Embed Size (px)
Citation preview

This article was downloaded by: [Akdeniz Universitesi]On: 20 December 2014, At: 11:38Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: MortimerHouse, 37-41 Mortimer Street, London W1T 3JH, UK
Neurocase: The Neural Basis of CognitionPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/nncs20
Supernumerary phantom limb after ischaemicstrokeM. Mazzoni a , C. Lucchin a , G. Meucci a , M. Vista a , P. Moretti a & F. Sartucci aa Department of Neurosciences , University of Pisa , Via Roma 67, Italy , 56126 PisaPublished online: 17 Jan 2008.
To cite this article: M. Mazzoni , C. Lucchin , G. Meucci , M. Vista , P. Moretti & F. Sartucci (1997) Supernumeraryphantom limb after ischaemic stroke, Neurocase: The Neural Basis of Cognition, 3:3, 223-230, DOI:10.1080/13554799708404057
To link to this article: http://dx.doi.org/10.1080/13554799708404057
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”)contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensorsmake no representations or warranties whatsoever as to the accuracy, completeness, or suitabilityfor any purpose of the Content. Any opinions and views expressed in this publication are the opinionsand views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy ofthe Content should not be relied upon and should be independently verified with primary sources ofinformation. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands,costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly orindirectly in connection with, in relation to or arising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Any substantial orsystematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution inany form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Neurocase (1997) Vol. 3, pp. 223-230 ( Oxford Universin Press 1997
REPLICA TION
Supernumerary Phantom Limb After lschaemic Stroke
M. Mazzoni, C. Lucchini, G. Meucci, M. Vista, P. Moretti and F. Sartucci
Department of Neurosciences, University of Pisa, Via Roma 67, 56126 Pisa, Italy
Abstract
We describe a case of supernumerary phantom llmb following focal cerebral ischaemia and discuss its neuropsychological, neurophysiopathological and neuroradiological features In llght of previous data in the literature. The Illusory perception of a phantom limb, seldom reported as a consequence of cerebral lesions, seems In this case to be due to the right subcortical damage altering sensory input to the higher somatosensory cortical areas involved In body image.
Introduction
The ‘phantom limb’ phenomenon, i.e. the illusory percep- tion of a non-existent limb, is a body image disorder commonly observed following traumatic or surgical amputation (90- 100% of cases according to Melzack and Bromage, 1973). It has also been reported, even if less frequently, as a consequence of peripheral or central nervous system lesions. In such cases, as the real limbs are still present and the erroneous perception is that of an extra arm or leg, the phenomenon is commonly called ‘phantom third limb’ or ‘supernumerary phantom limb’ (SPL) (Critchley, 1953).
This disorder has been reported to be particularly rare as a sequel to cerebral lesions (Denes, 1989); Cutting (1978) did not come across it even in a large sample of acute hemiplegic patients, studied with a specific questionnaire. However, such accounts may not reflect the true incidence of the phenomenon (Conomy, 1973; Mayeux and Benson, 1979), as patients and physicians alike tend to under- estimate the significance of the illusory perception.
To our knowledge, SPL cases have not been reported for almost 20 years and the description, in a short interval of time, of three new patients (Halligan er al., 1993; Halligan and Marshall, 1995; Worthington and Beevers, 1996) provides renewed interest in recent literature concerning this interesting issue. Halligan et al. (1993) reported the case of a 65-year-old man who experienced a SPL after a haematoma within the right basal ganglia; even if a CT scan also demonstrated a general cerebellar and cerebral
hemispheric atrophy (the patient had a history of alcohol abuse), the neuropsychological assessment resulted normal; the patient only exhibited a gross left neglect. In the second case, Halligan and Marshall (1995) described an 80-year-old man who complained of SPL after an ischaemic stroke in the territory of the right middle cerebral artery (no more details were available); he showed gross left neglect too. In both cases, the phenomenon lasted for a long time. Finally, the third case report (Worthington and Beevers, 1996) concerned a 72-year-old woman, who, after a right hemisphere stroke, exhibited a SPL. Neuro- imagings (CT scan and MRI) demonstrated a large right temporo-parietal infarct involving the insular cortex and the internal capsule. Neuropsychological assessment showed a mild cognitive impairment, including left neglect.
These three papers investigate the patient’s personal attitude towards SPL by means of detailed interviews, in order to understand how patients’ consciousness deals with this erroneous belief. In fact, all the patients showed confusion arising from the belief in the existence of the SPL and, consequently, from the attempt to rationalize it; this fact produced distress.
