Embed Size (px)
Citation preview

Supplementary appendixThis appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors.
Supplement to: Praz F, Spargias K, Chrissoheris M, et al. Compassionate use of the PASCAL transcatheter mitral valve repair system for patients with severe mitral regurgitation: a multicentre, prospective, observational, first-in-man study. Lancet 2017; 390: 773–80.
Appendix
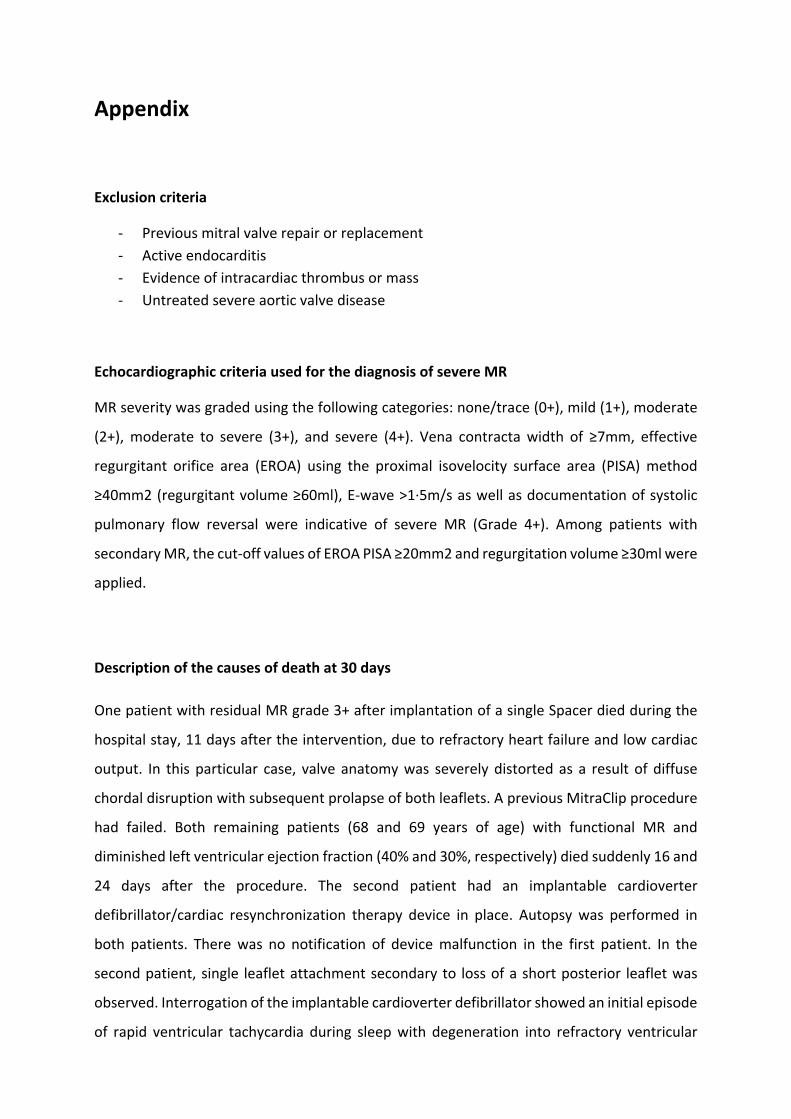
Exclusion criteria
‐ Previous mitral valve repair or replacement
‐ Active endocarditis
‐ Evidence of intracardiac thrombus or mass
‐ Untreated severe aortic valve disease
Echocardiographic criteria used for the diagnosis of severe MR
MR severity was graded using the following categories: none/trace (0+), mild (1+), moderate
(2+), moderate to severe (3+), and severe (4+). Vena contracta width of ≥7mm, effective
regurgitant orifice area (EROA) using the proximal isovelocity surface area (PISA) method
≥40mm2 (regurgitant volume ≥60ml), E‐wave >1∙5m/s as well as documentation of systolic
pulmonary flow reversal were indicative of severe MR (Grade 4+). Among patients with
secondary MR, the cut‐off values of EROA PISA ≥20mm2 and regurgitation volume ≥30ml were
applied.
