Embed Size (px)
Citation preview

Clinical Therapeutics/Volume 32, Number 3, 2010
March 2010 527
Accepted for publication January 12, 2010.doi: 10.1016/j.clinthera.2010.03.0100149-2918/$ - see front matter
© 2010 Excerpta Medica Inc. All rights reserved.
ABSTRACTBackground: Tumor lysis syndrome (TLS) is a
group of life-threatening metabolic complications that can occur after initiation of cancer chemotherapy. On-set of TLS in the middle of chemotherapy, however, has not been reported previously in patients with he-matologic malignancies.
Objective: We report a case of a patient who expe-rienced TLS of super-acute onset accompanied by hy-percytokinemia during chemotherapy treatment with a combination of doxorubicin (Adriamycin), bleomy-cin, vinblastine, and dacarbazine (ABVD).
Case summary: A 36-year-old Japanese man (height, 182 cm; weight, 83 kg; body surface area, 2.04 m2) was admitted to the hospital for the treatment of malignant lymphoma (clinical stage IVB Hodgkin’s lymphoma). Chemotherapy was initiated using the ABVD regi-men (doxorubicin [Adriamycin] 25 mg/m2 by 30-minute infusion, bleomycin 9 mg/m2 by 30-minute infusion, vinblastine 6 mg/m2 by bolus injection, and dacarba-zine 375 mg/m2 by 2-hour infusion). During the dacar-bazine infusion, the patient’s body temperature rose from 36.5°C to 42°C; he experienced a convulsion and then lost consciousness. The convulsion was not sup-pressed despite the use of diazepam (5 mg IV twice) and phenytoin (500 mg IV). The patient was then transferred to the intensive care unit and sedated us-ing a continuous infusion of midazolam (10 mg/h).Levels of serum lactate dehydrogenase, aspartate ami-notransferase, uric acid, blood urea nitrogen, and creatinine evaluated shortly after the ABVD regimen were outside normal limits. In addition, interleukin-6
(IL-6) concentrations were elevated to 54,220 pg/mL. Continuous hemodiafiltration was immediately per-formed to lower the elevated levels of IL-6. The next day, IL-6 concentrations decreased to 97 pg/mL, and the patient was weaned from ventilator support and sedation. The patient had no adverse effects after the event. According to the results of an assessment using the Naranjo adverse drug reaction probability scale (score = 3), the development of TLS in this patient was possibly related to the chemotherapy regimen.
Conclusions: ABVD chemotherapy was possibly associated with the super-acute onset of TLS in this patient. In addition, hypercytokinemia occurred with TLS, which led to pyrexia, convulsion, and loss of consciousness. (Clin Ther. 2010;32:527–531) © 2010 Excerpta Medica Inc.
Key words: tumor lysis syndrome, acute, lymphoma, hypercytokinemia.
INTRODUCTIONTumor lysis syndrome (TLS) is a group of life-threatening metabolic complications that can occur after initiation of cancer chemotherapy.1 Acute TLS frequently compli-cates the clinical course of lymphoproliferative malig-nancies.2–4 One of the most important factors in the pathogenesis of acute TLS is rapid cell lysis, which over-
Case Report
Super-Acute Onset of Tumor Lysis Syndrome Accompanied by Hypercytokinemia During Treatment of Hodgkin’s Lymphoma With ABVD Chemotherapy
Takaaki Suzuki, MS1; Masahiro Takeuchi, MD, PhD2; Hiromi Saeki, MS1; Shingo Yamazaki, MS1; Hitomi Koga, MS1; Daijiro Abe, MD, PhD2; Miki Nishimura, MD, PhD2; Chiaki Nakaseko, MD, PhD2; Hiromitsu Nakasa, PhD1; Hiroyoshi Nakamura, PhD1; Noritaka Ariyoshi, PhD1; and Mitsukazu Kitada, PhD1
1Division of Pharmacy, Chiba University Hospital, Chiba, Japan; and 2Division of Hematology, Department of Clinical Cell Biology, Chiba University Graduate School of Medicine, Chiba, Japan

528 Volume 32 Number 3
Clinical Therapeutics
ported information regarding the acute onset of TLS. The objective of the present report was to describe a patient who experienced TLS of super-acute onset ac-companied by hypercytokinemia during treatment with ABVD chemotherapy. Informed consent was ob-tained from the patient. Approval from an institu-tional review board was not required by the Chiba University Graduate School of Medicine (Chiba, Ja-pan) for this case report.