In the present paper, we report the neuropsychological, neurophysiopathological and neuroradiological features of a SPL case secondary to a right subcortical ischaemic stroke and we discuss it in the light of the previous literature, trying to analyse the origin of this phenomenon.
Correspondence to: Monica Mazzoni, Neuropsychology Laboratory, Department of Neurosciences, Via Roma 67, 1-561 26 Pisa, Italy. Tel: +39.50.592570. Fax: +39.50.550563
Dow
nloa
ded
by [
Akd
eniz
Uni
vers
itesi
] at
11:
38 2
0 D
ecem
ber
2014

224 M. Mazzoni et ul.
Case report
RZ, a 66-year-old right-handed male with 13 years of education, is a retired technical illustrator and was in good health up to 2 August 1989, when he suffered sudden weakness of the left limbs. Upon admission to our department, the patient was alert, temporally and spatially well orientated; he presented left lower VIIth nerve facial palsy, complete loss of motor strength in his left arm and leg, Babinski sign on the same side; sensitivity to light touch and proprioception were impaired. Clinically, there was no gross left neglect (RZ did not ignore objects and people in the left side of his egocentred space), while anosognosia was present in that the patient denied his hemiplegia and tried to get up and walk. A cranial com- puterized tomography (CT) scan (2 August 1989) showed a non-uniform, hypodense area in the right nucleocapsular region, extending to the corona radiata; an electro- encephalogram (EEG), performed on 3 August 1989, showed mild electric activity slowing (4-6 Hz theta activity) on right fronto-temporal areas of the scalp, without any evidence of sharp waves. During the following days, anosognosia decreased and disappeared 8 days later. At this time, the patient complained of the perception, which he himselfcriticized, of a ‘third arm’ which did not correspond to his paralysed upper limb; for this reason, he was referred to our laboratory. The typical features of anosognosia were absent: in fact, the patient could explain why he had been admitted to hospital, he acknowledged the fact that he could not move his left limbs (in particular, the upper one) and he was worried about his condition. Examination of the patient’s sensitivity confirmed the presence of global hypoaesthesia, involving the modalities of touch, pain, temperature, vibration, passive motion and position in the left part of the body, which was more pronounced in the upper limb and particularly evident in the hand, where a frank anaesthesia was revealed.
Whilst being interviewed about his SPL, he stated that he felt the ‘third arm’ move both spontaneously (‘. . . it often happens that, while I am sitting up in bed with my eyes closed and my left arm folded beside me, I feel a third hand reach into my pyjama pocket and the fingers begin to grope around, as if trying to find something; then I open my eyes, I see my real hand lying motionless on the bed sheets, and the sensation goes away . . .’), as well as in response to voluntary commands (‘. . . if, with my eyes closed, I try to raise my arms out in front of me, I feel the third arm lift itself up, too, like the right one . . .’).
This ‘third limb’ was perceived in its entirety, even if it was the hand and fingers which were felt most vividly, and it was always and only present when the patient’s eyes were closed: indeed, he denied ever having seen it (‘. . . I only feel it . . .’) and he perceived the SPL ‘. . . as a normal limb, just like it was before the stroke, but only a bit shorter., .’. There was no perception of altered weight or sensitivity. The phantom was not a source of paraesthesia or pain, and
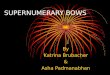
the sensation it transmitted most often was that of its fingers moving. The only contact in the environment w a the above mentioned one (i.e. with the pyjama pocket). The patient was asked to imagine visually the third limb: he reported that he could ‘. . . see prevalently the hand and especially the fingers . . . I imagine them like a normal hand and fingers’. Afterwards, he was asked to execute a drawing of the perception of his own body a n d he drew a human figure with two upper limbs, he lei1 one shorter than the right one (Fig. I ) ; asked if the left limb he had drawn was his own real one or the phantom limb, he said that it was the SPL and that he had not drawn his own real left limb ‘. . . because I could not feel it . . .’. RZ did not talk about the SPL with pleasure. While he spontaneously reported the onset of SPL during a physician’s visit, showing surprise because of ‘this strange thing’, he became reticent in response to specific questions about the SPL. He tried to minimize his trouble (‘. . . if I open my eyes, it is not there and I hope it will disappear’) and he did not ask himself what it could be and why it was there. When the physician explained to him that the SPL was only a sensation arising from his brain after a lesion (‘. . . i t is just like when you sleep on your arm and then you perceive pins and needles, but there are no real pins and needles’), RZ accepted this answer as rational: he was fully aware that he had two upper limbs, a right normal one and a left paralysed one. The SPL was only a perception, although a distressing one.