Description of the causes of death at 30 days
One patient with residual MR grade 3+ after implantation of a single Spacer died during the
hospital stay, 11 days after the intervention, due to refractory heart failure and low cardiac
output. In this particular case, valve anatomy was severely distorted as a result of diffuse
chordal disruption with subsequent prolapse of both leaflets. A previous MitraClip procedure
had failed. Both remaining patients (68 and 69 years of age) with functional MR and
diminished left ventricular ejection fraction (40% and 30%, respectively) died suddenly 16 and
24 days after the procedure. The second patient had an implantable cardioverter
defibrillator/cardiac resynchronization therapy device in place. Autopsy was performed in
both patients. There was no notification of device malfunction in the first patient. In the
second patient, single leaflet attachment secondary to loss of a short posterior leaflet was
observed. Interrogation of the implantable cardioverter defibrillator showed an initial episode
of rapid ventricular tachycardia during sleep with degeneration into refractory ventricular

fibrillation that could not be terminated, despite appropriate delivery of two antitachycardia
pacing bursts and six defibrillations. Both deaths were considered of cardiovascular origin, and
device failure contributing to the event cannot be excluded in the second patient.

Age
MR grade baseline
MR grade postprocedural
Challenging mitral valve anatomy Unsuitable mitral valve anatomy Surgical high risk criteria
Patient #1 65 3+ 0+
Short tethered PML (8mm) Large malcoaptation area Multiple clips anticipated
LV dysfunction (40%), s/p radiotherapy for treatment of Hodgkin’s lymphoma
Patient #2 73 3+ 1+
Short PML (10mm) Large malcoaptation area Multiple clips anticipated
Severe RV dysfunction
(DTI 5cm/s), GFR: 27ml/min
Patient #3 81 4+ 1+ Chordal disruption
Extensive flail of the PML Cleft of the PML in the grasping zone
Advanced age, idiopathic pulmonary fibrosis under home oxygen therapy
Patient #4 82 4+ 1+ Very short PML (6mm)
Flail AML
Advanced age, ischemic LV dysfunction (45%), persistence of severe MR despite complete percutaneous revascularization,
GFR: 35ml/min
Patient #5 82 4+ 1+ Carpentier IIIB with tethering of the PML
Severe annular dilation (71mm) Multiple clips anticipated
Advanced age, severe ischemic LV dysfunction (20%), GFR:
25ml/min
Patient #6 75 4+ 1+
Carpentier IIIB with bilateral tethering Short PML (10mm)
Annular dilation (61mm) Multiple clips anticipated
Ischemic LV dysfunction (40%), previous CABG, severe PAHT,
GFR 31ml/min, bilateral carotid stenosis (70%)
Patient #7 69 4+ 2+ Carpentier IIIB with tethering of the PML
Severe annular dilation (76mm) Multiple clips anticipated
Non‐ischemic severe LV dysfunction (30%), severe
osteoporosis with spine instability and impaired mobility, GFR 26ml/min
Patient #8 90 4+ 0+ Very short PML (6mm) Advanced age, severe non‐ischemic LV dysfunction (30%),
frailty (BMI 20.7kg/m2)
Patient #9 90 4+ 1+ Double prolapse PML (P2/P3 ; gap: 12mm)
Cleft of the PML Advanced age, acute cardiac decompensation
due to chordal rupture, GFR: 30ml/min
Patient #10 68 3+ 2+ Thickened short PML (10mm) Large malcoaptation area Multiple clips anticipated
Severe non‐ischemic LV dysfunction (30%), GFR: 40ml/min, Obesity BMI (38.5kg/m2)
Supplementary Table 1: Individual anatomical und risk criteria considered for patients enrolment
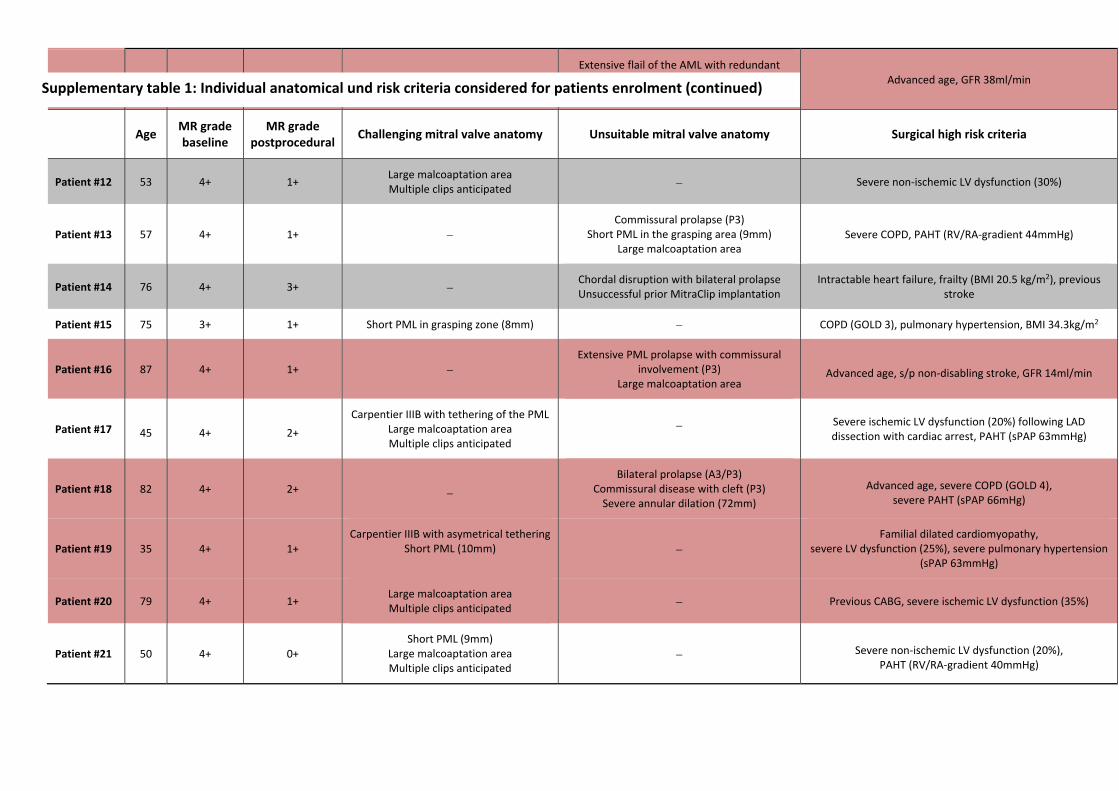
Patient #11 90 4+ 1+ Extensive flail of the AML with redundant tissue in the grasping area, short calcified
posterior leaflet (10mm) Advanced age, GFR 38ml/min
Age MR grade baseline
MR grade postprocedural
Challenging mitral valve anatomy Unsuitable mitral valve anatomy Surgical high risk criteria
Patient #12 53 4+ 1+ Large malcoaptation area Multiple clips anticipated
Severe non‐ischemic LV dysfunction (30%)
Patient #13 57 4+ 1+ Commissural prolapse (P3)
Short PML in the grasping area (9mm) Large malcoaptation area
Severe COPD, PAHT (RV/RA‐gradient 44mmHg)
Patient #14 76 4+ 3+ Chordal disruption with bilateral prolapse Unsuccessful prior MitraClip implantation
Intractable heart failure, frailty (BMI 20.5 kg/m2), previous stroke
Patient #15 75 3+ 1+ Short PML in grasping zone (8mm) COPD (GOLD 3), pulmonary hypertension, BMI 34.3kg/m2
Patient #16 87 4+ 1+ Extensive PML prolapse with commissural
involvement (P3) Large malcoaptation area
Advanced age, s/p non‐disabling stroke, GFR 14ml/min
Patient #17 45 4+ 2+
Carpentier IIIB with tethering of the PMLLarge malcoaptation area Multiple clips anticipated
Severe ischemic LV dysfunction (20%) following LAD dissection with cardiac arrest, PAHT (sPAP 63mmHg)
Patient #18 82 4+ 2+