CASE SUMMARYA 36-year-old Japanese man (height, 182 cm; weight, 83 kg; body surface area, 2.04 m2) was admitted to the hospital for the treatment of malignant lympho-ma. The patient had a history of reflux esophagitis, but no significant family history for appreciable dis-ease. He neither smoked nor drank, and his renal and hepatic functions were within normal range before treatment. No medication, over-the-counter drug, herbal product, or dietary supplement was taken at admission to the hospital or at initiation of chemo-therapy. A diagnosis of HL (clinical stage IVB) was made by confirmation of lymph node biopsy results, bone marrow aspiration, and immunohistologic stain-ing. The major lesion was in the neck region. Seven enlarged lymph nodes, elliptical in shape (maximum size: 25 mm [major axis] × 18 mm [minor axis]), were observed. Enlarged para-aortic lymph nodes and bone marrow infiltration were also observed.
Chemotherapy was initiated using the ABVD regi-men (doxorubicin [Adriamycin] 25 mg/m2 by 30-minute infusion, bleomycin 9 mg/m2 by 30-minute infusion, vinblastine 6 mg/m2 by bolus injection, and dacarba-zine 375 mg/m2 by 2-hour infusion). An indwelling infusion catheter was inserted into the left median cubital vein. Thirty minutes before administration of the chemotherapeutic agents, 4 mg IV of ondansetron was administered for the prevention of nausea. Doxo-rubicin, vinblastine, and bleomycin were administered with no adverse effects. Approximately 10 minutes af-ter initiation of the dacarbazine infusion (~100 mg had been infused), the patient complained of slight pain at the infusion site. His body temperature then rose from 36.5°C to 42°C; he began shivering and then became unconscious, with a drop in systolic blood pressure (from 148 to <80 mm Hg). Anaphylac-tic shock due to dacarbazine was initially suspected, and 200 mg IV of hydrocortisone was administered twice after the dacarbazine infusion was discontinued,
whelms normal renal excretory and cellular-buffering mechanisms; this leads to elevation of serum concen-trations of nuclear metabolites. TLS is characterized by hyperuricemia, hypocalcemia, hyperphosphatemia, and hyperkalemia, which may be associated with tet-any, renal failure, seizures, cardiac arrhythmias, and sudden death.1 Hydration and diuresis are fundamen-tal to the prevention and management of TLS. Ac-cording to a panel of experts in pediatric and adult hematologic malignancies and TLS, the use of sodium bicarbonate to alkalinize the urine has been recom-mended as part of TLS prevention and management strategies (eg, when using allopurinol).1 Allopurinol decreases the formation of uric acid and reduces the incidence of obstructive uropathy caused by uric acid precipitation in patients at risk for developing TLS. Recombinant urate oxidase (rasburicase) should also be considered for patients at high risk for developing hyperuricemia. For severe renal failure, renal replace-ment therapy has been used.
It was recently reported that TLS may be accompa-nied by hypercytokinemia in some cases.5 Hypercyto-kinemia, which induces an excessive inflammatory response, can be triggered by various critical illnesses (eg, sepsis, trauma) and cancer chemotherapy (especially in the treatment of hematologic malignancies).6,7
Hodgkin’s lymphoma (HL), which accounts for <10% of all malignant lymphomas in Japan and is re-ported to produce various types of cytokines,8–10 is considered one of the most curable forms of cancer in adults.11 Treatment of HL has progressed with the development of chemotherapeutic regimens over the last several decades.12–14 The combination of doxoru-bicin (Adriamycin), bleomycin, vinblastine, and dacar-bazine (ABVD) is the standard treatment regimen for early-stage and advanced HL. Satisfactory complete remission rates of up to ~80% using ABVD chemo-therapy, with or without radiation, have been reported in prospective multicenter trials. ABVD chemotherapy–related toxicities, especially with regard to hematopoi-etic stem cell toxicity and infertility, were tolerable.13
Life-threatening toxicities—such as pulmonary fibrosis caused by bleomycin, cardiomyopathy caused by doxo-rubicin, and secondary malignancies—may occur, how-ever. In addition, TLS has been reported as one of the serious adverse reactions in the treatment of HL.2
A brief literature search was conducted of MEDLINE (years: 1980–June 2009) using the terms acute, tumor, lysis, and syndrome to identify any previously re-
March 2010 529
T. Suzuki et al.
patible with those of acute TLS. In addition, concen-trations of interleukin (IL)-6 were markedly elevated from baseline (38 to 54,220 pg/mL [normal concen-tration, <4 pg/mL]). Continuous hemodiafiltration (CHDF) was then performed to lower the elevated IL-6 concentrations. A polymethylmethacrylate (PMMA) membrane hemofilter was placed in the blood circuit to adsorb cytokines in the circulating blood. Condi-tions for the PMMA-CHDF system were as follows: blood flow rate, 80 to 120 mL/min; dialysate flow rate, 500 to 1000 mL/h; and filtration rate, 300 to 500 mL/h. IL-6 concentrations decreased to 97 pg/mL the next day, and the patient was weaned from venti-lator support and sedation. The patient had no ad-verse effects after the event.
