Embed Size (px)
Citation preview
08/09/2015
1
Walter Mak, MD
Department of Medical Imaging
St. Michael’s Hospital
Walter Mak, MD
Department of Medical Imaging
St. Michael’s Hospital
Superficial Lumps and Bumps:Ultrasound Assessment
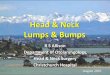
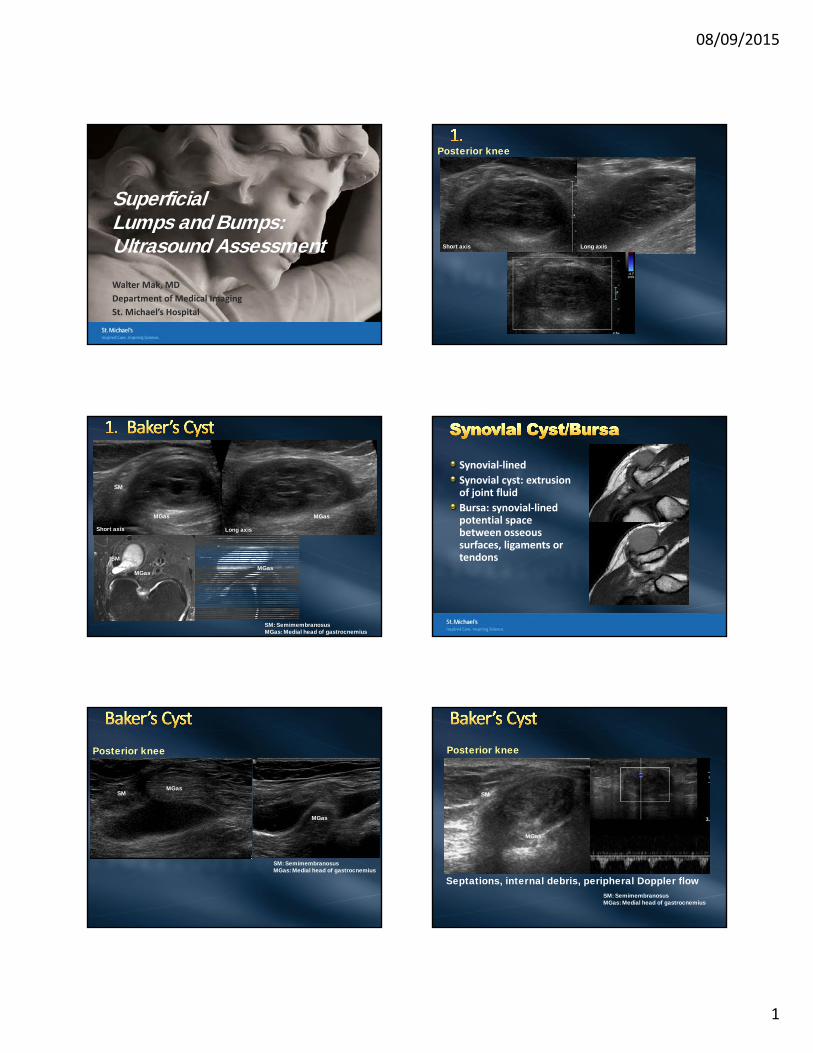
Posterior knee
Long axisShort axis
MGas
SM
MGas
MGasSM
MGas
SM: SemimembranosusMGas: Medial head of gastrocnemius
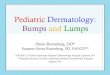
Long axisShort axis
Synovial‐lined
Synovial cyst: extrusion of joint fluid
Bursa: synovial‐lined potential space between osseous surfaces, ligaments or tendons
MGas
MGas
SM
SM: SemimembranosusMGas: Medial head of gastrocnemius
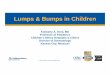
Posterior knee
MGas
SM
Septations, internal debris, peripheral Doppler flowSM: SemimembranosusMGas: Medial head of gastrocnemius
Posterior knee
08/09/2015
2
Long axis Short axis
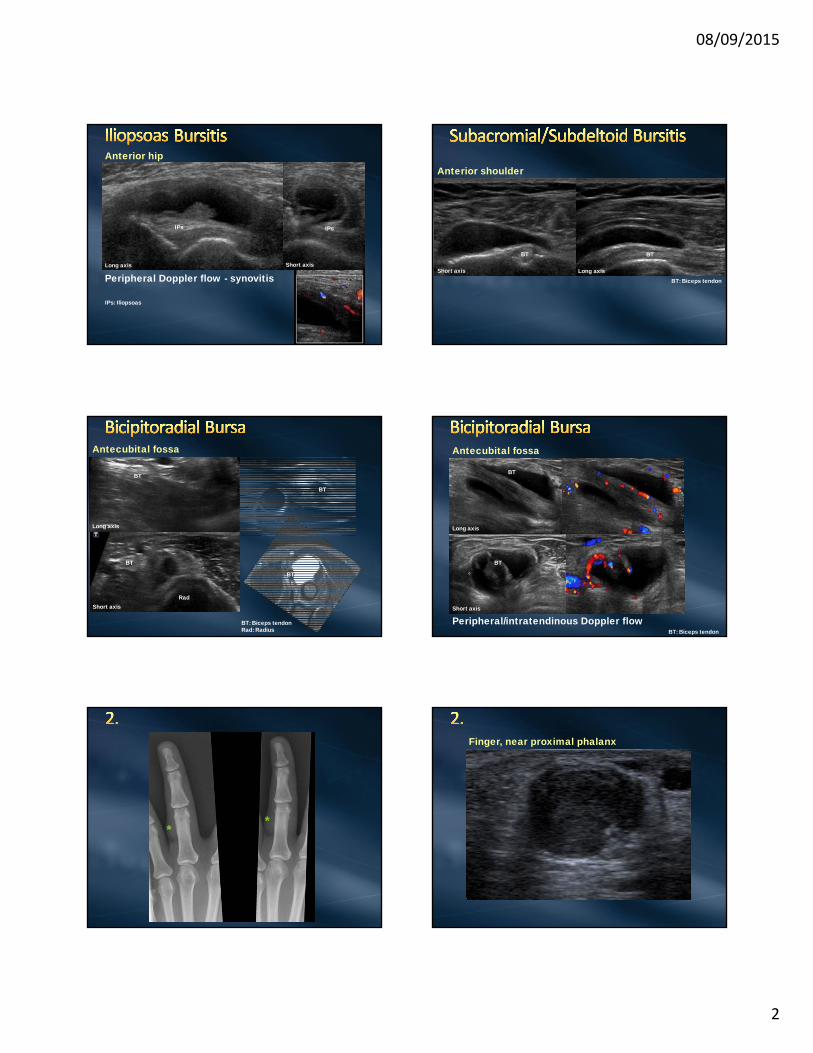
Peripheral Doppler flow - synovitis
Anterior hip
IPs
IPs: Iliopsoas
IPs
Anterior shoulder