Bilateral prolapse (A3/P3) Commissural disease with cleft (P3) Severe annular dilation (72mm)
Advanced age, severe COPD (GOLD 4), severe PAHT (sPAP 66mHg)
Patient #19 35 4+ 1+ Carpentier IIIB with asymetrical tethering
Short PML (10mm) Familial dilated cardiomyopathy,
severe LV dysfunction (25%), severe pulmonary hypertension (sPAP 63mmHg)
Patient #20 79 4+ 1+ Large malcoaptation area Multiple clips anticipated
Previous CABG, severe ischemic LV dysfunction (35%)
Patient #21 50 4+ 0+ Short PML (9mm)
Large malcoaptation area Multiple clips anticipated
Severe non‐ischemic LV dysfunction (20%), PAHT (RV/RA‐gradient 40mmHg)
Supplementary table 1: Individual anatomical und risk criteria considered for patients enrolment (continued)

Patients are listed in chronological order of treatment. The patients marked in red received two Spacers. Classification between challenging and unsuitable anatomy based on Boekstegers P et al, Clin Res Cardiol 2014; 103(2): 85‐96 and Hahn RT, Circ Res. 2016; 119(2): 341‐56.
MR: mitral regurgitation; PML: posterior mitral leaflet; AML: anterior mitral leaflet; LV: left ventricle; RV: right ventricle; DTI: Doppler tissue imaging; GFR: glomerular filtration rate; CABG: coronary artery bypass
grafting; PAHT: pulmonary artery hypertension; sPAP: systolic pulmonary artery pressure; s/p: status post; COPD: chronic obstructive pulmonary disease; GOLD: Global Initiative for Chronic Lung Disease; RA:
right atrium; BMI: body mass index.
Patient #22 55 3+ 1+ Short PML (9mm)
Large malcoaptation area Multiple clips anticipated
Severe ischemic LV dysfunction (20%)
Patient #23 80 4+ 2+
Bilateral prolapse (A2‐P2) Flail P2
Perforation A2
Advanced age, frailty (BMI 15kg/m2), s/p replacement of the ascending aorta for treatment of aortic dissection type A
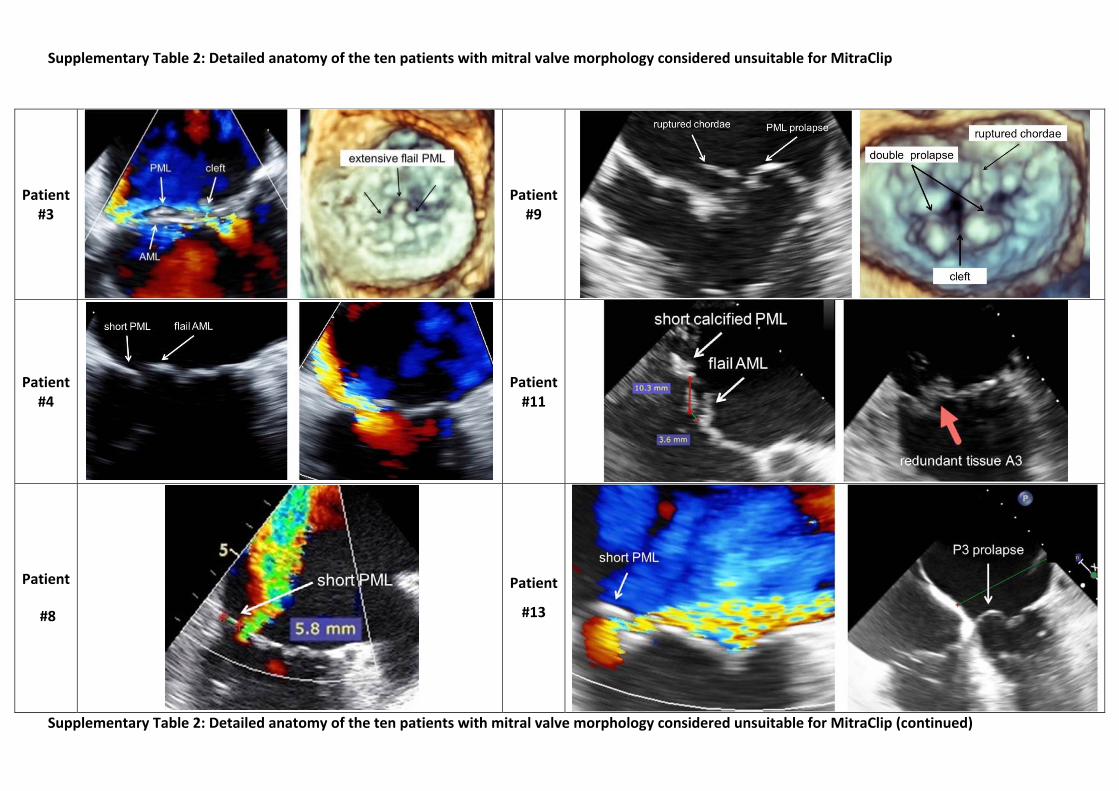
Supplementary Table 2: Detailed anatomy of the ten patients with mitral valve morphology considered unsuitable for MitraClip
Supplementary Table 2: Detailed anatomy of the ten patients with mitral valve morphology considered unsuitable for MitraClip (continued)
Patient #3
Patient#9
Patient #4
Patient#11
Patient
#8
Patient
#13

Patient #14
Patient#18
Patient #16
Patient#23

Supplementary Table 3: Procedural outcomes
Procedural outcomes N=23
Successful implantation of at least one device, n (%) 23 (100)
Technical success*, n (%) 22 (96)
Procedural mortality, n (%) 0
