Embed Size (px)
Citation preview

1
SUPPLEMENTAL ONLINE APPENDIX
For Cost-Effectiveness of Ensuring Hepatitis B Protection for Previously Vaccinated Healthcare Personnel By Thomas J. Hoerger, PhD, Christina Bradley, BS, Sarah F. Schillie, MD, MPH, MBA, Meredith Reilly, MPH, and Trudy V. Murphy, MD
The cost-effectiveness of ensuring hepatitis B protection among healthcare personnel
(HCP) with unknown response to vaccination by evaluating antibody to hepatitis B surface
antigen (anti-HBs) at matriculation or hire (pre-exposure), or by evaluating HCP for post-
exposure management after a reported blood or body fluid (BBF) exposure (post-exposure) has
been evaluated and published (Hoerger TJ, Bradley C, Schillie S, Reilly M, Murphy T. Cost-
effectiveness of ensuring hepatitis B protection for previously vaccinated healthcare personnel.
ICHE. 201X Month; XX(XX):XXXX-X). This online appendix provides additional details on
model inputs. It also presents cost-effectiveness results for 2 additional strategies for ensuring
hepatitis B protection among HCP with unknown response: pre-exposure challenge dose of
hepatitis B (HepB) vaccine and post-exposure evaluation with follow-up only for HCP exposed
to source patients with positive or unknown hepatitis B surface antigen (HBsAg) status. This
supplemental appendix presents the cost-effectiveness results of these 2 additional strategies for
trainees and non-trainees and provides greater detail on selected model inputs.
Model Inputs
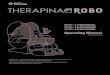
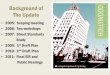
Key model input variables are presented in Table 1 of the published article. Decision tree
diagrams for the pre-exposure anti-HBs testing strategy and the post-exposure management
strategy are included in Figures A-1 and A-2. Exposure, seroprotection, and intervention cost
variables are described in more detail below.

2
Exposure Variables
Probability of Blood and Body Fluid Exposure
The annual probability of BBF exposure was calculated as the sum of the annual
probability of percutaneous exposure and the annual probability of mucosal exposure. The
annual probability of percutaneous exposure was set equal to the median self-reported
probability of exposure of HCP from 5 studies of percutaneous exposures published after 2000
(the Needlestick Safety and Prevention Act was signed into law in 2000).1-5 For one-way
sensitivity analyses, we used the lowest and highest reported values. The annual probability of
mucosal exposure was determined in a similar fashion, based on 4 studies.1-4 Based on evidence
that the percutaneous exposures are up to twice as likely among trainees as among non-trainees,
a panel of experts6 recommended multiplying the median percutaneous and mucosal rates by
1.75 to set the value for trainees. In addition, both probabilities included all exposures
experienced by the HCP, not just those the HCP reported to his or her employer. More than half
of percutaneous exposures were reported to the employer, compared with only 17% of mucosal
exposures. We accounted for reporting when we calculated the probability of infection from
source patients who are HBsAg-positive.6
Probability that Source Patient has Hepatitis B
The probability that the source patient is HBsAg-positive was 0.009. This figure was a
weighted average of figures from 3 healthcare systems in the United States (personal
communication, D. Nace, January 11, 2012; D. Weber, August 30, 2011, January 20, 2012; B.
McMahon, February 1, 2012), covering the years 2000–2012 and representing 7,170 exposures.
This figure assumes that the rate of HBsAg-positivity for unknown sources (estimated to account
for 6% of exposures) is the same as that for known sources. The value reflects the current

3
prevalence of hepatitis B virus (HBV) infection, which is lower now than in the 1990s and
earlier.
Probability of Serologic Evidence of Protection
The proportion of HCP with serologic evidence of protection (anti-HBs ≥10 mIU/mL)
differs between trainees and non-trainees. Trainees are more likely to have completed
vaccination at age <1 year. The median proportion of anti-HBs levels ≥10 mIU/mL
approximately 20 years later is 0.2 for persons vaccinated at <1 year of age, based on data
extrapolated from subjects followed for approximately 5 to 15 years.7-11 Most non-trainees
completed vaccination at age ≥1 year. The median proportion of anti-HBs levels ≥10 mIU/mL
measured approximately 20 years later is 0.8 for persons vaccinated at ≥1 year of age, based on
subjects followed for approximately 5 to 30 years.12-20 Low and high values for the one-way
sensitivity analyses are drawn from the range of proportions in studies for vaccination at age <1
and at age ≥1 year.
Among HCP whose anti-HBs level is <10 mIU/mL at time distant from vaccination, a
response to a single challenge dose of HepB vaccine is assumed to be evidence of protection. For
the model, response to a challenge dose of HepB vaccine is defined as the probability that an
HCP who received a complete series of HepB vaccine in the remote past and who currently has
anti-HBs <10 mIU/mL will reach anti-HBs ≥10 mIU/mL after the challenge dose. For trainees,
the proportion of responders (60%) is derived from U.S. subjects vaccinated at age <1 year who
were followed for approximately 5 to 15 years.8-11 For non-trainees, the proportion of responders
(75%) is derived from U.S. subjects vaccinated at age ≥1 year who were followed for
approximately 5 to 22 years.14,17,19 These values were extrapolated using linear trend lines fit to
available data.