Long axisShort axis
BT
BT: Biceps tendon
BT
BT
BT
BT
BT
Rad
BT: Biceps tendonRad: Radius
Antecubital fossa
Long axis
Short axis
Peripheral/intratendinous Doppler flow
BT
BT
BT: Biceps tendon
Antecubital fossa
Long axis
Short axis
* *
Finger, near proximal phalanx
08/09/2015
3
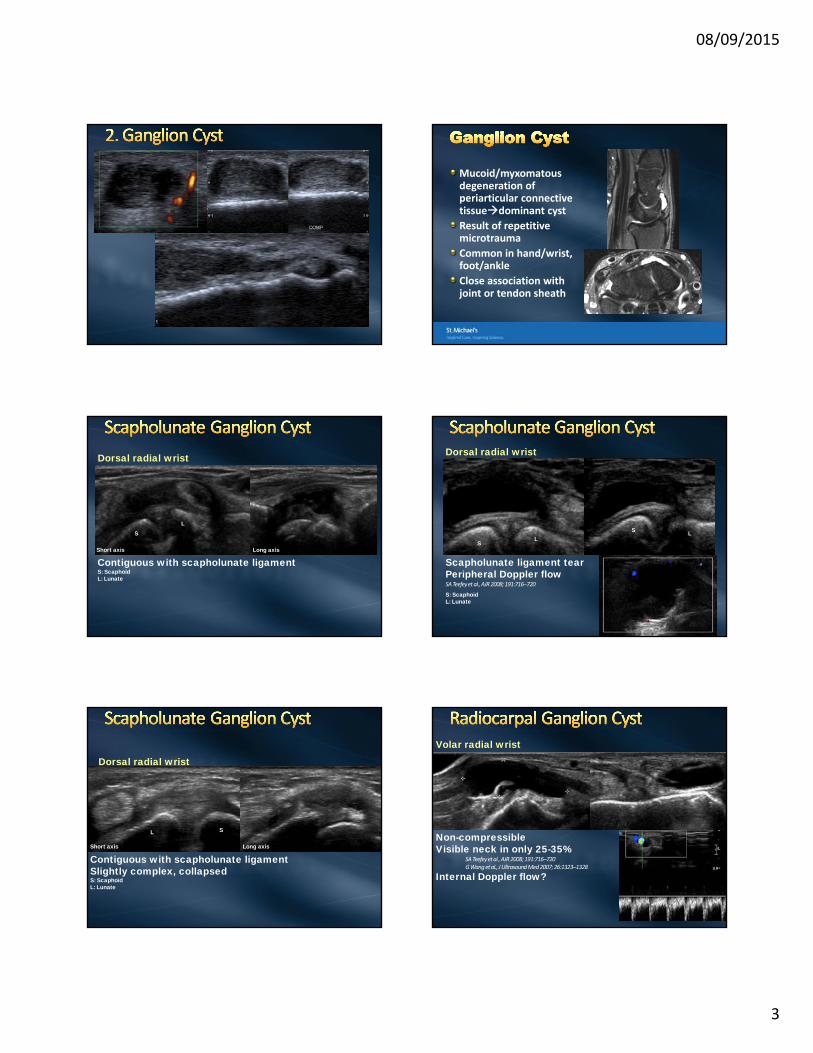
Mucoid/myxomatousdegeneration of periarticular connective tissuedominant cyst
Result of repetitive microtrauma
Common in hand/wrist, foot/ankle
Close association with joint or tendon sheath
Dorsal radial wrist
Contiguous with scapholunate ligamentS: ScaphoidL: Lunate
SL
Long axisShort axis
S: ScaphoidL: Lunate
Scapholunate ligament tearPeripheral Doppler flowSA Teefeyet al., AJR 2008; 191:716–720
Dorsal radial wrist
S LS
L
Dorsal radial wrist
Contiguous with scapholunate ligamentSlightly complex, collapsedS: ScaphoidL: Lunate
SL
Long axisShort axis
Volar radial wrist
Non-compressibleVisible neck in only 25-35%
SA Teefeyet al., AJR 2008; 191:716–720G Wang et al., J Ultrasound Med 2007; 26:1323–1328
Internal Doppler flow?
