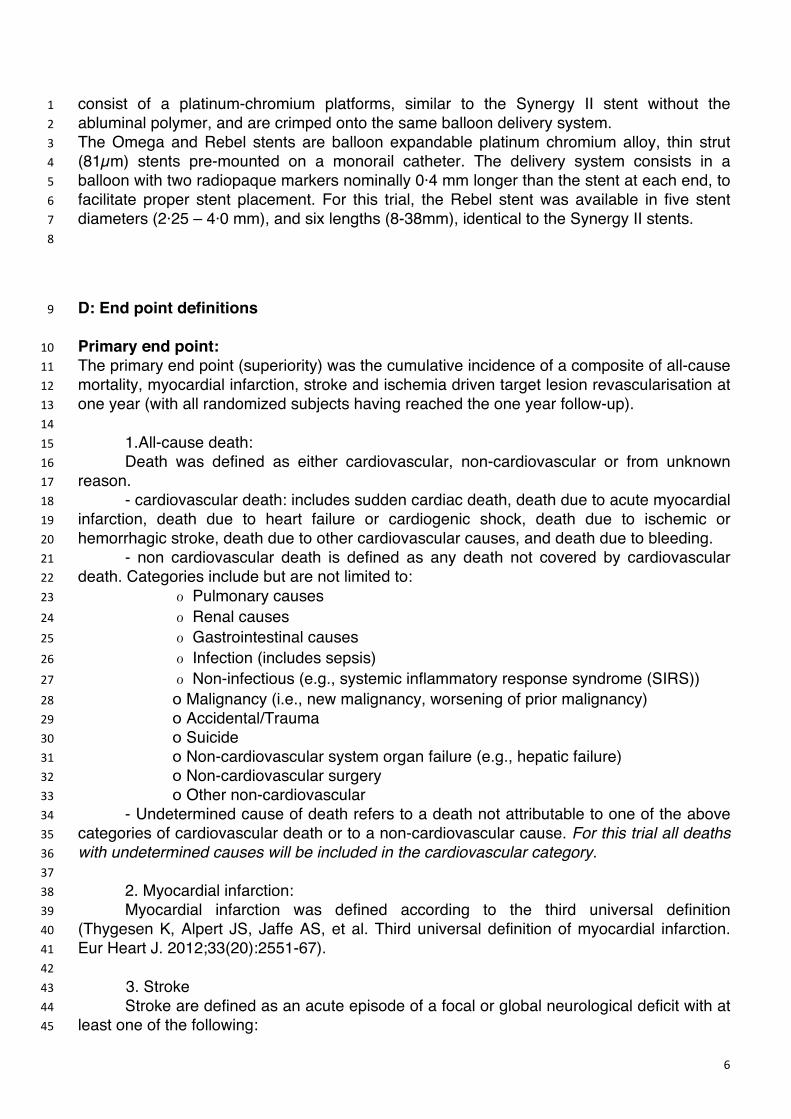
Primary end point: 10The primary end point (superiority) was the cumulative incidence of a composite of all-cause 11mortality, myocardial infarction, stroke and ischemia driven target lesion revascularisation at 12one year (with all randomized subjects having reached the one year follow-up). 13 14 1.All-cause death: 15 Death was defined as either cardiovascular, non-cardiovascular or from unknown 16reason. 17 - cardiovascular death: includes sudden cardiac death, death due to acute myocardial 18infarction, death due to heart failure or cardiogenic shock, death due to ischemic or 19hemorrhagic stroke, death due to other cardiovascular causes, and death due to bleeding. 20 - non cardiovascular death is defined as any death not covered by cardiovascular 21death. Categories include but are not limited to: 22 � Pulmonary causes 23 � Renal causes 24 � Gastrointestinal causes 25 � Infection (includes sepsis) 26 � Non-infectious (e.g., systemic inflammatory response syndrome (SIRS)) 27 ο Malignancy (i.e., new malignancy, worsening of prior malignancy) 28 ο Accidental/Trauma 29 ο Suicide 30 ο Non-cardiovascular system organ failure (e.g., hepatic failure) 31 ο Non-cardiovascular surgery 32 ο Other non-cardiovascular 33 - Undetermined cause of death refers to a death not attributable to one of the above 34categories of cardiovascular death or to a non-cardiovascular cause. For this trial all deaths 35with undetermined causes will be included in the cardiovascular category. 36 37 2. Myocardial infarction: 38 Myocardial infarction was defined according to the third universal definition 39(Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. 40Eur Heart J. 2012;33(20):2551-67). 41 42
3. Stroke 43 Stroke are defined as an acute episode of a focal or global neurological deficit with at 44least one of the following: 45
7
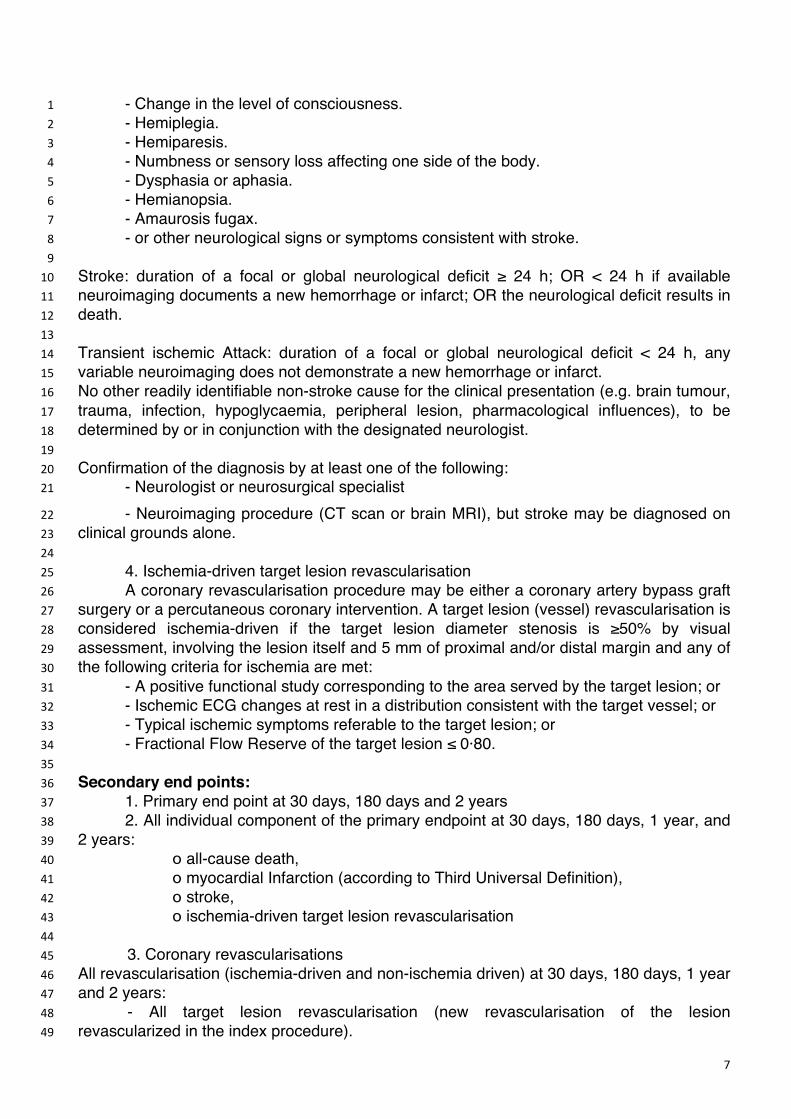
- Change in the level of consciousness. 1 - Hemiplegia. 2 - Hemiparesis. 3 - Numbness or sensory loss affecting one side of the body. 4 - Dysphasia or aphasia. 5 - Hemianopsia. 6 - Amaurosis fugax. 7 - or other neurological signs or symptoms consistent with stroke. 8 9Stroke: duration of a focal or global neurological deficit ≥ 24 h; OR < 24 h if available 10neuroimaging documents a new hemorrhage or infarct; OR the neurological deficit results in 11death. 12 13Transient ischemic Attack: duration of a focal or global neurological deficit < 24 h, any 14variable neuroimaging does not demonstrate a new hemorrhage or infarct. 15No other readily identifiable non-stroke cause for the clinical presentation (e.g. brain tumour, 16trauma, infection, hypoglycaemia, peripheral lesion, pharmacological influences), to be 17determined by or in conjunction with the designated neurologist. 18 19Confirmation of the diagnosis by at least one of the following: 20 - Neurologist or neurosurgical specialist 21
- Neuroimaging procedure (CT scan or brain MRI), but stroke may be diagnosed on 22clinical grounds alone. 23 24 4. Ischemia-driven target lesion revascularisation 25 A coronary revascularisation procedure may be either a coronary artery bypass graft 26surgery or a percutaneous coronary intervention. A target lesion (vessel) revascularisation is 27considered ischemia-driven if the target lesion diameter stenosis is ≥50% by visual 28assessment, involving the lesion itself and 5 mm of proximal and/or distal margin and any of 29the following criteria for ischemia are met: 30 - A positive functional study corresponding to the area served by the target lesion; or 31 - Ischemic ECG changes at rest in a distribution consistent with the target vessel; or 32 - Typical ischemic symptoms referable to the target lesion; or 33 - Fractional Flow Reserve of the target lesion ≤ 0·80. 34 35Secondary end points: 36 1. Primary end point at 30 days, 180 days and 2 years 37 2. All individual component of the primary endpoint at 30 days, 180 days, 1 year, and 382 years: 39 ο all-cause death, 40 ο myocardial Infarction (according to Third Universal Definition), 41 ο stroke, 42 ο ischemia-driven target lesion revascularisation 43 44 3. Coronary revascularisations 45All revascularisation (ischemia-driven and non-ischemia driven) at 30 days, 180 days, 1 year 46and 2 years: 47 - All target lesion revascularisation (new revascularisation of the lesion 48revascularized in the index procedure). 49
8
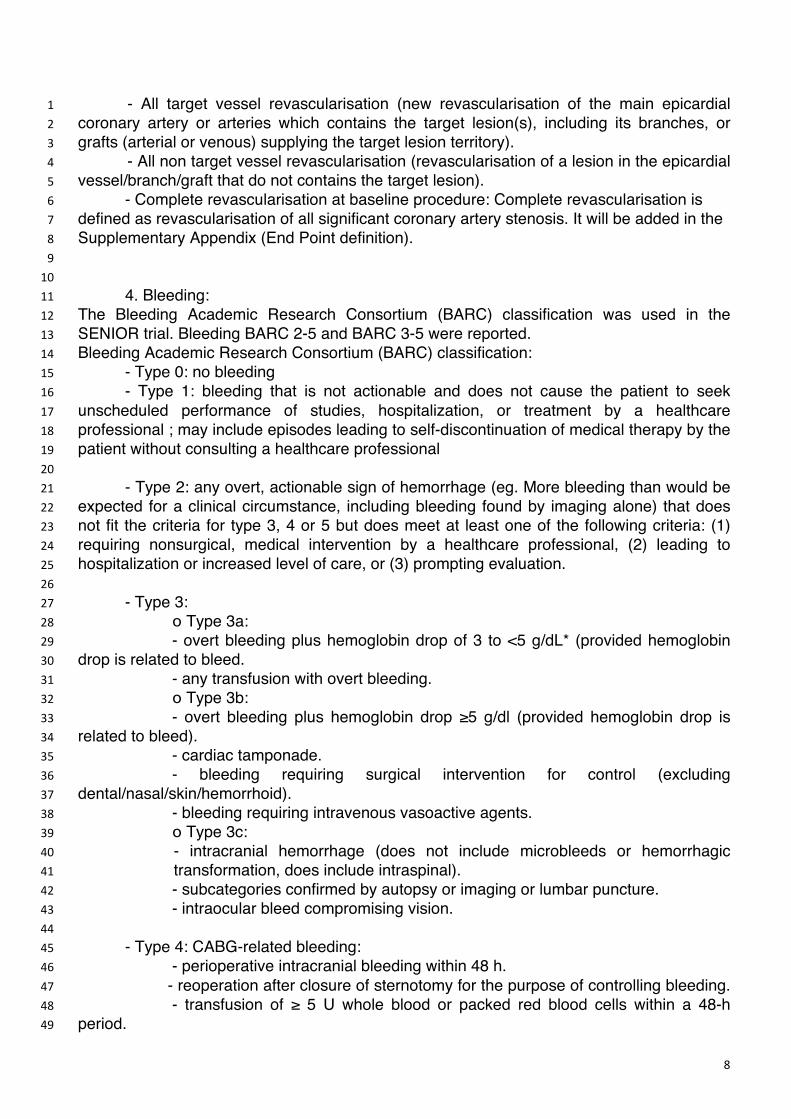
- All target vessel revascularisation (new revascularisation of the main epicardial 1coronary artery or arteries which contains the target lesion(s), including its branches, or 2grafts (arterial or venous) supplying the target lesion territory). 3 - All non target vessel revascularisation (revascularisation of a lesion in the epicardial 4vessel/branch/graft that do not contains the target lesion). 5 - Complete revascularisation at baseline procedure: Complete revascularisation is 6defined as revascularisation of all significant coronary artery stenosis. It will be added in the 7Supplementary Appendix (End Point definition). 8 9 10 4. Bleeding: 11The Bleeding Academic Research Consortium (BARC) classification was used in the 12SENIOR trial. Bleeding BARC 2-5 and BARC 3-5 were reported. 13Bleeding Academic Research Consortium (BARC) classification: 14 - Type 0: no bleeding 15 - Type 1: bleeding that is not actionable and does not cause the patient to seek 16unscheduled performance of studies, hospitalization, or treatment by a healthcare 17professional ; may include episodes leading to self-discontinuation of medical therapy by the 18patient without consulting a healthcare professional 19 20 - Type 2: any overt, actionable sign of hemorrhage (eg. More bleeding than would be 21expected for a clinical circumstance, including bleeding found by imaging alone) that does 22not fit the criteria for type 3, 4 or 5 but does meet at least one of the following criteria: (1) 23requiring nonsurgical, medical intervention by a healthcare professional, (2) leading to 24hospitalization or increased level of care, or (3) prompting evaluation. 25 26 - Type 3: 27 ο Type 3a: 28 - overt bleeding plus hemoglobin drop of 3 to <5 g/dL* (provided hemoglobin 29drop is related to bleed. 30 - any transfusion with overt bleeding. 31 ο Type 3b: 32 - overt bleeding plus hemoglobin drop ≥5 g/dl (provided hemoglobin drop is 33related to bleed). 34 - cardiac tamponade. 35 - bleeding requiring surgical intervention for control (excluding 36dental/nasal/skin/hemorrhoid). 37 - bleeding requiring intravenous vasoactive agents. 38 ο Type 3c: 39