4
Probability of Hepatitis Infection if BBF Exposure Occurs, Source Patient Has Hepatitis B, and
HCP Is Not Protected
The probability of infection varies depending on whether the exposure was percutaneous
or mucosal. The probability for percutaneous injuries is based on the probability of serological
evidence of HBV among HCP after sustaining a needlestick injury from a needle contaminated
with blood containing HBV (figures for needlestick injury were applied to all percutaneous
exposures). Specifically, the probability was calculated as follows21:
(Probability of infection when source HBeAg + [0.50] * Probability HBeAg
+ [0.345]) + (Probability of infection when source HBeAg − [0.30] *
Probability HBeAg − [0.655]) = 0.369
The equation accounts for the fact that source patients who are hepatitis B e-antigen
(HBeAg) positive are more infectious than source patients who are HBsAg-positive and HBeAg-
negative.
Similar data on infectivity do not exist for mucosal exposures. Because mucosal
exposures are considered to be less infectious than percutaneous exposures, we set the mucosal
probability of infection equal to half the percutaneous value.22
Because percutaneous exposures are more infectious and more likely to be reported than
mucosal exposures, the probability of infection after a reported BBF exposure differs from the
probability of infection after an unreported BBF exposure. Accordingly, we calculated separate
values for the probability of infection after a reported BBF exposure and the probability of
infection after an unreported BBF exposure.
Overall Probability of HBV Infection
The probability of infection in a 1-year period is calculated as follows:

5
(probability of BBF exposure) * (probability the source patient is HBsAg-positive) *
(probability HCP is not protected) * (probability of infection given source patient is HBsAg-
positive and HCP is not protected)
Total intervention costs of each strategy depend on the number of anti-HBs tests, number
of HepB vaccine doses, costs of source patient testing, additional costs to the employer
occupational health department, and—for infected HCP—medical costs of hepatitis B-related
treatment. HCP who become infected experience utility loss arising from hepatitis-related
complications. Parameters for these variables are shown in Table 1 in the published article.
Impact of Hepatitis B Infection
We used a hepatitis B cost-effectiveness model23 to calculate the lifetime consequences
of HBV infection. The model accounts for the fact that some acute HBV infections are
asymptomatic, whereas others require treatment that may include hospitalization or liver
transplantation; it also accounts for the 6% of acute infections in adults that progress to chronic
infection. For trainees, we calculated the present value of future hepatitis-related medical costs
and QALY losses for an acute infection at age 25. For non-trainees, we assumed that the
infection occurred at age 35. The choice of age at infection has relatively small effects on the
projected lifetime costs and QALY losses.
Protection after Revaccination (Challenge Dose plus Two Additional Doses)
Protection after revaccination was defined as the probability that an HCP who had
received a complete series of HepB vaccine in the remote past with anti-HBs <10 mIU/mL and
failed to reach anti-HBs ≥10 mIU/mL after a single additional (challenge) dose of vaccine will
reach anti-HBs ≥10 mIU/mL after 2 more doses of vaccine (complete revaccination). A value of