Emergent conversion to open‐heart surgery, n (%) 0
Single leaflet attachment, n (%) 1 (4)
Device embolization, n (%) 0
Implantation of more than one device, n (%) 6 (26)
ASD requiring closure, n (%) 0
Length of stay, days (range) 4±2 (1‐7)
Echocardiographic outcomes
Transseptal puncture height, cm (range) 4∙6±0∙5 (3∙5‐5∙5)
MVA after implantation, cm2 2∙9±1∙2
MR Grade at discharge (n=22)
0, n (%) 3 (14)
1+, n (%) 14 (63)
2+, n (%) 5 (23)
Mean MV gradient at discharge, mmHg 3±1
*according to MVARC N: number of patients; ASD: atrial septal defect; MR: mitral regurgitation; MVA: mitral valve area; MV: mitral valve

Supplementary Figure 1: The Edwards PASCAL delivery system
The Edwards PASCAL delivery system is composed of two distinct catheters, a steerable catheter and an implant catheter, introduced into a 22 French steerable guide sheath.

Supplementary Figure 2: Example of independent leaflet grasping
Example of differential grasping as seen by transesophageal echocardiography in a patient with functional mitral valve regurgitation with severe malcoaptation. A: The anterior mitral valve leaflet is grasped between the anterior Clasps and Paddles, whereas the posterior leaflet is still freely moving (Video 1). B: After careful repositioning of the system, the posterior leaflet can also be secured. Both leaflets are now in contact with the Paddles that can be closed (Video 2). LA: left atrium; LV: left ventricle; AML: anterior mitral leaflet; PML: posterior mitral leaflet.

Supplementary Figure 3: Change of MVA
A: Measure of the diastolic MVA before the procedure using multiplanar reconstruction; B: After implantation, each neo‐orifice is measured separately; C: The final 3D MVA is obtained by the addition of the area of each orifice; D: Scatterplot showing baseline MVA and change in MVA after implantation of one (white dots) and two devices (red dots). Considering the patients with one implant only, the change of the MVA can be approximated using the following formula: ΔMVA=0.5 x Baseline MVA – 0.3. An average MVA reduction of 47% was observed in the patients receiving one Spacer versus 59% in the patients with 2 implants. η2 and Cohen’s d corresponds to the effect size based on one‐way ANOVA. Curved lines represent the 95% confidence interval. In two patients 3D MVA could not be obtained due to insufficient echocardiographic quality.
