Embed Size (px)
Citation preview

1
SUPPLEMENTARY MATERIAL
Mutations in MEGF10, a regulator of satellite cell myogenesis, cause early‐
onset myopathy, areflexia, respiratory distress and dysphagia (EMARDD)
Clare V. Logan1*, Barbara Lucke2*, Caroline Pottinger3*, Zakia A. Abdelhamed1,7, David A. Parry1, Katarzyna Szymanska1, Christine P. Diggle1, Anne van Riesen2, Joanne E. Morgan1, Grace Markham1, Ian Ellis4, Adnan Y. Manzur5, Alexander F. Markham1, Mike Shires1, Tim Helliwell6, Mariacristina Scoto5, Christoph Hübner2, David T. Bonthron1, Graham R. Taylor1, Eamonn Sheridan1, Francesco Muntoni5, Ian M. Carr1, Markus Schuelke2§, Colin A. Johnson1§
1 Leeds Institute of Molecular Medicine, The University of Leeds, UK. 2 Department of Neuropediatrics and
NeuroCure Clinical Research Center, Charité Universitätsmedizin Berlin, Berlin, Germany. 3 Clinical Genetics Unit,
West Midlands Regional Genetics Service, Birmingham Women’s Hospital, Birmingham, UK. 4 Department of
Clinical Genetics, Alder Hey Children's Hospital, Liverpool, UK. 5 Dubowitz Neuromuscular Centre, Institute of
Child Health & Great Ormond Street Hospital for Children, London, UK. 6 Duncan Building, Royal Liverpool
University Hospital, Liverpool, UK. 7 Department of Anatomy & Embryology, Faculty of Medicine (Girls’ Section),
Al‐Azhar University, Cairo, Egypt.
* These authors contributed equally to this work.
§ These authors jointly directed the project.
Correspondence should be addressed to C.A.J. ([email protected]) or M.S. ([email protected]).
Nature Genetics: doi:10.1038/ng.995

2
SUPPLEMENTARY FIGURES
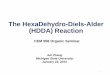
Supplementary Figure 1: Haplotype analysis of family B for the EMARDD locus on chromosome 5q23. The
indicated microsatellite markers were genotyped for all available individuals in generations III to V. The minimal
interval is indicated by the arrow (boundaries 119.1‐135.3 Mb) with the putative disease haplotype in black.
Segregation of other haplotypes is indicated by various patterned fills.
Nature Genetics: doi:10.1038/ng.995

marker Mb (B36.1)
D5S1505 119.10 962162852452 452452852452D5S2120 128.43 251741251741 541741251741D5S2110 130.88 562962762562 962562762562D5S2117 133.06 722DN422422 512422422422D5S816 135.30 732052232732 542732232732
D5S1505 119.10 852452452452852452452452852452962452962852962452962852962852162852D5S2120 128.43 251741541741741741541741741541251741251251251741251251251251741251D5S2110 130.88 762562962562562562962562562962562562562762562562562762562762962762D5S2117 133.06 422422512422422422512422422512722422722422722422722422722422DN422D5S816 135.30 232732542732732732542732732542732732732232732732732232732232052232
D5S1505 119.10 254 258D5S2120 128.43 147 147D5S2110 130.88 265 265D5S2117 133.06 224 224D5S816 135.30 237 245
EMARRD
Nature Genetics: doi:10.1038/ng.995

4
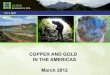
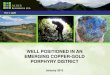
Supplementary Figure 2: Mutations identified in MEGF10 for five kindreds with EMARDD. (a) Upper panel:
scheme of MEGF10 genomic structure shows non‐coding exons as gray and coding (exons 3 to 26) as black lines.
The MEGF10 protein contains an extracellular EMI domain8,9, 17 EGF‐like repeats (blue boxes), a transmembrane
domain (TM) and two conserved intracellular motifs (NPXY and YXXL) of unknown function10. Lower panel:
mutations in EMARDD affected patients in families A to E, with changes in nucleotide and protein coding
indicated by arrows (red for nonsense or frameshift mutations, purple for a missense mutation). Affected
patient E.II:1 was compound heterozygous for the mutations (c.1325delC)+(c.2320T>C), causing the predicted
protein alterations (p.P442HfsX9)+(p.C774R). (b) ClustalX version 2 alignment11 of the indicated representative
MEGF10 orthologs against the human (H. sapiens) protein, showing the conservation of residue C774 (purple
arrow) in the 16th EGF‐like repeat.
Nature Genetics: doi:10.1038/ng.995