- intracranial hemorrhage (does not include microbleeds or hemorrhagic 40transformation, does include intraspinal). 41
- subcategories confirmed by autopsy or imaging or lumbar puncture. 42 - intraocular bleed compromising vision. 43 44 - Type 4: CABG-related bleeding: 45 - perioperative intracranial bleeding within 48 h. 46 - reoperation after closure of sternotomy for the purpose of controlling bleeding. 47 - transfusion of ≥ 5 U whole blood or packed red blood cells within a 48-h 48period. 49
9
- chest tube output ≥ 2L within a 24-h period. 1 2 - Type 5: fatal bleeding: 3
- Type 5a: probable fatal bleeding; no autopsy or imaging confirmation but 4clinically suspicious. 5- Type 5b: definite fatal bleeding; overt bleeding or autopsy or imaging 6confirmation. 7
8Bleeding complications (BARC 2-5 and 3-5) at 30 days, 180 days, 1 year and 2 years. 9 10 5. Net clinical benefit at 30 days, 180 days, 1 year and 2 years: 11Association of composite events (all-cause mortality, myocardial infarction, stroke, ischemia 12driven TLR, and bleedings BARC 2-5). 13 14 6. Stent thrombosis: 15Definite and probable stent thrombosis will be defined according to Academic Research 16Consortium at 30 days, 180 days, 1 year and 2 years. 17 - Timing of Stent Thrombosis 18 ο Acute stent thrombosis: 0 to 24 hours after stent implantation 19 ο Subacute stent thrombosis > 24 hours to 30 days after stent implantation 20 ο Late stent thrombosis > 30 days to 1 year after stent implantation 21 ο Very late stent thrombosis > 1 year after stent implantation 22 23Stent thrombosis is reported as a cumulative value over time and at the various individual 24time points specified above. Time 0 is defined as the time point after the guiding catheter 25has been removed and the subject has left the catheterization laboratory. 26 27 - Stent Thrombosis Definitions: 28 ο Definite Stent Thrombosis 29 Definite stent thrombosis is considered to have occurred by either 30angiographic or pathological confirmation: 31 a. Angiographic confirmation of stent thrombosis 32
The presence of a thrombus that originates in the stent or in the segment 5 33mm proximal or distal to the stent and presence of at least 1 of the following 34criteria within a 48-hour time window: 35 1. Acute onset of ischemic symptoms at rest 36 2. New ischemic ECG changes that suggest acute ischemia 37 3. Typical rise and fall in cardiac biomarkers (refer to definition of 38spontaneous MI: Troponin or CK-MB > 99th percentile of URL) 39
4. Non occlusive thrombus 40 Intracoronary thrombus is defined as a (spheric, ovoid, or irregular) non 41calcified filling defect or lucency surrounded by contrast material (on 42three sides or within a coronary stenosis) seen in multiple projections, or 43persistence of contrast material within the lumen, or a visible 44embolization of intraluminal material downstream. 45 5. Occlusive thrombus 46 TIMI 0 or TIMI 1 intra stent or proximal to a stent up to the most 47adjacent proximal side branch or main branch (if originates from the side 48branch). 49
10
Pathological confirmation of stent thrombosis. 1Evidence of recent thrombus within the stent determined at autopsy or 2via examination of tissue retrieved following thrombectomy. 3
4 ο Probable Stent Thrombosis 5 Clinical definition of probable stent thrombosis is considered to have occurred after6 intracoronary stenting in the following cases: 7
a. Any unexplained death within the first 30 days 8 b. Irrespective of the time after the index procedure, any myocardial 9infarction that is related to documented acute ischemia in the territory of the 10implanted stent without angiographic confirmation of stent thrombosis and in 11the absence of any other obvious cause. 12
E: Randomisation 13
Randomisation was carried out through a web-based system available 24h/d all year round 14and maintained by the Data Coordinating Center (Cardiovascular European Research 15Center, CERC, Massy, France). It was stratified by centre and by choice of antiplatelet 16agent, which was entered in the Interactive Web Response System (IWRS) before 17randomisation to avoid inequality between the two groups based on an unblinded 18physician’s decision. Also the duration of DAPT (1 to 6 months) was entered in IWRS before 19randomisation for the same reason. 20 21
22
F: Supplementary Tables and Figures 23
11
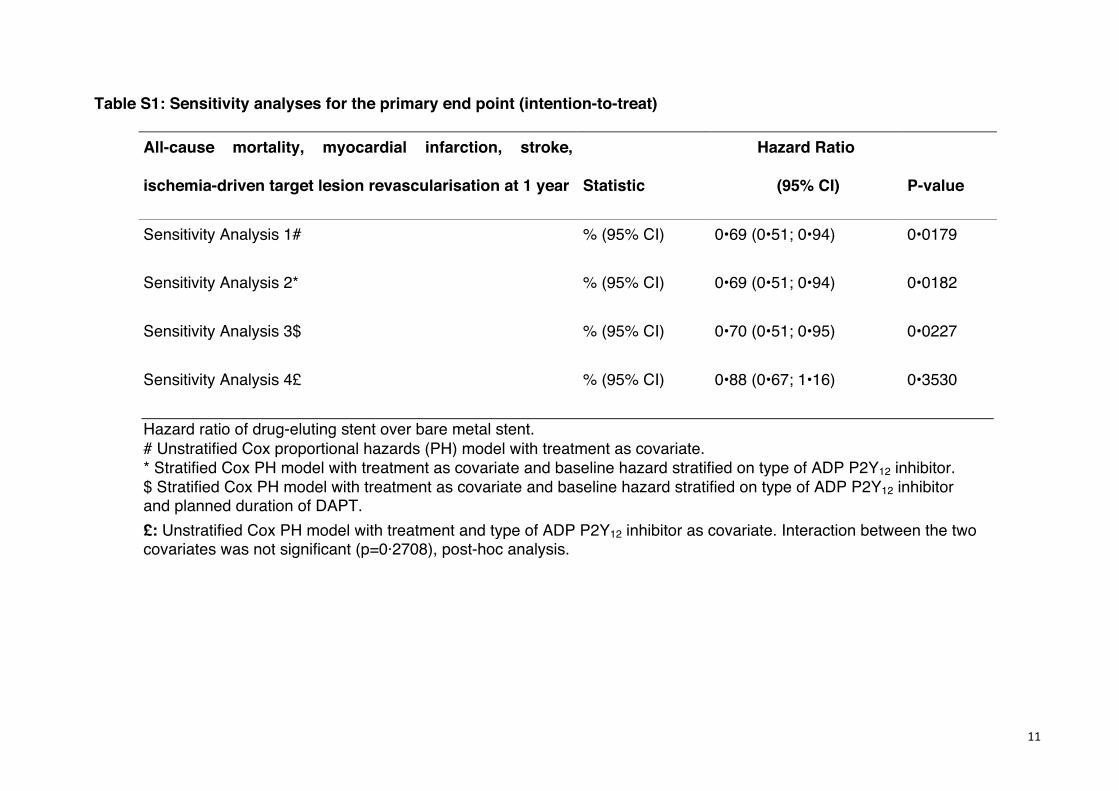
Table S1: Sensitivity analyses for the primary end point (intention-to-treat)
All-cause mortality, myocardial infarction, stroke,
ischemia-driven target lesion revascularisation at 1 year Statistic
Hazard Ratio
(95% CI) P-value
Sensitivity Analysis 1# % (95% CI) 0•69 (0•51; 0•94) 0•0179
Sensitivity Analysis 2* % (95% CI) 0•69 (0•51; 0•94) 0•0182
Sensitivity Analysis 3$ % (95% CI) 0•70 (0•51; 0•95) 0•0227
Sensitivity Analysis 4£ % (95% CI) 0•88 (0•67; 1•16) 0•3530
Hazard ratio of drug-eluting stent over bare metal stent. # Unstratified Cox proportional hazards (PH) model with treatment as covariate. * Stratified Cox PH model with treatment as covariate and baseline hazard stratified on type of ADP P2Y12 inhibitor. $ Stratified Cox PH model with treatment as covariate and baseline hazard stratified on type of ADP P2Y12 inhibitor and planned duration of DAPT. £: Unstratified Cox PH model with treatment and type of ADP P2Y12 inhibitor as covariate. Interaction between the two covariates was not significant (p=0·2708), post-hoc analysis.
12
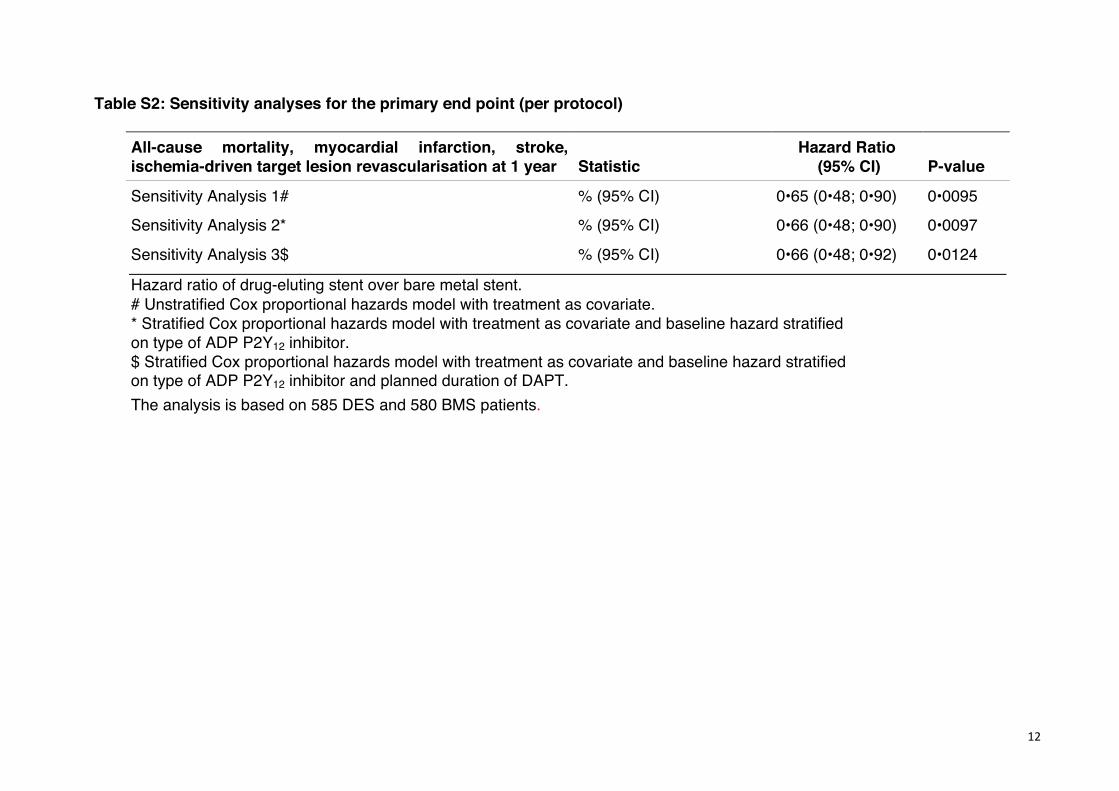
Table S2: Sensitivity analyses for the primary end point (per protocol)
All-cause mortality, myocardial infarction, stroke, ischemia-driven target lesion revascularisation at 1 year Statistic
Hazard Ratio (95% CI) P-value
Sensitivity Analysis 1# % (95% CI) 0•65 (0•48; 0•90) 0•0095
Sensitivity Analysis 2* % (95% CI) 0•66 (0•48; 0•90) 0•0097
Sensitivity Analysis 3$ % (95% CI) 0•66 (0•48; 0•92) 0•0124
Hazard ratio of drug-eluting stent over bare metal stent. # Unstratified Cox proportional hazards model with treatment as covariate. * Stratified Cox proportional hazards model with treatment as covariate and baseline hazard stratified on type of ADP P2Y12 inhibitor. $ Stratified Cox proportional hazards model with treatment as covariate and baseline hazard stratified on type of ADP P2Y12 inhibitor and planned duration of DAPT. The analysis is based on 585 DES and 580 BMS patients.
