Embed Size (px)
Citation preview

““SUPERBETTER”SUPERBETTER”Integrating Substance Use Disorder CareIntegrating Substance Use Disorder Care
Dr. Jack McCarthyDr. Jack McCarthyValerie Yv. Woolsey, MBAValerie Yv. Woolsey, MBA
BAART ProgramsBAART Programs

Overview
• BAART Programs– Who we are – What we do
• “What we talk about when we talk about SUD”– Overview of MAT and Opioid Treatment– Structured Narcotic Treatment Programs– Compliance, Retention, and Key Predictors of success
• Managed Care and the Integrated Care Payor Mix– Network adequacy– SBIRT and Health homes
• PPACA in California: Federal vs. State legislation– Network adequacy– Drug Medi-cal and the 1115 Waiver
• Comments and Questions
Strategic Role of Community Clinics: Strategic Role of Community Clinics: Meeting the Safety Net Provider ChallengeMeeting the Safety Net Provider Challenge
One of the biggest One of the biggest challenges as we look at challenges as we look at ourselves as a safety ourselves as a safety provider network is who provider network is who is driving the spend. Our is driving the spend. Our goal is goal is to to maximize maximize efficiency by making efficiency by making sure members are tied sure members are tied to providers who to providers who effectively manage effectively manage their care.their care.
Safety Net Perspective
1 1
Who We Are
That may mean we do That may mean we do not need more not need more providers, just key ones providers, just key ones who are focused, and to who are focused, and to whom new members whom new members can be directed in a way can be directed in a way that mimics medical that mimics medical home strategy to home strategy to maximize coordination maximize coordination of services. Simply of services. Simply contracting with payors contracting with payors offering products on the offering products on the Covered California Covered California exchange does not exchange does not address the full scope of address the full scope of integrated care.integrated care.
What That Means
Community health ommunity health providers are effective providers are effective because, being so because, being so intertwined with their intertwined with their neighborhoods, have neighborhoods, have been seen as the been seen as the original patient-directed original patient-directed centers who identify centers who identify health needs earlier and health needs earlier and design effective design effective community based community based solutions before others solutions before others even understand even understand underlying dynamicsunderlying dynamics
3322

BAART Programs
• Bay Area Addiction Research and Treatment “BAART” Programs was incorporated in 1977 to provide methadone treatment to the opiate addicted population in San Francisco. Since inception, BAART has grown in number of clinics and types of services it provides. We now operate 20 clinics in 5 states, providing a range of MAT, primary care and mental health services.
• Operating as a network of clinics that provide health care services to indigent populations, BAART’s mission is to provide people with cost-effective, comprehensive medical and other health care services through community linkages at its clinics and to make such services available to as many people as possible that seek them. By doing so, BAART Programs can foster the health, happiness and longevity of those individuals and can help them benefit our communities.
• BAART programming is co-located in it’s clinics or is coordinated through formal arrangements with other providers. We have the knowledge and resources to treat our patients from an integrative standpoint, combining primary care, mental health and substance abuse treatment services. This “one-stop-shop” approach to care decreases the likelihood of patients falling through the cracks when shuffled between providers.
• As a result, BAART clinics have become the medical home to many of the residents of our communities, decreasing unnecessary emergency room use and hospitalizations and decreasing disjointed care through our integrated care model.