08/09/2015
4
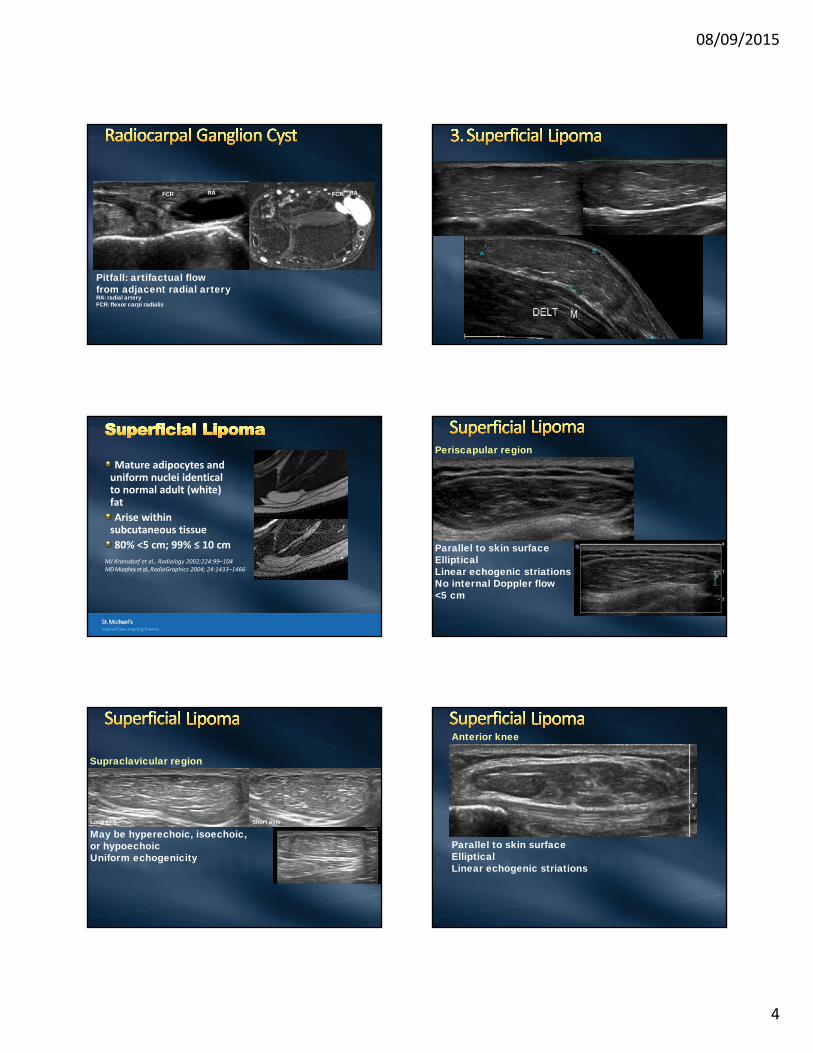
Pitfall: artifactual flow from adjacent radial artery
FCR FCR
RA: radial arteryFCR: flexor carpi radialis
RA RA
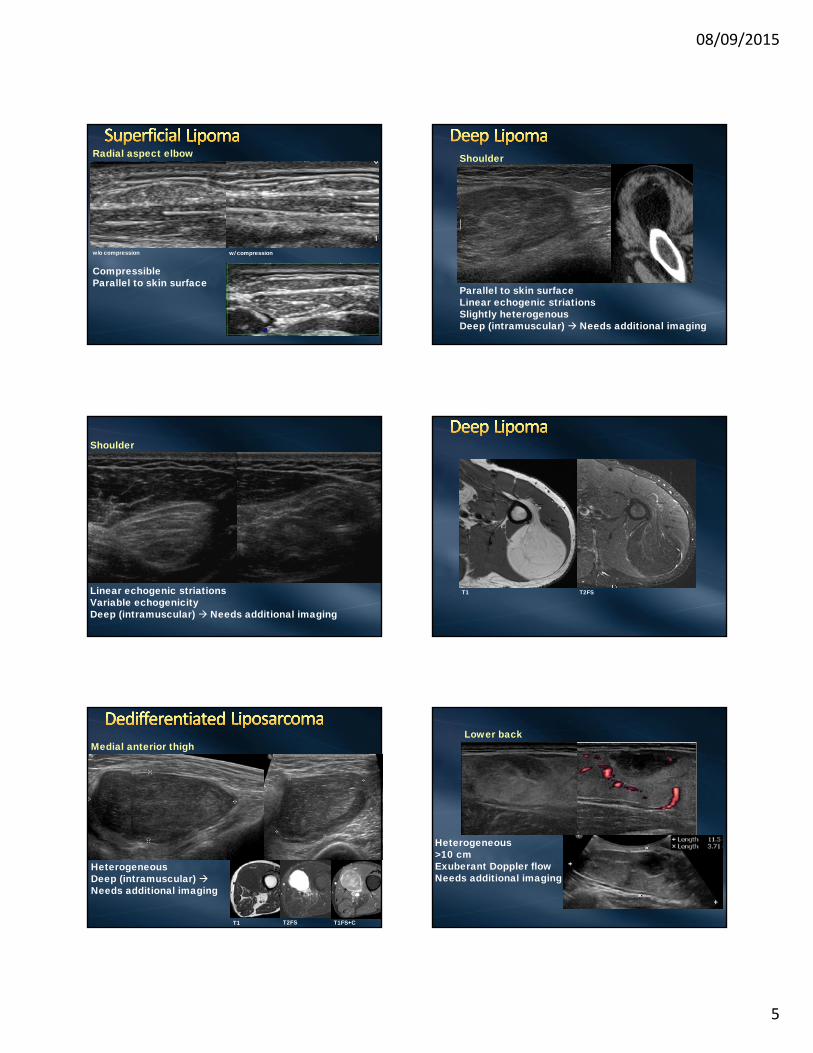
Mature adipocytes and uniform nuclei identical to normal adult (white) fat
Arise within subcutaneous tissue
80% <5 cm; 99% ≤ 10 cm
MJ Kransdorf et al., Radiology 2002;224:99–104MD Murpheyet al., RadioGraphics 2004; 24:1433–1466
Periscapular region
Parallel to skin surfaceEllipticalLinear echogenic striationsNo internal Doppler flow<5 cm
Supraclavicular region
Long axis Short axis
May be hyperechoic, isoechoic,or hypoechoicUniform echogenicity
Anterior knee
Parallel to skin surfaceEllipticalLinear echogenic striations
08/09/2015
5
Radial aspect elbow
CompressibleParallel to skin surface
w/o compression w/ compression
Shoulder
Parallel to skin surfaceLinear echogenic striationsSlightly heterogenousDeep (intramuscular) Needs additional imaging
Shoulder
Linear echogenic striationsVariable echogenicityDeep (intramuscular) Needs additional imaging
T1 T2FS
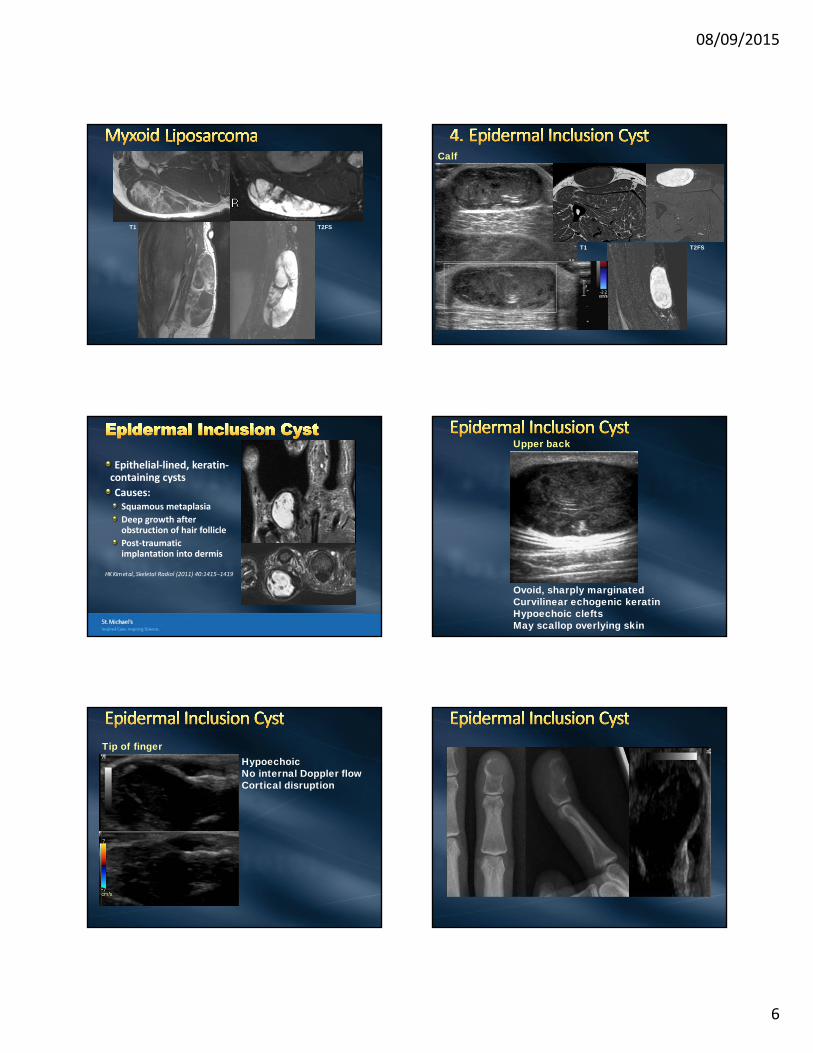
Medial anterior thigh
HeterogeneousDeep (intramuscular) Needs additional imaging
T1 T2FS T1FS+C
Lower back
Heterogeneous>10 cmExuberant Doppler flowNeeds additional imaging
08/09/2015
6
T1 T2FS
Calf
T1 T2FS
Epithelial‐lined, keratin‐containing cysts
Causes:Squamous metaplasia
Deep growth after obstruction of hair follicle