13
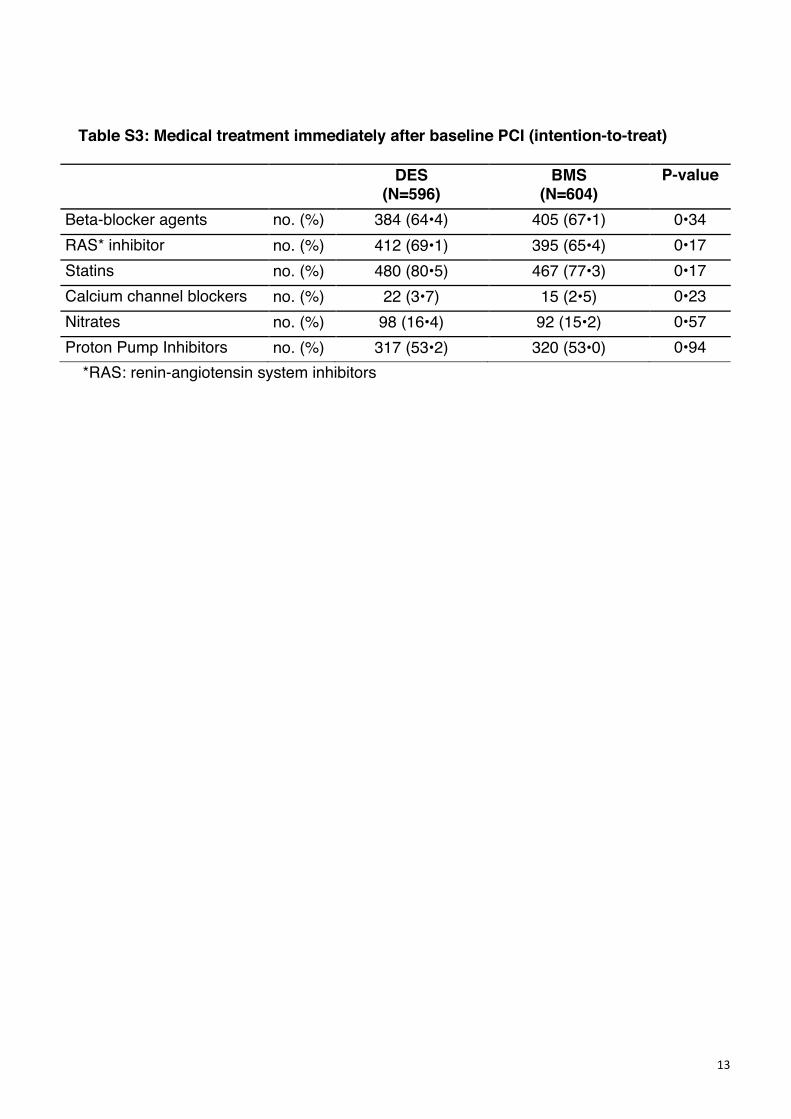
Table S3: Medical treatment immediately after baseline PCI (intention-to-treat)
DES (N=596)
BMS (N=604)
P-value
Beta-blocker agents no. (%) 384 (64•4) 405 (67•1) 0•34 RAS* inhibitor no. (%) 412 (69•1) 395 (65•4) 0•17 Statins no. (%) 480 (80•5) 467 (77•3) 0•17 Calcium channel blockers no. (%) 22 (3•7) 15 (2•5) 0•23 Nitrates no. (%) 98 (16•4) 92 (15•2) 0•57 Proton Pump Inhibitors no. (%) 317 (53•2) 320 (53•0) 0•94
*RAS: renin-angiotensin system inhibitors
14
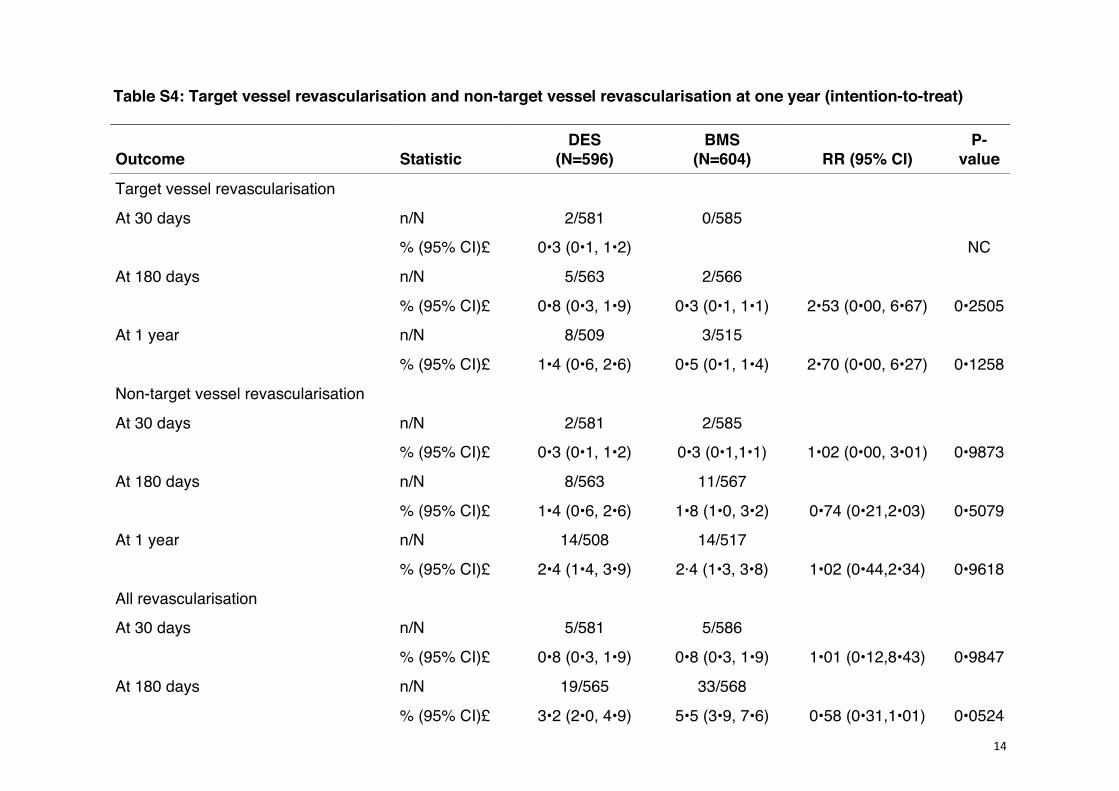
Table S4: Target vessel revascularisation and non-target vessel revascularisation at one year (intention-to-treat)
Outcome Statistic DES
(N=596) BMS
(N=604) RR (95% CI) P-
value
Target vessel revascularisation
At 30 days n/N 2/581 0/585 % (95% CI)£ 0•3 (0•1, 1•2) NC
At 180 days n/N 5/563 2/566 % (95% CI)£ 0•8 (0•3, 1•9) 0•3 (0•1, 1•1) 2•53 (0•00, 6•67) 0•2505
At 1 year n/N 8/509 3/515 % (95% CI)£ 1•4 (0•6, 2•6) 0•5 (0•1, 1•4) 2•70 (0•00, 6•27) 0•1258
Non-target vessel revascularisation
At 30 days n/N 2/581 2/585 % (95% CI)£ 0•3 (0•1, 1•2) 0•3 (0•1,1•1) 1•02 (0•00, 3•01) 0•9873
At 180 days n/N 8/563 11/567 % (95% CI)£ 1•4 (0•6, 2•6) 1•8 (1•0, 3•2) 0•74 (0•21,2•03) 0•5079
At 1 year n/N 14/508 14/517 % (95% CI)£ 2•4 (1•4, 3•9) 2·4 (1•3, 3•8) 1•02 (0•44,2•34) 0•9618
All revascularisation
At 30 days n/N 5/581 5/586 % (95% CI)£ 0•8 (0•3, 1•9) 0•8 (0•3, 1•9) 1•01 (0•12,8•43) 0•9847
At 180 days n/N 19/565 33/568 % (95% CI)£ 3•2 (2•0, 4•9) 5•5 (3•9, 7•6) 0•58 (0•31,1•01) 0•0524
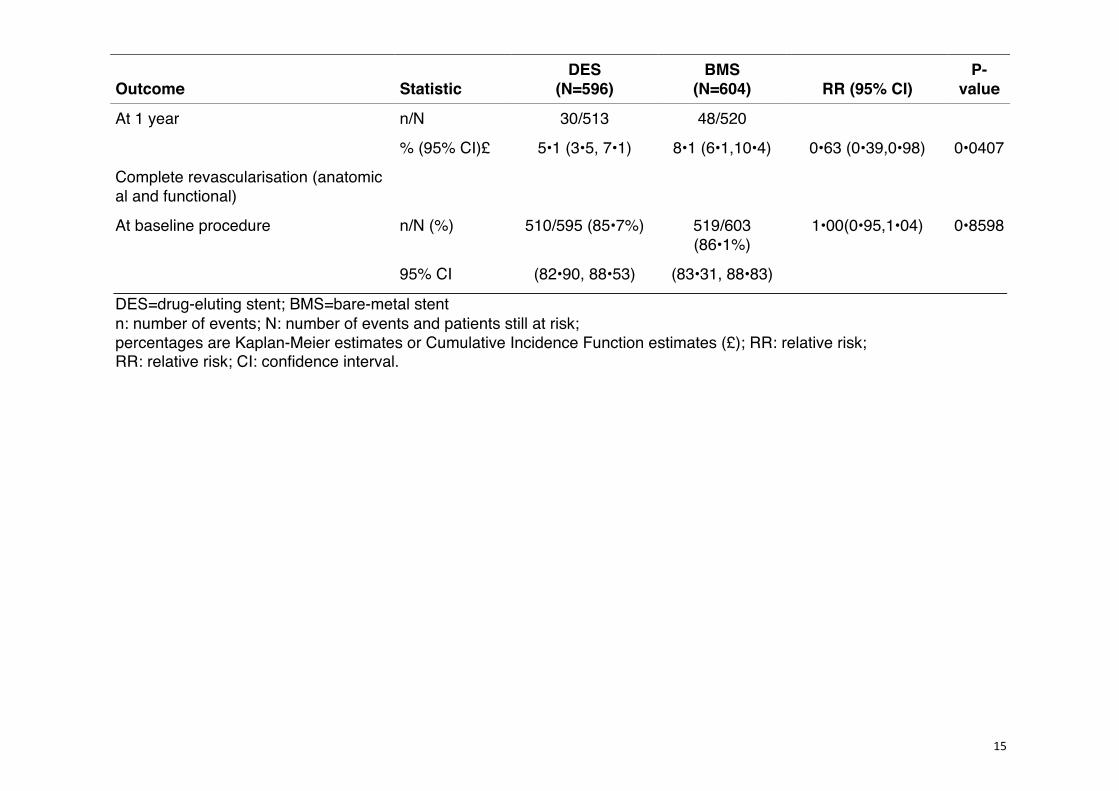
15
Outcome Statistic DES
(N=596) BMS
(N=604) RR (95% CI) P-
value
At 1 year n/N 30/513 48/520 % (95% CI)£ 5•1 (3•5, 7•1) 8•1 (6•1,10•4) 0•63 (0•39,0•98) 0•0407
Complete revascularisation (anatomical and functional)
At baseline procedure n/N (%) 510/595 (85•7%) 519/603 (86•1%)
1•00(0•95,1•04) 0•8598
95% CI (82•90, 88•53) (83•31, 88•83)
DES=drug-eluting stent; BMS=bare-metal stent n: number of events; N: number of events and patients still at risk; percentages are Kaplan-Meier estimates or Cumulative Incidence Function estimates (£); RR: relative risk; RR: relative risk; CI: confidence interval.