SUD and Mental Health Disease State ParametersSUD and Mental Health Disease State Parameters
11Medications or psychotherapy can address Medications or psychotherapy can address other symptoms or problems that are other symptoms or problems that are discovered in the course of evaluation and discovered in the course of evaluation and treatment.treatment.
Addictions are complex with multiple causes
Commonly, people with depressant Commonly, people with depressant addictions are also struggling with other addictions are also struggling with other mental disorders, such as anxiety or mental disorders, such as anxiety or depressiondepression
SUD typically not an isolated problem
33
A comprehensive evaluation (medical, psychological and social) to identify the variety of troubles that are fueling the drug abuse or misuse is key.
Counseling and tailored treatment help
According to the National Institute According to the National Institute on Drug Abuse (NIDA), addiction is on Drug Abuse (NIDA), addiction is a chronic, relapsing disease a chronic, relapsing disease characterized by compulsive drug-characterized by compulsive drug-seeking abuse and by long-lasting seeking abuse and by long-lasting chemical changes in the brain. chemical changes in the brain. While there is no cure for addiction, While there is no cure for addiction, users can get help to treat their users can get help to treat their disease. Drug use and abuse disease. Drug use and abuse typically begins with a gateway typically begins with a gateway drug, typically tobacco products and drug, typically tobacco products and alcohol.alcohol.
2
Multi-Disciplinary Approach to Treatment
• Detoxification/Medically Supervised Withdrawal– Uses a drug with a long half-life and low abuse potential– Uses a drug that is smoothly eliminated– Replaces abused drug with detox drub– Initiates drug free treatment– Taper the detox drug
• Maintenance Therapy– Prevents withdrawal– Diminishes drug craving– Blocks or attenuates the effects of heroin and other abused opiates– Increases retention rates in treatment– Is not a cure but allows participation in rehabilitation – Drugs include methadone, naltrexone, and buprenorphine
• Counseling – Establishing a Foundation of Recovery– Remember, you are not just treating one person

• Patient perspective, Descriptive model, personal narratives
• Biological model, Genes, endorphins, and mu opioid receptors
• Psychological model Psychoanalytic model Conditioned response model
Perspectives on AddictionPerspectives on Addiction

• Suffering is at the heart of addictive disorders
• Addiction is not about pleasure (reward) seeking, self-destructiveness, or oral dependency.
• Addicts have deficits in self-care. They struggle regulating emotions, self-esteem, relationships, and behaviors and they self-medicate distress and pain related to these difficulties.
Psychoanalytic Model: Deficits in Self-CarePsychoanalytic Model: Deficits in Self-Care

•Addicts receive poor care in the medical/psychiatric system (although it is getting better) because doctors/nurses are more afraid of being ‘conned’ than helping the patient.
•In the criminal justice system ignorance translates into abuse with the totally disproven notion that abuse serves deters drug use. In fact, it merely promotes drug use.
•This is a life threatening illness, i.e. accidental and deliberate overdoses, as well as neglect of other serious conditions.
Consequences of IgnoranceConsequences of Ignorance
• Is it primarily bad behavior?
• Is it primarily genetic or is a developmental disorder related to childhood abuse or neglect such that all it takes is exposure to a vicodin to ‘normalize endorphin function’ and trigger addiction?
• Is it primarily self-medication attempts to control mental illness, anxiety, depression, bi-polar?
The Etiology of AddictionThe Etiology of Addiction
• The drug as neuro-transmitter or hormone which becomes part of transmission system, e.g. endorphin system
• Chronic administration of opiates, legal or illegal, inhibits the production of both endorphin and mu-opioid receptors. It changes the chemistry and structure of the brain.
• Anxiety is the most devastating symptom of opiate withdrawal.
Biological ModelBiological Model

• No treatment works, in more than a random way which does not deal with the biology of withdrawal.
• Leave the patient in withdrawal they will relapse or worse
The Categorical Imperative of Opiate The Categorical Imperative of Opiate DependenceDependence

• Both are long acting, compared to opiates of abuse, and can be given once a day
• Neither cause an acute euphoria like short acting opiates and so are not normally opiates of abuse.
• Both are effective treatments of opiate addiction
• Both are effective treatments of chronic pain
• Both are opiates and have a similar withdrawal if abruptly stopped
What Are the Similarities Between Methadone What Are the Similarities Between Methadone
and Buprenorphine?and Buprenorphine?