Post‐traumatic implantation into dermis
HK Kim et al., Skeletal Radiol (2011) 40:1415–1419
Upper back
Ovoid, sharply marginatedCurvilinear echogenic keratin Hypoechoic cleftsMay scallop overlying skin
Tip of fingerHypoechoicNo internal Doppler flowCortical disruption

08/09/2015
7
Proximal lateral thigh
Long axis Short axis
Degloving injury of proximal thigh
Separation of fascia from subcutaneous tissue and vascular/lymphatic disruption
Collection containing blood, lymph, fat
Chronic: fusiform, hypoechoicGlobules of echogenic fatNo internal Doppler flow
Proximal lateral thigh
May be complex Globules of echogenic fatNo internal Doppler flow
Proximal lateral thigh
Globules of echogenic fatCompressible
w/o compression w/ compression
Proximal lateral thigh Proximal calf, near knee
Morel-Lavallée also observedabout the knee
Acute: may be lobulated,heterogeneousGlobules of echogenic fat
SG Tejwani et al., Am J Sports Med 2007; 35:1162‐1167
08/09/2015
8
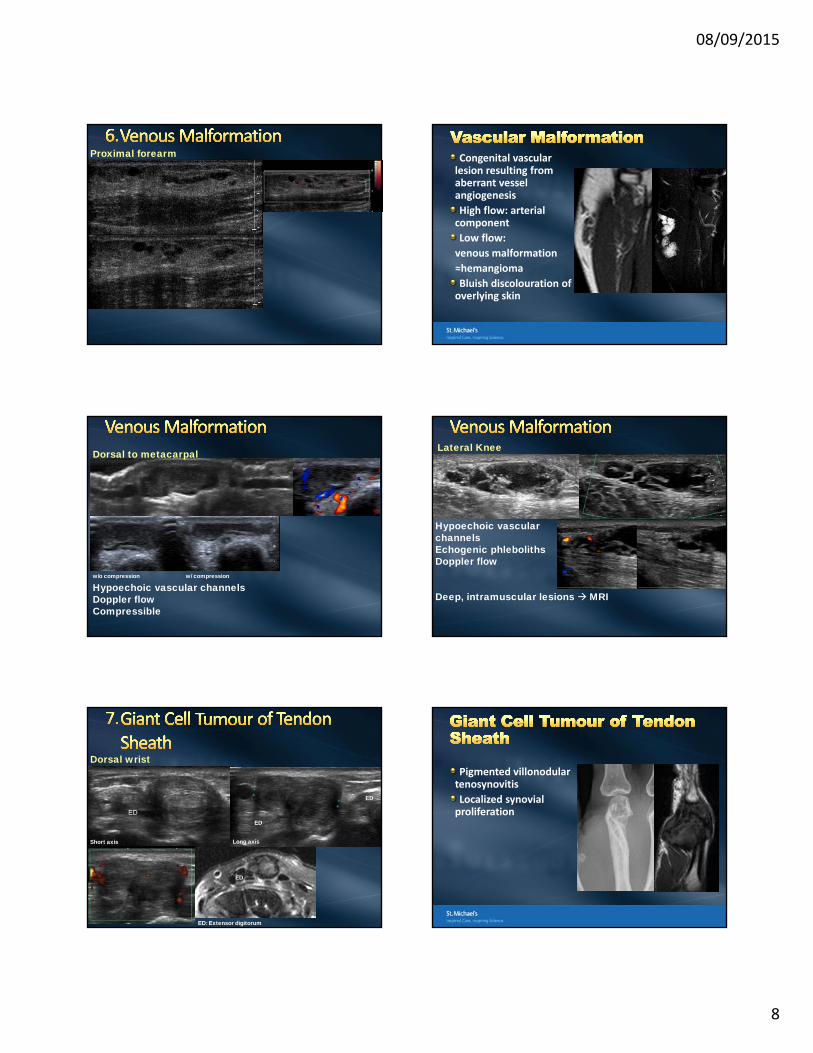
Proximal forearm Congenital vascular lesion resulting from aberrant vessel angiogenesis
High flow: arterial component
Low flow:
venous malformation
≈hemangioma
Bluish discolouration of overlying skin
Dorsal to metacarpal
w/o compression w/ compression
Hypoechoic vascular channels Doppler flowCompressible
Lateral Knee
Hypoechoic vascularchannelsEchogenic phlebolithsDoppler flow
Deep, intramuscular lesions MRI