16
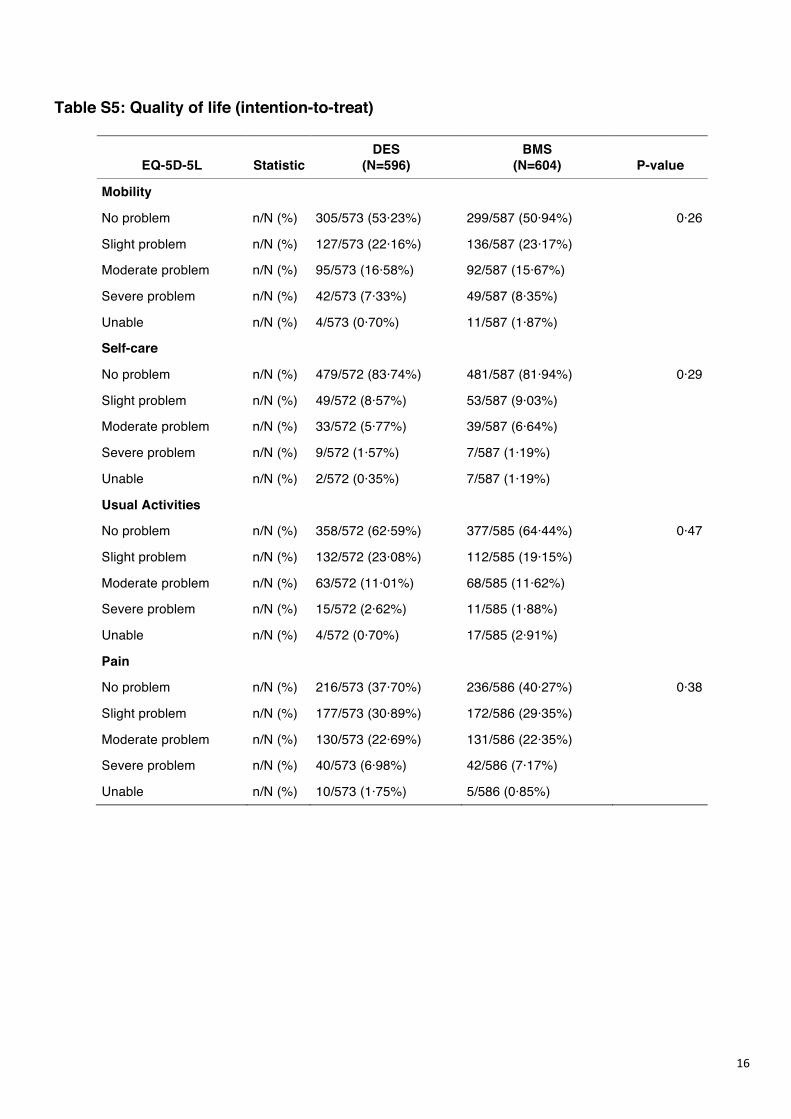
Table S5: Quality of life (intention-to-treat)
EQ-5D-5L Statistic DES
(N=596) BMS
(N=604) P-value
Mobility
No problem n/N (%) 305/573 (53·23%) 299/587 (50·94%) 0·26
Slight problem n/N (%) 127/573 (22·16%) 136/587 (23·17%)
Moderate problem n/N (%) 95/573 (16·58%) 92/587 (15·67%)
Severe problem n/N (%) 42/573 (7·33%) 49/587 (8·35%)
Unable n/N (%) 4/573 (0·70%) 11/587 (1·87%)
Self-care
No problem n/N (%) 479/572 (83·74%) 481/587 (81·94%) 0·29
Slight problem n/N (%) 49/572 (8·57%) 53/587 (9·03%)
Moderate problem n/N (%) 33/572 (5·77%) 39/587 (6·64%)
Severe problem n/N (%) 9/572 (1·57%) 7/587 (1·19%)
Unable n/N (%) 2/572 (0·35%) 7/587 (1·19%)
Usual Activities
No problem n/N (%) 358/572 (62·59%) 377/585 (64·44%) 0·47
Slight problem n/N (%) 132/572 (23·08%) 112/585 (19·15%)
Moderate problem n/N (%) 63/572 (11·01%) 68/585 (11·62%)
Severe problem n/N (%) 15/572 (2·62%) 11/585 (1·88%)
Unable n/N (%) 4/572 (0·70%) 17/585 (2·91%)
Pain
No problem n/N (%) 216/573 (37·70%) 236/586 (40·27%) 0·38
Slight problem n/N (%) 177/573 (30·89%) 172/586 (29·35%)
Moderate problem n/N (%) 130/573 (22·69%) 131/586 (22·35%)
Severe problem n/N (%) 40/573 (6·98%) 42/586 (7·17%)
Unable n/N (%) 10/573 (1·75%) 5/586 (0·85%)
17
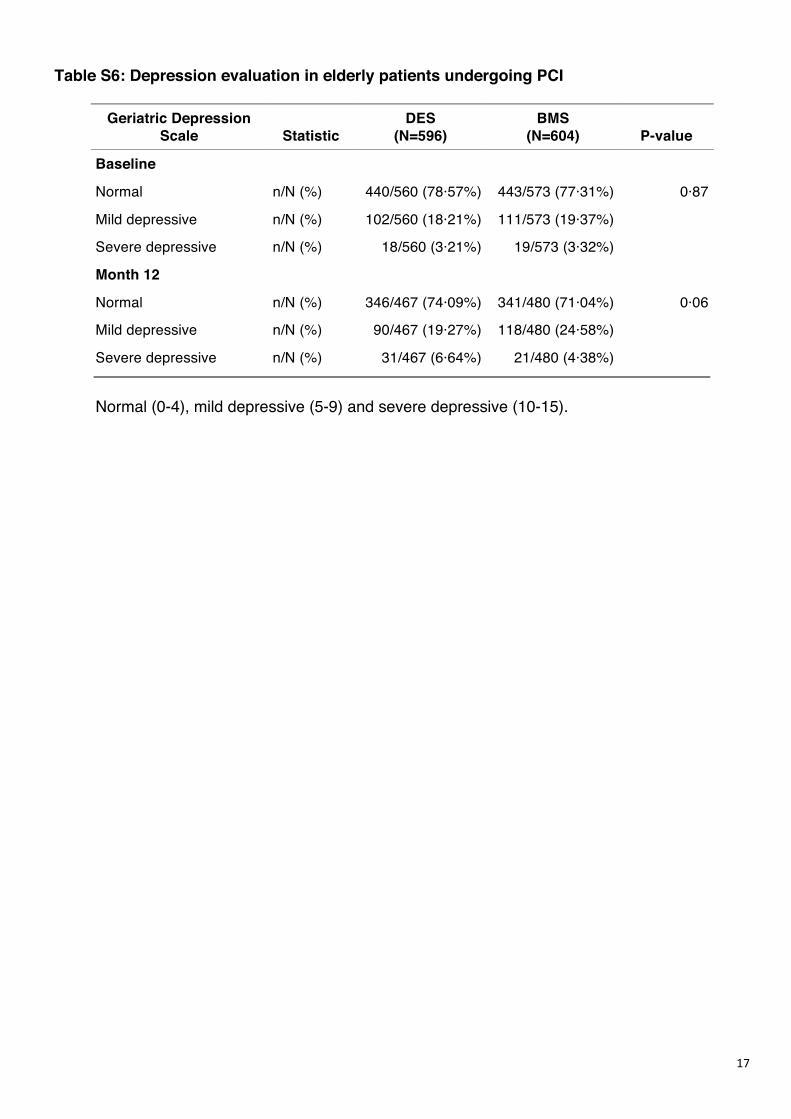
Table S6: Depression evaluation in elderly patients undergoing PCI
Geriatric Depression Scale Statistic
DES (N=596)
BMS (N=604) P-value
Baseline
Normal n/N (%) 440/560 (78·57%) 443/573 (77·31%) 0·87
Mild depressive n/N (%) 102/560 (18·21%) 111/573 (19·37%)
Severe depressive n/N (%) 18/560 (3·21%) 19/573 (3·32%)
Month 12
Normal n/N (%) 346/467 (74·09%) 341/480 (71·04%) 0·06
Mild depressive n/N (%) 90/467 (19·27%) 118/480 (24·58%)
Severe depressive n/N (%) 31/467 (6·64%) 21/480 (4·38%)
Normal (0-4), mild depressive (5-9) and severe depressive (10-15).
18
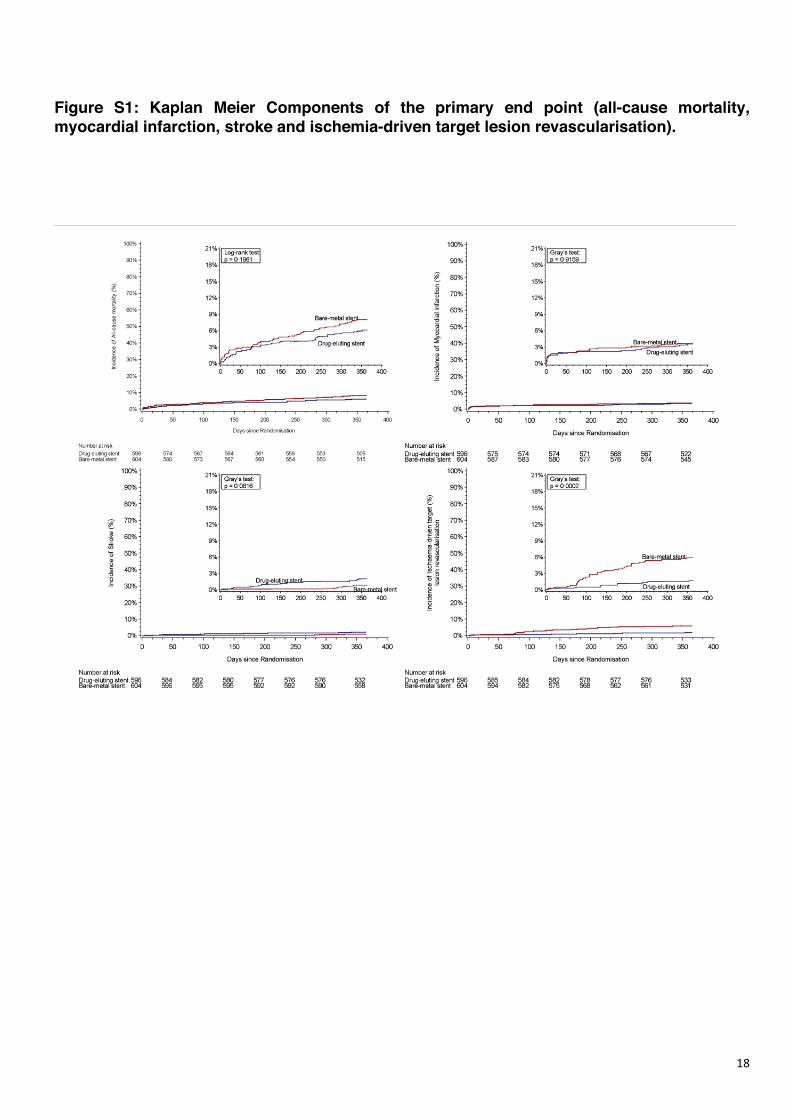
Figure S1: Kaplan Meier Components of the primary end point (all-cause mortality, myocardial infarction, stroke and ischemia-driven target lesion revascularisation).
19
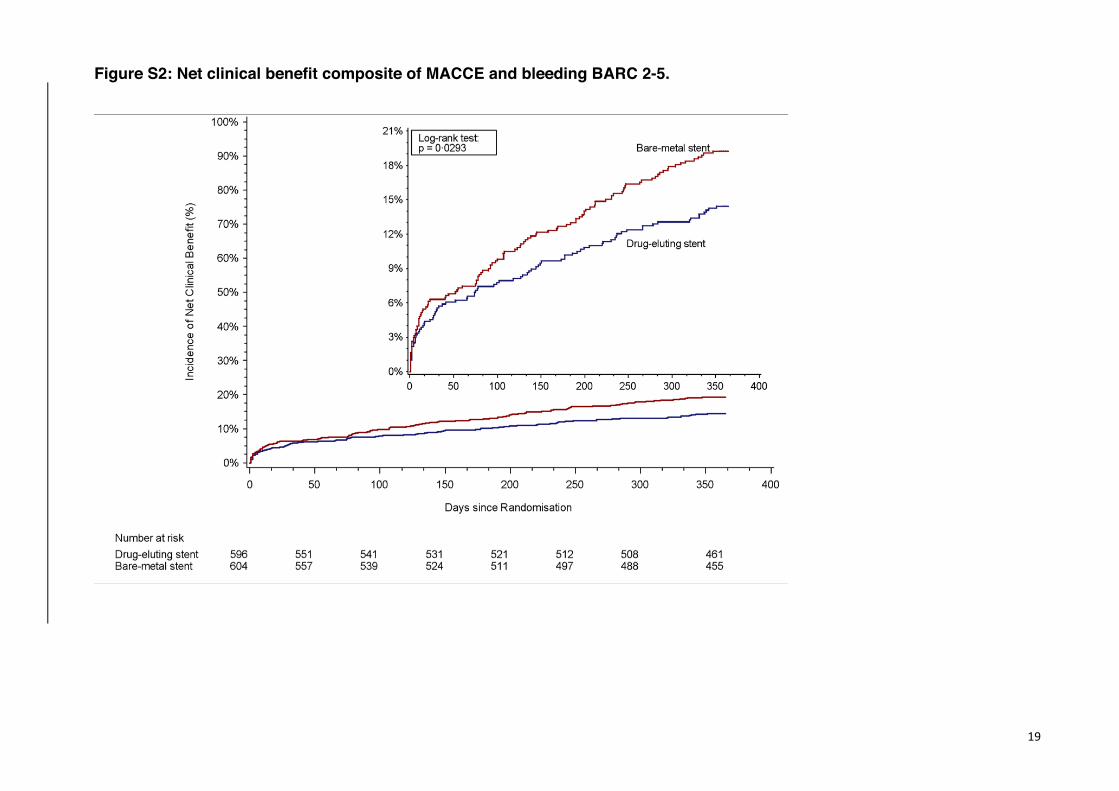
Figure S2: Net clinical benefit composite of MACCE and bleeding BARC 2-5.