A neuropsychological evaluation ( 1 8 August 1989; for a summary of the test battery see Table 1 ) showed the patient’s language, praxis, visual-perceptive gnosis, memory functions, abstract thinking, righdleft orientation, visual excursion and attention to be normal; a mild deficit in the constructional apraxia task was detected, proved by a distorted perspective in cube and house drawings. Among tasks used to test for the presence of neglect (cancellation test, Map of Italy Test, copying drawings, calculation task, modified Benton’s Visual Retention Test, Raven’s Pro- gressive Matrices 1938, Corsi’s block tapping task - both span and supra-span - and visual searching task), only the visual searching task showed a higher incidence of errors in the left space.
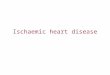
A magnetic resonance imaging (MRI) scan on 24 August 1989 revealed the presence of a large hnemorrhagic infarction, in the region supplied by the deep branches of the right middle cerebral artery, and associated thrombosis of the ipsilateral carotid siphon. The lesion involved the entire right lenticular nucleus, extending laterally to the external segment, medially to the internal segment of the capsula and superiorly to the head and body of the caudate nucleus and corona radiata (Fig. 2). Somatosensory evoked potentials (SEP) were recorded (25 August 1989) following unilateral stimulation of the median nerve at the wrist. SEP N20 and later components over the controlateral scalp could not be elicited by stimulating on the left side (Fig. 3). providing evidence of cortical deafferentation (Chiappa
Dow
nloa
ded
by [
Akd
eniz
Uni
vers
itesi
] at
11:
38 2
0 D
ecem
ber
2014

Supernumerary phantom limb 225
Fig. 1. The patient’s drawing of himself (18 August 1989).
et al., 1987; Mauguiere et af., 1987). For further details on the technical procedures employed in SEP recordings, see for example Sartucci et al. (1989).
The patient was discharged from hospital on 25 August 1989: he showed a slight recovery of strength in the lower left limb; the upper one remained paralysed, though a partial recovery of sensitivity to stimulation was evident at the proximal level, with persistence of distal hypoaesthesia, particularly in the fingers.
At a follow-up visit, nearly 24 years later (January 1992), the patient’s motor deficit appeared unchanged. Examina- tion of the patient’s sensitivity showed reduced perception of tactile, pain, thermal and vibratory stimuli over the left side of the face and the left upper limb; kinaesthetic sensitivity was impaired, with consistent errors in detecting finger movements, though the perception of whole-hand or thumb movement was less impaired. Although it had become less vivid the illusory perception of the ‘third limb’ persisted with the same characteristics as before; the
patient considered it an ‘annoying presence’, so he tried acupuncture to see if the SPL sensations diminished, without obtaining any result. Neuropsychological evalua- tion (22 January 1992) was normal (Table 1); a cranial CT scan (5 March 1992) showed stabilization of the right subcortical lesion and an EEG (26 March 1992) showed long 5-6 Hz theta activity sequences on the right hemi- sphere. SEP recordings were repeated (28 March 1992), and they yielded the same findings as in the first test.
Discussion This case closely resembles the descriptions of the ‘phantom third hand’ and the ‘supernumerary phantom’ reported following cerebral lesions (Critchley, 1953; Frederiks, 1963). The SPL is usually perceived to be shorter than the real one and is composed almost exclusively of the hand and the forearm; it is the source of anomalous positional perceptions which often involve contact with the thigh or thorax, and sometimes the phantom limb is perceived to be in motion, or at least capable of being moved.
RZ’s SPL occurred after a stroke in the area of the deep branches of the right middle cerebral artery, when post- onset anosognosia had disappeared and therefore, when the patient had become fully aware of his left hemiplegia and hemi-hypoaesthesia.
Worthington and Beevers (1996) emphasize the fact that the role of psychological factors cannot be excluded in SPL onset (‘a form of post-stroke adjustment reaction which provided the crucial trigger for the supernumerary limb experience’), especially until a ‘critical lesion’ has been discovered. The appearance of a SPL, after which RZ then became aware of his neurological deficit and was, therefore, without the masking effect of anosognosia, seems to be a confirmation of such a hypothesis. However, IU considered the third limb an ‘annoying presence’: in accordance with Halligan et al. (1993), psychodynamic accounts are difficult to accept in this situation.