Dorsal wrist
Long axisShort axis
ED: Extensor digitorum
ED
ED
ED
Pigmented villonodulartenosynovitis
Localized synovial proliferation
08/09/2015
9
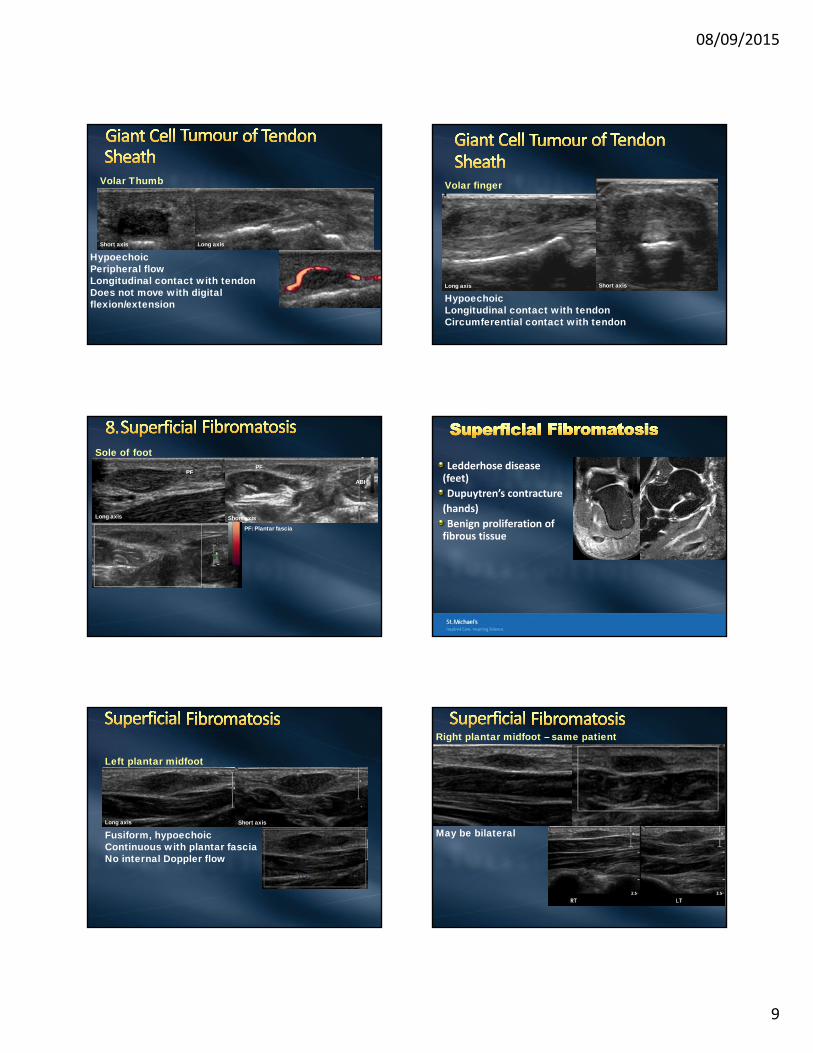
Volar Thumb
HypoechoicPeripheral flowLongitudinal contact with tendonDoes not move with digital flexion/extension
Long axisShort axis
Volar finger
HypoechoicLongitudinal contact with tendonCircumferential contact with tendon
Long axis Short axis
Sole of footPF
ABH
PF: Plantar fascia
Long axis Short axis
PFLedderhose disease (feet)
Dupuytren’s contracture
(hands)
Benign proliferation of fibrous tissue
Left plantar midfoot
Fusiform, hypoechoicContinuous with plantar fasciaNo internal Doppler flow
Long axis Short axis
Right plantar midfoot – same patient
May be bilateral
08/09/2015
10
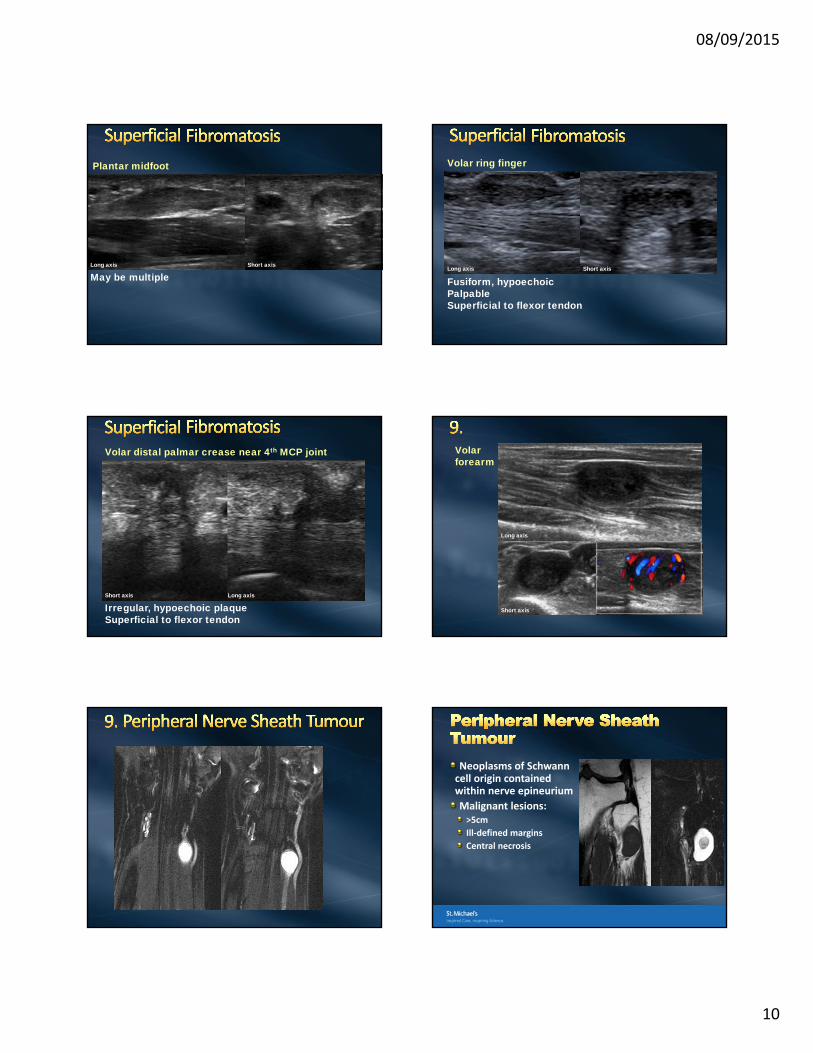
Plantar midfoot
May be multipleLong axis Short axis
Volar ring finger
Fusiform, hypoechoicPalpableSuperficial to flexor tendon
Long axis Short axis
Volar distal palmar crease near 4th MCP joint
Irregular, hypoechoic plaqueSuperficial to flexor tendon
Long axisShort axis
Volar forearm
Long axis
Short axis
Neoplasms of Schwann cell origin contained within nerve epineurium
Malignant lesions:>5cm
Ill‐defined margins
Central necrosis
08/09/2015
11
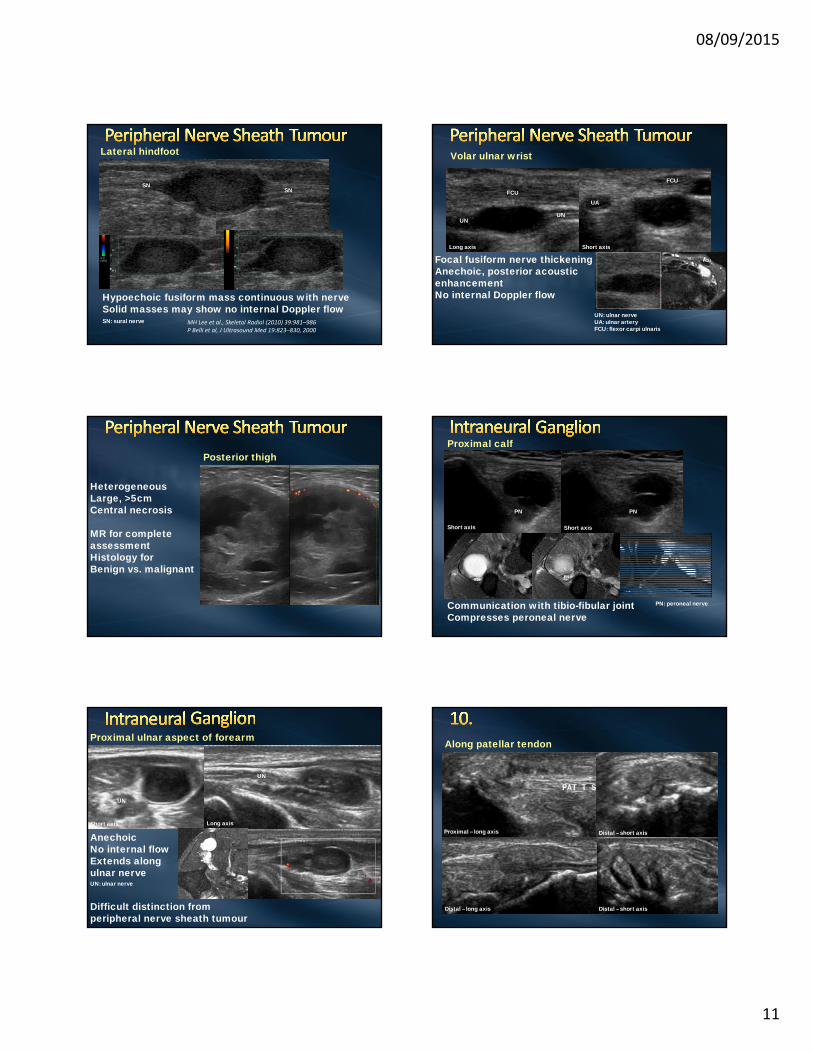
Lateral hindfoot
Hypoechoic fusiform mass continuous with nerveSolid masses may show no internal Doppler flow