protein: 1140 aa
126667001 126793010genomic:170.36 kb
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 20 21 22 23 24 25 26
NPXY YXXLTMEMI
MEGF10
family Bc.2288_2297dup
p.D766EfsX4
TGTC AA A A C GGA GC TG A A C G GA GC TG A C T GC GAC Q N G A E R S X
TGTC AA A A C GGA GCT G AC TGC G AC CA C AT T TC TG C Q N G A D C D H I S
transcript: 3423 ntATG TGA
family Cc.2301C>A
p.C767X
TGTC AA A A C GGA GCT G AC T G A G AC CA C AT T TC TG C Q N G A D X
wild-type
family Dc.3144T>G
p.Y1048X
wild-type
GGTT A GG TGG AGG X
GGTT A T G TGG AGG Y V E
family Ac.1559G>A
p.W520X
wild-type
GG AT A GC G CGGGG X
GG AT G GC G CGGGG W R G
GGGC AG Y GT ACT G Q R T
family Ec.2320T>C
p.C774R
wild-type
19
TC T A CC CS T
family Ec.1325delC
p.P442HfsX9
wild-type
TC T AC C CCA T G C C C TS T P C P
GGG CAG T GT AC T G Q C T
a
b C774
Nature Genetics: doi:10.1038/ng.995

6
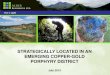
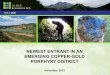
Supplementary Figure 3: Transcript and histopathological analysis of EMARDD muscle tissue. (a) Reverse‐
transcription PCR (RT‐PCR) analysis of the MEGF10 transcript. Total mRNA was extracted, reverse transcribed
and analyzed by semi‐quantitative PCR from a control muscle biopsy specimen and EMARDD patient B.V:1
muscle biopsy specimen. Adult muscle cDNA library (Clontech) was used as a positive (+ve) control, with a
reaction negative control (‐ve), as indicated. Transcripts were analyzed for MEGF10 (top panel) using a primer
pair between exons 18 to 20 (Supplementary Table 2). TP53 was used as a loading control (bottom panel). (b)
H&E stained longitudinal section of the deltoid muscle from EMARDD patient B.V:1. In comparison to the control
muscle, the fusion of myocytes into multinuclear myotubes or muscle fibers is incomplete with fewer myonuclei
per fiber, suggestive of defective myogenesis and incomplete myoblast fusion.
Nature Genetics: doi:10.1038/ng.995

+ve c
ontro
l
healt
hy co
ntrol
EMARDD patie
nt
-ve co
ntrol
MEGF10
TP53
ladde
r (bp
)
500400
300200100
500400
300200100
ab control
EMARDD patient (B.V:1)
Nature Genetics: doi:10.1038/ng.995

8
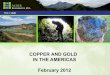
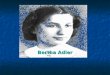
Supplementary Figure 4: Expression of the Megf10 transmembrane receptor in normal embryonic and adult
mouse tissues. (a) Western blotting of whole cellular extract from wild‐type mouse embryonic fibroblasts with a
rabbit polyclonal anti‐Megf10 antibody visualized a single band of the expected size of 120 kDa. (b)
Immunocytochemical (ICC) staining of a transverse section from the caudal neural tube of wild‐type E11 mouse
embryo with anti‐Megf10 (green channel) and Pax6 (red channel). Moderate Megf10 expression, in the ventral
ventricular zone, where Pax6 positive precursors develop into somatic motoneurons (arrowheads).
Immunohistochemical (IHC) staining of a midline sagittal section of wild‐type E15.5 female mouse embryo with
an anti‐Megf10 antibody (brown), counterstained with Mayer’s hematoxylin (purple) for (c) head structures and
CNS, and (d) visceral organs. High Megf10 expression in developing E15.5 embryonic (e) neocortex, particularly
the basement membrane and cortical plate, (f) skeletal muscle adjacent to the hip bone and (g) in muscles of
the anterior chest wall. Moderate expression in adult mouse (h) diaphragm muscles, (i) pectoralis major muscle,
and (j) cell bodies of the inter‐and motoneurons in the grey matter of adult mouse spinal cord. (k) High
expression in neuromuscular junctions (arrowheads), confirmed in an adjacent section by (l) colocalization of
Megf10 (red channel) with α‐bungarotoxin (green channel). Scale bars: (b) = 30 μm; (c & d) = 500 μm; (e to k) =
50 μm, with subdivisions of 10 μm; (l) = 50 μm. Abbreviations: AP, alar plate; BP, basal plate; cb, cerebellum; cc,
costal cartilage; co, cortex; FP, floor plate; h, heart; icm, intercostal muscles; li, liver; lu, lung; mb, mid‐brain; pm,
pectoralis major muscle; pvm, perivertebral spinal muscles; RP, roof plate; sm, skeletal muscle; ttm, transversus
thoracis muscle, sc, spinal cord; vms, ventral‐median sulcus; 3V, third ventricle; 4V, fourth ventricle.
Nature Genetics: doi:10.1038/ng.995