Besides, in the most recent SPL cases reporting a detailed description of the site and extension of the cerebral lesion (Halligan et al., 1993; Worthington and Beevers, 1996), as well as in our case, right subcortical damage is consistently evident with sparing of the cortex; even if lesions are large, it is likely that they play a critical role in SPL onset. A subcortical lesion could cause the interrup- tion of the input to the parietal cortex. This interruption is clearly shown, in our case, by the loss of SEP waves over the scalp. According to Levine (1990), and supported by Halligan et al. (1993), SPL could arise from a completion made by the parietal cortex specific for body image, in the absence of an input from the hypoanaesthesic limb. RZ’s SPL, noteworthy for its kinaesthetic aspects, as the patient only rarely reports anomalous positional percep- tions unassociated with or as the result of movement (in particular, RZ’s perceptions of the third limb involve either
Dow
nloa
ded
by [
Akd
eniz
Uni
vers
itesi
] at
11:
38 2
0 D
ecem
ber
2014

226 M. Mazzoni et al.
Table 1. RZ's performance on neuropsychological tests
Score Score Cut-olf 18 August 1989 22 January 1992
Language Spontaneous speech (description of an event)" Oral and written naming: pictures' Token test' Auditory wordpicture matchingh Written wordpicture matching' Word and sentence repetition' Verbal fluency - phonetic cues (F,A,S)d
- semantic cues (colours, animals, fruits, towns)e
Praxis Oral praxis' tdeomotor praxis' Ideational praxis' Constructional praxis - copying drawings*
- three-dimensional block constructional praxish
- disyllabic word span' - story recall' - 10-word list (trials to criterion)k - 10-word list (mean of recalled words)k
- Corsi's block tapping test' - span-plus-2 learning on Corsi's block tapping devicek
Memory Verbal tests
Immediate visual memory' Spatial tests
Attention Visual searching task' Simple reaction times"'
Weigl's Sorting TestC Raven's Progressive Matrices 1938e
Visuoperceptive gnosias Benton's Visual Retention Test (modified)g Street's Completion Testr
Visuospatial functions Cancellation teste Map of Italy Test'
Calculation task" Right-left orientation" Finger localization testP
Abstract thinking
10110 20120 36/36 20120 20120 20120 44 23.5
18/20 20120 14/14 416
29/29
6 32
8 6.50
20122 4.5 5
48/60 219 s
10/15 38/48
14/15 8/14
13/13 15/15
9211 06 N* N'
>32
> 20 > 12.38
>I5 216 2 13 25
2 26
2 4 > 15.76 < 14.32
:.6.58 2 IS
2 4 < 25
>:l8.53 < 223.29
>7.43 > 17.91
> 10 :.3.55
> 10.22
> :74
N = normal; * = left side was not assessed because of severe sensitivity deficit. References: "Basso e ta / . , 1979; 'Gainotti et al., 1976, 'De Renzi and Faglioni, 1978; dBorkowski et ul.. 1967; eSpinnler and Tognoni, 1087; 'De Renri cr ul . , 1966; gGainotti et ul., 1977; hBenton, 1968; 'De Renzi and Nichelli, 1975; JDe Renzi e ta / . , 1977a; kDe Renzi et al., 1977b; 'Gainotti et d., 1978; "'Mazzoni et d., 1987; "Grafman et al., 1982; "Benton, 1966; PGainotti et al., 1972.
voluntary movements - usually co-activation of the con- trolateral limb - or spontaneous movements). The SPL is also consistently abolished by visual input. These symptoms can be considered an expression of the cortical areas involved in body image, acting independently of peripheral afferences; the latter, as they are still connected to the sensory-motor areas, as well as to the regions involved in motor planning, could act unconstrained by peripheral feedback, thus producing sensations not match- ing reality. The critical role played by visual input in the manifestation of the phenomenon, derives from the fact that it represents the only remaining peripheral input able to exert feedback control on the neuron pools governing the
bodily cortical representation of the affected limb (Melzack and Bromage, 1973).