6
0.8 for both trainees and non-trainees was derived from 3 studies8,11,17 conducted in the United
States. Subjects in the studies were vaccinated both at <1 and ≥1 year of age.
Efficacy of HBIG
HBIG is provided to an HCP who is not protected and has been exposed to an HBsAg-
positive source patient. The efficacy of HBIG represents the probability that a non-protected
HCP would be protected against a recent HBV exposure after one dose of HBIG. A value of 0.8
for the efficacy of HBIG was derived from a review article and was based on 216 persons who
sustained percutaneous exposure to HBsAg positive material and 25 spouses exposed to acute
HBV infection.24
Intervention Cost Components
Intervention cost components and sources are shown in Table 1 in the published article.
Costs for laboratory tests come from the Medicare Clinical Laboratory Fee Schedule. For one-
way sensitivity analyses, low values were set 25% lower than base values. High values were
based on the list price that a medical student might be charged by a hospital laboratory, under the
assumption that such tests would not be covered by insurance because they are not medically
necessary. For probabilistic sensitivity analyses, the costs for laboratory tests are drawn from a
normal distribution with 95% confidence intervals that are ±25% of the base values.
Sensitivity Analyses
One-way and probabilistic sensitivity analyses are performed. For each run in
probabilistic sensitivity analyses, key input parameters are drawn from appropriate distributions
(beta and normal distributions for probabilities and costs, respectively). For the probability that
the source patient has HBV infection, we use a beta distribution with a mean of 0.009, based on
7,170 observations from 3 healthcare institutions. The resulting range of values in the

7
probabilistic sensitivity analysis is narrower than in the one-way sensitivity analysis (which
ranges from 0.003 to 0.10) (personal communication, D. Nace, January 11, 2012; D. Weber,
August 30, 2011, January 20, 2012; B. McMahon, February 1, 2012; A. Elward, September 1,
2011; H. Keyseling, August 31, 2011). The range in the one-way sensitivity analysis provides
information for HCP who serve patients at very low risk or very high risk for HBsAg-positivity.
The cost of vaccine and the cost of administering the vaccine are separately varied by a
multiplicative factor between 0.75 and 1.25 for one-way sensitivity analyses, with corresponding
normal distributions in the probabilistic sensitivity analyses.
Additional Strategies
Pre-Exposure “Challenge” Dose of HepB Vaccine
Under this strategy, the HCP receives 1 additional dose of HepB vaccine followed by
anti-HBs testing upon matriculation or hire. If the anti-HBs is ≥10 mIU/mL after the first dose,
the HCP is protected. If the anti-HBs is <10 mIU/mL after this dose, the HCP will receive 2
more doses of HepB vaccine and post-vaccination anti-HBs testing. If the HCP does not show
serologic evidence of protection after these additional doses, the HCP will be considered a
known non-responder.
Post-Exposure Evaluation with Follow-up Only for HCP Exposed to Source Patients with
Positive or Unknown HBsAg Status
Under this strategy, management only occurs if BBF exposure occurs, is recognized by
the HCP, and is reported to the employer. If no BBF exposure occurs, the HCP is not infected,
and no costs are incurred. If BBF exposure occurs but is not recognized or reported, the
probability of infection depends on the probability that the source patient is HBsAg-positive, the
probability the HCP is not protected, and the probability of infection given those parameters. If

8
BBF exposure occurs and is reported, the HCP will receive an anti-HBs test and the source
patient will be tested for hepatitis B surface antigen (HBsAg) simultaneously. If the anti-HBs is
≥10 mIU/mL, the HCP has serologic evidence of protection, and no further management occurs.
If the anti-HBs is <10 mIU/mL, management depends on whether the source patient is HBsAg-
positive or HBsAg-negative: if the source patient is HBsAg-positive, the HCP receives Hepatitis
B Immune Globulin (HBIG) and 1 additional dose of HepB vaccine, completes revaccination (a
total of 3 additional doses), and is tested for anti-HBs 1 to 2 months after the last HepB vaccine
dose. If the HCP still does not show serologic evidence of protection after these doses, the HCP
may be a nonresponder or be HBV infected based on the probability of infection given that the
source patient is HBsAg-positive and the HCP is not protected. If the source patient is unknown,
or unavailable for testing, management proceeds as if the source was HBsAg-positive. If the
source patient is HBsAg-negative, the HCP receives no HepB vaccine doses or HBIG.
Under each of the above scenarios, if the HCP is known to be protected, he or she is
deemed a known responder, no further management will occur, and the HCP will not become
infected. If a known non-responder has a reported BBF exposure and the source patient is
HBsAg-positive (or unknown), the HCP will receive 2 doses of HBIG. The HBIG will provide
additional protection against infection; however, some HCP will remain unprotected and face the
probability of infection given that the source patient is HBsAg-positive and the HCP is not
protected.
RESULTS
The probability that an HCP will be infected with HBV is shown for each management
strategy, applying the 95% assumption of sustained vaccine-induced protection (Table A-1).
With no intervention, the probability of infection is 4.779 per 100,000 HCP. The interventions