• Methadone is a pure opiate agonist.
• Buprenorphine is a mixed opiate with significant antagonist effects if given to people already on other opiates, i.e. it can cause an acute severe opiate withdrawal state, like narcan
• Buprenorphine is also a partial opiate, activating the opiate receptor to a lesser degree than methadone (at least at higher doses)
What Are the Physiological Differences What Are the Physiological Differences
Between Methadone and BuprenorphineBetween Methadone and Buprenorphine

• Common misperception• Addiction is misuse and unless the patient is abusing
methadone or bup, this analogy is wrong• Trading dependence on short acting opiates for
dependence on long acting opiates is accurate. This allows for brain stability and a return to endorphin homeostasis.
Trading One Addiction for Another??Trading One Addiction for Another??
Considerations for Treatment Options
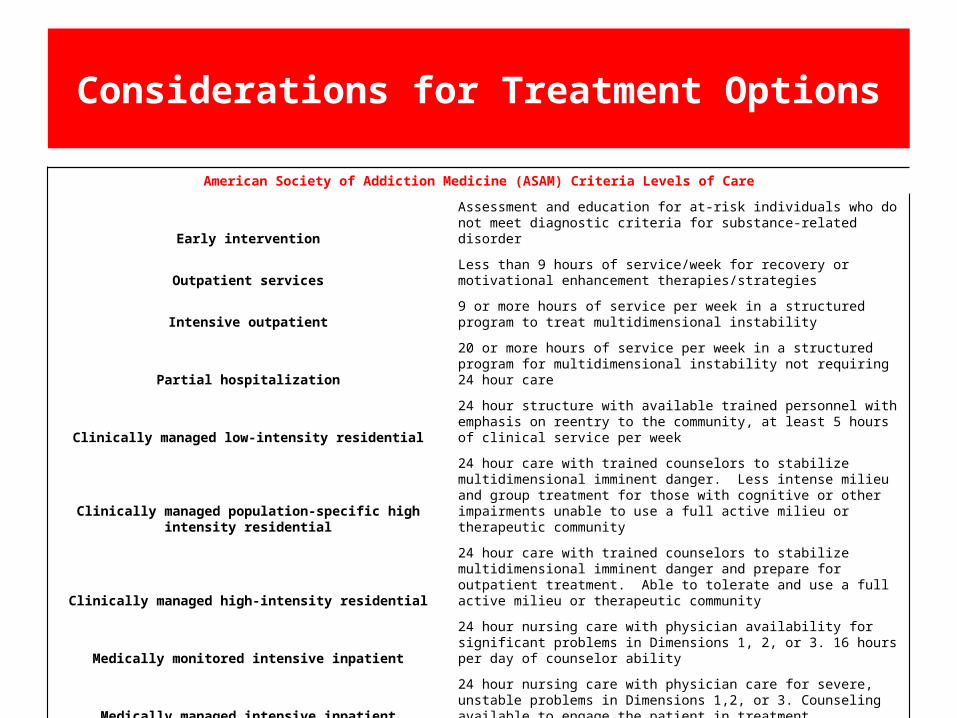
American Society of Addiction Medicine (ASAM) Criteria Levels of Care
Early interventionAssessment and education for at-risk individuals who do not meet diagnostic criteria for substance-related disorder
Outpatient servicesLess than 9 hours of service/week for recovery or motivational enhancement therapies/strategies
Intensive outpatient9 or more hours of service per week in a structured program to treat multidimensional instability
Partial hospitalization20 or more hours of service per week in a structured program for multidimensional instability not requiring 24 hour care
Clinically managed low-intensity residential24 hour structure with available trained personnel with emphasis on reentry to the community, at least 5 hours of clinical service per week
Clinically managed population-specific high intensity residential
24 hour care with trained counselors to stabilize multidimensional imminent danger. Less intense milieu and group treatment for those with cognitive or other impairments unable to use a full active milieu or therapeutic community
Clinically managed high-intensity residential
24 hour care with trained counselors to stabilize multidimensional imminent danger and prepare for outpatient treatment. Able to tolerate and use a full active milieu or therapeutic community
Medically monitored intensive inpatient24 hour nursing care with physician availability for significant problems in Dimensions 1, 2, or 3. 16 hours per day of counselor ability
Medically managed intensive inpatient
24 hour nursing care with physician care for severe, unstable problems in Dimensions 1,2, or 3. Counseling available to engage the patient in treatment
Opioid treatment program
Daily or several times weekly opioid medication and counseling abailable to maintain multidimensional stability for those with opioid use disorder
Considerations for Treatment Options
• ASAM talks about two different levels (ASAM Level 1 and ASAM level 2) and understanding the type of person who falls into those categories is important to determining the "how and what" treatment options would be appropriate.
• ASAM Level 1 is a more counseling focused approach where someone is a walk in patient who registers for 9 hours of face-time that educates them about their disease, talks about the physiological and psychological aspects of the disease, and how the effects can impacts them socially. It can also include medical discussions (translation: alcohol consumption contributes to diabetes) The group in this category are typically employed and function with a high level of self structure.
• ASAM level 2 patients fall into intensive outpatient (IOP) needs. It is a more intensive program requiring 19 hours of counseling and potentially medications. The primary difference with ASAM Level 1? People here are usually unemployed, require more structure, have a high level of recidivism and present with concomitant disorders - complicated social issues that require intensive work to understand what it is that is causing the behavior and require a lot of work to make their lives manageable.
• Comparatively, IOP has a very specific program structure and design. The list provided in a recent DHCS draft waiver document is very accurate; however, there is a range of subsets for most of the components described. While intake and the needs assessment that begin the process is fairly universal, it gets fuzzy after that. IOP services can be based on whether you want physical health, psychological health, or social well being to be addressed. Do you want a "low intensity" IOP (LIOP) for example? And counseling is also broad, where group counseling can have a "recovery" focus, or with a "family" family focus for example.
• In sum, FQHCs can do IOPs but it boils down to the business model an FQHC wants to design. It's about defining how broad a scope the provider is both willing and able to fund. What kind of staff do you want to employ and what is the cost? What kind of licensing will you require, especially if you are a medication assisted treatment facility, and the type and the volume of clientele that would be coming through your doors. You can opt for a bare minimum or a program that is highly matrixed and comprehensive, but you must then think through what the operational/clinical/financial costs would be for the design and subsequently whether you can secure a patient mix and payor reimbursement rate that will make the model financially feasible and sustainable.