Therefore, in our case, as well as in the previous ones (Halligan er al., 1993; Halligan and Marshall, 1995; Worthington and Beevers, 1996), the illusory perception could not be due to any generalized or partial cognitive decline, as proved by the general neuropsychological assessment which was within the normal range; the only symptom which is always present is that of neglect, but while in the previous cases a gross neglect is reported, RZ exhibited only a mild spatial inattention (not detectable clinically and by means of screening tests, such as the cancellation test, but noticeable only with a more sensitive
Dow
nloa
ded
by [
Akd
eniz
Uni
vers
itesi
] at
11:
38 2
0 D
ecem
ber
2014

Supernumerary phantom limb 227
Fig. 2. Magnetic resonance images (24 August 1989) show an extensive ischaernic infarction with haemorrhagic component in the region supplied by the deep branches of the right middle cerebral artery.
test, like the visual searching task, which contains more distractors) and not detected again at the follow-up assess- ment, in 1992.
The three theories proposed by Frederiks in 1963 in an attempt to explain the mechanisms underlying the illusory perception of limbs (regardless of the aetiology), although outdated, are still useful as a general schema, due to a present lack of modular cognitive models. These theories comprise:
1 Peripheral theory - considers the crucial factor to be persistent afferent input originating from the missing body part, whether it is lost through amputation or central nervous system (CNS) lesions.
2 Psychological theory - based on reported hallucinatory perceptions in some psychoses and the influence exerted by psychotherapeutic procedures and emotional states. Centrul theoty - considers the illusory perception to result from the autonomy andlor hyperactivity of deafierented CNS centres.
Frederiks (1963) emphasizes that, although each of the hypotheses serves to explain certain aspects of the anomaly, the most convincing overall is the so-called central theory. Several clinical and experimental findings support this hypothesis: phantom limbs due to amputation are usually relieved by controlateral cortical lesions (Head and Holmes, 191 1) ; phantom limbs, either with or without
3
Dow
nloa
ded
by [
Akd
eniz
Uni
vers
itesi
] at
11:
38 2
0 D
ecem
ber
2014

228 M. Mazzoni et al.
Ref. rg R
N9
L
.N13 N13
C 4 ?
Fig. 3. Somatosensory evoked potentials (25 August 1989) in response to unilateral stimulation of the median nerve, recorded at Erb’s points (Epl and Ep2). at the level of the 7th cervical vertebra ( C V ~ ) , and from the controlateral scalp (C3’ and C4’) 20 days after the patient had begun to sensc ihc presence of the ‘third upper limb on the left’. The numbers placed above the recordings indicate the latency of each component; Ref. indicates the referencc site employed (Fpz’). Note the absence of the N20 and later components following stimulation of the left median nerve.
amputation, may be determined by cortical irritative lesions, e.g. epileptic seizures (Riddoch, 1941 ; Critchley, 1953). Moreover, the use of some drugs (LSD, mescaline and ethanol), as well as toxaemia may alter these abnormal perceptual phenomena. Lastly, normal patients subjected to deep local anaesthesia may experience hallucinatory phenomena very much like those of the phantom limb syndrome (Jackson, 1884; Bartlet, 195 1 ; Thorpe, 1961 ; Melzack and Bromage, 1973; Wiegand, 1990). Also Levine’s hypothesis ( 1990) corresponds to the central theory, even if revised with the introduction of the ‘completion’ concept.
The three cases most recently reported in the literature (Halligan et al., 1993; Halligan and Marshall, 1995; Worthington and Beevers, 1996) are difficult to compare with RZ, as different clinical features were present: in all the patients there was gross neglect; in the first, a history of alcohol abuse, the presence of cortical and cerebellar atrophy dating back 2 years before the acute stroke; in the third mild cognitive impairment measured by several tests; but the most important feature was that all three patients believed in the presence of the SPL, and this fact caused them severe troubles when examiners presented them with logical assertions which caused confusion. RZ did not display such problems: after initial distress when speaking about the SPL (‘I fear people believe I am mad’), he under- stood, after the physician’s explanation, that the SPL was due to a perception created by his nervous system following cerebral damage and, hence, something annoying, but not
real. Nevertheless, some features in common should be emphasized, such as the long duration of the illusory perceptions, contrary to what is generally reported in the literature, as well as the side involved (right) and the subcortical location of the lesions, at least in one case.
Indeed, the presence of a sufficiently extensive sub- cortical lesion which spares the overlying cortex, may represent an essential condition for the occurrence of illusory perceptions and could also explain why s o few cases of supernumerary phantom limbs are on record. Finally, although all the cases recently reported in the literature, as well as RZ’s case, have been linked to right hemisphere lesions, the scarcity of the data does not allow us to make inferences on the relevance of the affected side at present (Frederiks, 1966; Halligan and Marshall, 1995).