Pax6 Megf10 merge
E11
FPBP
AP
RP
E15.5
a
c d
gf
bMEGF10120 kDa
co
3V 4V
mb
cb
sc
sc
pvmpm
hli
lu
pm cc
cc
icmttm
sm
adult
i
k
h
j
vms
e
VZ
IZ
CPMZ
BM
l α-bungarotoxinMegf10 merge
Nature Genetics: doi:10.1038/ng.995

10
Supplementary Figure 5: Expression of MEGF10 in EMARRD muscle. (a) IHC staining of deltoid muscle tissue
biopsy from EMARDD patient B.V:1, compared to transverse and longitudinal sections of control muscle tissue,
showing loss of MEGF10 protein in muscle fibers. (b) ICC staining of control muscle tissue for MEGF10 (red
channel), PAX7 (green channel) and DAPI (blue channel) shows MEGF10 expression and several PAX7+ satellite
cells (arrows), whereas EMARDD muscle from patient B.V:1 shows absence of MEGF10 protein expression and of
detectable PAX7+ nuclei.
Nature Genetics: doi:10.1038/ng.995

EMARDD patient (B.V:1)control
MEG
F10
control
EMARDDpatient(B.V:1)
MEGF10 PAX7 DAPI merge
100µm
100µm
a
b
30 µm
Nature Genetics: doi:10.1038/ng.995

12
SUPPLEMENTARY TABLES
Supplementary Table 1: Oligonucleotide primers used for sequence analysis and mRNA reverse transcription
analysis of MEGF10. The forward and reverse primers used for PCR and Sanger sequencing of all the exons in
MEGF10 are indicated. The RT18‐20 primer pair indicates the primers used for RT‐PCR.
exon forward primer reverse primer
1 CCCCACCCCCTCCAGCATCT CCCATCTCGCCCCACCTCAC 2 TCCCTGGCCAGTAGGAATCC TCCTTTCGCCACCCACGAAG 3 CCTCTCTCCTGGACCATGGA CACCACCTAATTTGCTAGCTATGAC 4 AGTCACTATGGAGTTGCAAATGG TAAGACAGGAGCAAGCCCTCAAT 5 CATAGATTGGCTTCAATAGGGAATC GTAGCAACCAGAGGGAAAAGGAATG 6 GAGGAACGGACTGAAGAAAATTATC CGTGGCATTTACACTATGCT 7 AAGCATTGCCATGGGTTGGG CCTAGACCCATCAGTAACTC 8 AACACAGAAAGCTTGTCTATTTTGG ATTTTGGAATCTTCAACCATCATGG 9 ATTTTCTTGCAGCCCTGTTCCCCAT CATTGAGGCTGTATAGCTACTTCTG 10 ATTGCAAGAGCAAAAAGCAGCTTCG CCAGAGTAGCCTAGAGGCAG 11 CCAAGCCTGGGAATGAAGTTTGAAT TTTCTCTCTCTCTTTAATGATGTGG 12 GAGAGGAAGTATAATTAGCATTGCC CGGAGGTCAGACACTGAATTTT 13 GCTGGGGCTTGCATCTCCAA TTCCAGTAGTTACCGAAGTTGG 14 TCCCTGTAAGAAGCGTTTGGGA GGTTTCAGTTTACTGGAAACCTTATCG 15 CTGCTGGTGATCCTCAGGTT GGACAAGTGAACCATTACACTCTCTTT 16 CCTCTAAAACTTTAACTAGATCCCG CCAGCTGCTCATTGGTAGCT 17 AGCTACCAATGAGCAGCTGG TTTAAAGTAGAATGTGTCTTTTAATTAGTC 18 GCTAACCTCTCACATGCAGG CTACAGGTCATTAGGAGAGG 19 CTGATGGCTCAGTGTCATTCAAGTT GAAGTAACCAGCCATCAGCTCAA 20 TCAATAGGAATCCCCTGAAAGGA GTAACCAATTATGCCATTTAGAGTTGTG 21 ATGAACTGAAAATATGCAGGCATTAGCA CTTTTCCAAACATAGAATTCTCTCAATG 22 CTGTTTTGTTATTTTGATTCCC CCCTTCCTCTCTCCCCAGCC 23 ACTCTAAGGACTGGTCCTCAATA TCTGCTATTGTGCTTTTTGATGCAAG 24 TTGCTGCAGTGGGAGATCCT TTGCTGTAGTAACTGACCACACTAA 25 TTCAGTGTGTAGAATTATGGAAACCTAG GAGACCCCATCTCAAAAAATACATAAAATA 26 CATGTTTTTAAAACCAGCATTTCCTTATAT AAAAATTGCCCACCGAATTGACTAA
RT18‐20 GCCATAATGGAGCTTTCTGC AACAGGTCCCAGTGATGTGG
Nature Genetics: doi:10.1038/ng.995