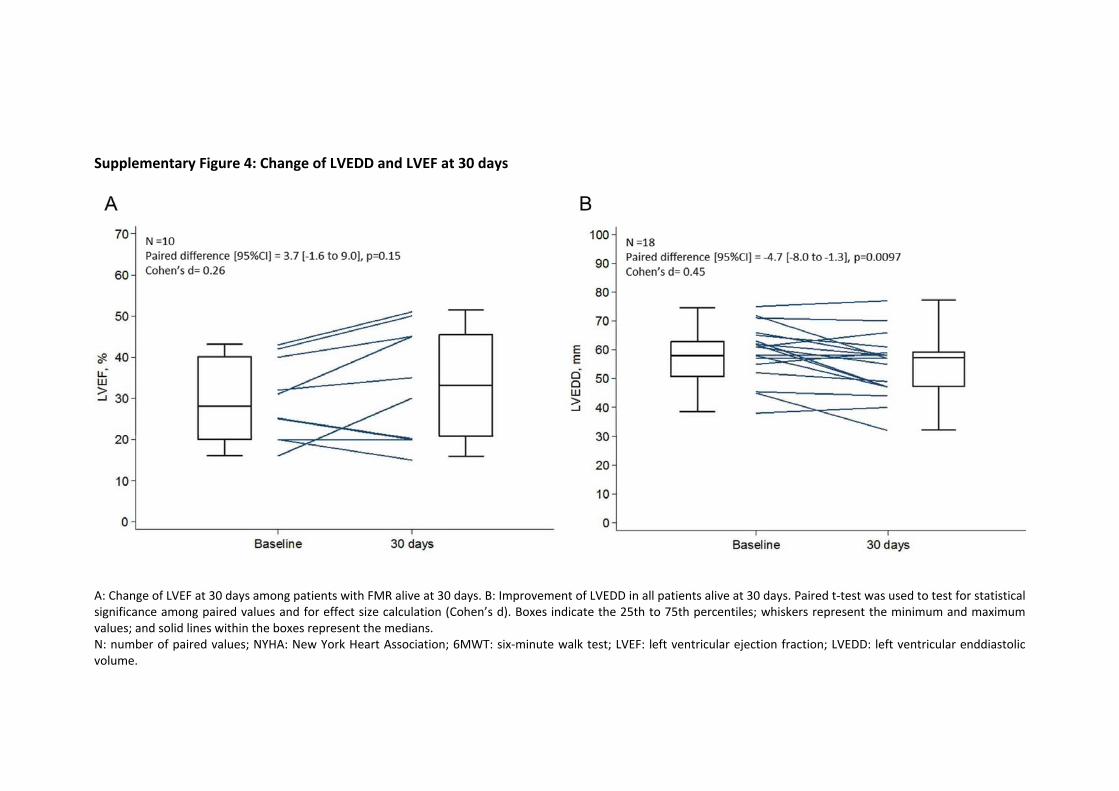
Supplementary Figure 4: Change of LVEDD and LVEF at 30 days
A: Change of LVEF at 30 days among patients with FMR alive at 30 days. B: Improvement of LVEDD in all patients alive at 30 days. Paired t‐test was used to test for statistical significance among paired values and for effect size calculation (Cohen’s d). Boxes indicate the 25th to 75th percentiles; whiskers represent the minimum and maximum values; and solid lines within the boxes represent the medians. N: number of paired values; NYHA: New York Heart Association; 6MWT: six‐minute walk test; LVEF: left ventricular ejection fraction; LVEDD: left ventricular enddiastolic volume.





