Acknowledgements
The authors are very grateful to Dr John C. Marshall and to three anonymous referees for their useful comments on earlier drafts of this paper.
References Bartlet JE. A case of organized visual hallucinations In an old ma11 with
cataract, and their relation to the phenomena of the phantom Ilmh Brain 1951; 74: 363-84.
Basso A, Capitani E, Vignolo LA. Influence of rehabilitation o i l
language skills in aphasic patients. Archives of Neurcllogy 1979; 36. 190-6.
Dow
nloa
ded
by [
Akd
eniz
Uni
vers
itesi
] at
11:
38 2
0 D
ecem
ber
2014

Supernumerary phantom limb 229
Benton AL. Problemi di neuropsicologia. Firenze: Editrice Universitaria Barbera, 1966.
Benton AL. La praxie constructive tridimensionelle. Revue de Psychologie Appliquee 1968: 18: 63-80.
Borkowski JC, Benton AL, Spreen 0. Word fluency and brain damage. Neuropsychologia 1967: 5: 135-40.
Chiappa KH. Interpretation of abnormal short-latency somatosensory evoked potentials. In: Halliday AM, Butler SR, Paul P, editors. A textbook of clinical neurophysiology. Chichester: John Wiley and Sons, 1987: 343-81.
Conomy JP. Disorders of body image after spinal cord injury. Neurology 1973; 23: 842-50.
Critchley M. The parietal lobes. London: Edward Arnold and Company, 1953.
Cutting J. Study of anosognosia. Journal of Neurology, Neurosurgery and Psychiatry 1978: 41: 548-55.
Denes G . Disorders of body awareness and body knowledge. In: Boller F, Grafman J. editors. Handbook of neuropsychology. Vol. 2. Amster- dam: Elsevier, 1989: 207-28.
De Renzi E. Faglioni P. Normative data and screening power of a shortened version of Token Test. Cortex 1978; 8: 364-81.
De Renzi E, Nichelli P. Verbal and non-verbal short-term memory impairment following hemispheric damage. Cortex 1975: 1 1 : 341 -54.
De Renzi E, Pieczuro A, Vignolo LA. Oral apraxia and aphasia. Cortex 1966: 2: 50-73.
De Renzi E. Faglioni P, Ruggerini C. Prove di memoria verbale di impiego clinico per la diagnosi di amnesia. Archivio di Psicologia. Neurologia e Psichiatria 1977a; 38: 303- 18.
De Renzi E, Faglioni P, Previdi P. Spatial memory and hemispheric locus of lesion. Cortex 1977b; 13: 424-33.
Frederiks JAM. Occurrence and nature of phantom limb phenomena following amputation of body parts and following lesions of the central and peripheral nervous system. Psychiatria, Neurologia, Neurochirurgia 1963: 66: 73-97.
Frederiks JAM. The diagnosis of disturbances of the body schema. Psychiatria. Neurologia, Neurochirurgia 1966: 69: 329-36.
Gainotti G, Cianchetti C, Tiacci C. The influence of the hemispheric side of lesion on non-verbal tasks of finger localization. Cortex 1972; 8:
Gainotti G, Caltagirone C, Miceli G . Sui rapporti fra alcune prove di intelligenza verbale e lesioni focali monoemisferiche. Acta Neurolo- gica 1976; 31: 370-81.
Gainotti G , Miceli G . Caltagirone C. Constructional apraxia in left brain- damaged patients: a planning disorder? Cortex 1977: 13: 109-18.
364-81.
Gainotti G . Caltagirone C, Miceli G. Immediate visual-spatial memory in hemisphere-damaged patients: impairment of verbal coding and perceptual processing. Neuropsychologia 1978; 16: 501 -7.
Grafman J. Passafiume D, Faglioni P, Boller F. Calculation disturbances in adults with focal hemispheric damage. Cortex 1982: 18: 37-49.
Halligan PW, Marshall JC. Derick TW. Three arms: a case study of supernumerary phantom limb after right hemisphere stroke. Journal of Neurology, Neurosurgery and Psychiatry 1993: 56: 159-66.
Halligan PW, Marshall JC. Supernumerary phantom limb after right hemisphere stroke. Journal of Neurology, Neurosurgery and Psychiatry 1995: 59: 341-2.