9
increase the probability that the HCP is protected. The pre-exposure challenge dose of HepB
vaccine produces the lowest probability of infection (0.652 per 100,000 HCP), followed by post-
exposure evaluation with follow-up only for HCP exposed to source patients with positive or
unknown HBsAg status (2.955 per 100,000 HCP). In the 1-year model, the pre-exposure
“challenge” dose of HepB vaccine has an incremental cost-effectiveness ratio (ICER) of
$4,507,834 and $6,352,660 per QALY relative to no intervention for trainees and non-trainees,
respectively. The post-exposure evaluation with follow-up only for HCP exposed to source
patients with positive or unknown HBsAg status has an ICER of $1,639,968 and $1,497,845 per
QALY relative to no intervention for trainees and non-trainees, respectively. When the analysis
is extended for 10 years, the ICERs (calculated relative to the no intervention scenario) for
trainees and non-trainees improve.
Table A-2 shows the results of the probabilistic sensitivity analyses for trainees in the 1-
year model. The median ICERs are relatively close to the base case analysis, while the mean
ICERs are higher because we assumed a high initial probability of protection resulting in low
incremental QALYs. The credible interval is wide, reflecting the uncertainty about initial
probability of protection.

10
REFERENCES FOR ONLINE APPENDIX
1. Boal WL, Leiss JK, Ratcliffe JM, Sousa S, Lyden JT, Li J, Jagger J. The national study
to prevent blood exposure in paramedics: rates of exposure to blood. Int Arch Occup
Environ Health. 2010 Feb;83(2):191-9. doi: 10.1007/s00420-009-0421-x.
2. Gershon RM, Qureshi KA, Pogorzelska M, et al. Non-hospital based registered nurses
and the risk of bloodborne pathogen exposure. Ind Health. 2007;45:695–704.
3. Gershon RM, Pearson JM, Sherman MF, et al. The prevalence and risk factors for
percutaneous injuries in registered nurses in the home health care sector. Am J Infect
Control. 2009;37:525–33.
4. Lipscomb J, Sokas R, McPhaul K, et al. Occupational blood exposure among unlicensed
home care workers and home care registered nurses: Are they protected? Am J Ind Med.
2009;52:563–70.
5. Trinkoff AM, Le R, Geiger-Brown J, Lipscomb J. Needle use, and needlestick injuries
among registered nurses. Infect Control Hosp Epidemiol. 2007;28(2):156–64.
6. Centers for Disease Control and Prevention (CDC). CDC guidance for hepatitis B virus
protection for healthcare personnel. MMWR. October XX, 2013 / XX(RRXX);X-XX.
7. Dentinger CM, McMahon BJ, Butler JC, et al. Persistence of antibody to hepatitis B and
protection from disease among Alaska Natives immunized at birth. Pediatr Infect Dis J.
2005;24:786–92.
8. Hammit LL, Hennessy TW, Fiore AE, et al. Hepatitis B immunity in children vaccinated
with recombinant hepatitis B vaccine beginning at birth: A follow-up study at 15 years.
Vaccine. 2007;25:6958–64.

11
9. Middleman AB, Baker C, Hu DJ, et al. Duration of immunity from hepatitis B vaccine
administered soon after birth among 16 to 19 year old youth in the United States.
Presented at Pediatric Academic Societies Meeting, Boston; April–May 2012.
10. Petersen KM, Bulkow LR, McMahon BJ, et al. Duration of hepatitis B immunity in low
risk children receiving hepatitis B vaccinations from birth. Pediatr Infect Dis J.
2004;23:650–5.
11. Samandari T, Fiore AE, Negus S, et al. Differences in response to a hepatitis B vaccine
booster dose among Alaskan children and adolescents vaccinated during infancy.
Pediatrics. 2007;120:e373–81.
12. Funderburke PL, Spencer L. Hepatitis B immunity in high risk healthcare workers.
AAOHN J. 2000;48:325–30.
13. McMahon BJ, Bruden DL, Petersen KM, et al. Antibody levels and protection after
hepatitis B vaccination: Results of a 15-year follow-up. Ann Intern Med. 2005;142:333–
41.
14. McMahon BJ, Dentinger CM, Bruden D, et al. Antibody levels and protection after
hepatitis B vaccine: Results of a 22-year follow-up study and response to a booster dose.
J Infect Dis. 2009 Nov 1;200:1390–6.
15. McMahon BJ. 30 year follow-up after hepatitis B vaccination in adults and children.
Presented at the Viral Hepatitis Prevention Board Meeting, Milan, Italy; November 2011.
16. Stevens CE, Toy PT, Taylor PE, et al. Prospects for control of hepatitis B virus infection:
Implication of childhood vaccination and long-term protection. Pediatrics. 1992;90:170–
3.