The infusion had been prepared by 2 pharmacists. The fluid of dacarbazine and the used formulations were saved separately. After the event occurred, the number of vials and dosage of the prepared dacarba-zine were checked, thus ruling out medication error.
but the symptoms continued to worsen. Tonic convul-sion occurred shortly after the hydrocortisone injection, and the patient was administered 5 mg IV of diaze-pam twice and 500 mg IV of phenytoin for suppression of convulsion by acute saturation of the blood pheny-toin concentration; the convulsion was not suppressed, however. The patient was then transferred to the in-tensive care unit (ICU) and underwent sedation with midazolam continuous infusion (10 mg/h) to suppress the status convulsion. Results of a computed tomog-raphy scan revealed no obvious cerebral hemorrhage.
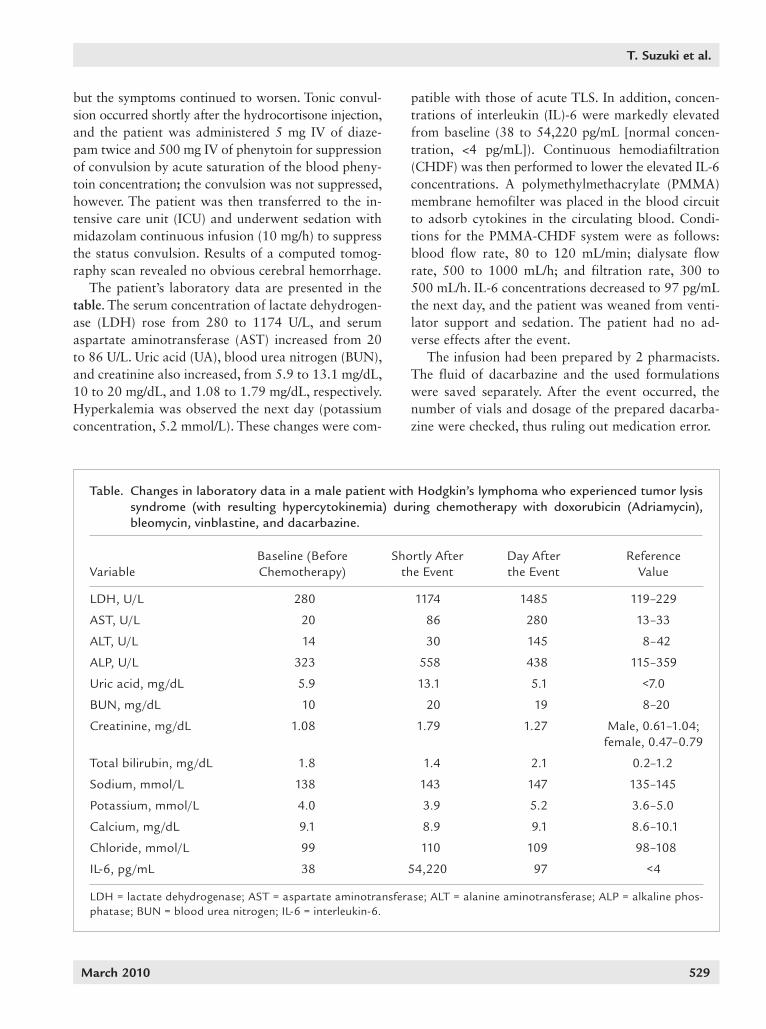
The patient’s laboratory data are presented in the table. The serum concentration of lactate dehydrogen-ase (LDH) rose from 280 to 1174 U/L, and serum aspartate aminotransferase (AST) increased from 20 to 86 U/L. Uric acid (UA), blood urea nitrogen (BUN), and creatinine also increased, from 5.9 to 13.1 mg/dL, 10 to 20 mg/dL, and 1.08 to 1.79 mg/dL, respectively. Hyperkalemia was observed the next day (potassium concentration, 5.2 mmol/L). These changes were com-
Table. Changes in laboratory data in a male patient with Hodgkin’s lymphoma who experienced tumor lysis syndrome (with resulting hypercytokinemia) during chemotherapy with doxorubicin (Adriamycin), bleomycin, vinblastine, and dacarbazine.