13
Supplementary Table 2: Clinical features of individuals with EMARDD (Early‐onset Myopathy; Areflexia; Respiratory Distress; Dysphagia) compared to infantile
SMARD type 1. a Families A and C were described previously and correspond to families 2 and 1 of ref. 7; b loss of ambulation at the age of 12.5 years; c normal function
of the neuromuscular junction (transmission) as verified by electrophysiology with normal amplitudes of the compound muscle action potential upon repetitive nerve
stimulation; d died of respiratory failure; e only nocturnal mechanical ventilation; # age at death; * features not observed in infantile SMARD1 (MIM #604320) in bold
print. Abbreviations: F, female; M, male; mo, months; nd, not determined.
Nature Genetics: doi:10.1038/ng.995

14
Pedigree ID A.II:1a A.II:2a B.IV:9 B.IV:10 B.V:1 C.II:3a C.II:4a D.IV:5 D.IV:6 E.II:1
Total MEGF10 mutation(s)
homozygous c.1559G>A, p.W520X; Exon 13c
homozygous c.2288_2297dup, p.D766EfsX4;
Exon 19
homozygous c.2301C>A, p.C767X; Exon 19
homozygous c.3144T>G, p.Y1048X; Exon 25
compound heterozygous c.1325delC, p.P442HfsX9Exon 12
c.2320T>C, p.C774R, Exon 19
Country of origin Sri Lanka (Tamil) Pakistan Qatar Turkey England Gender and years of age (# age at death) F15 M12 M(#12.5) M(#0.8) F2 F(#9) F1.1 M(#0.9) F(#0.9) M8
EARLY MYOPATHY features and associated results Decreased fetal movements + + ‐ ‐ ‐ + ‐ + + nd 5/9 + *High‐arched palate (++, cleft palate) nd nd ‐ nd ‐ ‐ ++ + + + 4/7 + Muscular hypotonia (++, at birth) ++ ++ + + + + ++ + ++ ++ 10/10 + Poor head control (++, severe) nd + nd nd nd ++ ++ + + ++ 6/6 + Facial weakness ‐ ‐ + nd ‐ + + + + + 6/9 + Finger contractures or equinovarus (++, at birth; +, at 6 mo) ++ ++ nd nd ‐ + ‐ + ++ + 6/8 + Weakness more marked in upper limbs nd + nd nd nd nd + + + ‐ 4/5 + Weakness more marked distally than proximally + + + nd + nd + nd nd ‐ 5/6 + Scoliosis + + + nd + + ‐ + + ++ 8/9 + *+++, walks; *++, stands; +, sits (with support) +++b (++) ‐ ‐ ‐ (+++) (+) ‐ ‐ +++ 5/10 + *Myopathic pattern on electromyography + + nd nd + + + nd ‐ + 6/7 + *Myopathic muscle tissue with variation in fiber size (++, additional fiber necrosis and replacement with fibrous/adipose tissue)
+ nd ++ nd + + + ‐ nd + 6/7 +
Normal serum creatine kinase activity + + + nd + nd + nd + + 7/7 +
AREFLEXIA feature and associated results Achilles tendon reflexes absent (++, all tendon reflexes absent) ++ ++ nd nd + ++ ++ ++ ++ ‐ 7/8 + Normal nerve conduction velocity +c + + nd + +c + + + + 9/9 +
RESPIRATORY DISTRESS features Respiratory distress (++, onset at birth; +, at 1 to 7 mo) ++ + + ++ + ++ ++ + + + 10/10 + Eventration of diaphragm on X‐ray or ultrasound ‐ ‐ + + ‐ + + + + nd 6/9 + Permanent mechanical ventilation (++, from 3‐7 mo; +, *from 18‐24 mo) + ++ ++ ‐d ++ + ++ ‐d ++e ++ 8/10 +
DYSPHAGIA feature Early feeding/swallowing difficulties (++, additional gastro‐esophageal reflux; +++, esophageal dilatation)
++ + ++ + + + ++ + +++ + 10/10 +
OTHER features *Ptosis (++, additional *slight strabismus) ‐ nd ‐ nd ‐ nd ‐ + ++ ‐ 2/7 + Tongue fasciculations ‐ ‐ ‐ nd ‐ nd ‐ ‐ + ‐ 1/8 + Abnormal electroencephalogram (++, additional epilepsy) ++ ++ + ‐ ‐ ‐ ‐ ‐ ‐ nd 3/9 +
Nature Genetics: doi:10.1038/ng.995

15
SUPPLEMENTARY METHODS
Sample preparation. Genomic DNA was isolated from peripheral venous blood by standard salt extraction. Total