20
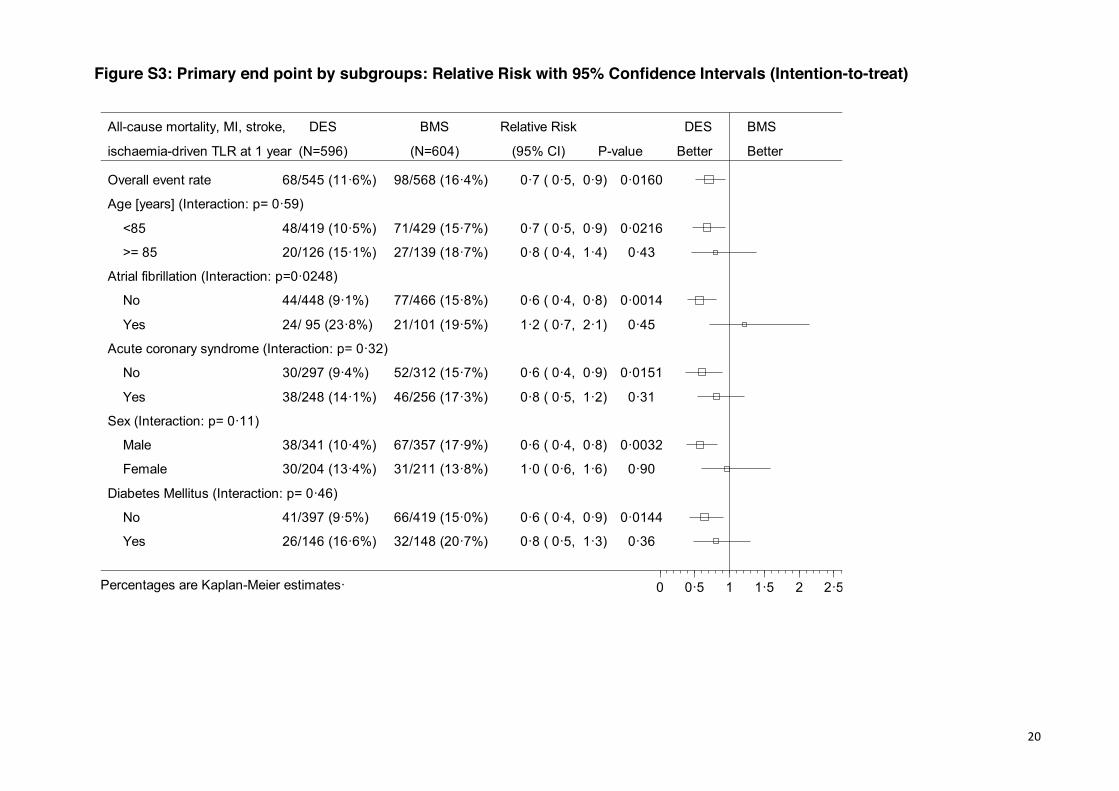
Figure S3: Primary end point by subgroups: Relative Risk with 95% Confidence Intervals (Intention-to-treat)
Overall event rate 68/545 (11·6%) 98/568 (16·4%) 0·7 ( 0·5, 0·9) 0·0160
Age [years] (Interaction: p= 0·59)
<85 48/419 (10·5%) 71/429 (15·7%) 0·7 ( 0·5, 0·9) 0·0216
>= 85 20/126 (15·1%) 27/139 (18·7%) 0·8 ( 0·4, 1·4) 0·43
Atrial fibrillation (Interaction: p=0·0248)
No 44/448 (9·1%) 77/466 (15·8%) 0·6 ( 0·4, 0·8) 0·0014
Yes 24/ 95 (23·8%) 21/101 (19·5%) 1·2 ( 0·7, 2·1) 0·45
Acute coronary syndrome (Interaction: p= 0·32)
No 30/297 (9·4%) 52/312 (15·7%) 0·6 ( 0·4, 0·9) 0·0151
Yes 38/248 (14·1%) 46/256 (17·3%) 0·8 ( 0·5, 1·2) 0·31
Sex (Interaction: p= 0·11)
Male 38/341 (10·4%) 67/357 (17·9%) 0·6 ( 0·4, 0·8) 0·0032
Female 30/204 (13·4%) 31/211 (13·8%) 1·0 ( 0·6, 1·6) 0·90
Diabetes Mellitus (Interaction: p= 0·46)
No 41/397 (9·5%) 66/419 (15·0%) 0·6 ( 0·4, 0·9) 0·0144
Yes 26/146 (16·6%) 32/148 (20·7%) 0·8 ( 0·5, 1·3) 0·36
All-cause mortality, MI, stroke,
ischaemia-driven TLR at 1 year
DES
(N=596)
BMS
(N=604)
Relative Risk
(95% CI) P-value
DES
Better
BMS
Better
0 0·5 1 1·5 2 2·5Percentages are Kaplan-Meier estimates·
21
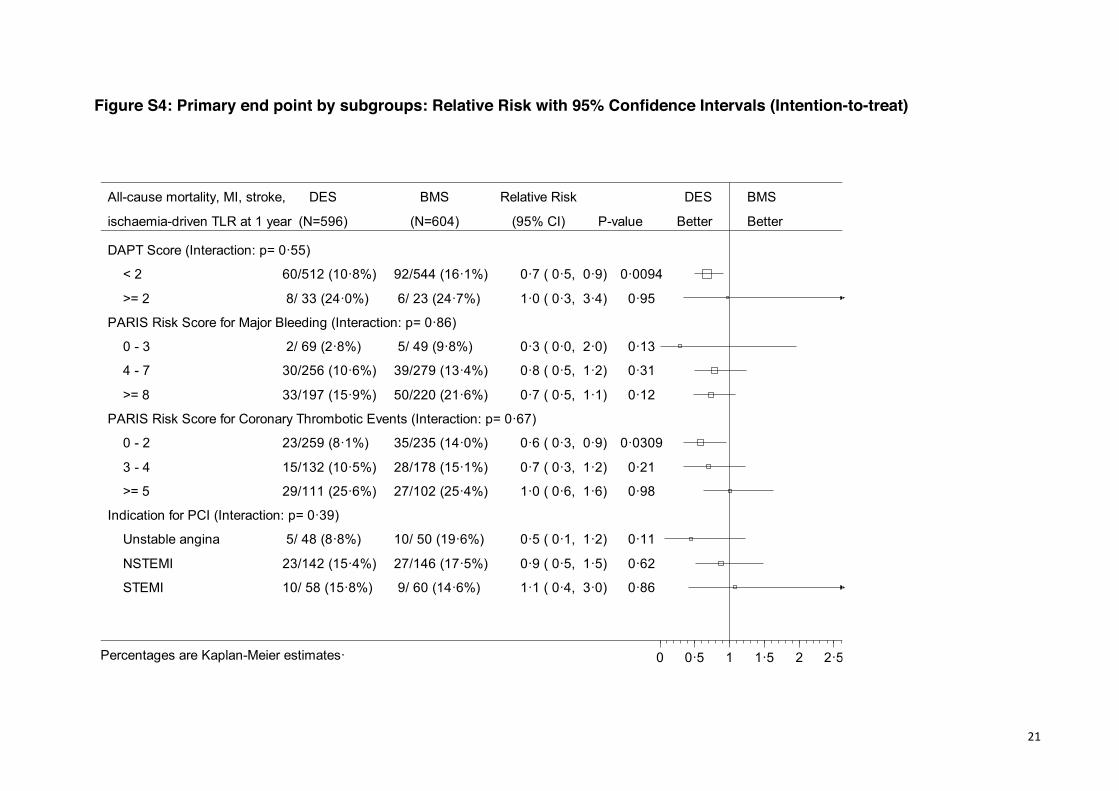
Figure S4: Primary end point by subgroups: Relative Risk with 95% Confidence Intervals (Intention-to-treat)
DAPT Score (Interaction: p= 0·55)
< 2 60/512 (10·8%) 92/544 (16·1%) 0·7 ( 0·5, 0·9) 0·0094
>= 2 8/ 33 (24·0%) 6/ 23 (24·7%) 1·0 ( 0·3, 3·4) 0·95
PARIS Risk Score for Major Bleeding (Interaction: p= 0·86)
0 - 3 2/ 69 (2·8%) 5/ 49 (9·8%) 0·3 ( 0·0, 2·0) 0·13
4 - 7 30/256 (10·6%) 39/279 (13·4%) 0·8 ( 0·5, 1·2) 0·31
>= 8 33/197 (15·9%) 50/220 (21·6%) 0·7 ( 0·5, 1·1) 0·12
PARIS Risk Score for Coronary Thrombotic Events (Interaction: p= 0·67)
0 - 2 23/259 (8·1%) 35/235 (14·0%) 0·6 ( 0·3, 0·9) 0·0309
3 - 4 15/132 (10·5%) 28/178 (15·1%) 0·7 ( 0·3, 1·2) 0·21
>= 5 29/111 (25·6%) 27/102 (25·4%) 1·0 ( 0·6, 1·6) 0·98
Indication for PCI (Interaction: p= 0·39)
Unstable angina 5/ 48 (8·8%) 10/ 50 (19·6%) 0·5 ( 0·1, 1·2) 0·11
NSTEMI 23/142 (15·4%) 27/146 (17·5%) 0·9 ( 0·5, 1·5) 0·62
STEMI 10/ 58 (15·8%) 9/ 60 (14·6%) 1·1 ( 0·4, 3·0) 0·86
All-cause mortality, MI, stroke,
ischaemia-driven TLR at 1 year
DES
(N=596)
BMS
(N=604)
Relative Risk
(95% CI) P-value
DES
Better
BMS
Better
0 0·5 1 1·5 2 2·5Percentages are Kaplan-Meier estimates·
22
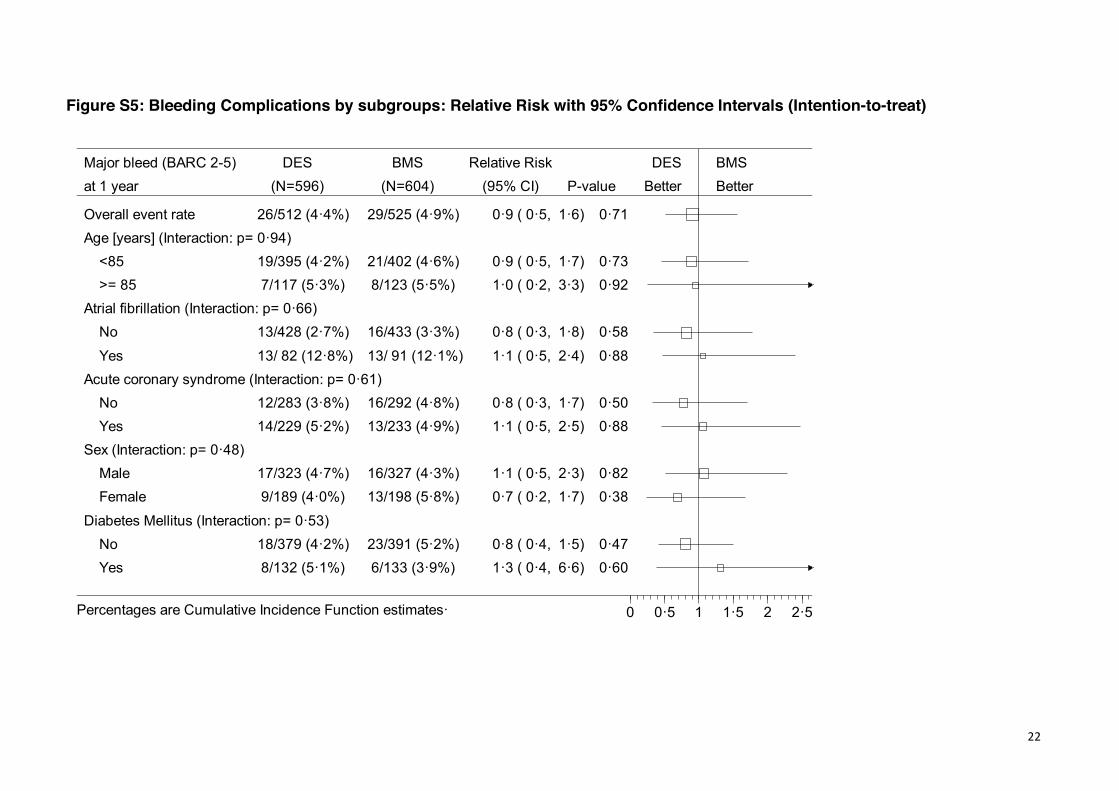
Figure S5: Bleeding Complications by subgroups: Relative Risk with 95% Confidence Intervals (Intention-to-treat)
Overall event rate 26/512 (4·4%) 29/525 (4·9%) 0·9 ( 0·5, 1·6) 0·71
Age [years] (Interaction: p= 0·94)
<85 19/395 (4·2%) 21/402 (4·6%) 0·9 ( 0·5, 1·7) 0·73
>= 85 7/117 (5·3%) 8/123 (5·5%) 1·0 ( 0·2, 3·3) 0·92