12
17. Tohme RA, Ribner B, Huey MJ, et al. Hepatitis B vaccination coverage and documented
seroprotection among matriculating healthcare students at an academic institution in the
United States. Infect Control Hosp Epidemiol. 2011;32:818–21.
18. Watson B, West DJ, Chilkatowsky A, et al. Persistence of immunologic memory for 13
years in recipients of a recombinant hepatitis B vaccine. Vaccine. 2001;19:3164–8.
19. Williams JL, Christensen CJ, McMahon BJ, et al. Evaluation of the response to a booster
dose of hepatitis B vaccine in previously immunized healthcare workers. Vaccine.
2001;19:4081–5.
20. Williams RE. Hepatitis B vaccination coverage among students at a U.S. health science
graduate school. Presented at the National Immunization Conference, Washington, DC;
March 30, 2011.
21. Centers for Disease Control and Prevention (CDC). Updated U.S. Public Health Service
guidelines for the management of occupational exposures to HBV, HCV, and HIV and
recommendations for postexposure prophylaxis. MMWR 2001;50(No. RR-11):page 3.
22. Centers for Disease Control and Prevention (CDC). Updated U.S. public health service
guidelines for the management of occupational exposures to HBV HCV, and HIV and
recommendations for postexposure prophylaxis. MMWR. 2001;50(RR-11):1–52.
23. Zhou F, Euler GL, McPhee SJ, et al. Economic analysis of promotion of hepatitis B
vaccination among Vietnamese-American children and adolescents in Houston and
Dallas. Pediatrics. 2003;111(6 pt 1):1289–96.
24. Maynard J. Passive immunization against hepatitis B: Review of recent studies and
comment on current aspects of control. Am J Epidemiol. 1978;107:77–86.

13
Table A-1. Results, 1- and 10-Year Analysis, Assuming 95% Sustained Vaccine Protection
Strategy
Probability
of Infection Cost QALY Loss
Cost per QALY
Saved (Relative to
No Intervention)
1-Year Analysis
(a) Trainees
No intervention 0.00004779 $0.34 −0.0000372 —
Pre-exposure “challenge” dose of
HepB vaccine
0.00000652 $145.34 −0.0000051 $4,507,834
Post-exposure evaluation with follow-
up only for HCP exposed to source
patients with positive or unknown
HBsAg status
0.00002955 $23.66 −0.0000230 $1,639,968
(b) Non-trainees
No intervention 0.0000273 $0.19 −0.0000180 —
Pre-exposure “challenge” dose of
HepB vaccine
0.0000037 $99.17 −0.0000025 $6,352,660
Post-exposure evaluation with follow-
up only for HCP exposed to source
patients with positive or unknown
HBsAg status
0.0000169 $10.50 −0.0000112 $1,497,845
10-Year Analysis
(a) Trainees
No intervention $3.00 −0.00033 —
Pre-exposure “challenge” dose of
HepB vaccine
$253.28 −0.00004 $889,659

14
Strategy
Probability
of Infection Cost QALY Loss
Cost per QALY
Saved (Relative to
No Intervention)
Post-exposure evaluation with follow-
up only for HCP exposed to source
patients with positive or unknown
HBsAg status
$199.90 −0.000130896 $1,009,594
(b) Non-trainees
No intervention $1.66 −0.0001581 —
Pre-exposure “challenge” dose of
HepB vaccine
$160.27 −0.00002 $1,161,709
Post-exposure evaluation with follow-
up only for HCP exposed to source
patients with positive or unknown
HBsAg status
$88.98 −0.0000773569 $1,101,432

15
Table A-2. Probabilistic Sensitivity Analyses, $ per QALY, Trainees, 1-Year Analysis for
95% Sustained Vaccine Protection
Initial Decision
Mean ICER
(Relative to No
Intervention)
Median ICER
(Relative to No
Intervention)
Credible Interval
(2.5 Percentile)
Credible Interval
(97.5 Percentile)
Pre-exposure “challenge”
dose of HepB vaccine
$30,403,939.97 $6,580,861.13 $1,277,253.44 $140,034,356.45
Post-exposure evaluation
with follow-up only for
HCP exposed to source
patients with positive or
unknown HBsAg status
$11,549,299.51 $2,387,585.58 $412,940.11 $53,286,004.75

16
Figure A-1. Pre-exposure anti-HBs testing strategy—TreeAge Decision Tree

17
Figure A-2. Post-exposure management strategy—TreeAge Decision Tree