RNA was extracted from muscle tissue with the TRIzol method (Invitrogen Inc.) and cDNA was synthesized with
the SuperScript III First‐Strand Synthesis system for RT‐PCR (Invitrogen Inc.)
SNP genotyping and data / variant annotation. SNP chip genotyping data were generated from Affymetrix
Genome‐Wide Human SNP Array 6.0 or 250K NSP chip (Aros Applied Biotechnology A/S, Denmark). Text
genotype output was annotated with SNPAnnotator (http://dna.leeds.ac.uk/snpannotator/). All discovered
mutations were absent in the data of the 1000 Genomes Project in either the heterozygote or homozygous
state: c.1325delC: 1141 individuals with a called genotype (862 with a PHRED scale quality score ≥30);
c.1559G>A: 1182 individuals with a called genotype (1032 with PHRED ≥30); c.2301C>A: 951 individuals with a
called genotype (749 samples PHRED ≥30); c.2320T>C: 1140 individuals with a called genotype (906 with PHRED
≥30); c.3144T>G variant: 1174 individuals with called genotype (1030 with PHRED ≥30).
Software development and requirements. Microsoft Visual Studio 2005 was used for programming with Visual
Basic. The PHASER program runs on Microsoft Windows XP, Vista and Windows 7, under the .NET framework
2.0. The stand‐alone graphical user interface program, description of the rule‐based algorithm, accompanying
documentation and all genotyping data files are freely available for download at http://dna.leeds.ac.uk/phaser.
Fine‐mapping of the EMARDD candidate region. We further investigated the putative region on chromosome
5q23 by genotyping with microsatellite markers. Suitable markers were identified using public genome
databases. Microsatellite markers were amplified by PCR with fluorescently‐labeled oligonucleotides using
standard methods. Primer sequences are available on request. PCR amplimers were separated on an ABI 3730
capillary DNA Sequencer and analyzed with GeneMapper 2.5 software (Applied Biosystems Inc.)
Targeted capture of genomic DNA. To enrich for sequences of interest we used the SureSelect™ Target
Enrichment (Agilent Inc.) “in‐solution method” for capture of coding exons within the target interval identified
for family B. Biotinylated oligonucleotide baits were designed by extracting all coding regions in the locus from
the UCSC genome browser for all UCSC Known Genes. These regions were uploaded to Agilent’s “eArray”
software (https://earray.chem.agilent.com/earray/) for automated oligonucleotide synthesis (in parallel with
regions for seven other unrelated loci as part of a collaborative experiment). Three micrograms of genomic DNA
was sheared and Illumina paired‐end adapters ligated according to Agilent’s SureSelect™ Library Prep protocol
version 1.0.1 (October 2009). Samples were size selected (200‐300 bp) on an agarose gel followed by 12 cycles
of PCR enrichment prior to hybridization to the SureSelect™ reagent for 24 hours at 65°C (following protocol
version 1.0.1). A post‐hybridization amplification step was performed and samples were subsequently cleaned
up with Ampure™ SPRI beads (Beckman Inc.)
Clonal sequencing. Libraries were denatured with NaOH and diluted to a final concentration of 12 pM, 120 μl of
which was hybridized onto a v5 single read flow cell (Illumina Inc.) following the manufacturer’s cluster station
Nature Genetics: doi:10.1038/ng.995