Atrial fibrillation (Interaction: p= 0·66)
No 13/428 (2·7%) 16/433 (3·3%) 0·8 ( 0·3, 1·8) 0·58
Yes 13/ 82 (12·8%) 13/ 91 (12·1%) 1·1 ( 0·5, 2·4) 0·88
Acute coronary syndrome (Interaction: p= 0·61)
No 12/283 (3·8%) 16/292 (4·8%) 0·8 ( 0·3, 1·7) 0·50
Yes 14/229 (5·2%) 13/233 (4·9%) 1·1 ( 0·5, 2·5) 0·88
Sex (Interaction: p= 0·48)
Male 17/323 (4·7%) 16/327 (4·3%) 1·1 ( 0·5, 2·3) 0·82
Female 9/189 (4·0%) 13/198 (5·8%) 0·7 ( 0·2, 1·7) 0·38
Diabetes Mellitus (Interaction: p= 0·53)
No 18/379 (4·2%) 23/391 (5·2%) 0·8 ( 0·4, 1·5) 0·47
Yes 8/132 (5·1%) 6/133 (3·9%) 1·3 ( 0·4, 6·6) 0·60
Major bleed (BARC 2-5)
at 1 year
DES
(N=596)
BMS
(N=604)
Relative Risk
(95% CI) P-value
DES
Better
BMS
Better
0 0·5 1 1·5 2 2·5Percentages are Cumulative Incidence Function estimates·
23
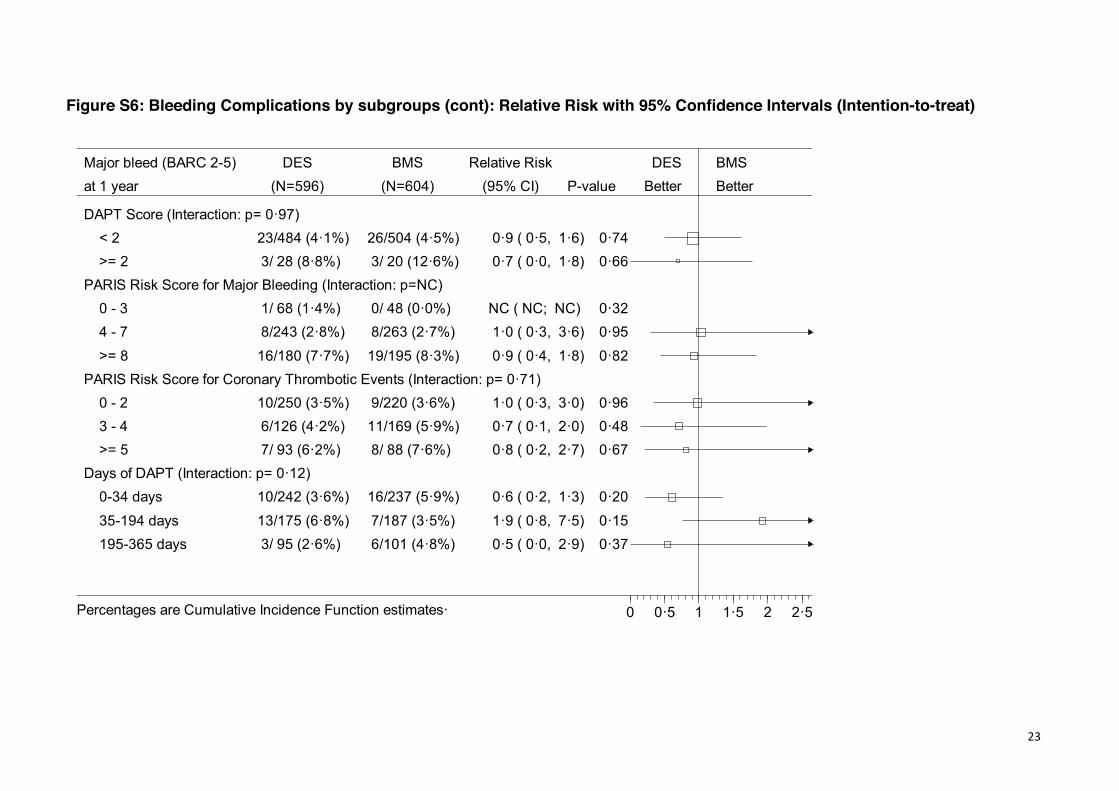
Figure S6: Bleeding Complications by subgroups (cont): Relative Risk with 95% Confidence Intervals (Intention-to-treat)
DAPT Score (Interaction: p= 0·97) < 2 23/484 (4·1%) 26/504 (4·5%) 0·9 ( 0·5, 1·6) 0·74 >= 2 3/ 28 (8·8%) 3/ 20 (12·6%) 0·7 ( 0·0, 1·8) 0·66PARIS Risk Score for Major Bleeding (Interaction: p=NC) 0 - 3 1/ 68 (1·4%) 0/ 48 (0·0%) NC ( NC; NC) 0·32 4 - 7 8/243 (2·8%) 8/263 (2·7%) 1·0 ( 0·3, 3·6) 0·95 >= 8 16/180 (7·7%) 19/195 (8·3%) 0·9 ( 0·4, 1·8) 0·82PARIS Risk Score for Coronary Thrombotic Events (Interaction: p= 0·71) 0 - 2 10/250 (3·5%) 9/220 (3·6%) 1·0 ( 0·3, 3·0) 0·96 3 - 4 6/126 (4·2%) 11/169 (5·9%) 0·7 ( 0·1, 2·0) 0·48 >= 5 7/ 93 (6·2%) 8/ 88 (7·6%) 0·8 ( 0·2, 2·7) 0·67Days of DAPT (Interaction: p= 0·12) 0-34 days 10/242 (3·6%) 16/237 (5·9%) 0·6 ( 0·2, 1·3) 0·20 35-194 days 13/175 (6·8%) 7/187 (3·5%) 1·9 ( 0·8, 7·5) 0·15 195-365 days 3/ 95 (2·6%) 6/101 (4·8%) 0·5 ( 0·0, 2·9) 0·37
Major bleed (BARC 2-5)at 1 year
DES(N=596)
BMS(N=604)
Relative Risk(95% CI) P-value
DESBetter
BMSBetter
0 0·5 1 1·5 2 2·5Percentages are Cumulative Incidence Function estimates·
24
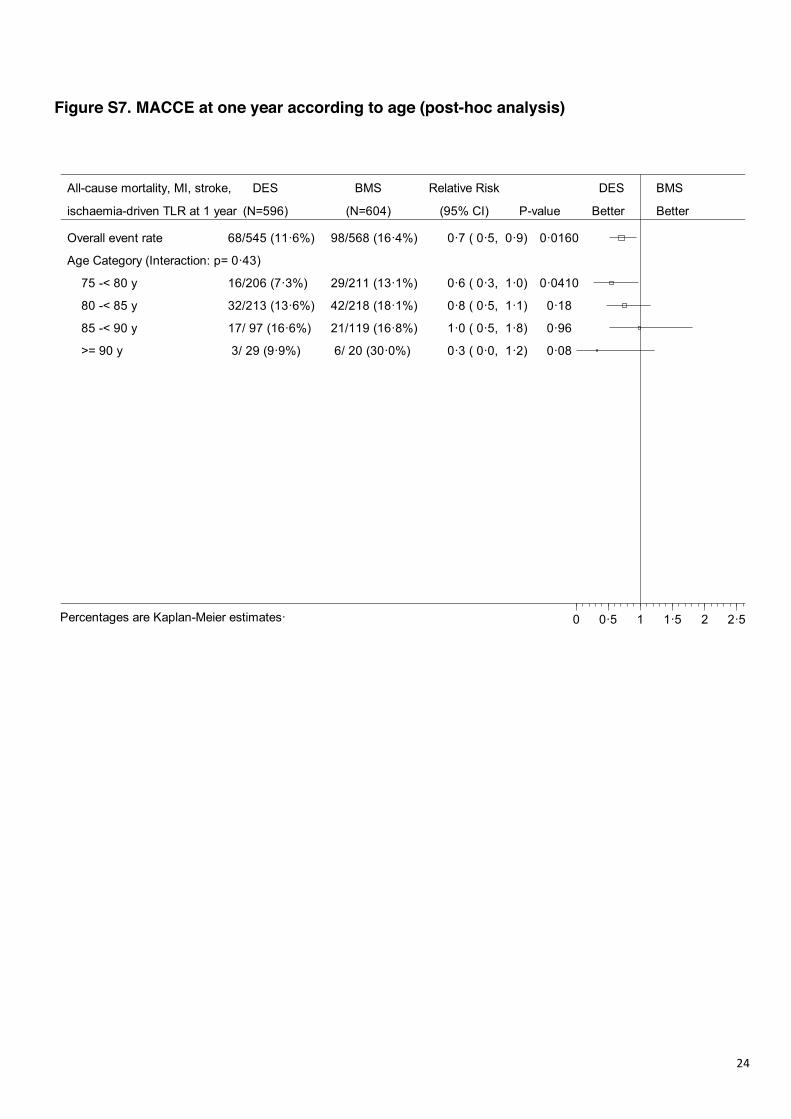
Figure S7. MACCE at one year according to age (post-hoc analysis)
Overall event rate 68/545 (11·6%) 98/568 (16·4%) 0·7 ( 0·5, 0·9) 0·0160
Age Category (Interaction: p= 0·43)
75 -< 80 y 16/206 (7·3%) 29/211 (13·1%) 0·6 ( 0·3, 1·0) 0·0410
80 -< 85 y 32/213 (13·6%) 42/218 (18·1%) 0·8 ( 0·5, 1·1) 0·18
85 -< 90 y 17/ 97 (16·6%) 21/119 (16·8%) 1·0 ( 0·5, 1·8) 0·96
>= 90 y 3/ 29 (9·9%) 6/ 20 (30·0%) 0·3 ( 0·0, 1·2) 0·08
All-cause mortality, MI, stroke,
ischaemia-driven TLR at 1 year
DES
(N=596)
BMS
(N=604)
Relative Risk
(95% CI) P-value
DES
Better
BMS
Better
0 0·5 1 1·5 2 2·5Percentages are Kaplan-Meier estimates·
25
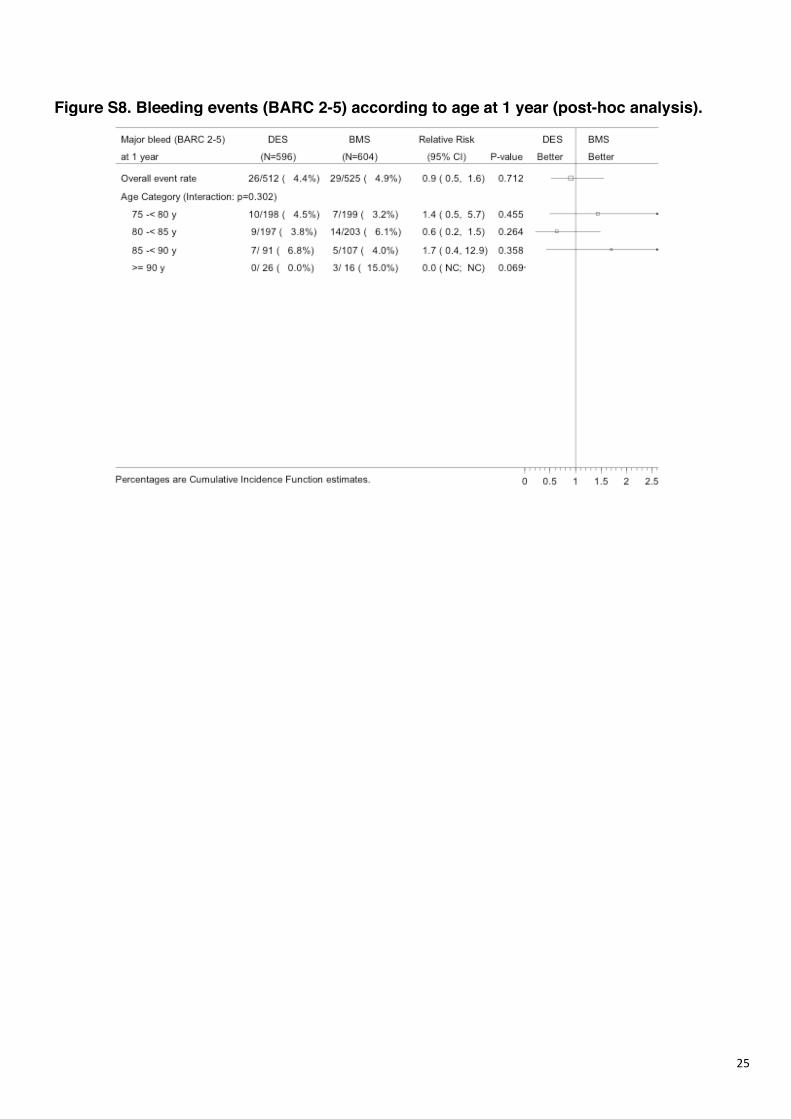
Figure S8. Bleeding events (BARC 2-5) according to age at 1 year (post-hoc analysis).