MH Lee et al., Skeletal Radiol (2010) 39:981–986P Belli et al, J Ultrasound Med 19:823–830, 2000
SNSN
SN: sural nerve
Volar ulnar wrist
Long axis Short axis
UN
UN: ulnar nerveUA: ulnar arteryFCU: flexor carpi ulnaris
Focal fusiform nerve thickeningAnechoic, posterior acousticenhancementNo internal Doppler flow
UN
UA
UA
FCU
FCU
FCU
Posterior thigh
HeterogeneousLarge, >5cmCentral necrosis
MR for completeassessmentHistology forBenign vs. malignant
Communication with tibio-fibular jointCompresses peroneal nerve
PN: peroneal nerve
PN
Proximal calf
PN
PN PN
Short axis Short axis
Proximal ulnar aspect of forearm
UN
UN: ulnar nerve
AnechoicNo internal flowExtends along ulnar nerve
UN
UN
Long axisShort axis
Difficult distinction from peripheral nerve sheath tumour
Along patellar tendon
Proximal – long axis
Distal – long axis Distal – short axis
Distal – short axis
08/09/2015
12
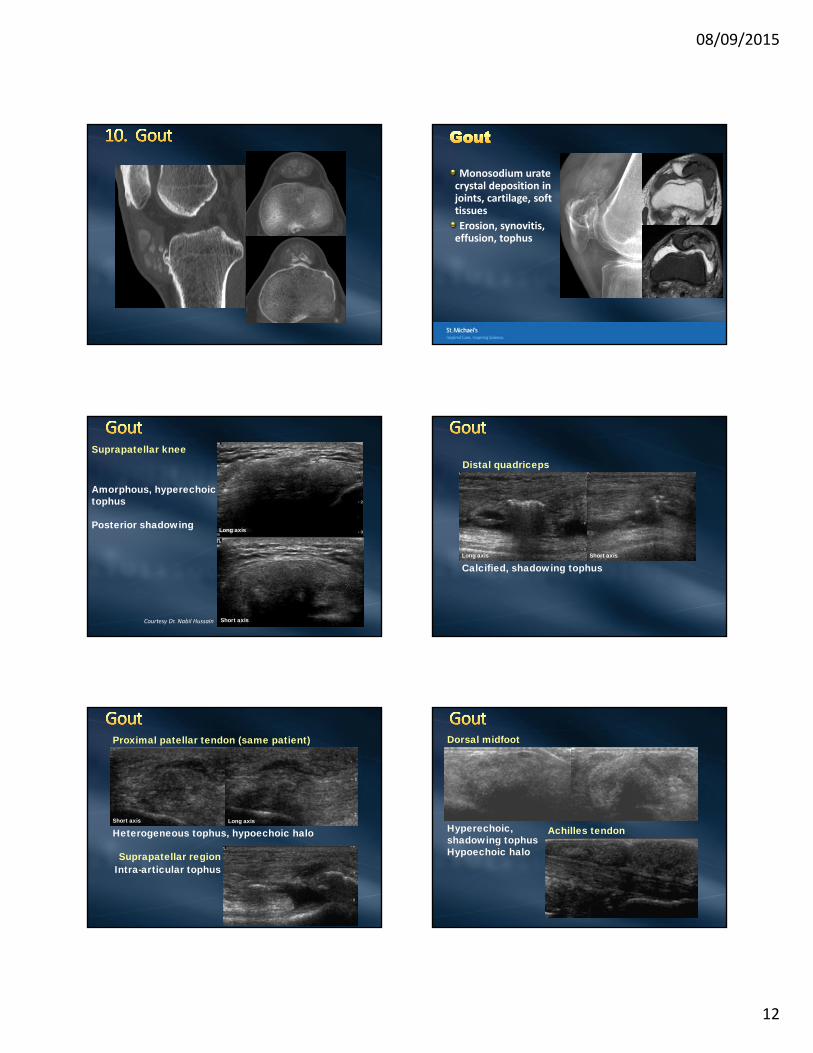
Monosodium uratecrystal deposition in joints, cartilage, soft tissues
Erosion, synovitis, effusion, tophus
Suprapatellar knee
Amorphous, hyperechoictophus
Posterior shadowing
Courtesy Dr. Nabil Hussain
Long axis
Short axis
Distal quadriceps
Calcified, shadowing tophusShort axisLong axis
Proximal patellar tendon (same patient)
Heterogeneous tophus, hypoechoic halo
Suprapatellar regionIntra-articular tophus
Long axisShort axis
Dorsal midfoot
Achilles tendonHyperechoic, shadowing tophusHypoechoic halo