A. Counselor Process:
– Assess patient for appropriateness of treatment-entails gathering using and treatment history to ensure patient is physically dependent on opioids
– Patient to breathalyzer– Consent for information to any prior treatment center– Complete intake packet on computer and print– Preliminary screening and check list-enter dates of prior treatment and state criteria– Sign up on medical board– Legal documents- HIPPA for– Authorization for use of protected health in formation– Acknowledgement of receipt of materials– Initial needs assessment and treatment plan– Consent packet done– Cal-OMS completed– Patient to front desk for UA and medical paperwork– Admissions data collection assessment– Fee assessment– Case note that details pertinent information gathered during intake– Assemble file and submit
Operational Anatomy of an Intake Process

Operational Anatomy of an Intake Process
B. Medical Process– Blood is drawn for basic panel which included rpr, blood also drawn for HIV test (paid for by
DPH)– PPD is applied– Medical history and physical exam is conducted– Urine collected for tox screen– Urine collected for other analysis– When indicated/needed may dip urine for immediate drug screen results– EKG may be conducted if indicated
C. Intake– H0001 Substance Use Assessment (1 Unit = 15 minutes) – 80053 Comprehensive Metabolic – 81001 Urinalysis – 85025 CBC with differential – 86592 STS (RPR) – 99203 Physical Examination (25 minutes) – H0020 Methadone Dosing (1 Unit = 1 Dose) – H0004 Individual Counseling (1 Unit= 15 minutes) Meth Panel Toxicology

HCPCS Codes Description Billing Unit Rate Per Unit
H0014-UA 21-day detox program, first 7 days per dose X
H0014-UB 21-day detox program, days 8-21 or all 21 days if recently seen per dose X
H0014-UC 21-day detox program, days 8-21, re-exam per dose X
H0001 Alcohol and Drug assessment 15 minutes X
H0020 Methadone Dosing per dose X
H0004 Individual Counseling 15 minutes X
H0004-HQ Group Counseling 15 minutes X
T1016 Case Management 15 minutes X
CPT Codes (LCSW, Psychologist)
90791 Psychiatric Evaluation
90792 Psychiatric Evaluation with medical services
90832 Individual Counseling 16-37 minutes
90834 Individual Counseling 38-52 minutes
90837 Individual Counseling 52+ minutes
90853 Group Counseling per event
Operational Anatomy of an Intake Process