Head H, Holrnes G . Sensory disturbances from cerebral lesions. Brain 191 I ; 34: 102-254.
Jackson JH. The Croonian lectures on evolution and dissolution of the nervous system. British Medical Journal 1884: 1: 591-3, 660-3,
Levine DN. Unawareness of visual and sensorimotor defects: a hypothesis. Brain and Cognition 1990: 13: 233-81.
Mayeux R. Benson DF. Phantom limbs and multiple sclerosis. Neurology 1979: 29: 724-6.
Mauguiere F, Gonnaud PM, Ibanez V, Schott B. Potentiels evoques somesthesiques precoces et deficits sensitifs dans les lesions thala- miques et juxta-talamiques. Revue Neurologique 1987: 143: 643-56.
Mazzoni M, Bonanni E, Bonuccelli U, Murri L. Comparison of the effects of barbexaclone and phenobarbital on epileptic patients. Current Therapy Research 1987: 42: 671-9.
Melzack R, Bromage PR. Experimental phantom limbs. Experimental Neurology 1973; 39: 261-9.
Riddoch G . Phantom limbs and body shape. Brain 1941: 64: 197-222. Sartucci F, Marconi F, Busso E, Rossi B, Murri L. Multimodality evoked
potentials in myotonic dystrophy. The Italian Journal of Neurological Sciences 1989; 10: 61-7.
Spinnler H, Tognoni G. Taratura e standardizzazione di test neuro- psicologici. The Italian Journal of Neurosciences 1987: Suppl 6.
Thorpe JG. Sensory deprivation. Journal of Mental Science 1961: 451: 1 047- 53.
Wiegand H. Das deafferentierungskonzept. Neurochirurgia 1990: 33: 97-9.
Worthington A, Beevers L. Two arms, three hands. A supernumerary phantom phenomenon after right middle cerebral artery stroke. Neurocase 1996; 2: 135-40.
Received on 10 June, 1996; resubmitted on 17 December, 1996; accepted on 15 January, 1997
703-7.
Dow
nloa
ded
by [
Akd
eniz
Uni
vers
itesi
] at
11:
38 2
0 D
ecem
ber
2014

230 M. Mazzoni et al.
Supernumerary phantom limb after ischaemic stroke
M. Mazzoni, C. Lucchini, G. Meucci, M. Vista, P. Moretti and F. Sartucci Abstract We describe a case of supernumerary phantom limb following focal cerebral ischaemia and discuss its neuropsychological, neurophysio- pathological and neuroradiological features in light of previous data in the literature. The illusory perception of a phantom limb, seldom reported as a consequence of cerebral lesions, seems in this case to be due to right subcortical damage altering sensory input to the higher somatosensory cortical areas involved in body image.
Journal Neurocase 1997; 3: 223-30
Neurocase Reference Number:
Primary diagnosis of interest
Author’s designation of case
Key theoretical issue
0 7 8
lschaemic stroke
RZ
0 Investigation of whether RZ’s case fits the central theory, which considers the illusory perception of a supernumerary phantom limb to result from the autonomy and/or hyperactivity of deafferented CNS centres
Key words: supernumerary phantom limb; body image; somatosensory evoked potentials
I . CT 2. MRI 3. SEP 4. EEG
Scan, EEG and related measures
Standardized assessment Laterality; spontaneous speech, oral and written naming, token test, oral wordpicture matching, written wordpicture matching, verbal fluency on phonetic and semantic cues; oral praxis, ideomotor praxis, utilization praxis, constructional praxis (copying drawings, three-dimensional block constructional praxis); disyllabic word span, story recall, 10-word list, immediate visual memory, Corsi’s block tapping test, span-plus-2 learning on Corsi’s block tapping device; visual searching task, reaction times; Weigl’s sorting test, Raven’s Progressive Matrices 1938; Benton’s Visual Retention Test (mod.), Street’s Completion Test; calculation task; right-left orientation; finger localization test
Other assessment
Lesion location Nil
0 Right lenticular nucleus, extending laterally to the external capsule, medially to the internal capsule and superiorly to the head and body of the caudate nucleus and corona radiata
Lesion type
Language lschaemic stroke with a haemorrhagic component
English
Dow
nloa
ded
by [
Akd
eniz
Uni
vers
itesi
] at
11:
38 2
0 D
ecem
ber
2014