08/09/2015
13
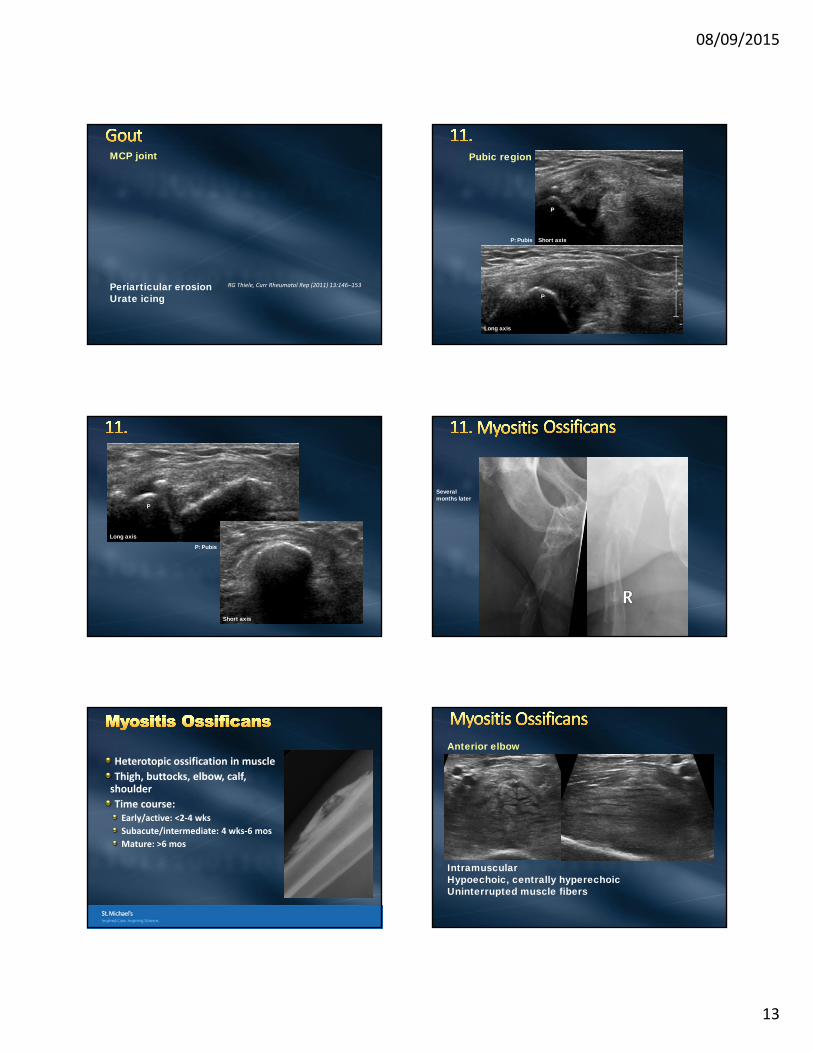
MCP joint
Periarticular erosionUrate icing
RG Thiele, Curr Rheumatol Rep (2011) 13:146–153
Pubic region
Long axis
Short axis
P
P: Pubis
P
P: Pubis
P
Long axis
Short axis
Severalmonths later
Heterotopic ossification in muscle
Thigh, buttocks, elbow, calf, shoulder
Time course:Early/active: <2‐4 wks
Subacute/intermediate: 4 wks‐6 mos
Mature: >6 mos
Anterior elbow
Intramuscular Hypoechoic, centrally hyperechoicUninterrupted muscle fibers
08/09/2015
14
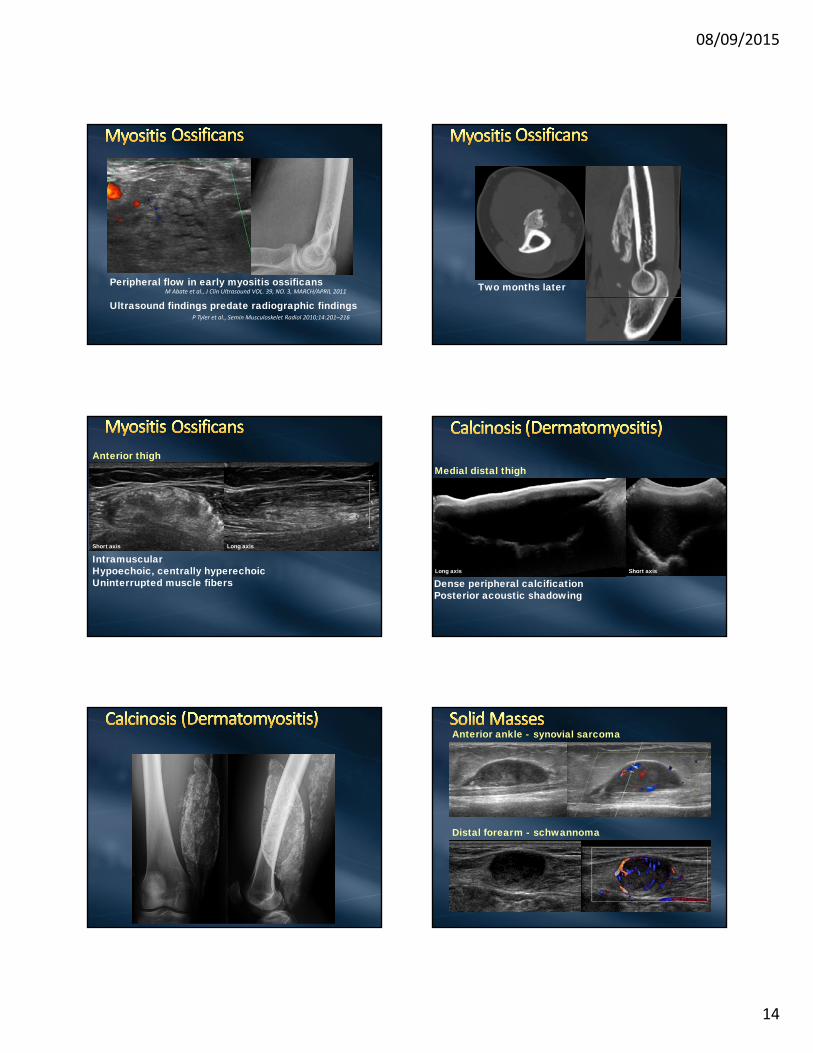
Peripheral flow in early myositis ossificans
Ultrasound findings predate radiographic findingsM Abate et al., J Clin Ultrasound VOL. 39, NO. 3, MARCH/APRIL 2011
P Tyler et al., Semin Musculoskelet Radiol 2010;14:201–216
Two months later
Anterior thigh
IntramuscularHypoechoic, centrally hyperechoicUninterrupted muscle fibers
Long axisShort axis
Medial distal thigh
Dense peripheral calcificationPosterior acoustic shadowing
Long axis Short axis
Anterior ankle -
Distal forearm -
synovial sarcoma
schwannoma
08/09/2015
15
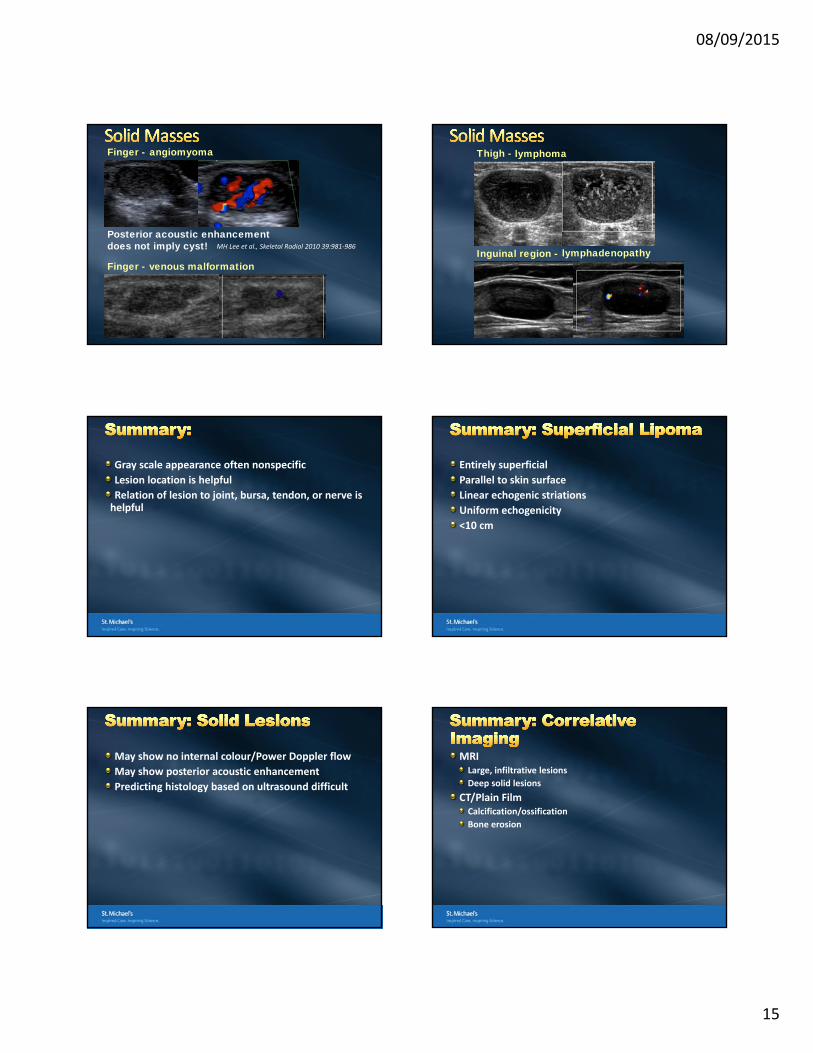
Finger -
Posterior acoustic enhancement does not imply cyst! MH Lee et al., Skeletal Radiol 2010 39:981‐986
Finger -
angiomyoma
venous malformation
Thigh -
Inguinal region -
lymphoma
lymphadenopathy
Gray scale appearance often nonspecific
Lesion location is helpful
Relation of lesion to joint, bursa, tendon, or nerve is helpful