Managed Care and Network Adequacy
• Network adequacy refers to a health plan’s ability to deliver the benefits promised by providing reasonable access to a sufficient number of in-network primary care and specialty physicians, as well as all and other health care services included under the terms of the contract. Taken together with the Essential Health Benefits (EHB) package, now required as a benefit level floor under the Affordable Care Act (ACA), network adequacy standards will determine what care is covered and how easily it can be obtained.
• States have taken different approaches in regulating the adequacy of health plan networks. The variation is due, in part, to the need for states to maintain robust health insurance markets by balancing access needs with the goals of controlling costs and attracting a healthy number of insurers. In many states, network adequacy requirements have historically applied only to Health Maintenance Organizations (HMOs), and not to other managed-care products such as Preferred Provider Organizations (PPOs). Because PPO products offer reimbursement for services obtained from both in-network and out-of-network providers, they present additional considerations and challenges.
• There are discrepancies that can arise with varying network adequacy standards and states have flexibility to resolve such issues individually.
Bridge to Reform Section 1115 Medicaid Demonstration Waiver
• Section 1115 of the Social Security Act gives the Secretary of Health and Human Services authority to waive provisions of major health and welfare programs authorized under the Act, including certain requirements of Medicaid Section 1115 also authorizes the Secretary to allow states to use federal Medicaid funds in ways that are not otherwise allowed under federal rules. In both cases, the Secretary must determine that the initiative is an “experimental, pilot, or demonstration project” that “is likely to assist in promoting the objectives of” the Medicaid program.
• The Bridge to Reform Medicaid Demonstration Waiver was approved in 2010 and made approximately $8 billion in federal Medicaid matching funds available to California over 5 year period to expand coverage to low income uninsured adults and preserve and improve the county based safety net. It allowed for the state to enroll Medicaid eligible seniors and persons with disabilities in managed care plans that meet specific readiness criteria
• Since 1994, California has developed what is arguably the most robust system of opiate treatment programs in the Country. There are currently approximately 145 licensed programs spanning much of the state providing timely access to major population centers and stretching into many suburban and rural areas such that a vast majority of patients live within 10 miles of an OTP
• The passage of legislation in 1997 establishing an evidence based FFS reimbursement system resulted in improved patient outcomes. Specifically the current system pays for two distinct units of service, medication administration and counseling services, each of which are empirically proven to result in the best possible patient outcomes and ensure efficiency and cost effectiveness.
• Rigorous multi-level oversight ensures program integrity. OTPs are regularly evaluated by county, state, federal and accreditation entities to ensure compliance in fiscal, operations, quality of care, medication oversight, and facility safety.
SUD and Primary Care Integration
SBIRT, Treatment, and Servics
Highly Concentrated Newly Highly Concentrated Newly insured and Medi-Cal patientsinsured and Medi-Cal patients
Fragmented Provider, Hospital, Payor Fragmented Provider, Hospital, Payor MarketMarket
QUESTIONS?
Dr. Jack McCarthy, BAART Bi-Valley Medical Clinic Dr. Jack McCarthy, BAART Bi-Valley Medical Clinic Valerie Yv. Woolsey, Director, Health Care Reform StrategyValerie Yv. Woolsey, Director, Health Care Reform Strategy
BAART ProgramsBAART Programs1111 Market Street 4th Floor San Francisco, CA 941031111 Market Street 4th Floor San Francisco, CA 94103
Phone: 415-552-7914 (San Francisco)Phone: 415-552-7914 (San Francisco)Phone: Phone: 916-974-8090 (Bi Valley/Sacramento)916-974-8090 (Bi Valley/Sacramento)





















![1010 woolsey[1]](https://img.pdfslide.us/doc/110x75/55a27ed71a28ab15408b465e/1010-woolsey1.jpg)