26
Figure S9: Time line of stent thrombosis during and after discontinuation of
thienopyridine treatment.
Post-hoc analysis.
27
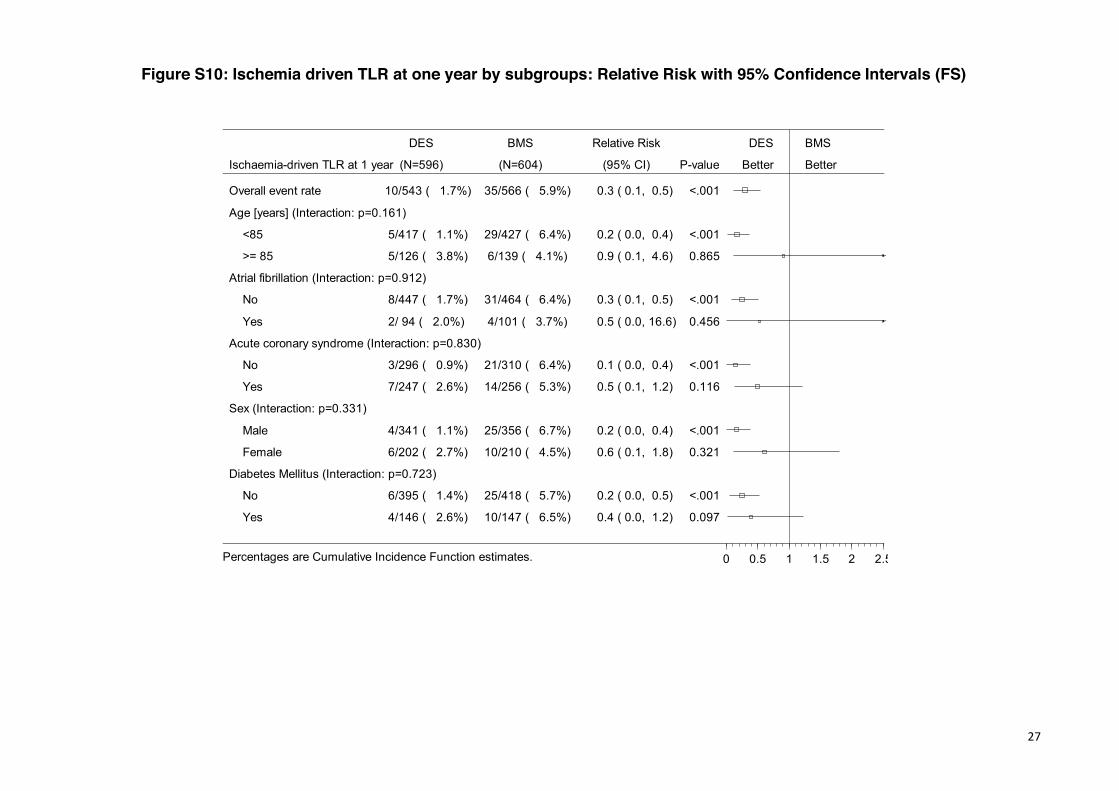
Figure S10: Ischemia driven TLR at one year by subgroups: Relative Risk with 95% Confidence Intervals (FS)
Overall event rate 10/543 ( 1.7%) 35/566 ( 5.9%) 0.3 ( 0.1, 0.5) <.001
Age [years] (Interaction: p=0.161)
<85 5/417 ( 1.1%) 29/427 ( 6.4%) 0.2 ( 0.0, 0.4) <.001
>= 85 5/126 ( 3.8%) 6/139 ( 4.1%) 0.9 ( 0.1, 4.6) 0.865
Atrial fibrillation (Interaction: p=0.912)
No 8/447 ( 1.7%) 31/464 ( 6.4%) 0.3 ( 0.1, 0.5) <.001
Yes 2/ 94 ( 2.0%) 4/101 ( 3.7%) 0.5 ( 0.0, 16.6) 0.456
Acute coronary syndrome (Interaction: p=0.830)
No 3/296 ( 0.9%) 21/310 ( 6.4%) 0.1 ( 0.0, 0.4) <.001
Yes 7/247 ( 2.6%) 14/256 ( 5.3%) 0.5 ( 0.1, 1.2) 0.116
Sex (Interaction: p=0.331)
Male 4/341 ( 1.1%) 25/356 ( 6.7%) 0.2 ( 0.0, 0.4) <.001
Female 6/202 ( 2.7%) 10/210 ( 4.5%) 0.6 ( 0.1, 1.8) 0.321
Diabetes Mellitus (Interaction: p=0.723)
No 6/395 ( 1.4%) 25/418 ( 5.7%) 0.2 ( 0.0, 0.5) <.001
Yes 4/146 ( 2.6%) 10/147 ( 6.5%) 0.4 ( 0.0, 1.2) 0.097
Ischaemia-driven TLR at 1 year
DES
(N=596)
BMS
(N=604)
Relative Risk
(95% CI) P-value
DES
Better
BMS
Better
0 0.5 1 1.5 2 2.5Percentages are Cumulative Incidence Function estimates.
28
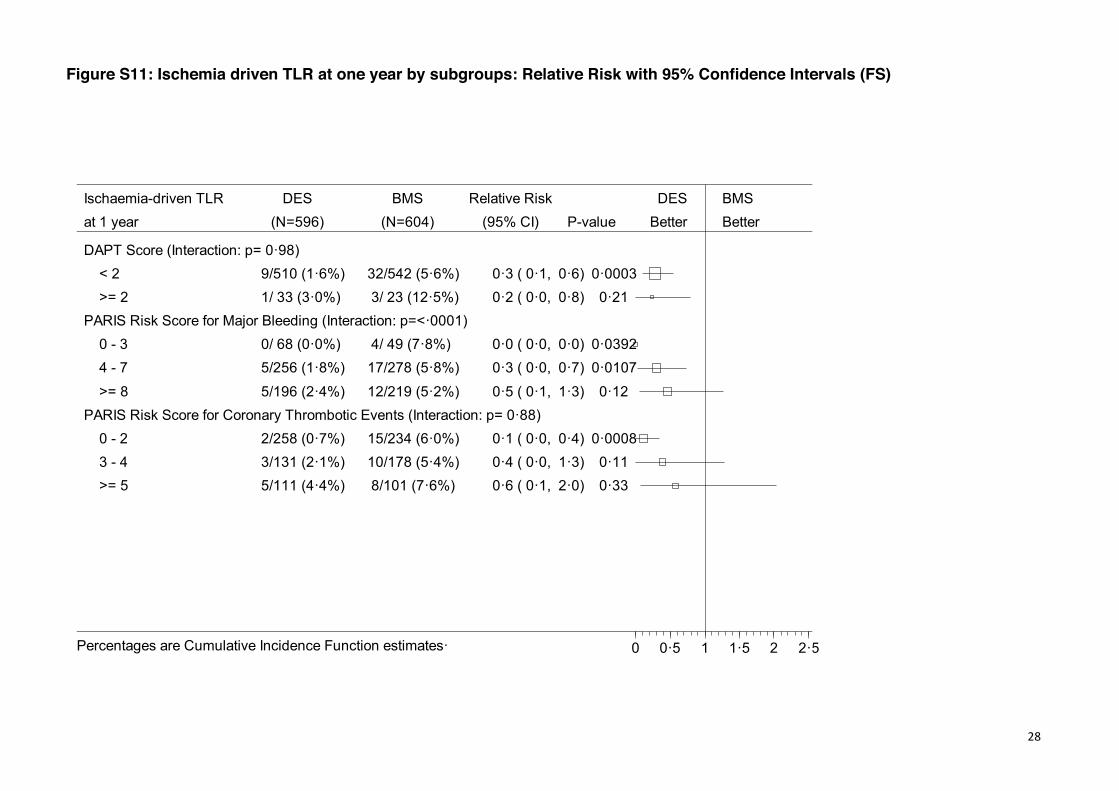
Figure S11: Ischemia driven TLR at one year by subgroups: Relative Risk with 95% Confidence Intervals (FS)
DAPT Score (Interaction: p= 0·98) < 2 9/510 (1·6%) 32/542 (5·6%) 0·3 ( 0·1, 0·6) 0·0003 >= 2 1/ 33 (3·0%) 3/ 23 (12·5%) 0·2 ( 0·0, 0·8) 0·21PARIS Risk Score for Major Bleeding (Interaction: p=<·0001) 0 - 3 0/ 68 (0·0%) 4/ 49 (7·8%) 0·0 ( 0·0, 0·0) 0·0392 4 - 7 5/256 (1·8%) 17/278 (5·8%) 0·3 ( 0·0, 0·7) 0·0107 >= 8 5/196 (2·4%) 12/219 (5·2%) 0·5 ( 0·1, 1·3) 0·12PARIS Risk Score for Coronary Thrombotic Events (Interaction: p= 0·88) 0 - 2 2/258 (0·7%) 15/234 (6·0%) 0·1 ( 0·0, 0·4) 0·0008 3 - 4 3/131 (2·1%) 10/178 (5·4%) 0·4 ( 0·0, 1·3) 0·11 >= 5 5/111 (4·4%) 8/101 (7·6%) 0·6 ( 0·1, 2·0) 0·33
Ischaemia-driven TLRat 1 year
DES(N=596)
BMS(N=604)
Relative Risk(95% CI) P-value
DESBetter
BMSBetter
0 0·5 1 1·5 2 2·5Percentages are Cumulative Incidence Function estimates·
29
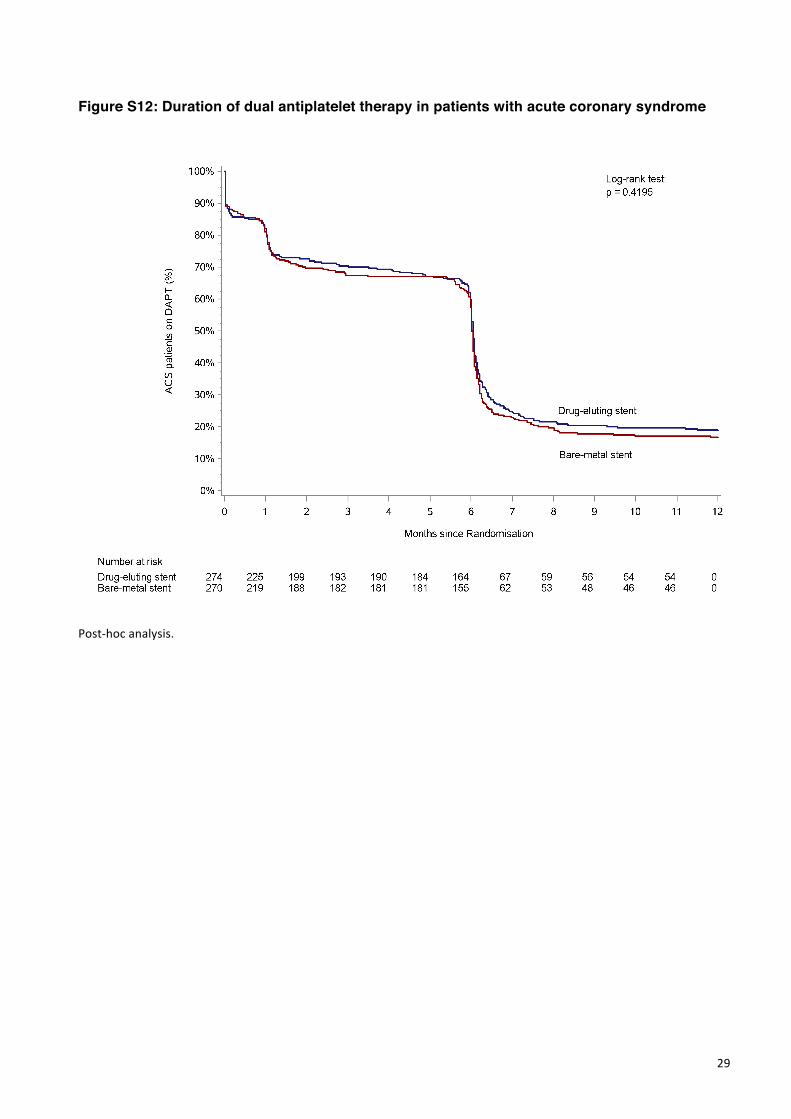
Figure S12: Duration of dual antiplatelet therapy in patients with acute coronary syndrome
Post-hocanalysis.