16
instructions. Samples were prepared for sequencing following Illumina’s standard amplification, linearization,
blocking, and primer hybridization protocols. The flow cell was then transferred to the Illumina GAIIx for
sequencing using an adapted single‐read protocol for 80 cycles. Whole genome alignment of qseq files to the
February 2009 human reference sequence (GRCh37/hg19 assembly) was performed using Novoalign short‐read
alignment software (Novocraft Technologies, Selangor, Malaysia). Alignments were processed in the SAM/BAM
format1 using SAMtools1, Picard and The Genome Analysis Toolkit (GATK)2,3 java programs in order to correct
alignments around indel sites and mark potential PCR duplicates. Variants within the candidate region were
called in the VCF format using the Unified Genotyper and DINDEL4 functions of GATK. Variants were filtered
using GATK on the basis of mapping quality, strand bias and genotype quality and known SNPs from dbSNP131
were removed.
Mutation analysis. We used the GeneScreen program5 (http://dna.leeds.ac.uk/genescreen/) to design PCR
primers that flanked all coding exons of the MEGF10 gene (Supplementary Table 1). Direct sequencing was
performed using the dideoxy chain termination method (ABI “BigDye 3.0” system) on an ABI 3730 DNA
Sequencer, and sequences analyzed using either GeneScreen or Chromas v2.0 software. All mutations were
verified bidirectionally.
Antibodies and conjugates
The following primary antibodies were used: rabbit polyclonal anti‐MEGF10 (Atlas Antibodies Inc.), and mouse
monoclonal anti‐PAX6 or anti‐PAX7 (Developmental Studies Hybridoma Bank, University of Iowa, USA).
Secondary antibodies and conjugates were Alexa‐Fluor 488‐ or Alexa‐Fluor 594‐conjugated goat anti‐mouse IgG
and goat anti‐rabbit IgG (Molecular Probes) and fluorescein‐α‐bugarotoxin (Biotium Inc.).
Western immunoblotting. 10 μg total soluble protein were extracted from frozen muscle biopsy sections and
analyzed by SDS‐PAGE (using 4‐12% acrylamide gradient gels) and Western immunoblotting according to
standard protocols using rabbit polyclonal anti‐MEGF10 at a final dilution of 1:1,000. Appropriate HRP‐
conjugated secondary antibody (Dako Inc.) was used (final dilution of 1:25,000) for detection by the enhanced
chemiluminescence “Femto West” Western blotting detection system (Pierce Inc.)
Immunohistochemistry. Wild‐type mouse embryos (embryonic age E15.5) were fixed in 2% [w/v] para‐
formaldehyde and embedded in paraffin. Thin sections (4 μm) were mounted onto slides, deparaffinized and
rehydrated by standard methods. Epitope recovery was obtained through boiling in 1 mM EDTA pH 8.0, for 15
min followed by 30 min cooling. Blocking and application of primary antibodies was performed as described6.
Rabbit polyclonal anti‐MEGF10 (Atlas Antibodies Inc.) was used for immunohistochemical studies. Appropriate
HRP‐conjugated secondary antibodies (Dako Inc.) were used (final dilutions of 1:10,000‐25,000). Sections were
developed in “Sigma Fast” 3,3’‐diaminobenzidine (DAB) with CoCl2 enhancer and counterstained with Mayer's
haematoxylin (Sigma‐Aldrich Co. Ltd.) for 2 min, dehydrated, cleared in xylene and mounted in DPX.
Frozen muscle tissue sections were allowed to warm to room temperature and fixed for 15 min in ice
cold acetone. All the subsequent steps were performed at room temperature. Following a rinse in wash buffer,
Nature Genetics: doi:10.1038/ng.995