Entirely superficial
Parallel to skin surface
Linear echogenic striations
Uniform echogenicity
<10 cm
May show no internal colour/Power Doppler flow
May show posterior acoustic enhancement
Predicting histology based on ultrasound difficult
MRILarge, infiltrative lesions
Deep solid lesions
CT/Plain FilmCalcification/ossification
Bone erosion
08/09/2015
16
A Baker’s cyst extends between which two structures?
A) Semimembranosus and medial head of gastrocnemius
B) Semitendinosus and medial head of gastrocnemius
C) Semitendinosus and sartorius
D) Semitendinosus and gracilis
E) Sartorius and gracilis
A Baker’s cyst is located between which two tendons?
A) Semimembranosus and medial head of gastrocnemius
B) Semitendinosus and medial head of gastrocnemius
C) Semitendinosus and sartorius
D) Semitendinosus and gracilis
E) Sartorius and gracilis
Which of the following is LEAST helpful in ultrasound assessment of a focal mass lesion?
A) Relationship to joint, nerve, or tendon
B) Presence of internal flow on colour/power Doppler
C) Posterior acoustic shadowing
D) Posterior acoustic enhancement
E) Lesion location
Which of the following is LEAST helpful in ultrasound assessment of a focal mass lesion?
A) Relationship to joint, nerve, or tendon
B) Presence of internal flow on colour/power Doppler
C) Posterior acoustic shadowing
D) Posterior acoustic enhancement
E) Lesion location
Thank you.