30
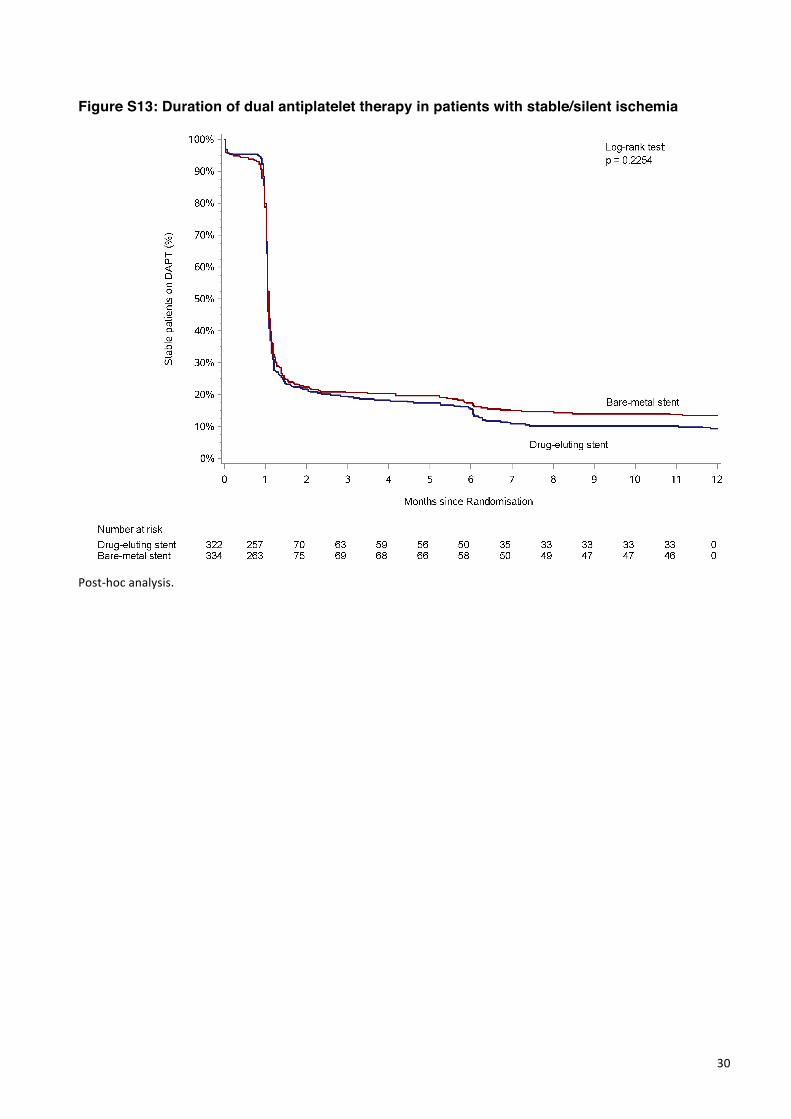
Figure S13: Duration of dual antiplatelet therapy in patients with stable/silent ischemia
Post-hocanalysis.
31
G: Authors affiliations.
Olivier Varenne (Service de Cardiologie, Hôpital Cochin, APHP, Paris, France and Université Paris Descartes, Sorbonne Paris-Cité, Paris France), Stéphane Cook (University & Hospital Fribourg. Fribourg, Switzerland), Georgios Sideris (Department of Cardiology - Inserm U942, Lariboisiere Hospital, AP-HP, Paris Diderot University, Paris, France), Sasko Kedev (University St. Cyril & Methodius, Skopje, Macedonia), Thomas Cuisset (Département de Cardiologie, CHU Timone, Marseille, France), Didier Carrié (Service de Cardiologie, CHU Toulouse Rangueil, University Paul Sabatier, Toulouse, France), Thomas Hovasse (Institut Cardiovasculaire Paris-Sud, Ramsay Générale de Santé, Massy, France), Philippe Garot (Institut Cardiovasculaire Paris-Sud, Ramsay Générale de Santé, Massy and Quincy, France), Rami El Mahmoud (Assistance Publique Hôpitaux de Paris - Hôpital Ambroise Paré Université Versailles-Saint Quentin en Yvelines, France), Christian Spaulding (Department of cardiology, Hôpital Européen Georges Pompidou, APHP, Paris Descartes University and Sudden Death Expert Center, INSERM U 990, Paris, France), Gérard Helft (Institut de Cardiologie, Hôpital Pitié-Salpétrière, APHP, Université Pierre et Marie Curie et IHU, Institute of Cardiometabolism and Nutrition, Hôpital Pitié-Salpétrière, Paris, France), José F. Diaz (Juan Ramón Jiménez University Hospital. Huelva, Spain), Salvatore Brugaletta (Cardiovascular Institute, Hospital Clinic, Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain), Eduardo Pinar (Hospital Universitario Virgen de la Arrixaca. Murcia, Spain), Josepa Fina Mauri (Hospital Universitari Germans Trias i Pujol, Badalona, Spain), Philippe Commeau (Département de Cardiologie Interventionnelle, Polyclinique Les Fleurs, Ollioules, France), Emmanuel Teiger (AP-HP, University hospital Henri Mondor, Interventional Cardiology Deparment, Créteil, France), Kris Bogaerts (Interuniversity Institute for Biostatistics and Statistical Bioinformatics, KU Leuven, Leuven, Belgium and University Hasselt, Hasselt, Belgium), Manel Sabate (Interventional Cardiology Unit; Cardiovascular Institute; Hospital Clinic; IDIBAPS; Barcelona; Spain), Marie-Claude Morice (Cardiovascular European Research Center, Massy, France), Peter R. Sinnaeve (University Hospitals Leuven - Department of Cardiovascular Medicine).
32
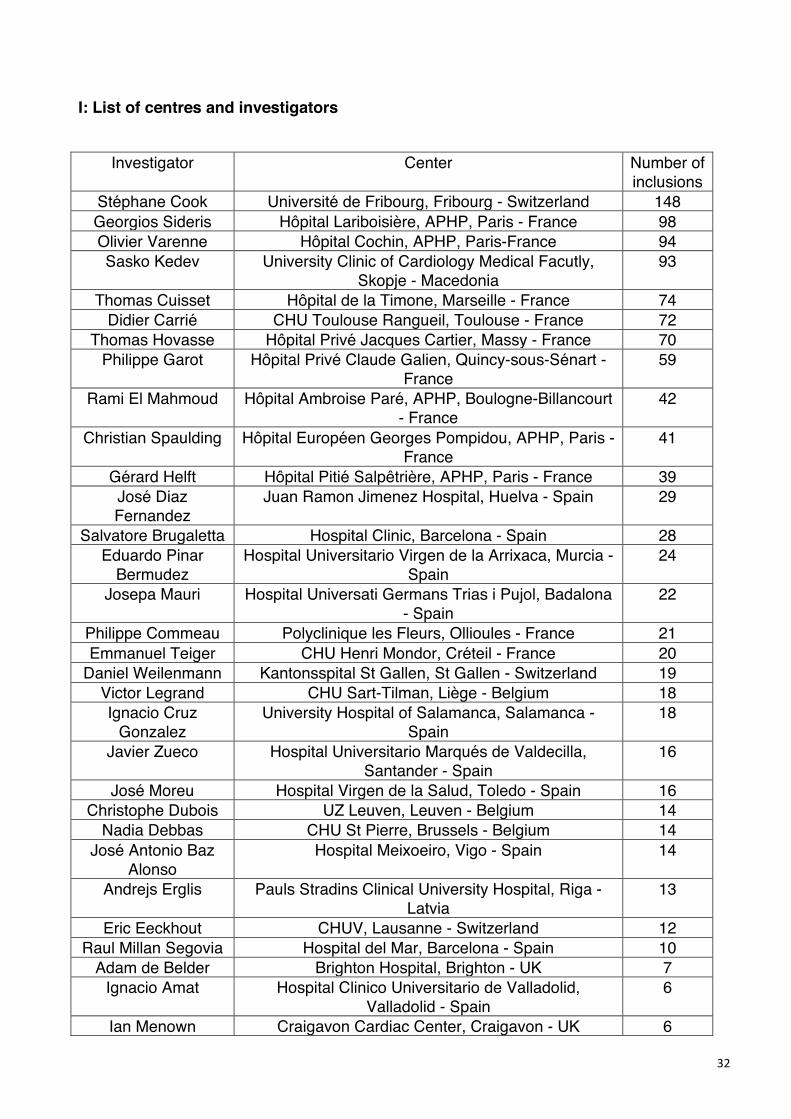
I: List of centres and investigators
Investigator Center Number of
inclusions Stéphane Cook Université de Fribourg, Fribourg - Switzerland 148 Georgios Sideris Hôpital Lariboisière, APHP, Paris - France 98 Olivier Varenne Hôpital Cochin, APHP, Paris-France 94 Sasko Kedev University Clinic of Cardiology Medical Facutly,
Skopje - Macedonia 93
Thomas Cuisset Hôpital de la Timone, Marseille - France 74 Didier Carrié CHU Toulouse Rangueil, Toulouse - France 72
Thomas Hovasse Hôpital Privé Jacques Cartier, Massy - France 70 Philippe Garot Hôpital Privé Claude Galien, Quincy-sous-Sénart -
France 59
Rami El Mahmoud Hôpital Ambroise Paré, APHP, Boulogne-Billancourt - France
42
Christian Spaulding Hôpital Européen Georges Pompidou, APHP, Paris - France
41
Gérard Helft Hôpital Pitié Salpêtrière, APHP, Paris - France 39 José Diaz Fernandez
Juan Ramon Jimenez Hospital, Huelva - Spain 29
Salvatore Brugaletta Hospital Clinic, Barcelona - Spain 28 Eduardo Pinar
Bermudez Hospital Universitario Virgen de la Arrixaca, Murcia -
Spain 24
Josepa Mauri Hospital Universati Germans Trias i Pujol, Badalona - Spain
22
Philippe Commeau Polyclinique les Fleurs, Ollioules - France 21 Emmanuel Teiger CHU Henri Mondor, Créteil - France 20
Daniel Weilenmann Kantonsspital St Gallen, St Gallen - Switzerland 19 Victor Legrand CHU Sart-Tilman, Liège - Belgium 18 Ignacio Cruz
Gonzalez University Hospital of Salamanca, Salamanca -
Spain 18
Javier Zueco Hospital Universitario Marqués de Valdecilla, Santander - Spain
16
José Moreu Hospital Virgen de la Salud, Toledo - Spain 16 Christophe Dubois UZ Leuven, Leuven - Belgium 14
Nadia Debbas CHU St Pierre, Brussels - Belgium 14 José Antonio Baz
Alonso Hospital Meixoeiro, Vigo - Spain 14
Andrejs Erglis Pauls Stradins Clinical University Hospital, Riga - Latvia
13
Eric Eeckhout CHUV, Lausanne - Switzerland 12 Raul Millan Segovia Hospital del Mar, Barcelona - Spain 10
Adam de Belder Brighton Hospital, Brighton - UK 7 Ignacio Amat Hospital Clinico Universitario de Valladolid,
Valladolid - Spain 6
Ian Menown Craigavon Cardiac Center, Craigavon - UK 6
33
Benjamin Wrigley New Cross Hospital, Wolverhampton - UK 6 Marco Caruso Arnas Civico Palermo, Palermo - Italy 5
Ramon Lopez Palop Hospital San Juan de Alicante, Alicante - Spain 5 Antonio Serra Hospital de la Santa Creu I Sant Pau, Barcelona -
Spain 5
Azfar Zaman Freeman Hospital, Newcastle Upon Tyne Hospitals 5 Jonathan Hill King’s College Hospital, London - UK 5 Florim Cuculi Kantonsspital Luzern, Luzern - Switzerland 4
Pasi Karjalainen Heart Center, Satakunta Central Hospital, Pori - Finland
2
Kari Kervinen Oulu University Hospital, Oulu - Finland 2 Ramon Calvino
Santos Hospital Universitario A Coruña, A Coruña - Spain 2
Claudiu Ungureanu Centre Hospitalier de Jolimont, La Louvière - Belgium
1
Simon Redwood Guy’s and St Thomas’ NHS Foundation Trust, London - UK
1










![Self-expandable metallic stents for the palliation of ...cancer-research-frontiers.org/wp-content/uploads/... · palliation of dysphagia in patients with esophageal cancer [9]. The](https://img.pdfslide.us/doc/110x75/5f0252b17e708231d403b3a8/self-expandable-metallic-stents-for-the-palliation-of-cancer-research-palliation.jpg)