17
endogenous peroxidase activity was blocked in “Menapath” peroxidase block (A. Menarini Diagnostics Ltd.,
Winnersh‐Wokingham, Berkshire, UK) for 10 min. Slides were rinsed in wash buffer and blocked in “Menapath”
casein block for 10 min. Primary antibody, optimally diluted x200 in Zymed (Invitrogen Ltd Paisley UK), was
applied to sections for 30 min and the slides again washed in buffer. Secondary antibody “Menapath” Polymer
HRP was incubated with the sections for 30 min. Following a final wash, sections were treated with “Menapath”
DAB for 5 minutes. Sections were counterstained in Mayer’s haematoxylin for 2 min, dehydrated, cleared in
xylene and mounted in DPX.
Immunofluorescence and confocal microscopy
Wild‐type mouse embryos (embryonic age E11) were embedded in OCT Compound (Tissue‐Tek Inc.) and snap‐
frozen in 2‐methylbutane chilled on dry ice. Thin fresh frozen sections (4 μm) were cut onto slides, allowed to air
dry and fixed in ice‐cold methanol (5 min at 4°C) or 2% paraformaldehyde (20 min at room temperature).
Permeabilization, blocking methods and immunofluorescence staining were essentially as described previously6.
Primary antibodies were used at final dilutions between 1:1,000 and 1:200. Secondary antibodies were diluted
1:500. Fluorescein‐α‐bugarotoxin for detection of neuromuscular junctions was diluted 1:1,000. Confocal images
were obtained using a Nikon Eclipse TE2000‐E system, controlled and processed by EZ‐C1 3.50 (Nikon Inc.)
software. Images were assembled using Adobe Illustrator CS2.
SUPPLEMENTARY NOTE
Informed consent was obtained from all participating families or patients, and subjects were recruited through
human genetics centers in Europe. All participating subjects underwent a detailed physical examination by
experienced pediatric neurologists. Ethical approval for this study was obtained from Leeds (East) Research
Ethics Committee (REC ref. no. 08/H1306/85) and from the Institutional Review Board of the Charité (ref. no.
EA2/092/06). A diagnosis of SMARD‐like phenotype was based on infantile presentation of muscular hypotonia
with respiratory distress (Table 1, Supplementary Table 2). In all patients mutations in IGHMBP2 and SMN1 had
been excluded.
Nature Genetics: doi:10.1038/ng.995

18
REFERENCES
1. Li, H. et al. Bioinformatics. 25, 2078‐2079 (2009).
2. McKenna, A. et al. Genome Res. 20, 1297‐1303 (2010).
3. DePristo, M.A. et al. Nat. Genet. 43, 491‐498 (2011).
4. Albers, C.A. et al. Genome Res. 6, 961‐973 (2011).
5. Carr, I.M. et al. J. Med. Genet. 48, 123‐130 (2011).
6. Dawe, H.R. et al. Hum. Mol. Genet. 16, 173‐186 (2007).
7. Hartley, L. et al. Neuromuscul. Disord. 17, 174‐179 (2007).
8. Holterman, C.E. et al. J. Cell. Biol. 179, 911‐922 (2007).
9. Callebaut, I. et al. Biochem. Biophys. Res. Commun. 300, 619‐623 (2003).
10. Wu, H.H. et al. Nat. Neurosci. 12, 1534‐1541 (2009).
11 Larkin,M.A. et al. Bioinformatics 23, 2947‐2948 (2007).
Nature Genetics: doi:10.1038/ng.995