VariableBaseline (Before Chemotherapy)
Shortly After the Event
Day After the Event
Reference Value
LDH, U/L 280 1174 1485 119–229
AST, U/L 20 86 280 13–33
ALT, U/L 14 30 145 8–42
ALP, U/L 323 558 438 115–359
Uric acid, mg/dL 5.9 13.1 5.1 <7.0
BUN, mg/dL 10 20 19 8–20
Creatinine, mg/dL 1.08 1.79 1.27 Male, 0.61–1.04; female, 0.47–0.79
Total bilirubin, mg/dL 1.8 1.4 2.1 0.2–1.2
Sodium, mmol/L 138 143 147 135–145
Potassium, mmol/L 4.0 3.9 5.2 3.6–5.0
Calcium, mg/dL 9.1 8.9 9.1 8.6–10.1
Chloride, mmol/L 99 110 109 98–108
IL-6, pg/mL 38 54,220 97 <4
LDH = lactate dehydrogenase; AST = aspartate aminotransferase; ALT = alanine aminotransferase; ALP = alkaline phos-phatase; BUN = blood urea nitrogen; IL-6 = interleukin-6.

530 Volume 32 Number 3
Clinical Therapeutics
condition (pyrexia, convulsion, and loss of conscious-ness) improved.
According to results of an assessment using the Naranjo adverse drug reaction probability scale (score = 3), the development of TLS in this patient was possi-bly related to the chemotherapy regimen.
With respect to anaphylaxis that was suspected at the event onset, an allergic mechanism was unlikely in this case because the patient received 7 more rounds of ABVD chemotherapy after this event without expe-riencing the same adverse reaction.
CONCLUSIONSABVD chemotherapy may possibly have been associated with the super-acute onset of TLS in this patient. In ad-dition, hypercytokinemia occurred with TLS, which led to pyrexia, convulsion, and loss of consciousness.
ACKNOWLEDGMENTSThe authors received no funding for this report.
The authors thank the ICU staff of Chiba Univer-sity Hospital for their assistance in performing CHDF. They also thank the nursing staff of the hematology ward for their cooperation.
The authors have indicated that they have no con-flicts of interest regarding the content of this article.
REFERENCES1. Coiffier B, Altman A, Pui CH, et al. Guidelines for the man-
agement of pediatric and adult tumor lysis syndrome: An evidence-based review [published correction appears in J Clin Oncol. 2010;28:708]. J Clin Oncol. 2008;26:2767–2778.
2. Mahajan A, Nirmal S, English MW, et al. Acute tumor lysis syndrome in Hodgkin disease. Med Pediatr Oncol. 2002;39:69–70.
3. Karagiannis A, Tsorlalis I, Kakafika A, et al. Acute renal failure due to tumor lysis syndrome in a patient with non-Hodgkin’s lymphoma. Ann Hematol. 2005;84:343–346.
4. Castro MP, VanAuken J, Spencer-Cisek P, et al. Acute tu-mor lysis syndrome associated with concurrent bio-chemotherapy of metastatic melanoma: A case report and review of the literature. Cancer. 1999;85:1055–1059.
5. Nakamura M, Oda S, Sadahiro T, et al. The role of hyper-cytokinemia in the pathophysiology of tumor lysis syn-drome (TLS) and the treatment with continuous hemo-diafiltration using a polymethylmethacrylate membrane hemofilter (PMMA-CHDF). Transfus Apher Sci. 2009;40:41– 47.
6. Annane D, Bellissant E, Cavaillon JM. Septic shock. Lancet. 2005;365:63–78.
DISCUSSIONAcute TLS has been reported previously in a pediatric patient with HL.2 Fifty hours after initiation of chemo-therapy consisting of vincristine (1.5 mg/m2) and pred-nisolone (40 mg/m2), creatinine and potassium concen-trations were increased to 2.2 mg/dL and 6.3 mg/dL, respectively. In our case, in addition to the increases in LDH, AST, UA, BUN, and creatinine concentrations, IL-6 concentrations were elevated.
Two major factors in the present case make it dis-tinct from other TLS cases reported thus far. One is onset time. TLS usually develops in a few days (1 day at the earliest) after the initiation of chemotherapy.2–4
Because there have been no previously reported cases of acute onset of TLS or massive cytokine release dur-ing the infusion, this was an unusual event and was thus unpredictable despite the staff’s experience with chemotherapy regimens. The other relevant factor was the presence of elevated concentrations of IL-6 as a biomarker of hypercytokinemia.15 IL-6 is a pleiotrop-ic cytokine capable of regulating proliferation, differ-entiation, and activity in a variety of cell types. IL-6 may also play a role in the development and progres-sion of cancer. IL-6 reportedly regulates chronic in-flammation, which can create a cellular microenviron-ment beneficial to cancer growth.15 It is also reported to be a growth factor for lymphatic, renal, bladder, and colorectal cancer cells and is involved in the con-trol of cell proliferation and apoptosis. Expression of IL-6, IL-7, and their receptors is a common feature of HL.8,16 In addition, the growth of HL cells is regulated by cytokines and cell contact–mediated interactions among HL cells and nonneoplastic reactive cells accu-mulating in HL-involved tissues. Stimulation of IL-6 from HL cells and fibroblasts in HL-involved lymph nodes by autocrine or paracrine stimulus of IL-7 can occur, resulting in elevated serum IL-6 concentra-tions.17 Concurrent and massive release of IL-6 from HL cells and the reactive cells might be attributable to HL cell lysis caused by chemotherapy. In the present case, the marked hypercytokinemia may have caused the pyrexia and convulsion that led to the patient’s critical and life-threatening clinical condition. The el-evated cytokine levels were decreased after CHDF. Based on a recent observational study, CHDF for cy-tokine removal in patients with hypercytokinemia has been performed even in cases without renal failure.5
The IL-6 level of 54,220 pg/mL was reduced to 97 pg/mL the day after CHDF was conducted, and our patient’s
March 2010 531
T. Suzuki et al.
17. Cattaruzza L, Gloghini A, Olivo K, et al. Functional coexpression of inter-leukin (IL)-7 and its receptor (IL-7R) on Hodgkin and Reed-Sternberg cells: Involvement of IL-7 in tumor cell growth and microenvironmental in-teractions of Hodgkin’s lymphoma. Int J Cancer. 2009;125:1092–1101.
(IL-6) and cancer. Eur J Cancer. 2008; 44:937–945.
16. Seymour JF, Talpaz M, Hagemeister FB, et al. Clinical correlates of ele-vated serum levels of interleukin 6 in patients with untreated Hodgkin’s disease. Am J Med. 1997;102:21– 28.
7. Lenz A, Franklin GA, Cheadle WG. Systemic inflammation after trau-ma. Injury. 2007;38:1336–1345.
8. Jücker M, Abts H, Li W, et al. Ex-pression of interleukin-6 and inter-leukin-6 receptor in Hodgkin’s dis-ease. Blood. 1991;77:2413–2418.
9. Klein S, Jücker M, Diehl V, Tesch H. Production of multiple cytokines by Hodgkin’s disease derived cell lines. Hematol Oncol. 1992;10:319–329.
10. Hsu SM, Xie SS, Hsu PL, Waldron JA Jr. Interleukin-6, but not interleukin- 4, is expressed by Reed-Sternberg cells in Hodgkin’s disease with or without histologic features of Cas-tleman’s disease. Am J Pathol. 1992; 141:129–138.
11. Diehl V, Stein H, Hummel M, et al. Hodgkin’s lymphoma: Biology and treatment strategies for primary, refractory, and relapsed disease. Hematology Am Soc Hematol Educ Pro-gram. 2003:225–247.
12. Duggan DB, Petroni GR, Johnson JL, et al. Randomized comparison of ABVD and MOPP/ABV hybrid for the treatment of advanced Hodg-kin’s disease: Report of an inter-group trial. J Clin Oncol. 2003;21: 607–614.
13. Bonadonna G, Zucali R, Monfar- dini S, et al. Combination chemo-therapy of Hodgkin’s disease with adriamycin, bleomycin, vinblastine, and imidazole carboxamide versus MOPP. Cancer. 1975;36:252–259.
14. Meyer RM, Gospodarowicz MK, Connors JM, et al, for the National Cancer Institute of Canada Clinical Trials Group, Eastern Cooperative Oncology Group. Randomized comparison of ABVD chemotherapy with a strategy that includes radia-tion therapy in patients with limited- stage Hodgkin’s lymphoma: Na-tional Cancer Institute of Canada Clinical Trials Group and the East-ern Cooperative Oncology Group. J Clin Oncol. 2005;23:4634–4642.
15. Heikkilä K, Ebrahim S, Lawlor DA. Systematic review of the association between circulating interleukin-6
Address correspondence to: Takaaki Suzuki, MS, Division of Pharmacy, Chiba University Hospital, 1-8-1 Inohana, Chuo-ku, Chiba 260-8677, Japan. E-mail: [email protected]